Embed Size (px)
Citation preview

Jaw-stretch reflex is weaker in patients afterorthognathic surgery
Yi Luo a, Peter Svensson b,c, Janek Dalsgaard Jensen d, Thomas Jensen d,Bjarne Neumann d, Lars Arendt-Nielsen a, Kelun Wang a,d,*
aCenter for Sensory-Motor Interaction (SMI), Department of Health Science and Technology, Faculty of Medicine,
Aalborg University, Fredrik Bajers Vej 7 D2, 9220 Aalborg, Denmarkb Section of Clinical Oral Physiology, School of Dentistry, University of Aarhus, Vennelyst Boulevard 9, DK-8000
Aarhus C, DenmarkcCenter of Functionally Integrative Neuroscience (CFIN), MindLab, Aarhus University Hospital, 44 Norrebrogade,
Aarhus, DenmarkdDepartment of Oral & Maxillofacial Surgery, Aalborg Hospital, Aalborg, Denmark
a r c h i v e s o f o r a l b i o l o g y 5 9 ( 2 0 1 4 ) 1 3 2 1 – 1 3 2 7
a r t i c l e i n f o
Article history:
Accepted 8 August 2014
Keywords:
Jaw-stretch reflex
Orthognathic surgery
Dentofacial deformities
Physiology
Masticatory muscles
Electromyography
a b s t r a c t
Objectives: The jaw-stretch reflex (JSR) was studied in both patients and healthy participants
in order to investigate the possible long-term impact of orthognathic surgery on the motor
function of the masticatory system.
Design: JSR was measured in patients before surgery (PC), 1 year after surgery (PS) and in
healthy controls (HC) (N = 31 in each group). JSR was evoked by a standardized stretch device
and recorded bilaterally from masseter and anterior temporalis muscles using surface
electromyography (EMG).
Results: The peak-to-peak amplitude (which was normalized to pre-stimulus EMG activity)
of JSRs in PC and PS were significantly smaller than in HC (P < 0.001; P < 0.001). The onset
latency in PS was significantly longer compared with HC (P < 0.05). The duration of JSR in PS
was significantly longer than in HC and PC (P < 0.001; P < 0.05).
Conclusion: Patients with dentofacial deformities are characterized by reduced JSR ampli-
tude. The delayed onset and elongated duration of JSR might be potential indicators of a
long-term surgical impact on the motor function of the masticatory system.
# 2014 Elsevier Ltd. All rights reserved.
Available online at www.sciencedirect.com
ScienceDirect
journal homepage: http://www.elsevier.com/locate/aob
1. Introduction
The jaw-stretch reflex (JSR) is a short-latency monosynaptic
reflex serving to maintain posture and to fine-tune the
voluntary movements of the mandible.1,2 JSR is described as
the brisk twitch of the jaw-closing muscles as a response to a
sudden stretch of the muscles. The major receptors to the
* Corresponding author at: Center for Sensory-Motor Interaction (SMI), DAalborg University, Fredrik Bajers Vej 7 D2, 9220 Aalborg, Denmark. T
E-mail address: [email protected] (K. Wang).http://dx.doi.org/10.1016/j.archoralbio.2014.08.0060003–9969/# 2014 Elsevier Ltd. All rights reserved.
stretch are the muscle spindles which are composed of
intrafusal muscle fibres and embedded in the bulky extrafusal
muscle fibres of the jaw-closing muscles. When stimulated,
the muscle spindle afferent signals are transmitted to many a-
motor neurons innervating the extrafusal muscle fibres via the
brain stem trigeminal motor nucleus and a brief synchronous
activation of the jaw-closing muscle motor units ensues.1 The
evaluation of JSR can provide essential information on the
epartment of Health Science and Technology, Faculty of Medicine,el.: +45 9940 8745; fax: +45 9815 4008.

a r c h i v e s o f o r a l b i o l o g y 5 9 ( 2 0 1 4 ) 1 3 2 1 – 1 3 2 71322
motor control of the muscular performance. JSR can be evoked
by tapping on the chin with a tendon hammer in a clinical
setting. More accurately, JSR can be induced by a standardized
jaw-stretch device which has been intensively used to study
JSR and allows a high degree of control with the stretch
stimulus.3,4
It has been suggested that several factors, such as
background electromyography (EMG) activity and bite posi-
tion, may affect JSR.4 The presence of chronic orofacial painful
conditions and experimental acute muscle pain has also been
well documented to facilitate JSR.5–7 The peak-to-peak ampli-
tude of JSR has been observed to increase during pain
condition. It has been suggested that the facilitation of JSR
in pain condition serves as a protective function since it may
reduce the jaw mobility, which as a result may reduce the
muscle pain.7–9
However, so far no studies have reported JSR recordings in
patients with dentofacial deformities or in patients after
orthognathic surgery (OS). Compared with healthy individua-
ls, patients with dentofacial deformities are characterized by
disharmonious dental and skeletal structures. It has been
reported that these patients tend to report more frequent
headache and more pain in the orofacial region.10,11 However,
it is not clear whether the different anatomic structures and
the presence of pain have certain influence on the JSR of these
patients. OS aims to improve the occlusal relationship, the
function of the masticatory system and the facial aesthetics in
these patients. After OS inevitable changes of structures take
place in various tissues of the masticatory system. In addition,
a somatosensory function alteration in the trigeminal region is
a common complication following OS.10,12 It has been
indicated that 15%–20% of patients reported ongoing pain 6
months to 1 year after OS.13,14
The aims of the present study were to investigate: (1) the
influence of dentofacial deformities on JSR, (2) the possible
long-term surgical impact of OS on JSR, and (3) the influence of
pain on JSR.
2. Materials and methods
2.1. Participants
Thirty-one patients (16 women and 15 men, mean age
28.2 years) were recruited 1 year after OS, subsequently
mentioned as the surgical patient group (PS). Thirty-one
age- and gender-matched patients were recruited before OS
and served as the patient control group (PC). Further, thirty-
one age- and gender-matched healthy participants served as
the healthy control group (HC).
Table 1 – Numbers of patients with various subgroups of den
Group Skeletal classification
Class I Class II Class III D
PS 2 18 11
PC 3 14 14
PC = patient control (patient before surgery); PS = surgical patient (patien
All the patients were recruited from the Department of Oral
and Maxillofacial Surgery, Aalborg Hospital, Denmark. Inclu-
sion criteria for both PS and PC group: a developmental dento-
skeleto-facial disharmony; complete dentitions (with the
exception of premolars in some cases due to orthodontic
treatment needs and with the exception of the third molars in
some cases); aged between 18 and 40 years; scheduled for a
combined orthodontic–orthognathic treatment. Exclusion
criteria for both PS and PC group: A congenital anomaly
(i.e., cleft lip and palate) or acute trauma; previous facial
surgery; pregnant at baseline; a medical condition associated
with systemic neuropathy (i.e., diabetes, hypertension, kidney
problems). The types of dentofacial deformities were well-
matched between PS and PC groups (Table 1). In the PS group,
twenty patients had been treated with Le Fort I maxillary
osteotomy (Le Fort I) in combination with bilateral sagittal split
ramus osteotomy (BSSRO) and eleven patients had received
single jaw surgery (six patients had undergone Le Fort I and
five patients had undergone BSSRO). All PS patients had
finished their orthodontic treatment and were without braces.
All PC patients were in the stage before or just at the beginning
of their orthodontic treatment, free of braces.
All healthy participants in the HC group were recruited
among students at Aalborg University. Inclusion criteria for
the HC group: complete dentitions (with the exception of third
molars in some cases); Class I skeletal and dental relation-
ships; aged between 18 and 40 years. Exclusion criteria for the
HC group: Previous facial surgery; jaw muscle/temporoman-
dibular joint (TMJ) pain, headaches, other symptoms of pain in
the craniofacial region or other parts of the body during the
past year; any jaw dysfunction (checked at the clinical
examination and by means of the questionnaires Research
Diagnostic Criteria for Temporomandibular Disorders (RDC/
TMD))15; pregnant at baseline; a medical condition associated
with systemic neuropathy (i.e., diabetes, hypertension, kidney
problems).
This study was approved by the local ethics committee
(Project number: N-2008-0057) in accordance with the Helsinki
Declaration II. Written informed consent was obtained from
all participants before they were included in the study. All
participants were identified by means of numbers only.
2.2. Self-reported pain and sensory testing
All patients were assessed using clinical examinations and the
questionnaires RDC/TMD.15 Further, they were diagnosed
with a corresponding subtype of TMD when applicable. For
patients with orofacial pain, the pain intensity of the last 6
months and at the time of the experiment was rated on a
numerical rating scale from 0 to 10 where 0 was ‘no pain’ and
tofacial deformities.
Vertical morphology abnomality Facial asymmetry
olichofacial Brachyfacial
8 2 3
9 3 3
t 1 year after surgery).

a r c h i v e s o f o r a l b i o l o g y 5 9 ( 2 0 1 4 ) 1 3 2 1 – 1 3 2 7 1323
10 was ‘the worst pain imaginable’. Furthermore, quantitative
sensory testing (including measurement of warm detection
threshold (WDT), cold detection threshold (CDT), heat pain
threshold (HPT), cold pain threshold (CPT), pressure pain
threshold (PPT), vibration detection threshold (VDT)) were
performed on the facial skin innervated by the trigeminal
second and third branches in patients after surgery to detect
possible sensory alterations other than pain. Data of HC group
were also recorded and set as reference. Then the percentage
of sensory alterations was counted for PS groups based on the
reference data. Detailed methods of quantitative sensory
testing in the orofacial region were described by our previous
study.16
2.3. Jaw-stretch reflex recording
JSR was evoked by the standardized jaw muscle stretch device
described by Miles.3 Briefly, a stainless-steel bite-bar was
mounted on a frame attached to the floor. A powerful
electromagnetic vibrator (Ling Dynamic Systems, model 406,
UK) imposed servo-controlled displacements of the lower jaw
bar. The displacement of the vibrator probe was measured
with a linear potentiometer (Sakae Type 20 FLP 30A-5 K, Japan)
mounted in parallel with the probe. Acceleration in the
vertical plane was measured by an accelerometer (Delta Tron1
Accelerometer Type 4399, Bruel & Kjær, Denmark) mounted on
the lower jaw bar.6 JSR was recorded from the masseter and
the anterior temporalis muscles on both sides. Bipolar
disposable surface electrodes (4 � 7 mm recording area, 720-
01-k, Neuroline; Medicotest) were placed 10 mm apart along
the central part of the masseter and the anterior temporalis
muscles on both sides. A reference electrode was attached to
the right wrist. Before the JSR recording the average
electromyography (EMG) value of the maximal voluntary
contraction (MVC) of the left masseter muscle was obtained
and was arbitrarily set as the 100% value for the subsequent
visual feedback. During JSR recording each participant was
instructed to bite on the jaw bars of the stretch device with the
incisors, exerting a 15% level of the EMG-MVC. The participant
achieved this by receiving visual feedback from markers
changing from red to green on a computer screen. When this
was achieved, the jaw bars were automatically triggered to
stretch the jaws. The initial distance between the jaw bars was
Fig. 1 – Electromyography
4.0 mm. The displacement between the bars was set as 1 mm
with a ramp time of 10 ms. For each individual, 20 sweeps of
stretch were averaged for analysis. The EMG signals were
amplified 2000–5000 times (Counterpoint MK2, DK), filtered
with bandpass 20 Hz to 1 kHz, sampled at 4 kHz and stored for
off-line analysis.
A special-purpose computer programme (Aalborg Univer-
sity) was subsequently used to analyze the JSR responses. All
the reflex parameters were determined objectively by using
the computer programme.4,6,9 The pre-stimulus EMG activity
was calculated from the rectified recordings of the 100 ms
interval prior to the stretch stimulus. The onset latency,
duration, and the peak-to-peak amplitude of JSR were
calculated from the non-rectified recordings. The peak-to-
peak amplitude was then normalized through the formula:
Normalized peak-to-peak amplitude = (peak-to-peak ampli-
tude/pre-stimulus EMG activity) � 100%. The purpose of the
normalization was to rule out the influence of different
background of pre-stimulus EMG activity and to eliminate the
influence of other factors which influence the absolute
magnitude of an EMG (skin thickness, skin impedance, muscle
size etc.) (Fig. 1 shows detailed components of JSR).
2.4. Statistical analysis
Pain frequencies were analyzed using the Chi-square test, and
pain scores were analyzed by an independent t-test. The data
of JSR parameters were analyzed using four-way repeated
measure ANOVA, with group and the presence of pain as
between-subject factors, and muscle (masseter, temporalis)
and side (left, right) as within-subject factors. Sphericity was
checked for between-subject factors before each repeated
measure ANOVA analysis. When sphericity was rejected, the
result of a Greenhouse–Geisser test was read instead. The
Bonferroni test was employed as the post hoc test. The
significance level was set as 0.05.
In order to demonstrate the size of the differences between
the two patient groups independently of the different units of
the JSR parameters, Z-transformation of data was conducted.
The data of healthy control group were set as the reference
data for Z-score transformation, and all the patients data were
transformed based on the reference data. The units of
parameters were eliminated after the transformation. The
of jaw-stretch reflex.
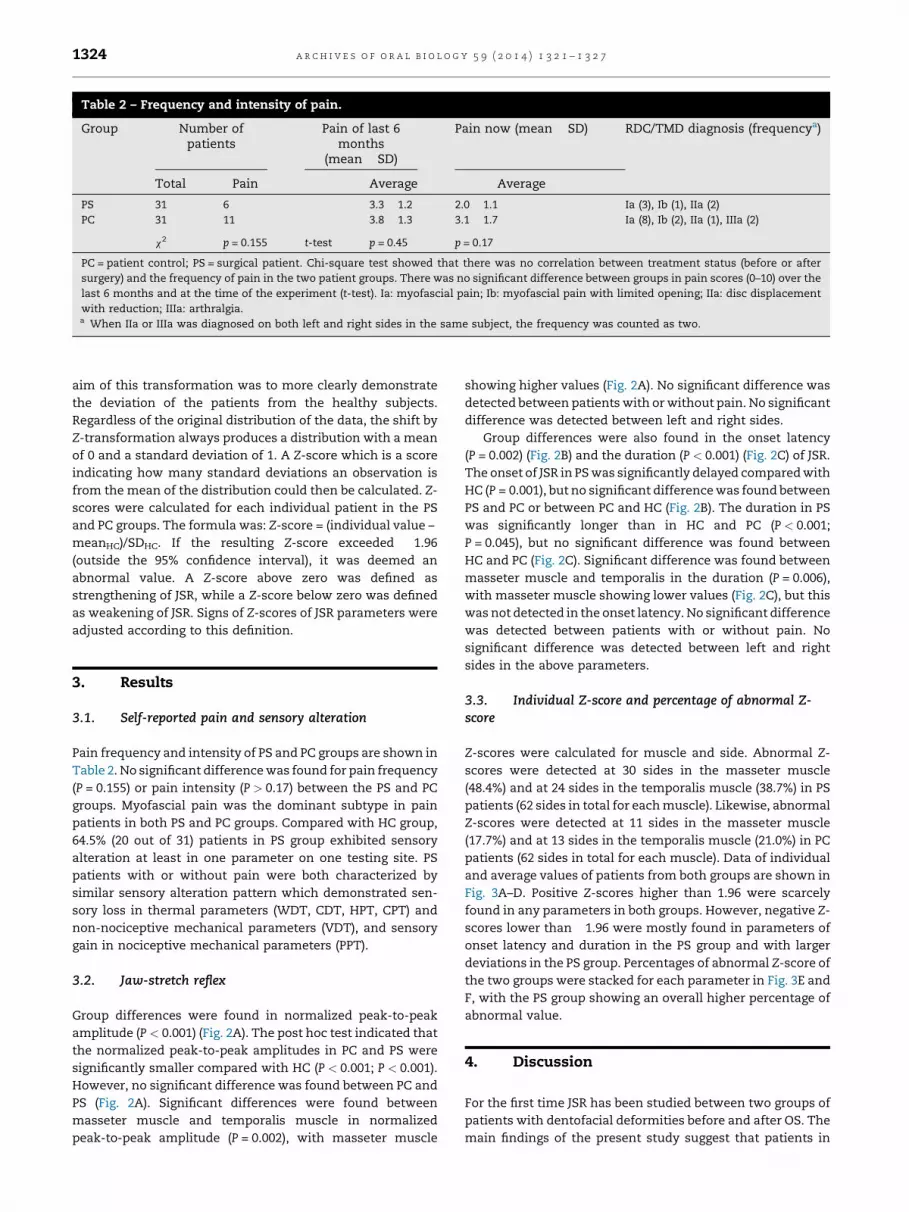
Table 2 – Frequency and intensity of pain.
Group Number ofpatients
Pain of last 6months
(mean � SD)
Pain now (mean � SD) RDC/TMD diagnosis (frequencya)
Total Pain Average Average
PS 31 6 3.3 � 1.2 2.0 � 1.1 Ia (3), Ib (1), IIa (2)
PC 31 11 3.8 � 1.3 3.1 � 1.7 Ia (8), Ib (2), IIa (1), IIIa (2)
x2 p = 0.155 t-test p = 0.45 p = 0.17
PC = patient control; PS = surgical patient. Chi-square test showed that there was no correlation between treatment status (before or after
surgery) and the frequency of pain in the two patient groups. There was no significant difference between groups in pain scores (0–10) over the
last 6 months and at the time of the experiment (t-test). Ia: myofascial pain; Ib: myofascial pain with limited opening; IIa: disc displacement
with reduction; IIIa: arthralgia.a When IIa or IIIa was diagnosed on both left and right sides in the same subject, the frequency was counted as two.
a r c h i v e s o f o r a l b i o l o g y 5 9 ( 2 0 1 4 ) 1 3 2 1 – 1 3 2 71324
aim of this transformation was to more clearly demonstrate
the deviation of the patients from the healthy subjects.
Regardless of the original distribution of the data, the shift by
Z-transformation always produces a distribution with a mean
of 0 and a standard deviation of 1. A Z-score which is a score
indicating how many standard deviations an observation is
from the mean of the distribution could then be calculated. Z-
scores were calculated for each individual patient in the PS
and PC groups. The formula was: Z-score = (individual value –
meanHC)/SDHC. If the resulting Z-score exceeded �1.96
(outside the 95% confidence interval), it was deemed an
abnormal value. A Z-score above zero was defined as
strengthening of JSR, while a Z-score below zero was defined
as weakening of JSR. Signs of Z-scores of JSR parameters were
adjusted according to this definition.
3. Results
3.1. Self-reported pain and sensory alteration
Pain frequency and intensity of PS and PC groups are shown in
Table 2. No significant difference was found for pain frequency
(P = 0.155) or pain intensity (P > 0.17) between the PS and PC
groups. Myofascial pain was the dominant subtype in pain
patients in both PS and PC groups. Compared with HC group,
64.5% (20 out of 31) patients in PS group exhibited sensory
alteration at least in one parameter on one testing site. PS
patients with or without pain were both characterized by
similar sensory alteration pattern which demonstrated sen-
sory loss in thermal parameters (WDT, CDT, HPT, CPT) and
non-nociceptive mechanical parameters (VDT), and sensory
gain in nociceptive mechanical parameters (PPT).
3.2. Jaw-stretch reflex
Group differences were found in normalized peak-to-peak
amplitude (P < 0.001) (Fig. 2A). The post hoc test indicated that
the normalized peak-to-peak amplitudes in PC and PS were
significantly smaller compared with HC (P < 0.001; P < 0.001).
However, no significant difference was found between PC and
PS (Fig. 2A). Significant differences were found between
masseter muscle and temporalis muscle in normalized
peak-to-peak amplitude (P = 0.002), with masseter muscle
showing higher values (Fig. 2A). No significant difference was
detected between patients with or without pain. No significant
difference was detected between left and right sides.
Group differences were also found in the onset latency
(P = 0.002) (Fig. 2B) and the duration (P < 0.001) (Fig. 2C) of JSR.
The onset of JSR in PS was significantly delayed compared with
HC (P = 0.001), but no significant difference was found between
PS and PC or between PC and HC (Fig. 2B). The duration in PS
was significantly longer than in HC and PC (P < 0.001;
P = 0.045), but no significant difference was found between
HC and PC (Fig. 2C). Significant difference was found between
masseter muscle and temporalis in the duration (P = 0.006),
with masseter muscle showing lower values (Fig. 2C), but this
was not detected in the onset latency. No significant difference
was detected between patients with or without pain. No
significant difference was detected between left and right
sides in the above parameters.
3.3. Individual Z-score and percentage of abnormal Z-score
Z-scores were calculated for muscle and side. Abnormal Z-
scores were detected at 30 sides in the masseter muscle
(48.4%) and at 24 sides in the temporalis muscle (38.7%) in PS
patients (62 sides in total for each muscle). Likewise, abnormal
Z-scores were detected at 11 sides in the masseter muscle
(17.7%) and at 13 sides in the temporalis muscle (21.0%) in PC
patients (62 sides in total for each muscle). Data of individual
and average values of patients from both groups are shown in
Fig. 3A–D. Positive Z-scores higher than 1.96 were scarcely
found in any parameters in both groups. However, negative Z-
scores lower than �1.96 were mostly found in parameters of
onset latency and duration in the PS group and with larger
deviations in the PS group. Percentages of abnormal Z-score of
the two groups were stacked for each parameter in Fig. 3E and
F, with the PS group showing an overall higher percentage of
abnormal value.
4. Discussion
For the first time JSR has been studied between two groups of
patients with dentofacial deformities before and after OS. The
main findings of the present study suggest that patients in
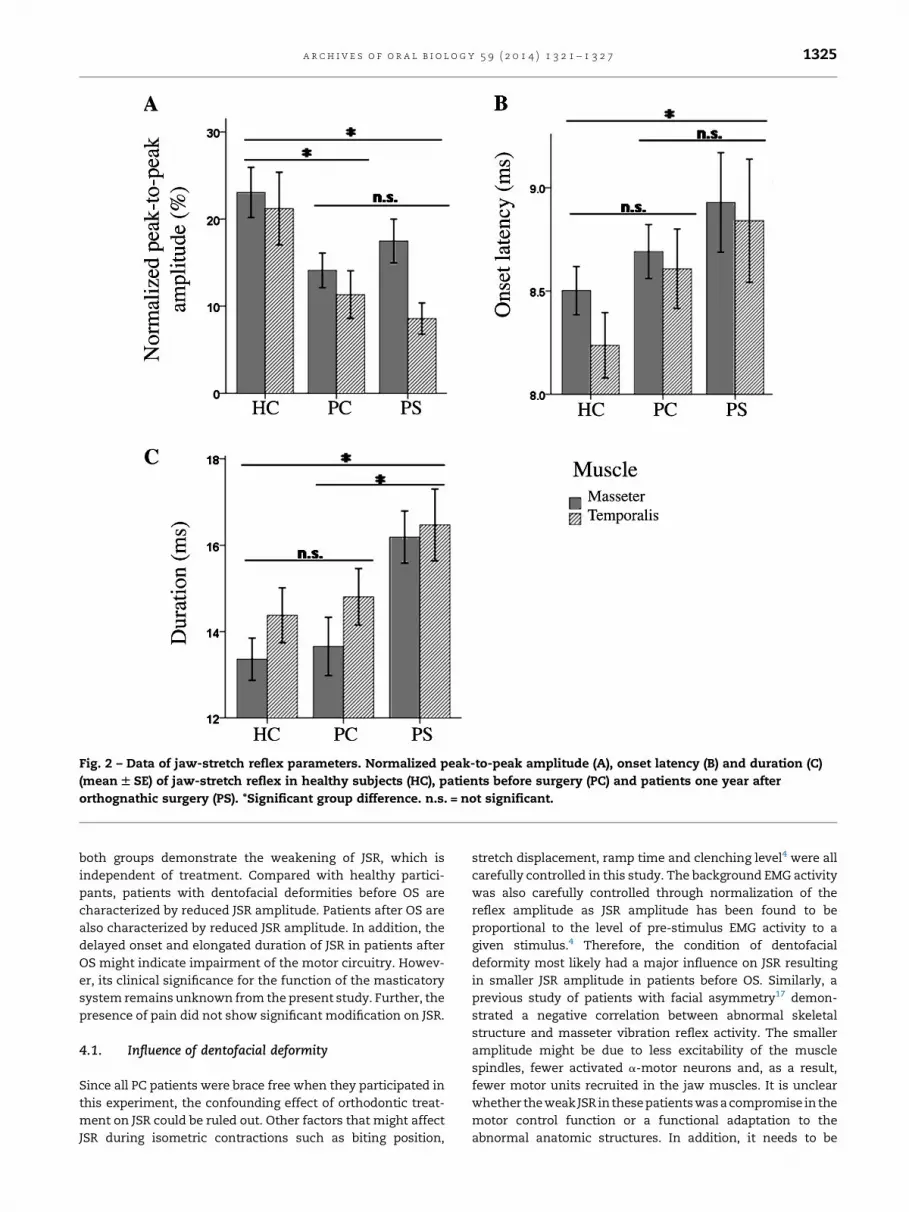
Fig. 2 – Data of jaw-stretch reflex parameters. Normalized peak-to-peak amplitude (A), onset latency (B) and duration (C)
(mean W SE) of jaw-stretch reflex in healthy subjects (HC), patients before surgery (PC) and patients one year after
orthognathic surgery (PS). *Significant group difference. n.s. = not significant.
a r c h i v e s o f o r a l b i o l o g y 5 9 ( 2 0 1 4 ) 1 3 2 1 – 1 3 2 7 1325
both groups demonstrate the weakening of JSR, which is
independent of treatment. Compared with healthy partici-
pants, patients with dentofacial deformities before OS are
characterized by reduced JSR amplitude. Patients after OS are
also characterized by reduced JSR amplitude. In addition, the
delayed onset and elongated duration of JSR in patients after
OS might indicate impairment of the motor circuitry. Howev-
er, its clinical significance for the function of the masticatory
system remains unknown from the present study. Further, the
presence of pain did not show significant modification on JSR.
4.1. Influence of dentofacial deformity
Since all PC patients were brace free when they participated in
this experiment, the confounding effect of orthodontic treat-
ment on JSR could be ruled out. Other factors that might affect
JSR during isometric contractions such as biting position,
stretch displacement, ramp time and clenching level4 were all
carefully controlled in this study. The background EMG activity
was also carefully controlled through normalization of the
reflex amplitude as JSR amplitude has been found to be
proportional to the level of pre-stimulus EMG activity to a
given stimulus.4 Therefore, the condition of dentofacial
deformity most likely had a major influence on JSR resulting
in smaller JSR amplitude in patients before OS. Similarly, a
previous study of patients with facial asymmetry17 demon-
strated a negative correlation between abnormal skeletal
structure and masseter vibration reflex activity. The smaller
amplitude might be due to less excitability of the muscle
spindles, fewer activated a-motor neurons and, as a result,
fewer motor units recruited in the jaw muscles. It is unclear
whether the weak JSR in these patients was a compromise in the
motor control function or a functional adaptation to the
abnormal anatomic structures. In addition, it needs to be

Fig. 3 – Individual and average Z-scores and percentage of abnormal Z-score of jaw-stretch reflex parameters in patients
(counted by side). PC = patient control (total sides n = 62); PS = surgical patient (total sides n = 62). (A) Z-score of masseter
muscle in PS patients; (B) Z-score of masseter muscle in PC patients; (C) Z-score of temporalis muscle in PS patients; (D) Z-
score of temporalis muscle in PC patients; (E) stacked percentage of abnormal Z-score for masseter muscle in PS and PC
groups; (F) stacked percentage of abnormal Z-score for temporalis muscle in PS and PC groups. Norm P–P = normalized
peak-to-peak amplitude.
a r c h i v e s o f o r a l b i o l o g y 5 9 ( 2 0 1 4 ) 1 3 2 1 – 1 3 2 71326
further elucidated whether different skeletal abnormalities
affect JSR differently, to which direction and to what extent.
4.2. Surgical impact
Three-dimensional mass structure changes take place after
OS. In order to take adaptation and relapse into account, the
data of the PS group were collected 1 year after OS. On the one
hand, due to the improvement of skeletal structures the
changes in position, orientation and length of muscles
towards normal range might affect the jaw muscle tone,
which might affect JSR. On the other hand, the invasive
surgical procedure and its complications, such as tissue
injuries and swelling, might also impact JSR. Reduced
amplitude and delayed onset of blink reflex have been
observed after OS due to damage to the mental nerve.18
Damage to the lingual nerve can lead to no or delayed jaw-
opening reflexes in rats.19 The mechanism of JSR is different
from the above reflexes, but it is similar that the cause of the
weakening of the JSR (reduced peak-to-peak amplitude and
delayed onset) might be due to the potential direct or indirect
surgical injuries to the nerve conduction pathway. The major
receptors of JSR are muscle spindles innervated by g-motor
neurons and the afferent signals are transmitted to the brain
stem by type Ia and II afferent fibres.20 Those fibres are
responsible for detecting information of changes in the muscle
length. The efferent signals from the trigeminal motor nucleus
then lead to an increase in the a-motor neuron innervated
muscle activity.1 It is possible that damage or modulation in
some parts of the circuit loop caused by OS might slow down
the nerve conduction, which might lead to the delaying of the
reflex. In turn, the synchronization of the action potentials in
different nerve fibres would be reduced, which might
consequently reduce the peak-to-peak amplitude and in-
crease the duration of the response.
4.3. Influence of pain
The presence of jaw muscle pain has been well documented to
facilitate JSR resulting in increased JSR amplitude.5,6 Although

a r c h i v e s o f o r a l b i o l o g y 5 9 ( 2 0 1 4 ) 1 3 2 1 – 1 3 2 7 1327
PC and PS patients reported TMJ/muscle pain, no significant
facilitation of JSR amplitude was found. This might be due to
the finding that the pain intensity of these patients was too
low (pain scores were around 2–3 out of 10) to modulate JSR.
Also, the total number of patients with pain might be relatively
small to show a significant difference. Another possible
explanation could be that the condition of dentofacial
deformities might serve as a more potent influential factor
on JSR which may offset the effect of pain.
5. Conclusions
In conclusion, the present results suggest that, compared with
healthy subjects, a weakening of JSR exists in patients both
before and after OS. Patients with dentofacial deformity are
characterized by reduced JSR amplitude. The delayed onset
and longer duration of JSR might be potential indicators of
long-term surgical impact on the motor function of the
masticatory system.
Funding
This study was supported by Det Obelske Familiefond of
Denmark (grant no. BG/mp 20112-16860 C1).
Competing interests
The authors declare no conflicts of interest.
Ethical approval
This study was approved by the Regional Ethical Committee of
North Jutland, Denmark. The Project number is N-2008-0057.
r e f e r e n c e s
1. Miles TS, Flavel SC, Nordstrom MA. Stretch reflexes in thehuman masticatory muscles: a brief review and a newfunctional role. Hum Mov Sci 2004;23(3–4):337–49.
2. Lund JP, Lamarre Y, Lavigne G, Duquet G. Human jawreflexes. Adv Neurol 1983;39:739–55.
3. Miles TS, Poliakov AV, Flavel SC. An apparatus for controlledstretch of human jaw-closing muscles. J Neurosci Methods1993;46(3):197–202.
4. Wang K, Svensson P. Influence of methodologicalparameters on human jaw-stretch reflexes. Eur J Oral Sci2001;109(2):86–94.
5. Cruccu G, Frisardi G, Pauletti G, Romaniello A, Manfredi M.Excitability of the central masticatory pathways in patients
with painful temporomandibular disorders. Pain1997;73(3):447–54.
6. Wang K, Svensson P, Arendt-Nielsen L. Effect of tonicmuscle pain on short-latency jaw-stretch reflexes inhumans. Pain 2000;88(2):189–97.
7. Cairns BE, Wang K, Hu JW, Sessle BJ, Arendt-Nielsen L,Svensson P. The effect of glutamate-evoked massetermuscle pain on the human jaw-stretch reflex differs in menand women. J Orofac Pain 2003;17(4):317–25.
8. Lund JP, Donga R, Widmer CG, Stohler CS. The pain-adaptation model: a discussion of the relationship betweenchronic musculoskeletal pain and motor activity. Can JPhysiol Pharmacol 1991;69(5):683–94.
9. Peddireddy A, Wang K, Svensson P, Arendt-Nielsen L.Stretch reflex and pressure pain thresholds in chronictension-type headache patients and healthy controls.Cephalalgia 2009;29(5):556–65.
10. Panula K, Finne K, Oikarinen K. Incidence of complicationsand problems related to orthognathic surgery: a review of655 patients. J Oral Maxillofac Surg 2001;59(10):1128–36.discussion 1137.
11. Baad-Hansen L, Arima T, Arendt-Nielsen L, Neumann-Jensen B, Svensson P. Quantitative sensory tests before and1(1/2) years after orthognathic surgery: a cross-sectionalstudy. J Oral Rehabil 2010;37(5):313–21.
12. Kim SG, Park SS. Incidence of complications and problemsrelated to orthognathic surgery. J Oral Maxillofac Surg2007;65(12):2438–44.
13. Joss CU, Thuer UW. Neurosensory and functionalimpairment in sagittal split osteotomies: a longitudinaland long-term follow-up study. Eur J Orthod 2007;29(3):263–71.
14. Phillips C, Essick G, Zuniga J, Tucker M, Blakey 3rd G.Qualitative descriptors used by patients followingorthognathic surgery to portray altered sensation. J OralMaxillofac Surg 2006;64(12):1751–60.
15. Dworkin SF, LeResche L. Research diagnostic criteria fortemporomandibular disorders: review, criteria,examinations and specifications, critique. J CraniomandibDisord 1992;6(4):301–55.
16. Matos R, Wang K, Jensen JD, Jensen T, Neuman B, SvenssonP, Arendt-Nielsen L. Quantitative sensory testing in thetrigeminal region: site and gender differences. J Orofac Pain2011;25(2):161–9.
17. Machida N, Yamada K, Takata Y, Yamada Y. Relationshipbetween facial asymmetry and masseter reflex activity. JOral Maxillofac Surg 2003;61(3):298–303.
18. Jaaskelainen SK, Peltola JK, Lehtinen R. The mental nerveblink reflex in the diagnosis of lesions of the inferioralveolar nerve following orthognathic surgery of themandible. Br J Oral Maxillofac Surg 1996;34(1):87–95.
19. Radwan Y, Thexton AJ. Recovery of the jaw-opening reflexafter lesions of the lingual nerve in the rat. J Dent Res1993;72(8):1198–205.
20. Tsukiboshi T, Sato H, Tanaka Y, Saito M, Toyoda H,Morimoto T, et al. Illusion caused by vibration of musclespindles reveals an involvement of muscle spindle inputs inregulating isometric contraction of masseter muscles. JNeurophysiol 2012;108(9):2524–33.





























