Embed Size (px)
Citation preview

Knee Surgery, Sports Traumatology, Arthroscopy
CT MEASUREMENTS PRIOR TO COMPUTER-ASSISTED TOTAL KNEEARTHROPLASTY DO NOT IMPROVE ROTATIONAL PLACEMENT OF THEFEMORAL COMPONENT A de Ladoucette Clinique de l'Union Boulevard
RATALENS 31240 SAINT JEAN Email : [email protected] author: A de Ladoucette
--Manuscript Draft--
Manuscript Number: KSST-D-11-00377R3
Full Title: CT MEASUREMENTS PRIOR TO COMPUTER-ASSISTED TOTAL KNEEARTHROPLASTY DO NOT IMPROVE ROTATIONAL PLACEMENT OF THEFEMORAL COMPONENT A de Ladoucette Clinique de l'Union BoulevardRATALENS 31240 SAINT JEAN Email : [email protected] author: A de Ladoucette
Article Type: Original Paper
Corresponding Author: aymard de ladoucette, MDclinique de l'UnionSaint Jean, FRANCE
Corresponding Author SecondaryInformation:
Corresponding Author's Institution: clinique de l'Union
Corresponding Author's SecondaryInstitution:
First Author: aymard de ladoucette, MD
First Author Secondary Information:
Order of Authors: aymard de ladoucette, MD
Order of Authors Secondary Information:
Abstract: Purpose: The aim of this study is to determine whether computer-assisted surgery(CAS) can gain more precision by utilizing information from pre-operative computedtomography (CT).Methods: Sixty-five patients undergoing total knee arthroplasty in 2008 were included.On pre- and post-operative CT, epicondylar and posterior condylar lines were drawnand the posterior condylar angle (PCA) between these two lines measured. During thesurgery, epicondylar and posterior condylar lines were also registered before and afterCAS-guided cuts were made. CAS was used to fix the orientation of the cutting guideon the distal femur at 3° of external rotation from the posterior condylar line.Results: There was no correlation between CT measurements and CASmeasurements. All orientations of the lines (relative to the horizontal) and anglesmeasured using CT were significantly different (p<0.05).Conclusion: No relationship was found between pre-operative CT measurements andperi-operative CAS measurements used to orient the femoral component. Dataobtained from CT cannot be used peri-operatively with CAS to improve rotationalsetting of the femoral component.Level of evidence: Therapeutic study. Level II.
Key words: computed tomography, computer assisted surgery, femoral rotation,epicondylar line, posterior condylar angle
Response to Reviewers: I have followed the advices from the reviewer and the manuscript had been correctedby SF edit. I have modified the tables and references according to both their advices. Ihope the manuscript now fullfill all the requirements needed for an acceptance.Yours sincerely
Powered by Editorial Manager® and Preprint Manager® from Aries Systems Corporation

Cover LetterClick here to download Cover Letter: cover letter.doc

CT MEASUREMENTS PRIOR TO COMPUTER-ASSISTED TOTAL KNEE
ARTHROPLASTY DO NOT IMPROVE ROTATIONAL PLACEMENT OF THE
FEMORAL COMPONENT
A de Ladoucette
Clinique de l’Union
Boulevard RATALENS
31240 SAINT JEAN
Email : [email protected]
Corresponding author: A de Ladoucette
Title Page

CT MEASUREMENTS PRIOR TO COMPUTER-ASSISTED TOTAL KNEE
ARTHROPLASTY DO NOT IMPROVE ROTATIONAL PLACEMENT OF THE
FEMORAL COMPONENT
Introduction
Outcome following total knee arthroplasty (TKA) depends on rigorous placement technique
[4, 29]. Rotational misalignment of the femoral component can cause anterior patellar or
medial femoro-tibial pain [11, 12, 15]. The femoral component must be implanted in external
rotation [10, 11, 19, 25]. The most acknowledged landmark for evaluating femoral rotation
remains the epicondylar line (ECL) [6, 16, 19, 27, 30].
Computed tomography (CT) allows reproducible and reliable measurement of femoral
epiphysis rotation before and after surgery [6, 8, 26]. Computer assisted surgery (CAS) is
reliable in the frontal alignment of the knee [7, 14, 31]. A few studies analyzed the
contribution of CAS to the rotational alignment of the femoral component [8, 19, 22, 23, 26].
CAS helps to visualize the same lines and measure the same angles as measured by CT. CAS
and CT give measurements that are accurate within one degree.
The aim of the present study is to determine whether there is a correlation between CT and
CAS measurements. If CAS is accurate as a guide for the rotation of the femoral component,
post-operative CT measurements of distal femur rotation should be predicted from pre-
operative CT and from pre- and post-cut (peri-operative) CAS measurements.
Materials and methods
All patients (n=65) undergoing TKA in 2008 with CAS using the Navitrack system
(Orthosoft, Montreal, Canada) at our institution were prospectively included.
CAS with the Navitrack system
The Navitrack (Orthosoft, Montreal, Canada) navigation system gives an image-free
application dedicated to the Natural Knee II prosthesis (NKII) (Zimmer, Warsaw, IN) [7,
31]. The version of Navitrack used in this study was exclusively developed for the NKII. The
use of the Navitrack system has been described previously [7, 21, 31]. Bolognesi et al. [7]
reported that, using this navigation system, 98% of the femoral components and 100% of the
*Blinded ManuscriptClick here to view linked References
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65

tibial components were placed within 3 degrees of the ideal radiographic goal position (90 ±
3°).
Surgical technique
The Natural Knee II approach, with the conventional ancillary system, was used to externally
rotate the femoral component at 3° from the posterior condylar line. This follows the
principles of the anatomical surgical technique [18]. While operating using CAS, after having
registered the posterior condylar line, the same principle were followed and, using CAS, the
cutting guide was systematically adjusted to 3° of external rotation from the posterior
condylar line. When CAS indicated that the cutting guide lay at the appropriate orientation,
the cutting guide was securely fixed to the bone and the cut was made. Before performing the
cut, it was always verified that this orientation was not markedly different from the orientation
that would have been applied if the surgery were performed without CAS using conventional
ancillary tools.
Radiographic evaluation
CT was performed pre-operatively and at three months post-procedure in order to measure the
rotation of the distal femur according to the protocol described by Hernandez et al. [13] and
Mahboubi et al. [20]. The posterior condylar line (CT PL) and the epicondylar line (CT ECL)
were measured according to the methods of Michaut et al. [21] (Fig. 1). The posterior
condylar angle (CT PCA), between the posterior condylar line and the epicondylar line, was
calculated as described by Richard et al. [24] (Fig. 1). Separate measurements were made by
an experienced radiologist and by the author. When a difference in measurement between the
two reviewers was noted, a common verification was undertaken.
CAS evaluation
Landmarks used for the registration of lines and angles with CAS were the same as those used
with CT (Fig. 2). The orientations of the posterior condylar line (CAS PL) were measured, as
it is known that registration of the epicondylar line is not accurate with CAS [7, 19]. The
rotation of the cutting guide from the posterior condylar line (CAS ER) was also registered,
just after fixing the cutting guide onto the bone. For each of these measurements a positive
result indicated an externally rotated angle.
Statistical analysis
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65

Pre- and post-operative quantitative variables on CT and quantitative variables measured peri-
operatively by CAS were compared using both Student’s parametric test and comparison of
variances (Levene’s and Bartlett's tests). Analysis of linear correlations between the results of
the CT and CAS measurements was performed using the Pearson test. Data were analyzed
using XLSTAT 2009 software (Addinsoft). Significance was accepted at p<0.05.
Results
Table 1 shows results of CAS and CT posterior condylar line orientation. The pre-operative
measurements of the posterior condylar line from CT differed significantly from those
obtained using CAS (p<0.001). Comparison of post-operative CT measurements with the
same post-operative CAS measurements indicates a significant difference (p<0.001).
Table 2 reports results of pre- and post-operative measurements. The post-CAS PL, measured
after cutting, is no more externally orientated than the rotation of the femoral epiphysis
measured with CAS before cutting (pre-CAS PL) (n.s.). The pre-operative rotation set to the
cutting guide with CAS (CAS ER) is statistically similar to the orientation of post-CAS PL
(n.s.). The post-operative CT posterior condylar angle (post-CT PCA) values were lower than
the pre-operative values (pre-CT PCA) but the difference was not statistically significant
(n.s.).
No significant correlations were found between the pre-operative and post-operative CT
measurements of the posterior condylar angles (Fig. 3).
Discussion
The most important finding of this study is that the femoral component is externally rotated
with CAS in patients treated with TKA. CAS was used according to the anatomic technique,
as would have been done with the conventional NKII ancillary [18]. A systematic external
rotation at 3° to the condylar posterior line was given to the antero-posterior femoral cutting
guide. It has long been known that the posterior condylar cut must not be parallel to the
posterior condylar line but must be more or less parallel to the epicondylar line, to favor
ligament balancing and patellar tracking [1, 3, 11, 19, 21, 25].
Location of the epicondylar line by CAS is neither accurate nor reliable [7, 19]. However,
Arima et al. [3] and Stöckl et al. [26] easily and accurately marked the posterior condylar line
using CAS. Moreover, CT measurement of the epicondylar and posterior condylar lines are
precise both pre- and post-operatively [6, 8, 21, 26, 27]. The PCA described by Richard et al.
[24] is the angle determined by CT between the epicondylar line and the posterior condylar
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65

line. This angle indicates precisely the distal femoral rotation [12, 21, 24, 29]. The anatomic
epicondylar line is the most reliable landmark for determining the orientation of the femoral
component [2, 4, 5, 9, 12, 17]. However, CAS inaccurately registers the epicondylar line [7,
15, 19]. As it was necessary in this study to link pre-operative CT measurements with peri-
operative CAS measurements; the posterior condylar line was the only line that could be used
both with CAS and with CT [3, 26]. As the posterior condylar angle is between the posterior
condylar line and the epicondylar line, only the posterior condylar angle could be used to link
pre-operative CT measurements with peri-operative CAS measurements.
This study was conducted to determine whether rotation of the femoral component set by
CAS before cutting was concordant with rotation measured on the post-cutting CAS and on
post-operative CT. Results confirmed that the measured post-cutting CAS external rotation is
statistically comparable to the pre-cutting CAS rotation, implying that what is set with CAS
before cutting matches the outcome after cutting.
The second aim was to determine whether the difference of CT posterior condylar angles
measured pre- and post-operatively was equivalent to the rotation applied peri-operatively
with CAS (CAS ER ).
The measured post-operative CT external rotation was smaller than the rotation that should
have been obtained if the CAS and CT measurements correlated. These results indicate a lack
of correlation between lines and angles measured by CT versus CAS even though the same
pre-operative landmarks were used with both. This absence of correlation is partly due to the
fact that CT can only measure bone references whereas CAS takes cartilage into account,
although the most prominent points of the posterior condyles are registered by both CT and
CAS. In osteoarthritis, posterior condylar cartilage wear is not as severe as distal condylar
cartilage wear. The normal postero-medial cartilage thickness is greater than that of the
postero-lateral compartment [28].
Another explanation for the difference between CT and CAS measurements is the fact that the
two systems use different reference planes. The CT reference is the true horizontal plane
whereas CAS uses a computer-calibrated plane at the onset of surgery. This calibration is
evaluated at the first stage of registration of the calibration CAS tools, from the plane set
while determining the center of the femoral head, and from the flexion/extension plane of the
knee.
The PCA measured with CAS is of no use. There is a lack of precision in recording
epicondylar reference points because of the presence of ligament and synovial tissues that
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65

cover the bone structures [7, 19]. The everted or tilted patella hides the lateral epicondylar
landmark and total exposure of the lateral condyle remains difficult [3, 6, 8, 21, 26].
The anatomical surgical technique to determine orientation of the femoral component was not
improved with the CAS system used in this study, contrary to the conclusion of Michaut et al.
[21] who used the same Navitrack CAS system and correlated it with CT measurements.
However, this is the first study to precisely measure and compare the posterior epicondylar
and condylar lines with CAS before and after condylar cuts with the pre- and post-operative
CT measurements. Several authors reported that CAS successfully directs the femoral
component in external rotation [8, 21, 22, 23, 26] as confirmed here.
This study has some limitations. First, it was designed to compare two systems that reference
several anatomical landmarks essential to the performance of TKA. These two systems, CAS
and CT, do not use the same reference plane, even if the lines and angles used refer to the
same landmarks. The data used for this study are exactly those provided before surgery by CT
or to the surgeon intraoperatively by CAS. This study did not compare the two techniques but
determined whether these two methods of measuring the torsion of the femoral distal
epiphysis could be used together during surgery. As noted by Lützner et al. [19], who used
another CAS system, the Navitrack CAS system used in this study does not offer more
precision than the usual surgical system without CAS in handling rotation of the femoral
component. What is measured peri-operatively with CAS is different than the pre- and
postoperative CT measurements. Yet, CAS has proven its efficacy for the alignment of the
inferior limb on the frontal and sagittal planes. It seems unnecessary to utilize pre-operative
CT to evaluate distal condylar torsion as it will have no use during the procedure, even with
CAS to help align the posterior cutting guide.
Conclusion
Pre- and post-operative CT was performed on 65 patients operated on using CAS for TKA.
The femoral component was to be set with an external rotation of 3° from the pre-operative
posterior condylar line. The cuts were controlled by CAS. The aim of this study was to
explore the relationship between pre-operative CT and peri-operative CAS measurements. No
correlations could be found between the lines and angles measured by CT and those measured
by CAS. CAS helps to externally rotate the femoral component but the external rotation
measured by CAS is totally different from that measured by CT. Pre-operative CT is of no
value in determining the exact rotation of the femoral component needed during CAS-guided
surgery to ensure that post-operative rotation complies with the preoperative goal.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65

References
1. Akagi M, Matsusue Y, Mata T, Asada Y, Horiguchi M, Lida M, Nakamura T (1999)
Effect of rotational alignment on patellar tracking in total knee arthroplasty. Clin
Orthop Relat Res 366:155-163.
2. Anouchi Y S, Whiteside L A, Kaiser A D, Milliano M T. (1993) The effects of axial
rotational alignment of the femoral component on knee stability and patellar tracking
in total knee arthroplasty demonstrated on autopsy specimens. Clin Orthop Relat Res
287:170-177
3. Arima J, Whiteside L A, Mccarthy D S, White S E. (1995) Femoral rotational based
on the anteroposterior axis, in total knee arthroplasty in a valgus knee. A technical
note. J Bone Joint Surg Am 77:1331-1334
4. Bargren J H, Blaha J D, Freemanf M A. (1983) Alignment in total knee arthroplasty.
Correlated biomechanical and clinical observations. Clin Orthop Relat Res 173:178-
183
5. Berger R A, Crossett L S, Jacobs J J, Rubash H E. (1998) Malrotation causing
patellofemoral complications after total knee arthroplasty. Clin Orthop Relat Res
356:144-153
6. Boisrenoult P, Scemama P, Fallet L, Beaufils P. (2001) La torsion epiphysaire distale
du fémur dans le genou arthrosique. Rev Chir Orthop Reparatrice Appar Mot 87:469-
476
7. Bolognesi M, Hofmann A. (2005) Computer navigation versus standard
instrumentation for tka: a single surgeon experience. Clin Orthop Relat Res 440:162-
169
8. Chauhan S K, Scott R G, Breidahl W, Beaver R J. (2004) Computer-assisted knee
arthroplasty versus a conventional jig-based technique a randomised, prospective trial.
J Bone Joint Surg Br 86: 372-377
9. Churchill D L, Incavo S J, Johnson C C, Beynnon B D. (1998) The transepicondylar
axis approximates the optimal flexion axis of the knee. Clin Orthop Relat Res
356:111-118
10. Eckhoff D G, Md, Bach J M, Spitzer V M, Reinig K D, Bagur M M, Baldini T H,
Rubinstein D R, Humphries S. (2003) Three-dimensional morphology and kinematics
of the distal part of the femur viewed in virtual reality. J Bone Joint Surg Am 85
(Suppl 4):97-104
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65

11. Fehring T K. (2000) Rotational malalignment of the femoral component in total knee
arthroplasty. Clin Orthop Relat Res 380:72-79
12. Galaud B, Beaufils P, Michaut M, Abadie P, Fallet L, Boisrenoult P. (2008) Torsion
distale fémorale du genou : comparaison de la mesure par tomodensitométrie et par
navigation peropératoire au cours des arthroplasties totales de genou. A propos de 70
cas. Rev Chir Orthop Reparatrice Appar Mot 94 573-579
13. Hernandez R J, Tachdjian M O, Poznanski A K, Dias L S. (1981) CT determination of
femoral torsion. Am. J. Radiol 137:97-102
14. Jenny J Y, Boeri C. (2001) Implantation d'une prothèse totale de genou assistée par
ordinateur. Rev Chir Orthop Reparatrice Appar Mot 87:645-652
15. Jenny J Y, Boeri C. (2004) Low reproducibility of the intra-operative measurement of
the transepicondylar axis during total knee replacement. Acta Orthop 75:74-77
16. Katz M A, Beck T D, Silber J S, Seldes R M, Lotke P A. (2001) Determining femoral
rotational alignment in total knee arthroplasty. Reliability of techniques. J
Arthroplasty 16:301-305
17. Kim Y K, Kim J S, Choi Y, Kwon O R.(2009) Computer-assisted surgical navigation
does not improve the alignment and orientation of the components in total knee
arthroplasty. J Bone Joint Surg Am 91:14-19
18. Lehnen K, Giesinger K, Warschkow R, Porter M, Koch E, Kuster M. (2011) Clinical
outcome using a ligament referencing technique in CAS versus conventional
technique. Knee Surg Sports Traumatol Arthrosc: 19:887-892
19. Lützner J, Krummenauer F, Wolf C, Günther K P, Kirschner S. (2008) Computer-
assisted and conventional total knee replacement a comparative, prospective,
randomised study with radiological and ct evaluation. J Bone Joint Surg Br 90:1039-
1044
20. Mahboubi S, Horstmann H. (1986) Femoral torsion: ct measurement. Radiology 160:
843-847
21. Michaut M, Beaufils P, Galaud B, Abadiea P, Boisrenoult P, Fallet L. (2008) Rotation
fémorale par navigation sur la base d’un scanner pré-opératoire dans l’arthroplastie
totale de genou : a propos de 70 cas. Rev Chir Orthop Reparatrice Appar Mot 94:580-
584
22. Mizu-Uchi H, Matsuda S, Miura H, Okazaki K, Akasaki Y, Iwamoto Y. (2008) The
evaluation of postoperative alignment in total knee replacement using a ct-based
navigation system. J Bone Joint Surg Br 90:1025-1031
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
23. Nagamine R, Miura, Inoue. (1998) Reliability of the antero posterior axis and the
posterior condylar axis for determining rotational alignment of the femoral component
in TKA. J Orthop Sci 3:194-198
24. Richard A, Berger Ra, Rubash H E, Seel M J, Thompsoann W H, Crossett L E. (1993)
Determining the rotational alignment of the femoral component in total knee
arthroplasty using the epicondylar axis. Clin Orthop Relat Res 86:40-47
25. Stiehl J B, Abbott B D. (1995) Morphology of the transepicondylar axis and its
application in primary and revision total knee arthroplasty. J Arthroplasty 10:785-789
26. Stöckl B, Nogler M, Rosiek R, Fischer M, Krismer M, Kessler O. (2004) Navigation
improves accuracy of rotational alignment in total knee arthroplasty. Clin Orthop
Relat Res 426:180-186
27. Suter T, Zanetti M, Schmid M, Romero J. (2006) Reproducibility of measurement of
femoral component rotation after total knee arthroplasty using computer tomography.
J Arthroplasty 21:744-748
28. Terukina M, Fujioka H, Yoshiya S, Kurosaka M, Makino T, Matsui N, Tanaka J.
(2003) Analysis of the thickness and curvature of articular cartilage of the femoral
condyle. Arthroscopy 19:969-973
29. Victor J, Van Doninck D, Labey L, Van Glabbeek F, Parizel P, Bellemans J. (2009) A
common reference frame for describing rotational alignment of the distal femur. J
Bone Joint Surg Br 91:683-690
30. Yoshino N, Takai S, Ohtsuki. (2001) Computed tomography measurement of the
surgical and clinical trans epicondylar axis of the distal femur in osteoarthritic knees. J
Arthroplasty 16:493-497
31. Zumstein M, Frauchiger L, Wyss D, Hess R, Ballmer P. (2006) Is restricted femoral
navigation sufficient for accuracy of total knee arthroplasty. Clin Orthop Relat Res
451:80-86
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65

Figure 1Click here to download high resolution image

Figure 2Click here to download high resolution image
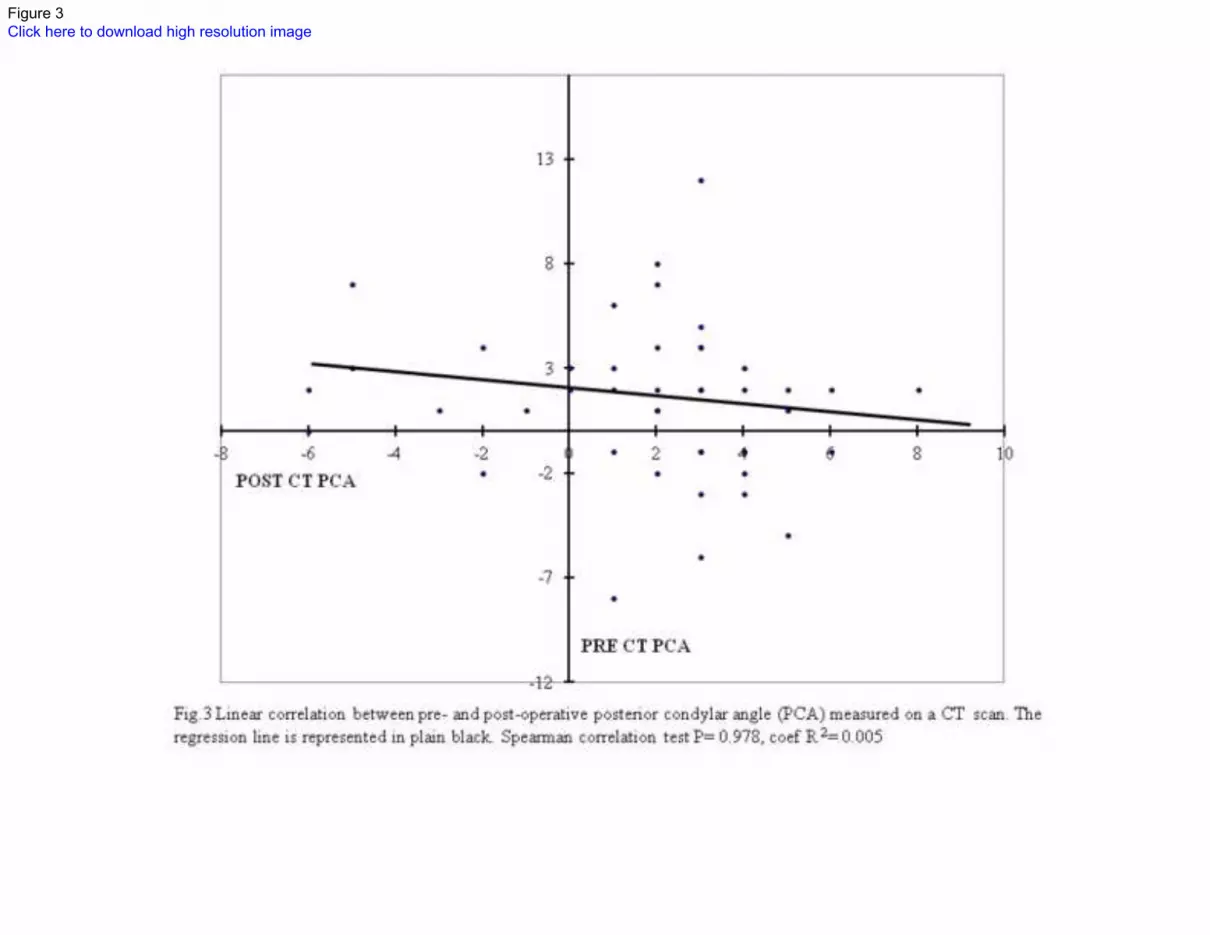
Figure 3Click here to download high resolution image

Pre- PL Post- PL
CT (°) 2 ± 9 1 ± 7
CAS (°) 2 ± 3 3 ± 2
p <0.001 <0.001
Table 1: Median ± standard deviation pre- and post-operative posterior condylar line (PL)
measured on computer tomography (CT) and with computer assisted surgery (CAS). For the
CAS measurements, ‘pre-’ indicates before the cut and ‘post-’ after the cut. Comparison of
variance (Levene test) (p<0.05). *The orientation of PL was calculated in relation to the
horizontal plane.
Table 1

CT PCA CT PL CT ECL CAS PL CAS ER
(°) (°)* (°)* (°)* (°)*
Pre-(operative) 2 ± 3 2 ± 9 3 ± 9 2 ± 3 3 ± 2
Post-(operative) 1± 4 1 ± 7 2 ± 6 3 ± 2
p n.s. n.s. n.s. n.s. n.s.
Table 2: Median ± standard deviation of posterior condylar angle (PCA), posterior condylar
line (PL), and epicondylar line (ECL) measured on computer tomography (CT) and with
computer assisted surgery (CAS). For the CAS measurements, ‘pre-’ indicates before the cut
and ‘post-’ after the cut. Pre-operative CAS rotation of the cutting guide (CAS ER) was
compared to post-CAS PL. Comparison of variance (Levene test) (p<0.05). *The orientation
of ECL, ER, and PL were calculated in relation to the horizontal plane.
Table 2





























