Embed Size (px)
Citation preview
A Study on
SHG Interventions in Eradicating Anaemia in Women in the Urban Slums of Motihari, Bihar
Submitted toXavier Institute of Management, Jabalpur
As Partial Fulfilment of the Requirements for the
Post Graduate Diploma in Rural Management June 2015
Under the Guidance ofDr. Jogendra Pathak
Submitted byMs. Stella Monica Topno
Xavier Institute of Management, Jabalpur (XIMJ)(An Educational Unit of XIDAS)
4th Mile, Mandla Road, Tilheri, Jabalpur (MP)

ACKNOWLEDGEMENT
Immeasurable appreciation and deepest gratitude for the help and support are extended to the following persons who in one way or another have contributed in making this study possible.
Fr. Alfred Toppo, Director, XIMJ, for giving me this opportunity to do my internship in APMAS and learn the real grass roots. I am thankful to Mr. Mehul Chauhan, Dean, XIMJ, for his support and guidance.
I am also thankful to Dr. J. Jha, Head of Department, RM, XIMJ, for giving his valuable time during the SIP orientation and provide us guideline.
My sincere thanks to Dr. Jogendra Pathak, Assistant Professor, XIMJ, for his time and effort in checking my study topic and giving me the continuous help whenever I had a break down.
Mr. Sunil Kumar Singh, Director, APMAS, Bihar, for his support, advices, guidance, valuable comments, suggestions and provisions that benefitted me much in the completion and success of this study.
The Project Officer, Mr. Sanjay Soni, APMAS, had taken many pains during fieldwork in collecting data and conducting Focus Group Discussions. In this regard my sincere thanks and tons of appreciation to him.
I am grateful to the Community Mobilisers of Nirdesh, Motihari, for their time and effort for conducting Focus Group Discussions for my study.
The SHG respondents, without whose sacrifices and contributions, who have spared their valuable time, this study would not been a reality, deserve the core of my appreciation and thanks. Lastly I am very thankful to my parents who have been a great inspiration and given me constant support throughout my study, without them this study would not be a successful.

CONTENTS
Declaration by student (i)
Declaration by guide (ii)
Acknowledgement (iii)
List of tables (iv)
List of figures (v)
List of abbreviations (vi)
Executive summary (vii)
1. Introduction 1-4
1.1 Background 1
1.2 Rationale of the study 1
1.3 Objective 1
1.4 Anaemia as a curse 2
1.5 Limitation of the study 4
1.6 Chapterisation 4
2. Research methodology 5-8
2.1 Research Design 5
2.2 Sample design 5
2.3 Method of Data collection 6
2.4 Method of data analysis 7
2.5 Project Period 7
3. Profile of the study area 8-10
3.1 About Motihari 8
4 Organisational Profile 11-14
4.1 APMAS 11

4.2 Vision 11
4.3 Mission 11
4.4 Core values 11
4.5 Thrust area 11
4.6 APMAS Activities 12
4.7 Sadhikaratha Foundation 13
4.8 Support Programme for Urban Reform 14
5. Analysis and Discussion 15-24
5.1 Target Area of the Study 15
5.2 SHG Groups Under Taken for Study 15
5.3 Poverty Level of SHG Members 15
5.4 Eating Habits of SHG Members 16
5.5 Symptoms of Anaemia in Women 18
5.6 Prevalence of Anaemia in Pregnant women and Lactating Mothers 19
5.7 Awareness Level of SHG 21
5.8 Government Interventions to Fight Anaemia 22
5.9 Government Schemes Related to Health of a woman 24
6. Findings and recommendations 25-27
6.0 Findings 25
6.1 Recommenations 26
6.2 Conclusion 27
7. Bibliography 28
Annexure (x)

LIST OF TABLES
S.No DESCRIPTION PAGE No.
3.1 Demographic details of Motihari 11
5.3 Poverty Levels of SHG Members 17
5.4.1 Intake of sufficient food by SHG women 19
5.5(a) Women feel numbness and coldness on the feet 20
5.5(b) Women falling sick all the time 20
5.6(c) Prevalence of Anaemia in Pregnant and lactating
women 22
5.7 Drinking of milk solves health issues 25

LIST OF FIGURES
S.No
DESCRIPTION
PAGE No.
5.4
Unavailability of nutrition
food to the women
18
5.4.1 SHG
women work empty
stomach
19
5.5(c) Paleness of
skin prevail in women
21
5.6(a) Women
being exposed to various
infections
5.6(b) Women
getting repeated attack of
Malaria
5.6(d) Women
facing irregular
menstruation cycle
5.6(e) Women
facing blood loss during
pregnancy

LIST OF ABBREVIATION
ABBREVIATION ACRONYM SHG Self Help Group
NABARD National Bank for Agricultural and Rural Development
MMR Maternal Mortality Rate
IFA Iron Folic Acid
NGO Non- Government Organisation
APMAS Mahil Abhivruddhi Society, Andhra Pradesh
FCRA Foreign Contribution Regulation Act
CSO Civil Society Organisation
SHPI Self-Help Promoting Institutions
MIS Management Information System
SPUR Support Programme for Urban Reform
APL Above Poverty Line
BPL Below Poverty Line
ICDS Integrated Child Development Service
SHSB State Health Society Bihar
ASHA Accredited Society Health Activist
WCD Women and Child Development
JSY Janani Suraksha Yojana
XIMJ Xavier Institute of Management, Jabalpur
XIDAS Xavier Institute of Development Action and Studies

EXECUTIVE SUMMARY
Self Help Group (SHG) is one of the powerful mobilizing movements started among the
poverty stricken people of rural area through which people realize their potential for
engaging in micro finance and sustainable livelihood. Now development has taken
another turn which focus on the urban development. People residing in urban slums are
living in a most utter poverty. SHG has taken them towards the self reliant movement
where people don’t have to depend on government schemes. SHG is a strong movement
which not only motivated the women but also the entire community. It has created a
positive impact not only on the livelihood of the people but also their education, health,
self confidence, decision making ability, participation and self reliant.
SHG comprises of group of micro entrepreneurs having homogeneous social and
economic backgrounds; all voluntarily coming together to save regular small sums of
money, mutually agreeing to contribute to a common fund and to meet their emergency
needs on the basis of mutual help. Credit has been recognized by the government and
banks, as a tool for poverty reduction, for several years. Despite the significant gains
made by the rural credit delivery system in terms of resource mobilization, geographical
coverage and functional reach in the last two decades, there has been deterioration in the
financial health of credit institutions.
OBJECTIVE
The broad objective of the present study is to see whether the SHGs are capable of
handling issues such as health, education and social in their community and also capable
of taking initiative to eradicate anaemia in women. The specific objectives of the current
study are i) to identify the problem of anaemia in pregnant women and lactating mothers
in study area, ii) to assess the awareness level of the disease anaemia among the SHGs of
the study area, iii) to know the Government interventions to eradicate anaemia in the
study area.

ABOUT ANAEMIA
Anemia is the most common disorder of the blood with it affecting about a quarter of
people globally. Iron-deficiency anemia affects nearly one billion. In 2013 anemia due to
iron deficiency resulted in about 183,000 deaths – down from 213,000 deaths in 1990. It is
more common in females than males among children, during pregnancy and in the
elderly. Anemia increases costs of medical care and lowers a person's productivity through
a decreased ability to work.
In Bihar, the Maternal Mortality Ratio (371 per 100,000 live births) is fourth highest in the
country and above the national average of 301. The high level of MMR can be attributed
to low level of institutional deliveries (23.2% compared to national figure 41%), high level
of anaemia among women (63.4% compared to national figure of 51.8%), low provision
of iron and folic acid tablets to ante-natal cases (8.1% compared to national figure of
20.4%), and low level of full ante-natal coverage (5.4% compared to national figure of
16.4%). Nutrition levels of pregnant women are troubling. For only 30 percent of their last
births, did mothers receive iron and folic acid supplements (IFA) and for only 10 percent
of the births did mothers consume IFA for the recommended 90 days or more.
METHODOLOGY
The research design adopted in the present study was descriptive research design. The
universe of the study is SHGs in Motihari, Bihar. Keeping the objectives in view, out of
174 SHGs in Motihari, 100 SHGs were selected from the slums. These SHGs were
selected according to strata. In Motihari, there are about 38 wards and 51 slums. The
strata were made according to the direction; North, South, East, And West and Central.
From each strata 5 slums were selected and from these 5 slums, 20 SHGs were selected
according to their grading (A,B and C). The SHGs of grade A are better performer as
they are punctual in their savings, loan and repayment and also participate in regular
monthly meetings. While, SHGs belong to grade B are average performer and grade C
are lowest performer.
DATA ANALYSIS
The data collected from the 100 SHGs, the data were entered into the SPSS software for
the analysis of the data and for better understanding of the study.
FINDINGS AND CONCLUSION
To sum up, this study was conducted to measure the awareness level of women about
anaemia and its causes. Through the field survey, it was observed that most women were
unaware about anaemia. They understood the disease of having low level of blood count
and they do not know its severe consequences. The study was also conducted to identify
the anaemia cases in the pregnant and lactating mothers, it was observed that most of the
women are anaemic but a mild one. Though iron folic acid tablets are given to them by the
Government but they are ignorant about its importance. Thirdly, a study was conducted on
the programmes and interventions running by the Government for the women and children
development and it was observed that these schemes an programmes are running
successfully but women are unaware about it.
During the field survey, it was observed that the SHG women have not taken any steps to
eradicate anaemia in women. Though these women are capable but they need a capacity
building. The quality of groups is quite low in the urban slums and even they are not
punctual in conducting the meetings. Overall, the status of the SHG movement in the town
appears to be aptly reflected by the monthly savings of the group.

CHAPTER 1
INTRODUCTION
1.1 Background
Self Help Group (SHG) are informal association of people especially women who
choose to come together to find ways to improve their living condition. It is one of the
powerful mobilizing movements started among the poverty stricken people of rural area
through which people realize their potential for engaging in micro finance and
sustainable livelihood. Now development has taken another turn which focus on the
urban development. People residing in urban slums are living in a most utter poverty. It
has created a positive impact not only on the livelihood of the people but also their
education, health, self confidence, decision making ability, participation and self reliant.
Consequently, SHG emerged as the most effective mechanism for delivery of micro-
finance services to the poor.
The Self Help Group is becoming one of the important means for the empowerment of
poor women in almost all developing countries. Despite the significant gains made by
the rural credit delivery system in terms of resource mobilization, geographical coverage
and functional reach in the last two decades, there has been deterioration in the financial
health of credit institutions. Implementation of government sponsored credit linked
poverty alleviation programmes with high transaction cost and default rate and thrusting
of public distribution system on cooperatives have affected the viability of rural lending.
To overcome this difficulty, governments as well as banks have made several innovative
strategies to improve the efficacy of the delivery of financial services to the rural poor,
especially women. The National Bank for Agriculture and Rural Development
(NABARD) was establishes in 1982 through an act of Parliament, as an apex
development agency for supporting and promoting agricultural and rural development in
an integrated manner. NABARD supports various credit delivery innovations which are
being implemented in different parts of the country such as Grameen bank replications,
Non-governmental networks, SHG federations and credit unions.
By encouraging women’s participation, it has created a great impact on their economy.
Women are getting access to bank credits and other formal financial institutions. They
are able to realize the importance of savings. Due to this, there has been an increment in
their salary and expense on food are been met. This improvement not only created a
great impact on their livelihood but also on their education by 43%, health 57%, self
confidence 89%, decision making ability 86%, self reliance 81% and participation in
local agencies 50%.
1.2 Rationale of the study
Despite the measures taken by the government to control anemia in pregnant women in
the last two decades, the severity of nutritional anemia continues to remain a public
health issue of great magnitude. Not only this, even social issues has been increased.
Due to this, families belong to below poverty line are facing problem as they are unable
to pay the bills, low income, insufficient food to eat and dependency.
As SHGs has taken a new turn, by taking initiatives, these women can solve their own
problem and other health issues. With their ability and awareness about the health issues
like anemia can cut down their expense in medicines and medical bills and they invest
money on their small business and their children’s education.
1.3 Objective
The broad objective of the present study is to see whether the SHGs are capable of
handling issues such as health, education and social in their community and also capable
of taking initiative to eradicate anemia in women. The specific objectives of the current
study are:
i. To identify the problem of anemia in pregnant women and lactating
mothers in study area.
ii. To assess the awareness level of the disease anemia among the SHGs
of the study area.
iii. To know the Government interventions to eradicate anemia in the
study area.

1.4 Anaemia as a curse
Anaemia is a condition in which the number of red blood cells or their oxygen-carrying
capacity is insufficient to meet physiologic needs, which vary by age, sex, altitude,
smoking, and pregnancy status. Iron deficiency is thought to be the most common cause of
anaemia globally, although other conditions, such as folate, vitamin B12 and vitamin A
deficiencies, chronic inflammation, parasitic infections, and inherited disorders can all
cause anaemia. In its severe form, it is associated with fatigue, weakness, dizziness and
drowsiness. Pregnant women and children are particularly vulnerable. It can also be
defined as a lowered ability of the blood to carry oxygen. When anemia comes on slowly
the symptoms are often vague and may include: feeling tired, weakness, shortness of
breath or a poor ability to exercise. Anemia that comes on quickly often has greater
symptoms which may include: confusion feeling like one is going to pass out, and
increased thirst. There needs to be significant anemia before a person becomes
noticeably pale. There may be additional symptoms depending on the underlying cause.
Causes of blood loss include trauma and gastrointestinal bleeding among others. Causes of
decreased production include iron deficiency, a lack of vitamin B12, thalassemia and a
number of neoplasms of the bone marrow among others. Causes of increased breakdown
include a number of genetic conditions such as sickle, infections like malaria and some
autoimmune diseases among others. Diagnosis in men is based on hemoglobin of less
than 130 to 140 g/L (13 to 14 g/dL) while in women it must be less than 120 to 130 g/L
(12 to 13 g/dL). Further testing is then required to determine the cause.
Anemia is the most common disorder of the blood with it affecting about a quarter of
people globally. Iron-deficiency anemia affects nearly 1 billion. In 2013 anemia due to
iron deficiency resulted in about 183,000 deaths – down from 213,000 deaths in 1990. It is
more common in females than males among children, during pregnancy and in the
elderly. Anemia increases costs of medical care and lowers a person's productivity through
a decreased ability to work.
In Bihar, the Maternal Mortality Ratio (371 per 100,000 live births) is fourth highest in the
country and above the national average of 301. The high level of MMR can be attributed
to low level of institutional deliveries (23.2% compared to national figure 41%), high level

of anaemia among women (63.4% compared to national figure of 51.8%), low provision
of iron and folic acid tablets to ante-natal cases (8.1% compared to national figure of
20.4%), and low level of full ante-natal coverage (5.4% compared to national figure of
16.4%). Nutrition levels of pregnant women are troubling. For only 30 percent of their last
births, did mothers receive iron and folic acid supplements (IFA) and for only 10 percent
of the births did mothers consume IFA for the recommended 90 days or more.
1.5 Limitation of the study
The limitations/constraints faced during the project were while collecting the primary data
from the field it was very difficult to gather women as SHGs. As it was harvesting time
most of the SHG members were not available for the meetings.
1.6 Chapterisation
The report has been divided into seven chapters. The first chapter deals with the
introduction of the study. The second chapter highlights the methodology used. The
chapter three illustrates the profile of the area where the study was conducted has been
discussed in. The chapter four describes in details about the organization. The analysis of
the study has been discussed in chapter five. The findings and recommendation is placed
in chapter six and that followed with conclusion, annexure, map, photographs and
questionnaires.

CHAPTER 2
RESEARCH METHODOLOGY
2.1 Research DesignThe research design adopted in the present study was descriptive research design. To
study the universe, it is necessary to understand characteristics of the universe or
population. The universe of the study was SHGs of Motihari living in the urban slums.
Keeping the topic in view it is important to understand the lifestyle and work style of the
SHGs and also know the activities conducted within the SHG meetings. Their ability will
determine whether these SHGs are capable of taking steps by themselves in solving
various issues.
2.2 Sample Design
The sampling design used to conduct the study was probability sampling. Probability
sampling is also known as random sampling. Under this sampling design, every item of
the universe has an equal chance of inclusion in the sample. Almost 50% of the slums
were covered to conduct the study. Random sampling ensures the law of statistical
regularity which states that if on an average the sample chosen is a random one, the
sample will have the same composition and characteristics as the universe.
2.2.1 UniverseThe universe of the study was 174 Self Help Groups of urban slums of Motihari. In
Motihari, there are about 38 wards in which in one ward the SHGs are non-functional.
These SHGs are one of the mobilising movements where most of women are benefitted
with the financial issues and also a livelihood. But there are some issues they face
regularly. Being in the urban area, they lack the facilities and also livelihood. They do
not have pucca1 houses to live on. They reside on the places where there is no drainage
system, no proper waste management system and face lot of health issues.
2.2.2 Sampling unit
1 Pucca: a house made of bricks and cement.

The sample unit for the study was 100 SHGs. These SHGs were selected from
selected 5 slums of 5 stratas in Motihari. From each 5 slums 20 SHGs were selected
randomly and every woman were given equal chance of inclusion while collecting
data.
2.2.3 Sampling technique
The sampling technique used was probability sampling because every SHG of the
universe has an equal chance of inclusion in the sample. In order to include every
sample, stratified random sampling was used. Because collecting data from every
SHG was a tough task so by grouping these SHGs according to their date of
formation made it easier to collect sample. According to the law of statistical
regularity, if on an average the sample chosen is a random one, the sample will have
the same composition and characteristics as the universe.
2.3 Method of Data collection
The methodology adopted in the present study was descriptive research design. The data
collected was both quantitative and qualitative in nature from primary and secondary
sources. The data was collected mainly through interviews, focus group discussions and
other participatory methods. Structured and unstructured interviews were conducted
with various stakeholders such as SHG president, secretary and treasurer, project officer
of the field, community mobiliser of the local NGO to understand both internal and
external environment of the SHGs.
The interview schedule consisted of 3 sections. The first section covered the profile or
general information of the SHGs. The second part dealt with the activities and meetings
of the SHGs and the third section dealt with the awareness level of the SHGs about the
anaemia in their community. Structured interviews were conducted with the district
officials such as Programme Officer of ICDS office, Medical Officer of Primary Health
Centre, Block Office, and Medical Deputy Superintendent of Sadar hospital
(Government hospital) and Sevikas2 of Anganwadis.
2 Sevika: Anganwadi worker (mostly female) works as nurse.
2.4 Method of Data analysis
The data collected from the field was entered in to the SPSS software for the analysis for
better understanding of the study.
2.5 Project Period
The duration of the project was for sixty days in which the data collection from the field
was for thirty days. And rest thirty days was dedicated for report and documentations.

CHAPTER 3
PROFILE OF THE STUDY AREA
3.1 About Motihari
Motihari is the headquarters of East Champaran district (Purbi Champaran district) (Tirhut
Division) in the Indian state of Bihar. On 1 December 1977, the Champaran district was
divided into the districts of Purbi Champaran (East Champaran) and Paschimi Champaran
(West Champaran). Motihari and Bettiah became headquarters of East Champaran district
and West Champaran district respectively.
3.1.1 Demographic Profile
In 2011, Purvi Champaran had population of 5,082,868 of which male and female were
2,674,037 and 2,408,831 respectively. In 2001 census, Purvi Champaran had a population
of 3,939,773 of which males were 2,077,047 and remaining 1,862,726 were females. Purvi
Champaran District population constituted 4.90 percent of total Bihar population. In 2001
census, this figure for Purvi Champaran District was at 4.75 percent of Bihar population.
There was change of 29.01 percent in the population compared to population as per 2001. In
the previous census of India 2001, Purvi Champaran District recorded increase of 29.27
percent to its population compared to 1991. The initial provisional data released by census
India 2011, shows that density of Purvi Champaran district for 2011 is 1,281 people per sq.
km. In 2001, Purvi Champaran district density was at 993 people per sq. km. Purvi
Champaran district administers 3,968 square kilometers of areas.
Average literacy rate of Purvi Champaran in 2011 were 58.26 compared to 37.54 of 2001. If
things are looked out at gender wise, male and female literacy were 68.02 and 47.36,
respectively. For 2001 census, same figures stood at 49.31 and 24.27 in Purvi Champaran
District. Total literate in Purvi Champaran District were 2,382,348 of which male and
female were 1,467,319 and 915,029 respectively. In 2001, Purvi Champaran District had
1,164,670 in its district.
With regards to Sex Ratio in Purvi Champaran, it stood at 901 per 1000 male compared to
2001 census figure of 897. The average national sex ratio in India is 940 as per latest reports

of Census 2011 Directorate. In 2011 census, child sex ratio is 923 girls per 1000 boys
compared to figure of 937 girls per 1000 boys of 2001 census data. In census enumeration,
data regarding child under 0-6 age were also collected for all districts including Purvi
Champaran. There were total 993,569 children under age of 0-6 against 837,642 of 2001
census. Of total 993,569 male and female were 516,736 and 476,833 respectively. Child
Sex Ratio as per census 2011 was 923 compared to 937 of census 2001. In 2011, Children
under 0-6 formed 19.55 percent of Purvi Champaran District compared to 21.26 percent of
2001. There was net change of -1.71 percent in this compared to previous census of India.
Table 3.1 Demographic details of Motihari
DESCRIPTION 2011 2001Actual Population 5,082,868 3,939,773
Male 2,674,037 2,077,047
Female 2,408,831 1,862,726
Population Growth 29.01% 29.27%
Sex Ratio (Per 1000) 901 897
Male Literacy 68.02 49.31
Female Literacy 47.36 24.27
Total Child Population (0-6) age
993,569 837,642
SOURCE: eastchamparan.nic.in
3.1.2 Geographic Details
Motihari is around 165 km from Patna, the capital of Bihar, 50 km from Bettiah, and 82 km
from Muzaffarpur. The city is close to Nepal. Birgunj, the second largest city of Nepal, is
55 km away. Motihari is the disctrict located in the western part of the Bihar (between 83°-
30' to 88°-00' longitude). Motihari is divided by a jheel called "Moti-Jheel". There is a bridge
which connects both the parts of town. On this bridge there are open markets of cloths, fish,
plastic items which are available at low cost. Meena Bazaar is a hub for all types of market:
Electronics, clothes, kitchen items, fruits, vegetables.

CHAPTER 4
ORGANIZATIONAL PROFILE
4.1 APMAS
APMAS is a technical resource organization registered under the Andhra Pradesh (Telangana
Area) Public Societies Registration Act, 1350 Fasli (No.3800 dated 14.06.2001) and
subsequently under Foreign Contribution Regulation Act (FCRA) on 28.10.2002
(No.010230543). It began its activities in Andhra Pradesh (AP) on 1st July 2001 and
subsequently expanded to more than a dozen states either through direct interventions or
through networking and alliances. These states include: Andhra Pradesh, Bihar, Chhattisgarh,
Gujarat, Jharkhand, Karnataka, Madhya Pradesh, Maharashtra, North-East (Assam &
Manipur), Odisha, Rajasthan, Uttar Pradesh (UP), and West Bengal.
4.2 Vision
A sustainable self-help movement in India.
4.3 Mission
To promote self-reliant people's institutions, especially Self-Help Groups (SHGs) and SHG
federations, in such a way as to realize their full potential for engaging in microfinance and
sustainable livelihoods, their members overcoming poverty and inequalities.
4.4 Core Values
1. Concern for quality.
2. Gender equality and social inclusion.
3. Self reliance.
4. Transparency and accountability.
5. Promote participation and democracy.
6. Continuous learning.
4.5 Thrust Areas
1. Capacitate self-help and livelihoods promoting institutions both in rural and urban
areas.

2. Promote natural resource management and sustainable livelihoods resulting in
desirable climate change practices and food security.
3. Reach out to unreached and underserved areas for addressing poverty and
inequalities.
4. Enhance partnerships, collaborations and alliances for linking, learning, up-scaling
and advocating.
5. Enhance research and advocacy for influencing policy decisions in favour of people’s
institutions engaged in microfinance and livelihoods.
4.6 APMAS Activities
APMAS core focus is building the capacities of the civil society organizations (CSOs), the
Self-Help Promoting Institutions (SHPIs) self-help groups (SHGs) and their federations,
people's organizations and government functionaries through trainings, research, advocacy
and livelihood promotion. It began its activities in Andhra Pradesh on 1 July 2001 APMAS
with the main objective of enhancing the quality and sustainability of the SHG movement and
community based inclusive interventions. It has been able to expand its horizon in terms of
significant interventions to Bihar, Uttar Pradesh, Madhya Pradesh and Orissa through direct
interventions and to Rajasthan, Gujarat, Maharashtra, Karnataka, Chhattisgarh, North-East,
Jharkhand and West Bengal through networking and alliances.
APMAS has made a successful, yet a very challenging journey over the past twelve years and
emerged as a trustworthy and credible resource organisation at the national and international
level in providing technical and managerial services to strengthen the SHGs, SHG
Federations and livelihood institutions. It has been remarkably successful in establishing
partnerships and collaboration with diverse stakeholders such as CBOs, NGOs, national and
international donors, State Governments, Planning Commission, NABARD, Banks, Research
and Academic institutions. APMAS has also made its impact felt in the international arena,
by providing its services in Bangladesh, Canada, Ethiopia, Germany, Thailand and Vietnam.
To meet the ever increasing of its clientele, APMAS has promoted a Section 25 Company -
Sadhikaratha Foundation in 2011.
4.7 Sadhikaratha Foundation
Sadhikaratha Foundation, a non-profit Company was incorporated on 13 January 2012 under
Section 25 of the Companies Act, 1956 (No.1 of 1956) promoted by APMAS. The Corporate
Identity Number of the Company is U85110AP2012NPL078569. The promoters and the first
Directors of the Company were the eminent personalities Shri. K. Madhava Rao, IAS (Retd)
and Ms. Nandita Ray, who with their vision and exemplary work, have been contributing to
the overall development of the society especially the underprivileged sections of the country.
Subsequently four other eminent personalities from various sectors have been invited to be
the Directors. The Foundation will expand its membership base up to eleven in near future.
4.7.1 Prime objectives of Sadhikaratha
1) To provide training and capacity building, monitoring and evaluation services for social
development projects, to women's groups including self help groups (SHGs) farmers,
government agencies, banks, NGOs, international agencies (donors and governments) and
any organization whether registered under any Act or unregistered, as well as to formal or
informal federations of such groups in all aspects leading to social and economic
empowerment of poor people and women and assist such groups in mobilizing financial,
technical and other resources from government agencies, national and international donor
agencies, banks, financial institutions and other organizations.
2) To provide services including research and evaluation in the area of social development
such as baseline studies, process monitoring, project evaluation, feasibility studies, material
development, developing rating tools / accreditation tools, establishing systems
(bookkeeping, auditing, MIS), product designing, NGO empanelment undertake advocacy
related to policy framework, awareness creation related to Self Reliant Cooperatives,
Community Based Organistion in the area of social, rural and urban development, health,
poverty reduction and to support those organizations which are engaged in economic
empowerment of poor people, including organizations, institutions and groups of the poor in
other developing countries in Asia, Africa and Latin America or any other part of the world.
3) To carry out all types of development programmes, including project implementation and
undertake all types of initiatives and interventions in the areas of gender equality, education,
poverty alleviation, watershed development, natural resource management, slum

development, rights based advocacy, climate change, renewable energy, natural resource
management, income and livelihood creation and support in any area in which development
activity and intervention is required and to create sustainable development by disseminating
appropriate products, services and technologies directly or through a network of independent
grass roots voluntary organizations and to bid for various social development projects as an
individual organization or as a consortium and to conduct various certificate and diploma
courses to the said qualified organizations, individuals.
4.8 Support Programme for Urban Reform (SPUR)
The project envisages to provide capacity building and handholding support to NGOs and
SHGs already formed in 28 ULBs (SPUR towns) of Bihar as well as formation of SHGs and
town level federations in 17 towns (non-SPUR towns). This project will be implemented by
Sadhikaratha Foundation with the technical support and guidance from APMAS.

CHAPTER 5
ANALYSIS AND DISCUSSIONS
The present chapter discusses the analysis of the primary data and secondary data collected
during the field survey for the present study.
5.1 Target Area of the Study
The table-1 in annexure depicts the target area of the study was 100 SHGs in the urban slums
of Motihari, Bihar. Out of 174 SHGs, 100 SHGs were selected as a sample size covering 18
wards.
5.2 SHG Groups Under Taken for Study
The table-2 in annexure discusses about the SHG, number of members, their way of
functioning and meetings. The number of SHG groups under taken for the study.
5.3 Poverty Level of SHG Members
The table 5.3 represents the poverty level of SHG members. There are 794 SHG members in
the studied sample out of their 474 are below poverty line and 320 are above poverty line.
Table 5.3 Poverty Levels of SHG Members
S.no Poverty Levels Number of SHG members
1 Below Poverty Line 474
2 Above Poverty Line 320
3 Both 0
4 No APL & BPL 0
5 Total 794 SOURCE: Primary data, 2015
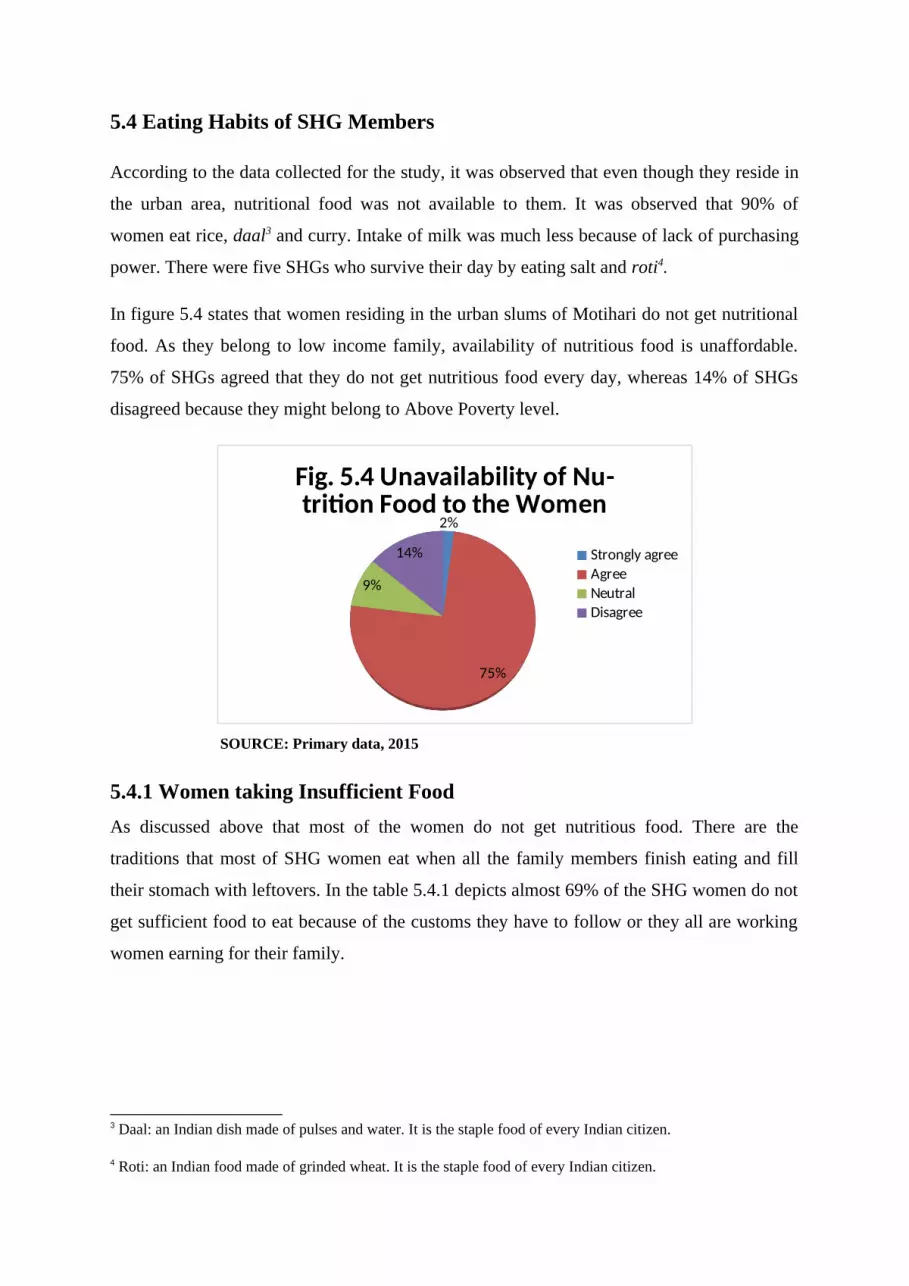
5.4 Eating Habits of SHG Members
According to the data collected for the study, it was observed that even though they reside in
the urban area, nutritional food was not available to them. It was observed that 90% of
women eat rice, daal3 and curry. Intake of milk was much less because of lack of purchasing
power. There were five SHGs who survive their day by eating salt and roti4.
In figure 5.4 states that women residing in the urban slums of Motihari do not get nutritional
food. As they belong to low income family, availability of nutritious food is unaffordable.
75% of SHGs agreed that they do not get nutritious food every day, whereas 14% of SHGs
disagreed because they might belong to Above Poverty level.
2%
75%
9%
14%
Fig. 5.4 Unavailability of Nu-trition Food to the Women
Strongly agreeAgreeNeutralDisagree
SOURCE: Primary data, 2015
5.4.1 Women taking Insufficient FoodAs discussed above that most of the women do not get nutritious food. There are the
traditions that most of SHG women eat when all the family members finish eating and fill
their stomach with leftovers. In the table 5.4.1 depicts almost 69% of the SHG women do not
get sufficient food to eat because of the customs they have to follow or they all are working
women earning for their family.
3 Daal: an Indian dish made of pulses and water. It is the staple food of every Indian citizen.
4 Roti: an Indian food made of grinded wheat. It is the staple food of every Indian citizen.

Table 5.4.1 Intake of sufficient food by SHG women
S.no Response No. Of SHGs Percentage of SHGs (%)
1 Strongly agree 2 2%
2 Agree 69 69%
3 Neutral 14 14%
4 Disagree 15 15%
5 Total 100 100% SOURCE: Primary data, 2015
From the study it was observed that most of the SHG women are working as a vendor,
domestic worker, laborers, etc. In the figure 5.4.1 depicts that 40% of SHG work empty
stomach as they had to get up early and go for vending or labor. The daily wages they earned
was their only source of income, whereas 21% of SHG women have their proper food
because either they belong to APL family or have more earning members.
Strongly agree Agree Disagree0%5%
10%15%20%25%30%35%40%45% 40% 39%
21%
Fig. 5.4.1 Women Working Empty Stomach
women work empty stomach
SOURCE: Primary data, 2015

5.5 Symptoms of Anaemia in Women
From the study conducted, it was observed almost all were working women engaging
themselves in different livelihood activities. Because of doing so much of physical activities
and no sufficient food to fill their stomach, they get fatigue or tired.
Table 5.5(a) Women feel numbness and coldness on the feet
S.no Response No. of SHGs Percentage of SHGs (%)
1 Strongly agree 17 17%
2 Agree 80 80%
3 Neutral 3 3%
4 Total 100 100% SOURCE: Primary data, 2015
Table 5.5(a) depicts that most of the women (80% of SHGs) feels numbness of their feet due
to tiredness. Feeling numbness in the foot is one of the symptoms of mild Anaemia. As of the
women are engaged in the work and when tiredness prevail, there is a chance of falling sick
every time. In table 5.5(b) states 60 % of SHGs often fall sick because of improper nutritional
diet, whereas 20% of SHGs says they are healthy because they eat enough food to fill their
stomach.
Table 5.5(b) Women falling sick all the time
S.no Response No. of SHGs Percentage of SHGs (%)
1 Agree 60 60%
2 Neutral 20 20%
3 Disagree 20 20%
4 Total 100 100% SOURCE: Primary data, 2015
Figure 5.5(c) depicts 72% of SHGs have paleness of skin and yellowness of eyes. It is one of
the symptoms mild Anaemia. 5% of SHGs do not have paleness of skin because of the proper
eating habits and intake of nutritious food.

7%
72%
16%5%
Fig. 5.5(c) Paleness of Skin in Women
Strongly agreeAgreeNeutralDisagree
SOURCE: Primary data, 2015
5.6 Prevalence of Anaemia in Pregnant women and Lactating Mothers
In this study certain indicators were used to identify Anaemia in pregnant women and
lactating mothers. In the figure 5.6(a) states 74% of the women are exposed to various
infections such as skin infections, urinal infections and allergies.
SOURCE: Primary data, 2015
As discussed above, similarly malarial infection is also one type of infection which leads to
repeated attack of fever. In the figure 5.6(b) given below states 78% of SHGs never suffered
from any malarial attack but only 6% of SHGs agreed that they have been suffering from
repeated attack of malaria.
12%
74%
13%
1%
Fig. 5.6(a) Women Exposed to Infections
Strongly agreeAgreeNeutralDisagree

Agree Neutral Disagree Strongly Disagree
0%
20%
40%
60%
80%
6%15%
78%
1%
Fig. 5.6(b) Prevalence of Malarial At -tack
Prevalence of Malarial at -tack
SOURCE: Primary data, 2015
From the table 5.6(c) states the prevalence of Anaemia in pregnant women and lactating
mothers. 83 SHGs agreed that during pregnancy and lactating period they feel fatigue and at
this most of the women are at vulnerable stage.
Table 5.6(c) Prevalence of Anaemia in Pregnant and lactating women
S. No Response Women feeling
weak during
pregnancy
Women feeling
weak during
lactating period
1 Strongly agree 14 17
2 Agree 83 83
3 Neutral 1 0
4 Disagree 2 0
5 Total 100 100 SOURCE: Primary data, 2015
In the figure 5.6(d) depicts that 44 % of women face irregular menstruation cycle. This
happens when hemoglobin level is low due to which irregularity of menstruation cycle and
this leads to lot of blood loss and anaemic but only 40% of women disagreed.
The data collected from Integrated Child Development Service and State Health Society
Bihar, observed out that 98/1000 women are suffering from mild Anaemia and most of cases
has not been recorded yet. There have been some severe anaemic cases especially among
pregnant women.

3%
44%
13%
40%
Fig. 5.6(d) Women Facing Irregu-lar Menstruation Cycle
Strongly agreeAgreeNeutralDisagree
SOURCE: Primary data, 2015
Figure 5.6 (e) states 48% of women face blood loss during delivery of baby. In the urban
slums, women mostly prefer delivery at home and without proper training sometimes they do
the process which leads to mishap cases. 21% of women do no face blood loss because they
prefer institution delivery which much safer for the baby and the mother.
48%
31%
21%
Fig. 5.6(e) Women Facing Blood Loss During Delivery
AgreeNeutralDisagree
SOURCE: Primary data, 2015
5.7 Awareness Level of SHG
When the SHG women were surveyed, it was observed 49% of SHGs were unaware about
the Anaemia and its causes and 52% of SHGs were not aware about the iron folic acid (IFA)
tablets which are available in free. This IFA tablet helps to recover the low blood count level
in the body and prevent Anaemia. Only 26% of SHGs were aware about the Anaemia but not
its causes and symptoms and 30% of women heard about IFA tablets as Anganwadis provide
this tablets in free.

Strongly Agree
Agree Neutral disagree Strongly Disagree
0%
10%
20%
30%
40%
50%
60%
24%
49%
1%
26%
0%
12%
52%
3%
30%
3%
women unaware about Anaemiawomen unaware about Iron Folic Tablets
Figure 5.7 Indicators showing the awareness level of SHGs SOURCE: Primary data, 2015
From the table 5.7 depicts that 54% of SHGs agreed that drinking milk can provide the
strength to the body to do the daily routine work. But during the study it was observed that
most of the women cannot afford milk because of low income.
Table 5.7 Drinking of milk solves health issues
S.no Response No. of SHGs Percentage of SHGs (%)1 Strongly Agree 3 3%2 Agree 54 54%3 Neutral 38 38%4 Disagree 5 5%5 Total 100 100%
SOURCE: Primary data, 2015
5.8 Government Interventions to Fight Anaemia
Government of India have been playing a major role for the development of health of the
women and child. As Anaemia is most common disease, Government came out with various
schemes and health care facilities. In the figure 5.8(a) states that 14% of SHG get IFA
through Anganwadi but 47% of SHG disagreed that they do not get IFA tablets from
Angawadi.

Strongly agree
Agree Neutral Disagree Strongly disagree
0%5%
10%15%20%25%30%35%40%45%50%
2%
14%
28%
47%
9%
Fig. 5.8(a) Availability of IFA in An-ganwadis
Availability of IFA in Anganwadis
SOURCE: Primary data, 2015
When survey was done in Anganwadis, it was observed that IFA tablets were not available to
them. It is the Integrated Child Development Service (ICDS) centre supplies these tablets to
the Anganwadis. But they had stopped supplying these tablets only ASHA worker can
provide IFA.
Neutral Disagree Strongly Disagree
0
10
20
30
40
50
60
Fig. 5.8(b) Government Hospitals Provie IFA Tablets
Government hospitals provie IFA tablets
SOURCE: Primary data, 2015
In the figure 5.8(b) depicts that 93% of SHGs understood the importance of immunization
during the pregnancy. Most of the pregnant women get immunization on time to prevent from
various infections.
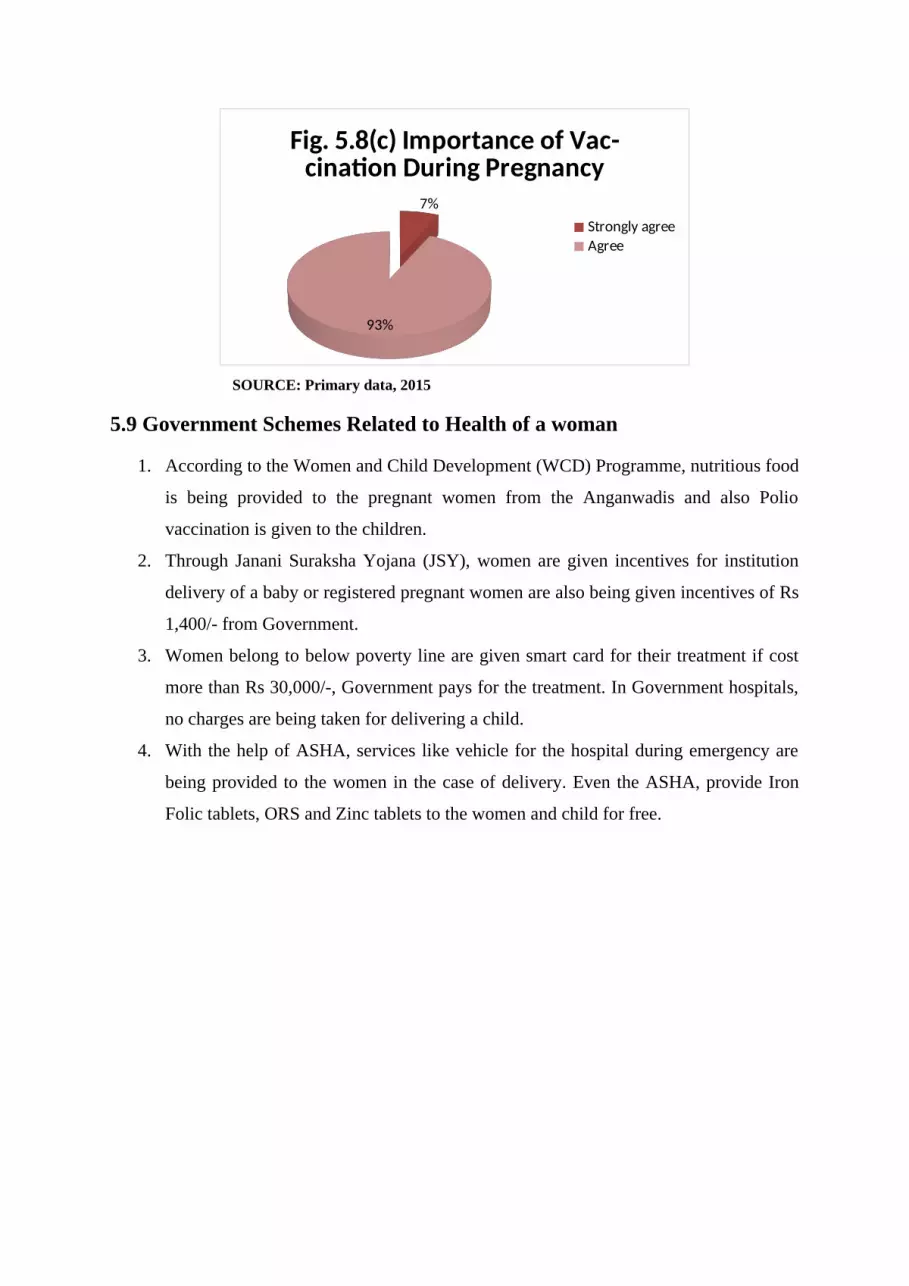
7%
93%
Fig. 5.8(c) Importance of Vac-cination During Pregnancy
Strongly agreeAgree
SOURCE: Primary data, 2015
5.9 Government Schemes Related to Health of a woman
1. According to the Women and Child Development (WCD) Programme, nutritious food
is being provided to the pregnant women from the Anganwadis and also Polio
vaccination is given to the children.
2. Through Janani Suraksha Yojana (JSY), women are given incentives for institution
delivery of a baby or registered pregnant women are also being given incentives of Rs
1,400/- from Government.
3. Women belong to below poverty line are given smart card for their treatment if cost
more than Rs 30,000/-, Government pays for the treatment. In Government hospitals,
no charges are being taken for delivering a child.
4. With the help of ASHA, services like vehicle for the hospital during emergency are
being provided to the women in the case of delivery. Even the ASHA, provide Iron
Folic tablets, ORS and Zinc tablets to the women and child for free.

CHAPTER 6
FINDINGS AND RECOMMENDATIONS
6.0 Findings
1. The target area of the study was 100 SHGs in the urban slums of Motihari, Bihar.
Out of 174 SHGs, 100 SHGs were selected as a sample size covering 18 wards.
2. There are 794 SHG members in which 474 are below poverty line and 320 are
above poverty line.
3. As they belong to low income family, availability of nutritious food is
unaffordable. 75 SHGs agreed that they do not get nutritious food every day,
whereas 14 SHGs disagreed because they might belong to Above Poverty level.
4. Almost 69% of the SHG women do not get sufficient food to eat because of the
customs they have to follow or they all are working women earning for their
family.
5. 60 % of SHGs often fall sick because of improper nutritional diet, whereas 20% of
SHGs says they are healthy because they eat enough food to fill their stomach.
6. 74% of the women are exposed to various infections such as skin infections,
urinal infections and allergies.
7. 78 SHGs never suffered from any malarial attack but only 6 SHGs agreed that they
have been suffering from repeated attack of malaria.
8. The prevalence of Anaemia in pregnant women and lactating mothers. 83 SHGs
agreed that during pregnancy and lactating period they feel fatigue and at this most
of the women are at vulnerable stage.

9. In the urban slums, women mostly prefer delivery at home and without proper
training sometimes they do the process which leads to mishap cases. 21% of
women do no face blood loss because they prefer institution delivery which much
safer for the baby and the mother.
10. Only 26% of SHGs were aware about the Anaemia but not its causes and
symptoms and 30% of women heard about IFA tablets as Anganwadis provide this
tablets in free.
11. 14% of SHG get IFA through Anganwadi but 47% of SHG disagreed that they do
not get IFA tablets from Angawadi.
12. 93% of SHGs understood the importance of immunization during the pregnancy.
Most of the pregnant women get immunization on time to prevent from various
infections.
6.1 Recommendations
1. There should be a regular monitoring of the Anganwadis functioning in the
Motihari.
2. As these women belong to poor family, there should consession in the price of
medicines they buy for the treatment.
3. There should be awareness health campaign about health and hygiene of the
women.
4. There should be a training programmes for SHG women about hygiene
practices and also a training session which provides basic knowledge about the
emergency cases during pregnancy.

6.2 ConclusionTo sum up, this study was conducted to measure the awareness level of women about
anaemia and its causes. Through the field survey, it was observed that most women were
unaware about anaemia. They understood the disease of having low level of blood count and
they do not know its severe consequences. The study was also conducted to identify the
anaemia cases in the pregnant and lactating mothers, it was observed that most of the women
are anaemic but a mild one. Though iron folic acid tablets are given to them by the
Government but they are ignorant about its importance. Thirdly, a study was conducted on
the programmes and interventions running by the Government for the women and children
development and it was observed that these schemes an programmes are running successfully
but women are unaware about it.
During the field survey, it was observed that the SHG women have not taken any steps to
eradicate anaemia in women. Though these women are capable but they need a capacity
building. The quality of groups is quite low in the urban slums and even they are not
punctual in conducting the meetings. Overall, the status of the SHG movement in the town
appears to be aptly reflected by the monthly savings of the group.

BIBLIOGRAPHY
Agarwal, D. K., Agarwal, K. N. & Tripathi, A. M. (1987) Nutritional status in rural pregnant women of Bihar and Uttar Pradesh. Ind. Pediatr. 24:119-125.
Kaveri Gill (2009),’a Primary Evaluation of Service Delivery under National Rural Health Mission (NRHM): Findings from a Study in Andhra Pradesh, Uttar Pradesh, Bihar and Rajasthan, Working Paper 1/2009.
United Nation Development Program, India, Human Development Report. New Delhi, India: Oxford University Press: 2011.
Acharya, A. (November 13, 2014) 'Evaluating a large scale community based intervention to improve pregnancy and new born health among rural poor in India', American Journal of Public Health .
Reddy, Raja. K (May 2005) ‘A study on Self Help Group (SHG)- Bank Linkage in Andhra Pradesh’, APMAS English Publications, Page: 1-3.
Reference
http://www.rchiips.org/nfhs/bihar_report.shtml retrieved on 20/05/2015 https://data.gov.in/keywords/district-level-household-and-facility-surveydlhs retrieved
on 22/05/2015 http://www.statehealthsocietybihar.org/ retrieved on 28/05/2015 http://www.gov.bih.nic.in/Profile/default.htm retrieved on 28/05/2015 http://gov.bih.nic.in/Profile/districts/eastchamparan.htm retrieved on 29/05/2015 www.apmas.org retrieved on 6/06/2015
ANNEXURESAnnexure-I (Schedule)
1. Women feel tired after working a day long.

(i) Strongly agree(ii) Agree(iii) Neutral(iv) Disagree(v) Strongly disagree
2. Most of the time women work empty stomach.(i) Strongly agree(ii) Agree(iii) Neutral(iv) Disagree(v) Strongly disagree
3. Women feel numbness or coldness in their hand and feet.(i) Strongly agree(ii) Agree(iii) Neutral(iv) Disagree(v) Strongly disagree
4. Women often fell sick within a month.(i) Strongly agree(ii) Agree(iii) Neutral(iv) Disagree(v) Strongly disagree
5. Women have pale skin and yellow eyes.(i) Strongly agree(ii) Agree(iii) Neutral(iv) Disagree(v) Strongly disagree
6. Women weren’t aware of Anaemia.(i) Strongly agree(ii) Agree(iii) Neutral(iv) Disagree(v) Strongly disagree
7. Till now no one had told them about Anaemia.(i) Strongly agree(ii) Agree(iii) Neutral(iv) disagree(v) strongly disagree
8. Women intake sufficient food after working whole day.(i) Strongly agree

(ii) Agree(iii) Neutral(iv) Disagree(v) Strongly disagree
9. Women get repeated attack of malaria(i) Strongly agree(ii) Agree(iii) Neutral(iv) Disagree(v) Strongly disagree
10. Women do not get nutritious food to eat(i) Strongly agree(ii) Agree(iii) Neutral(iv) Disagree(v) Strongly disagree
11. Intake of protein rich food can increase their blood level in the body(i) Strongly agree(ii) agree(iii) neutral(iv) disagree(v) strongly disgree
12. Women prefer Private hospital for their health check up(i) Strongly agree(ii) Agree(iii) Neutral(iv) Disagree(v) Strongly disagree
13. According to women, drinking milk can solve half of their health problem(i) Strongly agree(ii) Agree(iii) Neutral(iv) Disagree(v) Strongly disagree
14. Women were not aware of iron folic tablets.(i) Strongly agree(ii) Agree(iii) Neutral(iv) Disagree(v) Strongly disagree
15. Iron folic tablets are available in Anganbadi

(i) Strongly agree(ii) Agree(iii) Neutral(iv) Disagree(v) Strongly disagree
16. Anganbadi provide iron folic tablets to all the women(i) Strongly agree(ii) Agree(iii) Neutral(iv) Disagree(v) Strongly disagree
17. Government hospital provide iron folic tablets to the women(i) Strongly agree(ii) Agree(iii) Neutral(iv) Disagree(v) Strongly disagree
18. Women have been told that they are anemic.(i) Strongly agree(ii) Agree(iii) Neutral(iv) Disagree(v) Strongly agree
19. According to women, lack of nutritious food leads to anemia.(i) Strongly agree(ii) Agree(iii) Neutral(iv) Disagree(v) Strongly disagree
20. Women feel weak during their pregnancy(i) Strongly agree(ii) Agree(iii) Neutral(iv) Disagree(v) Strongly disagree
21. Women feel weak during their lactating period(i) Strongly agree(ii) Agree(iii) Neutral(iv) Disagree

(v) Strongly disagree22. Women have irregular menstruation cycle.
(i) Strongly agree(ii) Agree(iii) Neutral(iv) Disagree(v) Strongly disagree
23. Women face lot of blood loss during delivery.(i) Strongly agree(ii) Agree(iii) Neutral(iv) Disagree(v) Strongly disagree
24. Pregnant women intake iron folic acids when they are prescribed to take.(i) Strongly agree(ii) Agree(iii) Neutral(iv) Disagree(v) Strongly disagree
Annexure-II: Details about the slums of Motihari
S.no Name of the slumward no.
1 Ambedkar nagar 32 Badhai tola 183 Badka/nyka mathiya turha toli 174 Bajapatti 65 Balua bazar 286 Balua gopalpur harijan basti 287 Begumpur Belkhana 358 Belisarai 299 Belwanwa machua toli 2210 Bengali colony 2711 Chamarpatti, Chhatauni 1812 Chhatauni, muskim and brahman tola 1713 Chota bariyarpur 3814 Dewan toli 3315 Dih 1816 Dompatti 18

17 Gopalpur Mallah toli 3418 Harijan basti 1219 Indira nagar 1920 Kaanhi tola 3721 Khushbu nagar 1222 Kulahwara tola 123 Mahmud nagar 124 Maisthaan 1825 Mathiya dih harijan basti 1726 Mathiya dih noniya toli 1727 Mestar toli 3428 Musalpatti 1829 Nala basti raod 3430 Nehru stadium 2131 Paswan tola, Chhatauni 17
Annexure-III: SHG and total members
s.no SHGs name total members1 ansh samvardhan 82 baby samvardhan 73 bahu samvardhan 74 bajrang samvardhan 75 bandhan 106 bihar samvardhan 77 chameli samvardhan 78 champa samvardhan 69 chand samvardhan 710 chandan samvardhan 711 chandrama 8
12chandrama samvardhan 7
13 durga samvardhan 714 eid samvardhan 715 ekta 1016 ganesh 917 ganesh samvardhan 918 ganga 1019 ganga samvardhan 8

20 geeta samvardhan 721 gopal 822 gulab 823 gulab samvardhan 724 gulab samvardhan 1025 gulsan samvardhan 1026 jagorehna 7
27jay ambey
samvardhan 728 jay mata samvardhan 829 jeet samvardhan 730 jyoti samvardhan 1031 kajal 832 kamal samvardhan 733 kamal samvardhan 734 kamal samvardhan 935 kangan samvardhan 736 kanhaiya 1037 khushbu samvardhan 738 khushi samvardhan 839 kiran 740 kiran samvardhan 1041 kiran samvardhan 2 1242 laxman samvardhan 743 laxmi samvardhan 744 maa gauri samvardhan 1045 ma samvardhan 746 maa saraswati 847 mahadev samvardhan 748 mala 949 maszid samvardhan 850 maya samvardhan 851 meena samvardhan 1152 milan samvardhan 1053 nadi samvardhan 754 nagar samvardhan 755 payal samvardhan 856 phool 757 phool samvardhan 1058 phul samvardhan 759 prakash samvardhan 860 prity samvardhan 761 radha 762 raja 7

63 raja samvardhan 864 rakhi samvardhan 765 ram samvardhan 766 rani samvardhan 867 roshni 768 roshni samvardhan 1069 sahar samvardhan 770 saheli samvardhan 771 sahyog samvardhan 872 sakhi samvardhan 773 saloni samvardhan 1074 samsha samvardhan 775 saraswati 876 saraswati samvardhan 777 savitri samvardhan 878 seva samvardhan 779 shakti samvardhan 880 shankar samvardhan 781 shiv samvardhan 1082 shivani samvardhan 783 shivguru samvardhan 884 sita samvardhan 1185 tara samvardhan 886 ujala samvardhan 887 veena samvardhan 1088 ram samvardhan 789 rakhi samvardhan 790 radha 791 nagar samvardhan 792 maa samvardhan 993 kiran samvardhan 1094 kiran samvardhan 1295 khusbun samvardhan 996 khushbu samvardhan 897 kamal samvardhan 998 kamal samvardhan 799 chameli samvardhan 7100 champa samvardhan 7

Annexure-IV (Photographs)

Figure-1 Focus group discussion with SHG members of Badkanyka mathiya turha toli slum.
Figure-2 SHG members conducting monthly meeting
Annexure-V: Map of Bihar (SPUR projects)

SPUR towns
Non SPUR towns
Motihari district





























