Embed Size (px)
Citation preview

The Effect of Modafinil on Cognitive Function in Breast CancerSurvivors
Sadhna Kohli, PhD, MPH1, Susan G. Fisher, PhD2, Yolande Tra, PhD3, M. Jacob Adams,MD, MPH2, Mark E. Mapstone, PhD4, Keith A. Wesnes, PhD5, Joseph A. Roscoe6, and GaryR. Morrow, PhD, MS6
1Department of Medicine and Radiation Oncology, James. P. Wilmot Cancer Center, University ofRochester, Rochester School of Medicine and Dentistry, Rochester, New York2Department of Community and Preventive Medicine, University of Rochester, Rochester Schoolof Medicine and Dentistry, Rochester, New York3School of Mathematical Sciences, Rochester Institute of Technology, Rochester, NY4Department of Neurology, University of Rochester, Rochester School of Medicine and Dentistry,Rochester, New York5Cognitive Drug Research Ltd., Goring-on-Thames, UK6Department of Radiation Oncology, James. P. Wilmot Cancer Center, University of Rochester,Rochester School of Medicine and Dentistry, Rochester, New York
AbstractObjective—We conducted a randomized clinical trial examining the effects of modafinil inreducing persistent fatigue in patients following treatment for cancer and performed secondaryanalyses to assess the effect of modafinil on cognitive function.
Methods—Breast cancer patients who reported a score of ≥ 2 on the Brief Fatigue Inventory(BFI) were enrolled in the study. In Phase 1 (P1), patients received 200mg modafinil open-labelonce daily for 4 weeks. In Phase 2 (P2), patients with a positive response following P1 wererandomized either to an additional 4 weeks of modafinil or to placebo. Tests of memory andattention selected from the Cognitive Drug Research (CDR) computerized cognitive assessmentwere performed at baseline (before modafinil) and after completing Phase 1 and 2. The paireddifferences for each test score were subjected to a Wilcoxon's signed rank test.
Results—Of the 82 women who were enrolled, 76 completed P1 and 68 completed allassessments in the study. Modafinil had a significant effect on the Speed of Memory (p=0.0073)and Quality of Episodic Memory (p<0.0001) during P1 of the study. After randomization at week8, those patients who continued modafinil demonstrated significantly greater improvement inSpeed of Memory (p=0.029), Quality of Episodic Memory (p=0.0151) and mean Continuity ofAttention (p=0.0101) relative to the group switched to placebo.
Conclusion—We found that modafinil improved cognitive performance in breast cancersurvivors by enhancing some memory and attention skills. Although confirmation is needed, thesefindings suggest that modafinil may enhance quality of life in this patient population.
CORRESPONDING AUTHOR: Sadhna Kohli, PhD., MPH, Mayo Clinic, 200 First St SW, Rochester, MN [email protected].
NIH Public AccessAuthor ManuscriptCancer. Author manuscript; available in PMC 2010 June 15.
Published in final edited form as:Cancer. 2009 June 15; 115(12): 2605–2616. doi:10.1002/cncr.24287.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Keywordsmodafinil; cognitive function; memory; attention; breast cancer
IntroductionFollowing cancer treatment, some breast cancer survivors report cognitive impairment,which has commonly been attributed to the receipt of chemotherapy and colloquially termed“chemobrain” (1). Cognitive deficits identified by cancer survivors consist of a range ofdifficulties including memory and concentration problems that can emerge during cancertreatment and continue to have long-term effects for many months and years after itscompletion (2-8). Impairment of brain function profoundly affects cognition, psychologicalwell-being, and the ability to perform the usual activities of daily living.
Changes in cognitive function may be confused with or confounded by other problemscommonly associated with cancer and its treatment, such as depression, anxiety, and fatiguecaused by sleep deprivation (9-11). Although the phenomenon is not understood completely,cognitive deficits in cancer patients are assuming greater significance as cancer survivalimproves. Advances in basic sciences, imaging, and clinical sciences are beginning tounravel pathophysiologic mechanisms which may underlie this problem (12).Pharmacologic treatment options for cognitive deficits in cancer survivors are borrowedfrom diverse diseases including attention-deficit/hyperactivity disorder andneurodegenerative diseases (13,14). Conventional therapies soon may find new applications;for example, recent preclinical data suggest that modafinil (Provigil®) may have somecognitive-enhancing abilities, which may positively affect patients who experience“chemobrain”.
Modafinil is a novel wake-promoting agent that is effective and well tolerated in thetreatment of excessive sleepiness associated with narcolepsy and in persons with shift-worksleep disorder (15-19). The precise mechanism(s) through which modafinil promoteswakefulness is unknown. Modafinil has wake-promoting actions like those ofsympathomimetic agents including amphetamine and methylphenidate, although thepharmacologic profile of modafinil is not identical to that of the sympathomimetic amines.The recommended single daily dose range for narcolepsy is 100-400mg modafinil(Provigil®). These doses have wake-promoting efficacy comparable to 20-40mg doses ofmethylphenidate (20), which has been used previously in cognitive studies in patients withadvanced cancer (21).
We completed a study examining the effect of modafinil on fatigue and sleep complaints in82 breast cancer patients following completion of chemotherapy (22). Patients received 200mg modafinil once daily for one month. Of the 82 women enrolled, 76 completed the studyand began the study medication. A majority, 68 of the 76 women (90%) who completed theone-month study, reported improvement on all four measures of fatigue used (23-26), all p <0.001 (Figure 1). In addition, the Epworth Sleepiness Scale showed a 22% decrease (p <0.01), and the “disturbed sleep” symptom on the symptom inventory (27) decreased morethan 45% (p < 0.01).
Despite these findings, little is known about the causes of cognitive changes seen during andafter cancer treatment. It seems reasonable to assume that they are related, at least in part, toother psychological and biological treatment complaints such as fatigue, sleeping problemsand depression (10,28). The nature of the relationships among these variables, however,both at onset and over time remains unclear.
Kohli et al. Page 2
Cancer. Author manuscript; available in PMC 2010 June 15.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

To our knowledge, in spite of evidence that modafinil acts as a cognitive enhancer in healthysubjects (29-31), no study to date has examined the effect of modafinil on a wide range ofcognitive functions using a comprehensive and well-validated neuropsychological testbattery in cancer patients. Therefore, as modafinil was effective in reducing persistentfatigue in our primary study (22), we conducted secondary analyses to assess the effect ofmodafinil on cognitive function and to examine whether modafinil might act as a cognitiveenhancer in breast cancer patients who have completed treatment for cancer.
MethodsGeneral study procedures
Eighty-two breast cancer patients between the ages of 33 and 83 years, who were more thanone-month post-chemotherapy and/or radiation treatment for an initial diagnosis of cancer,able to swallow medication, and had a score of 2 or greater on a Brief Fatigue Inventory(BFI) (25) question of “fatigue worst”, and who completed participation in the primarystudy “Modafinil to Treat Persistent Fatigue in Patients Following Treatment for Cancer(22)” are included in this secondary analysis. These patients were approached for theprimary study by their medical oncologist either at a regularly scheduled appointment at theMedical Oncology clinic at the University of Rochester NY, by telephone or a standardizedletter in the mail. It was explained to the patients that fatigue is a subjective symptom withindividual meaning which may be described using a variety of words and phrases such as“weak and tired,” “no energy,” “can't get motivated,” or “trouble breathing” (32). Thepatient then completed question 3 of the BFI. If the patient responded to question 3 of theBFI with an answer of 2 or greater than 2, the patient was invited to participate in the study,however, if the patient responded with an answer of 1, the patient was considered ineligiblefor the study. The University of Rochester Research Subjects Review Board approved theprimary study, and all patients provided written informed consent.
In Phase 1 of the study, patients received one tablet of 100mg of modafinil once a day forthe first three days and then two tablets (200mg) open-label once daily for 4 weeks. In Phase2, patients with a positive response following Phase 1 were randomized either to anadditional 4 weeks of modafinil (200mg) or to placebo. Tests of memory and attentionselected from the Cognitive Drug Research (CDR) computerized cognitive assessment wereperformed at baseline (before modafinil) and after completing Phase 1 and 2.
Potential research subjects were excluded if they had taken modafinil previously, had takena psychostimulant or a monoamine oxidase inhibitor within the past 30 days, or werecurrently taking an anticoagulant, α-interferon, interleukin-2, or a corticosteroid. Individualswith a history of clinically significant cardiac disease, uncontrolled hypertension, alcohol ordrug abuse, severe headaches, glaucoma, seizure disorder, narcolepsy, psychotic disorder, oruncontrolled Tourette's syndrome were also excluded. If a steroidal contraceptive was beingused for fertility control, participants had to agree to use a barrier method of contraceptionduring the study and for one full menstrual cycle following the study.
RandomizationAfter four weeks of open-label modafinil, patients who met the eligibility criteria wererandomized to one of two trial arms by means of randomly ordered sealed envelopes.Participants were stratified by treatment regimen (completed chemotherapy alone orradiation alone or chemotherapy plus radiation) and were assigned to either continue 200mgmodafinil orally once each day or switch to a matching placebo orally once each day.
Kohli et al. Page 3
Cancer. Author manuscript; available in PMC 2010 June 15.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

AssessmentsThe Cognitive Drug Research (CDR) system was used to assess major domains of attentionand memory. The CDR system is designed to provide the drug development process with astable, practical, validated and sensitive platform to enable important cognitive andbehavioral effects of medicines to be captured and evaluated. Its validity, test-retestreliability and sensitivity have been demonstrated in several populations (33-36).
The CDR system comprises both custom-built tests (e.g. digit vigilance, spatial workingmemory) plus tests whose general methodology is widely known (simple and choicereaction time, word recall). All tests have been standardized, extensively validated, andimplemented with a software and hardware platform which enables responses to be recordedwith true millisecond accuracy.
The system has been used worldwide since 1984 in over 500 clinical trials. Data from thesystem have been the subject of over 100 peer-reviewed papers, more than 20 chapters, and300 published abstracts (37). An advantage of the CDR system is that many of the tests usedare generic and generally accepted for use in psychopharmacology research. Further,because it has been used in hundreds of studies, extensive normative data exists frompopulations ranging in age from 12 to 90 years.
In recent years CDR has identified major factors reflecting distinct and importantdimensions of human cognitive function. The measures which contribute to these factors arecombined to produce factor scores. These factor scores are unique to the CDR system andthus the CDR offers a highly sensitive way of assessing broad but distinct aspects ofcognitive function.
The sensitivity and reliability of these tests for detecting cognitive impairment in a variety ofclinical conditions (e.g., normal aging, depression, post stroke, schizophrenia, and attentiondeficit disorder, all of the major dementias, head trauma, and drug-induced cognitivechanges) have been demonstrated (38-45). The CDR battery is sensitive to treatment effects,including pharmacologic therapies (44-53).
Table 1 shows a summary of the measures contributing to the analyses of the CognitiveDrug Research (CDR) computerized assessment system.
Statistical AnalysisThe main objective of this study was to evaluate the efficacy of modafinil in alleviatingcognitive impairment in cancer patients following completion of cancer therapy. Powercalculations demonstrated that with our sample size of 34 subjects in each group, we wouldbe able to detect an effect size of 0.62 standard deviations, using a two-sided p-value of <0.05 for statistical significance. If the standard deviation of the change score was 1, then thedifference of change score detected was 0.62; if the standard deviation was 2, then thedifference detected was 2×0.62, with a power of 0.939. The primary independent variablewas treatment group, and the dependent variable was the change in scores afterrandomization (week 4 to week 8). The primary outcome measures chosen for thesecomparisons were the change in the factor scores of Speed of Memory and Continuity ofAttention with the rationale that those patients who experience “chemobrain”, self-reportproblems with their memory and concentration (54), and to investigate whether theseoutcomes may prove sensitive to modafinil. Differences in assessment scores using pairedsamples from baseline (week 0) to randomization (week 4) and baseline to post-treatment(week 8) were also compared across the entire study sample. If the distribution of thedifferences between pairs was non-normally distributed, the Wilcoxon's signed rank test wasused to assess the change within each treatment group. All statistical tests were two-sided
Kohli et al. Page 4
Cancer. Author manuscript; available in PMC 2010 June 15.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

and performed at the 5% level of significance. Data analysis was performed using SASsoftware version 9.1 (SAS Institute, Cary, North Carolina, USA).
ResultsSubject characteristics
Of the 82 eligible patients, six dropped out before completing the open-label phase: twocomplaining of anxiety, two reporting headaches, and one reporting nausea dropped outduring the first week (all were very slight with weights under 110 lbs), while a final patientfound herself unexpectedly pregnant midway through the study and was withdrawn (Figure2). The characteristics of the six participants who did not complete all assessments duringrandomization were very similar to those who did complete the study. The six patients werewhite, and most had received some college education. Most adverse events were consideredby the investigator to be mild or moderate in severity (defined as no or some limitation ofusual activities), occurred with greatest frequency during the first two weeks of open-labeltherapy, and were self-limited.
Seventy-six breast cancer survivors completed the one month open-label study (agerange=33-83 years, median age =54 years). These women were Caucasian (n=74, 97%),married n=51, (67%), had at least some college education (n=57. 75%), and the majority(n=45, 59%) were employed in professional occupations. All subjects had been treated withsurgery and chemotherapy with 65 (86%) also receiving radiation therapy.
Upon assessment at week 4, an additional eight patients failed to meet the eligibility criteriato continue onto the randomization phase of the study, because they showed noimprovement in fatigue during the open-label phase. The remaining 68 (83%) survivorswere randomized, and they all fully completed the assessments—open-label andrandomization—between weeks 0 and 8 of the study. These 68 are included in theseanalyses. Baseline descriptive data for both the open-label phase and drug and placebogroups following randomization are shown in Table 2.
The connection between aging and cancer is significant; more than 60% of all cancers occuramong those over age 65. There is little information regarding the effect of adjuvantchemotherapy on the older patient's cognitive abilities and whether the chemotherapy affectsthe patient's ability to maintain functional independence (55). The modafinil group mean agewas five years younger than the placebo group in this analysis, however, independent t-testsrevealed no statistically significant differences in age (P=0.066), education (P=0.921) oroccupation (P=0.182) between the two randomized groups: modafinil (N=34) and placebo(N=34). Finally, we examined differences in fatigue and depression between the groups. Inprevious research, both fatigue and depression have demonstrated a potential to affectcognitive performance. However, no statistically significant differences between drug andplacebo groups were observed for these variables (fatigue p=0.21 and depression p=0.46).
AnalysesCognitive Drug Research (CDR) battery—Overall results of the CDR composite meanscores are summarized in Table 3.
Open-label (week 0 to week 4)—In this study of 68 participants, the analysis of theprimary outcome factor, the Speed of Memory Index, revealed a significant effect ofmodafinil (mean change=240.003 seconds, p=0.0073,). This index was computed as acombination of four factors which included speed of numeric working memory, speed ofspatial working memory, speed of word recognition and speed of picture recognition (Figure
Kohli et al. Page 5
Cancer. Author manuscript; available in PMC 2010 June 15.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

3). There was also a statistically significant effect of modafinil on the Digit Vigilance test(one of the measures in Continuity of Attention; mean change 1.623 units, p=0.0014,) duringthe four weeks of modafinil therapy. However, modafinil produced no significant effect onthe composite Continuity of Attention (p=0.0568).
Three measures— immediate word recall (mean change 8.59375, p<0.001), wordrecognition accuracy (mean change 6.985 units, p=0.0002), picture recognition accuracy(mean change -138.281 seconds, p= 0.0054) in Quality of Episodic Secondary Memory alsoshowed a statistically significant mean improvement from baseline to week 4. Overall,significant improvement was observed in Quality of Episodic Secondary Memory (meanchange 26.826 units, p<0.0001) from baseline to week 4 (figure 3).
Modafinil showed no effect on Quality of Working memory (p=0.2475) nor on Power ofAttention (p=0.9031) in the open-label phase.
Randomization (drug vs. placebo, week 4 to week 8)—Randomization did not havea significant effect on each outcome measure of any one factor score. However, modafinildemonstrated a cumulative improvement from baseline to week 8 in composite Speed ofMemory scores (p=0.029) compared to placebo (p=0.116) and for composite Quality ofEpisodic Secondary Memory, the scores in the drug group show significant change(p=0.015) compared to the placebo group (p=0.155). Improvement was observed at the week4 visit and was maintained throughout the study.
About 70% of the subjects in the active drug group had an improvement in Continuity ofAttention from baseline to post-treatment (week 8), compared to 52% in the placebo group,but the difference was not significant (p=0.19). The active drug produces a better response,an improvement over the week 4 assessment where no significant effect was seen (Figure 4).At the final visit (week 8), mean Continuity of Attention improved for the modafinil group(p=0.010) compared with placebo (p=0.54).
There was no significant effect of modafinil on Quality of Working Memory or Power ofAttention during the randomization phase.
Study LimitationsThis secondary analysis has some limitations. The patients in this study tended to be moreeducated than the general population and were primarily Caucasian, making these resultsless generalizable to patients from minority groups or those of lower socioeconomic status.In addition, the original study recruited 82 breast cancer patients, but for the purpose of thisstudy, we have only analyzed data from the 68 patients who completed all three CDRassessments. Although this reduction in patient numbers may have resulted in a biasedsubsample, it should be remembered that patients were not randomized if they failed torespond to open-label modafinil in terms of the primary outcome of the original study—i.e.,fatigue, not cognitive improvement. Furthermore, as Table 1 demonstrates, the 68completers did not appear to differ from the 76 individuals who had no side effects, and thepurpose of this secondary analysis is to determine whether sufficient evidence indicates thatmodafinil improves cognitive function to support further trials to demonstrate this resultmore conclusively. For a future study, we propose a longitudinal design whereby patientsare recruited prior to chemotherapy and randomized to modafinil or placebo, and cognitiveperformance is evaluated before chemotherapy and again three and six month's post-chemotherapy. This strategy would directly establish the presence of cognitive deficitsrelated to chemotherapy and determine whether modafinil alleviated those deficits.
Kohli et al. Page 6
Cancer. Author manuscript; available in PMC 2010 June 15.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

DiscussionModafinil is a wakefulness- and alertness-enhancing agent currently approved for treatmentof excessive daytime sleepiness associated with narcolepsy, obstructive sleep apnea/hypopnea syndrome, and shift-work sleep disorder. Modafinil belongs to a class of drugscalled eugeroics (meaning “good arousal”). Its uniqueness lies in its ability to only“stimulate when stimulation is required” (56). As a result, the “highs and lows” associatedwith other stimulants such as amphetamine, are absent with eugeroics. Modafinil appears toproduce its effects via different neural mechanisms than conventional stimulants or otherpsychotrophic drugs with similar effects on wakefulness and alertness, and it does not seemto stimulate dopamine transmission in the brain or produce sympathomimetic effects.Although the precise mechanism of action of modafinil is unknown, numerous human andanimal studies have elucidated many of its characteristics. Modafinil has site-specific centralnervous system activity (57,58) and acts on a specific subset of brain pathways that regulatesleep and wakefulness. However, it does not bind to many receptors that are normallyinvolved in sleep/wake regulation, including those for norephinephrine, serotonin, dopamineand γ-aminobutyric acid. It does not have the effects on the extrapyramidal motor system—restlessness, hyperactivity, and irritability—that conventional stimulants exhibit, suggestingthat modafinil has the potential to act as a cognitive enhancer without the side-effectsproduced by other stimulants.
This study of modafinil, the first to examine cognitive function in patients followingtreatment for cancer, has demonstrated that 200mg of modafinil enhances Speed of Memorymaking patients both more accurate and faster at retrieving information. Although modafinilhad no significant effect at week 4 on Continuity of Attention, those participants whocontinued modafinil showed an improvement at week 8. Significant improvement was alsoseen in the Quality of Episodic Secondary Memory, indicating that patients treated withmodafinil were better able to store, retain, and retrieve both verbal and pictorial information.Modafinil was thus able to improve cognitive performance (memory and attention) inchemotherapy-treated breast cancer survivors.
Most of the effects of modafinil on the composite score of memory and some measures inattention were shown in the first post-baseline visit (week 4) and were sustained throughoutthe study and are similar to those previously noted in clinical studies of modafinil in otherpopulations (59-62). The findings of this study demonstrate that the duration of an open-label drug is an important factor that needs to be addressed when considering apharmacological intervention for a symptom. By commencing all our patients on 200mgdaily of modafinil and then dividing them into two groups where one group continued themedication and the other started taking an identical placebo, we were able to compare fourweeks of modafinil treatment with eight weeks.
Quality of life, as well as survival and potential for cure, is of paramount importance tocancer patients. Post-treatment survivorship issues have become a prominent concern incancer survivors and patients living with cancer. Cancer therapy-related cognitive decline,along with fatigue, anxiety, and depression, is one of the most common symptoms affectingquality of life (63,64). During the past decade, studies have been performed to define thistreatment-related cognitive decline and to study its prevalence and importance.Unfortunately, the precise etiology remains obscure for most patients with this debilitatingside-effect. A better molecular understanding of this cognitive dysfunction will likely lead tothe identification of therapeutic targets and ultimately better treatment.
Kohli et al. Page 7
Cancer. Author manuscript; available in PMC 2010 June 15.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Although larger studies are needed to confirm these findings, the results of our secondaryanalysis of a trial of modafinil suggest that it can considerably improve some cognitivefunction measures in breast cancer survivors.
AcknowledgmentsThe authors are indebted to all the volunteers for participation and to Cephalon, Inc., for providing the study drug.The study was supported by a grant from Cephalon, Inc., and NCI Grants U10-CA37420 and R25-CA102618.
The study was supported by a grant from Cephalon, Inc and NCI Grants U10-CA37420 and R25-CA102618.
References1. Huria A, Somlo G, Ahles T. Renaming “Chemobrain”. Cancer Invest. Sep; 2007 25(6):373–7.
[PubMed: 17882646]2. Wieneke MH, Dienst ER. Neuropsychological assessment of cognitive functioning following
chemotherapy for breast cancer. Psychooncology. 1995; 4:61–66.3. Van Dam FS, Schagen SB, Muller MJ, et al. impairment of cognitive function in women receiving
adjuvant treatment for high-risk breast cancer: High-dose versus standard-dose chemotherapy. JNatl Cancer Inst. 1998; 90:210–218. [PubMed: 9462678]
4. Schagen SB, van Dam FS, Muller MJ, et al. Cognitive deficits after postoperative adjuvantchemotherapy for breast carcinoma. Cancer. 1999; 85:640–650. [PubMed: 10091737]
5. Brezden CB, Phillips KA, Abdolell M, et al. Cognitive function in breast cancer patients receivingadjuvant chemotherapy. J Clin Oncol. 2000; 18:2695–2701. [PubMed: 10894868]
6. Kreukals BP, Van Dam FS, Ridderinkhof KR, Boogerd W, Schagen SB. Persistent NeurocognitiveProblems after Adjuvant Chemotherapy for Breast Cancer. CLIN Breast Cancer. Feb; 2008 8(1):80–7. [PubMed: 18501062]
7. Ferguson RJ, Ahles TA. Low Neuropsychologic Performance Among Adult Cancer SurvivorsTreated With Chemotherapy. Curr Neuro and Neurosc Rep. 2003; 3:215–222.
8. Castellon SA, Ganz PA, Bower JE, et al. Neurocognitive performance in breast cancer survivorsexposed to adjuvant chemotherapy and tamoxifen. J Clin Exp Neuropsychol. 2004; 26:955–969.[PubMed: 15742545]
9. Mehnert A, Scherwath A, Schirmer L, Schleimer B, Petersen C, Schultz-Kindermann F, Zander AR,Koch U. The association between neuropsychological impairment, self-perceived cognitive deficits,fatigue and health related quality of life in breast cancer survivors following standard adjuvantversus high-dose chemotherapy. Patient Education and Counseling. April; 2007 66(Issue 1):108–118. [PubMed: 17320337]
10. Bower JE. Behavioral symptoms in patients with breast cancer and survivors. J Clin Oncol. Feb 10;2008 26(5):768–77. [PubMed: 18258985]
11. Janz NK, Mujahid M, Chung LK, Lantz PM, Hawley ST, Morrow M, Schwartz K, Katz SJ.Symptom experience and quality of life of women following breast cancer treatment. J WomensHealth (Larchmt). Nov; 2007 16(9):1348–61. [PubMed: 18001192]
12. Miller AH, Ancoli-Israel S, Bower JE, Capuron L, Irwin MR. Neuroendocrine-immunemechanisms of behavioral comorbidities in patients with cancer. J Clin Oncol. Feb 20; 2008 26(6):971–82. [PubMed: 18281672]
13. Mar Fan HG, Clemons M, Xu W, Chemerynsky I, Breunis H, Braganza S, Tannock IF. Arandomised, placebo-controlled, double-blind trial of the effects of d-methylphenidate on fatigueand cognitive dysfunction in women undergoing adjuvant chemotherapy for breast cancer. SupportCare Cancer. Jun; 2008 16(6):577–83. [PubMed: 17972110]
14. Nelson CJ, Nandy N, Roth AJ. Chemotherapy and cognitive deficits: mechanisms, findings, andpotential interventions. Palliat Support Care. Sep; 2007 5(3):273–80. Review. [PubMed:17969831]
15. US Modafinil in Narcolepsy Multicenter Study Group. Randomized trial of modafinil for thetreatment of pathological somnolence of narcolepsy. Ann Neurol. 1998; 43:88–97. [PubMed:9450772]
Kohli et al. Page 8
Cancer. Author manuscript; available in PMC 2010 June 15.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

16. US Modafinil in Narcolepsy Multicenter Study Group. Randomized trial of modafinil for thetreatment of pathological somnolence of narcolepsy. Neurology. 2000; 54:1166–75. [PubMed:10720292]
17. Broughton RJ, Fleming JA, George CF, et al. Randomized, double-blind, placebo-controlledcrossover trial of modafinil in the treatment of excessive daytime sleepiness in narcolepsy.Neurology. 1997; 49:444–51. [PubMed: 9270575]
18. Moldofsky H, Broughton RJ, Hill JD. A randomized trial of the long-term, continued efficacy andsafety of modafinil in narcolepsy. Sleep Med. 2000; 1:231–43. [PubMed: 10828434]
19. Czeisler CA, Walsh JK, Roth T, Hughes RJ, Wright KP, Kingsbury L, Arora S, Schwartz JR,Niebler GE, Dinges DF. U.S. Modafinil for Excessive Sleepiness Associated with Shift-WorkSleep Disorder. N Engl J Med. 2005; 353:476–86. [PubMed: 16079371]
20. Jasinski DR. An evaluation of the abuse potential of modafinil using methylphenidate as areference. J Psychopharmacol. 2000; 14:53–60. [PubMed: 10757254]
21. Gagnon B, Low G, Schreier G. Methylphenidate hydrochloride improves cognitive function inpatients with advanced cancer and hypoactive delirium: a prospective clinical study. Rev PsychiatrNeurosci. 2005; 30(2):100–107.
22. Morrow GR, Ryan JL, Kohli S, Jean-Pierre P, Carroll J, Figueroa- Moseley C, Mustian KM,Hoffman M. Supportive Care in Cancer. 2006:583–687. Abstract 11-070. [PubMed: 17106659]
23. Yoshitake H. Three characteristic patterns of subjective fatigue symptoms. Ergonomics. 1978;21:231–233. [PubMed: 27351]
24. Mc Nair, DM.; Lorr, M.; Droppelman, LF. Manual for the Profile of Mood States. Educational andIndustrial Testing Service; San Diego: 1971.
25. Mendoza TR, Wang XS, Cleeland CS, Morrissey M, Johnson BA, Wendt JK, Huber SL. The rapidassessment of fatigue severity in cancer patients: Use of the Brief Fatigue Inventory. Cancer. 1999;85:1186–1196. [PubMed: 10091805]
26. Krupp LB, LaRocca NG, Muir-Nash J, Steinberg AD. The Fatigue Severity Scale. Application topatients with multiple sclerosis and systemic lupus erythematosus. Arch. Neurol. 1989; 46:1121–1123. [PubMed: 2803071]
27. Cleeland CS, Mendoza TR, Wang XS, Chou C, Harle MT, Morrissey M, et al. Assessing symptomdistress in cancer patients: the M.D. Anderson Symptom Inventory. Cancer. 2000; 89:1634–46.[PubMed: 11013380]
28. Booth-Jones M, Jacobsen PB, Ransom S, Soety E. Characteristics and correlates of cognitivefunctioning following bone marrow transplantation. Bone Marrow Transplant. 2005; 36:695–702.[PubMed: 16086044]
29. Baranski JV, Pigeau RA. Self-monitoring cognitive performance during sleep deprivation: effectsof modafinil, d-amphetamine and placebo. J Sleep Res. 1997; 6:84–91. [PubMed: 9377538]
30. Caldwell JA, Caldwell JL, Smythe NK, Hall KK. A double-blind, placebo-controlled investigationof the efficacy of modafinil for sustaining the alertness and performance of aviators: a helicoptersimulator study. Psychopharmacology. 2000; 150:272–282. [PubMed: 10923755]
31. Wesensten NJ, Belenky G, Kautz MA, Thorne DR, Reichardt RM, Balkin TJ. Maintainingalertness and performance during sleep deprivation: modafinil vs caffeine. Psychopharmacology.2002; 159:238–247. [PubMed: 11862356]
32. Winningham, ML.; Groenwald, SL.; Goodman, M.; Frogge, MH.; Yarbo, CH., editors. CancerSymptom Management. Jones and Barlett; Boston: 1996. p. 42-54.
33. Simpson P, Wesnes K, Christmas L. A computerized system for the assessment of drug-inducedperformance changes in young, elderly or demented populations. Br J Clin Pharmacol. 1987;27:711P–712P.
34. Wesnes KA, Ward T, Mcgintya, Petrini O. The memory enhancing effects of a gingko/biloba/Panax ginseng combination in healthy middle-aged volunteers. Psychopharmacology (Berl). 2000;152:353–61. [PubMed: 11140327]
35. Wesnes KA, Simmons D, Rook M, Simpson P. A double-blind placebo controlled trial of tanakanin the treatment of idiopathic cognitive impairment in the elderly. Hum Psychopharmacol. 1987;2:159–69.
Kohli et al. Page 9
Cancer. Author manuscript; available in PMC 2010 June 15.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

36. Wesnes KA, McKeith IG, Ferrara R, et al. Effects of rivastigmine on cognitive function indementia with Lewy bodies: a randomized placebo-controlled international study using thecognitive drug research computerized assessmebt system. Dement Geriatr Cogn Disord. 2002;13:183–92. [PubMed: 11893841]
37. http://www.cognitivedrugresearch.com/newcdr/38. O'Neill WM, Hanks GW, Simpson P, Fallon MT, Jenkins E, Wesnes KA. The cognitive and
psychomotor effects of morphine in healthy subjects: A randomised controlled trial of repeated(four) oral doses of dextropropoxyphene, morphine, lorazepam and placebo. Pain. 2000; 85:209–215. [PubMed: 10692620]
39. Walker MP, Ayre GA, Cumming JL, Wesnes K, McKeith IG, O'Brien JT, Ballard CG. Quantifyingfluctuation in Dementia with Lewy Bodies, Alzheimer's disease and vascular dementia.Neurology. 2000; 54:1616–1625. [PubMed: 10762503]
40. Parrott AC, Lees A, Garnham NJ, Jones M, Wesnes KA. Cognitive performance in recreationalusers of MDMA or `ecstasy': evidence for memory deficits. Journal of Psychopharmacology.1998; 12:79–83. [PubMed: 9584971]
41. Walker LG, Wesne KA, Heys SD, Walker MB, Lolley J, Eremin O. The cognitive effects ofrecombinant Interleukin-2 (rIL-2) therapy: a controlled clinical trial using computerisedassessments. European Journal of Cancer. 1996; 32A(13):2275–2283. [PubMed: 9038610]
42. Keith MS, Stanislav SW, Wesnes KA. Validity of a cognitive computerized assessment system inbrain-injured patients. Brain Injury. 1998; 12(12):1037–1043. [PubMed: 9876863]
43. Walker MP, Ayre GA, Cummings JL, Wesnes K, McKeith IG, O'Brien JT, Ballard CG. TheClinician Assessment of Fluctuation and the One Day Fluctuation Assessment Scale. The BritishJournal of Psychiatry. 2000; 177:252–256. [PubMed: 11040887]
44. Wesnes KA, McKeith I, Edgar C, Emre M, Lane R. Benefits of rivastigmine on attention indementia associated with Parkinson's disease. Neurology. 2005; 65:1654–6. [PubMed: 16301500]
45. Kennedy DO, Scholey AB, Wesnes KA. Modulation of cognition and mood followingadministration of single doses of Ginkgo biloba, ginseng and a ginkgo/ginseng combination tohealthy young adults. Physiology & Behaviour. 2002; 75:1–13.
46. Kennedy DO, Scholey AB, Wesnes KA. Dose Dependent Changes in Cognitive Performance andMood following Acute Administration of Ginseng to Healthy Young Volunteers. NutritionalNeuroscience. 2001; 4:295–310. [PubMed: 11842896]
47. Kennedy DO, Scholey AB, Wesnes KA. Differential, Dose Dependent Changes in CognitivePerformance Following Acute Administration of a Ginkgo biloba/Panax ginseng Combination toHealthy Young Volunteers. Nutritional Neuroscience. 2001; 4:399–412. [PubMed: 11842916]
48. Wesnes K, Faleni RA, Hefting NR, Hoogsteen G, Houben JJG, Jenkins E, Jonkman JHJ, LeonardJ, Petrini O, van Lier JJ. The cognitive, subjective and physical effects of a Ginkgo biloba/PanaxGinseng combination in healthy volunteers with neurasthenic complaints. PsychopharmacologyBulletin. 1997; 33(4):677–683. [PubMed: 9493479]
49. Wesnes KA, Ward T, McGinty A, Petrini O. The memory enhancing effects of a Ginkgo biloba/Panax ginseng combination in healthy middle aged volunteers. Psychopharmacology. 2000;152:353–361. [PubMed: 11140327]
50. Kennedy DO, Scholey AB, Wesnes KA. The dose-dependent cognitive effects of acuteadministration of ginkgo biloba to healthy young volunteers. Psychopharmacology. 2000;151:416–423. [PubMed: 11026748]
51. McKeith I, Del Ser T, Spano P, Emre M, Wesnes K, Anand R, Cicin-Sain A, Ferrara R, Spiegel R.Efficacy of rivastigmine in dementia with Lewy bodies: a randomised, double-blind, placebo-controlled international study. The Lancet. December.2000 3562000:2031–2036.
52. Wesnes KA, McKeith IG, Ferrara R, Emre M, Del Ser T, Spano PF, Cicin-Sain A, Anand R,Spiegel R. Effects of rivastigmine on cognitive function in dementia with Lewy bodies: arandomised placebo-controlled international study using the Cognitive Drug ResearchComputerised Assessment System. Dementia. 2001; 13(3):183–92.
53. Wesnes KA, Simpson PM, White L, Pinker S, Jertz, Murphy M, Siegfried K. Cholinesteraseinhibition in the scopolamine model of dementia. Annals of the New York Academy of Sciences.1991; 640:268–27. [PubMed: 1776749]
Kohli et al. Page 10
Cancer. Author manuscript; available in PMC 2010 June 15.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

54. Kohli S, Griggs JJ, Roscoe JA, Jean-Pierre P, Bole C, Mustian KM, Zangmeister J, Smith K, GrossH, Morrow GR. Self-Reported Cognitive Impairment in Cancer Patients. Journal of OncologyPractice. March.2007
55. Hurria A, Rosen C, Hudis C, et al. Cognitive function of older patients receiving adjuvantchemotherapy for breast cancer: a pilot prospective longitudinal study. J Am Geriatr Soc. 2006;54:925–931. [PubMed: 16776787]
56. http://health.howstuffworks.com/sleep-is-so-last-year.htm57. Lin JS, Hou Y, Jouvet M. Potential brain neuronal targets for amphetamine, methylphenidate and
modafinil-induced wakefulness, evidenced by c-mos immunocytochemistry, in the cat. Proc Natlacad Sci USA. 1996; 92:14128–33. [PubMed: 8943072]
58. Engber TM. Differential patterns of regional c-Fos induction in the rat brain by amphetamine andthe novel wakefulness-promoting agent modafinil. Neurosci lett. 1998; 24:95–8. [PubMed:9507929]
59. US Modafinil in Narcolepsy Multicenter Study Group. Randomized trial of modafinil as atreatment of pathological somnolence in narcolepsy. Ann Neurol. 198; 43:88–97.
60. US modafinil in Narcolepsy Multicenter Study Group. Randomized trial of modafinil as atreatment for the excessive daytime somnolence of narcolepsy. Neurology. 2000; 54:1166–75.[PubMed: 10720292]
61. Broughton RJ, Fleming JA, george CF, et al. Randomized, double-blind, placebo-controlledcrossover trial of modafinil in the treatment of excessive daytime sleepiness in narcolepsy.Neurology. 1997; 49:444–51. [PubMed: 9270575]
62. Mitler MM, Harsh J, Hirshkowitz M, Guilleminault C. Long-term efficacy and safety of modafinil(PROVIGIL®) for the treatment of excessive daytime sleepiness associated with narcolepsy. SleepMed. 2000; 1:231–43. [PubMed: 10828434]
63. Luoma ML, Hakamies-Blomqvist L. The meaning of quality of life in patients being treated foradvanced breast cancer: a qualitative study. Psychooncology. Oct; 2004 13(10):729–39. [PubMed:15386642]
64. Rugo HS, Ahles T. The impact of adjuvant therapy for breast cancer on cognitive function: currentevidence and directions for research. Semin Oncol. Dec; 2003 30(6):749–62. Review. [PubMed:14663776]
Kohli et al. Page 11
Cancer. Author manuscript; available in PMC 2010 June 15.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 1.Fatigue levels in post-treatment breast cancer patients receiving open-label modafinil (22).
Kohli et al. Page 12
Cancer. Author manuscript; available in PMC 2010 June 15.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 2.Patients who completed study at each time-point.
Kohli et al. Page 13
Cancer. Author manuscript; available in PMC 2010 June 15.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 3.Mean change from baseline for Quality of Episodic Memory and Speed of Memory DuringOpen-Label (N=76)
Kohli et al. Page 14
Cancer. Author manuscript; available in PMC 2010 June 15.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
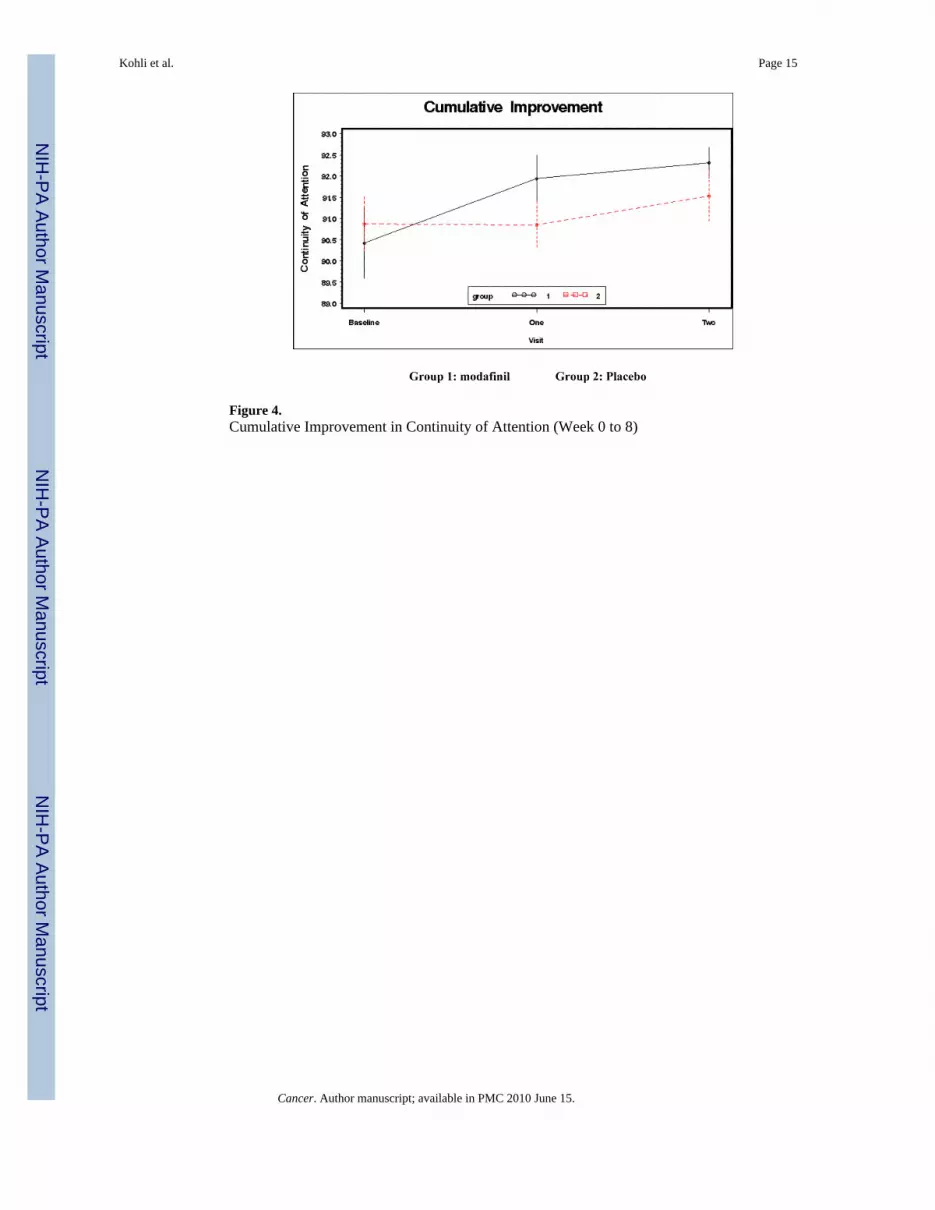
Figure 4.Cumulative Improvement in Continuity of Attention (Week 0 to 8)
Kohli et al. Page 15
Cancer. Author manuscript; available in PMC 2010 June 15.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Kohli et al. Page 16
Table 1
Measures Contributing to the Analyses of the Cognitive Drug Research (CDR) Computerized AssessmentSystem
Factor score and mean normative data for women aged 33-83 years Measures that contribute to the score
Quality of Episodic Secondary Memory (lower score is better) Mean: 199.3 Immediate word recall—word correctly recalled
Immediate word recall—intrusions
Immediate word recall—errors
Delayed word recall—word correctly recalled
Delayed word recall—intrusions
Delayed word recall—errors
Word recognition new stimuli—accuracy
Word recognition original stimuli—accuracy
Picture recognition new stimuli—accuracy
Picture recognition original stimuli—accuracy
Quality of Working Memory (lower score is better) Mean: 1.557 Numeric working memory
Speed of Memory (lower score is better) Mean: 3089 Speed of numeric working memory
Speed of word recognition
Speed of spatial working memory
Speed of picture recognition
Power of Attention (higher score is better) Mean: 1201 Simple reaction time
Choice reaction time
Digit vigilance—speed
Continuity of Attention (higher score is better) Mean: 89.71 Choice reaction time—accuracy
Digit vigilance—targets detected
Digit vigilance—false alarms
Cancer. Author manuscript; available in PMC 2010 June 15.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Kohli et al. Page 17
Table 2
Patient Demographic and Clinical Characteristics
Open-label (Week 0-4) N = 76 Modafinil (Week 4-8) N = 34 Placebo (Week 4-8) N = 34
Months since completed treatment:
Mean (SD) 22.8 (21.1) 22.1 (22.7) 22.1 (22.7)
Range 1-96 1-96 1-96
Age:
Mean (SD) 54.0 (10.3) 51.76 (8.6) 56.35 (11.4)
Range 33-83 33-70 36-83
Sex:
Female 76 (100%) 34 (100%) 34 (100%)
Ethnicity:
White 74 (97.4%) 34 (100%) 33 (97%)
Hispanic 1 (1.3%) 0 (0%) 0 (0%)
Black 1 (1.3%) 0 (0%) 1 (3%)
Education:
Completed Graduate Training 30 (39.5%) 14 (41%) 12 (35%)
Standard College or University (4 years) 20 (26.3%) 6 (17%) 12 (35%)
Partial College Training (<4 years) 7 (9.2%) 7 (21%) 0 (0%)
High School Graduate 19 (25%) 7 (21%) 10 (30%)
Marital Status:
Married 51 (67.1%) 23 (67%) 23 (67%)
Divorced 6 (7.9%) 1 (3%) 4 (12%)
Separated 1 (1.3%) 0 (0%) 1 (3%)
Single 11 (14.5%) 8 (24%) 2 (6%)
Widowed 7 (9.2%) 2 (6%) 4 (12%)
Previous surgery 76 (100%) 34 (100%) 34 (100%)
Previous chemotherapy 76 (100%) 34 (100%) 34 (100%)
Previous RT 65 (85.5%) 28 (82%) 29 (85%)
Other 43 (56.6%) 18 (53%) 21 (62%)
Cancer. Author manuscript; available in PMC 2010 June 15.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Kohli et al. Page 18
Table 3
Summary of composite scores* from CDR assessments across treatment groups during open label andrandomization.
Open Label (N=76) (week 0-4) Modafinil (N=34) (week 4-8) Placebo (N=34) (week 4-8)
Speed of Memory a
Week 0 4543.22 (1165.4)1,2,3 - -
Week 4 - 4439.69 (1071.92)1 4314.74 (1020.17)
Week 8 - 4232.10 (1031.1)2,4 4335.56 (915.82)3,4
Continuity of Attention b
Week 0 90.97 (3.79)5,6 - -
Week 4 - 92.00 (3.12) 90.94 (3.12)
Week 8 - 92.24 (2.09)5 91.59 (3.26)6
Quality of Episodic Memory a
Week 0 211.49 (49.65)7,8 - -
Week 4 - 237.37 (40.53)7,9 232.20 (52.99)
Week 8 - 219.65 (52.50)8,9,10 224.17 (54.02)10
Quality of Working Memory a
Week 0 1.82 (0.25) - -
Week 4 - 1.79 (0.38) 1.80 (0.43)
Week 8 - 1.82 (0.20) 1.70 (0.49)
Power of Attention b
Week 0 1275.08 (208.8) - -
Week 4 - 1228.24 (126.80) 1276.33 (153.89)
Week 8 - 1247.80 (139.04) 1275.44 (121.31)
Identical superscript numbers indicate a statistically significant difference between groups (p <= 0.05).
*mean and (standard deviation)
alower score better
bhigher score better
Cancer. Author manuscript; available in PMC 2010 June 15.





























