Embed Size (px)
Citation preview

http://imr.sagepub.com/Research
Journal of International Medical
http://imr.sagepub.com/content/39/6/2360The online version of this article can be found at:
DOI: 10.1177/147323001103900636
2011 39: 2360Journal of International Medical ResearchD Yildirim, B Gurses, B Gurpinar, B Ekci, B Colakoglu and A Kaur
SonoelastographyNodule or Pseudonodule? Differentiation in Hashimoto's Thyroiditis with
Published by:
http://www.sagepublications.com
can be found at:Journal of International Medical ResearchAdditional services and information for
http://imr.sagepub.com/cgi/alertsEmail Alerts:
http://imr.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Dec 1, 2011Version of Record >>
by guest on October 11, 2013imr.sagepub.comDownloaded from by guest on October 11, 2013imr.sagepub.comDownloaded from by guest on October 11, 2013imr.sagepub.comDownloaded from by guest on October 11, 2013imr.sagepub.comDownloaded from by guest on October 11, 2013imr.sagepub.comDownloaded from by guest on October 11, 2013imr.sagepub.comDownloaded from by guest on October 11, 2013imr.sagepub.comDownloaded from by guest on October 11, 2013imr.sagepub.comDownloaded from by guest on October 11, 2013imr.sagepub.comDownloaded from by guest on October 11, 2013imr.sagepub.comDownloaded from by guest on October 11, 2013imr.sagepub.comDownloaded from
The Journal of International Medical Research2011; 39: 2360 – 2369
2360
Nodule or Pseudonodule? Differentiationin Hashimoto’s Thyroiditis with
Sonoelastography
D YILDIRIM1, B GURSES2, B GURPINAR3, B EKCI4, B COLAKOGLU5 AND A KAUR6
¹Department of Radiology, and ³Department of Head and Neck Surgery, Kasimpasa MilitaryHospital, Beyoglu, Istanbul, Turkey; ²Department of Radiology, and 4Department of Surgery,Yeditepe University Hospital, Kozyatagi, Istanbul, Turkey; 5Department of Radiology, VKVAmerican Hospital, Nisantasi, Istanbul, Turkey; 6E-Sitopatoloji Laboratories, Nisantasi,
Istanbul, Turkey
Fine needle aspiration biopsy (FNAB) is thegold standard for the diagnosis oflymphoma in Hashimoto’s thyroiditis and isable to differentiate between benign,inflammatory or malignant nodules,classifying them as either true nodules orpseudonodules. This technique is, however,invasive. The present study aimed todifferentiate pseudonodules from truenodules by sonoelastography, a non-invasive technique, in 54 patients withHashimoto’s thyroiditis. The accuracy ofsonoelastography to differentiate betweentrue or pseudonodules was compared withthe gold standard FNAB and with grey scale
ultrasonography. The nodules werecategorized into three groups: non-demarcated hypoechogenic, demarcatedhyperecho genic, and demarcatedhypoechogenic. Sono elastography findingswere concordant with the cytopathologicalresults and demonstrated that sono -elastography was able to detect true thyroidnodules often misdiagnosed byconventional grey scale ultrasonography.Sonoelastography was found to haveincreased sensitivity for true nodulediagnosis compared with conventional greyscale ultrasonography and may eliminateunnecessary FNABs being carried out.
KEY WORDS: HASHIMOTO’S THYROIDITIS; THYROID NODULE; SONOELASTOGRAPHY; FINE NEEDLEASPIRATION BIOPSY
IntroductionHashimoto’s thyroiditis, also known aschronic lymphocytic thyroiditis, is anautoimmune disease mediated byautoantibodies that target thyroidperoxidase and/or thyroglobulin, and causethe gradual destruction of follicles in thethyroid gland. Hashimoto’s thyroiditis is oneof the most common causes ofhypothyroidism; it is up to 15 times more
common among women than men andaffects at least 2% of all women, with peakincidence between the ages of 30 and 50years, and may coexist with otherautoimmune disorders.1 – 4 Hashimoto’sthyroiditis is characterized by the presence ofT-lymphocytes and other leucocytes inthyroid tissue and can be associated withnon-Hodgkin’s lymphoma.1,2
Involvement of the thyroid gland in

2361
D Yildirim, B Gurses, B Gurpinar et al.Sonoelastography for nodule differentiation in Hashimoto’s thyroiditis
Hashimoto’s thyroiditis may beasymmetrical and means that surgicalconsultation is usually required.1 – 5
Diagnosis of lymphoma in Hashimoto’sthyroiditis, besides other primaryparenchymal neoplasms, depends onnodule differentiation in the thyroidgland.2,5 Fine needle aspiration biopsy(FNAB) can be used to differentiate betweenbenign, inflammatory or malignantnodules and classify them as either truenodules or pseudonodules.6 In nodulargoitre, cytology reveals abundant waterycolloid, small follicular cells with darknuclei that are arranged in monolayersheets, groups with follicle formation orsingle cells. On the other hand, FNABspecimens from patients with thyroiditiswho present with distinct nodules usuallyshow scant colloid, Hürthle cells, follicularcells, lymphocytes and few plasma cells.Lymphocytes are usually seen in thebackground, percolating between cellgroups and, in some cases, an intactlymphoid follicle may be seen.7 Despite itsaccuracy for diagnosis, FNAB is categorizedas a minimally invasive intervention.8 Incontrast, sonoelastography is a non-invasive method that differentiates betweentrue nodules and pseudonodules bydetermining the mechanical stiffness oftissue. The principle of sonoelastography isbased on tissue compression, whichproduces displacement (strain) within thetissue being analysed. Measurements showthat tissue strain is less in harder tissuecompared with soft tissue. By measuring thetissue strain induced by compression, it ispossible to estimate tissue hardness, whichmay be useful in diagnosing the degree oftissue cellularity.9 Depending on thecellularity or composition of the nodule,different levels of stiffness may be observedin thyroid lesions. The information gained
from sonoelastograms enables the relativestiffness of the lesion to be compared withthat of surrounding tissues and also withinthe thyroid itself.10 – 13 The strain images orelastograms can be displayed as a colourmap using new generation ultrasonography(US) systems.13 – 17
The present study analysed thedifferentiation status of nodules frompatients with Hashimoto’s thyroiditis bysonoelastography, as a way to diagnoselymphoma without unnecessary surgicalinterventions or invasive approaches.
Patients and methodsSTUDY POPULATIONThis multicentre, prospective, single-blindstudy was conducted at Kasimpasa MilitaryHospital, Yeditepe University Hospital andVKV American Hospital, Istanbul, Turkeyand recruited consecutive patients diagnosedwith Hashimoto’s thyroiditis between May2009 and May 2010. Inclusion criteria were:parenchymal echoheterogenity; elevatedblood levels of antithyroid antibodies(antithyroid peroxidase antibody andantithyroglobulin antibody); the presence ofnodular lesions where two observers agreedon the demarcation and echogenity asmeasured by US; a body mass index of 18 –30 kg/m2; and anteroposterior diameter ofthe thyroid gland of 8 – 30 mm where thelargest nodule had a diameter of between 8and 20 mm. All patients received a detailedclinical examination, including thyroidfunction tests, and thyroid autoantibodytitres were measured.The study protocol was approved by the
Institutional Review Board of YeditepeUniversity School of Medicine ClinicalResearch Evaluation Committee, Istanbul,Turkey. Verbal informed consent wasobtained from all patients included in thestudy.

2362
D Yildirim, B Gurses, B Gurpinar et al.Sonoelastography for nodule differentiation in Hashimoto’s thyroiditis
RADIOLOGICAL EVALUATIONGrey scale and Doppler US analyses of thethyroid gland and sonoelastographicevaluations were performed by differentradiologists (D.Y., B.C.) using the sameequipment (Acuson S2000™; Siemens,Erlangen, Germany). The patients weredivided into three groups according to theirgrey scale US results: group I consisted ofpatients with non-demarcatedhypoechogenic focal areas; group IIcomprised patients with demarcatedhyperechogenic focal areas; and group IIIwere those patients with demarcatedhypoechogenic nodular lesions. Of thesenodules, the most dominant lesion wasreferred to as ‘the focused lesion’. If thedominant lesion was purely demarcated orvascularized differently (less or more thannative parenchyma) according to US, it wasreferred to as a true nodule. If the nodule wasnot demarcated it was evaluated as apseudonodule. The dominant lesions werefurther studied by sonoelastography by adifferent radiologist (B.G.) who was blindedto the former US results. If the elasticity of thenodule was greater or lesser than the basalparenchymal elasticity and occupied ≥ 50%of the surface area of the nodule itself it wascategorized as a true nodule. If the nodulewas isoelastic it was categorized as apseudonodule. A 12 MHz linear transducerwas used in the sonoelastographicexamination. The transducer was pressedperpendicularly against the tissue andspecific receptors in the US system quantifiedthe compression and directed the examinerto standardize the amount of compression.This standardization is referred to as the‘quality factor’ and the manufacturer of theAcuson S2000™ system advises a value of 60– 80. Nodules that were classified as focusedlesions by US were then further analysed byFNAB (Fig. 1).
PATHOLOGICAL EVALUATIONAll specimens were stained with May–Grünwald–Giemsa solution and evaluatedby the same pathologist (A.K.), who wasblinded to the US and sonoelastographyresults. Results were recorded as either truenodules or pseudonodules of the thyroidgland. Adequacy of the specimens analysedwas evaluated according to the followingcriteria18: (i) specimens were adequate if atleast five groups of 10 cell clusters werepresent, whereas values less than that weretermed hypocellular; (ii) specimens with nocells present were termed acellular; (iii)specimens with many more cells thanconsidered as ‘adequate’ in (i) were termedhypercellular. Besides cellularity, neoplastic criteria were
also evaluated and taken into consideration.The cytological features of follicularneoplasms were hypercellularity withprominent nuclear overlapping andcrowding, whereas the cytological features ofpapillary thyroid carcinoma were anenlarged oval and irregular nucleus,eccentric and often multiple micronucleoli,fine pale chromatin, longitudinalintranuclear grooves and intranuclearpseudo-inclusions.10
STATISTICAL ANALYSESAll statistical analyses were performed usingSPSS® statistical software, version 15.0.1(SPSS Inc., Chicago, IL, USA) for Windows®.Continuous data are shown as mean ± SD.The χ2-test was used to compare non-parametric data (gender, age, gland andnodular vascularity) and one-way analysisof variance was used to determinestatistically significant variances ofparametric data (body mass index and theanteroposterior diameter of the lobe bearingthe nodule). The Kruskal–Wallis test wasperformed to compare dimensions of

2363
D Yildirim, B Gurses, B Gurpinar et al.Sonoelastography for nodule differentiation in Hashimoto’s thyroiditis
the nodules between patients. A value of P < 0.05 was considered to be statisticallysignificant.All data were interpreted and the
sensitivity, specificity, positive predictivevalue, negative predictive value andaccuracy value for each group werecalculated. Receiver operating characteristic(ROC) curves were prepared according to thespecificity and sensitivity values.Concordance between the two examiners
was checked by the SPSS program with theaid of the dataset in a cross-table format,and success rates and κ analyses for each USand sonoelastography reading were alsodetermined with this program. Correlationsbetween grey scale US imagery,sonoelastography and FNAB results weretested with the McNemar test.
ResultsA total of 168 patients were enrolled in the
FIGURE 1: (A) Grey scale ultrasonography and (B) a real-time sonoelastographycolour map image of tissue displacement (strain), showing a hypoechogenicpseudonodule at the posterior pole of the thyroid gland from a 33-year-old woman;the area of tissue strain (circled in B) is coloured the same as the basal gland (arrowsin A). (C) Grey scale ultrasonography during fine needle aspiration biopsy showingthe needle tip (arrow) in the region of the nodule. (D) Cytopathological examinationshowing lymphoid cells in various maturation levels, supporting the diagnosis ofHashimoto’s thyroiditis (May–Grünwald–Giemsa stain, × 400 original magnification)
A B
C D

2364
D Yildirim, B Gurses, B Gurpinar et al.Sonoelastography for nodule differentiation in Hashimoto’s thyroiditis
study and, of these, 54 (50 females, fourmales; mean ± SD age 41.9 ± 8.0 years) metthe inclusion criteria and were evaluatedfurther by biopsy and cytologicalexamination and included in the analyses.There were 33 patients in group I (non-demarcated hypoechogenic focal areas), 12in group II (demarcated hyperechogenicfocal areas); and nine in group III(demarcated hypoechogenic nodularlesions). Demographic and clinicalcharacteristics are shown in Table 1. Sonoelastography and US analyses
demonstrated different true nodule andpseudonodule numbers compared with theFNAB analysis (Table 2). In group I (non-demarcated hypoechogenic), US imagingshowed that all 33 cases had pseudonodulespresent, but no true nodules, although atleast one non-demarcated but suspiciousnodule was observed. In contrast, FNAB
analysis identified two cases as true nodulesand 31 cases as pseudonodules, which wereprobably due to thyroiditis.Sonoelastography identified one case with ademarcated strain as being a true nodule,whereas analysis of the other 32 cases gaveisoelastic measurements suggesting that theywere pseudonodules.Analysis by FNAB of the 12 cases in group
II (demarcated hyperechogenic) revealednine cases as true nodules (benign colloidalnodules) and three cases as pseudonodules(Table 2). Sonoelastography agreed with this,as determined by ‘aliasing’ on thesonoelastography images (‘aliasing’ is aterm used to describe the colour scatteringseen on the monitor caused by tissuemovement, compression or vibration:pseudonodules have similar colour andfeatures to the background, whereas truenodules have different colour and features
TABLE 1:Demographic and clinical data, according to nodule categorization, for the 54 patientswith Hashimoto’s thyroiditis who were included in this study
Non-demarcated Demarcated DemarcatedDemographic/clinical hypoechogenic hyperechogenic hypoechogenic Statisticalparameter (group I) (group II) (group III) significance
Total No. of patients 33 12 9 P = 0.001a
Females/males 31/2 11/1 8/1 NSa
Age, years 41.12 ± 6.78 42.33 ± 9.74 44.22 ± 10.09 NSb
Body mass index, kg/m2 23.85 ± 3.69 24.17 ± 3.04 23.17 ± 4.34 NSb
LocalizationRight 18 5 4 NSa
Left 12 6 4Isthmus 3 1 1
VascularizationIncreased 28 11 9 PV NSa
Normal 4 1 0 NV NSa
Decreased 1 0 0Largest nodule size, mm 11.64 ± 2.93 11.52 ± 2.66 11.49 ± 2.63 NSc
Anteroposterior diameter of 17.24 ± 4.71 16.70 ± 5.45 19.49 ± 4.96 NSb
related thyroid lobe, mm
Data presented as mean ± SD or n of patients.aχ2-test; bone-way analysis of variance; cKruskal–Wallis test.NS, not statistically significant (P > 0.05); PV, parenchymal vascularization; NV, nodule vascularization.

2365
D Yildirim, B Gurses, B Gurpinar et al.Sonoelastography for nodule differentiation in Hashimoto’s thyroiditis
compared with the background). Grey scaleUS imaging identified 12 cases of truenodules and none with pseudonodules.Three pseudonodules were demarcated ongrey scale US imaging but sonoelastographicassessment revealed identical colour‘aliasing’, which indicated isoelasticity of thenodular area in concordance withbackground parenchyma also affected byHashimoto’s thyroiditis.The nine cases in group III (demarcated
hypoechogenic) showed three cases as truenodules (benign colloidal nodules) and six aspseudonodules on FNAB analysis, whereas USimaging showed all nine cases as containingtrue nodules. Sonoelastography identified fivetrue nodules: three were concordant with thecytopathological results and were demarcatedin the strain images, whereas the other twowere falsely identified as true nodules (Table2). Four other cases in group III were correctlyidentified as pseudonodules onsonoelastography. No malignancy wasreported in the FNAB reports.For the differentiation of pseudonodules
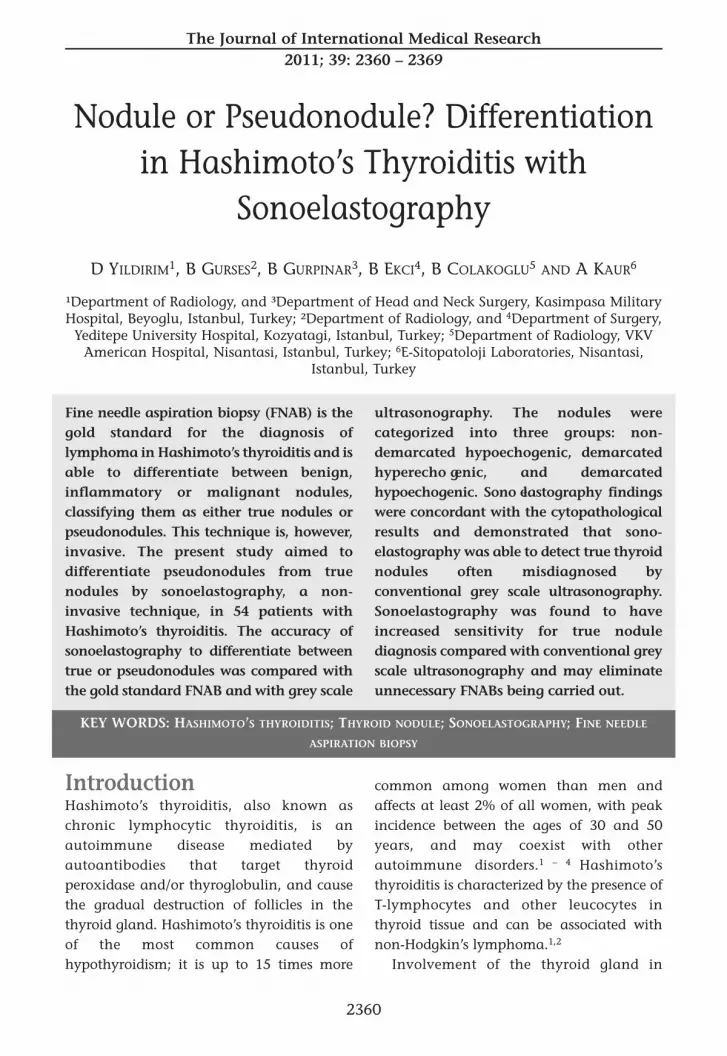
from true nodules, grey scale US analysis hada sensitivity of 85.7%, specificity of 77.5%,positive predictive value of 57.1%, negativepredictive value of 93.9% and accuracy of79.6%. Equivalent values for sono -elastography were sensitivity 92.9%,specificity 95.0%, positive predictive value86.7%, negative predictive value 97.4% andaccuracy 94.4%. The areas under the ROCcurves (success rates) were 0.816 for US and0.939 for sonoelastography (P = 0.0001; Fig.2). Comparison between US and FNAB gavea correlation of 54.4% between the twomethods, whereas sonoelastography versusFNAB demonstrated a correlation of 85.9%(κ analysis); both the US imaging andsonoelastography results significantlycorrelated with the results obtained by FNAB(P = 0.0001 for both, McNemar test).
TABLE 2:
Comparison of the ab
ility of fine needle aspiration biopsy (FN
AB), grey scale ultrasonography (U
S) and sonoelastography to
differentiate between pseud
onodules and true nodules in
Hashim
oto’s thyroiditis according to nodule categorization
FNAB
Grey scale US
Sonoelastography
(gold standard)
(conventional m
ethod)
(new
method)
Group
Pseu
donodules
True
nodules
Pseu
donodules
True
nodules
Pseu
donodules
True
nodules
Non-demarcated hypoechogenic
31 (94)
2 (6)
33 (100)
032 (97)
1 (3)
(group I; n= 33)
Demarcated hyperechogenic (group II;
3 (25)
9 (75)
012 (100)
3 (25)
9 (75)
n= 12)
Demarcated hypoechogenic (group III;
6 (67)
3 (33)
09 (100)
4 (44)
5 (56)
n= 9)
Data presented as
n(%) of patients.
2366
D Yildirim, B Gurses, B Gurpinar et al.Sonoelastography for nodule differentiation in Hashimoto’s thyroiditis
DiscussionHashimoto’s thyroiditis involves both theinflammatory process and noduledevelopment within the gland itself, and USis one of the most commonly used diagnostictools.19 Besides the presence of true thyroidnodules (adenomatous, hyperplastic orcolloidal nodules), basal inflammatorychanges such as fibrotic bands andpseudonodule development may also beseen.5 No criteria have been established,however, to diagnose and differentiate thetwo distinct groups of nodules by US.20 – 23
Thus, in cases where there are suspicions ofthe presence of real nodules, eitherconservative monitoring or biopsy/surgerymight be needed for diagnosis, but bothchoices have financial and timeimplications.23 – 25
Hashimoto’s thyroiditis and related nodularlesions have been widely studied.23 – 29 Theseprevious studies have focused on nodules > 1cm in size and achieved a low level of
accuracy (≤ 75%) for the differentiation ofmalignant and benign nodules. For nodules≤ 1 cm, sensitivity in the differentiation ofmalignant nodules was shown to decrease toas low as 37%.25 During evaluation ofmultiple nodular features (dimension,vascularity, contour-halo regularity,localization), sensitivity and accuracy mayincrease to 78%.24,25 These studies offer littleinformation about the differentiation statusof the nodules themselves. Often it is onlyreported that echogenic thyroid nodules arecommonly benign, or that hypoechogenicnodules must be closely observed.10 Theoccurrence of pseudonodular hypoecho -genicity in Hashimoto’s thyroiditis, however,has been reported as nearly 50%, due tobasal parenchymal echogenic changes andfibrotic bands.10
The present study focused specifically ondifferentiating between true nodules andpseudonodules in Hashimoto’s thyroiditispatients, comparing sonoelastography with
FIGURE 2: Receiver operating characteristic curves for (A) conventional grey scaleultrasonography and (B) sonoelastography in being able to differentiate between truenodules and pseudonodules in 54 patients with Hashimoto’s thyroiditis (area underthe curve [AUC] = 0.816 for conventional grey scale ultrasonography; AUC = 0.939for sonoelastography; P = 0.0001, McNemar test)
1.0A
0.8
0.6
Sens
itivi
ty
0.4
0.2
00 0.2 0.4
1 – specificity0.6 0.8 1.0
1.0B
0.8
0.6
Sens
itivi
ty
0.4
0.2
00 0.2 0.4
1 – specificity0.6 0.8 1.0

2367
D Yildirim, B Gurses, B Gurpinar et al.Sonoelastography for nodule differentiation in Hashimoto’s thyroiditis
US and FNAB analyses. Importantly, thestudy groups were clearly standardized inorder to ensure that differences were solelydue to the ability of the procedures todifferentiate between the nodular lesions.2
A number of different studies withvarious protocols related tosonoelastography have been published,including manual or automaticcompression, direct compression, or indirectcompression via the carotid pulse; however,the common purpose of these is todetermine the stiffness of the lesion tissue.30
It has also been reported that independentobservers may differ in their diagnosis ofmalignant thyroid nodules.31 Studies haveindicated, however, that measuring thestiffness index of nodules to differentiatemalign thyroid nodules from pseudonodulesmay be a promising technique.31 – 33 Thepresent study evaluated nodules inHashimoto’s thyroiditis patients usingconventional US and sono elastographystrain images to determine the demarcationof nodules, with FNAB as the gold standardfor comparison. The aim was to usesonoelastography to differentiatepseudonodules, which partially mimicnormal gland histology, from the truethyroid nodules using isoelastic strainimages demarcated with different ‘aliasing’patterns. This procedure quantified theamount of compression with a qualityfactor. We had no software to measure thestiffness index, so localization of the noduleswas mapped from the sonoelastographyimages and FNAB samples were takendirectly. The present study demonstratedthat sonoelastography was accurate in thedifferentiation between true nodules andpseudonodules in two ways. First, the false-positive pseudonodules decreased from 6%to 3% using sonoelastography. Secondly,echogenic nodules, where the correction
ratio could be as high as 25%, werefrequently reported as benign, which meantthat the main challenge was to differentiatethe hypoechogenic demarcated nodules.2,10
Sonoelastography corrected false results byas much as 45%. The increase in falsepositives (two of nine cases) is a tolerabledisadvantage of sonoelastography ratherthan misdiagnosing a real thyroid nodule.There were a number of limitations to the
present study: the quality factor was betweenthe determined limits set during the studyand the method was semiquantitative. As aresult, three different qualified observersretrospectively evaluated the recorded realtime images and compared the biopsylocalizations in order to eliminate anysubjectivity. The best way to evaluate thiswas to use the most appropriate statisticalassessment in a cross-table format to obtainsensitivity and specificity levels. Thesubgroups were evaluated separately andthe comparisons were calculated using themost commonly measured accuracy level.The main groups were compared forsignificance by all the parameters.34
The present study demonstrated thatsonoelastography can detect true thyroidnodules that are often misdiagnosed byconventional US. Comparison of values forsonoelastography and conventional USdemonstrated an increase in sensitivity from85.7% to 92.9%, specificity from 77.5% to95.0%, and accuracy from 79.6% to 94.4%,respectively. Thus, sonoelastography is anaccurate technique with which to identifynodular lesions of the thyroid gland, similarin sensitivity to FNAB, but avoiding the useof invasive biopsies or surgicalinterventions.
Conflicts of interestThe authors had no conflicts of interest todeclare in relation to this article

References 1 Volpé R. Autoimmune thyroiditis. In: The
Thyroid, 6th edn (Braverman LE, Utiger RD,eds). Philadelphia: Lippincott, 1991; pp 921 –933.
2 Takashima S, Matsuzuka F, Nagareda T, et al:Thyroid nodules associated with Hashimotothyroiditis: assessment with US. Radiology 1992;185: 125 – 130.
3 Pearce EN, Farwell AP, Braverman LE:Thyroiditis. N Engl J Med 2003; 348: 2646 –2655.
4 Hay ID: Thyroiditis: a clinical update. Mayo ClinProc 1985; 60: 836 – 843.
5 Guarda LA, Baskin HJ: Inflammatory andlymphoid lesions of the thyroid gland.Cytopathology by fine-needle aspiration. Am JClin Pathol 1987; 87: 14 – 22.
6 Mittendorf EA, Tamarkin SW, McHenry CR: Theresults of ultrasound-guided fine-needleaspiration biopsy for evaluation of nodularthyroid disease. Surgery 2002; 132: 648 – 654.
7 Baloch ZW, Cibas ES, Clark DP, et al: TheNational Cancer Institute Thyroid Fine NeedleAspiration State of the Science Conference: asummation. Cytojournal 2008; 5: 6.
8 Danese D, Sciacchitano S, Farsetti A, et al:Diagnostic accuracy of conventional versussonography-guided fine-needle aspirationbiopsy of thyroid nodules. Thyroid 1998; 8: 15 –21.
9 Garra BS, Cespedes EI, Ophir J, et al:Elastography of breast lesions: initial clinicalresults. Radiology 1997; 202: 79 – 86.
10 Yildirim D, Sanal HT, Kocaoglu M: Hyperechoicnodules in Hashimoto’s thyroiditis: correlationwith cytopathological findings; biopsy may notbe necessary at all. Yeditepe Med J 2009; 10: 183– 187.
11 Hall TJ: AAPM/RSNA physics tutorial forresidents: topics in US: beyond the basics:elasticity imaging with US. Radiographics 2003;23: 1657 – 1671.
12 Ophir J, Céspedes I, Ponnekanti H, et al:Elastography: a quantitative method forimaging the elasticity of biological tissues.Ultrason Imaging 1991; 13: 111 – 134.
13 Furukawa MK, Kubota A, Hanamura H, et al:Clinical application of real-time tissueelastography to head and neck cancer:evaluation of cervical lymph node metastasiswith real-time tissue elastography. NipponJibiinkoka Gakkai Kaiho 2007; 110: 503 – 505 [inJapanese, English abstract].
14 Giovannini M, Hookey LC, Bories E, et al:Endoscopic ultrasound elastography: the firststep towards virtual biopsy? Preliminary results
in 49 patients. Endoscopy 2006; 38: 344 – 348.15 Saftoiu A, Vilmann P, Hassan H, et al: Analysisof endoscopic ultrasound elastography used forcharacterisation and differentiation of benignand malignant lymph nodes. Ultraschall Med2006; 27: 535 – 542.
16 Gao L, Parker KJ, Lerner RM, et al: Imaging ofthe elastic properties of tissue: a review.Ultrasound Med Biol 1996; 22: 959 – 977.
17 Greenleaf JF, Fatemi M, Insana M: Selectedmethods for imaging elastic properties ofbiological tissues. Annu Rev Biomed Eng 2003; 5:57 – 78.
18 Goellner JR, Gharib H, Grant CS, et al: Fineneedle aspiration cytology of the thyroid, 1980to 1986. Acta Cytol 1987; 31: 587 – 590.
19 Erdogan M, Erdem N, Cetinkalp S, et al:Demographic, clinical, laboratory, ultra -sonographic, and cytological features ofpatients with Hashimoto’s thyroiditis: results ofa university hospital of 769 patients in Turkey.Endocrine 2009; 36: 486 – 490.
20 Frates MC, Benson CB, Charboneau JW, et al:Management of thyroid nodules detected at US:Society of Radiologists in Ultrasound consensusconference statement. Radiology 2005; 237: 794– 800.
21 Cappelli C, Pirola I, Cumetti D, et al: Is theanteroposterior and transverse diameter ratioof nonpalpable thyroid nodules a sonographiccriteria for recommending fine-needleaspiration cytology? Clin Endocrinol (Oxf) 2005;63: 689 – 693.
22 Cappelli C, Castellano M, Pirola I, et al: Thyroidnodule shape suggests malignancy. Eur JEndocrinol 2006; 155: 27 – 31.
23 Wang N, Xu Y, Ge C, et al: Association ofsonographically detected calcification withthyroid carcinoma. Head Neck 2006; 28: 1077 –1083.
24 Koike E, Noguchi S, Yamashita H, et al:Ultrasonographic characteristics of thyroidnodules: prediction of malignancy. Arch Surg2001; 136: 334 – 337.
25 Moon WJ, Jung SL, Lee JH, et al: Benign andmalignant thyroid nodules: US differentiation:multicenter retrospective study. Radiology 2008;247: 762 – 770.
26 Virmani V, Hammond I: Sonographic patternsof benign thyroid nodules: verification at ourinstitution. AJR Am J Roentgenol 2011; 196: 891– 895.
27 Isik S, Gokay F, Ozuguz U, et al: Comparison ofthe prevalence and sonographic features ofthyroid nodules accompanying autoimmunethyroid diseases. Endokrynol Pol 2010; 61: 658 –664.
• Received for publication 4 June 2011 • Accepted subject to revision 29 June 2011 • Revised accepted 14 October 2011
Copyright © 2011 Field House Publishing LLP
2368
D Yildirim, B Gurses, B Gurpinar et al.Sonoelastography for nodule differentiation in Hashimoto’s thyroiditis

28 Levenson JN, Santaella I, Wachtel MS, et al:Discordance between cytologic results inmultiple thyroid nodules within the samepatient. Acta Cytol 2010; 54: 673 – 678.
29 Mukasa K, Noh JY, Kunii Y, et al: Prevalence ofmalignant tumors and adenomatous lesionsdetected by ultrasonographic screening inpatients with autoimmune thyroid diseases.Thyroid 2011; 21: 37 – 41.
30 Dighe M, Bae U, Richardson ML, et al:Differential diagnosis of thyroid nodules withUS elastography using carotid artery pulsation.Radiology 2008; 248: 662 – 669.
31 Park SH, Kim SJ, Kim EK, et al: Interobserver
agreement in assessing the sonographic andelastographic features of malignant thyroidnodules. AJR Am J Roentgenol 2009; 193:W416 –W423.
32 Asteria C, Giovanardi A, Pizzocaro A, et al: US-elastography in the differential diagnosis ofbenign and malignant thyroid nodules. Thyroid2008; 18: 523 – 531.
33 Lyshchik A, Higashi T, Asato R, et al: Thyroidgland tumor diagnosis at US elastography.Radiology 2005; 237: 202 – 211.
34 Holte RC: Very simple classification rulesperform well on most commonly used datasets.Machine Learning 2008; 11: 63 – 91.
Author’s address for correspondenceDr Duzgun Yildirim
Department of Radiology, Iskenderun Military Hospital, Iskenderun, 31200 Antakya,Turkey.
E-mail: [email protected]
2369
D Yildirim, B Gurses, B Gurpinar et al.Sonoelastography for nodule differentiation in Hashimoto’s thyroiditis





























