Embed Size (px)
Citation preview
The
contribution
of community
pharmacy to
improving the
public’s health
REPORT 2
Evidence
from the UK
non peer-reviewed
literature
1990–2002
Alison Blenkinsopp
Claire Anderson
Miriam Armstrong
The
contribution
of community
pharmacy to
improving the
public’s health
REPORT 2
Evidence
from the UK
non peer-reviewed
literature
1990–2002
Alison BlenkinsoppProfessor of the Practice ofPharmacy, Department of Medicines Management,Keele University
Claire AndersonDirector of Pharmacy Practiceand Social Pharmacy,The Pharmacy School,University of Nottingham
Miriam ArmstrongChief Executive,PharmacyHealthLink

There are three reports in this series:
Report 1 Evidence from the peer-reviewed literature 1990 – 2001
Report 2 Evidence from the non peer-reviewed literature 1990 – 2002
Report 3 An overview of the evidence-base from 1990 – 2002 and
recommendations for action
Limited copies are available from PharmacyHealthLink at
1 Lambeth High Street, London SE1 7JN
Tel: 020 7572 2265
E-mail: [email protected]
Registered charity no: 1021335
Registered company no: 2768032
Published by the charity PharmacyHealthLink (previously known as the
Pharmacy Healthcare Scheme) and the Royal Pharmaceutical Society of Great
Britain, 1 Lambeth High Street, London SE1 7JN
First published 2003
© PharmacyHealthLink and the Royal Pharmaceutical Society of Great
Britain, 2003
Printed in Great Britain
ISBN 0 9538505 5 2
All rights reserved. No part of this publication may be reproduced, stored in
a retrieval system, or transmitted in any form by any means, without prior
permission of the copyright holder.
The publisher makes no representation, express or limited, with regard to
the accuracy of the information contained in this document and cannot
accept any legal responsibility or liability for any errors or omissions that
may be made.
The views expressed in this document are those of the authors and are not
necessarily intended to reflect the current policies of the Royal
Pharmaceutical Society of Great Britain or the charity PharmacyHealthLink.
CONTENTS
Joint Foreword by Sian Griffiths, Chair ofPharmacyHealthLink and David Haslam, Chairman ofCouncil of the Royal College of General Practitioners
Executive summary 1
1 Introduction 9
Aim of the review 9
Scope of the review 10
Activities included / excluded 10
Criteria for inclusion of evidence 11
Health Development Agency’s standards:Evidence Base 2000 11
National Service Frameworks: categorisation of evidence 12
2 Method 13
Identifying non peer-reviewed research 13
Review of research quality 13
Data abstraction and construction of the review 14
3 Results 15
Studies included and excluded 15
Presentation of findings 16
Health topics 17
Smoking cessation 17
Coronary heart disease – the use of aspirin in prevention 18
Drug misuse 19
Sexual health 20
Emergency hormonal contraception 21
Immunisation 26
Head lice 27
iii
Oral health 29
Mental health 30
Prevention of transmission of infection 31
Accidental injury prevention 32
Factors affecting the effectiveness of community pharmacy-based activities to improve health 33
Training 33
Use of pharmacy patient medication records 34
Design and use of pharmacy premises 35
Stakeholder views 40
Pharmacy users 40
Pharmacists 44
External stakeholders 50
4 Discussion 53
Scope and quality of the material 53
Where does the non peer-reviewed literaturesupport the findings of the peer-reviewed literature? 53
What new evidence does the non peer-reviewed literature contribute? 54
Health topics 55
Factors affecting the effectiveness of community pharmacy-based activities to improve health 55
Stakeholder views 56
5 Conclusions 59
References 61
Appendices
1 National Service Frameworks: categorisation of evidence 63
2 Details of reviewed evidence 64
iv
ACKNOWLEDGEMENTS
Principal authors
Professor Alison Blenkinsopp, Professor of the Practice ofPharmacy, Department of Medicines Management, KeeleUniversity
Dr Claire Anderson, Director of Pharmacy Practice andSocial Pharmacy, The Pharmacy School, University ofNottingham
Miriam Armstrong, Chief Executive, PharmacyHealthLink
Peer reviewer
Dr Alison Hill, Director of the Public Health ResourceUnit, Institute of Health Sciences, University of Oxford
Steering Group
Dr Terry Maguire, Vice Chair, PharmacyHealthLink (andSteering Group Chair)Dr Michael Varnam, Non-executive Director, HealthDevelopment AgencyNigel Graham, Head of Practice Directorate, RPSGB Dr Sue Ambler, Head of Practice Research Directorate,RPSGBZoe Whittington, Practice Research Manager, RPSGB
The Steering Group would also like to acknowledge theimportant contributions of certain individuals andorganisations to the production of this document. Inparticular Gul Root and Stephen Johnson from theDepartment of Health (England), Chris Miller fromSchering UK, the UK Schools of Pharmacy and ProfessorRoger Walker, Cardiff University and Professor ChristineBond, Aberdeen University for their comments on earlierdrafts.
v

FOREWORD
Since the first report in this series1 became available, themodernisation of the National Health Service across theUnited Kingdom and community pharmacy’s role withinthat has steadily progressed. The plans set out by the UKGovernment2 and devolved administrations3 outlined avision for developing the NHS and pharmacy services thatgave the needs of those who use the service much higherpriority and, especially, focused on improving access tocare.
Many initiatives that were outlined in those plans – forexample proposals for supplementary prescribing andLocal Pharmaceutical Service pilots – have now begun tobe put into practice and their potential for improvingservices to patients will soon become apparent. Bothgeneral medical practice and pharmacy have beenequally affected by these developments, which haveoften served to bring the two professions closer togetherto deliver better patient care.
One area for development that still remains relativelyunexplored is the potential contribution that communitypharmacy can make to improving the public’s health andhow it can work more closely with general medicalpractice to achieve this. In some instances – for examplein smoking cessation4 – there is a relatively good historyof co-operation between general practice, the NHSsmoking cessation services and community pharmacyacross the UK which has served to ensure that patients
vii
1 Anderson C, Blenkinsopp A and Armstrong M (2003). The contribution of community pharmacy to improving the public's health. Report 1: Evidence fromthe peer-reviewed literature 1990 – 2001. Launched at the British Pharmaceutical Conference inSeptember 2001 and is available on the website: www.rpsgb.org.uk/patientcare/.
2 For example, see the Department of Health policy documents: The NHS Plan: a plan for investment.A plan for reform (2000) and Pharmacy in the future: implementing the NHS Plan (2000).
3 For example, see the Scottish Executive documents: Our National Health: A plan for action, a plan for change (2000) and The right medicine: a strategy for pharmaceutical care in Scotland(2002); and the National Assembly for Wales document: Improving health in Wales – a plan forthe NHS and its partners (2001) and the Welsh Assembly Government consultation document:Remedies for success: a strategy for pharmacy in Wales (2002).
4 A survey of all UK NHS commissioning bodies was undertaken in 2002 to assess the existing number of health improvement projects that involved community pharmacies. The findingsindicated that the most common health topic by far for community pharmacists to be involvedwith was smoking cessation and that these projects were evenly spread throughout the UK. Seethe report Local pharmacy health development projects – testing models of implementation incommunity pharmacy (2002) – unpublished work available on request [email protected] or 020 7572 2265 – for more details.
have access to a comprehensive ‘stop smoking’ service ata local level. In other areas of prevention however – forexample sexual health and drug misuse services – there ismuch less evidence that these services are either inexistence or that there are plans for their development.
The main purpose of the second report is to outlineadditional evidence from the non peer-reviewedliterature indicating which health improvement topicsmight be appropriately tackled within a communitypharmacy setting and how these are best delivered.Relevant findings from the first report have also beenincluded to help this assessment.
In addition this report provides much more detail on therelationship between, and attitudes of, the differentstakeholders concerned with improving the public’shealth in a community pharmacy setting. Pharmacy users’views, in particular, provide a very interesting perspectiveon service provision that we hope will encourage healthservice planners and general medical practitioners tothink more broadly about how the ‘added value’ of easyaccess to community pharmacies might help deliver theirpublic health objectives.
Professor ProfessorSian Griffiths David HaslamPresident Chairman of CouncilFaculty of Public Royal College of GeneralHealth Medicine Practitioners
viii

EXECUTIVE SUMMARY
Aim
To identify and critically appraise the non peer-reviewedUK research on the contribution of communitypharmacists to improving the public's health.
Background
Community pharmacies and pharmacists have thepotential to contribute to the public’s health and there isa history of over two decades of developmental work inthis setting in the UK. The position of communitypharmacies straddles both public and private sectors, theformer primarily through a nationally-negotiated NHScontract to dispense prescriptions. Pharmacies’ dualhealth and commercial roles offer a unique opportunityto target activities towards healthy people as well asthose with existing health problems. For this to occur inthe most effective way, service commissioners need accessto the evidence of potential benefit – hence the currentliterature review.
Method
Sources of non peer-reviewed literature were identifiedthrough key informants, and a survey of academicdepartments of pharmacy and related subjects. Criteriawere developed for a review of research quality and a listof inclusion criteria for the review was constructed.
Results
In total, 45 studies were identified, 37 of which wereincluded in the review. The most common reason forexclusion was a low survey response rate. Communitypharmacists (27 studies), pharmacy users (22 studies) andprimary health care team members (7 studies) were themost frequently included participant groups. Twelvestudies involved the investigation of both pharmacist andstakeholder attitudes towards pharmacists’ role in healthimprovement. Thirteen studies addressed general healthissues and 24 covered specific health topics, of which the
1
most commonly studied were sexual health, includingemergency hormonal contraception (9 studies) and headlice management (4 studies).
Many of the findings from this review confirmed, oradded further information to, the findings from thepeer-reviewed literature (Report 1 of this series). To helpidentify the key discussion points the main findings ofthis report have been presented as answers to variousquestions.
Where does the non peer-reviewed literature provide confirmatory evidence of the findings of thepeer-reviewed literature?
The non peer-reviewed literature supported the findingsfrom the peer-reviewed literature in the following areas:
• Both community pharmacists and pharmacy users perceive pharmacists’ roles in improving the public’shealth to be primarily medicines-related.
• Public use of community pharmacies is almost universal but is low for general health advice.
• The actual experience of service users is generally more positive than their prior perceptions of accessto, and value of, advice and services from communitypharmacies.
• Pharmacists have concerns about the receptiveness of GPs and the public to any extended role for them inhealth improvement and, as a result, their willingnessto opportunistically offer general health advice isreduced.
• Pharmacy patient medication records were found to be effective in identifying ‘at risk’ patients to promptand enable pharmacist intervention for influenzavaccination.
• Training has a positive effect on pharmacists’ consultation and information-giving behaviour.
2
3
Where does the non peer-reviewed literature providenew evidence?
New or additional evidence was found in the followingareas:
Health topics
• Drug misuse services – the studies reviewed found that most drug misusers value community pharmacy-based services highly. Positive pharmacist attitudeswere correlated with higher levels of service provisionfor drug misusers but practising pharmacists hadmore negative opinions than undergraduatepharmacy students.
• Sexual health – public interest in the availability of advice on contraception and safer sex throughpharmacies is high. Whilst pharmacists expressconsiderable support for their involvement inpromoting safer sex and contraception, they reportthat they are rarely asked for such advice, and theyare reluctant to offer it proactively.
• Emergency hormonal contraception (EHC) – the review extended the available evidence on EHCsupply through community pharmacies, particularlythrough feedback from some 1600 users in threemajor studies. Pharmacy supply of EHC enables mostwomen to receive it within 24 hours of unprotectedsexual intercourse and services were highly rated bywomen. Feedback from pharmacist providers wasmainly positive and there was a clear wish to extendthe use of Patient Group Directions to enable supplyto under-16-year-olds.
• Head lice management – evidence based on evaluations of over 8600 head lice consultations intwo community pharmacies was reviewed. Qualityindicators included the percentage of consultationswhere no treatment was provided, requirements forproof of infestation, adherence to local treatmentformularies and feedback from users, pharmacistproviders and other health professionals. Overall
one-quarter to one-third of consultations resulted inno treatment being supplied. Adherence to treatmentformularies by community pharmacists was close to100%. Feedback from scheme users, pharmacistproviders and other health care professionals waspredominantly positive.
Factors affecting community pharmacy-basedactivities to improve health
The review extended the evidence on pharmacy users’views on privacy and confidentiality in the pharmacy.Most pharmacy users of potentially sensitive services – forexample EHC and head lice management – reportedadequate facilities for privacy in community pharmacybut a sizeable (up to 20%) minority consistentlyexpressed some concerns. The perceived concerns ofpharmacy users about privacy, however, are generally notborne out in the reports of actual experience, althoughcommunity pharmacists and users appear to havedifferent perceptions of what constitutes acceptablefacilities for maintaining privacy. Up to 20% of womenobtaining EHC from community pharmacies reportedhaving concerns about confidentiality and this washigher among those under 19 years of age.
The review showed that while community pharmacistsconsider leaflets to be an important component of theirtoolkit for improving the public’s health, passive displaysof leaflets may be missed by half of pharmacy customers.Multimedia technology appears to be a means ofengaging young and healthy pharmacy customers inhealth improvement activities.
Stakeholder views
The non peer-reviewed evidence shows that the newcommunity pharmacy service developments in EHC supplyand head lice management were well received by otherprimary care health professionals. The extent of sustainedjoint working between community pharmacists and othermembers of the primary health care team was low(although it is noteworthy that these studies were from
4
5
the mid-1990s). There was some evidence that jointworking might be improved by joint training.
Where does the non peer-reviewed literature indicatepotential for further development?
The following areas were identified as being worthy offurther research and investigation of feasibility:
• Use of aspirin in the prevention of coronary heart disease – pharmacists are perceived by people takingprophylactic aspirin as an appropriate potentialsource of advice on aspirin and heart disease. Thesepatients have unmet information needs that theyperceive could be met by pharmacists but generallythis is not done at present.
• Oral health – the evidence indicates that a more proactive approach by community pharmacists isneeded to maximise opportunities for improving oralhealth. Most requests for paediatric over-the-countermedicines in pharmacies were for named medicines,indicating that active intervention from thepharmacist would be needed to change purchasingpatterns towards sugar-free alternatives. Training andparticipation in oral health promotion activitiesappeared to increase pharmacists’ efforts to try tochange people’s medicine-buying behaviour.
• Mental health – little evidence was found on community pharmacist involvement in improvingmental health. A study of pharmacy users, however,showed that they purchase products to reduce stressand anxiety and take up leaflets available inpharmacies on these topics – particularly on sleepproblems and relaxation – indicating that there maybe a role for pharmacists to proactively offer moresupport. The vast majority of pharmacy users, though,did not name the pharmacist as their preferred sourceof advice on stress and anxiety.
• Prevention of transmission of infection – community pharmacists were found to have generally positiveattitudes towards involvement in prevention oftransmission of infection but to have variable
knowledge about the transmission of HIV, hepatitis Band hepatitis C. In conjunction with the findings fromimmunisation and drug misuse services, there appearsto be potential for further exploring the healthprotection role of community pharmacists.
• Accidental injuries: falls prevention – a pharmacy-based osteoporosis screening service involvingpharmacist and nurse input in one pharmacy wasfound to be feasible and identified women at risk ofosteoporosis. Women using the scheme valued theaccessibility offered by community pharmacy.
• Accidental injuries: medicines-related injuries – a study of unwanted medicines returned to communitypharmacies during a local campaign showed thatchanges in therapy and adverse effects fromtreatment were key reasons why excess quantities ofmedicines occurred in people’s homes. Subsequentdiscussions between the pharmacists and local GPsappeared to be useful for making changes inprescribing frequency to reduce wastage.
Discussion
The search of non peer-reviewed literature identifiedsome high quality research studies that usefullycontributed to the evidence base. In particular, studiesprovided a wealth of further evidence of users’ andstakeholders’ feedback on pharmacy services, identificationof the key elements of effective pharmacy-based healthimprovement activities and on the effectiveness ofvarious approaches to different health topics.
The non peer-reviewed studies were graded using thesame framework for research quality as that used forpeer-reviewed studies and hence were considered againstthe same standards.
The non peer-reviewed literature confirms some of thekey findings from the peer-reviewed literature (Report 1).Firstly, community pharmacists are generally viewed bythe public as experts who advise on medicines ratherthan on health and illness. Secondly, members of the
6
7
public report they are willing to receive furtherinformation on health issues from communitypharmacists but are not currently receiving this advice.Thirdly, community pharmacists can provide effectivehealth improvement activities for: smoking cessation;coronary heart disease prevention; immunisation (andidentification of high risk cases for intervention by usingpatient medication records); supply of EHC; head licemanagement; and drug misuse services. Lastly, traininghas the potential to significantly change communitypharmacists’ behaviour and positively orientate theirpractice towards health improvement.
In addition the ‘grey’ literature provided further detailsabout the perceived problems and acceptability ofcommunity pharmacists providing advice and services onsensitive health issues, such as the supply of EHC andhead lice management. Specifically there were importantfindings on pharmacy user perspectives of privacy andconfidentiality. Most users of these services reportedsatisfaction with the level of privacy available, but20–25% felt there was insufficient privacy. These findingssuggest that pharmacists need to consider whether theirpremises provide sufficient privacy to meet the needs ofall users. Data on perceptions of confidentiality ofpharmacy information came from EHC service users andindicate that about 20% had concerns aboutconfidentiality. These findings suggest that the pharmacyprofession should consider additional ways of informingthe public about the requirement for pharmacists tomaintain confidentiality.
The non peer-reviewed literature also demonstrates thepotential of community pharmacies to contribute toreductions in health inequalities. People living indeprived areas and who are less affluent are among themost frequent users of pharmacies.
Conclusion
The non peer-reviewed literature strengthens the overallpicture of evidence by: confirming the key findings ofReport 1; adding new material on specific health topics

and on the relationships between community pharmacistsand the primary health care team; and providing furtherinsights into pharmacist and user attitudes andbehaviours.
Users express a high degree of interest in the availabilityof further information and advice from pharmacists,although the pharmacist is not seen as a primary source.The research findings suggest considerable scope for jointworking of pharmacists, pharmacy users and healthcarecommissioners to develop pharmacies as a local andaccessible advice point complementary to existingservices.
Further research is needed to investigate the potentialrole of the community pharmacist in sexual health, oralhealth, mental health, the prevention of transmission ofinfection and accidental injuries. Research is also neededto track the development of collaborative workingbetween community pharmacists and other members ofthe primary health care team within the new NHSinfrastructure, and to measure any change in the public’sperception of the pharmacist’s role in providing healthimprovement activities. Evaluation of innovativeapproaches to services and premises development willalso be crucial to informing service design to meet theneeds of users, particularly in relation to queries aboutapproaching the pharmacist for general health adviceand perceptions about privacy and confidentiality.
8
9
1 INTRODUCTION
During the last decade there has been considerableinterest and activity in research into the public healthrole of community pharmacies. Despite an increasingnumber of initiatives (including a recent EuropeanCommission project)1 there were no recent reviews of thestrength of evidence for the wider implementation ofpublic health programmes in community pharmacies. Inaddition there was a broader need to clarify definitionsused to describe public health activities in pharmacies, toidentify which activities were most suited to a communitypharmacy setting and to determine which activitieswarranted further research investment.
To help address these issues the charityPharmacyHealthLink and the Royal PharmaceuticalSociety of Great Britain commissioned a critical review ofthe UK and international literature relating to thecommunity pharmacy’s contribution to improving thepublic’s health as part of a wider work programme todetermine what activities are most likely to be effectivein a community pharmacy setting and how they mightbest be provided.
Report 1 reviews the findings of the peer-reviewedliterature, which includes peer-reviewed journals andconference proceedings. Report 2 reviews the non peer-reviewed literature and examines aspects ofimplementation in more detail. The final report (Report3) summarises all the material reviewed and makesrecommendations for action.
Aim of the review
The aim was to identify and critically review the nonpeer-reviewed UK research on community pharmacists’contribution to improving the public’s health. Non peer-reviewed (‘grey’) literature was defined as research thatwas produced as a formal report or thesis but where thefindings were not available in peer-reviewed journals.
1 See www.univie.ac.at/phc for more details on this initiative.
Scope of the review
DefinitionsThe review included activities described by the followingwidely used definitions of health promotion and publichealth:
• Health promotionThe Ottowa Charter for Health Promotion (WHO, 1986)2
states that ‘Health promotion is the process of enablingpeople to increase control over, and to improve, their health’.
• Public healthPublic health has been defined as ‘the science and art ofpreventing disease, prolonging life and promoting healththrough the organised efforts of society’ (Achesoninquiry into the future development of the public healthfunction, 1988).3
Activities included / excluded
Specifically, the review included pharmacy activities forboth individuals and wider communities relating to:
• Promoting health and well-being (e.g. nutrition, physical activity).
• Preventing illness (e.g. smoking cessation, immunisation, travel health).
• Identifying ill health (e.g. screening and case finding).
• The maintenance of health for those with chronic or potentially long-term conditions (e.g. diabetes,asthma, hypertension).
The advice-giving role of the pharmacist in relation tothe treatment of acute self-limiting conditions, themanagement of minor illness, prescribing andprescription reviews was not included because it has beencovered elsewhere.4
10
2 WHO (1986). Ottowa Charter for Health Promotion. First international conference on Health Promotion, Ottowa, 21 November 1986. Geneva: World Health Organisation.
3 Public health in England: the report of the Committee of Inquiry into the future development of the public health function, Cm 289, 1988. London: The Stationery Office.
4 See, for example, The Public’s Use of Community Pharmacies as a Primary Health Care Resource (1998) – research carried out by the University of Manchester School of Pharmacy and the NationalPrimary Care Research and Development Centre for the Community Pharmacy Research Consortium.
11
The literature review focused on activities taking placewithin the community pharmacy setting or activitiescarried out by community pharmacists and their staff inother settings, for example, nursing homes. The work ofpharmacists in primary care and strategic roles wasincluded where relevant.
Criteria for inclusion of evidence
The majority of dissemination of research is based on ahierarchy of evidence with the randomised controlledtrial (RCT) as the ‘gold standard’. The literature in thefield of pharmacy practice/public health contains fewRCTs, and a substantial number of experimental studiesand descriptive work. This review used two approaches toassess the quality of evidence: (1) the HealthDevelopment Agency’s Evidence Base 20005 standards fortransparency, systematicity and relevance; and (2) thecategorisation of evidence according to the system usedby the Department of Health in its National ServiceFrameworks.6
Health Development Agency standards: Evidence Base 2000
• Transparency – evidence must include a clear and transparent account of how it was collated, whichsources of information have been consulted, who wasinvolved in collating the evidence, how the work wasfunded, a full disclosure of any analysis and findings.
• Systematicity – evidence identified must display clearly, regardless of the individual study, report orreview methodology, the process through which theevidence was gathered and assessed.
• Relevance – evidence must be judged to be relevant to health improvement, and in this instance to therole of community pharmacy.
5 See, for example, Health Development Agency's website (www.HDA-online.org.uk/evidence/eb2000): Evidence base – quality standards for evidence.
6 See, for example, page 11 of the National Service Framework (NSF) on Services for Older People,Department of Health, March 2001.
National Service Frameworks: categorisation ofevidence
The Department of Health categorises individual studiesaccording to the standard classification set out in itsNational Service Frameworks:
Evidence from research and other professional literature
A1 Systematic reviews that include at least one randomised controlled trial (RCT) e.g. systematicreviews from Cochrane or NHS Centre for Reviewsand Dissemination.
A2 Other systematic and high quality reviews which synthesise references.
B1 Individual RCTs.B2 Individual non-randomised,
experimental/intervention studies.B3 Individual well-designed non-experimental studies,
controlled statistically if appropriate. Includes studiesusing case control, longitudinal, cohort, matchedpairs or cross-sectional random samplemethodologies, and well-designed qualitativestudies, well-designed analytical studies includingsecondary analysis.
C1 Descriptive and other research or evaluation not in B (e.g. convenience samples).
C2 Case studies and examples of good practice.
D Summary review articles and discussions of relevant literature and conference proceedings not otherwiseclassified.
12
13
2. METHOD
Identifying non peer-reviewed research
Two sources were used:
• Key informants in England, Scotland, Wales and Northern Ireland.
• Schools of Pharmacy and postgraduate pharmacy and medicines management departments (n = 20) inEngland, Scotland, Wales and Northern Ireland.
Key informants were contacted and asked to identify anyreports of research involving pharmacists improvinghealth that had not subsequently been the subject ofpublication in peer-reviewed journals. Copies of thereports identified were obtained. The period forcollecting evidence was January 1990 to October 2002.
A named individual in each School of Pharmacy wascontacted by e-mail in February 2002, with a reminder inMarch 2002. Respondents were informed of the contextof the review (the role of the pharmacist in public healthand health promotion) and asked to identify relevantMSc, MPhil and PhD research submitted between 1990and 2002. They were asked to send a copy of the titlepage and abstract from each relevant thesis. Where theabstract contained insufficient information the individualresearch student was contacted to obtain it.
Review of research quality
Each item was read by one of the authors (AB) and thefollowing inclusion criteria were applied:
(i) Reported original research.(ii) Sufficient methodological detail on study
design, sampling and response rate.(iii) Adequate methodological design.(iv) For surveys, response rate: over 50%.(v) Topic within improving health remit.(vi) Reported within review timeframe.
Data abstraction and construction ofthe review
Data (see Appendix 2) were extracted from each itemand summarised under the following headings:
• Identifiers: title, author/s, source type (report, thesis), year of publication, evidence grade (usingDepartment of Health National Service Frameworkscategories – see Appendix 1)
• Objectives
• Study design
• Sample and response rate
• Key findings
• Other comments
A draft containing six items (four proposed for inclusion,two for exclusion) was then read by a second author (CA)and the project Steering Group. There was agreementabout application of the inclusion/exclusion criteria.
14
15
3. RESULTS
Studies included and excluded
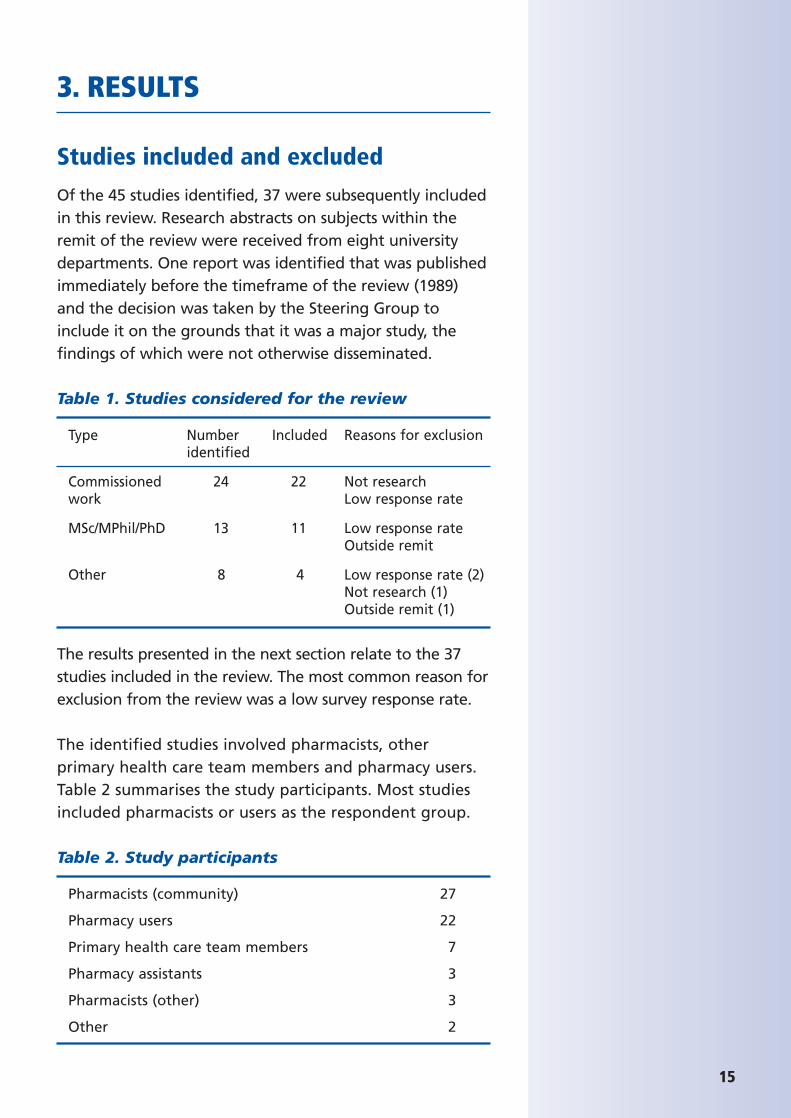
Of the 45 studies identified, 37 were subsequently includedin this review. Research abstracts on subjects within theremit of the review were received from eight universitydepartments. One report was identified that was publishedimmediately before the timeframe of the review (1989)and the decision was taken by the Steering Group toinclude it on the grounds that it was a major study, thefindings of which were not otherwise disseminated.
Table 1. Studies considered for the review
Type Number Included Reasons for exclusionidentified
Commissioned 24 22 Not researchwork Low response rate
MSc/MPhil/PhD 13 11 Low response rateOutside remit
Other 8 4 Low response rate (2)Not research (1)Outside remit (1)
The results presented in the next section relate to the 37studies included in the review. The most common reason forexclusion from the review was a low survey response rate.
The identified studies involved pharmacists, otherprimary health care team members and pharmacy users.Table 2 summarises the study participants. Most studiesincluded pharmacists or users as the respondent group.
Table 2. Study participants
Pharmacists (community) 27
Pharmacy users 22
Primary health care team members 7
Pharmacy assistants 3
Pharmacists (other) 3
Other 2
Ten of the studies involved community pharmacists aloneand eight involved users alone. Twelve studies involvedinvestigating both pharmacist and stakeholder attitudestowards pharmacists’ role in improving the public’shealth. Four studies included data collection onmedicines purchased from or returned to pharmacies. Sixprojects included small scale feasibility trials and one PhDthesis described the development and implementation ofan RCT on community pharmacists’ advice on smokingcessation. The latter was one of five sources where peer-reviewed publications had eventually resulted.
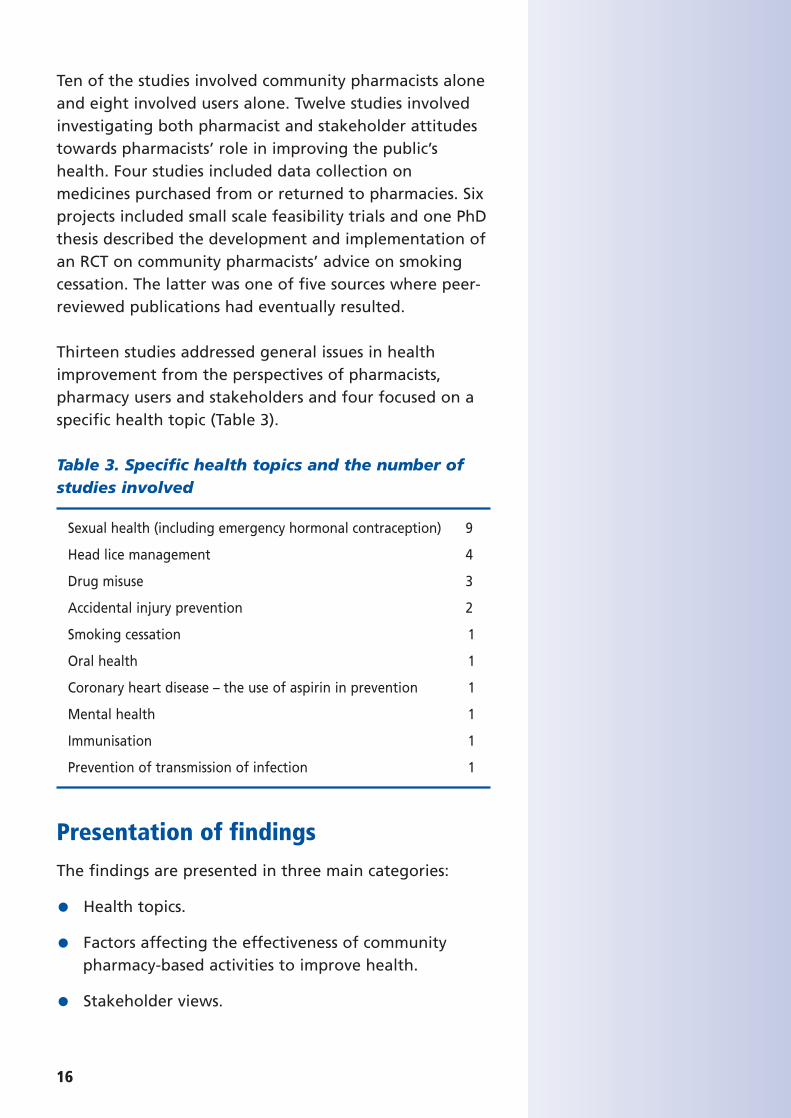
Thirteen studies addressed general issues in healthimprovement from the perspectives of pharmacists,pharmacy users and stakeholders and four focused on aspecific health topic (Table 3).
Table 3. Specific health topics and the number ofstudies involved
Sexual health (including emergency hormonal contraception) 9
Head lice management 4
Drug misuse 3
Accidental injury prevention 2
Smoking cessation 1
Oral health 1
Coronary heart disease – the use of aspirin in prevention 1
Mental health 1
Immunisation 1
Prevention of transmission of infection 1
Presentation of findings
The findings are presented in three main categories:
• Health topics.
• Factors affecting the effectiveness of community pharmacy-based activities to improve health.
• Stakeholder views.
16
17
The findings in the Results section have been presentedin a similar format to Report 1 on the peer-reviewedliterature with the key statements of evidence beinghighlighted in the text. This is followed by a briefsummary of the studies. Further points for analysis ordiscussion appear in side bars to the text. The keyevidence statements are presented in descending orderof strength of evidence (as classified by the Departmentof Health National Service Frameworks grading ofevidence – see Appendix 1).
Some key evidence statements arising from the peer-reviewed literature have been replicated here whererelevant to the findings of the non peer-reviewedliterature.
Please note that the findings presented here summarisethe evidence reviewed for these two Reports only andtherefore each evidence statement needs to beconsidered within the broader framework of factorsaffecting community pharmacy-based services. Thesefactors have been given some consideration in the formof analysis / discussion points for each topic presented inthe Results section of Reports 1 and 2, but a moregeneral overview of these factors and their influence ispresented in the Discussion sections of each report. Theanalysis/discussion points in this document refer to thenon peer-reviewed literature only.
Health topics
Smoking cessation
Relevant finding from peer-reviewed literature:
• Community pharmacists trained in behaviour change methods are effective in helping clients stop smoking(B1).
Key finding from non peer-reviewed literature:
• Training increases knowledge, self-confidence and positive attitude of pharmacists and their staff inrelation to smoking cessation (B1).
The systematic involvement of other pharmacy staff inservice provision was a feature of Sinclair’s trial of theeffect of training (B1: Sinclair 1997, p65). Pharmacy staffand pharmacists were invited to attend joint trainingevents with the intention of developing a practice teamapproach to the service. Training significantly increasedknowledge, self-confidence and positive attitudes aboutthe outcome of counselling in intervention teamscompared with controls.
Coronary heart disease – the use of aspirinin prevention
Relevant findings from peer-reviewed literature:
• Community pharmacy audits can identify self-initiated aspirin treatment and encourage referral for medicaladvice (B3).
• Community pharmacy-based monitoring of the use of prophylactic aspirin treatment shows promise butmore evidence is needed (B3).
Key findings from non peer-reviewed literature:
• The pharmacist is perceived by pharmacy users to be an appropriate potential source of advice on aspirinand heart disease (C1).
• Pharmacists are not perceived by patients taking aspirin to be currently providing the advice they need(C1).
• Patients taking aspirin prophylactically have unmet information needs that could be provided for bycommunity pharmacists (C1).
The pharmacist was found to be considered a highlyappropriate source of advice on both aspirin andcoronary heart disease (CHD) prevention in a telephoneinterview study with 108 people receiving aspirin (C1:Kinghorn 1998, p65). However, pharmacists were notconsidered to be providing this service currently, andperceived lack of privacy in pharmacy premises was anissue. The research identified information needs inrelation both to aspirin itself and CHD and its prevention.
18
Analysis / discussion point:The research findings showpotential benefit from a wholestaff approach in communitypharmacy, although there are nocomparative data whenpharmacists alone have providedthe service. Further research intothe effects of communitypharmacy team approaches onservice provision capacity, quitrates and number of peoplesetting a ‘quit date’ is needed.
Analysis / discussion point:The research findings suggest thatpatients taking aspirinprophylactically need moreinformation and advice than theyreceive at present and would findthe community pharmacist anacceptable source for this.Pharmacy users, however, reportnot receiving this advice possiblybecause patients are reluctant toask for further information, butalso perhaps because a lack ofprivacy was cited as an issue bysome. Given the clear evidence ofbenefit from prophylactic aspirinuse in the prevention of CHD andthat monitoring of the use ofaspirin purchased over the counterfrom community pharmacies isfeasible, primary careorganisations should be aware ofhow community pharmacy-basedservices might be integrated intolocal service provision as a meansof reducing rates of heart disease.
19
The findings indicate patient information needs thatcould be met through pharmacies.
Drug misuse
Relevant findings from peer-reviewed literature:
• Community pharmacy-based supervised methadone administration services can achieve high attendancerates and can be acceptable to clients (B3).
• Specific training needs have been identified for pharmacists participating in pharmacy-based needle-exchange schemes (C1).
Key findings from non peer-reviewed literature:
• Most drug misusers value community pharmacy-based services highly (B3).
• Practising pharmacists appear to have more negative opinions about drug misusers than undergraduatepharmacy students (B3).
• Positive pharmacist attitudes are correlated with higher service provision for drug misusers (B3).
• Training for pharmacists needs to include skills in translating technical terms into a suitable languagefor drug misusers (C1).
Three studies were identified, the first investigated theattitudes of pharmacy undergraduates, pharmacists andclients towards the pharmacist’s role in HIV and drugmisuse (B3: Sheridan 1995, p66), the second describedclient queries addressed to a pharmacist in a primary caredrugs agency service (C1: Scott 2000, p67) and the third astudy of community pharmacists and drug users’perspectives on service provision (B3: Matheson 1999,p66). Pharmacy undergraduates and practisingpharmacists were found to have positive professionalopinions and some negative personal opinions about HIVand drug misuse. The practising pharmacists tended tohave more negative personal opinions, suggesting aneffect from practice experience. Drug information queriesfrom drugs agency workers formed the most frequent
Analysis / discussion point:The research has identified arange of issues from service userand provider perspectives thathave implications for professionaleducation and training ofpharmacists and for the planningand organisation of services.Understanding the reasons fornegative attitudes frompharmacists not involved inservice provision will require thecollection of evidence-based datato support or refute pharmacistperceptions. Continued feedbackfrom service users can supply animportant part of this.
category of requests to the pharmacist, with numbersslightly higher for prescribed than non-prescribed drugs(C1: Scott 2000, p67). The key specialist skill required wasreported to be translating technical information intoterms used as part of the ‘drug culture’.
In a national study of attitudes of Scottish communitypharmacists and their practice in relation to services fordrug misusers, a postal questionnaire and interviewswere used. The questionnaire mapped provision ofservices by community pharmacies and exploredpharmacists’ attitudes. More positive attitudes werecorrelated with higher levels of service provision.Pharmacists had concerns about the effects on othercustomers of service provision for drug misusers. Drugmisusers valued services provided by communitypharmacies. The study showed the importance of therelationship between pharmacists, their staff and serviceusers. Some drug misusers reported negative experiencesthat had increased their feelings of stigma (B3: Matheson1999, p66).
Sexual health
Relevant findings from peer-reviewed literature:none relevant.
Key findings from non peer-reviewed literature:
• Public interest in the availability of advice on contraception and safe sex through pharmacies ishigh (B3).
• Quality and confidentiality were identified by pharmacy users as important considerations inselecting a pharmacy for advice on women’s health(B3).
• Pharmacists express support for involvement in promoting safer sex and contraception but are rarelyasked for such advice and are reluctant to offer it (B3).
• Male pharmacists perceive themselves as less knowledgeable and more embarrassed than femalepharmacists in discussing women’s health issues (B3).
20
Analysis / discussion point:The ‘grey’ literature confirms thereis a desire by the public for easyaccess to information on bothcontraception and safer sex (animportant finding in its own rightset against a backdrop ofincreasing rates of infection incertain sexually transmittedinfections and HIV/AIDS) and thatthey would be prepared to receivethis advice from pharmacists. Incomparison, the extent to whichpharmacists can offer adviceappears to be limited by theirtraining (in particular, howcomfortable they feel talkingabout sexual health issues) andtheir willingness to respond toenquiries. Health servicecommissioners need to consider
21
Two studies explored the community pharmacist’s role insexual health issues including safer sex and contraception(B3: Campbell Keegan 1992, p67; B3: Hughes 2000, p68).Although 86% of pharmacists thought that pharmacistshad an important role in promoting safer sex andcontraception, almost three-quarters reported beingasked for advice on contraception less than once a week.The researchers noted that pharmacists generally took areactive role, providing advice when asked (B3: CampbellKeegan 1992, p67). Public interest in the availability ofadvice from pharmacists was high, with 64% agreeingthat they would like more advice from the pharmacist oncontraception and safer sex (B3: Campbell Keegan 1992,p67). In Hughes’ (2002) study, involvement in sexualhealth promotion was found to be limited and to occurentirely as a result of customer queries. Many of thecommunity pharmacists who took part feltuncomfortable with this area of advice.
Community pharmacists’ knowledge of and attitudestowards women’s health were investigated in a study ofpharmacists and users (B3: McAree 2001, p69).Pharmacists, completing a postal questionnaire, reportedthat they were not embarrassed to discuss many sexualhealth issues although some concerns were expressedabout confidence and knowledge deficits. Malepharmacists perceived themselves as less knowledgeableand more embarrassed than did females. Users identifiedfactors that might influence their decision about whetherto use a community pharmacy including quality andconfidentiality.
Emergency hormonal contraception
Relevant findings from peer-reviewed literature:
• Emergency contraception can be effectively and appropriately supplied by pharmacists (B3).
• Pharmacists were positive about their experience of providing emergency hormonal contraception (EHC)(B3).
• Users were satisfied with the service pharmacists provided (C1).
how pharmacies might play agreater part in national and localsexual health strategies and alsoin reducing teenage pregnancyrates. Pharmacists’ access to up-to-date postgraduate training thatincorporates and encouragesnetworking with other localservice providers is likely to becrucial in increasing pharmacists’confidence in dealing with theseissues appropriately andeffectively.
Key findings from non peer-reviewed literature:
• Pharmacy supply of EHC enables most women to receive EHC within 24 hours of unprotectedintercourse (B3).
• Community pharmacies are highly rated by women as a source of supply and associated advice for EHC onprescription, by Patient Group Directions or over thecounter sale (B3).
• A small minority (10%) of women choose pharmacy supply of EHC in order to maintain anonymity (B3).
• Pharmacists report predominantly positive experiences of involvement in supply of EHC throughPatient Group Direction and over the counter (B3).
• Pharmacists wish their services for supply of EHC to develop in order to meet women’s needs at a locallevel, particularly through increased use of PatientGroup Directions to supply under-16-year olds (B3).
• The role of other pharmacy staff in provision of EHC services is reported by pharmacists to be importantbut there are no data to enable assessment of theircontribution (B3).
Six studies on emergency hormonal contraception (EHC)were identified, three explored consumer perspectivesand experiences, two focused on community pharmacistsand one included both. Three surveys investigated theexperiences of consumer and community pharmacists oneyear after EHC became available over the counter (B3:Lambeth, Southwark and Lewisham Health Action Zone2002, p69; C1: Pharmacy Alliance 2002a, p70; B3: PharmacyAlliance 2002b, p71).
Pre-deregulation
Two focus group studies on EHC, one with 14 communitypharmacists (B3: Seston, 2000, p72), the other with 10groups of users (B3: Edwards, 2000, p72) were reviewed.Both were conducted prior to the deregulation of EHCfrom prescription only to pharmacy medicine status.Pharmacists accorded EHC a special status in comparison
22
23
to other POM to P (prescription only medicine topharmacy medicine) switches and supported mandatorytraining. Users were positive about the POM to P switchincreasing accessibility and convenience. The consumerstudy identified the questions that women had aboutsafety and effectiveness of EHC together with ‘myths’about how often EHC could be taken and its effect onfuture fertility. Another study explored the attitudes ofcommunity pharmacists to pharmacy supply of EHC aspart of wider research on the role of pharmacists incontraception and sexual health advice (B3: Hughes 2000,p68). Community pharmacists saw more scope forinvolvement in EHC supply than in other aspects ofcontraception. Pharmacists’ reasons for support for EHCsupply included a perceived increase in their status aswell as a business opportunity.
A study of consumer and pharmacist perspectives onsupply of EHC in the first Patient Group Direction schemein Manchester included a questionnaire and focus groupswith scheme users, interviews with pharmacists and‘mystery shopper’ visits to pharmacies (C1: Anderson et al2001, p70). The scheme was highly-rated by users, whovalued the enhanced access to treatment. Most (85%)were content with the level of privacy available. Similarlymost were satisfied with perceived confidentiality of theconsultation, although those under 19 years of ageexpressed more concerns about this aspect. Some schemeusers had found difficulty in identifying whichpharmacies provided the service and when they wereopen, indicating a need for more effective publicity.Pharmacists were generally positive about theirinvolvement, viewing the scheme as valuable both to itsusers and to the profession of pharmacy. Somepharmacists expressed concerns about the increasedworkload generated by the scheme and about differentremuneration policies of pharmacist employers.
Post-deregulation
User views
Women purchasing EHC, receiving it on prescription orthrough a Patient Group Direction were asked to
complete a questionnaire by the pharmacist one yearafter EHC was deregulated to a pharmacy medicine (C1:Pharmacy Alliance 2002a, p70). From 250 pharmacies thatparticipated in the survey, 785 women (30%) returnedcompleted questionnaires. The results showed that justover half of the EHC was supplied as an NHS medicine,either as a prescription (42.4%) or under a Patient GroupDirection (13.6%), compared to 44% purchasing EHC overthe counter. Almost three-quarters (71%) of the womenaccessed EHC within 24 hours after unprotectedintercourse, an important consideration as the efficacy ofEHC is time-dependent, being most effective if takenwithin 24 hours after intercourse. There was a high levelof satisfaction with the amount of advice andinformation received from the pharmacist. Pharmacieswere highly rated as a suitable place to obtain anddiscuss EHC. Approximately one in ten women citedanonymity as a key reason for pharmacy purchase of EHC.
Women who had accessed EHC through a communitypharmacy Patient Group Direction scheme in one area ofLondon were surveyed as part of the evaluation of theprogramme (B3: Lambeth, Southwark and LewishamHealth Action Zone 2002, p69). In total 315 (20%) womenreturned the survey questionnaire, which was distributedthrough pharmacies participating in the scheme. Overall98% of user respondents were ‘Satisfied’ or ‘Verysatisfied’ with the service. The majority (90%) had felt‘Comfortable’ or ‘Very comfortable’ discussing theirrequest with the pharmacist. Overall one-quarter ofrespondents had concerns about confidentiality with theproportion being higher in women under 20 years of age.
Pharmacist views
In a national survey of community pharmacists’experience of selling and supplying EHC 1426 (64%)responded, of which 94% worked regularly in thepharmacy from which the survey was completed (B3:Pharmacy Alliance 2002b, p71). Almost all pharmacists(98.9%) said they would supply EHC on prescription and89.4% said they would sell it over the counter. Overall20% of respondents were already participating in a
24
25
scheme to provide EHC through a Patient GroupDirection and a further 51% said they would be willingto do so. These figures show a high level of commitmentfrom pharmacists to the supply of EHC and demonstratescope for extending Patient Group Direction supply.
The survey report was able to compare pharmacists’responses with those from a previous questionnaire in1997. In the current survey pharmacists disagreed thatover the counter availability had resulted in increasedpromiscuity or sexual activity, a concern that significantnumbers had expressed in 1997. In addition, pharmacistsdid not agree that they had found it difficult to dealwith teenagers’ requests for EHC, allaying anotherconcern expressed in 1997. These findings demonstratethat practical experience of supplying EHC over thecounter showed previous concerns to be unfounded.Instead pharmacists felt that over the counter availabilityof EHC had provided an opportunity to develop newcounselling skills and 91% reported undertaking trainingto prepare for their new role with EHC.
The survey also asked about pharmacists’ views onsupplying EHC to those under 16 years of age. Whilerespondents were not in favour of supplying EHC tounder-16s as an over the counter medicine, they did notagree that all under-16s requesting EHC from thepharmacy should be referred elsewhere. These findingssuggest that pharmacists wish to use their professionaljudgement when supplying EHC and this is furtherconfirmed by their support for the supply of EHC viaPatient Group Direction to females aged under 16 years.However, of the 284 pharmacists involved in PatientGroup Direction schemes, 66% (136) reported that under-16s were excluded from their local scheme. In addition,respondents agreed that the price of over the counterEHC was a deterrent to women purchasing it. Overall thefindings suggest that pharmacists believe that improvedaccess to EHC is needed for some women through NHSsupply under Patient Group Direction. The survey showedthat pharmacists are actively referring women for whomover the counter EHC is inappropriate to GPs (90%) and
family planning clinics (60%). Pharmacists reportedreceiving little feedback about either positive or negativeexperiences with EHC.
Pharmacists supplying EHC through a communitypharmacy Patient Group Direction scheme in one area ofLondon were surveyed as part of the evaluation of theprogramme (B3: Lambeth, Southwark and LewishamHealth Action Zone 2002, p69). The pharmacists identifiedthe important role of counter staff in managing waitingcustomers. They reported increased professional self-esteem as a result of taking part in the Patient GroupDirection scheme.
Immunisation
Relevant findings from peer-reviewed literature:
• Pharmacy patient medication records can be used for case-finding of ‘at risk’ clients to be invited forimmunisation and can increase the percentage of thetarget group immunised (B3).
Key findings from non peer-reviewed literature:
• Pharmacy patient medication records are effective in identifying and flagging ‘at risk’ patients to promptand enable pharmacist intervention for immunisation(B3).
A feasibility study was conducted of identification of ‘atrisk’ patients for influenza immunisation throughcommunity pharmacies (B3: Williams et al 1993, p73). Asystematic method using pharmacy patient medicationrecords was effectively used to identify such patients. Aquestionnaire given to those patients identified showedthat a significant percentage had not previously hadinfluenza immunisation. In comparison, an opportunisticmethod based on the presentation of influenza-likesymptoms and purchases of relevant over the countermedicines was less effective. The response frompharmacists using the opportunistic method was low andfeedback suggested this was due to lack of remuneration.
26
Analysis / discussion point:The findings from the non peer-reviewed literature demonstratethe high level of user andpharmacist acceptability of thepharmacy supply of EHC and alsothe effectiveness of increasedaccess within the time-sensitiveperiod (72 hours). There is anexpressed wish from pharmaciststo be supplying more EHC underPatient Group Direction,particularly to those under 16years of age and for women whofind the cost of over the countersupply prohibitive. In addition,pharmacy supply of EHC underPatient Group Direction would belikely to lead to pharmacy-basedservices becoming moreintegrated with other localservices and could potentiallyincrease referrals between majorservice providers. Furthermonitoring is needed into the useof, and outcomes of, pharmacysupply of EHC under PatientGroup Direction.
Analysis / discussion point:The literature demonstrates thepotential effectiveness ofsystematically using pharmacypatient m medication records toidentify high risk individuals forimmunisation. It is recommendedthat piloting of this system shouldbegin as soon as possible in theUK.
27
Head lice
Relevant findings from peer-reviewed literature:none relevant.
Key findings from non peer-reviewed literature:
• Pharmacists and health professionals appear positive about the service and express a wish for it to continue(B3).
• The majority of head lice management programmes require proof of infestation before treatment issupplied and between one-quarter and one-third ofconsultations result in no treatment beingrecommended (B3).
• Where treatment is supplied, community pharmacists’ adherence to the local formulary appears to beextremely high (approaching 100%) (B3).
• User feedback shows that head lice management services are generally well-received, but between 18%and 34% of scheme users report having someconcerns about privacy in the pharmacy during theconsultation (B3).
• Work is needed locally to ensure messages about treatment of head lice infestation are consistentbetween pharmacists, GPs, practice staff and schools(B3).
• There is some evidence that the cost of over the counter head lice treatments is a barrier toappropriate use. Community pharmacy supply oftreatment on the NHS should be explored in areaswhere this applies (C1).
Two reports evaluating community pharmacy provision ofhead lice management were reviewed (B3: Philips et al1999, p73; B3: National Pharmaceutical Association 2001,p74). A total of 5710 users accessed a scheme involving32 community pharmacies in three Primary Care Groupsin the three-month evaluation period (B3: Philips et al1999, p73). Most consultations were on behalf of children(76.8%) and were by females (67.4%). Almost all (94%)
of scheme users were exempt from prescription charges.Proof of infestation was required before treatment wassupplied and no treatment was recommended in one-third of consultations. Where treatment was supplied bythe pharmacist it conformed to the local formulary on99% of occasions. The scheme was well received by users,although 18% reported feeling embarrassed to discusshead lice with the pharmacist. GPs and school nursesrated the scheme highly.
A total of 1847 clients accessed a community pharmacy-based head lice management scheme covering twoPrimary Care Groups and 32 pharmacies (later extendedto 47) in Sunderland during a seven-month period (B3:National Pharmaceutical Association 2001, p74). Proof ofinfestation was required for treatment and was shown in77% of consultations, avoiding the use of chemicalinsecticides in 415 cases. The scheme was well received byusers and was rated ‘good’ or better by 82% of users.Roughly one-third said they were not able to have aprivate discussion in the pharmacy. Three-quarters ofusers said they intended to use regularly the head licecomb they had been given as part of the scheme. Almostthree-quarters of GPs reported that the service hadreduced the amount of time they spent dealing withhead lice infestation. Roughly one-third of GPs reportedthey ‘rarely’ (31%) or never (3%) saw the client whenprescribing head lice treatment. Over 90% of healthprofessionals wanted the service to continue and 66% ofGPs wanted it to be extended to cover other conditions.Pharmacists reported that 67% of initial consultationstook between 5 and 10 minutes and 93% said theywould be happy to continue the service.
Communication to enable consistency of informationabout head lice treatment was studied in a survey ofcommunity pharmacists, head teachers of primaryschools, school nurses and GPs in one locality (B3: Thomas2000, p75). The response rates for different groupsranged from 65–90%. Schools were found to provideinformation to parents that was sometimes out of dateand/or at odds with that being given by healthprofessionals. Some of the survey groups had different
28
29
preferences for treatment types, suggesting thatrecommendations would be likely to differ. Thomasconcluded that there was considerable potential forparents to be presented with conflicting and confusinginformation and identified a need to develop aconsistent approach.
In a community pharmacy-based study, staff in 34pharmacies recorded details of requests for head liceproducts on prescription and over the counter (C1:McGovern 2001 p75). Among 184 customers whocompleted a questionnaire, 69% said they intended torepeat the treatment application and 38% said theyintended to treat the whole family or all childrenregardless of whether head lice were found. Quantitiesprescribed and purchased were lower than thoserecommended in relevant guidelines. These findings raiseconcerns that head lice treatments may not be optimallyused, with risks of treatment failure and thedevelopment of resistance.
Oral health
Relevant findings from peer-reviewed literature:
• Pharmacists are asked by their customers to give advice on oral health but training received on thistopic is variable and evidence of their interventions islacking (B3).
Key findings from non peer-reviewed literature:
• Opportunities for pharmacists to recommend sugar-free medicines for children are limited as mostrequests from customers are for a named medicine (C1).
• Training and participation in oral health promotion activities appear to increase pharmacists’ intent to tryto change users’ behaviour (C1).
• Most pharmacy customers say they believe sugar-free medicines are important for children (C1).
• A more proactive approach by pharmacists is required to maximise opportunities for oral healthdevelopment (C1).
Analysis / discussion point:The use of community pharmacy-based services to treat head liceinfestations appears to be well-received by users and other healthprofessionals, although concernsabout privacy are expressed by asignificant minority of users. Thefinding that no treatment wasprovided in one-third of casesindicates that pharmacistsfollowed the protocol requirementfor examination and proof ofinfection. No evidence ofeffectiveness of treatment, orprevention of infestation or re-infestation were reported in thestudies reviewed. Furtherresearch to assess theeffectiveness and cost-effectiveness of these pharmacy-based interventions is requiredtogether with the need for localplanning and co-ordination oftreatment services and messages.
In a study of community pharmacists’ attitudes andpractice relating to sugar-free medicines, baselineinterviews were followed by a pharmacy-based healthpromotion campaign on this topic together witheducational events (C1: McGovern et al 1999, p76). Onre-interview, pharmacists’ attitudes towards sugar-free(SF) medicines were more positive. Many pharmacistsreported taking part in the health promotion campaign,participating in postgraduate education on oral health orreading relevant articles.
Data collection in the same study on sales of over thecounter paediatric medicines showed that most requestswere made for a named medicine and the pharmacist’srecommendation was sought in around 15% of cases.The percentage of pharmacists indicating they wouldattempt to persuade a purchaser of a sugar-containingmedicine to switch to a SF product had increased in thefollow-up interviews. The authors noted thatimprovements had occurred due to the educational andcampaign activities. They concluded that furtherimprovements could be made and that greaterproactivity by pharmacists would be needed (C1:McGovern et al 2000, p76).
Mental health
Relevant findings from peer-reviewed literature:none relevant.
Key findings from non peer-reviewed literature:
• Community pharmacies are used for the purchase of products to reduce stress and anxiety (C1).
• Most (87%) pharmacy users did not regard pharmacists as their preferred source of advice onstress and anxiety (C1).
• Around half of pharmacy staff were aware of relevant local self-help groups (C1).
• Pharmacy users take up leaflets on topics relating to stress and anxiety, with leaflets on sleep problemsand relaxation being most commonly selected (C1).
30
Analysis / discussion point:There appears to be somepotential for community pharmacystaff to be further involved in theprovision of services to promoteoral health. Some limitations onthis role, however, appear to belinked to pharmacy user requestsfor a specific named medicine thatpotentially presents a conflict ofinterest between the pharmacist’srole as a health professionalversus their business interests. Thisis an issue that needs to beaddressed locally through trainingand remuneration of services.Indeed, pharmacists in the studyreviewed seemed to be persuadedby training to try to encouragecustomers to purchase a SFalternative.
Analysis / discussion point:Although a highly-sensitive topic,there appears to be potential forpharmacy staff to offer supportand advice in relation to mentalhealth issues. At present themajority of pharmacy-basedsupport appears to be linked tomedicine sales. Pharmacy users,however, are also looking formore information and additionalsources of help as exemplified byleaflet uptake. In addition, somestaff have knowledge of relevantlocal services but it is not clearwhether this information is easilyaccessible to pharmacy users. Aspharmacists already provide andsuccessfully offer help on other
31
The involvement of pharmacy staff in the managementof stress and anxiety was the subject of a pilot study inone locality (C1: Reilly et al 2001, p77). A trainingevening was held, and a resource manual was producedand distributed to all pharmacies. Pharmacy customerswere asked to complete a questionnaire on frequency ofsymptoms, any treatments purchased and preferredsources of advice; 150 did so (90% response rate). The GPwas the preferred source of advice on stress and anxiety(76%), with friends (36%) and the pharmacist (13%) next.However, 33% of respondents reported that they hadpurchased a remedy to help their symptoms, indicatingopportunities for pharmacy staff to intervene (butinterventions, other than the sale of a product, were notrecorded). Just over half of the 24 pharmacy staffinterviewed were aware of local self-help groups andmight have been able to refer to them (although thestudy did not record whether they intervened or not).Leaflet uptake during the study ranged from 41 to 155per pharmacy with the most popular topics being sleepand relaxation guides.
Prevention of transmission of infection
Relevant findings from peer-reviewed literature:none relevant.
Key findings from non peer-reviewed literature:
• Pharmacists generally have positive attitudes towards involvement in prevention of transmission ofinfection (B3).
• Pharmacists knowledge about transmission of HIV, hepatitis B and hepatitis C is variable (B3).
A survey of community pharmacists found positiveattitudes towards involvement in activities and services toprevent transmission of HIV and hepatitis B and C (B3:Watson et al 2002, p77). Pharmacists’ knowledge aboutblood-borne diseases was found to be variable. The main
sensitive issues (e.g. emergencyhormonal contraception and headlice management) it is feasiblethat support could be extended tomental health issues, however, thecommon barriers to receivingadvice on sensitive topics(especially privacy andconfidentiality) would need to beaddressed before furtherpublicising these services. Inaddition, pharmacy-based servicesshould be integrated into otherrelevant local services, furthertraining provided and outcomesmonitored.
Analysis / discussion point:Pharmacists potentially have asignificant role to play inpreventing and reducing thetransmission of infections (seealso sections on Sexual health andImmunisation), however, currentevidence suggests theirinvolvement is mainly limited toopportunistic travel health advice(see for example, Report 4).1 Themain barriers to their increasedinvolvement are similar to thosecited for health developmentactivities in general, in particular alack of time, remuneration and ofa private area for consultation,however the importance of thetopic concerned and itsimplications for public health aresuch that further exploration andresearch into their potential role isurgently required.
1 Local Pharmacy Health Development Projects – Testing Models of Implementation in Community Pharmacy (2002). Unpublished work available on request from [email protected] 020 7572 2265.
barriers to extended involvement were perceived by thepharmacists to be time, availability of a private area andlack of remuneration.
Accidental injury prevention
Falls prevention
Relevant findings from peer-reviewed literature:none relevant.
Key findings from non peer-reviewed literature:
• A pharmacy-based osteoporosis screening service involving pharmacist and nurse input was found to befeasible and identified women at risk of osteoporosis(B3).
• Women using the scheme valued the accessibility offered by community pharmacy (B3).
One report of a community pharmacy-based osteoporosisscreening service was reviewed (B3: Martin-Hamblin-GfK2002, p78). The study was a small scale pilot in onepharmacy, where 228 women completed a riskassessment questionnaire. Of these, 49 were found to below risk and the remaining 179 had a bone scanconducted by a nurse in the pharmacy, from which 36were found to be osteoporotic and were referred to theGP for treatment. Most users (78%) were either invitedto take part by pharmacy staff or self-referred afterseeing a project poster in the pharmacy. While three-quarters rated the pharmacy as a more convenientlocation than their doctor’s surgery this did notnecessarily translate into intended future service use. Justover half the women said the convenience of thepharmacy would make them more likely to use theservice, suggesting that other factors played animportant part. Most users rated pharmacy staff asvery/extremely accessible (90%) and professional (83%).The nurse’s input was also highly valued, with over 90%rating as very/extremely knowledgeable and as givingvery/extremely clear explanations.
32
33
Medicines-related injuries
Relevant findings from peer-reviewed literature:none relevant.
Key findings from non peer-reviewed literature:
• Requests to patients to return unused medicines to the pharmacy result in large quantities of excessmedicines being identified (C1).
• Changes in therapy, the death of patients and adverse effects are important reasons why excess quantities ofmedicines occur in people’s homes (C1).
• Discussions between local health professionals appear to be useful in making changes to prescribingfrequency to prevent the accumulation of excessmedicines (C1).
A study in which data were collected on unwantedmedicines returned to community pharmacies showedthat the main reasons for return were a change intherapy, the death of the patient and adverse reactions(C1: McGovern et al 2001, p78). The most commonlyreturned medicines were for treating cardiovascularconditions. The authors note that there was someevidence of excessive prescribing. The results of the studywere subsequently discussed locally and changes in thefrequency of prescribing were agreed.
Factors affecting the effectiveness ofcommunity pharmacy healthdevelopment activity
Training2
Relevant findings from peer-reviewed literature:
• Community pharmacists trained in behaviour change methods are effective in helping clients stop smoking(B1).
• Training in smoking cessation techniques increases
Analysis / discussion point:Pharmacists and their staff have asubstantial amount of contactwith older people (who often havea high medicines intake) andpeople who require repeatdispensing during the normalcourse of their work (see sectionon Public use of communitypharmacies, p41). This places themin a good position to be able toidentify where the use ofmedicines may be predisposingthe user, or carer, to accidents inthe home or elsewhere. Thereview of medicines for high orfrequent users (as required bynational and local policies)presents an ideal opportunity forthe pharmacist to initiate adiscussion with the user or carerto identify potential risk factorsand help determine solutions tominimise these risks. Furtherresearch into the pharmacists’ rolein preventing accidents in othertarget groups, for examplechildren and young people, is alsowarranted.
2 See sections on Pharmacists (p44), Smoking cessation (p17), drug misuse (p19) and oral health (p29) for more details of studies reviewed.
pharmacists’ effectiveness in achieving higher quitrates (B1).
• Training in skin cancer prevention enhances knowledge and increases the opportunistic offeringof advice to clients by pharmacists (B1).
• Training increases the length of consultation between pharmacist and clients on health issues (B2).
• Training in health improvement increases the time that community pharmacists spend in consultationwith pharmacy users and also increases usersatisfaction (B3).
• Specific training needs have been identified for pharmacists participating in pharmacy-based needle-exchange schemes (C1).
Key findings of non peer-reviewed literature:
• Training has positive effects on the consultation and information-giving behaviour of communitypharmacy staff (B1).
• Training increases knowledge, self-confidence and positive attitudes of pharmacists and their staff inrelation to smoking cessation (B1).
• Postgraduate training produces positive changes in both attitudes and behaviour of communitypharmacists in relation to health improvementactivities (B3).
• Training for pharmacists needs to include skills in translating technical terms into a suitable languagefor drug misusers (C1).
• Training and participation in oral health promotion activities appear to increase pharmacists’ intent to tryto change users’ behaviour (C1).
Use of pharmacy patient medication records3
Relevant findings from peer-reviewed literature:
• Using pharmacy patient medication records to
34
3 See section on Immunisation (p26) for details of studies reviewed.
Analysis / discussion point:The research evidence identifiesthe effectiveness of training inchanging pharmacists’ practicebehaviours. Training also affectspharmacists’ confidence andattitudes and there is evidencethat pharmacists who haveundergone training will haveincreased involvement in healthimprovement activities. It istherefore key to the successfulimplementation of communitypharmacy-based healthimprovement programmes.
35
identify clients at ‘high risk’ of coronary heart diseaseis an effective method of identifying those most atrisk and instigating health promotion measures (B1).
• Pharmacy patient medication records can be used for case-finding of ‘at risk’ clients to be invited forimmunisation and can increase the percentage of thetarget group immunised (B3).
• Information routinely kept by community pharmacies on dispensed medication enables case-finding ofpatients for interventions in lipid management (C1).
Key findings from non peer-reviewed literature:
• Pharmacy patient medication records are effective in identifying and flagging ‘at risk’ patients to prompt andenable pharmacist intervention for immunisation (B3).
Design and use of pharmacy premises
Privacy,4 anonymity5 and confidentiality6
Relevant findings from peer-reviewed literature:
• Most pharmacy users perceive there is sufficient privacy in the pharmacy to discuss even sensitivesubjects (B2).
Key findings from non peer-reviewed literature:
• Community pharmacists and users appear to have different perceptions of what constitutes acceptablefacilities to maintain privacy (B3).
• Pharmacy users’ perceived concerns about privacy are generally not borne out in their reports of actualexperience (B3).
• Most users of potentially sensitive pharmacy services (e.g. emergency hormonal contraception; head licemanagement) report adequate facilities for privacy in
4 In this report the definition of ‘privacy’ used is: ‘Being able, or having the facilities, to hold aprivate discussion in the pharmacy at a convenient time for the client without being overheard.’
5 In this report the definition of ‘anonymity’ used is: ‘Where the client uses the pharmacy for advice or services with the explicit intention of remaining unidentified and/or untraceable.’
6 Pharmacists have a professional duty of confidentiality to all their clients, including not releasing information gained from a consultation to the client’s doctor without the client’sexpress permission.
Analysis / discussion point:Research findings show thepotential of community pharmacypatient medication records toidentify and target specific groupsof patients. Primary careorganisations need to considerhow this potential can beharnessed to contribute toachieving local health targets.
community pharmacy with a consistently sizeable (upto 20%) minority expressing concern (B3).
• A sizeable minority (up to 20%) of women obtaining emergency hormonal contraception from communitypharmacies reported having concerns aboutconfidentiality and this was higher among thoseunder 19 years of age (B3).
User views
The results of a self-completion questionnaire study ofusers suggests that the public may have a different viewof what constitutes appropriate facilities to enableprivate discussions. The researchers found that ‘two-thirds of the respondents would like to be able to talk tothe pharmacist in private, while only 5% had found andused such facilities to date’ (B3: Aston University/MELResearch 1991, p79).
In her study of the health information needs of peoplebuying aspirin for heart disease prevention, or receivingit on prescription, Kinghorn concluded that ‘pharmacypremises were considered by some to lack privacy’ (C1:Kinghorn 1998, p65).
The most important factor for users considering apharmacist for advice in a study on contraception andsafer sex was the availability of a quiet area, cited by41% of the 224 respondents (B3: Campbell Keegan 1992,p67). Quality and confidentiality of pharmacists’ advicewere identified by users as influencing possible use of acommunity pharmacy advisory service on women’s health(B3: McAree 2001, p69).
In a large interview study with pharmacy users, one-thirdsaid they would be willing to ask about a sensitive orpersonal problem in the pharmacy. Around two-thirdssaid there was insufficient privacy to discuss a sensitiveproblem in the pharmacy and only 18% believed thatprivacy was adequate. Women were significantly morelikely than men to say that they would discuss a sensitiveproblem with the pharmacist (C1: Coggans et al 2000, p79).
36
37
A study of user attitudes towards community pharmacy
supply of emergency hormonal contraception (EHC) prior
to deregulation from POM to P (prescription only
medicine to pharmacy medicine), or supply on Patient
Group Direction, involved 10 focus groups with women
who had used, or might use, EHC (B3: Edwards 2000,
p72). While women were positive about pharmacy supply
of EHC, the open pharmacy environment was a ‘major
concern’. The same study also found that participants
were concerned about confidentiality in the community
pharmacy setting and about what records would be kept
of the supply. It is not possible to tell from the findings
the distribution of these concerns between women who
were expressing their perceptions and those who had
used EHC. However, when pharmacy users are asked
about their actual experience rather than perceptions the
results are quite different as the results of consumer
studies conducted prior to and since wider access through
pharmacies to EHC demonstrate.
In a study of women who had all obtained EHC from
pharmacies by Patient Group Direction, most were
satisfied with the level of available privacy, although
approximately one in five felt there was insufficient
privacy for their discussion with the pharmacist (B3:
Lambeth, Southwark and Lewisham Health Action Zone
2002, p69).
In a national survey of womens’ experience of obtaining
EHC through community pharmacies, the setting was
highly rated as a suitable place to obtain and discuss EHC
by women receiving it on prescription, Patient Group
Direction or through over the counter purchase (B3:
Pharmacy Alliance 2002b, p71).
These findings suggest that many women find it
acceptable to discuss this sensitive subject in a community
pharmacy. The same study found that most women did
not have concerns about confidentiality and pharmacy
supply, although roughly one-quarter of women did.
Most (80%) women using a community pharmacy-basedosteoporosis screening service felt they were treated with‘complete’ privacy and confidentiality, with 18%reporting a ‘degree of privacy’ and 2% giving a negativerating (B3: Martin-Hamblin-GfK 2002, p78).
Just over two-thirds (68%) of the 600 pharmacycustomers interviewed in a Scottish study believed theirdiscussions in the pharmacy would be confidential.Women were significantly more likely than men to saythat confidentiality would be maintained (C1: Cogganset al 2000, p79).
Two reports of community pharmacy-based head licemanagement schemes included an assessment of users’perceptions of privacy. In the first study, 17.6% of 336users reported being embarrassed to speak to thepharmacist about head lice (B3: Philips et al 1999, p73).In the second study, 42% of users agreed that they wereable to discuss their problem in private, 34% said theywere not able to do this and 24% were ‘not bothered’about this aspect (B3: National PharmaceuticalAssociation 2001, p74).
Pharmacist views
The availability of a ‘quiet area’ in the communitypharmacy to provide a setting for private discussion wasexplored in several studies. In a large survey in the late1980s, 62% of community pharmacist respondentsreported that their premises had a suitable area or roomfor private discussion and one in four pharmaciesreported having a ‘consultation room’ (B3: Shafford &Sharpe 1989, p80).
Methods of provision of health information
Use of leaflets
Relevant findings from peer-reviewed literature:
• Awareness of pharmacy-based leaflets on health topics is higher for those clients taking prescribedmedicines (B3).
38
Analysis / discussion point:Feedback from pharmacy usersdemonstrates that pharmacy-based EHC and head licemanagement services are highlyrated. However, although mostusers report finding the level ofprivacy in pharmacies acceptable,a significant minority do not. Inaddition, around one in fivewomen receiving EHC wereunsure whether the informationwould be kept confidential. Thesefindings suggest that althoughcommunity pharmacists can play avaluable role in providing theseservices and believe they currentlyhave adequate facilities to do so,there is a need to be aware that asignificant minority of the publicstill report concerns over privacyand confidentiality. Suggestedaction to address these issueswould include reviewing thefacilities available for privatediscussion in communitypharmacies and greater publicityabout the terms and conditionsfor confidentiality that apply topharmacists and their staff.
39
Key findings from non peer-reviewed literature:
• Community pharmacists consider leaflets to be an important component of their health improvementtoolkit (B3).
• Passive displays of leaflets may be missed by half of pharmacy customers (C1).
The display and use of health promotion leaflets wasincluded in several studies. In Shafford and Sharpes’ largesurvey of community pharmacists 56% of respondentsbelieved leaflets to be of ‘great’ or ‘very great’importance and 45% reported displaying them (B3:Shafford & Sharpe 1989, p80). The findings of that studysuggested that pharmacists gave a higher priority todisplaying leaflets than to providing advice on healtheducation, indicating a preference for passive rather thanactive involvement. However, as passive displays ofleaflets were found to be missed by nearly half ofpharmacy customers (B3: Aston University/MEL 1991,p79), leaflet-based strategies are best viewed assupportive of medicines or health advice, or throughoffering an opportunity for further discussion, ratherthan an end in themselves.
Multimedia technology
Relevant findings from peer-reviewed literature:none relevant.
Key findings of non peer-reviewed literature:
• Multimedia technology may be a means of engaging young and healthy pharmacy customers in healthimprovement activities (C1).
A small experimental descriptive study assessed the usageof a multimedia touch screen kiosk in the communitypharmacy setting (C1: Hariri 1998, p81). Over 12,400people used the kiosk in six pharmacies. Usage was muchhigher in supermarket pharmacies compared with others,however, the completion rate for the software used wassimilar in the two groups at 31% and 37%. Most userswere relatively young (under 40 years) and data collected
on Body Mass Index (BMI) showed the majority to have a‘healthy’ figure of 25 or less. Observation studies showedthat older customers needed encouragement and ademonstration by the pharmacist before they used thekiosk. These results suggest that younger and healthierpharmacy customers are more willing and likely to usecomputer-based information points. The low completionrate suggests that further work is needed to developprogrammes with which this younger group will engagemore fully. The lower technology familiarity of olderpharmacy customers and their high frequency of use ofpharmacies also needs to be taken into account indesigning future strategies.
Stakeholder views
Pharmacy users
Relevant findings from peer-reviewed literature:
• User feedback from pharmacy-based health improvement activities is generally very positive (B3).
• Users’ awareness of community pharmacies as a source of general health advice is low (B3).
• Pharmacy users report having followed the health advice given by pharmacists with positive views onthe pharmacist’s input (B3).
• Most users perceive there is sufficient privacy in the pharmacy to discuss even sensitive subjects (B3).
• Community pharmacy-based supervised methadone administration services can achieve high attendancerates and be acceptable to clients (B3).
• User satisfaction with pharmacy-based immunisation services is high (C1).
• Users were generally satisfied with the emergency contraception service pharmacists provided (C1).
40
Analysis / discussion point:The means of provision of healthinformation to patients is rapidlydeveloping with the introductionof new technologies, for example,portable touch-screen kiosks, andthe public’s increasing access toelectronic information through theInternet. These technologies arealso being applied to the NHSwith the introduction andincreasing use of telephoneadvice-lines (e.g. NHS Direct inEngland) and NHS advice andservices via the Internet (e.g. NHSDirect On-Line). Pharmacists needto consider what are the mostappropriate ways of ensuring theirusers have access to theinformation they need. This cantake a variety of forms, such aswritten information, provided asleaflets or electronically. At thetime of writing there was notsufficient evidence to suggest thatone particular form was moreeffective than another. Instead itappears that different methods ofreceiving health informationdepend on individual userpreferences and characteristics.When a pharmacist, or staffmember, actively engages with aclient about their health needs itis possible to determine whatmethod of information provisionmight suit them best. At othertimes, neither pharmacy users northe pharmacist may be able, orwilling, to engage in furtherconsultation and at these timesthe provision of easily accessiblewritten, or electronic, healthinformation should be available tothose who require it.
41
Key findings from non peer-reviewed literature:
• Public use of community pharmacies is almost universal but is low for general health advice (B3).
• Community pharmacists are perceived as drugs experts rather than experts on health and illness (B3).
• Community pharmacies are highly rated by users as a source of supply and advice for emergency hormonalcontraception and head lice management (B3).
• The actual experience of service users appears to be more positive than their perceptions of access to andvalue of advice and services from communitypharmacies (B3).
The public’s use of community pharmacies
Public use of community pharmacies is high, with 94% ofrespondents in a large (517 adults) interview-basedsurvey having used a pharmacy in the previous year forone of three core reasons: obtaining prescriptionmedicines; ‘over the counter’ medicines purchase; healthylifestyles related advice (B3: BMRB 1996, p81). TheACORN (A Classification of Residential Neighbourhoods)classification was used in sampling.7 Reported use was forprescriptions (90% of respondents), over the countermedicines (30%) and seeking general health advice(10%). Use for general health advice was higher amongwomen, respondents with young children and those fromlower socio-economic groups. Respondents in the‘striving’ ACORN group live in the poorest conditions andcorrespond well with those in the ‘inner city’ group whoare the most frequent users of pharmacies. Overall 14%of respondents reported receiving unsolicited healthadvice from pharmacies. See Table 4.
7 See http://www.caci.co.uk/pdfs/acorn2001.pdf for more information on the ACORN classification.
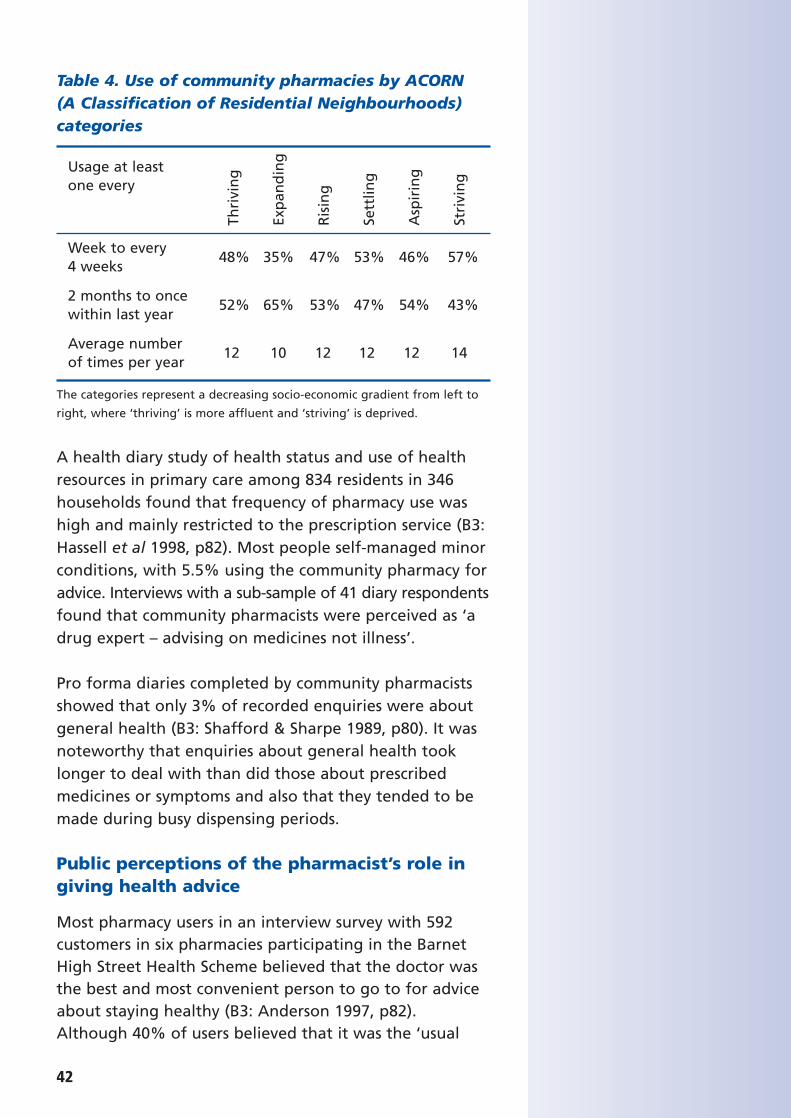
Table 4. Use of community pharmacies by ACORN (A Classification of Residential Neighbourhoods)categories
The categories represent a decreasing socio-economic gradient from left to
right, where ‘thriving’ is more affluent and ‘striving’ is deprived.
A health diary study of health status and use of healthresources in primary care among 834 residents in 346households found that frequency of pharmacy use washigh and mainly restricted to the prescription service (B3:Hassell et al 1998, p82). Most people self-managed minorconditions, with 5.5% using the community pharmacy foradvice. Interviews with a sub-sample of 41 diary respondentsfound that community pharmacists were perceived as ‘adrug expert – advising on medicines not illness’.
Pro forma diaries completed by community pharmacistsshowed that only 3% of recorded enquiries were aboutgeneral health (B3: Shafford & Sharpe 1989, p80). It wasnoteworthy that enquiries about general health tooklonger to deal with than did those about prescribedmedicines or symptoms and also that they tended to bemade during busy dispensing periods.
Public perceptions of the pharmacist’s role ingiving health advice
Most pharmacy users in an interview survey with 592customers in six pharmacies participating in the BarnetHigh Street Health Scheme believed that the doctor wasthe best and most convenient person to go to for adviceabout staying healthy (B3: Anderson 1997, p82).Although 40% of users believed that it was the ‘usual
42
Usage at least one every
Week to every4 weeks
48% 35% 47% 53% 46% 57%
2 months to once within last year
52% 65% 53% 47% 54% 43%
Average number of times per year
12 10 12 12 12 14
Thri
vin
g
Exp
and
ing
Ris
ing
Sett
ling
Asp
irin
g
Stri
vin
g
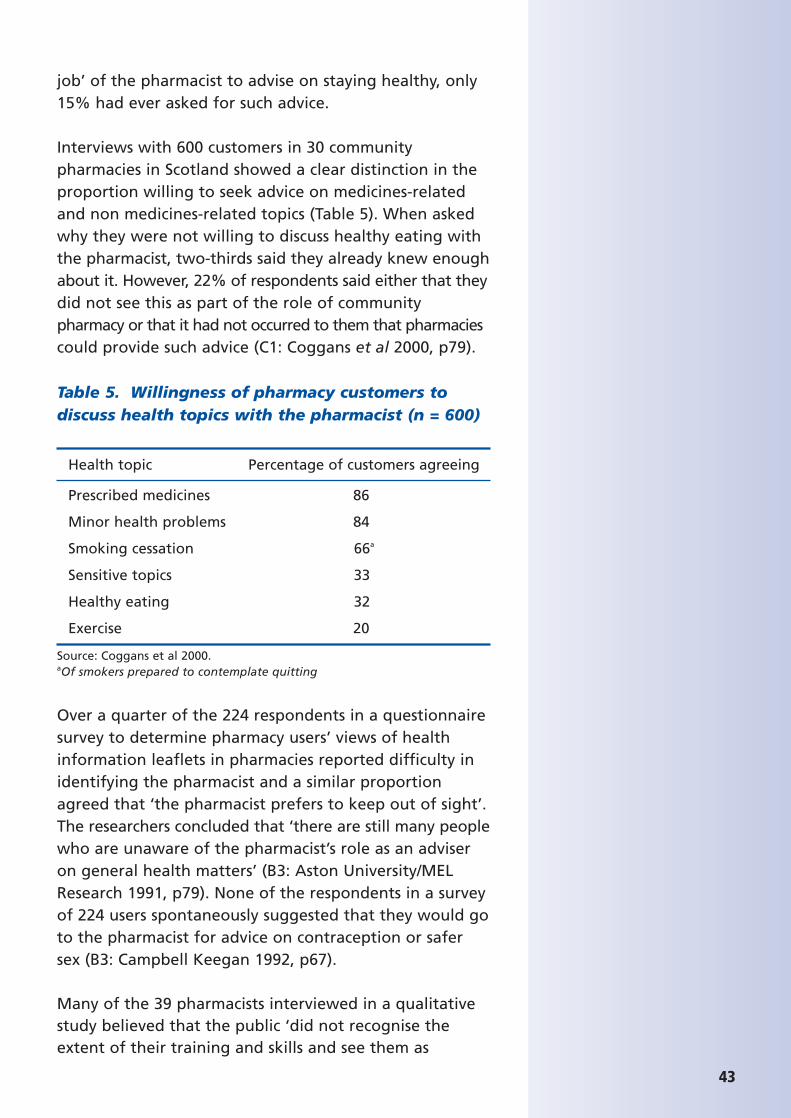
43
job’ of the pharmacist to advise on staying healthy, only15% had ever asked for such advice.
Interviews with 600 customers in 30 communitypharmacies in Scotland showed a clear distinction in theproportion willing to seek advice on medicines-relatedand non medicines-related topics (Table 5). When askedwhy they were not willing to discuss healthy eating withthe pharmacist, two-thirds said they already knew enoughabout it. However, 22% of respondents said either that theydid not see this as part of the role of communitypharmacy or that it had not occurred to them that pharmaciescould provide such advice (C1: Coggans et al 2000, p79).
Table 5. Willingness of pharmacy customers todiscuss health topics with the pharmacist (n = 600)
Health topic Percentage of customers agreeing
Prescribed medicines 86
Minor health problems 84
Smoking cessation 66a
Sensitive topics 33
Healthy eating 32
Exercise 20
Source: Coggans et al 2000.aOf smokers prepared to contemplate quitting
Over a quarter of the 224 respondents in a questionnairesurvey to determine pharmacy users’ views of healthinformation leaflets in pharmacies reported difficulty inidentifying the pharmacist and a similar proportionagreed that ‘the pharmacist prefers to keep out of sight’.The researchers concluded that ‘there are still many peoplewho are unaware of the pharmacist’s role as an adviseron general health matters’ (B3: Aston University/MELResearch 1991, p79). None of the respondents in a surveyof 224 users spontaneously suggested that they would goto the pharmacist for advice on contraception or safersex (B3: Campbell Keegan 1992, p67).
Many of the 39 pharmacists interviewed in a qualitativestudy believed that the public ‘did not recognise theextent of their training and skills and see them as
shopkeepers, not health educators’ (B3: Anonymous1993, p83). Pharmacists who participated in a largequestionnaire study were reported to be ‘keen for thepublic to be better educated about the role of thepharmacist in healthcare in general’ (B3: BMRB 1993, p84).
Users’ experience of advice and services in thepharmacy setting
Several studies were identified that obtained feedback fromusers about advice and services actually received, ratherthan their perceptions of, or attitudes to, receiving them.
Client feedback on the pharmacy supply of emergencyhormonal contraception (EHC) was obtained in twostudies. Women receiving EHC through a Patient GroupDirection in South London showed a high level ofsatisfaction with the service (B3: Lambeth, Southwarkand Lewisham Health Action Zone 2002, p69). A highlevel of satisfaction with community pharmacy supply ofEHC was also found in a national survey of womenreceiving the treatment on prescription, Patient GroupDirection or purchasing it over the counter (C1: PharmacyAlliance 2002a, p70). Pharmacies were highly rated as aplace to obtain and discuss EHC. A desire for anonymitywas the reason why 9.7% of women surveyed had optedfor over the counter purchase of EHC.
Users who received advice on women’s health in a pilotstudy in four pharmacies were reported to respondpositively (B3: McAree 2001, p69).
One study investigated the views of clients of pharmacydrug misuse services (B3: Sheridan 1995, p66). Clientsperceived pharmacists as service providers but not as asource of advice. Some clients reported positive experiencesof their interactions in pharmacies but others consideredthemselves to be stigmatised by community pharmacists.
Pharmacists
Relevant findings from peer-reviewed literature:
• Pharmacists attach a high degree of importance to health improvement activities (B3).
44
Analysis / discussion point:Use of community pharmacies forgeneral health advice tends to below among the public but appearsto be higher among women,respondents with young childrenand lower socio-economic groups.People living in areas ofdeprivation, high unemploymentor in inner cities are morefrequent users of communitypharmacies.
Both the public and communitypharmacists believe that theadvice-giving role of communitypharmacists on general healthissues is not widely recognised orutilised. As service developmentsoccur it may be necessary to runlocal campaigns to raise publicawareness of services on offer andto target those who would benefitmost from increased access, suchas those living in areas ofdeprivation or inner cities. Furtherresearch is required to investigatethe use of community pharmaciesby lower socio-economic groups,particularly in relation to advice-giving as well as the supply ofmedicines.
45
• Pharmacists are more comfortable with health improvement activities that are related to medicinesand need support to extend their portfolio of health-related work (B3).
• Pharmacists’ advice is more likely to be reactive than proactive (B3).
• Pharmacists’ concerns about being ‘intrusive’ in offering potentially unwelcome health advicepredisposes to a reactive stance (B3).
• Pharmacists were positive about their experience of providing emergency hormonal contraception (B3).
• Pharmacy staff appear positive about promoting the role of folic acid in pregnancy but there is no evidenceof the effects of intervention on behaviour (B3).
• Dispensing duties are widely reported as a key barrier to pharmacists’ greater involvement in healthimprovement activities (B3).
Key findings from non peer-reviewed literature:
• Training has positive effects on the consultation and information-giving behaviour of communitypharmacy staff (B1).
• Community pharmacists perceive health promotion activity as important but tend to spend little time onit in everyday practice (B3).
• Future roles in health improvement are largely perceived as medicines-related by communitypharmacists (B3).
• Community pharmacists have concerns about the receptiveness of GPs and patients to a greater role inhealth improvement and thus proactivity is reduced (B3).
• Postgraduate training produces positive changes in both attitudes and behaviour of communitypharmacists in relation to health improvementactivities (B3).
Priorities for advice-giving
Several studies explored where health improvementfeatured in community pharmacists’ priorities for advice-giving. When asked whether they believe that healthpromotion is important, most community pharmacistsagree. In a postal survey only 13.5% of 1330 respondentsrated health promotion as being of ‘little’ or ‘no’importance (B3: Health Promotion Authority Wales 1991,p83). While pharmacists perceive health promotion to beimportant it was also noted that ‘pharmacists’ healthpromotion role is reactive not proactive’ and that ‘thepharmacist’s role is very much oriented towards medicaladvice … health promotion happens during this process(B3: Anonymous 1993, p83). However, the priority thatpharmacists gave to health promotion in relation toother activities provides a different perspective. A surveyof 897 community pharmacists (response rate 58%) foundthat respondents attached ‘great importance’ to advice-giving on prescribed medicines (52%); over the countermedicines (45%) and health education (18%) (B3:Shafford & Sharpe 1989, p80).
The amount of time spent by community pharmacists onhealth promotion activities was estimated as 5% in onestudy (B3: Anonymous 1993, p83) while around three-quarters of pharmacists estimated that they spentbetween one and three hours a week on such activities(B3: BMRB 1993, p84).
Most community pharmacists who participated in a studyon contraception and sexual health saw their role as‘revolving around the provision and sale of medicines’(B3: Hughes 2000, p68). The most commonly mentionedareas for role development in the future in the samestudy were running clinics for diabetes and asthma,managing long-term medication, pharmacist prescribingand health promotion.
Provision of specific services
The numbers of pharmacies providing specific serviceswere measured in a questionnaire survey of allcommunity pharmacists in Wales (B3: Health Promotion
46
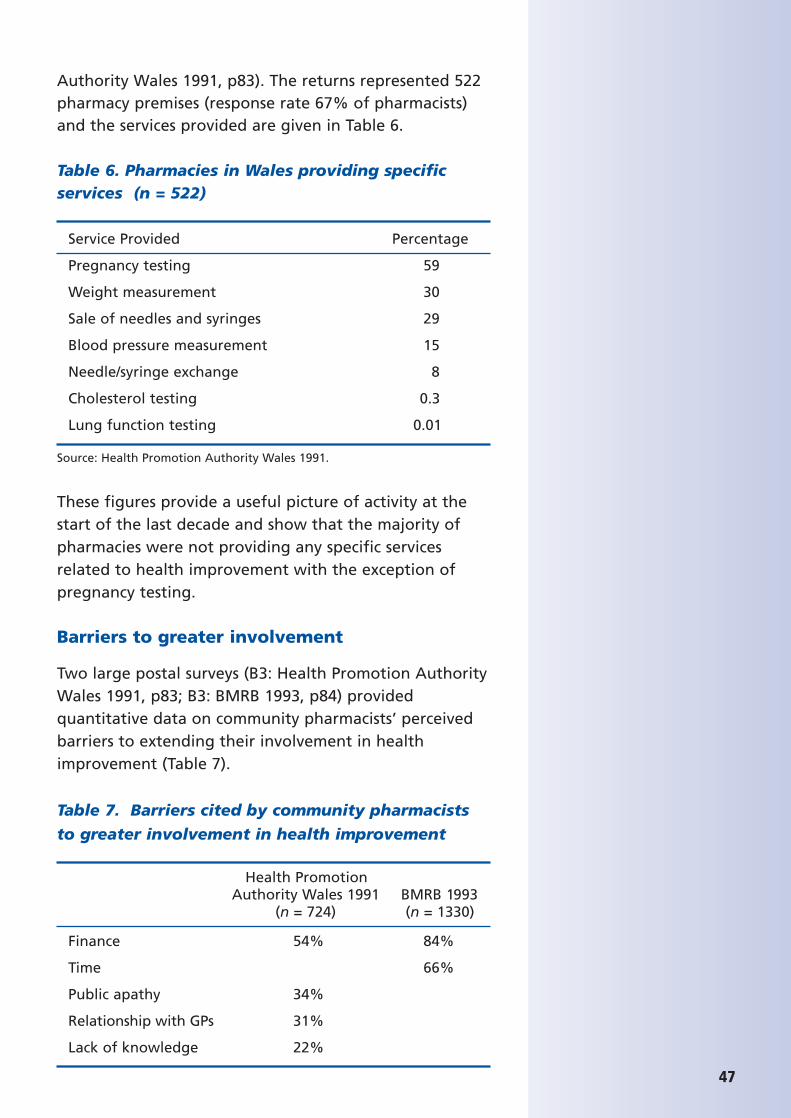
47
Authority Wales 1991, p83). The returns represented 522pharmacy premises (response rate 67% of pharmacists)and the services provided are given in Table 6.
Table 6. Pharmacies in Wales providing specificservices (n = 522)
Service Provided Percentage
Pregnancy testing 59
Weight measurement 30
Sale of needles and syringes 29
Blood pressure measurement 15
Needle/syringe exchange 8
Cholesterol testing 0.3
Lung function testing 0.01
Source: Health Promotion Authority Wales 1991.
These figures provide a useful picture of activity at thestart of the last decade and show that the majority ofpharmacies were not providing any specific servicesrelated to health improvement with the exception ofpregnancy testing.
Barriers to greater involvement
Two large postal surveys (B3: Health Promotion AuthorityWales 1991, p83; B3: BMRB 1993, p84) providedquantitative data on community pharmacists’ perceivedbarriers to extending their involvement in healthimprovement (Table 7).
Table 7. Barriers cited by community pharmacists
to greater involvement in health improvement
Health Promotion Authority Wales 1991 BMRB 1993
(n = 724) (n = 1330)
Finance 54% 84%
Time 66%
Public apathy 34%
Relationship with GPs 31%
Lack of knowledge 22%
Availability of finance and time-pressures werecommonly-perceived barriers that also featured in thepeer-reviewed evidence (Report 1). The Welsh datademonstrated pharmacists’ concerns about thereceptiveness of the public and of doctors to their healthpromotion activities. Perceptions of customers’ responseto health promotion advice were explored in a largequalitative study involving eight discussion groups and 18individual interviews with community pharmacists (B3:Hughes 2000, p68). Pharmacists were typically notproactive in health promotion, feeling that they couldonly respond to customer queries rather than initiatingdiscussions on health. Raising health promotion issueswith most clients was seen as ‘highly problematic’ as thepharmacist had no way of knowing who mightappreciate the advice and who might be offended (B3:Hughes 2000, p68).
Education and training
Undergraduate and pre-registration training
At the end of the 1980s pharmacists perceived that theirundergraduate and pre-registration training had notprepared them sufficiently for a role in healthimprovement. Almost three-quarters of communitypharmacists reported that their undergraduate educationgave them ‘no’ or ‘poor’ training in advice-giving onhealth education topics (B3: Shafford & Sharpe 1989,p80). In relation to pre-registration training, 48% ofcommunity pharmacists stated that their training hadprovided them with ‘no’ or ‘poor’ training in advice-givingon health education (B3: Shafford & Sharpe 1989, p80).
An educational intervention with pharmacy undergraduateswas shown to have a positive effect on knowledge aboutdrug misuse and HIV but a lesser effect on attitudestowards providing services (B3: Sheridan 1995, p66).
Postgraduate training
A questionnaire survey of 100 community pharmacists
48
Analysis / discussion point:Pharmacists’ attitudes to their rolein health promotion
Although the majority ofpharmacists rate their role in healthpromotion as being important,current activity levels are low dueto a reported combination ofbarriers including lack ofremuneration, time-pressures andperceptions of a negative responseto these activities by GPs and thepublic. However, a more recentlyconducted UK survey of currentactivity (Report 4)8 has revealed anexplosion in local communitypharmacy health improvementprojects being run in conjunctionwith NHS primary careorganisations in the following areas:
• smoking cessation;
• sexual health;
• drug misuse;
• prevention of heart disease;
• diabetes awareness;
• obesity and weight reduction;
• accident prevention;
• travel health;
• winter pressures,e.g. immunisation awareness;
• miscellaneous, e.g. campaigns specifically targeted at ethnicminority group, mental healthpromotion.
Further evaluation of these services(including means of remunerationand time spent in these activities)is necessary to accuratelydetermine the extent to whichthese reported barriers exist today.
8 Local Pharmacy Health Development Projects – Testing Models of Implementation in Community. Pharmacy (2002). Unpublished work available on request from [email protected]; 020 7572 2265.
49
(response rate 66%) found that just over half (53%) hadundertaken training in health promotion and overall86% said they would be willing to undertake furthertraining (B3: Dewsbury-Mason 1998, p84).
Pharmacists who received training as part of theirparticipation in a health promotion programme (HighStreet Health, HSH) expressed a desire to spend less timedispensing prescriptions and more time advisingcustomers. Training appeared to have resulted inpharmacists taking a more holistic view of health (B3:Anderson 1997, p82) an approach that is not generallypredominant among community pharmacists withouttraining (B3: Dewsbury-Mason 1998, p84). In addition,covert research on the HSH scheme showed thatparticipating pharmacists spent significantly longer withclients consulting on smoking cessation and that theyused leaflets more proactively (B3: Anderson 1997, p82).
Pharmacists in a focus group study were reported to be‘poor’ at identifying their own training needs in relationto the supply of EHC (B3: Seston et al 2000, p72), forexample, participants expressed concerns about ‘clinical’issues but these were generally ill-defined. There was anidentified need for training in how to conductconsultations for emergency contraception in a non-judgemental way. The need for training on EHC supply tofocus on consultation skills rather than technicalinformation was also found in a large qualitative study ofcommunity pharmacists (B3: Hughes 2000, p68).
In a study of the effect of training on smoking cessationadvice, most pharmacy staff reported that the traininghad led to a change in their consultations with customers(B1: Sinclair 1997, p65). Pharmacy teams that hadreceived training were not only significantly moreknowledgeable about smoking cessation but alsosignificantly more confident and positive about outcomesthan were controls (B1: Sinclair 1997, p65). In addition,customers rated their discussions more highly withpharmacy staff from the intervention group.
Education and training ofpharmacists in preparation for ahealth improvement role
Although pharmacists havereported their undergraduate andpre-registration training carried outin the late 1980s as being ‘non-existent’ or ‘poor’ in preparingthem for an advice-giving role, norecent data to allow comparisonswith the current situation wasidentified during the investigationfor this report.
In contrast, however, pharmacistswho have received post-graduatetraining in health improvement aresignificantly more positive inrelation to their advice-giving roleand expected health outcomes butthese findings should beinterpreted cautiously as it is likelythere is a ‘self-selection’ effect.There are, however, significantbenefits to be obtained for bothpharmacist providers andpharmacy users when pharmacistsundertake specific training in
External stakeholders
Relevant findings from peer-reviewed literature:none relevant.
Key findings from non peer-reviewed literature:
• The extent of sustained joint working between community pharmacists and other members of theprimary health care team is generally low but may beimproved by joint training (B3).
• Primary health care team members expressed some general anxieties about the wider role of communitypharmacy in promoting health but reported havingconfidence in individual pharmacists known to them(B3).
• New community pharmacy service developments such as EHC and head lice management were well-receivedby primary care health professionals (B3).
Extent of pharmacist involvement with primaryhealth care teams
The extent of joint working between communitypharmacists and other primary health care team (PHCT)members was explored using a mix of quantitative andqualitative methods in three studies. In a postal survey of373 community pharmacists (response rate 78%) 14% ofrespondents reported regular meetings with PHCTmembers, and participation in collaborative projects orinitiatives was reported by 13% (B3: Elliott 1996, p84).Some respondents commented that they had wished totake part but had not been invited to collaborate,indicating a reactive stance. Isolation from other healthprofessionals was widely reported in a study of barriersand opportunities to community pharmacists’ widerinvolvement in contraceptive and sexual health advice(B3: Hughes 2000, p68). In a study of advice on women’shealth issues, referrals from community pharmacists toother health professionals were found to be significantlyrelated to a knowledge of local referral procedures andopening hours (B3: McAree 2001, p69).
50
51
Data from interviews with pharmacists reporting jointworking in Elliott’s (1996) study suggested that thesurvey results overestimated the amount of collaborationand teamworking. Of 15 pharmacists who reported suchcollaboration, 10 had established continuous jointworking, while in the other five cases it was minimal orintermittent. It was noteworthy that pharmacistsdispensing higher numbers of prescriptions were morelikely to report collaboration. Close proximity to a GPsurgery with no other pharmacies close by was alsoassociated with collaborative work. Interviews withHealth Authority Pharmaceutical Advisers showed themto have a key role in organising local initiatives but thatsuch projects were for ‘limited time periods, with limitedfunding and inadequate evaluation and generallyinvolving an enthusiastic minority of pharmacists’ (B3:Elliott 1996, p84).
Effect of joint learning events with PHCTs
Local multidisciplinary health improvement workshops forPHCT members that community pharmacists were invitedto attend were evaluated prior to and following theirdelivery in a commissioned report (B3: Scott 1994, p85).Nine teams, each centred around one general medicalpractice, took part in the workshop. Interviews with over40 participants were conducted pre-workshop, then atone week and three months post-workshop. AlthoughPHCT members expressed confidence in individualpharmacists they often stated general concerns aboutcommunity pharmacy in relation to possible wider roles.The key concerns were around community pharmacists’lack of access to patients’ full medical history and aboutpotential conflicts of interest arising from commercialactivities. Nevertheless PHCT members werepredominantly positive towards pharmacists’involvement. The community pharmacists themselveswere pleased to have been invited to participate in theworkshop but expressed anxieties about what theywould be able to contribute and about how theirpresence would be received by PHCT members. Thisprofessional reticence contrasted with the attitude of
Analysis / discussion point:• Pharmacists report isolation
from other healthprofessionals as one of thebarriers to developing sexualhealth services.
• Referrals from pharmacists to other health professionals arehigher where pharmacy staffhave knowledge of relevantlocal services.
• Collaborative working is reported to be higher wherethe pharmacy dispenses highnumbers of prescriptions or isthe only pharmacy near a GPsurgery. This suggests thatcollaborative working iscurrently associated with theexisting mode of remunerationfor pharmacy services.
• PHCT members are generally positive about pharmacists’involvement in servicedevelopment, however,reservations exist aroundcommunity pharmacists’ lackof access to patients’ fullmedical history and aboutpotential conflicts of interestarising from commercialactivities.
• Joint training events between pharmacists and PHCTmembers appear to be usefulin promoting collaborativeworking but pharmacistsreport finding it difficult to findtime to leave the pharmacyand attend ‘team meetings’.

PHCT members, most of whom welcomed the idea ofpharmacist participation. Three months after theworkshop there was evidence of greater contact betweenpharmacists and the PHCT through specific joint eventsand the issuing of invitations by almost all the practicesto the community pharmacists to attend practicemeetings. However, attendance by pharmacists wasreported to be low due to difficulties in makingarrangements to leave the pharmacy premises.
52

53
4 DISCUSSION
Scope and quality of the materialA substantial number of studies (37) met the criteria forthe review, representing considerable investment ofresources by those conducting and commissioning theresearch. The scale of the research ranged from smalllocal studies to national surveys and the quality of moststudies was reasonable to good. A range ofmethodologies was used and the non peer-reviewedliterature was particularly rich in qualitative studies withpharmacists and users. Low response rates to surveys orrequests to participate in interviews was the mostcommon reason for a study to be excluded from thereview. It is noteworthy that most of the research withpharmacy users was based on convenience samples,hence these studies were graded as C1, although thequality of other aspects of the research was high and thestudies would otherwise have merited a higher grading.Given the methodological challenges of seeking toconstruct a systematic sample of a population of serviceusers it seems reasonable to accept that conveniencesamples might be considered adequate.
Some of the studies identified may have undergone aform of peer review process, especially commissionedresearch (although none of the reports considered madereference to such review). The research undertaken andsubmitted for higher degrees will have been subject to aform of peer review through the internal academicsupervision process and assessment by internal andexternal examiners. Nevertheless little of this work foundits way into the peer-reviewed literature. This body ofwork can help to inform the pharmacy profession andhealthcare commissioners about the future developmentof community pharmacy-based services.
Where does the non peer-reviewedliterature support the findings of thepeer-reviewed literature?The non peer-reviewed literature supports the findingsfrom the peer-reviewed literature in several main areas.
Firstly, that community pharmacists are viewed by thepublic as experts who advise on medicines rather thanhealth and illness. Secondly, that training has thepotential to change community pharmacists’ behaviourand orientate their practice towards effective healthimprovement activities. Thirdly, that the use of patientmedication records to identify pharmacy users ‘at risk’ ofcertain illnesses can be a very effective way to identifyand persuade this group to attend for consultation ortreatment. Fourthly, that the community pharmacyenvironment seems to be an appropriate setting todeliver certain health interventions including smokingcessation, the prevention of coronary heart disease(CHD), immunisations and the supply of emergencyhormonal contraception (EHC). Finally, that pharmacistsreport being reluctant to proactively offer health advicelest it be unwelcome to the client but are more likely toadvise on general health issues if medicines are involved.
What new evidence does the non peer-reviewed literature contribute?The non peer-reviewed literature provides new evidenceon community pharmacists’ public health role in relationto the primary health care team and on user andpharmacist perspectives of sensitive health topics such asEHC supply, head lice management and drug misuseservices. These findings are important because theydemonstrate the acceptability to pharmacy users ofseeking and receiving advice on sensitive health topicswithin the community pharmacy setting. Evaluations ofthe head lice programmes sought feedback from otherhealth professionals and demonstrated that GPs andschool nurses rated these services highly and wantedthem to continue.
The non peer-reviewed literature also provided furtherevidence of both pharmacy users’ perceptions of, andtheir feedback on, actual pharmacy services. The datademonstrated the difference in reported perceptions ofthose who have not consulted a pharmacist about asensitive topic and the experience of those who have.People who have used pharmacy services for healthdevelopment consultations (including sensitive health
54

55
issues) have a higher level of comfort about privacy andconfidentiality than those who have not.
In addition, the non peer-reviewed literature highlightsthat pharmacies are frequently used by people living indeprived areas and who are less affluent. Communitypharmacies have the potential to contribute to reductionin health inequalities because they are regularly accessedby those who are most likely to have poor health chances.
Health topics
The search of the non peer-reviewed literature revealedadditional health topics that had been provided in acommunity pharmacy-based setting and had beensufficiently evaluated for inclusion in this review. Topicsincluded: sexual health; head lice management; mentalhealth; the prevention of transmission of infection; andinjury prevention. More details on each health topic isprovided in the Results section.
Factors affecting the effectiveness ofcommunity pharmacy-based activities toimprove health
Several studies showed that some pharmacy usersexpressed concerns about the level of privacy incommunity pharmacies and that a pharmacy might beselected, or deselected, depending on the facilities forprivate discussion. This was found to be particularlyimportant in research on consumer attitudes to pharmacyadvice on contraception and sexual health. The results ofsurveys of women who obtained EHC from communitypharmacies were positive overall but indicate that forsome pharmacies there is a need to review facilities, withapproximately one in five women perceiving insufficientprivacy. Similarly, studies of head lice managementservices showed that some users expressed concernsabout the level of privacy during their consultation.Pharmacists can use this feedback to review how andwhere discussions are held in the pharmacy.
User perceptions of confidentiality were explored instudies on EHC and osteoporosis screening. The findings
suggest that publicity about the requirements forpharmacists and their staff to maintain confidentialitymay also be needed so that pharmacy users are moreaware of the pharmacist’s obligations to ensure bothprivacy and confidentiality where appropriate. It is alsopossible that user perceptions will change over time asmore pharmacies are refitted with provision for aconsulting room or an obvious ‘quiet area’, or becausepharmacies providing these facilities are preferablyselected by users.
Interestingly, there is some evidence of a gap betweenpharmacists’ and users’ perceptions of what mightconstitute ‘privacy’ in the pharmacy. While some healthtopics are perhaps more obviously sensitive (e.g. EHC)and may require a lot of privacy, pharmacists may seesome other topics as ‘routine’ and not necessarilyneeding such sensitive management (e.g. head licetreatment). Further research is needed to address thisissue and also track any changes in premisesdevelopment and the resulting use of pharmacies. It ispossible that user surveys recommended in theimplementation of clinical governance could also providedirect feedback to pharmacists and their staff.
Stakeholder views
User perceptions of community pharmacists
A common theme reported by users was that althoughthey had often identified specific information needs theydid not generally perceive the pharmacist as a source ofhealth advice. Instead users tended to cite the GP as thekey source of health information and advice but,nevertheless, they perceived the pharmacist as a highlyappropriate source of advice about the use of aspirin inCHD prevention and welcomed the increasedconvenience and access resulting from deregulation ofthe supply of EHC. These findings suggest that users aremore likely to accept the community pharmacist’s role ashealth adviser, at least initially, when related tomedicines supply.
56
57
Community pharmacists’ perceptions of theiradvice-giving role
Pharmacists also have concerns about doctors’ views oftheir involvement in health improvement. These areimportant barriers to opportunistic health improvementactivities and involvement in wider service provision.Given the sensitivity of certain health topics, such assexual health and obesity management, it isunderstandable that pharmacists might prefer to take areactive rather than proactive role on these issues,however in other areas, such as heart disease prevention,the non peer-reviewed research suggests that userswould already welcome information and advice from thepharmacist. Promotion of the pharmacist’s role ininformation giving to the public was suggested bypharmacists, in some studies, as a strategy to increaseutilisation of the pharmacist’s advice.
Community pharmacists and external stakeholders
The non peer-reviewed literature provides new evidenceon pharmacists’ health improvement role in relation tothe primary health care team. Research conducted in themid-1990s suggested low levels of collaborative workingbetween community pharmacists and other members ofthe primary health care team. The findings suggestedthat only 10% of community pharmacists had sustainablejoint working underway with local GPs. Multidisciplinaryworkshops were shown to increase shared understandingof the contribution that community pharmacists mightmake to health improvement as part of the primaryhealth care team and to lead to an increase in jointworking three months later. Pharmacists themselves werereticent about what contribution they might make toimproving health within this framework. Researchshowed that low awareness among communitypharmacists of local support groups and other agencies islikely to be a barrier to increasing referrals from thepharmacy to non-primary care services.
59
5 CONCLUSIONS
The non peer-reviewed literature strengthens the reviewof evidence by confirming the key findings of Report 1(the peer-reviewed literature), by adding new materialon health topics and on the relationships betweencommunity pharmacists and the primary health careteam, and by providing further insights into pharmacistand user attitudes and behaviours.
There is a high degree of expressed interest among usersin the availability of further information and advice frompharmacists, although the pharmacist is not seen as aprimary source. The research findings suggestconsiderable scope for joint working of pharmacists,users and healthcare commissioners to developpharmacies as a local and accessible advice pointcomplementary to existing services.
Since the review was conducted the modernisation of theNHS has continued at pace. Following announcementsfor structural reform and the devolution of decision-making to a more local level, there is a willingness topilot new ways of working to improve access and qualityof services and release a plethora of opportunities todevelop community pharmacy services in order to suit theneeds of the local population and to integrate moreclosely with existing NHS services. It is possible that thelevel of joint working between community pharmacistsand the primary health care team will already haveincreased as a result of recent initiatives, such as theimplementation of Patient Group Directions foremergency contraception and the development ofsmoking cessation services. In addition, increasingnumbers of community pharmacists are undertakingsession work with local GP practices for prescribing andmedication review purposes. It will be important tocontinue to track progress in this area and to ensure theintegration of the community pharmacist into theprimary health care team and local community from theperspective of health improvement.

Further research is also needed to measure any change inthe public’s perception of the pharmacists’ role in healthimprovement. Evaluation of innovative approaches toservices and premises development will also be crucial toinforming service design to meet the needs of users, andparticularly in relation to queries about approaching thepharmacist for general health advice and addressingperceptions about privacy and confidentiality.
60
REFERENCES
Anderson C (1997). Health promotion bycommunity pharmacists. PhD thesis,Department of Pharmacy, King’s College,London.
Anderson C, Bissell P, Sharma S & Sharma R.Manchester, Salford and Trafford HealthAction Zone (2001). Report into the provisionof Emergency Contraception in CommunityPharmacy Via Patient Group Directions,University of Nottingham.
Anonymous (1993). The PharmacyHealthcare Scheme (Qualitative study).Health Education Authority Research Report.London: Health Education Authority.
Aston University and MEL Research (1991).Consumer expectations of communitypharmaceutical services. Report to theDepartment of Health.
BMRB (1993). The Pharmacy HealthcareScheme (Quantitative study). HealthEducation Authority Research Report.London: Health Education Authority.
BMRB (1996). Baseline mapping study todefine access to and usage of communitypharmacy. Report commissioned by RoyalPharmaceutical Society of Great Britain.
Campbell Keegan (1992). Ask the pharmacist:advice on safer sex and contraception.Report commissioned by the PharmacyHealthcare Scheme Steering Group.
Coggans N, Johnson l, McKellar S, Grant L &Parr PM (2000). Health promotion incommunity pharmacy: perceptions andexpectations of consumers and healthprofessionals. Department of PharmaceuticalStudies, University of Strathclyde. Reportcommissioned by the Scottish Office.
Dewsbury-Mason C (1998). Communitypharmacists and health promotion training,activities and attitudes. MSc thesis, Universityof Kent.
Edwards L (2000). Levonelle – P status andwomen’s needs: qualitative research. Reportcommissioned by Schering Healthcare.
Elliott J (1996). The role of communitypharmacists in relation to the primaryhealthcare team. Report commissioned bythe Health Education Authority.
Hariri S (1998). Multimedia health promotionin community pharmacy. PhD thesis.Department of Pharmacy, King’s College,London.
Hassell K, Rogers A, Noyce P & Nicolaas G(1998). The public’s use of communitypharmacies as a healthcare resource. Reportto the Community Pharmacy ResearchConsortium.
Health Promotion Authority Wales (1991).Pharmacy Healthcare Scheme survey (Wales).Report. Health Promotion Authority Walesand Welsh School of Pharmacy.
Hughes K (2000). Pharmacists andcontraceptive and sexual health issues:qualitative research to inform of barriers andopportunities. Report to the HealthEducation Authority.
Kinghorn I (1998). The health educationneeds of patients buying or receiving aspirinon prescription for thromboprophylaxis. MScthesis, Department of MedicinesManagement, Keele University.
Lambeth, Southwark and Lewisham HealthAction Zone (2002). A timely service:Lambeth, Southwark and Lewisham HealthAction Zone project on access to emergencyhormonal contraception through accreditedcommunity pharmacies. Report. Lambeth,Southwark and Lewisham Health ActionZone.
Martin-Hamblin-GfK (2002). Report of theOsteoporosis Pharmacy Pilot Study.
61
Matheson C (1999). Community pharmacyservices for drug misusers: a study of theperspectives of service users and providers.PhD thesis, University of Aberdeen.
McAree DP (2001). Women’s health:community pharmacy care. PhD thesis. Schoolof Pharmacy, Queen’s University of Belfast.
McGovern EM, Lindsay H, Taylor A & BrysonSM (1999). Improving attitudes towardssugar-free medicines. ConferenceProceedings, UK Clinical PharmacyAssociation, Blackpool.
McGovern EM, Bryson SM, Lennie M, RoddickE & Anderson C (2001). Use of head liceproducts in three Local Healthcare Co-operatives. Conference 2001, RoyalPharmaceutical Society of Great Britain LocalHealth Care Cooperative.
McGovern EM, Tennant S & Mackay C (2001).Audit of returned medicines to communitypharmacies. Conference 2001, RoyalPharmaceutical Society of Great Britain LocalHealth Care Cooperative.
National Pharmaceutical Association (2001).Sunderland integrated head lice infectionmanagement service – an interim report.Report for the National PharmaceuticalAssociation.
Pharmacy Alliance (2002a). Emergencyhormonal contraception: customer survey.Report for Schering Healthcare.
Pharmacy Alliance (2002b). Emergencyhormonal contraception: pharmacy survey.Report for Schering Healthcare.
Philips Z, Whynes D, Parnham S, Slack R &Earwicker S (1999). The role of communitypharmacists in counselling patients andprescribing medication for the treatment ofhead lice. Report commissioned by theNational Pharmaceutical Association,Nottingham University.
Reilly V, Bresnen G & McGovern EM (2001).An examination of the role of thecommunity pharmacist in managing stressand anxiety. MSc thesis, School of Pharmacy,Liverpool John Moores University.
Scott J (2000). Development, implementationand evaluation of harm reduction techniquesfor drug users. PhD thesis, Robert GordonUniversity, Aberdeen.
Scott K (1994). Involvement of communitypharmacists in Health Education Authorityprimary healthcare team workshops – reporton qualitative evaluation. Reportcommissioned by the Health EducationAuthority.
Seston E, Holden K & Cantrill J (2000).Deregulation of hormonal emergencycontraception: pharmacists’ concerns andsupport needs. Report for RoyalPharmaceutical Society of Great Britain.
Shafford A & Sharpe K (1989). Thepharmacist as a health educator. ResearchReport 24. London: Health EducationAuthority.
Sheridan J (1995). HIV/AIDS and drug misuse:perspectives of pharmacy undergraduatesand pharmacists. PhD thesis, University ofLondon.
Sinclair HK (1997). Community pharmacy andsmoking cessation: training in behaviouralchange. PhD thesis, Department of GeneralPractice and Primary Care, University ofAberdeen.
Thomas G (2000). A study of the advice andtreatment recommended for head liceinfection in the Wrexham Local HealthGroup. MSc thesis, Department of MedicinesManagement. Keele University.
Watson L, Bond C & Gault, C (2003). A Surveyof community pharmacists onprevention of HIV and hepatitis B and C:current practice and attitudes inGrampian. J Public Health (In press).
Williams A, Bond CM, Winfield AJ, Calder G,Taylor R & Ritchie LD (1993). A public healthrole for the community pharmacist: a pilotstudy to identify patients who may beconsidered for influenza immunization.Report to the Scottish Office.
62
63
Appendix 1. National ServiceFrameworks: categorisation of evidence
The Department of Health categorises individual studiesaccording to the standard classification set out in itsNational Service Frameworks:
Evidence from research and other professional literature
A1 Systematic reviews which include at least one randomised controlled trial (RCT) e.g. systematicreviews from Cochrane or NHS Centre for Reviewsand Dissemination.
A2 Other systematic and high quality reviews which synthesise references.
B1 Individual RCTs.B2 Individual non-randomised,
experimental/intervention studies.B3 Individual well-designed non-experimental studies,
controlled statistically if appropriate. Includes studiesusing case control, longitudinal, cohort, matchedpairs or cross-sectional random samplemethodologies, and well-designed qualitativestudies, well-designed analytical studies includingsecondary analysis.
C1 Descriptive and other research or evaluation not in B (e.g. convenience samples).
C2 Case studies and examples of good practice.
D Summary review articles and discussions of relevant literature and conference proceedings not otherwiseclassified.
64
Appendix 2 Details of reviewed evidence
The abstracted papers are listed by health topic in the order thefindings are included in the ‘Results’ section of the report. Eachpaper has an evidence grading (see ‘Introduction – Criteria forinclusion of evidence’ and Appendix 1 for an explanation of thecategorisation of grade used).
Contents
Health Topics
Smoking cessation 65
Coronary heart disease – the use of aspirin in prevention 65
Drug misuse 66
Sexual health 67
Emergency hormonal contraception 69
Immunisation 73
Head lice 73
Oral health 76
Mental health 77
Prevention of transmission of infection 77
Accidental injury prevention 78
Factors affecting the effectiveness of community pharmacy-based activities to improve health 79
Stakeholder views 81
65
Title, authors, source type, year and evidencegrading Sinclair HK. Community pharmacy and smoking cessation:training in behavioural change. PhD thesis,Department of General Practice and Primary Care,University of Aberdeen (1997). B1
Objectives To develop and evaluate a trainingpackage for community pharmacists and theirassistants to improve the counselling in smokingcessation provided in community pharmacies.
Study design Randomised controlled trial(randomised by pharmacy to intervention andcontrol). Interviews to gain insight into thepharmacy support process. Intervention pharmacistsand pharmacy assistants were invited to attend atwo-hour training session. Outcome measure wasself-reported smoking cessation rates of the twogroups at one, four and nine months. A sub-sample of pharmacy customers (25 intervention;25 controls) were interviewed by telephone sixmonths after registration. Pharmacists completed aquestionnaire immediately after training and 2and 12 months later. Telephone interviews wereconducted with 20 pharmacy personnel.
Sampling and response rate All 76 non-cityGrampian community pharmacies were invited to
Title, authors, source type, year and evidencegrading Kinghorn IA.The health education needs of patients buying orreceiving aspirin on prescription forthromboprophylaxis. MSc thesis, Department ofMedicines Mamagement, Keele University (1998).C1
Objectives To establish the reason forpurchase/prescription of aspirin; assess thepatient’s knowledge of aspirin’s use and mode ofaction in coronary heart disease (CHD) prevention;assess patients’ knowledge of CHD risk factors;
participate and 62 (82%) agreed. All interventionpharmacies were represented at the training (40pharmacists and 54 assistants).
Key findings Pharmacy personnel thought thestage of change model was a good way ofunderstanding stopping smoking. Most reportedthat the training had made a difference to theway they counselled customers. At 2 and 12months the intervention pharmacy teams weresignificantly more knowledgeable, self-confidentand positive about the outcome of pharmacycounselling than controls.Customers (224 intervention; 268 controls) wererecruited to the study. Significantly moreintervention subjects were not smoking at eachfollow-up: one month 37% cf. 29%; four-months20% cf. 13%; nine-months 12% cf. 7%. Statisticalanalysis showed these findings to be robust toconfounders (sex, age, deprivation, nicotinedependency). Cluster randomization was found tohave a negligible effect. Intervention respondentswere significantly more likely to have discussedstopping smoking with pharmacy personnel (85%cf 62%). Intervention subjects rated theirdiscussion more highly, 34% cf 16% of controlsrated it as ‘very useful’.
identify key information needs of patients inrelation to aspirin; establish the acceptability ofadvice about aspirin in the pharmacy and patients’preferred content and format of advice.
Study design Telephone survey using a pre-piloted structured interview schedule (mean 23.2minutes). Patients buying or receiving aspirin onprescription were recruited from six communitypharmacies from a range of socio-economiclocations in Glasgow.
Sampling and response rate Of 148 individualswho were approached to take part, 128 (91.4%)
SMOKING CESSATION
CORONARY HEART DISEASE – THE USE OF ASPIRIN IN PREVENTION
Health Topics
agreed. Of these the researcher was able tocontact 108 during the study period.
Key findings 70 (64.8%) respondents receivedtheir aspirin on prescription and 38 had purchasedit. Most respondents were taking aspirin forsecondary prevention. Information needs wereidentified in relation to both aspirin and CHD
Title, authors, source type, year and evidencegrading Sheridan J.HIV/AIDS and drug misuse: Perspectives ofpharmacy undergraduates and pharmacists. PhDthesis, University of London (1995). B3
Objectives To investigate attitudes andknowledge of pharmacy undergraduates andcommunity pharmacists of HIV/AIDs and drugmisuse; to investigate community pharmacists’practice in relation to drug misuse and harmreduction services; to investigate clients’ views oncommunity pharmacy services for drug misusers.
Key findings Pharmacy undergraduates werefound to have positive professional opinions, butalso to hold some negative personal opinionsabout HIV and drug misuse. An educational
Title, authors, source type, year and evidencegrading Matheson C.Community pharmacy services for drug misusers: astudy of the perspectives of service users andproviders. PhD thesis, University of Aberdeen(1999). B3
Objectives To investigate the effect ofpharmacists’ attitudes to drug misusers on theservices provided and how services are delivered asperceived by the pharmacist and the drug misuser.
Study design Four methods were used. Astructured postal questionnaire collectedquantitative data from all community pharmacymanagers in Scotland on their attitudes towardsand level of involvement in service provision fordrug misusers (n = 1041). Telephone interviewswere conducted with a sub-sample of 45pharmacists to obtain in depth information. Face-to-face interviews with 124 drug misusers were
prevention. The pharmacist was considered highlyappropriate as a source of advice on both aspirinand CHD but pharmacists were not considered tobe providing this service currently. Pharmacypremises were considered by some to lack privacy.Personal input from the pharmacist was consideredimportant in information provision.
intervention was shown to have a significantpositive effect on knowledge but a less noticeableeffect on attitude.Over half of the community pharmacists weredispensing controlled drugs to drug misusers and13% were providing needle exchange. Communitypharmacists, like undergraduates, had positiveprofessional attitudes and some negative personalattitudes towards drug misuse. The latter tendedto be more negative, indicating that practiceexperience may have an effect.Drug misusers considered themselves to bestigmatised by community pharmacists, althoughsome reported positive experiences. Clientsperceived community pharmacists to be serviceproviders but not a source of advice.
conducted in four cities and adjacent rural areas.Observation of interactions between drug usersand community pharmacists was conducted andfield notes taken.
Sampling and response rate Questionnaireresponse rate: 79%.
Key findings Controlled drugs were dispensed todrug misusers by 61% of respondents. Methadonewas dispensed by 55% and methadoneadministration was supervised by 19%. Positiveattitudes were associated with higher levels ofservice provision. Pharmacists were motivated toprovide services by a desire to reduce the spread ofblood-borne diseases and to expand theirprofessional services. Barriers were concerns forthe effect on other customers, safety, workloadand inadequate remuneration.Drug misusers perceived providing clean injectingequipment and methadone dispensing as
66
DRUG MISUSE
67
important services. Drug misusers askedpharmacists for advice on general health and fewasked for advice related to drug misuse. Beingtreated discreetly and having a good relationshipwith the pharmacist/staff encouraged serviceuptake. Negative treatment promotedstigmatisation and precipitated negativebehaviour.
Title, authors, source type, year and evidencegrading Scott J.Development, implementation and evaluation ofharm reduction techniques for drug misusers.PhD thesis, Robert Gordon University (2000). C1
Objectives To explore the provision of apharmacist-led information and advice service at avoluntary sector drugs agency.
Study design Field study monitoring the role ofa pharmacist within a voluntary sector drugsservice. Members of the public and other externalcontacts could access the service one 3-hourafternoon session each week when the pharmacistwas present in the agency. Drug agency workershad telephone access to the pharmacistthroughout working hours.
Key findings A total of 77 contacts were madewith the pharmacist during the 26 weeks that theservice was in operation. Of the 77 contacts, 45were with Drugs Action workers, 25 with membersof the public and seven with workers from outsideorganisations.
Title, authors, source type, year and evidencegrading Campbell Keegan.Ask the pharmacist: advice on safer sex andcontraception. Report commissioned by PharmacyHealth Care Steering Group (1992). B3
Objectives Examine pharmacists’ views on theirrole on advising on safer sex and contraception;explore views on development and support needsfor this role; investigate consumer views onpharmacists as an information source on safer sex /contraception.
Study design Structured interviews withpharmacists (telephone) and consumers (face-to-
The author concluded that remuneration,professional endorsement and bettercommunication with other services wouldencourage pharmacists to provide servicesidentified by drug misusers, such as greateravailability of injecting equipment.
Members of the public were asked if they mightconsider asking the community pharmacist abouttheir query and most said not. The non-judgemental attitude associated with the drugsagency and its staff was cited as the main reasonwhy the query had been made there.Drug information was the commonest type ofquery (37% overall, numbers slightly higher aboutprescribed than non-prescribed drugs). Drugtesting was the next commonest (15%). About halfthe queries were answered using pharmacy ‘core’knowledge, a quarter with ‘specialist’ knowledgeand a quarter with both. The key specialist skillrequired was translating technical information intoterms used in the ‘drug culture’.
Other comments The findings indicate thatthere is a role for pharmacist query answeringwithin drugs agencies. Some specialist knowledgewas required. Client attitudes appear to be animportant barrier to information and advice-seeking in community pharmacies.
face). Qualitative telephone and face-to-faceinterviews with sub-sample of respondents.
Sampling and response rate ‘Clustered randomsample of pharmacies across the UK’. Four regions:north; south; Wales; Northern Ireland. Of 168pharmacists who were approached, 104 (62%)participated in the telephone interview; 63%worked for independents and 36% for chains.Qualitative interviews were conducted with 13pharmacists. 224 consumers took part in thequantitative interviews (49% male, 51% female).Qualitative interviews were conducted with 17consumers.
SEXUAL HEALTH
Key findings Of the pharmacists interviewed,86% thought that pharmacists have an importantrole in promoting safer sex / contraception and53% thought pharmacists should do more in thisarea. However, most (73%) pharmacists reportedbeing asked for advice on contraception less thanonce a week. The researchers state thatpharmacists generally took a reactive role,providing advice when asked.64% of consumers said they would like more
Title, authors, source type, year and evidencegrading Hughes K.Pharmacists and contraceptive and sexual healthissues: qualitative research to inform of barriersand opportunities. Report for Health EducationAuthority (2000). B3
Objectives Explore barriers and opportunitiesaround pharmacists working with contraceptiveand sexual health issues. To explore pharmacists’current knowledge and experience in sexualhealth; to investigate attitudes towards givingadvice and information on general health andsexual health; to consider support needs; toexplore issues around pharmacy involvement inthe provision of emergency hormonalcontraception.
Study design Group discussions with five to sixpharmacists plus individual interviews.
Sampling and response rate Eight discussiongroups and 18 interviews. Pharmacists wereexcluded if they disagreed with the statement ‘Ifeel that pharmacists have an important role toplay in improving the health of the general publicand promoting healthy lifestyles’. There were twogroups for each of: independents; independentchains; large chains; supermarkets. Four groupswere of pharmacists qualified for up to five years;the remainder for five or more years.
Key findings Most participants saw their role as‘revolving around the provision and sale ofmedicines’, advising people on how to takemedicines, and responding to queries aboutsymptoms and how best to treat them. Ways inwhich pharmacy might evolve in the future thatwere mentioned most often were running clinicsfor diabetes and asthma, managing long-termmedication, pharmacist prescribing and healthpromotion. Promoting the clinical and wider skills
advice on contraceptives / safer sex from thepharmacist. The most important factor inconsidering a pharmacist for advice was a quietarea (41%). No one spontaneously suggested theywould go to the pharmacist for advice on safer sexor contraception, 38% saying they would go totheir GP. However, on probing 30% reportedhaving gone to the pharmacist for advice oncontraception at some time in the past.
of pharmacists to the public was seen as desirable.Participants thought that pharmacy had been leftbehind in relation to nurse prescribing, smokingcessation services and other health promotionareas. Pharmacists were isolated from other healthprofessionals and each other. People did nottypically ask pharmacists about general health issues.Pharmacists were generally not proactive in healthpromotion. They felt they could only respond tocustomer queries and ‘raising health promotionissues with most clients was regarded as highlyproblematic’. There was no way of knowing whomight appreciate the advice and who might beoffended.Health promotion activity was more likely to beformalised in larger chains.The potential conflict of interest was raised wherehealth promotion advice might not require thepurchase of a product. While most pharmaciststhought that providing the right advice led tobenefits in the long term, there was discussionabout the losses and gains in becoming moreinvolved in health promotion.Across the sample, involvement in sexual healthpromotion was limited and entirely as a result ofcustomer queries. There was general agreementthat expanding the role of pharmacists in this areawas likely to be problematic. Many participantsfelt uncomfortable about this area of advice. Aprivate area was seen by most as essential. Whendiscussing EHC however participants generally sawmore scope for involvement. There was support forderegulation of EHC, which was seen to offer moreinvolvement in ‘prescribing’, increase pharmacists’status and provide a business opportunity.Concerns were expressed about liability, ethicalissues and potential abuse. Training needs werefelt to around consultation skills rather thanclinical information.
68
69
Title, authors, source type, year and evidencegrading McAree DP.Women’s health: community pharmacy care. PhDthesis abstract, School of Pharmacy, QueensUniversity of Belfast (2001). B3
Objectives To evaluate community pharmacists’knowledge, attitudes and competency in relationto women’s health; to introduce and evaluate apharmacy-based advice service for women.
Study design Pharmacists’ knowledge wasmeasured at baseline and following a distancelearning course using a postal questionnaire. Apostal questionnaire measured pharmacists’attitudes towards providing advice on women’shealth. 521 female Boots pharmacy customerswere interviewed face-to-face by a pre-registrationgraduate to identify health issues of importance towomen and to ascertain their opinions andreservations on aspects of a dedicated pharmacy-based service. Pilot study in four communitypharmacies.
Sampling and response rate Of 350pharmacists, 216 responded to the pre-course and133 to the post-course test.Response rate was 273 (47.5%) completed
Title, authors, source type, year and evidencegrading Lambeth, Southwark and LewishamHealth Action Zone.A timely service: Lambeth, Southwark & LewishamHealth Action Zone project on access to emergencyhormonal contraception through accreditedcommunity pharmacies. Lambeth, Southwark &Lewisham Health Action Zone (2002). Report. B3
Objectives To assess the knowledge andexperience of users of the emergency hormonalcontraception (EHC) Patient Group Direction (PGD)scheme.
Study design Questionnaire distributed to 1558service users at the community pharmacies. Thequestionnaire covered user satisfaction andincluded opportunities for qualitative comments.Four qualitative interviews with service users tovalidate context. Individual and group interviewswith participating pharmacists.
questionnaires from a valid random sample of 575. 602 questionnaires were distributed, 521completed and 81 refusals (response rate: 86.5%). Pharmacist feedback from feasibility study wasobtained through a seminar.
Key findings Of 350 pharmacists, 38 hadcompleted the distance learning course andshowed significant improvement in test scores. Theattitudinal survey showed that pharmacistsreported they were not embarrassed to discussmany women’s health issues. Some concerns wereexpressed about confidence and knowledgedeficits. Male pharmacists perceived themselves assignificantly less knowledgeable or moreembarrassed on a number of issues. Pharmacists’referral to other professionals was significantlyrelated to their knowledge of opening hours andreferral procedures.The customer survey identified a number of factorsthat might influence use of a pharmacy adviceservice including quality and confidentiality.Pharmacists in the pilot study documentedimprovement in competency and knowledge.Clients were reported to respond positively to theservice.
Sampling and response rate Response rate:20% (315).
Key findings Of the service user respondents98% reported being ‘satisfied’ or ‘very satisfied’with the service and 90% said they felt‘comfortable’ or ‘very comfortable’ discussing theirrequest with the pharmacist. 78% felt there wassufficient privacy for their discussion and 76%reported no concerns about confidentiality.Concerns about confidentiality were higher inthose under 20 years of age. Roughly 20% ofrespondents had concerns about privacy and/orconfidentiality.Provider pharmacist interviews highlighted theimportance of good counter staff who couldmanage waiting customers. No pharmacistmentioned difficulty with the record-keepingrequired for the project. Pharmacists reported anincrease in their professional self-esteem.
EMERGENCY HORMONAL CONTRACEPTION
Title, authors, source type, year and evidencegrading Anderson C, Bissell P, Sharma S &Sharma. R. Manchester, Salford and TraffordHealth Action Zone. Report into the provision of EmergencyContraception in Community Pharmacy Via PatientGroup Directions. University of Nottingham (2001).C1
Objectives Aims were to assess the knowledge,experiences and attitudes of service users (SUs); toexplore the perspectives of pharmacist providers;to assess how pharmacists were operating theservice.
Study design Questionnaire distributed toservice users by pharmacists. The 28-itemquestionnaire was structured with space foradditional comments. A sample of SUs were askedto participate in focus groups. Interviews with 24 pharmacists.‘Mystery shopper’ evaluation with researchersposing as SUs.International literature review on emergencyhormonal contraception provision.
Sampling and response rate Of 5020questionnaires distributed to 53 pharmacies, 490were returned (9.8%).
Key findings The age range of the 490respondents was 15–52 years; a mean of 25. 37%were in college or higher education, a quarterwere graduates and 14% were postgraduates.17% were aged 19 years or under. Almost all the
Title, authors, source type, year and evidencegrading Pharmacy Alliance.Emergency hormonal contraception: Customersurvey. Report for Schering Healthcare (May2002a). C1
Objectives To assess customers’ attitudes towardsavailability, sale and supply of emergencyhormonal contraception (EHC) from thecommunity pharmacy, and any information needsthey may have; to establish women’s views on thecommunity pharmacy and the communitypharmacist as sources of EHC supply and advice.
Study design Participating pharmacies (250)were selected as study sites from respondents to apharmacist questionnaire. The questionnaire wassent to 2219, and 1426 (64%) pharmacists
SUs (99%) said they were ‘very satisfied’ or‘satisfied’ with the way their emergency hormonalcontraception (EHC) request had been handled.99% indicated that they had received enoughinformation from the pharmacist. 85% felt therewas sufficient privacy; 80% were either‘unconcerned’ or ‘very unconcerned’ about theconfidentiality of their enquiry for EHC; 19% were‘concerned’ or ‘very concerned’ aboutconfidentiality and this was higher among under-19 years (28%). 70% of those who had used EHCbefore indicated that the pharmacy service was‘much better’ than their previous service provider.Awareness of the pharmacy service came fromfriends and family (30%), TV or radio (26%), GP(15%), pharmacy poster (14%) and NHS Direct(9%). Respondents indicated that weekdayevenings, Saturday mornings, afternoons andSunday mornings were the most convenient timeto access EHC. Focus group data showed that someparticipants had found it difficult to find outwhich pharmacies were providing the service andwhen they were open. A need was identified forinformation and advertising about the service.Most participating pharmacists expressed positiveviews about the service for both SUs andpharmacists. Some concerns were expressed aboutthe additional workload that providing the serviceimposed, variability in remuneration practicesbetween different pharmacy chain employers andlack of private space for conducting consultations.Few pharmacists reported that repeated use ofEHC was a problem in practice.
responded, of whom 435 were willing to take partand 250 were selected to do so. Selection criteriawere speed of return of questionnaire andnumbers of packs of Levonelle sold (based onUnichem data). Each pharmacist was asked torecruit 10 EHC customers to complete theconsumer survey. A ‘customer refusal count sheet’was provided to document refusals.
Sampling and response rate The overallresponse rate was 30% (785). There were threegroups of pharmacies: Pharmacy Alliance (PA),Moss Pharmacies and Unichem CommunityPharmacy Initiative (CPI) scheme. Consumerquestionnaires were returned for 59%, 40% and24% of these pharmacies respectively. Thepercentages of possible forms returned were 36%PA, 24% Moss and 16% CPI.
70
71
Key findings The mean age of the 785respondents was 26 years (range 14–53 years).80.8% were white and 19.2% non-white. EHC wasreceived on prescription by 42.4%, over thecounter sale by 44% and Patient Group Direction(PGD) by 13.6%. The 16–20 age group recordedthe highest level of access by PGD at 17.3%. Under16-year olds received EHC on prescription in two-thirds of cases and PGD in 14.3%, with 21.4% notreporting a source. Women over 20 years were thelargest group and more likely to buy EHC over thecounter. Monday was the commonest day forobtaining EHC (200, 27.7%), with Saturday 14.9%,and no major differences between Saturday andother days of the week. 71% of women accessed
Title, authors, source type, year and evidencegrading Pharmacy Alliance.Emergency hormonal contraception: Pharmacysurvey. Report for Schering Healthcare byPharmacy Alliance/Unichem (May 2002b). B3
Objectives To assess the attitudes of communitypharmacists in the UK towards the sale and supplyof emergency hormonal contraception (EHC) oneyear after its deregulation to a P medicine; todetermine the training undertaken by pharmacistsand assistants on EHC; to determine the reasonswhy some pharmacists do not supply EHC.
Study design A structured postal questionnairewas sent to all 2219 members of Pharmacy Alliance(802), Moss Pharmacies (773) and UniChem’sCommunity Pharmacy Initiative (CPI) scheme (644)in England, Scotland and Wales.
Sampling and response rate Response rate was56% after the initial mailing and 64% after onereminder. Response rates were 76% (613)Pharmacy Alliance; 72% Moss (554) and 40% (259)CPI. The age and gender profiles of respondentswere compared with Royal Pharmaceutical Societyof Great Britain data and found to be similar.There were no publicly available data with whichto compare the white/non-white respondentprofile.
Key findings 55% of respondents were male and69% were white. The mean age of respondentswas 41 years. Overall 94% reported that theyworked regularly in the pharmacy from which thesurvey was completed. Breakdown of respondents
EHC within 24 hours of unprotected intercourse.Speed of access and convenience were the mostcommon reasons reported for purchasing EHC overthe counter. Prior to the current supply of EHC,66.4% of women were aware that EHC wasavailable without a prescription. Respondentsrated a series of statements from 1 (stronglydisagree) to 5 (strongly agree). There was a highlevel of satisfaction with the amount of advice andinformation received, the median response being 4for both. Pharmacies were highly rated as asuitable place to obtain and discuss EHC, medianresponse 4 for both. Anonymity was cited by 9.7%of respondents as a key reason for pharmacypurchase of EHC.
by professional status was 58% managers, 31%owners, 7% locums (10% missing or other).Almost all (98.9%) respondents said they wouldsupply EHC on prescription and 89.4% said theywould sell EHC over the counter (OTC). EHC wasbeing supplied under Patient Group Direction(PGD) by 20% of respondents and a further 51%who were not participating in a PGD scheme saidthey would like to do so. Of the 284 pharmacistsinvolved in PGD schemes 66% (136) reported thatunder 16-year olds were excluded.Respondents were asked to rate a series ofstatements from 1 (strongly agree) to 5 (stronglydisagree) Pharmacists disagreed that OTCavailability had resulted in increasedpromiscuity/sexual activity (median response4).They supported the supply of EHC on PGD tounder 16-year olds (median response 2) and, whilethey were not in favour of OTC availability for thisgroup (median response 4), they did not agreethat all under 16-year olds requesting EHC from apharmacy should be referred elsewhere. Thissuggests that pharmacists wish to use theirprofessional judgement about supply. Pharmacistsdid not agree that they had found it difficult todeal with teenagers’ requests for EHC (medianresponse 4). Pharmacists felt that EHC availabilityOTC had provided an opportunity to develop newcounselling skills (median response 2). They agreedthat the price of the OTC product was a deterrentto patients buying it (median response 2).Most (91%, 1302) pharmacists reported that theyhad undertaken training on EHC. Centre for
Pharmacy Postgraduate Education (CPPE) workshops had been attended by 30% and CPPEdistance learning used by 56%. Manufacturers’support information was used by 52%. Three-quarters of respondents reported having a‘set protocol’ for sales of EHC. Women for whom
Title, authors, source type, year and evidencegrading Seston E, Holden K & Cantrill J.Deregulation of hormonal emergencycontraception: Pharmacists’ concerns and supportneeds. Report for Royal Pharmaceutical Society ofGreat Britain (2000). B3
Objectives To explore community pharmacists’views on the deregulation of emergency hormonalcontraception (EHC) from POM to P (prescriptiononly medicine to pharmacy medicine) and toexamine training and support needs related to theswitch.
Study design Focus groups with 14 communitypharmacists.
Sampling and response rate Two groups wereheld; one with community pharmacists alreadyproviding EHC under a Patient Group Direction (8),the other with no experience of providing EHC (6).Pharmacists worked for a variety of employersincluding multiples, small chains andindependents.
Title, authors, source type, year and evidencegrading Edwards L.Levonelle – P status and women’s needs:qualitative research. Report for Schering HealthCare (2000). B3
Objectives To explore women’s informationneeds in relation to the POM to P (prescriptiononly medicine to pharmacy medicine) switch ofemergency hormonal contraception (EHC).
Study design Ten focus groups with women whohad used / might use EHC.
Sampling and response rate Samplingstratified by social class and age/lifestage. Eachgroup comprised half who were users ofemergency contraception and half who were non-
OTC EHC was identified as inappropriate werereferred to GPs by over 90% of respondents and toFamily Planning Clinics by around 60%.Pharmacists reported little feedback from theircustomers about positive or negative outcomesafter use of EHC.
Key findings Pharmacists were ‘poor’ atidentifying their own individual training needs.Most participants supported mandatory trainingbefore ‘prescribing’ deregulated EHC. Pharmacistsexpressed concerns about ‘clinical’ issues and thesewere generally ill-defined. Some participants wereconcerned about how they would deal with under-age clients. There was an identified need fortraining for pharmacists in how to conductconsultations for EHC in a non-judgementalmanner. Pharmacists in both focus groupsexpressed concerns about possible ‘abuse’ of EHCalthough the authors comment that many of theseconcerns were based either on inaccurateinformation or subjective assumptions. Thepharmacists who were already supplying EHC saidthat their prior concerns had rarely materialised inpractice. The authors reported a sense that EHCwas accorded a special status by participants whencompared with other POM to P switches.
users but not ‘rejecters’. Those who said theywould ‘definitely’ only obtain EHC from the doctorwere excluded.
Key findings Participants were positive aboutconvenience / accessibility of EHC following theswitch. However, concerns were expressed aboutpossible abuse of EHC. Key questions were: is it OKfor me to do this?; what will my experience be if Ido this?; what will happen to me afterwards?; AmI in time?; How effective is it? ‘Myths’ identifiedwere worries about how often EHC could be takenand whether it might affect fertility in the longerterm. The open pharmacy environment was amajor concern, as was confidentiality / whatrecords would be kept.
72
73
Title, authors, source type, year and evidencegrading Williams A, Bond CM, Winfield AJ,Calder G, Taylor R & Ritchie LD. A public health role for the community pharmacist:a pilot study to identify patients who may beconsidered for influenza vaccination. Report to theScottish Office (1993). B3
Objectives To assess the potential for a publichealth role for community pharmacists usinginfluenza as a ‘tracer’ condition.To assess the community pharmacist’s facility toidentify patients who may be candidates forinfluenza immunisation.
Study design A systematic method (using patientmedication records: PMR) and an opportunisticmethod (with customers asking for advice aboutspecific symptoms or for influenza or requestingcertain over the counter medicines) were used. Thesystematic method was used in one health centrepharmacy with 30,000 patient records on the PMRsystem and the opportunistic method in 25pharmacies. In the systematic method a list of ‘atrisk’ factors was compiled based on age andprescribed medication. Patients were selectedrandomly from the computer-maintained list andtheir medication records checked for ‘at risk’factors. Records were selected in this way until 250eligible patients had been identified. Thecomputer file for each of these patients was thenflagged such that the patient would be identifiedthe next time they presented with a prescription.‘At risk’ patients were asked to complete a shortquestionnaire. Pharmacists in the ‘opportunistic’study were each given 10 questionnaires to begiven to customers.
Title, authors, source type, year and evidencegrading Philips Z, Whynes D, Parnham S, Slack R& Earwicker S.The role of community pharmacists in counsellingpatients and prescribing medication for thetreatment of head lice. Report commissioned bythe National Pharmaceutical AssociationNottingham University (1999). B3
Objectives To assess the usage, acceptability,
Sampling and response rate In theopportunistic study 37% of questionnaires werereturned.
Key findings The systematic method using PMRwas effective in identifying patients who would becandidates for influenza immunisation. 186patients completed a questionnaire, 99% of whomfell within an ‘at risk’ category. A significantproportion of patients (69%) had not previouslybeen immunised against influenza, and thispercentage was lower in patients with asthma(25%). The authors comment that the researchdemonstrated that PMRs have valuableapplications other than those associated with thedispensing process.The opportunistic method showed some potentialbut was hampered by a poor response fromcommunity pharmacists. However, for the 74people presenting with influenza-like symptoms,97% were identified as having one or more ‘atrisk’ factors. Feedback from the pharmacistsindicated that lack of remuneration was the mainreason for the low participation rate. Further workwould be needed to confirm its value.
Other comments The authors recommendedthat: a national study using the PMR methodshould be conducted with a concurrent advertisingprogramme and leaflets; that communitypharmacy data collection could be used to monitorinfectious disease outbreaks such as diarrhoea andinfestation; that remuneration should be given tothe pharmacist to cover time and the cost oftraining staff.
effectiveness and effects on costs of communitypharmacy, rather than general practice, being thefirst port of call for suspected head lice infestation
Study design Before (3 months) and after (3months) design in one health authority areainvolving 32 community pharmacies in threePrimary Care Groups and 120,000 registeredpatients. The scheme was continued beyond theinitial three months for a further 15 months and
IMMUNISATION
HEAD LICE
was monitored over this period. From January1998 community pharmacy was promoted as theprincipal source of advice and treatment for headlice. After training, pharmacists providededucation and counselling. Proof of infestationwas required before treatment was recommended.Pharmacists supplied treatment from an agreedformulary where needed and were paid a feeregardless of whether treatment was supplied.Community pharmacists recorded prescriptions andover the counter consultations about head lice forthree months prior to the study. During serviceprovision pharmacists used a Pharmacy Prescription(PP1) form for both exempt and non-exemptpatients. Prescribing Analysis and Costs (PACT) datawere used to assess changes in prescribing of headlice treatments. Questionnaire surveys of patients(convenience sample of users) and healthprofessionals were conducted.
Sampling and response rate Questionnairescompleted by 336 patients and 201 healthprofessionals (60 GPs, 42 pharmacists, 69headteachers and 30 school nurses). No responserates stated.
Key findings Most of the 5710 scheme users inthe three-month evaluation period were female(3846; 67.4%) and children (4383; 76.8%) andexempt from prescription charges (5394; 94%). Adistinct trend away from consultations with the GPand towards community pharmacy consultations
Title, authors, source type, year and evidencegrading National Pharmaceutical Association.Sunderland Integrated head lice infectionmanagement service – an interim report. Reportfor the National Pharmaceutical Association (2001).B3
Objectives To enable easier access to appropriatetreatment for head lice; to promote self-care.
Study design Two primary care groups provideda community pharmacy-based head licemanagement service. Participating pharmacists(initially from 32, later expanded to 47 pharmacies)were required to participate in training tofacilitate consistency of advice. Head teachers werealso invited to the training. From September 1999,GPs and community nurses were encouraged torefer clients to the pharmacy and not to prescribehead lice treatment. Pharmacists used a
was apparent within the first month of the schemeand continued throughout the evaluation period,with increasing self-referrals. Patients weretypically registered with a GP in the surroundingarea of the pharmacy used. No treatment wasrecommended in one-third of consultations. Priorto the scheme 30% of prescribed treatments werenon-formulary compared with over 99% formularyduring the scheme (malathion and 50ml or 55ml‘dose’). The ratio of prescribing of head licetreatments in the study area to the rest of thehealth authority area was 60% at baseline and fellto under 25% demonstrating decreased GPprescribing in the study area. Cost analysis showedthat community pharmacy consultations cost lessthan GP consultations for head lice. Thequestionnaire results showed that patients andhealth professionals viewed the new arrangementas at least as acceptable as the old.In total 336 questionnaires were completed bypatients, most of whom were women. While theoverall findings suggest that the scheme was well-received, 17.6% said they were embarrassed tospeak to the pharmacist about head lice. Aroundhalf reported previous head lice infection. Healthprofessionals were generally positive about thescheme, with GPs and school nurses finding it mostbeneficial. Head teachers had some concerns aboutthe need for parental education and for parents totake responsibility for checking hair and ensuringtreatment compliance.
prescription form HL1 to record consultations. Theformulary was malathion only, with a ‘dose’ of 2 x50ml. The nursing team carried out a telephonesurvey of a random sample of clients who hadused the service.
Sampling and response rate Questionnaireswere sent to GPs (38% response), surgery staff(54%), school nurses (68%), health visitors (28%),head teachers (57%) and pharmacists (87%).
Key findings Over a seven-month period 1847clients accessed the service, with 1432 provinginfection for 2897 household members. Mostclients were female and children. The use of achemical insecticide was avoided in 415 suspectedinfections. Pharmacists maintained 100%compliance with the local formulary, so all clientswere treated in accordance with local guidelines.
74
75
Prior to the service commencing, concerns hadbeen raised about a perceived lack of privacy incommunity pharmacies. The client survey showedthat 42% said they were able to discuss theirproblem in private, 34% said they were not able todiscuss their problem in private and 24% said theywere ‘not bothered’. The community pharmacyservice was rated as: excellent (28%), very good(34%), good (20%), average (8%) and poor (4%).Just over half the clients recalled having head liceinfection within the last two years. 98% reportedthey had understood what the pharmacist had saidand 66% said their treatment was successful (10%said it was not). 74% said they intended to use thehead lice detection comb (supplied by thepharmacist) on a regular basis.71% of GPs said that the service had reduced thetime they spent dealing with head lice infestation.Overall 34% said they rarely (31%) or never (3%)saw the client when prescribing head licetreatment. Over 90% of health professionals saidthey were happy for the service to continue andthe majority (67-85%) agreed that the service had
Title, authors, source type, year and evidencegrading Thomas G.A study of the advice and treatment recommendedfor head lice infection in the Wrexham LocalHealth Group area. MSc Thesis, Department ofMedicines Management, Keele University (2000).B3
Objectives To establish the thoughts and beliefsof different professional groups on head liceinfestations and treatment.
Study design Postal questionnaire to headteachers of junior and primary schools, schoolnurses, community pharmacists and GPs in oneLocal Health Group area in Wales.
Sampling and response rate Response rates:65% (13 of 20) GPs; 90% (27 of 30) community
Title, authors, source type, year and evidencegrading McGovern EM, Bryson SM, Lennie M,Roddick E & Anderson C.Use of head lice products in three Local HealthCare Co-operatives. Royal Pharmaceutical Societyof Great Britain Local Health Care Co-operative
‘made my life easier’. When asked if the serviceshould be extended to cover other conditions, 60%of pharmacists, 66% of GPs, 52% of surgery staff,62% of school nurses and 36% of health visitorsagreed.Pharmacists were positive about the scheme and93% said they would be happy to continue.Pharmacists reported that 67% of initialconsultations took 5–10 minutes with 29% takingless than 5 minutes and 5% more than 10 minutes.Overall the cost of the new service was similar tothe previous equivalent period, even though twicethe quantity of treatment was supplied under thenew service in line with treatment guidelinesrecommending two applications one week apart.
Other comments The authors comment that GP-time was previously used in dealing with head lice.They point out that the condition has noassociated health risks, implying that GP-timefreed by the scheme could be used to deal withmore serious conditions.
pharmacists; 84% (43 of 51) head teachers and73% (11 of 15) school nurses.
Key findings Head teachers and healthprofessionals were in agreement that head liceinfection was an increasing problem. Schools didprovide information to parents and thatinformation was sometimes out of date or inconflict with that given by health professionals.Head teachers and GPs tended to have apreference for physical methods of head liceremoval and the results suggest that this might berelated to their thoughts on the safety and efficacyof insecticides. Variation in the recommendationsmade by different respondent groups had thepotential to confuse parents. The authorconcluded that there was a need to develop aconsistent approach to advice and information ondetection and treatment of head lice.
Conference (2001). C1
Objectives To evaluate the use of head licepreparations.
Study design Thirty-four community pharmaciesrecorded requests for head lice treatments for one
month. Data collected included insecticidesupplied, whether on prescription or over thecounter and whether live lice had been found bythe customer. The pharmacies also recorded whenadvice was given and if not, why not.Pharmacists also asked the customers to completea questionnaire.
Sampling and response rate Of 62 pharmacies,34 (55%) participated.Questionnaires were returned by 184 (47%)customers.
Key findings Of 392 requests for head liceproducts received, 219 (56%) were for over thecounter (OTC) supply. Most requests (344, 87%)were for a pyrethroid product. Advice wasreported to have been given on 88% of occasionsunless the product had been used before (13) or
Title, authors, source type, year and evidencegrading McGovern EM, Lindsay H, Taylor A &Bryson SM.Improving attitudes towards sugar-free medicines.UK Clinical Pharmacy Association ConferenceProceedings, Blackpool (1999). C1
Objectives To determine pharmacists’ attitudesand practice towards recommending sugar-freemedicines.
Study design Interviews were conducted with100 community pharmacists in 1996 and repeatedin 1998. In the intervening period a sugar-free (SF)substitution list was circulated to pharmacists, andhealth promotion initiatives with support wereundertaken. Questions covered attitudes towardsprovision of SF medicines, whether the pharmacistmight attempt to persuade a customer to changeto an SF version and advice offered when a sugar-containing medicine was sold. Ten pharmaciescollected data for two weeks on all paediatric overthe counter medicines sold and customers wereasked about their attitudes towards SF medicines.
Key findings In 1996 and 1998 respectively, 35%and 64% of pharmacists said that sugar content of
advice had been given by the GP (10). Head licehad been found by the customer on 297 (75%)occasions.127 (69%) of customers said they intended torepeat the application and 69 (38%) intended totreat the whole family or all children irrespectiveof whether or not head lice was found. Thequantities of product supplied were less than thoserecommended in current guidelines.The authors note their concern that one-third ofcustomers did not intend to repeat the treatmentapplication and that over one-third intended totreat irrespective of whether or not other familymembers had head lice. It was concluded that thehigh cost of OTC treatment may be a barrier to useof appropriate quantities and to repeatapplications.
a medicine would affect their productrecommendation for a child. The percentage ofpharmacists saying they would try to persuade acustomer to change to a SF product increased from45 to 69%. Offering dental advice when a sugar-containing product was sold was reported by 8%of pharmacists in 1996 and 21% in 1998. In theintervening period 22 pharmacists had participatedin postgraduate education in oral health, 30 hadparticipated in a local health promotion initiativeon oral health and 76 reported having readrelevant articles.Most medicines for children (over 85% in bothaudits) were requested by name. Of the medicinesrecommended by the pharmacist the percentagethat were SF increased from 55% to 100%. Mostcustomers (60–70%) believed SF medicines to beimportant.The authors note that pharmacists’ attitudestowards SF medicines became more positive andthis resulted in increased provision. Neverthelessthey identified opportunities for furtherimprovement. They conclude that a more proactiveapproach is needed, especially with thosecustomers who believe SF medicines are important.
76
ORAL HEALTH
77
Title, authors, source type, year and evidencegrading Reilly V, Bresnen G & McGovern EM.An examination of the role of the communitypharmacist in managing stress and anxiety. MScThesis, Liverpool John Moores University (2001).C1
Objectives To assess the involvement ofcommunity pharmacists in the management ofstress and anxiety in one Local Health CareCooperative (LHCC).
Study design Training evening held forpharmacy staff in the LHCC area. Resource manualproduced for use by pharmacy staff. Interviewsconducted with 12 community pharmacists and 12pharmacy assistants. Pharmacy customers wereasked to complete a questionnaire on frequency ofsymptoms, any treatment purchased and preferredsources of advice. Records were kept of leaflets onmental health promotion issued by pharmacy staffand self-selected by customers.
Sampling and response rate Two-week study
Title, authors, source type, year and evidencegrading Watson L, Bond CM & Gault C.A survey of community pharmacists on preventionof HIV and hepatitis B and C: current practice andattitudes in Grampian. J Public Health (2003). B3
Objectives To assess the activity, knowledge andattitudes of community pharmacists in Scotland inprevention of HIV and hepatitis B and C infections.
Study design Questionnaire survey of all 970community pharmacies in 10 health boards inScotland.
Sampling and response rate Response rate:76% (740).
Key findings Most pharmacies (70%) wereproviding services for drug misusers. Nearly all(97%) stocked condoms. 59% of pharmacists
period where pharmacy customers were asked tocomplete the questionnaire.
Key findings Feedback on the training waspositive, although not all LHCC staff attended.Most (88%) of those interviewed thought it wasappropriate to offer advice about stress andanxiety management in the pharmacy. At least twosymptoms of stress/anxiety were recognised bytwo-thirds of interviewees. Just over half of thoseinterviewed knew about local self-help groups.150 (90% response) customers completed thequestionnaire. 88% reported that they hadexperienced symptoms of stress/anxiety and 49(33%) had purchased a remedy.Most people (76%) said the GP was their preferredsource of advice on stress/anxiety, friends (36%)and pharmacist (13%).866 leaflets were selected by customers with amedian of 98 per pharmacy (range 41–155). Themost popular resources were sleep and relaxationguides.
reported stocking extra strong condoms and twostocked dental dams. Just under two-thirds saidthey stocked leaflets relating to safer sex, HIV orhepatitis.Fewer than half reported having contact lists forlocal agencies dealing with drug-related or sexualhealth problems. Knowledge of blood-bornepathogens was mixed and pharmacists’ confidencein advice-giving was greater for HIV than foreither hepatitis B or C. Few pharmacists wereaware of recommendations for hepatitis Bvaccination. Most felt that in the futurepharmacists could have a greater role inprevention of these infections. The main barriersto greater involvement were time pressure, lack ofa private area and lack of training.
PREVENTION OF TRANSMISSION OF INFECTION
MENTAL HEALTH
Title, authors, source type, year and evidencegrading Martin-Hamblin-GfK. Osteoporosis Pharmacy Pilot Study (June 2002). B3
Objectives (1) To evaluate whether an osteoporosis screening
service model is effective from the perspectiveof patients, GPs, the primary care team and thepharmacist.
(2) To understand if the community pharmacy is an effective/suitable forum to identify patients athigh risk of future fracture.
(3) To gain an understanding of the programme’s impact on patients’ perception of the role ofthe pharmacy and the perceived benefits topatients.
(4) To understand if the Patient Group Direction element of the service model is effective toallow timely access to treatment (notimplemented, as Patient Group Direction notavailable for the pilot).
Study design Pilot osteoporosis screeningscheme based in one community pharmacy.Telephone interviews with clients (29 low risk fromassessment questionnaire; 75 low risk from bonescan; 29 osteoporotic). Unstructured interviewswith health professionals (pharmacist, pharmacyassistants, nurse, GPs, pharmaceutical advisors).Face to face interviews with pharmacy users in thetarget age group (60+ years).
Key findings Most clients were either invited totake part by pharmacy staff (43%) or saw a posterat the pharmacy (35%). Only 2% became aware ofthe service through posters at the GP surgery. 228
Title, authors, source type, year and evidencegrading McGovern EM, Tennant S & Mackay C.Audit of returned medicines to communitypharmacies. Royal Pharmaceutical Society of GreatBritain Local Health Care Cooperative Conference(2001). C1
Objectives To assess the quantities and types ofmedicines returned to community pharmacies.
Study design For four weeks 10 communitypharmacies recorded all medicines returnedexcluding those dispensed more than 12 monthsearlier and over the counter medicines. Data
patients completed a Risk Assessmentquestionnaire, of whom 49 (21%) were found tobe low risk. The remainder had a bone scan and 36were found to be osteoporotic.Most patients rated pharmacy staff asextremely/very accessible (90%) and professional(83%). Over 90% rated the knowledgeability andclarity of explanation by the nurse conducting thebone scan as extremely/very. The availability of thescreening service at a local pharmacy was highlyvalued (89% giving the top rating). Over three-quarters valued the ability of the pharmacist toprescribe medication without having to visit thedoctor. Three-quarters thought the pharmacysetting was more convenient than their doctor’ssurgery although only just over a half said thiswould make them more likely to use the service.Most said they would use the screeningprogramme again and would recommend it toothers. 80% of patients felt they were treatedwith complete privacy and confidentiality, with18% reporting ‘a degree’ of privacy andconfidentiality and 2% not being treated with anyprivacy and confidentiality. When asked to stateany perceived disadvantages, 5% said lack ofspace, 4% problems with the shop environmentand 2% no proper waiting room. 1% said thatdoctors were more knowledgeable.Commitment and enthusiasm of those involvedwas found to be a significant factor and theauthors say it should be ‘an importantconsideration in the selection of pharmaciesinvolved in any future scheme’.
recorded included the name of the medicine,quantity returned, reason for return andoriginating GP practice. The cost of each returneditem was calculated.
Key findings Over the four week period, 256items with a value of £2411 were returned by 100patients. The median number of returned itemswas 2 (range 1–17). The main reasons for return ofmedicines were because therapy had been altered(54% of patients) or the patient had died (16% ofpatients). Eleven patients (11%) returned 13 itemsbecause of an adverse reaction. The main
78
ACCIDENTAL INJURY PREVENTION
79
therapeutic category was cardiovascular (76 items,30%). The authors report there was evidence ofexcessive quantities having been prescribed. Threepharmacies and two general practitioner surgeries
Title, authors, source type, year and evidencegrading Aston University/MEL Research.Consumer expectations of communitypharmaceutical services. Report to the Departmentof Health (1991). B3
Objectives To determine consumer views ofhealth information leaflets.
Study design Self-completion postalquestionnaire.Consumers were asked if they had noticed anywritten material (leaflets or booklets) availablefree of charge at their pharmacy; if so, whetherthey had taken any away; if so, whether they hadfound the material useful.
Sampling and response rate 224 respondents.
Key findings Nearly two-thirds of ‘high users’ ofpharmacies had noticed leaflets and 37% had bothnoticed leaflets and taken them away to read. Forthe ‘general population’ 48% had noticed leafletsand 23% had noticed them and taken them away.13% of high users had seen and taken leaflets andrated them as very useful compared with 5% ofthe general population. Customers in younger
accounted for 61% and 68% of the returnsrespectively. The results were discussed locally andthe authors report that some changes toprescribing frequency were agreed.
(under 30 years and 30–44 years) age groups weremore likely to have seen leaflets (70%). However,these groups were less likely to have taken awayand read leaflets. In the ‘retired’ group, 40% hadseen them and 20% reported taking leaflets. Menand women were equally likely to have noticedleaflets but women were more likely to have takenthem away and read them.Over a quarter of respondents reported difficultyin identifying the pharmacist and a similarproportion believe ‘the pharmacist prefers to keepout of sight’. ‘Two-thirds of respondents would like to be ableto talk to the pharmacist in private, while only 5%had found and used such facilities to date’.Leaflets passively displayed were missed by nearlyhalf the consumers.The authors concluded ‘There are still many peoplewho are unaware of the pharmacist’s role as anadviser on general health matters’.
Other comments The authors comment thatelderly people were less likely to notice leafletsand to take them away.
Factors affecting the effectiveness of community pharmacy-basedactivities to improve health
Title, authors, source type, year and evidencegrading Coggans N, Johnson L, McKellar S, GrantL & Parr RM Health promotion in community pharmacy:perceptions and expectations of consumers andhealth professionals. Department ofPharmaceutical Sciences, University of StrathclydeReport commissioned by the Scottish Office (June2000). C1
Objectives The aims were to identify: (1) the aspects of health promotion to which
pharmacy customers were most receptive; (2) what methods are appropriate for delivery of
pharmacy health promotion.
Study design Semi-structured interviews with601 pharmacy customers; 30 pharmacists; 30pharmacy assistants. Interviews were taped andtranscribed. Setting: five health bo]ard areas inScotland. Delphi panel of 24 stakeholders incommunity health promotion for consensus onhow and in what ways community pharmacy cancontribute to the health of pharmacy customers.
Sampling and response rate Twenty customerswere interviewed in each of 30 participatingpharmacies. Customers were approached whenthey had completed their transaction (orsometimes while waiting for their prescription tobe dispensed). No refusal rate stated.
Title, authors, source type, year and evidencegrading Shafford A & Sharpe K.The pharmacist as a health educator. ResearchReport 24, Health Education Authority (1989). B3
Objectives To study the perceived and actualneeds of community pharmacists in order todevelop their role as health educators.
Study design Self-completion postal survey. Pro forma diary of health enquiries.
Sampling and response rate Survey sent to allcommunity pharmacists in North East ThamesRegional Health Authority (897). Response rate:58% after two reminders. Comparison of
pharmacy ownership type of responders withregional data showed a similar profile. Pro formadiary of health enquiries completed by self-selected sub-sample. The profile of pharmacyownership type was similar to regional profile.
Key findings Of the survey respondents, 61.7%reported having a suitable area or room forconfidential discussions. One in four pharmacieshad a consultation room. 74% reported that theirundergraduate education gave them ‘no’ or ‘poor’training in advice-giving on health educationtopics and 48% said this about their pre-registration training.
Authors comment that the sample included ahigher proportion of women, older people andprofessional people than the general population.
Key findings Of the customers interviewed, 37%had visited a pharmacy at least once a week, 17%at least once a fortnight, and 32% at least once amonth. Women reported visiting pharmacies moreoften than men. 86% were willing to discuss theirprescribed medicine with the pharmacist if theywere having problems. 84% were willing to seekpharmacy advice about minor health problems.Less than one-third (32%) were willing to seekadvice on healthy eating in the pharmacy. 22%said that either they did not see this as part of therole of community pharmacy or that it had notoccurred to them that pharmacies could providesuch advice. Among smokers who could beconsidered to be contemplating quitting, 66% feltpositive about obtaining advice on smokingcessation in the pharmacy. One-fifth (20%) werewilling to seek advice about exercise from thepharmacy.When asked about willingness to get help on asensitive or personal problem in the pharmacy,33% said yes and 52% said no. The pharmacy wasperceived to provide adequate privacy fordiscussion of sensitive topics by 18% of customers,with 68% saying no. 68% believed their discussionsin the pharmacy would be confidential, theremainder giving negative or uncertain responses.Women were significantly more likely than men tosay that they would discuss a sensitive subject andthat confidentiality would be maintained.Leaflets were seen by customers as a principalsource of information with 70% saying they
obtained information this way. Pharmacistsperceived sun protection, prescribed medicines andsmoking cessation as being the health topics mostacceptable to the public for pharmacyinvolvement. Diet, exercise and ‘sensitive topics’were seen as much less acceptable. Pharmacistswere ‘willing and eager’ to discuss a range ofhealth issues with customers, although there wassome reluctance in relation to lifestyle issues aswell as awareness of privacy as an issue.The Delphi group rated priority targets:1. Increase the proportion of customers who
perceive there to be enough privacy in thepharmacy to discuss something sensitive orpersonal.
2. Increase the proportion of pharmacy customers who believe that all discussions with pharmacistsare treated as confidential.
3. Increase public willingness to use community pharmacy for smoking cessation.
4. Increase the proportion of customers willing to discuss any problems with their prescribedmedicines with the pharmacist.
5. Maximise the availability and potential of health education leaflets.
Increasing public willingness to use pharmacies foradvice on healthy eating and exercise were rankedsixth and eighth respectively.
Other comments The authors comment that:(1) the findings indicate a widespread perceptionthat community pharmacy does not providesufficient privacy for discussion of sensitive topics;(2) there is a need to reassure the public aboutconfidentiality being part of pharmacy’sprofessional ethos.
80
81
45% reported displaying health education leafletsand 56% believed leaflets to be of ‘great’ or ‘verygreat’ importance. Advice-giving was reported asof ‘great importance’ on prescribed medicines by52% of respondents; over the counter medicinesby 45% and health education by 18%.Pro forma diaries of health enquiries showed that3% of recorded enquiries were on general healthqueries. The busiest time of day for these enquiriescoincided with the busiest time for dispensing. The
Title, authors, source type, year and evidencegrading Hariri, S.Multimedia health promotion in communitypharmacy. PhD thesis Department of Pharmacy,King’s College, London (1998). C1
Objectives To investigate the usability ofmultimedia touch screen kiosks as tools for healthpromotion within the community pharmacysetting; to examine the effect of such a kiosk onthe public’s use of their community pharmacy as asource of health information.
Study design A touch screen multimedia kioskwith the CardioPharm program was installedinitially in three community pharmacies (study 1)and subsequently in three supermarket pharmacies(study 2). Data were collected as users accessed thesoftware. Observation was conducted in thepharmacies (study 1). Interviews were conductedwith the pharmacists (study 1). Users in the threesupermarket pharmacies were asked to complete aquestionnaire.
Sampling and response rate Questionnaireresponse rate not known.
Key findings The total numbers of user
time taken to deal with general health queries waslonger than that for symptom, OTC or dispensedmedicine queries.The authors concluded that ‘at present, thegeneral public do not see the pharmacist as ageneral source of health information’ and that ‘itis important to educate and encourage the generalpublic to use the community pharmacist as asource of general health information’.
interactions were 847 in study 1 and 11,590 instudy 2. The completion rates were 31% and 37%respectively. Most users in both studies were agedbelow 40 and had a healthy Body Mass Index (BMI)of 25 or less.There was a significant increase in the healthpromotion activity of the pharmacies includingmore queries to the pharmacist and highernumbers of leaflets taken. Observation indicatedthat some older customers requiredencouragement and a demonstration by pharmacystaff before they used the kiosk.154 users completed the questionnaire in study 2.Most agreed that touch screen systems were agood method of providing information to thepublic. The majority agreed that the pharmacy wasan appropriate environment for informationkiosks. None of the users reported having askedpharmacy staff for information or advice.
Other comments Most customers who accessedthe software were in younger age groups. Thereasons for the low completion rate are notknown. Consideration needs to be given to how toengage older customers in use of such systems.
Stakeholder views
Title, authors, source type, year and evidencegrading BMRB InternationalBaseline mapping study to define access to andusage of community pharmacy. Reportcommissioned by Royal Pharmaceutical Society ofGreat Britain (March 1996). B3
Objectives To determine who uses what type ofpharmacy, when, for what (prescription medicine
related, over the counter medicine related, healthylifestyles) and in what locations.
Study design Face-to-face, in-home structuredinterviews with 517 adults aged 16 years or over.Inclusion criterion was that respondents had useda pharmacy for at least one of the corecomponents in the past year, either for themselvesor for someone else.
Title, authors, source type, year and evidencegrading Hassell K, Rogers A, Noyce P & Nicolaas GThe public’s use of community pharmacies as aprimary health care resource. Report to theCommunity Pharmacy Research Consortium(November 1998). B3
Objectives To map and describe what is currentlyknown about how the public use pharmacies. Toprovide retrospective and prospective data onpharmacy usage in the context of how otherprimary and secondary resources are used. Toexplore what influences the choice of primary careservice provider.
Study design Review of published literature.Secondary analysis of general populationhousehold survey and health diary data. Linkedqualitative study of interviews with users and non-
Title, authors, source type, year and evidencegrading Anderson C.Health promotion by community pharmacists. PhDthesis, King’s College, London (1997). B3
Objectives To investigate the effect of a trainingprogramme on the role of community pharmacistsin health promotion; to investigate consumers’perceptions of the community pharmacist’s role
Study design Interviews with pharmacists in theBarnet High Street Health (HSH) scheme (who hadparticipated in the training programme) and a‘control’ area. Covert study of pharmacists’ adviceon smoking cessation in 20 HSH pharmacies and 20controls. Consumer survey using questionnaireadministered in six HSH pharmacies. Telephonesurvey of health authority pharmaceutical advisersin England.
users of community pharmacies.
Sampling and response rate Survey of healthstatus and health care use by 834 residents in 346households. Sample drawn from three areas(urban, suburban, market town/semi-rural).Screening was used and frequent health serviceusers were over-sampled.Health diaries completed by 549 people in 215households. Interviews with sub-sample of 41 diaryrespondents.
Key findings Frequency of pharmacy use washigh, mainly restricted to the prescription service.Most people self-managed their conditions, with5.5% using the community pharmacy for advice.The pharmacist’s profile was perceived as ‘that of adrug expert – advising on medicines not illness’.
Sampling and response rate Ten HSH schemepharmacists and ten ‘controls’ were interviewed.592 consumers took part in six participatingpharmacies in the HSH scheme.
Key findings Interview data showed that theHSH pharmacists were more actively involved inhealth promotion and had a more holistic view ofhealth. They perceived different barriers toimplementing the health promotion role.Pharmacists who received training had increasedknowledge of health promotion, they expressed adesire to spend less time dispensing prescriptionsand more time advising customers.The covert research showed that HSH pharmacistsspent significantly longer in the consultation onsmoking cessation and used leaflets moreappropriately.
Sampling and response rate Random LocationSampling was used, using Enumeration Districts assampling points, with quota sampling.
Key findings Of those sampled, 94% were foundto have used a pharmacy in the last year for one ofthe three core reasons. On average pharmacieswere used once a month, with women andrespondents with children under five years morefrequent users. Other frequent users were those ininner cities and ‘striving’ ACORN (A Classificationof Residential Neighbourhoods) type. Least
frequent users were 16- to 24-year-olds and‘expanding’ ACORN type. Usage levels were: 90%prescriptions; 30% seeking advice on specificsymptoms/problems; 10% seeking general healthadvice. 16- to 24-year-olds had a ‘particularly low’usage for general health advice. Usage for thisreason was higher among women, respondentswith young children and C2DEs. Unsolicited healthrelated advice was reported by 14% of respondents.Over half (53%) of the people receiving this advicereceived it twice or more often.
82
83
Consumers believed that the doctor was the bestand most convenient person to go to for adviceabout staying healthy. 40% of consumers believedthat it was the ‘usual job’ of the pharmacist toadvise on staying healthy but only 15% had ever
asked for such advice. The telephone survey data showed that 57% ofhealth authorities reported at least some healthpromotion activity.
Title, authors, source type, year and evidencegrading Anonymous.The Pharmacy Healthcare Scheme (Qualitativestudy). Health Education Authority. ResearchReport (1993). B3
Objectives To examine the overall work of thePharmacy Healthcare Scheme from thepharmacist’s perspective; to look at the role of thepharmacist in health promotion.
Study design Qualitative interview studyconducted in parallel with quantitative survey.
Sampling and response rate Letter ofinvitation sent to 180 community pharmacies inEngland (including London), Scotland and Wales.Half were multiples and half independents. Halfwere ‘in town’ and half ‘out of town’. 21% (39) ofpharmacists agreed to be interviewed, 24%declined and 55% did not reply. London had an11% agreement rate and Edinburgh 50%. Of the39 interviewees 17 were from independents and22 from multiples.
Key findings The approximate time splitbetween dispensing / responding to symptoms andadmin/paperwork was 70/30%. None of thepharmacists identified a specific time allocation for
Title, authors, source type, year and evidencegrading Health Promotion Authority Wales.Pharmacy Health Care Scheme survey (Wales).Report.. Health Promotion Authority Wales &Welsh School of Pharmacy (1991). B3
Objectives Determine levels of health promotingactivities by community pharmacists in Wales; toidentify practical measures to increaseinvolvement.
Study design Self-completion postalquestionnaire.
Sampling and response rate 1081 pharmacistsin Wales (all practising pharmacists registeredsince 1940). Response rate: 67% (724) after two
health promotion. The report states that 5% ofoverall time (within dispensing / responding tosymptoms) was spent on health promotion.Although pharmacists perceived health promotionas important the researchers noted that:‘pharmacists’ health promotion role is reactive notproactive’; ‘the pharmacist’s role is very muchorientated towards medical advice, healthpromotion happens during this process’; ‘advice isprovided to the public on request as pharmacistsdo not provide health promotion advice directly’and ‘the pharmacist’s health promotion role isdeveloping – moving away from pure dispensing.‘A sizeable number’ of pharmacists believed thatthe public do not recognise the extent of theirtraining and skills and see them as shopkeepers,not health educators. Pharmacists reported beingisolated from the primary health care team, withno structured or formal communication channelsand little collaborative work.
Other comments The report recommendednational publicity to raise public awareness of thepharmacist’s role in health promotion. Research onthe public’s perceptions of pharmacy was alsorecommended.
reminders. The authors state that 522 pharmacypremises were represented in the survey returns.Comparison of years registered, gender andemployment status for responders, late respondersand non-responders showed similar profiles. Instatistical analysis P<0.001 assigned as significant.
Key findings Only 13.5% rated health promotionas being of ‘little’ or ‘no’ importance. Figures forspecific services/ activities were: pregnancy testing310; weight measurement 156; sale ofneedles/syringes 151; blood pressure measurement80; needle / syringe exchange 40; cholesteroltesting 16; lung function testing 7. 106 and 118respondents reported planning to introduce bloodpressure and cholesterol measurement respectively.

Title, authors, source type, year and evidencegrading BMRBPharmacy Healthcare scheme (Quantitative study).Health Education Authority. Report (1993). B3
Objectives Examine how pharmacists view theirrole in health promotion and health education; toobtain pharmacists’ views as users of the PharmacyHealthcare Scheme on its effectiveness.
Study design Pre-piloted postal questionnaire.
Sampling and response rate A total of 1986community pharmacies were sampled fromLondon, rest of England, Scotland, Wales andNorthern Ireland. Response rate: 67% after onereminder. A higher percentage (91%) of Bootspharmacists replied cf. 64% of others. At analysis,data were weighted to the profile of the originalsample to correct for differing response rates.
Key findings Of respondents, 45% worked forindependents and 18% at multiples with 50
Title, authors, source type, year and evidencegrading Dewsbury-Mason CCommunity pharmacists and health promotiontraining, activities and attitudes. MSc thesis,University of Kent (1998). B3
Study design Cross-sectional survey.Questionnaire to 100 community pharmacists inone UK area.
Sampling and response rate Response rate: 66%.
Title, authors, source type, year and evidencegrading Elliott J.The role of community pharmacists in relation tothe primary health care team. Reportcommissioned by the Health Education Authority(1996). B3
Objectives Identify a sample of communitypharmacists working with the primary health care
branches. Most pharmacists reported thatPharmacy Healthcare Scheme leaflets were left tobe picked up by customers with only a smallnumber of leaflets taken on the pharmacist’srecommendation. The researchers note that ‘thereis clearly a desire amongst many pharmacists tobecome more involved in the area of healthpromotion and education’. 77% reported spendingone, two or three hours a week on healthpromotion and most said this was increasing. 84%reported insufficient financial incentives and 66%insufficient time for health promotion. Pharmacistswere also ‘keen for the public to be bettereducated about the role of pharmacists in healthcare in general’.
Other comments Pharmacists ranked the relativeimportance of pharmacists being able to giveinformed advice on specific topics as: smoking54%; diet/nutrition 37%; family planning 21%;exercise 14%; drinking 13%.
Key findings A holistic view of health was notpredominant among community pharmacists andonly 5% identified health as ‘an absence of illness’.86% of pharmacists said they would be willing toundertake further training in health promotion.Just over half (53%) had undertaken some trainingin health promotion. Time, remuneration andpremises were seen as the main barriers toinvolvement in health promotion.
team; areas of collaboration; the extent to whichthe focus of collaboration involved healthpromotion; identify barriers to team working.
Study design Postal survey of pharmacistsInterviews with health authority pharmaceuticaladvisers (3), local pharmaceutical committeesecretaries (3), community pharmacists (15),primary care team members (9).
Barriers to health promotion activities werereported as: finance 54%; public apathy (34%);professional relationships with GPs (31%) and lackof knowledge (22%) .
Other comments Commentary notes that
‘Pharmaceutical Care: the future for communitypharmacy’ recommended that diagnostic andscreening services should be provided bycommunity pharmacies and discusses this aspect.
84
85
Sampling and response rate Questionnairesent to 373 community pharmacists in three areas(Cumbria, Liverpool, Northamptonshire). Responserate: 78% (290) after one reminder.Semi-structured interviews with sample of 15community pharmacists (self-reportedcollaboration with primary care team inquestionnaire) and other health professionals (9 of16 agreed to be interviewed) identified by the sub-sample of community pharmacists as working withthem.
Key findings Regular meetings with primaryhealth care team reported by 14% of surveyrespondents. Collaboration on projects orinitiatives reported by 13%. Collaboration focusedon prescribing and medicines. Pharmacistsdispensing higher prescription numbers were morelikely to report collaboration. Barriers tocollaboration were: lack of time; lack of funding;lack of opportunity to meet other healthprofessionals; perception that pharmacist’s input
not wanted. Seven of 18 pharmacists who madeadditional comments said they ‘had not beenasked’ to collaborate. Close proximity to the GPpractice with no other pharmacies nearby wasassociated with collaboration.Interview data suggested that survey resultsoverestimated the amount of collaboration andteamwork (10 of 15 pharmacists self-reportingcollaborative work were doing so, the remainderwere minimal or intermittent).Interviews with pharmaceutical advisers identifiedlocal initiatives organised by health authorities.However, these were ‘for limited time periods,with limited funding and inadequate evaluation’and generally involved an enthusiastic minority ofpharmacists.
Other comments One-third (32%) of pharmacistsreported that most of their prescriptions camefrom one GP practice; 19% from two; 21% fromthree to four; and 29% from more than four.
Title, authors, source type, year and evidencegrading Scott K.Involvement of community pharmacists in HealthEducation Authority (HEA) primary health careteam workshops – Report on qualitativeevaluation. Report for HEA (1994). B3
Objectives To explore: community pharmacists’perceptions of their role within primary care;primary health care team PHCT workers’perceptions of the community pharmacist; thenature and extent of working relationships; initialand longer term impact of pharmacist involvementin PHCT workshops.
Study design Nine practice teams were involved.Pre-workshop interviews with eight pharmacistsand 36 PHCT members. Interviews one week post-workshop with eight pharmacists and 32 PHCTmembers. Unclear how PHCT members wereselected. Three months post-workshop, groupinterview with eight pharmacists and postalquestionnaire to PHCT members (21 respondents).
Sampling and response rate Response rates:100% stage 1; 90% stage 2; 72% stage 3.
Key findings Community pharmacists were rarelymentioned spontaneously as part of the PHCT.
Although PHCT members expressed confidence inindividual pharmacists they often expressedconcerns about community pharmacy in general inrelation to possible wider roles. The main concernswere about pharmacists’ lack of access to patients’full medical history and about potential conflictsarising from commercial activities. Neverthelessmost PHCT members (particularly GPs, practicemanagers, practice nurses and district nurses)welcomed the idea of greater involvement ofcommunity pharmacists.While the community pharmacists were pleased tobe invited to attend the workshop they alsoexpressed anxieties about what they would beable to contribute and about how theirparticipation would be received by PHCT members.Three months after the workshop there wasevidence of greater contact (pharmacists invited topractice meetings by most practices) and a numberof joint activities (e.g. referral of diabetic patientsto the pharmacy by the diabetic nurse and viceversa; joint GP/pharmacist asthma session forschool nurses). Both pharmacists and practicesreported difficulties in pharmacists being able toleave their premises to attend practice meetings.

ISBN 0 9538505 5 2
Designed by A.R.T. Creative Partnership
What role, if any, should pharmacies play inimproving the health and well-being of thegeneral public? Situated, as they often are,at the heart of their communities, they arein a unique position to provide help andadvice on health matters to a completecross-section of society at the same time asdispensing medicines. But is there anyevidence that customers would actuallybenefit from such advice?
Bringing together, summarising andcategorising research papers on such diversetopics as stopping smoking, lipidmanagement and drug misuse, this reportprovides strong evidence that pharmaciescan indeed make a positive contribution toimproving the health of the nation – afinding that supports the recommendationof the recent Health Committee Inquiry intoPublic Health that ‘community pharmacistsplay a more active role in public health’.
By adopting some of the activities described,pharmacies across the country will not onlybe aiding the treatment of disease they willbe improving the health of their customersat the same time. This report will makeinteresting reading for all those concernedwith meeting health improvement targets,planning future services and integratingcommunity pharmacy activity with that ofthe wider NHS.





























