Embed Size (px)
Citation preview
Acta Neurochir (Wien) (1992) 116:23-32 :Acta N&?ochirurgica �9 Springer-Verlag 1992 Printed in Austria
Neurosurgical Experience with Tumours of the Pineal Region at Clinica Puerta de Hierro
J. Vaquero, J. Ramiro, R. Martinez, and G. Bravo
Department of Neurosurgery, Clinica Puerta de Hierro, Autonomous University, Madrid, Spain
Summary
The clinicopathological experience with 50 cases of pineal region tumours at Clinica Puerta de Hierro is presented. In this series, 88% of the patients were evaluated by CT-scan. Pineal region turnouts make up approximately 0.7 % of the intracranial expansive processes in the Spanish population. The largest group of lesions appearing in this localization is that of the germinomas (38%), followed by nontumoural lesions (20%) and tumours generally considered to be of the vicinity, such as meningiomas, gliomas and metastases (18 %), tumours of the pineal parenchyma (14%), and non-germinoma ger- minal tumours (10%).
In our series, in addition to an intracranial hypertension syn- drome, an ophthalmological and, to a minor degree, an endocrino- logical syndrome predominate in germ-cell tumours, with a cerebellar syndrome appearing in gliomas of the pineal region.
All the patients in the series diagnosed as having a germinoma and treated by irradiation are alive, and free of disease, after follow- up ranging from 2 to 20 years (mean: 8 years). The experience ob- tained with the present series supports the opinion that, in radio- sensitive tumours, surgical resection adds no therapeutic benefit to treatment with radiotherapy alone.
We suggest that when dealing with a turnout of the pineal region, CT-scan and clinical assessment now permit an initial selection of patients susceptible to surgery as a first therapeutic option, indicating those patients who, because they are considered to have either a "probable germinoma" or a "tumour of uncertain diagnosis", should undergo stereotaxic biopsy or trial radiotherapy and, only when this has proved a failure, should be subjected to open surgery.
Keywords: Brain tumour; pineal tumour, radiation therapy.
Introduction
Over the last 20 years, 50 patients with tumour of the pineal region were studied in the Service of Neu- rosurgery of Clinica Puerta de Hierro in Madrid. This series consists of 31 verified tumours and 19 unverified.
The purpose of this work is to report our clinico- pathological experience with these lesions and to ana- lyze the different therapeutic options which have been
used in this series. We have intentionally excluded su- prasellar germinomas as we consider that, given their anatomical location, their clinical picture is different. On the other hand, we have included nontumoural expansive processes to assess their relative incidence among the Spanish population with respect to the to- tality of pineal region masses.
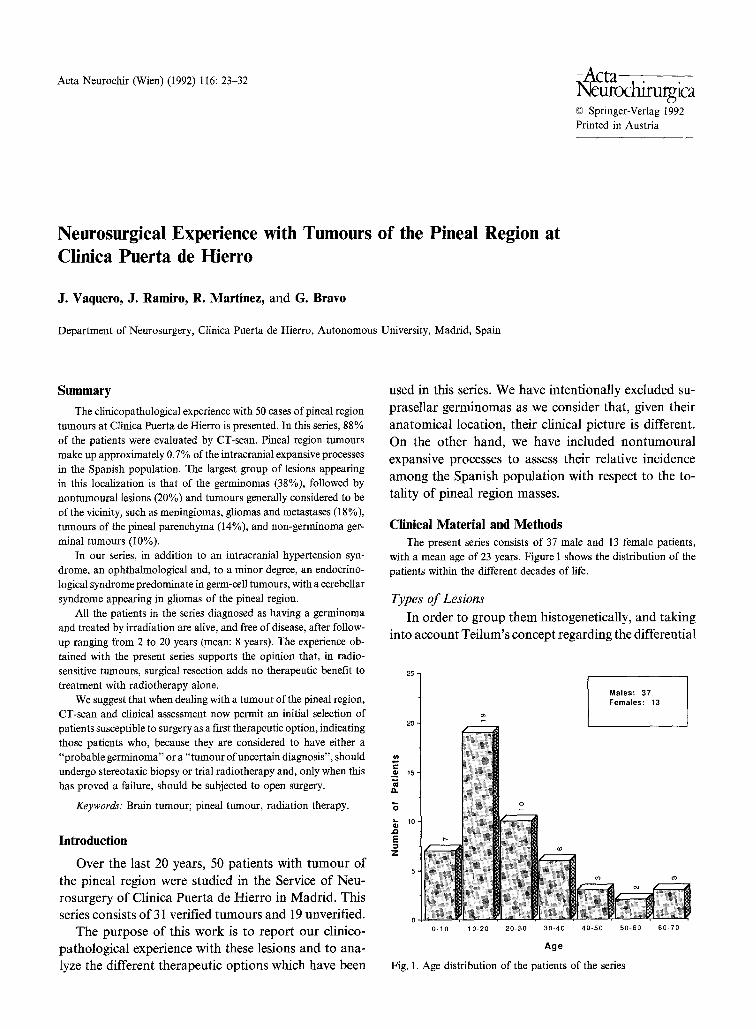
Clinical Material and Methods The present series consists of 37 male and 13 female patients,
with a mean age of 23 years. Figure 1 shows the distribution of the patients within the different decades of life.
Types of Lesions In order to group them histogenetically, and taking
into account Teilum's concept regarding the differential
2 5 -
r
O;
13.
JO E
20
16-
10"
0 - 1 0 1 0 - 2 0
o
2 0 - 3 0 3 0 - 4 0 4 0 - 5 0
Age
Fig. 1. Age distribution of the patients of the series
Males: 37 Females: 13
50-60 6 0 - 7 0
24 J. Vaquero et aL: Neurosurgical Experience with Tumours of the Pineal Region at Clinica Puerta de Hierro
Table 1. Classification and Number of Pineal Region Lesions Seen at the Clinica Puerta de Hierro from 1970 to 1989
- Germ-cell origin (24)
TUMOURS (40)
Gerrninoma (19)
Embryonal carcinoma (2)
Ohoriocarcinoma
--Endoderma[ sinus tumour
--Benign teratoma (1)
/Ep idermoid cyst - - T e r a t o i d (
\ Dermoid cyst
-- Malignant teratoma (2)
- Pineocytoma (4)
. _ ~ Pineoblastoma (3)
-- originNeur~176 b G licmas (5)
L Others
- - Meningioma (2) Mesodermic ~ _
- - o r i g i n (2) Others
-- Other tumours (2)
NON-TUMOURAL LESIONS (10) ~ Glial cysts (2)
Arachnold cysts (3)
Parasitic cysts (1)
Vascular hamartomas (4) Others
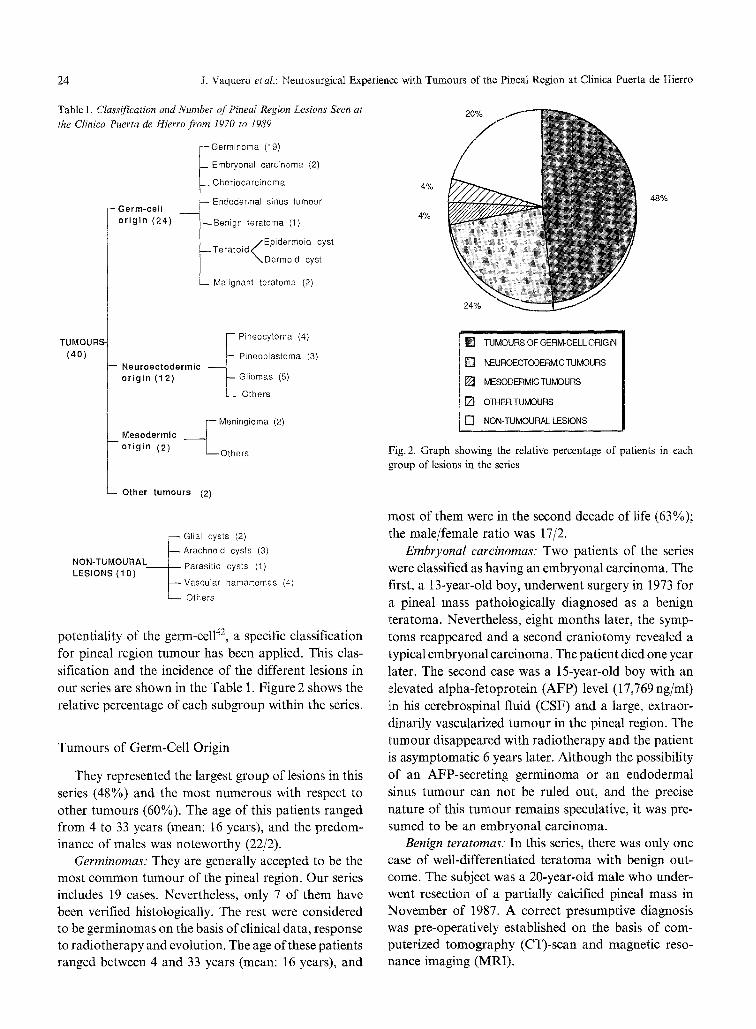
potentiality of the germ-cell 42, a specific classification for pineal region tumour has been applied. This clas- sification and the incidence of the different lesions in our series are shown in the Table 1. Figure 2 shows the relative percentage of each subgroup within the series.
Tumours of Germ-Cell Origin
They represented the largest group of lesions in this series (48%) and the most numerous with respect to other tumours (60%). The age of this patients ranged from 4 to 33 years (mean: 16 years), and the predom- inance of males was noteworthy (22/2).
Germinomas: They are generally accepted to be the most common tumour of the pineal region. Our series includes 19 cases. Nevertheless, only 7 of them have been verified histologically. The rest were considered to be germinomas on the basis of clinical data, response to radiotherapy and evolution. The age of these patients ranged between 4 and 33 years (mean: 16 years), and
4%
4%
48%
[ ] TUMOURS OF GERM-CELL ORIGIN
[ ] NEUROECTODERMIC TUMOURS
[ ] MESODERMIC TUMOURS
[ ] OTHER TUMOURS
[ ] NON-TUMOURAL LESIONS
Fig. 2. Graph showing the relative percentage of patients in each group of lesions in the series
most of them were in the second decade of life (63%); the male/female ratio was 17/2.
Embryonal carcinomas: Two patients of the series were classified as having an embryonal carcinoma. The first, a 13-year-old boy, underwent surgery in 1973 for a pineal mass pathologically diagnosed as a benign teratoma. Nevertheless, eight months later, the symp- toms reappeared and a second craniotomy revealed a typical embryonal carcinoma. The patient died one year later. The second case was a 15-year-old boy with an elevated alpha-fetoprotein (AFP) level (17,769 ng/ml) in his cerebrospinal fluid (CSF) and a large, extraor- dinarily vascularized tumour in the pineal region. The tumour disappeared with radiotherapy and the patient is asymptomatic 6 years later. Although the possibility of an AFP-secreting germinoma or an endodermal sinus tumour can not be ruled out, and the precise nature of this tumour remains speculative, it was pre- sumed to be an embryonal carcinoma.
Benign teratomas: In this series, there was only one case of well-differentiated teratoma with benign out- come. The subject was a 20-year-old male who under- went resection of a partially calcified pineal mass in November of 1987. A correct presumptive diagnosis was pre-operatively established on the basis of com- puterized tomography (CT)-scan and magnetic reso- nance imaging (MRI).
J, Vaquero et al.: Neurosurgical Experience with Tumours of the Pineal Region at Clinica Puerta de Hierro 25
Malignant teratomas: Two such cases are reported in our series. The first was a 32-year-old male with an AFP-secreting pineal tumour, that was treated with chemotherapy and radiotherapy after a ventriculoper- itonal shunt had been performed in another hospital. The patient died two years later due to bone marrow aplasia and sepsis, and necropsy revealed a terato- matous lesion mainly composed of epidermoid cystic tissue. The second case was a 14-year-old male whose tumour was surgically verified and irradiated. He died one year later.
Tumours of Neuroectodermal Origin
This group represented 24% of the cases in the series and 30% when only tumoural lesions are considered. The age range was 18 months to 63 years (mean: 24 years), and the male/female ration was 7/5.
Pineocytomas." Four patients of the present series were surgically treated for pineocytoma. These patients ranged in age between 12 and 44 years (mean: 22,5 years) with a male/female ration of 3/1. All the cases showed signs of neuronal differentiation in the pathological study, according to the criteria of Rubinstein 31, and they have been included in a previ- ously reported series 47.
Pineoblastomas." Three patients of the series, aged 18 months and 6 and 48 years, underwent removal of a pineoblastoma. All were females and they died, be- cause of their diseases, at ages of 4.9 and 55 years, respectively.
Gliomas: This subgroup consisted of five patients. Two male patients, with tumours pathologically di- agnosed as astrocytomas, were 3 and 2l years old, respectively, at operation, and they are alive, 12 and 4 years after surgery. A 6-year-old female underwent sur- gery for a malignant astrocytoma, and she died four months later due to progression of residual tumour. Two males were 50 and 63 years when a diagnosis of glioblastoma multiforme was established. One of these cases was surgically verified, and both patients died six months after diagnosis.
Tumour of Mesodermic Origin
In this subgroup, we include two patients success- fully operated on for meningioma affecting the pineal region. One was a 36-year-old female with seizures, and the other was a 60-year-old male with progressive loss of intellectual function. Both patients are symptom- free, after 6 and 4 years of follow-up.
Other Tumours
In this subgroup were two patients with metastatic tumours. One was a 64-year-old man with a confirmed bronchial carcinoma, who developed a single brain me- tastasis restricted to the pineal origin. He underwent a ventriculoperitoneal shunt as a palliative measure, and died one month later. The other case was a 37-year- old female, subjected to surgery for a pineal region tumour with brain stem involvement, which was found to be a melanoma. A few weeks after surgery, systemic dissemination from an alleged primary skin melanoma was disclosed, and she died two months after diagnosis.
Nontumoural Lesions
Ten patients of the series (20%) had expansive non- tumoural lesions: 2 glial cysts, 3 arachnoid cysts, 1 case of cysticerosis, 1 case of arteriovenous malformation, and 3 cavernous angiomas. Some of these cases have been described in detail previously 4.-46.
Clinical Syndromes
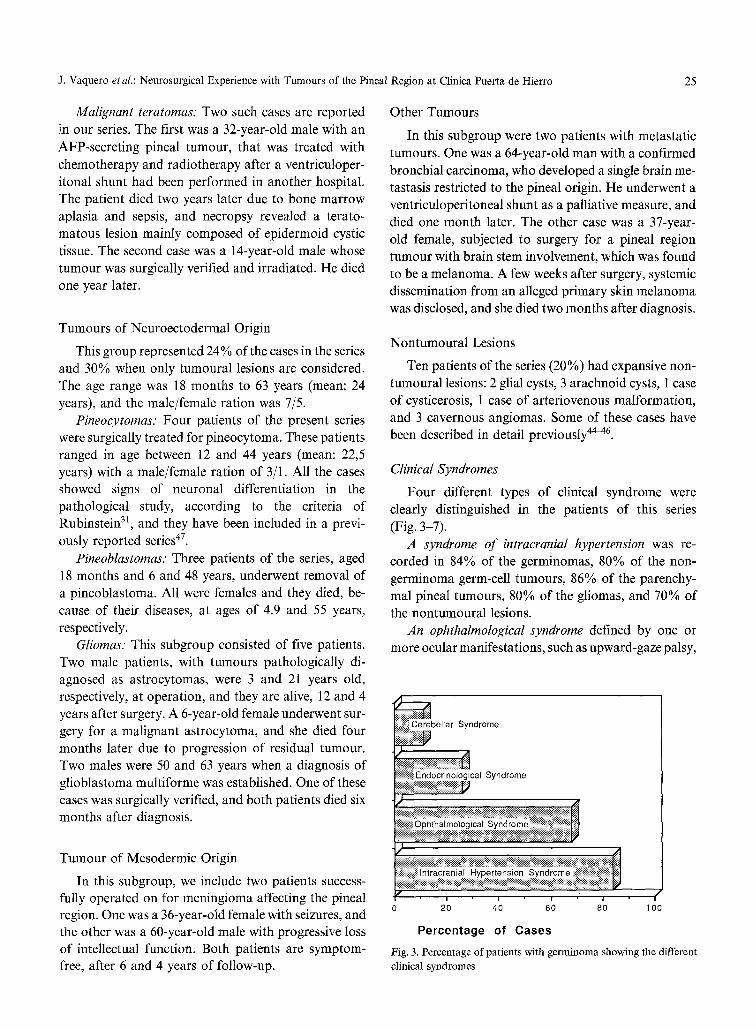
Four different types of clinical syndrome were clearly distinguished in the patients of this series (Fig. 3-7).
A syndrome of intracranial hypertension was re- corded in 84% of the germinomas, 80% of the non- germinoma germ-cell tumours, 86% of the parenchy- real pineal tumours, 80% of the gliomas, and 70% of the nontumoural lesions.
An ophthalmological syndrome defined by one or more ocular manifestations, such as upward-gaze palsy,
~ bellar Syndrome
os~:~jnoli~oal ynd me
. . . . . .
I i I I
0 20 40 60 80 1 O0
Percentage of Cases
Fig. 3. Percentage of patients with germinoma showing the different clinical syndromes
26 J. Vaquero eta/.: Neurosurgical Experience with Tumours of the Pineal Region at Clinica Puerta de Hierro
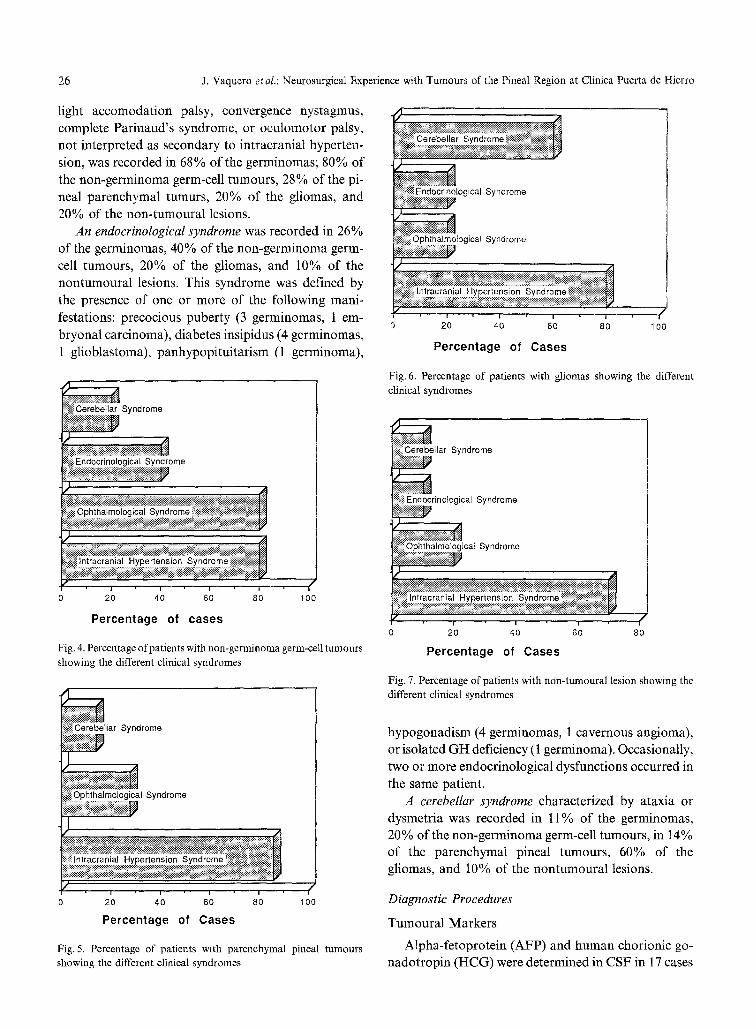
light accomodation palsy, convergence nystagmus, complete Parinaud's syndrome, or oculomotor palsy, not interpreted as secondary to intracranial hyperten- sion, was recorded in 68% of the germinomas; 80% of the non-germinoma germ-cell tumours, 28% of the pi- neal parenchymal tumurs, 20% of the gliomas, and 20% of the non-tumoural lesions.
An endocrinologieal syndrome was recorded in 26% of the germinomas, 40% of the non-germinoma germ- cell tumours, 20% of the gliomas, and 10% of the nontumoural lesions. This syndrome was defined by the presence of one or more of the following mani- festations: precocious puberty (3 germinomas, 1 em- bryonal carcinoma), diabetes insipidus (4 germinomas, 1 glioblastoma), panhypopituitarism (1 germinoma),
ndrome
ilii~: E:n:d ~ ~176 g::!c:a:~:,S Y:n d ! ~
iiiiiiiii ;;im'XCo;c' " ; ;o;;iiiii ii',N i iiiiNiiiii!i!i
iiii#~iiii~ii~iiii~ii~iiiiiiii~ii~ii~ii~i~N~iiii~ii~iiiiiiiiii~iii~i~ii~iiiiiii~iiii~iii~iiiiiiii~ii~i~iiii~ ~il
0 20 40 60 80 100
Percentage of cases
Fig. 4. Percentage of patients with non-germinoma germ-cell tumours showing the different clinical syndromes
Cerebellar Syndrome
I Syndrome
iNiNNiiiiiiii /
;g 7;;n;;i%;; eg;',o % ;o 'g:N!iiliiii i:iiii!iiiiiiii
20 40 60 80
Percentage of Cases
100
Fig. 5. Percentage of patients with parenchymal pineal tumours showing the different clinical syndromes
0 20 40 60 80 100
Percentage of Cases
Fig. 6. Percentage of patients with gliomas showing the different clinical syndromes
~ llar Syndrome
al Syndrome
N:~i%!i~ii;;i~:i!;::;iiiiii!~i~iiNi~i~i .:
I~i;il Intracranial Hypertens on Syndrome ~i~iii~il;;~ii!~iiiiiiiiii~i~!i
[g" , ,
0 2; 40 60
Percentage of Cases
L
J 80
Fig. 7. Percentage of patients with non-tumoural lesion showing the different clinical syndromes
hypogonadism (4 germinomas, 1 cavernous angioma), or isolated GH deficiency (1 germinoma). Occasionally, two or more endocrinological dysfunctions occurred in the same patient.
A cerebellar syndrome characterized by ataxia or dysmetria was recorded in 11% of the germinomas, 20% of the non-germinoma germ-cell tumours, in 14% of the parenchymal pineal tumours, 60% of the gliomas, and 10% of the nontumoural lesions.
Diagnostic Procedures
Tumoural Markers
Alpha-fetoprotein (AFP) and human chorionic go- nadotropin (HCG) were determined in CSF in 17 cases
J. Vaquero etal.: Neurosurgical Experience with Turnours of the Pineal Region at Clinica Puerta de Hierro 27
of the series, in which the final diagnoses were ger- minoma (9 cases), embryonal carcinoma (1 case), be- nign teratoma (1 case), pineocytoma (2 cases), astro- cytoma (2 cases) and glioblastoma (1 case). Positivity was found in only four cases. The first was a 7-year- old male with unverified tumour, undergoing preco- cious puberty and with elevated levels of HCG in CSF (400 mU/cc). This patient was initially presumptively diagnosed as having a choriocarcinoma, but his dra- matic response to radiotherapy and the benign outcome (symptom-free and no sign of disease 7 years later) led us to consider this case in the present series as possible HCG-secreting germinoma. Nevertheless, the true his- tological nature of this tumour remains a subject of speculation.
Another case, a 33-year-old male with diabetes in- sipidus and hypopituitarism, was found by CT-scan to have tumoural masses in the pineal and suprasellar regions, and the level of AFP in CSF was 320 ng/cc. His lesions disappeared rapidly with radiotherapy, and the patient is symptom-free and shows no evidence of disease 10 years later. On the basis of these data, a diagnosis of AFP-secreting germinoma has been es- tablished.
The third case corresponded to a 32-year-old male, treated with chemotherapy and radiotherapy, whose CSF AFP value was 1,845 ng/cc. The patient died two years after diagnosis and a presumptive diagnosis of malignant teratoma with areas of endodermal sinus tumour was established.
The fourth case was a 15-year old male with a highly vascularized tumour and AFP values in CSF of 17,769 ng/cc. The lesion disappeared with radiotherapy and, six years later, the patient is symptom-free and shows no signs of disease. Although in this case, as we reported earlier, the final diagnosis remains speculative, it was classified as a supposed embryonal carcinoma.
CSF Cytology
This was performed in 9 patients (6 germinomas, 1 benign teratoma, 1 malignant teratoma and 1 astro- cytoma), but did not reveal positivity in any of these cases.
CT-Scan
This investigation was carried out in 44 patients of the series (17 germinomas, 3 pineocytomas, 3 pineo- blastomas, 3 astrocytomas, 3 arachnoid cysts, 3 ca- vernous angiomas, 2 glioblastomas, 2 meningiomas, 2
metastases, 2 glial cysts, 1 benign teratoma, 1 malignant teratoma, 1 cystic cysticerosis, and 1 arteriovenous mal- formation). All the cases showed moderate to signifi- cant hydrocephalus at the time of CT-scan. In the larg- est group of germinomas, the characteristic CT-scan pattern was that of a hyperdense mass enhanced after contract administration (100%) and frequently envel- oping a rounded pineal calcification (40%).
CT-scan in pineocytomas showed calcification and cystic features, with an isodense tumoural zone that became enhanced after contrast administration.
In the CT-scan study of the 3 pineoblastomas of the series, 2 were found to be hyperdense and the third was isodense. All showed enhancement after contrast ad- ministration.
Magnetic Resonance Imaging (MRI)
This was performed in 6 of the most recent cases of the series (2 pineocytomas, 1 benign teratoma, 1 glial cyst, 1 astroeytoma and 1 metastatic tumour). The two cystic pineocytomas and the glial cyst showed hypo- intense signal on T1 and hyperintense signal on T2 weighted images. In the benign teratoma, MRI was useful in identifying areas of fatty tissue, blood an necrosis in the turnout.
Analysis of Treatment
Shunting Procedures
In 33 cases of the series (66%), a shunting procedure was performed to correct the hydrocephalus as a step prior to surgery of radiotherapy.
Surgical Approaches and Related Mortality
Surgery was performed in 29 cases (58%) of the series, either as an initial therapeutic attempt (23 cases) or after a lack of response to radiotherapy (6 cases). In 16 cases, a transcallosal approach was used, in 9 the approach was supracerebellar, and in 4, it was occipital trans-tentorial. Surgical mortality was 11% (1 caver- nous angioma operated on by the supracerebellar ap- proach and 2 germinomas with the transcallosal ap- proach). The cases treated surgically, after radiother- apy had failed, were 2 pineocytomas, 1 astrocytoma, 1 glioblastoma, 1 cavernous angioma and l glial cyst.
In the germinomas, the most frequent lesions in this series, surgery was the initial therapeutic strategy, ex- cepting shunting procedures, in 6 cases (31.5%), with a surgical mortality of 2 cases (33%).

28 J. Vaquero etai.: Neurosurgical Experience with Tumours of the Pineal Region at Clinica Puerta de Hierro
Radiotherapy
Thirty patients of the series received radiotherapy at on time or another. Because a radiosensitive turnout was suspected, a trial dose of 2,000 cGy was admin- istered to 22 patients, 15 of whom showed a sensitive response (13 supposed germinomas, 1 unverified em- bryonal carcinoma and 1 supposed malignant tera- toma). In these patients, radiotherapy was completed up to a total of 4,000 cGy holocranially, which was boosted to up to 5,000-5,500cGy over the tumoural region, with fractioned doses of 200 cGy/day, 5 days a week. Only 5 patients received prophylactic spinal ra- diotherapy (2 supposed germinomas, one of them AFP- secreting, 1 supposed embryonal carcinoma, and 2 pi- neoblastomas, one of whom developed arachnoid lum- bar seeding two years after spinal radiation). In all the cases, the dose covering the spine was 1,000-1,200 cGy.
Six of the seven patients that did not respond to trial radiotherapy underwent surgery. Their diagnosis, on the basis of pathological study, were pineocytoma in 2 cases and 1 case each of glioblastoma, cavernous angioma, glial cyst and astrocytoma.
Radiotherapy was used as the only treatment, ex- cepting shunting procedures, in 14 cases of the series (12 supposed germinomas, 1 unverified embryonal car- cinoma and 1 unverified glioblastoma), and as adjuvant to surgical resection in 11 verified tumours (4 germi- nomas, 3 pineoblastomas, 2 astrocytomas, 1 glioblas- toma and 1 malignant teratoma).
Chemotherapy
Only one subject in the series received chemotherapy with cisplatin, bleomycin and vinblastine, according to Einhorn's protocol 9. This case corresponds to the ma- lignant AFP-secreting teratoma mentioned above, but the exact diagnosis of which could be considered to be in doubt.
Patient Survival
Fifteen patients (30%) of the series died during fol- low-up. One subject, with a germinoma verified at nec- rospy, died of acute hydrocephalus prior to receiving any treatment. Another 2 with germinomas and 1 with cavernous angioma died of surgical complications, and the remaining 11 deaths were due to the patient's di- sease (2 metastatic tumours, 2 glioblastomas, 1 em- bryonal carcinoma, 2 malignant teratomas, 3 pineob- lastomas and 1 malignant astrocytoma).
In our series, except for the case in whom death was
due to acute hydrocephalus and the two patients who died after surgery, the remaining 16 germinoma pa- tients are presently alive and symptom-free, after fol- low-up ranging between 2 and 20 years (mean: 8 years). All were treated with radiotherapy, as the only treat- ment (12 cases), or as adjuvant treatment after surgery (4 cases).
The four pineocytomas of the present series, all sur- gically removed and without radiotherapy after sur- gery, are presently alive and symptom-free, after fol- low-up ranging between 3 and 7 years (mean: 4 years).
Although the criteria for choosing surgery as the initial therapeutic approach (elective surgery) or only once the ineffectiveness of radiotherapy had been dem- onstrated (selective surgery) were not established until the final years of the series, and after having gathered experience in the interpretation of clinical and CT-scan data, it is now possible to analyze retrospectively the consequences, in terms of survival, of having chosen one therapeutic alternative or another.
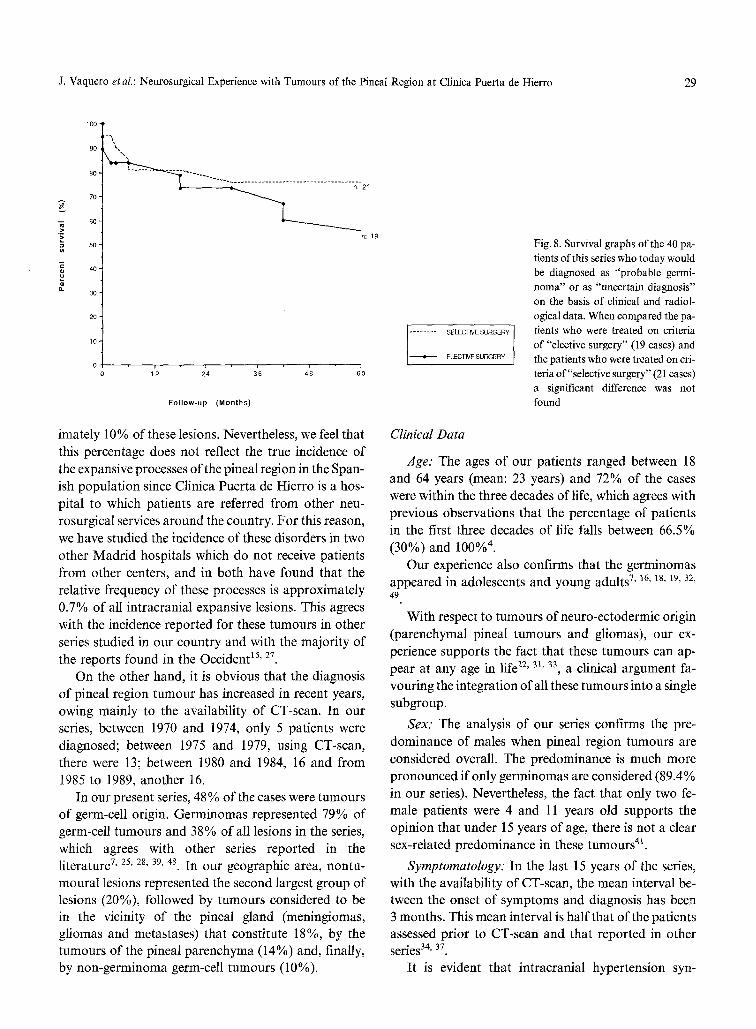
Thus, if we exclude the cases with obvious diagnosis (meningiomas, arachnoid cysts, arteriovenous malfor- mations, metastasis in patients with known carcinoma) in whom radiotherapy was not considered to be indi- cated as an initial option, as well as the patient who died of acute hydrocephalus immediately after admis- sion, and a supposed cavernous angioma where the patient refused treatment, the present series is reduced to 40 cases consisting of lesions which today would be interpreted as "probable germinomas" or of"uncertain diagnosis". Of these 40 cases, 19 were managed ac- cording to a criterion elective surgery, with a mortality of 10.5%, corresponding to 2 patients with germinoma (whose deaths may have been avoided if they had been treated according to the criterion of selective surgery), and 21 with criteria of selective surgery. In the group that underwent elective surgery, only 6 patients re- quired operation after confirmation of a lack of re- sponse to radiotherapy, with 17% mortality, corre- sponding to the cavernous angioma involving the brain stem mentioned above. A comparative analysis of sur- vival among the patients managed according to one criterion or another has not revealed significant dif- ferences (Fig. 8).
Discussion
Incidence
Over the last 20 years, some 5,000 cases of intra- cranial expansive processes have been studied in our hospital. Those of the pineal region represent approx-
J. Vaquero et al.: Neurosurgical Experience with Tumours of the Pineal Region at Clinica Puerta de Hierro 29
A
> -g
a} o.
100
90
80 '
7 0 -
6 0
5 0
4 0 -
3 0 -
20
1 0
0
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . n-'21 ---._..
n: 19
I I I I
12 2~4 36 48 60
Follow-up ( M o n t h s )
imately 10% of these lesions. Nevertheless, we feel that this percentage does not reflect the true incidence of the expansive processes of the pineal region in the Span- ish population since Clinica Puerta de Hierro is a hos- pital to which patients are referred from other neu- rosurgical services around the country. For this reason, we have studied the incidence of these disorders in two other Madrid hospitals which do not receive patients from other centers, and in both have found that the relative frequency of these processes is approximately 0.7% of all intracranial expansive lesions. This agrees with the incidence reported for these tumours in other series studied in our country and with the majority of the reports found in the Occident 15' 27
On the other hand, it is obvious that the diagnosis of pineal region tumour has increased in recent years, owing mainly to the availability of CT-scan. In our series, between 1970 and 1974, only 5 patients were diagnosed; between 1975 and 1979, using CT-scan, there were 13; between 1980 and 1984, 16 and from 1985 to 1989, another 16.
In our present series, 48 % of the cases were tumours of germ-cell origin. Germinomas represented 79% of germ-cell tumours and 38% of all lesions in the series, which agrees with other series reported in the literature 7, 25, 28, 39, 48. In our geographic area, nontu-
moural lesions represented the second largest group of lesions (20%), followed by tumours considered to be in the vicinity of the pineal gland (meningiomas, gliomas and metastases) that constitute 18~ by the tumours of the pineal parenchyma (14%) and, finally, by non-germinoma germ-cell tumours (10%).
I'-"i-'- SELECT/VE SURGERY
ELECTIVE SURGERY
Fig. 8. Survival graphs of the 40 pa- tients of this series who today would be diagnosed as "probable germi- noma" or as "uncertain diagnosis" on the basis of clinical and radiol- ogical data. When compared the pa- tients who were treated on criteria of "elective surgery" (19 cases) and the patients who were treated on cri- teria of"selective surgery" (21 cases) a significant difference was not found
Clinical Data
Age." The ages of our patients ranged between 18 and 64 years (mean: 23 years) and 72% of the cases were within the three decades of life, which agrees with previous observations that the percentage of patients in the first three decades of life falls between 66.5% (30%) and 100% 4 .
Our experience also confirms that the germinomas appeared in adolescents and young adults 7' ~6, ~8, 19, 32, 49
With respect to tumours of neuro-ectodermic origin (parenchymal pineal tumours and gliomas), our ex- perience supports the fact that these tumours can ap- pear at any age in life 22' 3~, 33, a clinical argument fa-
vouring the integration of all these tumours into a single subgroup.
Sex." The analysis of our series confirms the pre- dominance of males when pineal region tumours are considered overall. The predominance is much more pronounced if only germinomas are considered (89.4% in our series). Nevertheless, the fact that only two fe- male patients were 4 and 11 years old supports the opinion that under 15 years of age, there is not a clear sex-related predominance in these tumours 4~.
Symptomatology: In the last 15 years of the series, with the availability of CT-scan, the mean interval be- tween the onset of symptoms and diagnosis has been 3 months. This mean interval is half that of the patients assessed prior to CT-scan and that reported in other series34, 37
It is evident that intracranial hypertension syn-
30 J. Vaquero et aL: Neurosurgical Experience with Tumours of the Pineal Region at Clinica Puerta de Hierro
drome, related to hydrocephalus, predominates in our patients. In the present series, an ophthalmological syn- drome is frequent in germ-cell tumours, and a cerebellar syndrome in gliomas, possibly because of the infiltra- tion of the cerebellar peduncles. In our present expe- rience, although an endocrinological syndrome is rel- atively frequent in germ-cell neoplasms, its presence can not be considered a significant indication of the nature of a pineal region turnout.
Diagnostic Procedures and Management Criteria
In contrast to reports by other authors 8' 33, 43 CSF cytology has been of no diagnostic value in the man- agement of the tumours dealt with in this series.
Concerning the value of tumoural markers, our con- cept of their specificity has evolved in recent years. At the beginning of this study, we thought that the pos- itivity of AFP and HCG would rule out germinoma and point to a diagnosis of malignant germ-cell tumour, with tissue of endodermal sinus tumour or choriocar- cinoma, respectively 2' 18, 24, 35, 36, 50. Nevertheless, the observations of typical germinomas with AFP and HCG secretion 3' 12, 17, 20, 24, 26, 52 and our experience
with two unverified tumours with radiological data, response to radiotherapy and follow-up characteristics of typical germinomas, suggest that tumoural markers doubtfully can be considered specific for the establish- ment of the exact histological nature or the biological prognosis of a germ-cell tumour.
Although stereotactic biopsy has been advocated as useful in the management of pineal region tumours 22, this procedure has not been employed in the present series. Disadvantages and risks related to stereotactic biopsy of pineal masses include: the difficulty of ob- taining enough tissue in order to get an accurate his- tological diagnosis, considering that in germinal tu- rnouts there appear frequently areas with different de- grees of malignancy and variable histology; danger of injury to the surrounding venous structures; and even- tually the possibility of a tumoural seeding after the procedure 4. Nevertheless, the actual image-directed techniques permit the accurate stereotactic biopsy of pineal tumours in a safer way. For this reason, we now consider this procedure as one of the possible diagnostic techniques for to establish a therapeutic decision.
We agree with Jooma and Kendall 18 that nowadays CT-scan is very reliable in the initial assessment of a patient with a tumour of the pineal region, and when the pattern of a well-defined lesion, moderately hy- perdense, with homogenous enhancement after con-
trast administration 1~ 11, 14, 51, 53, is added to the clinical data, negativity in the tumoural markers, etc., and the patient is a young male, a diagnosis of "probable ger- minoma" can be established and the subject should be selected for trial radiotherapy.
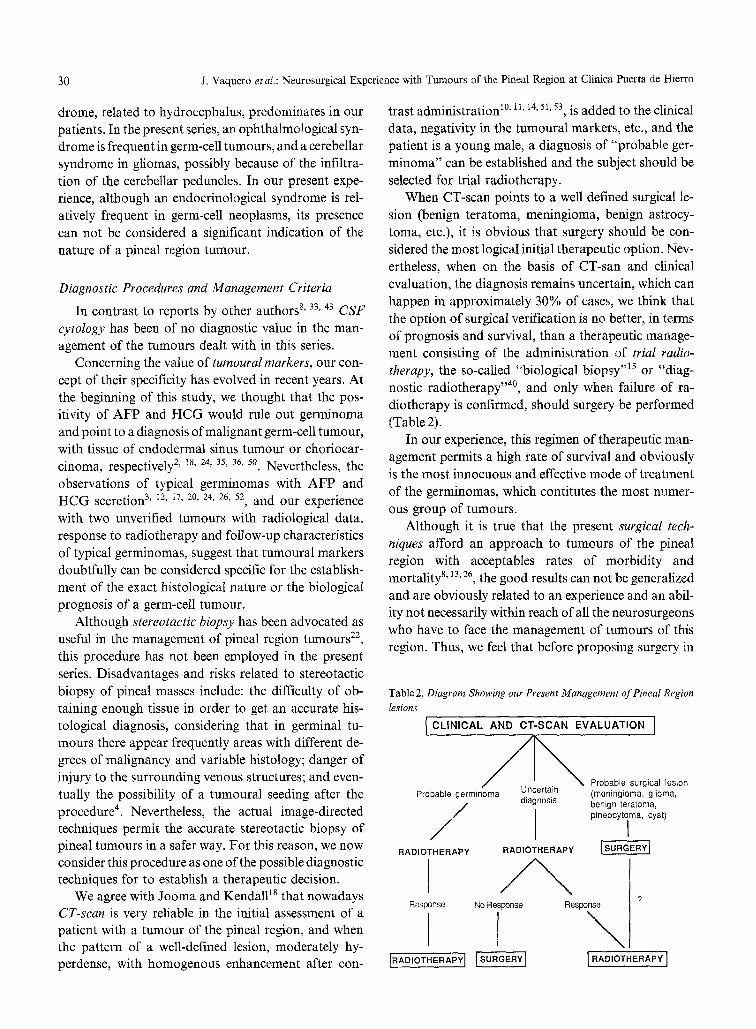
When CT-scan points to a well defined surgical le- sion (benign teratoma, meningioma, benign astrocy- toma, etc.), it is obvious that surgery should be con- sidered the most logical initial therapeutic option. Nev- ertheless, when on the basis of CT-san and clinical evaluation, the diagnosis remains uncertain, which can happen in approximately 30% of cases, we think that the option of surgical verification is no better, in terms of prognosis and survival, than a therapeutic manage- ment consisting of the administration of trial radio- therapy, the so-called "biological biopsy ''15 or "diag- nostic radiotherapy ''4~ and only when failure of ra- diotherapy is confirmed, should surgery be performed (Table 2).
In our experience, this regimen of therapeutic man- agement permits a high rate of survival and obviously is the most innocuous and effective mode of treatment of the germinomas, which contitutes the most numer- ous group of tumours.
Although it is true that the present surgical tech- niques afford an approach to tumours of the pineal region with acceptables rates of morbidity and mortalityS, 13, 26, the good results can not be generalized and are obviously related to an experience and an abil- ity not necessarily within reach of all the neurosurgeons who have to face the management of tumours of this region. Thus, we feel that before proposing surgery in
Table 2. Diagram Showing our Present Management of Pineal Region lesions
I CLINICAL AND CT-SCAN EVALUATION 1
Probable germinoma Uncertain diagnosis
RADIOTHERAPY RADIOTHERAPY
Response No Response
F IRAD,OTHERA
Probable surgical lesion (rneningiema, glioma, benign teratoma, pineocytoma, cyst)
I
? Response
\ [RAD,O HER PY i

J. Vaquero et al.: Neurosurgical Experience with Tumours of the Pineal Region at Clinica Puerta de Hierro 31
these lesions, it may be useful to remember a phrase
expressed by Davidoff6: " . . . I t is better to have a living patient, restored to good health, whose diagnosis lacks the stamp of certainty the microscope provides, than it is to have beautiful microphotographs from postmortem specimens".
It is obvious that with the therapeutic regimen that we propose there could be diagnostic errors, since some
tumours , such as pineoblastomas, which initially re- spond well to radiotherapy, can be misdiagnosed as
germinomas, as also can occur with some non-germi-
noma germ-cell tumours showing partial response to
radiotherapy. Nevertheless, we consider that these di- agnostic errors do not lead to significant therapeutic
errors since histological verification in these cases does not substantially modify the indication for radiother-
apy, the results o f which do not appear to be clearly enhanced by previous surgical resection 29.
Fur thermore , the a rgument that surgery o f pineal region tumours is hindered by pr ior radiotherapy 2I' 23, 38 does no t agree with our own experience nor with
that o f other authors. This measure has even come to
be recommended prior to surgery to reduce the tu- moura l vascularization and facilitate surgical resection 1, 43
With respect to CT-scan evaluation and manage-
ment o f pineocytomas, their cystic nature and calcifi- cations appear to be data to be taken into account in our cases; all o f them show signs o f neuronal differ-
entiation in the pathological study. The supposed be-
nign behaviour o f p ineocytomas with neuronal differentiation 31 correlates with our experience, and
suggests that postoperat ive radio therapy is not indi- cated in these tumours 47.
Our study shows that, in selected cases o f pineal region tumours , radiotherapy alone can achieve a high
rate o f cures, and support the opinion that surgical resection in mal ignant tumours does not enhance the benefits obtained with irradiation 5' 16. In our series, all
patients with supposed germinomas subjected to ra- d io therapy are alive and symptom-free, with a follow- up that ranged between 2 and 20 years (mean: 8 years).
On the other hand, we consider that prophylact ic spinal irradiation is not necessary in radiosensitive tu- mours o f the pineal region, in agreement with the opin- ion o f other authors 5 and with reported data that in unopera ted patients with pineal germ-cell tumour , spinal seeding is relatively u n c o m m o n 32. In our series,
only 5 patients received radio therapy of the spine, and one o f these subjects was the only case (a pineoblas- toma) that developed spinal seeding two years later.
References
1. Abay II EO, Laws ER, Grado GL, Bruckman JE, Forbes GS, Grmez MR, Scott M (1981) Pineal tumours in children and adolescents. J Neurosurg 55:889-895
2. Allen JS, Nisselbaum J, Epstein F, Rosen G, Schwartz MK (1979) Alphafetoprotein and human chorionic gonadotropin de- termination in cerebrospinal fluid. An aid to the diagnosis and management of intracranial germ cell tumours. J Neurosurg 51: 368-374
3. Arita N, Bitoh S, Ushio Y, Hayakawa T, Hasegawa H, Fujiwara M, Ozaki K, Parkhen L, Mori T (1980) Primary endodermal sinus tumour with elevated serum and CSF alphafetoprotein levels. J Neurosurg 53:244-248
4. Chang CG, Kageyama N, Kobayashi T, Yoshida J, Negoro M (1981) Pineal tumours: clinical diagnosis, with special emphasis on the significance of pineal calcification. Neurosurgery 8: 656- 667
5. Danoff B, Sheline GE (1984) Radiotherapy of pineal tumours. In: Neuwelt EA (ed) Diagnosis and treatment of pineal region turnouts. Williams and Wilkins, Baltimore
6. DavidoffLM (1967) Some considerations in the therapy ofpineal tumours. Rudolf Virchow lecture. Bull N Y Acad Med 43: 537- 561
7. De Girolami U, Schmidek H (1973) Clinicopathological study of 53 tumours of the pineal region. J Neurosurg 39:455-462
8. Edwards MSB, Hudgins RJ, Wilson CHB, Levin VA, Wara WM (1988) Pineal region tumours in children. J Neurosurg 68: 689-697
9. Einhorn LH, Donohue JP (1977) Cis-diamine dichloroplatinum, vinblastine and Neomycin combination chemotherapy in dis- seminated testicular cancer. Ann Intern Med 87:293-298
10. Futrell NN, Osborn AG, Cheson BD (1981) Pineal region tu- mours:'computed tomographic-pathologic spectrum. AJR 137: 951-956
11. Ganti SR, Hilal SK, Stein BM, Silver AJ, Mawad M, Sane P (1986) CT of pineal region tumours. AJR 146:451-458
12. Handa H, Yamashita J (1981) Current treatment of pineal tu- mours. Neurol Med Chir (Tokio) 21:147-154
13. Hoffman HJ (1984) Transcallosal approach to pineal tumours and the Hospital for sick children series of pineal region tumours. In: Neuwelt EA (ed) Diagnosis and treatment of pineal region tumours. Williams and Wilkins, Baltimore
14. Inoue Y, Takeuchi T, Tamaki M, Nin K, Hakuba A, Nishimura S (1979) Sequential CT observations of irradiated intracranial germinomas. AJR 132:361-365
15. Isamat F (1979) Tumours of the posterior part of the third ventricle: Neurosurgical criteria.: In: Advances and technical standards in neurosurgery, Vol 6. Springer, Wien New York
16. Jenkin RDT, Simpson WJK, Keen CW (1978) Pineal and su- prasellar germinomas. J Neurosurg 48:99-107
17. Jennings MT, Gelman R, Hochberg F (1984) Intracranial germ- cell tumours: natural history and pathogenesis. In: Neuwelt EA (ed) Diagnosis and treatment of pineal region tumours. Williams and Willdns, Baltimore
18. Jooma R, Kendall BE (1983) Diagnosis and management of pineal tumours. J Neurosurg 58:654-665
19. Koide O, Watanabe Y, Sato (1980) A pathologic survey of intracranial germinoma and pinealoma in Japan. Cancer 5: 2119-2130
32 J. Vaquero el al.: Neurosurgical Experience with Tumours of the Pineal Region at Clinica Puerta de Hierro
20. Kubo O, Yamashi N, Kamijo Y, Amano K, Kitamura K, De~ mura R (1977) Human chorionic gonadotropin produced by ectopic pinealoma in a girl with precocious puberty. J Neurosurg 7:101-105
21. Lapras C (1984) Surgical therapy of pineal region tumours. In: Neuwelt EA (ed) Diagnosis and treatment of pineal region tu- mours. Williams and Wilkins, Baltimore
22. Moser RP, Backlund EO (1984) Stereotactic techniques in the diagnosis and treatment of pineal region tumours. In: Neuwelt EA (ed) Williams and Wilkins, Baltimore
23. Neuwelt EA, Batjer HH (1984) Pre and postoperative manage- ment of pineal region turnouts and the occipital transtentorial approach. In: Neuwelt EA (ed) Diagnosis and treatment of the pineal region tumours. Williams and Wilkins, Baltimore
24. Neuwelt EA, Frenkel EP (1984) Germinoma and other pineal tumours: chemotherapeutic responses. In: Neuwelt EA (ed) Di- agnosis and treatment of pineal region turnouts. Williams and Wilkins, Baltimore
25. Neuwelt EA, Glasberg M, Frenkel E, Clark WK (1979) Malig- nant pineal region tumours. J Neurosurg 51:597-607
26. Neuwelt EA (ed) (1984) Diagnosis and treatment of pineal region tumours. Williams and Wilkins, Baltimore
27. Obrador S, Soto M, Gutierrez-Diaz JA (1976) Surgical man- agement of tumours of the pineal region. Acta Neurochir (Wien) 34:159-171
28. Onoyama Y, Ono K, Nakajima T, Hiraoka M, Abe M (1979) Radiation therapy of pineal tumours. Radiology 130:757-760
29. Pluchino F, Broggi G, Fornari M, Franzini A, Solero CL, A1- legranza A (1989) Surgical approach to pineal turnouts. Acta Neurochir (Wien) 96:26-31
30. Poppen JL, Marino R (1968) Pinealomas and tumours of the posterior portion of the third ventricle. J Neurosurg 28: 357- 364
31. Rubinstein JL (1982) Tumours of the central nervous system (Suppl). Atlas of tumour pathology. Armed Forces Institute of Pathology, Washington DC, pp 15-20
32. Sano K, Matsutani M (1981) Pinealoma (germinoma) treated by direct surgery and postoperative irradiation. A long-term follow-up. Child's Brain 8:81-97
33. Sano K (1976) Diagnosis and treatment of tumours in the pineal region. Acta Neurochir (Wien) 34:153-157
34. Schmidek HH (1977) Pineal tumours. Masson, New York 35. Shinoda J, Miwa Y, Sakai N, Yamada H, Shima H, Kato K,
Takahashi M, Shimokawa K (1985) Immunohistochemical study of placental alkaline phosphatase in primary intracranial germ-cell tumours. J Neurosurg 63:733-739
36. Shinomiya Y, Toya S, Iwata T, Hosada Y (1979) Radioim- munoassay of alpha-fetoprotein in children with primary intra- cranial tumour. Childs Brain 5:450-458
37. Smith NJ, El-Mahdi AM, Constable WC (1976) Results of ir- radiation of tumours in the region of the pineal body. Acta Radiol Ther Phys Biol 25:17-22
38. Stein BM (1984) Surgical therapy of benign pineal tumours. In: Neuwelt EA (ed) Diagnosis and treatment of pineal region tu- mours. Williams and Wilkins, Baltimore
39. Sung DI, Harisiadis L, Chang CH (1978) Midline pineal tumours and suprasellar germinomas: highly curable by irradiation. Ra- diology 128:745-751
40. Takakura K(1984)Intracranial germ celltumours. Clinical neu- rosurgery. Proceedings of the Congress of Neurological Sur- geons, New York N Y. Williams and Wilkins, Baltimore
41. Takakura K (1984) Nonsurgical pineal tumour therapy. The japanese experience. In: Neuwelt EA (ed) Diagnosis and treat- ment of pineal region tumours. Williams and Wilkins, Baltimore
42. Teilum G (1965) Classification of endodermal sinus tumour (me- soblastoma vitellinum) and so-called embryonal carcinoma of the ovary. APMIS 64:407-429
43. Ueki T, Tanaka R (1980) Treatment of prognoses of pineal tumours. Experience of 1 I0 cases. Neurol Med Chir (Tokyo)20: 1-26
44. Vaquero J, Carrillo R, Cabezudo J, Leunda G, Villoria F, Bravo G (1980) Cavernous angiomas of the pineal region. Report of two cases. J Neurosurg 53:833-835
45. Vaquero J, Carrillo R, Cabezudo JM, Nombela L, Bravo G (1981) Arachnoid cysts of the posterior fossa. Surg Neurol 16: 117-121
46. Vaquero J, Martinez R, Escand6n J, Bravo G (1988) Sympto- matic glial cysts of the pineal gland. Surg Neurol 30:468-470
47. Vaquero J, Ramiro J, Martinez R, Coca S, Bravo G (1990) Clinicopathological experience with pineocytomas: report of five surgically treated cases. Neurosurgery. 27:612-619
48. Ventureyra ECG (1981) Pineal region. Surgical management of tumours and vascular malformations. Surg Neurol 16:77-84
49. Waga S, Handa H, Yamashita J (1979) Intracranial germinomas: treatment and results. Surg Neurol 11: 167-172
50. Wilson ER, Takei K, Bikoff WT, O'Briens MS, Tindall GT, Boehm WM (1979) Abdominal metastase of primary intraeran- ial yolk sac tumours through ventriculoperitoneal shunts: report of three cases. Neurosurgery 5:356-364
51. Wood JH, Zimmerman RA, Bruce DA, Bilaniuk LT, Norris DG, Schut L (1981) Assessment and management of pineal- region and related turnouts. Surg Neurol 16:192-210
52. Yamagami T, Handa H, Yamashita J, Okumura T, Paine J, Hachara H, Furukawa F (1987) An immunohistochemical study of intracranial germ cell tumours. Acta Neurochir (Wien) 86: 33-41
53. Zimmerman RA, Bilaniuk LT, Wood JH, Bruce DA, Schut L (1980) Computed tomography of pineal, parapineal and his- tologically related tumours. Radiology 137:669-677
Correspondence and Reprints: Dr. Jesfls Vaquero Crespo, Ser- vicio de Neurocirugia, Clinica Puerto de Hierro, San Martin de Porres, 4, 28035-Madrid, Spain.





























