Embed Size (px)
Citation preview
The efficacy of soy isoflavones on menopausal vasomotor
symptoms: A review
Lindsay Gullen
University of British Columbia
333 University Way
Kelowna, BC
V1V 1V7
April 1, 2014
Abstract
Due to the risks associated with steroidal hormone
replacement therapy, many menopausal women are seeking
natural alternatives to treat vasomotor symptoms (VMS).
Research focusing on the effectiveness of phytohormones has
had mixed results, although soy-derived isoflavones have
provided promising treatment. This review investigates the
biochemistry and mode of action of soy isoflavones,
evaluates current research on the efficacy of soy
isoflavones on VMS, and makes recommendations for future
work in the field.
Keywords
hormone replacement alternatives, isoflavones, menopause,
phytoestrogen efficacy, soy, vasomotor symptoms
2
Abbreviations
FDA, Food and Drug Administration; HRT, hormone replacement
therapy; SERM, selective estrogen receptor modulators; SHBG,
Sex Hormone Binding Globlin; SPARE, Soy Phytoestrogens As
Replacement Estrogen; VMS, vasomotor symptoms
Graphical abstract
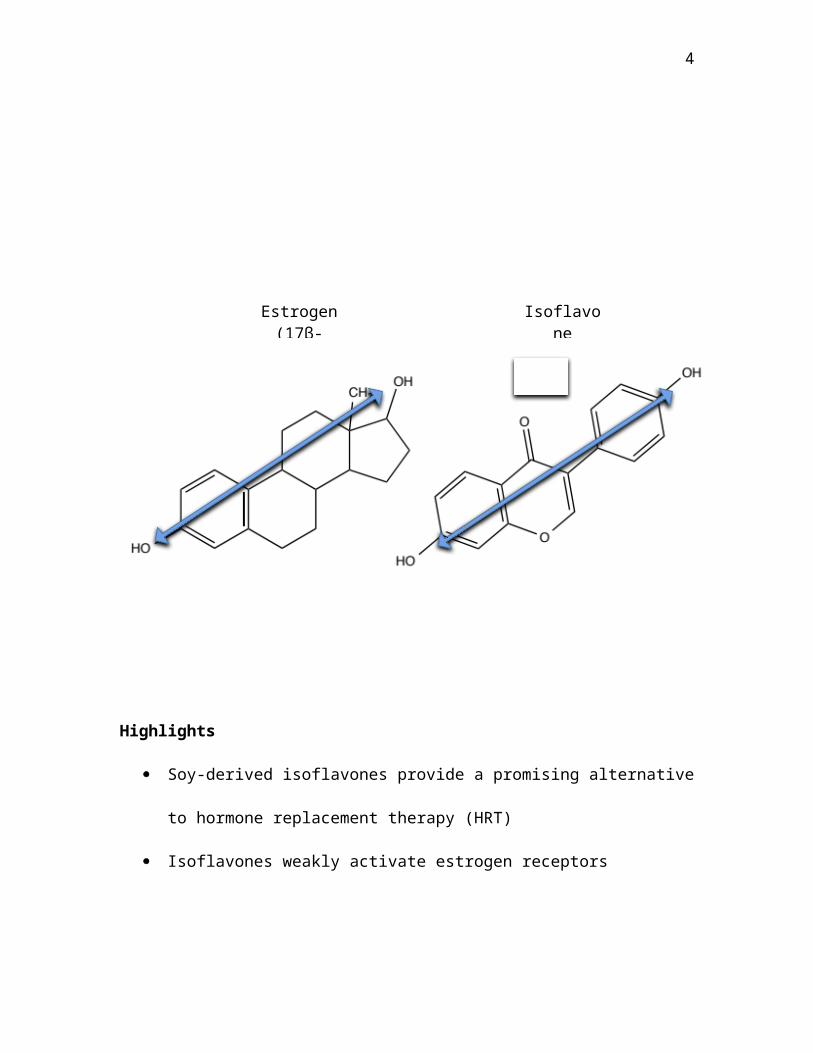
Soy-derived isoflavones contain two hydroxyl groups in
approximately the same positions as estradiol. Consequently,
isoflavones exhibit weakened but similar properties as
estradiol, such as decrease in menopausal vasomotor
symptoms.
3
Highlights
Soy-derived isoflavones provide a promising alternative
to hormone replacement therapy (HRT)
Isoflavones weakly activate estrogen receptors
Isoflavone
Estrogen(17β-
4
Clinical trials have shown mixed results in decreasing
vasomotor symptoms in menopausal women through use of
soy isoflavones
Future research must be conducted to improve
consistency amongst results, and to approve product by
FDA
1.0 Introduction
Menopause, or the “change of life”, is experienced by
women between the ages of 46 to 50 and involves the
termination of menstruation. The ovaries gradually lose
their capability of responding to the hormones responsible
for stimulation of ripening egg cells, and no longer produce
the sex hormone estrogen. The deficit in estrogen may lead
to a number of physiological changes, including vasomotor
symptoms (VMS) (Rathus et al., 2012).
VMS include a sudden onset of feeling hot (hot
flashes), looking reddened (hot flushes), and night sweats.
These subjective experiences occur due to the vasodilation
of blood vessels in the face and upper body. It is suggested
5
that deficiency in estrogen disturbs the hypothalamus and
offsets a number of hormonal pathways responsible for
temperature regulation (Rathus et al., 2012).
VMS are experienced globally by 22% to 74% of
menopausal women (Villaseca, 2012). Although these symptoms
are not a severe threat to health, they can negatively
impact a woman’s quality of life (Bedell et al., 2014). Some
women partake in steroidal hormone replacement therapy (HRT)
to help alleviate menopausal symptoms. Although HRT has been
clinically shown to be the most effective treatment for VMS,
only 10% to 15% of menopausal women in Western countries
currently use it (Brzezinksi and Debi, 1999). Women became
reluctant to use HRT after a 2002 study conducted by the
Women’s Health Initiative terminated an 8-year study early
due to an increase in breast cancer incidence amongst women
treated with HRT. Consequently, the Canadian Cancer Society
strongly discourages use of HRT unless menopausal symptoms
are severe and women are unable to use alternative
treatments (Rathus et al., 2012).
6
One area of growing research involves the use of
phytoestrogens as a non-steroidal substitute. Soybeans are
rich in isoflavones, which behave similarly to estradiol by
displaying weakened estrogenic effects (Albertazzi et al.,
1998; Bedell et al., 2014; Carmignani et al., 2010). The
objectives of this review are: (1) to investigate the
biochemistry and mode of action of soy isoflavones, (2) to
evaluate current research on the efficacy of soy isoflavones
on VMS and (3) to make recommendations for future work in
the field.
1.1 Biochemistry
Phytoestrogens, which are of plant origin, are non-
steroidal classes of compounds. When humans consume certain
plants, phytoestrogens can also be derived by the in vivo
metabolism of precursors (Brzezinksi and Debi, 1999).
Soybeans contain genistin, daidzin, and glycitin, which
belong to the phytoestrogen class of isoflavones. These
compounds consist of a heterocyclic structure and two
hydroxyl groups in approximately the same positions as
7
estradiol. Consequently, isoflavones are capable of binding
and activating estrogen receptors (Fig 1) (Alamo et al.,
2010).
Upon ingestion of soy products, bacteria in the gut
convert genistin, daidzin, and glycitin into active,
aglycone forms (genistein, daidzein, and glycitein). Gut
flora activate isoflavones from their glycone to aglycone
structures by removal of the sugar molecule via beta-
glucosidase (Alamo et al., 2010; Vincent and Fitzpatrick,
2000). Daidzein undergoes further modification by intestinal
flora producing equol, which is ten times more potent than
its precursor (Bedell et al., 2014).
Absorbed isoflavones can vary between individuals. Only
30%-50% of the human population is capable of producing
equol (Uehara et al., 2008). Moreover, diet, illness and
antibiotic use can cause intestinal flora populations to
fluctuate, thus impacting equol production (Bedell et al.,
2014). For example, Setchell and Cassidy (1999) found that
higher levels of equol were found in those with a diet high
in carbohydrates. Variations in gut flora may potentially
8
pose a problem in the administered dose, enabling relevant
research investigation.
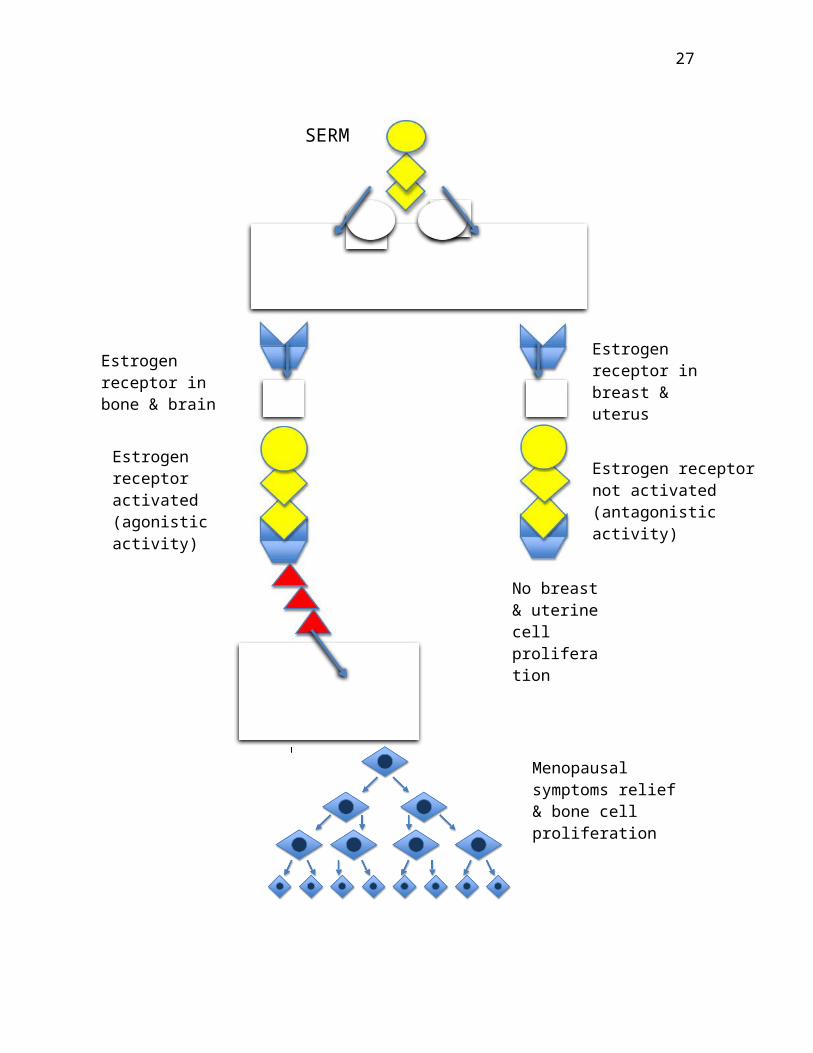
1.2 Mode of Action
All estrogens (including steroidal) are classified as
Selective Estrogen Receptor Modulators (SERMs) (Bedell et
al., 2014). Their effects are dependent on target tissues
and the concentration of circulating estrogen levels
(Carmignani et al., 2010). With high circulating
concentrations, isoflavones act as estrogen antagonists. In
menopausal women, where circulating estrogen is low,
isoflavones act as estrogen agonists (Vincent and
Fitzpatrick, 2000). For example, the soy-derived drug
Femarelle has agonistic activity in the brain and bone, thus
alleviating menopausal symptoms and increasing bone density.
However, the makers of Femarelle report antagonistic,
antiproliferative effects on breast and endometrial tissue
(Fig 2) (Yoles et al., 2004).
Although less potent than estradiol, isoflavones bind
to both alpha and beta estrogen receptors, with greater
9
affinity for the latter. Beta estrogen receptor stimulation
is responsible for antiproliferation in reproductive
tissues, whereas alpha estrogen receptor stimulation induces
breast and uterine growth and development (Villaseca, 2012).
Further complicating matters, isoflavones also have the
ability to bind to androgen
receptors, suppressing androgen receptor expression
(Hamilton-Reeves et al., 2007). Isoflavones also prompt the
synthesis of Sex Hormone Binding Globulin (SHBG), which
moderates circulating sex hormones (Villaseca, 2012). In
vitro studies have also shown inhibition of aromatase, an
enzyme involved in estrogen biosynthesis (Brzezinski and
Debi, 1999). It is critical to take these multiple stimuli
into consideration especially in the context of breast and
endometrial cancer.
2.0 Effects of soy-derived isoflavones on VMS
The research pertaining to the effects of soy-derived
isoflavones on VMS has been inconsistent (Table 1). Through
a randomized, double-blinded study, Murkies et al. (1995)
10
investigated the effects of a soy-rich diet in 58 women
between the ages of 30 to 70. Before the clinical trial,
women reported having experienced a frequency of 14 or more
hot flashes/week. In the first 2 weeks, the women recorded
the number of VMS experienced and their daily diet. Twenty-
eight women added 45g of soy flour to their daily diet for
12 weeks. The results were most prominent in weeks 6 to 12.
In comparison to those in the wheat-flour control group,
women who supplemented their diet with soy flour reported a
40% decrease in VMS frequency.
Albertazzi et al. (1998) had a larger sample of 104
postmenopausal women. Also in a double-blinded, randomized
study, 51 subjects aged 48 to 61 consumed 60g of soy protein
isolate on a daily basis (76mg isoflavones). In the control
group, 53 patients in an age range of 45 to 62 years were
assigned a 60g daily dose of casein placebo. After a 12-week
trial, the average number of VMS per 24 hours significantly
decreased in comparison to the control group, although the
difference was not very large. Mean VMS
11
decreased by 26% by week 3, 33% in week 4, and 45% by the
end of the experiment. In the casein group, VMS decreased
only by 30% after 12 weeks. These results compare poorly
with an 83% VMS reduction with steroidal hormone replacement
therapy. Unfortunately, 25 patients were unable to complete
the study (11 in soy group; 14 in placebo group) due to
gastrointestinal side effects such as bloating and
constipation, significantly reducing the data set by more
than 20%.
In a more recent study by Carmignani et al. (2010), soy
supplementation was found to have equal effects as low-dose
steroidal hormone therapy. Sixty women ranging from 40 to 60
years of age were randomly assigned a soy supplement
containing 90mg of isoflavones (n=20), 1 mg estradiol
(n=20), or a placebo (n=20). After 16 weeks, users of the
hormone therapy experienced a 45.6% decrease in VMS
frequency. Subjects using the soy supplement reported a
similar 49.8% decrease in VMS occurrence. Results differed
from the placebo group, which experienced a 28% decrease in
VMS.
12
Conversely, Brzezinski et al. (1997) did not report
any improvement in VMS between the placebo and
phytoestrogen-treatment group. One hundred forty five women
ranging from 43 to 65 years were randomly assigned to either
a treatment (n=78) or placebo (n=67). Women in the treatment
group consumed 25% of their caloric intake in phytoestrogen-
rich foods consisting of tofu, miso and soy beverage. After
12 weeks, SHBG serum levels significantly increased in women
in the treatment group (28%), and remained at baseline in
the placebo (7%). Moreover, subject phytoestrogen serum
levels (daidzein, equol, genistein) were significantly
increased in the phytoestrogen-rich diet (1086%, 1107%,
2089%), whereas women in the control group experienced no
change. VMS decreased in both the placebo (48%) and
phytoestrogen-treatment groups (50%). Although the treatment
group experienced slightly less VMS than the placebo, the
different was statistically insignificant.
The Soy Phytoestrogens As Replacement Estrogen (SPARE)
study in 2004 was funded by the National Institute of
Health. The study aimed to overcome past obstacles by
13
incorporating a larger sample size, longer clinical trial
and improved experimental design. Two hundred forty eight
women ages 45 to 60 who have progressed into menopause
within 5 years of enrollment were randomized into two
groups. Participants were assigned either daily 200mg soy
isoflavone (n=122) or a placebo (n=126) for 2 years. No
significant difference was found between the treatment and
control group after 2 years. Forty-eight percent of the
women in the soy isoflavone, and 32% in the placebo group
still reported having VMS (Chalupka, 2011; Levis et al.,
2010).
A study conducted by Quella et al. (2000) investigated
the effects of soy phytoestrogens on VMS in the survivors of
breast cancer. In a double-blinded, randomized trial,
patients with VMS were assigned to either a soy group (n=87)
or a placebo group (n=88). It should be noted that 68% of
patients were on the breast tissue antagonist drug,
tamoxifen, which may have influenced results. The groups
were instructed to take a tablet three times daily. The soy
group’s tablet was comprised of 50mg isoflavone (40%-45%
14
genistein, 40%-45% daidzein, and 10%-20% glycitein) totaling
to 150mg/day. After 4 weeks, the soy group was prescribed
the placebo and the placebo group was assigned the soy
tablet. In total, the experiment lasted 8 weeks. Out of all
the subjects, only 149 produced usable data by completing
the study. Results indicated no beneficial effects on VMS
with isoflavone supplementation.
A 2011 meta-analysis showed that 30 studies from 1999-
2011 displayed mixed results. According to Villaseca (2012),
most trials were of short duration and poor quality. Three
placebo-controlled studies indicated a significant decrease
in VMS frequency (61%, 74%, 50% reduction in the soy-
treatment compared to 21%, 43%, 38% reduction in the
placebo, respectively). Moreover, Villaseca (2012) reported
that more recent studies show greater VMS improvement
compared to older studies. A study where women took a high
dose of soy isoflavones (100mg/day) showed significant
improvement in VMS compared to placebo; however, a study
where women only took 40mg experienced VMS equivalent to
placebo. In defiance of relatively short experimental
15
durations, most studies have found that VMS alleviation is
most prominent within the first 12 weeks of treatment.
2.1 Critique of studies
In spite of conflicting results, there is evidence that
menopausal women may benefit from soy-derived isoflavones to
alleviate VMS. Inconsistent results may be attributed to:
participant dropout, failure to evaluate menopausal
progression, inconsistent administered dose, and variable
participant metabolism/adsorption of isoflavones.
2.1.0 Dropout rates
Many clinical trials faced challenges with high dropout
rates: 11 out of 58 participants in the Murkies et al.
(2008) study, 25 out of 104 in the Albertazzi et al. (1998)
study, 31 out of 145 in the Brzezinski et al. (1997) study,
and 26 out of 175 patients in the Quella et al. (2000) study
withdrew, often due to gastrointestinal side effects or lack
of participant compliance.
16
2.1.1 Evaluation of menopausal progression
VMS frequency and intensity typically predominate
during the first 2 years of menopause; consequently, VMS
improvement can be expected over time without medical
intervention (Bedell et al., 2014). Many studies, including
SPARE (Chalupka, 2011; Levis et al., 2010), failed to take
this phenomenon into account by involving postmenopausal
women who have progressed into menopause for up for 5 years.
The remaining studies failed to evaluate the duration
between menopausal onset and experimentation. The cancer-
survivor study conducted by Quella et al. (2000) involved
participants from 19-50+ years of age, thus a mix of
patients who have and have not yet reached menopause. Quella
et al. (2000) also failed to distinguish menopausal VMS from
symptoms attributed to chemotherapy side effects (Table 1).
2.1.2 Inconsistent administered dose
Administered dose has been inconsistent throughout
studies, ranging from 76mg/day to 200mg/day. Other studies
failed to investigate isoflavone concentrations, for
17
example, in the cases of Murkies et al. (1995) and
Brzezinski et al. (1997). Interestingly, the larger
isoflavone doses of 200mg/day (Levis et al., 2004) and 150
mg/day (Quella et al., 2000) failed to significantly differ
from the control groups. Perhaps partial antagonistic
effects of the SERM isoflavones are responsible for this
finding; however, more research regarding optimal dose must
be conducted.
2.1.3 Participant metabolism and absorption
Variable outcomes may have also been attributed to each
participant’s metabolism and absorption. As aforementioned,
the bioavailability of isoflavones is dependent on gut
flora. The extent of this biotransformation differs between
individuals and can vary as a result of diet, illness and
antibiotic use (Bedell et al., 2014; Setchell and Cassidy,
1999). Some studies considered the effects of antibiotics on
gut flora and excluded these candidates (Murkies et al.,
1995; Levis et al., 2010). Only Brzezinski et al. (1997)
implemented a strict macronutrient composition consisting of
50-55% carbohydrates. Ironically, Murkies et al. (1995) used
18
a wheat flour control group, which may have had equol-
synthesizing effects on gut flora.
2.2 Future work
Given that serious adverse side effects have seldom
been reported, isoflavones are a highly optimistic
alternative to HRT; however, it does not preclude from the
need to further our understanding. A comprehensive
literature search on the SERM properties of soy isoflavones
would provide a better knowledge of potential risks and
benefits in regards to breast cancer, bone health,
endometrial hyperplasia, and other menopausal symptoms. To
become approved by the FDA, more research pertaining to the
safety of soy isoflavones must be conducted.
Improved experimental design would ameliorate the
quality of the data, which may produce more consistent
results. By excluding participants who have progressed
through menopause for more than 2 years, researchers can
control for the suspected decline in VMS incidence. Optimal
isoflavone dose must also undergo further investigation to
19
balance antagonist/agonist effects. A tablet containing
isolated isoflavones may reduce the gastrointestinal
discomfort frequently reported with soy foods, which may
reduce participant dropout. Moreover, a diet with strict
macronutrient restrictions may be necessary to control for
increased biotransformation upon ingestion of carbohydrates.
Exclusion of individuals with recent illness and/or
antibiotic use may also improve results by considering the
roles of gut flora.
3.0 Concluding remarks
Soy isoflavones are an optimistic alternative to HRT
for menopausal women suffering from VMS. Isoflavones exhibit
weakened estrogenic effects on estrogen receptors depending
on the target tissue and concentration of circulating
estrogen levels.
Clinical trials of soy or isoflavone-supplemented diets have
investigated the relationship between soy intake and
alleviation of VMS. Inconsistent results were found amongst
the literature reviewed. Improved experimental design may
20
enhance consistency between future clinical trials and
reduce the common theme of high dropout rates in current
literature. Investigation of the biological mechanisms
involved with soy isoflavones would provide insight on the
safety of these supplements, and potential approval by the
FDA. Soy isoflavones in the treatment of VMS appear to be
promising, and deserve further research and consideration
for therapy.
References
Alamo, C., Lopez-Munoz, F., Guerra, J.A., Garcia-Garcia, P.,
2010. Soy isoflavones and their effects on menopause
symptoms. RPMP. 28, 281–318.
Albertazzi, P., Pansini, F., Bonaccorsi, G., Zanotti, L.,
Forini, E., De Aloysio, D., 1998. The effect of dietary soy
supplementation on hot flushes. Obstet. Gynecol. 91, 6–11.
21
Bedell, S., Nachtigall, M., Naftolin, F., 2014. The pros and
cons of plant estrogens for menopause. J. Steroid.
Biochem. Mol. Biol. 139, 225–236.
Brzezinski, A., Adlercreutz, H., Shaoul, R., Rosier, A.,
Shmueli, A., Tanos, V., Schenker, J.G., 1997. Short-term
effects of phytoestrogen-rich diet on postmenopausal
women. Menopause. 4, 89–94.
Brzezinski, A., Debi, A., 1999. Phytoestrogens: the
"natural" selective estrogen receptor modulators? Eur. J.
Obstet. Gynecol. Reprod. Biol. 85, 47–51.
Carmignani, L.O., Pedro, A.O., Costa-Paiva, L.H., Pinto-
Neto, A.M., 2010. The effect of dietary soy
supplementation compared to estrogen and placebo on
menopausal symptoms: a randomized controlled trial.
Maturitas. 67, 262–269.
Chalupka, S., 2011. Soy isoflavones for the prevention of
menopausal symptoms and bone loss--a safe and effective
alternative to estrogen? AAOHN J. 59, 504.
Hamilton-Reeves, J.M., Rebello, S.A., Thomas, W., Slaton,
J.W., Kurzer, M.S., 2007. Isoflavone-rich soy protein
22
isolate suppresses androgen receptor expression without
altering estrogen receptor-beta expression or serum hormonal
profiles in men at high risk of prostate cancer. J. Nutr.
137, 1769–75.
Levis, S., Strickman-Stein, N., Doerge, D.R., Krischer, J.,
2010. Design and baseline characteristics of the soy
phytoestrogens as replacement estrogen (SPARE) study—a
clinical trial of the effects of soy isoflavones in
menopausal women. Contemp. Clin. Trials. 13, 293–302.
Migliaccio, S., Anderson, J.J., 2003. Isoflavones and
skeletal health: are these molecules ready for clinical
application? Osteoporos. Int. 14, 361–388.
Murkies, A.L., Lombard, C., Strauss, B.J., Wilcox, G.,
Burger, H.G., Morton, MS., 1995. Dietary flour
supplementation decreases post-menopausal hot flushes:
effect of soy and wheat. Maturitas. 21, 189–195.
Quella, S.K., Loprinzi, C.L., Barton, D.L., Knost, J.A.,
Sloan, J.A., LaVasseur, B.I., Swan, D., Krupp, K.R.,
Miller, K.D., Novotny, P.J., 2000. Evaluation of soy
phytoestrogens for the treatment of hot flashes in
23
breast cancer survivors: A North Central Cancer Treatment
Group Trial. J. Clin. Oncol. 18, 1068–74.
Rathus, S.A., Nevid, J.S., Fichner-Rathus, L., Herold, E.S.,
McKay, A., 2012. Human Sexuality in a World of Diversity,
fourth ed. Pearson, Toronto.
Setchell, K.D., Cassidy, A., 1999. Dietary isoflavones:
biological effects and relevance to human health. J.
Nutr. 129, 758S–767S.
Uehara, M., Ishimi, Y., Katsumata, S., Suzuki, K., 2008.
Transformation of daidzein to equol and its
bioactivity. ACS Symp. Ser. Am. Chem. Soc. 993, 81–89.
Villaseca, P., 2012. Non-estrogen conventional and
phytochemical treatments for vasomotor symptoms: what needs
to be known for practice. Climacteric. 15, 115– 124.
Vincent, A., Fitzpatrick, L.A., 2000. Soy isoflavones: are
they useful in menopause? Mayo Clin. Proc. 75, 1174–
1184.
Yoles, I., Yogev, Y., Frenkel, Y., Hirsch, M., Nahum, R.,
Kaplan, B., 2004. Efficacy and safety of standard versus
low dose of Femarelle® (Tofupill) for the treatment of
24
menopausal symptoms. Clin. Exp. Obstet. Gynecol. 31,
123–126.
25
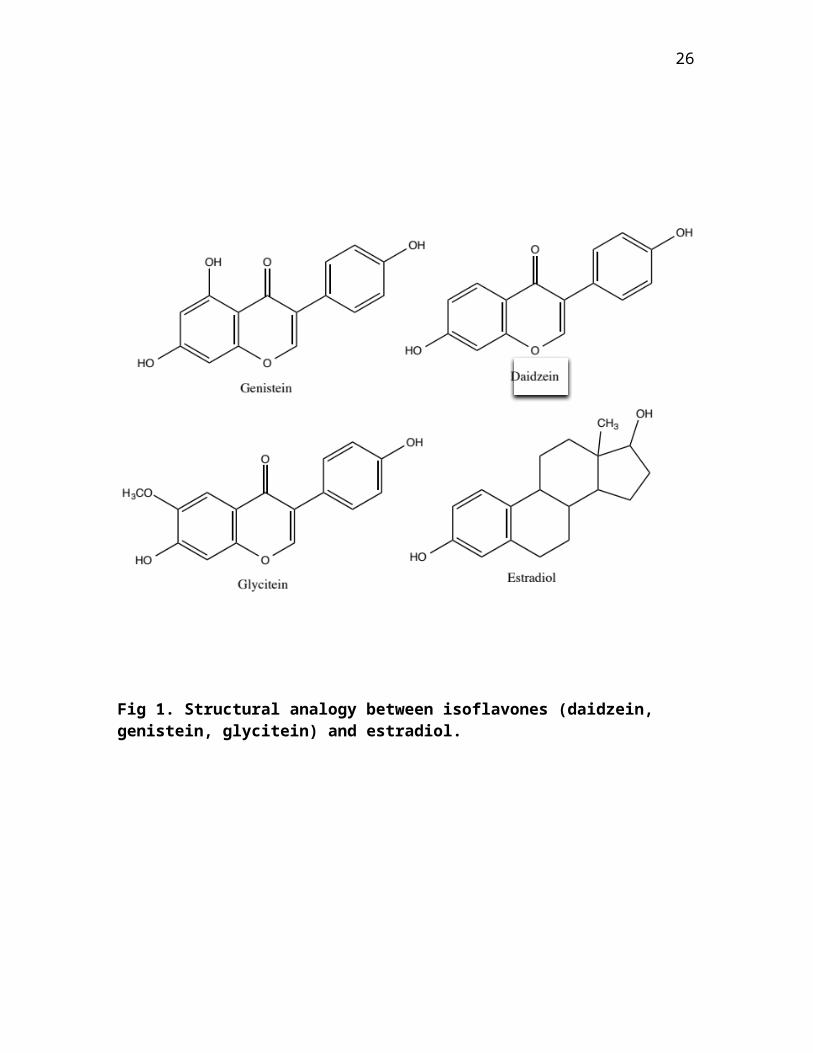
Fig 1. Structural analogy between isoflavones (daidzein, genistein, glycitein) and estradiol.
26
SERM
Estrogen receptor in bone & brain
Estrogen receptor in breast & uterus
Estrogen receptor not activated (antagonistic activity)
Estrogen receptor activated(agonistic activity)
No breast & uterine cell proliferation
Menopausal symptoms relief & bone cell proliferation
27





























