Embed Size (px)
Citation preview

Journal of Human Nutrition and Dietetics (1993), 6, 335-353
Nutrition knowledge, attitude to healthier eating and dietary intake in pregnant compared to non-pregnant women
A. S. Anderson,* D. Campbell and Richard Shepherdt Deportment of Obstetrics. University of Aberdeen, Aberdeen Maternity Hospital. Cornhill Rood, Aberdeen. UK; and tAFRC Institute of Food Research, Reading Laborotory, Eorley Gate, Whiteknights Road, Reading, UK
The nutrition knowledge, attitudes and dietary behaviour of a group of women in early pregnancy and a group of non-pregnant women were compared to ascertain the impact of pregnancy on diet. The main results indicate that pregnant women do eat differently from non-pregnan t women, in particular intakes of zinc and vitamin C. and the nutrient density of protein and sodium were higher and intakes of alcohol lower in the pregnancy group compared to the non-pregnant p u p . The group of pregnant women also tended to consume more milk and fruit and less chocolate, cakes and pastries compared to non- pregnant women. However, the differences in dietary behaviour between the two groups could not be accounted for by nutrition knowledge [the same in both groups). Higher scores for beliefs about ‘healthior eating’ and subjective norm were found in the early pregnancy group which might account for some of the observed differences between the groups. In addition. it is concluded that ‘historicity’ or a basic ‘knowledge’ of which foods to consume is prevalent in early pregnancy.
Key words: attitudes, diets, healthier eating, pregnancy.
Introduction
The role of diet in pregnancy has been highlighted recently following speculation about the intrauterine environment and subsequent adult health profiles (Barker, 1992). Studies of nutrient intake in preg- nancy are numerous (Black et al., 1986 Anderson & Lean, 1986 Thompson et al., 1989) but few have focused on differences in food habits, nutrient intakes and reasons for diet selection at this time. Pregnancy is
‘Correspondence: Dr A. Anderson, University of Glasgow Department of Human Nutrition, Glasgow Royal Infirmary, Alexandra Parade, Glasgow.
usually associated with changes in dietary intake (Taggart, 1!361; Tierson et al., 1985; Stewart et al., 1988). Food selection, meal patterns and food preparation may all be affected by a wide range of factors which may start in the first few weeks of preg- nancy and continue until the baby is delivered.
Many reasons for these dietary changes have been suggested. Firstly, there are a number of physical symptoms which might influence food intake. The early months of pregnancy are often associated with nausea and vomiting. Stewart et al. (1988) reported that 59% of 107 Scottish women suffered from vomiting in early
335

336 A. S. Anderson, D. Campbell and R. Shepherd
pregnancy and 32% altered their diets to alleviate symptoms. The details of dietary alterations were not given although it was suggested that some women may have altered their carbohydrate intake.
Another ‘digestion-associated’ symptom which is frequently found in pregnancy is constipation. Anderson (1984) reported that 38% of Cambridgeshire women claimed to have been constipated at some- time during pregnancy and 71% of suffer- ers used dietary manoeuvres including the addition of bran to foods, changing to whole-grain cereal and bread and increas- ing fruit and vegetable intakes. Some women also claimed to make dietary alter- ations such as eating brown sugar, choco- late and liquorice, presumably in response to social pressure from health profession- als and lay advice.
Some women also experience consider- able changes in appetite and thirst which together may account for the initial weight gain Forsum et al., 1988) observed at antenatal booking clinics. Maclntyre (1983) reported Aberdeen women in early preg- nancy as exhibiting compulsive eating and describing themselves as ‘starving’, al- though she also described women with a complete loss of appetite. Dietary cravings for foods normally considered inedible (pica) has also been described during pregnancy, including laundry starch, ice (Beerbohm-Schwab & Axelson, 1984), rocks, matchboxes and clay (Snow & John- son, 1978).
In addition to the dietary and life-style changes that women may undertake in response to physical symptoms during pregnancy, food selection may also be altered by voluntary actions aimed at op- timizing maternal health and pregnancy outcome. There is now widespread promo- tion, in the popular (Robarts. 1988). profes- sional (Thomas, 1988), scientific (Chamber- lain, 1986) and health education (HEC. 1989) literature for alterations in diet, alcohol intake and smoking habits to com- mence early in pregnancy (or even before conception), when the impact of these changes on fetal development and growth is likely to be most beneficial. From a practical point of view, it may be easierto
make changes in food habits and nutrient intake in early pregnancy before tiredness and increasing size become an obstacle to initiating new ideas and the focus of care changes from the needs of the baby in utero to the more practical aspects of the baby in its nursery surroundings.
Dietary advice has the potential to influ- ence knowledge about nutrition and atti- tudes towards nutrition. However, there is considerable debate on how nutrition knowledge and attitude might influence nutrition behaviour. Social-psychological theories suggest that knowledge, attitude and behaviour should be consistent, but a number of studies suggest that the rela- tionships between these variables are nei- ther simple nor automatic (Axelson et al., 1985).
Knowledge about nutrition may not necessarily be positively associated with nutrition behaviour. There is a general assumption that a greater knowledge of nutrition is likely to be accompanied by better (i.e. healthier) nutrition behaviour. However, being well informed does not mean that people will act according to one particular set of beliefs in promoting health and preventing disease. Information may be disregarded, altered or may even be used to justify existing behaviour rather than stimulate behavioural change. Thus, there is a general feeling amongst many nutrition educators that nutrition knowl- edge functions as a tool only if and when individuals are ready to make changes (Parraga, 1990).
Many workers have expressed the view that knowledge alone (or the persuasion process) is not enough to change behav- iour. Attitude change must mediate the process, i.e. a person must have knowledge of certain information but also feel it is important and probable (belief). The role of attitudes in food choice has been widely studied but results have varied according to the assessment methods.
One method which has been widely used in the area of food choice is the Theory of Reasoned Action (Ajzen & Fish- bein, 1980; also Bonfield, 1974; Dalton et al.. 1986 Shepherd & Stockley, 1987; Towler & Shepherd, 1992). The components of this

Diet in pregnant compared to non-pregnant women 337
I
(1) Behaviwral intention is used as a measure of behaviour (2) Attitude or personal f e e l i i (3) Social pressure from other persons (4) Predictors of attitude component (estimated attitude) (5) P r e d i i of wbjecth norm component (estimated subjwtive norm)
Nore: Behavioural intention= pIxA-+ Bpx SN
Relative weightings (fi) derived from multiple regression analysis
Aftiiude (A+Xbixei SuQecfh m = W B j xMq
Fig. 1. Relationship between attitudinal components.
model are presented in Figure 1. Within this model, beliefs and attitudes are as- sessed towards a behaviour, e.g. eating certain foods. The best predictor of this behaviour is assumed to be a conscious intention to perform the behaviour. Behav- ioural intention is predicted by two theor- etical constructs, the individual’s attitude (direct attitude) towards the behaviour and
the subjective norm (directive subjective norm). Attitudes towards the behaviour may be seen as an evaluation of how individuals perceive the behaviour or the personal feelings they have towards that behaviour. Subjective norm is the per- ceived social pressure (from other impor- tant people) to perform the particular be- haviour. In turn, these direct components

338 A. S. Anderson, D. Campbell and A. Shepherd
are predicted by estimated components. Direct attitudes are predicted by an estimated attitudes component which assesses beliefs about the outcomes of the behaviour (behaviour beliefs) and modi- fied by the individual’s evaluation of the expected outcomes (outcome evaluation). Estimated subjective norm is predicted from a set of normative beliefs about whether individuals feel that specific other people think that they should perform the behaviour and are modified by the motiva- tion to comply with the wishes of these people (Figure 1).
The aim of this study was to establish whether pregnancy acts as a stimulus to dietary change, eating habits and nutrient intake, and if it does whether alterations are attributable to a different degree of knowledge or to differences in attitude.
Methods
One hundred consecutive pregnant women who attended antenatal booking clinics at Aberdeen Maternity Hospital (AMH) were invited to take part in a survey about ‘eating during pregnancy’ by completing nutrition knowledge and attitude questionnaires and 4-day diet records. Socio-demographic characteristics of the women were obtained from the Aberdeen Maternity and Neo-natal Data- bank (Samphier & Thompson, 1981).
These pregnant women were matched for age and area of residence (using postal code) with non-pregnant women identified from the age/sex register from a large general practice. Subjects were sent a letter describing the study and advising them that they would be contacted in the forth- coming 2 weeks. A refusal slip and pre- paid envelope were also enclosed. Women were contacted by telephone or visited at home and an appointment made to com- plete the questionnaires. Women who could not be contacted and women who refused to participate were replaced by other women with similar age and residen- tial criteria. Personal information was col- lected by a brief questionnaire.
For all subjects nutrition knowledge was assessed by a questionnaire designed spe- cifically for this study but based on another questionnaire tested in the local popula- tion (Anderson et al., 1988). It contained a total of 19 questions. Three questions as- sessed nutrition terms. These items were defined as those which covered only nutri- tion terms with no reference given to any specific foods or the role of these nutrients in the diet. Five questions assessed the theoretical principles of good nutrition. These items were defined as those which examined the relationship between nutri- ents and health. Three of these theoretical questions asked about general health and two were based on specific health dis- orders. Eleven questions assessed the prac- tical applications of nutrition principles. These were defined as those items relating to specific foods. The final questionnaire was in a multiple-choice format designed for self-completion. All respondents were taken to a private area to answer the questionnaire to avoid discussing possible answers with others present.
For both groups of women, attitudes to healthier eating were assessed by a ques- tionnaire designed for the current study. This was presented after the knowledge questionnaire because it contained a defin- ition of healthier eating which might have influenced the answers to the knowledge questionnaire. The questions were pre- ceded by an introductory page containing the definition of healthier eating as ‘health- ier eating means increasing your intake of fibre-rich foods such as bread, potatoes, cereals and fruit and decreasing your in- take of foods high in fat such as dairy products, meat products and fried foods’ and instructions for answering the ques- tions (with an example).
The questionnaire was designed accord- ing to the Fishbein & Ajzen (1975) Expec- tancy Value Model. Following a number of pilot tests, the attitudes questionnaire comprised 27 questions, related to health- ier eating. These questions were in the form of statements with seven category Likert response scales (Likert, 1932). labelled only at extreme ends. For all the responses the centre of the response scales

Diet in pregnant compared to non-pregnant women 339
was taken as zero, and hence responses were scored -3 to +3, other than the motivation to comply questions which were scored 0-6 (Ajzen & Fishbein, 1980). These questions covered the five con- structs of the Expectancy Value Model and to measure these, questions (and re- sponses) had the following design. 1 Behavioural intention. Respondents were asked to rate their agreement/disa- greement with the statement ‘I intend to try healthier eating’. 2 Direct attitude. Four questions which described ‘healthier eating’ as beneficial, good, pleasant and desirable were pre- sented. These were rated using response scales labelled ‘strongly agree’ to ‘strongly disagree’ at extreme ends. 3 Direct subjective norm. This was assessed by two questions. They were: ‘Most people who are important to me think “I should try” or “be concerned about” healthier eating’. The response scales of these questions were labelled at extreme ends ‘strongly agree’ or ‘strongly disagree’. 4 Estimated attitude. This was assessed by constructing six pairs (one each for the behaviour belief and outcome evaluation) of statements on the relationship between ‘healthier eating’ and (i) increased food preparation, (ii) eating expensive food, (iii) poor (unappealing) taste, (iv) eating differently from the rest of the family, (v) maintaining health, and (vi) reducing the risks of coronary heart disease. The belief statements were assessed on the scale ‘strongly agree’ to ‘strongly disagree’ and corresponding evaluation state- ments on the scale ‘very desirable’ to ‘very undesirable’. 5 Estimated subjective norm. This was assessed by four pairs of statements (one each for normative belief and motivation to comply) which queried whether the respondent thought her doctor/partner/ family/friends would like her to try healthier eating and the respondent’s moti- vation to comply with the wishes of these referents. The statements on normative beliefs were assessed on the scale ‘strongly disagree’ to ‘strongly agree’ and corre- sponding motivation to comply items on
the scale of ‘wishing to do’ or ‘not to do’ what referents thought they ought to.
Salient belief items (behaviour beliefs and normative beliefs) were identified from group discussion work.
After completing the knowledge and attitude questionnaires all subjects were invited to record food intake by a diet record method (Edington et a]., 1989). Using this technique, food intake was recorded in a diet record book for 2 weekdays and 2 weekend days. Portions were described using household measures and with reference to food photographs. Cross-check questions designed to gain qualitative and quantitative data about 15 main food groups were also included. The diet record books were returned by post and assessed immediately for legibility and missing details. Women were contacted by telephone or letter if queries arose. Diet books were then coded with unit and subject number, day, date, food codes and meal times.
The weight of food portions used in the diet record books were derived, where possible, from the weighed intake data in the same population (Anderson, 1991), known weights of the portions portrayed in the photographs, weighing duplicate portions described as household measures and from published figures (Crawley, 1988).
The data were analysed at the AFRC Institute of Food Research, Norwich. The nutritional database consisted of McCance & Widdowson’s ‘7he Composition of Foods’ (Paul & Southgate, 1978). and supplemen- tary tables (Wiles et al., 1980; Tan et al., 1985). Local food data (e.g. butteries, scotch broth) were calculated from recipes, or provided by food manufacturers.
The mean daily nutrient intake for the diary data was calculated using the follow- ing equation: [(mean weekday intake x 5) +(weekend day 1 intake)+(weekend day 2 intake)]/7.
Statistical methods The level of significance used in the cur- rent study was 0.05. T-tests were used to

340
Table 1. Response rate for the study of diet in pregnant women compared to non-pregnant women
A. S. Anderson, D. Campbell and R. Shepherd
Early pregnancy Non-pregnant
n % n %
Numbers identified for study Number failing to participate
Reasons for failure Refuse Subjects unavailable No contact Moved from area No longer suitable Language problems
Numbers returning questionnaires Numbers returning diet diaries
100 5
100 5
244 149
100 61
0 4 0 0 0 1
95. 50
4
1
95 50
50 40 31 19 9 0
94 60
20 16 13 8 4
39 25
Two women failed to complete the knowledge questionnaire; one woman failed to complete the attitude questionnaire.
test the difference in means between samples. Pearson correlation coefficients were used to investigate the degree of association between two variables. Step- wise multiple regression was used to examine the joint relationship between a number of independent variables. The differences between the independent correlation coefficients were tested by con- version to Fishers’ Z statistics as described by Downie & Heath (1983).
Results
Subjects The response rate for women invited to take part in this study is presented in Table 1. There was a particularly poor response from non-pregnant women because of a postal strike which delayed invitations being delivered until the main holiday period and because many GP records were out of date. The characteristics of subjects participating in the study are presented in Table 2.
The characteristics of the two groups, the early pregnancy group (EPG) and the non-pregnant group (NPG), were similar,
except for marital status, parity and smok- ing habits. The differences in marital status and parity were anticipated because selecting women of child-bearing age who were not pregnant meant increasing the likelihood of women not living with partners and nulliparous women.
In the EPG there were similar charac- teristics between women who completed the questionnaire and the diaries (com- pared to women who completed only the questionnaire) for marital status, age, social class and parity although signifi- cantly more non-smokers completed diet diaries. In the NPG, there were significant differences between the women who com- pleted both questionnaires and diaries compared to those who completed ques- tionnaires only in parity and smoking status (~~ ‘7 .4 , d.f.=2, P<0.05; ~~‘10.7, d.f.=Z, P<O.O1), thus a higher proportion of women who had not had babies and a higher proportion of non-smokers com- pleted diet diaries. Thus the magnitude of differences detected between the EPG and NPG who completed diet diaries may be less than that found in a non-pregnant group which includes nulliparous women and smokers and deserves further con- sideration.

Diet in pregnant compared to non-pregnant women 341
TabJe 2. Diet in pregnant compared to non-pregnant women: characteristics of subjects who completed questionnaires
Early pregnancy. Non-pregnantt group group
11-93 (%) n--94 (W,)
Marital status Single Married Divorced Separated Co-habiting Info. missing
Age 15-20 21-30 31 -t Info. missing
Social class I-IIInm I I In m - V Info. missing
Parity 0 1+ Info. missing
Smoking status Non-smoker Smoker Info. missing
11 (12) 9 (10)
15 (16) 20 (21)
0 (01 0 (01
67 (72) 65 (69)
26 (28) 22 (231 41 (44) 30 (331 26 (28) 41 (44)
45 (48) 42 (45) 34 (37) 48 (51! 14 (15) 4 (4)
x*-o.68 d.f.-3 NS
X2=4.6 d.f.-2
NS
X2-6.2 d.f.=2 NS
43 (46) 32 (35) 18 (19)
57 (61) P==13.04 34 (363 d.f.==2 3 (31 P(O.01
Info. missing: (a) Eleven women failed to deliver babies at AMH (the majority having moved from
the area or miscarried) and no details were available from these women on marital status, social class, parity or smoking.
of partner/husband) because they claimed to have no partner (n-lo), or their partner/husband was unemployed, a full-time student or serving in HM forces and therefore not classified.
(b) In addition, 15 women had missing information for social cla,ss (based on occupation
(c) Details of parity were unavailable or uncertain for three cases. (d) Seven women declined to give information on smoking habits. t Info. missing: (a) Two women failed to provide info. on marital status. (b) Forty-one women had missing information for social class (based on occupation of
partner) because they claimed to have no partner (n-39) or their partner/husband was unemployed, a full-time student or serving in HM forcer; and therefore not classified.
(c) Details of parity were not given by four women. (d) Three women declined to give information on smoking habits.
342
Table 3. Nutrition knowledge component scores: pregnant and non-pregnant women
A. S. Anderson, D. Campbell and A. Shepherd
,.
Pregnant Non-pregnant women women
Maximum n Mean k s.d. score 1-test n Mean * s.d.
Nutrition terms 95 1.5 1 .o 94 1.4 1 .o 3 0.70 Theoretical
principles 93. 2.8 1.2 94 2.7 1.3 5 0.61 Practical
Total score 93’ 10.2 2.8 94 10.0 3.5 19 0.37 applications 95 5.9 1.8 94 5.9 1.3 11 0.00
~~~
Two women failed to complete these sections.
Table 4. Mean smres for the components of the attitude model
Pregnant women Non-pregnant women (n-95) ( n = W
Range of Component Mean f s.d. Mean f s.d. possible scores t-test
Intention 1.7 1.4 1.8 1.2 -3-3 -0.32 Direct
Direct
Estimated
Estimated
attitudes 7.3 4.w 7.8 3.3 -12-12 -0.94
sub. norm. 1.2 3.1 0.5 3.3 - 6 6 1.53
attitude 18.2 13.1 15.5 12.1 -18-18 1.49
sub. norm. 14.5 17.9 8.6 16.9 -36-36 2.28.
P<0.05. t n=94, one subject failed to answer all questions.
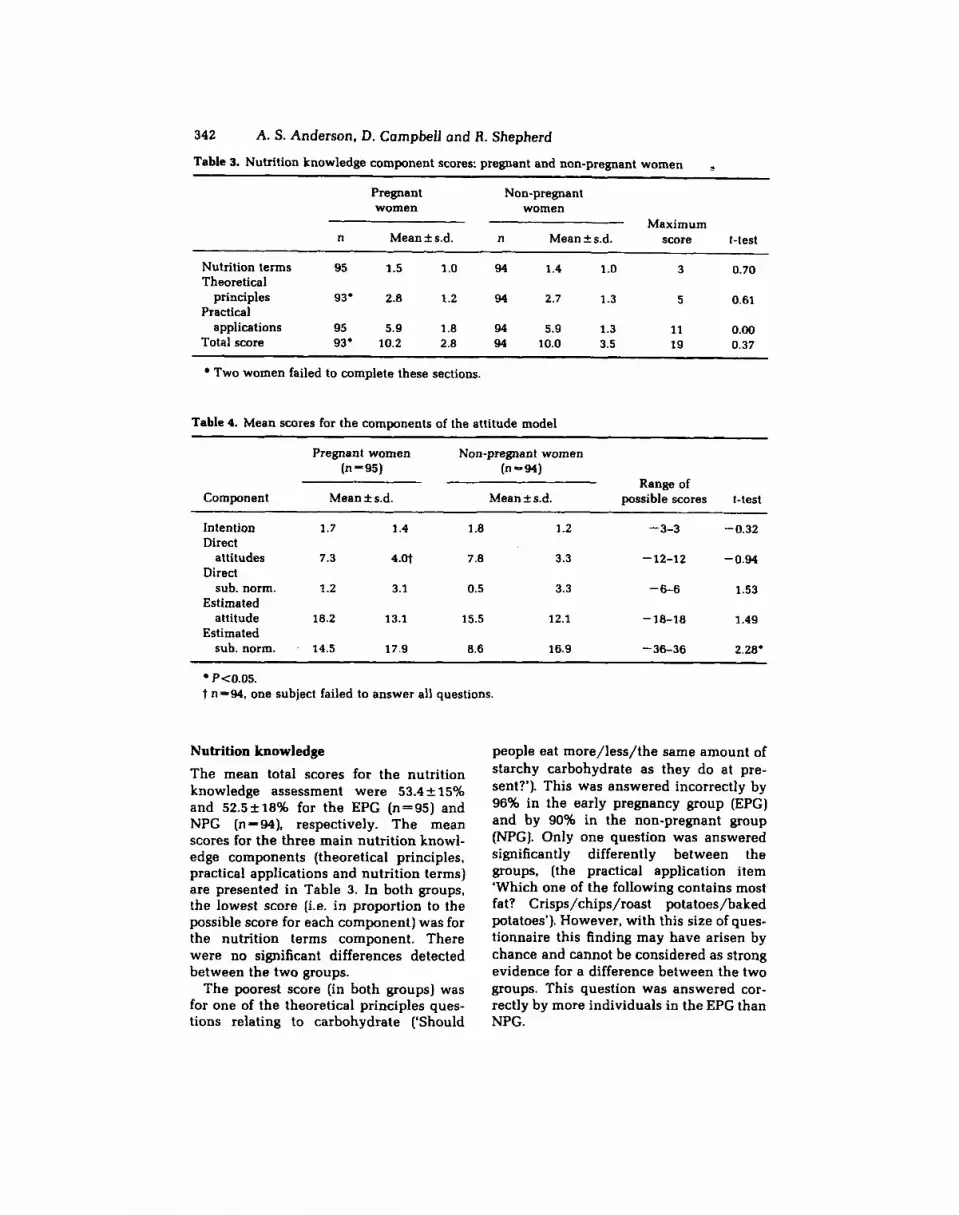
Nutrition knowledge The mean total scores for the nutrition knowledge assessment were 53.4 f 15% and 52.5*18% for the EPG (11-95) and NPG (n -a ) , respectively. The mean scores for the three main nutrition knowl- edge components (theoretical principles, practical applications and nutrition terms) are presented in Table 3. In both groups, the lowest score (i.e. in proportion to the possible score for each component) was for the nutrition terms component. There were no significant differences detected between the two groups.
The poorest score (in both groups) was for one of the theoretical principles ques- tions relating to carbohydrate (‘Should
people eat more/less/the same amount of starchy carbohydrate as they do at pre- sent?’). This was answered incorrectly by 96% in the early pregnancy group (EPG) and by 90% in the non-pregnant group (NPG). Only one question was answered significantly differently between the groups, (the practical application item ‘Which one of the following contains most fat? Crisps/chips/roast potatoes/baked potatoes’). However, with this size of ques- tionnaire this finding may have arisen by chance and cannot be considered as strong evidence for a difference between the two groups. This question was answered cor- rectly by more individuals in the EPG than NPG.

Diet in pregnant compared to non-pregnant women 343
Attitudinal factors In both groups of women there was a positive response to the behavioural inten- tion question on intention to try healthier eating (Table 4). High scores were also attained by both groups for the estimated attitudes and estimated subjective norm components. The EPG showed a signifi- cantly higher score in the estimated sub- jective norm component compared to the NPG. There were no other significant dif- ferences between these groups in these two components.
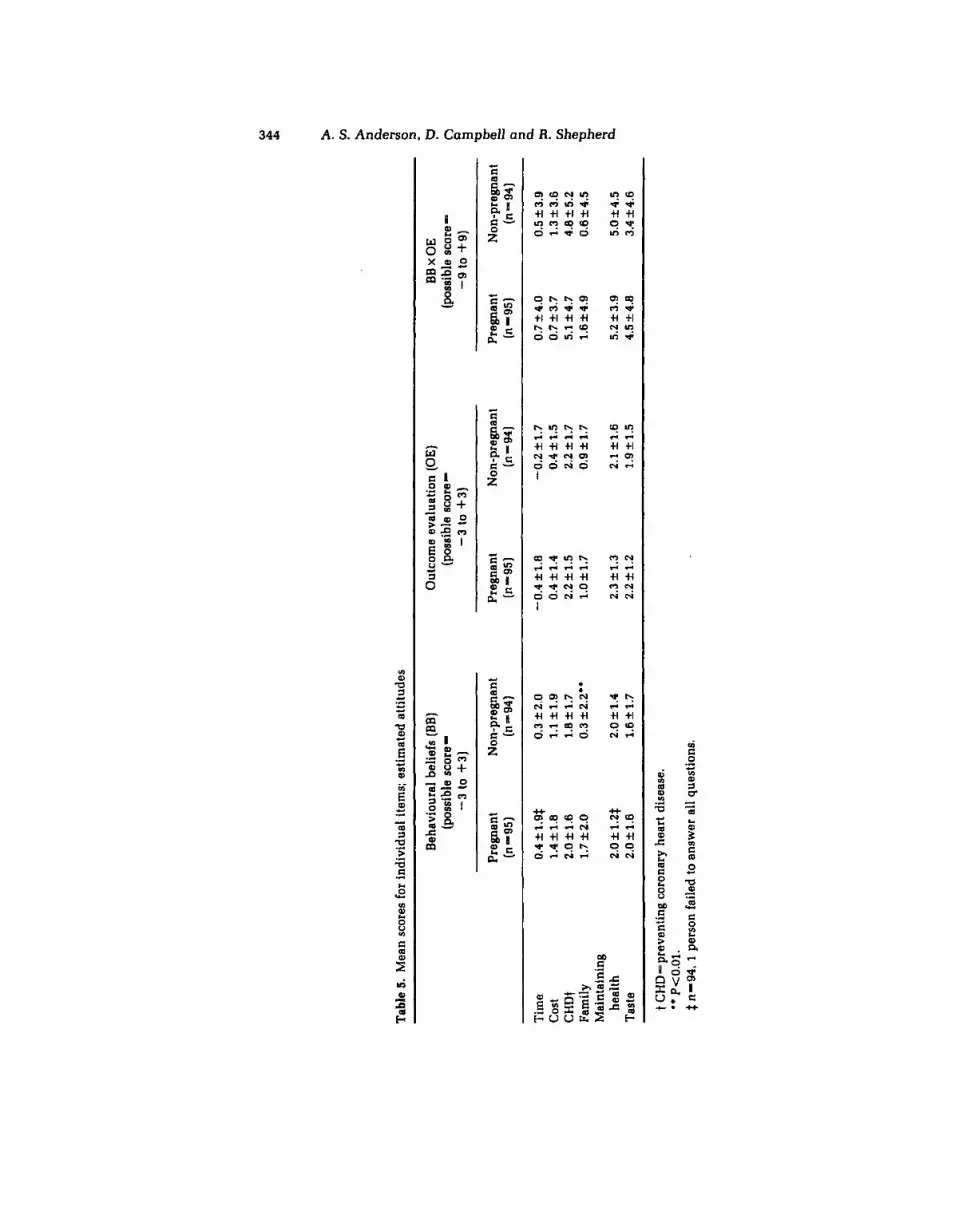
The results for individual questions in the estimated attitude components are presented in Table 5. In both groups the highest scores were recorded for the items on health maintenance and preven- tion of coronary heart disease. The lowest scores were for the outcome evaluation item on time, which suggested that women (both pregnant and non-pregnant) thought it desirable to spend more time preparing food. Compared to the NPG, significantly higher scores were found in the EPG for the behaviour belief item on family, which suggested that women in early pregnancy thought it less likely that ‘healthier eating’ would mean eating differently from the rest of their family.
Results for individual questions in the estimated subjective norm component are presented in Table 6. In both groups the highest score was for the items relating to doctors. The lowest score was for the items on friends which was particularly low in the normative belief component for the NPG suggesting that these women feel their friends are not concerned about healthier eating choices of the respondent. Compared to the NPG, there was a signifi- cantly higher score for the estimated sub- jective norm item on doctors (both in the normative beliefs and motivation to com- ply components) in the early pregnancy group, which was accompanied by a higher score for the normative beliefs item on family.
Using stepwise multiple regression analysis, 44.9 and 16.8% of variance in behavioural intention could be predicted
by attitude and subjective norm compo- nents in the early pregnancy and non- pregnant groups, respectively. In both groups the strongest relationship with behavioural intention was with attitude and intention (Figs 2 and 3). The relation- ship between subjective norm and inten- tion was considerably weaker and failed to reach significance in non-pregnant women. In both groups there was a significant correlation between estimated and direct components.
The correlations between attitude and intention for early pregnant and non- pregnant groups were significantly differ- ent (r-0.66 (EPG), 0.39 (NPG), 2-2.65, P<O.O1) as were the correlations between the two groups for subjective norm and intention (r=-0.35 (EPG), 0.04 (NPG); 2-2.21, Pt0.05). These findings indicate a stronger relationship between intention and both attitude and subjective norm in pregnant women compared to non-preg- nant women. These results also suggest that the items identified in the original pilot tests may not be so relevant for non- pregnant women. Correlations between individual beliefs and behavioural inten- tion were calculated and compared be- tween the pregnant and non-pregnant groups. There were significant differences between the correlations of the pregnant and non-pregnant groups for the behav- iour belief items on coronary heart dis- ease (0.38 and 0.00 for pregnant and non- pregnant women, respectively, n ==a, P<0.05) and maintaining health (0.43 and 0.00 for pregnant and non-pregnant women, respectively, n -94, P<0.05) in- dicating a stronger relationship of these beliefs with intention to change to a healthier diet in pregnant women. The correlation between maintaining health and intention was also significantly higher (0.45 and 0.12 for pregnant and non-pregnant women, respectively, n - 94, P(0.05) in the [behaviour beliefx outcome evaluation items] component, which also stresses the importance of this item in the pregnant group of women.
Tab
le 5
. M
ean
scor
es f
or in
divi
dual
item
s; e
stim
ated
att
itud
es
~ ~~
~
Beh
avio
ural
bel
iefs
(BB
) O
utco
me
eval
uatio
n (O
E)
BB x
OE
P 2 9 %
Preg
nant
N
on-p
regn
ant
Preg
nant
N
on-p
regn
ant
Preg
nant
N
on-p
regn
ant
- (1
1-95
) (1
1-94
) (n-951
(n--941
(11-
95)
(11-
94)
P
(pos
sibl
e sc
ore=
(p
ossi
ble
scor
e=
(pos
sibl
e sc
ore-
-3
to
+3
) -3
to
+3)
-9
to
$9)
ii
?Ir 1.
3 f 3
.6
VJ z
Tim
e 0.
4 f 1
.9$
0.3 f 2
.0
-0.4
f1.0
-0
.2
f1.7
0.
7 f4
.0
0.5 f 3
.9
cost
1.
4 f 1
.8
1.1
f1.9
0.
4 f 1.
4 0.
4 f 1
.5
0.7 f
3.7
CH
Dt
2.0 f 1
.6
1.8 f 1
.7
2.2 f 1.5
2.2 f 1.
7 5.1 f 4
.7
4.8 f 5.
2 Fa
mily
1.
7 f2.0
0.3 f2.2**
1.0 f
1.7
0.9
f1.7
1.
6f4.
9 0.
6 f 4.
5 M
aint
aini
ng
heal
th
2.0 f 1.2$
2.0 f 1
.4
2.3
f1.3
2.1
f1.6
5.
2 f 3
.9
5.0 f 4.
5 T
aste
2.
0f1.
6 1.
6 f 1
.7
2.2 f 1.2
1.9f
1.5
4.5 k 4
.0
3.4 k 4.
6
Q 3 2.
~~
~
t CH
D-p
reve
ntin
g co
rona
ry h
eart
dis
ease
. **
P<O
.Ol.
$ 11
-94,
1
pers
on f
aile
d to
ans
wer
all
ques
tion
s.

g
-3
to +3)
0 to
4-6)
(pos
sibl
e sc
ore
-18
to +
la)
3
Tab
le 6
. M
ean
scor
es fo
r in
divi
dual
item
s; e
stim
ated
sub
ject
ive
norm
I-. 5'
%
Nor
mat
ive
belie
fs (
NB
) M
otiv
atio
n to
com
ply
(MC
) (p
ossi
ble
scor
e - (p
ossi
ble
scor
e-
NB x
MC
Preg
nant
N
on-p
regn
ant
(n - 95
) (n
=94)
Pr
egna
nt
Non
-pre
gnan
t Pr
egna
nt
Non
-pre
gnan
t 2
(11-
95)
(n=
94)
(n -95)
(n-9
4)
n 3
Part
ner
0.9
2 0.2
0.6 f 1.7
2.4 f 1.7
2.1 * 1.
9 2.9f 5.2
1.92 5.7
7J
Frie
nds
0.1 k 1
.7
-0.2 f 1.7
1.8 f
O.2
1.8 *1.8
1.0f4.6
0.8 f 4.
1 a
Fam
ily
0.7f1.6
0.2 + 1
.7.
3.0 f 1.7
2.8 f 1
.9
3.4 It 5.6
1.8 f 6.0
i; $ D
octo
r 1.5f1.6
1.0 f 1
.7'
4.7 f 1
.4
3.9+1.7***
7.3 k
8.6
4.5 f 7.6.
' P(0.05,
** P
<O.O
l, **
* P<O
.OO
l.

346 A. S. Anderson, D. Campbell and R. Shepherd
b,=0.45
r-0.04 R-0.41
r=O.3Q P 4.001 +I P N S 8-0.14
Behaviour beliefs Normative beliefs X X ubieclive
Eslh.ted amtude
ryHm
Outcome evaluation Motivation to comply
(1) Behaviwral intention is used as a measure of behaviour (2) A t t i i or personal feelings (3) Social pressure from other persons (4) Predictors of attitude component (estimated attitude) (5) Predictors of subjective norm component (estimated subjective norm)
Note: Behavioural intention=fhx Aa+&x SN
Relative weghtings (f3) derived from multiple regression analysis
Atlifude (&)=Xbixei Subjective nom= XNBj x Mcj
Fig. 2. Relationship between attitudinal components: pregnant women (n-95).
Dietary intake Daily nutrient intake ( 2 s.d.) of both groups of women are presented in Table 7. The EPG consumed significantly higher amounts of zinc and vitamin C and lower amounts of alcohol compared to the NPG.
The nutrient density of protein (35.9 f 6.4 g/lOOO kcal, 33.4 f 6.5 g/lOOO kcal. P<0.05), vitamin C (39.6f30 mg/1000 kcal, 28.6 k 22 mg/1000 kcal.
P<0.05) and sodium (1485 f 305 mg/1000 kcal, 1338 2275 mg/1000 kcal, P<o.O1) were significantly greater and alcohol (0.4 f 1.2 mg/1000 kcal, 3.5 f 5.0 mg/1000 kcal, P<O.o01) was significantly lower in the pregnant and non-pregnant groups, respectively. The energy compositions for both groups are presented in Table 8 and compared with guidelines for health (NACNE, 1983) and COMA (1991) recom-

Diet in pregnant compared to non-preiynant women
(I)
347
Behaviwral intention
1 r = 0.M P4.001 p d . 8 3
P4.001 (4) I_
r = 0.35 P4.001 B*=O.Oe
R-0.67]
(W
(ei)
Behaviwr beliefs X
Eslbmtd .rmhde
Outcome evaluation 1
(1) Behavioural intention is used as a measure of behaviour (2) Attitude or personal feelings (3) Social pressure from other persons (4) predictors of attitude component (estimated attitude) (5) Predictors of subjective norm component (estimated subjec-ve norm)
Note: Behavioural intention= Btx A a+ B.x SN
Relative weightings (B) d e M from multiple regression analysis
Attihrde (&)=Zbi x ei Sllb@tknOfTilnonn=~BjXMCj
Fig. 3. Relationship between attitudinal components: non-pregnant women (n-95).
mendations. The percentage of energy derived from alcohol was significantly lower in the EPG and both groups had intakes well below the maximum levels discussed by NACNE (1983) for non-preg- nant women. In both groups, the percen- tage of energy derived from fat, carbo- hydrate and protein failed to reach levels recommended for maintenance of health and prevention of disease.
The main sources of fat, carbohydrate and dietary fibre in both groups were
examined. There was a trend for women in the EPG to derive more fat from milk. The higher quantities of fat derived from milk can be accounted for by a greater consump- tion of total milk (222 and 162 g), higher consumption of whole milk (130 and 73 g) and lower consumption of skimmed milk (73 and 130 g) in the group of EPG and NPG, respectively. The group of non-preg- nant women derived a higher percentage of fat from chocolate, confirmed by the weight of chocolate consumed in both

348
Table 7. Mean daily nutrient intake in early pregnancy and non-pregnant groups
A. S. Anderson, D. Campbell and A. Shepherd
Early
BroUP group (n-50) (n-60)
pregnant Non-pregnant
Nutrient Unit Mean s.d. Mean s.d.
Energy kcals 2000 427 2020 434
Protein g 71.3 19.2 66 .6 ' 16.3 Fat g 88.3 20.0 90.2 24.7 Total carbohydrate 8 244.2 64.9 238.2 62.3
Sugar 8 94.6 42.3 91.8 42.3 Dietary fibre 18.4 7 .8 16.2 5 .8
Alcohol f3 0 .9 2.5 6 . 9 10.0".
Mineral intake Sodium Potassium Calcium Magnesium Iron Zinc
Vitamin intake Thiamin Riboflavin Nicotinic acid Tryptophan Vitamin C Vitamin B, Vitamin B,2 Free folic acid Total folic acid Pantothenic acid Biotin Retinol Carotene Vitamin D Vitamin E
mg 2910 616 2680 758 mg 2970 737 2880 681 mg 860 295 841 287 mg 271 87 270 82 mg 11.7 4 .8 11.6 5.1 mg 9.2 3 .6 8.2 2.5.
1 .2 1 .7
16.8 14.6 81.3
1 .3 4
70 153
3.7 19.3
729 2295
2 . 0 4 . 9
0 .4 0 .7 5.1 4 .2
64.9 0 . 4 5 .4
34.6 71.9 1 .3 9 .6
875 2080
1.0 1 . 8
1.1 1 .5
15.7 13.5 57.1
1.1 3.2
58 136
3 .4 17.2
567 1925
2.2 4 . 6
0 .3 0 . 5 5 . 1 3 . 4
45.1. 0 . 3 3 .0
28.3 50.5 1 . 7 7 .9
642 1953
1 . 2 1 . 6
PtO.05. *** P<O.OOl
Table 8. Energy composition in pregnant and non-pregnant women compared to nutritional guidelines for long-term health (NACNE. 1983) and dietary reference values (DHSS; COMA, 1991)
Pregnant Non-pregnant group group NACNE guidelines
(n - 50) (n = 60) Energy composition mean * s.d. mean f s.d. (1 It (2 H COMA
Protein energy (%) 14.3 2 3 13.2+3* 11 11 15 Fat energy (%] 39.7 k 5 40.2 k 5 34 30 35 CHO energy (%) 45.8 & 5 44.2 & 6 50 55 50 Alcohol energy (%) 0.2 & 1 2.4&4**' 5 4 NA
P<O.O5, *** P<0.001. t Short-term goal for the 1980s. $. Long-term goal.

Diet in pregnant cornpored to non-pregnant women 349
groups (16.5 and 18.6 g per day per con- sumer in the EPG and NPG, respectively). Similarly the amount of fat derived from cakes and pastries appears to be slightly higher in the NPG. Further analysis shows that this is due to the total weight of these items consumed rather than selection of a small amount of very high fat pastries (16.9 and 18.3 gper day per consumer in the EPG and NPG, respectively).
The sources of carbohydrate were simi- lar in both groups. There appeared to be a trend for women in the EPG to consume more fruit and potatoes although only fruit consumption seems to be notably higher (fruit: 108 and 63 g per day per consumer and 80 and 77 g of potatoes per day per consumer in the EPG and NPG, respec- tively). The sources of dietary fibre suggest that women in the early pregnancy group derive more of their dietary fibre intake from fruit which is in agreement with the weights of fruit described above.
Discussion
Response rate Overall, the response rate of pregnant women for this study illustrates the im- pression that many women are happy to participate in detailed dietary surveys of this nature. The refusal rate by non-preg- nant women seems high by comparison to the response by pregnant women. The final number of non-pregnant women who par- ticipated does however make the compari- son between the two groups appropriate. Reasons for failing to participate by non- pregnant women have been indicated but it should be noted that the method for recruiting subjects which allowed non- pregnant women to refuse more easily (e.g. a written refusal rather than a face to face refusal) may also have contributed. The response also illustrates difficulties in re- cruiting subjects who are not currently dependent on health services (i.e. not readily available and not necessarily moti- vated to helping health-service personnel). A letter of introduction from the subject’s
general practitioner may have improved response rates, although it is clear that an up to date register is crucial to this type of survey work.
The non-pregnant women returned most diaries (64% compared to 53% in the early pregnancy group). It seems likely that women who were not going to participate in diet surveys would have refused to participate and been selected out at an earlier stage and thus it is tempting to speculate that these people may have had poorer diets. The pregnant and non-preg- nant groups were similar in age although other characteristics varied considerably. The difference in smoking habit between the two groups was unexpected. This find- ing may have been accounted for by a greater number of smokers declining to participate in health-related studies. The higher proportion of smokers in the EPG may have diminished some of the true differences between the groups as smoking is consistently associated with a lower intake of all nutrients in pregnancy (Haste et a]., 1990) and in non-pregnant women and men (Herbert et a]., 1990).
Nutritional knowledge The mean total scores for both groups suggest that most of the topics covered in the nutrition knowledge questionnaire were familar to the respondents. The fail- ure of most of the respondents to provide the correct answer about ‘starchy carbo- hydrates’ confirms the views of Bradley 81 Theobald (1988) that the public remain unaware of the NACNE guideline to in- crease starch intake. The relatively low score for the nutrition terms component is clearly an important issue for nutrition labelling.
The lack of difference in nutrition knowledge between the two groups sug- gests that women in early pregnancy have not sought or been exposed to nutrition information because of their pregnancy. Alternatively, it might be argued that women had received nutrition advice but that it made no impact on their nutrition knowledge.

350 A. S. Anderson, D. Campbell and A. Shepherd
Attitudinal factors The definition of healthier eating offered advantages in that it included both food and nutrients in its description and could be easily understood by both the subject and the researcher. The major disadvan- tage of the definition was that many foods (i.e. those not specified) may not have been considered by the subject answering the question. The appropriateness of relating intake of specific nutrients with attitudinal measures may have been limited for nutri- ents other than fat or fibre (or carbohydrate by implication of bread, potatoes and cereals). Overall, in each question, how- ever, respondents were asked about ‘healthier eating’ as a single concept or single-action health behaviour in line with the theoretical base of this attitudinal model.
The results of the behavioural intention question indicate that both pregnant and non-pregnant women are equally likely to want to change to healthier eating. The main beliefs of healthier eating reducing the risks of heart disease and helping to maintain health also seem to be widely held by both groups of women. The nega- tive responses for the evaluation item on time suggest preparation time is not a particularly relevant concern to either group. This may relate to the life-styles of these women where sufficient time for cooking is generally available or simply that other issues are of more importance.
In the estimated subjective norm compo- nent there are interesting differences be- tween the EPG and NPG. The overall difference in scores between the two groups for this component strongly sug- gests that pregnant women are more sensi- tive to the social pressure from referents named in the questionnaire. This may relate to a general feeling of vulnerability which is said to be particularly acute in the presence of medical personnel. The higher scores in the NPG for the items on doctors strongly support the evidence (Bailey, 1988) that pregnant women believe doctors to be important referents in relation to healthy eating advice.
The response to the items on doctors
may have been anticipated in a health-care environment. The high score for the moti- vation to comply item also suggests that an excellent opportunity is provided in doc- tor-patient meetings to promote healthier eating. Pregnant women also seem more likely to comply with other family mem- bers than non-pregnant women which may evolve from the existence of and increased interest from kin to the addition of a new baby.
Behavioural intention is more closely linked with attitude in the EPG than in the NPG. This suggests that other factors, which have not been identified, play a much stronger predictive role in the NPG, e.g. habit (Towler & Shepherd, 1992).
Although a causal role cannot be as- sumed between the beliefs and evaluation items on maintaining health and intention to try healthier eating, the strength of the association between these variables strongly suggests they may play a role in food choice. The concept that Scottish women are likely to perceive the role of diet in this limited, rather narrow role is in agreement with the findings of Stewart et al. (1988) who described Scottish women as exhibiting a basic pragmatism in relation to diet and pregnancy. The difference between the groups for the associations between intention and the belief items on heart disease and maintaining health suggests that these beliefs are more likely to encourage pregnant women to try healthier eating. This suggests that preg- nant women are more likely to change their diets because of behaviour beliefs related to health and it is these beliefs that account for the stronger association between intention and attitudes.
Dietary intake
The reasons for the differences between the two groups are unclear although there are a number of possible explanations. Firstly, women may have made a con- scious effort to improve their food intake in line with health advice. For example, avoiding alcohol (or reducing the amount consumed), eating more fruit, increasing intakes of milk, and caution over con-

Diet in pregnant compared to non-pregnant women 351
sumption of chocolate, cakes and pastries are good examples of basic dietary advice which are widely promoted (HEA, 1988). However, these differences in food intake may in fact be a response to physical symptoms such as thirst, changes in taste, food cravings and aversions, nausea and vomiting or tiredness (which might pro- voke a change in evening activities such as going to a ‘pub’ or ‘disco’ where alcohol is usually consumed) (Taggart, 1961; MacIn- tyre, 1983; Tierson et a]., 1985; Stewart et al.. 1988). Another reason for dietary change might be alterations in social cir- cumstances which arise during pregnancy and result in new food patterns, e.g. work- ing less outside the home resulting in more time spent in the house eating snacks (although these may be more relevant in later pregnancy). It is also possible that a subconscious change in food-selection may result from changed daily priorities (e.g. less time is spent thinking about food for supper and more time spent on maternity considerations). There are also anecdotal reports of social pressure in NE Scotland for women not to consume alcohol during pregnancy.
Most of the differences detected in nutri- ent intake between pregnant and non- pregnant women are consistent with diet- etic advice for pregnancy (protein density, vitamin C and alcohol) which has been promoted in written and verbal forms by health professionals over the last 2 decades (Scottish Health Education Group, 1980). Current dietary principles promoted for good health (increase fibre and carbohy- drate, decrease fat) are evidently perceived as less important than the traditional prin- ciples of diet for pregnancy. The margi- nally higher intake of sodium among preg- nant women is not in line with current health advice but may relate to changes in taste (Tierson et ol., 1985) widely experi- enced in early pregnancy. Taste changes may also account for the increased con- sumption of fruit although Stewart et al. (1988) suggest that Scottish women make a conscious effort to increase their vitamin C intake.
Another possible influence on dietary changes during pregnancy is historicity.
Historicity refers to behaviours which are accepted during the socialisation process and become part of ‘objective reality’. Baric & MacArthur (1978) observed that norms relating to alcohol intake during pregnancy exhibited a high level of historicity with 74% of women reporting that they ‘just knew’ what they should do about alcohol intake during pregnancy. Baric & Mac- Arthur (1978) concluded that ‘the norm concerning alcohol consumption during pregnancy derives its coercive power al- most solely from its attribute of historicity’. However, Stewart et ol. (1988) suggest that some food selections during pregnancy are influenced by historicity and some by health educators, but it is impossible to separate out these influences.
In the present study, the similarity in nutrition knowledge between the two groups suggests that pregnant women are not motivated to alter their dietary habits by an increased level of knowledge. The present results suggest that pregnant women are likely to be influenced by social pressure from doctors and family members which implies that these important indivi- duals could provide valuable support for dietary change. It is unclear exactly how health advice, physical symptoms and sub- conscious actions dictate dietary intake. It is possible that historicity plays a role in food selection during pregnancy and that this operates through behaviour beliefs and normative beliefs which in turn affect attitude and subjective norm which then influence behavioural intention thus ac- counting for some of the differences in dietary intake observed between women in early pregnancy compared to non-preg- nant women. In conclusion, it is the combi- nation of intentionalities, attitudes and reasoned appraisal of social pressures which plays the causal role in food and diet selection during pregnancy.
Acknowledgments
Our thanks to staff in the University of Aberdeen Department of General Practice, Andy Walker, AFRC Institute of Food Research, Norwich for helping with com-

352
puting and to Mrs Lorna Hudson for typing this manuscript.
A. S. Anderson, D. Campbell and R. Shepherd
Crawley, H. (1988) Food Portion Sizes. Ministry of Agriculture, Fisheries and Food.
Dalton, S.S., Linke, R.A. 8 Simko, M.D. (1986) Worksite food choices: An investigation of intended and actual selections. J. Nutr. Ed. 18.
DOH (1991) Dietary Reference Values for Food Energy and Nutrients for the United Kingdom.
References Report on Health 8 Social Subjects No. 41. London: HMSO.
Ajzen. 1. 8 Fishbein. M. [I9801 Understanding Downie, N.M. &'Heath, R.W. (1983)Bosic Statisti-
This study was funded by a from The Health Promotion Research Trust.
182-187.
Attitudes and Predicting Sociol Behavior. pp. 3-91. Englewood Cliffs, NJ: Prentice-Hall.
Anderson, AS. (1984) Constipation during preg- nancy: Incidence and methods used in its treatment in a group of Cambridgeshire women. Health Visitor 57, 363.
Anderson, A.S. 8 Lean, M.E.J. (1986) Dietary intake in pregnancy. A comparison between 49 Cambridgeshire women and current rec- ommended intake. Hum. Nutr: Appl. Nutr. MA, 40-48.
Anderson, A.S., Umapathy, D., Palumbo. L. & Pearson. D.W.M. (1988) Nutrition knowledge assessed by a structured questionnaire in a group of medical inpatients. J. Hum. Nutr. 6. Diet. 1, 3 9 4 6 .
Anderson, AS. (1991) Food and nutrition during pregnancy: attitudes, knowledge and practice. PhD Thesis, Aberdeen University.
Axelson. M.L.. Federline. T.L. 8 Brinberg, D. (1985) A meta-analysis of food- and nutrition- related research. 1. Nutr. Ed. 17(2), 51-54.
Bailey, S. (1988) The needs of antenatal patients. The Practitioner 22(232). 727-729.
Barker, D.J.P. (Ed.) (1992) The Fetal and Infant Origins of Adult Disease. London: Br. Med. J.
Baric, L. 8 MacArthur, C. (177) Health norms in pregnancy. Br. J. Prev. Soc. Med., 31, 30-38.
Beerbohm-Schwab, E.B. & Axelson, M.L. (1984) Dietary changes of pregnant women: compul- sions and modifications. Ecology of Food b Nutrition 14. 143-153.
Black, A.E.. Wiles, S.J. 8 Paul, A.A. (1986) The nutrient intake of pregnant and lactating mothers of good socio-economic status in Cambridge. Br. J. Nutr. 56, 59-72.
Bonfield, E.H. (1974) Attitude, social influences, personal norm and intention interactions as related to brand purchase behaviour. J. Mar- keting Research XI, 379-389.
Bradley, A. & Theobald, A. (1988) The effects of dietary modification as defined by NACNE on the eating habits of 28 people. J. Hum. Nutr. Diet. 1, 105-114.
Chamberlain, G. (1986) Prepregnancy care. In Prepregnancy Care. eds. Chamberlain, G. & Lumley, J. Chichester: J. Wiley 8 Sons.
" cal Methods. N.Y.: Harper 8 Rew.
Edington, J., Thorogood, M., Geekie, M., Ball, M. 8 Mann. J. (1989) Assessment of nutritional intake using dietary records with estimated weight. J. Hum. Nutr. Diet. 61, 407-414.
Fishbein, M. 8 Ajzen, I. (1975) Belief, Intention and Behaviour: An Introduction to Theory and Research. Reading, MA: Addison-Wesley.
Forsum. E.. Sadurskis, A. 8 Wager, J. (1988) Resting metabolic rate and body composition of healthy Swedish women during pregnancy. Am. J. Clin. Nutr. 47, 942-947. *-
Haste, F.M.. Brooke, O.G., Anderson, H.R.. Bland, J.M., Shaw. A., Griffin, J. 8 Peacock, J.L. (1990) Nutrient intakes during pregnancy: observations on the influence of smoking and social class. Am. J. C h . Nub. 51. 29-36.
HEA (1988) Look After Your Heart-A Simple Guide to Feeling Fitter, Looking Better and Living Longer. London: HEA.
HEC (1984) The Pregnancy Book. London: HEC. Herbert. J.R. 8 Kabout, G.C. (1990) Differences in
dietary intake associated with smoking status. Am. J. Clin. Nutr. 44. 135-143.
Likert. R. (1932) A technique for the measure- ment of attitudes. Arch. Psychol. 1 4 0 , ~
MacIntyre, S. (1983) The management of food in pregnancy. In The Sociology of Food and Eating. ed. A. Murcott. pp. 123. Aldershot, Hants, UK Gower Publishing Co.
National Advisory Committee on Nutrition Edu- cation (1983) Proposals for Nutritional Guide- lines for Health Education in Britain. London: Health Education Council.
Parraga. I.M. (1990) Determinants of food con- sumption. J. Am. Diet. Assoc. 90(5), 661-663.
Paul, A.A. 8 Southgate, D.A.T. (1978) McCance and Widdowson's 'The Composition of Foods'. London: HMSO.
Robarts, P.J. (1988) Preparing for Pregnancy. London: Faber & Faber.
Samphier, M. 8 Thompson, B. (1981) The Aberdeen Maternity and Neonatal Databank. In Prospective Longitudinal Research. eds. Medinck S.A. 8 Baert, A.E. Oxford University Press.
Scottish Health Education Group (1980) The

Diet in pregnant compared to non-pregnant women 353
Book of the Child. Edinburgh: Scottish Health Education Group. p. 13.
Shepherd, R. 8 Stockley, L. (1987) Nutrition knowledge, attitudes and fat consumption. J. Am. Diet. Ass. 87, 615-619.
Snow, L.F. & Johnson. S.M. (1978) Folklore, food. female reproductive cycle. Ecology of Food and Nutrition 7. 4149.
Stewart, J., Wheeler, E. 8 Schofield, C. (1988) Regional differences in British attitudes to diet in pregnancy: Priorities and prag- matism. Ecol. Fd. Nutr. 42. 211-229
Taggart, N. (1961) Food habits in pregnancy. Symposium Proceedings 10, 3540.
Tan, S.J.. Wenlock, R.W. & Buss, D.H. (1985) Immigrant Foods. Second supplement to McCance and Widdowson's 'The Composition of Foods'. London: HMSO.
Thomas, B. (Eds) (1988) Manual of Dietetic
Practice. pp. 245-255. Oxford: Blackwell Scientific Publications.
Thompson, B.. Skipper, D., Fraser. C., Hewitt, A. & Hunter, D. (1989) Dietary intake of Aberdeen primigravidae in 1950/51 and 1984/85. J. Hum. Nutr. Diet 2, 345-359.
Tierson, F.D.. Olsen, C.L. 8 Hook, E.B. (1985) Influence of cravings and aversions on diet in pregnancy. Ecology of Food and Nutrition 17,
Towler. G. & Shepherd, R. (1992)Modification of Fishbein and Ajzen's theory of reasoned ac- tion to predict chip consumption. Food Qual- ity and Preference 3. 37-45.
Wiles, S.J., Nettleton, P.A., Black, A.E. 81 Paul, A.A. (1980) The nutrient composition of some cooked dishes eaten in Britain: A supplemen- tary food composition table. J. Hum. Nutr. 34. 189-223.
117-129.
MS accepted May 1993





























