Embed Size (px)
Citation preview

1
Acute Kidney Injury

2
I. Anatomy
II. Epidemiology
III. Mortality & Cost
IV. Diagnosis, Assessment, & Management
V. Treatment
VI. Limitations and Unmet Clinical Needs
Outline: Acute Kidney Injury

3
Anatomy

4
• The urinary tract consists of kidneys, adrenal glands, ureters, bladder, urethra and all associated blood vessels.
Renal System Anatomy
• Kidneys are often donated.
• It is not uncommon for an individual to be able to live without one kidney.
KIDNEYS
URETERS
BLADDERURETHRA
ADRENAL GLANDS
4

5
• The kidney is supplied with blood by the renal artery.
Kidney Anatomy
• Each renal artery branches and eventually the blood feeds into the medulla and the nephrons, or functional units of the kidney.
RENAL PELVIS
CORTEX
RENAL MEDULLA
RENAL ARTERY
RENAL VEIN
URETER
5

6
• A tubular structure called the nephron filters blood to form urine.
Nephron
• Blood is filtered through the glomerulus into the Bowman's capsule which empties into a tubule that is also part of the nephron.
• A glomerulus and its surrounding Bowman's capsule constitute a renal corpuscle, the basic filtration unit of the kidney.
• The glomerulus is a group of capillaries that perform the first step of filtering blood.
URINE FORMATION
Blood Flow
Afferent Arteriole
Efferent Arteriole
EXCRETION
Renal Tubule
FILTRATION
NEPH
RO
N
Glomerulus
Additional Waste
Solutes and Waste
SECRETION
REABSORPTION Renal Corpuscle

7
Epidemiology

8
Acute Kidney Injury
• Acute kidney injury (AKI) is a rapid loss of kidney function including:
– Rapid time course (less than 48 hours)
– Rise in serum creatinine
– Reduction in urine output (oliguria)
Mehta RL, Kellum JA, Shah SV et al. Crit Care. 2007;11(2):R31.

9
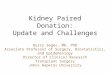
Number of AKI Hospitalizations: 1979 to 2002
National Center for Health Statistics, National Hospital Discharge Survey.Centers for Disease Control and Prevention.
700,000
600,000
500,000
400,000
300,000
200,000
100,000
45,000,000
40,000,000
35,000,000
25,000,000
15,000,000
30,000,000
20,000,000
10,000,000
5,000,000
001980 1982 1984 1986 1988 19981996199419921990 2000 2002
All Hospitalizations AKI

10
A Dramatic Rise in Kidney Injury
60
50
40
30
20
10
0
Rat
e (P
er 1
0,00
0 Po
pula
tion)
Year
1980 1985 1990 1995 2000 2005
Total (all types)
Chronic
Unspecified
Acute
Adapted from International Classification of Diseases, 9 th Rev., Center for Disease Control and Prevention. 2008.

11
Patients at Risk for Kidney Injury
• Adults with diabetes or hypertension are at an increased risk of developing chronic kidney disease (CKD) or injury.
• Other risk factors include cardiovascular disease, obesity, elevated cholesterol, and a family history of CKD.
National Chronic Kidney Disease Fact Sheet 2010. U.S. Department of Health and Human Services. Centers for Disease Control and Prevention.
Overall
20-44 Years45-65 Years
65+ Years
MaleFemale
Non-Hispanic WhiteNon-Hispanic Black
Mexican American
0 10 20 30 40 50
Percent (%)

12
AKI Risk Factors
• Sepsis
• Age > 65 years
• Presence of infection
• Low cardiac output
• Major surgery
• Trauma
• Cancer
• Hypervolemia (fluid overload)
• Cirrhosis
• Certain medications
Dennen P, Douglas IS, Anderson R. Crit Care Med. 2010;38:261-75.Kidney Disease: Improving Global Outcomes (KDIGO). 2008.

13
AKI Causes
Environmental exposures • Trauma• Medications
Sepsis • Increases LOS• 32.4% of AKI
Ischemia • Inflammatory mediators in tubules
Physiological • Pre-renal• Intrinsic• Post-renal
Unknown • Consider renal biopsy

14
HOSPITAL LENGTH OF STAY ICU LENGTH OF STAY
AKI Causes: Sepsis
Bagshaw SM, George C, Bellomo R et al. Crit Care. 2008;12:R47.
Sepsis accounted for 32.4% of all hospitalized patients with AKI.
Over 42% of all sepsis diagnoses also had an AKI diagnosis.
Sepsis is the most common cause of AKI in the ICU.
Day
s
Day
s
RIFLE Category RIFLE Category
None Risk Injury FailureNone Risk Injury Failure
6
5
4
3
2
1
0
25
20
15
10
5
0
Non-Septic AKISeptic AKI
Non-Septic AKISeptic AKI

15
INFLAMMATORY MEDIATORS OF ISCHEMIC AKI
AKI Causes: Ischemia
• Ischemia can lead to AKI through the induction of inflammatory mediators that induce cell death in the kidney tubules– Reactive oxygen species
– Cytokines
– Chemokines
– Macrophages
Adapted from Aiello S and Noris M. Kidney Int. 2010;78:1208-10.
Lymphocytes
Neutrophils
Chemokines
Macrophages
ROS
Vasoconstrictors
Dendritic Cells
Interstitium
Endothelium
Tubular Urinary Lumen
Proximal Tutules
Adhesion Molecules
Apoptosis, Cell Injury, Oxidative Stress

16
PRE-RENAL
AKI Causes: Physiological
• Low blood pressure
• Low blood volume
• Heart failure
• Arterial changes leading to kidney
• Glomerulonephritis
• Acute tubular necrosis (ATN)
• Acute interstitial nephritis (AIN)
• Benign prostatic hyperplasia
• Kidney stones
• Obstructed urinary catheter
• Bladder stone
• Bladder, ureteral or renal malignancy
Thadhani R, Pascual M, Bonventre JV. N Engl J Med. 1996;334(22):1448-60.
Decreased blood flow to the kidney
INTRINSIC (RENAL)
Damage to the kidney itself
POST-RENAL
Urinary tract obstruction

17
CONSIDER RENAL BIOPSY
There are cases of AKI with no known cause
Uncertain or competing diagnoses where treatment differs with definitive diagnosis
Young patients
AKI Causes: Unknown

18
GFR assessed from measured or estimated GFR. Estimated GFR does not reflect measured GFR in AKI as accurately as in CKD. Kidney damage assessed by pathology, urine, or blood markers, imaging, and – for CKD – presence of a kidney transplant. AKD, acute kidney diseases and disorders; AKI, acute kidney injury; CKD, chronic kidney disease; GFR, glomerular filtration rate; NKD, no known kidney disease; SCr, serum creatinine.
Definitions of AKI, CKD, and AKD
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl 2012; Volume 2, Issue 1:1–126.
Functional Criteria Structural Criteria
AKI Increase in SCr by 50% within 7 days, OR Increase in SCr by 0.3 mg/dL (26.5 μmol/L) within 2 days OR oliguria
No criteria
CKD GFR < 60 mL/min for > 3 months Kidney damage > 3 months
AKD AKI, OR GFR < 60 mL/min for < 3 months, ORDecrease in GFR by ≥ 35% or increase in SCr by > 50% for < 3 months
Kidney damage for < 3 months
NDK GFR ≥ 60 mL/minStable SCr
No damage

19
Chronic Kidney Disease
• CKD is a slow loss of kidney function over time.
STAGE CHARACTERISTICS
Slightly diminished function; kidney damage* with normal or relatively high GFR (≥ 90 mL/min/1.73 m2).
Mild reduction in GFR (60–89 mL/min/1.73 m2) with kidney damage*.
Moderate reduction in GFR (30–59 mL/min/1.73 m2).
Severe reduction in GFR (15–29 mL/min/1.73 m2). Preparation for renal replacement therapy.
Established kidney failure (GFR <15 mL/min/1.73 m2), or permanent renal replacement therapy.
* Kidney damage is defined as pathological abnormalities or markers of damage, including abnormalitiesin blood or urine test or imaging studies.
• Many elderly patients have CKD despite creatinine values that are “normal” (~1.0).
1
2
3
4
ESRD

20
• AKI can occur on top of CKD– Many patients have CKD at baseline
– AKI can increase severity of CKD
CKD vs. AKI
Adapted from Dear JW and Yuen PST. Kidney Int. 2008;74:7-9.
CKD
AKI
ESRDESRD
CKD

21
AKI With or Without Chronic Kidney Disease
• AKI can be diagnosed in patients with chronic kidney disease (CKD).
• AKI can also increase the incidence of CKD.
Cerda´ J, Lameire N, Eggers P et al. Clin J Am Soc Nephrol. 2008;3:881-6.
Ren
al F
unct
ion
100
80
60
40
20
0
AKI to ESRD
AKI on CKD
AKI to CKD
Full Recovery
Insult
Time

22
Cumulative Incidence of CKD by Exposure Status (Recovered AKI vs. Controls) in Patients With Normal Baseline Kidney Function
Bucaloiu ID, Kirchner HL, Norfolk ER et al. Kidney Int. 2012 Mar;81(5):477-85.
1.0
0.8
0.6
0.4
0.2
0
Prop
ortio
n of
Pat
ient
s W
ithou
t CK
D
Months Since Index Hospitalization
0 6 12 18 24 30 36 42 48 54 60 66 72
AKIControls

23
Additional Comorbid Pathologies
• Diabetes mellitus
• Ischemic heart disease
• Congestive heart failure
• Hypertension
Bagshaw SM. Nephrol Dial Transplant. 2008;23(7):2126-8.
MOST COMORBID CONDITIONS ARE INFLAMMATORY OR CARDIOVASCULAR
MOST COMORBID CONDITIONS ARE INFLAMMATORY OR CARDIOVASCULAR

24
Mortality & Cost

25
AKI Increases Hospital Length of Stay and Associated Costs
AKI = INCREASING COST AND LENGTH OF STAY

26
AKI Associated Length of Stay (LOS)
Barrantes F, Tian J, Vazquez R, Amoateng-Adjepong Y et al. Crit Care Med. 2008;36:1397-403.
OUTCOME TOTAL AKI NON-AKI P VALUE
RRT rate, N (%) 18 (4.7) 18 (15.0) 0 (0.0) < 0.01
Hospital LOS, Median
Survived 8.0 14.0 7.0 < 0.01
Died 11.0 14.0 9.0 0.25
Total 9.0 14.0 7.0 < 0.01
MICU LOS, Median
Survived 3.0 6.0 3.0 < 0.01
Died 5.0 5.0 4.5 0.71
Total 3.0 5.0 3.0 < 0.01
RRT, renal replacement therapy; MICU, medical intensive care unit; NROF, non-renal organ failure.

27
OUTCOME TOTAL AKI NON-AKI P VALUE
Mortality, N (%)
≥ 2 NROFs 66 (31.9) 41 (50.6) 25 (19.8) < 0.01
< 2 NROFs 32 (18.4) 14 (35.8) 18 (13.3) < 0.01
1 NROF 19 (15.8) 9 (34.6) 10 (10.6) < 0.01
2 NROFs 25 (22.5) 16 (44.4) 9 (12.0) < 0.01
3 NROFs 27 (40.9) 19 (59.4) 8 (23.1) < 0.01
4 NROFs 11 (44.0) 6 (54.5) 5 (35.7) < 0.01
Total 98 (25.7) 55 (45.8) 43 (16.4) < 0.01
Barrantes F, Tian J, Vazquez R, Amoateng-Adjepong Y et al. Crit Care Med. 2008;36:1397-403.
RRT, renal replacement therapy; MICU, medical intensive care unit; NROF, non-renal organ failure.
AKI Associated Length of Stay (LOS)

28
AKI Cost by Creatinine Level
N = 2892, 1236, 351, 105, 4060, 1967, 714, 352, and 1160 for respective AKI criteria. Results are relative to those without the change indicated. Multivariable analyses were adjusted for age, gender, DRG weight, and ICD-9-CM categories of cardiovascular, respiratory, malignant, and infectious diseases.
Chertow GM, Burdick E, Honour M et al. J Am Soc Nephrol. 2005;16:3365–70.
↑ SCr ≥ 0.5 + baseline SCr < 2.0 mg/dl

29
AKI Costs Can Increase Following Surgery
No AKI Mild AKI Moderate AKI Severe AKI
RIFLE Criteria None R I F
Mortality (%) 2.3 5.1 12.9 26.0
ICU Costs $13,836 $21,775 $28,872 $49,328
ICU Length of Stay (Days)
1.4 2.4 3.5 5.4
Dasta JF, Kane-Gill SL, Durtschi AJ et al. Nephrol Dial Transplant. 2008;23:1970-74.
INCREASING SEVERITY FOLLOWING CARDIAC SURGERY

30
Mortality Associated With Changes in SCr
Criterion Unadjusted OR (95% CI)
Age- and Gender-Adjusted OR (95%
CI)Multivariable OR
(95% CI)b
Area under ROC Curve
↑ SCr ≥ 0.3 mg/dl 6.9 (5.2 to 9.0) 6.6 (5.0 to 8.7) 4.1 (3.1 to 5.5) 0.84
↑ SCr ≥ 0.5 mg/dl 11.1 (8.7 to 14.2) 10.6 (8.3 to 13.6) 6.5 (5.0 to 8.5) 0.86
↑ SCr ≥ 1.0 mg/dl 19.9 (15.1 to 26.1) 19.0 (14.4 to 25.0) 9.7 (7.1 to 13.2) 0.84
↑ SCr ≥ 2.0 mg/dl 36.4 (24.3 to 54.6) 37.7 (25.0 to 56.9) 16.4 (10.3 to 26.0) 0.83
↑ SCr by 25% 4.0 (3.0 to 5.2) 3.9 (3.0 to 5.2) 2.0 (1.2 to 3.9) 0.83
↑ SCr by 50% 5.9 (4.6 to 7.5) 5.8 (4.6 to 7.5) 4.4 (3.4 to 5.7) 0.84
↑ SCr by 100% 8.9 (6.9 to 11.4) 9.2 (7.1 to 11.8) 6.5 (4.9 to 8.6) 0.84
↑ SCr by 50% to a minimum peak of 2.0 mg/dl
16.9 (12.8 to 22.3) 15.9 (12.0 to 21.0) 7.9 (5.8 to 10.9) 0.84
↑ SCr ≥ 0.5 mg/dl with baseline SCr < 2.0 mg/dl or ↑ SCr ≥ 1.0 mg/dl with baseline SCr ≥ 2.0 and < 5.0 mg/dl
11.0 (8.6 to 14.0) 10.5 (8.2 to 13.4) 6.5 (5.0 to 8.5) 0.86
N = 2892, 1236, 351, 105, 4060, 1967, 714, 352, and 1160 for respective AKI criteria. Results are relative to those without the change indicated. Multivariable analyses were adjusted for age, gender, DRG weight, and ICD-9-CM categories of cardiovascular, respiratory, malignant, and infectious diseases.
Chertow GM, Burdick E, Honour M et al. J Am Soc Nephrol. 2005;16:3365–70.

31
ICU MORTALITY2ICU MORTALITY1
Morbidity and Mortality
60
50
40
30
20
10
0
60
50
40
30
20
10
0No AKI AKI Sepsis Sepsis +
AKI
1. Clermont G, Acker CG, Angus DC et al. Kidney Int. 2002;62(3):986-96.2. Hoste EA, Lameire NH, Vanholder RC et al. J Am Soc Nephrol. 2003;14(4):1022-30.
Perc
ent
Perc
ent

32
Diagnosis, Assessment, & Management

33
Traditional Methods of Measurement

34
15 60
Normal
1200
Kidney Failure Kidney Disease
Creatinine and GFR
• Creatinine– Breakdown product of creatine
– Exclusively filtered out by the kidneys (no resorption)
– Estimates renal function
• GFR– Glomerular filtration rate
– Volume of creatinine cleared per unit time
– Some equations also take age and sex into account
eGFR Value

35
AKI Diagnosis
Serum Creatinine (mg/dL) Diagnosis AKI
CaseBaselin
eDay
1Day
2Day 3
Day 7
Criterion 1:
50% from Baseline
Criterion 2: ≥ 0.3 mg/dL
Rise in ≤ 48 Hours
A 1.0 1.3 1.5 2.0 1.0 Yes Yes
B 1.0 1.1 1.2 1.4 1.0 No Yes
C 0.4 0.5 0.6 0.7 0.4 Yes No
D 1.0 1.1 1.2 1.3 1.5 Yes No
E 1.0 1.3 1.5 1.8 2.2 Yes Yes
F ? 3.0 2.6 2.2 1.0 Yes No
G ? 1.8 2.0 2.2 1.6 ? Yes
H ? 3.0 3.1 3.0 2.9 ? No
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl 2012; Volume 2, Issue 1:1–126.

36
Estimated Baseline SCr
Age (Years) Black Males (mg/dL
[μmol/L])
Other Males (mg/dL
[μmol/L])
Black Females (mg/dL
[μmol/L])
Other Females (mg/dL
[μmol/L])
20-24 1.5 (133) 1.3 (155) 1.2 (106) 1.0 (88)
25-29 1.5 (133) 1.2 (106) 1.1 (97) 1.0 (88)
30-39 1.4 (124) 1.2 (106) 1.1 (97) 0.9 (80)
40-54 1.3 (115) 1.1 (97) 1.0 (88) 0.9 (80)
55-65 1.3 (155) 1.1 (97) 1.0 (88) 0.8 (71)
> 65 1.2 (106) 1.0 (88) 0.9 (80) 0.8 (71)
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl 2012; Volume 2, Issue 1:1–126.

37
AKI Staging
Serum Creatinine (mg/dL)
CaseBaselin
eDay
1Day
2Day 3
Day 7
Reference Creatinine
Max AKI Stage
A 1.0 1.3 1.5 2.0 1.0 1.0 2
B 1.0 1.1 1.2 1.4 1.0 1.0 1
C 0.4 0.5 0.6 0.7 0.4 0.4 1
D 1.0 1.1 1.2 1.3 1.5 1.0 1
E 1.0 1.3 1.5 1.8 2.2 1.0 2
F ? 3.0 2.6 2.2 1.0 1.0 3
G ? 1.8 2.0 2.2 1.6 ? ≥ 1
H ? 3.0 3.1 3.0 2.9 ? ?
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl 2012; Volume 2, Issue 1:1–126.

38
RRT, renal replacement therapy; MICU, medical intensive care unit; NROF, non-renal organ failure.
GFR/SCr Algorithm
Is GFR decreased or is serum creatinine increased?
Is SCr increasing or GFR decreasing?
Does the decrease in GFR or increase in SCr resolve within 3 months?
Yes > 3 monthsNoYes < 3 months
NKD AKD without AKI AKI AKD
without AKI AKIAKD without AKI
CKD + AKD without AKI
CKD + AKICKD
No Yes-D Yes-I
No Yes-D Yes-I
No Yes-D Yes-I
Yes-D, change in SCr meets AKD criteria but not AKI criteria
CKD worse
CKD stable
CKD worse
CKD stable
CKD new NKD CKD
new NKD
No Yes No Yes No Yes No Yes
AKD, acute kidney disease/disorder; AKI, acute kidney injury; CKD, chronic kidney disease; GFR, glomerular filtration rate; NKD, no known kidney disease; SCr, serum creatinine
GFR/SCr
NKD AKD CKD
CKD + AKD without AKI
CKD + AKI
AKD without AKI AKI
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl 2012; Volume 2, Issue 1:1–126.

39
GFR Over the Course of AKI
Injury
Diagnosis (Future with Biomarkers)
Diagnosis (2011)
Prerenal Azotemia
Time (Days)
GFR
Maladaptive Response
Repair Response
• Prerenal azotemia can progress to kidney injury.
• After the initial sharp drop in GFR, there is further injury from secondary effects.
• Early immune response can be maladaptive and contribute to further injury.
• After injury, GFR does not recover immediately after return of renal blood flow.
Winterberg PD and Lu CY. Am J Med Sci. 2011 Aug 3.

40
Other Methods of Diagnosis
• Serum– Urea nitrogen
• Pathology– Kidney biopsy
• Imaging– Ultrasound, CT, MRI, nuclear renal scan
• Urine– Fractional excretion (sodium, urea), protein/creatinine ratio,
sediment (casts, WBCs, eosinophils), enzyme activity

41
KDIGO is a global non-profit foundation dedicated to improving the care and outcomes of kidney disease patients worldwide.
Assembled working group of eighteen thought leaders to establish global clinical practice guidelines for AKI
New guidelines just published.
Physicians Can Take Action With Early Assessment of AKI
KDIGO Initiative to Set Guidelines KDIGO AKI Guidelines
41
High Risk 1 2 3
Avoid subclavian catheters
Consider ICU admission
Consider Renal Replacement Therapy
Check for changes in drug dosing
Consider Renal Replacement Therapy
Check for changes in drug dosing
Consider alternatives to radiocontrast procedures
Avoid hyperglycemia
Monitor serum creatinine and urine output
Consider functional hemodynamic monitoring
Ensure volume status and perfusion pressure
Discontinue all nephrotoxic agents when possible
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl 2012; Volume 2, Issue 1:1–126.

42
Physicians Can Take Action With Early Assessment of AKI
42
KDIGO AKI Guidelines
High Risk 1 2 3
Avoid subclavian catheters if possible
Consider ICU admission
Consider Renal Replacement Therapy
Check for changes in drug dosing
Consider Renal Replacement Therapy
Check for changes in drug dosing
Consider alternatives to radiocontrast procedures
Avoid hyperglycemia
Monitor serum creatinine and urine output
Consider functional hemodynamic monitoring
Ensure volume status and perfusion pressure
Discontinue all nephrotoxic agents when possible
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl 2012; Volume 2, Issue 1:1–126.

43
Current Thinking
• Focus is now on inflammation-mediated organ injury in addition to renal blood flow.
• AKI leads to progressive injury and a spectrum of functional kidney problems.– Serial AKI leading to CKD
• Injury vs. decreased filtration
• New terminology– AKI rather than acute renal failure (ARF)

44
• The care of patients with acute kidney injury is very poor.
Key Findings in Assessment of AKI Care
Hussein HK, Lewington AJP, Kanagasundaram NS. Brit J Hosp Med. 2009;70:M104–7.Stewart JAD. Brit J Hosp Med. 2009;70(7):372-3.
• Acutely unwell patients are not being recognized.
• Education about acute kidney injury must improve.
• Patients are dying from predictable and avoidable renal failure.
• The failings in the care of patients are largely clinical.– Poor assessment of risk
– Inadequate basic intervention
– Missed complication

45
Deficiencies in the Diagnosis and Care of AKI Patients
69%
31%
Care of AKI patient
Good Practice
Room for Improvement
Over 60% had room for improvement
31%
34%
35%
AKI outcome
UnavoidableAKI
Avoidable AKI
Over 30% had avoidable AKI
Not Specified
54%46%
AKI risk assessment
AdequateInadequate
> 50% had inadequate risk assessment
43%57%
Delay in recognition of AKI
AcceptableUnacceptable
Delay
43% had unacceptable recognition delay
Acute Kidney Injury: Adding Insult to Injury. NCEPOD. 2009.
FINDINGS FOR ADMITTED PATIENTS THAT DIED FROM HOSPITAL ACQUIRED AKI

46
Lack of AKI Recognition Resulted in Inadequate Consultations
31%
69%
Referral to nephrologist
No
Yes
Only 31% referred to nephrologist
21%
79%
Was referral to nephrologist timely?
1 in 5 are referred late
Yes
No
21%
79%
Patients that would have benefitedfrom critical care
Several should have been moved to critical care
No
Yes20%
80%
Need for nephrologist in group not referred
Yes
Another 20% should have been referred
No
Acute Kidney Injury: Adding Insult to Injury. NCEPOD. 2009.
FINDINGS FOR ADMITTED PATIENTS THAT DIED FROM COMMUNITY AND HOSPITAL ACQUIRED AKI

47
Many Omissions in AKI Management
Acute Kidney Injury: Adding Insult to Injury. NCEPOD. 2009.

48
Classification and Assessment
• RIFLE– Classifies AKI into three levels of severity (Risk, Injury, and Failure)
and includes two clinical endpoints (Loss and End-stage renal disease)
– Severity is determined from the increase in CR and decrease in UO
Bellomo R, Ronco C, Kellum JA et al. Crit Care. 2004;8(4):R204–12.
No AKI
Risk (Minor AKI)Cr x 1.5 or GFR decreases > 25% or UO < 0.5 ml/kg/hr x 6 hr
Injury (Moderate AKI)CR x 2.0 or GFR decreases > 50% or < 0.5 ml/kg/hr x 12 hr
Failure (Severe AKI)Cr x 3.0 or GFR decreases > 75% or Cr ≥ 4 mg/dl or < 0.3 ml/kg/hr x 24 hr or anuria x 12 hr
LossOn dialysis > 1 month
ESRDOn dialysis > months

49
Classification and Assessment
• Acute Kidney Injury Network (AKIN)– Stage 1 is similar to RIFLE-R but includes abrupt reduction in function.
– RIFLE-I and F are the same as stages 2 and 3.
– Stage 3 includes patients who need any renal replacement therapy.
No AKI
Stage 1Cr x 1.5 or ≥ 0.3 mg/dl or UO < 0.5 ml/kg/hr x 6 hr
Stage 2CR x 2.0 or UO < 0.5 ml/kg/hr x 12 hr
Stage 3Cr x 3.0 or UO < 0.3 ml/kg/hr x 24 hr or anuria x 12 hr
Mehta RL, Kellum JA, Shah SV et al. Crit Care. 2007;11(2):R31.
NOT in AKIN classification
NOT in AKIN classification

50
Classification and Assessment
• Kidney Disease: Improving Global Outcomes (KDIGO)– Similar to AKIN
– Adds values to creatinine levels as well as fold increase
– Stage 3 also includes patients who need renal replacement therapy.
No AKI
Stage 1Cr ≥ 26 μmol/L within 48 hrs or ≥ 1.5 to 1.9 or UO < 0.5 mL/kg/hr for > 6 hr
Stage 2CR ≥ 2 to 2.9 or UO < 0.5 ml/kg/hr x 12 hr
Stage 3Cr ≥ 354 μmol/L or ≥3 or UO < 0.3 ml/kg/hr x 24 hr or anuria x 12 hr
NOT in KDIGO classification
NOT in KDIGO classification
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl 2012; Volume 2, Issue 1:1–126.

51
Renal Disease Landscape
Renal disease landscape developed at the 2006 Acute Kidney Injury Network Congress in Vancouver, British Columbia, Canada. AKI, acute kidney injury; R, RIFLE risk (AKI stage I); I, RIFLE injury (AKI stage II); F, RIFLE failure (AKI stage III); AKD, acute kidney disease; ARF, acute renal failure; RRT, renal replacement therapy; CKD, chronic kidney disease; ESRD, end-stage renal disease.
Kellum JA. Crit Care Med. 2008;36[Suppl]:S141–5.
StagesI II III IV V
CKDAKD
I (R)
II (I)
III (F)
?
Biomarkers?
Exists for < or > 90 Days
Fulfills Criteria within 48 Hours?
RRT
“ARF”
Dialysis
ESRDAKI

52
The concept of AKI includes both volume-responsive and volume-unresponsive conditions.
Conceptual Model for Development and Clinical Course of AKI
High Risk
Volume Responsive AKI Volume Unresponsive AKI
Hypovolemia
Hypervolemia
Therapeutic Window
Kidney Function
Eurolemia
Biomarkers
Mortality
TraditionalSensitive
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl 2012; Volume 2, Issue 1:1–126.

53
• Kidney damage is not required for diagnosis of AKI.
Markers of Kidney Damage in AKD and CKD
Markers AKD CKD
Pathology X X
Urinary markers
RBC/casts X X
WBC/casts X X
RTE/casts X X
Fine and coarse granular casts X X
Proteinuria X X
Blood markers (tubular syndromes) X X
Imaging
Large kidneys X X
Small kidneys - X
Size discrepancy - X
Hydronephrosis X X
Cysts X X
Stones X X
History of kidney transplantation - XAKD, acute kidney diseases and disorders; CKD, chronic kidney disease; RBC, red blood cells; RTE, renal tubular epithelial cells; WBC, white blood cells.
• In the presence of AKI, findings of kidney damage do not indicate a separate AKD diagnosis.
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl 2012; Volume 2, Issue 1:1–126.

54
Treatment

55
Treatment Options
• Treatment options are limited– Fluid therapy
– Vasopressors or inotropes
– Treatment of underlying sepsis
– Renal replacement therapy
• Further limited by inadequate diagnostic tools

56
Dialysis Solution
Waste Fluid
Peritoneal Catheter
External Catheter
Renal Replacement Therapy
• Hemodialysis
• Peritoneal dialysis
• Hybrid therapies– Sustained low-efficiency dialysis
• Kidney transplantation
ArteryVein
Blood from Dialysis Machine
Blood to Dialysis MachineGraft

57
Dialysis
• Intermittent renal replacement therapy (IRRT)– Less than 24 hours in each 24 hour period
– Two to seven times per week
• Continuous renal replacement therapies (CRRT)– Continuous without any interruption throughout each day
IRRT CRRT
Dwell
Volu
me
Time
Outflow
Inflow
Volume
Time (Minutes)
Residual Volume
0 15 30 45 60
[Inflow = Outflow]
Last Drain
Tota
l Exc
hang
e Vo
lum
e (V
ip)

58Vesconi S, Cruz DN, Fumagalli R et al. Crit Care. 2009;13(2):R57.
Dose of RRT and Mortality in AKI
TOTAL CRRT
< 35 ml/kg/hour ≥ 35 ml/kg/hour P
Length of ICU stay (days) 13 (6.5 to 26) 15 (9 to 28) 8 (4 to 18) < 0.001
Patients who survived 19 (11 to 32) 19.5 (12 to 33.5) 15 (8 to 26) 0.063
Patients who died 10 (4 to 19) 12 (6 to 20) 4.5 (3 to 9.5) < 0.001
Duration of MV (days) 10 (4 to 19) 12 (5 to 21) 5 (2.5 to 13) < 0.001
Patients who survived 14 (4.5 to 22) 14 (5 to 24) 7 (4 to 17) 0.031
Patients who died 8.5 (3 to 17) 10 (5 to 18) 4 (2 to 9.5) < 0.001
TOTAL IRRT
< 6 sessions/week ≥ 6 sessions/week P
Length of ICU stay (days) 14 (6.5 to 23) 18 (15 to 31) 9.5 (6 to 18) 0.023
Patients who survived 11 (6 to 20) 18 (13 to 35) 8 (5.5 to 14) 0.008
Patients who died 17 (12 to 23) 18 (17 to 23) 15 (12 to 22) 0.597
Duration of MV (days) 8 (1 to 17) 14 (5 to 21) 6 (0 to 14) 0.030
Patients who survived 5 (0 to 13) 12 (3 to 24) 2.5 (0 to 10) 0.026
Patients who died 17 (11 to 21) 18 (17 to 21) 14 (8 to 18) 0.252

59
Limitations & Unmet Needs

60
Serum Creatinine
• Gold standard, but far from ideal
• Not sensitive to kidney insults that don’t affect filtration
• Creatinine is affected by non-renal factors:– Protein intake
– Muscle mass
– Age
– Race
– Sex
• In AKI it takes 24-48 hours for serum creatinine to rise.– As much as 50% of kidney function can be lost in that time

61
Urine Output
• May be misleading
Legrand M and Payen D. Ann Intensive Care. 2011;1:13.
• A minimum of 6 hours must pass to determine urine output.
• Nonsustained decreases of urine output do not necessarily imply decreased GFR.– Can represent a physiological
renal adaptation for homeostasis

62
NO. OF PATIENTS
REFERENCE TP FP FN TN NGAL CUTOFF (NG/ML)
SENSITIVITY (%; 95% CI)
SPECIFICITY (%; 95% CI)
Mishra et al, 2005 (p) 14 3 6 48 > 25 70.0 (45.7-87.2) 94.1 (82.8-98.5)
Mishra et al, 2005 (u) 20 1 0 50 > 50 100.0 (80.0-100.0) 98.0 (88.2-99.9)
Wagener et al, 2006 11 23 5 42 > 400 68.8 (41.5-87.9) 64.6 (51.7-75.8)
Dent et al, 2007 38 5 7 73 > 150 84.4 (69.9-93.0) 93.6 (85.0-97.6)
Zappitelli et al, 2007 12 7 4 16 > 10 75.0 (47.4-91.7) 69.6 (47.0-85.9)
Hirsch et al, 2007 (p) 8 1 3 79 >100 72.7 (39.3-92.7) 98.8 (92.3-99.9)
Hirsch et al, 2007 (u) 8 0 3 80 > 100 72.7 (39.3-92.7) 100.0 (94.3-100.0)
Wagener et al, 2008 44 172 24 186 > 450 64.7 (52.1-75.6) 52.0 (46.7-57.2)
Bennett et al, 2008 78 8 21 89 >150 78.8 (69.2-86.1) 91.8 (83.9-96.1)
Ling et al, 2008 10 8 3 19 -- 76.9 (46.0-93.8) 70.4 (49.7-85.5)
Koyner et al, 2008 (p) 8 13 10 41 > 280 44.4 (22.4-68.7) 75.9 (62.1-86.1)
Koyner et al, 2008 (u) 12 19 6 35 > 550 66.7 (41.2-85.6) 64.8 (50.6-77.0)
Nickolas et al, 2008 20 16 3 502 > 80 87.0 (65.3-96.6) 96.9 (94.9-98.2)
Lima et al, 2008 5 12 1 34 -- 83.3 (36.5-99.1) 73.9 (58.6-85.3)
Wheeler et al, 2008 19 74 3 47 > 140 86.4 (64.0-96.4) 38.8 (30.3-48.2)
Xin et al, 2008 2 8 1 22 > 250 66.7 (12.5-98.2) 73.3 (53.8-87.0)
Cruz et al, 2009 47 46 17 191 > 150 73.4 (60.7-83.3) 80.6 (74.9-85.3)
Makris et al, 2009 (CIN) 5 6 1 44 60 90.0 (54.1-99.5) 88.0 (75.0-95.0)
Makris et al, 2009 (ICU) 6 7 1 17 > 190 85.7 (42.0-99.3) 70.8 (48.8-86.6)
Constantin et al, 2009 43 1 9 35 > 155 82.7 (69.2-91.3) 97.2 (83.8-99.9)
Tuladhar et al, 2009 (p) 7 13 2 28 > 420 77.8 (40.2-96.1) 68.3 (51.8-81.4)
Tuladhar et al, 2009 (u) 8 9 1 32 > 390 88.9 (50.7-99.4) 78.1 (62.0-88.9)
Haase-Fielitz et al, 2009 18 17 5 60 > 150 78.3 (55.8-91.7) 77.9 (66.8-86.3)
Sensitivity and Specificity of Studies for NGAL to Predict AKI
Haase M, Bellomo R, Devarajan R et al. Am J Kidney Dis. 2009;54:1012-24.

63
BIOMARKER NEEDS
AKI Biomarkers
BIOMARKERS
• IL-18
• NGAL
• KIM1
• L-FABP
• Cystatin C
• Early detection
• Differential diagnosis
• Prognosis
MOST AKI MARKERS ARE NOT FDA APPROVED
AND AVAILABLE ONES DO NOT MEET CURRENT CLINICAL NEEDS.

64
Possible Utility of New Biomarkers
• Early detection
• Differential diagnosis
• Prognosis– Predict need for dialysis
– Reversibility
– Risk of death

65
Unmet Clinical Needs
• AKI is difficult to assess.
• Mortality is high and it carries a very high cost.
• Currently available methodologies and biomarkers are not meeting clinical needs.
• New biomarkers are on the horizon to assistwith AKI risk assessment.