Embed Size (px)
Citation preview
Burns 31 (2005) 37–44
www.elsevier.com/locate/burns
The stigma of burns
Perceptions of burned patients’ relatives when facing
discharge from hospital
L.A. Rossia,*, V. da S.C. Vilab, M.M.F. Zagoa, E. Ferreirac
aDepartamento de Enfermagem Geral e Especializada, Escola de Enfermagem de Ribeirao Preto,
WHO Collaborating Center for Nursing Research Development, Universidade de Sao Paulo,
Av. Bandeirantes, 3900, CEP 14040-902 Ribeirao Preto, Sao Paulo, BrazilbDepartamento de Enfermagem e Fisioterapia da Universidade Catolica de Goias, Sao Paulo, Brazil
cUnidade de Queimados da Faculdade de Medicina de Ribeirao Preto, Universidade de Sao Paulo, Brazil
Accepted 13 July 2004
Abstract
The objective of this ethnographic study was to investigate the cultural meanings reported by 25 relatives of burned patients about
their loved one’s impending hospital discharge. Data were collected by means of participant observation and semi-structured interviews
conducted during hospital visiting hours, and support group meetings with relatives. The following inter-related phases were considered in
the analysis process: reading of the material and data reduction (selection of data using the objective of the study as a guide), data display,
conclusion outlining, and verification. Following this process, the data were coded and similar codes were grouped into categories. It was
found that the relatives of burned patients felt afraid when faced with the prospect of hospital discharge. Their descriptions reveal the
family’s feelings and attitudes in face of other people’s reactions, and in face of the patient’s own reactions in the context of possible changes
in their social roles.
# 2004 Elsevier Ltd and ISBI. All rights reserved.
Keywords: Burns; Culture; Rehabilitation
1. Introduction
In the recent years, advancements in the treatment of
burns have resulted in a higher rate of survival of patients
with serious injuries. Many of them suffer major sequelae.
Even when they become independent, such patients require
gradual adjustments to the psychological stress of the acute
and traumatic changes in their lifestyles [1].
The development of this type of trauma includes three
phases. The resuscitation phase, which corresponds to the
first 48–72 h following the burn, is characterized by
uncertainty regarding potential outcomes and the struggle
for survival [2]. In this critical care phase, the most
common psychological and psychiatric symptoms are
* Corresponding author. Fax: +55 16 6333271.
E-mail address: [email protected] (L.A. Rossi).
0305-4179/$30.00 # 2004 Elsevier Ltd and ISBI. All rights reserved.
doi:10.1016/j.burns.2004.07.006
delirium followed by anxiety, sleep disturbance, and
confusion [3]. Patients also experience discomfort, pain
and fear [1]. At this stage, the patient’s attention is focused
on survival and the physiological factors on which it
depends [4].
The second phase, acute rehabilitation, begins with the
improvement of physical conditions and is the period when
the patient is submitted to surgery and when various other
painful procedures are carried out, such as, wound cleansing
and dressings. The patient may exhibit depression, anxiety,
and acute stress disorder or other psychological difficulties
such as nightmares, sleep problems, and behavioral
regression [5]. In this phase, the family members display
fear and anxiety stemming from the performance of
procedures and expectations concerning their results.
Finally, the long-term rehabilitation phase of recovery
begins when patients leave the hospital [5] and face other
L.A. Rossi et al. / Burns 31 (2005) 37–4438
people in the social world. During this last phase, patients
and relatives begin to express their expectations regarding
the difficulties to be faced during reintegration into everyday
life.
Since relatives can be a major source of social support
to patients surviving burns [1,4,6], it is important to assess
their perception of the rehabilitation process [1]. Relatives
of burned patients, because they experience all the phases
of burn recovery in a similar way as their loved ones do [6],
may feel a mixture of happiness and fear in relation to what
is to come as hospital discharge approaches. The fear,
anguish, and doubts that become part of the relatives’
everyday lives may also hinder the recovery of burn
victims. Family members, not only the patient, are
psychologically traumatized by the impact of a severe
burn [7]. Their inter-relationships, as well as the way they
cope with problems and seek support, are essential aspects
for the well-being of groups and individuals sharing the
same environment. When one of its members is ill or
suffers a trauma, the family unit is also affected in its
capacity to adapt and cope with the resultant demands
[8,9]. In this aspect, burns represent a terrible trauma for
the family as it involves the family members’ feelings of
loss, grief, and guilt. In these situations, the family is
required to show special flexibility and capability of
adapting to new situations [8].
During the weekly family group meetings held at the
Burns Unit of the Ribeirao Preto Medical School Clinical
Hospital (HCFMRP), where this study was conducted, it has
been observed that positive attitudes from relatives
regarding the situations experienced by burned patients
seem to be important for patient recovery. In view of the
possibility of being discharged from hospital, patients and
relatives frequently express their expectations concerning
the difficulties they may face during social reintegration and
redefinition of family roles. They anticipate the need for
commitment, acceptance, responsibility, and a great deal of
dedication.
In a review, Shenkman and Stechmiller [1] have reported
that psychological adaptation in individuals who have
suffered burns tends to occur approximately 1 year after the
trauma. During the first year, burn victims may experience
post-traumatic neurosis and depression, expressing feelings
of helplessness and hopelessness [1]. These feelings can be
more or less aggravated, depending on their family and the
social environment the burned person lives in.
Since family members may experience feelings, which
are similar to those of the patient’s [6], their attitudes are
very important because, in spite of suffering, they are
expected to help the patient. The changes stemming from the
trauma may be valued or devalued by family members and,
consequently, their reactions may or may not be helpful to
the patient. Consequently, relatives’ reactions influence
patients’ rehabilitation process as negatively or positively.
Blakeney et al. [10] assessed adolescents survivors of severe
childhood burn injuries for indicators of psychopathology
and for factors that might enhance psychosocial adjustment
and found that positive psychological adjustment was
predicted by higher family cohesion, independence, and
more open expressiveness within the family. In a study of
social support and post-burn adjustment, Davidson et al. [11]
concluded that when relatives or friends express feelings of
acceptance and support, they can help the patient in his/her
social reintegration. However, although those people are
frequently the major social supporters, they may also feel
pressured by the psychological needs of the disfigured
person. Support is very important even for families who
seem to be very strong [12].
The health-care team can influence the success of
rehabilitation. They can work with the family in order to
minimize the relatives’ psychological anguish and promote
means to relieve suffering [13], to decrease conflict, and also
to enhance stability and cohesion [12]. In this process, it is
important to consider that relatives’ reactions are social and
cultural constructions and need to be evaluated and
discussed by professionals.
Shenkman and Stechmiller [1] studied the impact of
morbidity and other sequelae on burn victims and their
relatives after hospital discharge and verified that, unlike
patients, relatives expressed more concern regarding the
support that patients would need to function after
hospitalization. In another study, using a qualitative
approach, the concerns and needs of burned patients’
relatives were shown to be about the patient’s physical and
psychological needs; the major sources of support reported
were family and friends, burn center staff, and spirituality
[13].
Several authors studied the importance of family
participation during the hospitalization and rehabilitation
processes [10–18]. Some of these researchers documented
the importance of the support provided to family members in
support group meetings with the health-care team [14–18].
The following were found to be critical to successful or
unsuccessful adaptation of a burned patient: the family
members’ reactions in respect to the notion that their burned
family member has experienced a chronic problem; their
abilities to support and help with treatments; and the many
associated problems stemming from the rehabilitation
process in the social world the patient must return to [15].
Although the importance of the family’s role as a support
for the social reintegration of a burned patient has been
highly emphasized, no study has been found which address
the cultural meanings that family members attribute to the
possibility of living with a person who has been traumatized
by burning. This was, therefore, the focus of this
investigation. It is part of a previous study aimed at
identifying the cultural meanings that relatives attributed to
their participation in the process of caring for a burned
person and the care strategies they reported [19]. This paper
identified the cultural meanings reported by a group of
relatives of burned people as they faced the prospective of
hospital discharge in Ribeirao Preto, Brazil.

L.A. Rossi et al. / Burns 31 (2005) 37–44 39
2. Method
The 25 participants in this ethnographic study were
relatives or people close to patients admitted to the Burns
Unit of the HCFMRP. The participants were over 21 years
old, reported that they had close attachment with the patient,
and could participate in caregiving after hospital discharge.
The first author (L.A.R.) collected the data by means of
participant observation and semi-structured interviews
conducted during hospital visiting hours and support group
meetings with relatives. One or more relatives from each
family were allowed to participate in the support group
meetings. When selecting interview participants, an attempt
was made to identify key informants, i.e., relatives or close
friends who would be willing to provide information and
would be available to tell us about the phenomenon.
After the Ethics and Research Committee of the institution
had approved the study, fieldwork began. Twenty-five
relatives who met the inclusion criteria were interviewed
from January to September 2000, after reviewing and signing
a consent form. The frequency of contact with relatives varied
according to the severity of the patient’s condition, need for
support from relatives, and researchers’ availability. It was
observed that, generally, relatives of patients with more severe
burns visited the hospital and participated in meetings more
frequently. Twenty-two meetings were held with family
members, lasting, on average, 60 min each. During the data
collection period, all the activities performed by relatives,
while staying in the Burns Unit, were observed and field
notes written after each observation or interaction period.
The formal interviews were guided by the following initial
questions: What is it like to have a relative (or a friend) who
has been burned? How do you feel in relation to your relative
(or friend)? What is going to happen when your relative (or
friend) returns home? What do you intend to do when s/he
returns home? How do you think you can help him/her?
Informal interviews were also carried out. In some cases,
more than one member from the same family was
interviewed. Six members participated only in the informal
interviews and meetings. As a consequence, the number
used as identification of family members surpasses the
number of patients. Each participant was assigned an
identification code (a number and a letter that indicate the
relationship: Mother – M; Wife – W; Father – F; Grandmother
– GM; Sister –S; Aunt – A and Researcher – R).
The data obtained from participant observation, informal
interviews, and field notes were, when even possible, typed
directly into a computer. The data from semi-structured
interviews were recorded on tape and transcriptions were
later entered into a computer.
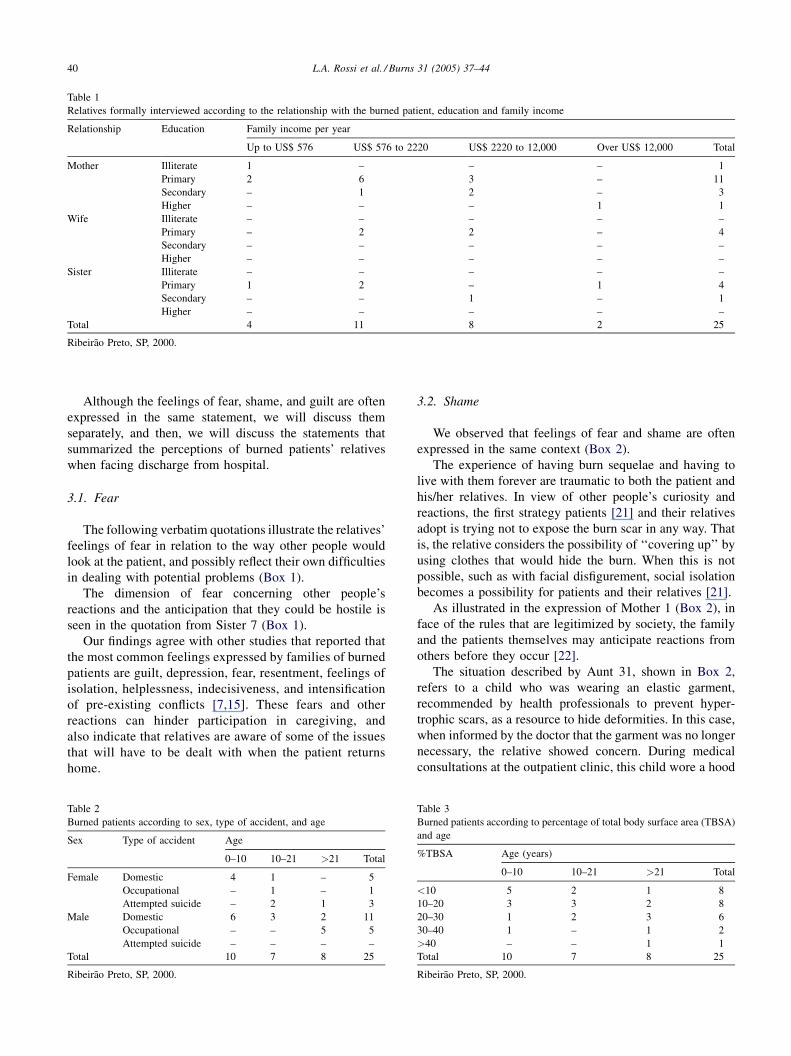
2.1. Characteristics of the 25 relatives formally
interviewed and of the burned patients
Twenty-five relatives of burned patients were formally
interviewed. Of the 25 relatives, 24 had started school, but
19 finished only the first grade. Only one family member
finished higher education, having an income higher than
US$ 12,000. Mothers were the patients’ closest relatives
(16), followed by sisters (5) (Table 1).
Tables 2 and 3 show that 17 patients were less than 21
years of age. That fact can explain the higher number of
mothers participating in this study. We observed in two
families, in which the wives had offered to take care of their
husband, that the mothers in law also showed interest in
sharing the care. Only three patients had burns covering
more than 30% of the TBSA. Of all the patients, whose
families participated in this study, only one did not have
functional sequelae or visible scars.
2.2. Data analysis
The following inter-related phases were considered in the
analysis process: exhaustive reading of interviews and data
reduction, data display, conclusion outlining, and verifica-
tion. The reading and the data reduction that refer to the
process of selecting, focusing, simplifying, abstracting, and
transforming data, started as data were collected. At first, the
first author attempted to select data or ideas featuring
important concepts by carefully reading the information as it
was collected and organized, focusing on the objective of the
study as a guide. Following this process, the data were
coded, and similar codes were grouped into categories. Each
unit was described and conceptualized [20].
In order to check the codes and categories created, three
other experienced researchers were requested to conduct the
same procedure using randomly selected data records
(approximately 10 pages, including interviews and field
notes). Only one researcher made a suggestion, i.e., to
rename a code, which was accepted. No other codes were
introduced by means of this procedure.
Several concepts were identified, two of which are
presented here: relatives’ perspectives of impeding hospital
discharge and the cultural meanings concerning their
responses.
3. Results and discussion
The information collected from participant observation
as well as formal interviews showed that the most outstanding
aspects were the feelings and behaviors expressed by
families in relation to the sequelae presented by patients.
It was found that the relatives of burned patients felt
afraid when they faced the prospect of hospital discharge.
Their descriptions reveal the family’s feelings and reactions
in face of other people’s reactions, and in face of the
patient’s own reactions in the context of possible changes in
their social roles.
Fear, shame, and guilt were the feelings reported by many
of the burned patients’ relatives when they were requested to
talk about the upcoming discharge from hospital.
L.A. Rossi et al. / Burns 31 (2005) 37–4440
Table 1
Relatives formally interviewed according to the relationship with the burned patient, education and family income
Relationship Education Family income per year
Up to US$ 576 US$ 576 to 2220 US$ 2220 to 12,000 Over US$ 12,000 Total
Mother Illiterate 1 – – – 1
Primary 2 6 3 – 11
Secondary – 1 2 – 3
Higher – – – 1 1
Wife Illiterate – – – – –
Primary – 2 2 – 4
Secondary – – – – –
Higher – – – – –
Sister Illiterate – – – – –
Primary 1 2 – 1 4
Secondary – – 1 – 1
Higher – – – – –
Total 4 11 8 2 25
Ribeirao Preto, SP, 2000.
Although the feelings of fear, shame, and guilt are often
expressed in the same statement, we will discuss them
separately, and then, we will discuss the statements that
summarized the perceptions of burned patients’ relatives
when facing discharge from hospital.
3.1. Fear
The following verbatim quotations illustrate the relatives’
feelings of fear in relation to the way other people would
look at the patient, and possibly reflect their own difficulties
in dealing with potential problems (Box 1).
The dimension of fear concerning other people’s
reactions and the anticipation that they could be hostile is
seen in the quotation from Sister 7 (Box 1).
Our findings agree with other studies that reported that
the most common feelings expressed by families of burned
patients are guilt, depression, fear, resentment, feelings of
isolation, helplessness, indecisiveness, and intensification
of pre-existing conflicts [7,15]. These fears and other
reactions can hinder participation in caregiving, and
also indicate that relatives are aware of some of the issues
that will have to be dealt with when the patient returns
home.
Table 2
Burned patients according to sex, type of accident, and age
Sex Type of accident Age
0–10 10–21 >21 Total
Female Domestic 4 1 – 5
Occupational – 1 – 1
Attempted suicide – 2 1 3
Male Domestic 6 3 2 11
Occupational – – 5 5
Attempted suicide – – – –
Total 10 7 8 25
Ribeirao Preto, SP, 2000.
3.2. Shame
We observed that feelings of fear and shame are often
expressed in the same context (Box 2).
The experience of having burn sequelae and having to
live with them forever are traumatic to both the patient and
his/her relatives. In view of other people’s curiosity and
reactions, the first strategy patients [21] and their relatives
adopt is trying not to expose the burn scar in any way. That
is, the relative considers the possibility of ‘‘covering up’’ by
using clothes that would hide the burn. When this is not
possible, such as with facial disfigurement, social isolation
becomes a possibility for patients and their relatives [21].
As illustrated in the expression of Mother 1 (Box 2), in
face of the rules that are legitimized by society, the family
and the patients themselves may anticipate reactions from
others before they occur [22].
The situation described by Aunt 31, shown in Box 2,
refers to a child who was wearing an elastic garment,
recommended by health professionals to prevent hyper-
trophic scars, as a resource to hide deformities. In this case,
when informed by the doctor that the garment was no longer
necessary, the relative showed concern. During medical
consultations at the outpatient clinic, this child wore a hood
Table 3
Burned patients according to percentage of total body surface area (TBSA)
and age
%TBSA Age (years)
0–10 10–21 >21 Total
<10 5 2 1 8
10–20 3 3 2 8
20–30 1 2 3 6
30–40 1 – 1 2
>40 – – 1 1
Total 10 7 8 25
Ribeirao Preto, SP, 2000.

L.A. Rossi et al. / Burns 31 (2005) 37–44 41
Box 3. – Relatives’ feelings of guiltM-5: We keep feeling guilty.
F-27: The day before, I had burned ants using alcohol,
and then, the next day, she did the same thing and
burned herself. I was her teacher. I burned this girl;
it’s my fault. I keep thinking, she will never have a
boyfriend.
M-25: My mother tells me that I was not a good
mother (at this moment, the mother’s eyes were
watering).
M-24: I was alone with the three children and he (her
husband) was playing soccer, and now he is blaming
me, he tells me that I didn’t care for the boy as well as
I should have.
Box 1. – Relatives’ feelings of fearM-1: I am only afraid that my neighbors will say
something.
R: Why?
M-1: Because they do, I am afraid they will say some-
thing about her face, that’s all.
W-19: I am afraid, you know, that people will react
when we are at home, because he’s not the same
person, he’s very different now, many things change,
I think that he will be very rebellious.
S-7: I think that I suffer as much as she does. I think
that she is going to suffer a lot, now she will realize
that she won’t be able to get ready to go out the way
she used to. She will feel that other people are
mistreating her.
covering his whole head and face. He would only take it off
when the doctor asked him to do so to evaluate scar healing.
Although it was not our aim to investigate health
professionals’ perspectives during their contacts with
relatives in the group of meetings and at visiting hours, we
did observe that the professionals’ attention was focused on
physical rehabilitation. The professionals working at this
Burns Unit mainly focused on explaining what types of
sequelae could develop and how they could be prevented,
rather than understanding the patients’ and their relatives’
perspectives.
3.3. Guilt
As we can see in examples shown in Box 3, relatives of
burned patients feel guilty because they may somehow have
contributed to the occurrence of the accident or because they
were not able to prevent it. Hence, they also feel ashamed
because they broke a socially legitimized rule by imposing
on others the need to live with a person who does not meet
accepted cultural standards.
Guilt and shame have been regarded as ‘‘guardians of
social rules’’. They are the foundations of the moral order in a
Box 2. – Relatives’ feelings of shameGM-28: When he goes home, a lot of people will go
there to see him. Will he be able to wear a T-shirt?
Because people will see the ugly arm, I thought if he
puts clothes on, that would hide it a little, no one will
ask about it.
A-31: He won’t want to stop wearing it (elastic gar-
ments); he wears it to hide himself. (. . .) He is
ashamed because of his pals from school.
M-1: My God! I feel embarrassed. I stay in all day. I
won’t even go out into the street. Now, my neighbors
go to my house to ask how T’s face and skin are. I feel
that they apparently want the child’s face to be
scarred. They also want to come to the hospital to
visit only because of curiosity, to tell others what T’s
face is like.
world where individuals would not seek goals without an
interest [23]. Therefore, guilt, as a type of sanction, is
associated with individual change in relation to what is
legitimized by society as good. Shame is associated with
society values, which, in the same way, subordinate people to
a set of hierarchies, by means of legitimized norms and
beliefs. This demonstrates that society is concerned with the
maintenance of things as they are and not with changing them
[23].
Guilt involves specific acts, whether performed or not, and
is characterized as a highly individual emotion, whereas
shame involves a feeling of weakness and is characterized as a
social emotion that reaffirms people’s interdependence [24].
3.4. The stigma of burns and loss of control: perceptions of
burned patients’ relatives when facing discharge from
hospital.
The stigma associated with burn sequelae and the
perceptions of loss of control expressed by family members
are shown in Box 4.
Box 4 showed, in the first example, the verbatim
quotation of Mother 1 about the expressions in face of
other people’s reactions. In this case, this mother’s feelings
can influence the child’s treatment by, for instance, avoiding
leaving home or changing daily routines in an attempt to
hide her child. The child is unable to influence this behavior,
as she is only 1 year old. Very often the healed burn has a
repulsive appearance and people tend to avoid the disfigured
person. Such clearly visible changes make a significant
impact on patients and relatives alike.
As we can also see in Box 4, Mother (17) compares the
burn situation to another traumatic experience, that of
having cancer. Cancer has been regarded as something
unfair and unpredictable, and it forces us to face our lack of
control over our own or other people’s deaths [22]. ‘‘Perhaps
most fundamentally, cancer symbolizes our need to make
moral sense of Why me?, which scientific explanations
cannot provide’’ [22]. Cancer has been described as
something cruel, an immoral predator, an enemy, a

L.A. Rossi et al. / Burns 31 (2005) 37–4442
Box 4. – Perceptions of burned patients’ relativeswhen facing discharge from hospitalM-1: I will have to come by bus (to the hospital for a
follow-up). I don’t want to bring her by bus because
everybody will stare at her. Some people are curious,
even on the bus. When we will get on it, everyone will
move away; it’s always the same.
M-17: The world of a burned patient is one known
only by those in it; it must be like the world of cancer.
M-29: I keep asking up to this day: Why my daughter?
There were two girls, and of course, I didn’t want the
other one to get burned, but why my daughter again?
She had already broken her arm. The Bible says that
we may have accidents, but why her?
W-8: It’s disturbing; I didn’t want anything bad to
happen to him any more than I would want it to
happen to myself, especially considering that he’s
my child’s father. I don’t know, I wish it hadn’t
happened, but it has happened, there is no way
out. I will help him with whatever he needs, but I
just can’t accept it. Because, you see, there were four
people, but only he got hurt like this. Up to this day, I
still can’t believe that this has happened. I don’t
know – I don’t have words to say, because seeing
your husband like this and not being able to do
anything is sad.
F-26: I had to think my daughter had died in order to
accept the one who is there. It is difficult to hear your
child ask for a new hand as a Christmas gift. What
could I tell her? She thought that, under the burned
skin, there was a new skin, that she could remove the
scars as if they were a mask. Later, with the results of
the surgeries, she began to realize that it wasn’t like
that, and she is angry.
M-15: God wanted it like this; He knows what He
does. He is the one who knows it all, we don’t.
S-18: Only God knows what to do. What has he done
to deserve this?
mysterious disease that involves the whole self and is
associated with hopelessness and fear of death [25]. Similar
to cancer, burns mean a loss of something; they mean the
death of a person who used to have a certain appearance and
who, in a few seconds, becomes another, disfigured person,
as stated by Father 26. The lack of control makes us feel
vulnerable. Thus, relatives want to reject the situation and
change it, as illustrated by the examples of verbatim
quotations expressed by Mother 29 and Wife 8.
Although they are not regarded as a disease, burn
outcomes are stigmatizing. Disfiguring deformities, like
bizarre actions stemming from mental illnesses, are
stigmatizing because they break cultural conventions
concerning what is acceptable in terms of appearance and
behavior, while invoking other cultural categories of what is
ugly, feared, alien or inhuman [22]. A stigmatized individual
is disqualified for full social acceptance. S/he is a person
who exhibits a weakness, a defect, or a deficiency in the view
of society [26]. Therefore, fear arises of losing one’s job or
of being mistreated, i.e., of not being treated with respect
and dignity.
A burn mark or that of another type of trauma that calls
attention due to the bearer’s difference in relation to other
members of society are sources of discrimination and pre-
judice as, in burn sequelae, inequality means inferiority.
Standing out in a negative way means being disadvantaged
[27].
Stigma also carries a religious meaning [21]. A burn mark
can be considered something that labels a person as a sinner
and wicked, and that the difference or aberration is somehow
justified, i.e., if something bad happens to someone it is
because s/he deserves punishment. In the relatives’
accounts, there is a reason for accident occurrence that is
attributed to God’s decision.
Religion, which is here understood as a system of
symbolic meanings, provides humans with a basis for the
interpretation of facts in situations when reality seems to
confront them with their human limits for coping with pain
and suffering, lack of moral orientation, or the unexplainable
[28]. Then, the question Why me? arises. Parents of burned
people ask questions such as these and others: Why my child?
Why now? [29]. The relatives in our study also asked these
questions. The answers are religious or metaphysical. Some
relatives may interpret the accident as a punishment or
warning from God, as a test, or as a way of bringing the
family closer together [29].
Suffering is closely related to the burn stigma. To
Kleinman [22] ‘‘in stigmatized disorders, the stigma can
begin with the societal reaction to the condition: that is to
say, a person is labeled, shunned, derided, disconfirmed, and
degraded by those around him/her, though usually not by the
immediate family’’.
We can also see in Box 4 the perspective of Father 26,
who expresses difficulties in dealing with his daughter. In
this situation, it was observed that the accident made family
relationships even more difficult. Father 26 claimed to have
accepted his 12-year-old daughter’s physical changes, but at
the same time, he stated that he had to think his daughter had
‘‘died’’ so that he could let this new disfigured child be born.
He said that due to the fact that he could not cope with the
problem on a daily basis, he moved away out of the home.
He later returned, but reported that he intended to move
away again. Problems in family relationships that were
already fragile prior to the accident may be aggravated at a
time when the burn victim most needs support.
The disease may be located on one individual’s tissues, but
the experience of having it will embody the person’s whole
social circle, family, friends, other close people, as well as his/
her employment [22]. The feelings of fear and demoralization
are rarely restricted to the patient himself/herself.
When the patient realizes that permanent body changes
have occurred, s/he reacts with fear, horror and anger, and so
do other people in his/her family and social circles [29].
Therefore, when a family member is affected, as in the case
of a burn injury, changes will occur in the organization and

L.A. Rossi et al. / Burns 31 (2005) 37–44 43
functioning of the family system as a whole [8]. The burn
affects the whole family and ignoring this fact may seriously
affect the patient’s reintegration to his/her family and
community. Family problems must be anticipated and taken
into account by health professionals [30]. To that end, health
professionals must understand the family members’ and the
patients’ perspectives.
The relatives reported other feelings and attitudes
stemming from the fear of facing the social world, such
as, sadness, anger, denial, resignation, and/or anxiety. These
feelings and attitudes are related to the burn stigma and loss
of control. They may further complicate family participation
in caregiving and the patient’s relationships when returning
home.
Such feelings may either not be clearly expressed by
relatives and patients or may be unconscious. Thus, they may
remain unnoticed by health professionals who are not
experienced in the care of patients in that situation. Instead,
these professionals may focus on aspects of care that are very
often not shared by patients and their relatives, such as, the
recovery of structure and function. Even when health
professionals focus on the recovery of physical appearance,
sometimes they do it based on perspectives that are inherent
to professional health-care systems, not on what is important
for patients and their families [22]. For instance, we observed
that when patients and relatives were informed that the
recovery of an injury or the result of a graft was ‘‘excellent’’,
they (patients and relatives) would frequently expect that it
could be better from their perspectives. Consequently, they
thought the result is not good enough. A ‘‘good result’’ would
be to recover the condition that existed prior to the trauma.
Unfortunately, these views are stimulated by science fiction
miracles about plastic surgeries, and some patients seek
imagined outcomes at other specialized centers, hoping that
their present situations are not definitive.
3.5. Final considerations
Although this investigation is limited by the feature of its
sample, the findings help to understand the relatives of
burned patients’ attitudes and feelings as they face the
prospective of hospital discharge.
Their descriptions reveal the family’s feelings and
attitudes in face of other people’s reactions, and in face
of the patient’s own reactions in the context of possible
changes in their social roles. Relatives feel fear and shame
when patients resume social living, because they are
imposing on others a co-existence with people who no
longer meet the accepted patterns. In view of this situation,
the relatives think about the possibility of trying not to
expose the sequelae, and change daily routines in an attempt
to hide the patient. The relatives also asked about the reasons
for the accident and some of them interpreted the accident as
a punishment.
The family’s role in delivering care to a burned person is
very important, not only with respect to the technical aspects
involved in caregiving, but particularly with respect to
psychosocial aspects. Working with the family to promote
cohesion, reduces conflict, and increases stability [11].
However, in order to act effectively, relatives need to be
given support. Such support may consist simply of the
opportunity to be heard and to express the fears related to
returning to their social world, now changed by having a
loved one who has been burned.
It is important to conduct other studies focusing on
cultural meanings of burns attributed by health professionals
and by burned patients and their relatives, as well as on the
family’s feelings and ways of coping.
Acknowledgements
We are grateful to the Conselho Nacional de Desenvol-
vimento Cientifico e Tecnologico (CNPq), Brazil, for
financial support. We thank Prof. Virginia Hayes, School
of Nursing, University of Victoria, Vancouver, Canada, for
her valuable collaboration.
References
[1] Shenkman B, Stechmiller J. Patient and family perception of projected
functioning after discharge from a burn unit. Heart Lung 1987;16(5):
490–6.
[2] Avni J. The severe burns. Adv Psychosomatic Med 1980;10:
57–77.
[3] Patterson DR, Everett JJ, Bombardier CH, Questad KA, Lee VK,
Marvin JA. Psychological effects of severe burn injuries. Psychol Bull
1993;113(2):362–78.
[4] Steiner H, Clark Jr WR. Psychiatric complications of burned adults: a
classification. J Trauma 1977;17(2):134–43.
[5] Adcok RJ, Boeve SA, Patterson DR. Psychologic and emotional
recovery. In: Carrougher GJ, editor. Burn Care and Therapy, Cap.
13. St. Louis: Mosby, 1998. p. 329–57.
[6] Watkins P, Cook L, May R, Still Jr JM, Lutterman A, Purvis J.
Postburn psychologic adaptation of family members of patients with
burns. J Burn Care Rehabil 1996;17:78–92.
[7] Bowden M, Feller I. Family reaction to a severe burn. Am J Nurs
1973;73(2):317–9.
[8] Patterson JM. Promoting resilience in families experiencing stress.
Pediatr Clin North Am 1995;42(1):47–63.
[9] Friedemann ML. The concept of family nursing. J Adv Nurs 1989;
14:211–6.
[10] Blakeney P, Herndon D, Desai M, Beard S, Wales-Seales P. Long-term
psychosocial adjustment following burn injury. J Burn Care Rehabil
1988;9:661–5.
[11] Davidson TN, Bowden ML, Tholen D, James MH, Feller I. Social
support and post-burn adjustment. Arch Phys Med Rehabil 1981;
62(6):274–8.
[12] LeDoux J, Meyer III WJ, Blakeney PE, Herndon DN. Relationship
between parental emotional states family environment and the beha-
vioural adjustment of pediatric burn survivors. Burns 1998;24(5):
425–32.
[13] Partridge J, Robinson E. Psychological and social aspects of burns.
Burns 1995;21(6):453–7.
[14] Thompson R, Boyle D, Teel C, Wambach K, Cramer A. A qualitative
analyses of family member needs and concerns in the population of
patients with burns. J Burn Care Rehabil 1999;20(6):487–96.

L.A. Rossi et al. / Burns 31 (2005) 37–4444
[15] Cahners SS. Group meetings benefit families of burned children.
Scand J Plast Reconstr Surg 1979;3(1):169–71.
[16] Cahners SS, Bernstein NR. Rehabilitating families with burned chil-
dren. Scand J Plast Reconstr Surg 1979;13(1):173–5.
[17] Barnes A, Budd L. Family-centred burn care. Can Nurse 1999;95(6):
24–7.
[18] McHugh ML, Dimitroff K, Davis ND. Family support group in a burn
unit. Am J Nurs 1979;79(12):2148–50.
[19] Rossi LA. O processo de cuidar da pessoa que sofreu queimaduras:
significado cultural atirbuıdo por familiares (The process of caring for
burned patients: cultural significance attributed by relatives). Rev Esc
Enferm USP 2001;35(4):335–6.
[20] Miles MB, Huberman AM. Qualitative data analysis: an expanded
sourcebook, 2nd ed. London: Sage Publications; 1994.
[21] Bergamasco EC, Rossi LA, Amancio ACG, Carvalho EC. The body
image of patients with burn sequelae: evaluation through the critical
incident technique. Burns 2002;28(1):23–8.
[22] Kleinman A. The Illness Narratives: Suffering, Healing and the
Human Condition. Los Angeles: Basic Books; 1988.
[23] Rosaldo MZ. Toward an anthropology of self and feeling. In:
Shweder RA, Levine RA, editors. Culture theory: essays on mind,
self, and emotion. New York: Cambridge University Press; 1997. p.
137–57.
[24] Lynd HM. On Shame and the Search for Identity. New York: Science
Editions; 1961.
[25] Lupnton D. Medicine as a Culture: Illness, Disease and Body in
Western Societies. London: Sage Publications Ltd.; 2000.
[26] Goffman ES. Stigma Notes on the Management of Spoiled Identity.
New Jersey: Prentice Hall; 1963.
[27] Montanari PMNS. Jovens e deficiencia: comportamento e corpos
desviantes (Youth and deficiency: conduct and defect corps). In:
Schor N, Mota M do SFT, Branco VC, editors. Cadernos Juventude,
Saude e Desenvolvimento. Brasılia, Brasil: Ministerio da Saude,
1999. pp. 97–108.
[28] Geertz C. The Interpretation of Cultures. New York: Basic Books;
1973.
[29] Knudson-Cooper MS. Adjustment to visible stigma: the case of the
severely burned. Soc Sci Med 1981;15B:31–44.
[30] Blumenfield M, Schoeps M. Reintegrating the healed burned adult into
society: psychological problems and solutions. Clin Plast Surg 1992;
9:599–605.





























