Embed Size (px)
Citation preview

Science in Context 21(2), 201–227 (2008). Copyright C© Cambridge University Pressdoi:10.1017/S0269889708001695 Printed in the United Kingdom
The Administrative Stabilization of Vaccines: Regulatingthe Diphtheria Antitoxin in France and Germany,1894–1900
Volker Hess
Institute for the History of Medicine, Charite Berlin
Argument
It is well known that the development of a diphtheria anti-toxin serum evolved in a competitiverace between two groups of researchers, one affiliated with Emil Behring in Berlin and Marburg,and another affiliated with Emile Roux in Paris. Proceeding on the basis of different theoreticalassumptions and experimental practices, the two groups developed a therapeutic serum almostsimultaneously. But the standardized substance they developed took on very different forms inthe two countries. In Germany the new serum was marketed in the private sphere and subjectedto state regulations, becoming a kind of prototype of industrial medications. In France, however,the same substance was marketed as a gift of science to humanity and distributed through thecommunal health care system. This article demonstrates how a new medication emergedfrom the efforts to produce, market, regulate, distribute, and apply it in the two respectivecountries. It attributes the difference to the negotiations between the respective actors (scientists,industrialists, politicians, officers, and the public) and institutions (firms, academies, privateand public institutes, legislative bodies, professional corporations). I develop this argument onthree different levels: First, I stress the importance of the institutional foundations of serumproduction; second, I illustrate the decisive role played by existing “ways of regulating” in therapid development of new legal statutes; and third, I describe the consequences that flowed fromthe respective administrative organization of marketing and dissemination. In sum, I explorehow an experimental object was transformed into an object of the public health system andstabilized by administrative means.
At the eighth International Congress of Hygiene in Budapest in early September1894, Emile Roux described the successful results of experiments using the diphtheria-antitoxin serum that had been developed at the Pasteur Institute. Likewise in Septemberof 1894, Emil Behring presented his results to the Society of German Natural Scientistsand Physicians in Vienna. The two approaches differed neither in principle, nor intheir procedure. The race to develop a diphtheria serum had come to a very similarconclusion, but had evolved out of two very different experimental systems. AfterBehring published his observations on the favorable therapeutic effects of blood serumdrawn from immunized guinea pigs in early 1890 (Behring and Kitasato 1890), the

202 Volker Hess
research group working around Emile Roux reoriented its research. Up until that time,the group working at the Institute Pasteur had pursued the development of an activeinoculation and had experimented with attenuated cultures of the diphtheria agent(Mendelsohn 1996, chap. 5), stressing the importance of environmental factors and thePasteurian concept of terrain. Adopting the experimental system used in Berlin, Frenchresearchers quickly achieved success and developed a stable system of equestrian serumproduction. In early 1894 the Hopital des Enfants Malades could begin the first largeclinical trials, so that the French research group actually moved ahead of their Germancounterparts (Weindling 1991). When both the German and French press finallyhailed their national heroes in the fall of 1894, the different experimental cultures hadbeen largely transformed into a – for the most part – common production process(see Jonathan Simon’s contribution in this volume). There was hardly any differencebetween the measures of standardization used to stabilize and close the experimentalsystem, and those used to scale up to industrial production levels. Efforts at industrialexploitation appeared, therefore, to have largely blurred the distinction between Frenchmicrobiology and German bacteriology (Mendelsohn 1996). The production processesin Garches and Hoechst were virtually identical. Likewise, differences in testingprocedures were minor: the weight of the guinea pigs varied slightly because Frenchresearchers were in principle sceptical of tests on living animals (see Ulrike Kloppel’scontribution in this volume). And like the German serum, the French serum was alsoable to rescue a sick child from the dangers of diphtheria quickly and reliably. Indeed,the “natural logic” of immunization and the industrial drive for uniformity appear tohave eliminated every variation between the once distinct experimental cultures.
Yet if one considers not just the therapeutic effectiveness of the diphtheria antitoxinserum, but also what was done with the new therapy, it quickly emerges that, in spiteof the serums’ apparent similarities, two very different products were introduced ondifferent sides of the river Rhine. In the German empire, the industrial component ofthe serum was not limited to the production process; in many ways, diphtheria antitoxinserum was labeled as a pharmaceutical specialty: First, diphtheria antitoxin serum couldbe purchased on the open market, even though dispensation was channeled throughpharmacies. Second, multiple producers developed their own brand identities andcompeted openly for market share. Third, diphtheria antitoxin serum became a kindof prototype for modern medicines, its procedural controls, production documentation,use of serial numbers, and continuous batch-testing anticipating essential elements ofmodern drug laws. In effect, diphtheria antitoxin serum became the model for a newkind of drug oversight.
In the French case, however, diphtheria antitoxin serum was established as a serviceof the public health system: First, the serum was not distributed through pre-existingchannels for marketing drugs, but instead through an institution created especially forthis purpose, the Service antidiphterique. Second, the production of diphtheria antitoxinserum was, for the most part, immune from market forces and financed through annualcontributions from various communities and regions. Third, the state’s role was reduced

Administrative Stabilization of Vaccines in France and Germany, 1894–1900 203
to formal certification of the producer. Scientists were more or less given responsibilityfor overseeing the new therapy. In short: if the German diphtheria antitoxin serum wasa prototypical product of the pharmaceutical industry based on the rules of a capitalistmarket economy, then the French counterpart embodied the bounty of humanitarianand scientific accomplishments that were institutionalized and expanded upon as partof the civic public health service.
This article demonstrates that this distinction was chiefly the result of bringingdiphtheria antitoxin serum to the medical marketplace as a pharmaceutical product. Inthat process, as I will argue first, the institutional anchorage of the serum productionwas crucial. Second, public and state oversight of the drugs played an important role,given that the status of medications was regulated by legal statute. Third, the marketingand distribution of approved medicines – that is to say, the path and mode of theirsupply – was of considerable importance because they configured the institutional,professional, and day-to-day contact with diphtheria antitoxin serum. Of course,in practice these three aspects cannot be clearly differentiated from one another.Rather, the regulation of medications was inextricably linked with their productionsites and, in turn, their distribution was affected by important structural aspects ofpublic health systems. Hence, in this article I will subsume all three aspects under theterm administrative stabilization, while recognizing that they each represented differentadministrative procedures that drew on the same material in shaping different objects.
If the reasoning behind the decision-making process and administrative frameworkclearly differed in France and Germany, it was in part because of the historical dramathat pressured medical officials to resort to existing models. But as the first sectionof this article shows, those models were not based on past experience with vaccines,but rather with regulations governing medicines. Therefore, the first question to beanswered is why medical officials believed it was necessary to intervene in this way. Inthe second part of this article I will examine the temporal dynamics of events in orderto illustrate the pressures that politicians and bureaucrats faced. In the third section Iwill compare the regulative schemes that were developed and adopted by bureaucratsin France and Germany. And finally, I will show that the form and qualities attributedto diphtheria antitoxin serum in the marketplace depended in crucial ways upon thechoreography and implementation of these stabilizing schemes.
1. Establishing Precedence: The Diphtheria Antitoxin Serum
After scientists announced their findings on diphtheria antitoxin serum in the fall of1894, medical officials began a hectic race to deal with the consequences of the newdiscovery. In Germany, officials from state medical agencies and the Prussian Instituteof Infectious Diseases met on 24 October to discuss how to implement the procedure.By February of 1895 and after only a few meetings, they established a legal frameworkthat took effect on 1 April of the same year. The response in France was equally

204 Volker Hess
swift: By mid-October a delegation from the Academie de Medecine had visited thelaboratories in the Rue Dutot on behalf of the ministry of the interior and, after briefconsultations within the French government, recommended complete liberalization ofthe production, marketing, and sale of the serum (Ministere de l’Interieur 1896, 4).Parliament reacted equally swiftly, deliberating draft legislation in its session on 26November 1894 before voting it into law after long discussions on 25 April 1895.
The haste with which state medical officials on both sides of the Rhine set aboutimplementing regulations and laws governing the new vaccination method is surprising.Diphtheria antitoxin serum was certainly not the first substance derived from animals tobe used to fight infectious diseases. On the contrary, by this time there existed more thana century of experience inoculating for cow-pox. By the end of the eighteenth century,Jenner’s method of vaccination had been developed into a stable technique that wasintroduced into many medical codes in western and central Europe, thereby attaininga secure place within the traditional regimes of public health services (Dixon 1962;Huerkamp 1985). Vaccination also provided the backdrop for Pasteur’s astonishingsuccess. He himself emphasized that his sensational vaccination against anthrax in1881 was an artificial vaccine that differed from Jenner’s serum (Geison 1995, 172).Hence, the method developed by Emil Behring and others in the early 1890s (i.e.vaccination using substances derived from animal fluids) was not a fundamentally newprocedure, even though it was based on a new model of transmission of an antitoxicor “antifermentative” principle (Behring 1890).
Consequently, other explanations are required to explain the pressing need thatmedical officials saw for new regulations. Some of those explanations have beenexplored in other chapters of this volume on the discovery and production of diphtheriaantitoxin serum: First, diphtheria antitoxin serum was an artificial product. Although itmight be considered a “natural substance” derived from the blood of specially treatedanimals, it was nevertheless an especially fragile object. As an experimental object(see Ulrike Kloppel’s paper in this volume) it had been just as difficult to stabilizeas the procedure by which it was transformed into an industrial object (see JonathanSimon’s paper in this volume). Thus, unlike traditional vaccinations that essentiallymimicked nature, diphtheria antitoxin serum was a child of the laboratory. The skillsand tacit knowledge needed to produce it situated it closer to new, industrially producedmedicines. Yet if one describes diphtheria antitoxin serum as an artificial product, thenit defies classification within the framework of new vaccines. Although causing muchpanic as it spread, rabies was an uncommon illness; and vaccinations against it, althoughthey too generated much concern, remained very rare, limited to a few dozen cases.On the other hand, anthrax and chicken-pox were veterinary problems that lay outsidethe scope of public health-care administration. Diphtheria however, was another caseentirely. Second, at the end of the nineteenth century, diphtheria was one of the mostwidespread infectious diseases. Diphtheria and croup were ranked as the fifth mostcommon causes of death. Together they comprised a large portion of infant (7 per1,000) and child (2.5 per 1,000) mortality, and eighty per cent of all diphtheria patients

Administrative Stabilization of Vaccines in France and Germany, 1894–1900 205
were under ten years of age.1 Although rabies vaccines were prototypes for a new kindof vaccination, their status remained exceptional and marginal; with the introduction ofdiphtheria antitoxin serum, however, the prospect of an artificially produced vaccinebeing adopted into the regulatory regime emerged. Early clinical trials had alreadyraised hopes of widespread application (Behring 1893). This implied, third, a whollydifferent order of magnitude of dispensation. Whereas it was certainly possible to travelto Pasteur in Paris after being bitten by a rabid dog, the dissemination of diphtheriaantitoxin serum via hospitals and practicing physicians involved large-scale planningand organization that was beyond the means of a single, centralized dispensary. Andto ensure the safe handling of the vaccine, one could not rely on local oversight andcontrol. In addition, as we shall see, serum production in both the German Empireand France was never concentrated in one place.
But it seems to me that a fourth reason was ultimately most decisive: diphtheriaantitoxin serum claimed to have therapeutic effects. In this regard it differedcategorically from existing forms of vaccination that offered only prophylacticprotection.2 Even Pasteur’s fabulous treatment of rabies had not deviated from thetemplate of vaccination, because it worked only in the interval between the infectionand actual outbreak of the fatal disease. By contrast, all the protagonists of diphtheriaantitoxin serum insisted that it was a therapeutic treatment. And that had importantconsequences: in strictly formal terms, as a remedy diphtheria antitoxin serum belongedin the class of internal therapeutica, i.e. medications. Whereas according to the logic ofadministrative rationality it would have required further justification for a prophylacticvaccination to be subjected to official oversight, in the case of medications suchoversight was long-established practice. Conversely and by the same logic, exceptionaljustification would have been necessary for diphtheria antitoxin serum not to besubjected to official oversight.
The traditional public health system did not regulate vaccinations, but it did provideseveral mechanisms to ensure that medications were safe. These mechanisms were allmore or less organized around pharmacies. On the one hand, pharmacists were requiredto fill doctors’ prescriptions with due care; and for that, early modern medical law hadgranted them extensive privileges. On the other hand, all production and sale outsideof pharmacies was prohibited. This was especially true for so-called secret remedies.The methods used in their production lay outside the public domain of the materiamedica. In addition, medical officials used pharmacopoeia to stipulate which kinds ofmedicine pharmacists were required to have in stock and how they were to be madeand stored. The corporate privileges of pharmacists were never seriously challengedby industrialization. On the contrary, the role of pharmacists as key elements in the
1 Between 1891 and 1893 approximately 36,000 children under the age of five died of diphtheria in Prussia(Baginski 1913, 336). In France the mortality rate was 64 per 100,000.2 The French law of 25 April 1895 explicitly precluded Jenner’s vaccination.

206 Volker Hess
regulation of medications was strengthened as one can see by the changes in thepharmacopoeia in the nineteenth century (Hickel 1973).
As part of these developments, pharmacists became increasingly responsible for thequality control of medications. The Prussian Arzneibuch set down extensive guidelinesfor chemical analysis and testing. Even the emergence of factory-made medicinesdid not fundamentally alter these principles of state medical regulation. Whereaspharmacists’ monopoly over the production process was gradually rolled back, theywere increasingly responsible for ensuring the quality and purity of factory madeingredients and even medicines. In principle, therefore, pharmacists were requiredto subject the batches of manufactured ingredients received from Hoechst, Bayer, orother manufacturers to chemical analysis before selling them. The great importancegiven to regulating the drugs market is evidenced by the fact that the imperial decreeon the “marketing of drugs” was among the very first decrees issued by the imperialgovernment after unification in 1871 (later revisions appeared in 1875, 1890, and 1901).They regulated the responsibilities of pharmacists, listing in two special appendixes allformulas (Appendix A) as well as all drugs and chemical substances (Appendix B) thatpharmacists were permitted to market and sell (Ernst 1975). These included medicinesthat had been industrially or proto-industrially produced and that were marketedthrough pharmacies. Dispensing “powerful drugs” was subjected to further regulationsin Prussia in 1878 – and in the Empire after 1891 – that drew up lists of all prescriptiondrugs und formulas.3 With that, the definition of what counted as a medicine dependedessentially upon whether it appeared on the list drawn up according to an Imperialdecree; and once classed as a prescription drug, the therapeutic character of the formulawas irrevocably fixed.
In fact, it was the status of the medicine that caused formal problems for medicalofficials in Germany. In its very first deliberations, the Imperial Health Officerecognized that because carbolic acid had been added as a supplement, diphtheriaantitoxin serum might well be classed as a “compound” according to Appendix A,thus prohibiting its sale outside pharmacies. However once industry succeeded inmarketing the serum without using preservatives, this problem vanished. Nor did thisruling cover the case of diphtheria antitoxin serum being used to immunize patients,i.e. its prophylactic application to the relatives of sick patients. Ministry of Interiorofficials therefore suggested that diphtheria antitoxin serum be classed as a “powerful
3 The inclusion of factory-made medicines in this system would be a worthy topic of further inquiry. On theone hand, the pharmaceutical industry wanted their formulas included among the medicines that pharmacistswere required to stock. On the other hand, however, they naturally tried to prevent them from being classedas a prescription drug. As early as 1882 the pharmacopoeia included the first industrially produced medicinesin its extensive list of common pharmaceuticals, including recommended dosages. In 1887 Prussia established astanding commission charged with revising the Arzneibuch, and in 1901 that commission was reconstitutedas a subcommittee of the Reichsgesundheitsrat in the Imperial Health Office. From 1891 onward, leadingrepresentatives of the German pharmaceutical industry sat on the commission as advisors on the inclusionof industrially produced medicines in the Arzneibuch (Hickel 1977; Wimmer 1994, 47–67).

Administrative Stabilization of Vaccines in France and Germany, 1894–1900 207
drug” that required a physician’s prescription.4 But these formal rules circumvented thequestion of how new cures could be integrated into the traditional system regulatingthe production and sale of medicines. Given the delicate procedures that were requiredto evaluate the medicine (see Axel Huntelmann’s paper in this volume), strategies thathad been developed to test other industrially produced medicines seemed impractical,because one would have had to burden pharmacists with the responsibility of chemicallyanalyzing compounds and their purity.
But Prussian medical officials had yet another method for ensuring drug safetythat dated back to the early nineteenth century: licensing as a secret remedy (Hess2007). More or less industrially or proto-industrially produced medicines were includedamong the secret remedies, although unlike the factory-made medicines their formulasand compounds were known only to their producers. Upon certification, secretremedies too were permitted to be sold only in pharmacies, although because theirrecipes were unknown, the pharmacist did not test their quality. Instead, Prussianofficials made the license to sell secret remedies contingent upon evidence that theremedy was therapeutically new, harmless, and effective. This evidence was providednot by third party experts, but by official state experts that tested both the compositionand the clinical usefulness of the formula. As we shall see, this model of testing secretremedies served as a template for the procedure developed by German medical officialsto test diphtheria antitoxin serum.
Diphtheria antitoxin serum also encountered a legal loop-hole in France. UnlikeGermany, the French state observed a laissez-faire policy when it came to marketingdrugs. The revolutionary law of 21 Germinal in year 11 (11 April 1803) remained inforce into the 1940s. It both confirmed pharmacists’ privilege as the sole producer anddistributor of medicines and forbade any marketing and selling of secret remedies –a proscription that in spite of the growth in the industrial production of medications(specialites) remained in force, at least formally, well into the twentieth century(Chauveau 2006). Additional provisions governed the evaluation of new medicationsby scholarly societies (Kibleur 1999), so that control and oversight lay in large part inthe hands of professional organizations. According to a decree of 20 December 1820,upon its reestablishment the Academie de Medecine assumed sole responsibility forthe certification of new therapies. A further decree of 3 May 1850 abolished eventhe strictly formal confirmation of the certification by the Ministry of the Interior.Although the physicians’ organization was a corporate institution funded by the Frenchstate, in regulating specialties it retained a high degree of autonomy (Weisz 1995): itlaid down the procedural rules, determined the criteria for passing judgment, stipulatedthe standards to be applied to scientific and practical testing and finally, in the event of a
4 Letter to the State Secretary of the Interior, 20 November 1894, including the minutes for the “Meetingconcerning diphtheria serum on 26 October 1894,” BA, R 86, No. 1846. The ensuing Imperial Order of 31December 1894 saw the diphtheria serum included as a “category B” medicine according to paragraph two ofthe Imperial Order of 27 January 1890.

208 Volker Hess
favorable decision by the general assembly, published the formula of the new medicinein the Bulletin de l’Academie (Ramsey 1994a). In general, publication of the formula wastantamount to formal recognition since the codex, i.e. the French equivalent to theGerman Arzneibuch, was rarely revised. It was not until an order of 13 July 1926 that adistinction was made between secret remedies and factory-made medicines. Accordingto that order, the latter was required to carry a label stating the active ingredient anddosage. The law of 11 September 1941 finally gave industrially produced medicationswell-defined legal status.5
In other words, French law made no distinction between secret remedies andindustrially produced medication. Neither were covered by code. The same was alsotrue for diphtheria antitoxin serum to the extent that it was considered a medicine.The corporation of French doctors, by its inspection of the production sites andits vote of the Seance on 15 October 1894, overwhelmingly sanctioned the newtherapy (Straus 1984). And this professional sanction persisted in spite of the factthat diphtheria antitoxin serum mirrored illegal secret remedies in so far as it could bemanufactured outside the framework of traditional modes of production in pharmacies.It is therefore by no means a paradox that the case of diphtheria antitoxin serum forcedFrench legislators to consider state licensing and testing of medicines for the first time(Chauveau 2004). But officials were left with little time for such deliberations.
2. Bottling the Genie
Roux’s lecture on the new therapy at the Hygiene conference in Budapest gave riseto unprecedented press coverage in France. Newspapers reported on events almostdaily. A mere day after Roux had spoken, the newspaper Figaro trumpeted anothervictory by the Pasteur Institute in the “war against croup.” Figaro’s man in Budapest wasGaston Calmette (1858–1914), brother of the Pasteurian Albert Calmette (1863–1933).Gaston would himself later become director of the renowned French daily. Calmetteset the stage on which Roux’s discovery would play itself out: as an “oeuvre francaise,exclusivement francaise” in the service of science and humanity (Calmette 1894a). Aweek later, Figaro published another article on rates of cure in the paediatric hospitalin Paris (Anonymous 1894a). Finally, on September 20, Gaston Calmette launcheda fundraiser designed to secure financial backing for the new therapy: between fiveand six million Francs were needed to found a hospital dedicated to the treatment
5 To this day, some historians continue to argue that prohibiting patents on medicines slowed the industry’sdevelopment (i.e. Chauveau 1999). Imperial law in Germany did not protect drugs as such (Stoffschutz) and thisprobably helped rather than hindered the rise of the pharmaceutical industry. German law did, however, makeprovision for protecting the production process (Verfahrenschutz). But because these restrictions were often easyto circumvent, pharmaceutical companies resorted to cartels in order to protect the marketing of their products(Wimmer 1994).

Administrative Stabilization of Vaccines in France and Germany, 1894–1900 209
of diphtheria and other infectious diseases. With donations amounting to as little as30,000 Francs, the Pasteur Institute would be able to treat all children – not just thosein the two hospitals in Paris – using Roux’s method (Calmette 1894b).
The call for donations unleashed an enormous wave of public support. Donationsquickly surpassed 30,000 Francs, rising to more than 150,000 Francs in just a few weeks.By the end of the following year, the institute boasted donations of exactly 998,309francs (AIP, No 9287). Donations were received not just from wealthy individuals who,by virtue of their social status, were obliged to contribute significant amounts of moneyto the cause. Countless small, even tiny donations were collected. Surviving recordsin the Pasteur Institute (Direction, 1888–1940) indicated that most donors contributedamounts between 10 and 150 Francs: The mayor of Eauze (Gers) sent 30 Francs, theMoniteur du Puy de Dome in Clermont-Ferrand collected 107,40 Francs, and the Parisianphysician Dr Regeard contributed 100 Francs following the successful treatment of hisson. As one of the driving forces behind the subscription, Figaro supported fund raisingwith constant reports in its pages (i.e. Daremberg 1894; Anonymous 1894b). At regularintervals, daily papers listed donors and their contributions, thus publicly celebratingthe generosity and humanity of the Republic and its citizens.
Not surprisingly therefore, public pressure on the Pasteur Institute was great. Thepolitical establishment added to the pressure by publicly praising the institute. And on 23October the French president Jean Casimir-Perrier (1847–1907) visited the pediatrichospital where the diphtheria wards were located and a day later the “laboratoirespecialement affecte a la serum” in the Rue Dutot. Not to be outdone, the Frenchgovernment granted the institute a large piece of property near Paris (Villeneuve-l’Etang) so that it could begin serum production on a mass scale. The 2nd Cuirassiers-Regiment donated thirty horses and the city of Paris provided an annual subsidy,so that by the end of October 1894 construction of L’annexe (or Garcher as it latercame to be known) could begin. The expansive plant included stalls for more thanone hundred horses and 3,500 laboratory animals, alongside the requisite laboratoriesfor the extraction and processing of the serum. Serum production began in earlyDecember of 1894 (AIP, No. 9372). Thus, in just a few months, the Pasteur Institutehad constructed an entire plant to produce serum on an industrial scale and increasedproduction from 1,500 doses between February and October 1894 to 50,000 dosesbetween October 1894 and February 1895 (AIP, No. 9265).
Such impressive numbers appeared to confirm the French model. Pasteur enjoyedexceptional success in rallying public support. In the wake of the sensational rabiesvaccine, formal subscriptions had raised some 2 million Francs, thereby establishingthe financial basis on which his private institute was founded (Pasteur 1888). Thedonations of French citizens had enabled the building of production facilities for theserum independent of state interests and because those facilities were dedicated solelyto science, promised to guarantee the well-being of the general public. The prospectof Services graduits, i.e. the free dispensation of diphtheria antitoxin serum to all sickand needy individuals, was both a tacit and expressly stated expectation of subscribers.

210 Volker Hess
Consequently, deliberations in the political senate proceeded on the assumption thatthe production, marketing, and quality control of diphtheria antitoxin serum would beensured by the Pasteur Institute. Although a private institute, its commitment to thepublic weal seemed to guarantee reliable, widespread distribution of the new vaccine.As a result, parliament focused chiefly on embedding the new therapy in the establishedregime of drug oversight. Proper oversight appeared to be assured by the demand thatthe serum’s production be supervised by a trained pharmacist.
Observers in Germany viewed the French model with a certain amount of envy.When officials in the Imperial Health Office began debating how to go aboutimplementing appropriate rules governing the production and use of the serum, Parisseemed to be the standard of choice. According to the minutes of their deliberations,the example set by Paris was praised as “the most fortuitous and in many other respectsthe most elegant solution to come out of France in recent times.” Officials wereunanimous in their praise for the idea of granting a research institute the sole right toproduce the serum and of “providing [the serum] to everyone free of cost” (BA, R86, 1646, Report of 24 October 1894). As Behring reported to his co-worker ErichWernicke in a letter of 24 October 1894, the main result of the meeting was to beginplanning a German Pasteur Institute.
But the stormy developments of the previous months had long since discreditedthis option. Behring had been in close contact with Hoechst since 1892 and Hoechstwas interested in developing an industrial production process for Behring’s discovery(Throm 1995, 47–50). The Ministry of Culture viewed this cooperation with thenascent pharmaceutical industry with favor.6 For his part, Behring supported researchto the tune of 10,000 Marks per year, just as Robert Koch’s state-supported tuberculosismedicine was being exposed as a “harmony of illusions” (Gradmann 2004). In a letterto Erich Wernicke dated 30 March 1892, however, Behring insisted that diphtheriaantitoxin serum was private property and therefore, after joining the Prussian Institutefor Infectious Diseases, continued his research work in a strictly private capacity so asto avoid his contractual obligations.7
This alliance between research and industry was not unusual. On the contrary,it was encouraged and supported by the state (Meinel 1992). Prussian ministries inparticular had an exclusive, cooperative relationship in mind that would facilitatebetter relations between industry and the state. For ministerial officials, whether ornot a prospective research institute would be funded by the state or by industry was of
6 Schering and Hoechst simply outgrew their status of craft producers. In both countries, many apothecarieswere established around the production of specialties, but at that time it was only in Germany that some weretransformed into pharmaceutical firms (Huhle-Kreutzer 1989).7 All employees of the Prussian Institute for Infectious Diseases were required to sign an affidavit certifyingthat profits derived from in-house research belonged solely to the director of the institute (i.e. Robert Koch).Furthermore, upon leaving the institute they were required to report all the results of their research and submit“all notes and protocols” (BA, R 86, No 3801) (see Gradmann 2000).

Administrative Stabilization of Vaccines in France and Germany, 1894–1900 211
secondary concern, as long as serum production could be overseen from one centralplace. Yet such hopes were dashed when in March of 1894 the Schering company inBerlin announced the production of a serum twenty times stronger than the standard(see above). Unlike Hoechst, Schering had grown from a local pharmacy and nowpromised that by “perfecting the techniques of immunization and using new methodsto concentrate the serum, the immunization effects of the anti-toxin solution wouldrise to new heights” (Throm 1995, 57).
This announcement generated considerable pressure. Behring’s research group tookthe announcement seriously, especially since Rudolf Virchow supported the serumresearch at Schering. Facing growing competition, Hoechst was forced to speed up itsefforts to begin industrial production. A race to get the product to market in Germancountries began. On 1 August 1894 Hoechst began by bringing “Behring’s diphtheria-medicine” to the market. However at this stage, neither the debate about the time-span and degree of immunization was resolved, nor was the construction at Hoechst’sproduction site completed. The surprise announcement in Budapest aggravated thissituation, as German publishers began to imitate their French colleagues. The publisherof the Berliner Lokal-Anzeiger, August Scherl (1849–1921) initiated calls for a Germansubscription (Huntelmann 2006). In the state of Mecklenburg, the Duke and Duchessthemselves appealed for donations. Demand for the serum was enormous.
In this situation, all plans to build an imperial production facility that wouldensure oversight and control of the serum proved to be illusory. This would firstof all have involved reaching an agreement with the competing firms and losingcontrol over the process. Even though the seemingly natural production processmeant that no patent protection was in the offing, Prussian ministries neverthelessrespected Behring’s transfer of the production process to Hoechst.8 Second of all,this question affected more than just the investments of two competitors. As thepublic dispute between Behring’s research group and Virchow’s serum researchersillustrates, competition was not restricted to the marketing of a commercial product,but also involved scientific recognition of the serum’s therapeutic value. Based ontheir own measurements, Emil Behring and Paul Ehrlich considered Schering’s serumto be inadequate and far below the reported strength (Behring 1894a; idem 1894b).In turn, Schering’s scientists deemed Behring’s serum to be sub-standard and histesting procedures idiosyncratic; they rightly charged Behring with having altered hismethod on several occasions (Aronson 1894; Buchner 1894). No matter how practicalPrussian officials believed it would be to consolidate serum production in a centralfacility (for which experts believed forty horses would suffice), in the fall of 1894 thiswould have meant reconciling conflicting economic interests as well as arbitrating a
8 German patent law – thanks to the lobbying of the chemical industry – protected the production process, butnot the product itself. Hence, only the brand “Behrings Diphtherie-Heilmittel” was protected. Consequently,in the fall of 1894 Behring applied for a US patent that provided protection for the product itself.

212 Volker Hess
scientific dispute. Hence, the plan to create a German Pasteur Institute was quicklyabandoned.9
Industrial competition and scientific disagreement played an important role in allfurther plans to regulate the new medicine in Imperial Germany. If medical officialshad had to deal simply with one producer who, on top of it all, was contractuallyobliged to work together with Ehrlich and Behring, their problems would have beensolved. As things stood, however, the growing number of production facilities led tofears that “occasionally sub-standard or contaminated batch of serum” would make itonto the market. Consequently, the key issue became the administrative stabilizationof the therapy, i.e. the “uniform measurement of the so-called Normaltiter.”10 Thisrepresented the technical precondition that enabled the effectiveness of sera producedby different manufacturers to be tested and compared.
At the same time, events quickly overtook the French model, eclipsing itsparadigmatic status. The monopoly held by the Pasteur Institute over the productionand distribution of the serum was more quickly questioned than responsible officialscould have wished. In spite of the euphoria surrounding the success of the subscription,it soon emerged that the Pasteur Institute was unable to meet the high expectations.Hopes of sufficiently increasing production within three months so that the needsof rural areas could be met, proved to be illusory. Finally, in April of 1895 it wasofficially announced that, for the time being, Paris could not be expected to providesufficient serum to meet the needs of the service antidiphterique. Consequently, the publicexpectations that had been raised by claims that the subscription would provide freeand comprehensive coverage, were sorely disappointed: Why, asked city officials inBordeaux in early November 1894, should cities support a subscription from whichthey seemed to derive no advantage?11 A similar debate unfolded in Lyon. There thedirector of the Bureau of Hygiene had to admit to the local mayor that it would takeParisian labs more than two months to deliver the serum and that even those supplieswere reserved for hospitals and the impoverished patients of the bureaux de bienfaisance.Given this precarious situation, he recommended following the example of other largecities and building a civic laboratory in the Bureau of Hygiene.12
Indeed, similar deliberations occurred in all large cities. Officials in Marseillecommitted 10,000 Francs toward the construction of the city’s vaccination facility.In Toulouse a committee comprised of physicians was created to dispense free ofcharge the serum that the local veterinary school, headed by Emmanuel Leclainche(1861–1953), had produced using two horses (Anonymous 1894c). With the same
9 Later, medical officials brought up this plan whenever they sought to extract financial concessions frompharmaceutical companies.10 Minutes of the meeting of 24 October 1894, BA, R 86, No. 1646.11 Indeed, during 1895 the Pasteur Institute received no donations from the local administration in theDepartment of Gironde (AIP, files of the Direction).12 Letter of the director of the office of hygiene in Lyon, M. Roux, to the mayor of Lyon, Dr. Gailleton, 6November 1894; Archives Municipales, Lyon, fiche 1125 WP 023-2

Administrative Stabilization of Vaccines in France and Germany, 1894–1900 213
aims in mind, the city of Le Puy organized a large meeting at which the fatherand brother of Louis Martin, who worked at the Adnexe Garches in Paris, appealedfor support. In Rouen the local newspaper managed to raise some 77,000 Francs inless than two months for the bacteriological laboratory there (Journal de clinique et detherapeutique infantiles, vol. 3, 1895; No. 1, Thursday, 3 January 1895). And in Nancythe civic administration was not content to simply build the local deport for the PasteurInstitute, but also founded an Institut antidiphterique pour l’Est de la France (Revue Medicalede l’Est 1894, 692). Similar efforts were also undertaken in Lille, Montpellier, Le Havre,and Grenoble (Zeiss and Bieling 1940, 174).
Bordeaux is a good example of how local production sites were set up. Thedriving force behind efforts there was the local medical faculty’s microbiologist, GabrielJean Hypolite (born 1858). Hypolite had been appointed professor of experimentalmedicine in 1892 and – like many of his contemporaries – had studied microbiologyunder Roux and Alexandre Yersin before founding the faculty’s bacteriologicallaboratory in Bordeaux. Stalls for three horses were constructed on the grounds ofthe local fire station. The financial costs were not great: the city estimated the costfor stalls, feed, and personnel at 5,500 Francs per annum and for the acquisition ofinstruments and animals at a further 2,500 Francs. By the end of January 1895, twohorses had been immunized, a third was supposed to follow, and a fourth was addedto the program. According to the estimates of city officials, the serum acquired fromone horse alone was deemed sufficient to treat fifty patients, i.e. more than enough tomeet the city’s needs. The distribution of the serum lay ultimately in the hands of themedical faculty: every dispensation of the serum required bacteriological certificationof the diphtheria agent. The bacteriological laboratory provided special test-kits (smalltubes with in vitro culture and spatula) to physicians across the region. Within 24hours of receiving the specimens, the laboratory issued a diagnosis and the accordantauthorization to receive the serum.
Increasingly, the enthusiasm that had been generated among the sponsors of thepublic subscription lessened. In early 1895 the Pasteur Institute finally lost its monopolyover production and distribution – and with that also its oversight and control of theserum.13 In spite of all the practical difficulties, local initiatives were surprisinglysuccessful. Rouen and Bordeaux began serum production in early 1895. Rouen waspreparing three horses for serum production. In May of 1895 even the Prefect ofBordeaux went so far as to contribute to local serum production, expanding municipalservice to cover the entire department.
All attempts to put the genie back in the bottle came too late. Even as debatecontinued on a new law governing the “production, sale and distribution of therapeutic
13 This might also be attributable to Emile Roux’s new style of institutional leadership. Roux didn’t share LouisPasteur’s secretive proclivities. Instruction in microbiology was based on models adapted from Berlin, producingtrained physicians and scholars and disseminating standardized methods and practices (Mendelsohn 1996, chap.6).

214 Volker Hess
serum and other analogous products,” the number of producers multiplied rapidly.Parliamentary speakers repeatedly emphasized that the law was not intended “toensconce a monopoly.” But because the marketing and sale of serum had alreadybegun, urgent action was needed to ward off the looming threats to public health.In keeping with traditional views on drug safety, parliamentarians were worried aboutimpurities and the transmission of infectious substances from animals to humans.14 Thesuggestion that permission could be granted for just a few months or years was rejectedon grounds of public safety and the need for rapid intervention. Instead, the Frenchgovernment secured passage of a law on 25 April 1895 that permitted – with somerestrictions and reservations – the industrial production of medicines.
3. Administering Oversight
Initially, the pressure of events forced officials in both Germany and France to treatdiphtheria antitoxin serum according to existing laws. In both countries, diphtheriaantitoxin serum was a prescription drug available only in pharmacies. Likewise in bothcountries, medical officials were aware that traditional forms of oversight and controlwere insufficient for the new medicine: diphtheria antitoxin serum could neither bemade nor tested for purity (or effectiveness) in the pharmacies. Given this situation,both countries resorted to rules used to test and certify secret remedies.
French law made the Consultative Committee of Public Health (CCHP = Comiteconsultative d’hygiene publique) and the Academy of Medicine (Academie de Medecine)responsible for certification. And according to an enabling law of 15 May 1895, thatresponsibility was exercised through a newly created serum commission (Ministere del’Interieur 1895). The serum commission was comprised of 15 members. By law, slightlymore than half were drawn from the ranks of the Academy of Medicine and the CCHP;slightly less than half were representatives from the Service de Hygiene and the Assistancepublique, officials from other ministries, and economic interest groups.15 A general
14 Of course the hormone therapy of Brown-Sequard played an important role in spreading such fears (L’annexe1209 1895; L’annexe 1245 1895). The therapy involved injecting men with extracts from animal testicles withthe aim of physically rejuvenating them and enhancing their sexual potency.15 The representatives of the comite de direction des services de l’hygiene included Henri Monod (1843–1911),director of the assistance publique; Adrien Proust (1834–1903), professor of hygiene at the medical faculty inParis; Andre Chantemesse (1851–1919)∗; Raoul Bompard, chief official for economic issues in the ForeignMinistry; C. Nicolas, state councilor and chief official for labor and industry in the Ministry of Commerce; andDelaunay-Belleville, president of the Parisian chamber of commerce; and after 30 September 1884 the standingsecretary of the Academy of Medicine, Etienne-Jules Bergeron (1817–1900). Of eight other members, fourhailed from the ranks of the academy: Edmond Nocard (1850–1903)∗; Emile Duclaux (1840–1904)∗; IsidoreStraus (1845–1896)∗; and Jacques-Joseph Grancher (1843–1907)∗. Four were from the CCPH: Anne GabrielPouchet, pharmacologist (1851–1938)∗; Francois Jules Ogier (1853–1913) Chef du Laboratoire de Toxicologie ala Prefecture Paris; Leon Henri Thoinot (1858–1915); and Arnold Just Netter (1855–1936)∗. The comite alsoincluded Paul Camille Hippolyte Brouardel (1837–1906), professor for forensic medicine at the medical faculty

Administrative Stabilization of Vaccines in France and Germany, 1894–1900 215
impression of the commission’s work can be gleaned from the minutes of its regularmeetings. Certification depended on the results of an inspection of the productionfacilities. In most cases, of the 15 members on the commission, only two examined theproduction sites: Arnold Just Netter (1855–1936) and Edmond Nocard (1850–1903).
To judge by the minutes of the serum commission, these visits were usually aformality. Inspectors examined the location and arrangement of the rooms, checkedthe instruments used to extract and process the serum, visited the horses’ quarters andobserved their health and diet, and scrutinized the procedures used to fill and labelthe serum bottles. Surviving reports suggest that the serum itself was not tested. Itwas not the effectiveness of the serum, but rather the expertise of the producer andthe cleanliness of the production site that were inspected – a procedure comparableto that used to inspect pharmacies. For example, permission for the civic laboratoryin Bordeaux to produce serum was based on the assessment that “everything is wellorganized, the laboratory equipment is second-to-none.”
Follow-up inspections were uncommon. In the material I have studied, there wereno cases of additional site inspections. The work of the serum commission can thereforebe interpreted as similar to that of a certification board, acting as a gate-keeper thatonly controls access to the market, but with no obligation to oversee further practice,let alone the quality of the serum produced. Once a laboratory had been officiallysanctioned, it could produce and market the certified serum according to its ownstandards. This is how the French medical administration renewed traditional forms ofprofessional oversight. Quality control of the serum proceeded according to the modelestablished by the Academy of Medicine, where French physicians autonomouslyjudged the usefulness of new therapeutic procedures and medicines. Although theseorgans of quality control were authorized and sanctioned by the state, the evaluativeprocedures, testing conditions, and the criteria applied toward the evaluation lay withinthe exclusive jurisdiction of medical professionals. In other words, the public drama ofhaving a medication certified was choreographed as a decision of medical professionals,and not as an act of state approbation. This traditional form of oversight of secretremedies was sanctioned by the scientific and professional expertise of supervisoryactors or – to put it another way – was an exercise of power by a corporately constitutedprofession (Brockliss and Jones 1997, 622–650).
As far as therapeutic use was concerned, the actual decision likewise lay within thejurisdiction of the medical profession – or to be more precise, a new caste within theprofession. The two inspectors were both closely associated with the Pasteur Institute.Netter was the dissertation advisor of the Pasteurian Jacques-Joseph Grancher (1843–1907) and Nocard was a veterinarian and director of the veterinary school at Alfortwho, as a member of the Pasteur Institute, had played a decisive role in industrializing
in Paris, who – as president of the committee of the Direction des Services de l’Hygiene – headed the serumcommission. Later the comite included Ernest Cadet de Gassicourt (1826–1900), a pediatrician at the HopitalTrousseau and Auguste Chauveau (1827–1891)∗. The Pasteurians are marked with an asterisk (∗).
216 Volker Hess
serum production. A number of other Pasteurians were also members of the serumcommission (cf. footnote 15). As a consequence, members who had been affiliatedwith the institute comprised a majority on the commission.
In general, those subject to the commission’s oversight were also students of Pasteuror former employees of the institute, where they had learned the procedures involvedin immunization and serum production. In Bordeaux the chief physician HypoliteGabriel Ferre had been a student at the Pasteur Institute; in Rouen, Charles Nicolle(1866–1936) had been a student of Roux und Metchnikoff; and in Lille the facilitieswere a formal part of the local Pasteur Institute run by Calmettes. Other facilities werefounded as annexes to medical faculties: the physician d’Astros was the chief protagonistin Marseille, while in Montpellier funds were collected to construct an institute forserum production under the direction of the microbiologist Poujol. The facilities ofDumont in Le Havre, Mace in Nancy, Arlong in Lyon, as well as Fernand Berlios andJourdan in Grenoble were either directly or indirectly affiliated with the faculty.
It no doubt made sense to grant Pasteurians a central role in overseeing diphtheriaantitoxin serum production for no one else had the necessary expertise and technicalqualifications. At the same time, however, this effectively made the Pasteur Institute agatekeeper: it was not only made responsible for its own serum production, but alsoparticipated in the certification and oversight of each of its potential competitors. Thestrategic position and industrial monopoly of the Pasteur Institute were based on thiscircumvention of any “separation of powers” in exercising state control. That said,however, contemporary debates give no indication that anyone objected.
German officials were also aware that overseeing diphtheria antitoxin serumdemanded technical and scientific expertise that, for the time being, could only behad from the researchers themselves. In Berlin, representatives of the serum producerswere included in deliberations on the criteria and standards to be used for testingand certification. But German officials chose a different approach in order to involveexperts in administrative oversight: they established a special inspection site that beganwork early February 1895. Initially the facility was attached to the Prussian Institute forInfectious Diseases. From the summer of 1896 it became a full-blown Royal Institutefor Serum Research and Testing, before moving to Frankfurt in 1899, where it exists tothis day as the Paul Ehrlich Institute. The details of the development and organizationof this institute and its testing procedures have been investigated (Throm 1995), mostrecently and extensively by Axel Huntelmann (Huntelmann 2007b). Therefore, I wishto limit my analysis to the essentials.
According to the edict of 25 February 1895, producers were required to send asample of every large batch of serum to Berlin for inspection. There the therapeuticquality of the diphtheria antitoxin serum would be determined by comparing it toa standard. This was difficult for two reasons. First, the actual evaluation involvedhighly sophisticated techniques that even the experts described as “extremely difficult”because the procedure developed by Paul Ehrlich to standardize the effects of serumdemanded first that the diphtheria toxin be standardized. Second, every batch of serum
Administrative Stabilization of Vaccines in France and Germany, 1894–1900 217
was tagged with an Operation Number and continuously documented on its way fromthe initial harvesting of the blood, to the preparation and bottling by the producer, thento the quality control facility, and finally through distribution to the final point of sale inthe pharmacy. Thus, certification of a batch of serum for therapeutic purposes involvedan enormous amount of bureaucratic paperwork. Furthermore, the sample extractedfrom each batch at the quality control facility was used not just for a single evaluation,but also to evaluate quality over time: a part of each sample was preserved for testingat regular intervals in the future. If these later tests failed, the entire batch could berecalled. After 1 April 1895, only diphtheria antitoxin serum that had passed throughthis rigorous testing regime was allowed on the German market. And so virtuallysimultaneously on both sides of the Rhine, legal and administrative procedures wereput in place that stabilized the serum as a kind of medicine. However, in each case, theprocedures were organized very differently. Three elements are worthy of note here:
1. Controlling the product vs. controlling the producer: The relentless inspection ofdiphtheria antitoxin serum lay at the heart of German serum control. Its qualitywas controlled in two ways. First, in keeping with the tradition of inspectingpharmacies, there was a pharmaceutical inspection of the hygienic conditions ofproduction and inspection of the purity of the serum. In addition, a state officialwas dispatched to the laboratory of the pharmaceutical company to observe theblood being drawn and processed and the serum being bottled. Second, therewas a pharmacological inspection which evaluated the effectiveness of the serumaccording to standardized criteria. In other words, the administrative inspectionprocedure involved an important aspect of state intervention, in that it stabilizedthe therapeutic value of the serum. By contrast, the focal point of the Frenchcertification process was the producer: in France, the facility and the technical andprofessional qualifications of the manufacturer were inspected, but not the serum’stherapeutic effectiveness. Instead, the certification process was more a matter ofthe producer belonging to the medical community, or better still to the greatPasteurian family.
2. Public control vs. personal control: In strictly formal terms, serum regulationwas implemented in both countries by the state. The new quality controlfacility was hardly a counterpart to the new serum commission in France. Thedegree of institutionalization is the least of the differences. The French serumcommission was a representative organ that included various actors (ministerialofficials, politicians, and leading figures from business, commerce, science, andthe academy). Ministerial bureaucrats had little influence on the selection of therepresentatives. Most were appointed because of the status-group they belonged to(for example as members of the Academie) and had only indirect connections tothe commission. The commission’s expertise was based only in part on professionalcompetence; the personality and authority of its members was far more important.The decisions of the commission acquired their authority by virtue of the offices of
218 Volker Hess
its CCHP members, the professional reputations of its academicians, the politicalpower of its ministerial officials, or the social status of, for example, the president ofthe chamber of commerce. In Germany, however, the serum facility was establishedas a technical office. Its influence and remit depended on its official function,because without official approval, no serum could be brought to market. Theserum facility was a systematic component of the Prussian medical bureaucracy,where – in the tradition of the Scientific Deputation – it functioned as an expertin the art, i.e. Kunstrichter (see Broman 1998). Naturally, the expertise of the serumfacility was based heavily on the technical competence and scientific authority ofPaul Ehrlich. It is noteworthy, however, that Ehrlich still held neither an academicnor a political post. In fact it seems that it was Ehrlich’s abstinence from social,political, and professional power that predestined him to take up this new office.The power of his institution, however, derived from the state’s influence over theproduction and marketing of the serum and was exercised through bureaucraticinstruments.
3. Forms vs. informal consent: We know more about the German quality controlfacility because every single step in the production process was comprehensivelydocumented. In France, on the other hand, the serum commission issuedonly very cursory reports. It would be a mistake to attribute the Germanbureaucracy’s penchant for documentation to a national style, be it of Imperial orPrussian provenance. Instead, the surviving documents reflect a central functionalcomponent of the bureaucratic regime: Operation numbers and forms comprisedthe interface between the central inspection facility and the local production sites,where the administrative techniques of serum control were implemented. Thespatial separation of testing and production was the occasion for, but not the cause ofthe excessive formalism. The circulating forms bridged not only the spatial divide,but also different social worlds. They made serum control transparent even to ill-informed ministerial bureaucrats and critical pharmaceutical producers. Becausethe formal processes of using forms translated every step of the process into theterminology and rationality of bureaucrats, it enabled all of the actors to understandthe decisions that had been made. The doubts and criticisms that were frequentlyvoiced were silenced by reference to the protocols, thus shifting interpersonalconflicts into a more formal sphere of interaction.16 State intervention in serumoversight lay – as far as the performative drama of its implementation is concerned– outside the normal nepotistic networks. Naturally, in Germany there was aclose association between the inspectors (Ehrlich and his team) and the inspected(Behring et al.), but this association was embedded in a formalized system ofregulations and the extent of personal commitments or dependencies resulting
16 One example is the dispute between Behring and Ehrlich that arose after the introduction of a newexperimental toxin. After the process was revealed, the dispute was ameliorated, but not entirely eliminated(Throm 1995).

Administrative Stabilization of Vaccines in France and Germany, 1894–1900 219
from the operationalized evaluation process was, in general, limited. Admission intothe circle of certified producers is an example of such an operationalized process:in Germany, admission was formally confirmed by a one-time enrollment fee of1,000 Marks; but in France, admission depended on the respect and recognitionthat the producer enjoyed in the eyes of the commission. Consequently, it’s notknown if and how site inspection in France was organized and carried out. Sincethere was no bureaucratic intervention in the evaluation process between the siteexamination and the certification decision, no paper-trails or files were produced.Instead, we can assume that an informal consensus between the regulators and theregulated was a decisive factor: as Pasteurians they shared a common vocabularyand set of convictions, common knowledge, and techniques, so much so that notranslation into tables and forms was necessary.
4. Market Performance
Marketing and distribution were also organized differently in the two countries. InGermany, an order issued on 31 December 1894 permitted diphtheria antitoxinserum to be sold only by pharmacists, thus confirming their traditional monopoly.Nevertheless, many producers competed against each other in a medical marketplace.Alongside Schering and Hoechst, the Merck company began production in late 1895.In April of that year in Hamburg, Carl Enoch had also sought certification as a producer.And after the turn of the century other producers entered the market: in 1901 Proscherand Muller sought state certification of their serum; in 1910 the Sachsische Serumwerkdid the same (Throm 1995). All producers were subject to state controls if they wantedto keep their products on the market.17 Although those controls ensured that thesera were very similar, producers advertised their respective sera using different brand-names (“Diphtherie-Heilserum Merck,” “Schering’s Diphtherieserum,” “Behring’sDiphtherie-Heilmittel Hoechst”). Advertisements, rebates, and price-wars were thetechniques used to commercialize serum that was ultimately produced, marketed, andsold as an industrial product.
In France, by contrast, officials confronted with the unexpected success of the largesubscription had to face the problem of distributing diphtheria antitoxin serum freeof charge. In anticipation of future mass production, a circular dated 14 January 1895ordered that the Service graduit be associated with the institutions of community healthservices. Appointed by the prefects of the departments, the Bureaus d’assistance medicalegraduite would be responsible for the local depots, which would be equipped and
17 The Pasteur Institute, which had cooperated with the hygiene inspection agency in Wurttemberg, ceasedmarketing its diphtheria serum on the grounds that inspecting serum production in Paris according to Germanstandards (and using German state officials) was unprofitable.
220 Volker Hess
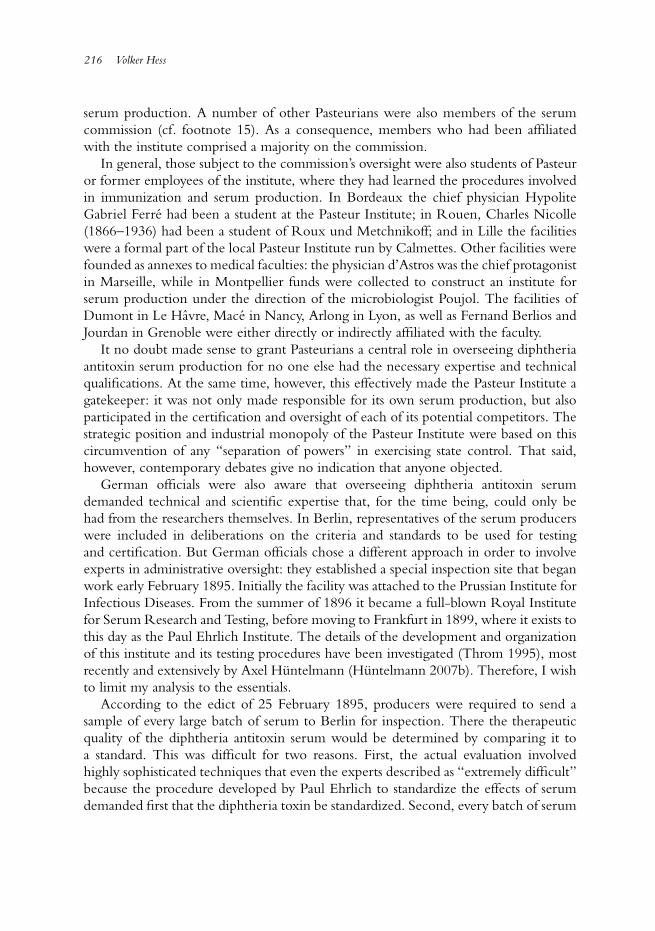
Table 1. Number of Communities Served by the Institute Bousson-Bertrand in Montpellier
Department 1897 1898 1899 1900 1901
Herault 168 186 231 237 238Aude 46 258 279 284 297Gard 106 111 124 127 129Pyrenees Orientales 18 27 43 48 56Lozere 27 27 27 27 27Vaucluse 14 22 27 27 30Aveyron 2 5 5 7 9Tarn - 3 15 19 20Var - 1 1 1Total 381 640 751 777 807
supplied by the Pasteur Institute. Local producers of serum adhered to this model.They eagerly took up the slack once the Institute Pasteur failed to meet its ownambitious goals.
A good example is the local serum production in Montpellier where the foundingof an institute in 1897 was made possible by Mme Bousson-Bertrand. The widow ofa professor of medicine in Montpellier, she donated 300,000 Francs to the city forresearch and treatment of diseases related to public hygiene. An official subscriptionraised a further 184,000 Francs so that new laboratory rooms could be built nearthe prestigious university’s main building. The institute was closely affiliated with themedical faculty. Its board was chaired by the dean of the medical faculty and its othermembers were elected for tenures of seven years by secret ballot of the medical faculty.Alongside the diphtheria serum (prepared according to Ramon’s method), the instituteproduced other sera for streptococous, rabies, and typhus in the late 1890s and launchedan extensive program of diagnostic examinations.
Like the Pasteur Institute, the Montpellier Institute wished to dispense the serumfree of charge. However, the operation costs of the institution (10,000–15,000 Francsin the 1890s) couldn’t be met by interest earned on the foundation’s endowment.Instead, the institute was supported by the ministry of agriculture (4,000 Francs) andespecially by the city of Montpellier. The city’s dignitaries financed not only a chairin microbiology, but also subsidized the institute annually to the tune of 2,000 Francs.According to reports, this Subvention annuelle became the institute’s most importantpillar of support. In return, supplies of serum in the communal depot were replenishedon a regular basis (see Table 1).
The city of Montpellier was not the only community to purchase this Service graduitby providing an annual subsidy to the producers. Within a year of its founding, theinstitute supplied the local depots of more than 350 communities that had participatedin the subscription. In later years, the numbers rose constantly. Finally, by 1900 around
Administrative Stabilization of Vaccines in France and Germany, 1894–1900 221
800 communities in nine departments were having their serum depots replenished inexchange for an annual subsidy.
Other serum producers copied this model. In Bordeaux the prefect contributed3,000 Francs toward ensuring that the department’s serum depot was adequatelysupplied. For its part, the community of Arcachon promised a yearly subsidy of 500Francs for regular delivery. And the general public viewed the subscription as themonetary equivalent of free access to the serum (see Jonathan Simon’s contributionin this volume). Hence, it would be a mistake to believe that free access meant thatthere was no cost. Instead, the production, marketing, and distribution of the Frenchdiphtheria antitoxin serum involved an economy with somewhat different moral values:
1. The French model avoided the appearance of commercialization. The relationshipbetween a “donation” or “contribution” and the provision of diphtheria antitoxinserum was a direct one and was usually stipulated in a contract. But the objectnegotiated in the contract was not the serum, but a humanitarian service providedto sick patients, i.e. the Service graduit. There is no indication of a direct one-to-one relationship between the quantity of serum required and the amount of thedonation, as would have been the case in a commercial transaction. Instead, thecontract involved a negotiation of moral virtues such as altruism, beneficence, andgenerosity. In dispensing serum free of charge, the serum producers appeared tobe selfless helpers and benefactors of humanity, and the subscribers appeared to benoble and magnanimous patrons.
2. The Service graduit was a component of a different kind of risk management.According to this model, the cost of diphtheria treatment was conceived as a riskthat burdened neither the individual, nor the larger collective group. Instead, it wasunderstood to be a matter for local community services, which were responsiblefor the medical treatment and care of their citizens. Diphtheria antitoxin serumwas therefore incorporated into the decentralized organization of local medicalservices that had been built up following the Franco-Prussian war (Ramsey 1994b;Murard and Zylberman 1996).
3. The French model continued to be shaped by the idea of prevention. Althoughstockpiles were created for emergencies, the administration in many communitieswere built on the model of the Vaccin Jennerien or service vaccinal. Warding offan epidemic was a recurrent argument for the construction of depots that weresupervised by the local epidemic doctor (Medecin de l’epidemie) who oversawserum dispensation. The depot itself was a prophylactic facility: the stockpileswere reserved for an outbreak and every three months one-third of the stock wasreplaced to ensure that there was always sufficient serum on hand.18
18 This model of decentralized prophylaxis explains the high number of horses used for serum production inFrance, something that historians have puzzled over.
222 Volker Hess
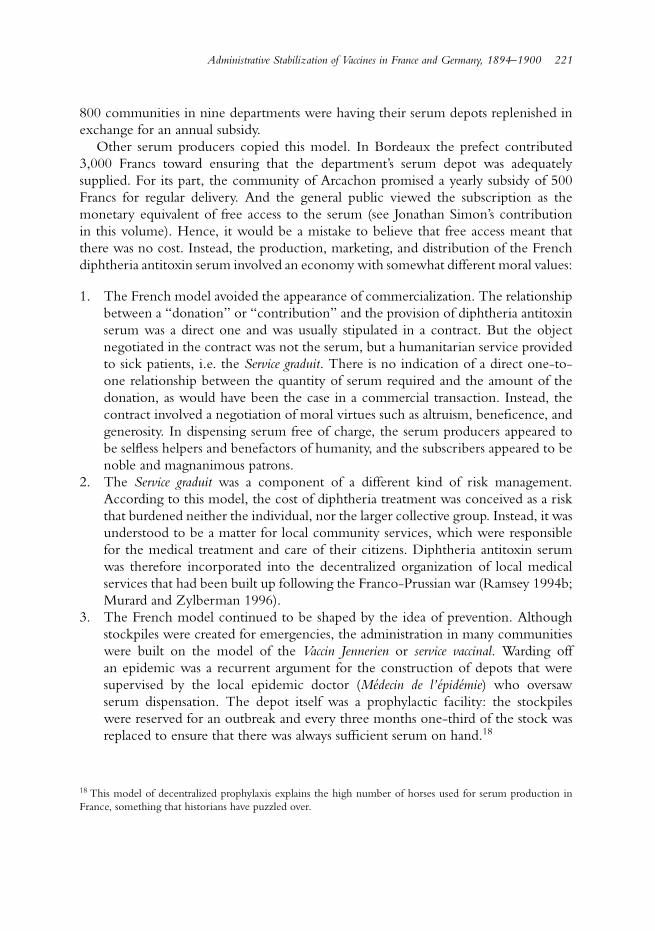
Table 2. Service de la serotherapie from 14 February to 3 December 1895 (AIP, No9270-9276)
Expenses Income
Horse Purchases 26,011 Subscription 998.309Construction 179.105 State subsidy 80.000Material 205.779 Bottles paid 420.148Office and Packaging 58.895 Other income 17.160Stalls in Grenelle and Alfort 43.905Personnel 7.431Grand total 521.113 1.515.618
In France all efforts to supply the new serum were organized around thehumanitarian model of the Service graduit. Yet to this day it is often overlooked thatfree distribution was restricted to the poor and needy charges of public hospitals andnursing homes. As in Germany, all other citizens of the French Republic had topurchase the serum as merchandise from their local pharmacies. Likewise, the sale ofdiphtheria antitoxin serum played an important role for producers like the PasteurInstitute. Nevertheless, the myth survives that the Pasteur Institute had no commercialinterest in the production of the serum.
This is only partially correct. It may well be that the prospect of monetary gaindid not motivate the scientists working in Roux’s group. At least no plans havesurvived indicating that scientists in Paris or other peripheral production sites triedto calculate anticipated profits, as was commonplace at Hoechst, Schering, and otherserum producers. Nevertheless, the financial advantages for the Pasteur Institute weresignificant. The numbers published in the annual reports leave no doubt about this.In 1895, a good portion of the nearly 200,000 doses produced by the so-called Serviceantidiphterique were sold for profit. In that year alone, the sales and subscriptionsgenerated a net profit for the institute of nearly one million Francs (see Table 2).Other producers also sold their serum, but couldn’t match such profits. For examplein 1898 the Institute in Montpellier produced 5.700 doses, of which 228 were sold forprofit (Fabrege 1901).
If today one is inclined to accept the image of independence, humanity, and scientificethos that these institutions projected, it is essentially because of the mechanismsdeployed in the performative choreography of oversight, marketing, and distribution ofthe diphtheria serum. The same was true for Germany, where, as a commercial productof the nascent pharmaceutical industry, diphtheria antitoxin serum was standardizedand tailored to suit the competitive environment of a liberal marketplace. Yet thistoo is a self-serving representation that needs correction. Unfettered capitalism wasalso held in check in Germany, albeit behind the scenes. As mentioned above, theprice of medicines was set by a so-called Medizinaltaxe, a tradition dating back to early

Administrative Stabilization of Vaccines in France and Germany, 1894–1900 223
modern times. The sale price was fixed by the state, in this case by the Ministry ofCulture. Naturally the serum producers were invited to participate in setting these pricecontrols. Yet the cards they held in this game of poker were poor, because as part oftheir oversight responsibilities, medical officials had regular access to the accounts of thepharmaceutical producers and were thus able to accurately assess the economic returnon sales (Huntelmann 2007a). The state was willing to see producers make substantialprofits,19 but it insisted on preferential supply for hospitals and other community carefacilities. These institutions could order the serum at half the official price; and officialprescriptions allowed the discounted serum to be purchased in pharmacies (Throm1995). For years to come medical officials insisted that “for social and ethical reasons[the state] absolutely had to maintain its right to set prices.”20
5. Conclusion
By the time diphtheria antitoxin serum had been marketed virtually simultaneously inGermany and France in 1894, it had been largely expunged of its experimental qualities.The scientists in Paris and Berlin had reached a consensus about the therapeutic value,medical function, and scientific status of the new serum. But the marketing of thesequalities, which had been stabilized in an arduous and difficult process, was by nomeans predetermined. Instead, as this paper has demonstrated for cases of France andGermany, diphtheria antitoxin serum was subjected to very different procedures onceit left the experimental world of the laboratory. These procedures were cruciallyinfluenced by the regulatory environments in which they were deployed. Thesedifferent environments transformed what had once been an experimental object intoa mass commercial product on one side of the Rhine, and into an integrative elementin public health care and a cornerstone in the foundation of the community healthservices on the other side. A boundary object acquired its respective and characteristicqualities via inspection, marketing, and sale.
In Germany the administrative framework and bureaucratic implementation ofthe serum testing produced a mass commercial product that displaced the traditionalresponsibilities of the pharmacist onto an industrial production process. Once thebottles of serum received the official certification stamp in the factory, they weresubjected to multiple inspections that molded the product in important ways: First, theofficial certification stamp took the place of traditional forms of quality control thathad now been shifted forward to a point that lay prior to the serum’s dispensation andsale in pharmacies. Second, the official certification stamp guaranteed the quality of theproduct over time, so that trust in the professional and technical work of the pharmacist
19 According to Throm 1995, the profits accruing to Hoechst (including Behring’s portion) amounted in 1895to 706,770 (353,385); in 1896 to 320,584 (160,292); and in 1897 to 345,500 (141,508) Marks.20 GStA PK, Rep. 92, AI Nr. 244, Althoff to Behring, 22 May 1904.

224 Volker Hess
became superfluous. Third, the state labeling and packaging requirements for the serumvials allowed consumers to determine the commercial class of the serum, because theymade it possible to compare the different contents offered by different producers. So theproduction of diphtheria antitoxin serum anticipated later developments. Diphtheriaantitoxin serum was a highly standardized product: it was produced according touniform Imperial standards, subject to rigorous quality control, split into differentproduct lines, and marketed under constant product supervision. The German versionof diphtheria antitoxin serum thus became a prototype of the kind of normed industrialproduct that, in the early twentieth century, would be spawned by war, rationalization,and Taylorism (Berz 2001; Mehrtens 1999).
French law, on the other hand, stressed scientific autonomy in the productionof serum and refrained from direct state intervention. Instead, oversight of serumproduction was left mainly to a scientific elite. The serum was deployed not as acommercial product, but rather as a service provided by a nascent community healthcare system. It involved not the amalgamation of an exchange value on the one hand anda curative value on the other as in Germany; instead, it was based on a correspondencebetween scientific ethos and social responsibility and was more concerned about thecompetence and integrity of the producers than about comparative testing of batch-samples. The currency of this procedure was backed up by a moral economy that restedon trust in science’s commitment to general truth and public well-being.
Neither its biological source, nor its experimental origin provided diphtheriaantitoxin serum with its ultimate and defining characteristics. These characteristicsemerged only from the negotiations between actors from very different social worldsand the interaction between medical professionals, industrial producers, state officials,and not least an engaged and critical public. The administrative arrangement of thesenegotiations stabilized the diphtheria anti-toxin serum, creating different objects in therespective French and German contexts.
Acknowledgments
This article was supported by Deutsche Forschungsgemeinschaft as part of the project“Industrialization of Experimental Knowledge” (HE 2220/4) from 2004 to 2007. Fortheir remarks, suggestions, and material support I wish to thank my colleagues in theproject Axel Huntelmann, Ulrike Kloppel, and Jonathan Simon.
Abbreviations of the archives used
BA = Bundesarchiv Berlin.AIP = Archives d’Institut Pasteur (Paris).GStA PK = Geheimes Staatsarchiv, Preußischer Kulturbesitz (Berlin).
Administrative Stabilization of Vaccines in France and Germany, 1894–1900 225
References
Anonymous. 1894a. “Au congres de Budapest. La decouverte du docteur Roux.” Le Figaro 17 September.Anonymous. 1894b. “Chroniques documentaires: L’antitoxie.” Le Figaro 9 October.Anonymous. 1894c. “Le vaccin du croup.” Le Jour.Aronson, Hans. 1894. “Weitere Untersuchungen uber Diphtherie und das Diphtherie-Antitoxin.” Berliner
klinische Wochenschrift 15–19:356–358; 425–427; 453–456.Baginski, Adolf. 1913. Diphtherie und diphtherischer Croup. Specielle Pathologie und Therapie Vol VII,
edited by Hermann Nothnagel and Lothar von Frankl-Hochwart. 2nd revised edition. Wien:Holder.
Behring, Emil Adolf von. 1890. “Uber Desinfection, Desinfectionsmittel und Desinfectionsmethoden.”Zeitschrift fur Hygiene und Infectionskrankheiten 9:395–478.
Behring, Emil Adolf von. 1893. Die Geschichte der Diphtherie: mit besonderer Berucksichtigung derImmunitatslehre. Leipzig: G. Thieme.
Behring, Emil Adolf von. 1894a. “Zur Diphtherieheilungsfrage.” Deutsche Medicinische Wochenschrift15:343.
Behring, Emil Adolf von. 1894b. “Zur Diphtherieheilungsfrage – Bemerkungen zu vorstehenderEntgegnung.” Deutsche Medicinische Wochenschrift 17:385.
Behring, Emil Adolf von and S. Kitasato. 1890. “Uber das Zustandekommen der Diphtherie-Immunitatund der Tetanus-Immunitat bei Thieren.” Deutsche Medizinische Wochenschrift 16:1113–1114.
Berz, Peter. 2001. 08/15. Ein Standard des 20. Jahrhunderts. Munchen: Fink.Brockliss, Lawrence and Colin Jones. 1997. The Medical World of Early Modern France. Oxford, NY:
Clarendon.Broman, Thomas. 1998. “The Habermasian Public Sphere and Science in the Enlightment.” History of
Science 36:123–149.Buchner, Hans. 1894. “Ueber die naturlichen Hulfskrafte des Organismus gegenuber Krankheit-
serregern.” Munchener medizinische Wochenschrift 30:543–544.Calmette, Gaston. 1894a. “La guerison du croup a l’Institut Pasteur.” Le Figaro 9 September.Calmette, Gaston. 1894b. “Pour la vaccin du croup.” Le Figaro 20 September.Chauveau, Sophie. 1999. L’invention pharmaceutique. La pharmacie francaise entre l’Etat et la societe au XXe
siecle. Paris: Institut d’Edition Sanofi-Synthelabo.Chauveau, Sophie. 2004. “Le statut legal du medicament en France au XIXe et XXe siecles.”
Ms. Lyon.Chauveau, Sophie. 2006. “Genese de la ‘securite sanitaire’. Les produits pharmaceutiques en France aux
XIXe et XXe siecles.” Revue d’histoire moderne et contemporaine 51:88–117.Daremberg, G[eorges]. 1894. “La guerison de la diphterie.” Le Figaro 26 September.Dixon, Cyril William. 1962. Smallpox. London: J. & A. Churchill.Ernst, Elmar. 1975. Das “industrielle” Geheimmittel und seine Werbung. Arzneifertigwaren in der zweiten Halfte
des 19. Jahrhunderts in Deutschland. Wurzburg: jal-verlag.Fabrege, Frederic. 1901. Institut Bousson-Bertrand. Montpellier: Jean Martel Aine.Geison, Gerald L. 1995. The Private Science of Louis Pasteur. Princeton, NJ: Princeton Univ. Press.Gradmann, Christoph. 2000. “Money, Microbes, and More: Robert Koch, Tuberculin and the Foundation
of the Institute for Infectious Diseases in Berlin in 1891.” History and Philosophy of the Life Sciences22:55–79.
Gradmann, Christoph. 2004. “A Harmony of Illusions: Clinical and Experimental Testing of RobertKoch’s Tuberculin 1890–1900.” Studies in History and Philosophy of Biological and Biomedical Sciences35:465–481.
Hess, Volker. 2007. “Secrets, Bureaucracy and the Public: Drug Regulation in Prussia of the Early 19thCentury.” In Ways of Regulating: Drug Trajectories V, edited by Jean-Paul Gaudilliere and Volker Hess.Berlin: Max Planck-Institut fur Wissenschaftsgeschichte.
226 Volker Hess
Hickel, Erika. 1973. Arzneimittel-Standardisierung im 19. Jahrhundert in den Pharmakopoen Deutschlands,Frankreichs, Großbritanniens und der Vereinigten Staaten von Amerika. Stuttgart: WissenschaftlicheVerlagsgesellschaft mbH.
Hickel, Erika. 1977. “Das Kaiserliche Gesundheitsamt und die chemische Industrie im ZweitenKaiserreich (1871–1918).” In Medizin, Naturwissenschaft, Technik und das Zweite Kaiserreich, edited byGunter Mann and Rolf Winau. 64–86. Gottingen: Vandenhoeck und Ruprecht.
Huerkamp, Claudia. 1985. “The History of Smallpox Vaccination in Germany: A First Step in theMedicalisation of the General Public.” Journal of Contemporary History 20:617–635.
Huhle-Kreutzer, Gabriele. 1989. Die Entwicklung arzneilicher Produktionsstatten aus Apothekenlaboratorien,dargestellt an ausgewahlten Beispielen. Stuttgart: Deutscher Apothekenverlag.
Huntelmann, Axel C. 2006. “Das Diphterie-Serum und der Fall Langerhans.” Medizin, Gesellschaft undGeschichte 24:71–104.
Huntelmann, Axel C. 2007a. “Two cultures of regulation: The production and state control ofDiphtheria serum at the end of the nineteenth century in France and Germany.” Hygiea Internationalis7:99–119.
Huntelmann, Axel C. 2007b. “Evaluation and standardisation as a practical technique of administration:The example Diphtheria-serum.” In Evaluations: Standardising Pharmaceutical Agents 1890–1960, editedby Chistoph Gradmann and Jonathan Simon. Basingstoke: Macmillan.
Kibleur, Pascale. 1999. “L’evaluation et la validation des remedes par la Societe Royale de Medecine(1778–1793).” In Les therapeutiques. Savoirs et usages, edited by Olivier Faure, 73–85. Lyon: Merieux.
L’annexe 1209. 1895. “Le rapport de loi relative a la preparation, a la vente, et a la distribution des serumstherapeutiques et autres produits analogues (4 mars 1895).” Journal officiel de la Republique Francaise74:247.
L’annexe 1245. 1895. “Le rapport de loi relative a la preparation, a la vente, et a la distribution des serumtherapeutiques et autres produits analogues (28 mars 1895).” Journal officiel de la Republique Francaise74:313–316.
Mehrtens, Herbert. 1999. “Schmidts Schaufel (9,5 kg). Frederick W. Taylors Techniken des‘Scientific Managments’.” In Normalitat und Abweichung. Studien zur Theorie und Geschichte derNormalisierungsgesellschaft, edited by Werner Sohn and Herbert Mehrtens, 85–106. Opladen, Wiesbaden:Westdeutscher Verlag.
Meinel, Christoph, ed. 1992. Die Allianz von Wissenschaft und Industrie – August Wilhelm Hofmann (1818–1892): Zeit, Werk, Wirkung. Weinheim: VCH.
Mendelsohn, Andrew. 1996. “Cultures of Bacteriology: Formation and Transformation of a Science inFrance and Germany, 1870–1914.” Department of History. Princeton: Princeton University Press.
Ministere de l’Interieur. 1895. Serums therapeutiques et autres produits analogues. Legislation et reglementation.Extraits du tome XXV du recuil du comite consultatif d’hygiene publique de France et des actes officiels del’administration sanitaire. Melun: Imprimerie adminstrative.
Ministere de l’Interieur 1896. Serums therapeutiques et autres produits analogues: Legislation et reglementation.Extraits du tome XXVI du recuil du comite consultatif d’hygiene publique de France et des actes officiels del’administration sanitaire. Melun: Imprimerie adminstrative.
Murard, Lion, and Patrick Zylberman. 1996. L’hygiene dans la Republique. Le sante publique en France, oul’utopie contrariee 1870–1918. Paris: Fayard.
Pasteur, Louis. 1888. Inauguration de lInstitut Pasteur le 14 novembre 1888 ein presence de M. le President de laRepublique. Compte rendu. Sceaux: Charaire et fils.
Ramsey, Matthew. 1994a. “Academic Medicine and Medical Industrialism: The Regulation of SecretRemedies in France.” In French Medical Culture in the Nineteenth Century, edited by Ann La Berge andMordechai Feingold, 25–78. Amsterdam: Rodopi.
Ramsey, Matthew. 1994b. “Public Health in France.” In The History of Public Health and the Modern State,edited by D. Porter, 45–118. Amsterdam etc: Rodopi.
Straus, Isidore. 1984. “Sur la serumtherapie.” Bulletin de l’Academie de Medecine 32:329–333.

Administrative Stabilization of Vaccines in France and Germany, 1894–1900 227
Throm, Carola. 1995. Das Diphtherieserum. Ein neues Therapieprinzip, seine Entwicklung und Markteinfuhrung.Stuttgart: WVG.
Weindling, Paul. 1991. “Emile Roux et la diphtherie.” In L’Institut Pasteur. Contributions a son histoire.Ouvrage realise a partir des communications presentees au colloque international sur l’histoire de l’Institut Pasteur6–10. juin 1988, edited by Michel Morange, 136–143. Paris: Editions la Decouverte.
Weisz, Georges. 1995. The Medical Mandarins. The French Academy of Medicine in the Nineteenth and EarlyTwentieth Centuries. New York: Oxford UP.
Wimmer, Wolfgang. 1994. “Wir haben fast immer was Neues”: Gesundheitswesen und Innovationen der Pharma-Industrie in Deutschland, 1880–1935. Berlin: Duncker & Humblot.
Zeiss, Heinz and Richard Bieling. 1940. Behring. Gestalt und Werk. Berlin: Bruno Schultz.







![[Adverse events following diphtheria, pertussis and tetanus vaccinations and factors associated with severity]](https://img.pdfslide.net/doc/110x75/635475e9c1c6b761fb0eab55/adverse-events-following-diphtheria-pertussis-and-tetanus-vaccinations-and-factors.jpg)






















