Embed Size (px)
Citation preview
NEW RESEARCH
Psychiatric Disorders in Extremely PretermChildren: Longitudinal Finding at Age
11 Years in the EPICure StudySamantha Johnson, Ph.D., CPsychol., Chris Hollis, Ph.D., MRCPsych., Puja Kochhar, B.Sc.,
Enid Hennessy, M.Sc., Dieter Wolke, Ph.D., Dipl-Psych, CPsychol.,Neil Marlow, D.M., FMedSci.
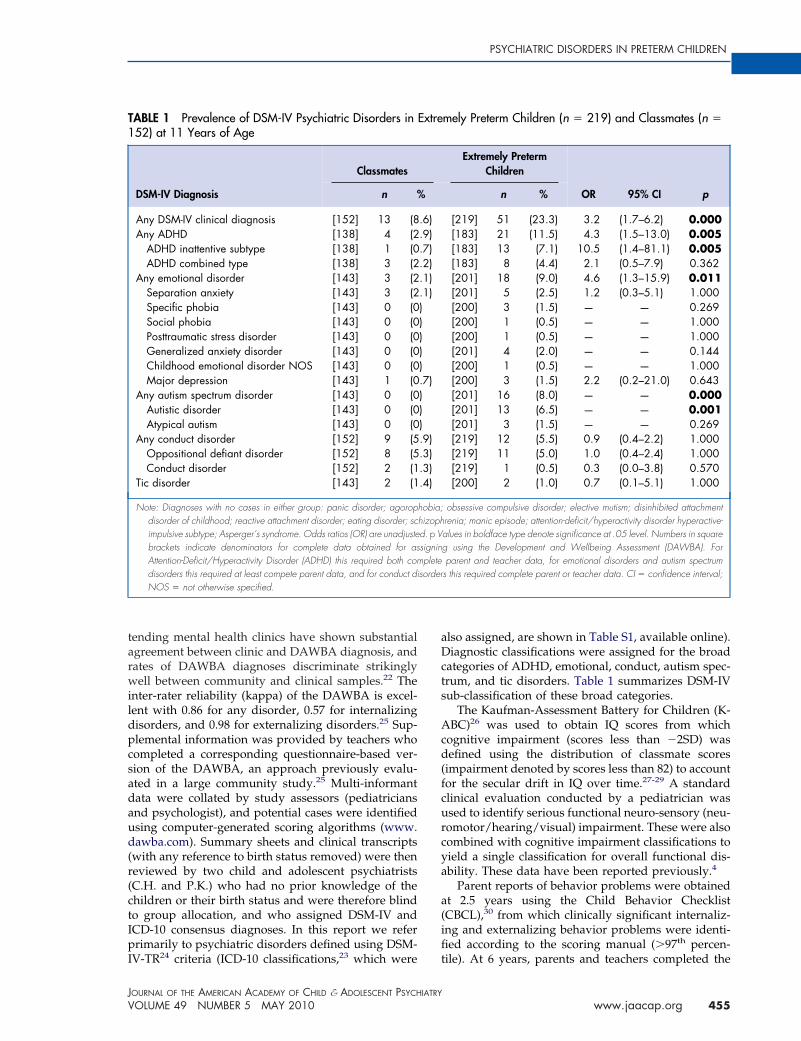
Objective: To investigate the prevalence and risk factors for psychiatric disorders in extremelypreterm children. Method: All babies born �26 weeks gestation in the United Kingdom andIreland from March through December 1995 were recruited to the EPICure Study. Of 307 survivorsat 11 years of age, 219 (71%) were assessed alongside 153 term-born classmates. Parents completeda structured psychiatric interview about their child, and teachers completed a correspondingquestionnaire from which DSM-IV diagnoses were assigned for 219 (100%) extremely pretermchildren and 152 (99%) classmates. An IQ test and a physical evaluation were also administered.Longitudinal data were available for extremely preterm children. Results: Extremely pretermchildren were more than three times more likely to have a psychiatric disorder than classmates(23% vs. 9%; odds ratio [OR] � 3.2; 95% confidence interval [CI] � 1.7, 6.2). Risk was significantlyincreased for: attention-deficit/hyperactivity disorder (ADHD; 11.5% vs. 2.9%; OR � 4.3; CI � 1.5to 13.0), with increased risk for ADHD inattentive subtype (OR � 10.5; CI � 1.4 to 81.1) but notADHD combined subtype (OR � 2.1; CI � 0.5 to 7.9); emotional disorders (9.0% vs. 2.1%; OR �4.6; CI � 1.3 to 15.9), with increased risk for anxiety disorders (OR � 3.5; CI � 1.0 to 12.4); andautism spectrum disorders (8.0% vs. 0%; p � .000). Psychiatric disorders were significantlyassociated with cognitive impairment (OR � 3.5; CI � 1.8 to 6.4). Parent-reported behavioralproblems at 2.5 and 6 years were independent predictors of psychiatric disorders at 11 years.Conclusions: Extremely preterm children are at increased risk for ADHD, emotional disorders,and autism spectrum disorders at 11 years of age. The mechanism of association with psychiatricdisorder may include both cognitive impairment and early traumatic experiences that have animpact on both child and parent. Early screening for cognitive and behavioral problems mayidentify those at greatest risk. J. Am. Acad. Child Adolesc. Psychiatry, 2010;49(5):453–463. KeyWords: extremely preterm, psychiatric disorders, risk factors, ADHD, autism
bpstcatTlmisfi
T he sequelae of very preterm birth have beenincreasingly well documented since the 1990s,when significant improvements in neonatal
intensive care were paralleled by an increase insurvival rates for extremely preterm births.1 Popu-lation-based studies have shown that children bornextremely preterm (�26 weeks) or with extremelylow birth weight (ELBW; �1,000 g) are at high riskfor later cognitive, neuromotor, and sensory mor-
This article is the subject of an editorial by Dr. Joan L. Luby onpage 439.Supplemental material cited in this article is available online.
m
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 49 NUMBER 5 MAY 2010
idity, which are present in up to 50% of extremelyreterm survivors at 11 years of age.2-4 Althoughevere cerebral palsy, blindness, and deafness con-inue to pose threats, it is increasingly clear thatognitive impairments are the most prevalent dis-bility, accounting for the vast majority of func-ional disability in this population at school age.4
here is also increasing evidence of a high preva-ence of more subtle, neuropsychological impair-
ents in this population, with studies document-ng deficits in a range of visuo-spatial processes,ensorimotor skills, and attention and executiveunctions,5,6 with learning disabilities documentedn up to 40% of extremely preterm survivors in
iddle childhood.7 Emerging studies have also
453www.jaacap.org

p(ay7(mimaaa
ctceatcmds1mddt
sdargwttitrrpasW
MT(ga(f1acv
JOHNSON et al.
shown a significant excess of parent- and teacher-reported behavioral and emotional problems inthese children, with studies most consistently iden-tifying greatest risks for problems in domains ofattention, concentration, and social relationshipswith peers.8,9 Clinically significant behavioral prob-lems, identified by both parent and teacher reports,have been found in up to 20% of extremely pretermchildren at 6 years of age, with attention-deficit/hyperactivity disorder (ADHD) symptoms re-ported in up to 31% of survivors.10,11 The mostrecent reports have also identified an increasedprevalence of social and communication difficultiesand autism spectrum disorder (ASD) symptoms inthis population.9,12,13
The vast majority of previous studies haveused screening questionnaires to assess behav-ioral problems. Four studies that have used di-agnostic psychiatric evaluations have reported22% to 28% prevalence of clinical diagnoses inlow-birthweight (�2,000 g)14,15 and very-low-birthweight (�1,500 g) children at school age,16,17
with greatest risk for anxiety disorders andADHD. Two studies also report a significantlyincreased prevalence of ASD of 1% to 2%.14,17
However, these studies included all childrenborn with low birthweight who were thus farmore gestationally mature. These populationsare likely to be at considerably less risk thanextremely preterm children, given the significantassociation of adverse neuro-cognitive outcomeswith decreasing gestational age at birth.18,19 Thehigh prevalence of neuro-morbidity in extremelypreterm children4 makes it likely that psychiatricproblems may also be increased despite contin-ued improvements in care and in survival. Todate, the prevalence of diagnosed psychiatricdisorders in a contemporary population of ex-tremely preterm survivors has not been system-atically investigated.
The objectives of this study were to investigatethe prevalence, correlates, and precursors of psy-chiatric disorders in a whole population of ex-tremely preterm children at 11 years of age.
METHODAll babies born at �26 weeks gestation and admittedfor neonatal intensive care in the United Kingdom andIreland from March through December 1995 (n � 811)were identified as part of the EPICure Study.20 Subse-quent follow-up studies were conducted at 2.5, 6, and11 years of age of all surviving infants, including
singleton and multiple births. Parental consent was iJOURN
454 www.jaacap.org
rovided for formal assessments on 283 (92%) and 24178%) of 308 survivors at 2.5 years21 and 6 years ofge,3 respectively. Most recently, of 307 survivors at 11ears of age, 11 (4%) moved abroad, and the parents of7 (25%) did not provide consent. The remaining 21971%) children were assessed (median age: 10 years, 11
onths; range: 121 to 145 months). Information relat-ng to perinatal variables and neonatal course were
ostly available for all extremely preterm children,nd longitudinal data were available for 213 of 219ssessed at 2.5 years and for 202 of 219 who were alsossessed at 6 years.
At the 6-year follow-up, for each extremely pretermhild attending mainstream school, a child born aterm was selected randomly where possible from threelassmates closest in age and of the same sex andthnicity.3 At 11 years, where the preterm child was atdifferent school to the original 6-year classmate, or
he original classmate declined to participate, a newlassmate was selected where possible using the sameethodology, resulting in 43 new comparison chil-
ren.4,7 Thus 153 classmates for whom parental con-ent was obtained were assessed at 11 years (median:0 years 11 months; range: 117 to 147 months). Class-ates were not selected for extremely preterm chil-
ren in special schools. There were no significantifferences in age, sex, and ethnicity between ex-
remely preterm children and classmates.Parents and children were given information
heets, and parents provided informed consent. Chil-ren were assessed by a pediatrician and psychologistt school. As school assessments were scheduled by aesearch manager, and as pediatricians and psycholo-ists had no prior contact with participants, assessorsere thus blind to children’s group allocation at the
ime of testing. To obtain behavioral data, parents andeachers completed questionnaires, and parents partic-pated in a structured psychiatric interview regardingheir child’s behavior. Transcripts obtained from pa-ental assessments and teacher questionnaires wereeviewed by two independent child and adolescentsychiatrists who had no prior knowledge of the childnd were thus blind to study group allocation. Thetudy was approved by the Southampton and South
est Hampshire NHS Research Ethics Committee.
easureshe Development And Well Being Assessment
DAWBA),22 a structured psychiatric evaluation re-arding children’s development and behavior, wasdministered to parents via a telephone interview92%) or parents participated in an online version (8%)rom which information required for assigning ICD-023 and DSM-IV-TR24 diagnoses of childhood psychi-tric disorders was obtained. The questions and itemsovered by the telephone and on-line DAWBA inter-iew were identical. In previous validation studies,
ndependent DAWBA reassessments of children at-
AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 49 NUMBER 5 MAY 2010
aDcts
Acd(fcurcya
a(ifi
PSYCHIATRIC DISORDERS IN PRETERM CHILDREN
tending mental health clinics have shown substantialagreement between clinic and DAWBA diagnosis, andrates of DAWBA diagnoses discriminate strikinglywell between community and clinical samples.22 Theinter-rater reliability (kappa) of the DAWBA is excel-lent with 0.86 for any disorder, 0.57 for internalizingdisorders, and 0.98 for externalizing disorders.25 Sup-plemental information was provided by teachers whocompleted a corresponding questionnaire-based ver-sion of the DAWBA, an approach previously evalu-ated in a large community study.25 Multi-informantdata were collated by study assessors (pediatriciansand psychologist), and potential cases were identifiedusing computer-generated scoring algorithms (www.dawba.com). Summary sheets and clinical transcripts(with any reference to birth status removed) were thenreviewed by two child and adolescent psychiatrists(C.H. and P.K.) who had no prior knowledge of thechildren or their birth status and were therefore blindto group allocation, and who assigned DSM-IV andICD-10 consensus diagnoses. In this report we referprimarily to psychiatric disorders defined using DSM-
TABLE 1 Prevalence of DSM-IV Psychiatric Disorders in152) at 11 Years of Age
DSM-IV Diagnosis
Classmates
n %
Any DSM-IV clinical diagnosis [152] 13 (8Any ADHD [138] 4 (2
ADHD inattentive subtype [138] 1 (0ADHD combined type [138] 3 (2
Any emotional disorder [143] 3 (2Separation anxiety [143] 3 (2Specific phobia [143] 0 (0Social phobia [143] 0 (0Posttraumatic stress disorder [143] 0 (0Generalized anxiety disorder [143] 0 (0Childhood emotional disorder NOS [143] 0 (0Major depression [143] 1 (0
Any autism spectrum disorder [143] 0 (0Autistic disorder [143] 0 (0Atypical autism [143] 0 (0
Any conduct disorder [152] 9 (5Oppositional defiant disorder [152] 8 (5Conduct disorder [152] 2 (1
Tic disorder [143] 2 (1
Note: Diagnoses with no cases in either group: panic disorder; agoropdisorder of childhood; reactive attachment disorder; eating disorder; scimpulsive subtype; Asperger’s syndrome. Odds ratios (OR) are unadjustebrackets indicate denominators for complete data obtained for asAttention-Deficit/Hyperactivity Disorder (ADHD) this required both comdisorders this required at least compete parent data, and for conduct diNOS � not otherwise specified.
IV-TR24 criteria (ICD-10 classifications,23 which were t
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 49 NUMBER 5 MAY 2010
lso assigned, are shown in Table S1, available online).iagnostic classifications were assigned for the broad
ategories of ADHD, emotional, conduct, autism spec-rum, and tic disorders. Table 1 summarizes DSM-IVub-classification of these broad categories.
The Kaufman-Assessment Battery for Children (K-BC)26 was used to obtain IQ scores from which
ognitive impairment (scores less than �2SD) wasefined using the distribution of classmate scores
impairment denoted by scores less than 82) to accountor the secular drift in IQ over time.27-29 A standardlinical evaluation conducted by a pediatrician wassed to identify serious functional neuro-sensory (neu-omotor/hearing/visual) impairment. These were alsoombined with cognitive impairment classifications toield a single classification for overall functional dis-bility. These data have been reported previously.4
Parent reports of behavior problems were obtainedt 2.5 years using the Child Behavior ChecklistCBCL),30 from which clinically significant internaliz-ng and externalizing behavior problems were identi-ed according to the scoring manual (�97th percen-
mely Preterm Children (n � 219) and Classmates (n �
Extremely PretermChildren
OR 95% CI pn %
[219] 51 (23.3) 3.2 (1.7–6.2) 0.000[183] 21 (11.5) 4.3 (1.5–13.0) 0.005[183] 13 (7.1) 10.5 (1.4–81.1) 0.005[183] 8 (4.4) 2.1 (0.5–7.9) 0.362[201] 18 (9.0) 4.6 (1.3–15.9) 0.011[201] 5 (2.5) 1.2 (0.3–5.1) 1.000[200] 3 (1.5) — — 0.269[200] 1 (0.5) — — 1.000[200] 1 (0.5) — — 1.000[201] 4 (2.0) — — 0.144[200] 1 (0.5) — — 1.000[200] 3 (1.5) 2.2 (0.2–21.0) 0.643[201] 16 (8.0) — — 0.000[201] 13 (6.5) — — 0.001[201] 3 (1.5) — — 0.269[219] 12 (5.5) 0.9 (0.4–2.2) 1.000[219] 11 (5.0) 1.0 (0.4–2.4) 1.000[219] 1 (0.5) 0.3 (0.0–3.8) 0.570[200] 2 (1.0) 0.7 (0.1–5.1) 1.000
obsessive compulsive disorder; elective mutism; disinhibited attachmentrenia; manic episode; attention-deficit/hyperactivity disorder hyperactive-alues in boldface type denote significance at .05 level. Numbers in squareg using the Development and Wellbeing Assessment (DAWBA). Forparent and teacher data, for emotional disorders and autism spectrums this required complete parent or teacher data. CI � confidence interval;
Extre
.6)
.9)
.7)
.2)
.1)
.1)))))).7)))).9).3).3).4)
hobia;hizophd. p Vsigninplete
sorder
ile). At 6 years, parents and teachers completed the
455www.jaacap.org
Mdtsadsiivrptb
RDEywniadsn
PDemcp(
JOHNSON et al.
Strengths and Difficulties Questionnaire (SDQ)31 fromwhich scores above the 90th percentile have beenpreviously proposed to best identify children withclinically significant problems.31 The distribution ofclassmates scores were used to classify clinically sig-nificant difficulties in emotional, conduct, inattention/hyperactivity, and peer problems and for total behav-ioral difficulties. Congruence between parent andteacher reports of clinically significant difficulties wasused to classify pervasive problems in each domain.These data have been reported previously.10 Neonataldata were obtained at discharge from hospital forextremely preterm children. Parental socio-economicstatus (SES) at 11 years was classified into four cate-gories using the UK National Statistics Socio-EconomicClassification (I—Professional/Managerial; II—Inter-mediate; III—Routine/Manual; IV—Unemployed).32
Data AnalysisData were double-entered and verified. SPSS and Stata(S.J., E.H.) were used to compare rates of psychiatricdiagnoses between extremely preterm children andclassmates using two-tailed Fisher’s exact tests fordichotomous outcomes. Results are reported as oddsratios (OR) with 95% confidence intervals (CI). The riskof psychiatric diagnosis was further investigated ex-cluding children with neurosensory and cognitive im-pairment. Adjusted OR were investigated with sex andSES (I/II vs. III/IV) as covariates using logistic regres-sion. As adjustment for these variables had no signif-icant effects, unadjusted OR are reported throughout.Neonatal and neurodevelopmental outcome variablesat 2.5 and 6 years were used in univariate logisticregression to predict psychiatric diagnoses. A multi-variate forward stepwise procedure was applied toidentify independent factors associated with psychiat-ric diagnoses (adjusted OR) at three time points: neo-
TABLE 2 Factors Independently Associated with PsychiatAge
Variable
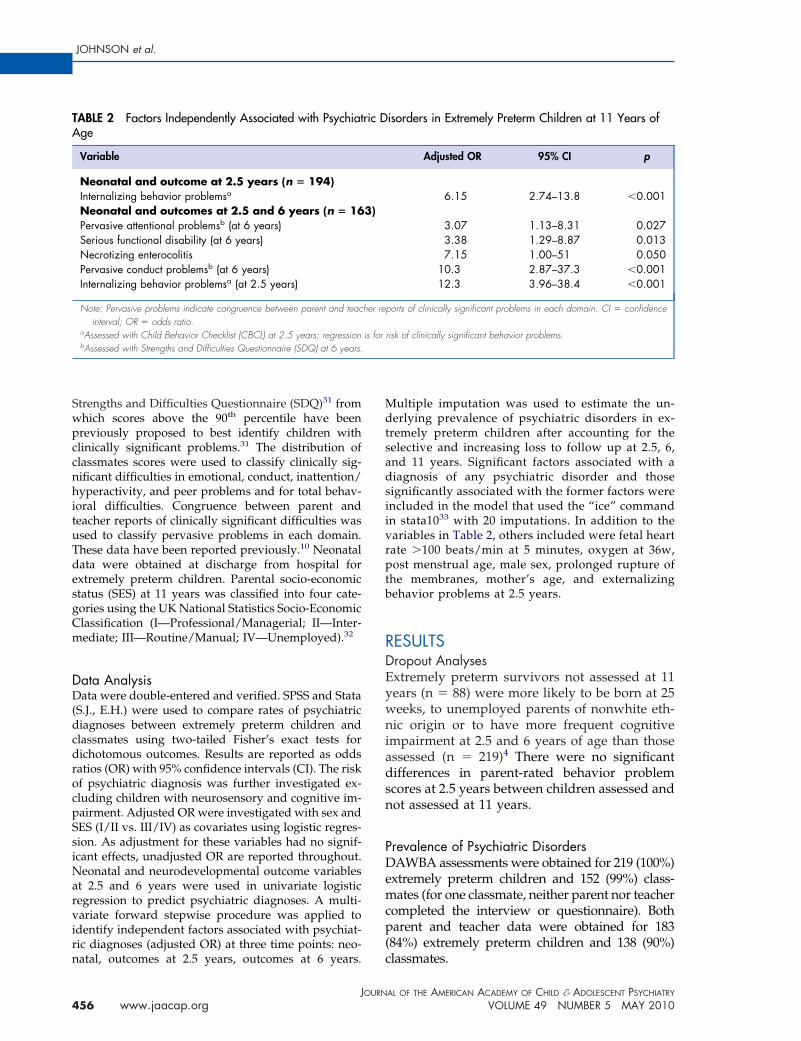
Neonatal and outcome at 2.5 years (n � 194)Internalizing behavior problemsa
Neonatal and outcomes at 2.5 and 6 years (n � 16Pervasive attentional problemsb (at 6 years)Serious functional disability (at 6 years)Necrotizing enterocolitisPervasive conduct problemsb (at 6 years)Internalizing behavior problemsa (at 2.5 years)
Note: Pervasive problems indicate congruence between parent and teacinterval; OR � odds ratio.
aAssessed with Child Behavior Checklist (CBCL) at 2.5 years; regressionbAssessed with Strengths and Difficulties Questionnaire (SDQ) at 6 years.
natal, outcomes at 2.5 years, outcomes at 6 years. c
JOURN
456 www.jaacap.org
ultiple imputation was used to estimate the un-erlying prevalence of psychiatric disorders in ex-
remely preterm children after accounting for theelective and increasing loss to follow up at 2.5, 6,nd 11 years. Significant factors associated with aiagnosis of any psychiatric disorder and thoseignificantly associated with the former factors werencluded in the model that used the “ice” commandn stata1033 with 20 imputations. In addition to theariables in Table 2, others included were fetal heartate �100 beats/min at 5 minutes, oxygen at 36w,ost menstrual age, male sex, prolonged rupture of
he membranes, mother’s age, and externalizingehavior problems at 2.5 years.
ESULTSropout Analysesxtremely preterm survivors not assessed at 11ears (n � 88) were more likely to be born at 25eeks, to unemployed parents of nonwhite eth-
ic origin or to have more frequent cognitivempairment at 2.5 and 6 years of age than thosessessed (n � 219)4 There were no significantifferences in parent-rated behavior problemcores at 2.5 years between children assessed andot assessed at 11 years.
revalence of Psychiatric DisordersAWBA assessments were obtained for 219 (100%)
xtremely preterm children and 152 (99%) class-ates (for one classmate, neither parent nor teacher
ompleted the interview or questionnaire). Botharent and teacher data were obtained for 183
84%) extremely preterm children and 138 (90%)
isorders in Extremely Preterm Children at 11 Years of
Adjusted OR 95% CI p
6.15 2.74–13.8 �0.001
3.07 1.13–8.31 0.0273.38 1.29–8.87 0.0137.15 1.00–51 0.050
10.3 2.87–37.3 �0.00112.3 3.96–38.4 �0.001
orts of clinically significant problems in each domain. CI � confidence
risk of clinically significant behavior problems.
ric D
3)
her rep
is for
lassmates.
AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 49 NUMBER 5 MAY 2010

wtfbocgdeOpfgcddoi
AOan(aAwtC(pla
OdOdcwtas
COfd(td
PSYCHIATRIC DISORDERS IN PRETERM CHILDREN
Extremely preterm children were more likelyto have a psychiatric disorder (23.3%) than class-mates (8.6%) (OR � 3.2, CI 1.7 to 6.2; Table 1).
Overall, 87 (40%) extremely preterm childrenand 2 (1.3%) classmates had serious cognitiveimpairment, and 35 (16%) extremely pretermchildren had serious neuro-sensory impairmentcompared with none of the classmates. Theseoutcomes have been published in detail else-where.4 Although there was no significant differ-ence in the rate of disorders among extremelypreterm children with and without neurosensoryimpairment (29% vs. 22%; OR � 1.4; CI � 0.6 to3.1), children with cognitive impairment weresignificantly more likely to have a disorder (37%vs. 14%; OR � 3.5; CI � 1.8 to 6.4). The preva-lence of psychiatric disorders in extremely pre-term children remained significantly increasedafter excluding children with neurosensory im-pairment but not after excluding those with cog-nitive impairment (Table 3). Using multiple im-putation to correct for selective loss to follow-up,the estimated proportion of all extremely pre-term survivors with psychiatric disorders rosemarginally from 23.3% to 25% (CI � 19.4% to31.1%).
Attention-Deficit/Hyperactivity DisorderAttention-deficit/hyperactivity Disorder (ADHD)was the most prevalent psychiatric disorder amongextremely preterm children, who were 4.3 timesmore likely to have ADHD compared with class-mates. The greatest risk was for ADHD inattentivesubtype (ADHD-I; Table 1). Of the four classmateswith ADHD, three (75%) had ADHD-combinedsubtype. In contrast, among the 21 extremely pre-term children with ADHD, eight (38%) had ADHDcombined subtype and 13 (62%) had ADHD-I.There was a nonsignificant trend toward increasedprevalence of ADHD in boys compared with girlsamong both classmates (5.1% vs. 1.3%; OR � 4.2;CI � 0.4 to 41.2) and preterm children (16.5% vs.7.1%; OR � 2.6; CI � 0.98 to 6.7). Children withcognitive impairment were five times more likelyto have ADHD than those without (20.8% vs. 5.4%;OR � 4.6; CI � 1.7 to 12.5). After excluding childrenwith cognitive impairment, the risk of ADHD inextremely preterm children was halved and nolonger significant (Table 3).
Emotional DisorderExtremely preterm children were four times
more likely to have an emotional disorder than wJOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 49 NUMBER 5 MAY 2010
ere classmates. All three classmates with emo-ional disorders had separation anxiety and wereemale. Extremely preterm children had aroader range of emotional disorders; of these, 14f 18 children had anxiety disorders, the mostommon of which were separation anxiety andeneralized anxiety disorder (Table 1). Anxietyisorders accounted for the significant excess ofmotional disorders overall (anxiety disorders:R � 3.5; CI � 1.0 to 12.4). Among extremelyreterm children, there were no significant dif-
erences in rates of emotional disorders by sex,estational age, neurosensory impairment, orognitive impairment. The risk for emotionalisorders was unaffected after excluding chil-ren with neurosensory impairment, and wasnly marginally lower after excluding cognitive
mpairment (Table 3).
utism Spectrum Disorderverall, 16 (8%) extremely preterm children had
utism spectrum disorder (ASD) compared withone of the classmates (Table 1). Of these, 136.5%) had autistic disorder, and 3 (1.5%) atypicalutism; none had Asperger’s disorder or otherSDs. Extremely preterm children with ASDere more likely to be male (OR � 3.9; CI � 1.2
o 12.4), to have cognitive impairment (OR � 3.7;I � 1.2 to 11.1), and to have functional disability
4.2; 1.3 to 13.6) than were their preterm counter-arts without ASD. Detailed analyses of corre-
ates and risk factors for ASD in this populationre published elsewhere.34
ppositional Defiant Disorder and Conductisorderppositional defiant disorder (ODD) and con-uct disorder (CD) were not significantly in-reased in extremely preterm children comparedith classmates (Table 1). Among extremely pre-
erm children, ODD/CD was not significantlyssociated with sex, gestational age, or neurosen-ory or cognitive impairment.
omorbid Psychiatric Disordersverall, 13 (5.9%) extremely preterm children and
our (2.6%) classmates had comorbid psychiatricisorders. Among extremely preterm children, 38
17.4%) had one disorder, nine children (4.1%) hadwo disorders, and four (1.9%) had more than twoisorders. Among classmates, these proportions
ere nine (5.9%), two (1.3%) and two (1.3%) respec-457www.jaacap.org
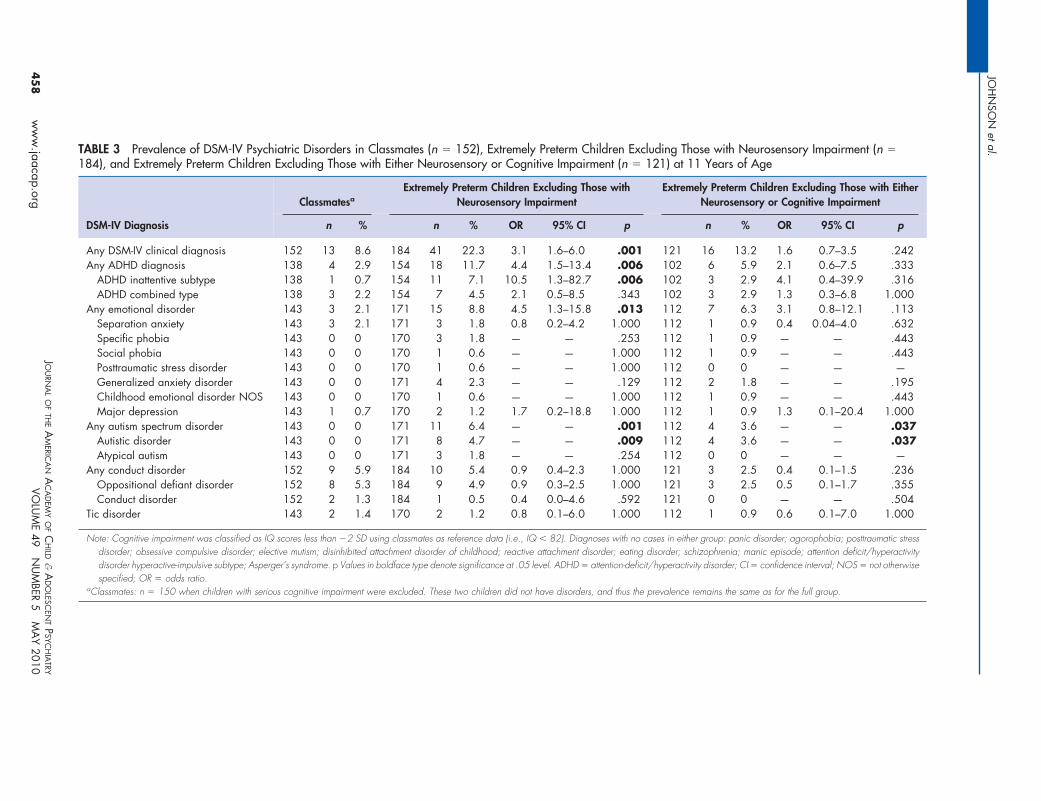
TABLE 3 Prevalence of DSM-IV Psychiatric Disorders in Classmates (n � 152), Extremely Preterm Children Excluding Those with Neurosensory Impairment (n �184), and Extremely Preterm Children Excluding Those with Either Neurosensory or Cognitive Impairment (n � 121) at 11 Years of Age
DSM-IV Diagnosis
ClassmatesaExtremely Preterm Children Excluding Those with
Neurosensory ImpairmentExtremely Preterm Children Excluding Those with Either
Neurosensory or Cognitive Impairment
n % n % OR 95% CI p n % OR 95% CI p
Any DSM-IV clinical diagnosis 152 13 8.6 184 41 22.3 3.1 1.6–6.0 .001 121 16 13.2 1.6 0.7–3.5 .242Any ADHD diagnosis 138 4 2.9 154 18 11.7 4.4 1.5–13.4 .006 102 6 5.9 2.1 0.6–7.5 .333
ADHD inattentive subtype 138 1 0.7 154 11 7.1 10.5 1.3–82.7 .006 102 3 2.9 4.1 0.4–39.9 .316ADHD combined type 138 3 2.2 154 7 4.5 2.1 0.5–8.5 .343 102 3 2.9 1.3 0.3–6.8 1.000
Any emotional disorder 143 3 2.1 171 15 8.8 4.5 1.3–15.8 .013 112 7 6.3 3.1 0.8–12.1 .113Separation anxiety 143 3 2.1 171 3 1.8 0.8 0.2–4.2 1.000 112 1 0.9 0.4 0.04–4.0 .632Specific phobia 143 0 0 170 3 1.8 — — .253 112 1 0.9 — — .443Social phobia 143 0 0 170 1 0.6 — — 1.000 112 1 0.9 — — .443Posttraumatic stress disorder 143 0 0 170 1 0.6 — — 1.000 112 0 0 — — —Generalized anxiety disorder 143 0 0 171 4 2.3 — — .129 112 2 1.8 — — .195Childhood emotional disorder NOS 143 0 0 170 1 0.6 — — 1.000 112 1 0.9 — — .443Major depression 143 1 0.7 170 2 1.2 1.7 0.2–18.8 1.000 112 1 0.9 1.3 0.1–20.4 1.000
Any autism spectrum disorder 143 0 0 171 11 6.4 — — .001 112 4 3.6 — — .037Autistic disorder 143 0 0 171 8 4.7 — — .009 112 4 3.6 — — .037Atypical autism 143 0 0 171 3 1.8 — — .254 112 0 0 — — —
Any conduct disorder 152 9 5.9 184 10 5.4 0.9 0.4–2.3 1.000 121 3 2.5 0.4 0.1–1.5 .236Oppositional defiant disorder 152 8 5.3 184 9 4.9 0.9 0.3–2.5 1.000 121 3 2.5 0.5 0.1–1.7 .355Conduct disorder 152 2 1.3 184 1 0.5 0.4 0.0–4.6 .592 121 0 0 — — .504
Tic disorder 143 2 1.4 170 2 1.2 0.8 0.1–6.0 1.000 112 1 0.9 0.6 0.1–7.0 1.000
Note: Cognitive impairment was classified as IQ scores less than �2 SD using classmates as reference data (i.e., IQ � 82). Diagnoses with no cases in either group: panic disorder; agorophobia; posttraumatic stressdisorder; obsessive compulsive disorder; elective mutism; disinhibited attachment disorder of childhood; reactive attachment disorder; eating disorder; schizophrenia; manic episode; attention deficit/hyperactivitydisorder hyperactive-impulsive subtype; Asperger’s syndrome. p Values in boldface type denote significance at .05 level. ADHD � attention-deficit/hyperactivity disorder; CI � confidence interval; NOS � not otherwisespecified; OR � odds ratio.
aClassmates: n � 150 when children with serious cognitive impairment were excluded. These two children did not have disorders, and thus the prevalence remains the same as for the full group.
JOH
NSO
Netal.
JOU
RNA
LO
FTH
EA
MERIC
AN
AC
AD
EMY
OF
CH
ILD&
AD
OLESC
ENT
PSYC
HIA
TRY
VOLU
ME
49N
UM
BER5
MA
Y2010
45
8w
ww
.jaacap.org

2rsrptqnarasct
sinatrwcrtAcspgopnArp
metgfidiaeaAptb
PSYCHIATRIC DISORDERS IN PRETERM CHILDREN
tively. Among children with psychiatric disorders,extremely preterm children were no more likely tohave comorbid disorders than classmates (25.5%vs. 30.8%; p � .732). Of 21 extremely pretermchildren with ADHD, 10 (47%) had comorbid psy-chiatric disorder: five (24%) had an ASD, 4 (19%)had an emotional disorder, and 6 (29%) had ODD/CD. Of four classmates with ADHD, all had acomorbid psychiatric disorder, of whom three(75%) had ODD/CD and one (25%) had an emo-tional disorder.
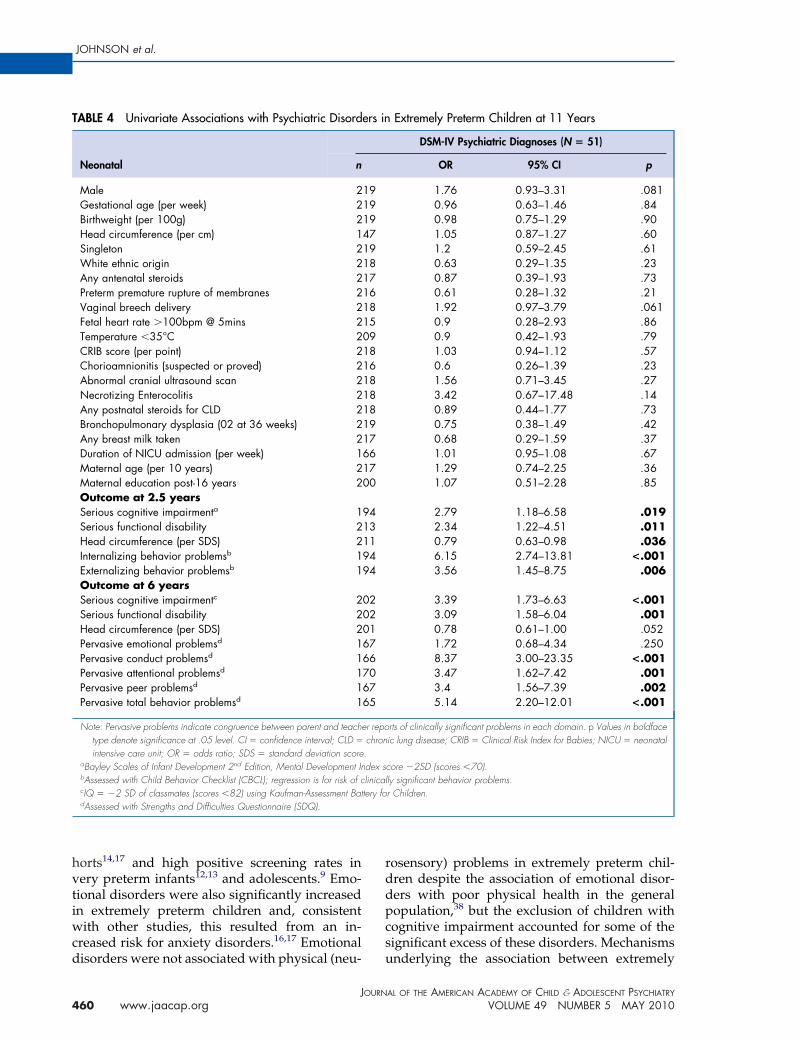
Precursors of Psychiatric Diagnoses at 11 Yearsin Extremely Preterm ChildrenNone of the neonatal variables examined weresignificantly associated with psychiatric diag-noses on univariate analyses. However, the riskwas marginally significant (p � .1) for boys andfor children born through vaginal breech deliv-eries (Table 4). In contrast, developmental out-comes at 2.5 years were significantly associatedwith psychiatric diagnoses, the strongest associ-ation with parent-reported internalizing behav-ior problems. At 6 years, there were strong asso-ciations with pervasive conduct problems andoverall behavioral difficulties, and moderate pre-diction by serious cognitive or functional disabil-ity, attention, and peer problems (Table 4).
On multivariate analyses, no neonatal variableswere independent predictors of psychiatric disor-der at age 11 years; however male sex, breechdelivery, and necrotizing enterocolitis (NEC) weremarginally significant (p � .10). By 2.5 years, par-ent-reported internalizing behavior problems wasthe only significant independent variable, althoughmale sex, NEC, and functional disability at 2.5years were marginally associated with increasedrisk. At 6 years, NEC, functional disability, inter-nalizing behavior problems at 2.5 years, and per-vasive conduct and attention problems at 6 yearshad independent associations with psychiatric di-agnoses (Table 2). Overall, parent-reported inter-nalizing behavior problems at 2.5 years and perva-sive conduct problems at 6 years were strongpredictors of psychiatric diagnoses at 11 years.
DISCUSSIONThis is the first investigation of the prevalence ofpsychiatric disorders in a whole population ofextremely preterm children. The 23% prevalenceand nearly threefold increased risk for psychiat-
ric disorders observed is commensurate with the cJOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 49 NUMBER 5 MAY 2010
2% to 28% prevalence and associated risk ratioseported in LBW/very LBW cohorts.14-17 Recenttudies of extremely preterm/ELBW children haveeported 29% to 40% prevalence of behavioralroblems in middle childhood.9,10,14,35 However,
hese are based on symptom counts from screeninguestionnaires, and the rates of confirmed diag-oses that require impairment are typically lower,s found in the present study. The 23% prevalenceeported may slightly underestimate the true prev-lence, as multiple imputation used to account forelective dropout increased the prevalence of psy-hiatric disorders to 25% in the surviving popula-ion.
Studies using behavioral screening mea-ures8,9,10,35-37 and diagnostic evaluations14,16,17
ncreasingly point to an “extremely preterm phe-otype” characterized by inattention and socialnd emotional problems, which is highlighted inhe present results. Consistent with previouseports, the most frequent psychiatric disorderas ADHD for which the magnitude of risk was
onsistent with previous studies reporting oddsatios of 2 to 4 in other cohorts.11 We noted thathis was attributable to the increased risk forDHD inattentive subtype rather than ADHD
ombined subtype, and that ODD/CD was lesstrongly associated with ADHD in extremelyreterm children than in classmates and in theeneral population.38 This has been noted previ-usly,14,16,39,40 prompting authors to suggest thatreterm survivors are more susceptible to cog-itive impairments that are associated withDHD-inattentive subtype (ADHD-I) and are
elatively protected from developing conductroblems.39-41
It has also been suggested that ASD may beore closely associated with neuro-cognitive and
nvironmental factors in this population. Al-hough ASD is considered to have a largelyenetic origin in the general population, autisticeatures are strongly associated with cognitivempairment12 and abnormal cerebral findingsuring the neonatal period13 and adolescence40
n extremely preterm children. We found thatutism spectrum disorder was associated withxtreme prematurity, which may be a marker forn environmental origin, or risk modifier, forSD. The 8% prevalence of ASD observed in theresent study was markedly higher than the 0.6%
o 0.9% reported in the general population,38,42
ut was expected, given recent reports of in-
reased rates of ASD in LBW/very LBW co-459www.jaacap.org
rddpcs
JOHNSON et al.
horts14,17 and high positive screening rates invery preterm infants12,13 and adolescents.9 Emo-tional disorders were also significantly increasedin extremely preterm children and, consistentwith other studies, this resulted from an in-creased risk for anxiety disorders.16,17 Emotional
TABLE 4 Univariate Associations with Psychiatric Disord
Neonatal n
Male 2Gestational age (per week) 2Birthweight (per 100g) 2Head circumference (per cm) 1Singleton 2White ethnic origin 2Any antenatal steroids 2Preterm premature rupture of membranes 2Vaginal breech delivery 2Fetal heart rate �100bpm @ 5mins 2Temperature �35°C 2CRIB score (per point) 2Chorioamnionitis (suspected or proved) 2Abnormal cranial ultrasound scan 2Necrotizing Enterocolitis 2Any postnatal steroids for CLD 2Bronchopulmonary dysplasia (02 at 36 weeks) 2Any breast milk taken 2Duration of NICU admission (per week) 1Maternal age (per 10 years) 2Maternal education post-16 years 2Outcome at 2.5 yearsSerious cognitive impairmenta 1Serious functional disability 2Head circumference (per SDS) 2Internalizing behavior problemsb 1Externalizing behavior problemsb 1Outcome at 6 yearsSerious cognitive impairmentc 2Serious functional disability 2Head circumference (per SDS) 2Pervasive emotional problemsd 1Pervasive conduct problemsd 1Pervasive attentional problemsd 1Pervasive peer problemsd 1Pervasive total behavior problemsd 1
Note: Pervasive problems indicate congruence between parent and teachetype denote significance at .05 level. CI � confidence interval; CLD �
intensive care unit; OR � odds ratio; SDS � standard deviation scoreaBayley Scales of Infant Development 2nd Edition, Mental Development InbAssessed with Child Behavior Checklist (CBCL); regression is for risk of ccIQ � �2 SD of classmates (scores �82) using Kaufman-Assessment BatdAssessed with Strengths and Difficulties Questionnaire (SDQ).
disorders were not associated with physical (neu- u
JOURN
460 www.jaacap.org
osensory) problems in extremely preterm chil-ren despite the association of emotional disor-ers with poor physical health in the generalopulation,38 but the exclusion of children withognitive impairment accounted for some of theignificant excess of these disorders. Mechanisms
Extremely Preterm Children at 11 Years
DSM-IV Psychiatric Diagnoses (N � 51)
OR 95% CI p
1.76 0.93–3.31 .0810.96 0.63–1.46 .840.98 0.75–1.29 .901.05 0.87–1.27 .601.2 0.59–2.45 .610.63 0.29–1.35 .230.87 0.39–1.93 .730.61 0.28–1.32 .211.92 0.97–3.79 .0610.9 0.28–2.93 .860.9 0.42–1.93 .791.03 0.94–1.12 .570.6 0.26–1.39 .231.56 0.71–3.45 .273.42 0.67–17.48 .140.89 0.44–1.77 .730.75 0.38–1.49 .420.68 0.29–1.59 .371.01 0.95–1.08 .671.29 0.74–2.25 .361.07 0.51–2.28 .85
2.79 1.18–6.58 .0192.34 1.22–4.51 .0110.79 0.63–0.98 .0366.15 2.74–13.81 <.0013.56 1.45–8.75 .006
3.39 1.73–6.63 <.0013.09 1.58–6.04 .0010.78 0.61–1.00 .0521.72 0.68–4.34 .2508.37 3.00–23.35 <.0013.47 1.62–7.42 .0013.4 1.56–7.39 .0025.14 2.20–12.01 <.001
rts of clinically significant problems in each domain. p Values in boldfaceic lung disease; CRIB � Clinical Risk Index for Babies; NICU � neonatal
core �2SD (scores �70).ly significant behavior problems.r Children.
ers in
191919471918171618150918161818181917661700
9413119494
0202016766706765
r repochron.dex slinicaltery fo
nderlying the association between extremely
AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 49 NUMBER 5 MAY 2010

e(optndcrArnnp
dbrmarKlrctneCusrs
d(stibtnsu(iapmtsd
PSYCHIATRIC DISORDERS IN PRETERM CHILDREN
preterm birth and anxiety disorder require fur-ther investigation and should take into accountthe impact of traumatic events on parental men-tal health and parent-child relationships.43,44
At first sight, the lack of significant associa-tions with neurosensory impairment suggeststhat psychiatric disorders are not related to thetype of focal brain injuries often associated withpreterm birth. Such focal injuries are detectableby standard ultrasound imaging techniques usedat the time of this study, and the risk factors forsuch injuries have hardly changed over the lasttwo decades for very preterm children.45 How-ever, the association of psychiatric disorders andother deficits (e.g., language, learning abilities) invery or extremely preterm children with cogni-tive impairment in this and other studies46,47
suggests that these disorders may result fromglobal changes in functional architecture, brainanatomy, or connectivity that is evidenced inearly MRI studies.48,49 These range from reducedbrain volume, reduced cortical folding to punc-tate white matter lesions, decreased cortical com-plexity, and diffuse and excessive high signalintensity in MRI48-51 not easily detectable in ul-trasound. These are not predicted by usual neo-natal risk factors but may show up in functionaldeficits in early development.
We did not find a relationship between psychi-atric disorders and neonatal variables. Other stud-ies, typically focused on specific psychopathology,have failed also to find a significant associationwith neonatal variables,9,14,16 whereas some reportindependent associations with neonatal ultra-sound abnormalities.13,15 In the present study,parent-reported behavior problems at 2.5 years(i.e., early behavioral deficits) and 6 years werethe strongest precursors of disorders at 11 years.However, the lack of significant associations withneonatal variables should be interpreted withcaution because of low statistical power. Giventhe small number of clinical cases, the inclusionof more than five variables risks overfitting themodel for multivariate analyses. A number ofvariables were marginally significant (p � .1) onboth univariate and multivariate analyses, in-cluding male sex, vaginal breech delivery, andNEC, and significant associations were noted onunivariate analyses for the majority of outcomesreflecting neuro-cognitive sequelae.
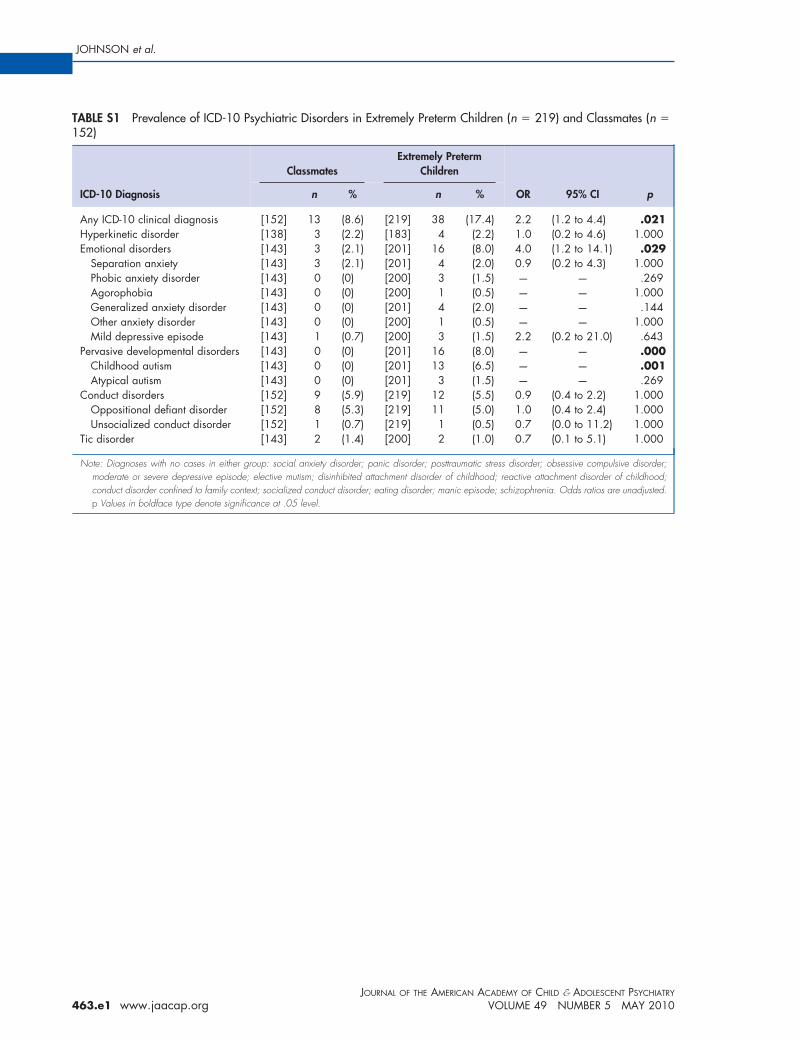
Prevalence estimates were based on DSM-IVdiagnostic criteria. When ICD-10 diagnostic cri-
teria for hyperkinetic disorder were applied, no aJOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 49 NUMBER 5 MAY 2010
xcess was found for extremely preterm childrenTable S1, available online). ICD-10 classificationf hyperkinetic disorder requires the presence ofervasive hyperactivity and impulsivity in addi-
ion to inattention; this significantly reduces theumber of extremely preterm children meetingiagnostic criteria. The application of DSM-IVriteria thus has greater sensitivity for ADHD-elated behaviors given the inclusion of anDHD-inattentive subtype classification. For this
eason, we have reported rates of DSM-IV diag-oses and would advocate the use of these diag-ostic criteria in future research with pretermopulations.
The strengths of this study include the use ofiagnostic evaluations to classify psychiatric andehavioral disorders. The DAWBA has excellenteliability and validity,22,25 and was the principaleasure of psychopathology in the British child
nd adolescent mental health surveys38 and otherecent general population studies in the Unitedingdom.52 The prevalence for psychiatric prob-
ems in the classmates were comparable to thoseeported in these UK population studies.38 Psy-hiatric data were collected for all children ratherhan for a subset identified as at risk, and diag-oses were made by consensus between twoxperienced clinical raters blind to birth status.ognitive ability was assessed by psychologistssing objective standardized tests, and neurosen-ory function was evaluated by experienced neu-odevelopmental pediatricians. All study asses-ors were blind to group allocation.
Limitations of the study include the use ofifferent behavioral scales at age 2.5 years
CBCL) and 6 years (SDQ). However, compari-ons between the CBCL and SDQ have indicatedhat both have similar sensitivity and specificityn detecting clinical caseness despite the SDQeing a much shorter instrument.53 For predic-ive purposes, we used the more reliable exter-alizing and internalizing clusters rather thanpecific subscales of the CBCL. Furthermore, wesed the CBCL (�97th percentile) and SDQ�90th percentile) recommended cut-off points todentify “clinical” risk cases in the regressionnalyses. A further limitation was the lack ofsychiatric self-report at 11 years. Although thisay have led to possible underreporting of emo-
ional disorders (typically less sensitive to ob-erver report), it is less likely to have affectedetection of ADHD or ASD, which are typically
ssessed at this age by combination of parent and461www.jaacap.org

nRtffd
JOHNSON et al.
teacher report. Finally, as in most longitudinalstudies,54,55 selective dropout of families withhigher social risk and children with more cogni-tive problems occurred. However, using estima-tion functions, the “true” prevalence was onlymarginally underestimated in our study. Fur-thermore, recent empirical evidence and simula-tions indicate that the validity of regression mod-els is only marginally affected even after selectivedropout.52
In conclusion, almost one quarter of ex-tremely preterm children had a psychiatricdisorder at 11 years of age. The most frequentpsychiatric conditions were ADHD (12%),emotional disorders (9%), and ASD (8%).Global cognitive impairment and early parent-reported internalizing symptoms, likely to bethe result of insult to normal brain develop-ment and the superimposed risk of acquiredbrain injury, mediate the risk of psychiatricdisorder associated with extremely prematurebirth. These results have implications for re-search and clinical practice. Extremely pretermbirth allows the study of white to gray matterbrain development as it occurs using newneonatal imaging approaches.45 This may iden-tify how key structures of the brain are alteredand their association to the functional pheno-type for extremely preterm children.56,57 Clini-cally, the findings suggest that much greateremphasis than that so far should be placed onearly cognitive and psychological monitoring
of extremely preterm children for emerging124:717-728.
1
1
1
1
JOURN
462 www.jaacap.org
europsychiatric and emotional disorders.outine cognitive and behavioral screening
hroughout the preschool period may help toacilitate early psychiatric referral and there-ore be beneficial for extremely preterm chil-ren and their families. &
Accepted February 4, 2010
Dr. Johnson is with the Institute for Women’s Health, University CollegeLondon and the School of Clinical Sciences, University of Nottingham,UK; Drs. Hollis and Kochhar are with the Developmental PsychiatrySection, Division of Psychiatry, University of Nottingham, UK; DrHennessy is with Barts and The London School of Medicine andDentistry, Queen Mary University of London, UK; Dr. Wolke is with theHealth Sciences Research Institute, University of Warwick, UK; Dr.Marlow is with University College London, UK.
This study was supported by the Medical Research Council (MRC), UK.
We are indebted to the EPICure 1 Study Group, which includespediatricians in 276 maternity units in the UK whose contributionwas invaluable. We are also indebted to the many children andparents for their continued participation in the EPICure Study.Co-investigators were Neil Marlow (University of Nottingham;Chief Investigator), Kate Costeloe (Queen Mary University ofLondon ), Enid Hennessy (Queen Mary University of London), JanetStocks (University College London), and Elizabeth Draper (Univer-sity of Leicester). Study assessors were Rebecca Trikic, RebeccaSmith, Samantha Johnson (Psychologists), Susan Thomas, VictoriaRowell, and Joseph Fawke (Pediatricians).
Support for DAWBA data collection and analysis was provided byProfessor Robert Goodman (Institute of Psychiatry, Kings CollegeLondon).
Disclosure: Drs. Johnson, Hollis, Kochhar, Hennessy, Wolke, andMarlow report no biomedical financial interests of potential conflicts ofinterest.
Correspondence to: Prof. Chris Hollis, Developmental Psychiatry,South Block E Floor, Queen’s Medial Centre, Nottingham, NG72UH, UK; e-mail: [email protected]
0890-8567/10/©2010 American Academy of Child and Adoles-cent Psychiatry
DOI: 10.1016/j.jaac.2010.02.002
REFERENCES1. Wilson-Costello D, Friedman H, Minich N, Fanaroff AA, Hack M.
Improved survival rates with increased neurodevelopmental dis-ability for extremely low birth weight infants in the 1990s.Pediatrics. 2005;115:997-1003.
2. Hack M, Taylor HG, Drotar D, Schluchter M, Cartar L, Andre-ias L, et al. Chronic conditions, functional limitations, andspecial health care needs of school-aged children born withextremely low-birth-weight in the 1990s. J Am Med Assoc.2005;294:318-325.
3. Marlow N, Wolke D, Bracewell MA, Samara M. Neurologic anddevelopmental disability at six years of age after extremelypreterm birth. N Engl J Med. 2005;352:9-19.
4. Johnson S, Fawke J, Hennessy E, Rowell V, Thomas S, Wolke D,et al. Neurodevelopmental disability through 11 years in childrenborn before 26 weeks of gestation: the EPICure Study. Pediatrics.2009:e249-e257.
5. Marlow N, Hennessy E, Bracewell M, Wolke D. Motor andexecutive function at 6 years of age following extremely pretermbirth. Pediatrics. 2007;120:793-804.
6. Aarnoudse-Moens CSH, Weisglas-Kuperus N, van Goudoever JB,Oosterlan J. Meta-analysis of neurobehavioral outcomes in verypreterm and/or very low birth weight children. Pediatrics. 2009;
7. Johnson S, Hennessy E, Smith R, et al. Academic attainment andspecial educational needs in extremely preterm children at 11years. The EPICure Study. Arch Dis Child Fetal Neonatal Ed.2009;94:F283-F289.
8. Hille E, Ouden Ad, Saigal A, Wolke D, Lambert M, Whitaker A,et al. Behavioral problems in children who weight 1000g or less atbirth in four countries. Lancet. 2001;357:1641-1643.
9. Hack M, Taylor HG, Schluchter M, et al. Behavioral outcomes ofextremely low birth weight children at age 8 years. J Dev BehavPediatr. 2009;30:122-130.
0. Samara M, Marlow N, Wolke D. Pervasive behavior problems at6 years of age in a total-population sample of children born at 25weeks of gestation. Pediatrics. 2008;122:562-573.
1. Bhutta A, Cleves M, Casey P, Cradock M, Anand K. Cognitiveand behavioral outcomes of school-aged children who wereborn preterm. A meta-analysis. J Am Med Assoc. 2002;288:728-737.
2. Kuban KCK, O’Shea TM, Allred EN, et al. Positive screening on theModified Checklist for Autism in Toddlers (M-CHAT) in extremelylow gestational age newborns. J Pediatr. 2009;154:535-540.
3. Limperoloulos C, Bassan H, Sullivan NR, et al. Positive screeningfor autism in ex-preterm infants: prevalence and risk factors.
Pediatrics. 2008;121:758-765.AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 49 NUMBER 5 MAY 2010

3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
5
5
5
5
5
PSYCHIATRIC DISORDERS IN PRETERM CHILDREN
14. Elgen I, Sommerfelt K, Markestad T. Population based, controlledstudy of behavioral problems and psychiatric disorders in lowbirthweight children at 11 years of age. Arch Dis Child FetalNeonatal Ed. 2002;87:F128-F132.
15. Whitaker AH, Van Rossem R, Feldman JF, et al. Psychiatricoutcomes in low-birth-weight children at age 6 years: relation toneonatal cranial ultrasound abnormalities. Arch Gen Psychiatry.1997;54:785-9.
16. Botting N, Powls A, Cooke R, Marlow N. Attention deficithyperactivity disorder and other psychiatric outcomes in verylow birthweight children at 12 years. J Child Psychol Psychiatry.1997;38:931-941.
17. Indredavik MS, Vik T, Heyerdahl S, et al. Psychiatric symptomsand disorders in adolescents with low birth weight. Arch DisChild Fetal Neonatal Ed. 2004;89:F445-F450.
18. Johnson S. Cognitive and behavioral outcomes following verypreterm birth. Semin Fetal Neonatal Med. 2007;12:363-373.
19. Saigal S, Doyle L. An overview of mortality and sequelae ofpreterm birth from infancy to adulthood. Lancet. 2008;371:26-269.
20. Costeloe K, Hennessy E, Gibson A, Marlow N, Wilkinson A. TheEPICure Study: outcomes to discharge from hospital for infantsborn at the threshold of viability. Pediatrics. 2000;106:659-671.
21. Wood N, Marlow N, Costeloe K, Gibson A, Wilkinson A. Neu-rologic and developmental disability after extremely pretermbirth. N Engl J Med. 2000;343:378-384.
22. Goodman R, Ford T, Richards H, Gatward R, Meltzer H. TheDevelopment and Well-Being Assessment: description and initialvalidation of an integrated assessment of child and adolescentpsychopathology. J Child Psychol Psychiatry Allied Disc. 2000;41:645-655.
23. World Health Organization. The ICD-10 Classification of Mentaland Behavioral Disorders. Geneva, Switzerland: World HealthOrganization, 1992.
24. American Psychiatric Association. Diagnostic and Statistical Man-ual of Mental Disorders, Fourth Edition, Text Revision. 4th ed.Washington, DC: American Psychiatric Association, 2000.
25. Ford T, Goodman R, Meltzer H. The British Child and AdolescentMental Health Survey 1999: the prevalence of DSM-IV disorders.J Am Acad Child Adolesc Psychiatry. 2003;42:1203-1211.
26. Kaufman AS, Kaufman NL. Kaufman Assessment Battery forChildren. Circle Pines, MN: American Guidance Service, 1983.
27. Wolke D, Ratschinski G, Ohrt B, Riegel K. The cognitive outcomeof very preterm infants may be poorer than often reported: anempirical investigation of how methodological issues make a bigdifference. Eur J Pediatr. 1994;153:906-915.
28. Johnson S, Wolke D, Marlow N. Outcome monitoring in pretermpopulations: measures and methods. Zeitschr Psychologie/J Psy-chol. 2008;216:135-146.
29. Flynn J. Searching for justice: the discovery of IQ gains over time.Am Psychol. 1999;54:5-20.
30. Achenbach TM. The Manual for the Child Behavior Checklist/4-18 and 1991 Profile. Burlington, VT: University of Vermont,Department of Psychiatry, 1991.
31. Goodman R. Psychometric properties of the strengths and diffi-culties questionnaire. J Am Acad Child Adolesc Psychiatry.2001;40:1337-1345.
32. Office for National Statistics. The National Statistics Socio-Eco-nomic Classification User Manual: Palgrave Macmillan, 2005.
33. Royston P. Multiple imputation of missing values. Stata J. 2004;4:227-241.
34. Johnson S, Hollis C, Kochhar P, et al. Autism spectrum disordersin extremely preterm children. J Pediatr. 2010;156:525-531.
35. Farooqi A, Hagglof B, Sedin G, Gothefors L, Serenius F. Mentalhealth and social competencies of 10- to 12-year-old children born
at 23 to 25 weeks of gestation in the 1990s: a Swedish nationalprospective follow-up study. Pediatrics. 2007;120:118-133.JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 49 NUMBER 5 MAY 2010
6. Anderson P, Doyle LW. Neurobehavioral outcomes of school-agechildren born extremely low birth weight or very preterm in the1990s. J Am Med Assoc. 2003;289:3264-3272.
7. Saigal S, Pinelli J, Hoult L, Kim MM, Boyle M. Psychopathologyand social competencies of adolescents who were extremely lowbirth weight. Pediatrics. 2003;111:969-975.
8. Green H, McGinnity A, Meltzer H, Ford T, Goodman R. Mentalhealth of children and young people in Great Britain. Basingstoke,Hampshire, UK: National Statistics, 2005.
9. Szatmari P, Saigal S, Rosenbaum P, Campbell D. Psychopathol-ogy and adaptive functioning among extremely low birthweightchildren at eight years of age. Dev Psychopathol. 1993;5:345-357.
0. Indredavik MS, Skranes JS, Vok T, et al. Low-birth-weight ado-lescents: psychiatric symptoms and cerebral MRI abnormalities.Pediatr Neurol. 2005;33:259-266.
1. Wolke D. Psychological development of prematurely born chil-dren. Arch Dis Child. 1998;78:567-570.
2. Williams JG, Brayne CEG, Higgins JPT. Systematic review ofprevalence studies of autism spectrum disorders. Arch Dis Child.2006;91:8-15.
3. Muller-Nix C, Forcada-Guex M, Pierrehumbert B, et al. Prematu-rity, maternal stress, and mother-child interactions. Early HumDev. 2004;79:145-158
4. Jotzo M, Poets CF. Helping parents cope with the trauma ofpremature birth: an evaluation of a trauma-preventive psycho-logical intervention. Pediatrics. 2005;115:915-919.
5. Hintz R, O’Shea M. Neuroimaging and neurodevelopmentaloutcomes in preterm infants. Semin Perinatol. 2008;32:11-19.
6. Wolke D, Meyer R. Cognitive status, language attainment andprereading skills of 6-year-old very preterm children and theirpeers: the Bavarian Longitudinal Study. Dev Med Child Neurol.1999;4:94-109.
7. Wolke D, Samara M, Bracewell M, Marlow N. Specific languagedifficulties and school achievement in children born at 25 weeksof gestation or less. J Pediatr. 2008;152:256-262, e251.
8. Kapellou O, Counsell SJ, Kennea N, et al. Abnormal corticaldevelopment after premature birth shown by altered allometricscaling of brain growth. PLoS Med. 2006;3:1382-1390.
9. Inder TE, Warfield SK, Wang H, Huppi P, Volpe J. Abnormalcerebral structure is present at term in premature infants. Pedi-atrics. 2005;115:286-294.
0. Rees S, Inder T. Fetal and neonatal origins of altered braindevelopment. Early Hum Dev. 2005;81:753-761.
1. Hart AR, Whitby EW, Griffiths PD, Smith MF. Magnetic reso-nance imaging and developmental outcome following pretermbirth: review of current evidence. Dev Med Child Neurol. 2008;50:655-663.
2. Wolke D, Waylen A, Samara M, et al. Selective drop-out inlongitudinal studies and non-biased prediction of behavior dis-orders. Br J Psychiatry. 2009;195:249-256.
3. Klasen H, Woerner W, Wolke D, et al. Comparing the Germanversions of the Strengths and Difficulties Questionnaires (SDQ-Deu) and the Child Behavior Checklist. Eur J Child AdolescPsychiatry. 2000;9:271-276.
4. Wolke D, Söhne B, Ohrt B, Riegel K. Follow-up of pretermchildren: important to document dropouts. Lancet. 1995;345:447.
5. Hille ETM, Weisglas-Kuperus N, van Goudoever JB, et al. Fol-low-up care of high-risk infants functional outcomes and partic-ipation in young adulthood for very preterm and very low birthweight infants: the Dutch Project on Preterm and Small forGestational Age Infants at 19 Years of Age. Pediatrics. 2004;114:1377-1397.
6. Ment LR, Kesler S, Vohr B, et al. Longitudinal brain volumechanges in preterm and term control subjects during late child-hood and adolescence. Pediatrics. 2009;123:503-511.
7. Abernethy LJ, Palaniappan M, Cooke RWI. Quantitative magnetic
resonance imaging of the brain in survivors of very low birthweight. Arch Dis Child. 2002;87:279-283.463www.jaacap.org
JOHNSON et al.
TABLE S1 Prevalence of ICD-10 Psychiatric Disorders in152)
ICD-10 Diagnosis
Classmates
n %
Any ICD-10 clinical diagnosis [152] 13 (8.6)Hyperkinetic disorder [138] 3 (2.2)Emotional disorders [143] 3 (2.1)
Separation anxiety [143] 3 (2.1)Phobic anxiety disorder [143] 0 (0)Agorophobia [143] 0 (0)Generalized anxiety disorder [143] 0 (0)Other anxiety disorder [143] 0 (0)Mild depressive episode [143] 1 (0.7)
Pervasive developmental disorders [143] 0 (0)Childhood autism [143] 0 (0)Atypical autism [143] 0 (0)
Conduct disorders [152] 9 (5.9)Oppositional defiant disorder [152] 8 (5.3)Unsocialized conduct disorder [152] 1 (0.7)
Tic disorder [143] 2 (1.4)
Note: Diagnoses with no cases in either group: social anxiety disorder;moderate or severe depressive episode; elective mutism; disinhibitedconduct disorder confined to family context; socialized conduct disordep Values in boldface type denote significance at .05 level.
Extremely Preterm Children (n � 219) and Classmates (n �
Extremely PretermChildren
OR 95% CI pn %
[219] 38 (17.4) 2.2 (1.2 to 4.4) .021[183] 4 (2.2) 1.0 (0.2 to 4.6) 1.000[201] 16 (8.0) 4.0 (1.2 to 14.1) .029[201] 4 (2.0) 0.9 (0.2 to 4.3) 1.000[200] 3 (1.5) — — .269[200] 1 (0.5) — — 1.000[201] 4 (2.0) — — .144[200] 1 (0.5) — — 1.000[200] 3 (1.5) 2.2 (0.2 to 21.0) .643[201] 16 (8.0) — — .000[201] 13 (6.5) — — .001[201] 3 (1.5) — — .269[219] 12 (5.5) 0.9 (0.4 to 2.2) 1.000[219] 11 (5.0) 1.0 (0.4 to 2.4) 1.000[219] 1 (0.5) 0.7 (0.0 to 11.2) 1.000[200] 2 (1.0) 0.7 (0.1 to 5.1) 1.000
panic disorder; posttraumatic stress disorder; obsessive compulsive disorder;attachment disorder of childhood; reactive attachment disorder of childhood;r; eating disorder; manic episode; schizophrenia. Odds ratios are unadjusted.
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 49 NUMBER 5 MAY 2010463.e1 www.jaacap.org





























