Embed Size (px)
Citation preview
1
Non-invasive prenatal genetic testing: A study of public
attitudes
Susan E. Kelly* and Hannah R. Farrimond
ESRC Centre for Genomics in Society (Egenis)
University of Exeter
POSTPRINT: PUBLISHED IN PUBLIC HEALTH GENOMICS
Citation: Kelly, S.E. & Farrimond, H.R. (2012) Non-invasive prenatal genetic testing: A
study of public attitudes. Public Health Genomics, 15 (2): 73-81.
Key Words: Non-invasive prenatal diagnosis, public attitudes, Q methodology, antenatal
screening
*Corresponding author:
Susan E. Kelly
Senior Research Fellow
Egenis
University of Exeter
Byrne House
St. German’s Road
Exeter
Devon EX4 4PJ
Telephone: +44 (0)1392 269140
Fax: +44 (0)1392 264676
2
Abstract
Background/Objectives
Non-invasive prenatal genetic diagnostic (NIPD) tests are being developed using cell-free
fetal DNA in the maternal circulation. NIPD tests avoid or reduce the need for invasive
diagnostic procedures for conditions like Down syndrome. Discussion of ethical and
social implications of these techniques is increasing. We report findings from a study of
public attitudes relevant to the introduction of NIPD. A key aim was to examine the range
of attitudes relevant to NIPD within a diverse sample.
Methods
Qualitative analysis of written free text ‘first responses’ to a written neutral description of
NIPD as part of a Q-methodology study conducted with a purposive sample of the UK
population (N=71).
Results
The majority (63%) of respondents described their first response as positive. However,
respondents displayed ambivalence, expressing positive views of individual/medical
rationale for NIPD and unease concerning public health rationale and societal
implications. Unease related to eugenic reasoning underlying existing prenatal testing,
‘too much control’ in reproduction, commercial provision, information and support
requirements for expanded testing, and limiting the use of testing.
Conclusions
These findings suggest that regulating and monitoring commercial provision of NIPD
services, and monitoring introduction and clinical use, are a public preference.

3
Introduction
Technologies for performing non-invasive prenatal diagnosis (NIPD) utilizing cell free
fetal DNA have been under development since 1997 [1]. Several approaches, particularly
for fetal chromosomal abnormalities such as Down Syndrome, are in clinical trials and
nearing clinical availability. Discussion of broader application of these techniques in
many countries is taking place and can be expected to increase [2]. NIPD is anticipated to
raise a number of ethical and social concerns, including those associated with existing
prenatal diagnostic practices as well as concerns raised by the specific characteristics of
NIPD technologies currently or in the foreseeable future. This paper reports results from
a study of public attitudes relevant to the introduction of NIPD technologies, conducted
in the United Kingdom where prenatal testing regimes are well established aspects of
antenatal care. Qualitative analysis of written ‘first responses’ to a brief, neutral
description of NIPD, elicited as part of a Q methodology study, is discussed in light of
the developing ethical and social implications literature on NIPD.
Background
Current prenatal testing regimes for aneuploidies and some other conditions involve
multiple screening procedures that progressively identify pregnancies deemed to be at
sufficiently high risk to warrant the offer of diagnostic testing of fetal DNA [3]. The
current most widely used methods for obtaining a fetal sample for prenatal diagnosis are
amniocentesis and chorionic villus sampling, both of which carry a small risk of
miscarriage.1 These risks may factor into the decision making of some women and their
partners considering diagnostic testing, and play a role in the clinical management of
some conditions. Screening tests offered in the first and second trimesters of pregnancy,
alone or in association with an ultrasound scan, do not carry this risk [4] [5]. The
distinction between screening and diagnostic testing, and their connection to different
levels of ‘invasiveness’ and risk, have been defining features of antenatal care and
associated testing for several decades. Therefore, NIPD promises to alter many of the
assumptions, practices and experiences of prenatal testing, by providing definitive
1 A loss rate of 1 in 200 from amniocentesis is based on recommendations by the Centers for Disease
Control and Prevention (CDC) and endorsed by the American College of Obstetricians and
Gynecologists (ACOG), both in the USA.
4
chromosomal or molecular information about the fetus without presenting a risk to the
pregnancy.
Current approaches to NIPD utilise cell free fetal ribonucleic acids (cffDNA and
cffRNA) in a sample of maternal blood to diagnosis a limited range of conditions [6].
CffDNA and cffRNA can be detected as early as four weeks gestation, and reliably from
7 weeks [7] [8]. Three possible applications or scenarios of cffDNA/RNA NIPD are
projected:
Targeted diagnostic use to reduce the need for invasive testing in at risk
pregnancies, and to improve clinical management – e.g., NIPD is in limited
clinical use for fetal Rhesus D blood type and inherited sex-linked genetic
disorders [8]. The possibility is raised of extension to most single gene disorders
[9].
In conjunction with or as replacement for current multi-stage screening pathways.
A significant focus of NIPD development efforts is a single non-invasive
diagnostic step for fetal aneuploidies such as Down Syndrome [8], raising the
possibility of wider application of diagnosis for these conditions.
As commercial services offered directly to the consumer in standalone clinics,
over the counter, or over the internet. Commercial, direct-to-consumer products
using cffDNA techniques are currently available to test prenatally for paternity
and fetal sex.
Research on public attitudes relevant to NIPD
The limited social science research on NIPD published to date has focused primarily on
the acceptability of non-invasive testing to pregnant women. A survey of the preferences
of high-risk women undergoing invasive testing found that almost all would request
confirmatory invasive testing following an abnormal result from an NIPD blood test [10].
Roughly half would seek invasive testing following a normal non-invasive testing result.
5
Overall, the authors concluded that women having invasive diagnostic testing welcome a
non-invasive procedure, and that its availability (as part of a multi-step testing pathway)
would decrease invasive testing by approximately 50%.
Public attitudes toward reproductive genetic testing for health purposes have been found
to be broadly positive, in the few public attitude studies reported. A public consultation
in the UK in 2004-2005 found qualified support for expanding prenatal screening
programmes. Concerns included that newly added conditions be ‘serious’ or ‘severe’,
have known or clear forms of inheritance, or be conditions for which no treatment is
available [11]. In the USA, an attitude survey found a generally positive response to
reproductive genetic testing for health related purposes while, overall, public attitudes
were complex and nuanced [12]. Singer [13], in a telephone survey conducted in the
USA found that attitudes toward prenatal testing were overwhelmingly favorable, with
about two thirds of the respondents saying they would want to undergo such tests
themselves (or would want their partner to do so) and believing that the tests will do more
good than harm. However, information about reproductive genetic testing was not widely
dispersed in society, and attitudes toward testing for genetic defects, and attitudes toward
abortion if tests are positive, appeared to be quite distinct. Over time, Singer has found
decreasingly favourable public attitudes in the USA toward selective abortion in case of a
genetic defect [14].
We are not aware of any published empirical research on public attitudes toward the
introduction of NIPD. However, NIPD is now at a stage of development, including
increasing media reporting of early clinical trial results, to suggest that research into
relevant public attitudes is timely. While the few studies conducted on public attitudes
toward prenatal testing to date indicate societal support for current practices, they also
indicate that public attitudes are complex, nuanced, and potentially contradictory (see
15).
Q methodology study on public attitudes relevant to NIPD

6
This paper reports the results of qualitative analysis of study participants’ written ‘first
responses’ to NIPD after reading a short factual introduction to the topic. These were
obtained in the context of a Q methodology study of public attitudes relevant to NIPD2
[16]. The overall aim of the study was to identify the range of viewpoints on NIPD
amongst a sample of the UK public with a diversity of experiences and demographic
characteristics. Q methodology was chosen for this study as it fits with a social
constructionist perspective that a multiplicity of discourses, sometimes conflicting, is
available in any culture from which understanding of new technologies or subjective
experience of health, illness and health care, can be reached [17] [18] [19]. Q
methodology is a useful method through which to investigate public responses to
emerging technologies, particularly as it does not ask for responses to hypothetical
scenarios [20]. It is also useful for researching public discourses concerning controversial
or sensitive topics, as it can be conducted by post (as here), allowing the participant to
consider and respond without the need for immediate social interaction with a researcher
[21]. Q methodology has advantages over qualitative interviews which, although more
naturalistic, are limited where participants have little knowledge of or experience with a
technology. Q methodology has had a resurgence of use in health and illness research
[18] [19] [21] [22] [23] [24] [25].
Q methodology combines factor analysis with qualitative interpretation to identify a set
of common ‘viewpoints’ amongst a sample (for detailed descriptions of Q methodology
see [26]). Respondents are asked to sort, or rank, statements on or relevant to a topic on
the basis of the extent to which they agree, disagree or feel neutral about them.
Quantitative analysis of these sorts is conducted to identify a set of statistically separate
‘accounts’, while interpretation is aided by analysis of written, qualitative responses
Results of our Q sort analysis of attitudes toward NIPD are reported elsewhere [16].
For this study, we included a pre-sorting step to provide respondents an introduction to
NIPD. This constituted a brief, neutral paragraph describing NIPD technologies, located
2 ESRC Study: ‘Is easier always better?: investigating public attitudes towards non-
invasive prenatal technologies’ Initiated January 2009.
7
at the front of the Q booklet. We undertook a pilot test of the description to ensure it was
not leading or biased, and was easily understandable. The description did not identify
ethical or societal issues, but focused solely on key characteristics of emerging tests (i.e.,
blood test, performed early in pregnancy, diagnostic accuracy, avoids the physical risks
of invasive procedures, could open the possibility of testing for a wider range of
conditions, may be available as a commercial service). Immediately following this
description was a free text space in which participants were asked to provide a written
‘first response’. This process was also pilot tested. All respondents provided a written
first response to the NIPD description.
Our objective in soliciting ‘first responses’ to the topic of NIPD was two-fold. Firstly,
participants needed to be introduced to technological parameters of NIPD so that they
had enough information to make informed judgements about the social, ethical and other
issues as required in the Q-sorting task. Secondly, we aimed to understand what the
participants themselves perceived as the key benefits and concerns of NIPD when first
presented with the options. First response data can indicate what participants find salient
from among the multiple attitudes they hold relevant to the topic [27] or, put differently,
elicit the salient social schema(s) through which they understand a topic (e.g., [28]). First
responses thus represent what respondents themselves bring to understanding of an issue
outside of elicitation effects from an interviewer or the Q sort process.
Respondents were sent the research materials by post and completed the tasks on their
own. Separate interviews were not conducted.
We conducted a thematic analysis of these written first responses (N=71). Each author
conducted a thematic analysis separately; these were combined for re-analysis, from
which the final thematic scheme emerged. Representative quotes from these written
responses are included to illustrate the themes.
Sample

8
The aim of this study was to investigate public understandings of NIPD both among those
often selected in study samples (e.g., pregnant women and their partners, those in high
risk pregnancies) but also among those who are not (men, those without children, a broad
age range, those with little experience of genetic disorders or disabilities). Therefore, we
sought a diverse sample using a purposive sampling strategy (see [29]). Inclusion criteria
were UK individuals aged 18 and 60 of both genders. Participants were recruited via a
range of media sources from the South West of the UK. Participants were given a £15
voucher upon completion of the study booklet.
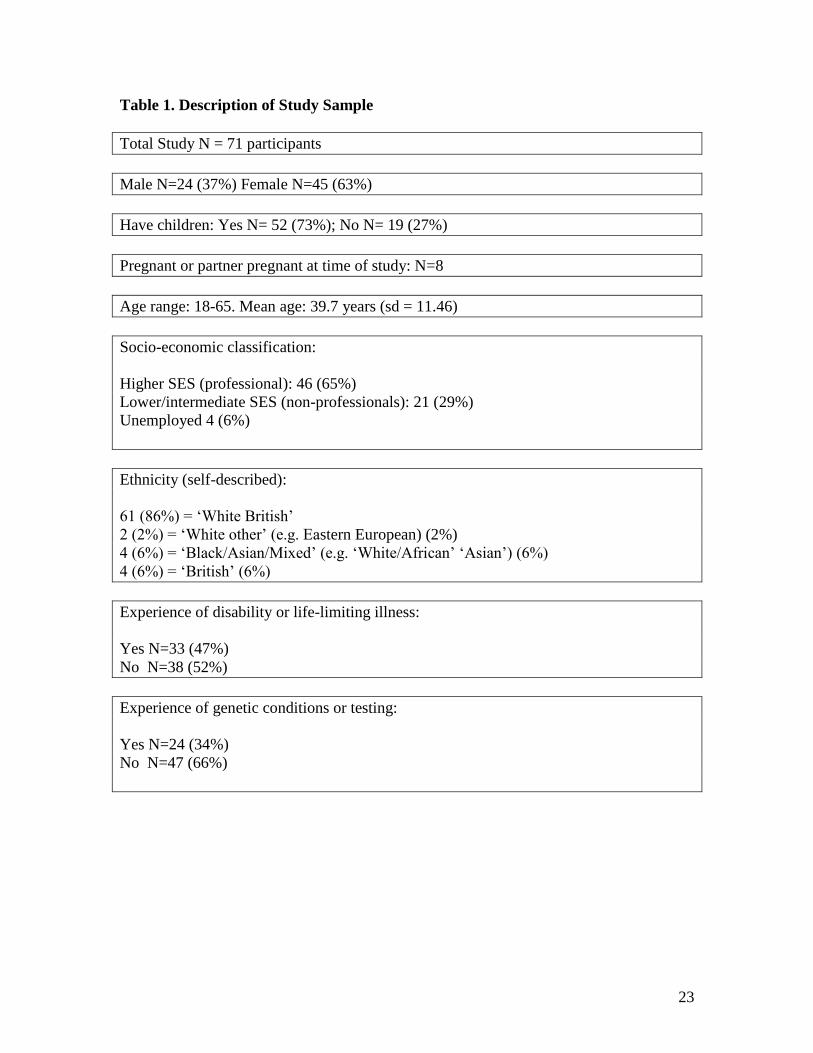
Ninety-seven participants responded to the initial invitation to take part and were sent
study packs. Seventy-one completed packs were returned in total (73% response rate). A
demographic profile of the participants is found in Table 1.
The study was approved by the Humanities and Social Science Ethics Committee at the
University of Exeter.
Findings
First response – positive or negative
We initially coded each response as positive or negative (and respondents frequently used
this language). The majority (45 or 63%) of first responses was positive concerning
NIPD. However, nearly half (23) of these contained a caveat after the initial positive
response. For example:
The pluses are it would present less risk to the foetus (e.g., the trauma of invasive
testing & anxiety for pregnant women). However the administration of testing
would need to be carefully devised to prevent abuse. A plethora of bio-ethical
issues are present. (Female, 37 years old, one child, familial and work experience
with disability, speech therapist)
Five responses were explicitly ambivalent, as in the following examples:
9
My immediate thought is that I feel very much divided on this subject. In terms of
science this is a huge step forward, but then the moral implications of this are
equally significant. (Male, 33 years old, no children, no experience of genetic
conditions or disability, academic administrative staff)
NIPD has to be beneficial if it helps parents to know of problems that could occur.
But I am concerned that tests would become to (sic) easily ‘in use’ and used
unnecessarily. (Female, 48, 3 children, looking after home/family)
Twenty-one responses focused only on negative issues and concerns with the technology.
The easier & more reliable tests become, the more society will adopt a ‘why
weren’t you terminated?’ attitude to disabled people & their parents (especially
their mothers). Why is the medical profession trying so hard to eliminate
individuals with Down Syndrome? (Female, 55 years old, three children, familial
experience with genetic conditions and disability, looking after home/family)
Key Themes
Challenge to ‘public health’ rationale for prenatal screening and testing programmes
and support for individual/medical rationale
This theme encompasses responses we coded as challenging the public health rationale
underlying prenatal testing programmes. Responses in this theme did not represent NIPD
as raising new social and ethical questions, but as extending or exacerbating concerns
with existing practices. Challenges to the public health rationale fell into two primary
categories: those reflecting a disability critique (what one respondent termed ‘fatal
discrimination against the disabled’), and those reflecting unease over the notion of
‘choosing’ children (as one respondent put it, ‘this amount of choice is going down the
wrong path societally’). These responses suggest that unease exists in public attitudes
concerning the public health rationale and societal implications of prenatal screening
10
programmes, and of their expansion. Respondents expressing this theme varied in terms
of experiences with disability and having children.
The following quotes are representative of this theme:
There are already groups in society – both medical & lay persons who presently
regard current pre-natal screening as a method of reducing the incidence of all
disability, therefore promoting attitudes towards perfection. I fear that, in general,
NIPD will exacerbate this attitude. (Female, 54 years old, no children, familial
and work-related experience with genetic conditions and disability, teacher of the
deaf )
Clearly it’s better to have non-invasive testing as invasive testing has its own
risks. But – how far are we willing to go along the lines of testing and deciding
who has the right to be born? (Male, 66 years old, 4 children and partner
pregnant, no experience of genetic conditions or disability, manufacturing
manager)
It will, and should, open up much moral debate, particularly around abortion and
eugenics. (Female, 36 years old, no children, no experience of genetic conditions
or disability, nurse)
Nonetheless, there was considerable support for what might be termed medical/individual
rationale for prenatal screening and testing programmes. Many respondents expressed
seeing the value of prospective parents including prenatal screening decisions in seeking
healthy outcomes for their offspring. Specifically, respondents mentioned that earlier
testing is a benefit, as it should promote easier decision making and, particularly, give
prospective parents ‘more time to prepare’ for an indentified outcome.
11
‘Safer’ testing was identified as a particular benefit. Significantly, and in contrast to the
above representations of challenges to societal implications of expanded testing, many
respondents included the view that ‘expectant parents should have choice’.
I think they are a good idea if it makes it easier and safer for the woman and baby.
Accuracy is important so I think it’s a good idea. (Male, 34 years old, one child,
no experience of genetic conditions or disability, computer programmer)
I think non-invasive prenatal testing is a very positive step forward. Invasive tests
may put the baby at risk & therefore many women may decide against it –
whereas most will be happy with blood tests. (Female, 64 years old, two children,
familial experience with a genetic condition, retired school teacher)
However, an exception to the positive view of the individual level medical benefits of
NIPD was concern about increased anxiety associated with NIPD procedures. The
following quotes exemplify this response, suggesting that while public attitudes toward
testing outcomes and rationale are generally positive, the process of testing and the
decisions involved are understood to be difficult.
Regardless of the advantages (safety, accessibility, etc.) these tests will still create
stress through anxiety and apprehension and the necessity of making decisions.
(Female, 55 years old, three children, familial experience with genetic conditions
and disability, looking after home/family)
I’m a bit uneasy about the idea – when my wife was pregnant, I wasn’t crazy
about the tests we had, not so much because of the risks, but because of not
knowing what I’d do with the information if tests came back with difficult results.
(Male, 30, one child, no experience with genetic conditions or disability, part-
time school teacher)
12
Generally better than the poorly understood risk options currently available, but I
am slightly uneasy that too much testing causes a lot of anxiety and puts pressure
on people to test and act on the tests. (Female, 35 years old, one child, some
experience of genetic conditions, looking after home/family)
I think it will lead to added anxiety in pregnancy and to women having more
abortions. (Male, 48, familial experience of autism, unemployed mail deliverer)
Concern about commercial availability of NIPD services
Many responses reflected concern about the implications of commercial availability of
NIPD testing. A number of respondents worried about NIPD offered in a commercial
setting without ‘appropriate advice and guidance’, particularly ‘as the range of tests
increases’. In particular, it was perceived that commercially provided services would
allow for ‘misuse’ (primarily defined as testing for ‘trivial or vague’ reasons) and there
was strong concern about monitoring, medical oversight, and support. For example:
Any testing which avoids physical risks to the foetus and which can be carried out
earlier in the pregnancy can only be beneficial as long as the results are accurate. I
would feel happier for the testing to be carried out by a health professional as
opposed to the consumer to be sure it was done correctly and any worrying results
investigated by the health professionals using their knowledge and expertise.
(Female, 46, three children, no experience of genetic conditions or disability,
teaching assistant)
The possibilities sound very positive; but some concerns about possible
misuses/abuses in the commercial sphere – e.g. insurance companies
granting/denying cover on the basis of test results. (Male, 54, three children,
familial experience with a genetic condition, publisher)
13
It’s a good thing but must be supported with proper counseling & medical &
emotional care afterwards. (Female, 41 years old, three children, some experience
of genetic conditions, university lecturer)
Positive overall but concerned that people will be able to obtain results in a
commercial environment without appropriate advice and guidance available.
(Male, 59, two children, familial experience with a disability, IT consultant)
Ambivalence
As the above discussions indicate, ambivalence constituted a strong theme throughout the
responses. While many saw benefits for pregnant women and families, there was
expression of fear that NIPD will exacerbate societal attitudes perceived to be associated
with current prenatal screening, particularly promoting attitudes toward ‘perfection’ in
reproduction. A number of respondents also expressed that decisions associated with
current prenatal testing programmes are difficult, and perhaps currently not adequately
supported.
I think it’s good to be able to test for disabilities as some parents won’t be able to
deal with them and their child will have a poor quality of life, but where do you
draw the line? (Female, 23, no children but currently pregnant, no personal
experience with genetic conditions or disabilities, employment consultant)
It could be useful, but primarily isn’t for the health of the pregnant woman. It will
be used to identify disabled babies and women will be put under extra pressure
awaiting results, and then encouraged by media to terminate suspect pregnancies.
(Female, 42, three children, much experience with childhood disability,loooking
after home/family)
Not sure ‘easy’ information is necessarily a good thing. I wonder whether people
may not opt to have them without thinking about what they will do with the result.

14
(Female, 33, one child, work-related experience of disability, speech therapist -
adult)
It is inevitable with advances in medicine, screening will become more
sophisticated. However, this will result in major dilemmas for expectant parents.
It is very difficult to decide whether to terminate a pregnancy if it is likely the
baby will have a genetic or other disorder and we would have to bear in mind that
when the child is older, cures may be found for that disorder. (Female, 59, three
children, no experience with genetic conditions or disability, self-employed
artist).
Limits
According to this set of public responses, NIPD raises questions about limits on the use
of prenatal genetic diagnosis. This theme is expressed through much of the above
discussion, particularly in concerns about possible availability of testing outside of the
health service context, and because testing would be ‘easier’. These concerns, and the
ambivalence described above, suggest that a system of monitoring the use of testing
would be in accordance with public attitudes. Further, they suggest a role for public
engagement in any expansion of conditions tested for beyond the existing availability of
tests. The following are representative of concerns about limits on testing use:
The improvements over safety for mother and child through NIPD will no doubt
be welcomed. Moreover, where it merely replaces current screening techniques I
see little room for controversy. However, as soon as the technology broadens its
range, it presents serious dangers of misuse and abuse by both companies and
parents as they are given more control over the design of their children. (Male, 21,
no children, no experience with genetic conditions or disability, student)
It sounds like NIPD could easily get out of hand, with the possibilities of misuse
and data mishandling. (Female, 37, one child, familial experience with disability,
teaching assistant)
15
Abortion more common. Could abort a foetus for something a person could
develop later in life. The system could be abused to give choice of hair, eye, even
skin colour. (Male, 46, three children, no experience of genetic conditions or
disability, maintenance worker)
Discussion
Our findings reflect previous studies in identifying generally positive attitudes toward
risk reduction in prenatal testing. However, public attitudes toward the prospective
introduction of non-invasive prenatal genetic diagnostic testing also reflected
ambivalence regarding public health rationale and societal impacts of earlier and easier
prenatal genetic diagnosis. Many were divided - often within one response - concerning
benefits and drawbacks. A major divide was between perceptions of medical benefit to an
individual pregnant woman/couple, where NIPD is generally viewed in a positive light,
and societal implications of expansion of choice, particularly ‘too much choice’, which
was often viewed negatively. While this may not reflect new societal and ethical
concerns, it suggests that expansions from existing prenatal testing practices, may re-
open debate on societal and ethical implications of prenatal screening, particularly debate
about limits.
Concerns about limits appeared to be connected to societal implications regarding
normalisation of a quest for ‘perfection’ and lack of tolerance of disability, and to a
perceived likely expansion in abortions. Concern about limits was also connected to
commercial, and particularly direct-to-consumer, access to testing which places decision
making solely in the hands of consumers, suggesting the important role of health
professionals as gatekeepers. NIPD also raised for many concerns about non-medical
uses of tests.
The association of existing prenatal screening practices with eugenic rationale appears to
have a strong place in public attitudes in this UK sample, particularly as expressed
16
through language reflecting the ‘disability critique’. Such critiques have argued that
existing prenatal testing practices are a form of discrimination against people living with
a target condition (e.g., Down Sydrome), and that the routine availability of testing leads
to material and/or ‘expressive’ harm [30]. Further, critiques from these perspectives have
suggested that the availability of testing has an impact on social attitudes and contributes
toward the stigmatisation of people with the condition [30] [31] [32].
Respondents also expressed the view that current prenatal testing practices cause anxiety
for pregnant women, pose moral dilemmas, and require counselling and support of health
professionals. The need for support, counselling and guidance from health professionals
was expressed strongly with regard to NIPD, and appeared to be one of the factors in
negative responses to the commercial availability of services. These responses raise the
question of whether current information provision and counselling models are sufficient
for expanded genetic diagnostic applications of NIPD, in the public view.
Because the question of limits on prenatal testing can be connected to societal practices
regarding abortion, concerns about limits as reflected in public attitudes in this sample
suggest that implications for legal approaches to abortion should be considered. As Hall
et al. [33] state, regarding the UK context, ‘controversial uses of technology can become
a routine part of practice without legal and ethical analysis, and … the NHS is part of the
broader social system. As such, it would be short-sighted to assume that the use of
cffDNA technologies within the NHS will not raise questions about abortion’ (p. 14).
Similar concerns may apply in other national and health system contexts (for example, in
the USA where states are empowered to enact legislation concerning abortion access).
We present this analysis against the backdrop of existing ethical and social debates about
prenatal testing, and a developing literature on NIPD. Many ethical and social debates
associated with existing prenatal diagnostic practices have not been resolved, and may be
exacerbated or revisited with the introduction of NIPD. In relevant literatures, association
continues between prenatal genetic diagnosis with selective termination of an affected
fetus and past eugenic practices, as well as current strands of eugenic debate [34] [35].

17
Reducing the incidence of conditions of interest in the population is an implicit goal in
the availability of screening programmes [36]. Hovering in the background of these
debates are questions of what constitutes, and what measures are appropriate, to forward
the public’s health. These concerns are countered, to some extent and nonetheless
debatably, by the individualising discourses and practices of reproductive autonomy and
informed choice. Nonetheless, debate continues over how effective current prenatal
genetic counselling practices are in ensuring informed choice, and how they might be
improved [37] [38].
Existing prenatal testing practices have been criticised for normalising termination of
pregnancy for fetal abnormality, and for profoundly impacting the individual and social
experience of pregnancy [39]. The possibility of identifying fetal abnormality via
screening and invasive testing has led to a social phenomena of the ‘tentative pregnancy’
in which public disclosure of pregnancy is only made after no problems with fetal health
have been identified [39]. Connecting these critiques are concerns that women feel
pressure, whether within clinical, familial, or broader social contexts, to test and
terminate to avoid giving birth to an affected child [40]. Many studies have identified that
the decision to test is often not well informed, but rather seen as routine practice [41] [42]
[43]. The question of how severe or ‘serious’ a condition should be to be subject to
prenatal testing continues to be debated [44] [45]. These concerns were also reflected in
the ‘first responses’ analysed in this study.
Several analysts have sought to determine whether NIPD raises new social and ethical
issues, in a growing number of publications [1] [33] [36] [46] [47] [48] [49] [50] [51]
[52]. While acknowledging the advantages of NIPD over current practices in terms of
earlier and safer testing, most identify social and ethical concerns beyond those identified
with current prenatal testing practices. Primary among these is the need for carefully
considered counselling and informed consent procedures, especially should NIPD replace
current multi-step testing with a one-step diagnostic test. Other issues follow from the
ease with which the maternal blood sample for testing could be obtained. These include
fetal sexing for non-medical reasons; prenatal paternity testing; normalisation of testing

18
for minor abnormalities; testing being offered for a wider range of conditions without
sufficient scrutiny (similar to the ‘specification creep’ identified in [33]); and an increase
in the number of abortions performed due to higher numbers of women undergoing
diagnostic testing. The commercial potential of a blood sample based test has also been
raised, given the relative simplicity with which a sample can be provided. The possibility
of expanded forms of testing offered commercially raise considerable ethical, as well as
regulatory, concerns. Many of these ‘new’ concerns were raised by participants in this
study.
This data-set of ‘first responses’ was gathered from a purposive sample of the public and
does not constitute a random sample from which to generalize. Some self-selection of
participants may have occurred with regard to prior interest in prenatal testing or
disability, although over half reported no experience of disability or genetic disorders.
The methodology used does present a literacy bias and this is reflected in the generally
educated sample and in the written quotes presented. Nonetheless, these study results
have an important purpose in outlining parameters of concern for the public in relation to
NIPD. Research into public attitudes is important in providing the societal backdrop to
decisions made about prenatal testing for genetic conditions at institutional and individual
levels. As Rapp [53] has pointed out, lay individuals and communities create explicit and
implicit norms around reproductive choice, termination and disability. These norms form
the ‘public life’ in which prospective parents will make their private (or not so private)
choices about NIPD. Examining public attitudes is particularly important in the case of
prenatal testing given criticisms of the limited public discussion of routine
implementation of current practices.
References
1. Lo YWD, Corbetta N, Chamberlain PF et al.: DNA in maternal plasma and serum.
Lancet 1997; 350: 485-487.
2. de Jong A, Dondorp W, de Die-Smulders CEM, Frints SGM, de Wert GMWR:. Non-
invasive prenatal testing: ethical issues explored. Eur J Hum Genet 2010;18: 272-277.
19
3. Driscoll, DA, Gross SJ for the Professional Practice and Guidelines Committee (2008) First
trimester diagnosis and screening for fetal aneuploidy. Genet Med 2008; 10(1):73–75.
4. American College of Obstetricians and Gynecologists: Screening for fetal
chromosome abnormalities. ACOG Practice Bulletin Obstet Gynecol 2007;109: 217–
227.
5. Benn PA, Campbell WA, Zelop CM, Ingardia C, Egan JF: Stepwise sequential
screening for fetal aneuploidy. Obstet Gynecol 2007;197: 312.e1–312.e5.
6. Lo YM, Tsui NB, Chiu RW et al. Plasma placental RNA allelic ratio permits
noninvasive prenatal chromosomal aneuploidy. Nat Med 2007; 13:218-223.
7. Illanes S, Denbow M, Kailasam C, Finning K, Soothill P: Early deterction of cell-free
fetal DNA in maternal plasma. Early Hum Dev 2007; 83: 563-566.
8. Hahn S, Chitty LS: Noninvasive prenatal diagnosis: current practice and future
perspectives. Curr Opin Obstet Gynecol 2008; 20(2):146-51.
9. Norbury G, Norbury,CJ: Non-invasive prenatal diagnosis of single gene disorders:
How close are we? Semin Fetal Neonatal Med 2008;13(2): 76-83.
10. Zamerowski ST, Lumley MA, Arreola RA, Dukes K, Sullivan L: Favorable attitudes
toward testing for chromosomal abnormalities via analysis of fetal cells in maternal
blood. Genet Med 2001; 3: 301-9.
11. People Science & Policy. Choosing the Future: Genetics and Reproductive Decision-
Making Analysis of responses to the consultation Final report prepared for The Human
Genetics Commission, May, 2005.
12. Genetics and Public Policy Center. Reproductive Genetic Testing: What America
Thinks. Washington, DC, 2004, www.DNApolicy.org.
13. Singer E: Public attitudes toward genetic testing. Popul Res Policy Rev, 1991;10(3):
235-255.
14. Singer E, Corning AD, Antonucci T: Attitudes toward genetic testing and fetal
diagnosis, 1990-1996. J Health Soc Behav, 1999;40: 429-445.
15. Kelly SE: Choosing not to choose: reproductive responses of parents of children with
genetic conditions or impairments. Sociol Health Illn 2009; 31(1): 81–97.
16. Farrimond HR, Kelly SE: Non-invasive prenatal genetic tests: Public understandings
of bioethical issues. In preparation.
20
17. Brown SR: Q methodology and qualitative research. Qual Health Res 1996; 6: 561-
567.
18. Eccleson C, Williams ACDC, Stainton Rodgers W; Patients' and professionals'
understandings of the causes of chronic pain: Blame, responsibility and identity
protection. Soc Sci Med 1997; 45: 699-709.
19. Stainton Rogers W. (1991). Exploring health and illness: An exploration of diversity.
Hemel Hempstead: Harvester Wheatsheaf.
20. Farrimond HR, Kelly SE: ‘It made me think’: Researching public attitudes to
emerging technologies using Q-methodology. In preparation.
21. Farrimond HR, Joffe H, Stenner P: A Q-methodological study of smoking identities.
Psychology & Health 2010 iFirst.
22. Risdon A, Eccleston C, Crombez G, McCracken L; How can we learn to live with
pain? A Q-methodological analysis of the diverse understandings of acceptance of
chronic pain.. Soc Sci Med 2003; 56: 375-386.
23. Baker R; Economic rationality and health and lifestyle choices for people with
diabetes. Soc Sci Med 2006; 63: 2341-2353.
24. Hughner RS, Kleine SS; Variations in lay health theories: Implications for consumer
health care decision making. Qual Health Res 2008; 18: 1687-1703.
25. Bryant LD, Green, JM, Hewison J; Understandings of Down's syndrome: A Q
methdological investigation. Soc Sci Med 2006; 63: 1188-1200.
26. Stenner P, Watts S, Worrell M: Q methodology, in Willig C and Stainton Rodgers W
(eds.), The Sage Handbook of Qualitative Research in Psychology, London, Sage
Publications, 2008: 215-239.
27. Farrimond H, Joffe H: Pollution, peril and poverty: The stigmatisation of British
smokers, J Community Applied Soc Psych 2006;16: 481-491.
28. Fiske ST; Taylor SE: Social Cognition: From Brains to Culture. Columbus, OH,
McGraw-Hill, Inc.: 2007.
29. Watts S , Stenner P: Doing Q methodology: theory, method and interpretation. Qual
Res Psych 2005; 2: 67-91.
30. Parens E, Asch A: Prenatal testing and disability rights. Washington, DC,
Georgetown University Press, 2000.
21
31. Parens E, Asch A: Disability rights critique of prenatal genetic testing: reflections and
recommendations. Ment Retard Dev Disabil Res Rev 2003; 9: 40-47.
32. Shakespeare T: Choices and Rights: Eugenics, genetics and disability equality.
Disabil Soc 1998;13(5): 665 — 681.
33. Hall A, Bostanci A, John S: Ethical, legal and social issues arising from cell-free fetal
DNA technologies. Appendix III to the report: Cell-free fetal nucleic adids for non-
invasive prenatal diagnosis, PHG Foundation, Cambridge UK, 2009.
34. Hubbard R: Eugenics and prenatal testing. Int J Health Serv 1986; 16(2): 227-242.
35. Raz A:’Important to test, important to support’: attitudes toward disability rights and
prenatal diagnosis among leaders of support groups for genetic disorders in Israel. Soc
Sci Med 2004; 59:1857–1866.
36. Newson AJ: Ethical aspects arising from non-invasive fetal diagnosis. Semin Fetal
Neonatal Med 2008; 13L:103-108.
37. Clarke A: 1992. Is non-directive genetic counseling possible? Fetal Diagn Ther 1992;
47(5): 304-305.
38. Marteau TM, Dormandy E: Facilitating informed choice in prenatal testing: How well
are we doing? Am J Med Genet C Semin Med Genet 2001; 106(3): 185 – 190.
39. Rothman BK: The tentative pregnancy: how amniocentesis changes the experience of
motherhood. New York, WW Norton, 1993.
40. Browner C, Press N: The normalization of prenatal diagnostic screening; in Ginsberg
FD and Rapp R (eds.) Conceiving the new world order: the global politics of
reproduction, Berkeley, University of California Press, 1995.
41. Markens S, Browner CH, Press N: ’Because of the risks’: how US pregnant women
account for refusing prenatal screening. Soc Sci Med 1999; 49: 359–369.
42. Green JM, Hewison J, Bekker HL, Bryant LD, Cuckle HS: Psychosocial aspects of
genetic screening of pregnant women and newborns: a systematic review. Health Technol
Assess 2004;8: 1–124.
43. Ritchie K, Boynton J, Bradbury I, et al: Routine ultrasound scanning before 24 weeks
of pregnancy. Health Technology Assessment Report 5, NHS Quality Improvement
Scotland, Glasgow, 2004.
22
44. Boyle RJ, Savulescu J: 2003. Prenatal diagnosis for ‘minor’ genetic abnormalities is
ethical. Am J Bioeth 2003;3(1): W-IF 3.
45. Strong C: Tomorrow’s prenatal genetic testing. Should we test for ‘minor’ diseases?
Arch Fam Med 1993; 2: 1187-1193.
46. Wright CF, Burton H: The use of cell-free fetal nucleic acids in maternal blood for
non-invasive prenatal diagnosis. Hum Reprod Update 2009;15: 139-151.
47. Wright CF: Cell-free fetal nucleic acids for non-invasive prenatal diagnosis. Report of
the UK expert working group, PHG Foundation, Cambridge, UK, 2009.
48. Wright C, Chitty LS: Cell-free fetal DNA and RNA in maternal blood: implications
for safer antenatal testing. Br Med J 2009; 339: b2451.
49. Benn PA, Chapman AR: Practical and ethical considerations of noninvasive prenatal
diagnosis. JAMA 2009;301: 2154-2156.
50. Schmitz D, Netzer C, Henn W: An offer you can’t refuse? Ethical implications of
non-invasive prenatal diagnosis. Nat Rev Genet 2009;10: 515.
51. Schmitz D, Henn W, Netzer C: Commentary: No risk, no objections? Ethical pitfalls
of cell-free fetal DNA and RNA testing. Br Med J 2009;339: b2690.
52. Smith RP, Lombaard H, Soothill PW: The obstetrician’s view: ethical and societal
implications of non-invasive prenatal diagnosis. Prenat Diagn 2006; 26: 631-634.
53. Rapp R. Testing women, testing the fetus: The social impact of amniocentesis in
America. New York and London, Routledge, 2000.
23
Table 1. Description of Study Sample
Total Study N = 71 participants
Male N=24 (37%) Female N=45 (63%)
Have children: Yes N= 52 (73%); No N= 19 (27%)
Pregnant or partner pregnant at time of study: N=8
Age range: 18-65. Mean age: 39.7 years (sd = 11.46)
Socio-economic classification:
Higher SES (professional): 46 (65%)
Lower/intermediate SES (non-professionals): 21 (29%)
Unemployed 4 (6%)
Ethnicity (self-described):
61 (86%) = ‘White British’
2 (2%) = ‘White other’ (e.g. Eastern European) (2%)
4 (6%) = ‘Black/Asian/Mixed’ (e.g. ‘White/African’ ‘Asian’) (6%)
4 (6%) = ‘British’ (6%)
Experience of disability or life-limiting illness:
Yes N=33 (47%)
No N=38 (52%)
Experience of genetic conditions or testing:
Yes N=24 (34%)
No N=47 (66%)





























