Embed Size (px)
Citation preview

Substance Abuse, Vol. 20, No. 1, 1999
A Pilot Project: Continuing Education for Pharmacistson Substance Abuse Prevention
Antonnette Graham, Ph.D.,1,5 Judie Pfeifer, M.Ed.,2 Jeanne Trumble, M.S.W.,3and E. Don Nelson, Pharm.D.4
The American Association of Colleges of Pharmacy advocates that pharmacistscan have a significant impact on substance abuse prevention provided they receiveadequate training. Continuing education programs are needed to enable practicingpharmacists to augment their limited education. This paper examines the processthe Society of Teachers of Family Medicine (STFM) used to develop a pilotcontinuing education program for pharmacists. With limited literature and a smallnumber of pharmacy teaching about substance abuse, input on topics and trainingmethods was obtained from a convenience sample of practicing pharmacists toenhance the information from the pharmacist faculty regarded as content experts.Results of this pilot study revealed lack of agreement between faculty and practicingpharmacists regarding the prioritizing of content and educational methods. Conse-quently, input must be obtained from targeted audiences instead of relying solelyon the advice of identified academic content experts when designing continuingeducational programs. Other professions should consider this process when design-ing continuing education programs. Pharmacists are poised to play an importantrole in the prevention of substance abuse problems, but they need continuingeducation about substance abuse.
1Department of Family Medicine, School of Medicine, Case Western Reserve University, Cleveland,Ohio.
2Department of Family Medicine, School of Medicine, University of Wisconsin—Madison, Madison, Wis-consin.
3American Academy of Addiction Psychiatry, Prairie Village, Kansas.4Department of Pharmacology and Cell Biophysics, School of Medicine, University of Cincinnati, Cincin-nati, Ohio.
To whom correspondence should be addressed at Department of Family Medicine, Case WesternReserve University, 10900 Euclid Avenue, Cleveland, Ohio 44106-4950.
KEY WORDS: continuing education; prevention; substance abuse; pharmacists.
33
0889-7077/99/0300-0033$16.00/1 © 1999 Association for Medical Education and Research in Substance Abuse

INTRODUCTION
In 1993, the Society of Teachers of Family Medicine (STFM) was awarded the"Health Care Professional Training and Technical Assistance—Medical SpecialistsContract" from the Center for Substance Abuse Prevention (CSAP). The purposeof the contract was to design, develop, and deliver continuing education programsfor dentists, pharmacists, physicians, and physician assistants to improve their knowl-edge, skills, and attitudes regarding substance abuse prevention. The contract fo-cused on preparing these professionals to integrate prevention concepts and behav-iors into their practices and on encouraging them to become involved in a range ofcommunity-based prevention activities. Curricula were developed for the physician,dental, and physician assistants professions by a core team representing universityfaculty from each respective discipline. The curricula were based on the faculty'sextensive teaching experiences and were supported by an ample literature reviewregarding substance abuse education. The curriculum was delivered at daylongcontinuing educational programs.
Developing curriculum for the pharmacy profession could not follow the abovemodel. The medical, dental, and physician assistant professions had an ample litera-ture and educational experts to guide their curriculum development, but pharmacyeducation did not. A literature search revealed that pharmacists receive little informa-tion during their formal academic education about substance abuse and few pharmacyeducational content experts could be identified. A vast literature exists regarding theavailability of information on program planning for professional education (1-4), butno citations were found regarding continuing education programs on substance abusefor practicing pharmacists. Because of these limitations, the STFM project team de-cided to survey practicing pharmacists and the academic pharmacy professionals whocould be identified as substance abuse content experts regarding critical topics andapplicable formats for a substance abuse continuing education program. Current liter-ature holds a wealth of information supporting the value of the pharmacist's role indrug abuse prevention such as counseling smokers who ask about nicotine patches,informing patients/customers about fetal alcohol syndrome, labeling medications thatinteract with alcohol, warning clients about mixing alcohol with prescription drugs,and providing guidance to clients who purchase needles and syringes (5-7). However,since pharmacists lack the educational background, most are not prepared to performthese tasks as effectively as possible.
This paper focuses on pharmacists' need for continuing substance abuse preven-tion education, the process used in developing a pilot continuing educational curricu-lum project and direction for others interested in developing programs for pharma-cists or other health care professionals. It describes a process used for curriculardevelopment when limited background literature in the content of interest, i.e.,alcohol and drug abuse education, is available. It points out the hazards in assumingthat academic content experts can identify the topics and methods of instructionthat practicing professionals desire in continuing education programs. Finally, itdescribes important functions pharmacists can perform as part of the health careteam to improve patient care and decrease costs if they have adequate knowledgeabout substance abuse prevention.
Graham, Pfeifer, Trumble, and Nelson34
Continuing Education for Pharmacists on Abuse Prevention
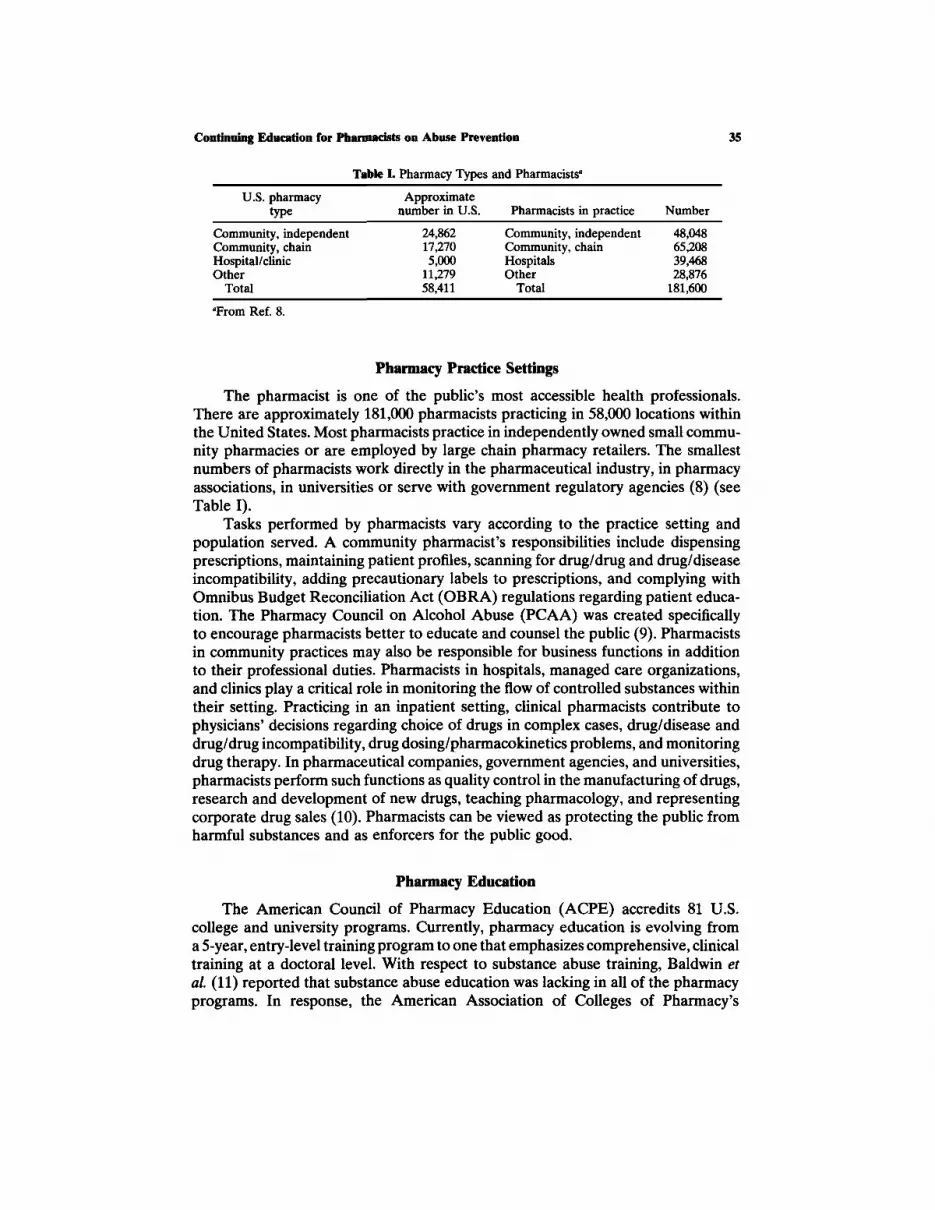
Table I. Pharmacy Types and Pharmacistsa
U.S. pharmacytype
Community, independentCommunity, chainHospital/clinicOther
Total
Approximatenumber in U.S.
24,86217,2705,000
11,27958,411
Pharmacists in practice
Community, independentCommunity, chainHospitalsOther
Total
Number
48,04865,20839,46828,876
181,600aFrom Ref. 8.
Pharmacy Practice Settings
The pharmacist is one of the public's most accessible health professionals.There are approximately 181,000 pharmacists practicing in 58,000 locations withinthe United States. Most pharmacists practice in independently owned small commu-nity pharmacies or are employed by large chain pharmacy retailers. The smallestnumbers of pharmacists work directly in the pharmaceutical industry, in pharmacyassociations, in universities or serve with government regulatory agencies (8) (seeTable I).
Tasks performed by pharmacists vary according to the practice setting andpopulation served. A community pharmacist's responsibilities include dispensingprescriptions, maintaining patient profiles, scanning for drug/drug and drug/diseaseincompatibility, adding precautionary labels to prescriptions, and complying withOmnibus Budget Reconciliation Act (OBRA) regulations regarding patient educa-tion. The Pharmacy Council on Alcohol Abuse (PCAA) was created specificallyto encourage pharmacists better to educate and counsel the public (9). Pharmacistsin community practices may also be responsible for business functions in additionto their professional duties. Pharmacists in hospitals, managed care organizations,and clinics play a critical role in monitoring the flow of controlled substances withintheir setting. Practicing in an inpatient setting, clinical pharmacists contribute tophysicians' decisions regarding choice of drugs in complex cases, drug/disease anddrug/drug incompatibility, drug dosing/pharmacokinetics problems, and monitoringdrug therapy. In pharmaceutical companies, government agencies, and universities,pharmacists perform such functions as quality control in the manufacturing of drugs,research and development of new drugs, teaching pharmacology, and representingcorporate drug sales (10). Pharmacists can be viewed as protecting the public fromharmful substances and as enforcers for the public good.
Pharmacy Education
The American Council of Pharmacy Education (ACPE) accredits 81 U.S.college and university programs. Currently, pharmacy education is evolving froma 5-year, entry-level training program to one that emphasizes comprehensive, clinicaltraining at a doctoral level. With respect to substance abuse training, Baldwin etal. (11) reported that substance abuse education was lacking in all of the pharmacyprograms. In response, the American Association of Colleges of Pharmacy's
35

Graham, Pfeifer, Trumble, and Nelson
(AACP) Substance Abuse Education and Assistance Special Interest Group (SIG)prepared curriculum guidelines. The recommended course content included psy-chosocial aspects of alcohol and other drug use; pharmacology and toxicology ofabused substances; identification, intervention, and treatment of people with ad-dictive diseases; and legal issues. The final goal was to identify the potential roleof the pharmacist in community drug abuse education and prevention.
In 1993, the AACP established a Committee on Substance Abuse CourseContent. The Committee conducted a survey to determine the implementation rateof the new curricular guidelines. An 83% (N = 62) response rate was obtained (12)(see Table II). Approximately half of the respondents indicated changing theirexisting substance abuse curriculum to include either a required or an electivecourse.
Role of the Pharmacist in the Prevention of Substance Abuse Problems
Pharmacists have one of the best positions in the health care delivery networkto provide consumer information and counseling about substance abuse. Recentpublic polls (13) indicate that pharmacists are viewed as the most trusted healthprofessionals on scales of honesty and ethical standards. Pharmacists' knowledgeof pharmacology, toxicology, drug interactions, and drug therapy makes them aconvenient and reliable source of substance abuse information.
METHODS
In order to obtain information regarding pertinent content and relevant formatfor continuing education, input was gathered from interviews with practicing phar-macists and pharmacists identified as academic substance abuse content experts.In July 1995 members of the STFM project team conducted one-on-one interviewswith 21 practicing pharmacists. This convenience sample included female and malepharmacists and pharmacists from a variety of work settings and diverse geographiclocations. A standardized format developed for the interview was used to collectthe information. Three pharmacists were specified as academic substance abusecontent experts based upon their substance abuse knowledge, their familiarity withcurriculum developed for pharmacy education, and their experience in substance
36
Table II. Percentage of Programs Implementing Various Aspects of Recommended SubstanceAbuse Curriculuma
PsychosocialPharmacology/toxicologyIdentification/intervention/treatmentLegal issues
Required curriculum (%)
41633954
Elective curriculum (%)
44434029
aFrom Ref. 11.

abuse prevention programs. Although there is a mandate to increase alcohol anddrug education in pharmacy education, as of yet, there is not a cadre of identifiedcore pharmacy faculty with substance abuse expertise. Because the requirementsfor being designated a content expert ensured knowledge regarding the curricularneeds necessary for an adequate pharmacy education in substance abuse, only threepersons could be identified nationally.
RESULTS
Delivery Methods
In response to questions regarding the best system for delivering continuingsubstance abuse prevention education (see Table III), practicing pharmacists pre-ferred that substance abuse training be included in the university curricula or bedisseminated to practitioners in the field via seminars and journal articles. Methodssuch as satellite broadcasts, computerized programs, and other electronic deliverysystems were the least preferred delivery system among practitioners. Contentexperts, however, preferred the technical educational delivery systems (electronic,satellite, computer) over conventional instructional and training methods. Bothhighly rated the use of continuing education seminars.
Educational Needs
The practicing pharmacists listed information about street drug patterns astheir top priority, while the content experts felt that the need for more information
Table III. Summary Ranking of Survey Question: The Best Way toEducate/Train Pharmacists About Alcohol, Tobacco, and Other
Drug (ATOD) Prevention Is ...
Response
Pharmacy school curriculumLocal CEU seminarsJournal articlesNational/regional meetingsSelf-instructed pencil/paperSelf-instructed electronicTV satelliteATOD briefing material800/900 phone numbersComputer CDs/software
Rank
Practicingpharmacists
(n = 21)
123456789
10
Contentexperts(n = 3)
2366541471
Continuing Education for Pharmacists on Abuse Prevention 37

Graham, Pfeifer, Trumble, and Nelson
Table IV. Summary Ranking of Survey Question: What Aspects ofPharmacists' Knowledge Base About Alcohol, Tobacco, and Other Drug
Most Need Educational Attention?
Response
Street drug patternsMed/psy aspects of alcoholTreatment of substance abuse problemsLocal treatment programsPharmacology of street drugsInteractions — street/scripts/alcoholLegal aspects — drug distribution
Rank
Practicingpharmacists
(n = 21)
1234567
Contentexperts(n = 3)
5321674
about local treatment was of premier importance (see Table IV). Information aboutmedical/psychiatric aspects and treatment of substance abuse problems were listedsecond and third by each group, however, practicing pharmacists felt that themedical psychiatric aspect was more important than the treatment of substanceabuse, and the content experts felt that the opposite was true. The other topicswere prioritized quite differently.
Abuse Prevention
With respect to the pharmacists' role in abuse prevention, again there wasvariation between the practicing pharmacists' and the content experts' responses(Table V). Practicing pharmacists felt that their greatest role in substance abuseprevention activities was giving patient advice, talking with community and schoolgroups, and providing handout literature. Content experts agreed that pharmacistsshould give talks to community and school groups, but felt that they should target
Table V. Summary Ranking of Survey Question: How Do You EnvisionPharmacists Engaging in Alcohol, Tobacco, and Other Drug (ATOD)
Prevention Activities?
Response
Giving patient adviceGiving talks to community/school groupsProviding handoutsTargeting populations (youth, women)Changing curriculumChanging alcohol/tobacco lawsMedia ATOD prevention campaignsWorking in national organizationsDisplaying posters
Rank
Practicingpharmacists
(n = 21)
123456789
Contentexperts(n = 3)
617145236
38

Continuing Education for Pharmacists on Abuse Prevention
Table VI. Summary Ranking of Survey Question: What Are Pharmacists'Greatest Strengths for Doing Prevention Work?
Response
Daily contact with publicOpportunity to deal with interactionsActive and visible in communityKnowledge of drugsVery organized
Rank
Practicingpharmacists
(n = 21)
12345
Contentexperts(n = 3)
23415
specific groups and be involved with media prevention campaigns. Table VI illus-trates that practicing pharmacists rank their daily contact with the public as theirprimary strength in conducting prevention activities, while the content experts feltthat the pharmacists' strength lay in their overall knowledge of drugs. Table VIIshows that both practicing pharmacists and content experts viewed basic preventioninformation as pharmacists' greatest ATOD need.
DISCUSSION
The limited amount of information in the literature about continuing educationprograms on substance abuse prevention for pharmacists and the scant number ofcontent experts point to the need for increased curriculum development for practic-ing pharmacists. The educational need is augmented by knowledge of the valuableroles pharmacists can play in the prevention of substance abuse, the improvementin patient care, and the decrease in health care costs if they have expertise insubstance abuse prevention. Pharmacists have not had the educational opportunitiesthat other health care professionals have obtained regarding substance abuse educa-tion. This initiative from CSAP to STFM is one of the first federal programs toinclude pharmacists. Although much more work has to be done regarding substanceabuse education for the pharmacy profession, this paper points out some beginningareas of importance.
Table VII. Summary Ranking of Survey Question: What Are Pharmacists'Greatest Alcohol, Tobacco, and Other Drug Prevention Needs?
Response
Basic information about preventionPackaged information/ideasInformation on community resourcesExamine preventive attitudes
Rank
Practicingpharmacists
(n = 21)
1234
Contentexperts(n = 3)
1321
39

Because of the limited literature on substance abuse education for pharmacists,information from faculty content experts was obtained and broadened by surveyinga convenience sample of practicing pharmacists. Comparing the information fromthe practicing pharmacists and the content experts revealed variability regardingthe best delivery method for training, the knowledge required, and the role andstrength of the pharmacists in drug abuse prevention activities.
The pharmacists' ranking of educational delivery systems is consistent with a1982 survey conducted by Nelson (14) regarding preferred teaching/training formatsthat indicated that practicing pharmacists preferred lecture/discussion over othertraining methods. With the proliferation of technology in the 14 years since Nelson'sstudy, one would expect a shift toward technical delivery systems. The continuingpreference for traditional teaching methods may be related to the practitioner'sfamiliarity with lecture/discussion as the method most utilized in university prepara-tion programs.
The response inconsistency among the two groups could also be the result ofdiffering levels of technical literacy and availability of technology. According tomany of the practicing pharmacists surveyed, computer and/or electronic technologyis not readily available or widely used in community practice settings and, therefore,is not a viable instructional choice. Networking capabilities are especially out ofreach for most independent pharmacists or pharmacists in small community prac-tices. Other practitioners commented that they were computer illiterate and wouldhave no interest in computer-driven educational programming. In contrast, contentexperts usually work in university settings and their environments more frequentlyincorporate technology in conducting day-to-day operations. Consequently, theymay be unfamiliar with the lack of computer literacy and technology in the private,community-based settings.
The ranking of daily contact with the public as their primary strength in conduct-ing prevention activities by practicing pharmacists is consistent with the public pollfindings on trust in pharmacists. The value of contact with the public is also supportedby Brown's (15) suggestions for the role that pharmacists play in prevention. Hisspecifications for pharmacists in drug abuse prevention include advising patientsabout potential abused drug-therapeutic drug interactions, providing informationto shift attitudes against substance abuse and participating in community substanceabuse activities. Similarly, MacDonald (16) supports the role of pharmacists in drugeducation and prevention and identifies the crucial role of alerting people to theconsequences of drug use.
In addition to OBRA at the federal level, most states now have laws mandatingpharmacies to provide some form of patient counseling, which according to Ringel(17), usually must be face-to-face with a pharmacist. The state mandate for counsel-ing and the trust the American public has in pharmacists offers them the optimalopportunity to provide prevention messages. Bohach (18) claimed that pharmacistshave "both a moral and a professional responsibility" to fight actively against drugabuse. However, to be a viable partner in the fight against drug abuse, pharmacistsmust first be educated about addiction; second, be acquainted with resources thatprovide current information about drug abuse; and third, be given practical ideason incorporating drug abuse prevention and education activities into the day-to-
40 Graham, Pfeifer, Trumble, and Nelson

day operations of community pharmacy practice. Ringel (17) further notes thatpatient drug education and counseling not only can be cost effective, but may alsoimprove patient outcomes.
Additional comments offered by the practicing pharmacists suggested thatHMOs and other managed-care pharmacy settings are ideal sites in which to pilota pharmacist substance abuse prevention program. These respondents felt that, inthe HMO setting, cutting costs by diminishing prescription abuse, as well as alcoholand tobacco use, would act as an incentive to motivate pharmacists to obtaincontinuing education on substance abuse concerns. Heenan (19) postulates that awell-designed managed care prescription drug benefit program can contribute tooverall higher-quality and more cost-effective patient care. In discussing the roleof the pharmacists in the overall managed care plan, Ringel (17) suggests thatthe pharmacists should have a role in reviewing physicians' prescribing practices.Although not mentioned by either the practicing pharmacists or the content experts,pharmacists can provide a prevention service by giving feedback to physiciansregarding refill patterns of controlled substances. Prescription abuse must not beoverlooked as a source of drug problems for patients. All too often, thinking aboutdrug abuse is limited to illegal drug use, whereas the misuse of legal drugs or theinteraction with alcohol is forgotten. For example, Graham and Parran (20) foundfew physicians document having asked about the use of alcohol prior to prescribingbenzodiazepines.
Von Ferber et al. (21) note that drugs often seem to be prescribed forirrational reasons in primary health care. When the prescriptions of primary healthcare providers were analyzed and discussed with the physicians, a remarkableimprovement in the quality and cost effectiveness of drug therapy was noted.Physicians who were offered personal educational visits by clinical pharmacistsalong with a series of mailed "unadvertisements" reduced their prescribing ofthe target drugs by 14% compared with controls (22). In an analysis of theeconomic effects of an experimental educational outreach program by clinicalpharmacists with 435 physicians, it was estimated that implementation of theprogram for 10,000 physicians would lead to projected drug savings (to Medicaidonly) of $2,050,000, compared with resource costs of $940,000 (23). Johnson andBootman (24) reported that drug-related morbidity and mortality cost the UnitedStates economy more than $76 billion annually in direct patient care expenditures,account for 28.9% of all hospital admissions, and cause 200,000 deaths. Alliancesbetween prescribing physicians and pharmacists are extremely valuable in con-taining costs associated with Pharmaceuticals and providing consistent, reinforcingmessages to the public. The result is a healthier bottom line that balances qualityand costs.
Limitations in this paper focus on the sample. The sample may not be represen-tative since it is small and was not randomized. The practicing pharmacists moreinterested in this topic may have been more likely to respond to the request to beinterviewed. Further, the differences noted between the two groups could merelybe an artifact, the result of predictable, random variation among groups. Futurestudies, building on these preliminary data, need to secure a larger, more representa-tive sample.
Continuing Education for Pharmacists on Abuse Prevention 41
CONCLUSION
The literature clearly supports the notion that pharmacists are potentiallypowerful drug abuse prevention agents provided they are given the necessary train-ing and materials to be effective. This pilot project suggests the importance offormats that are adaptable to various practice settings as well as to a variety ofpersonal learning styles or preferences as a critical aspect in developing substanceabuse curricula for practicing pharmacists. Before developing programming, thispilot project points out the significance of obtaining input from the practicingpharmacists regarding topics and formats. For the enhancement of patient safetyand cost containment, the pharmacist's role in the health care team should beincreased. Consequently, continuing education must increase so that the pharmacistcan assume a more integrated active role in the prevention of substance abuseproblems.
ACKNOWLEDGMENTS
The authors acknowledge collaboration in the design and implementation ofthis project by the other members of the CSAP Medical Specialists Program Team:Michael Fleming, M.D., M.P.H., James Finch, M.D., Richard Blondell, M.D., Rich-ard Brown, M.D., M.P.H., Ardis Davis, M.S.W., Carmela Cannova, M.B.A., andRoger Sherwood, C.A.E. This work was supported in part by Contract 277-93-1029 from the Center for Substance Abuse Prevention to the Society of Teachersof Family Medicine.
REFERENCES
1. Cevero RM: Effective Continuing Education for Professionals. San Francisco: Jossey-Bass; 19882. Heimlich JE, Norland E: Developing Teaching Style in Adult Education. San Francisco: Jossey-
Bass; 19943. Vella J: Learning to Listen, Learning to Teach: The Power of Dialogue in Educating Adults. San
Francisco: Jossey-Bass; 19944. Knox AB: Strengthening Adult Continuing Education. San Francisco: Jossey-Bass; 19935. Odd RW, Fowler G, Woodhouse K, Farren C, Henningfield JE, West R, Foulds J: Comments on
Foulds' editorial: Does nicotine replacement therapy work? Addiction 1994; 89(4):431-4396. Small WE: America's top problem drug. Am Pharm 1979; 19(13):57. Mayer-Frederick S: "Pharmacists: Warn your clients: "Drinks and drugs don't mix." Presented at
the North American Congress on Alcohol and Drug Problems, San Francisco, CA; Dec 22,19748. National Association of Chain Drug Stores: Overview of the U.S. chain drug store industry. Alexan-
dria, VA; July 5, 19959. Nelson ED: Pharmacists roles in alcohol and drug abuse services. Alcohol Health Res World
1983; 8(1):21-2310. Pharmacy Council on Alcohol Abuse Newsletter, undated11. Baldwin JN, Light KE, Stock C, Ives TJ, Crabtree BL, Miederhoff PA, Tommasello A, Levine PJ:
Curricular guidelines for pharmacy education: Substance abuse and addictive disease. Am J PharmEduc 1991; 55:311-316
12. Baldwin JN, Dole EJ, Levine PJ, Light KE, Murawski MM, Stock C, Tommasello A, WaterhouseGAW: Survey of pharmacy abuse substance course content. Am J Pharm Educ Suppl 1994; 58:478-51S, 157S-158S
42 Graham, Pfeifer, Trumble, and Nelson

13. Rural Health Research Center, Seattle, WA: Are rural independent pharmacies an endangeredspecies? Rural Health News, 1994; 1(3):1, 10
14. Nelson ED. Substance abuse education in pharmacy: Current status and needs. Report to theFederal Health Professions Task Force on Substance Abuse (HPTFSA); Apr 21, 1982
15. Brown RL: Alcohol and drug problems: Wisconsin pharmacists can make a difference. Wisc Pharm1995; Feb: 8-16
16. MacDonald DI: What is government's role in connection with prevention of drug abuse? PharmTimes 1987; 3(3):22-129
17. Ringel M: Look who's giving doctors clinical advice. Med Econ 1994; Nov 21:143-15418. Bohach C: Getting involved in drug abuse education and prevention. In: Redda KK, Walker CA,
Barnett G, eds., Cocaine, Marijuana, Designer Drugs: Chemistry, Pharmacology, and Behavior.Boca Raton, FL: CRC Press, 1989:31-37
19. Heenan J: Prescription drug benefits in a managed care plan: Balancing quality and costs. MedInterface 1994; 7(1):84-92
20. Graham AV, Parran TV, Jaen CR: Physician failure to record alcohol use history when prescribingbenzodiazepines. J Substance Abuse 1992; 4:179-185
21. Von Ferber L, Luciano A, Koster I, Krappweis J: Drug utilization research in primary healthcare as exemplified by physicians' quality assessment groups. Int J Clin Pharmacol Ther Toxicol1992; 30(11):453-455
22. Avorn J, Soumerai SB: Improving drug-therapy decisions through educational outreach: a random-ized controlled trial of academically based "detailing." N Engl J Med 1983; 308(24):57-63
23. Soumerai SB, Avorn J: Economic and policy analysis of university-based drug "detailing." MedCare 1986; 24(4):313-331.
24. Johnson JA, Bootman JL: Drug related morbidity and mortality: A cost-of illness model. ArchIntern Med 1995; 150:1949-1956
Continuing Education for Pharmacists on Abuse Prevention 43





























