Embed Size (px)
Citation preview

1998;31;992-1001 J. Am. Coll. Cardiol.Bernies, A Distante, I Marco, J Fajadet, and A Zanchetti
L Gregorini, J Marco, C Palombo, M Kozakova, GB Anguissola, B Cassagneau, M blocking agents
Postischemic left ventricular dysfunction is abolished by alpha-adrenergic
This information is current as of July 12, 2011
http://content.onlinejacc.orglocated on the World Wide Web at:
The online version of this article, along with updated information and services, is
by on July 12, 2011 content.onlinejacc.orgDownloaded from

MYOCARDIAL ISCHEMIA
Postischemic Left Ventricular Dysfunction Is Abolished byAlpha-Adrenergic Blocking Agents
LUISA GREGORINI, MD, FESC, JEAN MARCO, MD,* CARLO PALOMBO, MD,†MICHAELA KOZAKOVA, MD, PHD,† GIAN BATTISTA ANGUISSOLA, MD,BERNARD CASSAGNEAU, MD,* MONIQUE BERNIES, MD,*ALESSANDRO DISTANTE, MD, FESC,† ISABELLE MARCO, MD,* JEAN FAJADET, MD,*ALBERTO ZANCHETTI, MD, FESC
Toulouse, France and Milan and Pisa, Italy
Objectives. We sought to evaluate the efficacy of alpha-adrenergic blocking agents in counteracting left ventricular (LV)dysfunction occurring after transient ischemia in humans.
Background. The mechanisms underlying postischemic LVdysfunction are largely unknown.
Methods. Percutaneous transluminal coronary angioplasty(PTCA) provides a clinical model of ischemia and reperfusion. In50 patients undergoing coronary stenting for 77 6 5% stenosis, LVfunction was monitored by transesophageal echocardiographyduring and 30-min after PTCA. Fifteen minutes after stenting, 15patients received 12 mg/kg body weight of the alpha-blockerphentolamine intracoronarily, 15 patients received 600 mg/kg ofthe alpha1-blocker urapidil intravenously, 10 patients received thecombination of phentolamine and 1.2 mg of propranolol intra-coronarily, and 10 patients received saline.
Results. Fifteen minutes after successful coronary dilation,significant contractile dysfunction occurred in previously isch-emic and nonischemic myocardium. LV dysfunction was accom-
panied by an increase in coronary resistance and diffuse vasocon-striction. Alpha-blockers counteracted LV dysfunction andcoronary resistance and the increase in vasoconstriction. Phen-tolamine and urapidil increased global LV shortening from 34 69% to 45 6 8% and to 49 6 8%, respectively (p < 0.05). After theadministration of propranolol combined with phentolamine, LVdysfunction remained unchanged (34 6 6%), as in control sub-jects.
Conclusions. LV dysfunction occurs after PTCA, as described inanimal models after ischemia. Alpha-blockers abolished LV,macrocirculatory and microcirculatory dysfunction, whereas thealpha-blocker effect was prevented by combining alpha- andbeta-blockers. The evidence of diffuse rather than regional dys-function, together with the opposite effects of alpha- and beta-blockade, supports the hypothesis of neural mechanisms elicitingpostischemic LV dysfunction.
(J Am Coll Cardiol 1998;31:992–1001)©1998 by the American College of Cardiology
In 1935 brief periods of myocardial ischemia in open chestdogs (1) were reported to impair systolic shortening. In 1975Heyndrickx et al. (2) described, in conscious dogs, that briefperiods of myocardial ischemia, too brief to cause necrosis,were followed by a long-lasting impairment of contractilefunction and of regional blood flow (3), a phenomenon thatwas later called myocardial “stunning” (4). In humans percu-taneous transluminal coronary angioplasty (PTCA), clinicallyused as a means to correct coronary artery stenoses, entails the
induction of periods of transient ischemia. However, it iscontroversial whether or not transient ischemia, as producedby PTCA in humans, leads to left ventricular (LV) dysfunction(5–7). It has been shown that coronary artery constrictionoccurs soon after dilation (8) and persists for a rather long time(9). In addition, coronary vascular resistance has been reportedto increase (10) and coronary flow reserve to be impaired(11–13). In a previous study (10) we have shown that PTCA inpatients produces a delayed coronary artery constriction that ismediated by activation of alpha-adrenergic mechanisms, likelyto be reflexly induced by stretching of the dilated coronaryartery and stimulation of coronary mechanoreceptors (14–16).This coronary artery constriction was diffuse and not limited tothe dilated artery, and furthermore was simultaneously accom-panied by an increase of coronary artery resistance (10). Theintracoronary injection of drugs interfering with sympatheticnervous system activity was able to counteract the reduction incoronary diameter and the increase in coronary artery resis-tance.
The goal of the present investigation was to test the
From the Clinica Medica Generale, Ospedale Maggiore-IRCCS, Universityof Milano, Milano, Italy; *Clinique Pasteur, Centre de Cardiologie Interventio-nelle, Toulouse, France; and †CNR, Clinical Physiology Institute, Pisa, Italy.This study was supported by institutional funds from the University of Milan(MURST 60%). Hewlett Packard Germany provided the echocardiographicequipment used in this study; Hewlett Packard Italiana S.P.A. provided techno-logic assistance in the acquisition of the data presented here.
Manuscript received July 17, 1997; revised manuscript received December30, 1997, accepted January 13, 1998.
Address for correspondence: Prof. Luisa Gregorini, Clinica Medica, Osped-ale Maggiore-IRCCS, University of Milano, Via Francesco Sforza 35, 20122,Milano, Italy. E-mail: [email protected].
JACC Vol. 31, No. 5April 1998:992–1001
992
©1998 by the American College of Cardiology 0735-1097/98/$19.00Published by Elsevier Science Inc. PII S0735-1097(98)00055-2
by on July 12, 2011 content.onlinejacc.orgDownloaded from
hypothesis that, in humans, transient myocardial ischemia, asinduced by PTCA, is followed by LV dysfunction. As anadditional goal we assessed whether counteracting post-PTCAreflex coronary artery constriction and the simultaneous in-crease in coronary vascular resistance by means of alpha-blockers (10), thus allowing for a fuller restoration of flow,might prove beneficial to LV performance (2,3).
MethodsPatients. We studied 50 patients (9 women and 41 men,
mean age 61 6 11 years) undergoing coronary dilation fol-lowed by coronary stenting for 77 6 5% (mean 6 SD)epicardial vessel stenosis. Vessel diameters were measured byquantitative coronary angiography (Artrek) (17). Three diam-eters were prospectively chosen on the basal angiogram alongthe PTCA vessel (stenosis, normal reference and distal level)and one at the distal level of the control vessel (Table 1),following the schema previously reported by us as well as byother investigators (8–10). The same diameters were subse-quently measured in the following conditions. Thirty patientshad left anterior descending coronary artery (LAD) stenosis,and 12 had right coronary artery (RCA) and 8 had leftcircumflex lesions. All patients were admitted to the CliniquePasteur for recurrent or unstable angina. All gave written,informed consent to the study, which had been approved by theClinique Pasteur Ethical Committee.
Medical treatment. All patients were pretreated with con-ventional antianginal drugs such as nitrates, calcium antago-
Abbreviations and Acronyms
CBF(V) 5 coronary blood flow (velocity)CSA 5 cross-sectional area (cm2)CVRi 5 coronary vascular resistance indexFAC 5 percent fractional area changeLAD 5 left anterior descending coronary arteryLV 5 left ventricularPTCA 5 percutaneous transluminal coronary angioplastyRCA 5 right coronary arteryTEE 5 transesophageal echocardiographyWTH 5 percent systolic wall thickening
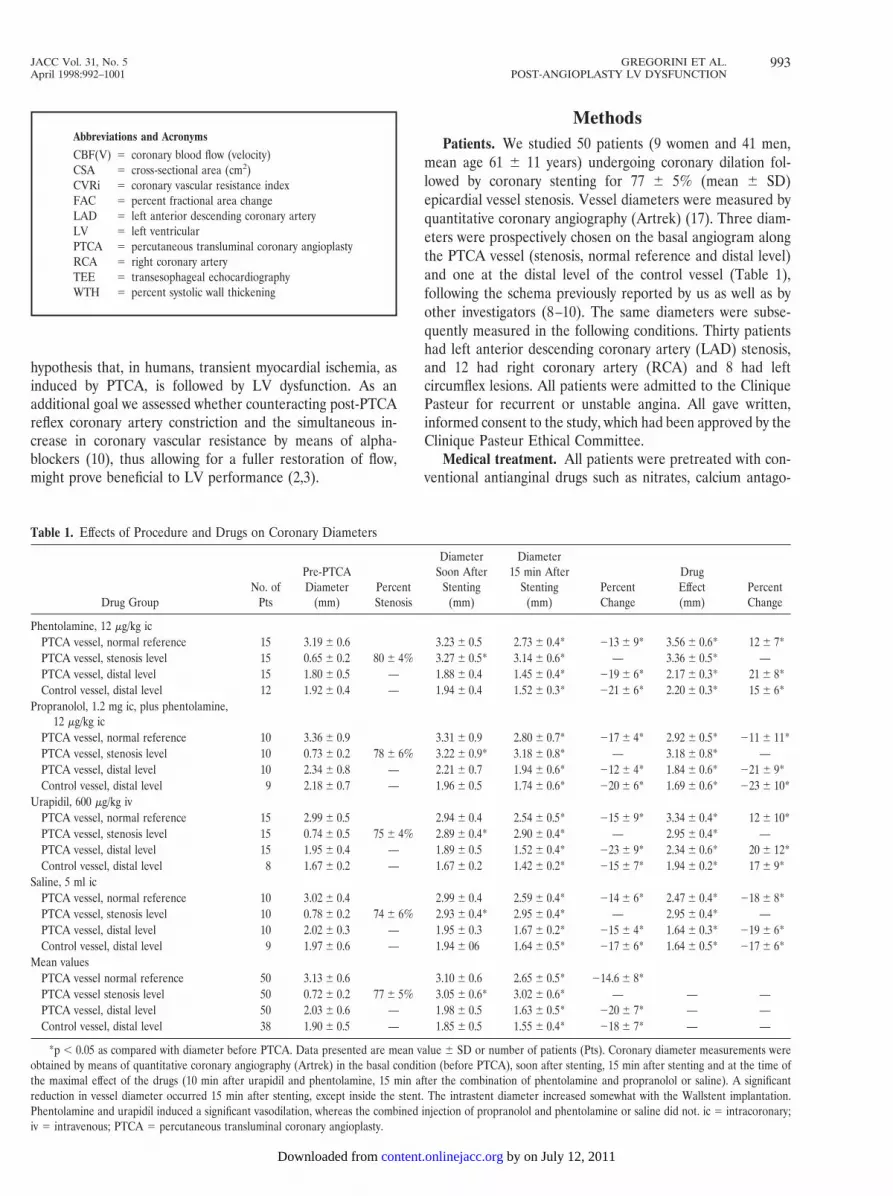
Table 1. Effects of Procedure and Drugs on Coronary Diameters
Drug GroupNo. of
Pts
Pre-PTCADiameter
(mm)PercentStenosis
DiameterSoon After
Stenting(mm)
Diameter15 min After
Stenting(mm)
PercentChange
DrugEffect(mm)
PercentChange
Phentolamine, 12 mg/kg icPTCA vessel, normal reference 15 3.19 6 0.6 3.23 6 0.5 2.73 6 0.4* 213 6 9* 3.56 6 0.6* 12 6 7*PTCA vessel, stenosis level 15 0.65 6 0.2 80 6 4% 3.27 6 0.5* 3.14 6 0.6* — 3.36 6 0.5* —PTCA vessel, distal level 15 1.80 6 0.5 — 1.88 6 0.4 1.45 6 0.4* 219 6 6* 2.17 6 0.3* 21 6 8*Control vessel, distal level 12 1.92 6 0.4 — 1.94 6 0.4 1.52 6 0.3* 221 6 6* 2.20 6 0.3* 15 6 6*
Propranolol, 1.2 mg ic, plus phentolamine,12 mg/kg ic
PTCA vessel, normal reference 10 3.36 6 0.9 3.31 6 0.9 2.80 6 0.7* 217 6 4* 2.92 6 0.5* 211 6 11*PTCA vessel, stenosis level 10 0.73 6 0.2 78 6 6% 3.22 6 0.9* 3.18 6 0.8* — 3.18 6 0.8* —PTCA vessel, distal level 10 2.34 6 0.8 — 2.21 6 0.7 1.94 6 0.6* 212 6 4* 1.84 6 0.6* 221 6 9*Control vessel, distal level 9 2.18 6 0.7 — 1.96 6 0.5 1.74 6 0.6* 220 6 6* 1.69 6 0.6* 223 6 10*
Urapidil, 600 mg/kg ivPTCA vessel, normal reference 15 2.99 6 0.5 2.94 6 0.4 2.54 6 0.5* 215 6 9* 3.34 6 0.4* 12 6 10*PTCA vessel, stenosis level 15 0.74 6 0.5 75 6 4% 2.89 6 0.4* 2.90 6 0.4* — 2.95 6 0.4* —PTCA vessel, distal level 15 1.95 6 0.4 — 1.89 6 0.5 1.52 6 0.4* 223 6 9* 2.34 6 0.6* 20 6 12*Control vessel, distal level 8 1.67 6 0.2 — 1.67 6 0.2 1.42 6 0.2* 215 6 7* 1.94 6 0.2* 17 6 9*
Saline, 5 ml icPTCA vessel, normal reference 10 3.02 6 0.4 2.99 6 0.4 2.59 6 0.4* 214 6 6* 2.47 6 0.4* 218 6 8*PTCA vessel, stenosis level 10 0.78 6 0.2 74 6 6% 2.93 6 0.4* 2.95 6 0.4* — 2.95 6 0.4* —PTCA vessel, distal level 10 2.02 6 0.3 — 1.95 6 0.3 1.67 6 0.2* 215 6 4* 1.64 6 0.3* 219 6 6*Control vessel, distal level 9 1.97 6 0.6 — 1.94 6 06 1.64 6 0.5* 217 6 6* 1.64 6 0.5* 217 6 6*
Mean valuesPTCA vessel normal reference 50 3.13 6 0.6 3.10 6 0.6 2.65 6 0.5* 214.6 6 8*PTCA vessel stenosis level 50 0.72 6 0.2 77 6 5% 3.05 6 0.6* 3.02 6 0.6* — — —PTCA vessel, distal level 50 2.03 6 0.6 — 1.98 6 0.5 1.63 6 0.5* 220 6 7* — —Control vessel, distal level 38 1.90 6 0.5 — 1.85 6 0.5 1.55 6 0.4* 218 6 7* — —
*p , 0.05 as compared with diameter before PTCA. Data presented are mean value 6 SD or number of patients (Pts). Coronary diameter measurements wereobtained by means of quantitative coronary angiography (Artrek) in the basal condition (before PTCA), soon after stenting, 15 min after stenting and at the time ofthe maximal effect of the drugs (10 min after urapidil and phentolamine, 15 min after the combination of phentolamine and propranolol or saline). A significantreduction in vessel diameter occurred 15 min after stenting, except inside the stent. The intrastent diameter increased somewhat with the Wallstent implantation.Phentolamine and urapidil induced a significant vasodilation, whereas the combined injection of propranolol and phentolamine or saline did not. ic 5 intracoronary;iv 5 intravenous; PTCA 5 percutaneous transluminal coronary angioplasty.
993JACC Vol. 31, No. 5 GREGORINI ET AL.April 1998:992–1001 POST-ANGIOPLASTY LV DYSFUNCTION
by on July 12, 2011 content.onlinejacc.orgDownloaded from

nists (diltiazem, 180 to 360 mg/day) and antiplatelet drugs(aspirin, 250 mg/day for at least 7 days, and ticlopidine, 250 mgtwice daily for the preceding 72 h). If it was part of the ongoingtherapy, beta-blockers were withdrawn 72 h before the study.At the beginning of the dilation procedure patients receivedneuroleptic analgesia with droperidol (2 to 10 mg intrave-nously) and phenoperidine (0.6 to 1 mg intravenously) (10).The doses were adjusted during the study to keep the patientsedated. Heparin, 150 U/kg, was used for anticoagulation.Nitric oxide donors, linsidomine (1 mg) and isosorbide dini-trate (1.5 mg) were injected before balloon inflation to makethe final stent expansion match, in diameter, with the vessel ina state of dilation. Nitric oxide donors were always adminis-tered after obtaining baseline coronary diameters and pre-PTCA LV function.
Measurements of LV function. Beginning 10 min beforethe dilation procedure and continuously throughout the study,up to 30 min after stent deployment, LV function was contin-uously monitored by means of transesophageal echocardiogra-phy (TEE) (18) using a 5.0-MHz multiplane probe (SONOS2500, Hewlett Packard Co.). Before positioning the guidingcatheter, with the patient already sedated, the TEE probe wasintroduced and a transgastric view of the left ventricle at thelevel of papillary muscles was obtained (short-axis view). Theimages were acquired on a SVHS Panasonic videotape re-corder and subsequently analyzed by means of a Freeland-TomTec Imaging System with Integrated Cardiac AnalysisSoftware, Version 5, to obtain quantitative analysis. Starting40 ms after the electrocardiographic (ECG) R wave, eightframes through a single cardiac cycle were automaticallyselected and digitized. Afterward the frames with maximal andminimal LV area were selected and end-diastolic and end-systolic endocardial borders were manually traced. Global andregional LV function were automatically calculated as percentfractional area change (FAC) and percent systolic wall thick-ening (WTH), respectively, according to the following formu-las:
FAC ~%! 5~LV end-diastolic area 2 LV end-systolic area!
LV end-diastolic area3 100;
WTH ~%! 5Systolic 2 Diastolic wall thickness
Diastolic wall thickness3 100.
LV diastolic area was also used as an indirect index ofpreload (19).
For regional LV analysis, diastolic and systolic wall thick-nesses and WTH were assessed from the short-axis view at 0,3, 6 and 9 o’clock, with zero representing the posterior wall(RCA-supplied region), 3 the lateral wall (region supplied byleft circumflex coronary artery), 6 the anterior wall (LAD-supplied region) and 9 the mid-septum (LAD-supplied regionor RCA-supplied region in case of a dominant RCA). In thefinal evaluation, regions were also defined as PTCA andnon-PTCA, depending on the vessel that underwent dilation.
FAC and WTH were calculated in 1) the basal condition(before PTCA); 2) soon after coronary stenting; 3) 15 min after
coronary stenting (i.e., when coronary artery constriction hasbeen described [8–10]); and 4) 5 to 15 min after pharmacologicintervention.
Intraobserver variability was assessed by having one ob-server (G.B.A.) remeasure FAC and WTH twice in 10 subjectsat all phases of the study. To assess interobserver variability in15 subjects, the same indexes were measured also by a secondobserver (M.K.) at all phases of the study.
Coronary blood flow velocity. Phasic and mean coronaryblood flow velocity (CBFV, cm/s) were obtained with a pulsedDoppler flow meter (Triton Technology, model 100-1000-20C)and 3F Doppler catheters (Nyros-Sorin) that were positioned;10 mm above the stenosis, as previously described (10). Thetechnique has been fully validated (20). The Doppler catheterwas withdrawn during coronary dilation and reinserted overthe wire in the same position after coronary stenting. TwoECG leads were continuously recorded. Arterial blood pres-sure was measured through the guiding catheter at the coro-nary ostium. Cross-sectional area (CSA) was obtained with theaid of quantitative coronary angiography (Artrek) (17). Coro-nary blood flow (CBF) (ml/min) and a calculated index ofcoronary vascular resistance (CVRi) were obtained as previ-ously described (21). In view of the approximations inherent inthis procedure, we report only directional and relative varia-tions as percent changes (mean 6 SD) from pre-PTCA values.
Coronary stenting. Two or three balloon inflations of3 min, each followed by 2 min of reperfusion, were performedto predilate the artery before inserting the stents. A single stentor multiple stents (Palmaz-Schatz, GT-Roubin II or Wall-Stent) were implanted in the lesion to properly reconstruct theanatomy of the vessel. Stents were deployed with a 20/30-sballoon inflation followed by other high pressure inflations (3to 5 inflations at 18 to 22 atm for 30/60 s) to expand the strutsup to the nominal normal reference vessel diameter (Table 1).The smallest guiding catheter size compatible with the type ofstent was chosen, and the tip of the guiding catheter wasslightly withdrawn from the coronary ostium, when not re-quired by the procedure, to avoid flow reductions.
Pharmacologic interventions. Fifteen minutes after coro-nary stenting and after documenting LV function, 15 patientsreceived 12 mg/kg of phentolamine intracoronarily (nonselec-tive alpha-blocker: Regitin, 10-mg vials, Novartis, Switzer-land), 15 patients received 600 mg/kg of urapidil (24,25)intravenously (from 35 to 48 mg intravenously) (alpha1-selective blocker: Ebrantil, 50-mg vials, Byk Gulden, Germany)and 10 patients received the combination of 12 mg/kg ofphentolamine and 1.2 mg of propranolol (nonselective beta-sympathetic blocker: Inderal, 5-mg vials, Zeneca) intracoro-narily. As the alpha1-blocker we chose urapidil because thisdrug induces a central serotoninergic activation of brain5HT1A receptors, which may be responsible for the smallnessof reflex tachycardia, despite the pronounced vasodilation(22,23). The doses of alpha- and beta-blockers were lower thanthose used in other studies (24) and were titrated to obtain analpha- or beta-blocking effect without decreasing blood pres-sure (10). In 10 control subjects, 5 ml of warm saline was
994 GREGORINI ET AL. JACC Vol. 31, No. 5POST-ANGIOPLASTY LV DYSFUNCTION April 1998:992–1001
by on July 12, 2011 content.onlinejacc.orgDownloaded from

injected intracoronarily. The short-axis view was monitored byTEE for an additional 15 min to assess the effects of differentpharmacologic interventions. All study investigators, exceptthe one responsible for drug dilution, were unaware of theadministered agent. All off-line measurements were performedin a blinded manner.
Statistical analysis. The results are expressed as the meanvalue 6 SD. One- or two-way analysis of variance for repeatedmeasures was performed with a commercial package, as ap-propriate. To assess statistical significance between the groups,the Scheffe F test was applied, with a value of p , 0.05 assignificant. In view of the large interindividual variability of theabsolute values, multiple comparisons between the groupswere performed with normalized data (%). Regression analysiswas performed by the least squares technique. Agreementbetween the readings performed by two observers was evalu-ated by estimating the consistent bias between readings, asrecommended by Bland and Altman (25) for the comparisonof two methods of clinical measurements.
ResultsEffect of coronary stenting on LV function and on coronary
diameters. Fractional area change and end-diastolic areameasured at various conditions are shown in Figure 1. Coro-nary stenting slightly increased FAC from 41 6 9% to 43 6 7%(mean of all patients). After stenting, myocardial functionprogressively worsened in all myocardial regions, reaching itslowest level 15 min later, as indicated by a decrease in FAC
from 43 6 7% soon after stenting to 34 6 9% 15 min aftercoronary stenting (p , 0.05 vs. before PTCA) (Fig. 1). Also,LV diastolic area significantly increased 15 min after coronarystenting. The changes in regional function are more clearlyshown in Figure 2 and Table 2. Soon after coronary stenting,systolic thickening significantly increased in the myocardiumsupplied by the dilated vessel, whereas no changes wereobserved in normally perfused regions. Surprisingly, 15 minlater, the reduction in thicknesses and in systolic thickeningoccurred not only in PTCA regions but also in surroundingterritories that did not undergo transient ischemia (non-PTCAregions). Figure 3 represents the computer printouts of systolicand diastolic LV endocardial contour of two different pa-tients—one receiving urapidil and the other a combination ofphentolamine and propranolol 15 min after coronary stenting.Both patients showed a clear increase in percent systolicthickening soon after stenting and severe worsening 15 min
Figure 1. Left ventricular FAC (top) (%, mean 6 SD) and diastolicarea (cm2) (bottom) obtained from the endocardial diastolic andsystolic contours (TomTec) before PTCA (Pre-PTCA), soon aftercoronary stenting (Post-Stent), 15 min after stenting (15 min Post-S)and after pharmacologic interventions. Phentolamine and urapidilsignificantly increased FAC and decreased diastolic area. When alpha-and beta-blockers combined or saline was injected, no effects on FACor diastolic area were observed. No changes in diastolic area wereobserved after drug administration versus pre-PTCA condition. 5 minPhe 5 5 min after intracoronary (ic) phentolamine injection; Phe 5phentolamine; Pro 5 propranolol; 5 min Ura 5 5 min after urapidilintravenous injection; 15 min Saline 5 15 min after saline.
995JACC Vol. 31, No. 5 GREGORINI ET AL.April 1998:992–1001 POST-ANGIOPLASTY LV DYSFUNCTION
by on July 12, 2011 content.onlinejacc.orgDownloaded from

later. The occurrence of LV global dysfunction correspondedto diffuse coronary artery constriction (Table 1). In fact, 15 minafter stenting, a 220 6 7% and 218 6 7% reduction incoronary diameter, as compared with the diameter beforePTCA (p , 0.05), was measured at the distal level of thedilated and control vessel, respectively.
Intraobserver variabilities for FAC and WTH were 4.2 62.1% and 4.4 6 3.0%, respectively. Interobserver variabilitiesfor the same indexes were 5.7 6 3.0% and 5.3 6 3.2%,respectively. A plot of the difference between the two observ-ers for each measurement versus the mean of the two mea-surements showed a mean difference of 0.14 6 2.63% and20.25 6 2.55%, respectively, with good agreement because allpoints but two were within 62 SD (Fig. 4).
Figure 2. Systolic wall thickening (mean 6 SD) measured in myocar-dial regions undergoing coronary dilation (top) and in regions notsubtended by the dilated vessel (bottom). Systolic wall thickeningsignificantly increased soon after coronary stenting only in PTCAregions, whereas 15 min after dilation a significant reduction occurredin myocardium both subtended and not subtended by the dilatedvessel. Five minutes after the injection, phentolamine and urapidilsignificantly increased systolic thickening. When the combination ofpropranolol and phentolamine was simultaneously injected or salinewas administered to control subjects, the impairment in systolicthickening was still present. Pro 1 Phe 5 propranolol combined withphentolamine.
Tabl
e2.
Wal
lThi
ckne
ssan
dSy
stol
icTh
icke
ning
No.
ofPt
s
Pre-
PTC
ASo
onA
fter
Sten
ting
15m
inA
fter
Sten
ting
3–5
min
Afte
rD
rugs
DW
TSW
TW
THD
WT
SWT
WTH
DW
TSW
TW
THD
WT
SWT
WTH
PTC
Are
gion
sU
rapi
dil,
600
mg/
kg15
0.89
60.
11.
216
0.3
376
240.
936
0.1*
1.40
60.
2*51
65*
0.83
60.
1*1.
056
0.2*
266
17*
0.99
60.
1*1.
516
0.2*
536
17*
Phe,
12m
g/kg
,plu
sPr
o,1.
2m
g10
0.92
60.
11.
286
0.1
386
150.
966
0.1*
1.40
60.
1*45
612
*0.
906
0.1*
1.13
60.
1*26
611
*0.
896
0.1*
1.09
60.
1*25
610
*
Phe,
12m
g/kg
150.
866
0.1
1.20
60.
340
616
0.89
60.
1*1.
316
0.3*
476
16*
0.81
60.
1*1.
046
0.2*
286
18*
0.90
60.
1*1.
356
0.2*
506
17*
Salin
e,5
ml
100.
816
0.1
1.12
60.
237
624
0.87
60.
1*1.
306
0.2*
496
12*
0.76
60.
1*0.
956
0.2*
246
15*
0.75
60.
1*0.
976
0.2*
226
16*
Mea
n50
0.87
60.
11.
216
0.2
386
200.
916
0.1*
1.35
60.
2*48
611
*0.
826
0.1*
1.04
60.
2*26
616
*N
on-P
TCA
regi
ons
Ura
pidi
l,60
0m
g/kg
150.
926
0.1
1.34
60.
247
621
0.97
60.
1*1.
466
0.2*
506
150.
886
0.1*
1.20
60.
2*37
615
*1.
006
0.1*
1.60
60.
2*60
616
*Ph
e,12
mg/
kg,p
lus
Pro,
1.2
mg
100.
916
0.1
1.34
60.
248
615
0.93
60.
11.
426
0.1*
426
120.
936
0.1
1.18
60.
2*27
611
*0.
936
0.1
1.25
60.
2*34
69*
Phe,
12m
g/kg
150.
866
0.1
1.27
60.
249
618
0.90
60.
1*1.
366
0.2*
516
180.
816
0.1*
1.08
60.
2*33
619
*0.
926
0.1*
1.40
60.
2*52
616
*Sa
line,
5m
l10
0.88
60.
11.
306
0.2
506
160.
946
0.1*
1.43
60.
3*52
615
0.80
60.
1*1.
076
0.1*
356
17*
0.81
60.
1*1.
106
0.1*
366
17*
Mea
n50
0.89
60.
11.
316
0.2
496
170.
956
0.1*
1.42
60.
2*50
615
0.85
60.
1*1.
136
0.2*
336
18*
*p,
0.05
asco
mpa
red
with
valu
esbe
fore
perc
utan
eous
tran
slum
inal
coro
nary
angi
opla
sty
(PTC
A).
Dat
apr
esen
ted
are
mea
nva
lue
6SD
.Int
raco
rona
ry(ic
)phe
ntol
amin
e(P
he)a
ndin
trav
enou
s(iv
)ura
pidi
lsig
nific
antly
incr
ease
ddi
asto
licwa
llth
ickn
ess(
DW
T),s
ysto
licwa
llth
ickn
ess(
SWT)
and
perc
ents
ysto
licwa
llth
icke
ning
(WTH
),wh
erea
safte
rthe
com
bine
din
ject
ion
ofpr
opra
nolo
l(Pr
o)an
dph
ento
lam
ine
oraf
ters
alin
e,D
WT,
SWT
and
WTH
rem
aine
dun
chan
ged.
Myo
card
ialt
hick
ness
and
thic
keni
ngof
regi
ons
subt
ende
dby
vess
els
unde
rgoi
ngor
notu
nder
goin
gan
giop
last
yar
ere
port
edas
PTC
Aan
dno
n-PT
CA
regi
ons,
resp
ectiv
ely.
996 GREGORINI ET AL. JACC Vol. 31, No. 5POST-ANGIOPLASTY LV DYSFUNCTION April 1998:992–1001
by on July 12, 2011 content.onlinejacc.orgDownloaded from

Effect of stenting on CBF and CVRi. The effects of coro-nary stenting on blood flow measurements obtained in theproximal dilated coronary vessel are reported as normalizedmean (6SD) values in Figure 5. Average basal CBFV was9.2 6 2 cm/s; CSA was 11.3 6 4 mm2; CBF was 61.7 623 ml/min; and CVRi was 1.69 6 0.5 U. With the conditionbefore drug injections (before PTCA, soon after and 15 minafter stenting) similar in all groups, the data were groupedtogether. Soon after stent implantation no changes wereobserved in CBFV, CSA, CBF and CVRi. In fact, CBFVincreased by 15.3 6 12% (p 5 NS), CSA by 2.5 6 6% (p 5 NS)and CBF by 18.3 6 16% (p 5 NS), whereas CVRi decreasedby 215.4 6 11% (p 5 NS). Fifteen minutes after coronarystenting, CBFV decreased by 223.6 6 16%, CSA by 218.5 612% and CBF by 238.4 6 15% (p , 0.05), whereas CVRiincreased by 66.2 6 13% (p , 0.05) (Fig. 5).
Hemodynamic effects of drugs. The intravenous injectionof urapidil transiently (1 to 2 min) decreased mean (6SD)arterial pressure (from 87 6 8 to 73 6 9 mm Hg, p , 0.05) anddid not change heart rate. The intracoronary injection of12 mg/kg of phentolamine did not significantly change thehemodynamic variables, whereas 1.2 mg of propranolol com-
bined with 12 mg/kg of phentolamine significantly affectedblood pressure and heart rate.
Effects of drugs on LV dysfunction. Thirty minutes afterPTCA a diffuse reduction in fractional systolic shortening andthickening and significant coronary artery constriction werepersisting in patients who received intracoronary saline (Fig. 1and 2, Tables 1 and 2). Both the alpha1-adrenergic blockerurapidil and the nonselective alpha-blocker phentolamine sig-nificantly improved SWT and counteracted coronary arteryconstriction (Tables 1 and 2, Fig. 2). When the beta-sympathetic blocker propranolol was combined with phentol-amine, no significant changes in SWT or in coronary diame-ters, as compared with 15 min after stenting, were observed. Infact, LV dysfunction and vasoconstriction were persisting, as inpatients receiving saline. As shown in Figure 3, LV dysfunctionwas abolished by the intravenous injection of urapidil (topright panel), whereas it persisted after the administration ofpropranolol and phentolamine (bottom right panel).
Effect of drugs on CBF and coronary vascular resistance.The intracoronary administration of phentolamine or urapidilsignificantly increased CBF by 74.8 6 21% and 51.9 6 19%,respectively, and decreased CVRi by 246 6 11% and 235 69%, respectively (p , 0.05) (Fig. 5). The combined adminis-tration of propranolol and phentolamine, as well as saline, didnot change CBF or CVRi, as compared with 15 min aftercoronary stenting, when a condition of global LV dysfunctionwas present.
DiscussionOur study provides clear evidence that coronary stenting,
despite the removal of a flow-limiting stenosis, is followed by asignificant impairment of LV myocardial function (2–4), whichis associated with a significant reduction in flow. The beneficial
Figure 4. A plot of the differences in measured values between twoobservers, both for FAC and systolic thickening (THK), versus themean of measured values.
Figure 3. Digitized printouts from the short-axis(SAX) left ventricular images by TEE (TomTecImaging System) obtained from drawing the sys-tolic and diastolic endocardial contour of twopatients undergoing beta1-blockade and alpha-and beta-blockade 15 min after stenting. Theupper sequence shows images of Patient 41 (33-year old man) who had a 95% mid-LAD stenosis.Before PTCA, hypokinesia of the mid and poste-rior septum was present. Soon after stent implan-tation, the hypokinesia disappeared. Fifteen min-utes after stenting, a significant global reductionof LV FAC occurred. The intravenous injectionof 34 mg of urapidil abolished LV dysfunction.The lower sequence shows printouts of Patient 50(53-year old man) who had a 82% mid-RCAstenosis. After stenting, FAC increased to 43%.Fifteen minutes after dilation, a significant globalLV dysfunction (30% FAC) occurred. The intra-coronary injection of propranolol and phentol-amine did not modify FAC.
997JACC Vol. 31, No. 5 GREGORINI ET AL.April 1998:992–1001 POST-ANGIOPLASTY LV DYSFUNCTION
by on July 12, 2011 content.onlinejacc.orgDownloaded from

effect of intracoronary alpha-blockers suggests a causative roleof reflex sympathetic interaction.
Effect of coronary stenting on LV function. The observa-tion that coronary stenting is followed by LV dysfunction is inagreement with a previous report by Sheiban et al. (7), whodescribed the occurrence of myocardial stunning in patientsundergoing 5-min balloon inflations. In our study, two infla-tions of 3 min were performed to predilate the coronary artery,but additional inflations followed by very short reperfusionswere carried out to deploy the stent. These additional highpressure inflations may have further increased the arterystretching, which has been demonstrated, in animal studies, toactivate cardiac sympathetic afferent fibers (14–16,26,27) andmay have exerted a cumulative ischemic effect. Our observa-tion is at variance with the results of other studies (5,6) thatassessed ventricular function during a shorter interval from theend of the last inflation (5) or after a single 1-min inflation (6).In contrast to previous reports, in our study LV function wasassessed with the aid of continuous TEE, which has beenshown to allow reliable quantitative measurement of LV globaland regional function (18,19). In fact, the TEE short-axis viewdisplays in sequence systolic and diastolic excursions andsimultaneously allows measurement of systolic and diastolicthickness, as well as thickening in myocardial wall sectorssupplied by different coronary rami.
Effect of coronary stenting on flow and resistance. Theoccurrence of global LV dysfunction corresponded in timingand time course to the angiographic phenomenon of coronaryartery constriction, which is also a diffuse phenomenon involv-ing both dilated and nonmanipulated control vessels, as previ-ously observed by us (10) and other investigators (28). More-
over, vasoconstriction was also demonstrated to occur afterPTCA along renal (27) and limb (29) vessels. The reduction inepicardial coronary artery diameter was followed by a simul-taneous microvascular constriction. Both these phenomena areabolished by alpha-adrenergic blockade (10). For this study, weselected a cohort of patients who, because of the irregularanatomy of their plaques, would be better treated by coronarystenting, which allows for complete dilation of the lesion andremoves the mechanical obstruction to flow. This is, to ourknowledge, the first demonstration, in humans, that flowreductions occur simultaneously with LV dysfunction, al-though the relation between the reduction in regional coronaryperfusion and cardiac function has been demonstrated for along time in animal studies (3,30). Indeed, in our patients, thereduction in systolic shortening and the evidence of macrovas-cular and microvascular perfusion abnormalities were moresensible indexes of postischemic LV dysfunction (31), ascompared with ECG changes, which were negligible 15 minafter stenting.
LV dysfunction. Regional rather than global contractileLV dysfunction is commonly believed to occur as a conse-quence of regional ischemia, with sparing of areas not involvedin the ischemic process (2–4,7,31). This observation comesfrom animal studies, in particular from conscious dog modelsin which a close correlation between regional blood flow andregional contractile function was found after transient myocar-dial ischemia (2–4,31–33). In particular, in animal models, anincrease in regional vascular resistance and a reduction ofvasodilator responsiveness to intravenous adenosine and pa-paverine were observed to occur simultaneously with thepresence of LV dysfunction (32,33). In contrast, we have
Figure 5. CBFV, CSA, CBF and CVRi calculatedas percent changes from basal values (average[6SD] basal values 9.2 6 0.7 cm/s, 11.3 6 4.2 mm2,61.7 6 23 ml/min and 1.69 6 0.5 U, respectively).Because the conditions before drug injections(Soon After Stent and 15 min After Stent) weresimilar in all groups, these data were groupedtogether. Coronary stenting did not affect CBFV,CSA or CBF. Fifteen minutes after the end of thedilation procedure, a significant increase in CVRiwas observed. Phentolamine and urapidil reducedCVRi, whereas no effects were observed after thecombination of propranolol and phentolamine.*p , 0.05 versus pre-PTCA values.
998 GREGORINI ET AL. JACC Vol. 31, No. 5POST-ANGIOPLASTY LV DYSFUNCTION April 1998:992–1001
by on July 12, 2011 content.onlinejacc.orgDownloaded from

observed that in humans, brief coronary balloon occlusionsinduce LV dysfunction, which also occurs in regions notundergoing transient ischemia. In contrast to previous reports(5–7) that did not observe global LV dysfunction, our obser-vation may have been favored by acquiring images by means ofTEE. Our observation is in agreement with the recent findingthat remote regional dysfunction is present in patients withmyocardial infarction and single-vessel disease (34). Our find-ings are also consistent with evidence of an altered vasodilatorreserve and metabolism in the myocardium supplied by appar-ently normal coronary arteries (35,36) in patients with single-vessel disease or in patients with coronary spastic angina (37).In fact, our data suggest that coronary artery constriction, areduction in CBF and an increase in coronary vascular resis-tance are different facets simultaneously accompanying LVdysfunction. The apparently smooth aspect of the coronarytree on the angiogram does not exclude the presence of adiffusely altered endothelium (21,38) or of subendothelialplaques (39), which cause the artery to react paradoxically tophysiologic vasodilator stimuli such as acetylcholine (40,41),serotonin (40,42–44), adenosine (13,45) and others (40). Thediscrepancies observed in our study as compared withprevious reports may also be ascribed to a diffusely alteredendothelium.
Myocardial dysfunction is usually thought to reflect anadjustment of coronary flow to preserve the perfusion contrac-tion matching in several acute and chronic ischemic states (4),including coronary vasospasm (46) occurring in the absence ofa flow-limiting stenosis, and is often considered a protectionmechanism (47) by which the ischemic myocardium slows therate of adenosine triphosphate utilization (48) and preservesits cells from an energy supply reduction by a decrease ofenergy demand (2–4). Adrenergic vasoconstriction might bebeneficial in the presence of ischemia by lessening transmuralsteal during myocardial hypoperfusion (47). Obviously, thisinterpretation must be at least partly revised as a consequenceof the observation that LV dysfunction also occurs in parts ofthe myocardium that are not ischemic and have not undergonea transient restriction of blood flow during the PTCA procedure.
Role of alpha-adrenoreceptors in LV dysfunction. Theobservation that the myocardium not exposed to transient flowstandstill undergoes mechanical dysfunction suggests that neu-ral mechanisms may play a major role in this phenomenon.Cardio-cardiac sympathetic reflexes, which have been de-scribed in animals (14–16,28,47,48) and hypothesized in hu-mans (10,29,30), may represent the link between the areasubjected to transient ischemia and other LV regions andexaggerate the effects of mechanisms such as “oxyradical”production (32,33,49), calcium overload (32,50,51) or releaseof endothelial factors (52). In fact, experimental studies sug-gest that impaired calcium homeostasis, resulting in a transientcalcium overload, might be involved in myocardial stunning(7,50,51). All of our patients were pretreated with full doses ofcalcium antagonists, which attenuate myocardial stunning incase of pretreatment (51). This treatment might have reducedthe occurrence of LV dysfunction. Although coronary stenting
is likely to extensively damage the endothelium of the dilatedvessel, endothelial factors might have contributed to thedelayed occurrence of vasoconstriction. Local nitric oxiderelease, likely following wall shear stress changes induced bystenosis removal, may be responsible for the significant in-crease in systolic thickening, which soon after dilation wasobserved only in regions supplied by the dilated vessel. Inaddition, endothelin release might have influenced the changesin vessel diameter (52). Indeed, in vivo shear stress–dependenttone or nitric oxide–induced vasodilation is modulated byinhibition of the adrenergic vasoconstriction (53,54). Althoughwe did not measure total peripheral resistance, the hypothesisthat the effect of alpha-blockers might in part be ascribed to anunloading of the LV is made unlikely by the observation thatsignificant changes in blood pressure or in LV diastolic areadid not occur at the time of post-drug measurements. Indeed,in our patients, the injection of alpha-blockers increased SWTand myocardial shortening after infusion (55), counteractingLV dysfunction and the abnormalities in macrocirculatory andmicrocirculatory coronary flow, whereas the simultaneous ad-ministration of beta- and alpha-blockers blunted the effect ofalpha-blockers alone, unmasking the presence of a beta-sympathetic inotropic and vasodilator tone (56). After coro-nary stenting, mechanical, contractile, macrocirculatory andmicrocirculatory adjustments take time. This might be due tothe fading effect on cardiac contractility (57) of nitratesadministered intracoronarily to better adjust the final stent sizeto a dilated vessel, or it may be due to shear stress mechanismsoccurring soon after coronary dilation (8,57). Indeed, in hu-mans, at variance with experimental models in which a sympa-thetic reflex occurs in seconds, the sympathovagal interaction isreported to be impaired 2 weeks after acute myocardialinfarction (58). The inotropic effect of phentolamine on re-duced LV performance in acute myocardial infarction wasreported previously by Walinsky et al. (59), who hypothesizeda reflex increase in sympathetic tone 48 h after acute myocar-dial infarction. In line with this previous study (59), our datasuggest the testable hypothesis that the administration ofalpha-blockers might be beneficial in improving LV dysfunc-tion after PTCA.
Conclusions. Coronary stenting corrects the mechanicalobstruction to flow but does not induce an immediate recoveryof LV function. Conductance and resistance artery constrictionoccurred simultaneously with global LV dysfunction as inter-related functional and clinical facets of the same phenomenon.Alpha-sympathetic blockers counteract LV dysfunction, induc-ing a better perfusion, whereas the combination of alpha- andbeta-blockers has the opposite effect. Neural mechanisms aremost likely regulating these phenomena by cross-talk interac-tion. These observations may open potential and promisingtherapeutic perspectives.
References1. Tennant R, Wiggers CJ. The effect of coronary occlusion on myocardial
contraction. Am J Physiol 1935;112:351–61.
999JACC Vol. 31, No. 5 GREGORINI ET AL.April 1998:992–1001 POST-ANGIOPLASTY LV DYSFUNCTION
by on July 12, 2011 content.onlinejacc.orgDownloaded from

2. Heyndrickx GR, Millard RW, McRitchie RJ, Maroko PR, Vatner SF.Regional myocardial function and electrophysiological alterations after briefcoronary occlusion in conscious dogs. J Clin Invest 1975;56:978–85.
3. Heyndrickx GR, Baig H, Nellens P, Lusen I, Fishbein RC, Vatner SF.Depression of regional blood flow and wall thickening after brief coronaryocclusions. Am J Physiol 1978;234:H653–9.
4. Braunwald E, Kloner RA. The stunned myocardium: prolonged postisch-emic ventricular dysfunction. Circulation 1982;66:1146–9.
5. Serruys PW, Wijns W, van den Brand M, et al. Left ventricular performance,regional blood flow, wall motion and lactate metabolism during transluminalcoronary angioplasty. Circulation 1984;70:24–36.
6. Labovitz AJ, Lewen MK, Kern M, Vandormael M, Deligonul U, KennedyHL. Evaluation of left ventricular systolic and diastolic dysfunction duringtransient myocardial ischemia produced by angioplasty. J Am Coll Cardiol1987;10:748–55.
7. Sheiban I, Tonni S, Benussi P, Marini A, Trevi GP. Left ventriculardysfunction following transient ischemia induced by transluminal coronaryangioplasty: beneficial effects of calcium antagonists against post-ischemicmyocardial stunning. Eur Heart J 1993;14 Suppl A:14–21.
8. Fischell TA, Derby G, Tse TM, Stadius ML. Coronary artery vasoconstric-tion routinely occurs after percutaneous transluminal coronary angioplasty:a quantitative arteriographic analysis. Circulation 1988;78:1323–34.
9. El Tamimi H, Davies GJ, Hackett D, Sritara P, Crea F, Maseri A. Abnormalvasomotor changes early after coronary angioplasty: a quantitative arterio-graphic study of their time course. Circulation 1991;84:1198–202.
10. Gregorini L, Fajadet J, Robert G, Cassagneau B, Bernis M, Marco J.Coronary vasoconstriction following percutaneous transluminal coronaryangioplasty is attenuated by antiadrenergic agents. Circulation 1994;90:985–7.
11. Kern MJ, Deligonul U, Vandormael M, et al. Impaired coronary vasodilatorreserve in the immediate post coronary angioplasty period: analysis ofcoronary artery flow velocity indexes and regional cardiac venous efflux.J Am Coll Cardiol 1989;13:860–72.
12. Uren NG, Crake T, Lefroy D, de Silva R, Davies GJ, Maseri A. Delayedrecovery of coronary resistive vessel function after coronary angioplasty.J Am Coll Cardiol 1993;21:612–21.
13. Sunamura M, di Mario C, Piek J, et al. Intracoronary Doppler guidanceduring angioplasty: the Doppler Endpoints Balloon Angioplasty Trial Eu-rope (DEBATE) study. Results of the second interim analysis. In: de FeyterPJ, di Mario C, Serruys PW, editors. Quantitative Coronary Imaging.Rotterdam, The Netherlands: Barjesteh, Meeuwes & Co, 1995:258–9,267–86.
14. Malliani A, Schwartz PJ, Zanchetti A. A sympathetic reflex elicited byexperimental coronary occlusion. Am J Physiol 1969;217:703–9.
15. Brown AM, Malliani A. Spinal sympathetic reflexes initiated by coronaryreceptors. J Physiol (Lond) 1971;212:685–705.
16. Heusch G, Deussen A, Thamer V. Cardiac sympathetic nerve activity andprogressive vasoconstriction distal to coronary stenoses: feed-back aggrava-tion of myocardial ischemia. J Auton Nerv Syst 1985;13:311–26.
17. Mancini GBJ, Simon SB, Mc Gillem MJ, LeFree MT, Friedman HZ, VogelRA. Automated quantitative coronary arteriography: morphologic andphysiologic validation in vivo of a rapid digital angiographic method.Circulation 1987;75:452–60.
18. Kremer PF, Cahalan MK, Beaupre PN. Intraoperative myocardial ischemiadetected by means of transesophageal echocardiography. Circulation 1983;68:332–8.
19. Konstadt SN, Thys SD, Mindich BP, Kaplan JA, Goldman M. Validation ofquantitative intraoperative transesophageal echocardiography. Anesthesiol-ogy 1986;65:418–24.
20. Wilson RF, Laughlin DE, Ackell PH, et al. Transluminal, subselectivemeasurement of coronary artery blood flow velocity and vasodilator effect inman. Circulation 1985;72:82–92.
21. Nabel EG, Ganz P, Gordon JB, Alexander RW, Selwyn AP. Dilation ofnormal and constriction of atherosclerotic coronary arteries caused by coldpressor test. Circulation 1988;77:43–52.
22. Gillis RA, Dretchen KL, Namath I, et al. Hypotensive effect of urapidil: CNSsite and relative contribution. J Cardiovasc Pharmacol 1987;9:103–8.
23. Kolassa N, Beller KD, Sanders KH. Involvement of brain 5HT1A receptor inthe hypotensive response to urapidil. Am J Cardiol 1989;64:7D–10D.
24. Hogdson JMcB, Cohen MD, Szentpetery S, Thames MD. Effects of regional
a- and b-blockade on resting and hyperemic coronary blood flow inconscious, unstressed humans. Circulation 1989;79:797–809.
25. Bland MJ, Altman DG. Statistical method for assessing agreement betweentwo methods of clinical measurement. Lancet 1986;1:307–9.
26. Buffington CW, Feigl EO. Adrenergic coronary vasoconstriction in thepresence of coronary stenosis in the dog. Circ Res 1981;48:416–23.
27. Minisi AJ, Thames MD. Activation of cardiac sympathetic afferents duringcoronary occlusion: evidence for reflex activation of the sympathetic nervoussystem during transmural myocardial ischemia in the dog. Circulation1991;84:357–67.
28. Indolfi C, Piscione F, Rapacciuolo A, et al. Coronary artery vasoconstrictionafter successful single angioplasty of the left anterior descending artery.Am Heart J 1994;128:858–64.
29. Indolfi C, Piscione F, Ceravolo R, et al. Limb vasoconstriction aftersuccessful angioplasty of the left anterior descending coronary artery.Circulation 1995;92:2109–12.
30. Vatner SF. Correlation between acute reductions in myocardial blood flowand function in conscious dogs. Circ Res 1980;47:201–7.
31. Distante A, Rovai D, Picano E, et al. Transient changes in left ventricularmechanics during attacks of Prinzmetal angina: a two-dimensional echocar-diographic study. Am Heart J 1984;108:440–6.
32. Bolli R. Myocardial “stunning” in man. Circulation 1992;86:1671–91.33. Bolli R, Zughaib M, Li XY, et al. Recurrent ischemia in the canine heart
causes recurrent bursts of free radical production that have a cumulativeeffect on contractile function: a pathophysiological basis for chronic myo-cardial “stunning.” J Clin Invest 1995;96:1066–84.
34. Kramer CM, Rogers WJ, Theobald TM, Power TP, Petruolo S, Reichek N.Remote noninfarcted region dysfunction soon after first anterior myocardialinfarction: a magnetic resonance tagging study. Circulation 1996;94:660–6.
35. Sambuceti GM, Parodi O, Giorgetti A, et al. Microvascular dysfunction incollateral-dependent myocardium. J Am Coll Cardiol 1995;26:615–23.
36. Uren NG, Maccarini P, Gistri R, de Silva D, Camici PG. Altered coronaryvasodilator reserve and metabolism in myocardium subtended by normalarteries in patients with coronary artery disease. J Am Coll Cardiol 1995;26:650–8.
37. Okumura K, Yasue H, Matsuyama K, et al. Diffuse disorder of coronaryartery vasomotility in patients with coronary spastic angina: hyperreactivityto the constrictor effect of acetylcholine and the dilator effect of nitroglyc-erin. J Am Coll Cardiol 1996;27:45–62.
38. Schachinger V, Zeiher AM. Quantitative assessment of coronary vasoreac-tivity in humans in vivo: importance of baseline vasomotor tone in athero-sclerosis. Circulation 1995;92:2087–94.
39. Liebson PR, Klein LW. Intravascular ultrasound in coronary atherosclerosis:a new approach to clinical assessment. Am J Cardiol 1992;123:1643–60.
40. Furchgott RF. Role of endothelium in responses of vascular smooth muscle.Circ Res 1983;53:557–73.
41. Ludmer PL, Selwyn AP, Shook TL, et al. Paradoxical acetylcholine inducedcoronary artery constriction in patients with coronary artery disease. N EnglJ Med 1986;315:1046–51.
42. Vanhoutte PM, Houston DS. Platelet, endothelium and vasospasm. Circu-lation 1985;72:728–34.
43. Golino P, Piscione F, Willerson JT, et al. Divergent effects of serotonin oncoronary artery dimensions and blood flow in patients with coronaryatherosclerosis and control patients. N Engl J Med 1991;324:641–8.
44. McFadden EP, Clarke JG, Davies GJ, Kaski JC, Haider AW, Maseri A.Effect of intracoronary serotonin on coronary vessels in patients with stableangina and patients with variant angina. N Engl J Med 1991;324:648–54.
45. Kern MJ, Deligonul U, Tatineni S, Serota H, Aguirre F, Hilton TC.Intravenous adenosine: continuous infusion and low dose bolus administra-tion for determination of coronary vasodilator reserve in patients with andwithout coronary artery disease. J Am Coll Cardiol 1991;18:718–29.
46. Mathias P, Kerin NZ, Blevins RD, Cascade P, Rubenfire M. Coronaryvasospasm as a cause of stunned myocardium. Am Heart J 1987;113:383–5.
47. Nathan HJ, Feigl EO. Adrenergic vasoconstriction lessens transmural stealduring coronary hypoperfusion. Am J Physiol 1986;250:H645–53.
48. Reimer KA, Hill ML, Jennings RB. Prolonged depletion of ATP and of theadenine nucleotide pool due to delayed resynthesis of adenine nucleotidefollowing reversible myocardial ischemic injury in dogs. J Mol Cell Cardiol1981;13:229–37.
49. Hearse DJ. Stunning: a radical re-view. Cardiovasc Drug Ther 1991;5:853–76.
1000 GREGORINI ET AL. JACC Vol. 31, No. 5POST-ANGIOPLASTY LV DYSFUNCTION April 1998:992–1001
by on July 12, 2011 content.onlinejacc.orgDownloaded from

50. Ehring T, Heusch G. Stunned myocardium and the attenuation of stunningby calcium antagonists. Am J Cardiol 1995;75 Suppl E:61E–67E.
51. Przklenk K, Kloner RA. Role of verapamil on postischemic “stunned”myocardium: importance of the timing of the treatment. J Am Coll Cardiol1988;11:614–23.
52. McClellan G, Weisberg A, Rose D, Winegrad S. Endothelial cell storage andrelease of endothelin as cardioregulatory mechanism. Circ Res 1994;75:85–96.
53. Tesfamariam B, Cohen RA. Inhibition of adrenergic vasoconstriction byendothelial cell shear stress. Circ Res 1988;63:720–5.
54. Zanzinger J, Czachurski J, Seller H. Inhibition of sympathetic vasoconstric-tion is a major principle of vasodilatation by nitric oxide in vivo. Circ Res1994;75:1073–7.
55. Kitakaze M, Hori M, Sato H, et al. Beneficial effects of a1-adrenoceptoractivity on myocardial stunning in dogs. Circ Res 1991;68:1322–39.
56. Vatner SF, Hintze TH. Mechanism of constriction of large coronary arteriesby b-adrenergic receptor blockade. Circ Res 1983;53:389–400.
57. Kelly RA, Han X. Nitrovasodilators have (small) direct effects on cardiaccontractility: is this important? Circulation 1997;96:2493–5.
58. Lombardi F, Sandrone G, Perpruner S, et al. Heart rate variability as anindex of sympathovagal interaction after acute myocardial infarction. Am JCardiol 1987;60:1239–45.
59. Walinsky P, Chatterjee K, Forrester J, Parmley WW, Swan HJ. Enhancedleft ventricular performance with phentolamine in acute myocardial infarc-tion. Am J Cardiol 1974;33:37–41.
1001JACC Vol. 31, No. 5 GREGORINI ET AL.April 1998:992–1001 POST-ANGIOPLASTY LV DYSFUNCTION
by on July 12, 2011 content.onlinejacc.orgDownloaded from

1998;31;992-1001 J. Am. Coll. Cardiol.Bernies, A Distante, I Marco, J Fajadet, and A Zanchetti
L Gregorini, J Marco, C Palombo, M Kozakova, GB Anguissola, B Cassagneau, M blocking agents
Postischemic left ventricular dysfunction is abolished by alpha-adrenergic
This information is current as of July 12, 2011
Citations http://content.onlinejacc.org#otherarticles
This article has been cited by 9 HighWire-hosted articles:
Rights & Permissions
http://content.onlinejacc.org/misc/permissions.dtltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://content.onlinejacc.org/misc/reprints.dtl
Information about ordering reprints can be found online:
by on July 12, 2011 content.onlinejacc.orgDownloaded from





























