Embed Size (px)
Citation preview
JMIR Preprints Dhala et al
Rapid Implementation and Innovative Applications ofa Virtual ICU during the COVID-19 Pandemic: A Case
Study
Atiya Dhala, Farzan Sasangohar, Bita Kash, Faisal Masud
Submitted to: Journal of Medical Internet Researchon: May 12, 2020
Disclaimer: © The authors. All rights reserved. This is a privileged document currently under peer-review/communityreview. Authors have provided JMIR Publications with an exclusive license to publish this preprint on it's website forreview purposes only. While the final peer-reviewed paper may be licensed under a CC BY license on publication, at thisstage authors and publisher expressively prohibit redistribution of this draft paper other than for review purposes.
https://preprints.jmir.org/preprint/20143 [unpublished, non-peer-reviewed preprint]
JMIR Preprints Dhala et al
Table of Contents
Original Manuscript ....................................................................................................................................................................... 4Supplementary Files ..................................................................................................................................................................... 15
Figures ......................................................................................................................................................................................... 16Figure 1 ...................................................................................................................................................................................... 17Figure 2 ...................................................................................................................................................................................... 18Figure 3 ...................................................................................................................................................................................... 19Figure 4 ...................................................................................................................................................................................... 20
https://preprints.jmir.org/preprint/20143 [unpublished, non-peer-reviewed preprint]
JMIR Preprints Dhala et al
Rapid Implementation and Innovative Applications of a Virtual ICU duringthe COVID-19 Pandemic: A Case Study
Atiya DhalaMD, ; Farzan Sasangohar; Bita KashPhD, ; Faisal MasudMD,
Corresponding Author:Farzan SasangoharPhone: +19794582337Email: [email protected]
Abstract
Background: Coronavirus disease-2019 (COVID-19) necessitated the rapid increase of highly infectious disease intensive careunit space.
Objective: The Virtual Intensive Care Unit (vICU) at Houston
Method: st Hospital. Overall responses from patients, families, and physicians are positively in favor of continued vICU care;however, further research is required to examine the impact of innovative applications of tele-critical care in the treatment ofcritically ill patients.
Methods: Planned vICU implementation was redirected to meet emerging needs of COVID-19 intensive care units’ conversion,including alterations to staged rollout timing, virtual and in-person staffing, and scope of application. With the majority ofhospital critical care physician workforce redirected to rapidly expanded COVID-19 ICUs, the non-COVID-19 ICUs weremanaged by cardiovascular surgeons, cardiologists, neurosurgeons, and acute care surgeons. HMH expanded the vICU programto fill the newly depleted critical care expertise in the non-COVID-19 units to provide urgent, emergent, and code blue support toall ICUs.
Results: Virtual family visitation via a Consultant Bridge, palliative care delivery, and specialist consultation for COVID-19patients exemplify the successful adaptation of vICU implementation. COVID patients, isolated and separated from their familiesto prevent the spread of infection, were able to virtually see and hear their loved ones, bolstering the mental and emotional statusof those patients. Many families expressed gratitude for the ability to see and speak with their loved ones. The vICU alsoprotected medical staff and specialists assigned to COVID units, reducing exposure and conserving personal protectiveequipment.
Conclusions: Tele-critical care has been established as an advantageous mechanism for the delivery of critical care expertiseduring the expedited rollout of vICU at Houston
(JMIR Preprints 12/05/2020:20143)DOI: https://doi.org/10.2196/preprints.20143
Preprint Settings
1) Would you like to publish your submitted manuscript as preprint?Please make my preprint PDF available to anyone at any time (recommended).Please make my preprint PDF available only to logged-in users; I understand that my title and abstract will remain visible to all users.Only make the preprint title and abstract visible.No, I do not wish to publish my submitted manuscript as a preprint.
2) If accepted for publication in a JMIR journal, would you like the PDF to be visible to the public?Yes, please make my accepted manuscript PDF available to anyone at any time (Recommended). Yes, but please make my accepted manuscript PDF available only to logged-in users; I understand that the title and abstract will remain visible to all users (see Important note, above). I also understand that if I later pay to participate in <a href="https://jmir.zendesk.com/hc/en-us/articles/360008899632-What-is-the-PubMed-Now-ahead-of-print-option-when-I-pay-the-APF-" target="_blank">JMIR’s PubMed Now! service</a> service, my accepted manuscript PDF will automatically be made openly available.Yes, but only make the title and abstract visible (see Important note, above). I understand that if I later pay to participate in <a href="https://jmir.zendesk.com/hc/en-us/articles/360008899632-What-is-the-PubMed-Now-ahead-of-print-option-when-I-pay-the-APF-" target="_blank">JMIR’s PubMed Now! service</a> service, my accepted manuscript PDF will automatically be made openly available.
https://preprints.jmir.org/preprint/20143 [unpublished, non-peer-reviewed preprint]
JMIR Preprints Dhala et al
Original Manuscript
https://preprints.jmir.org/preprint/20143 [unpublished, non-peer-reviewed preprint]
JMIR Preprints Dhala et al
Original Paper
Dhala, Atiya MD, FACP1; Sasangohar, Farzan PhD2,3; Kash, Bita PhD3,4; Masud, Faisal MD, FCCP,FCCM1,5
1Department of Surgery, Houston Methodist Hospital2Department of Industrial and Systems Engineering, Texas A&M University3Center for Outcomes Research, Houston Methodist Hospital4School of Public Health, Texas A&M University 5Departments of Anesthesiology and Critical Care and Houston Methodist DeBakey Heart andVascular Center, Houston Methodist Hospital
Correspondence to Farzan Sasangohar, PhD, 3131 TAMU, College Station TX 77843, USA. Tel: 979-458-2337; fax: 979-458-4299; e-mail: [email protected]
Rapid Implementation and Innovative Applications ofa Virtual ICU during the COVID-19 Pandemic: A CaseStudy
Abstract
Background: Coronavirus disease-2019 (COVID-19) necessitated the rapid increase of highlyinfectious disease intensive care unit space.Objective: The Virtual Intensive Care Unit (vICU) at Houston Methodist Hospital (HMH) was utilizedamidst the 2019 novel coronavirus disease (COVID-19) outbreak. This paper details noveladaptations and rapid expansion of the vICU applied towards patient-centric solutions whileprotecting the staff and patients’ families during the pandemic. Methods: Planned vICU implementation was redirected to meet emerging needs of COVID-19intensive care units’ conversion, including alterations to staged rollout timing, virtual and in-personstaffing, and scope of application. With the majority of hospital critical care physician workforceredirected to rapidly expanded COVID-19 ICUs, the non-COVID-19 ICUs were managed bycardiovascular surgeons, cardiologists, neurosurgeons, and acute care surgeons. HMH expanded thevICU program to fill the newly depleted critical care expertise in the non-COVID-19 units to provideurgent, emergent, and code blue support to all ICUs.Results: Virtual family visitation via a Consultant Bridge, palliative care delivery, and specialistconsultation for COVID-19 patients exemplify the successful adaptation of vICU implementation.COVID patients, isolated and separated from their families to prevent the spread of infection, wereable to virtually see and hear their loved ones, bolstering the mental and emotional status of thosepatients. Many families expressed gratitude for the ability to see and speak with their loved ones.The vICU also protected medical staff and specialists assigned to COVID units, reducing exposureand conserving personal protective equipment. Conclusions: Tele-critical care has been established as an advantageous mechanism for the deliveryof critical care expertise during the expedited rollout of vICU at Houston Methodist Hospital. Overallresponses from patients, families, and physicians are positively in favor of continued vICU care;
https://preprints.jmir.org/preprint/20143 [unpublished, non-peer-reviewed preprint]
JMIR Preprints Dhala et al
however, further research is required to examine the impact of innovative applications of tele-critical care in the treatment of critically ill patients.
Keywords: Intensive Care Units; Critical Care; Pandemics; SARS Coronavirus; Telemedicine; InfectionControl; COVID-19
Introduction
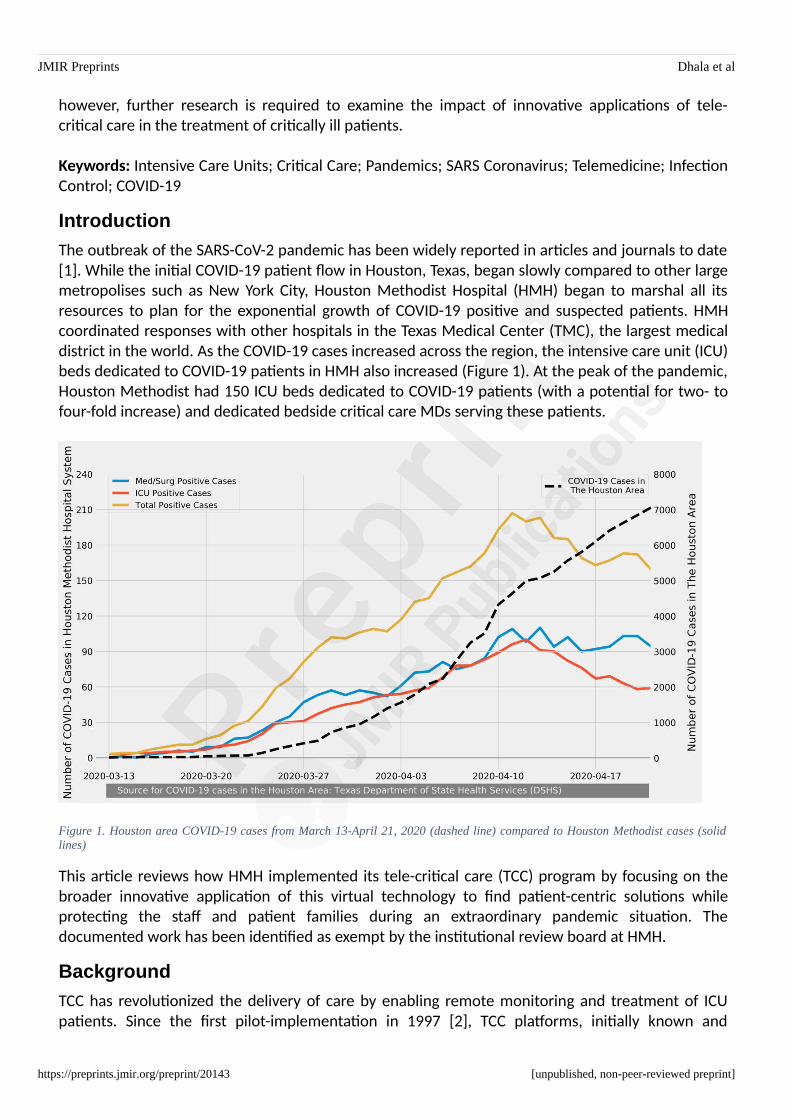
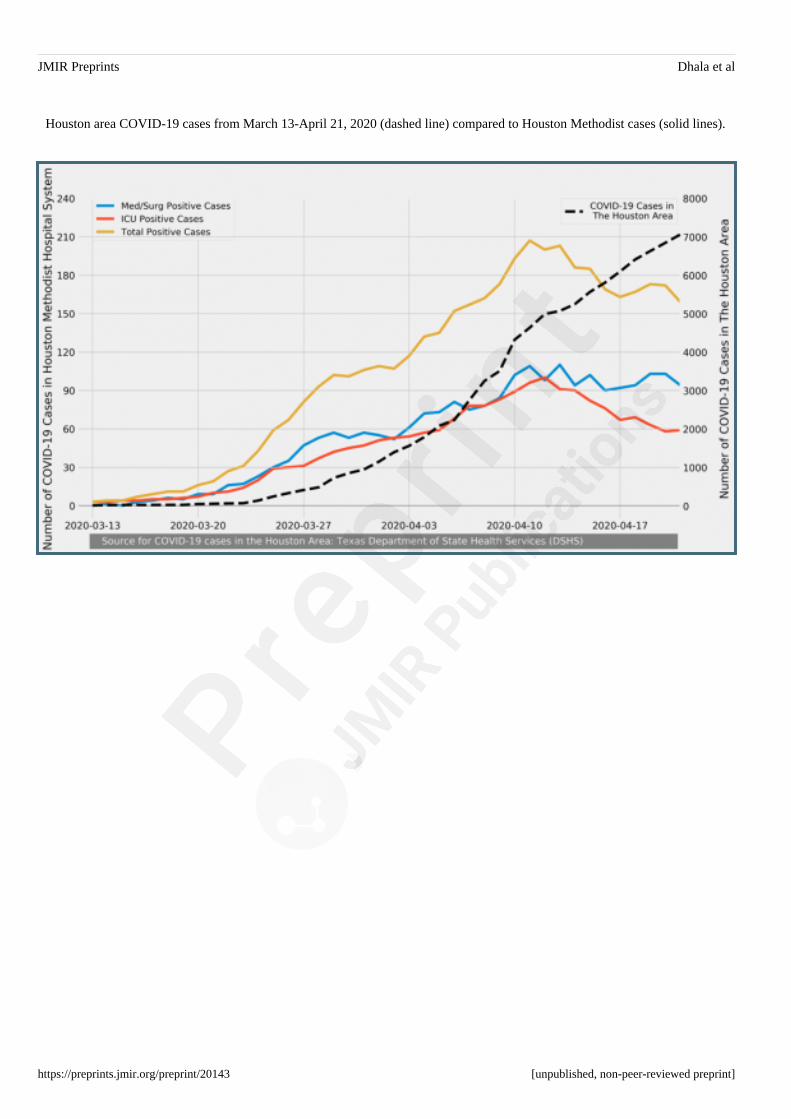
The outbreak of the SARS-CoV-2 pandemic has been widely reported in articles and journals to date[1]. While the initial COVID-19 patient flow in Houston, Texas, began slowly compared to other largemetropolises such as New York City, Houston Methodist Hospital (HMH) began to marshal all itsresources to plan for the exponential growth of COVID-19 positive and suspected patients. HMHcoordinated responses with other hospitals in the Texas Medical Center (TMC), the largest medicaldistrict in the world. As the COVID-19 cases increased across the region, the intensive care unit (ICU)beds dedicated to COVID-19 patients in HMH also increased (Figure 1). At the peak of the pandemic,Houston Methodist had 150 ICU beds dedicated to COVID-19 patients (with a potential for two- tofour-fold increase) and dedicated bedside critical care MDs serving these patients.
Figure 1. Houston area COVID-19 cases from March 13-April 21, 2020 (dashed line) compared to Houston Methodist cases (solidlines)
This article reviews how HMH implemented its tele-critical care (TCC) program by focusing on thebroader innovative application of this virtual technology to find patient-centric solutions whileprotecting the staff and patient families during an extraordinary pandemic situation. Thedocumented work has been identified as exempt by the institutional review board at HMH.
Background
TCC has revolutionized the delivery of care by enabling remote monitoring and treatment of ICUpatients. Since the first pilot-implementation in 1997 [2], TCC platforms, initially known and
https://preprints.jmir.org/preprint/20143 [unpublished, non-peer-reviewed preprint]

JMIR Preprints Dhala et al
trademarked as eICUs, have extended access to resources (e.g., critical care physicians, specializedconsults, and nurses), have provided a wide range of decision-support tools, and have allowedmonitoring and analysis of a large amount of physiological data [3]. While recent studies show largevariability on mortality impacts of TCCs, for instance, in Kahn et al.’s 2016 national effectivenessstudy [4], the positive impacts on the length of stay, cost, and quality of care have contributed toincreased popularity and adoption rate [5-6]. A 2017 survey of 722 hospitals worldwide (672 in theUnited States) showed that 35% had formal tele-critical care programs [6].
Houston Methodist vICUBefore the onset of the COVID-19 pandemic, HMH launched its innovative TCC program, branded asthe Virtual Intensive Care Unit or vICU, to augment the critical care services being provided in itsICUs. The HMH vICU has three main components: the operations center, the bedside team, and theaudio-visual (AV) communication infrastructure linking the two. The operations center, located atHMH’s main campus at TMC provides a central command capability where the Virtual MDs (vMDs)and Virtual RNs (vRNs) connect and monitor patients’ status using the AV equipment installed inpatient rooms. The AV communication infrastructure includes a camera in the patient rooms with360-degree pan, tilt, and zoom capability so that the vMDs and vRNs can examine the patient andalso focus on IV fluids, drip rates, monitors, ventilator settings, and, of course, communicate withthe patients, their visiting families, and the bedside providers.
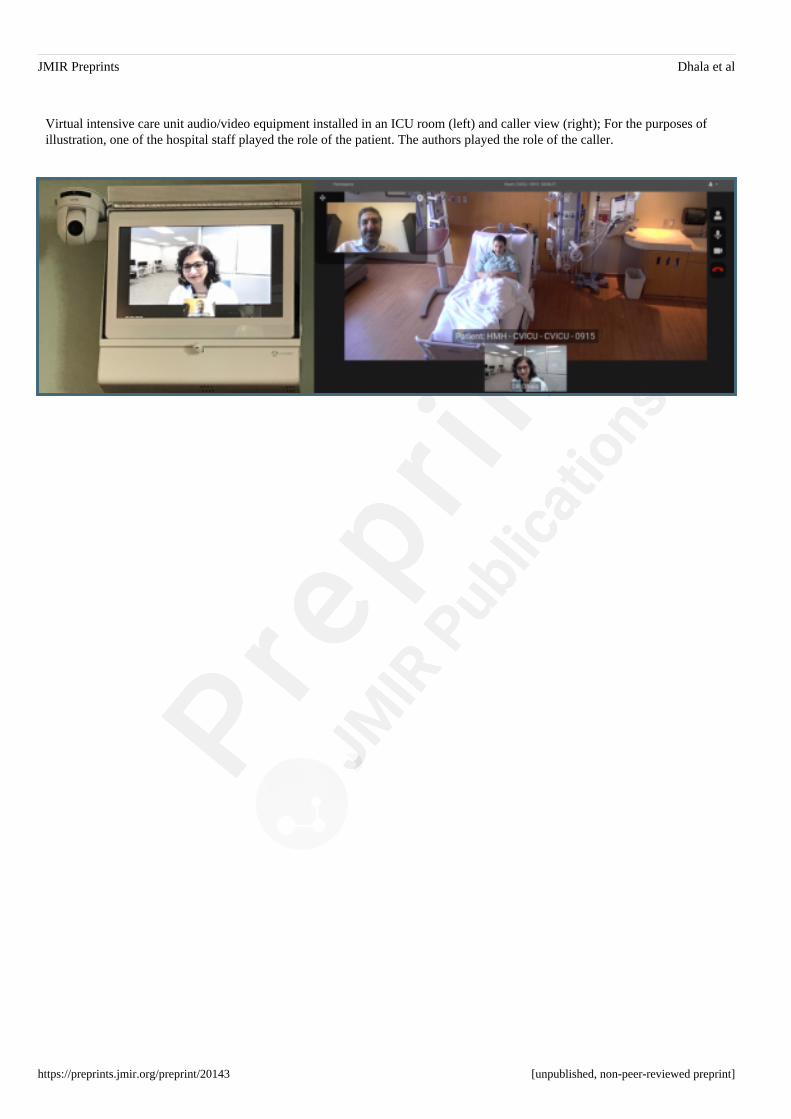
For emergent/urgent calls, the bedside teams can access the vICU by pressing a virtual alert buttonin each room to engage a vMD or vRN from the operations center. The vMDs and the vRNs cancamera-in within seconds to respond. In addition, the operations center can connect a consultant oran expert from any remote location through an application called Consultant Bridge. The operationscenter staff can send a text or email a link to the consultant to “bridge” them into the patient’sroom. The consultant bridge allows the vMD, the consultant, and the bedside team to have a three-way video call using the cameras and monitors already installed in the ICU patient rooms (Figure 2).
Figure 2. Virtual intensive care unit audio/video equipment installed in an ICU room (left) and caller view (right); For the purposes ofillustration, one of the hospital staff played the role of the patient. The authors played the role of the caller.
Initially, the vICU staff consisting of one vMD and two vRNs provided nocturnal coverage for HMH’s36-bed Neuro-ICU. To ensure a smooth transition and to minimize any disruptions to existingprocesses, the implementation plan called for a step-wise roll-out of vICU to the other three units:Medical ICU (MICU), Cardiovascular ICU (CVICU) and Cardiac ICU (CICU). The vICU process requiredthat all of the staff’s expectations be clearly defined and workflows integrated appropriately whilenurturing a robust and productive relationship with the bedside teams. The vICU and the ICU teams
https://preprints.jmir.org/preprint/20143 [unpublished, non-peer-reviewed preprint]
JMIR Preprints Dhala et al
initiated a collaborative effort to design the essential workflows almost four months before theactual launch of the vICU.
Methods
ICU Expansions in Response to COVID-19 Surge
The expected surge of the COVID-19 pandemic suddenly necessitated a change in the rollout planfor the vICU. To fully prepare for the surge, HMH forecasted the number of beds that might beneeded during the peak of the outbreak. At the time, the vICU had already started providingcoverage to the Neuro-ICU during the night shift. The next unit scheduled to go live with vICUcoverage was the 24-bed MICU. Instead, on March 12th, 2020, the MICU became the first dedicatedCOVID-19 ICU at HMH. The novelty of the coronavirus, combined with the complexity of treatingCOVID-19 patients, forced HMH to redirect all of its critical care intensivists to the COVID-19 units,providing 24-hour bedside coverage.
Staffing Changes in Response to COVID-19 Surge
By March 26th, 2020, the first COVID-19 ICU had reached near capacity, requiring a seconddedicated COVID-19 ICU, which was created by converting the 36-bed Neuro-ICU. By April 8th,2020, the Neuro-ICU had also reached full capacity, and a third COVID-19 ICU was set up byconverting a 19-bed step-down unit. For all of the COVID-19 ICUs, the staffing ratio for intensivist topatients was 1:8 to 1:12 during the day and 1:12 to 1:18 during the night. Since the hospital hadredirected all of the critical care physician-workforce to the COVID-19 ICUs, the non-COVID-19 ICUswere managed by cardiovascular surgeons, cardiologists, neurosurgeons, and acute care surgeons.
To fill out the newly depleted critical care expertise in the non-COVID-19 ICUs, HMH expanded thenight vICU program to provide urgent, emergent, and code blue support for all ICUs, including theCOVID-19 ICUs. The bedside teams in the non-COVID-19 ICUs had advanced practice providers(APPs) that reached out to the vMDs for critical care support and admitted medicine overflowpatients with the vMDs at night. HMH’s next step in the surge planning was to open up the vICU inthe daytime, providing critical care support from vMDs and vRNs during the day for non-COVID-19ICUs.
In the first week of April, HMH began surveillance testing of its medical staff, and many frontlineemployees tested positive for COVID-19. All the COVID-19-positive workers, although asymptomatic,were taken off clinical duties from ICUs, and the resulting staff shortages expedited the vICUintegration with the rest of the ICUs. Before staff shortages, the vICU staff was only providingsupport for emergent/urgent and code blue situations. However, the expanded vICU staff began tocover admissions and triage during the night for more comprehensive integration.
Results
ICU Expansions in Response to COVID-19 Surge
It is well documented that family engagement has an enormous positive impact by decreasinganxiety, confusion, agitation, and delirium in the ICU patient [8-10]. Evidence suggests that
https://preprints.jmir.org/preprint/20143 [unpublished, non-peer-reviewed preprint]
JMIR Preprints Dhala et al
separating families from the patients can adversely impact the patient’s feelings of security and ofultimate outcome [11].
During the COVID-19 pandemic, nearly all hospitals disallowed visitors for adult in-patients,including all COVID-19 and non-COVID-19 ICU patients. While video chat technology (e.g., FaceTime,Skype) is commonly available among patients and their families, in an ICU setting with a highlyinfectious, critically-ill cohort of patients, who may be sedated and frequently intubated, the use ofsuch common technology was not feasible as it would require staff to bring in and position theequipment (e.g., smartphone or tablet) while using personal protective equipment (PPE).
However, the vICU infrastructure provided a readily available and much more accessible means ofconnecting the COVID-19 patients and families. HMH began to offer this technology to the familiesfor emotional support and improved patient care. Two virtual RNs (in the operation center) weretasked with reaching out to the bedside teams and collaborating with the bedside nurses,physicians, and unit managers to gain access to the patients’ families. Family members receivedlinks on their smartphones that instantly connected them with their loved one’s ICU room, using theConsultant Bridge feature. The vICU patients logged about 20-40 calls per day using the ConsultantBridge during this period. Because restrictions on visitors also applied to non-COVID-19 patients andtheir families, the Consultant Bridge was used for all ICU patients. The results of a short post-callquality assessment survey showed an overwhelming satisfaction with access to the patient usingvICU technology.
Palliative Care for ICU Patients
In standard palliative care situations, family members are involved in the decision-making process atthe bedside. However, in a pandemic situation, when the family members cannot be near theirterminally-ill loved ones, the vICU technology may provide a vehicle to carry out the critical stepswith the full participation of the palliative care team and the family members. Similar to regularvisitations, we used the Consultant Bridge feature of vICU to enable palliative care.
Staffing Changes in Response to COVID-19 Surge
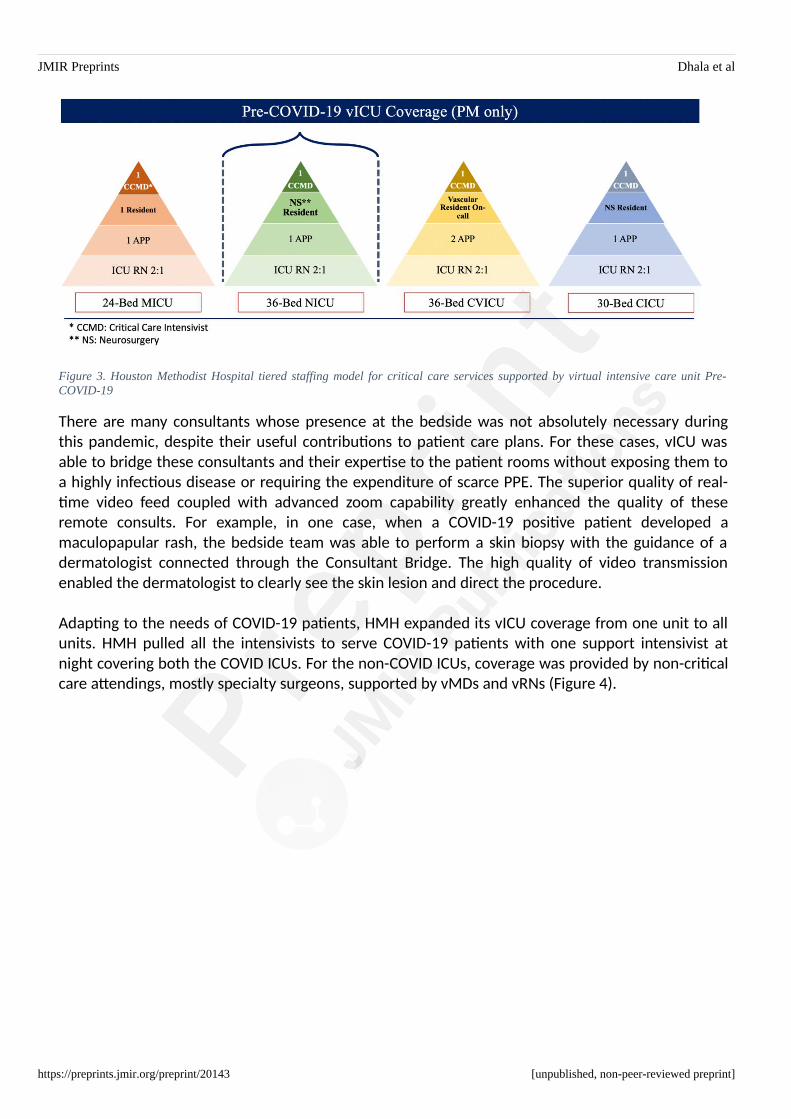
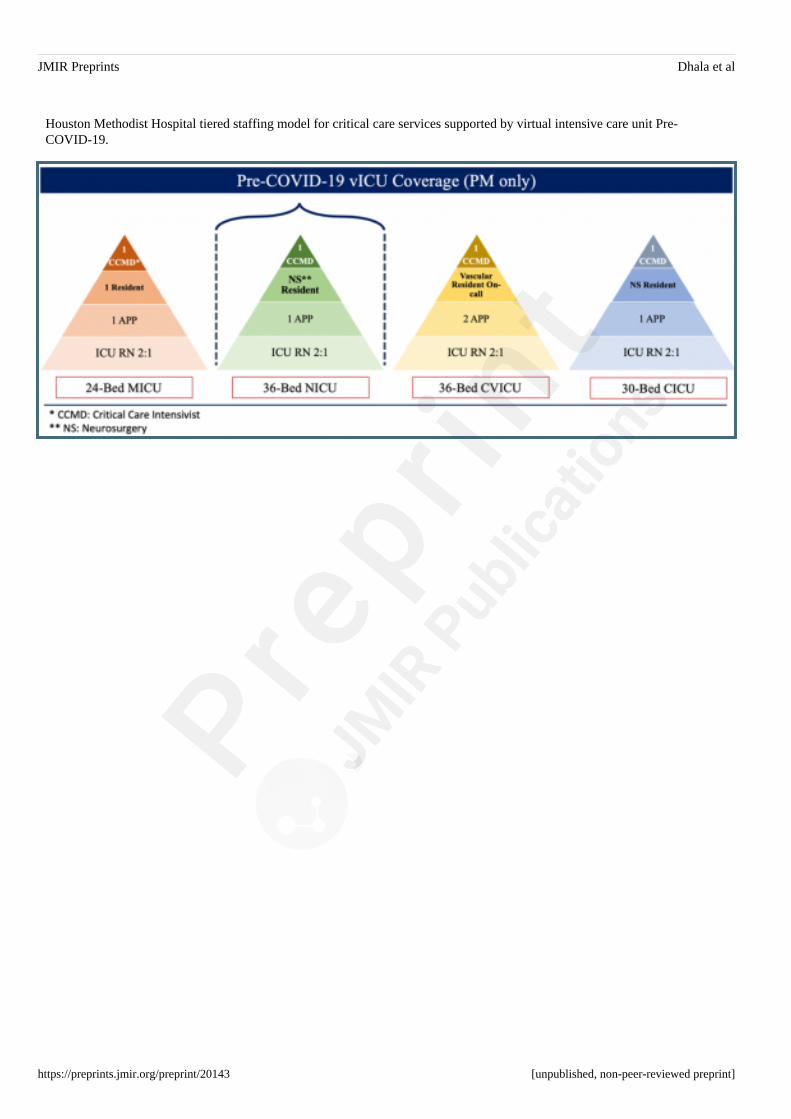
Demands of the COVID-19 pandemic resulted in a tiered staffing model with vICU providingessential support to all the ICUs. This model bears a strong resemblance to the tiered staffing modeldescribed by the Society of Critical Care Medicine for surge planning [7]. Prior to the COVID-19pandemic, HMH had commenced its vICU program, providing nocturnal coverage for the Neuro-ICUcombined with full workflow implementation. During this period, HMH used four in-houseintensivists and the following staffing ratios: 2:1 for ICU RNs; 1 APP for 24-beds; 1 resident on-call inthe night; and 1 critical care bedside MD per unit (4 in total) (Figure 3).
https://preprints.jmir.org/preprint/20143 [unpublished, non-peer-reviewed preprint]
JMIR Preprints Dhala et al
Figure 3. Houston Methodist Hospital tiered staffing model for critical care services supported by virtual intensive care unit Pre-COVID-19
There are many consultants whose presence at the bedside was not absolutely necessary duringthis pandemic, despite their useful contributions to patient care plans. For these cases, vICU wasable to bridge these consultants and their expertise to the patient rooms without exposing them toa highly infectious disease or requiring the expenditure of scarce PPE. The superior quality of real-time video feed coupled with advanced zoom capability greatly enhanced the quality of theseremote consults. For example, in one case, when a COVID-19 positive patient developed amaculopapular rash, the bedside team was able to perform a skin biopsy with the guidance of adermatologist connected through the Consultant Bridge. The high quality of video transmissionenabled the dermatologist to clearly see the skin lesion and direct the procedure.
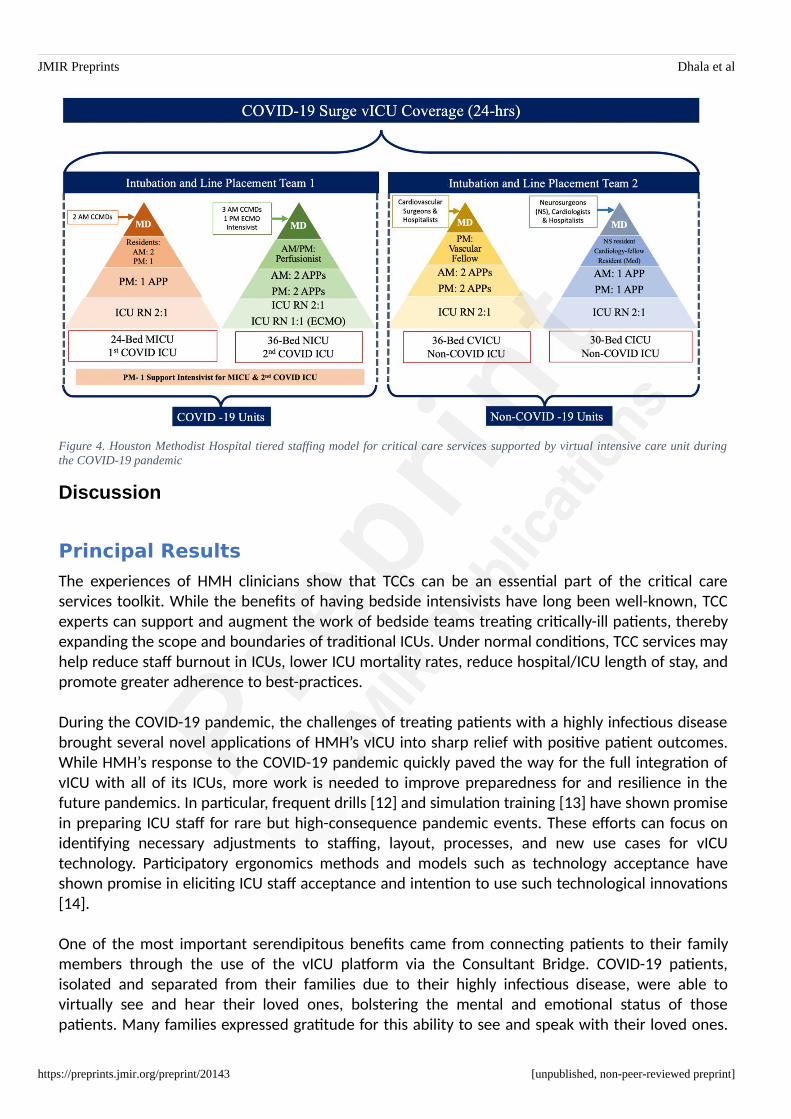
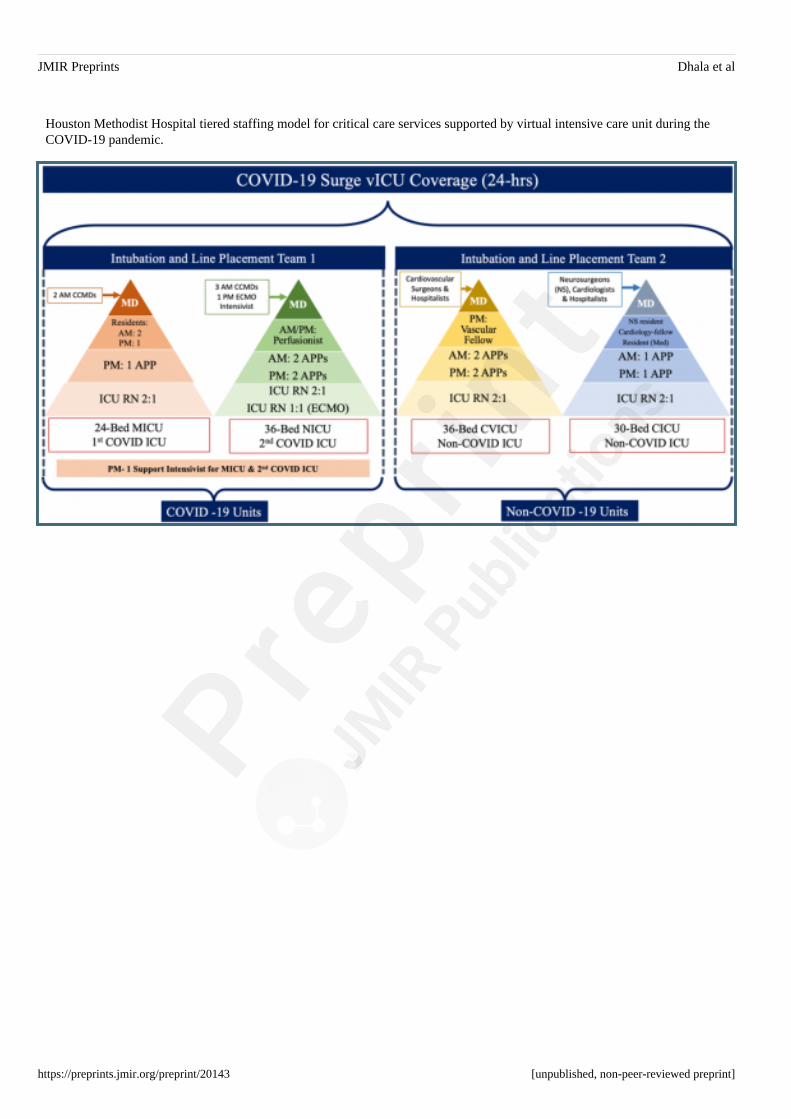
Adapting to the needs of COVID-19 patients, HMH expanded its vICU coverage from one unit to allunits. HMH pulled all the intensivists to serve COVID-19 patients with one support intensivist atnight covering both the COVID ICUs. For the non-COVID ICUs, coverage was provided by non-criticalcare attendings, mostly specialty surgeons, supported by vMDs and vRNs (Figure 4).
https://preprints.jmir.org/preprint/20143 [unpublished, non-peer-reviewed preprint]
JMIR Preprints Dhala et al
Figure 4. Houston Methodist Hospital tiered staffing model for critical care services supported by virtual intensive care unit duringthe COVID-19 pandemic
Discussion
Principal Results
The experiences of HMH clinicians show that TCCs can be an essential part of the critical careservices toolkit. While the benefits of having bedside intensivists have long been well-known, TCCexperts can support and augment the work of bedside teams treating critically-ill patients, therebyexpanding the scope and boundaries of traditional ICUs. Under normal conditions, TCC services mayhelp reduce staff burnout in ICUs, lower ICU mortality rates, reduce hospital/ICU length of stay, andpromote greater adherence to best-practices.
During the COVID-19 pandemic, the challenges of treating patients with a highly infectious diseasebrought several novel applications of HMH’s vICU into sharp relief with positive patient outcomes.While HMH’s response to the COVID-19 pandemic quickly paved the way for the full integration ofvICU with all of its ICUs, more work is needed to improve preparedness for and resilience in thefuture pandemics. In particular, frequent drills [12] and simulation training [13] have shown promisein preparing ICU staff for rare but high-consequence pandemic events. These efforts can focus onidentifying necessary adjustments to staffing, layout, processes, and new use cases for vICUtechnology. Participatory ergonomics methods and models such as technology acceptance haveshown promise in eliciting ICU staff acceptance and intention to use such technological innovations[14].
One of the most important serendipitous benefits came from connecting patients to their familymembers through the use of the vICU platform via the Consultant Bridge. COVID-19 patients,isolated and separated from their families due to their highly infectious disease, were able tovirtually see and hear their loved ones, bolstering the mental and emotional status of thosepatients. Many families expressed gratitude for this ability to see and speak with their loved ones.
https://preprints.jmir.org/preprint/20143 [unpublished, non-peer-reviewed preprint]
JMIR Preprints Dhala et al
We have observed a tremendous potential in using this technology and believe that even non-ICUunits may benefit from some form of telepresence technology to facilitate family engagement.While challenges related to privacy and security exist, a recent attitude shift towards viewing familymembers as partners in shared decision-making [15] sets the stage for a potential “open” virtualICU.
One of the significant contributors to burnout among HMH ICU providers was the anxiety associatedwith PPE shortages and exposure [16]. The use of the vICU provided a unique level of protection tothe medical staff assigned to COVID-19 units. The ICU staff were given local access to patient roomsby vICU enabled laptops that allowed the bedside doctors and nurses to camera-into the patient’sroom without having to don and doff protective gear each time when checking on a patient. Suchremote access reduced the usage of PPEs, which were already in short supply. The vICU’s ConsultantBridge also allowed specialty consultants from extracorporeal membrane oxygenation (ECMO)specialists, cardiology to endocrinology to examine a COVID-19 patient virtually.
Limitations
During the surge period, all of the critical care physicians were conscripted to work in the COVID-19ICUs, leaving the non-COVID-19 patients to be managed by non-critical care physicians and surgeonswith support and oversight by critical care specialists in the vICU. While this adaptive behavior was agood indicator of resilience, the development of protocols informed by simulated and proactiveefforts may provide more explicit guidelines for future staffing adjustments. In addition, while thetiered staffing model documented here shows promise for future pandemic surge planning, morework is warranted to improve this model and develop generalizable guidelines for optimal andflexible allocation of resources during a pandemic.
Conclusions
Tele-critical care has been established as an advantageous mechanism for the delivery of criticalcare expertise. The current COVID-19 pandemic has brought to light multiple new usefulapplications that could be transformative in how tele-critical care is perceived and deployed in thefuture, especially during highly infectious disease outbreaks. However, further research is requiredto examine the impact of innovative applications of tele-critical care in the treatment of critically illpatients.
Acknowledgments
Authors do not have any sources of funding to report.
Conflict of interest
Authors do not have any conflicts of interest or
Abbreviations
APP: advanced practice providersAV: audiovisualCICU: cardiac intensive care unit
https://preprints.jmir.org/preprint/20143 [unpublished, non-peer-reviewed preprint]
JMIR Preprints Dhala et al
COVID-19: coronavirus disease 2019CVICU: cardiovascular intensive care unitECMO: extracorporeal membrane oxygenationHMH: Houston Methodist HospitalICU: intensive care unitMICU: medical intensive care unitNeuro-ICU: neurology intensive care unitPPE: personal protective equipmentTCC: tele-critical careTMC: Texas Medical CentervICU: virtual intensive care unitvMD: virtual medical doctorvRN: virtual registered nurse
References
1. Santangelo, G. New NIH resource to analyze COVID-19 literature: The COVID-19 portfoliotool. Available at: https://nexus.od.nih.gov/all/2020/04/15/new-nih-resource-to-analyze-covid-19-literature-the-covid-19-portfolio-tool/. Accessed April 21, 2020.
2. Rosenfeld BA, Dorman T, Breslow MJ, et al: Intensive care unit telemedicine: Alternateparadigm for providing continuous intensivist care. Crit Care Med 2000; 28(12):3925–31.
3. Celi LA, Hassan E, Marquardt C, et al: The eICU: It’s not just telemedicine. Crit CareMed 2001; 29(8):N183-N189.
4. Kahn JM., Le TQ, Barnato AE, et al: ICU telemedicine and critical care mortality: A nationaleffectiveness study. Med Care 2016; 54(3):319.
5. Udeh C, Udeh B, Rahman N, et al: Telemedicine/virtual ICU: Where are we and where arewe going? Methodist Debakey Cardiovasc J 2018; 14(2):126-133.
6. Subramanian S, Pamplin JC, Hravnak M, et al: Tele-Critical Care: An update from theSociety of Critical Care Medicine Tele-ICU Committee. Crit Care Med 2020; 48(4):553-561.
7. Halpern NA, Tan KS, Society of Critical Care Medicine Ventilator Taskforce: US ICUresource availability for COVID-19. Version 2, March 25, 2020. Available at:https://sccm.org/getattachment/Blog/March-2020/United-States-Resource-Availability-for-COVID-19/United-States-Resource-Availability-for-COVID-19.pdf. Accessed April 21,2020.
8. Volland J, Fisher A, Drexler D: Delirium and dementia in the intensive care unit: increasingawareness for decreasing risk, improving outcomes, and family engagement. Dimens CritCare Nurs 2015; 34(5):259-264.
9. Ely EW. The ABCDEF bundle: science and philosophy of how ICU liberation serves patientsand families. Crit Care Med. 2017 Feb; 45(2):321.
10. Marra A, Ely EW, Pandharipande PP, et al: The ABCDEF bundle in critical care. Crit CareClin 2017; 33(2):225-243.
11. Giannini A: The "open" ICU: Not just a question of time. Minerva Anestesiol 2010; 76(2):89.12. King MA, Niven AS, Beninati W, et al. Evacuation of the ICU: Care of the critically ill and
injured during pandemics and disasters: CHEST consensus statement. Chest 2014;146(4):e44S-e60S.
13. Brazzi L, Lissoni A, Panigada M, et al: Simulation-based training of extracorporealmembrane oxygenation during H1N1 influenza pandemic: The Italian experience. SimulHealthc 2012; 7(1):32-34.
14. Kowitlawakul Y: The technology acceptance model: predicting nurses' intention to usetelemedicine technology (eICU). Comput Inform Nurs 2011; 29(7):411-418.
https://preprints.jmir.org/preprint/20143 [unpublished, non-peer-reviewed preprint]
JMIR Preprints Dhala et al
15. Azoulay E, Chaize M, Kentish-Barnes N. Involvement of ICU families in decisions: Fine-tuning the partnership. Ann Intensive Care 2014; 4(1):37.
16. Sasangohar F, Jones SL, Masud FN, et al: Provider burnout and fatigue during COVID-19pandemic: Lessons learned from a high-volume intensive care unit. Anesth Analg 2020 Apr 9;epub ahead of print. doi:10.1213/ANE.0000000000004866
https://preprints.jmir.org/preprint/20143 [unpublished, non-peer-reviewed preprint]
JMIR Preprints Dhala et al
Supplementary Files
https://preprints.jmir.org/preprint/20143 [unpublished, non-peer-reviewed preprint]
JMIR Preprints Dhala et al
Figures
https://preprints.jmir.org/preprint/20143 [unpublished, non-peer-reviewed preprint]
JMIR Preprints Dhala et al
Houston area COVID-19 cases from March 13-April 21, 2020 (dashed line) compared to Houston Methodist cases (solid lines).
https://preprints.jmir.org/preprint/20143 [unpublished, non-peer-reviewed preprint]
JMIR Preprints Dhala et al
Virtual intensive care unit audio/video equipment installed in an ICU room (left) and caller view (right); For the purposes ofillustration, one of the hospital staff played the role of the patient. The authors played the role of the caller.
https://preprints.jmir.org/preprint/20143 [unpublished, non-peer-reviewed preprint]
JMIR Preprints Dhala et al
Houston Methodist Hospital tiered staffing model for critical care services supported by virtual intensive care unit Pre-COVID-19.
https://preprints.jmir.org/preprint/20143 [unpublished, non-peer-reviewed preprint]
JMIR Preprints Dhala et al
Houston Methodist Hospital tiered staffing model for critical care services supported by virtual intensive care unit during theCOVID-19 pandemic.
Powered by TCPDF (www.tcpdf.org)
https://preprints.jmir.org/preprint/20143 [unpublished, non-peer-reviewed preprint]





























