Embed Size (px)
Citation preview

Twenty-four–Hour Blood Pressure and MRI as Predictive Factorsfor Different Outcomes in Patients With Lacunar Infarct
Y. Yamamoto, PhD; I. Akiguchi, PhD; K. Oiwa, PhD; M. Hayashi, MD; T. Kasai, MD; K. Ozasa, PhD
Background and Purpose—A long-term follow-up study was conducted in patients with lacunar infarct to assess how24-hour blood pressure monitoring values and MRI findings, in particular lacunar infarcts and diffuse white matterlesions, can predict subsequent development of dementia and vascular events, which include cerebrovascular andcardiovascular events.
Methods—One hundred seventy-seven patients were tracked for a mean of 8.9 years of follow-up. Documented eventscomprise the development of dementia and the occurrence of vascular events. The predictors for developing dementiaand vascular events were separately evaluated by Cox proportional hazards analysis.
Results—Twenty-six patients developed dementia (0.17/100 patient-years). Male sex (relative risk [RR], 4.2; 95% CI, 1.2to 14.7), cognitive impairment (RR, 3.0; 95% CI, 1.0 to 8.5), confluent DWML (moderate: RR, 7.1; 95% CI, 1.6 to 31.5;severe: RR, 35.8; 95% CI, 7.2 to 177.3), and nondipping status (RR, 7.1; 95% CI, 2.2 to 22.0) were independentpredictors for dementia. Forty-six patients suffered from vascular events (3.11/100 patient-years). Diabetes mellitus(RR, 5.7; 95% CI, 2.7 to 11.9), multiple lacunae (moderate: RR, 6.4; 95% CI, 2.5 to 15.8; severe: RR, 8.5; 95% CI, 3.1to 23.3), and high 24-hour systolic blood pressure (�145 mm Hg versus �130 mm Hg) (RR, 10.3; 95% CI, 1.3 to 81.3)were independent predictors for vascular events.
Conclusions—Predictors for developing dementia and vascular events appear to differ. Male sex, confluent diffuse whitematter lesions, and nondipping status were independent predictors for subsequent development of dementia, whilediabetes mellitus, multiple lacunae, and high 24-hour systolic blood pressure were independent predictors for vascularevents. (Stroke. 2002;33:297-305.)
Key Words: blood pressure monitoring, ambulatory � dementia, vascular � lacunar infarction � white matter
Lacunar infarcts are small, deep infarcts caused by theobstruction of small penetrating arteries.1 Despite the
fact that lacunar infarcts account for only 15% to 20% of allcerebral infarcts in Western countries,2–4 they probably con-stitute up to 30% to 40% of all cerebral infarcts in Japan.5,6
Compared with other stroke subgroups, lacunar infarcts areassociated with low early-case fatality and recurrent strokerates.4,6–9 Nonetheless, a certain percentage of vascular de-mentia that is due to small-vessel disease is believed to stemfrom the symptomatic lacunar infarct cohort.10,11 Althoughseveral studies have evaluated the prognosis of lacunarinfarcts, very few studies have thoroughly analyzed long-termoutcomes of lacunar infarction, which includes the risk of notonly cerebrovascular and cardiovascular events but also thedevelopment of dementia.6
Hypertension, on the other hand, has been generallythought to be the most common cause of lacunar infarcts,although there remains much controversy over the risk factorsfor lacunar infarcts.12 Since the introduction of ambulatoryblood pressure monitoring (ABPM) devices, it has been
consistently reported that target organ damage and cardiovas-cular morbidity and mortality are more closely correlatedwith ambulatory blood pressure (ABP) than casual bloodpressure (BP).13,14 Moreover, a nondipping status, that is, astate whereby patients exhibit either an absence of or areduced nocturnal BP dip, was reported to correlate withmore advanced target organ damage and worsened prognosisthan patients who maintained dipping status.15 Accordingly,ABP values are of prognostic value for the prediction ofsubsequent morbid events in patients with essential hyperten-sion.15–17 The prognostic value of ABP for cerebrovasculardisease, however, has never been investigated, thus prompt-ing us to pose the question of how ABP could potentiallycontribute to the prediction of long-term outcomes in patientswith lacunar infarct.
In addition, it has also been previously noted that patientswith silent lacunar infarcts18 and diffuse white matter lesions(DWML),6,19,20 as detected by MRI, might potentially be atgreater risk for stroke recurrence or death. We thus conductedthis prospective study to elucidate how the combination of
Received February 28, 2001; final revision received September 4, 2001; accepted September 21, 2001.From the Department of Neurology, Kyoto Second Red Cross Hospital (Y.Y., K. Oiwa, T.K., M.H.); Department of Neurology, Kyoto University
Hospital (I.A.); and Department of Social Medicine and Cultural Sciences, Kyoto Prefectural University of Medicine (K. Ozasa) (Japan).Correspondence to Y. Yamamoto, PhD, Department of Neurology, Kyoto Second Red Cross Hospital, 355-5 Haruobicho Kamigyoku, Kyoto 602,
Japan. E-mail [email protected]© 2002 American Heart Association, Inc.
Stroke is available at http://www.strokeaha.org
297
Case Report
by guest on July 14, 2015http://stroke.ahajournals.org/Downloaded from by guest on July 14, 2015http://stroke.ahajournals.org/Downloaded from by guest on July 14, 2015http://stroke.ahajournals.org/Downloaded from

ABP values and MRI findings can help to predict thelong-term outcome of patients with lacunar infarct.
Subjects and MethodsPatient SelectionBetween January 1987 and December 1991, 623 patients wereconsecutively admitted to the Department of Neurology at the KyotoSecond Red Cross Hospital in Japan for first-ever symptomaticischemic stroke. This group included 209 patients with symptomaticlacunar infarcts. Symptomatic lacunar infarct patients were definedas those patients who showed an acute onset of a focal neurologicaldeficit lasting �24 hours that was consistent with a lacunar syn-drome.1 Patients who showed cortical infarcts or subcortical infarctsin which diameters were �15 mm on MRI were excluded. Fivepatients who were diagnosed with dementia, 2 patients with severerenal failure, and 7 patients with lower basilar branch syndrome wereexcluded, leaving 195 patients. Of these 195 patients, 177 patientsunderwent both MRI and ABPM, without prior administration ofantihypertensive agents for �4 weeks. Subsequently, either ouroutpatient clinic or family physicians tracked the 177 patients. Allpatients consented to participate in this study.
Conventional Risk FactorsHypertension was defined as systolic BP (SBP) �140 mm Hg and/ordiastolic BP (DBP) �90 mm Hg measured with the patient in asitting position on at least 2 different occasions with no administra-tion of antihypertensive agents for 2 weeks after ictus or previous useof antihypertensive agents. Diabetes mellitus was defined as fastingglucose level �140 mg/dL or use of antidiabetic medication.Dyslipidemia was defined as fasting total cholesterol level �220mg/dL and/or fasting triglyceride level �200 mg/dL without admin-istration of any antihyperlipidemic agents. Cigarette smoking wasdefined as regularly smoking at the time of stroke. Complications ofcardiac disease, including old myocardial infarctions, angina pecto-ris, congestive heart failure, atrial fibrillation, and cardiomyopathy,were also identified.
Magnetic Resonance ImagingMRI scans were performed with the use of 1.5-T superconductingmagnets (Shimazu, SMT 150X). MRIs were performed from 5 to 14days after ictus. Transverse T2-weighted scans (repetition time, 2500ms; echo time, 90 ms) and proton density images (repetition time,2500 ms; echo time, 20 ms) were obtained at a slice thickness of8 mm. Lacunae and DWML were then evaluated against baselineMRI. Lacunae were defined as penetrating artery occlusions 3 to15 mm in diameter in horizontal sections with high intensity on bothT2-weighted and proton density images. Lacunae were locatedwithin the basal ganglia, thalamus, internal capsule, corona radiata,and pons. DWML were defined as diffuse hyperintensities that werelocated in the subcortical and periventricular white matter withT2-weighted images and proton density images. For the baselineMRI, the number of lacunae was first counted and then graded asfollows: grade 0, absent; grade 1, 1 to 2 lacunae; grade 2, 3 to 5lacunae; and grade 3, 6 lacunae. DWML were defined and gradedaccording to the classification of Schmidt et al21: grade 0, absent;grade 1, punctuate; grade 2, becoming confluent; and grade 3,confluent. Hyperintense periventricular caps and smooth halos werenot counted as DWML. The baseline MRIs were evaluated by 2authors (Y.Y. and I.A.), who were blinded to both the BP data andthe results.
ABPM and Casual BPThe 24-hour BP data were recorded with a portable automaticrecorder (ABPM-630, Nippon Corin Co) at 30-minute intervals, overa 24-hour period from 1 PM to 1 PM the following day. ABPM wasperformed from 14 to 30 days after ictus without administration ofantihypertensive agents. Average values were calculated as follows.The SBP and DBP were averaged over successive 30-minuteintervals throughout the 24-hour period. The mean daytime (6 AM to
10 PM) and nighttime (10:30 PM to 5:30 AM) values were alsocalculated.
The degree of the nocturnal BP dip (nocturnal dip) was calculatedas follows: (mean daytime values�mean nighttime values)/meandaytime values. Nondippers were arbitrarily defined as essentialhypertensive patients who did not exhibit a �10% nocturnal dip inSBP.13 Because a large number of lacunar infarct patients would beclassified as nondippers on the basis of such criteria, we classifiedpatients who did not exhibit a �5% nocturnal dip in SBP asnondippers; the remaining subjects were classified as dippers.According to recent guidelines,22,23 patients were divided into tertilesof ABP values for daytime SBP: 1, low tertile �135 mm Hg; 2,middle tertile 135 to 150 mm Hg; and 3, high tertile �150 mm Hg;for daytime DBP: 1, low tertile �80 mm Hg; 2, middle tertile 80 to90 mm Hg; and 3, high tertile �90 mm Hg; for nighttime SBP: 1,low tertile �120 mm Hg; 2, middle tertile 120 to 140 mm Hg; and 3,high tertile �140 mm Hg; for nighttime DBP: 1, low tertile�70 mm Hg; 2, middle tertile 70 to 80 mm Hg; and 3, high tertile�80 mm Hg; for 24-hour average SBP: 1, low tertile �130 mm Hg;2, middle tertile 130 to 145 mm Hg; and 3, high tertile �145 mm Hg;and for 24-hour average DBP: 1, low tertile �75 mm Hg; 2, middletertile 75 to 85 mm Hg; and 3, high tertile �85 mm Hg.
BP was also measured with the patient in a sitting position bystandard mercury sphygmomanometers in the morning when ABPMwas performed. This was designated the casual BP. According to theWorld Health Organization/International Society of Hypertensionguidelines, patients were divided into 3 tertiles of casual BP valuesfor SBP: 1, low tertile �160 mm Hg; 2, middle tertile 160 to180 mm Hg; and 3, high tertile �180 mm Hg; and for DBP: 1, lowtertile �100 mm Hg; 2, middle tertile 100 to 110 mm Hg; and 3, hightertile �110 mm Hg.
Dementia ScaleAt approximately the time when ABPM was performed, the overallseverity of dementia was evaluated with the Clinical DementiaRating Scale (CDR),24 with information from the neurological,neuropsychological, and functional examinations. The cognitiveability of all patients was also evaluated with Hasegawa’s DementiaRating Scale Revised (HDSR).25 This evaluation scores cognitiveimpairment via 5 subtests that measure orientation, general informa-tion, calculation, memory recall, and memorization. The maximumscore is 30 points, with low scores reflecting more extensivecognitive impairment. This test battery is widely used in Japan toevaluate cognitive impairment.10,18 The patients were diagnosed withdementia if either the CDR score was �1 or the score on the HDSRwas �20 and the state of dementia met the criteria of the Diagnosticand Statistical Manual of Mental Disorders, Revised Third Edition.26
Cognitive impairment was defined as CDR score of 0.5 or HDSRscore of 21 to 26. Patients who could be diagnosed with dementiaafter a stroke recurrence with large cortical infarcts were notevaluated as dementia developed.
Patient Follow-UpAfter the patients were discharged from the hospital, approximatelyhalf of the patients were followed on a monthly basis in ouroutpatient clinic; the remaining patients were tracked by their familyphysicians. Approximately 20% of those tracked by family physi-cians visited our clinic once a year for regular examination, includingMRI and/or ultrasonography. When patients were referred to familyphysicians, the physicians were informed regarding patient charac-teristics, study protocol, and the method of evaluating dementia withthe use of the CDR. The outcome of patients followed monthly in ouroutpatient clinic or readmitted to our hospital for subsequent strokereoccurrence or cardiovascular events was identified directly byattending physicians. Patients who were tracked by their familyphysicians were intermittently reviewed over the years to recordclinic BP, drug therapy, and the occurrence of cerebrovascular andcardiovascular events or the development of dementia. On occur-rence of new events, family physicians and patients or familymembers were requested to notify our department. Finally, weperformed telephone interviews directly for all patients or their
298 Stroke January 2002
by guest on July 14, 2015http://stroke.ahajournals.org/Downloaded from

families to confirm final outcomes on December 1999. Documentedevents consisted of development of dementia and the occurrence ofcerebrovascular and cardiovascular events. Cerebrovascular andcardiovascular events were classified as vascular events. Cerebro-vascular and cardiovascular deaths, which were classified as vasculardeaths, and nonvascular death, which was defined as death due tocauses other than cardiovascular and/or cerebrovascular diseases,such as cancer, pneumonia, or other unrelated diseases, were alsoidentified. When patients were suspected to exhibit cognitive declineon an office visit, evaluation with CDR and HDSR was performed.Newly developed dementia was diagnosed according to the afore-mentioned definition. Recurrent stroke attack was diagnosed onrapid onset of a localized neurological deficit. Cardiovascular eventsincluded myocardial infarct, angina pectoris, ruptured aneurysm, andprogressive heart failure. For patients followed in our outpatientclinic or by their family physicians, antihypertensive treatment wasprovided on the basis of office BP levels, with �160/95 mm Hg asthe goal for control. All patients were treated with 82 to 164 mg ofacetylsalicylic acid or 200 mg of ticlopidine.
Statistical AnalysisEvent rates are presented as the number of events per 100 patient-years based on the ratio of the observed number of events to the totalnumber of patient-years of exposure. The study population wasanalyzed with 2 different models. In the first model, all patients weredichotomized into 2 groups: those with and without subsequentdementia. In the second model, all patients were dichotomized into2 groups: those with and without subsequent vascular events. Thefollow-up period was defined as the time interval between the24-hour BP monitoring and either the last follow-up in uncompli-cated patients or the development of the first morbid event in theother groups. Different morbid events were separately counted forthe same person, but only the first event was considered whenvascular events occurred more than twice. In the 2 different models,variables were initially compared between 2 groups with and withoutevents. Continuous variables were expressed as mean�SD, andcategorized variables were given as the percentage of patients soaffected. A comparison of clinical variables between the 2 groupswas performed with a �2 test; BP data were analyzed with Student’st test. In both models, the effect of predictive factors on survival wasevaluated by Cox proportional hazards analysis. Predictive factorsincluded in the Cox proportional hazards analysis were age (�50sversus 60s, �50s versus 70s, �50s versus 80s), sex (male andfemale), conventional risk factors (yes or no), cognitive impairment(yes or no), MRI findings (grade 0 to 1 versus grade 2 and grade 0to 1 versus grade 3), and ABPM values, including daytime, night-time, and 24-hour average BP (low tertile versus middle tertile andlow tertile versus high tertile), nocturnal BP dip (dippers versusnondippers), and casual BP values (low tertile versus middle tertileand low tertile versus high tertile). Complications of cardiac diseasewere not included as a predictive factor because the number wassmall. Age and sex were simultaneously analyzed. Age- and sex-adjusted relative risks (RRs) and 95% CIs were calculated forindividual factors by a Cox proportional hazards analysis with theuse of Stat-View 5.0. Probability values �0.05 were consideredsignificant. Predictive factors found to be significant by age- andsex-adjusted univariate analysis were examined with multivariateanalysis. Among various ABP values such as daytime BP, nighttimeBP, and 24-hour BP values, only the ABP value exhibiting highestRR by age- and sex-adjusted univariate analysis was used formultivariate Cox proportional hazards analysis.
ResultsGeneral DataThe study population consisted of 177 patients. There were110 men and 67 women aged 69.1�8.6 years (mean�SD),ranging from 47 to 86 years. Lacunar syndrome included puremotor hemiparesis (n�102), sensorimotor stroke (n�39),pure sensory stroke (n�18), dysarthria–clumsy hand syn-
drome (n�12), and miscellaneous (pure dysarthria; n�6).The study population was analyzed with 2 different out-comes, which include the development of dementia and theoccurrence of vascular events. The demographics, conven-tional risk factors, MRI findings, number of cognitive impair-ments, casual BP values, and ABP values at baseline aredisplayed in Table 1 for the first model and in Table 2 for thesecond model.
Model 1: Newly Developed DementiaTwenty-six patients developed dementia during a meanfollow-up period of 8.7�3.0 years (0.17/100 patient-years).The average CDR score for these 26 patients was 0.27�0.15at baseline and 1.73�0.4 at the time of diagnosis of dementia.Seventeen patients were diagnosed with dementia at ouroutpatient clinic. The HDSR scores for these 17 patientsranged from 26.8�3.4 at baseline to 16.4�3.4 at the time ofdiagnosis. These 17 patients also developed lacunae andDWML on the basis of follow-up MRI, suggesting that mostpatients could be classified with vascular dementia. Sixpatients showed evidence of cerebrovascular events, 3 died ofcardiovascular events, and 4 died of nonvascular causes.
Table 3 presents the RRs and 95% CIs for developingdementia by Cox proportional hazards analysis. Developingdementia was significantly associated with male sex, cogni-tive impairment, confluent DWML (grade 0 to 1 versus grade2 and grade 0 to 1 versus grade 3), and nondipping status bymultivariate analysis.
Model 2: Vascular EventsForty-six patients suffered from vascular events during amean follow-up period of 8.5�3.2 years (3.11/100 patient-years). Vascular events consisted of 35 cerebrovascularevents and 11 cardiovascular events. Cerebrovascular eventsincluded 19 patients with lacunar infarcts, 5 patients withcerebral cortical infarcts, 2 patients with vertebrobasilarartery occlusive disease, 3 patients with cerebral hemor-rhages, and 6 patients with unidentified acute stroke. Twenty-eight patients were identified on readmission to our hospital.Eleven patients died of cerebrovascular events. Cardiovascu-lar events included myocardial infarction in 6, angina pectorisin 2, congestive heart failure in 1, ruptured aneurysm in 1, andunidentified acute heart disease in 1 patient. Seven patientswere identified on readmission to our hospital. Eight patientsdied of cardiovascular events.
Table 4 presents the RRs and 95% CIs for developingdementia by Cox proportional hazards analysis. Because24-hour SBP value exhibited the highest RR by age- andsex-adjusted univariate analysis, it was used for multivariateCox proportional hazards analysis. Diabetes mellitus, multi-ple lacunae (grade 0 to 1 versus grade 2 and grade 0 to 1versus grade 3), and 24-hour SBP (low tertile versus hightertile) emerged as independent predictors for vascular eventsafter multivariate analysis.
Nonvascular DeathFifteen patients died of nonvascular causes, which included 4patients who died of neoplastic diseases, 5 patients who diedof pneumonia, 1 patient who died of asphyxia, and 5 patients
Yamamoto et al Predictive Factors for Different Outcomes in Lacunar Infarct Patients 299
by guest on July 14, 2015http://stroke.ahajournals.org/Downloaded from
who died of unknown causes. Four patients developed de-mentia, but no patients suffered from vascular events.
DiscussionThe present study identified different sets of predictivefactors for different outcomes. It is of particular note thatpredictors for vascular events and dementia appear to differ.Diabetes mellitus, multiple lacunae, and high ambulatorySBP values were independent predictors for vascular events,while nondipping status, the highest degree of multiplelacunae, and confluent DWML were independently associ-ated with the development of dementia.
The highest degree of 24-hour SBP exhibited higher RRfor vascular events than casual BP, daytime and nighttimeSBP, and diastolic ABP. Several studies have assessed theprognostic value of ABPM in essential hypertension.14–17,27,28
The present study is in agreement with these results, showingthat higher ABP values at baseline can predict a higher rate ofoccurrence of vascular events. Our results are also consistentwith these reports in that SBP appears to yield greaterprognostic information than DBP.16,17 It is likely that aconsiderable proportion of treated patients have not achievedtarget BP levels, despite BP control during the follow-upperiod.29,30
In contrast, ABP values were not revealed to be a signifi-cant predictor for subsequent development of dementia, evenby univariate analysis. The relationship between BP andcognitive function is controversial in the elderly.31 Someresearchers found high BP to be related to dementia,32–34
while another researcher reported low BP to be linked with a
higher prevalence of dementia in the elderly.35 Skoog et al36
demonstrated that a previously elevated BP tended to declineover time in patients who subsequently developed dementia.We have also recently reported that patients with lacunarinfarct who subsequently develop both lacunae and DWML,together with a cognitive decline, exhibit a decline in theaverage 24-hour BP over the course of the disease.37,38 Inconsideration of such results, it might be postulated that aninitially elevated BP may lead to multiple lacunae andDWML, followed by a gradual decline in cognitive abilitiesthat occurs in conjunction with a decline in BP. It thusremains possible that before patients’ entry into the presentstudy, BP values may have already begun to decline inpatients who subsequently developed dementia. The possibil-ity that vascular dementia progressed, regardless of BP level,is also not excluded.
There are increasing numbers of studies on ABPM inpatients with lacunar infarct. The majority of previous studiesusing 24-hour BP measurements have demonstrated thatnondipping status correlates with the occurrence and theextent of DWML or lacunar infarct.38–43 We reported byprospective study that the development of symptomatic orasymptomatic lacunar infarct and DWML was associatedwith a reduced nocturnal BP dip in patients with a history oflacunar infarct.39,44 In contrast, other studies suggested thatexcessive nighttime BP dip correlated with extensive DWMLand lacunar infarct.45–47 On the other hand, short-term BPvariability was reported as a risk factor for small-vesseldisease or Binswanger’s disease.39,48
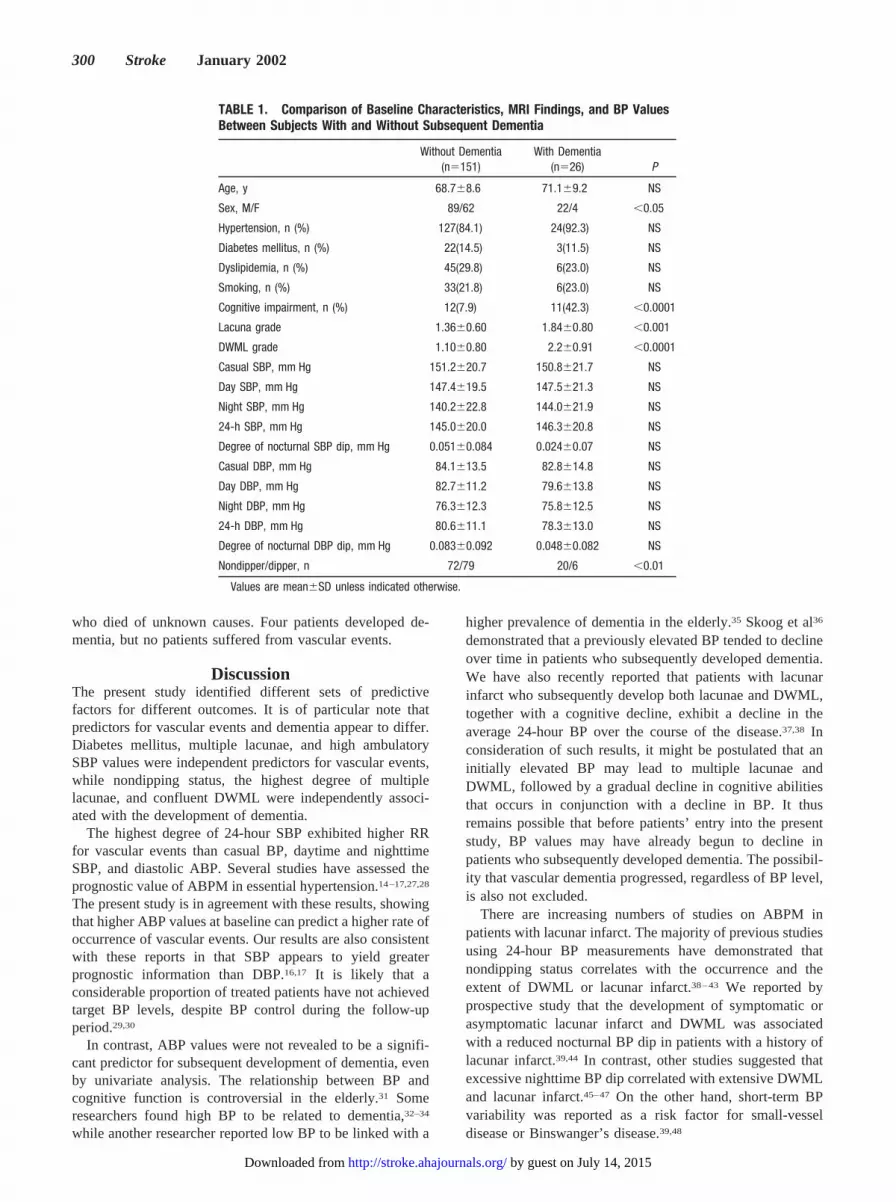
TABLE 1. Comparison of Baseline Characteristics, MRI Findings, and BP ValuesBetween Subjects With and Without Subsequent Dementia
Without Dementia(n�151)
With Dementia(n�26) P
Age, y 68.7�8.6 71.1�9.2 NS
Sex, M/F 89/62 22/4 �0.05
Hypertension, n (%) 127(84.1) 24(92.3) NS
Diabetes mellitus, n (%) 22(14.5) 3(11.5) NS
Dyslipidemia, n (%) 45(29.8) 6(23.0) NS
Smoking, n (%) 33(21.8) 6(23.0) NS
Cognitive impairment, n (%) 12(7.9) 11(42.3) �0.0001
Lacuna grade 1.36�0.60 1.84�0.80 �0.001
DWML grade 1.10�0.80 2.2�0.91 �0.0001
Casual SBP, mm Hg 151.2�20.7 150.8�21.7 NS
Day SBP, mm Hg 147.4�19.5 147.5�21.3 NS
Night SBP, mm Hg 140.2�22.8 144.0�21.9 NS
24-h SBP, mm Hg 145.0�20.0 146.3�20.8 NS
Degree of nocturnal SBP dip, mm Hg 0.051�0.084 0.024�0.07 NS
Casual DBP, mm Hg 84.1�13.5 82.8�14.8 NS
Day DBP, mm Hg 82.7�11.2 79.6�13.8 NS
Night DBP, mm Hg 76.3�12.3 75.8�12.5 NS
24-h DBP, mm Hg 80.6�11.1 78.3�13.0 NS
Degree of nocturnal DBP dip, mm Hg 0.083�0.092 0.048�0.082 NS
Nondipper/dipper, n 72/79 20/6 �0.01
Values are mean�SD unless indicated otherwise.
300 Stroke January 2002
by guest on July 14, 2015http://stroke.ahajournals.org/Downloaded from

Nondipping status has been suggested to be a potentialpredictor of cerebrovascular and cardiovascular morbidity andmortality in hypertensive patients.14–17,27,28 In the present study,however, nondipping status was not shown to be independentmarker of the risk for vascular events, although it was revealedto be significant by univariate analysis. It was found, however,that nondipping status independently predicted the subsequentdevelopment of dementia after adjustment for multiple lacunaeand DWML. Nondipping status was reported to be associatedwith altered autonomic regulation44,49 and sodium-sensitive–type hypertension.50,51 It is conceivable that altered autonomicregulation can impair neurogenic control of cerebral circulationover time, resulting in a chronic ischemic state in the brain.Whether sodium-sensitive–type hypertension can facilitate thedevelopment of vascular dementia due to small-artery diseaseshould also be investigated.44
The presence of multiple lacunae was found to be a significantpredictor for vascular events, while confluent DWML was foundto be an independent predictor for subsequent development ofdementia. Multiple lacunae appeared to supersede the impor-tance of confluent DWML for the risk for vascular events; on theother hand, DWML appeared to supersede multiple lacunae inthe progression of dementia. Uehara et al52 reported that silentlacunar infarcts in the basal ganglia were associated withgeneralized atherosclerosis, including carotid and coronary ar-tery disease, while silent infarcts in subcortical white matterwere not associated with such a disease process. Previousreports53,54 have also demonstrated that silent lacunae occur in
conjunction with a background of atherosclerosis. Consequently,patients with multiple lacunae appear to have both disseminatedarteriolosclerosis, which may be caused by longstanding hyper-tension,1 and generalized atherosclerosis. Such patients are thusconsidered to be prone to recurrent stroke. Kobayashi et al18
conducted a prospective study demonstrating that althoughsubcortical silent brain infarcts were identified as an independentpredictor of subsequent symptomatic brain infarcts or brainhemorrhage, DWML were not found to be a predictor. Thefindings of the present study correlate well with those ofKobayashi et al.18
The nature of confluent DWML, in contrast, has typicallybeen reported to be chronic white matter ischemia resultingfrom injury to the long penetrating arteries.55,56 ConfluentDWML is speculated to be facilitated by excessive fall inBP,45–47,57,58 including orthostatic dysregulation59 and post-prandial hypotension.60 Prospective studies, however, supportthe view that high BP may accelerate confluent DWML.44,61
The present study also suggests that nighttime BP increaserather than excessive nighttime BP dip correlates well withthe development of dementia. Larger longitudinal studies toclarify the optimal BP level to prevent the development ofDWML are necessary.
Reduced cerebral blood flow accompanied by an increasedoxygen extraction fraction has also been observed in nonde-mented patients with confluent DWML.62,63 Misery perfusionmight represent a predisposition for chronic ischemia in whitematter over a long period, resulting in more extensive white
TABLE 2. Comparison of Baseline Characteristics, MRI Findings, and BP ValuesBetween Subjects With and Without Subsequent Vascular Events
Without VascularEvents
(n�131)
With VascularEvents(n�46) P
Age, y 69.2�8.4 68.7�9.6 NS
Sex, M/F 84/47 26/20 NS
Hypertension, n (%) 107(81.6) 44(95.6) �0.05
Diabetes mellitus, n (%) 10(7.6) 15(32.6) �0.0001
Dyslipidemia, n (%) 32(24.4) 19(41.3) �0.01
Smoking, n (%) 27(20.6) 12(26.0) NS
Cognitive impairment, n (%) 15(11.4) 8(17.3) �0.05
Lacuna grade 1.33�0.56 1.72�0.79 �0.001
DWML grade 1.22�0.93 1.39�0.84 NS
Casual SBP, mm Hg 146.2�21.8 155.7�22.4 �0.01
Day SBP, mm Hg 144.8�20.3 154.9�16.2 �0.01
Night SBP, mm Hg 137.1�22.8 151.3�18.6 �0.001
24-h SBP, mm Hg 142.2�20.4 153.7�16.4 �0.001
Degree of nocturnal SBP dip, mm Hg 0.057�0.085 0.017�0.07 �0.01
Casual DBP, mm Hg 82.7�13.1 85.0�22.7 NS
Day DBP, mm Hg 81.7�11.8 83.7�10.9 NS
Night DBP, mm Hg 75.0�12.2 79.7�12.1 �0.05
24-h DBP, mm Hg 79.5�11.6 82.3�10.9 NS
Degree of nocturnal DBP dip, mm Hg 0.087�0.093 0.052�0.08 �0.05
Nondipper/dipper, n 61/70 29/17 �0.05
Values are mean�SD unless indicated otherwise.
Yamamoto et al Predictive Factors for Different Outcomes in Lacunar Infarct Patients 301
by guest on July 14, 2015http://stroke.ahajournals.org/Downloaded from

TABLE 3. Results of Cox Proportional Hazards Regression Analysis of Predictors ofSubsequent Dementia
Age- and Sex-Adjusted Univariate Analysis Multivariate Analysis
RR 95% CI P RR 95% CI P
Age50s vs 60s 3.88 0.485–31.07 0.201 2.31 0.226–23.7 0.47950s vs 70s 5.54 0.708–43.3 0.102 4.4 0.424–45.6 0.21450s vs 80s 11.55 1.34–99.2 0.025 8.53 0.824–88.4 0.072
Sex 2.44 0.835–7.16 0.102 4.25 1.22–14.7 0.022Hypertension 2.15 0.499–9.27 0.325 � � � � � � � � �Diabetes mellitus 0.877 0.201–3.82 0.86 � � � � � � � � �Dyslipidemia 0.45 0.134–1.51 0.198 � � � � � � � � �Smoking 1.05 0.408–2.74 0.906 � � � � � � � � �Cognitive impairment 8.01 3.39–18.9 �0.0001 3.01 1.05–8.59 0.036Lacuna grade
0–1 1 � � � � � � � � � � � � � � �2 4.03 1.65–9.82 0.0021 2.38 0.878–6.47 0.0883 4.84 1.41–16.6 0.012 3.36 0.725–15.6 0.121
DWML grade0–1 1 � � � � � � � � � � � � � � �2 9.7 2.56–36.6 0.0008 7.13 1.63–31.5 0.0093 42.6 11.3–160.0 �0.0001 35.8 7.23–177.3 �0.0001
Casual SBP, mm Hg�160 1 � � � � � � � � � � � � � � �160–180 0.421 0.120–1.60 0.174 � � � � � � � � ��180 1.42 0.561–5.48 0.354 � � � � � � � � �
Day SBP, mm Hg�135 1 � � � � � � � � � � � � � � �135–150 0.67 0.193–2.35 0.535 � � � � � � � � ��150 1.39 0.545–3.54 0.49 � � � � � � � � �
Night SBP, mm Hg�120 1 � � � � � � � � � � � � � � �120–140 1.66 0.438–6.35 0.453 � � � � � � � � ��140 2.21 0.624–7.83 0.219 � � � � � � � � �
24-h SBP, mm Hg�130 1 � � � � � � � � � � � � � � �130–145 0.574 0.142–2.32 0.436 � � � � � � � � ��145 1.31 0.503–3.41 0.58 � � � � � � � � �
Casual DBP, mm Hg�100 1 � � � � � � � � � � � � � � �100–110 1.44 0.516–2.79 0.493 � � � � � � � � ��110 0.978 0.287–2.67 0.89 � � � � � � � � �
Day DBP, mm Hg�80 1 � � � � � � � � � � � � � � �80–90 0.897 0.336–2.39 0.827 � � � � � � � � ��90 0.989 0.339–2.88 0.989 � � � � � � � � �
Night DBP, mm Hg�70 1 � � � � � � � � � � � � � � �70–80 0.998 0.367–2.71 0.998 � � � � � � � � ��80 0.957 0.338–2.71 0.655 � � � � � � � � �
24-h DBP, mm Hg�75 1 � � � � � � � � � � � � � � �75–85 0.62 0.218–1.79 0.625 � � � � � � � � ��85 1.07 0.395–2.94 0.882 � � � � � � � � �
Dipper vs nondipper 3.07 1.21–7.79 0.018 7.13 2.21–22.09 0.001
Age and sex were analyzed simultaneously.
302 Stroke January 2002
by guest on July 14, 2015http://stroke.ahajournals.org/Downloaded from

TABLE 4. Results of Cox Proportional Hazards Regression Analysis of Predictors ofSubsequent Vascular Events
Age- and Sex-Adjusted Univariate Analysis Multivariate Analysis
RR 95% CI P RR 95% CI P
Age50s vs 60s 1.07 0.463–2.5 0.864 0.779 0.272–2.22 0.6450s vs 70s 0.909 0.375–2.2 0.831 1.73 0.592–5.08 0.31550s vs 80s 1.27 0.415–3.91 0.672 1.94 0.517–7.32 0.324
Sex 0.866 0.465–1.61 0.65 1.04 0.505–2.15 0.909Hypertension 6.81 0.93–49.9 0.0589 � � � � � � � � �Diabetes mellitus 5.66 3.01–10.6 �0.0001 5.76 2.77–11.9 �0.0001Hyperchoresterolemia 2.3 1.25–4.22 0.0072 1.8 0.855–3.825 0.12Smoking 0.981 0.436–2.2 0.963 � � � � � � � � �Cognitive impairment 2.16 0.949–4.9 0.066 � � � � � � � � �Lacuna grade
0–1 1 � � � � � � � � � � � � � � �2 6.44 2.92–14.1 �0.0001 6.42 2.59–15.8 �0.00013 14.4 5.94–35.3 �0.0001 8.57 3.14–23.3 �0.0001
DWML grade0–1 1 � � � � � � � � � � � � � � �2 2.78 1.40–553 0.0034 1.22 0.571–2.61 0.6053 3.15 1.24–8.24 0.019 1.6 0.537–4.7 0.398
Casual SBP, mm Hg�160 1 � � � � � � � � � � � � � � �160–180 2.69 0.534–13.6 0.229 � � � � � � � � ��180 4.81 0.96–24.1 0.056 � � � � � � � � �
Day SBP, mm Hg�135 1 � � � � � � � � � � � � � � �135–150 5.23 1.15–23.7 0.031 � � � � � � � � ��150 9.96 2.37–41.8 0.0017 � � � � � � � � �
Night SBP, mm Hg�120 1 � � � � � � � � � � � � � � �120–140 1.58 0.287–8.71 0.598 � � � � � � � � ��140 9.72 2.32–40.5 0.0018 � � � � � � � � �
24-h SBP, mm Hg�130 1 � � � � � � � � � � � � � � �130–145 3.79 0.392–36.6 0.539 2.66 0.268–26.4 0.402�145 20.6 2.82–150.8 0.0028 10.3 1.32–81.3 0.025
Casual DBP, mm Hg�100 1 � � � � � � � � � � � � � � �100–110 1.76 0.627–3.96 0.347 � � � � � � � � ��110 1.54 0.601–3.64 0.361 � � � � � � � � �
Day DBP, mm Hg�80 1 � � � � � � � � � � � � � � �80–90 1.91 0.906–4.02 0.089 � � � � � � � � ��90 1.53 0.669–3.51 0.312 � � � � � � � � �
Night DBP, mm Hg�70 1 � � � � � � � � � � � � � � �70–80 1.37 0.51–3.69 0.529 � � � � � � � � ��80 3.5 1.53–8.00 0.0029 � � � � � � � � �
24-h DBP, mm Hg�75 1 � � � � � � � � � � � � � � �75–85 1.83 0.71–4.71 0.211 � � � � � � � � ��85 3.25 1.32–7.98 0.01 � � � � � � � � �
Dipper vs nondipper 2.06 1.09–3.87 0.024 0.772 0.355–1.67 0.512
Age and sex were analyzed simultaneously.
Yamamoto et al Predictive Factors for Different Outcomes in Lacunar Infarct Patients 303
by guest on July 14, 2015http://stroke.ahajournals.org/Downloaded from

matter ischemia and thus leading to Binswanger’s disease.64
Although confluent DWML has been reported to predictcerebrovascular and cardiovascular events or death,6,19,20,65
no study, to our knowledge, has ever demonstrated thatconfluent DWML can be used as an independent predictor forsubsequent dementia. In addition, as previously suggested,cognitive impairment was also found to be an independentpredictor for dementia.66,67
Diabetes mellitus was revealed to be an independentpredictor for vascular events and nonvascular death. Diabetesmellitus has been established as an independent risk factor forischemic stroke by prospective epidemiological studies.68,69
The widespread large-vessel atherosclerosis observed in thecerebral and general circulation of diabetic patients probablycontributes to an enhanced risk of vascular events. It is alsoreasonable to state that diabetic patients may be prone tononvascular deaths, such as those that result from infectiousdiseases.
Although the results of this study are encouraging, certainlimitations should be addressed. First, the outcome for 56patients (31.6%) was identified according to reports fromfamily physicians. Nonetheless, our partnership with familyphysicians has been well established, and the informationfrom family physicians and patients’ families correspondedwell. Second, because the main purpose of this study was tothoroughly assess predictors for different outcomes afterlacunar infarct, limited examinations, ie, CDR and HDSR,were used to assess cognitive function. It may be insufficientto diagnose dementia with the use of only the CDR at a familyphysician’s office. Additionally, identification of the time ofdementia development by a family physician may have beenambiguous. Third, vascular workup was lacking becausecarotid Doppler ultrasonography and MR angiography werenot performed for every patient.
The present study represents the first study to thoroughlyanalyze long-term outcomes of lacunar infarct patients withthe use of ABPM and MRI. It is particularly noteworthy thatdistinct predictive factors were revealed for the developmentof dementia and vascular events. Confluent DWML and anondipping status appear to represent independent predictorsfor subsequent development of dementia, while diabetesmellitus, multiple lacunae, and high 24-hour SBP valueappear to be independent predictors for vascular events.Incidence of subsequent vascular events can be reduced bystricter BP control. The pathogenic mechanism of nondippingstatus should also be investigated further to reduce the risk ofvascular dementia.
AcknowledgmentThe authors are grateful to Christopher Hurt for reviewing themanuscript.
References1. Fisher CM. Lacunar infarcts: a review. Cerebrovasc Dis. 1991;1:
311–320.2. Bamford J, Sandercock P, Jones L, Warlow C. The natural history of
lacunar infarction: the Oxfordshire Community Stroke Project. Stroke.1987;18:545–551.
3. Sacco SE, Whisnant JP, Broderick JP, Phillips SJ, O’Fallon WM. Epi-demiological characteristics of lacunar infarcts in a population. Stroke.1991;22:1236–1241.
4. Clavier I, Hommel M, Besson G, Noelle B, Perret J. Long-term prognosisof symptomatic lacunar infarcts: a hospital-based study. Stroke. 1994;25:2005–2009.
5. Suzuki K, Kutsuzawa T, Takita K, Ito M, Sakamoto T, Hirayama A, ItoT, Ishida T, Oonishi H, Kawakami K, Hirota K, Ogasawara T, Yoshida J,Tamura T, Hattori S, Iwabuchi S, Karouji Y, Waga T, Oosato Y, YazakiK, Saito T, Oouchi T, Kojima S. Clinico-epidemiologic study of stroke inAkita, Japan. Stroke. 1987;18:402–406.
6. Miyao S, Takano A, Teramoto J, Takahashi A. Leukoaraiosis in relationto prognosis for patients with lacunar infarction. Stroke. 1992;23:1434–1438.
7. Gandolfo C, Moretti C, Dall’Agata D, Primavera A, Brusa G, Loeb C.Long-term prognosis of patients with lacunar syndromes. Acta NeurolScand. 1986;74:224–229.
8. Salgado AV, Ferro JM, Gouveia-Oliveira A. Long-term prognosis offirst-ever lacunar strokes: a hospital-based study. Stroke. 1996;27:661–666.
9. Samuelsson M, Soderfeldt B, Olsson GB. Functional outcome in patientswith lacunar infarction. Stroke. 1996;27:842–846.
10. Ueda K, Kawano H, Hasuo Y, Fijishima M. Prevalence and etiology ofdementia in a Japanese community. Stroke. 1992;23:798–803.
11. Loeb C, Gandolfo C, Croce R, Conti M. Dementia associated withlacunar infarction. Stroke. 1992;23:1225–1229.
12. You R, McNeil JJ, O’Malley HM, Davis SM, Donnan GA. Risk factorsfor lacunar infarction syndromes. Neurology. 1995;45:1483–1487.
13. Shimada K, Kawamoto A, Matsubayashi K, Ozawa T. Silent cerebro-vascular disease in the elderly: correlation with ambulatory pressure.Hypertension. 1990;16:692–699.
14. Verdecchia P, Schillaci G, Guerrieri M, Gatteschi C, Benemio G, BoldriniF, Porcellati C. Diurnal blood pressure changes and left ventricularhypertrophy in essential hypertension. Circulation. 1990;81:528–536.
15. Verdecchia P, Porcellati C, Schillaci G, Borgioni C, Ciucci A, BattistelliM, Guerrieri M, Gatteschi C, Zampi I, Santucci A, Santucci C, Reboldi G.Ambulatory blood pressure: an independent predictor of prognosis inessential hypertension. Hypertension. 1994;24:793–801.
16. Khattar RS, Swales JD, Banfield A, Dore C, Senior R, Lahiri A. Pre-diction of coronary and cerebrovascular morbidity and mortality by directcontinuous ambulatory blood pressure monitoring in essential hyper-tension. Circulation. 1999;100:1071–1076.
17. Staessen JA, Thijs L, Fagard R, O’Brien ET, Clement D, Leeuw PW,Mancia G, Nachev C, Palatini P, Parati G, Tuomilehto J, Webster J.Predicting cardiovascular risk using conventional vs ambulatory bloodpressure in older patients with systolic hypertension. JAMA. 1999;282:539–546.
18. Kobayashi S, Okada K, Koide H, Bokura H, Yamaguchi S. Subcorticalsilent brain infarction as a risk factor for clinical stroke. Stroke. 1997;28:1932–1939.
19. van Swieten JC, Kappelle LJ, Algra A, Latum C, Koudstaal PJ, van GijnJ. Hypodensity of the cerebral white matter in patients with transientischemic attack or minor stroke: influence on the rate of subsequentstroke. Ann Neurol. 1992;32:177–183.
20. Inzitari D, Cadelo M, Marranci ML, Pracucci G, Pantoni L. Vasculardeath in elderly neurological patients with leukoaraiosis. J Neurol Neu-rosurg Psychiatry. 1997;62:177–181.
21. Schmidt R, Fazekas F, Kleinert G, Offenbacher H, Gindl K, Payer F,Freidl W, Niederkorn K, Lechner H. Magnetic resonance imaging signalhyperintensities in the deep and subcortical white matter: a comparativestudy between stroke patients and normal volunteers. Arch Neurol. 1992;49:825–827.
22. Imai Y, Nagai K, Sakuma M, Sakuma H, Minami N, Munakata M,Hashimoto J, Yamagishi T. Ambulatory blood pressure of adults inOhazama, Japan. Hypertension. 1993;22:900–912.
23. Guideline Subcommittee. 1999 World Health Organization-InternationalSociety of Hypertension guideline for the management of hypertension.J Hypertens. 1999;17:151–183.
24. Hughes CP, Berg L, Danziger WL, Coben LA, Martin R. A new clinicalscale for staging of dementia. Br J Psychiatry. 1982;140:566–572.
25. Hasegawa K. Evaluation of dementia in the aged. J Geriatr PsychiatrMed. 1984;3:308–314.
26. American Psychiatric Association. Diagnostic and Statistical Manual ofMental Disorders, Revised Third Edition. Washington, DC: AmericanPsychiatric Association; 1987.
27. Ohkubo T, Imai Y, Tsuji I, Nagai K, Watanabe N, Minami N, Itoh O,Bando T, Sakuma M, Fukao A, Satoh H, Hisamichi S, Abe K. Predictionof mortality by ambulatory blood pressure monitoring versus screening
304 Stroke January 2002
by guest on July 14, 2015http://stroke.ahajournals.org/Downloaded from

blood pressure measurements: a pilot study in Ohazama. J Hypertens.1997;15:357–364.
28. Perloff D, Sokolow M, Cowan R. The prognostic value of ambulatoryblood pressures. JAMA. 1983;249:2792–2798.
29. Kernan WN, Viscoli CM, Brass LM, Makuch RW, Sarrel PM, HorowitzRI. Blood pressure exceeding national guideline among women afterstroke. Stroke. 2000;31:415–419.
30. Makino Y, Kawano Y, Minami J, Yamaguchi T, Takishita S. Risk ofstroke in relation to level of blood pressure and other risk factors intreated hypertensive patients. Stroke. 2000;31:48–52.
31. Guo Z, Fratiglioni L, Winblad B, Viitanen M. Blood pressure and per-formance on the Mini-Mental State Examination in the very old: cross-sectional and longitudinal data from the Kungsholmen project. Am JEpidemiol. 1997;145:1106–1113.
32. Swan GE, Carmelli D, Larue A. Systolic blood pressure tracking over 25to 30 years and cognitive performance in older adults. Stroke. 1998;29:2334–2340.
33. Luner LJ, Masaki K, Petrovitch H, Foley D, Havlik RJ. The associationbetween midlife blood pressure levels and late-life cognitive function: theHonolulu-Asia aging study. JAMA. 1995;274:1846–1851.
34. Tzourio C, Dufouil DP, Alperovitch A. Cognitive decline in individualswith high blood pressure: a longitudinal study in the elderly. Neurology.1999;53:1948–1952.
35. Guo Z, Viitanen M, Fratiglioni L, Winblad B. Low blood pressure anddementia in elderly people: the Kungsholmen project. BMJ. 1996;312:805–808.
36. Skoog I, Lernfelt B, Landahl S, Palmertz B, Andreasson LA, Nilsson L,Persson G, Oden A, Svanborg A. 15-Year longitudinal study of bloodpressure and dementia. Lancet. 1996;347:1141–1145.
37. Yamamoto Y, Akiguchi I, Oiwa K, Hayashi M, Imai K. Twenty-four-hour blood pressure changes in the course of lacunar disease. Cere-brovasc Dis. 2001;11:100–106.
38. Tomonaga M, Yamanouchi H, Tohgi H, Kameyama M. Clinicopatho-logical study of progressive subcortical encephalopathy (Binswangertype) in the elderly. J Am Geriatr Soc. 1982;30:961–965.
39. Tohgi H, Chiba K, Kimura M. Twenty-four-hour variation of bloodpressure in vascular dementia of Binswanger type. Stroke. 1991;7:477–483.
40. Goldstein IB, Bartzokis G, Hance DB, Shapiro D. Relationship betweenblood pressure and subcortical lesions in healthy elderly people. Stroke.1998;29:765–772.
41. Kukla C, Sander D, Schwarze J, Wittich I, Klingelhofer J. Changes ofcircadian blood pressure patterns are associated with the occurrence oflacunar infarction. Arch Neurol. 1998;55:683–688.
42. Sander D, Winbeck, Klingelhofer J, Conrad B. Extent of cerebral whitematter lesions is related to changes of circadian blood pressure rhyth-micity. Arch Neurol. 2000;57:1302–1307.
43. Yamamoto Y, Akiguchi I, Oiwa K, Satoi H, Kimura J. Diminishednocturnal blood pressure decline and lesion site in cerebrovasculardisease. Stroke. 1995;26:829–833.
44. Yamamoto Y, Akiguchi I, Oiwa K, Hayashi M, Kimura J. Adverse effectof nighttime blood pressure on the outcome of lacunar infarct patients.Stroke. 1998;29:570–576.
45. Nakamura K, Oita J, Yamaguchi T. Nocturnal blood pressure dip instroke survivors: a pilot study. Stroke. 1995;26:1373–1378.
46. Kario K, Matsuo T, Kobayashi H, Imiya M, Mastuo M, Shimada K.Nocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients: advanced silent cerebrovascular damage inextreme dippers. Hypertension. 1996;27:130–135.
47. Watanabe N, Imai Y, Nagai K, Tsuji I, Satoh H, Sakuma M, Sakuma H,Kato J, Onodera-Kikuchi H, Yamada M, Abe F, Hisamichi S, Abe K.Nocturnal blood pressure and silent cerebrovascular lesions in elderlyJapanese. Stroke. 1996;27:1319–1327.
48. Marti-Fabregas J, Valencia C, Lopez-Contreras J, Roca-Cusachs A, SoleMJ, Garcia-Sanchez C, Marti-Vilalta JL. Blood pressure variability in
Binswanger’s disease and isolated lacunar infarction. Cerebrovasc Dis.2001;11:230–234.
49. Kohara K, Nishida W, Maguchi M, Hiwada K. Autonomic nervous functionin non-dipper essential hypertensive subjects: evaluation by power spectralanalysis of heart rate variability. Hypertension. 1995;26:808–814.
50. Uzu T, Kimura G. Diuretics shift circadian rhythm of blood pressure fromnondipper to dipper in essential hypertension. Circulation. 1999;100:1635–1638.
51. Campese VM. Salt sensitivity in hypertension: renal and cardiovascularimplications. Hypertension. 1994;23:531–550.
52. Uehara T, Tabuchi M, Mori E. Risk factors for silent cerebral infarcts insubcortical white matter and basal ganglia. Stroke. 1999;30:378–382.
53. Longstreth BC, Manolio TA, Bryan N, Jungreis CA, Price TR. Lacunarinfarcts defined by magnetic resonance imaging of 3660 elderly people:the Cardiovascular Health Study. Arch Neurol. 1998;55:1217–1225.
54. Brott T, Tomsick T, Feinberg W, Johnston C, Biller J, Broderick J, KellyM, Frey J, Schwartz S, Blum C, Nelson JJ, Chambless L, Toole J.Baseline silent cerebral infarction in the Asymptomatic Carotid Athero-sclerosis Study. Stroke. 1994;25:1122–1129.
55. Furuta A, Ishii N, Nishihara Y, Horie A. Medullary arteries in aging anddementia. Stroke. 1991;22:442–446.
56. Fazekas F, Kleinert R, Offenbacher H, Schmidt R, Kleinert G, Payer F,Rander H, Lechner H. Pathologic correlates of incidental MRI whitematter signal hyperintensities. Neurology. 1993;43:1683–1689.
57. Chamorro A, Pujol J, Saiz A, Vila N, Vilanova JC, Alday M, Blanc R.Periventricular white matter lucencies in patients with lacunar stroke: amarker of too high or too low blood pressure? Arch Neurol. 1997;54:1284–1288.
58. Leeuw FE, Groot JC, Oudkerk M, Kors JA, Hofman A, Gijn J, BretelerMMB. Atrial fibrillation and the risk of cerebral white matter lesions.Neurology. 2000;50:1795–1800.
59. Matsubayashi K, Okumiya K, Wada T, Osaki Y, Fujisawa M, Doi Y,Ozawa T. Postural dysregulation in systolic blood pressure is associatedwith worsened scoring on neurobehavioral function tests and leuko-araiosis in the older elderly living in a community. Stroke. 1997;28:2169–2173.
60. Kohara K, Jiang Y, Igase M, Takata Y, Fukuoka T, Okura T, Kitami Y,Hiwada K. Postprandial hypotension is associated with asymptomaticcerebrovascular damage in essential hypertensive patients. Hypertension.1999;33:565–568.
61. Schmidt R, Fazekas F, Kappeller P, Schmidt H, Hartung HP. MRI whitematter hyperintensities: three-year follow up of the Austrian Stroke Pre-vention Study. Neurology. 1999;53:132–139.
62. Meguro K, Hatazawa J, Yamaguchi T, Itoh M, Matsuzawa T, Ono S,Miyazawa H, Hishinuma T, Yanai K, Sekita Y, Yamada K. Cerebralcirculation and oxygen metabolism associated with subclinical periven-tricular hyperintensity as shown by magnetic resonance imaging. AnnNeurol. 1990;28:378–383.
63. Yao H, Sadoshima S, Ibayashi S, Kuwabara Y, Ichiya Y, Fujishima M.Leukoaraiosis and dementia in hypertensive patients. Stroke. 1992;23:1673–1677.
64. Bennett DA, Wilson RS, Gilley DW, Fox JH. Clinical diagnosis ofBinswanger’s disease. J Neurol Neurosurg Psychiatry. 1990;53:961–965.
65. Briley DP, Haroon S, Sergent SM, Thomas S. Does leukoaraiosis predictmorbidity and mortality? Neurology. 2000;54:90–94.
66. Rockwood K, Wentzel C, Hachinski V, Hogan DB, MacKnight C,McDowell I. Prevalence and outcomes of vascular cognitive impairment.Neurology. 2000;54:447–451.
67. Flicker C, Ferris SH, Reisberg B. Mild cognitive impairment in theelderly: predictors of dementia. Neurology. 1991;41:1006–1009.
68. Stegmayr B, Asplund K. Diabetes as a risk factor for stroke: a populationperspective. Diabetologia. 1995;38:1061–1068.
69. Davis PH, Dambrosia JM, Schoenberg BS, Schoenberg DG, Pritchard A,Lilienfeld AM, Whisnant JP. Risk factors for ischemic stroke: a pro-spective study in Rochester, Minnesota. Ann Neurol. 1987;22:319–327.
Yamamoto et al Predictive Factors for Different Outcomes in Lacunar Infarct Patients 305
by guest on July 14, 2015http://stroke.ahajournals.org/Downloaded from

The article “Twenty-four–Hour Blood Pressure and MRI as Predictive Factors for DifferentOutcomes in Patients With Lacunar Infarct” by Yamamoto et al1 was incorrectly published underthe heading Case Report instead of Original Contribution. The journal Stroke regrets thisunfortunate error and offers sincere apologies to Dr. Yamamoto and his coauthors.
1[Correction for Vol 33, Number 1, January 2002. Pages 297–305.](Stroke. 2002;33:883.)© 2002 American Heart Association, Inc.
Stroke is available at http://www.strokeaha.org
883
Correction

Y. Yamamoto, I. Akiguchi, K. Oiwa, M. Hayashi, T. Kasai and K. Ozasain Patients With Lacunar Infarct
Hour Blood Pressure and MRI as Predictive Factors for Different Outcomes−Twenty-four
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 2002 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke 2002;33:297-305Stroke.
http://stroke.ahajournals.org/content/33/1/297World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org/content/33/3/883.full.pdfAn erratum has been published regarding this article. Please see the attached page for:
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOnce the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Strokein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on July 14, 2015http://stroke.ahajournals.org/Downloaded from




























![[Dissecting aortic aneurysm simulating an acute myocardial infarct]](https://img.pdfslide.net/doc/110x75/63558f23922cbb7c550ca86c/dissecting-aortic-aneurysm-simulating-an-acute-myocardial-infarct.jpg)
