Embed Size (px)
Citation preview

Oral Oncology (2007) 43, 204–212
ava i lab le at www.sc iencedi rec t . com
journal homepage: ht tp : / / in t l .e lsevierheal th .com/ journals /oron/
Lip defects due to tumor excision: Aproposof 899 cases
O. Papadopoulos a,b, P. Konofaos a,*, Z. Tsantoulas b, C. Chrisostomidis b,M. Frangoulis b, P. Karakitsos c
a Second Department of Propedeutic Surgery of Athens University, Laiko General Hospital of Athens, Attica, Greeceb Department of Plastic and Reconstructive Surgery, A Sygros Hospital, Athens, Greecec Department of Cytopathology, University General Hospital ATTIKON, Athens, Greece
Received 4 February 2006; received in revised form 27 February 2006; accepted 27 February 2006Available online 20 July 2006
Summary Reconstructive surgery of the lips after resection of tumors requires a completeunderstanding of the anatomy of this region. Most lip cancers remain localized and grow slowly,with a propensity for superficial rather than vertical spread. From January 1983 to December of2005, 899 patients underwent reconstructive surgery for skin tumors involving the lips. SCCswere the most frequent skin tumors on male patients whereas BCCs were most common onthe female patients. The lower lip was the anatomic zone most frequently involved in our ser-ies. Preoperative evaluation of the patients was performed in all cases. In the last five-years,we have performed preoperative fine needle aspiration (FNA) biopsy of the tumor. The FNAsample was then examined by ThinPrep technique (Cytolyt; Cytyc, Co, Boxborough, MA,USA). In our series, from the 550 patients who had a five-year follow-up we observed 62 recur-rences of the primary tumor. The five-year recurrence rate was 11.28%. The aim of this retro-spective study is to report our experience in the treatment of lips tumors with selectivecombination of treatment modalities.
�c 2006 Elsevier Ltd. All rights reserved.
KEYWORDSLip tumors;Lip defects;ThinPrep technique;Lip reconstruction
1d
Af
Introduction
Reconstructive surgery of lip defects due to cancer appearsto be a unique challenge to the plastic surgeon because of
368-8375/$ - see front matter �c 2006 Elsevier Ltd. All rights reservedoi:10.1016/j.oraloncology.2006.02.015
* Corresponding author. Present address: 36, Megistis Street,thens 11364, Attica, Greece. Tel.: +30 210 8668192/6977404371;ax: +30 210 8668192.
E-mail address: [email protected] (P. Konofaos).
the prominent location, elegant form, and important func-tions of the lips. Resection of lip tumors causes both func-tional and aesthetic deficiencies. Oral competence,maximum oral aperture, mobility, sensation (when possi-ble), and aesthetically pleasing results should be the aimsof reconstruction of lip defects.
Reconstructive surgery of the lips after resection oftumors requires a complete understanding of the anatomyof this region. The lips are a three-layered structure
.

Lip defects due to tumor excision 205
composed of skin, an inner layer of muscle, and mucosa.The major feature of both the upper and the lower lip isthe vermilion, composed of modified mucosa that is devoidof minor salivary glands. The vermilion represents themucocutaneous junction between the inner mucosa andouter skin, and it is of great cosmetic importance. Theupper lip is composed of three units: two lateral wingsand a median portion, the plithrum. The lower lip consistsof a single unit demarcated superiorly by the vermilon–skinjunction, inferiorly by the chin crease, and laterally by thenasolabial lines. The major muscle of the lips is the orbic-ularis oris, which provides sphincteric function for the oralcavity. Other associated muscles include the zygomaticusmajor and minor, levator anguli oris, levator labii superi-oris, depressor anguli oris, depressor labii inferioris, riso-rius, mentalis, buccinator, and platysma muscles.1,2 Thevascular supply is via labial branches of the facial arteryand veins, lying between the orbicularis musculature andoral mucosa.3
The sensory innervation is derived from the mandibularbranch of the trigeminal nerve (V3) via the mental nerve.The motor nerves to the lip muscles arise from the buccaland marginal mandibular branches of cranial nerve VII.The lymphatic drainage of the upper lip and the lateral thirdof the lower lip are to submandibular nodes. The centralthird of the lower lip may drain into the submental lymphnodes on either side.
Basal cell carcinomas (BCCs) develop almost exclusivelyon the upper lip,4 whereas squamous cell carcinomas (SCCs)develop almost exclusively on the lower lip. Only 5% ofsquamous cell cancers of the lips occur on the upperlip.4,5 In contrast to SCCs of the oral cavity, SCCs of the lipsdo not have the tendency for regional lymph node spread.6
Most lip cancers remain localized and grow slowly, with apropensity for superficial rather than vertical spread.Although recommendations on the margin of normal tissue
Figure 1 Tumors type
necessary for adequate cancer resection have varied, a10 mm margin is generally preferred.
The aim of this retrospective study is to report our expe-rience in the treatment of lips tumors with selective combi-nation of treatment modalities.
Patients and methods
From January 1983 to December of 2005, 899 patientsunderwent reconstructive surgery for skin tumors involvingthe lips. All the patients referred to the Second Departmentof Propedeutic Surgery of Athens University and to theDepartment of Plastic Surgery of A Sygros Hospital. Fivehundred and ninety patients were male and 309 patientswere female. In our series, the majority of the patients(516 patients) (57.4%) were between 40 and 70 years oldat the time of the operation. In addition, 326 patients(36.3%) were over 70 years old and only 57 patients (6.3%)were under 40 years old.
SCCs were the most common tumors (467 patients), fol-lowed by BCCs (217 patients), actinic cheilitis (73 patients),leukoplakias (52 patients), hemangiomas (26 patients),malignant melanomas (10 patients) and other types (54 pa-tients). In our series, SCCs were the most frequent skin tu-mors on male patients whereas BCCs were most common onthe female patients. The lower lip was the anatomic zonemost frequently involved in our series (Fig. 1).
Preoperative evaluation of the patients was performedin all cases. In the last five-years, we have performed pre-operative fine needle aspiration (FNA) biopsy of the tumor.The FNA sample was then examined by ThinPrep technique(Cytolyt; Cytyc, Co, Boxborough, MA, USA). The TP smearswere prepared according to directions in the Operator’sManual.7 TP smears of all FNA were prepared from needlerisings obtained following FNA biopsies of lips tumors. The
s according to sex.

206 O. Papadopoulos et al.
collected material was transferred to a vial containing fix-ating (Cytolyt; Cytyc, Co, Boxborough, MA, USA). The sam-ple was then collected after centrifugation of the vial at1300g for 5 min. In cases of bloody samples, additionalCytolyt solution washes were necessary, until the samplebecame clear. The supernatant was then discarded andthe material was transferred to a vial with cytopreserva-tive solution (PreservCyt; Cytyc, Co). The histological re-sult of excised tumor sampling was considered the finaldiagnosis. We performed 170 FNA biopsies. The excised tis-sue was sent for pathological evaluation of the surgicalmargins. The excision was considered wide when the dis-tance between the tumor and surgical margins wasP1.0 cm. Surgical margins were defined as intralesionalif they were microscopically positive; in these cases, wepreferred to perform additional excision before startingthe reconstruction.
Selection of the appropriate operation for the patientwas the most important part of the process, although skill-ful execution of the procedure was also of great impor-tance. Resection of the tumor in each case consisted ofremoval of an adequate margin of healthy tissue, which de-pended on the location, the size of the tumor, and the gen-eral condition of the patient. Patients with cutaneousmelanomas of the lips were treated by excision as deepand wide as indicated, even if reconstruction could be aproblem after such an excision.
The excision of the tumor was followed by a regional ther-apeutic lymph nodes dissection in the cases in which thelymph nodes involvement was clinically evident. We pre-ferred to perform radical neck lymph nodes dissection ratherthan the modified radical neck dissection. Evaluation oflymph nodes status was done by physical examination and/or CT of the head, neck and chest area in cases with palpa-ble lymph nodes or positive sentinel lymph node. Since2004, we have performed sentinel lymph node (SLN) biopsyon patients with SCCs, before tumor excision. We have alsoperformed SLN biopsy on patients with malignant melanoma,since 2000.
The elective reconstructive procedure was performed, inthe majority of the cases, under local anesthesia with seda-tion or general anesthesia and infiltration with xylocaine 1%with epinephrine 1:200000 so as to decrease bleeding. Thechoice of the appropriate reconstructive procedure wasbased upon three major criteria: the size and the locationof the defect after tumor excision and the functional andaesthetic deficit created. The most important aestheticlandmark was the white roll.
Reconstruction of lip defects must have under consid-eration the following principles: (1) Identical or similartissues should be preferred for reconstruction. (2) Thecloser the donor tissue is situated to the defect, themore likely is the tissue match. (3) Natural landmarksand aesthetic units should always be restored. (4) Sym-metry and balance are the mainstays of an aestheticacceptable final result. (5) Proper realignment of theorbicularis oris fibers maintain the sphincter functionand minimizes distortion during facial animation. Whenapproaching lip reconstruction, one should first assessthe lesion and attempt to determine the amount of mu-cosa, muscle, and skin that will be involved before inci-sions are made.
Free skin or mucosa grafts can be used for reconstructionof superficial lip defects or vermilion defects. On the otherhand, full thickness lip defects can be restored with eitherwedge excision and direct closure if the defect is 61/3 ofthe lip length or local or regional flaps if the defect is>1/3 of the lip length.
Results
Surgical procedures were tolerated well by all the patients.Average hospital stay was 1–2 days for the inpatients,including those who had staged operations or complicationnecessitating second operation. The results were estimatedfrom an oncological, functional, and aesthetic point ofview.
Using the TP technique adequate material was observedin 162 out of 170 examined lesions. The TP technique suc-cessfully established the benign (15 actinic cheilitis, 10 leu-koplakias, seven labial lentigines) or malignant (70 SCCs, 54BCCs, four malignant melanomas) nature of the lesions inthe 160 cases out of 162 cases with adequate material(Fig. 2). The eight cases with inadequate material includedone case of SCC, two cases of actinic cheilitis, two cases ofleukoplakia, two cases of kaposi sarcomas and one case ofmetastatic adenocarcinoma. In the two cases of SCCs TPtechnique revealed only normal cells.
TP technique results were correlated with the final histo-logical diagnosis. Of the 73 cases of SCCs confirmed by his-tological diagnosis, 70 were also revealed by TP. Of the 54cases of BCCs confirmed by histological diagnosis, 54 werealso revealed by TP. Of the 17 cases of Actinic Cheilitis con-firmed by histological diagnosis, 15 were also revealed byTP. Of the 12 cases of leukoplakias confirmed by histologi-cal diagnosis, 10 were also revealed by TP. In five patientswith SCCs the histological examination was repeated twotimes so that the pathologist could reach a diagnosiswhich was also revealed by TP. The reliability of the TPtechnique was evaluated by the determination of sensitiv-ity, specificity, positive predictive value (PPV), negativepredictive value (NPV), and overall accuracy (OA) (Tables1 and 2).
We performed 10 radical neck lymph nodes dissections.SLN biopsy was done on 15 patients with SCCs (11 patients)and malignant melanoma (four patients). The result wasnegative on 10 cases. The next step of the operation wasthe repair of the defect
Excision of the tumor was followed by reconstruction ofthe defect. We performed wedge excision in the form of a Vor W and direct closure on 573 cases, total vermilioectomyon 291 cases, various types of flaps on 120 cases and fullthickness skin grafts on two cases. All the above are summa-rized in Table 3.
Patients were examined at least three times in the firstpostoperative year and one time from second to fifth post-operative year during routine follow-up. Only 550 patientshad sufficient medical records with a five year follow-up,while for 100 patients follow-up was short. There was insuf-ficient data for 249 patients. Out of stayed patients com-bined with low socioeconomic and mental status patientswere the main reasons for this high percentage of insuffi-cient medical records, concerning our study. Follow-up

Table 1 Correlation between TP technique results andhistological diagnosis
Results TP Histological diagnosis
SCCs 70 73BCCs 54 54Actinic chelitis 15 17Leukoplakias 10 12Labial lentigines 7 7Malignant melanomas 4 4Kaposi sarcomas 0 2Metastatic adenocarcinoma 0 1Inadequate material 8 0With normal limits 2 0
Total 170
Table 3 Surgical procedures
Type of surgical treatment Patients
Excision–direct closure 573Vermilioectomies 291Flaps 120(1) LocalAbbe’s flap 66Estlander’s flap 20Dufourmentel’s flap 21Nasolabial flap 7Various 3(2) Regional 1Frontal 1Platysma 1Pectoralis major flapSplit thickness skin graft 2
Table 4 Follow-up of the patients
Patients
Five-year follow-up 550Insufficient medical records 249Follow-up < 1 year 100
Figure 2 (a) Basal cell carcinoma of the lip (PAP ·40, Papanicolaou Stain, magnification ·40). (b) Squamous cell carcinoma of thelip (PAP ·40, Papanicolaou Stain, magnification ·40). (c) Malignant melanoma of the lip (PAP ·40, Papanicolaou Stain, magnification·40).
Lip defects due to tumor excision 207
was done on all patients mostly by the operating surgeon.All the above are summarized in Table 4.
Complications were divided into two groups: (1) Earlycomplications, which occurred during the first month. Weobserved three patients with hematoma formation, and 15patients with wound infection. (2) Late complications,which occurred after the first month. We noticed one deathfrom a recurrent SCC. Moreover, we observed 62 patients
Table 2 TP technique diagnostic accuracy
Type of diagnosis Sensitivity Specifity PPV NPV OA
TP technique 98.68% 100.00% 100.00% 83.33% 98.76%
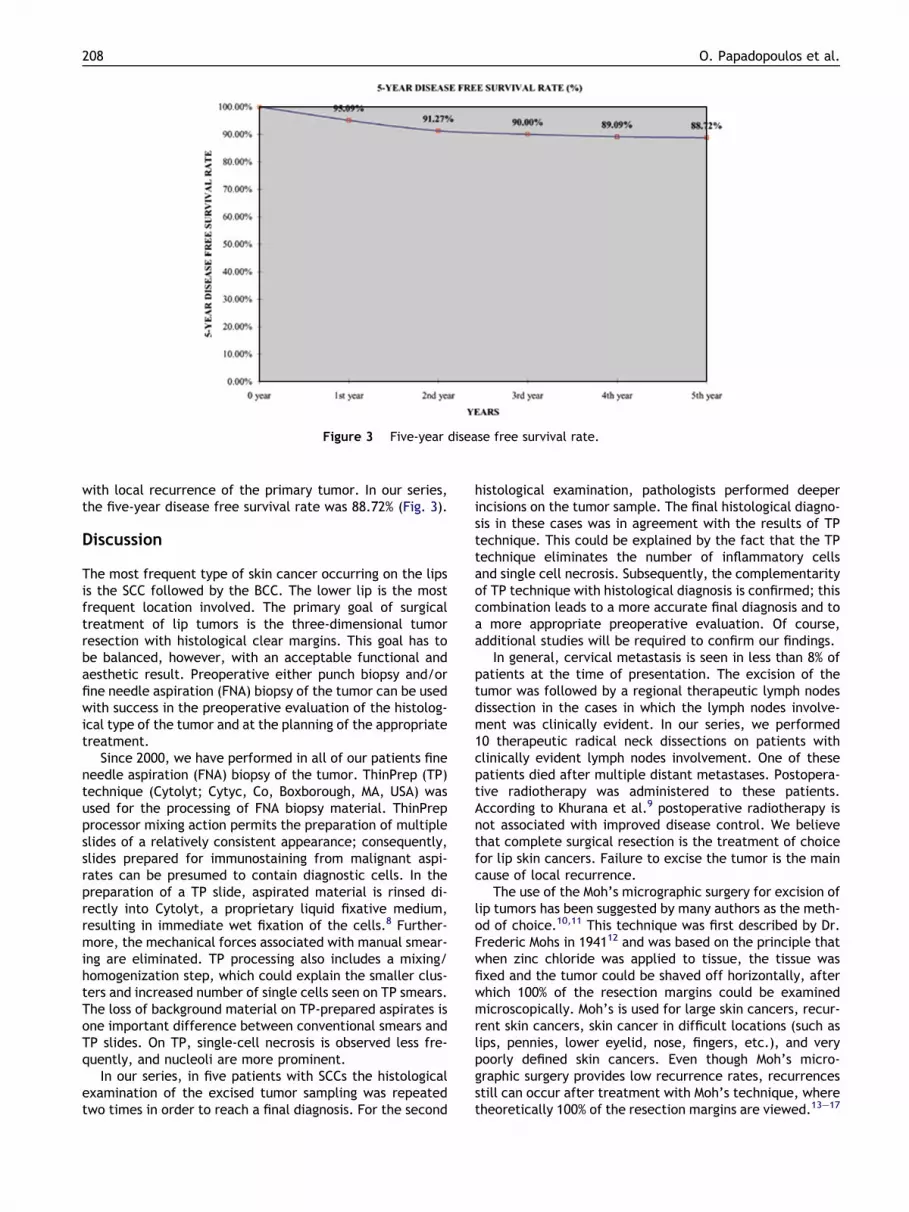
Figure 3 Five-year disease free survival rate.
208 O. Papadopoulos et al.
with local recurrence of the primary tumor. In our series,the five-year disease free survival rate was 88.72% (Fig. 3).
Discussion
The most frequent type of skin cancer occurring on the lipsis the SCC followed by the BCC. The lower lip is the mostfrequent location involved. The primary goal of surgicaltreatment of lip tumors is the three-dimensional tumorresection with histological clear margins. This goal has tobe balanced, however, with an acceptable functional andaesthetic result. Preoperative either punch biopsy and/orfine needle aspiration (FNA) biopsy of the tumor can be usedwith success in the preoperative evaluation of the histolog-ical type of the tumor and at the planning of the appropriatetreatment.
Since 2000, we have performed in all of our patients fineneedle aspiration (FNA) biopsy of the tumor. ThinPrep (TP)technique (Cytolyt; Cytyc, Co, Boxborough, MA, USA) wasused for the processing of FNA biopsy material. ThinPrepprocessor mixing action permits the preparation of multipleslides of a relatively consistent appearance; consequently,slides prepared for immunostaining from malignant aspi-rates can be presumed to contain diagnostic cells. In thepreparation of a TP slide, aspirated material is rinsed di-rectly into Cytolyt, a proprietary liquid fixative medium,resulting in immediate wet fixation of the cells.8 Further-more, the mechanical forces associated with manual smear-ing are eliminated. TP processing also includes a mixing/homogenization step, which could explain the smaller clus-ters and increased number of single cells seen on TP smears.The loss of background material on TP-prepared aspirates isone important difference between conventional smears andTP slides. On TP, single-cell necrosis is observed less fre-quently, and nucleoli are more prominent.
In our series, in five patients with SCCs the histologicalexamination of the excised tumor sampling was repeatedtwo times in order to reach a final diagnosis. For the second
histological examination, pathologists performed deeperincisions on the tumor sample. The final histological diagno-sis in these cases was in agreement with the results of TPtechnique. This could be explained by the fact that the TPtechnique eliminates the number of inflammatory cellsand single cell necrosis. Subsequently, the complementarityof TP technique with histological diagnosis is confirmed; thiscombination leads to a more accurate final diagnosis and toa more appropriate preoperative evaluation. Of course,additional studies will be required to confirm our findings.
In general, cervical metastasis is seen in less than 8% ofpatients at the time of presentation. The excision of thetumor was followed by a regional therapeutic lymph nodesdissection in the cases in which the lymph nodes involve-ment was clinically evident. In our series, we performed10 therapeutic radical neck dissections on patients withclinically evident lymph nodes involvement. One of thesepatients died after multiple distant metastases. Postopera-tive radiotherapy was administered to these patients.According to Khurana et al.9 postoperative radiotherapy isnot associated with improved disease control. We believethat complete surgical resection is the treatment of choicefor lip skin cancers. Failure to excise the tumor is the maincause of local recurrence.
The use of the Moh’s micrographic surgery for excision oflip tumors has been suggested by many authors as the meth-od of choice.10,11 This technique was first described by Dr.Frederic Mohs in 194112 and was based on the principle thatwhen zinc chloride was applied to tissue, the tissue wasfixed and the tumor could be shaved off horizontally, afterwhich 100% of the resection margins could be examinedmicroscopically. Moh’s is used for large skin cancers, recur-rent skin cancers, skin cancer in difficult locations (such aslips, pennies, lower eyelid, nose, fingers, etc.), and verypoorly defined skin cancers. Even though Moh’s micro-graphic surgery provides low recurrence rates, recurrencesstill can occur after treatment with Moh’s technique, wheretheoretically 100% of the resection margins are viewed.13–17

Lip defects due to tumor excision 209
Eliezri et al., and Dzubow both report cases where the scartissue (in case of biopsy scar or a recurrent BCC) is not com-pletely excised and therefore tumor is missed.13,14 More-over, skin carcinomas may sometimes recrudesce,independently of the clear limits of the lesion. We preferto remove completely the tumor en block with a safety mar-gin of adjacent normal tissue in all directions, minimizingthe probability of recurrence.
Since 2000, we have used sentinel lymph node (SLN)biopsy in cases of cutaneous melanoma of the lips. After2004 we have used SLN biopsy in cases of neglected SCCsof the lips (diameter P 2 cm). The technique of intraopera-tive lymphatic mapping and selective lymphadenectomywas introduced for melanoma patients by Morton et al.18
Because of the successful results with melanoma, investiga-tors tried to incorporate the technique into the treatmentof several other solid skin tumors such as SSCs. The risk ofregional lymph node metastases is 4% for T1 lesions and20% for T2 or greater lesions. Because of the relativelylow incidence of nodal metastasis in T1 lesions, primaryexcision of the tumor with adequate margins is often suffi-cient for cure. We prefer the SLN biopsy especially to theyoungest patients with central tumor location, from anunnecessary lymph node dissection of the area. The abilityof sentinel lymphadenectomy to identify regionally meta-static cutaneous SCC remains to be further clarified.19
After tumor resection, the aims of reconstruction mustbe to maintain oral competence, maximum oral aperture,mobility, sensation when possible, and maximize aestheticresult. The restoration of a natural appearance should notbe the only mainstay of reconstruction; adequate lip func-tion is of equal importance. When defects involve more thanone lip, more complex reconstructive procedures are re-quired. The lip curtain must be of adequate height, sen-sated and possess adequate extrinsic and intrinsicmusculature.
The lower vermilion is the most common site of neoplas-tic lesions since it is the target of solar radiation injury.Small lesions can be excised in fusiform fashion and closedprimarily. Incisions should be placed in the radially orientedrelaxed skin tension lines.3 When the defect is limited toless than one third of the lower vermilion, a vermilion–mus-cle advancement flap based on the axial labial artery maybe used to resurface the area of the defect.20 When simpleadvancement is inadequate, a triangular musculomucosalV–Y advancement flap can be used. Kawamoto21 describeda vermilion lip switch flap for correction of cases involvinglarge defects of vermilion. A transverse, centrally basedmusculomucosal flap is designed on the lower lip and thenis elevated and turned upward 180� and sutured into thedeficient portion of the upper lip. The flap is divided at12–14 days. In cases of extensive premalignant lesions ofthe lip vermilioectomy is indicated. In this operation thevermilion is resected from the white roll to the contact areaof the upper and lower lip. Repair of the defect is done byadvancement of labial mucosa, which is then redraped overthe underlying orbicularis musculature. The plane of dissec-tion is between the uninvolved mucosa and underlying mus-culature. This method decreases the inward retraction ofthe lip, which occurs with primary closure, avoiding irrita-tion by the lower lip hairs, and producing a better contour.
Tongue mucosal flaps22–25 have been described for ver-milion reconstruction. They are rarely preferred becausethey are an unpleasant experience for the patient.
Reconstruction of lower lip defects is eased by the lackof a dominant central structure such as the philtrum, andthe greater laxicity of soft tissues. These properties allowfor better mobilization of tissues adjacent to the defectwithout causing obvious distortion. Defects 61/3 of the hor-izontal length of the lower lip may be repaired with directclosure in three layers: mucosa, muscle, and skin. The pa-tient’s age, elasticity, and redundancy of adjacent soft tis-sue determine the size of the defect that can be closeddirectly.
In our series, we used the rhomboid-shaped transpositionflap of Dufourmentel26 for cutaneous small defects of theupper or lower lip. The flap is located next to the primary de-fect in a way that facilitates direct closure of the donor site.
Four flaps are mainly used for repair of defects withlength between 1/3 and 2/3 of the horizontal length ofthe lower lip (medium defects). These are the Abbe flap,the Karapandzic flap, the Bernard–Burow’s procedure andthe Estlander flap.
The Abbe flap27 (Fig. 4) can be used for medium defectswhich do not involve the commissure and in cases wherethere is sufficient lower lip tissue for reconstruction. Theflap is designed at the junction of the middle and lateralthirds of the upper lip so that neither the philtrum nor thecommissure is affected. Then the flap is elevated and ro-tated along the vascular pedicle so as to fill the defect.The main potential disadvantages of this procedure are:(1) the total flap loss either intraoperatively or postopera-tively, (2) the fact that it is a two stage reconstruction be-cause the pedicle of the flap is divided after 14–21 days andthe patient remains for this period of time with his lips ap-posed. The aesthetic result is generally better than thatseen with the Bernard–Burow’s procedure and the Kara-pandzic flap.
The Karapandzic flap28 is mainly used for medium lowerlip defects that do not require new lip tissue for reconstruc-tion and that are either located centrally or more laterallywhere they involve a portion of the commissure. The incisionis carried circumorally to the alar base bilaterally. The inci-sion is made in full thickness through skin, muscle, and mu-cosa medially. Laterally, at the level of the commissures theskin is incised only down to subcutaneous tissue. The flapsare rotated inward to fill the defect. The oral sphincter re-mains intact and functional after this procedure. The mainpotential disadvantages of this procedure are: (1) unsightlyscarring, (2) the potential for microstomia which can be par-ticularly troublesome to patients who use dentures.
The Bernard–Burow’s procedure is used for reconstruc-tion of the lower lip in cases where there is not adequatelip soft tissue after tumor excision. In the original opera-tion, full-thickness triangles of cheek tissue are excised oneach side of the upper lip, providing relief room for the low-er cheek flaps to be advanced medially. This original opera-tion has undergone multiple modifications which aim atimproving the functional and aesthetic result. Main poten-tial disadvantages of this procedure are: (1) incompleterecovery of sensation and mobility in the lip tissue, (2) scarcontracture at the commissure causing an unusual ‘smiley

Figure 4 (a) Squamous cell carcinoma of the lower lip. (b) Abbe flap and its pedicle. (c) Final result. (d) Natural appearance of thelower lip.
210 O. Papadopoulos et al.
face’, (3) color mismatch of the reconstructed vermilionwith adjacent vermilion, (4) drooling. Through modifica-tions by Freeman29 and Webster et al.30 skin and subcutane-ous tissue are excised in a more lateral position placing thescar in the nasolabial fold and resulting in improved postop-erative sensation of the reconstructed lip.
The Estlander flap is used for reconstructions of defectsthat involve the commissure and is impossible to be repairedby the Karapandzic flap. It is a laterally based lip switchflap, pivoting around the corner of the mouth. The flap isdesigned on the upper lateral lip at a size equivalent toone half of the lower lip defect. This is a one step procedureand it has the same potential disadvantages like Abbe pro-cedure with one main exception, the rounded appearancewith poor angle definition of the commissure.
Reconstruction of defects P2/3 of the horizontal lengthof the lower lip (large defects) is a challenging problem. Areasonable degree of oral function and competence arethe mainstays in this type of reconstruction. When there issufficient remaining lip or cheek tissue the Bernard’s proce-dure is the method of choice for reconstruction of large low-er lip defects. Another choice is the Karapandzic flap whichis used for repair of medially located large lower lip defects.In massive lip defects free tissue transfer or a distant pedi-
cle flap provides the most consistent results. We prefer theuse of the pedicled musculocutaneous flap of platysma forfilling such defects. In cases where the defect involves themandible, an osteomusculocutaneous flap (either free orpedicled) should be used for reconstruction. We use thepedicled musculocutaneous flap of pectoralis major musclecombined with the 4th rib for reconstruction of this type ofdefects (Fig. 5).
Upper lip defects due to tumor excision are less commonthan lower ones. Reconstruction of upper lip defects is moredifficult due to the presence of central structures-like nose,columella. Regional and distant flaps for repair of upper lipdefects may provide more acceptable functional and aes-thetic results than comparable procedures for the lower lip.
Reconstruction of small upper lip defects (61/3 of thehorizontal length of the lip) depends on the location ofthe defect. When the defect involves only the upper lip tis-sue, with intact vermilion, a nasolabial flap from the ipsilat-eral side can be used for repair of the defect. The flap (skinand subcutaneous tissue) is either superiorly or inferiorlybased and is rotated into place from a position adjacentto the defect. The donor side is closed primarily along thenasolabial fold. Laterally located defects can be closed withprimary closure. Medially located defects can be closed with

Figure 5 (a) Squamous cell carcinoma of the lower lip involving the mandible. (b) Resection of the tumor and part of themandible. (c) Pedicled musculocutaneous flap of pectoralis major muscle combined with the fourth rib for reconstruction of thedefect. (d) Final result.
Lip defects due to tumor excision 211
direct closure after perialar crescentic skin excisions andrelease of upper buccal sulcus to allow medial advancementof the lip tissue. The excision involves skin and subcutane-ous tissue.
Location of the defect is the main criterion for the typeof reconstruction of medium defects of the upper lip (>1/3and 62/3 of the horizontal length of the lip). Centrally lo-cated defects can be closed after perialar crescentic exci-sions either with primary closure if the defect is <1/2 ofthe horizontal length of the upper lip or with the use of
Figure 6 Five-year recurrence rate acc
an Abbe flap or a Karapandzic flap for defects >1/2 of thehorizontal length of the upper lip. We believe that for thesedefects the use of an Abbe flap is the best choice for recon-struction due to better functional and aesthetic results. Lat-erally positioned medium defects must be considered in thecontext of presence or absence of commissure involvement.When the commissure is not involved an Abbe flap can beused for repair of the defect. An Estlander flap can be usedfor filling of the defect when there is involvement of thecommissure. If the defect involves the philtrum, the combi-
ording to type of surgical treatment.

212 O. Papadopoulos et al.
nation of a controlateral perialar crescentic excision withthe use of an Estlander flap is the method of choice for re-pair of the defect.
Repairing of large upper lip defects (>2/3 of the horizon-tal length of the lip) depends on the adequacy or not of theadjacent cheek tissues. When there are adequate adjacentcheek tissues for reconstruction the method of choice is theBernard–Burow’s procedure. The upper lip is replaced withmidcheek tissue. Burow’s triangles are excised laterally tothe lower lip, on both sides, and laterally to each alar base.The triangular excisions involve only skin and subcutaneoustissue. The cheek tissue is then advanced medially to createthe new upper lip. Vermilion reconstruction is undertakenusing mucosa from the advanced cheek flaps. Laterallylocated large upper lip defects can be repaired with thecombination of a unilateral upper lip Bernard–Burow’sprocedure and a controlateral perialar crescentic excision.When there is inadequate adjacent cheek tissue for recon-struction free tissue transfer or a distant pedicle flap canbe used for filling the defect.
A successful reconstruction should derive from carefulpreoperative planning, knowledge of the anatomy, and useof sound surgical techniques. Flawless operative techniqueis important for a successful outcome. The use of prophylac-tic perioperative antibiotics is imperative. Gentle handlingof tissues, meticulous hemostasis, and judicious placementof drains are of paramount importance. Careful postopera-tive wound inspection is necessary, for the early detectionof septic complications or wound healing impairment.
In our series, from the 550 patients who had a five-yearfollow-up we observed 62 recurrences of the primary tumor.The five-year recurrence rate was 11.28%. According to typeof surgical treatment, surgical excision followed by directclosure was the type of surgery with the highest five-yearrecurrence rate (10.82%), even though the histological diag-nosis was negative for positive margins in the majority ofcases (Fig. 6). We believe that these findings were due tolimited margin of adjacent normal tissue and the low gradeof differentiation of these tumors. Ancillary studies areneeded to confirm our findings.
In conclusion, we suggest that postoperatively, patientsshould have systemic annual follow-ups. Individual riskassessment should be routine, and those at a particular highrisk, such as those with previous skin tumors, require moreintensive monitoring. It is essential for the plastic andreconstructive surgeon to be familiar with the particularprocedures used in eyelid reconstruction. He should haveclose cooperation with the patient to succeed in performinga suitable outcome.
References
1. Freilinger G, Gruber H, Happak W, Pechmann U. Surgicalanatomy of the mimic muscle system and the facial nerve:Importance for reconstructive and aesthetic surgery. PlastReconstr Surg 1987;80:686–90.
2. Zide BM. Deformities of the lips and cheeks. In: McCarthy JG,editor. Plastic Surgery, Vol. 3. Philadelphia: WB SaundersCompany; 1990. p. 2009–56.
3. Galyon SW, Frodel JL. Lip and perioral defects. OtolaryngolClin North Am 2001;34:647–66.
4. Zitsch RP. Carcinoma of the lip. Otolaryngol Clin North Am1993;26:265–77.
5. Cruse CW, Radocha RF. Squamous cell carcinoma of the lip.Plast Reconstr Surg 1987;80:787–91.
6. Luce EA. Carcinoma of the lower lip. Surg Clin North Am1986;66:3–11.
7. Cytyc ThinPrep 2000 Operator’s Manual, . Boxborough(MA): Cytyc; 1997.
8. Silverman JF, Finley JL, O’Brien KF, et al. Diagnostic accuracyand role of immediate interpretation of fine needle aspirationbiopsy specimens from various sites. Acta Cytol1989;33:791–6.
9. Khurana VG, Mentis DH, O’Brien CJ, Hurst TL, Stevens GN,Packham NA. Parotid and neck metastases from cutaneoussquamous cell carcinoma of the head and neck. Am J Surg1995;170(5):446–50.
10. Mohs F. Chemosurgery: A microscopically controlled method ofcancer excision. Arch Surg 1941;42:279–95.
11. Baker NJ, Webb AA, Macpherson D. Surgical management ofcutaneous squamous cell carcinoma of the head and neck. Br JOral Maxillofac Surg 2001;39:87–90.
12. Zide MF, Adnot J. Lower lip cancer: Mohs micrographic surgeryand reconstruction as a multidisciplinary effort. J Oral Max-illofac Surg 1997;55:818–25.
13. Eliezri YD, Cohen PR. Cancer recurrence following Mohsmicrographic surgery: A mechanism of tumor persistence. PlastReconstr Surg 1992;90:121–5.
14. Dzubow LM. False-negative tumor-free margins following Mohssurgery. J Dermatol Surg Oncol 1988;14:600–2.
15. Smeets NW, Stavast-Kooy AJ, Krekels GA, et al. Adjuvantcytokeratin staining in Mohs micrographic surgery for basal cellcarcinoma. Dermatol Surg 2003;29:375–7.
16. Hruza GJ. Mohs micrographic surgery local recurrences. JDermatol Surg Oncol 1994;20:573–7.
17. Rapini RP. Pitfalls of Mohs micrographic surgery. J Am AcadDermatol 1990;22:681–6.
18. Morton DL, Wen DR, Wong JH, et al. Technical details ofintraoperative lymphatic mapping for early stage melanoma.Arch Surg 1992;127:392–9.
19. Kontio R, Leivo I, Leppanen E, Atula T. Sentinel lymph nodebiopsy in oral cavity squamous cell carcinoma without clinicallyevident metastasis. Head Neck 2004;26:16–21.
20. Goldstein MH. A tissue expanding vermilion myocutaneous flapfor lip repair. Plast Reconstr Surg 1984;73:768–70.
21. Kawamoto HK. Correction of major defects of the vermilionwith a cross-lip vermilion flap. Plast Reconstr Surg1979;64:315–8.
22. Guerrero-Santos J. Use of a tongue flap in secondary correctionof cleft lips. Plast Reconstr Surg 1969;44:368–71.
23. Jackson IT. Use of tongue flaps to resurface lip defects andclose palatal fistulae in children. Plast Reconstr Surg1972;49:537–41.
24. Guerrero-Santos J, Castaneda A, Barba JA. Surgery for correc-tion of labial angiomas. Arch Surg 1967;94:728–33.
25. Zarem HA, Greer Jr DM. Tongue flap for reconstruction of thelips after electrical burns. Plast Reconstr Surg 1974;53:310–2.
26. Dufourmentel G. Le fermetur des pertes de substance cutaneelimitees. Ann Chir Plast 1962;7:61.
27. Abbe R. A new plastic operation for the relief of deformity dueto double harelip. Plast Reconstr Surg 1968;42:481–3.
28. Karapandzic M. Reconstruction of lip defects by local arterialflaps. Br J Plast Surg 1974;27:93–7.
29. Freeman BS. Myoplastic modification of the Bernard cheilo-plasty. Plast Reconstr Surg 1958;21:453–60.
30. Webster RC, Coffey RJ, Kelleher RE. Total and partial recon-struction of the lower lip with innervated muscle bearing flaps.Plast Reconstr Surg 1960;25:360–71.




























