Embed Size (px)
Citation preview

Rapid Prototyping JournalError analysis of FDM fabricated medical replicasIhab El-Katatny S.H. Masood Y.S. Morsi
Article information:To cite this document:Ihab El-Katatny S.H. Masood Y.S. Morsi, (2010),"Error analysis of FDM fabricated medical replicas", Rapid Prototyping Journal,Vol. 16 Iss 1 pp. 36 - 43Permanent link to this document:http://dx.doi.org/10.1108/13552541011011695
Downloaded on: 01 March 2016, At: 20:55 (PT)References: this document contains references to 13 other documents.To copy this document: [email protected] fulltext of this document has been downloaded 936 times since 2010*
Users who downloaded this article also downloaded:Kun Tong, Sanjay Joshi, E. Amine Lehtihet, (2008),"Error compensation for fused deposition modeling (FDM) machine bycorrecting slice files", Rapid Prototyping Journal, Vol. 14 Iss 1 pp. 4-14 http://dx.doi.org/10.1108/13552540810841517Sung-Hoon Ahn, Michael Montero, Dan Odell, Shad Roundy, Paul K. Wright, (2002),"Anisotropic material properties of fuseddeposition modeling ABS", Rapid Prototyping Journal, Vol. 8 Iss 4 pp. 248-257 http://dx.doi.org/10.1108/13552540210441166Antonio Armillotta, (2006),"Assessment of surface quality on textured FDM prototypes", Rapid Prototyping Journal, Vol. 12 Iss 1pp. 35-41 http://dx.doi.org/10.1108/13552540610637255
Access to this document was granted through an Emerald subscription provided by emerald-srm:594641 []
For AuthorsIf you would like to write for this, or any other Emerald publication, then please use our Emerald for Authors serviceinformation about how to choose which publication to write for and submission guidelines are available for all. Please visitwww.emeraldinsight.com/authors for more information.
About Emerald www.emeraldinsight.comEmerald is a global publisher linking research and practice to the benefit of society. The company manages a portfolio ofmore than 290 journals and over 2,350 books and book series volumes, as well as providing an extensive range of onlineproducts and additional customer resources and services.
Emerald is both COUNTER 4 and TRANSFER compliant. The organization is a partner of the Committee on Publication Ethics(COPE) and also works with Portico and the LOCKSS initiative for digital archive preservation.
*Related content and download information correct at time of download.
Dow
nloa
ded
by N
atio
nal I
nstit
ute
of T
echn
olog
y T
iruc
hira
ppal
li A
t 20:
55 0
1 M
arch
201
6 (P
T)

Error analysis of FDM fabricated medicalreplicas
Ihab El-Katatny, S.H. Masood and Y.S. Morsi
Faculty of Engineering and Industrial Science, Swinburne University of Technology, Melbourne, Australia
AbstractPurpose – Recent advancement in fused deposition modelling (FDM) rapid prototyping technology has made it a viable technology for application inreconstructive surgery. The purpose of this paper is to investigate the errors generated during the fabrication stage of complex anatomical replicasderived from computed tomography coupled with the technique of FDM.Design/methodology/approach – An evaluation on the errors generated during the fabrication process of two anatomical parts (skull or mandible)for different human sizes (infant, female or male) is carried out. A comparison between the linear measurements of 11 landmarks on the virtual modelof a skull and nine for the mandible of patient specific and its replica is conducted. Furthermore, eight landmarks are chosen to evaluate the bonethickness variation over the fabricated replicas.Findings – Although the FDM technology proved the ability to manufacture and to fit prosthesis to a patient’s unique proportions quickly and withrelatively low cost, the model accuracy is a key factor to the applicability of such technology. The results show undersized replicas with an overallabsolute average deviation of 0.24 per cent with an average standard deviation of 0.16 per cent of the skull models and 0.22 per cent with a0.11 per cent standard deviation of the mandibles. Furthermore, a high level of accuracy is reflected in the representation of the measured bonethickness with deviations in the order of 100th of a millimetre being reported.Originality/value – The paper demonstrates an outstanding accuracy using FDM process for the fabrication of anatomical replicas using models ofdifferent human sizes and gender in comparison to other established rapid prototyping techniques.
Keywords Rapid prototypes, Modelling, Human anatomy, Computer aided design, Error analysis
Paper type Research paper
1. Introduction
The rapid prototyping technology is becoming increasinglyimportant as a manufacturing method for many medicaldevices. Several studies were carried out in order to evaluatethe technology in comparison with traditional fabricationmethods. (Santler et al., 1998) carried out a comparison inregard to the production method and accuracy between twomodels produced by stereolithography (SLA) and milling.They concluded that both methods are sufficiently accuratefor clinical use. However, SLA replicas are preferable inspecial cases necessitating fine structures and complex internalgeometry. A similar conclusion was reached by Sarment et al.(2003) highlighting the use of Stereolithographic guidesallowing for improved implant placement where significantreduction to the average distance between the plannedimplants and actual osteotomies was reported in comparisonto the traditional surgical guidance methods.Although the advantage of such a technique is evident,
developing an understanding of the entire manufacturingprocess, starting from the image generation to the endproduct as well as identifying all possible sources of error isessential in assisting such techniques. In 1997, Bouyssie et al.
(1997) investigated the accuracy of complex anatomicalreplicas derived from X-ray computed tomography (CT) datalinked to the rapid prototyping techniques of SLA. In theirstudy, two mandible replicas were manufactured by SLA. Thedry mandibles were embedded in gelatin to reduce air-boneinterface and to simulate the presence of surrounding softtissues. Dimensional comparisons were undertaken betweennine landmarks both on the original bone and on its replica bythree different observers. Absolute and relative differenceswere calculated, relative differences being expressed aspercentages. They concluded that the differences betweenthe various measurements are either positive or negative,which indicate that the replica can be over or under-dimensioned. Absolute differences range from 0.0 to0.24mm. Globally, the original mandible is slightly morevoluminous than the replica, with a mean difference ofþ0.06mm. The average absolute difference is 0.12mm, witha standard mean error of 0.02mm reported.Another study carried out by Choi et al. (2002) examines
the effect of the threshold value on the accuracy of 3D virtualmodels as well as the errors generated during the productionof medical rapid prototyping (RP) models using SLAtechnique, etc. In their study, 12 landmarks were used forlinear measurement, eight for craniomaxillary and four for themandible. They concluded that the absolute mean deviationThe current issue and full text archive of this journal is available at
www.emeraldinsight.com/1355-2546.htm
Rapid Prototyping Journal
16/1 (2010) 36–43
q Emerald Group Publishing Limited [ISSN 1355-2546]
[DOI 10.1108/13552541011011695]
Support from Australian Research Council (ARC) under ARC Linkagegrant is gratefully acknowledged.
Received: 20 November 2008Revised: 9 April 2009Accepted: 14 April 2009
36
Dow
nloa
ded
by N
atio
nal I
nstit
ute
of T
echn
olog
y T
iruc
hira
ppal
li A
t 20:
55 0
1 M
arch
201
6 (P
T)

between the original dry skull and the RP model over the 16
linear measurements was 0.62-0.35mm (0.56-0.39 per cent),
which is smaller than the values reported in previous studies.Furthermore, they developed a relationship called the “dumb-
bell” effect which describes that the effect of threshold valuedepending on whether a measurement is internal or external.
Although knowledge of the optimal threshold value is
important to enhance model accuracy, it cannot bedetermined from a limited number of RP models. A similar
investigation was carried by Nizam et al. (2006). Their studyof the dimensional accuracy of the skull models produced
using the rapid prototyping technology of SLA was aimed at
validating the system for clinical applications at HospitalUniversity Sains Malaysia. SLA technique was used to
fabricate a replica model of four dried human adult skulls.
Eight linear measurements were repeatedly made betweenidentified point landmarks on each of the original skulls and
its replica using an electronic digital caliper. They concludedthat the overall absolute difference between the four human
adult skulls and its replica models was 0.59mm with a
standard deviation of 0.89mm. Furthermore, the meanpercentage of 0.54 per cent with a standard deviation of 0.62
per cent was recorded.Meakin et al. (2004) evaluated the accuracy of a replica of a
sheep’s lumbar vertebra using data from a CT scan andutilising the fused deposition modelling (FDM) technique.
Vernier callipers and laser scanning techniques were used to
compare the measured data between the original and itsreplica. They concluded that apart from the spinous process
width, over five linear measurements, there was an absolutemean deviation of 1.36mm, and 0.77mm of absolute
standard deviation. Furthermore, in comparison to the
other rapid prototyping techniques a similar level ofaccuracy was achieved. Apart from the pervious study, the
primary focus was on the evaluation of selective laser sintering
(SLS) and SLA techniques. However, recent developments inusing poly(e-caprolactone) and other biocompatible material
in an FDM machine have opened the door for such atechnique to be widely used especially for scaffolds fabrication
in tissue engineering applications. While it is essential to
identify all possible sources of errors which may occur duringthe manufacturing process such as: errors generated during
medical imaging (Bouyssie et al., 1997) as well as the virtualmodel generation (Choi et al., 2002), the objective of this
study is to evaluate the accuracy in the fabrication stage of the
medical replica based on different human sizes and genderusing the rapid prototype technique of FDM.
2. Model fabrication
Figure 1 shows the overall production stages of skullfabrication using FDM technique. A 3D representation of
the craniomaxillary of a patient specific was generated usingInVesalius (2008) software. In order to differentiate the hard
tissues from the surrounding soft tissues a segmentation
technique with threshold values ranging between 1,200 and4,000 were applied. Upon completion of segmentation, data
is converted to an standard tessellation language (STL) fileformat which is imported to Materialise (2004) software. In
Magics software, the 3D volume of the patient’s
craniomaxillary was edited and distortions resulting frommetallic implants and errors due to partial volume effects were
corrected. Furthermore, morphology operations, Boolean
operations and cavity fill were used to generate a high-
resolution contour suitable for most rapid prototype
techniques.In the second step, Stratasys (2004) software was used to
prepare the model for fabrication. The model orientation was
chosen and a model support was created. A slice algorithm
was invoked and a tool-path plan was also generated. The
tool-path information was then converted into machine codes
for physical model fabrication. FDM3000 was used in the
replica fabrication with operating specifications as shown in
Table I. The replica was produced in a slice fashion using
ABS as the fabricated material and soluble support material.
The final stage involved the removal of the support material as
well as cleaning and polishing the product. The fabrication
procedure shown below refers to the male skull fabricated
replica. However, a similar process for different skull sizes
(female and infant) and mandibles (male, female and infant)
fabrication was conducted. Figure 2 shows the final fabricated
models of using FDM technique.
3. Dimensional analysis
Based on Garwin (2006), 11 pre-determined positions on the
cranium as well as nine mandible landmarks were selected for
linear measurement analysis. Table II shows the linear
measurement definition of these landmarks. Figure 3 shows
the physical locations of these landmarks. Furthermore, eight
landmarks were used to evaluate the accurate presentation of
bone thickness variations over the parts which were
Figure 1 Fabrication process of the skull replica using FDM3000
CT InVesalius software2 D slice image 3D render model Regain of interst
3D fabricated modelFDM 3,000
3D tool-path ModelInsight software
3D virtual modelMagics Software
Table I Operating specifications of FDM3000
Modeller: FDM 3000Model material ABS P400 Nozzle type: T12
Support material Soluble P400SR Nozzle type: T12
Slice height 0.2540 mm
Part fill style Perimeter/rasters Depth of contours 6.3500 mm
Part interior style Solid – fine Part interior depth 1.0160 mm
Contour width 0.5080 mm Part raster width 0.5080 mm
Error analysis of FDM fabricated medical replicas
Ihab El-Katatny, S.H. Masood and Y.S. Morsi
Rapid Prototyping Journal
Volume 16 · Number 1 · 2010 · 36–43
37
Dow
nloa
ded
by N
atio
nal I
nstit
ute
of T
echn
olog
y T
iruc
hira
ppal
li A
t 20:
55 0
1 M
arch
201
6 (P
T)
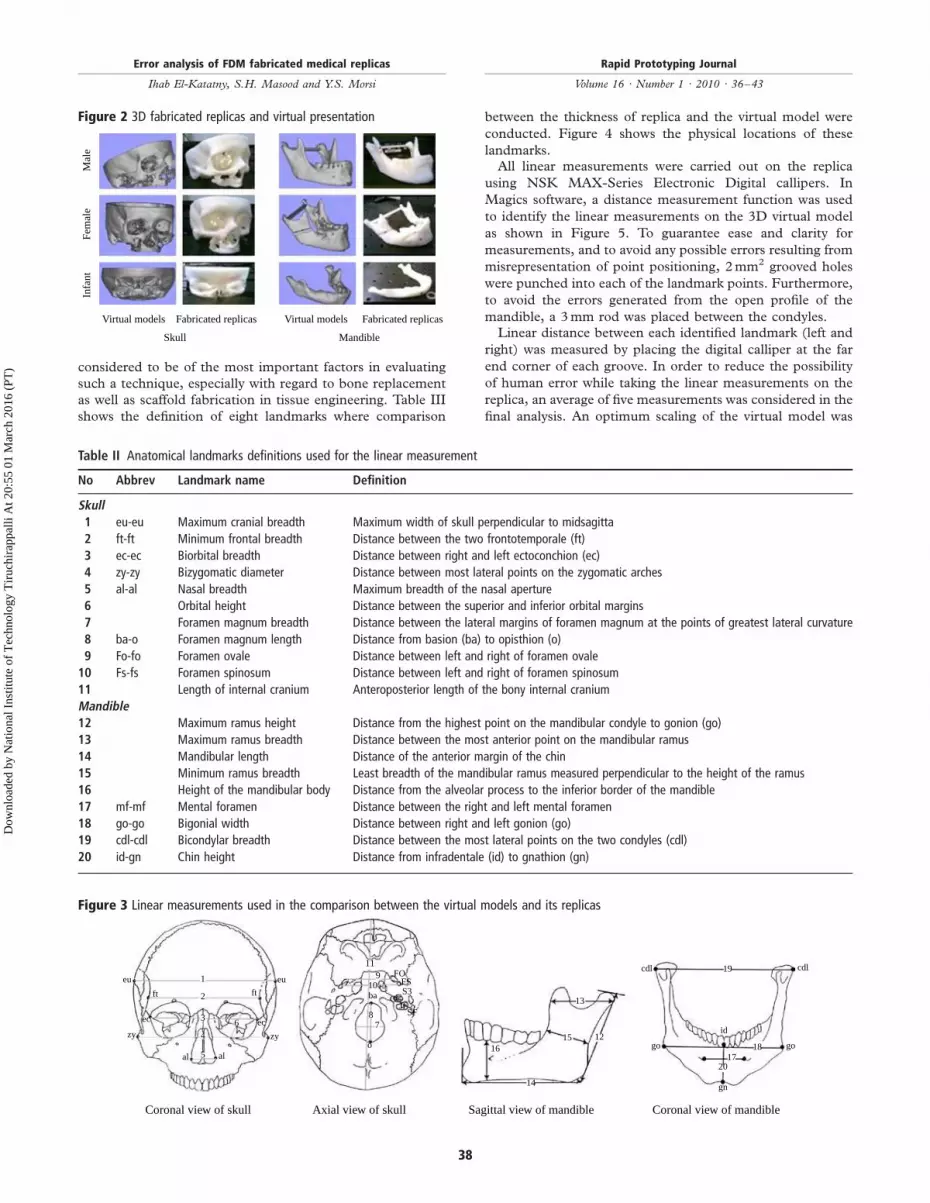
considered to be of the most important factors in evaluating
such a technique, especially with regard to bone replacement
as well as scaffold fabrication in tissue engineering. Table III
shows the definition of eight landmarks where comparison
between the thickness of replica and the virtual model were
conducted. Figure 4 shows the physical locations of these
landmarks.All linear measurements were carried out on the replica
using NSK MAX-Series Electronic Digital callipers. In
Magics software, a distance measurement function was used
to identify the linear measurements on the 3D virtual model
as shown in Figure 5. To guarantee ease and clarity for
measurements, and to avoid any possible errors resulting from
misrepresentation of point positioning, 2mm2 grooved holes
were punched into each of the landmark points. Furthermore,
to avoid the errors generated from the open profile of the
mandible, a 3mm rod was placed between the condyles.Linear distance between each identified landmark (left and
right) was measured by placing the digital calliper at the far
end corner of each groove. In order to reduce the possibility
of human error while taking the linear measurements on the
replica, an average of five measurements was considered in the
final analysis. An optimum scaling of the virtual model was
Figure 3 Linear measurements used in the comparison between the virtual models and its replicas
Coronal view of skull
alal 5
46 ec
zy
ft
eu
119
10ba
87
o
S3CC
JFSF
FOFS
16
14
15
13
12
cdl
go go
gn
2017
18
id
19 cdl
3
2
1
ft
eu
zy
ec
Axial view of skull Sagittal view of mandible Coronal view of mandible
Figure 2 3D fabricated replicas and virtual presentation
Infa
ntM
ale
Fem
ale
Virtual models Fabricated replicas Virtual models Fabricated replicas
Skull Mandible
Table II Anatomical landmarks definitions used for the linear measurement
No Abbrev Landmark name Definition
Skull1 eu-eu Maximum cranial breadth Maximum width of skull perpendicular to midsagitta
2 ft-ft Minimum frontal breadth Distance between the two frontotemporale (ft)
3 ec-ec Biorbital breadth Distance between right and left ectoconchion (ec)
4 zy-zy Bizygomatic diameter Distance between most lateral points on the zygomatic arches
5 al-al Nasal breadth Maximum breadth of the nasal aperture
6 Orbital height Distance between the superior and inferior orbital margins
7 Foramen magnum breadth Distance between the lateral margins of foramen magnum at the points of greatest lateral curvature
8 ba-o Foramen magnum length Distance from basion (ba) to opisthion (o)
9 Fo-fo Foramen ovale Distance between left and right of foramen ovale
10 Fs-fs Foramen spinosum Distance between left and right of foramen spinosum
11 Length of internal cranium Anteroposterior length of the bony internal cranium
Mandible12 Maximum ramus height Distance from the highest point on the mandibular condyle to gonion (go)
13 Maximum ramus breadth Distance between the most anterior point on the mandibular ramus
14 Mandibular length Distance of the anterior margin of the chin
15 Minimum ramus breadth Least breadth of the mandibular ramus measured perpendicular to the height of the ramus
16 Height of the mandibular body Distance from the alveolar process to the inferior border of the mandible
17 mf-mf Mental foramen Distance between the right and left mental foramen
18 go-go Bigonial width Distance between right and left gonion (go)
19 cdl-cdl Bicondylar breadth Distance between the most lateral points on the two condyles (cdl)
20 id-gn Chin height Distance from infradentale (id) to gnathion (gn)
Error analysis of FDM fabricated medical replicas
Ihab El-Katatny, S.H. Masood and Y.S. Morsi
Rapid Prototyping Journal
Volume 16 · Number 1 · 2010 · 36–43
38
Dow
nloa
ded
by N
atio
nal I
nstit
ute
of T
echn
olog
y T
iruc
hira
ppal
li A
t 20:
55 0
1 M
arch
201
6 (P
T)

utilised in order to produce a clear and accurate presentation
of the points of interest and liner distance values were
acquired at corresponding exact locations on the replica as
shown in Figure 5. Table IV shows each of linear
measurements on the virtual model and their replicas. Thedifference between the measurements is also presented in
terms of mm and percentages.
4. Results and discussion
Figure 6 shows the linear deviation of the skull models over 12
landmarks. The error values varied between minimum errorsof 0.02mm and a maximum error of 0.25mm with an average
deviation of 0.108mm. The deviation is reported to be in
the negative with an under-dimensioned representation of the
replica in comparison to the virtual model. Also, the figureshows that apart from a few scatter points the error is
concentrated in the range between 0.07 and 0.15mm with an
average deviation of 0.1mm.
With regard to the mandible study, similar observations
with an under-dimensioned representation of the replica incomparison to the virtual model were presented. Errors
ranged between a minimum of 0.035mm and maximum of0.2mm with an average of 0.079mm reported. Furthermore,the error over various landmarks was concentrated in the
range between 0.05 and 0.08mm as shown in Figure 7. Inaddition greater accuracy was achieved with the mandiblefabrication which had an average error in the order of a
hundredth of a millimetre, whereas the skull showed errors inthe order of a tenth of a millimetre.The influences of themeasured distance aswell as the shape of
the replicated organs on the errors generated during thefabrication stage were investigated. The fitted curves in
Figure 8 shows that the errors reported are random withrespect to the measured distance. In addition, the shape of thereplica has no influence in the fabricated errors where different
error trends for the samemedical organ were observed as shownin Figure 8(a) and (b).
Figure 4 Anatomical landmarks used for bone thickness measurement
Coronal view of skull Sagittal view of skull Coronal view of mandible
gn
gogo
cdl
I
cdl
zyzy
al al
eueu
ecec
Figure 5 Linear measurements of landmarks for the 3D virtual model
Coronal view of skull Axial view of skull Sagittal view of mandible Coronal view of mandible
Table III Anatomical landmark definitions used for bone thickness measurement
No Abbrev Landmark name Definition
Skull1 al Alare The most lateral points on the nasal aperture in a transverse plane
2 ec Ectoconchion The intersection of the most anterior surface of the lateral border of the orbit and a line bisecting the orbit along
its long axis
3 eu Euryon The points on opposite sides of the skull that form the termini of the line of greatest cranial breadth
4 l Lambda The ectocranial midline point where the sagittal and lambdoidal sutures intersect
5 zy Zygion Instrumentally determined as the most lateral point on the zygomatic arch
Mandible6 cdl Condylion laterale The most lateral point on the mandibular condyle
7 gn Gnathion The most inferior midline point on the mandible
8 go Gonion A point along the rounded posteroinferior corner of the mandible between the ramus and the body
Error analysis of FDM fabricated medical replicas
Ihab El-Katatny, S.H. Masood and Y.S. Morsi
Rapid Prototyping Journal
Volume 16 · Number 1 · 2010 · 36–43
39
Dow
nloa
ded
by N
atio
nal I
nstit
ute
of T
echn
olog
y T
iruc
hira
ppal
li A
t 20:
55 0
1 M
arch
201
6 (P
T)

With regard to the accuracy of bone thickness fabrication, as
shown in Figure 9, a high degree of accuracy of bone
thickness fabrication was observed. An average of less than
0.03mm deviation between the bone thickness of the replica
and its virtual model with the error ranges from 0.007 to
0.064mm were reported.Table V outlines the overall absolute difference between the
skull virtual model and its replicas were in the range between
0.21 and 0.27 per cent with a standard deviation ranging
between 0.12 and 0.2 per cent. With regard to the mandible
the overall absolute difference between the virtual model and
its replica are in the range of 0.15-0.32 per cent with a
standard deviation range between 0.08 and 0.14 per cent.
Furthermore, as shown in Table VI(a), a high level of
accuracy is reported with the reduction of absolute error
percentage to less than half in comparison with the errors
reported in the recent studies by Nizam et al. (2006) and
Choi et al. (2002). This was further reduced to almost one-
tenth in comparison with earlier studies by Kragskov et al.
(1996), Barker et al. (1994) and Lill et al. (1992). Despite
the majority of the studies being carried out on the
comparison between the dry skull and its fabricated replica,
the reduction of the errors remained in the vicinity of 50
per cent in comparison to that reported by Choi et al.
(2002). In his study, the errors between the virtual model
and its rapid prototype replica for the same landmark and
Figure 6 Linear deviations between the skull virtual models and replicas over 11 landmarks
Errors of the skull models fabrication
00.010.020.030.040.050.060.070.080.090.1
0.110.120.130.140.150.160.170.180.190.2
0.210.220.230.240.250.26
0 1 2 3 4 5 6 7 8 9 10 11 12
Landmarks no.
Err
or (
mm
)
Infant Female Male
Table IV Mean and percentage of the absolute differences for the linear measurements
Infant Female Male
Virtual Replica
Absolute
difference Virtual Replica
Absolute
difference Virtual Replica
Absolute
difference
No mm mm mm % mm mm mm % mm mm mm %
Skull1 118.07 117.98 0.087 0.07 122.20 122.13 0.069 0.06 139.21 139.12 0.090 0.06
2 78.25 78.12 0.126 0.16 85.54 85.42 0.122 0.14 95.05 94.98 0.073 0.08
3 71.34 71.25 0.094 0.13 81.26 81.16 0.093 0.11 91.47 91.43 0.031 0.03
4 86.44 86.32 0.121 0.14 111.53 111.40 0.127 0.11 117.57 117.37 0.193 0.16
5 17.39 17.31 0.076 0.44 23.13 23.05 0.082 0.35 22.95 22.86 0.092 0.40
6 19.72 19.69 0.029 0.15 29.64 29.48 0.152 0.51 33.01 32.98 0.029 0.09
7 24.85 24.80 0.052 0.21 24.38 24.30 0.085 0.35 26.33 26.25 0.078 0.30
8 23.42 23.33 0.088 0.38 27.99 27.89 0.095 0.34 33.74 33.62 0.115 0.34
9 37.08 36.94 0.133 0.36 37.47 37.33 0.145 0.39 32.64 32.45 0.192 0.59
10 46.98 46.88 0.093 0.20 43.88 43.66 0.219 0.50 46.67 46.43 0.241 0.52
11 136.62 136.51 0.106 0.08 161.70 161.56 0.140 0.09 178.80 178.71 0.086 0.05
Mandible12 24.44 24.37 0.071 0.29 48.85 48.81 0.039 0.08 63.32 63.26 0.065 0.10
13 25.27 25.20 0.070 0.28 36.86 36.80 0.060 0.16 42.29 42.21 0.073 0.17
14 43.96 43.81 0.142 0.32 55.51 55.45 0.054 0.10 85.32 85.25 0.065 0.08
15 19.66 19.59 0.066 0.34 26.99 26.92 0.069 0.26 32.45 32.39 0.059 0.18
16 14.57 14.50 0.072 0.49 22.56 22.49 0.068 0.30 29.13 29.04 0.082 0.28
17 28.37 28.28 0.095 0.33 37.94 37.88 0.060 0.16 42.84 42.72 0.117 0.27
18 60.62 60.54 0.080 0.13 83.12 83.08 0.046 0.06 88.13 88.07 0.067 0.08
19 76.36 76.16 0.201 0.26 102.60 102.48 0.120 0.12 109.64 109.56 0.071 0.06
20 18.58 18.50 0.075 0.40 21.88 21.77 0.110 0.50 30.20 30.15 0.041 0.14
Error analysis of FDM fabricated medical replicas
Ihab El-Katatny, S.H. Masood and Y.S. Morsi
Rapid Prototyping Journal
Volume 16 · Number 1 · 2010 · 36–43
40
Dow
nloa
ded
by N
atio
nal I
nstit
ute
of T
echn
olog
y T
iruc
hira
ppal
li A
t 20:
55 0
1 M
arch
201
6 (P
T)

measurement techniques were also found and compared as
reported in Table VI(b).
5. Conclusion
Studies on the skull showed an average of absolute mean
differences of 0.108mm (0.24 per cent) and average standard
deviations of 0.048mm (0.16 per cent). There was a similar
range of errors with regarded to the mandible replicas
showing an average absolute mean difference of 0.079mm(0.22 per cent) and an average standard deviation of
0.031mm (0.11 per cent). Furthermore, a high level ofaccuracy with the regard to the bone thickness fabrication was
recorded with errors in the range of a hundredth of amillimetre. The fabricated replicas demonstrated negative
presentations in comparison to the virtual models with
Figure 8 Relationship between the error and measured distance for skull (a) and mandible (b) models
The relationship between errors and linear measurement of the skull models fabrication
00.010.020.030.040.050.060.070.080.090.1
0.110.120.130.140.150.160.170.180.190.2
0.210.220.230.240.250.26
0 10 20 30 40 50 60 70 80 90 100 110 120 130 140 150 160 170 180 190
Linear measurement (mm)
Err
or (
mm
)
Infant Female Male
The relationship between errors and linear measurement of the mandible models fabrication
00.010.020.030.040.050.060.070.080.090.1
0.110.120.130.140.150.160.170.180.190.2
0.210.22
0 10 20 30 40 50 60 70 80 90 100 110 120
Linear measurement (mm)
Err
or (
mm
)Infant Female Male
(a) (b)
Figure 7 Linear deviations between the mandible virtual models and replicas over six landmarks
Errors of the mandible models fabrication
00.010.020.030.040.050.060.070.080.090.1
0.110.120.130.140.150.160.170.180.190.2
0.210.22
11 12 13 14 15 16 17 18 19 20 21
Landmarks no.
Err
or (
mm
)
Infant Female Male
Figure 9 Linear deviation of bone thickness fabrication for skull and mandible replicas
Errors of the skull and mandible models fabrication
00.0020.0040.0060.0080.01
0.0120.0140.0160.0180.02
0.0220.0240.0260.0280.03
0.0320.0340.0360.0380.04
0.0420.0440.0460.0480.05
0.0520.0540.0560.0580.06
0.0620.064
al ec eu l ez cdl gn go
Landmarks
Err
or (
mm
)
Infant skull Female skull
Male skull Infant mandibleMale mandible Man mandible
Error analysis of FDM fabricated medical replicas
Ihab El-Katatny, S.H. Masood and Y.S. Morsi
Rapid Prototyping Journal
Volume 16 · Number 1 · 2010 · 36–43
41
Dow
nloa
ded
by N
atio
nal I
nstit
ute
of T
echn
olog
y T
iruc
hira
ppal
li A
t 20:
55 0
1 M
arch
201
6 (P
T)

under-sized replicas over all the linear measurementsobserved. The anatomical parts (skull or mandible) as wellas the replicated size (infant, male and female) seem to havenot much influence on the fabrication accuracy using FDMtechnique. Outstanding fabrication accuracy in comparison toother rapid prototype technology was demonstrated.Furthermore, the use of FDM technique in the fabricationof various anatomical parts to a high level of accuracy isevident.
References
Barker, T.M., Earwaker, W.J.S. and Lisle, D.A. (1994),“Accuracy of stereolithographic models of humananatomy”, Australasian Radiology, Vol. 38 No. 2, pp. 106-11.
Bouyssie, J.F., Bouyssie, S., Sharrock, P. and Duran, D.(1997), “Stereolithographic models derived from X-raycomputed tomography reproduction accuracy”, Surgicaland Radiologic Anatomy, Vol. 19 No. 3, pp. 193-9.
Choi, J.Y.,Choi, J.H.,Kim,N.K.,Kim,Y.,Lee, J.K.,Kim,M.K.,Lee, J.H. andKim,M.J. (2002), “Analysis of errors inmedicalrapid prototyping models”, International Journal of Oral andMaxillofacial Surgery, Vol. 31 No. 1, pp. 23-32.
Garwin, A. (2006), Measuring Adult Human Remains (adaptedfrom: Buikstra and Ubelaker (1994) and Moore-Jansen et al.(1994), ANTH 6 – Forensic Anthropology).
InVesalius (2008), InVesalius Software, Centro de PesquisasRenato Archer, Campinas, available at: www.cenpra.gov.br/promed/software.htm
Kragskov, J., Sindet-Pedersen, S., Gyldensted, C. and Jensen,K.L. (1996), “A comparison of three-dimensional
computed tomography scans and stereolithographic
models for evaluation of craniofacial anomalies”, Journal
of Oral and Maxillofacial Surgery, Vol. 54 No. 4, pp. 402-12.Lill, W., Solar, P., Ulm, C., Watzek, G., Blahout, R. and
Matejka, M. (1992), “Reproducibility of three-dimensional
CT-assisted model production in the maxillofacial area”,
British Journal of Oral and Maxillofacial Surgery, Vol. 30
No. 4, pp. 233-6.Materialise (2004), Magics v9.9, Materialise, Leuven,
available at: www.materialise.com/magicsMeakin, J.R., Shepherd, D.E.T. and Hukins, D.W.L. (2004),
“Fused deposition models from CT scans”, British Journal
of Radiology, Vol. 77 No. 918, pp. 504-7.Nizam, A., Gopal, R.N., Naing, L., Hakim, A.B. and
Samsudin, A.R. (2006), “Dimensional accuracy of the skull
models produced by rapid prototyping technology using
stereolithography apparatus”, Orofacial Sciences, Vol. 1,
pp. 60-6.Santler, G., Karcher, H., Gaggl, A. and Kern, R. (1998),
“Stereolithography versus milled three-dimensional models:
comparison of production method, indication, and
accuracy”, Computer Aided Surgery, Vol. 3 No. 5, pp. 248-56.Sarment, D.P., Sukovic, P. and Clinthorne, N. (2003),
“Accuracy of implant placement with a stereolithographic
surgical guide”, International Journal of Oral and
Maxillofacial Implants, Vol. 18 No. 4, pp. 571-7.Stratasys (2004), Insight, V3.1, Stratasys, Eden Prairie, MN,
available at: www.stratasys.com
Table VI Previous study results compared with current study results
Mean of absolute
difference
Standard deviation of
absolute difference
Comparison models mm % mm %
(a)
Our study Skull virtual model – FDM replica 0.11 0.24 0.05 0.16
Nizam et al. (2006) Dry skull – SLA replica 0.59 0.54 0.89 0.62
Choi et al. (2002) Dry skull – SLA replica 0.62 0.56 0.53 0.39
Kragskov et al. (1996) 3D CT image – SLA replica 1.98 3.59 1.2 2.67
Barker et al. (1994) Dry skull – SLA replica 1.90 2.54 1.48 1.38
Lill et al. (1992) Dry skull – milled replica 1.47 2.19 0.94 1.37
(b)
Our study Skull virtual model – FDM replica 0.11 0.24 0.05 0.16
Choi et al. (2002) Skull virtual model – SLA replica 0.57 0.82 0.62 0.52
Table V Overall mean and percentage differences between the virtual model and its replica
Skull Mandible
Mean of absolute
difference
Standard deviation
of absolute
difference
Mean of absolute
difference
Standard deviation
of absolute
difference
mm % mm % mm % mm %
Infant 0.091 0.21 0.031 0.12 0.097 0.32 0.046 0.10
Female 0.121 0.27 0.043 0.17 0.070 0.19 0.028 0.14
Male 0.111 0.24 0.069 0.20 0.071 0.15 0.021 0.08
Average 0.108 0.24 0.048 0.16 0.079 0.22 0.031 0.11
Error analysis of FDM fabricated medical replicas
Ihab El-Katatny, S.H. Masood and Y.S. Morsi
Rapid Prototyping Journal
Volume 16 · Number 1 · 2010 · 36–43
42
Dow
nloa
ded
by N
atio
nal I
nstit
ute
of T
echn
olog
y T
iruc
hira
ppal
li A
t 20:
55 0
1 M
arch
201
6 (P
T)

About the authors
Ihab El-Katatny is a Research Engineer at Faculty ofEngineering and Industrial Sciences at Swinburne Universityof Technology. His research interests are in rapid prototyping,reconstructive surgery and computational fluid dynamics.
S.H. Masood is a Professor of Manufacturing Engineering atSwinburne University of Technology. He is the ProgramCoordinator of Postgraduate Programs in AdvancedManufacturing Technology at Swinburne. His research
interests are in rapid prototyping, fused deposition
modelling, rapid manufacturing, tissue engineering scaffolds
and CAD/CAM. S.H. Masood is the corresponding author
and can be contacted at: [email protected]
Y.S. Morsi is a Professor of Mechanical Engineering and
leader of Biomechanics and Tissue engineering research
group at Swinburne University of Technology. His research
interests are in biomedical devices, biomechanics, tissue
engineering and nanofabrication.
Error analysis of FDM fabricated medical replicas
Ihab El-Katatny, S.H. Masood and Y.S. Morsi
Rapid Prototyping Journal
Volume 16 · Number 1 · 2010 · 36–43
43
To purchase reprints of this article please e-mail: [email protected]
Or visit our web site for further details: www.emeraldinsight.com/reprints
Dow
nloa
ded
by N
atio
nal I
nstit
ute
of T
echn
olog
y T
iruc
hira
ppal
li A
t 20:
55 0
1 M
arch
201
6 (P
T)

This article has been cited by:
1. Wael Khalil, Mostafa EzEldeen, Elke Van De Casteele, Eman Shaheen, Yi Sun, Maryam Shahbazian, Raphael Olszewski,Constantinus Politis, Reinhilde Jacobs. 2016. Validation of cone beam computed tomography–based tooth printing usingdifferent three-dimensional printing technologies. Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology 121, 307-315.[CrossRef]
2. Alberto Boschetto, Luana Bottini. 2016. Design for manufacturing of surfaces to improve accuracy in Fused Deposition Modeling.Robotics and Computer-Integrated Manufacturing 37, 103-114. [CrossRef]
3. Chandra Bortolotto, Esmeralda Eshja, Caterina Peroni, Matteo A. Orlandi, Nicola Bizzotto, Paolo Poggi. 2016. 3D Printing ofCT Dataset: Validation of an Open Source and Consumer-Available Workflow. Journal of Digital Imaging 29, 14-21. [CrossRef]
4. Martin Leary, Tomas Kron, Cameron Keller, Rick Franich, Peta Lonski, Aleksandar Subic, Milan Brandt. 2015. Additivemanufacture of custom radiation dosimetry phantoms: An automated method compatible with commercial polymer 3D printers.Materials & Design 86, 487-499. [CrossRef]
5. Eddie T. W. Tan, Ji Min Ling, Shree Kumar Dinesh. 2015. The feasibility of producing patient-specific acrylic cranioplastyimplants with a low-cost 3D printer. Journal of Neurosurgery 1-7. [CrossRef]
6. Alberto Boschetto, Luana Bottini. 2015. Surface improvement of fused deposition modeling parts by barrel finishing. RapidPrototyping Journal 21:6, 686-696. [Abstract] [Full Text] [PDF]
7. M. Fantini, F. De Crescenzio, L. Ciocca, F. Persiani. 2015. Additive manufacturing to assist prosthetically guided boneregeneration of atrophic maxillary arches. Rapid Prototyping Journal 21:6, 705-715. [Abstract] [Full Text] [PDF]
8. Qian Peng, Zhangui Tang, Ousheng Liu, Zhiwei Peng. 2015. Rapid prototyping-assisted maxillofacial reconstruction. Annalsof Medicine 47, 186-208. [CrossRef]
9. Jose Miguel Pinto, Cristobal Arrieta, Marcelo E. Andia, Sergio Uribe, Jorge Ramos-Grez, Alex Vargas, Pablo Irarrazaval, CristianTejos. 2015. Sensitivity analysis of geometric errors in additive manufacturing medical models. Medical Engineering & Physics37, 328-334. [CrossRef]
10. A. Boschetto, L. Bottini. 2014. Accuracy prediction in fused deposition modeling. The International Journal of AdvancedManufacturing Technology 73, 913-928. [CrossRef]
11. D. J. Thomas, M. A. B. Mohd Azmi, Z. Tehrani. 2014. 3D additive manufacture of oral and maxillofacial surgical models forpreoperative planning. The International Journal of Advanced Manufacturing Technology 71, 1643-1651. [CrossRef]
12. J. Santolaria, R. Jiménez, M. Rada, F. Loscos. 2014. Error compensation method for improving the accuracy of biomodelsobtained from CBCT data. Medical Engineering & Physics 36, 397-404. [CrossRef]
13. S.H. MasoodAdvances in Fused Deposition Modeling 69-91. [CrossRef]14. A. Noriega, D. Blanco, B. J. Alvarez, A. Garcia. 2013. Dimensional accuracy improvement of FDM square cross-section parts
using artificial neural networks and an optimization algorithm. The International Journal of Advanced Manufacturing Technology69, 2301-2313. [CrossRef]
15. Mika Salmi, Kaija-Stiina Paloheimo, Jukka Tuomi, Jan Wolff, Antti Mäkitie. 2013. Accuracy of medical models made by additivemanufacturing (rapid manufacturing). Journal of Cranio-Maxillofacial Surgery 41, 603-609. [CrossRef]
16. Cristobal Arrieta, Sergio Uribe, Jorge Ramos‐Grez, Alex Vargas, Pablo Irarrazaval, Vicente Parot, Cristian Tejos. 2012.Quantitative assessments of geometric errors for rapid prototyping in medical applications. Rapid Prototyping Journal 18:6,431-442. [Abstract] [Full Text] [PDF]
17. Eduardo Gomes Ferraz, Lucio Costa Safira Andrade, Aline Rode dos Santos, Vinicius Rabelo Torregrossa, Maria do RosarioSantos Freire, Viviane Almeida Sarmento. 2011. Effect of different surface processing protocols in three-dimensional images forrapid prototyping. Advances in Engineering Software 42, 332-335. [CrossRef]
Dow
nloa
ded
by N
atio
nal I
nstit
ute
of T
echn
olog
y T
iruc
hira
ppal
li A
t 20:
55 0
1 M
arch
201
6 (P
T)





























