Embed Size (px)
Citation preview
J o u r n a l o f t h e A m e r i c a n P h a r m a c i s t s A s s o c i a t i o n japha.org MAR/APR 2014 | 54:2 | JAPhA 241
RESEARCH
Pharmacists’ training, perceived roles, and actions associated with dispensing controlled substance prescriptionsMarc L. Fleming, Jamie C. Barner, Carolyn M. Brown, Marv D. Shepherd, Scott A. Strassels, and Suzanne Novak
Received August 13, 2013, and in revised form December 18, 2013. Accepted for pub-lication December 19, 2013.
Marc L. Fleming, PhD, is Assistant Professor, Department of Pharmaceutical Health Outcomes and Policy, College of Pharmacy, University of Houston, TX; at the time of the research, he was a doctoral candidate at University of Texas at Austin. Jamie C. Barner, PhD, is Professor; Carolyn M. Brown, PhD, is Professor; Marv D. Shepherd, PhD, is Professor; Scott Strassels, PhD, was Assistant Professor; and Suzanne Novak, MD, PhD, is Adjunct Professor, Health Outcomes and Pharmacy Practice Division, College of Pharmacy, University of Texas at Austin.
Correspondence: Marc L. Fleming, PhD, Department of Pharmaceutical Health Outcomes and Policy, University of Hous-ton College of Pharmacy, 1441 Moursund Street, Houston, TX 77030. Fax: 832-842-8383. E-mail: [email protected]
Disclosure: The authors declare no con-flicts of interest or financial interests in any product or service mentioned in this article, including grants, employment, gifts, stock holdings, or honoraria.
Funding: Supported by an unrestricted educational grant from Reckitt Benckiser Pharmaceuticals, Inc.
Acknowledgments: Texas community pharmacists for their participation in the study and Patrick Knue, former Program Administrator of the Texas Department of Public Safety Prescription Program.
Previous presentation: International Soci-ety for Pharmacoeconomics and Outcomes Research International Meeting, New Or-leans, LA, May 20, 2013.
Abstract
Objectives: To examine situations that prompt pharmacists to access a pre-scription drug monitoring program (PDMP) database and management of opioid abuse/addiction; assess pharmacists’ actions when abuse is suspect-ed; and describe pharmacists’ tasks when dispensing controlled substance prescriptions (CSPs) and their related continuing pharmacy education (CPE).
Design: Cross-sectional mail survey of 1,000 randomly selected pharmacists.
Setting: Texas from February 2012 to April 2012.
Participants: 1,000 Texas community pharmacists.
Intervention: Mail survey instrument.
Main outcome measures: Prompts to use a PDMP and pharmacists’ views, actions, and related CPE programs
Results: The usable response rate was 26.2%. Pharmacists were more sup-portive of mandated PDMP use by physicians than by pharmacists (mean ± SD 4.1 ± 1.2 versus 3.2 ± 1.5; P <0.001), based on a 5-point Likert scale (1, strongly disagree, to 5, strongly agree). Most pharmacists would be prompt-ed to use a PDMP if the prescription contains mistakes (68.1%) or the patient requests an early refill (66.3%). Bivariate statistics showed that men phar-macists, those with BSPharm degrees, and pharmacists ≥50 years of age re-ported a greater number of CPE hours related to prescription opioid abuse and pain management. An analysis of variance showed that pharmacy own-ers reported significantly more (P <0.05) CPE compared with manager and staff pharmacists.
Conclusion: Older pharmacists with a BSPharm degree may be more will-ing to provide counseling to patients with opioid addiction based on their work experience and additional CPE related to controlled substances. As PDMP use becomes more prevalent, pharmacists should be prepared to in-teract and counsel patients identified with aberrant controlled prescription drug use and properly deliver pain management care. Additionally, schools of pharmacy curricula must prepare new pharmacists to prevent abuse and diversion, as well as intervene when aberrant use is identified.
Keywords: Pharmacists, prescription drug abuse, diversion, prescription drug monitoring, opioid addiction.
J Am Pharm Assoc. 2014; 54:241–250.doi: 10.1331/JAPhA.2014.13168
Downloaded From: http://japha.org/ by a University of Houston User on 05/11/2014

J o u r n a l o f t h e A m e r i c a n P h a r m a c i s t s A s s o c i a t i o njapha.org242 JAPhA | 54:2 | MAR/APR 2014
RESEARCH dispensing controlled substance prescriptions
sional judgment” when there is any doubt about legiti-macy.12 Where doubt exists, pharmacists do not have to dispense CSPs. The National Center on Addiction and Substance Abuse (CASA) at Columbia University conducted a national survey of pharmacists about how often they performed tasks associated with dispensing CSPs.13 Only about one-half reported always validating the prescriber’s U.S. Drug Enforcement Administration (DEA) number (51.1%) and consulting patient records (52.1%) before dispensing. Only 57% reported always checking for contraindications, and a mere 11.7% said they ask if the patient is taking any other CSPs.
Pharmacists must be aware of the tactics used by patients seeking to divert CSPs for illicit purposes.14 Patients have illegally altered legitimate prescriptions by changing the quantity (e.g., from 30 to 80) to obtain a larger supply. Other tactics include forging prescrip-tions on stolen prescription pads, calling in bogus pre-scriptions from what purports to be a doctor’s office, and photocopying prescriptions. In the CASA survey, 62.2% of pharmacists said they were somewhat confident in their ability to recognize patient attempts at diversion.13
In Wisconsin, 87% of responding pharmacists re-ported being confident in recognizing when a patient is attempting to divert CSPs.9 Before the availability of online-accessible PDMPs, some pharmacists reported relying on their “gut instinct” to detect diversion.13 Additionally, in a recent survey on PDMP use among Rhode Island and Connecticut pharmacists, 78.6% of responding pharmacists reported using insurance rejec-tion of prescription opioids to detect diversion.15 Based on the aforementioned literature, pharmacists are faced with the challenge of providing patient care while also trying to determine the legitimacy of CSPs.
PDMPs provide pharmacists with the opportunity to detect abuse and diversion. In the past, when phar-macists’ suspected abuse, most (92.8%) would call the prescribing physician.13 However, one study showed that the majority of participating pharmacists found it somewhat difficult to communicate with physicians about patients with aberrant CSP use.10 When pharma-cists suspect that patients are abusing or diverting CSPs, the necessary actions to address the situation are not always clear. Nearly one-half (47.6%) of pharmacists in the CASA study reported contacting the police in such instances.13 Pharmacists also sometimes tell patients that the medication is out of stock to avoid dispensing it.15
A lack of adequate education and training related to pain management and addiction has been reported in prior studies of pharmacists.16,17 In one study of New Hampshire health care providers, pharmacists were least likely to feel prepared to counsel patients with pain compared with physicians and nurses.16 Similarly, 50% of responding pharmacists in Wisconsin reported receiving only “fair” or “poor” training on opioids and pain management.9 In the CASA survey, about one-half
At a Glance
Synopsis: This survey-based study of 1,000 ran-domly selected community pharmacists in Texas found age- and education-related differences in their propensity to counsel patients with prescrip-tion opioid addiction. The authors found that older pharmacists with a BSPharm degree may be more willing to provide counseling to patients with opioid addiction and attributed this to great-er work experience and continuing pharmacy ed-ucation related to controlled substances. This need for greater training, the authors note, is bolstered by the increasing prevalence of online databases that allow pharmacists to access patient history of prescription drug use.
Analysis: Findings from this study—one of the first to assess the types of situations that would prompt pharmacists to access prescription drug monitoring program databases—suggest that pharmacists are con-fident in denying prescriptions based on patient history. More than one-third of survey participants also agreed that pharmacists should play a role in helping manage addiction, with only one-quarter feeling the need to no-tify law enforcement when suspecting abuse.
The Centers for Disease Control and Prevention has determined that prescription opioid abuse remains
a national epidemic.1 The Substance Abuse and Mental Health Services Administration’s Drug Abuse Warning Network reported that misuse of pharmaceuticals was associated with more than 1.3 million emergency de-partment visits in 2010.2
To combat this epidemic, 47 states and the District of Columbia have implemented prescription drug moni-toring programs (PDMPs) in which patients’ controlled substance prescription (CSP) data can be accessed by pharmacists and prescribers.3–6 PDMPs are state-operat-ed electronic databases containing the records of CSPs dispensed from community pharmacies in their respec-tive states.3 Some states monitor other drugs with abuse potential (e.g., tramadol).5 In many states, the PDMP da-tabase is made available to prescribers and pharmacists via an online Web portal that enables providers to view the data before prescribing or dispensing CSPs.3,7
In the absence of online-accessible PDMPs, commu-nity pharmacists have been faced with the challenge of determining whether to dispense CSPs based primar-ily on a patient’s medication profile (i.e., refill history), appearance, and demeanor.8–10 Pharmacists must also perform tasks in practice that are specific to dispensing CSPs in the community pharmacy setting. At the time of this research study, Texas was in the process of launch-ing an online PDMP.11
Pharmacists have a duty to verify that CSPs are for a legitimate medical reason and must exercise “profes-
Downloaded From: http://japha.org/ by a University of Houston User on 05/11/2014

J o u r n a l o f t h e A m e r i c a n P h a r m a c i s t s A s s o c i a t i o n japha.org MAR/APR 2014 | 54:2 | JAPhA 243
dispensing controlled substance prescriptions RESEARCH
of pharmacists reported receiving CPE in identifying abuse and addiction, with 48% reporting they received CPE in diversion prevention.13 Additionally, only one-half of pharmacists in the CASA survey reported re-ceiving “good” or “excellent” training in preventing abuse and diversion of CSPs. These findings indicate the need for pharmacists to receive continued training in the areas of pharmacy practice related to dispensing CSPs and may also highlight possible gaps in pharmacy education.
Other issues explored in previous studies have fo-cused on pharmacists’ knowledge, attitudes toward chronic pain management, and stocking18–21 or dispens-ing of opioids,9,22 but few studies have included infor-mation regarding prompts to use PDMPs. In the study conducted by Green et al.,17 pharmacists reported using the PDMP to screen for prescription drug abuse, as well as using their professional judgment. The most reported method for detecting doctor shopping was insurance rejection (77.9%), followed by professional judgment (73.1%). Among PDMP users in Connecticut, the PDMP was thought to be useful in reducing both abuse and di-version.
Fleming et al.23 and Gavaza et al.24 conducted stud-ies in Texas and Virginia, respectively, both of which ex-amined pharmacists’ intention to employ a PDMP using the theory of planned behavior. While the Texas study was conducted prior to PDMP online access for phar-macists, it found that pharmacists in the state reported a strong intention (mean ± SD, 7.7 ± 2.4; scale range, –9 to +9) to use the PDMP once it was made available. The Virginia study also found that pharmacists intended to use the PDMP when questions about validity of a pre-scription exist (5.3 ± 4.6; –9 to +9).
To gain access to state PDMP data, pharmacists must first register with the state PDMP governing entity to obtain login and password credentials.11,25 Ulbrich et al.26 conducted a study in Ohio to determine why phar-macists may or may not be registered for access with the state PDMP. Among those who had not registered, the time it takes to access data was cited as the primary reason. Pharmacists who did register for access cited the ability to prevent doctor shopping as their primary rea-son for doing so. In Kentucky, only 16% of pharmacists were registered for PDMP access in 2010,27 and in Maine, only 13% of pharmacists were registered for their PDMP in 2009.28 These data are indicative of the slow adoption of PDMPs among pharmacists when programs are ini-tially launched.
Although use is relatively low among pharma-cists, especially when compared with physicians,29 the number of reports used by pharmacists has steadily increased. For example, at the end of 2012 in Virginia, 2,954 pharmacists were registered for PDMP access and represented 8.1% of requested patient reports (i.e., pa-tient data queries) among all authorized users of the PD-
MP data.30 As of June 2013, the number of pharmacists registered for PDMP access in Virginia had increased to 4,212 and they accounted for 23% of requested patient reports.31
Because they serve as both patient advocates and CSP gatekeepers, pharmacists are in a unique posi-tion.32,33 They must make decisions regarding appro-priate dispensing, and their professional opinions may differ from that of the prescriber. Pharmacists are also responsible for ensuring that patients do not overuse CSPs or divert them for illegal use.12,34,35 Implementation of PDMPs with online access should better enable phar-macists to help avoid overuse and diversion by provid-ing necessary patient data for more informed decision making.
The Texas PDMP, officially launched in August 2012, is known as Prescription Access in Texas (PAT). Texas is one of six states in which the PDMP is under the authority of a law enforcement entity.3 It is unclear how this may affect pharmacists’ perceptions of the PDMP or influence their intention to use it. Before PAT, PDMP pa-tient reports were available to the pharmacist-in-charge within 30 to 45 days via mail or fax.36 Fleming et al.29 reported that states with manual PDMP reporting (i.e., no online data access) averaged less than 15 requests per year. Considering the prescription drug abuse epi-demic, coupled with PAT being under the authority of a law enforcement entity, we wanted to examine how pharmacists plan to interact with PAT once available and understand pharmacists’ current actions in the ab-sence of PAT.
ObjectivesThe purpose of this study was to examine situations that would prompt pharmacists to access a patient’s CSP his-tory using an online-accessible PDMP database and to assess pharmacists’ views on managing opioid addic-tion. The study also explored the actions taken by phar-macists who suspect abuse, the tasks associated with dispensing CSPs, and CPE training related to pain man-agement/diversion.
MethodsStudy designThe study population comprised licensed Texas com-munity pharmacists practicing in the state as of Septem-ber 1, 2011. A cross-sectional survey design was used to collect data from 1,000 randomly selected Texas com-munity pharmacists. The Texas State Board of Pharmacy allows for public access to the list of currently practicing pharmacists. The list contains pharmacists’ home ad-dress, employment type (e.g., community chain), license status, gender, employer name and location, and posi-tion (e.g., staff). A random number generator was used to select 1,000 pharmacists from a list of 10,694 actively licensed Texas community pharmacists who listed a pri-
Downloaded From: http://japha.org/ by a University of Houston User on 05/11/2014

J o u r n a l o f t h e A m e r i c a n P h a r m a c i s t s A s s o c i a t i o njapha.org244 JAPhA | 54:2 | MAR/APR 2014
RESEARCH dispensing controlled substance prescriptions
mary address in Texas. Pharmacists who listed their pri-mary employment type as hospital, consultant, or other nondirect-patient-contact practice setting (e.g., mail ser-vice) were excluded from the study. Additionally, two potential respondents were excluded from the sample denominator—one for conflict of interest and one who called the researchers upon receipt of the prenotice post-card and indicated he did not dispense CSPs. The final study population comprised the remaining 998 com-munity pharmacists. This research was part of a larger study to examine pharmacists’ intention to use a PDMP database when faced with questions regarding validity of a prescription and/or patient need for a controlled medication.23
The University of Texas Institutional Review Board approved the study.
Survey instrumentThe questions from the survey instrument, which as-sessed pharmacists’ views and actions related to dis-pensing CSPs, were developed from prior literature13 with input from the Texas Department of Public Safety and the study authors. The questions were representa-tive of four categories concerning pharmacy practice issues related to controlled prescription drugs: (1) pa-tient behavior (prompts) that would lead pharmacists to query PDMP data and pharmacists’ views on opioid ad-diction/diversion management; (2) actions when abuse suspected; (3) pharmacy practice tasks when dispensing CSPs; and (4) pharmacist-reported CPE and training re-lated to CSPs (e.g., pain management).
To better understand when pharmacists might query PDMP data, the questions addressed the frequency with which certain patient behaviors would prompt PDMP use. Specifically, the pharmacists were asked how the following scenarios would trigger their decision to use the PDMP: a new patient, a patient preferring to pay cash, mistakes or irregularities in a written prescription, and an early refill request. Additionally, the pharmacists were asked if they discuss treatment with buprenor-phine or buprenorphine/naloxone with patients or pre-scribers when opioid addiction is suspected. The afore-mentioned items were assessed on a 5-point Likert item scale (1, never, to 5, always). Another question asked if pharmacists should manage opioid addiction as they do other chronic diseases (e.g., hypertension). Since PDMP registration and use is not mandatory, pharmacists were also asked about support for mandated PDMP use for themselves and for prescribers. These statements were assessed using a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree).
The next section of the survey asked pharmacists about actions they would take when suspecting patient abuse, such as notifying law enforcement, refusing to fill the prescription, calling the prescriber, documenting the incident, and counseling the patient about addiction.
These statements were assessed using a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). The two questions regarding addiction counsel-ing and opioid management were summated to assess pharmacists’ overall perception of managing opioid ad-diction in the pharmacy. Pharmacists were also asked about the frequency of tasks that are typically associated with dispensing CSPs. CPE and training hours related to abuse/addiction, diversion, and pain management in the past 5 years were also assessed. These three ques-tions were combined to represent an overall scale for CPE.
Demographic and practice characteristics were col-lected regarding age, gender, race/ethnicity, highest pharmacy degree achieved, practice setting, daily pre-scription count, Internet access, position/title, employ-ment status (e.g., full-time), years of community experi-ence, and practice location (e.g., rural).
Data collectionThe questionnaire was pretested with eight community pharmacists with varied backgrounds and experience to ensure content validity and clarity of all questions and answers. Comments from the pretest group were evalu-ated and minor modifications to the survey were incor-porated.
Mail merge was used to personalize the pre-notice postcards and cover letters for each potential respon-dent. A modified version of Dillman’s tailored design method was employed to maximize the quantity and quality of survey responses.37
A pre-notice postcard was sent to the sample of ran-domly selected pharmacists 3 days before the question-naire. The postcard alerted pharmacists to the nature of the questionnaire and allowed them the opportunity to opt out of receiving further notification from the re-searchers.
There were two separate mailings of the question-naire. The second mailing, which went out 2 weeks after the first, contained an updated cover letter thanking pre-vious respondents and encouraging non-respondents to complete the questionnaire and return it within 2 weeks of receipt. None of the questionnaires were returned as undeliverable.
Data analysisDescriptive statistics (frequencies, means, and standard deviations) were performed when appropriate. Pear-son’s correlation (perception of opioid addiction man-agement) and Cronbach’s alpha (CPE) were used to as-sess scale reliabilities. Bivariate statistics using a paired samples t test was used to assess whether pharmacists’ views on mandatory use by pharmacists versus physi-cians differed significantly.
Independent samples t tests and one-way analysis of variance (ANOVA) were used to assess statistical
Downloaded From: http://japha.org/ by a University of Houston User on 05/11/2014

J o u r n a l o f t h e A m e r i c a n P h a r m a c i s t s A s s o c i a t i o n japha.org MAR/APR 2014 | 54:2 | JAPhA 245
dispensing controlled substance prescriptions RESEARCH
significance of demographic and practice characteristics regarding perception of opioid addiction management and CPE related to dispensing CSPs.
The a priori level of significance for all statistical tests was set at P <0.05. Data were analyzed using SAS 9.3 for Windows.
ResultsDemographicsOf the surveys assumed delivered (n = 998) and usable responses (n = 261), the response rate was 26.2%. Demo-graphics and practice characteristics of respondents are presented in Table 1.
Respondents were 50.3 ± 13.7 years of age and pri-marily men (52.1%), white (65.8%), and holders of a BSPharm degree (69.7%). Many were working in com-munity chain pharmacies (40.9%) as staff pharmacists (41.3%) or pharmacy managers (40.9%). The mean (± SD) number of prescriptions dispensed daily was 275.2 ± 158.2. Pharmacists reported 22.3 ± 14.4 years of commu-nity pharmacy experience, and 42.6% of them worked in a suburban area.
Pharmacists’ PDMP prompts and opioid addiction/diversion managementThe following items were measured on a scale from 1 (strongly disagree) to 5 (strongly agree). Pharmacists were asked about their agreement with a statutory re-quirement for PDMP use. A paired t test showed that pharmacists were more supportive of a statutory re-quirement for prescribers (4.1 ± 1.2) than for pharma-cists (3.2 ± 1.5), P <0.001. Pharmacists were also asked how often specific situations would trigger them to use the PDMP (Table 2). Almost one-half of respondents (48.1%) reported that patients who prefer to pay cash would always trigger PDMP use. Mistakes or irregu-larities in prescriptions (68.1%) and early refill requests (66.3%) would also always trigger PDMP use.
Pharmacists’ actionsPharmacists were asked about their level of agreement with actions taken in response to suspected abuse (Table 3). Survey respondents were neutral in regard to noti-fying law enforcement (44.0%) and counseling patients about addiction (35.1%). However, the majority agreed or strongly agreed with either refusing to dispense the prescription (51.6%) or documenting the incident (79.1%). When asked whether pharmacists should man-age opioid addiction in a similar manner to other chron-ic diseases, respondents were primarily neutral (30.4%), although 16.0% strongly agreed with the scenario. Pharmacists were more likely to express disagreement (2.2 ± 1.0) with dispensing prescriptions for controlled medications if faced with uncertainty. The two items comprising the scale on pharmacists’ overall percep-
tion of opioid addiction management were significantly correlated, based on Pearson’s correlation coefficient (r = 0.40, P <0.001). Pharmacists with a bachelor’s degree were more favorable regarding perception of opioid ad-diction management than pharmacists with a PharmD (t = 2.36, P = 0.02).
Table 1. Sample demographic and practice characteristics (n = 261)a
VariableFrequency (%)b (unless
otherwise noted)
Age (years) Mean ± SD, 50.3 ± 13.7Number of prescriptions dispensed daily Mean ± SD, 275.2 ± 158.2Community pharmacy experi-ence (years) Mean ± SD, 22.3 ± 14.4Gender Men 136 (52.1) Women 125 (47.9)Race/ethnicity (n = 257)a
White/non-Hispanic 169 (65.8) Asian American/Pacific Islander 30 (11.7) Black/non-Hispanic 29 (11.3) American Indian/Alaska Native 26 (10.1) Mexican American/Hispanic 3 (1.2)Education BSPharm 182 (69.7) PharmD 76 (29.1) MSPharm/residency 2 (0.8) PhD 1 (0.4)Pharmacy practice setting (n = 259)a
Community chain 106 (40.9) Grocery store (e.g., Kroger, H-E-B) 57 (22.0) Community independent 55 (21.2) Mass merchandiser (e.g., Walmart) 32 (12.4) Outpatient/clinic pharmacy 9 (3.5)Current position/title (n = 259)a
Staff 107 (41.3) Manager/pharmacist-in-charge 106 (40.9) Relief/prn 27 (10.4) Owner 18 (7.0) Pharmacy resident 1 (0.4)Pharmacy practice location (n = 256)a
Suburban 109 (42.6) Urban 102 (39.8) Rural 45 (17.6)
Abbreviations used: BSPharm, Bachelor of Science in Pharmacy; MSPharm, Master of Pharmacy; PharmD, Doctor of Pharmacy; PhD, Doctor of Philosophy; prn, as needed.aNumbers do not always total 261 due to missing data.bSum of percentages may not equal 100.0% due to rounding.
Downloaded From: http://japha.org/ by a University of Houston User on 05/11/2014

J o u r n a l o f t h e A m e r i c a n P h a r m a c i s t s A s s o c i a t i o njapha.org246 JAPhA | 54:2 | MAR/APR 2014
RESEARCH dispensing controlled substance prescriptions
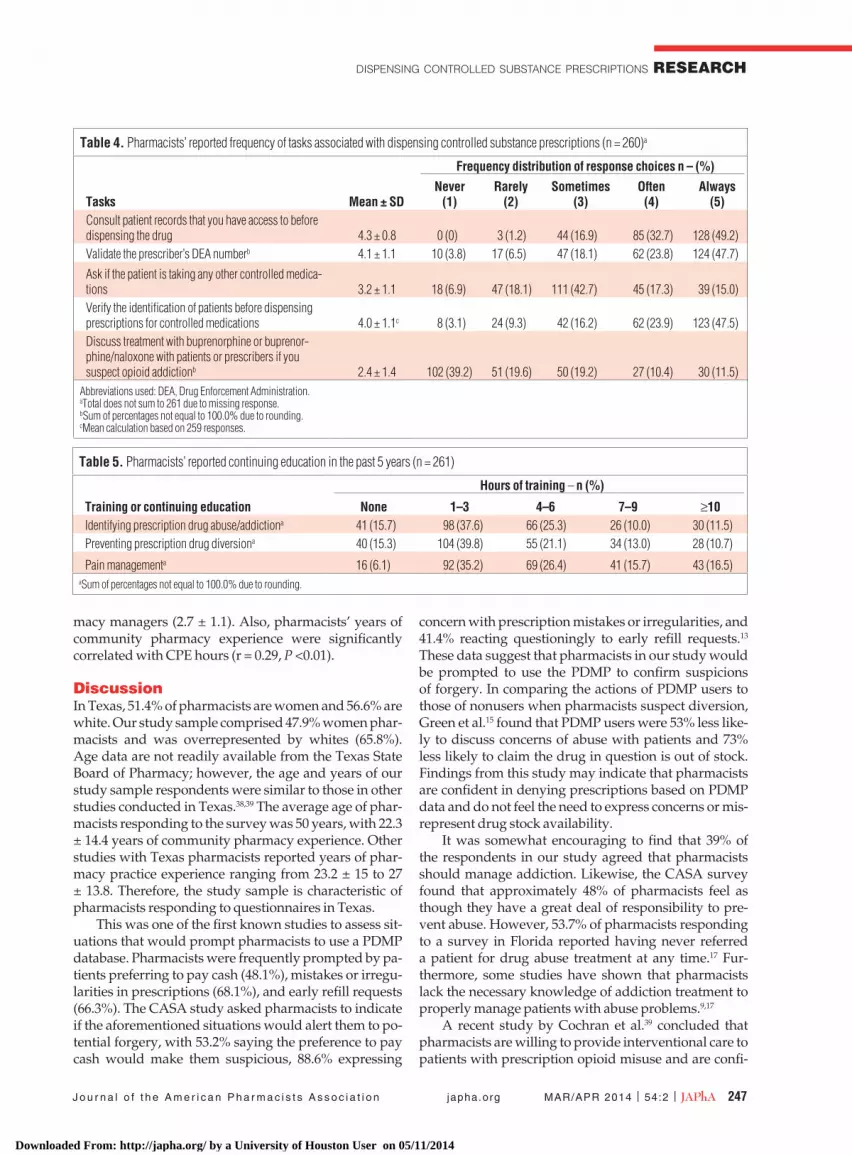
Pharmacists’ tasksPharmacists were surveyed about the frequency of tasks typically associated with dispensing controlled medi-cations (Table 4). They reported always consulting pa-tient records before dispensing a controlled medication (49.2%), validating DEA numbers (47.7%) and verifying patient identification (47.5%). However, 42.7% of re-spondents said they sometimes inquire about other con-trolled medications. When asked if they discuss treat-ment with buprenorphine or buprenorphine/naloxone, 39.2% said never, while 11.5% said always.
Pharmacists’ CPE activitiesPharmacists reported receiving 1–3 hours of training in the past 5 years on identifying prescription drug abuse/addiction (37.6%) and preventing drug diversion (39.8%), while approximately 15% reported no training at all in these areas. Regarding pain management, 35.2%
reported at least 1–3 hours of training, with only 6.1% re-porting no training (Table 5). The Cronbach’s alpha for the combined CPE scale was 0.89.
T test results revealed that women pharmacists re-ported fewer CPE hours in the past 5 years than men pharmacists related to prescription drug abuse, diver-sion, and pain management (t = –2.17, P = 0.03). Phar-macists with a BSPharm degree reported higher mean CPE hours (t = 2.79, P <0.01). Additionally, pharmacists under the age of 50 years reported fewer hours of CPE hours compared with those aged 50 and above (t = –2.97, P <0.01).
One-way ANOVA revealed a significant difference in reported CPE/training hours by position (i.e., staff, manager, and owner). Post-hoc analysis using Tukey’s honestly significant difference (HSD) test showed that mean ± SD hours for owners (3.5 ± 1.1) were significant-ly higher than for staff pharmacists (2.7 ± 1.1) or phar-
Table 2. Pharmacists’ reported mean and frequency distribution of events that would prompt PDMP use (n = 260)a
Frequency distribution of response choices – n (%)
Events Mean ± SDNever
(1)Rarely
(2)Sometimes
(3)Often (4)
Always (5)
New patient 3.7 ± 1.1 8 (3.1) 14 (5.4) 108 (41.5) 49 (18.8) 81 (31.2)Patient prefers to pay cashb 4.2 ± 1.0 6 (2.3) 8 (3.1) 35 (13.5) 86 (33.1) 125 (48.1)Mistakes or irregularities in the written prescriptionb 4.6 ± 0.8 3 (1.2) 3 (1.2) 18 (6.9) 59 (22.7) 177 (68.1)Refill request that is too earlyb 4.6 ± 0.7c 2 (0.8) 1 (0.4) 20 (7.8) 64 (24.8) 171 (66.3)
aTotal does not sum to 261 due to missing response. bSum of percentages not equal to 100.0% due to rounding.
cMean calculation based on 258 responses.
Table 3. Mean and frequency distribution of pharmacists’ reported actions when suspecting abuse of controlled medication and pharmacists’ opinions regarding management of opioid addiction (n = 259)a
Frequency distribution of response choices – n (%)
Actions Mean ± SDStrongly disagree
(1)Disagree
(2)
Neither agree nor disagree
(3)Agree
(4)Strongly agree
(5)Notify law enforcement 2.9 ± 1.1 37 (14.3) 42 (16.2) 114 (44.0) 41 (15.8) 25 (9.7)Refuse to dispense the prescriptionb 4.4c ± 0.8 4 (1.6) 1 (0.4) 21 (8.1) 99 (38.4) 133 (51.6)
Call the prescriber 4.5c ± 0.7 1 (0.4) 5 (1.9) 14 (5.4) 89 (34.5) 149 (57.8)Document the incidentb 4.2c ± 0.9 3 (1.2) 9 (3.5) 42 (16.3) 72 (27.9) 132 (51.2)
Counsel patient about addictions 3.0 ± 1.2 35 (13.5) 47 (18.2) 91 (35.1) 50 (19.3) 36 (13.9)ItemOpioid addiction should be managed by pharmacists similar to other chronic diseases (e.g., hypertension)b 3.1d ± 1.3 41 (16.0) 38 (14.8) 78 (30.4) 59 (23.0) 41 (16.0)
aTotal does not sum to 261 due to missing responses.bSum of percentages not equal to 100.0% due to rounding.cMean calculation based on 258 responses.dMean calculation based on 257 responses.
Downloaded From: http://japha.org/ by a University of Houston User on 05/11/2014
J o u r n a l o f t h e A m e r i c a n P h a r m a c i s t s A s s o c i a t i o n japha.org MAR/APR 2014 | 54:2 | JAPhA 247
dispensing controlled substance prescriptions RESEARCH
macy managers (2.7 ± 1.1). Also, pharmacists’ years of community pharmacy experience were significantly correlated with CPE hours (r = 0.29, P <0.01).
DiscussionIn Texas, 51.4% of pharmacists are women and 56.6% are white. Our study sample comprised 47.9% women phar-macists and was overrepresented by whites (65.8%). Age data are not readily available from the Texas State Board of Pharmacy; however, the age and years of our study sample respondents were similar to those in other studies conducted in Texas.38,39 The average age of phar-macists responding to the survey was 50 years, with 22.3 ± 14.4 years of community pharmacy experience. Other studies with Texas pharmacists reported years of phar-macy practice experience ranging from 23.2 ± 15 to 27 ± 13.8. Therefore, the study sample is characteristic of pharmacists responding to questionnaires in Texas.
This was one of the first known studies to assess sit-uations that would prompt pharmacists to use a PDMP database. Pharmacists were frequently prompted by pa-tients preferring to pay cash (48.1%), mistakes or irregu-larities in prescriptions (68.1%), and early refill requests (66.3%). The CASA study asked pharmacists to indicate if the aforementioned situations would alert them to po-tential forgery, with 53.2% saying the preference to pay cash would make them suspicious, 88.6% expressing
concern with prescription mistakes or irregularities, and 41.4% reacting questioningly to early refill requests.13 These data suggest that pharmacists in our study would be prompted to use the PDMP to confirm suspicions of forgery. In comparing the actions of PDMP users to those of nonusers when pharmacists suspect diversion, Green et al.15 found that PDMP users were 53% less like-ly to discuss concerns of abuse with patients and 73% less likely to claim the drug in question is out of stock. Findings from this study may indicate that pharmacists are confident in denying prescriptions based on PDMP data and do not feel the need to express concerns or mis-represent drug stock availability.
It was somewhat encouraging to find that 39% of the respondents in our study agreed that pharmacists should manage addiction. Likewise, the CASA survey found that approximately 48% of pharmacists feel as though they have a great deal of responsibility to pre-vent abuse. However, 53.7% of pharmacists responding to a survey in Florida reported having never referred a patient for drug abuse treatment at any time.17 Fur-thermore, some studies have shown that pharmacists lack the necessary knowledge of addiction treatment to properly manage patients with abuse problems.9,17
A recent study by Cochran et al.39 concluded that pharmacists are willing to provide interventional care to patients with prescription opioid misuse and are confi-
Table 4. Pharmacists’ reported frequency of tasks associated with dispensing controlled substance prescriptions (n = 260)a
Frequency distribution of response choices n – (%)
Tasks Mean ± SDNever
(1)Rarely
(2)Sometimes
(3)Often(4)
Always(5)
Consult patient records that you have access to before dispensing the drug 4.3 ± 0.8 0 (0) 3 (1.2) 44 (16.9) 85 (32.7) 128 (49.2)Validate the prescriber’s DEA numberb 4.1 ± 1.1 10 (3.8) 17 (6.5) 47 (18.1) 62 (23.8) 124 (47.7)
Ask if the patient is taking any other controlled medica-tions 3.2 ± 1.1 18 (6.9) 47 (18.1) 111 (42.7) 45 (17.3) 39 (15.0)Verify the identification of patients before dispensing prescriptions for controlled medications 4.0 ± 1.1c 8 (3.1) 24 (9.3) 42 (16.2) 62 (23.9) 123 (47.5)Discuss treatment with buprenorphine or buprenor-phine/naloxone with patients or prescribers if you suspect opioid addictionb 2.4 ± 1.4 102 (39.2) 51 (19.6) 50 (19.2) 27 (10.4) 30 (11.5)
Abbreviations used: DEA, Drug Enforcement Administration.aTotal does not sum to 261 due to missing response.bSum of percentages not equal to 100.0% due to rounding.cMean calculation based on 259 responses.
Table 5. Pharmacists’ reported continuing education in the past 5 years (n = 261)
Hours of training – n (%)
Training or continuing education None 1–3 4–6 7–9 ≥10Identifying prescription drug abuse/addictiona 41 (15.7) 98 (37.6) 66 (25.3) 26 (10.0) 30 (11.5)Preventing prescription drug diversiona 40 (15.3) 104 (39.8) 55 (21.1) 34 (13.0) 28 (10.7)
Pain managementa 16 (6.1) 92 (35.2) 69 (26.4) 41 (15.7) 43 (16.5)aSum of percentages not equal to 100.0% due to rounding.
Downloaded From: http://japha.org/ by a University of Houston User on 05/11/2014
J o u r n a l o f t h e A m e r i c a n P h a r m a c i s t s A s s o c i a t i o njapha.org248 JAPhA | 54:2 | MAR/APR 2014
RESEARCH dispensing controlled substance prescriptions
dent in their ability to provide such care. Texas pharma-cists in the Cochran et al. study were mainly indepen-dent pharmacists.
Our study results indicated pharmacy owners tend-ed to obtain CPE hours related to pain management and addiction, while the Cochran et al. study suggests that independent pharmacists in Texas are more engaged re-garding abuse and diversion.
Pharmacists must balance “policing” patients with providing care.32 Some within the profession advocate that pharmacists take a more active role in counseling patients with opioid addiction. However, results from our study were similar to those of the CASA study re-garding pharmacists’ actions when abuse is suspected. The only major difference in our study was that just 25.5% of pharmacists expressed agreement with noti-fying law enforcement when suspecting abuse, com-pared with 47.6% in the CASA survey. Some pharma-cists expressed willingness to discuss buprenorphine/naloxone with patients or prescribers when abuse is suspected, but more than one-half (58%) acknowledged seldom doing so. In a study of Michigan pharmacists, 96% agreed that pharmacists should communicate with the prescriber if patient abuse is suspected.10
Pharmacists must consider many factors when dis-pensing CSPs, especially given the nature of the pre-scription drug abuse epidemic. One of the objectives of our study was to describe how often pharmacists engage in specific tasks related to dispensing CSPs. The results of this study are similar to those reported by CASA.13 Regarding consulting patient records before dispensing, respondents in the CASA study reported doing so often or always 81.4% of the time, compared with 81.9% of the time in this study. Pharmacists in the CASA study said they validated the prescriber’s DEA number 68.2% of the time (compared with 71.6% in our study) and asked patients if they are taking other con-trolled medications often to always 36.1% of the time (compared with 32.3% in our study). It should be noted that although the prescription drug abuse problem was initially recognized in 2005, the media attention and prevalence of online-accessible PDMPs was much lower at that time than it is today.
Prior studies have reported that gaps exist in phar-macists’ education on pain management, prescription drug abuse, and diversion.13,17 The CASA survey found that pharmacists received minimal training on pain management and diversion while in school. In Florida, pharmacists reported receiving 2 or fewer hours of ad-diction and substance abuse education during pharma-cy school, with 29% saying they received no education at all on these topics.17 Comparatively, a study of West Virginia pharmacists revealed that 57.7% of pharmacists agreed that their formal education in pain management is adequate to provide good patient care.22 Pharmacists in our study reported receiving at least 1–3 hours of
training in the past 5 years on abuse/addiction (84.3%), drug diversion (84.7%), and pain management (93.9%). Still, approximately 15% reported no training on abuse/addiction or drug diversion. Green et al.15 reported that 66.8% of respondents said they had CPE related to opi-oids and pain management in the past 5 years. In a sepa-rate study of Indiana pharmacists, only 22% reported postgraduate education on addiction.40 Interestingly, the mean length of time of pharmacy practice in the In-diana study was 22 years.
Considering the ongoing epidemic of prescription drug abuse, pharmacists should be trained to address opioid addiction. With increasing access to PDMPs, pharmacists now have a tool to better detect aberrant behaviors of patients taking CSPs.15 Some pharmacists are now using PDMPs as screening tools to detect abuse and diversion (e.g., doctor shopping). In general, edu-cation and training has been reported as inadequate in these areas. Lack of proper training has been associated with a fear to dispense CSPs and a decreased likelihood of pharmacists providing interventional counseling. Furthermore, Wenthur et al.40 found that approximately 75% of pharmacists felt a need for more emphasis on ed-ucation and training on drug withdrawal and the phar-macology of addiction. Pharmacy schools should evalu-ate their curricula to ensure future pharmacists can meet the needs of patients requiring opioid therapy, as well as prevent misuse among those with patterns of abuse.
LimitationsThe results of this study should be considered in light of several limitations. Response bias could have potential-ly influenced the results. In our study, as well as other state reports on PDMP use, many respondents seemed interested in the topic of diversion and the PDMP. In the survey of Kentucky pharmacists regarding PDMP ef-fectiveness, only 23% of non-PDMP users provided re-sponses.27 Such a low response rate may not adequately capture the tasks and actions regarding CSP dispensing of pharmacists who are more ambivalent toward the PDMP.
While previous studies of pharmacists have as-sessed the impact of knowledge concerning pain man-agement and opioids, our study did not. Texas has a special prescription pad requirement for the prescribing of Schedule II medications; therefore, studies assessing CSP dispensing may be less generalizable to states with-out such restrictions.41
Additionally, Texas pharmacists report CPE re-quirements upon license renewal every 2 years, which may have influenced their ability to recall the number of CPE hours in the past 5-year period.
ConclusionCompared with women pharmacists, men pharmacists received more CPE related to CSPs. Pharmacists aged
Downloaded From: http://japha.org/ by a University of Houston User on 05/11/2014

J o u r n a l o f t h e A m e r i c a n P h a r m a c i s t s A s s o c i a t i o n japha.org MAR/APR 2014 | 54:2 | JAPhA 249
dispensing controlled substance prescriptions RESEARCH
50 years and older obtained more CPE related to CSPs. Those pharmacists with a BSPharm degree were more favorable of counseling and managing patients with opioid addiction. As PDMP use becomes more preva-lent, it is increasingly important to understand how pharmacists interact and counsel patients with addic-tive patterns of prescription opioid use. Only a certain segment of pharmacists appear engaged in preventing diversion and are thus more likely to use the PDMP during patient care. These results may indicate student pharmacists are not receiving adequate training related to prescription drug abuse and addiction treatment and that most training is based on work experience. Wom-en pharmacists may also be less comfortable than men pharmacists in confronting patients about prescription opioid misuse. Moreover, community pharmacists must advance beyond denying CSPs where appropriate and provide interventional counseling and referrals when necessary. Other essential elements for pharmacist in-volvement include improving pharmacists’ knowledge of appropriate opioid addiction treatment with pharma-cologic agents and participating in collaborative agree-ments involving pain management.
It is important to note that pharmacists in many studies have expressed an interest in training on pain management and addiction. Future research should be conducted to determine why this demand for education and training remains unmet. The opioid epidemic was less prevalent even 10 years ago; therefore, practicing pharmacists must seek training in this area to become more knowledgeable. Pharmacy employers should seize this opportunity to develop training programs that address education gaps. Pain management and addic-tion training in pharmacy school curricular core courses must be considered moving forward. With the expan-sion of PDMPs, especially state interconnectivity, more research will be needed to determine how pharmacists can best incorporate PDMPs into community practice and influence appropriate patient care.
References1. Paulozzi LJ, Jones CM, Mack KA, et al. Vital signs: overdoses of pre-
scription opioid pain relievers—United States, 1999–2008. MMWR Morb Mortal Wkly Rep. 2011;60(43):1487-1492.
2. Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality. The DAWN Report: High-lights of the 2010 Drug Abuse Warning Network (DAWN) findings on drug-related emergency department visits. www.samhsa.gov/data/2k12/DAWN096/SR096EDHighlights2010.htm. Accessed August 4, 2012.
3. Blumenschein K, Fink JL III, Freeman PR, et al. Review of prescription drug monitoring programs in the United States. http://chfs.ky.gov/NR/rdonlyres/85989824-1030-4AA6-91E1-7F9E3EF68827/0/KASPE-REvaluationPDMPStatusFinalReport6242010.pdf. Accessed May 3, 2011.
4. Drug Enforcement Administration, Office of Diversion Control. State Prescription Drug Monitoring Programs: Questions and Answers—What is the difference between HRPDMP and NASPER? www.deadi-version.usdoj.gov/faq/rx_monitor.htm#10. Accessed September 29, 2011.
5. National Allicance for Model State Drug Laws. Prescription drug moni-toring programs (Administration of PDMPs); Executive summary—prescription drug abuse, addiction and diversion: Overview of State Legislative and Policy Initiatives, Part 1 (March 2014). www.namsdl.org/prescription-monitoring-programs.cfm. Accessed May 1, 2014.
6. U.S. Government Accountability Office. Prescription drugs: state moni-toring programs provide useful tool to reduce diversion. http://www.gao.gov/products/GAO-02-634. Accessed April 25, 2010.
7. Griggs CA, Weiner SG. 271 prescription monitoring programs: current use and impressions. Ann Emerg Med. 2011;58(4):S268.
8. Brushwood DB. From confrontation to collaboration: collegial account-ability and the expanding role of pharmacists in the management of chronic pain. J Law Med Ethics. 2001;29(1):69-93.
9. Joranson DE, Gilson AM. Pharmacists’ knowledge of and attitudes to-ward opioid pain medications in relation to federal and state policies. J Am Pharm Assoc. 2001;41(2):213-220.
10. Koski RR. Pharmacists’ perceptions of controlled substance abuse in the rural upper peninsula of Michigan. J Am Pharm Assoc. 2006;46(6):751-753.
11. Texas Department of Public Safety. DPS launches online version of Texas prescription drug monitoring program. www.dps.texas.gov/director_staff/public_information/pr080212.htm. Accessed August 3, 2012.
12. Drug Enforcement Administration, Office of Diversion Control. Phar-macist’s manual: an informational outline of the Controlled Substances Act. 2010 ed. www.deadiversion.usdoj.gov/pubs/manuals/pharm2/pharm_manual.pdf. Accessed October 19, 2010.
13. National Center on Addiction and Substance Abuse at Columbia Uni-versity. Under the counter: the diversion and abuse of controlled pre-scription drugs in the U.S. www.casacolumbia.org/addiction-research/reports/under-the-counter-diversion-abuse-controlled-perscription-drugs. Accessed April 29, 2009.
14. Blumenschein K. Prescription drug diversion: fraudulent tactics utilized in the community pharmacy. Am J Pharm Educ. 1997;61(2):184-188.
15. Green TC, Mann MR, Bowman SE, et al. How does use of a prescription monitoring program change pharmacy practice? J Am Pharm Assoc. 2013;53(3):273-281.
16. Furstenberg CT, Ahles TA, Whedon MB, et al. Knowledge and attitudes of health-care providers toward cancer pain management: a compari-son of physicians, nurses, and pharmacists in the state of New Hamp-shire. J Pain Symptom Manage. 1998;15(6):335-349.
17. Lafferty L, Hunter TS, Marsh WA. Knowledge, attitudes and practices of pharmacists concerning prescription drug abuse. J Psychoactive Drugs. 2006;38(3):229-232.
18. Green CR, Ndao-Brumblay SK, West B, et al. Differences in prescription opioid analgesic availability: comparing minority and white pharmacies across Michigan. J Pain. 2005;6(10):689-699.
19. Greenwald BD, Narcessian EJ. Opioids for managing patients with chronic pain: community pharmacists’ perspectives and concerns. J Pain Symptom Manage. 1999;17(5):369-375.
Downloaded From: http://japha.org/ by a University of Houston User on 05/11/2014

J o u r n a l o f t h e A m e r i c a n P h a r m a c i s t s A s s o c i a t i o njapha.org250 JAPhA | 54:2 | MAR/APR 2014
RESEARCH dispensing controlled substance prescriptions
20. Kanner RM, Portenoy RK. Unavailability of narcotic analgesics for am-bulatory cancer patients in New York City. J Pain Symptom Manage. 1986;1(2):87-89.
21. Morrison RS, Wallenstein S, Natale DK, et al. “We don’t carry that”—failure of pharmacies in predominantly nonwhite neighborhoods to stock opioid analgesics. N Engl J Med. 2000;342(14):1023-1026.
22. Ponte CD, Johnson-Tribino J. Attitudes and knowledge about pain among West Virginia pharmacists. J Am Pharm Assoc. 2007;47(3):379-382.
23. Fleming ML, Barner JC, Brown CM, et al. Using the theory of planned behavior to examine pharmacists’ intention to utilize a prescrip-tion drug monitoring program database. Res Social Adm Pharm. 2014;10(2):285-296.
24. Gavaza P, Fleming M, Barner JC. Examination of psychosocial predic-tors of Virginia pharmacists’ intention to utilize a prescription drug monitoring program using the theory of planned behavior. Res Social Adm Pharm. 2014;10(2):448-458.
25. Perrone J, DeRoos FJ, Nelson LS. Prescribing practices, knowl-edge, and use of prescription drug monitoring programs (PDMP) by a national sample of medical toxicologists, 2012. J Med Toxicol. 2012;8(4):341-352.
26. Ulbrich TR, Dula CA, Green CG, et al. Factors influencing community pharmacists’ enrollment in a state prescription monitoring program. J Am Pharm Assoc. 2010;50(5):588-594.
27. Blumenschein K, Fink JL, Freeman PR, Kirsh KL, Steinke DT, Talbert JC. Independent Evaluation of the Impact and Effectiveness of the Kentucky All Schedule Prescription Electronic Reporting Program (KASPER). 2010. http://chfs.ky.gov/NR/rdonlyres/24493B2E-B1A1-4399-89AD-1625953BAD43/0/KASPEREvaluationFinalReport10152010.pdf. Ac-cessed November 10, 2010.
28. Sorg M, LaBrie S, Parker W. Analysis and evaluation of participation by prescribers and dispensers in the Maine state prescription monitoring program. 2009. http://mcspolicycenter.umaine.edu/files/pdf/PMP%20Report%20Final%20Nov09.pdf. Accessed July 24, 2012.
29. Fleming ML, Chandwani H, Barner JC, Weber SN, Okoro TT. Prescrib-ers and pharmacists requests for prescription monitoring program (PMP) data: does PMP structure matter? J Pain Palliat Care Pharmaco-ther. 2013;27(2):136-142.
30. Virginia Department of Health Professions. Virginia Prescription Moni-toring Program: 2012 program statistics. www.dhp.virginia.gov/dhp_programs/pmp/pmp_reports.asp. Accessed October 13, 2013.
31. Virginia Department of Health Professions. Third Quarter 2013 Pro-gram Statistics. 2014. www.dhp.virginia.gov/dhp_programs/pmp/pmp_reports.asp. Accessed May 1, 2014.
32. Tommasello AC. Substance abuse and pharmacy practice: what the community pharmacist needs to know about drug abuse and depen-dence. Harm Reduction Journal. 2004;1(3):263-271.
33. Wallace J. The pharmacist’s role in managing chronic opioid therapy. Curr Pain Headache Rep. 2006;10(4):245-252.
34. Brushwood DB. From confrontation to collaboration: collegial account-ability and the expanding role of pharmacists in the management of chronic pain. J Law Med Ethics. 2001;29(1):69-93.
35. Gasbarro R. Does the Rx look suspicious? Pharmacists need to strike a careful balance when handling questionable prescriptions for drugs with abuse potential. Am Drug. 1999;216(1):48(44).
36. Texas Department of Public Safety. Texas Prescription Program: Overview. www.txdps.state.tx.us/RegulatoryServices/prescription_program. Accessed December 6, 2013.
37. Dillman DA, Smyth JD, Christian LM. Internet, mail, and mixed-mode surveys: the tailored design method. 3rd ed. Hoboken, NJ: John Wiley and Sons, Inc; 2009.
38. Gavaza P, Brown CM, Lawson KA, et al. Examination of pharmacists’ in-tention to report serious adverse drug events (ADEs) to the FDA using the theory of planned behavior. Res Social Adm Pharm. 2011;7(4):369-382.
39. Griggs SK, Brown CM. Texas community pharmacists’ willingness to participate in pharmacist-initiated emergency contraception. J Am Pharm Assoc. 2007;47(1):48-57.
40. Wenthur CJ, Cross BS, Vernon VP, et al. Opinions and experiences of Indiana pharmacists and student pharmacists: the need for addiction and substance abuse education in the United States. Res Social Adm Pharm. 2013;9(1):90-100.
41. Texas Department of Public Safety. Texas Prescription Program: The Prescription Forms. 2011. www.txdps.state.tx.us/RegulatoryServices/prescription_program/prescriptionforms.htm. Accessed June 10, 2011.
Downloaded From: http://japha.org/ by a University of Houston User on 05/11/2014

Appendix 1
Survey of Pharmacists’ Perceptions Regarding Utilization of the Texas Prescription Drug Monitoring Program (PDMP) Database
In the very near future, the Texas Department of Public Safety (DPS) will provide pharmacists with access to patients’ controlled medication data via the Texas Prescription Drug Monitoring Program (PDMP). Information most likely available to you will include: patient name, date of birth, address, drug name, dosage, dispensing dates, pharmacy and prescriber information. We are interested in factors that would influence your intention to utilize the Texas PDMP database when it becomes available to you via a secure password protected website. When you receive prescriptions for controlled medications, we are interested in those instances when you: • Suspect a prescription is fraudulent or have questions about the patient-‐doctor relationship.
-‐Referred to in the questionnaire as PRESCRIPTION VALIDITY. • Want to confirm a legitimate medical need for the prescription or you suspect patient abuse or addiction.
-‐Referred to in the questionnaire as PATIENT NEED.
Please consider both VALIDITY of the prescription, as well as PATIENT NEED (as described above) when completing the survey below. For each item below (e.g., 1a, 1b, etc.) please circle the number that corresponds to your choice using the scales listed. INTENTIONS 1. When the validity of the prescription for controlled medication/patient need is in question…
a. I intend to utilize the PDMP database Extremely unlikely Neutral
Extremely likely
-‐3 -‐2 -‐1 0 1 2 3 b. I will try to utilize the PDMP database Definitely
false Neutral Definitely
true -‐3 -‐2 -‐1 0 1 2 3 c. I plan on utilizing the PDMP database Strongly
disagree Neutral Strongly agree
-‐3 -‐2 -‐1 0 1 2 3
PERCEPTIONS
2. When the validity of the prescription for controlled medication/patient need is in question, my utilizing the PDMP is a. Bad Neutral Good
-‐3 -‐2 -‐1 0 1 2 3
b. Inconvenient Neutral Convenient -‐3 -‐2 -‐1 0 1 2 3
c. Harmful Neutral Beneficial -‐3 -‐2 -‐1 0 1 2 3
d. Worthless Neutral Valuable
-‐3 -‐2 -‐1 0 1 2 3
e. Useless Neutral Useful -‐3 -‐2 -‐1 0 1 2 3
Proceed to next page
Downloaded From: http://japha.org/ by a University of Houston User on 05/11/2014
2
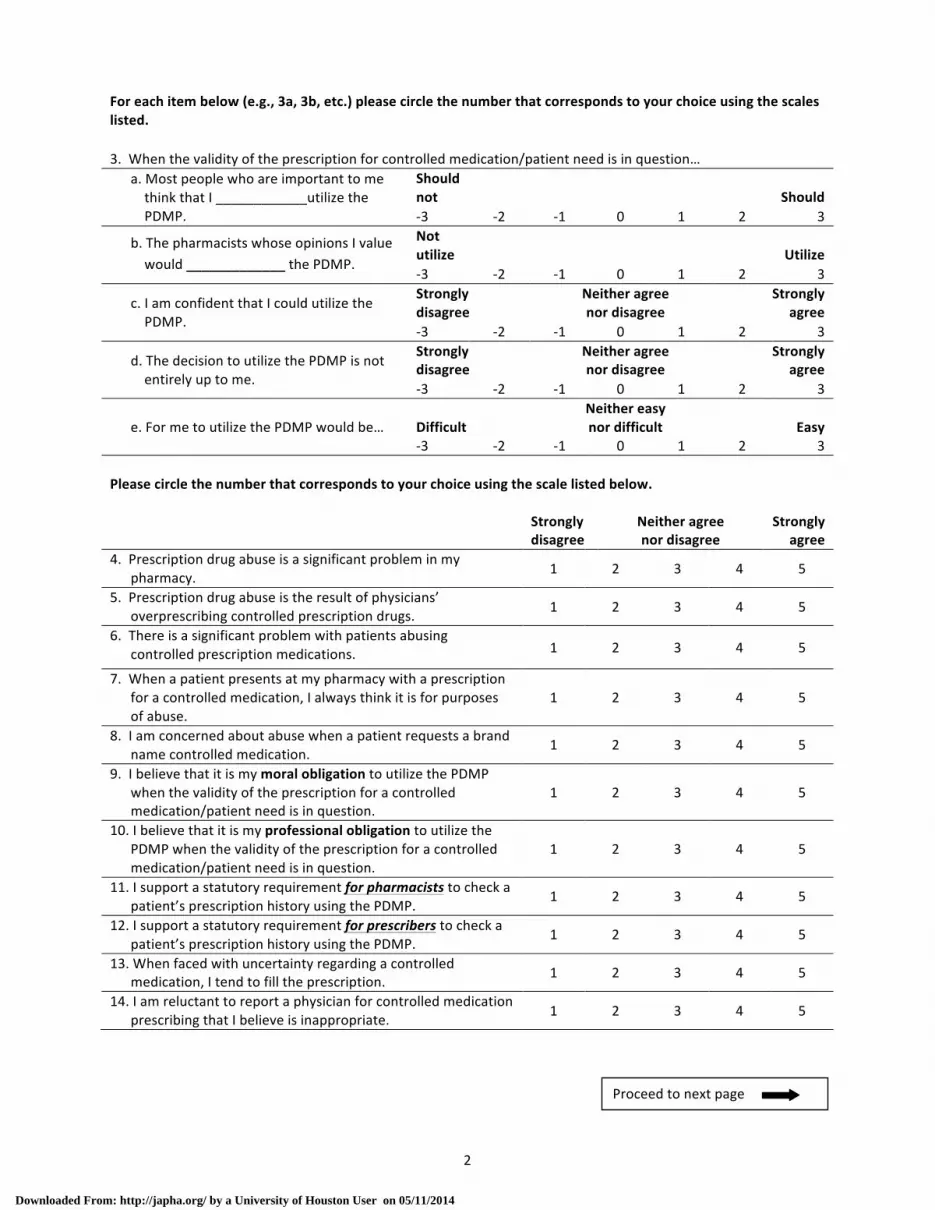
For each item below (e.g., 3a, 3b, etc.) please circle the number that corresponds to your choice using the scales listed. 3. When the validity of the prescription for controlled medication/patient need is in question…
a. Most people who are important to me think that I ____________utilize the PDMP.
Should not Should -‐3 -‐2 -‐1 0 1 2 3
b. The pharmacists whose opinions I value would _____________ the PDMP.
Not utilize Utilize -‐3 -‐2 -‐1 0 1 2 3
c. I am confident that I could utilize the PDMP.
Strongly disagree
Neither agree nor disagree
Strongly agree
-‐3 -‐2 -‐1 0 1 2 3
d. The decision to utilize the PDMP is not entirely up to me.
Strongly disagree
Neither agree nor disagree
Strongly agree
-‐3 -‐2 -‐1 0 1 2 3
e. For me to utilize the PDMP would be… Difficult Neither easy nor difficult Easy
-‐3 -‐2 -‐1 0 1 2 3 Please circle the number that corresponds to your choice using the scale listed below.
Strongly disagree
Neither agree nor disagree
Strongly agree
4. Prescription drug abuse is a significant problem in my pharmacy. 1 2 3 4 5
5. Prescription drug abuse is the result of physicians’ overprescribing controlled prescription drugs. 1 2 3 4 5
6. There is a significant problem with patients abusing controlled prescription medications. 1 2 3 4 5
7. When a patient presents at my pharmacy with a prescription for a controlled medication, I always think it is for purposes of abuse.
1 2 3 4 5
8. I am concerned about abuse when a patient requests a brand name controlled medication.
1 2 3 4 5
9. I believe that it is my moral obligation to utilize the PDMP when the validity of the prescription for a controlled medication/patient need is in question.
1 2 3 4 5
10. I believe that it is my professional obligation to utilize the PDMP when the validity of the prescription for a controlled medication/patient need is in question.
1 2 3 4 5
11. I support a statutory requirement for pharmacists to check a patient’s prescription history using the PDMP.
1 2 3 4 5
12. I support a statutory requirement for prescribers to check a patient’s prescription history using the PDMP.
1 2 3 4 5
13. When faced with uncertainty regarding a controlled medication, I tend to fill the prescription. 1 2 3 4 5
14. I am reluctant to report a physician for controlled medication prescribing that I believe is inappropriate. 1 2 3 4 5
Proceed to next page
Downloaded From: http://japha.org/ by a University of Houston User on 05/11/2014

3
PERCEPTIONS ABOUT POTENTIAL OUTCOMES OF PDMP Next, we would like to determine your beliefs about utilizing the Texas controlled prescription medication database. Please circle the number that corresponds to your choice using the scales listed below. 15. How likely do you think the following outcomes will be if you utilize the PDMP when the validity of the
prescription for controlled medication/patient need is in question? Very
unlikely Neutral Very likely
a. Decrease doctor shopping -‐3 -‐2 -‐1 0 1 2 3
b. Deny controlled medication based on inaccurate data in the PDMP
-‐3 -‐2 -‐1 0 1 2 3
c. Decrease diversion of controlled medication -‐3 -‐2 -‐1 0 1 2 3
d. Violate patient privacy (HIPAA) -‐3 -‐2 -‐1 0 1 2 3
e. Increase risk of pharmacist liability -‐3 -‐2 -‐1 0 1 2 3
f. Consume too much time to access data -‐3 -‐2 -‐1 0 1 2 3
g. Improve appropriate controlled medication use -‐3 -‐2 -‐1 0 1 2 3
h. Decrease pharmacy hopping (i.e., using multiple pharmacies)
-‐3 -‐2 -‐1 0 1 2 3
i. Decrease pharmacy profitability -‐3 -‐2 -‐1 0 1 2 3
16. Even though you may not agree with the outcomes listed, how good or bad do you feel each of the following
outcomes would be if you utilize the PDMP when the validity of the prescription for controlled medication/patient need is in question?
Extremely bad Neutral
Extremely good
a. Decrease doctor shopping -‐3 -‐2 -‐1 0 1 2 3
b. Deny controlled medication based on inaccurate data in the PDMP
-‐3 -‐2 -‐1 0 1 2 3
c. Decrease diversion of controlled drugs -‐3 -‐2 -‐1 0 1 2 3
d. Violate patient privacy (HIPAA) -‐3 -‐2 -‐1 0 1 2 3
e. Increase risk of pharmacist liability -‐3 -‐2 -‐1 0 1 2 3
f. Consume too much time to access data -‐3 -‐2 -‐1 0 1 2 3
g. Improve appropriate controlled medication use
-‐3 -‐2 -‐1 0 1 2 3
h. Decrease pharmacy hopping (i.e., using multiple pharmacies)
-‐3 -‐2 -‐1 0 1 2 3
i. Decrease pharmacy profitability -‐3 -‐2 -‐1 0 1 2 3
Proceed to next page
Downloaded From: http://japha.org/ by a University of Houston User on 05/11/2014

4
PERCEPTIONS AND INFLUENCE OF INDIVIDUALS OR GROUPS Next we are interested in what individuals or groups would influence your intention to utilize the PDMP. Please circle the number that corresponds to your choice using the scales listed below. 17. How likely is it that each of the following individuals or groups would think that you should utilize the PDMP
when the validity of the prescription for controlled medication/patient need is in question? Very
unlikely Neutral Very likely
a. Regulatory agencies/law enforcement (e.g., TSBP, DPS, DEA)a
-‐3 -‐2 -‐1 0 1 2 3
b. Pharmacy owners/employers -‐3 -‐2 -‐1 0 1 2 3
c. Prescribers (e.g., MD, NP, PA)b -‐3 -‐2 -‐1 0 1 2 3
d. Patients -‐3 -‐2 -‐1 0 1 2 3
e. Patient privacy advocates -‐3 -‐2 -‐1 0 1 2 3
f. Pharmaceutical manufacturers/wholesalers -‐3 -‐2 -‐1 0 1 2 3
g. Other pharmacists -‐3 -‐2 -‐1 0 1 2 3 aTSBP-‐Texas State Board of Pharmacy; DPS-‐Texas Department of Public Safety; DEA-‐Drug Enforcement Administration bMD-‐Medical Doctor; NP-‐Nurse Practitioner; PA-‐ Physician Assistant
18. Generally speaking, how likely are you to do what the following individuals or groups would want you to do
when it comes to utilizing the PDMP when the validity of the prescription for controlled medication/patient need is in question? Very
unlikely Neutral Very
likely a. Regulatory agencies/law enforcement
(e.g., TSBP, DPS, DEA)a -‐3 -‐2 -‐1 0 1 2 3
b. Pharmacy owners/employers -‐3 -‐2 -‐1 0 1 2 3
c. Prescribers (e.g., MD, NP, PA)b -‐3 -‐2 -‐1 0 1 2 3
d. Patients -‐3 -‐2 -‐1 0 1 2 3
e. Patient privacy advocates -‐3 -‐2 -‐1 0 1 2 3
f. Pharmaceutical manufacturers/wholesalers -‐3 -‐2 -‐1 0 1 2 3
g. Other pharmacists -‐3 -‐2 -‐1 0 1 2 3 aTSBP-‐Texas State Board of Pharmacy; DPS-‐Texas Department of Public Safety; DEA-‐Drug Enforcement Administration bMD-‐Medical Doctor; NP-‐Nurse Practitioner; PA-‐Physician Assistant
Proceed to next page
Downloaded From: http://japha.org/ by a University of Houston User on 05/11/2014
5
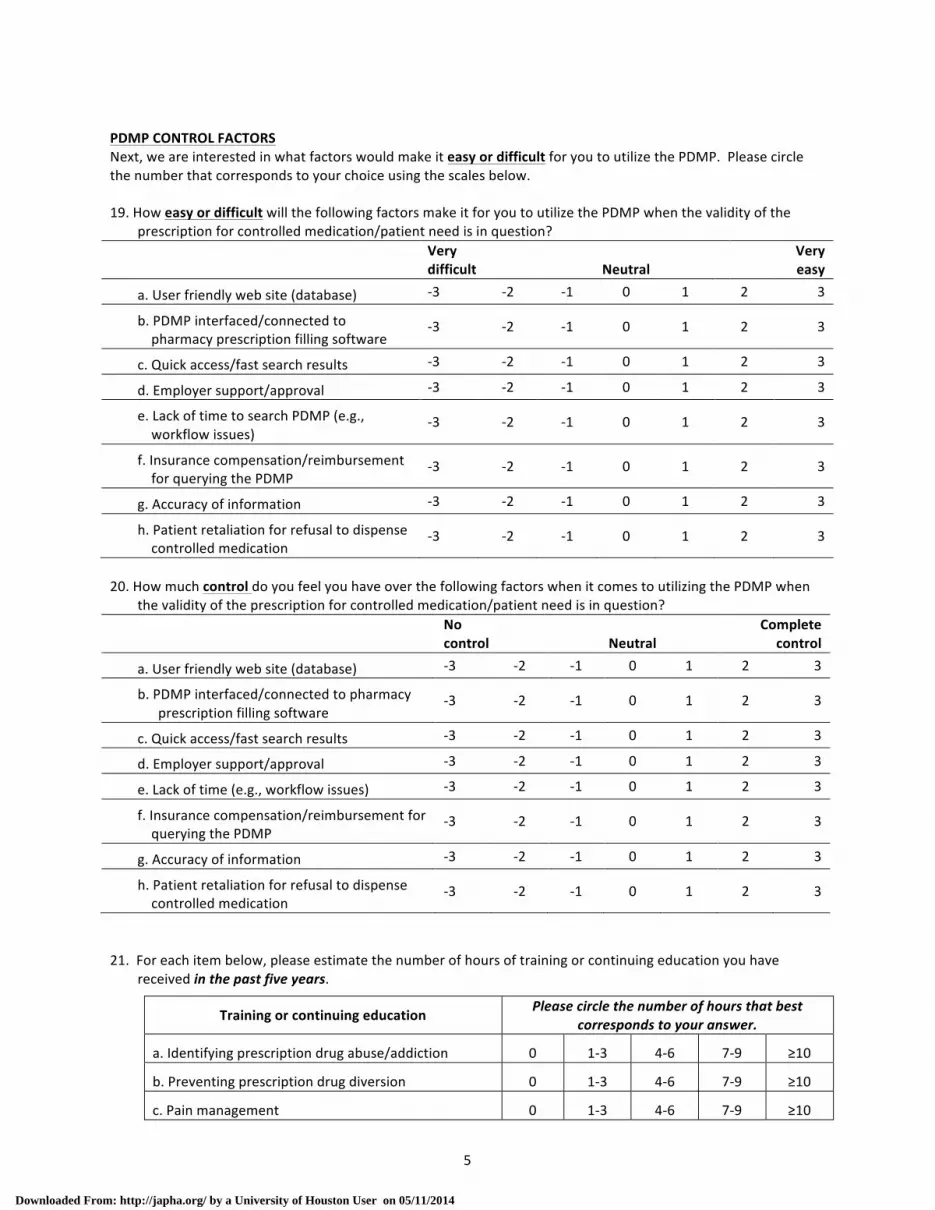
PDMP CONTROL FACTORS Next, we are interested in what factors would make it easy or difficult for you to utilize the PDMP. Please circle the number that corresponds to your choice using the scales below. 19. How easy or difficult will the following factors make it for you to utilize the PDMP when the validity of the
prescription for controlled medication/patient need is in question? Very
difficult Neutral Very easy
a. User friendly web site (database) -‐3 -‐2 -‐1 0 1 2 3
b. PDMP interfaced/connected to pharmacy prescription filling software
-‐3 -‐2 -‐1 0 1 2 3
c. Quick access/fast search results -‐3 -‐2 -‐1 0 1 2 3
d. Employer support/approval -‐3 -‐2 -‐1 0 1 2 3
e. Lack of time to search PDMP (e.g., workflow issues)
-‐3 -‐2 -‐1 0 1 2 3
f. Insurance compensation/reimbursement for querying the PDMP
-‐3 -‐2 -‐1 0 1 2 3
g. Accuracy of information -‐3 -‐2 -‐1 0 1 2 3
h. Patient retaliation for refusal to dispense controlled medication
-‐3 -‐2 -‐1 0 1 2 3
20. How much control do you feel you have over the following factors when it comes to utilizing the PDMP when
the validity of the prescription for controlled medication/patient need is in question? No
control Neutral Complete
control
a. User friendly web site (database) -‐3 -‐2 -‐1 0 1 2 3
b. PDMP interfaced/connected to pharmacy prescription filling software
-‐3 -‐2 -‐1 0 1 2 3
c. Quick access/fast search results -‐3 -‐2 -‐1 0 1 2 3
d. Employer support/approval -‐3 -‐2 -‐1 0 1 2 3
e. Lack of time (e.g., workflow issues) -‐3 -‐2 -‐1 0 1 2 3
f. Insurance compensation/reimbursement for querying the PDMP
-‐3 -‐2 -‐1 0 1 2 3
g. Accuracy of information -‐3 -‐2 -‐1 0 1 2 3
h. Patient retaliation for refusal to dispense controlled medication
-‐3 -‐2 -‐1 0 1 2 3
21. For each item below, please estimate the number of hours of training or continuing education you have
received in the past five years.
Training or continuing education Please circle the number of hours that best corresponds to your answer.
a. Identifying prescription drug abuse/addiction 0 1-‐3 4-‐6 7-‐9 ≥10
b. Preventing prescription drug diversion 0 1-‐3 4-‐6 7-‐9 ≥10
c. Pain management 0 1-‐3 4-‐6 7-‐9 ≥10
Downloaded From: http://japha.org/ by a University of Houston User on 05/11/2014

6
PHARMACISTS’ ACTIONS Next, we would like to know how you generally handle situations related to suspected diversion, abuse, and dispensing of controlled prescription medications in your pharmacy.
22. How often would the following trigger you to utilize the PDMP database? Never Sometimes Always
a. New patient 1 2 3 4 5 b. Patient prefers to pay cash 1 2 3 4 5 c. Mistakes or irregularities in the written prescription 1 2 3 4 5 d. Refill request that is too early 1 2 3 4 5 e. Please list any other triggers
23. When you are dispensing a controlled prescription medication, how often do you perform the following tasks? Never Sometimes Always
a. Consult patient records that you have access to before dispensing the drug 1 2 3 4 5
b. Validate the prescriber’s DEA number 1 2 3 4 5 c. Ask if the patient is taking any other controlled medications 1 2 3 4 5 d. Verify the identification of patients prior to dispensing prescriptions for controlled medications 1 2 3 4 5
e. Discuss treatment with buprenorphine (Subutex®) or buprenorphine/naloxone (Suboxone®) with patients or prescribers if you suspect opioid addiction
1 2 3 4 5
f. Please list any other tasks
24. If you suspected a patient of abusing controlled drugs, you would…
Strongly disagree
Neither agree nor disagree
Strongly agree
a. Notify law enforcement 1 2 3 4 5 b. Refuse to fill the prescription 1 2 3 4 5 c. Call the prescriber 1 2 3 4 5 d. Document the incident 1 2 3 4 5 e. Counsel patient about addiction 1 2 3 4 5
Strongly disagree
Neither agree nor disagree
Strongly agree
25. Opioid addiction should be managed by pharmacists similar to other chronic diseases (e.g., hypertension)? 1 2 3 4 5
DEMOGRAPHIC/PRACTICE CHARACTERISTICS Finally, we would like to know a little about you and your practice setting. Please check the response or write in your responses where appropriate. 26. What is your gender? ! Female ! Male 27. What year were you born? ____________
Proceed to next page
Proceed to next page
Downloaded From: http://japha.org/ by a University of Houston User on 05/11/2014

7
28. Which of the following best describes your ethnic/racial background? Please check all that apply.
! African American/non-‐Hispanic Black ! Caucasian/non-‐Hispanic White ! American Indian or Alaska Native ! Mexican American/Hispanic ! Asian American/Pacific Islander ! Other (please specify): ___________
29. What is your highest level of pharmacy education?
! B.S. Pharmacy ! M.S. Pharmacy or Residency ! Pharm.D. ! Other (please specify): _______________
30. Which of the following best describes your current primary practice setting? ! Community Independent (3 or fewer stores under common ownership) ! Community Chain (4 or more stores under common ownership; e.g., CVS, Walgreens) ! Grocery Store Chain (e.g., Kroger, HEB) ! Mass Merchandiser (e.g., Target, Walmart) ! Outpatient/Clinic Pharmacy ! Other (please specify): ____________
31. On average, how many prescriptions does your pharmacy fill per day? __________ prescriptions per day 32. Does your pharmacy have internet access? ! Yes ! No ! Unsure 33. What is your current pharmacist position/title at your primary place of employment?
! Relief/PRN ! Owner ! Staff ! Other (please specify): ___________ ! Manager/Pharmacist-‐in-‐charge
34. Are you employed full-‐time or part-‐time at your primary work site? ! Full-‐time (greater than or equal to 30 hours per week)
! Part-‐time (less than 30 hours per week)
35. How many years have you been practicing community pharmacy? ________years 36. Which of the following best describes your primary practice location? ! Rural ! Suburban ! Urban Please provide any other comments that you may have in the box below. If you would like to receive an aggregate summary of the results, please email Marc Fleming at [email protected]. Please fold the questionnaire and place it in the enclosed envelope. Seal the envelope and drop it in any mailbox. No postage is necessary.
THANK YOU FOR YOUR PARTICIPATION!
Downloaded From: http://japha.org/ by a University of Houston User on 05/11/2014





























