Embed Size (px)
Citation preview

SUPERFIClAL BLADDER CANCER: NEW STRATEGIES IN DIAGNOSIS AND TREATMENT 0094-0143/00 $8.00 + .OO
MUTATION OF CELL CYCLE REGULATORS AND THEIR IMPACT
ON SUPERFICIAL BLADDER CANCER
Farhang Rabbani, MD, FRCSC and Carlos Cordon-Cardo, MD, PhD
Bladder cancer is one of the most common malignancies occurring worldwide. The rates for these tumors are highest in developed countries, where they rank as the sixth most frequent neoplasm.189 Bladder cancer devel- ops more predominantly in males, with a sex ratio of 3 to 1, suggesting sex-linked etiologic factors. In the United States, bladder cancer ranks as the fourth most common malignancy among men and the sixth most common among women. Approximately 90% of malig- nant tumors arising in the urinary bladder are of epithelial origin, the majority being transitional cell carcinomas (TCC), which are the focus of this review.Iz4
The proper diagnosis, management, and overall control of bladder cancer are major clinical challenges in oncology. Because the modality of therapy primarily depends on morphologic evaluation and clinical staging, the diagnosis carries significant conse- quences. The natural history of bladder can- cer has revealed that morphologically similar tumors presenting in any assigned stage or grade may behave in radically different fash- i o n ~ . ” ~ This observation has precluded the ability to predict clinical outcome in a given case. Recently, new information has become
available regarding the principles that govern the cell cycle and cell fate. Moreover, clinical and basic research has linked mutations of genes known to be involved in regulating cell cycle and apoptotic pathways with underly- ing processes of tumorigenesis and tumor progression.
Based on morphologic evaluation and natu- ral history, urothelial neoplasms have been classified into two groups having distinct be- havior and prognosis: (1) low-grade tumors (always papillary and usually superficial) and (2) high-grade tumors (either papillary or nonpapillary and often invasive).lz4 Clinically, superficial bladder tumors (stages Ta, Tis, and T1) account for 75% to 85% of neoplasms, whereas the remaining 15% to 25% are inva- sive (T2, T3, T4) or metastatic (N+ , M + ) lesions at the time of initial presentation. More than 70% of patients with superficial tumors have one or more recurrences after initial treatment, and about one third of these patients have progression of disease and eventually die. For these reasons, new meth- ods are needed to identify and monitor pa- tients presenting with high-risk superficial tu- mors who are at risk for recurrent and invasive carcinoma. Additional problems
From the Department of Urology (FR) and the Department of Pathology (CCC), Memorial Sloan-Kettering Cancer Center, New York, New York
UROLOGIC CLINICS OF NORTH AMERICA
VOLUME 27 - NUMBER 1 - FEBRUARY 2000 83
84 RABBANI & CORDON-CARD0
arise in patients who present with invasive disease. Despite aggressive surgical resection and adjuvant radiotherapy, chemotherapy, or both, the overall cure rate is limited to 20% to 50%. Because selection criteria to determine treatment for a particular tumor in a particu- lar patient are incompletely defined, new bio- logic determinants are needed for proper se- lection and monitoring of therapy in patients with bladder tumors.
CHROMOSOMAL ALTERATIONS IN BLADDER CANCER
Cytogenetic Studies
Genetic Studies
Genetic changes in bladder cancer were first identified by cytogenetic studies. Unlike leukemias in which the most common cytoge- netic changes are translocations, bladder can- cers more commonly have structural and nu- merical chromosome changes. Initial studies identified monosomy of chromosome 94, 43 and interstitial deletions of chromosome 1343 as frequent events. In a review of the litera- ture, Sandberg and Bergerlz7 found that the most common cytogenetic changes in de- creasing order of frequency were -9 or 9q-, +7,1p-, lq-, 5q-, i(5p), l lp-, 6p-, 6q-, 17p-, 2q-, 3p-, +8, +ll, 21q-, and -Y.
Fluorescence In Situ Hybridization
Fluorescence in situ hybridization (FISH) is a technique using nonradioactive centromere- specific probes to study numerical chromo- some aberrations."' The advantages of FISH assays over cytogenetic studies are that cells need not be dividing and smaller samples can be used; however, the disadvantage is that with centromeric probes, deletions and trans- locations cannot be identified. This technique is more sensitive than flow cytometry for the detection of quantitative DNA aberrations.'%
Using FISH assays, Hopman and co-work- e r ~ ~ ~ reported monosomy for chromosome 9 in 9 of 24 low-grade TCCs and trisomy for chromosomes 1, 7, and 11 in five, two, and one case, respectively. Smeets and co-work-
e r ~ ~ ~ ~ compared karyotyping and FISH for the detection of numerical chromosome 9 aberra- tions, and found concordance between the two techniques. FISH complements classical chromosome counting and flow cytometry, allowing efficient recognition of the chromo- somes involved in cases in which there is an imbalance between different chromo- s o m e ~ . ~ ~ , 138 Nevertheless, interlaboratory studies of FISH have shown that variability in FISH results increases significantly when analysis is performed in two separate labora- t ~ r i e s . ~ ~
In a study using FISH with pericentromeric sequence-specific DNA probes, Waldman and c o - w ~ r k e r s ~ ~ ~ identified monosomy of chro- mosome 9 in 8 of 21 cases of superficial TCC and tetrasomy for chromosome 7 and 11 in 6 of 22 cases and 5 of 20 cases of superficial TCC, respectively. Sandberg and BergerlZ7 re- ported loss of chromosome 9 in near diploid low-grade tumors and gains in the number of chromosomes 7, 8,4 and 20. Loss of chromo- some 9 may be underrepresented in high ploidy tumors, whereas the extra chromo- somes 7, 8, 4, and 20 could be spurious (ow- ing to the polyploid status of the tumors).127 Wagner and c o - w ~ r k e r s ~ ~ ~ identified a sig- nificant difference in the incidence of 8p22 deletions between pTa tumors (3 of 33) and pT1 tumors (8 of 19) (P=O.O05).
Study of more specific molecular alter- ations has been possible using gene-specific probes in interphase cytogenetics to assess gene amplification and specific gene losses. Using a dual labeling hybridization assay, Sauter and c o - w ~ r k e r s ~ ~ ~ reported E X B B - 2 amplification in 10 of 141 bladder tumors. Amplification of ERBB-2 was found only in tumors with aneusomy of chromosome 17 and was more common in pT2-pT4 (9 of 64) than in pTa-pT1 (1 of 68) tumors (P=O.O13). All tumors with ERBB-2 amplification dem- onstrated erbB-2 overexpression. Other inves- tigators have reported overexpression of c- erbB-2/neu in as many as 99 of 249 (39%) cases of TCC.79 In another experiment using a similar dual-labeling hybridization technique, Sauter and c o - w ~ r k e r s ~ ~ ~ identified a clean- cut MYC amplification (40 to 150 copies/ cell) in 3 of 87 bladder tumors, with low-level MYC amplification in 32 of the remaining 84
MUTATION OF CELL CYCLE REGULATORS AND SUPERFICIAL BLADDER CANCER 85
tumors. Low-level MYC gains were signifi- cantly more frequent in lower stage and lower grade tumors, suggesting a role for chromosome 8 alterations in bladder cancer progression.
Using a similar approach, TP53 gene dele- tion was identified in 4 of 43 pTa tumors, 18 of 43 pT1 tumors, and 29 of 58 pT2-pT4 tu- mors ( P = O.OOOl), correlating with grade as well.132 Other researchers have also demon- strated a correlation between TP53 deletion and grade, stage, S-phase fraction, and DNA pl0idy.8~ FISH analysis has demonstrated nul- lisomy for chromosome Y in 23 of 68 (34%) tumors; however, this finding did not corre- late with tumor grade, stage, or Ki67 stain- ing.137 Neuhaus and c o - w ~ r k e r s ~ ~ ~ studied 105 bladder tumors (67 pTa, 38 pT1) by FISH using centromere probes for chromosome Y, 1, and 17. In pTa tumors, polysomies of chro- mosome 1 and 17 were associated with an increased risk of recurrence and polysomy 17 with an increased risk of progression; how- ever, no association between polysomy and prognosis was identified in pT1 tumors. Pol- ysomy Y did not impart a worse prognosis in either pTa or pT1 tumors. Nemoto and co- workers102 have also reported that the per- centage of hyperdiploid cells for chromo- somes 7, 11, and 17 is highly correlated with increasing grade and stage. Balhzs and col- leagues6 studied 17 superficial bladder tu- mors for genomic deletions at 9p21 using gene-specific probes for the CDKN2 and IFNA genes. They found homozygous deletions for CDKN2 without homozygous IFNA deletion in 5 of 17 tumors, deletion of IFNA without deletion of CDKN2 in one tumor, and deletion of both genes in one tumor.
Recently, this approach has been applied together with microdissection techniques to study the earliest molecular alterations in tu- morigenesis. Hartmann and co-workerss mi- crodissected urothelium from 12 patients with urothelial hyperplasia and simultaneous or subsequent superficial papillary tumors. Ad- ditionally, 12 biopsy specimens with histolog- ically normal urothelium were studied. Ten of 14 (71%) hyperplasias showed monosomies or partial deletions of chromosome 9 (nine at 9p21, five at 9q22). In seven of eight patients with genetic alterations in the hyperplasias,
the genetic change was also present in the papillary tumor. Six of 12 normal urothelium samples also demonstrated chromosome 9 al- terations. Sauter and co-w~rkers '~~ also found no association between loss of chromosome 9 and increased grade or stage, p53 expression, or Ki67 staining. Together, these studies indi- cate that loss of chromosome 9 is an early event in bladder cancer development.
Fluorescence in situ hybridization has also been used to study urine and bladder wash
w o r k e r ~ ~ ~ prospectively evaluated 40 bladder wash samples (26 TCC, 14 benign lesions by histologic confirmation) by conventional cy- tology, flow cytometry, and FISH to detect aberrations on chromosomes 8 and 12. There was concordance among the three techniques in 19 of 31 samples (61%). The false-negative and false-positive rates were 38.5% and O%, respectively, for cytology, 28.5% and 20%, re- spectively, for flow cytometry, and 27% and 0%, respectively, for FISH.
specimens.15, 89, 118. 123, 178. 188 Cajulis and co-
Comparative Genomic Hybridization
Comparative genomic hybridization (CGH) allows detection of losses and gains of DNA sequences as a function of chromosome loca- tion throughout the genome, based on simul- taneous hybridization of differentially labeled tumor and normal DNA to normal chromo- some spreads. Use of CGH has identified ge- netic alterations at loci previously unreported in bladder cancer.66 Analysis of 26 bladder tumors by CGH revealed losses on Up, llq, 8p, 9, 17p, 3p, and 12q in more than 20% of tumors and gains in over 10% at 8q21, 13q21- 34, lq31, 3q24-26, and 1 ~ 2 2 . ~ Voorter and ~ o - w o r k e r s ~ ~ ~ compared CGH analysis in 14 bladder TCCs with restriction fragment length polymorphism (RFLP) analysis and FISH, identifying distinct amplifications on
and 22q11-13. Sauter and co-w~rkers '~~ ana- lyzed 79 bladder tumors (28 pTa, 28 papillary pT1,23 pT2-pT4) by CGH. pTa tumors had a lower number of aberrations than pT1 lesions: mean, 2.3 for pTa versus 6.5 for pT1; mean deletions, 1.4 for pTa versus 3.1 for pT1; mean gains, 0.9 for pTa versus 3.5 for pT1; mean amplifications, 0.1 for pTa versus 0.5 for pT1.
3~22-24, 10~13-14, 12q13-15, 17q22-23, 18pl1,
86 RABBANI & CORDON-CARD0
The most frequent (>lo%) alterations in pTa tumors were deletions of 9q (15 of 28) and 9p (11 of 28), gains of l q (4 of 28), and losses of chromosome Y (7 of 25). The most frequent alterations in pT1 tumors were deletions at the Y chromosome (8 of 18), 2q (10 of 28), 8p (9 of 28), 9p (5 of 28), 9q (5 of 28), l lq (7 of 28), and l l p (6 of 28) and gains of l q (15 of 28), 3p (5 of 28), 6p (5 of 28), 8q (10 of 28), lop (5 of 28), 17q (8 of 28), and 20q (5 of 28). A similar number and type of aberrations were found in pT2-pT4 tumors as in pT1 tu- mors.
The major strength of CGH is amplification detection, with high-level amplification found at 1q22-24, 3p24-25, 5p15, 6p22, 8q21-22,
20q13, Xpll-13, and Xq21.135 Mahdy and asso- ciatesH3 reported that the chromosomal aber- ration detection rate by FISH for chromo- somes 7, 8, 9, 10, 11, and 17 was 50% in TI tumors and 100% in T2-T4 tumors when compared with CGH. The agreement was 100% for the 8q24 locus and 50% for the TP53 locus.
10~12.1-14, llq13, 12q15-21, 13q31-33, 17q12,
ALTERATIONS OF ONCOGENES IN BLADDERCANCER
RAS
The RAS genes (Harvey-, Kirsten-, and N- RAS) are a family of oncogenes that produce a 21-kd membrane-bound protein, p21, in- volved in signal transduction.'" The first mu- tation of the RAS family of oncogenes was identified in codon 12 of the H-RAS gene (GGC-GTC [Gly-Val]) in bladder cancer cell lines.122, 155 In addition to codon 12, codon 61 has been identified as a "hot spot" of H- RAS oncogene a ~ t i v a t i o n . ~ ~ Valenzuela and G r ~ f f e n ' ~ ~ first reported a mutation in codon 12 of the K-RAS gene ( G A [Gly-Asp]) in a bladder cancer cell line. Other investigators have subsequently reported mutations in other codons of the R A S genes. Grimmond and associates49 reported a heterozygous mu- tation at codon 59 of K-RAS (GCA+ACA [Ala-Thr]) in a grade I1 TCC. Bos and co- workers" have reported a mutation in codon 61 of N-RAS (CAA-CGA [Gln-+Arg]). Co-
hen and Levinson2" have identified a muta- tion A+G at position 2719 of intron-D of the H-RAS gene that causes a tenfold increase in gene expression.
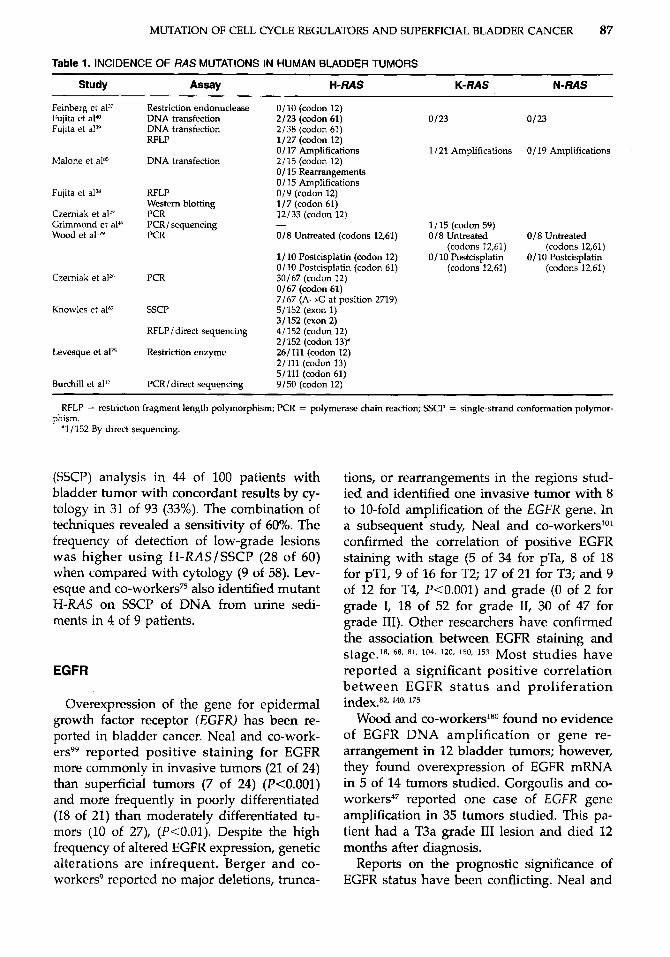
The mutation frequency of RAS genes in bladder cancer has been controversial (Table 1). Early studies using DNA transfection assays identified a mutation frequency of 5% to 15%,39, 40, 85 whereas more recent reports using polymerase chain reaction (PCR)-based assays have found a much higher frequency of mutations, up to 45%.26, 27 Czerniak and co- workers26 observed a GGC-GTC [Gly+Val] substitution at codon 12 of H-RAS in 30 of 67 tumors, with a higher frequency in aneuploid (56%) than in diploid (28%) tumors and a higher frequency in high-grade tumors: grade I (O%), grade I1 (44%), grade I11 (65%). Viola and c o - w ~ r k e r s ' ~ ~ have also reported in- creased RAS p21 expression in high-grade bladder tumors. Other investigators have not reported this association with grade. Lev- esque and c o - ~ o r k e r s ~ ~ reported the GGC+GTC [Gly-+Val] substitution at codon 12 of H-RAS in 26 of 111 tumors, a mutation at codon 13 (Gly-Kys) in 2 of 111, and muta- tions at codon 61 in 5 (Glu+Arg in three, Glu+Lys in one, Glu+Leu in one); however, no difference in mutation frequency was noted across tumor grades (43% for grade I, 27.6% for grade 11, 30% for grade 111). Burchill and co-workers'2 found point mutations in 9 of 50 bladder tumors at codon 12 of H-RAS (GGC+GTC [Gly+Val] in eight and GGC+GAC [Gly+Asp] in one) with no asso- ciation between mutation frequency and tu- mor grade and stage.
Other researchers have not found a high frequency of RAS mutations. Knowles and Williamson67 reported H-RAS mutations in 8 of 152 tumors by direct sequencing. Muta- tions were present at codon 12 in 4 of 152 (GGC+TGC [Gly-Cys] in two, GGC+AGC [Gly-+Asp] in one, and GGC-GAC [Gly+ Ser] in one), at codon 13 in 1 of 152 (GGT+ GTT [Gly+Val]), and at codon 61 in 3 of 152 (CA-CGG [Gln+Arg] in two and CAG+ CTG [Gln+Leu] in one).
Urine sediments have been studied for H- R A S mutations. Fitzgerald and co-~orkers~~ reported mutations in exon 1 of H-RAS by single-strand conformation polymorphism
MUTATION OF CELL CYCLE REGULATORS AND SUPERFICIAL BLADDER CANCER 87
Table 1. INCIDENCE OF /?AS MUTATIONS IN HUMAN BLADDER TUMORS
Study Assay H-RAS K- RAS N- RAS
Feinberg et al" Fujita et a P Fujita et al"'
Malone et aln5
Fujita et al?"
Czerniak et a127 Grimmond et aPY Wood et allN
Czerniak et a12h
Knowles et aF7
Levesque et a175
Burchill et all2
Restriction endonuclease DNA transfection DNA transfection RFLP
DNA transfection
RFLP Western blotting PCR PCRI sequencing PCR
PCR
SSCP
RFLPI direct sequencing
Restriction enzyme
PCR/direct sequencing
0/10 (codon 12) 2/23 (codon 61) 0/23 0/23 2/38 (codon 61) 1/27 (codon 12) 0/17 Amplifications 1 /21 Amplifications O/ 19 Amplifications 2/15 (codon 12) O/ 15 Rearrangements 0/15 Amplifications 0 /9 (codon 12) 1/7 (codon 61) 12/33 (codon 12)
0 /8 Untreated (codons 12,61) 0/8 Untreated 0/8 Untreated (codons 12,61) (codons 1261)
1/10 Postcisplatin (codon 12) 0/10 Postcisplatin 0/10 Postcisplatin 0/10 Postcisplatin (codon 61) (codons 12,61) (codons 12,61) 30/67 (codon 12) 0/67 (codon 61) 7/67 (A-tG at position 2719) 5/152 (exon 1) 3/152 (exon 2) 4/152 (codon 12) 2/152 (codon 13)' 26/111 (codon 12) 2/111 (codon 13) 5/11] (codon 61) 9/50 (codon 12)
1/ 15 (codon 59) -
~ ~ ~~~~~~
RFLP = restrictton fragment length polymorphism; PCR = polymerase chain reaction; SSCP = single-strand conformation polymor- phism.
'1 / 152 By direct sequencing
(SSCP) analysis in 44 of 100 patients with bladder tumor with concordant results by cy- tology in 31 of 93 (33%). The combination of techniques revealed a sensitivity of 60%. The frequency of detection of low-grade lesions was higher using H-RASISSCP (28 of 60) when compared with cytology (9 of 58). Lev- esque and co-workers" also identified mutant H-RAS on SSCP of DNA from urine sedi- ments in 4 of 9 patients.
EGFR
Overexpression of the gene for epidermal growth factor receptor (EGFR) has been re- ported in bladder cancer. Neal and co-work- e r ~ ~ ~ reported positive staining for EGFR more commonly in invasive tumors (21 of 24) than superficial tumors (7 of 24) (P<O.OOl) and more frequently in poorly differentiated (18 of 21) than moderately differentiated tu- mors (10 of 27), (P<O.Ol). Despite the high frequency of altered EGFR expression, genetic alterations are infrequent. Berger and co- workers9 reported no major deletions, trunca-
tions, or rearrangements in the regions stud- ied and identified one invasive tumor with 8 to 10-fold amplification of the EGFR gene. In a subsequent study, Neal and co-workerslO' confirmed the correlation of positive EGFR staining with stage (5 of 34 for pTa, 8 of 18 for pT1, 9 of 16 for T2; 17 of 21 for T3; and 9 of 12 for T4, P<O.OOl) and grade (0 of 2 for grade I, 18 of 52 for grade 11, 30 of 47 for grade 111). Other researchers have confirmed the association between EGFR staining and
reported a significant positive correlation between EGFR status and proliferation
Wood and co-workers180 found no evidence of EGFR DNA amplification or gene re- arrangement in 12 bladder tumors; however, they found overexpression of EGFR mRNA in 5 of 14 tumors studied. Gorgoulis and co- w o r k e r ~ ~ ~ reported one case of EGFR gene amplification in 35 tumors studied. This pa- tient had a T3a grade I11 lesion and died 12 months after diagnosis.
Reports on the prognostic significance of EGFR status have been conflicting. Neal and
Stage.'% 68, 81, 104, 120, 150, 153 Most studies have
index.82, 140.175
88 RABBANI & CORDON-CARD0
co-workers'"" initially reported on 101 pa- tients with bladder cancer (34 pTa, 18 pT1, 16 T2, 21 T3, and 12 T4). EGFR [relative risk (RR) = 3.42, P<O.OOl] and stage (RR = 1.85, P<O.OOOl) were independently predictive of bladder cancer death in all 101 patients. In the group of 52 patients with superficial bladder tumors, only EGFR (RR = 2.28, R0.03) was independently predictive of time to recur- rence; EGFR (RR = 22.1, P<O.OOOl) and tu- mor multiplicity (RR = 1.37, P<0.05) were independently predictive of time to progres- sion. In an update on this original cohort including 212 patients, Mellon and co-work- er@ reported that stage, grade, and EGFR status were independently predictive of blad- der cancer death in the entire cohort. In the group of 113 patients with superficial bladder tumors, only size was independently pre- dictive of time to recurrence, and size and EGFR status were independently predictive of time to progression.8s EGFR status was 80% sensitive and 93% specific in predicting stage progression in T1 grade I11 lesions. Lipponen and EskelinenB1 have also reported EGFR to be an independent predictor of overall and recurrence-free survival in Ta-TI tumors. Al- though some studiest7, have supported the finding of EGFR as an independent prognos- tic factor, others have not.104,
Theodorescu and co-worker~'~~ have sug- gested that the strong association between EGFR status and progression to invasive bladder cancer may be accounted for by en- hanced cellular motility. Using the T24 cell line, which overexpresses EGFR, these re- searchers demonstrated that T24 cells transfected with antisense EGFR have slower growth and lack proliferative and motility re- sponses to exogenous EGF.159 The presence of an H-XAS mutation at codon 12 of the T24 cells suggests that this EGFR motility signal- ing is RAS-independent.
I2l, 153
ERBB-2
The ERBB-2 (HER-2/neu) gene encodes a 185-kd cell surface glycoprotein, p185HER-2 / neu, with extensive homology to EGFR. Zhau and co-workers'" first reported ERBB-2 gene amplification by Southern blotting in 2 of 24
high-grade TCCs, with c-erbB-2 / neu expres- sion in 23 of 34 (67.6%) patient specimens by Western blotting and in 26 of 35 (74.3%) by immunohistochemistry. Wood and associ- ates's' also detected amplification and possi- ble structural rearrangement of the ERBB-2 gene by Southern blotting in 1 of 12 bladder tumors. This patient with a pT3aNOMO lesion had sixfold DNA amplification and displayed both mRNA and protein overexpression. Of 14 tumors analyzed by Northern blotting, 5 (36%) overexpressed mRNA without gene amplification, with 3 of these tumors dis- playing protein overexpression.
Several investigators have reported the ad- verse prognostic significance of p185HER-2/ neu. Sat0 and co-w~rkers '~~ studied the prog- nostic significance of p185HER-2 /neu protein expression in 88 patients undergoing surgery for bladder cancer. p185HER-2/neu protein was expressed in 23 of 88 patients (26%), cor- relating with grade (K0.05) . p185HER-2 /neu protein expression was a significant adverse predictor of survival, independent of tumor grade and stage. The actuarial 5-year disease- free and overall survival rates were 48.5% and 65.5%, respectively, for p185HER-2/ neu- negative tumors versus 9.7% and 41.8%, re- spectively, for p185HER-2 / neu-positive tu- mors. Gorgoulis and co-workers4' identified amplification of ERBB-2 in 4 of 35 (11Y0) TCCs; all 4 patients had muscle-invasive le- sions and died within 12 months of diagnosis. Underwood and associates164 studied 236 bladder tumors in 89 patients with recurrent lesions, 20 tumors in patients with no recur- rence, and 10 normal bladder controls for ERBB-2 gene amplification and p185HER-2/ neu protein overexpression. ERBB-2 gene am- plification was observed in 16 of 89 patients with recurrent disease but not in patients with nonrecurrent tumors or in control pa- tients. Of 43 patients with progressive dis- ease, 14 had ERBB-2 gene amplification. ERBB-2 gene amplification (RR = 2.45, P<0.02) and p185HER-2/neu protein expres- sion were significant independent predictors of death owing to bladder cancer. Korkolo- poulou and colleagues68 studied 106 patients with bladder TCC, reporting a positive corre- lation of p185HER-2 / neu protein expression with grade, stage, and nonpapillary configu-
MUTATION OF CELL CYCLE REGULATORS AND SUPERFICIAL BLADDER CANCER 89
ration. p185HER-2 / neu expression and tumor stage were independent predictors of disease- free survival.
Other investigators have failed to identify an adverse outcome with p185HER-2/neu overexpression. Tetu and co-worker~'~~ stud- ied 256 Ta-T1 bladder tumors by immuno- staining for p185HER-2/ neu protein, describ- ing positive staining in 21 (8.2%), with a significant association with T1 stage, multifo- cality, high grade, p53 expression, and aneu- ploidy; however, p185HER-2 / neu expression did not correlate with time to recurrence. Contrary to other reports, two studies have demonstrated a superior disease-specific sur- vival in patients with positive p185HER-2/ neu expression on univariate analysis;lO4* lZ1 however, this expression was not a significant independent predictor in the one study per- forming multivariate analysis.1n4
MDM2
The MDMZ gene is a proto-oncogene lo- cated on chromosome 12 (12q13-14) that en- codes for a 90-kd nuclear protein, mdm2.In6 Mdm2 binds to p53, inhibiting its transcrip- tional activityIn6 and targeting it for degrada- tion through the proteo~orne.~~, 69 MDM2 gene amplification was first reported in bladder cancer by L i a n e ~ ~ ~ and Habuchi5* and their co-workers. Lianes and colleague^^^ identified 1 of 40 patients with MDM2 amplification; this patient had stage T1 TCC. Nuclear over- expression (>20% of cells) of mdm2 was seen in 26 of 87 patients (30%). Mdm2 overexpres- sion was more common in papillary Ta tu- mors (five of eight) when compared with muscle-invasive tumors (16 of 66), (P = 0.023). Mdm2 overexpression was more common in low-grade lesions (50% of grade I versus 17% of grade I11 lesions, P = 0.0005). Habuchi and colleagues51 identified 2 of 50 patients with MDM2 amplification. One patient had a met- astatic high-grade renal pelvic tumor with sevenfold amplification, whereas the other had a pT3 grade I11 bladder cancer with five- fold amplification of MDMZ.
Barbareschi and co-workers7 reported mdm2 overexpression (immunoreactivity in
>5% of cells) in 5 of 25 bladder tumors, with absence of p53 overexpression in four of these five. Conversely, mdm2 immunoreactivity was absent in 13 of 14 cases with p53 overex- pression. Sigalas and co-worker~'~~ have ob- served alternatively spliced MDM2 gene tran- scripts more frequently in muscle-invasive tumors (four of seven) when compared with superficial Ta-TI tumors (1 of 16) (P = 0.017). Four of the five alternative splice variants lacked p53-binding domain sequences, with these four showing loss of p53 binding.14' Schmitz-Drager and co-worker~'~~ studied 200 bladder tissue specimens for p53 and mdm2 expression, evaluating significant indepen- dent predictors of progression in the 61 pa- tients with superficial bladder cancer. Speci- mens showing muscle invasion had a lower incidence of mdm2 overexpression: 1 of 10 in dysplasia, 5 of 28 in pTis, 20 of 82 in pTa, 20 of 41 in pT1, and 5 of 23 in pT2-pT3b. Multifocal disease and p53 accumulation, but not mdm2 overexpression, were independent predictors of tumor progression.
Cyclin D1
In mammalian cells, the D-type cyclins, through their interactions with cyclin-depen- dent kinases, drive the cell through the G,/S restriction point.62 Cyclin D1 is a member of the G, cyclins involved in regulation of this restriction point.%, 96 Lee and c o - ~ o r k e r s ~ ~ first evaluated cyclin D1 overexpression in blad- der cancer. Overexpression of cyclin D1 was observed in 24 of 51 (47%) grade I, 13 of 65 (20%) grade 11, and 0 of 45 grade I11 lesions, and in 14 of 41 (34%) pTa, 13 of 63 (21%) pT1, and 0 of 20 pT2-pT4 tumors. Shin and associates145 did not find a correlation be- tween cyclin D1 overexpression and tumor grade. Tumors with cyclin D1 expression of more than 50% recurred more rapidly when compared with tumors with cyclin D1 expres- sion of 50% or less. Nevertheless, overexpres- sion of cyclin D1 was not associated with shortened overall survival in patients with muscle-invasive tumors.
90 RABBANI & CORDON-CARDO
ALTERATIONS OF TUMOR SUPPRESSOR GENES
Alterations in the TP53 Pathway
TP53 Gene
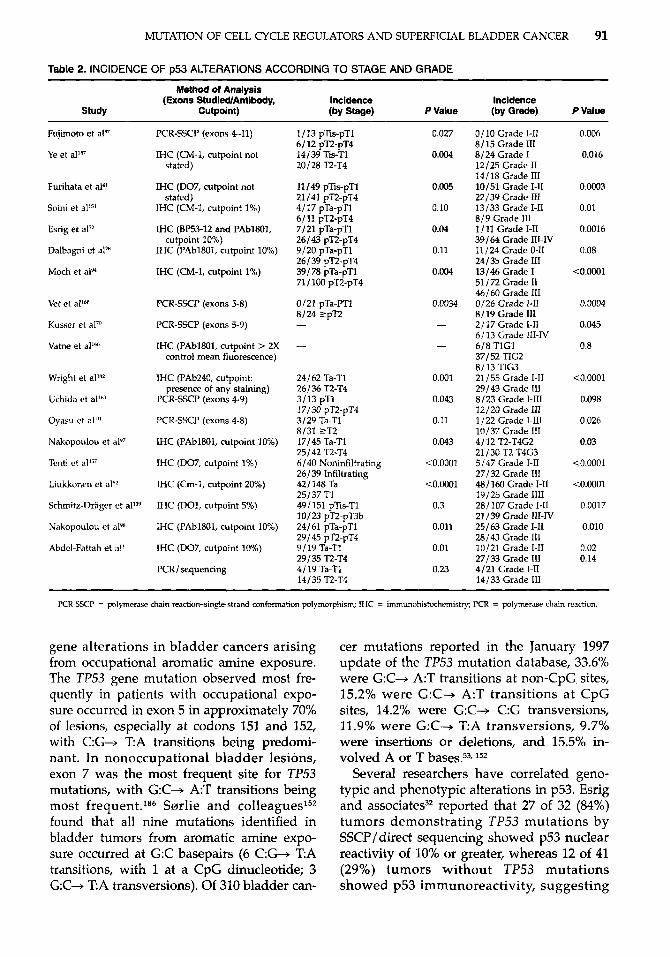
The TP53 tumor suppressor gene has been mapped to chromosome 17q13 and is com- posed of 11 exons.12h Following the observa- tion of the importance of TP53 mutations in colorectal t umor~ ,~ several investigators eval- uated the role of TP53 in bladder tumor de- velopment. Tsai and associates16' reported al- lelic loss of chromosome 17p in 15 of 24 (63%) informative cases. In a subsequent study by the same investigators, allelic loss of chromo- some 17p was found to be more common in high-grade tumors (0 of 10 in grade I1 versus 20 of 31 in grade III-IV).'07 Sidransky and co-workers146 identified genetic alteration of TP53 in 11 of 18 (61%) patients with invasive bladder cancer, consisting of ten point muta- tions and one 24-base pair deletion. Presti and co-worker~"~ reported a higher incidence of chromosome 17p deletions in invasive bladder tumors (3 of 7 in pTis-pTa versus 22 of 27 in pT1-pT4). Subsequently, other re- searchers have demonstrated a higher fre- quency of TP53 gene mutations in invasive (versus superficial) bladder cancer and high- grade lesions.37* 'I1, 163, Immunohistochemical studies of primary tumor samples have dem- onstrated overexpression of p53 protein in patients with invasive and high-grade blad- der tumors." Table 2 summarizes the inci- dence of p53 alterations, according to tumor stage and grade, in the published literature.
Most point mutations of the TP53 gene in human cancer have been identified in four regions (amino acid residues 117-142, 171-181, 234-258, and 270-286).76 In a review of the literature, Abdel-Fattah and co-workers' found that 58% of TP53 mutations in exons 4 to 9 reported in bladder TCC were in exon 8, 30% in exon 7,27% in exon 5, 13% in exon 6, 4% in exon 4, and 1% in exon 9. Fujimoto and c o - ~ o r k e r s ~ ~ identified TP53 mutations in eight high-grade lesions, seven of which were invasive. There were five base pair sub-
"References 1, 28, 32, 41, 82, 91, 94, 97, 98, 113, 139, 143, 144, 151, 157, and 187.
stitutions (three transversions and two transi- tions), two base pair deletions, and one 21- base pair deletion.37 Oyasu and associates"' identified 12 point mutations (nine transitions and three transversions), one base pair dele- tion, and one 7-base pair deletion. Xu and co-workers*M found TP53 mutations in 13 of 28 patients with grade I1 to I11 multifocal TCC using DNA sequence analysis. Analysis of 17 recurrences in five patients revealed the identical mutation found in the primary tu- mor in all except one patient, suggesting monoclonality of multifocal TCC. Goto and c011eagues~~ studied the pattern of TP53 muta- tions in 42 patients with synchronous (32) or metachronous (10) multifocal lesions. TP53 mutations were identified in 42 of 84 (50%) bladder tumors from 22 of 42 (52%) patients. Nine patients had identical mutations with or without additional mutations in the multiple carcinomas, eleven patients had discordant mutations, and two patients had a mutation in one tumor but not the other. It was con- cluded that multiple bladder tumors may be of common or independent origin.
Some investigators have suggested that the mutation pattern observed reflects the type of carcinogen involved.52, 163 Habuchi and co- w o r k e r ~ ~ ~ reported that although the inci- dence of TP53 mutations was not higher in smokers, four of ten mutations in smokers were A:T+G:C transitions compared with 0 of 10 mutations in nonsmokers. All eight base substitutions observed in squamous cell carci- nomas occurred at G:C sites, whereas 6 of 18 (33%) mutations in TCCs were base substitu- tions at A:T Expanding on this study, Warren and co-worker~'~~ identified a higher proportion of base pair substitutions at CpG dinucleotides in schistosomal bladder cancer (18 of 34) than in non-schistosomal bladder cancers (25 of 103), (odds ratio, 3.5; P = 0.003). Most of the mutations in Egyptian tu- mors were in exons 5 and 6, whereas in non- Egyptian tumors, exon 7 and 8 mutations were most common. Warren and colleagues have postulated that the excess of transitions at CpG dinucleotides in schistosomal bladder cancer results from nitric oxide produced by the inflammatory response provided by the schistosomal eggs.
Yasunaga and co-workers186 studied TP53
MUTATION OF CELL CYCLE REGULATORS AND SUPERFICIAL BLADDER CANCER 91
Table 2. INCIDENCE OF p53 ALTERATIONS ACCORDING TO STAGE AND GRADE
Method of Analysis (Exons StudiedlAntibody, Incidence Incidence
Study Cutpoint) (by Stage) P Value (by Grade) P Value
Fujimoto et al"
Ye et allR7
Furihata et a14'
Soini et al's'
Esrig et aP2
Dalbagni et a12"
Moch et alY4
Vet et a P
Kusscr et al"l
Vatne et all"
Wright et altQ
Uchida et allh'
Oyasu ct al"'
Nakopoulou et alY7
Tenti ct all5'
Liukkonen et al"'
Schmitz-Drager et all"
Nakopoulou et alqH
Abdcl-Fattah et all
PCR-SSCP (exons 4-11)
IHC (CM-1, cutpoint not stated)
IHC (D07, cutpoint not
IHC (CM-1, cutpoint 1%)
IHC (BP53-12 and PAbl801,
IHC (PAbl801, cutpoint 10%)
IHC (CM-1, cutpoint 1%)
stated)
cutpoint 10%)
PCR-SSCP (exons 5-8)
PCR-SSCF (exons 5-9)
IHC (PAbl801, cutpoint > 2X control mean fluorescence)
IHC (PAb240, cutpoint:
PCR-WP (exons 4 9 )
PCR-SSCP (exons 4-8)
IHC (PAbl801, cutpoint 10%)
IHC (D07, cutpoint 1%)
IHC (Cm-1, cutpoint 20%)
IHC (D01, cutpoint 5%)
presence of any staining)
IHC (PAbl801, cutpoint 10%)
IHC (DO7, cutpoint 10%)
PCRIsequendng
1 I13 pTis-pT1
14/39 Tis-T1 6 / 12 pT2-pT4
20128 T2-T4
11 149 pEs-pT1 21/41 pT2-pT4 4/17 pTa-pT1
7/21 pTa-pT1 26/43 pT2-pT4 9/20 pTa-pT1 26/39 pT2-pT4 391 78 pTa-pTl
6 111 pT2-pT4
71 1100 pT2-pT4
0121 pTa-IT1 8/24 2pT2 -
24/62 Ta-TI
3/13 pT1 17/30 pT2-pT4 3 129 Ta-TI 8/31 ZT2 17/45 Ta-T1 25 / 42 T2-T4 6/40 Noninfiltrating 26/39 Infiltrating 421 148 Ta 25/37 T1 49/15] plis-Tl 10123 pTZpT3b 24/61 pTa-pT1 29/45 pT2-pT4 9 119 Ta-TI
4/ 19 Ta-T1
26 136 T2-T4
29 I35 T2-T4
14/35 T2-T4
0.027
0.004
0.005
0.10
0.04
0.11
0.004
0.0034
-
-
0.001
0.043
0.11
0.043
<0.0001
<0.0001
0.3
0.011
0.01
0.23
01 10 Grade 1-11 8/15 Grade III 8/24 Grade I 12/25 Grade I1 14/18 Grade 111 lO/Sl Grade 1-11 22/39 Grade 111 13/33 Grade 1-11 819 Grade III 1 I11 Grade 1-11 39/64 Grade IU-IV 11/24 Grade 0-11 24/35 Grade 111 13/46 Grade I 51 / 72 Grade I1 46/60 Grade 111 0/26 Grade 1-11 8 / 19 Grade I11 2/17 Grade 1-11 61 13 Grade 111-IV 618 TlGl 371 52 TIC2 8/ 13 TIG3 21/55 Grade 1-11 29/43 Grade I11 8 123 Grade 1-111 12/20 Grade 111 1/22 Grade 1-111 10137 Grade 111
21 130 T2-T4G3 5/47 Grade 1-11 27/32 Grade I11 481 160 Grade 1-11 19/25 Grade 1111 281107 Grade 1-11 21/39 Grade 111-IV 25/63 Grade 1-11 28/43 Grade 111 10121 Grade 1-11 27/33 Grade 111 4/21 Grade 1-11 14/33 Grade I11
41 12 T2-T4G2
0.006
0.016
0.0003
0.01
0.0016
0.08
<0.0001
0.0004
0.045
0.8
<0.0001
0.098
0.026
0.03
<0.0001
<0.0001
0.0017
0.010
0.02 0.14
~~~~~ ~ ~ ~~~~~ ~ ~~~ ~
PCR-SSCI' 7 polymerase chain reactionsingle-strand conformation polymorphism; IHC = immunohistochemistry; PCR = polymerase chain reaction.
gene alterations in bladder cancers arising from occupational aromatic amine exposure. The TP53 gene mutation observed most fre- quently in patients with occupational expo- sure occurred in exon 5 in approximately 70% of lesions, especially at codons 151 and 152, with C:G+ T:A transitions being predomi- nant. In nonoccupational bladder lesions, exon 7 was the most frequent site for TP53 mutations, with G:C+ A:T transitions being most frequent.186 Sarrlie and colleagues152 found that all nine mutations identified in bladder tumors from aromatic amine expo- sure occurred at G:C basepairs (6 C:G+ TA transitions, with 1 at a CpG dinucleotide; 3 G:C+ T A transversions). Of 310 bladder can-
cer mutations reported in the January 1997 update of the TP53 mutation database, 33.6% were G:C+ A:T transitions at non-CpG sites, 15.2% were G:C+ A:T transitions at CpG sites, 14.2% were G:C+ C:G transversions, 11.9% were G:C+ T:A transversions, 9.7% were insertions or deletions, and 15.5% in- volved A or T b a s e ~ . 5 ~ , ' ~ ~
Several researchers have correlated geno- typic and phenotypic alterations in p53. Esrig and associates32 reported that 27 of 32 (84%) tumors demonstrating TP53 mutations by SSCP/ direct sequencing showed p53 nuclear reactivity of 10% or greater, whereas 12 of 41 (29%) tumors without TP53 mutations showed p53 immunoreactivity, suggesting
92 RABBANI & CORDON-CARDO
that immunohistochemistry may be more sen- sitive than SSCP. Four of six tumors with mutations in exon 5 had no detectable immu- noreactivity, suggesting that heterogeneity of p53 immunoreactivity may be related to the site of the TP53 gene mutation.32 Cordon- Cardo and associatesz2 reported p53 nuclear immunoreactivity of greater than 20% in 26 of 42 bladder tumors. A mobility shift on SSCP was identified in 1 of 16 cases with undetectable p53 staining, 2 of 12 cases with 20% to 60% nuclear positivity, and 11 of 14 cases with 70% or greater nuclear positivity. Receiver-operator characteristic curve analy- sis using nine different cut points for defining positive nuclear staining as it relates to PCR- SSCP / sequencing revealed an area under the curve of 90.3'%,.22 Using a cut-off of 10% p53 immunoreactivity, Vet and co-workers'hy found p53 immunostaining in 7 of 33 tumors with n o mutations by PCR-SSCP and reactiv- ity in six of eight tumors with mutations iden- tified by PCR-SSCP/ sequencing. The 23% in- cidence of p53 overexpression in the absence of mobility shift on SSCP may partially be accounted for by the known occurrence of false-negative results by SSCP.
Some investigators have been skeptical of the value of immunohistochemical p53 ex- pression as a prognostic factor, given the dis- crepancy with different antibodies and the use of frozen section versus paraffin blocks. Gardiner and c o - ~ o r k e r s ~ ~ found that com- parison of the CM-1 and PAbl801 antibodies in 16 patients in whom frozen sections were available yielded identical results in ten and a difference of one category in p53 staining in the remaining six. Comparison of the PAbl801 and DO7 antibodies in 26 paraffin sections revealed identical results in 21 cases, a difference of one category of p53 staining in 4, and a difference of two categories in 1 case. A comparison of 14 cases for which both frozen and paraffin specimens were available revealed identical results or a difference of one category in p53 staining in 5 cases and a difference of two or more categories in 9
Abclel-Fa ttah and associates' have used mi- crodissection o f paraffin-embedded sections and PCR-based direct sequencing to examine the association between p53 nuclear immuno-
cases.
staining and the presence of TP53 mutations. Microdissection of p53-immunopositive re- gions in 10 samples with TP53 mutations con- firmed the presence of mutations in all. Two cases had an unequivocal homozygous pat- tern of TP53 mutation. Microdissection of p53-immunonegative regions from these 10 samples revealed that 3 of 10 had the identical mutations previously found, suggesting that these were false-negatives for immunohisto- chemistry; however, microdissection of p53- immunopositive and immunonegative re- gions from 13 samples positive for p53 but with wild-type TP53 genotype revealed no mutations in either the p53-immunopositive or negative regions.'
Analysis of bladder washings for TP53 mu- tations has been shown by some investigators to complement mutational analysis of the pri- mary tumor samples. Vet and c o - ~ o r k e r s ' ~ ~ studied bladder washings and synchronous tumors of 15 patients for the presence of TP53 mutations. In two patients, the mutation pres- ent in the tumors was not detected in the bladder washings, and, in one patient, the mutation in the bladder washings was not present in the tumor specimen [sensitivity of 75% (6 of €9, specificity of 86% (6 of 7)].I7O Xu and c o - w o r k e r ~ ~ ~ ~ found that the TP53 mutation seen in the primary tumors was detectable in 24 of 30 urine samples collected at initial diagnosis or follow-up screening in eight patients with mutations; the remaining six patients had negative cystoscopic exami- nations. Nevertheless, 6 of 24 urine samples in which mutations were detected had nega- tive cystoscopy, suggesting long-term persis- tence of tumor cell clones within the bladder in patients with a likelihood of recurrence. Okuno and co-workers"Js reported a sensitiv- ity of 89% and specificity of 95% for p53 immunohistochemistry on culture of exfoli- ated cells from urine compared with p53 im- munohistochemistry of surgical specimens (accuracy, 92.1%). Righi and c~-workers~*~ re- ported that p53 immunohistochemistry of urine cytology did not improve diagnostic accuracy (sensitivity of 23.5% and specificity of 75% for the detection of bladder cancer versus cystoscopic biopsy).
Following the initial reports of TP53 alter- ations in bladder cancer, numerous investiga-
MUTATION OF CELL CYCLE REGULATORS AND SUPERFICIAL BLADDER CANCER 93
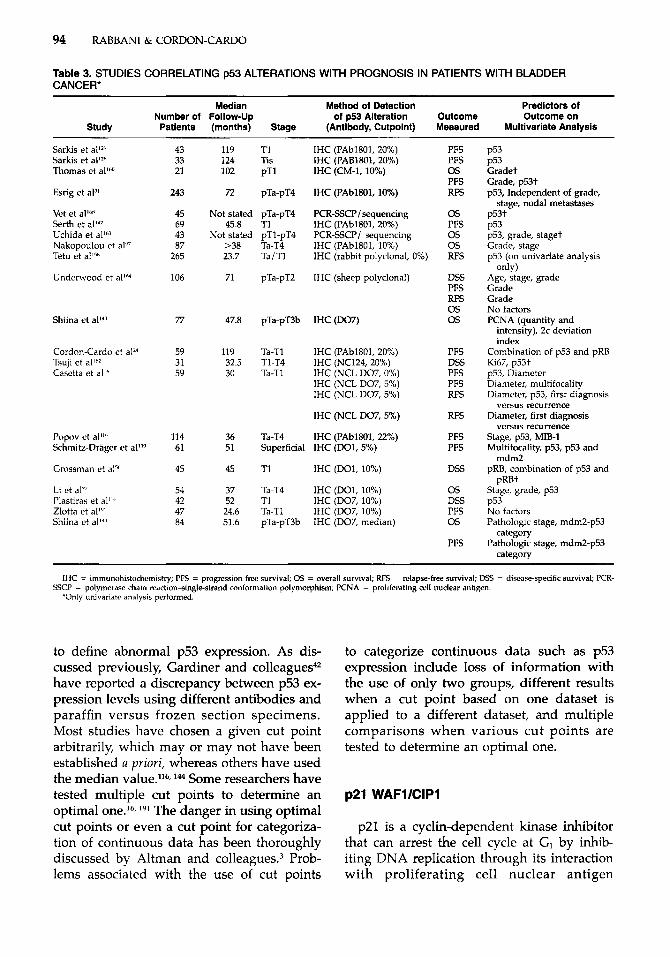
tors evaluated the prognostic significance of TP53 alterations with respect to disease recur- rence, progression, and death owing to blad- der cancer. Sarkis and associates128, lZy identi- fied p53 expression (using a cut point of 20% immunoreactivity) as the only significant pre- dictor of progression-free survival in a group of 43 patients with T1 bladder cancer (RR= 11.4, P = 0.002)12y and a group of 33 patients with carcinoma in situ (RR = 8.9, P = 0.004).1ul In a much larger study of 243 patients with pTa-pT4 bladder cancer, Esrig and co-work- e r ~ ~ ' identified p53 as a significant predictor of recurrence-free survival, independent of grade, stage, and lymph node metastases. Subsequent investigators have confirmed the prognostic significance of p53 overexpression in superficial (Ta, Tis, T1) bladder cancer (Ta- ble 3).* Studies that have included patients with both superficial and muscle-invasive bladder cancer have also identified p53 over- expression as a poor prognostic factor.n, 'I6,
l h 2 Two studies have assessed the prognos- tic significance of TP53 mutations as detected by PCR-SSCP and direct sequencing, identi- fying TP53 mutation as a predictor for death on univariate analysis.'63, Other studies have failed to identify p53 overexpression as an independent prognostic factor. t
Several investigators have evaluated the co- operative effects of p53 alterations with those of other cell cycle regulators. The retinoblas- toma gene, RB, encodes a 110-kd protein, pRB, which is a target for the enzymatic activ- ity of cyclin-Cdk complexes.2y In its under- phosphorylated functionally active form, pRB acts as a negative regulator of the cell cycle at the G, I S transition. Cordon-Cardo and co- worke r~~~ investigated the prognostic signifi- cance of altered p53 and pRB expression when compared with the presence of one or neither abnormality in a group of 59 patients with Ta-T1 bladder TCCs. In comparison with patients with p53- (expression <20%) and pRb + (detectable) tumors, patients with p53+ (>20%) and pRb- (undetectable) tu- mors had a 10.2-fold increased risk of pro- gression (P = 0.0035) on multivariate analy- sis. Patients with p53 - /pRB - or p53 + /
'References 16, 24, 50, 71, 114, 139, 142, 158, and 160. tReferences 13, 97, 110, 143, 148, 164, 167, and 191.
pRB+ tumors had a 4.5-fold increased risk of tumor progression when compared with patients with p53- /pRB+ tumors (P = 0.050). In a similar study of 45 patients with pT1 disease, Grossman and colleagues5" found that patients with an abnormality in p53 (>lo%) or pRB (negative or homoge- neous positive staining pattern) had a worse progression-free survival when compared with patients with normal p53 ( 4 0 % ) or pRB (heterogeneous positive) status (P = 0.04). Patients with alterations in both p53 and pRB had an even lower progressive-free survival (P = 0.005). Shiina and associates'+' evaluated the clinical significance of the simultaneous evaluation of p53 and mdm2 in 84 patients with pTa-pT3b bladder cancer. Multivariate analysis revealed that pathologic stage and p53-mdm2 category were significant indepen- dent predictors of overall survival and pro- gression-free survival. Overall survival and progressive-free survival were highest in pa- tients with p53 - and mdm2 - tumors.
The status of p53 expression has also been evaluated as a predictor of response to ther- apy. Because at least one third of patients with superficial bladder cancer (Ta, Tis, T1) will not respond to intravesical bacillus Cal- mette-Gukrin (BCG) therapy, p53 has been studied as a potential predictor of response to therapy. Lacombe and associate^^^ exam- ined 196 tissue specimens from 98 patients (22 Ta, 57 Tis, 19 T1) obtained immediately before and after intravesical BCG therapy. Pre-BCG p53 overexpression did not predict response to BCG therapy; however, pre-BCG p53 overexpression, response to BCG, and pre-BCG stage were all independent pre- dictors of disease progression. In patients with residual disease after BCG (nonrespond- ers), post-BCG p53 overexpression was the only independent predictor of disease pro- gression. Other investigators have confirmed the finding that pre-BCG p53 status cannot be used to predict clinical response to BCG therapy.".
Although a large body of literature has been published on the prognostic clinical sig- nificance of p53 expression in tumor samples, difficulty in interpretation arises from the many different antibodies and the wide range of cut points (detectable to 22%, Table 3) used
94 RABBANI & CORDON-CARD0
Table 3. STUDIES CORRELATING p53 ALTERATIONS WITH PROGNOSIS IN PATIENTS WITH BLADDER CANCER*
Median Method of Detection Predictors of Number of Follow-Up of p53 Alteration Outcome Outcome on
Study Patients (months) Stage (Antibody, Cutpoint) Measured Multivariate Analysis
Sarkis et Sarkis et all2” Thomas et a]’”
Esrig et a P
Vet et alnhx Serth et all” Uchida et al“” Nakopoulou et al”’ Tetu et al“”
Underwood et allM
Shiina ct
Cordon-Cardo et a P Tsuji et a l L 2 Casetta et all”
J’opov ct al”“ Srhmitz-Drager et a P
Crossman et alY’
Li et al” I’lastiras et al”” Zlotta et a P Shiina et all”
43 119 T1 33 124 Tis 21 102 pT1
243 72 pTa-pT4
45 Not stated pTa-pT4 69 45.8 T1 43 Not stated pT1-pT4 87 >38
265 23.7
106 71
77 47.8
59 119 31 32.5 59 30
114 36 61 51
45 45
54 37 42 52 47 24.6 84 51.6
?a-T4 Ta / T1
pTa-pT2
pTa-pT3b
Ta-TI T1-T4 Ta-T1
Ta-T4 Superficial
Tl
Ta-T4 T1 Ta-T1 pTa-pT3b
IHC (PAbl801. 20%) IHC iPAB1801; 20%) IHC (CM-I, 10%)
IHC (PAblSOl,lO%)
PCR-SSCP/sequencing
PCR-SSCP/ sequencing
IHC (rabbit polyclonal, 0%)
IHC (sheep polyclonal)
IHC (PAblBOl, 20%)
IHC (PAbl801, 10%)
IHC (D07)
IHC (PAbl801, 20%) IHC (NC124, 20%) IHC (NCL D07, 0%) IHC (NCL D07,5%) IHC (NCL D07,5%)
IHC (NCL D07,5%)
IHC (PAbl801,22%) IHC (D01,5%)
IHC (D01, 10%)
IHC (D01, 10%) IHC (D07, 10%) IHC (D07,10%) IHC (D07, median)
PFS PFS 0s PFS RFS
0s PFS 0 s 0s RFS
DSS PFS RFS 0s 0s
PFS DSS PFS PFS RFS
RFS
PFS PFS
DSS
0 s DSS PFS 0 s
PFS
P53 P53 Gradet Grade, p53t p53, Independent of grade,
stage, nodal metastases o53t b53 p53, grade, staget Grade, stage p53 (on uiivariate analysis
Age, stage, grade Grade Grade No factors PCNA (quantity and
only)
intensity), 2c deviation index
Combination of p53 and pRB Ki67, p53t p53, diameter Diameter, multifocality Diameter, p53, first diagnosis
versus recurrence Diameter, first diagnosis
versus recurrence Stage, p53, MIB-1 Multifocality, p53, p53 and
pRB, combination of p53 and mdm2
uRBt r - Stage, grade, p53 P53 N o factors Pathologic stage, mdm2-p53
category Pathologic stage, mdm2-p53
category ~~
IkIC = immunohistochemistry; PFS = progression-free survival; 0s = overall survival; RFS = relapse-free survival; Dss = disease-specific survival; PCR-
*Only univariate analysis performed. SSCP = polymerase chain reaction-single-strand conformation polymorphism; PCNA = proliferating cell nuclear antigen.
to define abnormal p53 expression. As dis- cussed previously, Gardiner and colleagues42 have reported a discrepancy between p53 ex- pression levels using different antibodies and paraffin versus frozen section specimens. Most studies have chosen a given cut point arbitrarily, which may or may not have been established a priori, whereas others have used the median value.116, 144 Some researchers have tested multiple cut points to determine an optimal one.16, ly1 The danger in using optimal cut points or even a cut point for categoriza- tion of continuous data has been thoroughly discussed by Altman and colleague^.^ Prob- lems associated with the use of cut points
to categorize continuous data such as p53 expression include loss of information with the use of only two groups, different results when a cut point based on one dataset is applied to a different dataset, and multiple comparisons when various cut points are tested to determine an optimal one.
p21 WAFl/CIPl
p21 is a cyclin-dependent kinase inhibitor that can arrest the cell cycle at GI by inhib- iting DNA replication through its interaction with proliferating cell nuclear antigen

MUTATION OF CELL CYCLE REGULATORS AND SUPERFICIAL BLADDER CANCER 95
(PCNA).55, 173 Induction of p21 by wild-type p53 provides a mechanism for the latter to mediate its growth-suppressive Sev- eral investigators have reported on p21 WAFl /CIPl alterations in bladder cancer. Malkowicz and co-workerss4 found p21 ex- pression to be decreased in invasive tumors when compared with superficial bladder tu- mors. p21 expression was significantly de- creased in all tumors that had TP53 mutations by PCR-SSCP analysis (1 of 14 superficial and 6 of 14 invasive tumors). Novel mutations were reported in exon 2 of p21 WAFl/CIPl in 4 of 28 tumors. Lacombe and co-workersn reported a low incidence (2 of 27) of p21 WAFl / CIPl mutations in bladder cancer, with both cases displaying wild-type TP53. p21 expression has been reported to be higher in lower stage and lower grade bladder tu- mor~ . '~
Controversy exists regarding the prognostic significance of p21 expression in bladder can- cer. Lipponen and co-workersso analyzed bladder tumors (25 Ta, 68 T1, 53 T2, 26 T3, and 14 T4) from 186 patients for p21 expres- sion. Increased p21 expression correlated with aneuploid tumors, an Sphase fraction greater than lo%, mitotic index, apoptotic index, p53 positivity, and PCNA; however, overall sur- vival rates in patients with Ta-T1 disease were similar with p21 expression greater than 10% and less than or equal to 10%. Zlotta and co- w o r k e r ~ ' ~ ~ reported a similar positive correla- tion between p21 and p53 expression. Al- though p21 overexpression (>lo%) was asso- ciated with a shorter recurrence-free survival on univariate analysis, p21 was not an inde- pendent prognostic indicator on multivariate analy~is.'~' Using a cut point of 10% for p21 reactivity, Stein and c o - ~ o r k e r s ' ~ ~ reported that p21 expression was a significant pre- dictor of tumor recurrence ( P = 0.0017) and survival (P = 0.006), independent of tumor grade, stage, lymph node status, and p53 sta- tus on multivariate analysis. Patients with p53-altered/p21+ tumors had a similar rate of recurrence and survival as patients with p53 wild-type tumors, suggesting that main- tenance of p21 expression seems to abrogate the adverse effects of p53 alterations. Patients with p53-altered/p21- tumors had a worse
prognosis than patients with p53-altered / p21f tumors.
Alterations in the Retinoblastoma Pathway
RB Gene
The retinoblastoma gene, RB, was the first tumor suppressor gene isolated.36 Inactivation of the RB gene was reported in 5 of 16 inde- pendent human bladder cancer cell lines,61 suggesting that loss of RB function may have a role in bladder cancer. To investigate this hypothesis, Takahashi and c o - ~ o r k e r s ' ~ ~ transfected an RB expression plasmid under control of the human P-actin promoter into the bladder carcinoma cell line HTB9, which lacks pRB expression. RB + transfectants lacked the ability to form colonies in semi- solid medium, and their growth rate and tu- morigenicity were significantly decreased, suggesting a role for RB as a tumor suppres- sor gene in bladder cancer. Other researchers have subsequently confirmed the inhibition of tumorigenicity observed with re-introduc- tion by retrovirus-mediated gene transfer of wild-type RB gene into bladder cancer cell lines.46 Ishikawa and c o - ~ o r k e r s ~ ~ first re- ported absent pRB expression in 2 of 14 high- grade, invasive bladder tumors when com- pared with 0 of 16 low-grade noninvasive tumors, suggesting a role for loss of pRB in tumor progression.
Alterations in the RB gene have been re- ported more commonly in high-grade and invasive bladder tumors. Cairns and associ- a t e ~ ~ ~ found loss of heterozygosity (LOH) at the RB locus in 2 of 31 grade I, 8 of 25 grade 11, and 18 of 38 grade 111 lesions (P<0.005), and in 2 of 48 pTa/pTl lesions and 26 of 46 pT2-pT4 lesions (P<O.OOl). Xu and co-work- e r ~ ' ~ ~ correlated LOH and pRB protein expres- sion; 15 of 17 samples with LOH had altered pRB expression, and 31 of 36 informative samples without LOH had normal pRB ex- pression (P<O.OOl). A higher incidence of al- tered pRB expression was reported in high- grade and muscle-invasive tumors. Cordon- Cardo and have assessed pRB ex-
96 RABBANI & CORDON-CARDO
pression in 48 primary bladder tumors using immunohistochemistry. pRB expression was classified as negative (<lo%), heterogeneous (10% to 50%), and homogeneous (>50%), with the first two categories considered as altered pRB expression. There was a trend toward a higher incidence of altered pRB ex- pression in muscle-invasive tumors (14 of 38) when compared with superficial tumors (1 of 10) (P = 0.10). Other investigators have confirmed this correlation with stage and grade using immunohistochemistry or LOH to define RB
Analysis of the RB gene with PCR-SSCP and direct sequencing has not revealed this correlation with stage and grade. Miyamoto and co-workersg3 found eight mutations (27%) in 30 patients with bladder cancer, with no difference in incidence across grades (1 of 10 in grade I, 4 of 8 in grade 11, 3 of 12 in grade 111 lesions) or stages (4 of 19 in pTa/pTl and 4 of 11 in pT2-pT4). Five of 15 informative cases displayed LOH at the RB locus, with RB mutations present in three.
Altered pRB expression has also been re- ported to impart a worse prognosis in bladder cancer. Cordon-Cardo and associatesz3 first re- ported on pRB as a prognostic indicator in bladder cancer. Patients with positive pRB expression had a significantly higher survival on univariate analysis when compared with patients with altered pRB expression (P <0.001), with the difference still observed when analysis was limited to muscle-invasive tumors (P<O.OOl). In a subsequent report, Cordon-Cardo and colleaguesz4 reported a co- operative effect between p53 and pRB expres- sion on tumor progression in patients with superficial bladder cancer, a finding con- firmed by other researchers for both superfi- cialso and invasive bladder cancer.25
p 76INK4NCDKN2
The cyclin-dependent kinase inhibitors are a family of negative cell cycle regulators that bind to and inhibit the catalytic activity of cyclins and cyclin-dependent kinases.zl, The INK4A and INK4B genes map to the short arm of chromosome 9 (9p21), with INK4A encoding a 16-kd protein, ~ 1 6 , ’ ~ ~ and INK4B encoding a 15-kd protein, p15? The p16 and
p15 proteins complex with Cdk4 and Cdk6, inhibiting pRB phosphorylation at GI in the cell cycle. Recently, a second INK4A product, ~ 1 9 “ ~ , has been described that interacts with mdm2 and blocks mdm2-induced p53 degra- dation and transactivational ~ilencing.”~
Orlow and co-workerslo8 evaluated the fre- quency of INK4A and INK4B gene alterations in 110 patients with bladder TCC (31 Ta/Tis/ T1, 79 T2+). Homozygous deletion of the lNK4A and INK4B genes was observed in 11 and 9 bladder tumors, respectively. Homozy- gous deletion of the INK4A and INK4B gene was observed in 8 of 11 samples with homo- zygous deletion of lNK4A. Exclusive loss of either gene was observed in three cases. Hem- izygous deletion of INK4A or INK4B was seen in eight cases, gene rearrangement in three, and point mutations in none. Superficial tu- mors had a higher incidence of INK4A dele- tions or rearrangements (10 of 30) when com- pared with muscle-invasive lesions (11 of 79), (P<O.Ol). Low-grade lesions had a higher in- cidence of INK4A alterations (4 of 9 grade I, 4 of 17 grade 11, and 6 of 58 grade 111) (P<O.Ol). INK4B alterations were also more frequent in superficial (9 of 31) versus muscle- invasive (9 of 69) lesions (P<O.Ol).
In addition to genetic alterations (muta- tions and deletions), hypermethylation of the promoter region of INK4A has been described as an alternate mechanism of gene silencing and hence p16 inactivation.4, 45, 9o Aka0 and co-workers2 studied 38 urothelial cancers, identifying one base substitution in exon 2 (2.6%), six homozygous deletions (16.2%), and hypermethylation of the 5’ CpG island on exon 1 in 12 lesions (37.5%). All tumors with genetic alterations and 9 of 12 hyper- methylated tumors had absent p16 expres- sion. Orlow and c~-workers*~~ analyzed tis- sues from 121 patients with Ta and T1 bladder cancer. INK4A gene deletion was observed in 17 of 121 (14.1Y0), point mutations in 2 of 64 (3.1%), and de novo methylation of the p16 promoter in 7 of 47 (14.9%) evaluable cases. Of the 17 tumors with loss of lNK4A exon 2, 13 were homozygous and 4 heterozygous. Among nine homozygously deleted cases available for analysis of the INK4A exon l p (encoding ~ 1 9 ~ ~ ) and INK4B, all cases had a concomitant deletion of these loci. One case
MUTATION OF CELL CYCLE REGULATORS AND SUPERFICIAL BLADDER CANCER 97
showed deletion of the lNK4A exon l p with- out deletion of the surrounding loci. pl6-neg- ative phenotype correlated with deletion and methylation status. Although INK4A deletion status was a significant predictor of recur- rence on univariate analysis, only tumor mul- tiplicity was significant on multivariate analy- sis. Other investigators have shown that tumors having LOH at 9p21 and a mutation or deletion of the remaining lNK4A allele have absent p16 and high pRB expression.6 This finding may account for the poor prog- nosis recently reported with high pRB reactiv- ity.2s
E2F- 1 Gene
E2F-1 is a transcription factor that binds to the retinoblastoma protein, pRB. Although transfection assays have supported an onco- gene role for the transcription factor E2F- l,h4, h5 murine knock-out models for E2F-1 have suggested a role as a tumor suppressor gene.34*18s In the only published study of E2F- 1 performed in 133 patients with bladder can- cer, Rabbani and co-workers119 observed E2F- 1 nuclear reactivity of less than 5% in 53 patients and expression levels of 5% to 75% in the remaining 80 patients. E2F-1 nuclear reactivity correlated inversely with pRB nu- clear reactivity. A previously unreported polymorphism, GGC+AGC [Gly+Ser] at co- don 393 of exon 7 was identified in 7 of 133 patients with no correlation with E2F-1 nuclear reactivity. E2F-1 nuclear reactivity and suspicion of vascular invasion were the only significant independent predictors of progression to metastases and death.
References
1. Abdel-Fattah R, Challen C, Griffiths TR, et al: Alter- ations of TP53 in microdissected transitional cell carcinoma of the human urinary bladder: High fre- quency of TP53 accumulation in the absence of de- tected mutations is associated with poor prognosis. Br Cancer 772230, 1998
2. Akao T, Kakehi Y, Itoh N, et al: A high prevalence of functional inactivation by methylation modifica- tion of plGINK4A/CDKN2/MTSI gene in primary urothelial cancers. Jpn J Cancer Res 88:1078, 1997
3. Altman DG, Lausen 8, Sauerbrei W, et al: Dangers of using “optimal” cutpoints in the evaluation of prognostic factors. J Natl Cancer Inst 86:829, 1994
4. Atkin NB, Baker M C Cytogenetic study of ten carci- nomas of the bladder: Involvement of chromosomes 1 and 11. Cancer Genet Cytogenet 15:253, 1985
5. Baker SJ, Fearon ER, Nigro JM, et al: Chromosome 17 deletions and p53 gene mutations in colorectal carcinomas. Science 244217, 1989
6. Balazs M, Carroll P, Kerschmann R, et al: Frequent homozygous deletion of cydin-dependent kinase in- hibitor 2 (MTSI, p16) in superficial bladder cancer detected by fluorescence in situ hybridization. Genes Chromosomes Cancer 19234, 1997
7. Barbareschi M, Girlando S, Fellin G, et al: Expres- sion of mdm-2 and p53 protein in transitional cell carcinoma. Urol Res 2349, 1995
8. Benedict WF, Lemer SP, Zhou J, et ak Level of retinoblastoma protein expression correlates with p16 (MTS-l/INK4A/CDKN2) status in bladder can- cer. Oncogene 18:1197, 1999
9. Berger MS, Greenfield C, Gullick WJ, et al: Evalua- tion of epidermal growth factor receptors in bladder tumours. Br J Cancer 56:533, 1987
10. Berridge MJ: Inositol lipids and cell proliferation. Biochim Biophys Acta 907:33, 1987
11. Bos JL, Verlaan-de VM, Marshall CJ, et a1 A human gastric carcinoma contains a single mutated and an amplified normal allele of the Ki-ras oncogene. Nucleic Acids Res 14:1209, 1986
12. Burchill SA, Neal DE, Lunec J: Frequency of H-ras mutations in human bladder cancer detected by direct sequencing. Br J Urol 73:516, 1994
13. Burkhard FC, Markwalder R, Thalmann GN, et al: Immunohistochemical determination of p53 overex- pression: An easy and readily available method to identify progression in superficial bladder cancer? Urol Res 25 (suppl 1):31, 1997
14. Cairns P, Proctor AJ, Knowles MA: Loss of heterozy- gosity at the RB locus is frequent and correlates with muscle invasion in bladder carcinoma. Oncogene 62305, 1991
15. Cajulis RS, Haines GK, Frias-Hidvegi D, et al: In- terphase cytogenetics as an adjunct in the cytodi- agnosis of urinary bladder carcinoma: A compara- tive study of cytology, flow cytometry and interphase cytogenetics in bladder washes. Anal Quant Cytol Histol 16:1, 1994
16. Casetta G, Gontero P, Russo R, et al: p53 expression compared with other prognostic factors in OMS grade-I stage-Ta transitional cell carcinoma of the bladder. Eur Urol32229, 1997
17. Chow NH, Liu HS, Lee EI, et al: Significance of urinary epidermal growth factor and its receptor expression in human bladder cancer. Anticancer Res 17:1293, 1997
18. Chow NH, Tzai TS, Lin SN, et al: Reappraisal of the biological role of epidermal growth factor receptor in transitional cell carcinoma. Eur Urol 24140, 1993
19. Clasen S, Schulz WA, Gerharz CD, et a1 Frequent and heterogeneous expression of cyclin-dependent kinase inhibitor WAFl/p21 protein and mRNA in urothelial carcinoma. Br J Cancer 77515, 1998
20. Cohen JB, Levinson AD: A point mutation in the last jntron responsible for increased expression and transforming activity of the c-Ha-ras oncogene. Na- ture 334319, 1988
21. Cordon-Cardo C Mutations of cell cycle regulators: Biological and clinical implications for human neo- plasia. Am J Pathol 147545, 1995
22. Cordon-Cardo C, Dalbagni G, Saez GT, et al: p53 mutations in human bladder cancer: Genotypic ver- sus phenotypic patterns. Int J Cancer 56:347, 1994
98 RABBANI & CORDON-CARD0
23. Cordon-Cardo C, Wartinger D, Petrylak D, et al: Altered expression of the retinoblastoma gene prod- uct: Prognostic indicator in bladder cancer. J Natl Cancer Inst M1251, 1992
24. Cordon-Cardo C, Zhang ZF, Dalbagni G, et al: Co- operative effects of p53 and pRB alterations in pri- mary superficial bladder tumors. Cancer Res 57:1217, 1997
25. Cote RJ, Dunn MD, Chatterjee SJ, et al: Elevated and absent pRb expression is associated with blad- der cancer progression and has cooperative effects with p53. Cancer Res 58:1090, 1998
26. Czerniak 8, Cohen GL, Etkind P, et al: Concurrent mutations of coding and regulatory sequences of the Ha-ras gene in urinary bladder carcinomas. Hum Pathol 23:1199, 1992
27. Czemiak 8, Deitch D, Simmons H, et a1 Ha-ras gene codon 12 mutation and DNA ploidy in urinary bladder carcinoma. Br J Cancer 62762, 1990
28. Dalbagni G, Presti JC, Jr, Reuter VE, et al: Molecular genetic alterations of chromosome 17 and p53 nu- clear overexpression in human bladder cancer. Di- agn Mol Pathol 24, 1993
29. De Caprio JA, Ludlow JW, Lynch D, et al: The product of the retinoblastoma susceptibility gene has properties of a cell cycle regulatory element. Cell 581085, 1989
30. el-Deiry WS, Tokino T, Velculescu VE, et al: WAFI, a potential mediator of p53 tumor suppression. Cell 75:817, 1993
31. Esrig D, Elmajian D, Groshen S, et al: Accumulation of nuclear p53 and tumor progression in bladder cancer. N Engl J Med 331:1259, 1994
32. Esrig D, Spruck CH, Nichols PW, et al: p53 nuclear protein accumulation correlates with mutations in the p53 gene, tumor grade, and stage in bladder cancer. Am J Pathol 143:1389, 1993
33. Feinberg AP, Vogelstein B, Droller MJ, et a1 Muta- tion affecting the 12th amino acid of the c-Ha-ras oncogene product occurs infrequently in human cancer. Science 220:1175, 1983
34. Field SJ, Tsai FY, Kuo F, et al: E2F-1 functions in mice to promote apoptosis and suppress prolifera- tion. Cell 85549, 1996
35. Fitzgerald JM, Ramchurren N, Rieger K, et al: Iden- tification of H-ras mutations in urine sediments complements cytology in the detection of bladder tumors. J Natl Cancer Inst 87129, 1995
36. Friend SH, Bemards R, Rogelj S, et al: A human DNA segment with properties of the gene that pre- disposes to retinoblastoma and osteosarcoma. Na- ture 323:643, 1986
37. Fujimoto K, Yamada Y, Okajima E, et al: Frequent association of p53 gene mutation in invasive blad- der cancer. Cancer Res 521393, 1992
38. Fujita J, Nakayama H, Onoue H, et al: Frequency of active ras oncogenes in human bladder cancers associated with schistosomiasis. Jpn J Cancer Res 78:915, 1987
39. Fujita J, Srivastava SK, Kraus MH, et a1 Frequency of molecular alterations affecting ras protoonco- genes in human urinary tract tumors. Proc Natl Acad Sci U S A 82:3849, 1985
40. Fujita J, Yoshida 0, Yuasa Y, et al: Ha-ras oncogenes are activated by somatic alterations in human uri- nary tract tumours. Nature 309:464, 1984
41. Furihata M, Inoue K, Ohtsuki Y, et al: High-risk human papillomavirus infections and overexpres- sion of p53 protein as prognostic indicators in tran-
sitional cell carcinoma of the urinary bladder. Can- cer Res 53:4823, 1993
42. Gardiner RA, Walsh MD, Allen V, et al: Immunohis- tological expression of p53 in primary pT1 transi- tional cell bladder cancer in relation to tumour pro- gression. Br J Urol 73:526, 1994
43. Gibas Z, Prout GR, Jr, Connolly JG, et al: Nonran- dom chromosomal changes in transitional cell carci- noma of the bladder. Cancer Res M1257, 1984
44. Gonzalez-Zulueta M, Bender CM, Yang AS, et al: Methylation of the 5' CpG island of the p16/ CDKNZ tumor suppressor gene in normal and transformed human tissues correlates with gene si- lencing. Cancer Res 554531, 1995
45. Gonzalgo ML, Hayashida T, Bender CM, et al: The role of DNA methylation in expression of the p19/ p16 locus in human bladder cancer cell lines. Cancer Res 583245, 1998
46. Goodrich DW, Chen Y, Scully P, et al: Expression of the retinoblastoma gene product in bladder carci- noma cells associates with a low frequency of tumor formation. Cancer Res 521968, 1992
47. Gorgoulis VG, Barbatis C, Poulias I, et al: Molecular and immunohistochemical evaluation of epidermal growth factor receptor and c-erb-B-2 gene product in transitional cell carcinomas of the urinary blad- der: A study in Greek patients. Mod Pathol 8:758, 1995
48. Goto K, Konomoto T, Hayashi K, et al: p53 muta- tions in multiple urothelial carcinomas: A molecular analysis of the development of multiple carcinomas. Mod Pathol 10:428, 1997
49. Grimmond SM, Raghavan D, Russell PJ: Detection of a rare point mutation in Ki-ras of a human blad- der cancer xenograft by polymerase chain reaction and direct sequencing. Urol Res 20121, 1992
50. Grossman HB, Liebert M, Antelo M, et al: p53 and RB expression predict progression in T1 bladder cancer. Clin Cancer Res 4:829, 1998
51. Habuchi T, Kinoshita H, Yamada H, et al: Oncogene amplification in urothelial cancers with p53 gene mutation or MDM2 amplification. J Natl Cancer Inst 861331, 1994
52. Habuchi T, Takahashi R, Yamada H, et al: Influence of cigarette smoking and schistosomiasis on p53 gene mutation in urothelial cancer. Cancer Res 53:3795, 1993
53. Hainaut P, Soussi T, Shomer 8, et al: Database of p53 gene somatic mutations in human tumors and cell lines: Updated compilation and future pros- pects. Nucleic Acids Res 25:151, 1997
54. Hannon GJ, Beach D: p15INK4B is a potential ef- fector of TGF-beta-induced cell cycle arrest. Nature 371257, 1994
55. Harper JW, Adami GR, Wei N, et al: The p21 Cdk- interacting protein Cipl is a potent inhibitor of G1 cyclin-dependent kinases. Cell 75805, 1993
56. Hartmann A, Moser K, Kriegmair M, et al: Frequent genetic alterations in simple urothelial hyperplasias of the bladder in patients with papillary urothelial carcinoma. Am J Pathol 154:721, 1999
57. Haupt Y, Maya R, Kazaz A, et al: Mdm2 promotes the rapid degradation of p53. Nature 387:296, 1997
58. Hopman AH, Moesker 0, Smeets AW, et al: Numer- ical chromosome 1, 7, 9, and 11 aberrations in blad- der cancer detected by in situ hybridization. Cancer Res 51644, 1991
59. Hopman AH, Poddighe PJ, Smeets AW, et al: Detec- tion of numerical chromosome aberrations in blad-
MUTATION OF CELL CYCLE REGULATORS AND SUPERFICIAL BLADDER CANCER 99
der cancer by in situ hybridization. Am J Path01 135:1105, 1989
60. Hopman AH, van Hooren E, van de Kaa CA, et al: Detection of numerical chromosome aberrations using in situ hybridization in paraffin sections of routinely processed bladder cancers. Mod Pathol 4503, 1991
61. Horowitz JM, Park SH, Bogenmann E, et al: Fre- quent inactivation of the retinoblastoma anti-onco- gene is restricted to a subset of human tumor cells. Proc Natl Acad Sci U S A 872775, 1990
62. Hunter T, Pines J: Cyclins and cancer. Cyclin D and CDK inhibitors come of age [see comments]. Cell 79(part 2):573, 1994
63. Ishikawa J, Xu HJ, Hu SX, et al: Inactivation of the retinoblastoma gene in human bladder and renal cell carcinomas. Cancer Res 51:5736, 1991
61. Johnson DG, Cress WD, Jakoi L, et a1 Oncogenic capacity of the E2F1 gene. Proc Natl Acad Sci U S A 91:12823, 1994
65. Johnson DG, Schwarz JK, Cress WD, et al: Expres- sion of transcription factor E2F1 induces quiescent cells to enter S phase. Nature 365349, 1993
66. Kallioniemi A, Kallioniemi OP, Citro G, et al: Identi- fication of gains and losses of DNA sequences in primary bladder cancer by comparative genomic hybridization. Genes Chromosomes Cancer 12213, 1995
67. Knowles MA, Williamson M: Mutation of H-ras is infrequent in bladder cancer: Confirmation by sin- gle-strand conformation polymorphism analysis, designed restriction fragment length polymor- phisms, and direct sequencing. Cancer Res 53:133, 1993
68. Korkolopoulou P, Christodoulou P, Kapralos P, et al: The role of p53, MDM2 and c-erb B-2 oncoproteins, epidermal growth factor receptor and proliferation markers in the prognosis of urinary bladder cancer. Pathol Res Pract 193:767, 1997
69. Kubbutat MH, Jones SN, Vousden KH: Regulation of p53 stability by Mdm2. Nature 387299, 1997
70. Kusser WC, Mia0 X, Glickman BW, et al: p53 muta- tions in human bladder cancer. Environ Mol Muta- gen 24:156, 1994
71. Lacombe L, Dalbagni G, Zhang ZF, et al: Overex- pression of p53 protein in a high-risk population of patients with superficial bladder cancer before and after bacillus Calmette-Guerin therapy: Correlation to clinical outcome. J Clin Oncol 14:2646, 1996
72. Lacombe L, Orlow I, Silver D, et al: Analysis of p21 WAF1 /CIP1 in primary bladder tumors. Oncol Res 8:409, 1996
73. Lebret T, Becette V, Barbagelatta M, et al: Correlation between p53 over expression and response to bacil- lus Calmette-Guerin therapy in a high risk select population of patients with T1G3 bladder cancer. J Urol 159:788, 1998
74. Lee CC, Yamamoto 5, Morimura K, et al: Signifi- cance of cyclin D1 overexpression in transitional cell carcinomas of the urinary bladder and its correla- tion with histopathologic features. Cancer 79:780, 1997
75. Levesque l', Ramchurren N, Saini K, et a1 Screening of human bladder tumors and urine sediments for the presence of H-ras mutations. Int J Cancer 55:785, 1993
76. Levine AJ, Momand J, Finlay CA: The p53 tumour suppressor gene. Nature 351:453, 1991
77. Li 8, Kanamaru H, Noriki S, et al: Reciprocal expres-
sion of bcl-2 and p53 oncoproteins in urothelial dys- plasia and carcinoma of the urinary bladder. Urol Res 26235, 1998
78. Lianes P, Orlow I, Zhang ZF, et al: Altered patterns of h4DMZ and TP53 expression in human bladder cancer [see comments]. J Natl Cancer Inst 863325, 1994
79. Lipponen P: Expression of c-erbB-2 oncoprotein in transitional cell bladder cancer. Eur J Cancer 29A749, 1993
80. Lipponen P, Aaltomaa S, Eskelinen M, et al: Expres- sion of p21 (wafl/cipl) protein in transitional cell bladder tumours and its prognostic value. Eur Urol 34237, 1998
81. Lipponen F, Eskelinen M: Expression of epidermal growth factor receptor in bladder cancer as related to established prognostic factors, oncoprotein (c- erbB-2, p53) expression and long-term prognosis. Br J Cancer 69:1120, 1994
82. Liukkonen TJ, Lipponen PK, Helle M, et al: Immu- noreactivity of bcl-2, p53 and EGFr is associated with tumor stage, grade and cell proliferation in superficial bladder cancer. Finnbladder 111 Group. Urol Res 25:1, 1997
83. Mahdy E, Yoshihiro S, Zech L, et a1 Comparison of comparative genomic hybridization, fluorescence in situ hybridization and flow cytometry in urinary bladder cancer. Anticancer Res 19:7, 1999
84. Malkowicz SB, Tomaszewski JE, Linnenbach AJ, et a1 Novel p21WAFl /CIPI mutations in superficial and invasive transitional cell carcinomas. Oncogene 13:1831, 1996
85. Malone PR, Visvanathan KV, Ponder BA, et al: On- cogenes and bladder cancer. Br J Urol57664, 1985
86. Matsushime H, Roussel MF, Ashmun RA, et al: Col- ony-stimulating factor 1 regulates novel cyclins dur- ing the G1 phase of the cell cycle. Cell 65:701, 1991
87. Matsuyama H, Pan Y, Mahdy EA, et al: p53 deletion as a genetic marker in urothelial tumor by fluores- cence in situ hybridization. Cancer Res 54:6057,1994
88. Mellon K, Wright C, Kelly P, et a1 Long-term out- come related to epidermal growth factor receptor status in bladder cancer. J Urol 153:919, 1995
89. Meloni AM, Peier AM, Haddad FS, et al: A new approach in the diagnosis and follow-up of bladder cancer: FISH analysis of urine, bladder washings, and tumors. Cancer Genet Cytogenet 71:105, 1993
90. Merlo A, Herman JG, Mao L, et a1 5' CpG island methylation is associated with transcriptional silenc- ing of the tumour suppressor pl6/CDKNZ/MTSl in human cancers. Nat Med 1:686, 1995
91. Miyamoto H, Kubota Y, Shuin T, et a1 Analyses of p53 gene mutations in primary human bladder can- cer. Oncol Res 5245, 1993
92. Miyamoto H, Shuin T, Ikeda I, et al: Loss of hetero- zygosity at the p53, RB, DCC and APC tumor sup- pressor gene loci in human bladder cancer. J Urol 155:1444, 1996
93. Miyamoto H, Shuin T, Torigoe S, et al: Retinoblas- toma gene mutations in primary human bladder cancer. Br J Cancer 71:831, 1995
94. Moch H, Sauter G, Moore D, et al: p53 and erbB- 2 protein overexpression are associated with early invasion and metastasis in bladder cancer. Virchows Arch A Pathol Anat Histopathol423329,1993
95. Moore DH, Epstein L, Reeder J, et al: Interlaboratory variability in fluorescence in s i b hybridization anal- ysis: The NCI Bladder Tumor Marker Network. Cy- tometry 25:125, 1996
100 RABBANI & CORDON-CARD0
96. Motokura T, Bloom T, Kim HG, et al: A novel cyclin encoded by a bcll-linked candidate oncogene [see comments]. Nature 350:512, 1991
97. Nakopoulou L, Constantinides C, Papandropoulos J, et al: Evaluation of overexpression of p53 tumor suppressor protein in superficial and invasive tran- sitional cell bladder cancer: Comparison with DNA ploidy. Urology 46:334, 1995
98. Nakopoulou L, Vourlakou C, Zervas A, et al: The prevalence of bcl-2, p53, and Ki-67 immunoreactiv- ity in transitional cell bladder carcinomas and their clinicopathologic correlates. Hum Pathol 29:146, 1998
99. Neal DE, Marsh C, Bennett MK, et al: Epidermal- growth-factor receptors in human bladder cancer: Comparison of invasive and superficial tumours. Lancet 1:366, 1985
100. Neal DE, Sharples L, Smith K, et al: The epidermal growth factor receptor and the prognosis of bladder cancer. Cancer 65:1619, 1990
101. Neal DE, Smith K, Fennelly JA, et al: Epidermal growth factor receptor in human bladder cancer: A comparison of immunohistochemistry and ligand binding. J Urol 141:517, 1989
102. Nemoto R, Nakamura I, Uchida K, et al: Numerical chromosome aberrations in bladder cancer detected by in situ hybridization. Br J Urol 75470, 1995
103. Neuhaus M, Wagner U, Schmid U, et al: Polysomies but not Y chromosome losses have prognostic sig- nificance in pTa/pTl urinary bladder cancer. Hum Pathol 30:81, 1999
104. Nguyen PL, Swanson PE, Jaszcz W, et al: Expression of epidermal growth factor receptor in invasive transitional cell carcinoma of the urinary bladder: A multivariate survival analysis. Am J Clin Pathol 101:166, 1994
105. Okuno H, Kakehi Y, Ogawa 0, et al: Immunocyto- chemical detection of p53 in cultures of exfoliated cells from urine of patients with urothelial cancers. Jpn J Cancer Res 87718, 1996
106. Oliner JD, Kinzler KW, Meltzer PS, et al: Amplifica- tion of a gene encoding a p53-associated protein in human sarcomas. Nature 358:80, 1992
107. Olumi AF, Tsai YC, Nichols PW, et al: Allelic loss of chromosome 17p distinguishes high grade from low grade transitional cell carcinomas of the bladder. Cancer Res 50:7081, 1990
108. Orlow I, Lacombe L, Hannon GJ, et al: Deletion of the p16 and p15 genes in human bladder tumors. J Natl Cancer Inst 871524, 1995
109. Orlow I, LaRue H, Osman I, et al: Deletions of the INK4A gene in superficial bladder tumors: Associa- tion with recurrence. Am J Pathol 155105, 1999
110. Ovesen H, Horn T, Steven K Long-term efficacy of intravesical bacillus Calmette-Guerin for carcinoma in situ: Relationship of progression to histological response and p53 nuclear accumulation. J Urol 1571655, 1997
111. Oyasu R, Nan L, Szumel RC, et al: p53 gene muta- tions in human urothelial carcinomas: Analysis by immunohistochemistry and single-strand conforma- tion polymorphism. Mod Pathol 8170, 1995
112. Pages F, Flam TA, Viellefond A, et al: p53 status does not predict initial clinical response to bacillus Calmette-Guerin intravesical therapy in T1 bladder tumors. J Urol 159:1079, 1998
113. Pfister C, Buzelin F, Casse C, et al: Comparative analysis of MiBl and p53 expression in human blad- der tumors and their correlation with cancer pro- gression. Eur Urol 33278, 1998
114. Plastiras D, Moutzouris G, Barbatis C, et al: Can p53 nuclear over-expression, Bcl-2 accumulation and PCNA status be of prognostic significance in high- risk superficial and invasive bladder tumours? Eur J Surg Oncol 25:61, 1999
115. Pomerantz J, Schreiber-Agus N, Liegeois NJ, et al: The Ink4a tumor suppressor gene product, pl9Arf, interacts with MDM2 and neutralizes MDM2's inhi- bition of p53. Cell 92713, 1998
116. Popov Z, Hoznek A, Colombel M, et al: The prog- nostic value of p53 nuclear overexpression and MIB- 1 as a proliferative marker in transitional cell carci- noma of the bladder. Cancer 80:1472, 1997
117. Presti JC, Jr, Reuter VE, Galan T, et al: Molecular genetic alterations in superficial and locally ad- vanced human bladder cancer. Cancer Res 51:5405, 1991
118. Pycha A, Mian C, Haitel A, et al: Fluorescence in situ hybridization identifies more aggressive types of primarily noninvasive (stage pTa) bladder cancer. J Urol 1572116, 1997
119. Rabbani F, Richon VM, Orlow I, et al: Prognostic significance of transcription factor E2F-1 in bladder cancer: Genotypic and phenotypic characterization. J Natl Cancer Inst 91:874, 1999
120. Ravery V, Colombel M, Popov 2, et al: Prognostic value of epidermal growth factor-receptor, T138 and T43 expression in bladder cancer. Br J Cancer 71:196, 1995
121. Ravery V, Grignon D, Angulo J, et al: Evaluation of epidermal growth factor receptor, transforming growth factor alpha, epidermal growth factor and c-erbB2 in the progression of invasive bladder can- cer. Urol Res 25:9, 1997
122. Reddy El', Reynolds RK, Santos E, et al: A point mutation is responsible for the acquisition of trans- forming properties by the T24 human bladder carci- noma oncogene. Nature 300:149, 1982
123. Reeder JE, Morreale JF, OConnell MJ, et al: Loss of the CDKN2A/pl6 locus detected in bladder irriga- tion specimens by fluorescence in situ hybridization. J Urol 158:1717, 1997
124. Reuter VE, Melamed MR The lower urinary tract. In Stemberg SS (ed): Diagnostic Surgical Pathology. New York, Raven Press, 1989, p 1355
125. Righi E, Rossi G, Ferrari G, et al: Does p53 immuno- staining improve diagnostic accuracy in urine cytol- ogy? Diagn Cytopathol 17436, 1997
126. Rotter V, Prokocimer M: p53 and human malignan- cies. Adv Cancer Res 57:257, 1991
127. Sandberg AA, Berger CS: Review of chromosome studies in urological tumors. Cytogenetics and mo- lecular genetics of bladder cancer. J Urol 15l(part 2):545, 1994
128. Sarkis AS, Dalbagni G, Cordon-Cardo C, et al: Asso- ciation of P53 nuclear overexpression and tumor progression in carcinoma in situ of the bladder. J Urol 152:388, 1994
129. Sarkis AS, Dalbagni G, Cordon-Cardo C, et al: Nu- clear overexpression of p53 protein in transitional cell bladder carcinoma: A marker for disease pro- gression. J Natl Cancer Inst 85:53, 1993
130. Sat0 K, Moriyama M, Mori S, et al: An immunohis- tologic evaluation of C-erbB-2 gene product in pa- tients with urinary bladder carcinoma. Cancer 70:2493, 1992
131. Sauter G, Carroll P, Moch H, et al: c-myc Copy number gains in bladder cancer detected by fluo- rescence in situ hybridization. Am J Pathol 1461131, 1995
MUTATION OF CELL CYCLE REGULATORS AND SUPERFICIAL BLADDER CANCER 101
132. Sauter G, Deng G, Moch H, et al: Physical deletion of the p53 gene in bladder cancer: Detection by fluorescence in situ hybridization. Am J Pathol 144:756, 1994
133. Sauter G, Gasser TC, Moch H, et al: DNA aberra- tions in urinary bladder cancer detected by flow cytometry and FISH. Urol Res 25(suppl 1):37, 1997
134. Sauter G, Moch H, Carroll P, et al: Chromosome-9 loss detected by fluorescence in situ hybridization in bladder cancer. Int J Cancer 6499, 1995
135. Sauter G, Moch H, Mihatsch MJ, et al: Molecular cytogenetics of bladder cancer progression. Eur Urol 33(suppl 4):9, 1998
136. Sauter G, Moch H, Moore D, et al: Heterogeneity of erbB-2 gene amplification in bladder cancer. Cancer Res 532199, 1993
137. Sauter G, Moch H, Wagner U, et al: Y chromosome loss detected by FISH in bladder cancer. Cancer Genet Cytogenet 82163, 1995
138. Schapers R, Smeets W, Hopman A, et a1 Heteroge- neity in bladder cancer as detected by conventional chromosome analysis and interphase cytogenetics. Cancer Genet Cytogenet 70:56, 1993
139. Schmitz-Drager BJ, Kushima M, Goebell P, et al: p53 and MDM2 in the development and progression of bladder cancer. Eur Urol32487, 1997
140. Serio G: PCNA/cyclin expression in transitional cell carcinomas of the human bladder: Its correlation with Ki-67 and epidermal growth factor receptor immunostainings. Pathologica 86161, 1994
141. Serrano M, Hannon GJ, Beach D: A new regulatory motif in cell-cycle control causing specific inhibition of cyclin D/CDK4. Nature 366:704, 1993
142. Serth J, Kuczyk MA, Bokemeyer C, et al: p53 immu- nohistochemistry as an independent prognostic fac- tor for superficial transitional cell carcinoma of the bladder. Br J Cancer 71201, 1995
143. Shiina H, Igawa M, Nagami H, et al: Immunohisto- chemical analysis of proliferating cell nuclear anti- gen, p53 protein and nm23 protein, and nuclear DNA content in transitional cell carcinoma of the bladder. Cancer 781762, 1996
144. Shiina H, Igawa M, Shigeno K, et al: Clinical sig- nificance of mdm2 and p53 expression in bladder cancer: A comparison with cell proliferation and apoptosis. Oncology 56239,1999
145. Shin KY, Kong G, Kim WS, et a1 Overexpression of cyclin D1 correlates with early recurrence in super- ficial bladder cancers. Br J Cancer 751788, 1997
146. Sidransky D, Von Eschenbach A, Tsai YC, et al: Identification of p53 gene mutations in bladder can- cers and urine samples. Science 252706, 1991
147. Sigalas I, Calvert AH, Anderson JJ, et al: Altema- tively spliced mdm2 transcripts with loss of p53 binding domain sequences: Transforming ability and frequent detection in human cancer. Nat Med 2912, 1996
148. Skopelitou A, Hadjiyannakis M, Dimopoulos D, et al: p53 and c-jun expression in urinary bladder tran- sitional cell carcinoma: Correlation with proliferat- ing cell nuclear antigen (PCNA) histological grade and clinical stage. Eur Urol 31:464, 1997
149. Smeets W, Schapers R, Hopman A, et al: Concor- dance between karyotyping and in situ hybridiza- tion procedures in the detection of monosomy 9 in bladder cancer. Cancer Genet Cytogenet 71:97, 1993
150. Smith K, Fennelly JA, Neal DE, et a1 Characteriza- tion and quantitation of the epidermal growth factor receptor in invasive and superficial bladder tumors. Cancer Res 49:5810, 1989
151.
152.
153.
154.
155.
156.
157.
158.
159.
160.
161.
162.
163.
164.
165.
166.
167.
168.
Soini Y, Turpeenniemi-Hujanen T, Kame1 D, et a1 p53 Immunohistochemistry in transitional cell carci- noma and dysplasia of the urinary bladder corre- lates with disease progression. Br J Cancer 68:1029, 1993 Ssrlie T, Martel-Planche G, Hainaut P, et al: Analysis of p53, pl6MTS, p21WAF1 and H-ras in archived bladder tumours from workers exposed to aromatic amines. Br J Cancer 77:1573, 1998 Sriplakich S, Jahnson S, Karlsson MG: Epidermal growth factor receptor expression: Predictive value for the outcome after cystectomy for bladder cancer? BJU Int 83498, 1999 Stein JP, Ginsberg DA, Grossfeld GD, et al: Effect of p21WAF1/ CIPl expression on tumor progression in bladder cancer. J Natl Cancer Inst 90:1072, 1998 Tabin CJ, Bradley SM, Bargmann CI, et al: Mecha- nism of activation of a human oncogene. Nature 300.143, 1982 Takahashi R, Hashimoto T, Xu HJ, et al: The retino- blastoma gene functions as a growth and tumor suppressor in human bladder carcinoma cells. Proc Natl Acad Sci U S A 88:5257, 1991 Tenti P, Zappatore R, Romagnoli S, et al: p53 Over- expression and human papillomavirus infection in transitional cell carcinoma of the urinary bladder: Correlation with histological parameters. J Pathol 17865, 1996 Tetu B, Fradet Y, Allard P, et al: Prevalence and clinical significance of HER/2neu, p53 and Rb ex- pression in primary superficial bladder cancer. J Urol 155:1784, 1996 Theodorescu D, Laderoute KR, Gulding KM: Epi- dermal growth factor receptor-regulated human bladder cancer motility is in part a phosphatidylino- sitol 3-kinase-mediated process. Cell Growth Differ 9:919, 1998 Thomas DJ, Robinson MC, Charlton R, et al: P53 expression, ploidy and progression in pT1 transi- tional cell carcinoma of the bladder. Br J Urol 73:533, 1994 Tsai YC, Nichols PW, Hiti AL, et al: Allelic losses of chromosomes 9, 11, and 17 in human bladder can- cer. Cancer Res 5044, 1990 Tsuji M, Kojima K, Murakami Y, et al: Prognostic value of Ki-67 antigen and p53 protein in urinary bladder cancer: Immunohistochemical analysis of radical cystectomy specimens. Br J Urol 79:367,1997 Uchida T, Wada C, Ishida H, et al: p53 Mutations and prognosis in bladder tumors. J Urol 1533097, 1995 Underwood MA, Reeves J, Smith G, et al: Overex- pression of p53 protein and its significance for re- current progressive bladder tumours. Br J Urol 77:659, 1996 Valenzuela DM, Groffen J: Four human carcinoma cell lines with novel mutations in position 12 of c-K-ras oncogene. Nucleic Acids Res 14843, 1986 Vatne V, Maartmann-Moe H, Hoestmark J: Flow cytometric DNA and p53 analysis in superficially infiltrating bladder carcinoma. Anticancer Res 142735, 1994 Vatne V, Maartmann-Moe H, Hoestmark J: The prognostic value of p53 in superficially infiltrating transitional cell carcinoma. Scand J Urol Nephrol 29491, 1995 Vet JA, Bringuier PP, Poddighe PJ, et al: p53 Muta- tions have no additional prognostic value over stage in bladder cancer. Br J Cancer 70:496, 1994
102 RABBANI & CORDON-CARD0
169. Vet JA, Bringuier PP, Schaafsma HE, et al: Compari- son of P53 protein overexpression with P53 muta- tion in bladder cancer: Clinical and biologic aspects. Lab Invest 73:837, 1995
170. Vet JA, Hessels D, Marras SA, et al: Comparative analysis of p53 mutations in bladder washings and histologic specimens. Am J Clin Patholl10647,1998
171. Viola MV, Fromowitz F, Oravez S, et al: ras Onco- gene p21 expression is increased in premalignant lesions and high grade bladder carcinoma. J Exp Med 161:1213, 1985
172. Voorter C, Joos S, Bringuier PP, et al: Detection of chromosomal imbalances in transitional cell carci- noma of the bladder by comparative genomic hy- bridization. Am J Pathol 146:1341, 1995
173. Waga S, Hannon GJ, Beach D, et al: The p21 inhibi- tor of cyclin-dependent kinases controls DNA repli- cation by interaction with PCNA. Nature 369:574, 1994
174. Wagner U, Bubendorf L, Gasser TC, et al: Chromo- some 8p deletions are associated with invasive tu- mor growth in urinary bladder cancer. Am J Pathol 151:753, 1997
175. Wagner U, Sauter G, Moch H, et al: Patterns of p53, erbB-2, and EGF-r expression in premalignant lesions of the urinary bladder. Hum Pathol 26:970, 1995
176. Waldman FM, Carroll PR, Kerschmann R, et al: Cen- tromeric copy number of chromosome 7 is strongly correlated with tumor grade and labeling index in human bladder cancer. Cancer Res 51:3807, 1991
177. Warren W, Biggs PJ, el-Baz M, et al: Mutations in the p53 gene in schistosomal bladder cancer: A study of 92 tumours from Egyptian patients and a compari- son between mutational spectra from schistosomal and non-schistosomal urothelial tumours. Carcino- genesis 1&1181, 1995
178. Wheeless LL, Reeder JE, Han R, et al: Bladder irriga- tion specimens assayed by fluorescence in situ hy- bridization to interphase nuclei. Cytometry 17:319, 1994
179. Wood DP, Jr, Anderson AE, Fair R, et al: Ras onco- gene point mutations in bladder cancer resistant to cisplatin. Urol Res 20313, 1992
180. Wood DP, Jr, Fair WR, Chaganti RS: Evaluation of epidermal growth factor receptor DNA amplifica-
tion and mRNA expression in bladder cancer. J Urol 147:274, 1992
181. Wood DP, Jr, Wartinger DD, Reuter V, et al: DNA, RNA and immunohistochemical characterization of the HER-Z/neu oncogene in transitional cell carci- noma of the bladder. J Urol 146:1398, 1991
182. Wright C, Thomas D, Mellon K, et al: Expression of retinoblastoma gene product and p53 protein in bladder carcinoma: Correlation with Ki67-index. Br 1 Urol 75:173, 1995
183. Xu HJ, Cairns P, Hu SX, et al: Loss of RB protein expression in primary bladder cancer correlates with loss of heterozygosity at the RB locus and tumor progression. Int J Cancer 53:781, 1993
184. Xu X, Stower MJ, Reid IN, et al: Molecular screening of multifocal transitional cell carcinoma of the blad- der using p53 mutations as biomarkers. Clin Cancer Res 21795, 1996
185. Yamasaki L, Jacks T, Bronson R, et a1 Tumor induc- tion and tissue atrophy in mice lacking E2F-1. Cell 85:537, 1996
186. Yasunaga Y, Nakanishi H, Naka N, et al: Alterations of the p53 gene in occupational bladder cancer in workers exposed to aromatic amines. Lab Invest 77:677, 1997
187. Ye DW, Zheng JF, Qian SX, et al: Expression of p53 product in Chinese human bladder carcinoma. Urol Res 21:223, 1993
188. Zhang FF, Arber DA, Wilson TG, et al: Toward the validation of aneusomy detection by fluorescence in situ hybridization in bladder cancer: Comparative analysis with cytology, cytogenetics, and clinical fea- tures predicts recurrence and defines clinical testing limitations. Clin Cancer Res 3:2317, 1997
189. Zhang Z-F, Steineck G: Epidemiology and etiology of bladder cancer. In Raghavan D, Scher HI, Leibel SA, et a1 (eds): Principles and Practice of Genitouri- nary Oncology. Philadelphia, JB Lippincott, 1996, p 215
190. Zhau HE, Zhang X, von Eschenbach AC, et al: Am- plification and expression of the c-erb B-2/neu proto-oncogene in human bladder cancer. Mol Car- cinog 3:254, 1990
191. Zlotta AR, Noel JC, Fayt I, et a1 Correlation and prognostic significance of p53, p21WAF1/ CIPl and Ki-67 expression in patients with superficial bladder tumors treated with bacillus Calmette-Guerin in- travesical therapy. J Urol 161:792, 1999
Address reprint requests to Carlos Cordon-Cardo, MD
Director, Division of Molecular Pathology Memorial Sloan-Kettering Cancer Center
Room S-801 1275 York Avenue
New York, NY 10021
E-mail: [email protected]





























