Embed Size (px)
Citation preview
© 2007 McGraw-Hill Higher Education. All rights reserved.
Movement in Adulthood
Chapter 15
© 2007 McGraw-Hill Higher Education. All rights reserved.
Objectives• Explain the shift to a life-span approach to
the study of motor development• Describe balance and postural sway in
adulthood• Describe the key issues associated with
falls in adulthood• Explain walking patterns of adulthood• Explain key issues and factors associated
with driving and older adulthood• Describe adult performance on selected
motor activities
© 2007 McGraw-Hill Higher Education. All rights reserved.
Objectives • Describe activities of daily living in adulthood• Explain age of peak proficiency as it relates to key
“physical skills”• Explain adult performance during high arousal• Describe movement speed in adulthood• Explain movement decline with age• Describe sports related injuries to baby boomers
and older adults• Explain key issues associated with teaching
movement skill to older adults• List and explain the World Health Organization
Heidelberg Guidelines
© 2007 McGraw-Hill Higher Education. All rights reserved.
“We are an aging population and because
of this, the study of adulthood is important. We need to ensure that older adults have every
possible chance of maintaining a high quality
of life.”
© 2007 McGraw-Hill Higher Education. All rights reserved.
Introduction• Recall that motor development is the
study of the changes in motor behavior over the lifespan
• A widely accepted definition, but not practically applied
• Movement in adulthood completes the approach in lifespan motor development
© 2007 McGraw-Hill Higher Education. All rights reserved.
Introduction• There is an increase interest in
adulthood because, as a nation, we are getting older
• Since 1900 we have– 3 times more people over age 65 yr– 8 times more people ages 65-74 yr– 16 times more people ages 75-84 yr– 31 times more people over age 85 yr!
© 2007 McGraw-Hill Higher Education. All rights reserved.
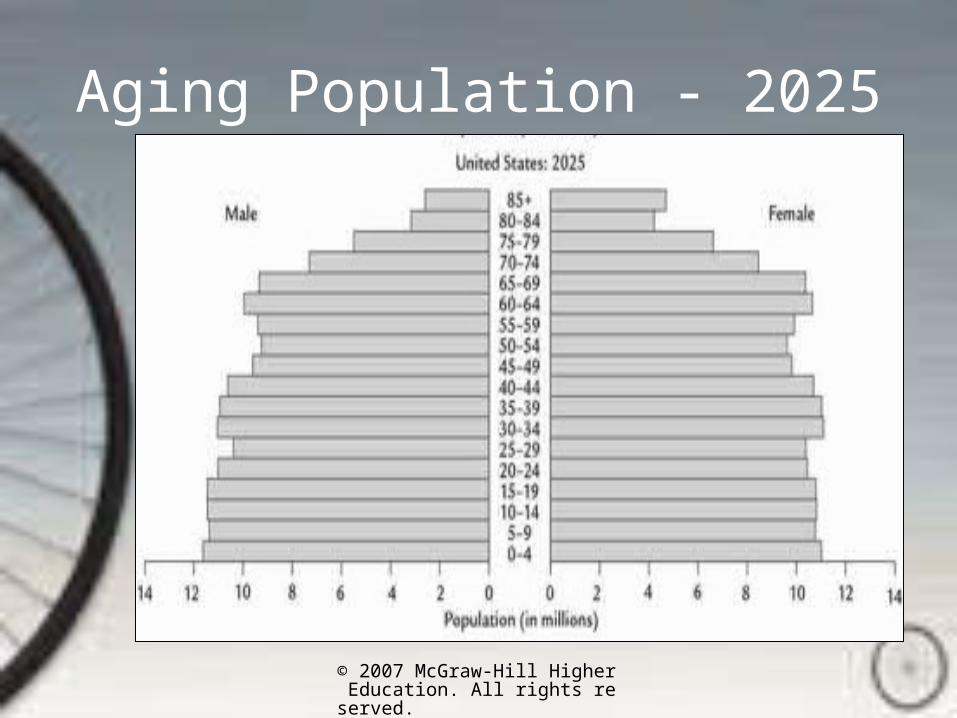
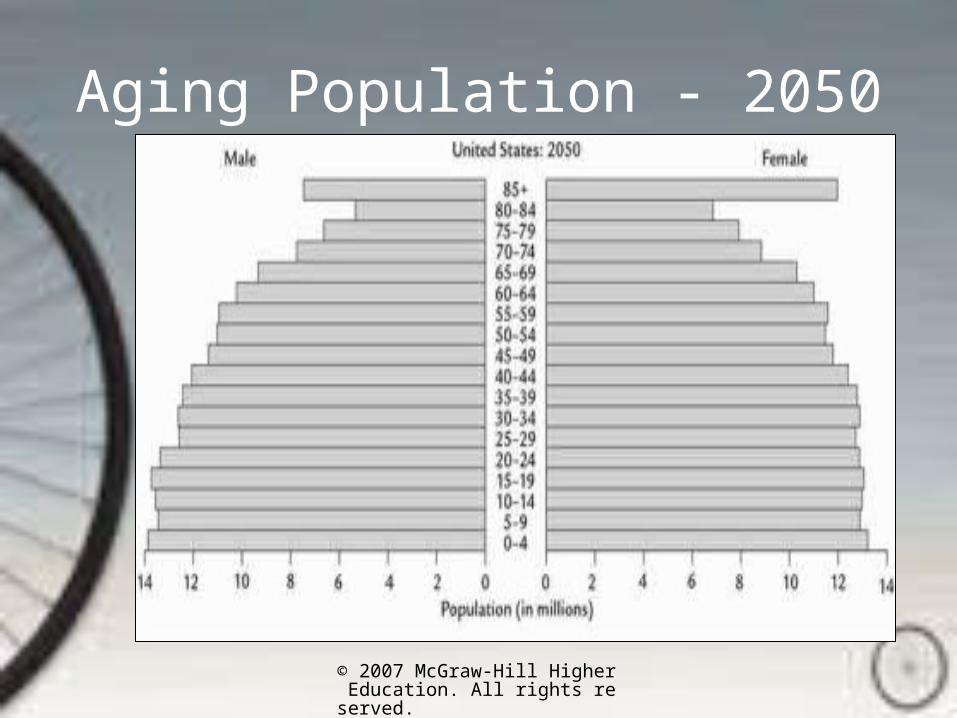
Introduction• We are an aging population
– It is estimated, that there will be 800,000 centenarians by 2050
– Today, 4/5 of all centenarians are women
• There is a need to advance knowledge concerning adulthood in order to reduce the older adult’s dependence on society and the financial drain that may result
© 2007 McGraw-Hill Higher Education. All rights reserved.
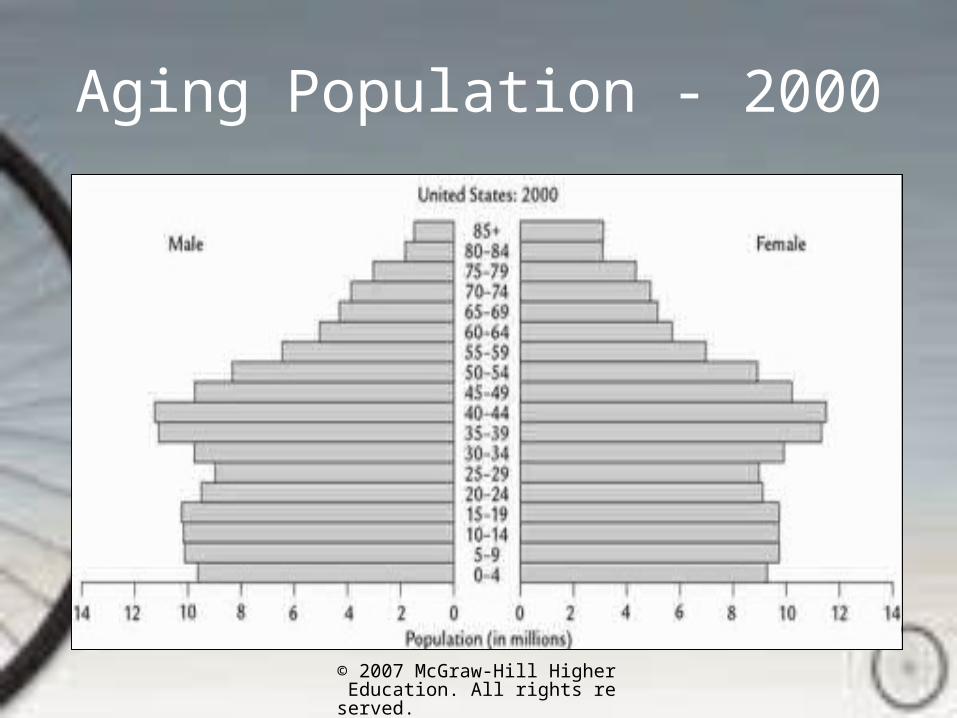
Aging Population - 2000
© 2007 McGraw-Hill Higher Education. All rights reserved.
Aging Population - 2025
© 2007 McGraw-Hill Higher Education. All rights reserved.
Aging Population - 2050
© 2007 McGraw-Hill Higher Education. All rights reserved.
Introduction
“The study of motor development in adulthood will provide older adults every possible chance of
maintaining a high quality of life through their old
age.”
© 2007 McGraw-Hill Higher Education. All rights reserved.
Balance and Postural Sway• The incidence of falls increases with
age
• Balance is studied to determine its role in the etiology of falling
• The process of automatic control with balance that develops during childhood reverses in late adulthood– Balance becomes more of a conscience
effort
© 2007 McGraw-Hill Higher Education. All rights reserved.
Balance and Postural Sway
•“Postural sway is a nearly imperceptible back and forth motion designed to assist the body in maintaining upright or standing position.”
© 2007 McGraw-Hill Higher Education. All rights reserved.
Balance and Postural Sway• Postural sway is gradually refined
during childhood
• During the 6th decade, a gradual deterioration is seen
• By age 80 yr, postural control may look like that seen in children between the ages of 6 and 9 yr
© 2007 McGraw-Hill Higher Education. All rights reserved.
Balance and Postural Sway
• When somatosensory and visual information is incongruent with postural sway, older adults may lose balance completely
• Postural sway is higher in women throughout adulthood
© 2007 McGraw-Hill Higher Education. All rights reserved.
Balance and Postural Sway• Loss of balance control may be due to:
– Decreasing ability of the central nervous system to control movement
– Reduction of the number of cells in the cerebellum and brain stem
– Decreased capacity in using proprioceptive information
• With age, the adult receives less accurate information concerning position of the body parts
© 2007 McGraw-Hill Higher Education. All rights reserved.
Falls• Falls are the leading cause of nonfatal and
fatal injury in older Americans• One in three Americans over the age of 65
falls each year, and 20% to 30% of those who fall suffer serious injury such as hip fractures or head traumas, severely affecting quality of life and risk of premature death
• Falls also diminish mobility and quality of life due to fears of falling again
© 2007 McGraw-Hill Higher Education. All rights reserved.
Falls• More accidental deaths in the elderly are
due to falls than all other reasons– In 1994, 7000 elderly people died as a result of
a fall– More than 11,000 Americans aged 65 and older
died from fall-related injuries in 2003
• The number of falls increases with age• Poor vision, increased medication, and
lower foot raise during walking contribute to falls
© 2007 McGraw-Hill Higher Education. All rights reserved.
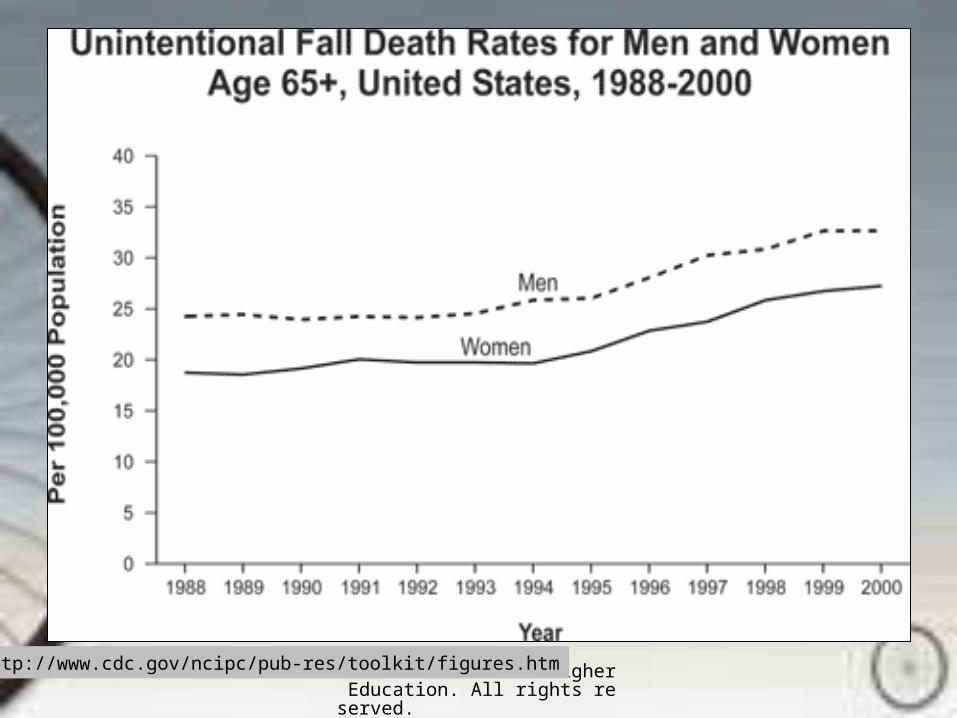
Falls• Women fall more than men, but men
suffer greater medical consequences and mortality
• Fractures occur in 5% of all falls
• Hip fractures occur in 1 % of all falls– 50% of those hospitalized will die within
1 year
• 53% of falls are due to tripping
© 2007 McGraw-Hill Higher Education. All rights reserved.
Falls • Half of the elderly who fall never
regain functional walking
• Several simple steps and precautions, including implementing a physical activity program, can help decrease the incidence of falls
© 2007 McGraw-Hill Higher Education. All rights reserved.
http://www.cdc.gov/ncipc/pub-res/toolkit/figures.htm
© 2007 McGraw-Hill Higher Education. All rights reserved.
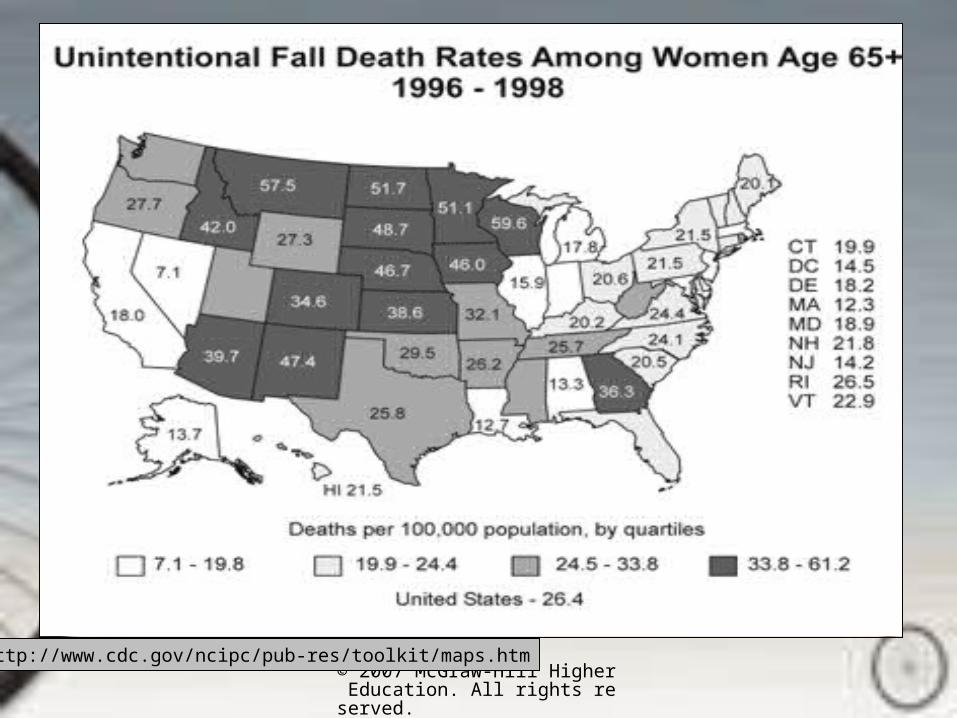
http://www.cdc.gov/ncipc/pub-res/toolkit/maps.htm

© 2007 McGraw-Hill Higher Education. All rights reserved.
http://www.cdc.gov/ncipc/pub-res/toolkit/maps.htm
© 2007 McGraw-Hill Higher Education. All rights reserved.
Falls • Causes of falls
– Predispositional• Related to inherent physiology or cognitive
ability
– Situational • Linked to the environment surrounding the
fall
© 2007 McGraw-Hill Higher Education. All rights reserved.
Falls• Predispositional
Causes– Balance problems– Declining flexibility– Disease– Reduced joint
mobility– Declining strength– Slower reaction
time– Poor vision– Difficulty walking
• Situational Causes– Alcohol use– Improper clothing– Darkness– Environmental
obstacles– Medication– Rushing
© 2007 McGraw-Hill Higher Education. All rights reserved.
Falls • Vision
– An important factor in maintaining postural stability
• Poor lighting• Reduced vision
• Medications– Increase risk of falling– Diuretics found to increase risk of falling 1.6x– Beta-blockers increase falls in women by 2x
© 2007 McGraw-Hill Higher Education. All rights reserved.
Falls • Gait
– Older adults who have gait characteristics such as walking fast and taking fast steps or long steps relative to height are likely to fall
– The incidence of tripping is determined less by a walker’s ability to recover from the fall than by walking characteristics
© 2007 McGraw-Hill Higher Education. All rights reserved.
Strategies to Avoid Falls• Remove or decrease environmental
obstacles in the home
• Maintain a physically active lifestyle – Decreasing strength, flexibility, and
muscular and cardiovascular endurance contribute to gait changes
– An active adult is less likely to become ill
© 2007 McGraw-Hill Higher Education. All rights reserved.
Strategies to Avoid Falls
• Exercise– An intervention that is very effective in
reducing falls– Better balance– Fewer falls
© 2007 McGraw-Hill Higher Education. All rights reserved.
“An exercise program that significantly increases
strength, maintains a body weight and composition that are efficient for locomotion,
and improves balance should decrease the number of falls
seen in older people.”
(Spirduso, 1995)
© 2007 McGraw-Hill Higher Education. All rights reserved.
More Information on Falls
• Centers for Disease Control and Prevention. http://www.cdc.gov/ncipc/pub-res/toolkit/SummaryOfFalls.htm
• Facts, risks factors, prevention
© 2007 McGraw-Hill Higher Education. All rights reserved.
Walking Patterns in Adulthood• Compared to children, adults
– Have fewer balance problems• COG is lower
– Are more efficient and less energetic walkers– Take longer strides because of longer legs– Have decreased hip flexion and extension
during the stride– Require less rearward force to slow the forward
momentum following heel strike
© 2007 McGraw-Hill Higher Education. All rights reserved.
Walking Patterns in Adulthood• Presenile gait: 7th decade of life
– Decrease in velocity– Reduction in power during push-off phase– Increase double support phase time– Decrease in step length– Increase in step width– Decrease in step height– More prone to making contact with flat foot– Greater tendency to out-toe
• Complete explanations for these changes are unknown
© 2007 McGraw-Hill Higher Education. All rights reserved.
Walking Patterns in Adulthood• Many believe changes in gait occur
due to– Age-related decline in skeletal muscle– Decline in the central and peripheral
nervous systems– Behavioral changes
• Fear of falling• Depression
– Increase in disease– Reduced physical activity
© 2007 McGraw-Hill Higher Education. All rights reserved.
Walking Patterns in Adulthood
• Walking speed decreases– Normal adult = 1.4 m/s– > 70 yr = 1.2 m/s for men; 1.1 m/s for
women
• Women have trouble executing a 40 cm step
© 2007 McGraw-Hill Higher Education. All rights reserved.
Walking Patterns in Adulthood• Older walkers adopt a more
conservative pattern– Shorter steps
• Decreasing stride and step length
– Slower paced• Improves balance• Reduces risk of falling
– Out-toeing• A technique used to improve lateral stability
when balance declines
© 2007 McGraw-Hill Higher Education. All rights reserved.
Walking Patterns in Adulthood
• In older walkers– Step height decreases– Ankle extension is reduced– Hip extension is greater during the stride

© 2007 McGraw-Hill Higher Education. All rights reserved.
Driving and Older Age• The number of accidents rises
dramatically after the age of 75 yr– Decline in vision– Decline in reaction time– Decline in some cognitive abilities– Increase in disease
© 2007 McGraw-Hill Higher Education. All rights reserved.
Driving and Older Age• Older drivers are
– Passive– Ignore rights of way– Miss important traffic signs– Cause 3-5x more damage from their
accidents
• However, older drivers are involved in fewer accidents than younger drivers
© 2007 McGraw-Hill Higher Education. All rights reserved.
Driving and Older Age• Although older drivers compensate for
their loss of functional abilities, there is an increased anxiety about losing freedom as driving ability decreases– When older adults loose their ability to
drive• It is more difficult to stay engaged with
society• It is hard to maintain dignity
© 2007 McGraw-Hill Higher Education. All rights reserved.
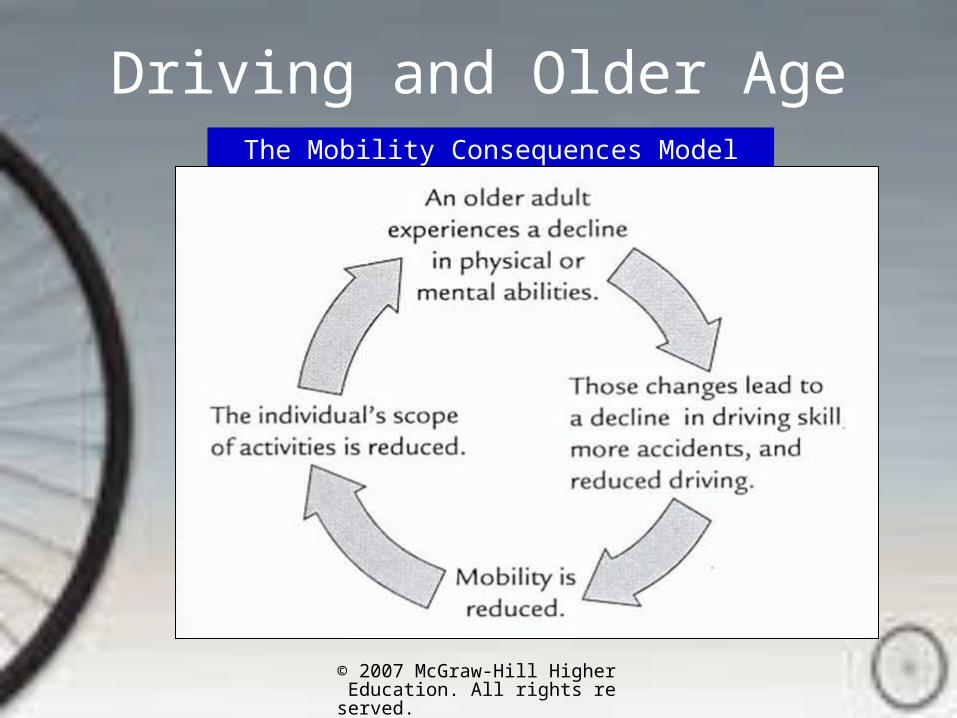
Driving and Older AgeThe Mobility Consequences Model
© 2007 McGraw-Hill Higher Education. All rights reserved.
Adult Performance on Selected Motor Activities
• Vertical jump– Active women had similar patterns to
college-aged women• Velocity of extension was slower, however
• Older women who have remained active are typically able to – Move faster with greater coordination– Display a greater range of motion– Transfer weight more easily– Maintain a more erect posture
© 2007 McGraw-Hill Higher Education. All rights reserved.
Adult Performance on Selected Motor Activities
• Older adults with decreased flexibility– Have trouble putting on socks and shoes– Cannot get out of a chair– Have trouble supinating and pronating in
normal daily activities
• Difficulty in movement leads to a cycle of more inactivity
© 2007 McGraw-Hill Higher Education. All rights reserved.
Activities of Daily Living (ADLs)• One of the biggest fears of the elderly
is the loss of ability in the ADLs– Eating– Rising from a chair– Getting in and out of bed– Brushing teeth– Dressing– Bathing

© 2007 McGraw-Hill Higher Education. All rights reserved.
Instrumental Activities of Daily Living (IADL)
• Cooking
• Shopping
• Doing laundry
• Walking
• Talking medication
• Personal finances
© 2007 McGraw-Hill Higher Education. All rights reserved.
ADL and IADL• Of those who are institutionalized
– 97% have ADL limitations lasting 6 months or longer
• Most common ADLs lasting 6 months or longer are – Bathing– Getting around inside– Getting in and out of bed
© 2007 McGraw-Hill Higher Education. All rights reserved.
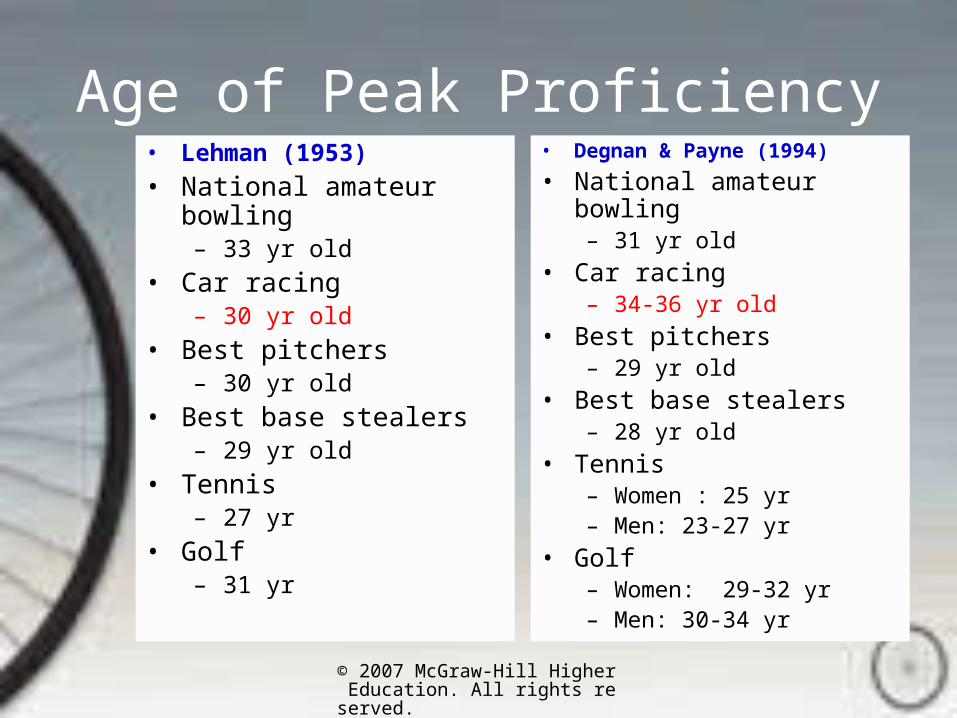
Age of Peak Proficiency• Chronological age and outstanding
performances– Age and achievement by Harvey Lehman
(1953)
• Updated age and outstanding performances– Age and peak performances in adulthood:
1953-1993 by Degnan & Payne (1994)
© 2007 McGraw-Hill Higher Education. All rights reserved.
Age of Peak Proficiency• Lehman (1953)
• National amateur bowling– 33 yr old
• Car racing– 30 yr old
• Best pitchers– 30 yr old
• Best base stealers– 29 yr old
• Tennis– 27 yr
• Golf– 31 yr
• Degnan & Payne (1994)
• National amateur bowling– 31 yr old
• Car racing– 34-36 yr old
• Best pitchers– 29 yr old
• Best base stealers– 28 yr old
• Tennis– Women : 25 yr– Men: 23-27 yr
• Golf– Women: 29-32 yr– Men: 30-34 yr
© 2007 McGraw-Hill Higher Education. All rights reserved.
Age of Peak Proficiency• Vigorous skills deteriorate early
– Peak performance occurs before the age of 30 yr
– Tennis, football, ice hockey
• Less vigorous skills deteriorate more slowly– Rifle / pistol shooting, bowling, billiards
© 2007 McGraw-Hill Higher Education. All rights reserved.
Adult Performance During High Arousal
• Situations of high arousal call for high cognitive demands during performance
• Young adults perform better when a need arises for compensating for nonoptimal levels of arousal or increased competitive distraction
© 2007 McGraw-Hill Higher Education. All rights reserved.
Adult Performance During High Arousal
• Decrease in ability– May be due to an age-related decline in
ability to deal with the increased cognitive demand of high-arousal movement situations
– Target tissues may begin to respond differently to hormonal actions which can affect metabolic rate
© 2007 McGraw-Hill Higher Education. All rights reserved.
Adult Performance During High Arousal
• The decline in motor performance during times of high arousal is reversible– Drug therapy – beta adrenergic blocks– Relaxation training and refocusing the
attention during the high-arousal periods of competition
© 2007 McGraw-Hill Higher Education. All rights reserved.
Movement Speed in Adulthood• Running speed
– Speed for short distances normally declines considerably with age
– Relative running speed for longer distances may not be affected
© 2007 McGraw-Hill Higher Education. All rights reserved.
Movement Speed in Adulthood• Reaction time
– Reaction time is used to determine the status of the central nervous system for cognitive function
– “The interval from presentation of an unanticipated stimulus until the beginning of the response”
© 2007 McGraw-Hill Higher Education. All rights reserved.
Movement Speed in Adulthood• Reaction time
– Declines systematically in adults – Level of urgency required for a task
affects decision time
© 2007 McGraw-Hill Higher Education. All rights reserved.
Movement Speed in Adulthood• Movement time
– “Interval from the initiation of the movement until its termination”
• Short and simple – press a button• Sophisticated – running
– Declines systematically in adults
© 2007 McGraw-Hill Higher Education. All rights reserved.
Movement Speed in Adulthood• Activities requiring more complex
processing of information will lead to a greater rate of slowing
• The amount of decline is related to the complexity of the task
© 2007 McGraw-Hill Higher Education. All rights reserved.
Movement Speed in Adulthood• Spatial transposition involves relating
one signal at one position to a response at another position– Releasing a button when a light stimulus
appears
© 2007 McGraw-Hill Higher Education. All rights reserved.
Movement Speed in Adulthood• Symbolic translations
– Requires the subject to respond to a signal by a predetermined number or code
– Blue stimulus light appears and the subject must press the first in a series of buttons; yellow stimulus light appears and a second set of responses is required, etc.
• This type of movement results in disproportionate slowing in older subjects
© 2007 McGraw-Hill Higher Education. All rights reserved.
Movement Speed in Adulthood• Last-in-first-out hypothesis
– Neural and muscular capability to perform simple movement acts or those that fall into the category of spatial transpositions, is developed early in life and appears to be somewhat resistant in aging
– More coordinated, goal-oriented, or complicated movements, such as the symbolic translations, are not developed until late in life and decline earlier
© 2007 McGraw-Hill Higher Education. All rights reserved.
Movement Speed in Adulthood• Other reasons for the decline
– Number of functional neurons and muscle fibers they innervate decline
– More intense neural stimulations are required to elicit response (threshold level increases)
– Older people are willing to sacrifice speed for accuracy
• Speed/accuracy trade off
– Older people are less willing to train using near-maximal explosive effort
© 2007 McGraw-Hill Higher Education. All rights reserved.
Is a Movement Decline Inevitable with Age?
• Movement decline does not have to begin as early or as abruptly as it does for many
• By taking an active role in daily habits, movement regression/decline can be delayed
• The decline can be avoided with compensatory strategies, exercise, and practice
© 2007 McGraw-Hill Higher Education. All rights reserved.
Is a Movement Decline Inevitable with Age?
• “Compensation for the movement decline to maintain high levels of performance can be achieved so that speed, strength, and endurance do not severely decline.”
© 2007 McGraw-Hill Higher Education. All rights reserved.
Is a Movement Decline Inevitable with Age?
• Paul Spangler knew that pacing is often an effective way to compensate for speed
• Until his death at age 95 yr, he was still running marathons
© 2007 McGraw-Hill Higher Education. All rights reserved.
Is a Movement Decline Inevitable with Age?
• Other forms of compensation– Long- and short-term anticipation of
movement• Short term – focusing on a player’s movement in
a game• Long term – getting enough rest before a game
– Speed/accuracy tradeoff• Commonly used by skilled athletes
– Older adults have higher expectations for their performances
© 2007 McGraw-Hill Higher Education. All rights reserved.
Effects of Exercise on the Movement Decline
• By staying active the movement decline can be delayed– Even in the physically frail, a
moderate exercise program can reverse movement decline
• Inactivity leads to more inactivity and a variety of biological changes
© 2007 McGraw-Hill Higher Education. All rights reserved.
Effects of Exercise on the Movement Decline
• A program of physical activity will lead to increased capacities of all the body’s systems
© 2007 McGraw-Hill Higher Education. All rights reserved.
Effects of Practice on the Movement Decline
• Practice of a specific movement activity is an effective way to postpone or avoid movement regression and improve specific movements
• Older adults show greater improvement with practice than do younger adults
© 2007 McGraw-Hill Higher Education. All rights reserved.
An active exercising lifestyle can postpone or avoid many types of movement decline
© 2007 McGraw-Hill Higher Education. All rights reserved.
ACSM Position Stand• Strongly supports regular exercise for
older adults• Exercise offsets numerous functional
declines– Muscle mass, flexibility, cardiovascular
endurance, strength• 10-30% increase in maximal endurance
levels (same as in young adults)
• Decrease in risk of many diseases– Heart disease, diabetes, osteoporosis
© 2007 McGraw-Hill Higher Education. All rights reserved.
ACSM Position Stand• June 1, 1998
POSITION STAND The Recommended Quantity and Quality of Exercise for Developing and Maintaining Cardiorespiratory and Muscular Fitness, and Flexibility in Healthy Adults
POSITION STAND Exercise and Physical Activity for Older Adults
• ACSM Position Stands
© 2007 McGraw-Hill Higher Education. All rights reserved.
ACSM Position Stand• Exercise may increase longevity
– By decreasing the incidence of disease
• Exercise improves….– Bone health– Postural stability– Reduction in number of falls– Preservation of cognitive ability– Reduction in depression– Enhanced feelings of self control and
efficacy
© 2007 McGraw-Hill Higher Education. All rights reserved.
Effects of Exercise on the Movement Decline
• Physical frailty is modifiable with low-intensity exercise
• Active older adult responses are similar to young active adults – Reaction time– Choice reaction time– Response time tasks
• Why reaction time improves
• Increase in blood flow– Improve brain function
• Arousing effect of exercise– Improve speed – May decrease accuracy
• Active muscles influence neurons
© 2007 McGraw-Hill Higher Education. All rights reserved.
Physical Activity Trends in Adulthood
• Most adults choose not to be active, but the trend is changing– 10% of adult populations from England,
Canada, Australia, and USA were aerobically active
• Aerobically active– “engaged in vigorous activities during
leisure time on an average of at least three occasions weekly for 20-30 minutes or more per occasion” (1994)
© 2007 McGraw-Hill Higher Education. All rights reserved.
Physical Activity Trends in Adulthood
• As many as a third of all people who are asked about their physical activity, fall into the “sedentary” category– Sedentarism is a lifestyle choice
• When older adults choose to be active, the activity usually requires less energy
• Men are usually involved in more vigorous activity
© 2007 McGraw-Hill Higher Education. All rights reserved.
Physical Activity and Mortality • A Danish study conducted a
longitudinal study beginning in 1964 on subjects who were age 50 yr
• 1999 – subjects were 85 yr• <1/3 lead sedentary life• Active elders demonstrated a lower
mortality, fewer heart attacks and hip fractures
• More independent life

© 2007 McGraw-Hill Higher Education. All rights reserved.
Sports Related Injuries• Consumer Product Safety
Commission (2000)– Sports related injuries increased in Baby
Boomers by 30% from 1991-1998• Due to greater participation
– 80 million people (30% of population)– $19 billion– Cycling and basketball accounted for
largest injury rate

© 2007 McGraw-Hill Higher Education. All rights reserved.
Sports Related Injuries• Popular sports with increased injuries
– Bicycling– Golf– Soccer– Basketball– Exercise - Running– Weightlifting– In-line skating

© 2007 McGraw-Hill Higher Education. All rights reserved.
Sports Related Injuries• Deaths
– Bicycling (290/year)• 2x rate seen in children• More children wear helmets than adults
– Swimming (67/year)– Skiing (7/year)
© 2007 McGraw-Hill Higher Education. All rights reserved.
Sports Related Injuries• Injuries in persons 65 yr or older
– Significant increase in injury from 1990-1996 of 54%
• Greater involvement
– Bicycle riding injuries increased 75%– Exercising injuries increased 173%
• Falling, tripping, strains
• Proper safety ear and proper precautions can reduce injuries in the elderly
© 2007 McGraw-Hill Higher Education. All rights reserved.
Teaching Movement Skill to the Older Adult
• Teachers of motor skill for the older adult should be trained professionals
• Currently, too few quality programs exist
© 2007 McGraw-Hill Higher Education. All rights reserved.
Teaching Movement Skill to the Older Adult
• Programs should– Consult current research on an older adult’s
needs– Provide strategies to motive older adults– Provide a program that is safe and secure
• Health problems; poor vision; hearing problems
– Consider the needs of belonging, affection, and identification of older adults
© 2007 McGraw-Hill Higher Education. All rights reserved.
Teaching Movement Skill to the Older Adult
• Other recommendations– When teaching, concentrate on
psychological readiness by• Maintaining eye contact• Standing near group• Address participants by name• Inform the participant about the
importance of learning a skill
© 2007 McGraw-Hill Higher Education. All rights reserved.
Teaching Movement Skill to the Older Adult
• Other recommendations– Teach appropriate attentional strategies– Teach a skill in the actual sequence in
which it will happen and under realistic circumstances
– Reduce speed and complexity of incoming information
– Recognize short-term memory deficits and slower recall abilities
© 2007 McGraw-Hill Higher Education. All rights reserved.
The World Health Organization Heidelberg Guidelines
• Guidelines for facilitating the development of strategies, policies, in population and community based intervention programs aimed at maintaining and/or increasing the level of physical activity for all older adults (1997)
© 2007 McGraw-Hill Higher Education. All rights reserved.
The World Health Organization Heidelberg Guidelines
• Evidence– Physical activity
improves health and can be fun
– Physical activity improves ADL and IADLs
– Physical activity must be regular and continuous
– Physical activity promotes well-being, physical and psychological health, and independent living
• Benefits– Physiological– Psychological– Social
• Societal reasons for physical activity– Cost of long-term
health care– Society can benefit
from the wisdom of older persons
© 2007 McGraw-Hill Higher Education. All rights reserved.
The World Health Organization Heidelberg Guidelines
• Promoting / facilitating increased activity– Influence health
policy at all levels– Involve all those who
work with older adults
• Motivating factors– Fun!– Companionship– Independence– Improves health
• Barriers to physical activity– Lack of knowledge of
activity in older adults– Lack of support
© 2007 McGraw-Hill Higher Education. All rights reserved.
The World Health Organization Heidelberg Guidelines
• Recommended parameters– Make programs affordable– Expensive equipment and large
spaces are not needed– Individual and group activities– Regular, daily activities
© 2007 McGraw-Hill Higher Education. All rights reserved.





























