Embed Size (px)
Citation preview

Paediatric and Perinatal Epidemiology 1988, 2, 138-147
The perinatal morbidity and mortality survey of Jamaica 19 86-1 9 87
Deanna Ashley, Affette McCaw-Binns and Karen Foster- Williams Ministry of Health and Department of Child Health, University of the West Indies, Jamaica
Summary. The Jamaican Perinatal Morbidity and Mortality Survey was conducted between September 1986 and August 1987. A total of 10 310 consecutive births were identified and mothers interviewed in the first 2 months (main cohort study), 1405 neonatal admissions were evaluated over a 6-month period (morbidity study), and 1855 perinatal deaths and 73 late neonatal deaths identified over 12 months (mortality study)-55% of the deaths were given a postmortem examination. The perinatal mortality rate for the cohort study was 38.1 per 1000 births. This was 36.6 percent higher than the 1982 estimate of 27.9/1000 based on deliveries at the Victoria Jubilee Hospital, a specialist maternity institution which has at least 13 000 deliveries per annum.
Introduction
Jamaica is an island nation of 4411 square miles and 2.3 million people in the Caribbean Sea south of Cuba and West of Haiti (Figure 1) between the Equator and the Tropic of Cancer. The centre is mountainous, rising to 2500 metres. The climate is tropical. The gross national product in 1986 was US$2124 million with a mean annual per capita income of US$909.'
The health services are fairly well organised and distributed. Expansion of primary care services in the 1970s has placed 90% of the population within 5 miles of one of 364 health centres which provide basic antenatal, postnatal, child health, curative and domiciliary services.
Address for correspondence: Dr D. Ashley, Ministry of Health, 10 Caledonia Avenue, Kingston 5, Jamaica, West Indies.
138

Morbidity and mortality in Jamaica 139
70*
ATLANTIC
OCEAN
4AMil
$aS,,,,
'a .:I.
20'
P E R T RICC c
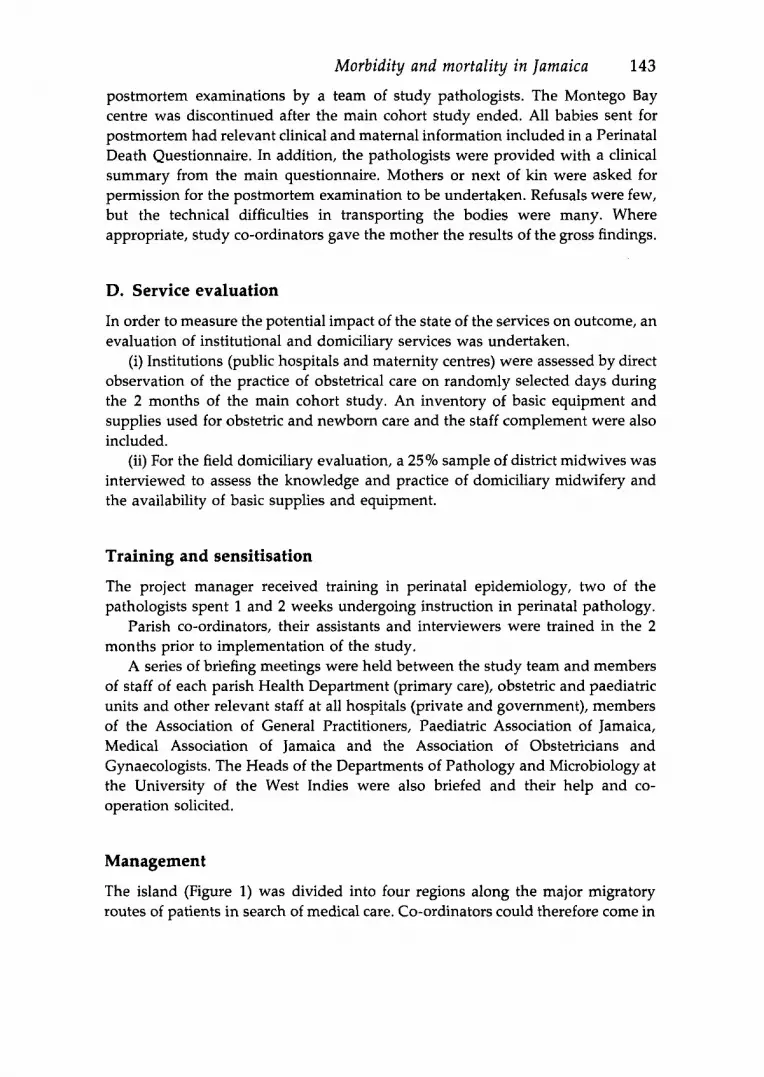
Figure 1. Jamaica: parishes, regional administrative areas and distribution of hospitals. West: lO=Westmoreland; 9=Hanover; 8=St James; 7=Trelawny. South: l l=S t Eliza- beth; 12=Manchester; 13=Clarendon. North East: 6=St Ann; 5=St Mary; 4=Portland. South East: 14=St Catherine; 1/2=Kingston and St Andrew; 3 =St Thomas.
The island is divided into 14 administrative units called parishes each of which has at least one hospital providing basic maternal, general medical and general surgical services. Facilities vary from the most basic at Type C hospitals to a wider range of specialist services at the three Type A tertiary care institutions which provide specialist obstetrical, neonatal and paediatric care. The latter are located in the cities of Kingston and Montego Bay. In all, on the island, there are a total of 20 public and six private hospitals.
The most recently published figures give a crude birth rate of 24 per 1000 (1985),* crude death rate of 6 per 1000 (1985),2 and infant mortality rate of 27per 1000 livebirths (1980).3 The estimated perinatal mortality rate in 1982 was 27.9 per 1000,4 based on a detailed study of births at the large public maternity hospital in Kingston.
Background to the study
Perinatal and neonatal mortality are important indicators of the health status of the population and also reflect the status of the health services. Monitoring of

140 D. Ashley et al. these variables in Jamaica, however, has been very difficult and the data generated through registration of stillbirths and infant deaths have been very unreliable.
Under-registration of infant deaths for example, was found to be as high as 33% in one parish, and only 37% of early neonatal deaths were registered in 1982.5 The registered stillbirth rate (1984) was reported to be 5.9 per 1000, known to be a gross underestimate given the knowledge that the rate for deliveries occurring in public hospitals was more than double that figure.
Lowry6 reported that perinatal mortality rates for the University Hospital had not changed over a 10-year period: for the years 1963-1965 the rate was 35.1, for 1973-1975 the rate was 38.8. This, in spite of the fact that as a matter of hospital policy only women booking in the first trimester are accepted for delivery. There are no emergency unbooked admissions and few transfers from other hospitals to the University Hospital.
The Child Mortality Study of 1972 clearly demonstrated the extent of under- reporting of early infant deaths. Following publication of the findings of that study, we were challenged and encouraged by Professor Neville Butler in 1979 and spurred on by the Paediatric Association of Jamaica to carry out a perinatal morality survey in Jamaica.
A project proposal with draft questionnaires was submitted in December 1984 and funding approved in June 1985. It was agreed that the study would be implemented through the University of the West Indies’ Child Health Depart- ment, although the principal investigators were full time employees of the Ministry of Health. Preparatory work for implementation of the study was initiated in December 1985.
Aims and objectives
The overall aim of this study was to provide information required to improve the maternal and child care services and reduce perinatal morbidity and mortality in Jamaica.
Specific objectives
Mortality
1. To determine the stillbirth and neonatal mortality rate (early and late). 2. To determine the clinical and pathological causes of these deaths. 3. To identify maternal and environmental characteristics associated with increased risk of stillbirths and neonatal deaths. 4. To identify clinical characteristics (in the mother or newborn) predictive of death of the fetus or infant.

Morbidity and mortality in Jamaica 141
Morbidity
1. To identify the infants who get ill in the neonatal period and determine the causes of neonatal morbidity. 2. To identify maternal, environmental and clinical characteristics predictive of serious neonatal morbidity. 3. To determine whether criteria used to identify pregnancies at high risk of mortality also adequately identify those at high risk of major morbidity.
Low birthweight
1, To identify the birthweight distribution and birthweight-specific mortality and morbidity rates. 2. To determine maternal, environmental and clinical factors associated with: (a) low birthweight associated with short gestation; (b) low birthweight associated with growth retardation.
Health care services
1. To describe operational problems and constraints within the current manage- ment of obstetric and neonatal services. 2. To assess levels of basic equipment and facilities at different levels of care and their potential impact on morbidity and mortality. 3. To develop appropriate risk scores or check lists for use at different levels of care. 4. To revise norms and procedures for use at the primary care level. 5. To develop norms and procedures for use at the secondary care level. 6 . To modify or redesign (as appropriate) the basic, post-basic and in-service training for all staff involved in perinatal services. 7. To revise the national strategy and programmes to reduce perinatal mortality.
Methodology
In order to achieve the objectives of the study, observation periods of different lengths were required in order to attain adequate sample sizes. The survey was divided into four components: (a) main cohort study (2 months), (b) neonatal morbidity (6 months), (c) perinatal mortality (12 months) and (d) service evaluation to run concurrent with the cohort study.
Organisation and administration of the study
A 15 member Steering Committee was established in January 1986 to act as an

142 D. Ashley et al.
advisory body -providing the necessary input advice and critique in the organisation and implementation of the study. This included obstetricians, paediatricians, pathologists and midwives.
Staffing There were two full-time professional members of staff employed on the study - the Study Administrator (A.M-B) and the Paediatric Research Officer (K.F-
At the field level, each parish had a co-ordinator with responsibility for managing study activities and supervising the team of interviewers. The eight larger parishes had an assistant co-ordinator also. Full-time interviewers were assigned to the hospitals and a core of district midwives (field interviewers) were selected to interview mothers delivering at home. A nominal cash incentive (J$2/ $US0.36) was offered to other members of the primary health care team who brought the occurrence of a delivery to the attention of the field interviewers.
A team of four pathologists (in Kingston and in Montego Bay) performed postmortems with the assistance of the Paediatric Research Officer.
W).
A. The main cohort
In this phase, all pregnant women were included who had a live birth, or stillbirth of 500g or more, during the 2-month period 1 September-31 October 1986, regardless of the place of delivery. These women were interviewed and their babies examined, usually within the first 48 hours after delivery. Between 6 weeks and 3 months after delivery mothers and their infants were again interviewed and examined at postnatal clinics. Those persons who went to private doctors or who failed to show up for their clinic appointments were visited at home to facilitate completion of the follow-up questionnaire.
B. Morbidity component
All babies with major illnesses admitted to any of the neonatal care units in any of the eight hospitals with paediatric consultants were included in the morbidity study. Each case had a neonatal admission questionnaire completed by the attending paediatrician and the mother was interviewed. The survivors were followed up at 6 weeks.
C. Mortality component
Stillbirths (fresh or macerated) and neonatal deaths were transferred (where possible) to either of three institutions (Montego Bay - 1, Kingston - 2) for
Morbidity and mortality in Jamaica 143
postmortem examinations by a team of study pathologists. The Montego Bay centre was discontinued after the main cohort study ended. All babies sent for postmortem had relevant clinical and maternal information included in a Perinatal Death Questionnaire. In addition, the pathologists were provided with a clinical summary from the main questionnaire. Mothers or next of kin were asked for permission for the postmortem examination to be undertaken. Refusals were few, but the technical difficulties in transporting the bodies were many. Where appropriate, study co-ordinators gave the mother the results of the gross findings.
D. Service evaluation
In order to measure the potential impact of the state of the services on outcome, an evaluation of institutional and domiciliary services was undertaken,
(i) Institutions (public hospitals and maternity centres) were assessed by direct observation of the practice of obstetrical care on randomly selected days during the 2 months of the main cohort study. An inventory of basic equipment and supplies used for obstetric and newborn care and the staff complement were also included.
(ii) For the field domiciliary evaluation, a 25% sample of district midwives was interviewed to assess the knowledge and practice of domiciliary midwifery and the availability of basic supplies and equipment.
Training and sensitisation
The project manager received training in perinatal epidemiology, two of the pathologists spent 1 and 2 weeks undergoing instruction in perinatal pathology.
Parish co-ordinators, their assistants and interviewers were trained in the 2 months prior to implementation of the study.
A series of briefing meetings were held between the study team and members of staff of each parish Health Department (primary care), obstetric and paediatric units and other relevant staff at all hospitals (private and government), members of the Association of General Practitioners, Paediatric Association of Jamaica, Medical Association of Jamaica and the Association of Obstetricians and Gynaecologists. The Heads of the Departments of Pathology and Microbiology at the University of the West Indies were also briefed and their help and co- operation solicited.
Management
The island (Figure 1) was divided into four regions along the major migratory routes of patients in search of medical care. Co-ordinators could therefore come in

144 D. Ashley et al.
contact with persons in adjacent parishes where a mother may have had antenatal care or been delivered.
Co-ordinators would visit hospitals daily in the first phase (September and October 1986) and at least twice weekly in the second phase (November 1986 to August 1987) to keep track of deliveries, neonatal admissions and deaths, collect completed questionnaires and ensure their submission to the national office. The mail service was not to be used as this can sometimes be unreliable with long delivery delays. All material was to be transferred by messenger or by the co- ordinators themselves.
Each parish co-ordinator was provided with a supervisor’s manual setting out guidelines for completion and preliminary processing of the questionnaires as well as administrative procedures and the maintenance of a register of all deliveries and deaths in the parish during the study period.
Interviewers were also provided with manuals which outlined basic interview- ing techniques and took them through each question on the relevant question- naires. Administrative procedures were outlined.
Hospitals participating in the morbidity survey were provided with neonatal admission forms and newborn nursery charts to guarantee the collection of uniform basic information on the neonate. The neonatal admission questionnaires were for completion on discharge (or death) of the infant.
Each mother who attended between 6 weeks and 3 months post-delivery was presented with a certificate on which was included her child’s study number. At 1 year of age the infants were sent birthday cards. These were used in the hope that they will facilitate subsequent follow-up studies of the cohort.
The questionnaires
Eight questionnaires were developed, pre-tested and finally used in the study; all but the pathology questionnaire were precoded. 1. The main questionnaire contained information on past obstetric history, social and environmental factors, the antenatal period, labour and delivery. Infants were examined and supplementary information from institutional records included. Antenatal, intrapartum and postpartum data were supplemented by other hospital, clinic or doctor’s records as necessary. Often this entailed collaboration between parish co-ordinators, especially where antenatal records were required. 2. The follow-up questionnaire contained sections relating to the postnatal status of the mother and the infant. The questionnaire was completed by interviewing the mother, and examining both mother and infant. 3. The neonatal admission form was completed by the attending paediatrician or study research paediatrician for each newborn admitted to newborn nurseries before the age of 28 days.

Morbidity and mortality in Jamaica 145
Prior to the implementation of the study a standardised newborn nursery chart was introduced in all nurseries to facilitate completion of the neonatal admissions questionnaire. 4. The infant death/stillbirth form summarised information on the particulars of death including place and time and a brief clinical history of the events surrounding labour, delivery and the immediate postpartum period which may have contributed to the outcome. 5. A maternal death questionnaire was developed to collect basic information on mothers dying during the l-year study period, recording date and place of delivery and date and cause of death. 6. The pathology questionnaire provided a detailed guide for the postmortem examination of the infant on a systematic basis and was completed by the study pathologists at the time of postmortem. 7. The institutional service evaluation questionnaire consisted of three parts: (a) a schedule of observation of practice of maternal care, (b) an equipment inventory, (c) a staff inventory. 8. The domiciliary evaluation questionnaire provided a methodology for measur- ing knowledge and practice of domiciliary midwifery and the availability of supplies and equipment for this purpose.
Data processing Questionnaires were checked by the clerical staff and reviewed by the Study Administrator, the paediatrician and a small team. These questionnaires were then microfilmed prior to being coded and the data were put on transcription sheets. These sheets were then transferred to a private data processing company for data entry and computer editing (range and logic tests). This was supervised by the statistician at the Health Information Unit of the Ministry of Health.
Preliminary results There were 10 310 births during the main cohort study, 8956 (87%) of these were followed up in the postnatal period. A total of 393 deaths were identified in the main cohort giving a perinatal mortality rate of 38.1 per 1000 total births.
There were 1405 neonatal admissions to specialist units during the &month study period.
A total of 1855 fetal and early neonatal and 73 late neonatal deaths were identified during the l-year study. Postmortem examinations were undertaken on 1021 of the 1855 perinatal deaths yielding an overall postmortem rate of 55%.
A total of 78 midwives were interviewed for the domiciliary service evaluation. Observations were done at all public hospitals and maternity centres.
The maternal mortality rate for the year was 10.4 per 10 000 births, unchanged since a confidential enquiry into all maternal deaths was undertaken for the years 1980-1 982?

146 D. Ashley et al.
Discussion
The perinatal mortality rate identified for the 2-month cohort study represents a minimum estimate, It is possible that we have missed some of the deliveries and perinatal deaths in those rural parishes with a high rate of home deliveries attended by traditional untrained birth attendants (nanas). In addition, we feel that there may well be a number of early neonatal deaths occurring after the mother had left hospital. Although there was a high follow-up rate (87%) which exceeded 95% in rural parishes, it is likely that the group of mothers not traced will include many such deaths.
The morbidity survey results are eagerly anticipated as this is the first time such a survey has been attempted anywhere. The questionnaire is currently being adapted for use in a number of studies in Europe and elsewhere.
A data verification process will begin shortly to determine which births may have been missed by checking the Registrar General’s records of births registered for the cohort study period.
In order to achieve the aims of the survey, specific analyses of the data are being undertaken by various members of the Ministry of Health and the university departments. The large amount of data collected on substantial numbers of births, deaths, and neonatal admissions should ensure that statisti- cally reliable results will be obtained.
Acknowledgements
This vital and extensive study has been financed by the International Develop- ment Research Centre of Canada. Dr Jean Golding provided invaluable assistance in the preliminary drafting of questionnaires, training the project administrator and guiding the coding and analysis of the data. Dr Jean Keeling, Consultant in Paediatric Pathology, John Radcliffe Maternity Hospital has trained and guided the pathologists through postmortem examination and analysis of the findings. Mr Terry Shenton, Department of Child Health, Bristol and Ms Carol Gayle, Ministry of Health, Jamaica have been the main computer programmers.
The team of pathologists and paediatricians along with the co-ordinators, their assistants, the interviewers, the co-operative Jamaican mothers and their babies made the study a reality.
References
1 Planning Institute of Jamaica. Economic and Social Survey, 1986. 2 Statistical Institute of Jamaica. Demographic Statistics, 1986. 3 Desai, P., Hanna, B.F., Melville, B.F. et a l . Infant mortality rate in three parishes of Western Jamaica, 1980. West lndies Medical Journal (1983) 3283. 4 Ashley, D., Gayle, C., Fox, K. A Retrospective Study of Perinatal and Neonatal Mortality at the Victoria jubilee Hospital in 1982 (1985) Ministry of Health, Jamaica. (Mimeo).

Morbidity and mortality in Jamaica 147
Figueroa, J.P., McCaw, A.M., Wint, 0.A. Review of Primary Health Care in Jamaica,
Lowry, M., Hall, J., Sparke, B. Perinatal Mortality in Childhood. PAHO Scientific
Puffer, R.R., Serrano, C.V. Patterns of Mortality in Childhood. PAHO Scientific
Walker, G., Ashley, D., McCaw, A. et al. Maternal mortality in Jamaica. Lancet 1986;
5 1977-1982. PAHO Project Consultancy Report. Washington, DCPAHO. 6 Publication No. 262. Washington, DC: PAHO, 1973. 7 Publication No. 262. Washington, DC: PAHO, 1973. 8 k486-488.
Book review
Prevention of Accidental Poisoning in Childhood. Edited by W.H.J. Rogrnans. European Consumer Product Safety Organisation, Amsterdam. US$15, pp. 157.
This is a disappointing book. It reports a conference in Brussels organized under the auspices of the Commission of the European Community in November 1985. Much of the data in the book is from poisons units rather than from presentations to accident and emergency departments or hospital wards and the whole book is poison rather that child orientated. So much so that the only paediatrician who took part was Hugh Jackson, who gave his usual thoughtful and clear presentation.
The section on the use of household products was confined largely to the use of such things as metal polish and detergents, both of which are not seriously toxic in children. The chapter on ingestion of caustics made no mention of the use of steroids in acute management. One looked in vain for a section where the clinical assessment of the toxicity of different household products was discussed.
The contribution on ‘Intoxication by Analgesics’ by Dr Proudfoot, an adult physician, made little of the success of child resistant containers in reducing childhood analgesic poisoning in this country and in America. There was a helpful contribution from a packaging consultant, Mr P.W.S. Win, on the effectiveness, costs and benefits of child resistant containers. He made the sensible conclusion in a complicated situation that the manufacturer should not be left to his own devices. This kind of interpretation is relatively rare in the book and one was left with the feeling that there was little that was raised in this conference to increase the safety of children from accidental poisoning. Nevertheless some of the recommendations and suggestions for action at the end are useful, particularly on the need to use child resistant containers but to restrict their use to medicines and household products of proven toxicity.
J.R. SIBERT























![[2021] JMCC Comm 42 - Supreme Court of Jamaica](https://img.pdfslide.net/doc/110x75/633455a662e2e08d490294c9/2021-jmcc-comm-42-supreme-court-of-jamaica.jpg)





