Embed Size (px)
Citation preview

To investigate the nature of the inflammatory response in facioscapu- lohumeral muscular dystrophy (FSHD), we analyzed mononuclear cells in muscle sections obtained from 18 FSHD patients and 8 controls. Monoclonal antibodies reactive for T cells, T cell subsets, B cells, and NK cells were used for cell typing. Macrophages were identified by acid phosphatase reaction. The localization of perforin, granzyme A, MHC-I and -11, dystrophin, and a-actinin antigens was also examined. We found that all FSHD patients, both familiar and sporadic cases, had greater amounts of mononuclear cellular infiltrates in muscle than con- trols, in whose specimens only few extra vascular mononuclear cells were counted. Seventy-two percent (13 of 18) of the patients had more than 50 inflammatory mononuclear cells per 1000 muscle fibers, and 33% (6 of 18) patients had numerous inflammatory cells exceeding 600 per 1000 muscle fibers (1835 & 482 SE). Nonnecrotic fibers invaded by mononuclear cells with either T8+, perforin+, or granzyme A + were not observed in FSHD, while a few degenerating fibers were superficially invaded by T cells and macrophages. Occasional T cells were observed moving through the blood vessel wall. The increased number of ne- crotic fibers was paralleled by an increased number of inflammatory cells ( r = 0.783, P = 0.0001). Genetic analysis, using the probes p13E- 11, pFR-1, D4S139, and D4S163, was done in 6 patients (3 familiar, 3 sporadic) who had numerous inflammatory infiltrates. These 6 patients had small (<28 kb) EcoRl fragments associated with the disease, and the disease was linked to 4q35. These results suggest that, in chromo- some b l inked FSHD: (1) inflammatory changes in muscle are a com- mon histological feature; (2) mononuclear cellular infiltrates may en- hance muscle fiber damage; but (3) T-cell-mediated cytotoxicity directed against muscle fibers is unlikely. We speculate that the im- mune effector mechanism in FSHD is different from that in previously reported inflammatory myopathies and Duchenne muscular dystrophy. 0 1995 John Wiley & Sons, Inc. Key words: facioscapulohumeral muscular dystrophy inflammatory response lymphocyte subsets genetic diagnosis
MUSCLE & NERVE Suppl2:S56-S66 1995
INFLAMMATORY RESPONSE IN FACIOSCAPULOHUMERAL MUSCULAR DYSTROPHY (FSHD): IMMUNOCYTOCHEMICAL AND GENETIC ANALYSES
KllCHl ARAHATA, MD, TADAYUKI ISHIHARA, MD, HlDETOSHl FUKUNAGA, MD, SATOSHI ORIMO, MD, JE HYEON LEE, PhD, KANAKO GOTO, BS, and IKUYA NONAKA, MD
From the National Institute of Neuroscience (NCNP), Tokyo, Japan (Drs Arahata, Orimo, and Lee, Ms Goto, and Dr Nonaka); National Higashi- Saitama Hospital, Saitama, Japan (Dr. Ishihara); National Minami-Kyushu Hospital, Kagoshima, Japan (Dr. Fukunaga); and Kanto Chuo Hospital, Tokyo, Japan (Dr. Orimo).
Welfare, Japan, Grants-in-Aid for Scientific Research (B) and Develop- mental Scientific Research from the Ministry of Education, Science, and Culture, Japan; a research grant from the Uehara Memorial Foundation; and by a research grant from the Muscular Dystrophy Association (USA) (K.A )
Acknowledgments: We thank Dr. Hideo Sugita (President, NCNP, Japan) for his helpful discussion and advice, Drs. ~ u n e R. Frants, cisca wi]. menga, Egben Bakker, and G ~ ~ . J ~ ~ B van Ommen (Department of G ~ . netics Leiden Universitv. Leiden. The Netherlands) and Barbara Weiffen-
Address reprint requests to Dr Kiichi Arahata. MD, Department of Neu- rOmUSCUlar Research, National Institute of Neuroscience, NCNP, 4-1-1 ogawa-higashi' Kodaira, Tokyo ' 8 7 , Japan
bach (Collaborative Research lnc , Waltham, MA) for their very kind technical help, and providing us the plasmids This study was supported by Research Grants 91A1208 and 5A-2 from the Ministry of Health and
CCC 0148-639X/95/S20S56-11 0 1995 John Wiley & Sons Inc
S56 Facioscapulohurneral Muscular Dystrophy MUSCLE & NERVE Supplement 2 1995

Facioscapulohumeral muscular dystrophy (FSHD) is an inherited disease transmitted in an autosomal-dominant f a ~ h i o n . ' ~ , ~ ' ~ ' ~ ~ ~ ~ The dis- ease locus has been mapped to chromosome 4q,28,394',47,48251 although genetic heterogeneity exists in rare fa mi lie^.^^,^^ Both males and females have a 50% chance of inheriting the gene from an affected parent, but the gene may also be defective because of a new m ~ t a t i o n . ' ~ ~ ~ ~ , ~ ~ , ~ ~ A recently identified probe, p13E-11 (D4F104Sl), usually de- tects specific smaller (<28 kb) EcoRI fragments that cosegregate with FSHD'7,27,4','6,49,'2; dele- tions of the tandemly repeated 3.2- (or 3.3) -kb KpnI units (D4Z4) in the EcoRI fragment are
ever, the molecular genetic mechanisms underly- ing the disease are still unclear. The p13E-11 probe has since been mapped to the 4q35-qter re- gion distal to the D4S139 locus (cen-D4S139- D4F35S 1-D4F104S 1-FSHD-tel),4694Y754 and the probe is considered to have immediate diagnostic value for FSHD, although this probe can be used as a tightly linked polymorphic marke~-. '~*~'
Inflammatory changes in muscle are frequently (40-80%) observed in FSHD patients and some- times become very marked.8,9,'2 In 1948, Ogryzlo described a small focal accumulation of lympho- cytes in muscle in a sporadic patient with facio- scapulohumeral atrophy.33 In 1955, Nattrass re- ported an adult patient with severe polymyositis who was initially thought to have sporadic FSHD because of the presence of symmetrical wasting of facial, scapular, and upper-arm muscles3' More than 15 similar patients have since been re-
and the presence of FSH syndrome due to an inflammatory myopathy has been ~ons idered .~ Facial muscle involvement has been reported in about 7-11% of patients diag- nosed with polymyosi t i~."~~~ Massive inflamma- tory cellular infiltration in muscle also occurs in those FSHD patients who have a positive family
In addition, in the first family re- ported by Bacq et aL5 both the affected mother and her daughter had inflammatory changes in muscle, suggesting the possibility that the inflam- matory response in FSHD is intrinsically involved with the disease process. Although some studies have analyzed inflammatory cellular subsets in pa- tients with a clinical diagnosis of FSH myopathy of FSHD,'5x21 genetic analysis has not been accom- plished. We still do not know the relationship be- tween inflammatory infiltrates and dystrophic muscle histology (necrosis, phagocytosis, regener- ation, variation in fiber size, and proliferation of connective tissues), and therefore, the significance
thought to cause the d i ~ e a s e . ~ ~ ~ ' ~ ~ ~ " ~ ' ~ " " . ~ ~ HOW-
ported,7,1 1,19,23,29,38,44,55
of these cellular infiltrates in FSHD muscle re- mains unclear.
We have recently examined a total of 158 Jap- anese individuals that included 18 unrelated FSHD families with 38 affected and 73 healthy family members, as well as 35 Japanese controls, for genetic diagnosis, using the probes p13E-11 and pFR- 1 .I7 In our patient population, the probes detected DNA rearrangements associated with FSHD; i.e., most of the Japanese FSHD patients (97.4%) had specific small (<28 kb) EcoRI frag- ments which cosegregated with the disease, and the disease was linked to chromosome 4q35. In contrast, none of the patients with neurogenic scapuloperoneal muscular atrophy had small EcoRI fragments associated with the disease.
In the present study, we examined subsets of mononuclear cells in the muscles of 18 patients with FSHD and 8 controls, using qualitative and quantitative immunocytochemistry to elucidate the role of the inflammatory response in FSHD. We also accomplished DNA-based genetic analysis of the 6 FSHD patients who had numerous mononu- clear cellular infiltrates in muscle, using the probes p13E-11 and pFR-1.
MATERIALS AND METHODS
Analysis of Mononuclear Cell Subsets in Muscle. Clinical Materials. Limb muscle specimens (ob- tained from biceps bracii) were examined for di- agnostic purposes, after informed consent was ob- tained from the subjects. The muscle specimens were flash frozen in isopentane chilled with liquid nitrogen. Specimens from 18 patients with FSHD [9 familiar, 9 sporadic; 6-62 years old; 29 +- 18 years (SE)] and 8 controls (unrelated, with no known myopathy and no histologic abnormality by ordinary examinations) were studied. The diagno- sis of FSHD was based on the clinical, histological, and electromyographic finding^.^','"^"^^ Nine of the 18 FSHD patients had elevated serum creatine kinase (CK) activity; and the overall mean value was 378 * 65 (SE) U/L (normal 12-280).
The antibodies used in this study were: monoclonal antibodies reactive for T cells, T-cell subsets (T4, TS), B cells, NK cells, MHC-I and -11 antigens, and polyclonal anti- perforin and -granzyme A antigens. The specific- ity of each antibody has been described previous- Iy.2-4,13,34 Monoclonal antibodies for dystrophin (4C5) and a-actinin (AB- 1) were also used in some cases. Affinity-purified fluorescein isothiocyanate (F1TC)-labeled goat F(ab')2 anti-mouse and anti-
Immunoreugents.
Facioscapulohumeral Muscular Dystrophy MUSCLE & NERVE Supplement 2 1995 S57
rabbit IgG were obtained from Tago Inc., and used as the second layer antibodies.
Immunocytochemistry. Four-micron serial cryo- stat sections were thawed on gelatinized cover slips, fixed in 100% ice-cold acetone for 5 min, air-dried for 30 min, soaked in 0.1% Nonidet-P40 for 3 min, and then preincubated with PBS containing 2% BSA and 5% heat-inactivated normal goat serum at pH 7.4. The sections were incubated with primary antibodies for 2 h at 37°C and with sec- ondary antibodies (10 pg/mL) for 1 h at room tem- perature. The sections were mounted in a glycerol- based medium, and observed under a Zeiss Axiophot microscope with epifluorescence. Speci- ficity of the immunostaining was examined by replacement of the primary antibody with con- trol mouse myeloma IgG or preimmune rabbit serum.
Quantitative Analysis of Mononuclear Cells in Mus- cle. For quantitative analysis, a region that con- tained at least 1000 muscle fibers was selected at random in each specimen, and the same region was analyzed in each serial section. We counted all muscle fibers and all reactive cells for each anti- body in the randomly chosen region, and calcu- lated the average cell number per 1000 muscle fi-
bers. The analysis was done according to sites of accumulation, as described.23'"
Genetic Analysis of FSHD Patients with Numerous In. flammatory Infiltrates in Muscle. Probes. The probes used in this study were p13E-11 (0.8-kb in- sert in pBS isolated by SacIIEcoRI double- digestion, kindly provided by Dr. Rune R. Frants) and our own pFR-1 l 7 (1.1-kb fragment isolated by HindIII/HincII double digestion from the 4.9-kb KpnI fragment of the plasmid pSMl kindly sup- plied by Dr. Barbara Weiffenbach). We also used other 4q35 markers (D4S139, D4S163). These probes were labeled with 32P-dCTP for Southern blot analysis, using a Random Primed DNA Label- ing Kit (Boehringer).
Southern Blot Hybridization. Fifteen micro- grams of genomic DNA (isolated from peripheral blood lymphocytes) was digested with the restric- tion enzyme EcoRI at 37°C for 12 h, as recom- mended by the manufacturer's protocol. The DNA was separated on 0.3% HGT agarose gel for 72 h at 15 mA (0.5 V/cm), and was then transferred to H ybond N (Amersham). Hybridization was carried out overnight at 65°C. The filter was thoroughly washed in 1 x SSC/O.l% SDS for 1 h at 60"C, fol-
~ ~~
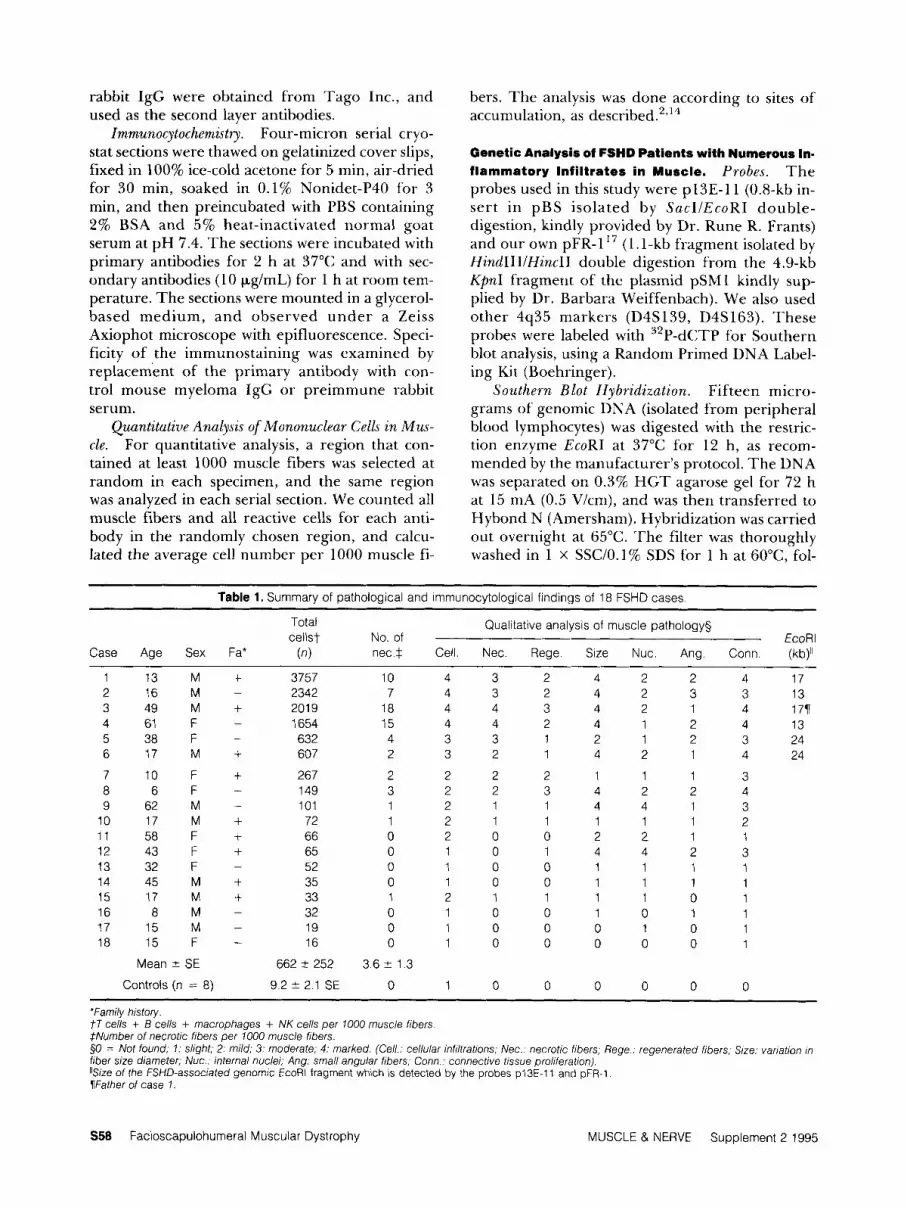
Table 1. Summary of pathological and immunocytological findings of 18 FSHD cases ~ ~~~
Total cellst No of EcoRl
Case Age Sex Fa* (n) nec* Cell Nec Rege Size Nuc Ang Conn (kb)Ii
Qualitative analysis of muscle pathology§
1 13 M + 2 1 6 M - 3 4 9 M + 4 61 F -
5 38 F 6 1 7 M +
7 10 F + 8 6 F - 9 6 2 M -
10 17 M + 11 58 F + 12 43 F + 13 32 F -
14 45 M + 15 17 M +
-
16 a M - 17 15 M - 18 15 F -
Mean 2 SE
Controls (n = 8)
3757 2342 201 9 1654 632 607
267 149 101 72 66 65 52 35 33 32 19 16
662 2 252
9.2 2 2.1 SE
10 4 3 2 4 2 2 7 4 3 2 4 2 3
18 4 4 3 4 2 1 15 4 4 2 4 1 2 4 3 3 1 2 1 2 2 3 2 1 4 2 1
2 2 2 2 1 1 1 3 2 2 3 4 2 2 1 2 1 1 4 4 1 1 2 1 1 1 1 1 0 2 0 0 2 2 1 0 1 0 1 4 4 2 0 1 0 0 1 1 1 0 1 0 0 1 1 1 1 2 1 1 1 1 0 0 1 0 0 1 0 1 0 1 0 0 0 1 0 0 1 0 0 0 0 0
3.6 2 1.3
0 1 0 0 0 0 0
4 17 3 13 4 177 4 13 3 24 4 24
3 4 3 2 1 3 1 1 1 1 1 1
0
*Family history. j 7 cells + B cells + macrophages + NK cells per 1000 muscle fibers. #Number of necrotic fibers per 1000 muscle fibers. 50 = Not found; 1: slight; 2 mild; 3: moderate; 4: marked. (Cell.: cellular infiltrations; Nec.. necrotic fibers, Rege.. regenerated fibers; Slze: vanation In fiber size diameter; Nuc . internal nuclei; Ang: small angular fibers; Conn : connective tissue proliferation). "Size of the FSHD-associated genomic EcoRl fragment which is detected by the probes p13E-11 and pFR-1 Father of case 1.
S58 Facioscapulohumeral Muscular Dystrophy MUSCLE & NERVE Supplement 2 1995

-2 0 2 4 6 8 10 12 14 16 18 20 nec. fibers
FIGURE 1. Positive correlation is shown between the total number of inflammatory cells and the number of necrotic muscle fibers per 1000 muscle fibers in FSHD. ( r = 0.783, P = 0.0001).
lowed by autoradiography for 2 4 h using a BAS 2000 image analyzer, and for 3 days using Konica AX film with an intensifying screen.
RESULTS
inflammatory Infiltrates. A summary of the patho- logical and immunocytochemical findings is shown in Table 1. In control muscles, only a few [9.2 k 2.1 (SE) per 1000 muscle fibers] extravascular mononuclear cells were observed. All 18 patients with FSHD (9 familiar, 9 sporadic) had much higher total numbers of inflammatory mononu- clear cells (T cells + B cells + macrophages + NK cells), with the mean value being 662 k 252 (SE) per 1000 muscle fibers (range 16-3757). Six of
these patients had numerous inflammatory cells, exceeding 600 per 1000 muscle fibers [835 * 482 (SE), range 607-3757]; the remaining 12 patients had small to moderate amounts of inflammatory cells [76 & 21 (SE), range 16-2671. There was no significant difference in total number of the in- flammatory cells between FSHD patients who had a positive family history and those who had no family history (clinically new mutations). Although the average number of necrotic fibers (confirmed by complement C9 and C5b-9 membrane attack complex) per 1000 muscle fibers was low [3.6 ? 1.3 (SE)] in FSHD, this number increased in parallel with the number of the inflammatory cells ( r = 0.783, P = 0.0001) (Table 1, Fig. 1). Chronic dys- trophic changes, characterized by the presence of either regenerated fibers, fiber size variation, in- creased connective tissue elements, or internal nu- clei, were found in all FSHD muscles examined (Table 1).
In the 6 FSHD patients who had numerous cellular infiltrates, B cells were most abundant at perivascular sites, accounting for 25.4 * 5.0% of the total. The T4/T8 ratio at the perivascular site was 1.51 i 0.55, and N K cells were least abundant (Table 2). Macrophages accounted for about one third of all mononuclear cells. At the endomysial site, T cells were most abundant (Table 2), inflam- matory cells were diffusely scattered, and there were no nonnecrotic muscle fibers invaded by mononuclear cells that included T 8 + , perforin+, or granzyme A+ cells. Only a few degenerating
~~ ~
Table 2. Quantitative analysis of mononuclear cells in FSHD
Cell type or marker Perivascular
cells Perirnysial
cells Endomysial
cells
FSHD with numerous (>600 cells per 1000 fibers) cellular infiltrates (n = 6) B cells (B1 +) (%) 8.1 t 5.3t Macrophages (%) 23.6 -+ 12.9 35.6 2 11.1 T cells ( T l l + ) (%) 56.4 2 12.6
T 8 + K cells (%) 46.5 2 11.6 64.5 2 18.7 T 4 + n cells (%) 61.1 2 14.1 42.2 2 14.4 T4+K8+ ratio 1.51 2 0 55* 0.86 2 0.37
B/T ratio 0.52 i 0.14* 0.16 2 0. lOt
25.4 2 5.0*
5 1 . 0 2 11 9
Leu-7+ cells (%) 8.1 2 3.3 11.1 2 4.7
B cells (B1+) (%) 4.7 2 7.4 1.9 2 3.9 FSHD with sparse to mild (<300 cells per 1000 fibers) cellular infiltrates (n = 12)
Macrophages (%) 37.1 2 29.0 32.4 5 17.7 T cells ( T l l + ) (%) 66.5 2 18 1
T 8 + n cells (%) 57.1 2 31.6 53 7 2 19.8 T 4 + n cells (%) 57.2 2 31.4 52.0 -+ 20.5
0.96 2 0.67 T4+n8+ ratio 0.85 2 0.73 BIT ratio 0.05 2 0.08 0.03 2 0.06 Leu-7+ cells (%) 18.6 2 17 6 17.6 2 14 3
58.2 2 28.8
6 3 2 5 2 * 2 3 6 2 1 0 1 7 0 1 2 1 1 5 6 5 9 2 1 6 0 4 2 5 2 1 6 8 0 79 2 0 67 0 1 0 + 0 0 8 * 1 0 1 2 - 4 6
0 4 2 1 0 2 2 6 2 1 9 7 7 9 0 2 1 7 5 5 7 O r 1 7 3 4 7 5 2 1 9 1 0 84 2 0 77 0 04 2 0 01 2 0 0 2 1 9 1
Values are expressed as mean ? SD Significantly dffferent from the values in FSHD with sparse to mild cellular infdtrates 'P < 0 005 and f P < 0 025
Facioscapulohumeral Muscular Dystrophy MUSCLE & NERVE Supplement 2 1995 S59

FIGURE 2. Muscle biopsies of FSHD patients often have a relatively normal appearance, although there is some variation in size, in the presence or absence of an internal nucleus, in endomysial fibrosis, and in numbers of mononuclear cells (a: H & E). Changes in fiber size diameter often become prominent with large and very small fibers being exhibited (b: mGT). Consecutive frozen sections obtained from FSHD patients were stained with H & E (c) and rnGt (e), and immunoreacted for dystrophin (d) and a-actinin (f). Note, partially degenerating fibers in the center are focally surrounded by and superficially invaded by mononuclear cells, but no nonnecrotic fibers are invaded by mononuclear cells. (a and b: x125; c-f: x250).
fibers were surrounded by and superficially in- vaded by mononuclear cells (Fig. 2). In contrast, blood vessels were frequently surrounded by a compact collection of cells (Fig. 3) and were often invaded by T4+ and T8+ T cells (Fig. 4). Presum- ably, these cells were passing through the vessel wall.
The overall perivascular (PV), perimysial (PMY), and endomysial (EMY) average cell counts per 1000 fibers in FSHD were, respectively: T cells, 97, 56, 277; B cells, 43, 6, 30; Leu-7+ cells, 14, 5 , 33;
Leu-l l+ cells, 2, 1, 2; and macrophages, 40, 32, 81. The T4/T8 ratios were 1.1, 0.7, and 1.0, re- spectively.
MHC-I expression was not detected in control muscle fibers, but was found in the surface mem- branes of a few muscle fibers in FSHD (Fig. 3). Vascular endothelial cells and mononuclear cells expressed MHC-I in both control and FSHD mus- cles. MHC-I1 expression was limited to vascular endothelial cells and some mononuclear cells (Fig. 3).
S60 Facioscapulohumeral Muscular Dystrophy MUSCLE & NERVE Supplement 2 1995

FIGURE 3. Inflammatory cells in FSHD. Serial sections were stained with H & E and reacted for T11, E l , HLA-I, and HLA-II markers, and acid phosphatase (AP). The perivascular exudates are intermingled with predominantly T and B cells. HLA-I antigen is expressed in all inflammatory cells, vascular endothelial cells, and in the plasma membrane of some adjacent muscle fibers. HLA-II antigen is expressed in vascular endothelial cells and in some inflammatory cells, but not in the plasma membrane of the muscle fiber ( ~ 2 5 0 ) .
Genetic Analysis. Genetic analysis was accom- plished in the 6 FSHD patients (from 5 unrelated families) who had numerous mononuclear cellular infiltrates. The disease in these patients was linked to 4q35 (Fig. 5) and the patients’ specimens exhib- ited small (<28 kb) EcoRI fragments (13-24 kb) that cosegregated with the disease (Figs. 5-7, and Table 1) .
DISCUSSION
The presence of inflammatory cellular infiltrates in the skeletal muscle of patients with FSHD is one of the characteristic features of the disease, and can be observed in 40-80% of patient^,^"'^^ while general histological changes in FSHD muscle are rather nonspecific (variations in fiber size, scat- tered small angulated fibers, etc.). In the present
study, 6 of 18 (33%) FSHD patients had marked inflammatory cellular exudates in muscle, with a mean value of 1835 ? 482 (SE) cells per 1000 mus- cle fibers (range 607-3756), these changes being paralleled by increasing numbers of necrotic fi- bers. Genetic analysis revealed that FSHD was linked to chromosome 4q35 in these 6 patients (3 familiar, 3 sporadic) and that they had FSHD- associated small EcoRl fragments (<28 kb) de- tected by the probes p13E-ll and pFR-1 (Table 1, Figs. 5-7). The remaining 12 patients had less marked inflammatory infiltrates, but still showed more inflammatory cells [76 * 21 (SE), range 16- 2671 than the controls [9.2 k 2.1 (SE)]. Thus, our findings suggest that inflammatory cellular re- sponse in muscle is a common histological feature of chromosome 4-associated FSHD in both famil-
Facioscapulohumeral Muscular Dystrophy MUSCLE & NERVE Supplement 2 1995 S61

FIGURE 4. Perivascular inflammatory cells in FSHD. The T4+ cells are most prominent at perivascular sites. Both T4+ and T8+ cells are seen occasionally moving through the vessel wall (arrow), but they do not invade the adjacent nonnecrotic muscle fibers (x410).
I I Markers Alleles I14S139 P, p, 3,1,5,6 UJS163 A,u ,3 ,4 ,5 ,6
47 I 16
p13E-ll/ EcoRI D4S139 / TaqI 46 47 48 49 50 46 47 48 49 50
kb
47.0- 34.6-
23.1-
FIGURE 5. Southern blot analysis of a FSHD patient (case 6:49) and his family in whose muscle specimen numerous inflammatory infiltrates were shown (p13E-11 probe). Each affected member had a small (24 kb) fragment (arrow) associated with the disease; this feature was not detected in the healthy family member^.^^,^' Other chromosome 4q35 markers (D4S139, D4S163) revealed that the disease in this family was associated with chromosome 4q35.
S62 Facioscapulohumeral Muscular Dystrophy MUSCLE 8, NERVE Supplement 2 1995

1 2 3 4 5 6 7 8
kb
48.5- 38.4- 33.5- 29.9- 2 4 . 8 - 22.6-
19.4-
17.1-
15.0-
12.1-
10.1-
+
4
8.6- 8.3-
FIGURE 6. Genetic analysis of FSHD patients in whose mus- cle specimens numerous inflammatory infiltrates were shown. Southern blot tests for EcoR1-digested genomic DNA from the families of cases 1 and 2 (pFR-1 probe). Both the father of case 1 (lane 1 : case 3) and his son (lane 3: case 1) had small (17 kb) EcoRl fragment (arrow). Case 2 (lane 8) showed a small (13 kb) EcoRl fragment (arrowhead) which was absent in both parents (lanes 5 and 6) , suggesting the presence of a de novo DNA rearrangement in the patient.
iar and sporadic patients. However, patients with polymyositis who have facial muscle involvement (about 8-1 1 %) have been rep~rted,"~" but we do not know whether the disease in these reported patients is linked to chromosome 4q. We speculate that at least some of the familiar patients with polymyositis who have facial and shoulder-girdle ~ e a k n e s s ~ , ~ , * ~ and the sporadic patients who have restricted distribution in the face and shoulder musc~es7,11,19,23,29,38,44,55 represent clinical vari- ants of chromosome 4-linked FSHD. Most of these patients show only limited clinical benefit with cor- ticosteroid treatment, and have progressive muscle
The nature of the inflammatory response in FSHD muscle seems to differ from that observed in inflammatory myopathies (Fig. 8). In polymyo- sitis (PM) and inclusion body myositis (IBM), but not in dermatoinyositis (DM), cytotoxic T-cell
WeakneSS.23,29,30,32,38,55
n - FSHDwith
EZ72 OtherFSHD
0 Controls
u numerous cellular infiltrates
v
v) Y c 4 !?
n J+ m
0 - b 2
5 n
z
I I I 1 0 1 5 2 0 2'5 k 2 8 k b
EcoRl fragment size detected by the probes pl3E-11 and pFR-1
FIGURE 7. Size distribution of the genomic EcoRl fragment associated with FSHD in 23 unrelated Japanese families and 35 controls. Probes p13E-11 and pFR-1 were used. All 6 pa- tients (five families) who had numerous inflammatory infil- trates in muscle are shown (black columns).
(CTL)-mediated muscle fiber injuries occur, and endomysial mononuclear cells (mostly T cells) fo- cally surround, invade, and finally replace nonne- crotic muscle fiber^."'^'^ Perforin+ and granzyme A + cells appear among these invading cells, and 10-12% of the endomysial T 8 + cells are shown to be double positive for p e r f 0 1 - h . ~ ~ In FSHD muscle, in contrast, we found no invasion of T8+, per- forin+, or granzyme A + cells into nonnecrotic fi- bers (Fig. 8), although a few degenerating fibers were focally surrounded by andlor superficially in- vaded by mononuclear cells (most being T cells and macrophages) (Fig. 2). These findings suggest that there is no CTL-mediated immune effector mechanism directed against muscle fibers in FSHD.
There are several similarities in the mononu- clear cell subsets at perivascular sites in FSHD and DM,*,14 i.e., the high percentage of B cells, the high T4/T8 ratios, and the close proximity of T 4 + cells to B cells. Nonnecrotic muscle fibers invaded by mononuclear cells are also essentially absent in both diseases (CTL-mediated muscle fiber injury is thus unlikely in these diseases). However, w e found no complement deposition on blood vessels in FSHD (data not shown). Perifascicular atrophy and ischemic changes or infarction of muscle are not observed in FSHD. Therefore, the immune ef- fector mechanism of FSHD must be different from that observed in DM.
Comparison of the immunocytochemical find- ings in FSHD and DMD is of interest, since pa- tients with these muscular dystrophies often show
Facioscapulohumeral Muscular Dystrophy MUSCLE & NERVE Supplement 2 1995 563

Macrophages
Nec fibers
7 cells \ 5 i y 100 200 300 /SO0 60D,
Nonnecrotic fibers invaded by mononuclear cells
FIGURE 8. Endomysial T cell counts, frequency of necrotic muscle fibers, and frequency of nonnecrotic muscle fibers invaded by mononuclear cells per 1000 muscle fibers in inclusion body myositis (IBM), polymyositis (PM), Duchenne muscular dystrophy (DMD), and FSHD. Values represent means in 8 biopsy specimens each of IBM, PM, DMD,3 and 18 biopsy specimens of FSHD.
numerous inflammatory infiltrates in m ~ s c l e . ~ , ' ~ ' ~ ~ In DMD, although the number of nonnecrotic fi- bers invaded by T cells is low and the invading cells remain at a superficial level, it is possible that the CTL-mediated immune effector mechanism may exis t2,3, 14 (Fig. 8). In contrast, in FSHD, only de- generating fibers are focally surrounded and su- perficially invaded by mononuclear cells (Fig. 2), nonnecrotic fibers are not invaded by mononu- clear cells (Fig. 8), and the surfaces of the adjacent muscle fibers appear normal (Fig. 4). Amounts of necrotic fibers also differ in the two diseases. DMD muscles have 4.1 times more necrotic fibers than FSHD (Fig. 8), but the number of endomysial in- flammatory T cells is 4.7 times greater in FSHD (Fig. 8).2,3,14 These findings suggest that the cellu- lar infiltrations in FSHD muscle do not simply represent nonspecific events triggered by muscle fiber necrosis of dystrophic origin. Therefore, it is conceivable that different immune effector mechanisms may be responsible for these two dis- eases.
We found the increasing number of necrotic fibers in FSHD to parallel the increased number of inflammatory cells (Fig. 1). Thus, it appears that inflammatory infiltrates in FSHD may accelerate secondary muscle fiber breakdown, since the cel- lular response in FSHD may not be caused simply by muscle fiber necrosis, as discussed above. This possibility is supported by clinical observations that
inflammatory myopathy with FSH distribution shows rapid progression of weakness, occasional my- algia, and marked to moderately elevated serum CK level, which may respond transiently to corticoste- roid treatment but not sustained.23,29930,32,38.5j
Finally, the finding that abundant T cells accu- mulate in the perivascular site of FSHD muscle is of note. In the blood vessels, occasional mononu- clear cells were observed moving through vessel walls (Fig. 4). The migration of mononuclear cells from the bloodstream is known to be initiated by a variety of signaling molecules produced locally by cells (mainly in connective tissue) or by comple- ment activation, by which vessel walls become more permeable.' In 50-70% of FSHD patients, exuda- tive retinal vasculopathy with capillary telangiecta- sis, microaneurysms, and capillary closure have been reported.".l6 Although retinal vasculopathy has not been proven as part of the disease, associ- ation of the two diseases is extremely interesting. Leaky capillaries in the retina imply analogous cap- illary abnormality in muscle. '' Our immunocyto- chemical observations in FSHD muscle, together with our genetic analysis of FSHD patients, suggest the presence of a T-cell-mediated effector re- sponse directed against either connective tissue and/or vascular elements and/or altered muscle fi- ber component(s) produced by dystrophic muscle fiber degeneration or by other means, in FSHD muscle.
S64 Facioscapulohurneral Muscular Dystrophy MUSCLE & NERVE Supplement 2 1995

REFERENCES
1. Albert B, Bray D, Lewis J, Raff M, Roberts K, Watson JD (eds): Molecular Biology of the Cell (3rd ed). New York, Gar- land Publishing Co., Inc., 1944, pp 1164-1 165.
2. Arahata K, Engel AG: Monoclonal antibody analysis of mononuclear cells in myopathies. I: Quantitation of subsets according to diagnosis and sites of accumulation and dem- onstration and counts of muscle fibers invaded by T cells. Ann Neurol 1984; 16: 193-208.
3. Arahata K, Engel AG: Monoclonal antibody analysis of mononuclear cells in myopathies. IV: Cell-mediated cyto- toxicity and muscle fiber necrosis. Ann Neurol 1988;23: 168-173.
4. Arahata K, Engel AG: Monoclonal antibody analysis of mononuclear cells in myopathies. V: Identification and quantitation of T8+ cytotoxic and T 8 + suppressor cells. Ann Neurol 1988;23:493-499.
5. Bacq M, Telerman-Toppet N, Coers C: Familiar myopa- thies with restricted distribution, facial weakness and in- flammatory changes in affected musc1es.J Neurol 1985;23 1 : 295-300.
6. Bailey RO, Marzulo DC, Hans MB: Infantile facioscapulo- humeral muscular dystrophy: new observations. Acta Neurol Scand 1986;74:51-58.
7. Bates D, Stevens JC, Hudgson P: “Polymyositis” with in- volvement of facial and distal musculature: one form of the facioscapulohumeral syndrome? J Neurol Sci 1973; 19: 105-1 08.
8. Bodensteiner JB, Schochet SS: Facioscapulohumeral mus- cular dystrophy: the choice of a biopsy site. Muscle Nerue 1986;9:544-547.
9. Brooke MH, Engel WK: The histologic diagnosis of neu- romuscular diseases: review of 79 biopsies. Arch Phys Med Rehabil 1966;47:99-12 I .
10. Brouwer OF: Clinical and Genetic Aspects of Facioscapulohum- era1 Muscular Dystrophy. Thesis, Leiden University, Leiden, The Netherlands, 1993.
11. Carroll JE, Silverman A, Isobe Y, Brown WR, Kelts KA, Brooke MH: Inflammatory myopathy, IgA deficiency, and intestinal malabsorption.] Pediat 1976;89:2 16-219.
12. Dubowitz V, Brooke MH: Muscle biopsy: a modern approach. London, Saunders, 1973, pp 202-212.
13. Emslie-Smith A, Arahata K, Engel AG: Major histocompat- ibility complex class I antigen expression, immunolocaliza- tion of interferon subtypes, and T cell-mediated cytotox- icity in myopathies. Hum Pathol 1989;20:224-231.
14. Engel AG, Arahata K: Mononuclear cells in myopathies: quantitation of functionally distinct subsets, recognition of antigen-specific cell-mediated cytotoxicity in some diseases, and implications for the pathogenesis of the different in- flammatory myopathies. Hum Pathol 1986; 17:704-721.
15. Figarella-Branger D, Pellissier JF, Serratrice G, Pouget J, Bianco N: Etude immunocytochimique des formes inflam- matoires de myopathies facio-scapulo-humerales et corre- lation avec d’autres myosites. Ann Pathol (Paris) 1989;9:
16. Fitzsimons RB, Gurwin EB, Bird AC: Retinal vascular ab- normalities in facioscapulohumeral muscular dystrophy. Brain 1987;110:631-648.
17. Goto K, Lee JH, Matsuda C, Hirabayashi K, Kojo T, Na- kamura A, Mitsunaga Y, Furukawa T, Sahashi K, Arahata K: DNA rearrangements in Japanese facioscapulohumeral patients: clinical correlations. Neuromusc Disord (in press).
18. Griggs RC, Tawil R, Storvic D, Mendell JR, Altherr MR: Genetics of facioscapulohumeral muscular dystrophy: new mutations in sporadic cases. Neurology 1993;43:2369-2372.
19. Heathfield KWG, Williams JRB: Diagnosis of polymyositis. Lancet 1960; 1: 1157-1 161.
20. Hewitt JE, Lyle R, Clark LN, Valleley EM, Wright TJ, Wij- menga C, van Deutekom JCT, Francis F, Sharpe PT, Hofker M, Frants RR, Williamson R: Analysis of the tan-
100-108.
dem repeat locus D4Z4 associated with facioscapulohum- era1 muscular dystrophy. H u m M o l Genet 1994;3: 1287-1 295.
21. Honda H, Mano Y, Takahashi A: Inflammatory changes in affected muscles of facioscapulohumeral dystrophy. J Neu- rol 1987;234:408411.
22. Jerusalem T: Die bioptische-histologische differential diag- nose der polymyositis und der progressiven muskel dystro- phie. Dtsch Z Neruenhezlk 1967;191:125-141.
23. Kaner J , Zuniga J, Teasdall RD: The facioscapulohumeral syndrome: a report of two cases. Hen9 Ford Hasp Med J 1982;30:33-36.
24. Lee JH, Goto K, Matsuda C, Arahata K: Characterization of a 3.3-kb KpnI tandemly repeated unit in the facioscapu- lohumeral muscular dystrophy (FSHD) gene region on chromosome 4q35. Muscle Nerve (this issue).
25. Lee JH, Goto K, Sahashi K, Nonaka I, Matsuda C, Arahata K: Cloning and mapping of a very short (10 kb) EcoRI fragment associated with facioscapulohumeral muscular dystrophy (FSHD). Muscle Nerve (this issue).
26. Lunt PW, Compston DAS, Harper PS: Estimation of age dependent penetrance in facioscapulohumeral muscular dystrophy by minimizing ascertainment bias. J Med Genet 1989;26:755-760.
27. Lunt PW: Workshop report: Report of the Sixth lnterna- tional Workshop on Facioscapulohumeral Muscular Dys- trophy: San Francisco, 11 November 1992; and current guidelines for clinical application of DNA rearrangements at locus D4S810. Neuromusc Disord 1994;4:83-86.
28. Mills KA, Buetow KH, Xu Y, Ritty TM, Mathews KD, Bo- drug SE, Wijmenga C, Balazs I, Murray JC: Genetic and physical mapping on chromosome 4 narrows the localiza- tion of the gene for facioscapulohumeral muscular dystro- phy (FSHD) AmJ Hum Genet 1992;51:432439.
29. Munsat TL, Piper D, Cancilla P, Mednick J : Inflammatory myopathy with facioscapulohumeral distribution. Neurology 1972;22:335-347.
30. Munsat TL, Bradley WG: Serum creatine phosphokinase levels and predonisone treated muscle weakness. Neurology 1977;27:96-97.
3 1. Munsat TL: Facioscapulohumeral muscular dystrophy and the scapuloperoneal syndrome, in Engel AG, Banker BQ (eds): Myology. New York, McGraw-Hill, 1986, pp 1251- 1266.
32. Nattrass FJ: Discussion on the clinical and electromyo- graphic aspects of polymyositis. Proc Royal Soc Med 1955; 49:105-107.
33. Ogryzlo MA: Chronic inflammatory lesions of skeletal mus- cle in rheumatoid arthritis and in other diseases. Arch Pathol 1948;46:301-312.
34. Orimo S, Koga R, Goto K, Nakamura K, Arai M, Tamaki M, Sugita H, Nonaka I, Arahata K: Immunohistochernical analysis of perforin and granzyme A in inflammatory my- opathies. Neuromusc Disord 1994;4:2 19-226.
35. Padberg GW: Facioscapulohumeral Disease. Thesis, Leiden University, Leiden, The Netherlands, 1982.
36. Padberg GW, Lunt PW, Koch M, Fardeau M: Facioscapu- lohumeral muscular dystrophy, in Emery AEH (ed): Diag- nostic Criteria for Neuromuscular Disorders. Baarn, ENMC, 1994, pp 19-24.
37. Pearson CM: Polymyositis and related disorders, in Walton J N (ed): Disorders of Voluntary Muscle (2nd ed). Boston, Little Brown & Co., 1969, p 504.
38. Rothstein TL, Carlson CB, Sumi SM: Polymyositis with facioscapulohumeral distribution. Arch Neurol 197 1 ;25:
39. Sarfarazi M, Wijmenga C, Upadhyaya M, Weiffenbach B, Hyser C, Mathews K, Murray J, Gilbert J, Pericak-Vance M, Lunt P, Frants R, Jacobsen S, Harper P: Regional mapping of facioscapulohumeral muscular dystrophy gene on 4q35: combined analysis of an international consortium. Am J Hum Genet 1992;51:396403.
40. Upadhyaya M, Lunt PW, Sarfarazi M, Broadhead W, Owen
3 1 3-3 19.
Facioscapulohumeral Muscular Dystrophy MUSCLE & NERVE Supplement 2 1995 S65

M, Harper PS: DNA marker applicable to presymptomatic and prenatal diagnosis of facioscapulohumeral disease. Lancet 1990;336: 1320-1 32 1.
41. Upadhyaya M, Lunt PW, Sarfarazi M, Broadhead W, Daniels J, Owen M, Harper PS: A closely linked DNA marker for facioscapulohumeral disease on chromosome 4 q . J M e d Genet 1991;28:665-671.
42. Upadhyaya M, Jardine P, Maynard J, Farnham J, Sarfarazi M, Wijmenga C, Hewitt JE, Frants RR, Harper PS, Lunt PW: Molecular analysis of British facioscapulohumeral dys- trophy families for 4q DNA rearrangements. Hum Mol Genet 1 993; 2:98 1-987.
43. van Deutekom JCT, Wijnienga C, van Tienhoven EAE, Gruter A-M, Hewitt JE, Padberg GW, van Ommen G-JB, Hofker MH, Frants RR: FSHD associated DNA rearrange- ments are due to deletions of integral copies of a 3.2 kb tandemly repeated unit. Hum Mol Genet 1993;2:2037-2042.
44. Walton JN, Adams RD: Polymyositis. Edinburg, E 8c S Liv- ingston Ltd., 1958.
45. Walton J, Gardner-Medwin D: The muscular dystrophies, in Walton J (ed): Divorders of VoluntaT Muscle. Edinburgh, Churchill Livingstone Ltd., 1988, pp 519-568.
46. Weiffenbach B, Dubois J, Storvick D, Tawil R, Jacobsen SJ, Gilbert J , Wijmenga C, Mendell JR, Winokur S, Altherr MR, Schultz P, Olandt S, Frants RR, Pericak-Vance M, Griggs RC: Mapping the facioscapulohumeral muscular dystrophy gene is complicated by chromosome 4q35 re- combination events. Nature Genet 1993;4: 165-169.
47. W'Jmenga C, Frants RR, Brouwer OF, Moerer P, Weber JL, Padberg GW: Localization of- facioscapulohumeral muscu- lar dystrophy gene on chromosome 4. Lancet 1990;336: 651-653.
48. Wijmenga C, Padberg GW, Moerer P, Wiegant J , Liem L, Brouwer OF, Milner ECB, Weber JL, van Ommen G-JB, Sandkuyl LA, Frants RK: Mapping of facioscapulohumeral
muscular dystrophy gene to chromosome 4q35-qter by multipoint linkage analysis and in situ hybridization. Ge- nomia 199 l ;9:570-575.
49. Wijmenga C, Hewitt JE, Sandkuijl LA, Clark LN, Wright TJ, Dauwerse HG, Gruter A-M, Hofker MH, Moerer P, Williamson R, van Ommen G-JB, Padberg GW, Frants RR: Chromosome 4q DNA rearrangements associated with facioscapulohumeral muscular dystrophy. Nature Genet
50. Wijmenga C, Brouwer OF, Padberg GW, Frants RR: Transmission of a de novo mutation associated with facio- scapulohumeral muscular dystrophy. Lancet 1992;340: 985-986.
5 1. Wijmenga C: Fucioscapulohumerul Muscular Dystrophy: from Genetic Mupping towards Gene Cloning. Thesis, Leiden Uni- versity, Leiden, The Netherlands, 1993.
52. Wijmenga C, Frants RR, Hewitt JE, van Deutekom JCT, van Gee1 M, Wright TJ, Padberg GW, Hofker MH, van Ommen G-JB: Molecular genetics of facioscapulohumeral muscular dystrophy. Neuromuc Disord 1993;3:487-491.
53. Winokur ST, Bengtsson U, Feddersen J , Mathews KD, Weiffenbach B, Bailey H, Markovich RP, MurrayJC, Was- muth JJ, Altherr M R , Schutte BC: The DNA rearrange- ment associated with facioscapulohumeral muscular dys- trophy involves a heterochromatin-associated repetitive el- ement: implications for a role of chromatin structure in the pathogenesis of the disease. Chromosome Res 1994;2: 225-234.
54. Wright TJ, Wijmenga C, Clark LN, Frants RR, Williamson R, Hewitt JE: Fine mapping of the FSHD gene region ori- entates the rearranged fragment detected by the probe p13E-11. Hum Mol Genet 1993;2:1673-1678.
55. Wulff JD, Lin JT, Kepes JJ: Inflammatory facioscapulo- humeral muscular dystrophy and Coats syndrome. Ann Neurol 1982; 12:398401.
1992;2:26-30.
S66 Facioscapulohumeral Muscular Dystrophy MUSCLE & NERVE Supplement 2 1995
















![[Reliability of the CINtec p16INK4a immunocytochemical test in screening cervical precancerous lesions]](https://img.pdfslide.net/doc/110x75/636144814b9aa63a9e00a9c7/reliability-of-the-cintec-p16ink4a-immunocytochemical-test-in-screening-cervical.jpg)












