Embed Size (px)
Citation preview
(Revised 05/18)
Lower Columbia College Head Start/EHS/ECEAP
Eligibility, Recruitment, Selection, Enrollment, Attendance (ERSEA)
Table of Contents
1. Application
a. Head Start/Early Head Start/ECEAP Application (English & Spanish) (Revised 05/18)
b. Enrollment Postcard (English & Spanish) (Revised E: 08/10; S: 03/10)
c. No Income Statement (Revised 05/18)
d. Release of Confidential Information (English & Spanish) (Revised 05/17)
d1. Parent/Guardian Permission to Reveal or Obtain Confidential Information Procedure (Rev. 05/17)
e. Change of Status Form (Revised 07/14)
f. Adult Permission to Reveal or Obtain Confidential Information (Revised 11/13)
2. Attendance
a. Attendance and Meal Count Instructions (Revised 03/18)
b. Attendance and Meal Count Form (ChildPlus Report 2315)
b1. Daily Infant Meal Record (Revised 09/17)
c. Attendance Policy and Procedure (Revised 08/17)
d. (Vacant)
e. EHS Attendance Policy and Procedure (Revised 06/16)
e1. EHS Attendance Tracking Form (Revised 12/13)
e2. EHS Prenatal Attendance Tracking Form (Revised 12/13)
f. 3-5 Child Attendance Letter (English & Spanish) (Revised 07/10)
f1. EHS Home Base Child Attendance Letter (English & Spanish) (C: E-07/10; R: S-07/11)
f2. EHS Home Base Unable to Contact Letter (Revised 07/12)
g. (Vacant)
g1. EHS Home Base Attendance/Agreement Plan with Parent/Guardian (Revised 06/16)
3. Enrollment of Families
a. Selection of Families Policy and Procedure (English & Spanish) (Revised 02/16)
b. Statement of Eligibility (Revised 07/16)
b1. Verification of Homeless Status (Created 04/11)
c. EHS Enrollment of Families (English & Spanish) (Revised 02/16)
d. Head Start Selection Criteria Score Sheet (English & Spanish) (Revised 02/16)
d1. EHS Selection Criteria Score Sheet (English & Spanish) (Revised 02/16)
e. Enrollment of Families Policy and Procedure (English & Spanish) (Revised 07/17)
4. Intake of families
a. Intake Appointment & Forms Checklist (Revised 03/15)
a1. EHS Intake/Enrollment Visit (Revised 08/16)
a2. Prenatal Intake/Enrollment Visit (Revised 06/16)
5. Recruitment
a. Recruitment Policy and Procedure (Revised 02/12)
b. HS/EHS/ECEAP Rack Card (recruitment) (English & Spanish) (Revised 02/18)
c. Head Start/EHS/ECEAP Poster (Revised 02/18)
d. QRC Card (recruitment) (English & Spanish) (Created 02/18)
e. Logo Use Procedure & Guide (Created 02/18)
f. Logos (Created 02/18)
6. Community Assessment
a. Community Assessment Policy & Procedure (Revised 07/10)
ERSEA 1a
(C: 04/14; R: 05/18)
LOWER COLUMBIA COLLEGE HEAD START/EHS/ECEAP Physical Address: 1720 – 20th Avenue, Longview, WA 98632
Mailing Address: PO Box 3010, Longview, WA 98632 (360) 442-2800 FAX: (360) 442-2819
E-mail: [email protected] Website: http://lowercolumbia.edu/head-start/index.php
Eligibility Application Please fill in the form completely and accurately. All information will be kept confidential. It will be used to help us determine if your family is eligible for services and to prioritize your placement on the waiting list. If you have any questions about this application, or need any help in completing it, please call us. We will be glad to help!
For Pregnant Applicants: Pregnant Applicant Name: Due Date:
Are you working on your High School Diploma or GED? Yes No
For Child Applicants: Child’s Name: Date of Birth: (First, Middle, Last)
Sex: Male Female Language(s) Child Speaks: Address: Home: (Address) (City) (Zip)
Mailing (if different): (Address) (City) (Zip)
Are there any areas you would like support / resources for your child? Yes – check all that apply No Dental Health Physical Health Former Foster Child Nutrition/Eating
Vision Hearing Speech
Abuse/Neglect Behavior Learning Difficulties
Primary Parent/Guardian Information One or two parent household? One Two
Parent/Guardian’s Name: (First, Middle, Last)
Date of Birth: Relationship to Child: (Ex: Mother, Father, Foster Parent, Grandparent, Step Parent, etc.)
Telephone: (Cell) (Home) (Work) (Other)
E-mail address:
In what language do you prefer to communicate: English Spanish Other
Are you or your spouse/partner working on your High School Diploma or GED? Yes No
Secondary Parent/Guardian Information Lives in home with child? Yes No
Parent/Guardian’s Name: (First, Middle, Last)
Date of Birth: Relationship to Child: (Ex: Mother, Father, Foster Parent, Grandparent, Step Parent, etc.)
Telephone: (Cell) (Home) (Work) (Other)
E-mail address:
In what language do you prefer to communicate: English Spanish Other
ERSEA 1a
(C: 04/14; R: 05/18)
Past participation in Head Start/EHS/ECEAP? No Yes If yes, Within past 3 years? Transferred from another Head Start/ECEAP?
Is this child on an IEP/IFSP (Special Education)? No Yes – Name of the school district/provider:
Special Agency Referral from:
Is this child’s family currently receiving Child Protective Services (CPS)? Yes No
Is this child’s family currently receiving Family Assessment Response (FAR) services? Yes No
Does this household receive subsidized housing, such as housing voucher or cash assistance for housing? Yes No
Do you have needs for yourself or other family members? Yes – check all that apply No Disability/Unable to Work Drug/Alcohol Issues Incarcerated Parent Family Violence
Learning Disabilities Mental Health/Illness Health Issues
Abuse/Neglect Domestic Violence Chronic Illness in Family
Family Size and Income Number of people in your household that your income supports:
Is your family homeless? Yes No
Is your family currently receiving TANF benefits? Yes Client ID # No Formerly
Is your family receiving Supplemental Security Income (SSI)? Yes No Family
Member Amount Per (for example: week,
month, year) Annual Amount Description (for example: SSI,
Job, Child Support)
$ $
$ $
$ $
Please bring proof of your family income for the last calendar year or the last 12 months with this application. Bring copies of all that apply: W-2 forms, income tax return, TANF benefits, unemployment summary, child support, social security, financial aid, SSI, pay stubs.
Emergency Contacts Primary Name: (First, Last) (Relationship to child)
Address: City: State: Zip:
Telephone: (Cell) (Home) (Work)
Secondary Name: (First, Last) (Relationship to child)
Address: City: State: Zip:
Telephone: (Cell) (Home) (Work)
Lower Columbia College Head Start/ECEAP does not discriminate against any person on the basis of race, color, national origin, disability, or age in admission, treatment, or participation in its programs, services and activities, or in employment.
I certify that this eligibility information is true. I understand that the information in this application will be held in confidence within the agency and is accessible to me during normal business hours.
Parent/Guardian Signature _______________________________________ Date __________________________
ERSEA 1a
(C: 04/14; R: 05/18)
LOWER COLUMBIA COLLEGE HEAD START/EHS/ECEAP Dirección Física: 1720 – 20th Avenue, Longview, WA 98632
Dirección Postal: PO Box 3010, Longview, WA 98632 (360) 442-2800 FAX: (360) 442-2819
Correo Electrónico: [email protected] Sitio web: http://lowercolumbia.edu/head-start/index.php
Solicitud de Elegibilidad Por favor llene este formulario con la información completa y correcta. Toda la información se mantendrá confidencial. Esta información será usada para ayudarnos a determinar si su familia es elegible para los servicios y la prioridad de su solicitud en la lista de espera. Si usted tiene alguna pregunta acerca de esta solicitud o si necesita ayuda para completarla, por favor llámenos. ¡Estaremos encantados de ayudarle!
Para Mujeres Embarazadas: Nombre de la solicitante embarazada: Fecha de Parto:
¿Está tomando clases para sacar su diploma o GED? Sí No
Para Niños: Nombre del Niño: Fecha de Nacimiento: (Primero, Segundo, Apellidos)
Sexo: Masculino Femenino Idioma(s) que el niño sabe hablar:
Dirección: De casa: (Dirección) (Ciudad) (Código Postal)
Postal (si es diferente): (Dirección) (Ciudad) (Código Postal)
¿Quisiera ayuda o recursos para su niño en alguna área? Sí – Por favor marque todos que correspondan No
Salud Dental Salud Física Niño previamente colocado en
un hogar de padres temporales Nutrición/Comer
Vista Oído Habla
Maltrato/Negligencia Comportamiento Dificultades para Aprender
Información del Padre/Madre/Tutor ¿Están uno o dos padres en la casa? Uno Dos Nombre del Padre/Madre/Tutor: (Primero, Segundo, Apellidos)
Fecha de Nacimiento: Relación con el niño: (Ej.: Madre, Padre, Padre de Cuidado Temporal, Abuela, Padrastro, etc.)
Teléfono: (Celular) (Casa) (Trabajo) (Otro)
Dirección de Correo Electrónico:
¿En qué idioma prefiere la comunicación?: Inglés Español Otro ¿Está usted o su esposo/pareja tomando clases para sacar su diploma o GED? Yes No
Información del Padre/Madre/Tutor (en la misma casa) ¿Vive en la misma casa que el niño? Sí No Nombre del Padre/Madre/Tutor: (Primero, Segundo, Apellidos)
Fecha de Nacimiento: Relación con el niño: (Ej.: Madre, Padre, Padre de Cuidado Temporal, Abuela, Padrastro, etc.)
Teléfono: (Celular) (Casa) (Trabajo) (Otro)
Dirección de Correo Electrónico:
¿En qué idioma prefiere la comunicación?: Inglés Español Otro
ERSEA 1a
(C: 04/14; R: 05/18)
¿Ha participado Ud. anteriormente en el Head Start, EHS o ECEAP? No Sí Si es que sí, ¿Fue en los 3 años pasados? ¿Se está cambiando de otro programa del Head Start o ECEAP?
¿Tiene este niño un IEP o IFSP (Educación Especial)? No Sí – Nombre del Distrito Escolar o Proveedor:
Agencia Especial que lo remitió:
¿Está la familia de este niño actualmente recibiendo servicios de Servicios de Protección Infantil (CPS)? Sí No
¿Está la familia de este niño actualmente recibiendo servicios de Respuesta de Evaluación Familiar (FAR)? Sí No
¿Recibe esta familia subvenciones para la vivienda, como un bono o ayuda en efectivo para vivienda? Sí No
¿Tiene usted o un miembro de su familia alguna necesidad? Sí – Favor de marcar todos que correspondan No Discapacidad/No puede Trabajar Problemas de Drogas o Alcohol Padre o Madre Encarcelado Violencia Familiar
Problemas de Aprendizaje Salud/Enfermedad Mental Problemas de Salud
Maltrato/Negligencia Violencia Doméstica Enfermedades Crónicas
en La Familia
Ingreso y Número de Personas en la Familia Número de personas que viven en el hogar y dependen de sus ingresos:
¿Son ustedes una familia sin hogar? Sí No
¿Recibe su familia beneficios de TANF? Sí N° de cliente No Anteriormente
¿Recibe su familia beneficios de Seguridad de Ingreso Suplementario (SSI)? Sí No Miembro
de la Familia Cantidad Por(por ejemplo: semana,
mes, año) Cantidad Anual Descripción (por ejemplo:
Trabajo, Pensión Alimenticia, SSI)
$ $
$ $
$ $
Por favor, entregue con esta solicitud comprobantes de los ingresos de su familia durante el año pasado o de los últimos 12 meses. Entregue copias de todos que correspondan: formularios W-2, declaración de los impuestos sobre el ingreso, beneficios de TANF, reporte de desempleo, manutención de niños, seguridad social, ayuda financiera estudiantil, SSI, talones de pago.
Contactos de Emergencia
Primario Nombre: (Primero, Segundo, Apellidos) (Relación al niño)
Dirección: Ciudad: Estado: Código Postal:
Teléfono: (Celular) (Hogar) (Trabajo)
Secundario Nombre: (Primero, Segundo, Apellidos) (Relación al niño)
Dirección: Ciudad: Estado: Código Postal:
Teléfono: (Celular) (Casa) (Trabajo)
Lower Columbia College Head Start/ECEAP no discrimina a ninguna persona en base a su raza, color, nacionalidad, discapacidad o edad, para la admisión, tratamiento o participación en sus programas, servicios y actividades o en empleo.
Yo certifico que la información para elegibilidad es verdadera. Entiendo que la información en esta solicitud será usada confidencialmente por la agencia y que estará accesible para mí durante las horas normales de trabajo.
Firma del Padre/Madre/Tutor(a) _________________________________________ Fecha _____________________________
Thank you for your recent interest in Lower Columbia College Head Start/EHS/ECEAP.
Your application is complete; however our classes are full at this time. We will
contact you when an opening is available for your child.
In order to process your child’s application, we need you to bring in or mail
whichever documents show your total income for the last 12 months or
calendar year: Income Tax form 1040 and W-2’s for the previous year; Public
Assistance: TANF, SSI, WCCC; Unemployment history; Social Security, Child
Support, etc.
We have tried to contact you by phone with no success. Please contact us
at 442-2800 with a current phone number and address.
Telephone 442-2800
FAX 442-2819
Thank you for your recent interest in Lower Columbia College Head Start/EHS/ECEAP.
Your application is complete; however our classes are full at this time. We will
contact you when an opening is available for your child.
In order to process your child’s application, we need you to bring in or mail
whichever documents show your total income for the last 12 months or
calendar year: Income Tax form 1040 and W-2’s for the previous year; Public
Assistance: TANF, SSI, WCCC; Unemployment history; Social Security, Child
Support, etc.
We have tried to contact you by phone with no success. Please contact us
at 442-2800 with a current phone number and address.
Telephone 442-2800
FAX 442-2819
Thank you for your recent interest in Lower Columbia College Head Start/EHS/ECEAP.
Your application is complete; however our classes are full at this time. We will
contact you when an opening is available for your child.
In order to process your child’s application, we need you to bring in or mail
whichever documents show your total income for the last 12 months or
calendar year: Income Tax form 1040 and W-2’s for the previous year; Public
Assistance: TANF, SSI, WCCC; Unemployment history; Social Security, Child
Support, etc.
We have tried to contact you by phone with no success. Please contact us
at 442-2800 with a current phone number and address.
Telephone 442-2800
FAX 442-2819
Thank you for your recent interest in Lower Columbia College Head Start/EHS/ECEAP.
Your application is complete; however our classes are full at this time. We will
contact you when an opening is available for your child.
In order to process your child’s application, we need you to bring in or mail
whichever documents show your total income for the last 12 months or
calendar year: Income Tax form 1040 and W-2’s for the previous year; Public
Assistance: TANF, SSI, WCCC; Unemployment history; Social Security, Child
Support, etc.
We have tried to contact you by phone with no success. Please contact us
at 442-2800 with a current phone number and address.
Telephone 442-2800
FAX 442-2819
Lower Columbia College
Head Start/EHS/ECEAP
1600 Maple Street
PO Box 3010
Longview, WA 98632
Lower Columbia College
Head Start/EHS/ECEAP
1600 Maple Street
PO Box 3010
Longview, WA 98632
Lower Columbia College
Head Start/EHS/ECEAP
1600 Maple Street
PO Box 3010
Longview, WA 98632
Lower Columbia College
Head Start/EHS/ECEAP
1600 Maple Street
PO Box 3010
Longview, WA 98632
Gracias por su reciente interés en el Programa del
Lower Columbia College Head Start/ECEAP.
Su solicitud está completa, sin embargo en estos momentos nuestras clases
están Completas. Nosotros lo contactaremos cuando haya una vacante
disponible para su niño.
En orden de procesar la solicitud de su niño, necesitamos que nos traiga o
envíe por Correo cualquiera de los documentos que comprueben sus ingre
sos totales por los últimos 12 meses o del calendario annual: Forma 1040 de
Income Tax y W-2 del año pasado, Asistencia Pública: TANF, SSI, WCCC;
Historial de Desempleo; Social Security, Pensión Alimenticia, etc.
Hemos tratado de contactarlo por teléfono sin éxito. Por favor llámenos al
442-2800 para darnos su número de teléfono y domicilio actuales,
Telephone 442-2800
FAX 442-2819
Gracias por su reciente interés en el Programa del
Lower Columbia College Head Start/ECEAP.
Su solicitud está completa, sin embargo en estos momentos nuestras clases
están Completas. Nosotros lo contactaremos cuando haya una vacante
disponible para su niño.
En orden de procesar la solicitud de su niño, necesitamos que nos traiga o
envíe por Correo cualquiera de los documentos que comprueben sus ingre
sos totales por los últimos 12 meses o del calendario annual: Forma 1040 de
Income Tax y W-2 del año pasado, Asistencia Pública: TANF, SSI, WCCC;
Historial de Desempleo; Social Security, Pensión Alimenticia, etc.
Hemos tratado de contactarlo por teléfono sin éxito. Por favor llámenos al
442-2800 para darnos su número de teléfono y domicilio actuales,
Telephone 442-2800
FAX 442-2819
Gracias por su reciente interés en el Programa del
Lower Columbia College Head Start/ECEAP.
Su solicitud está completa, sin embargo en estos momentos nuestras clases
están Completas. Nosotros lo contactaremos cuando haya una vacante
disponible para su niño.
En orden de procesar la solicitud de su niño, necesitamos que nos traiga o
envíe por Correo cualquiera de los documentos que comprueben sus ingre
sos totales por los últimos 12 meses o del calendario annual: Forma 1040 de
Income Tax y W-2 del año pasado, Asistencia Pública: TANF, SSI, WCCC;
Historial de Desempleo; Social Security, Pensión Alimenticia, etc.
Hemos tratado de contactarlo por teléfono sin éxito. Por favor llámenos al
442-2800 para darnos su número de teléfono y domicilio actuales,
Telephone 442-2800
FAX 442-2819
Gracias por su reciente interés en el Programa del
Lower Columbia College Head Start/ECEAP.
Su solicitud está completa, sin embargo en estos momentos nuestras clases
están Completas. Nosotros lo contactaremos cuando haya una vacante
disponible para su niño.
En orden de procesar la solicitud de su niño, necesitamos que nos traiga o
envíe por Correo cualquiera de los documentos que comprueben sus ingre
sos totales por los últimos 12 meses o del calendario annual: Forma 1040 de
Income Tax y W-2 del año pasado, Asistencia Pública: TANF, SSI, WCCC;
Historial de Desempleo; Social Security, Pensión Alimenticia, etc.
Hemos tratado de contactarlo por teléfono sin éxito. Por favor llámenos al
442-2800 para darnos su número de teléfono y domicilio actuales,
Telephone 442-2800
FAX 442-2819
Lower Columbia College
Head Start/ECEAP
1600 Maple Street
PO Box 3010
Longview, WA 98632
Lower Columbia College
Head Start/ECEAP
1600 Maple Street
PO Box 3010
Longview, WA 98632
Lower Columbia College
Head Start/ECEAP
1600 Maple Street
PO Box 3010
Longview, WA 98632
Lower Columbia College
Head Start/ECEAP
1600 Maple Street
PO Box 3010
Longview, WA 98632
ERSEA 1c
(C: 08/99; R: 05/18)
Lower Columbia College Head Start/ECEAP/EHS No Income Statement
Child’s Name
Parent(s) Name My basic needs (food, shelter and utilities) have been met for the last 12 months in the following ways:
Food
Shelter
Transportation
Utilities
Insurance
Household Needs
Other
I certify that the information contained in this affidavit is complete and accurate to the best of my knowledge. I understand that if I knowingly give false information or misrepresentation of my income, it may result in disqualification from the program. Signature Date signed
Signature Date signed
ERSEA 1c
(C: 08/99; R: 04/11)
LOWER COLUMBIA COLLEGE HEAD START/EHS/ECEAP
Verification of Undocumented Income
This form is to be completed and signed by the parent or guardian who is unable to provide the
regular income verification documents:
Income Tax form for the previous year;
W-2 forms for the previous year;
Public Assistance--TANF (Temporary Assistance for Needy Families) TANF benefits or
services include: cash payments, job training, vouchers, transportation and subsidized
child care, such as Working Connections Child Care (WCCC).
SSI (Supplemental Security Income);
Unemployment history;
Social Security statement for 12 months;
Financial Aid.
My family’s source of income has been provided in the following way for the past year.
What are your living arrangements and/or employment status?
Who provides food and shelter for your family?
_________________________ _________________________ Signature of Parent or Guardian Child’s Name _________________________ _________________________ Signature of Staff Member Date
Verification of Undocumented Income ERSEA 1c
(R: 04/11; C: 08/99)
LOWER COLUMBIA COLLEGE HEAD START/EHS/ECEAP
Verificación de Ingresos sin Comprobante
Esta forma deberá ser llenada y firmada por el Padre de Familia o Tutor que no puede
proporcionar los documentos regulares de verificación de ingresos.
Forma de los Impuestos del año anterior;
Forma W-2 del año anterior;
Asistencia Pública--TANF (Temporary Assistance for Needy Families) beneficios de
TANF o servicios incluidos como: pagos en efectivo, capacitación para empleo, vales,
transportación o ayuda para la guardería, tal como Working Connections Child Care
(Pago para la Guardería de sus Hijos).
SSI (Seguridad de Ingreso Suplementario);
Comprobantes de desempleo;
Informe del Social Security (Seguro Social) de los últimos 12 meses;
Ayuda financiera a estudiantes
La fuente de ingresos para mi familia durante el año pasado, fue de la siguiente manera.
¿Cuál fue su situación de vivienda y/o empleo?
¿Quién proporciona alimentación y vivienda para su familia?
_________________________ _________________________ Firma del Padre o Tutor Nombre del Niño _________________________ _________________________ Firma del Personal Fecha
ERSEA 1d1
(C: 06/04; R: 05/17)
Lower Columbia College Head Start/EHS/ECEAP
Parent/Guardian Permission to Reveal or Obtain Confidential Information Form Procedure
Parent/guardians will be requested to complete Parent/Guardian Permission to Reveal or
Obtain Confidential Information forms ERSEA 1d (Release of Information forms) for their
student’s:
Current School District;
Primary Health Care Provider; and
Dentist
Parent/guardians will also be requested to complete releases for other applicable educational
and/or health/social services agencies their student currently or previously received services
from.
Completion of Parent/Guardian Permission to Reveal or Obtain Confidential Information
forms will primarily occur during:
Look to see what is in cp.net under the enrollment tab. In right hand corner, view the
attachments (#). Click on attachments. It will list the attachments (ROIs). You can then
click on the ROI and view it or print it.
A release that was completed in the spring (April-May 2017) does not need to be
recompleted until it expires.
For Spanish language families, have the parent/guardian sign the ROI in Spanish on one
side and English on the other side.
Scheduled Intake Appointments; and
New releases must be completed at the Welcome Visits of Returning students regardless
of the expiration dates of releases already on file.
Early Head Start Intake/Enrollment Visits and First Visits for new program year.
During the school year, as the ongoing needs and/or providers of services change for a student,
parent/guardian may be requested to complete additional release(s).
Placement of Parent/Guardian Permission to Reveal or Obtain Confidential Information
form is an original and copy:
Send the original to the Program Assistant.
If DST staff obtains the original ROI, they will place a copy in the red working file prior
to sending the original to the Program Assistant. The copy will be shredded upon return
of the original.
The Program Assistant will database into the health module of ChildPlus.net; initial and
date bottom corner of original ROI; scan and attach the original ROI into the enrollment
module of ChildPlus.net; and send the original to the DST.
The original is placed in the site file.
Use of The Parent/Guardian Permission to Reveal or Obtain Confidential Information
form:
At the request of the parent/legal guardian and/or an appropriate staff member, staff will
print a copy of the pertinent ROI from the database and attach to the request.
ERSEA 1d1
(C: 06/04; R: 05/17)
The exchange of information is for the purpose of supporting the ongoing care of the
student.
Releases and Mental Health:
Intake and Welcome Visits: We won’t be automatically requesting for parents to initial
and sign the mental health line on releases at intake or initial visits. (Primary Care
Physician or School District releases)
Unusual Expectations: If the individual or guardian responsible for signing for the child
requests that we coordinate with a Mental Health Provider at intake or initial visit or asks
us to help them in setting up something related to a mental health referral, we would need
a release and for them to initial the mental health line.
Document that they discussed this desire in the intake notes or family services notes and
any additional information they shared with any specific requests. The mental health
consultants will document in the mental health module.
Referrals for Observations or to Assist in Making a Mental Health Referral: When
making a referral for an individual observation, we will request that the person/guardian
sign a release related to Mental Health if there is treatment or records they would like to
have considered or that needs to be considered in order to develop supportive strategies.
The Family Advocate or Child/Family Development Specialist or Mental Health
Consultant may request records specific to Mental Health when an observation is
occurring and share, with the child’s parent/guardian, that this information will be kept
confidential and document that they have done this in a family services note or mental
health module. If a person/family has questions about how their Mental Health
information may be used/shared/coordinated, the Mental Health Consultant is available to
follow-up and answer some questions.
Staff may also follow up with mental health consultants about questions related to
providing informed consent.

ERSEA 1d
LOC ID __________
Lower Columbia College Head Start/EHS/ECEAP (C: 04/03; R: 05/17)
PO Box 3010 – Longview, WA 98632 360-442-2800 FAX 360-442-2819
Email: [email protected]
Lower Columbia College Head Start/EHS/ECEAP
Parent/Guardian Permission to Reveal or Obtain Confidential Information
Please complete this form with ALL information.
Child's Name: DOB:
Address: Phone:
City/State:
I hereby authorize Lower Columbia College Head Start/EHS/ECEAP to provide/receive information
to/from the following individual/agencies:
Name of Individual/Agency:
Address: Phone:
City, State, Zip: Fax #:
My authorization is for the use and disclosure of the following information: ___ Immunizations ___ Record of Health Care Provider Visits ___ Physical Exam ___ Statements of Charges & Payments
___ Medication ___ Lab Reports
___ Surgery ___ Reports of x-rays & Other Images
___ Dental ___ Educational
___ Mental Health (_____ initials) ___ IEP
___ Screening/Assessment ___ IFSP ___ AIDS (Acquired Immunodeficiency Syndrome) or HIV (Human Immunodeficiency Virus) information
___ Other: ___ All of the above
My authorization pertains to information generated on the following date(s) or in the following
time period:
Released in the following manner: Copies by mail Copies by email Copies by fax Copies to be picked-up
Chart Review by RN Health Consultant Other:
All methods listed
My authorization is given freely with the understanding that:
I may refuse to sign this permission form and my refusal will not adversely affect my enrollment.
I may revoke this authorization at any time in writing, except where information has already been
released based upon my prior authorization.
A photocopy or fax of this authorization is as valid as the original.
Lower Columbia College Head Start/EHS/ECEAP, its director, officers, employees and agents
are hereby released from any legal responsibility or liability for disclosure of the
above information to the extent indicated and authorized herein.
This information will be used for the following purpose:
At the request of the parent/legal guardian and/or Lower Columbia College Head
Start/EHS/ECEA Program for ongoing care.
I understand that the information used or disclosed pursuant to this authorization may be subject to re-disclosure
and no longer protected under federal law. However, I also understand that federal or state law may restrict
re-disclosure of HIV/AIDS information, mental health information and genetic information. This authorization
expires 18 months from the date of signing unless revoked or otherwise specified above.
Parent/Legal Guardian's Name (Please Print) Child's Name (Please print)
Parent/Legal Guardian's Signature Date Relationship to Child
Permission to Reveal or Obtain Confidential Information ERSEA 1d
LOC ID __________
Lower Columbia College Head Start/EHS/ECEAP (C: 04/03; R: 05/17)
PO Box 3010 – Longview, WA 98632 360-442-2800 FAX: 360-442-2819
Email: [email protected]
Lower Columbia College Head Start/EHS/ECEAP
Autorización de los Padres/Tutores para Revelar u Obtener Información Confidencial
Por favor, complete esta forma con TODA la información.
Nombre del niño: Fecha de Nacimiento:
Domicilio: Número de teléfono:
Ciudad/Estado:
Por medio de la presente autorizo al Lower Columbia College Head Start/EHS/ECEAP a proporcionar y/o recibir
información a/de la siguiente persona/agencia:
Nombre de la persona/agencia:
Domicilio: Teléfono:
Ciudad, Estado, C. Postal: Fax #:
Mi autorización es para el uso y /o revelación de la siguiente información:
____ Vacunas ____ Registro de las visitas al Doctor
____ Exámenes Médicos ____ Estados de cuenta de costos y pagos
____ Medicamentos ____ Reportes de laboratorio
____ Cirugías ____ Reportes de Rayos X y otras imágenes
____ Dental ____ Educacional
____ Salud Mental (_______ iniciales) ____ Plan Individual de Educación (IEP)
____ Exámenes/Evaluaciones ____ IFSP
____ SIDA (Síndrome de Inmunodeficiencia Adquirida) o HIV (Human Immunodeficiency Virus)
____ Otros: ___________________________ ____ Todos los listados
Mi autorización corresponde a la información generada en las siguientes fechas o durante el siguiente período de
tiempo:
La información podrá ser proporcionada de la siguiente manera:
Copias por correo Copias por email Copias por fax Las copias deberán ser recogidas
Expediente revisado por la RN Consejera de Salud Otras:
Todas métodos listados
Mi autorización es otorgada libremente con el entendimiento de que:
Puedo negarme a firmar este permiso.
Puedo revocar esta autorización por escrito en cualquier momento, excepto cuando la información ya se haya dado
con base en mi anterior autorización.
Una fotocopia o fax de esta autorización es tan válida como una original.
El Head Start/EHS/ECEAP del Lower Columbia College, su director, funcionarios, empleados y agentes son
liberados de cualquier responsabilidad legal u obligación por la revelación de la información anteriormente indicada
y autorizada.
Esta información será usada para el siguiente propósito:
A petición del Padre/Tutor Legal y/o el Programa del Head Start/EHS/ECEAP del Lower Columbia College
para la atención acordada.
Yo entiendo que la información usada o revelada conforme a esta autorización quizá sea sujeta a mayor revelación y que ya
no esté protegida bajo las leyes federales. Sin embargo, yo también entiendo que las leyes federales o estatales quizás
restrinjan la revelación de información acerca de HIV/AIDS, información de salud mental e información genética. Esta
autorización se vencerá 18 meses después de la fecha en que se firmó, a menos que se cancele antes o se especifique otra
fecha más arriba.
Nombre del Padre/Tutor Legal (Por favor, escríbalo) Nombre del Niño (Por favor, escríbalo)
Nombre y firma del Padre/Tutor Legal Fecha Relación con el niño
NEW FORM ERSEA 1e
Lower Columbia College Head Start/EHS/ECEAP
CHANGE OF STATUS
(to be completed by staff)
Original: Site File Copies: Main Office, Emergency Notebook, and Bus (if applicable) (C: 06/01; R: 07/14)
Child’s Name:
Child’s Name:
Parent’s Name:
Address:
City:
(Please Circle: ADD or DELETE or CHANGE) Phone:
Home
Cell
Cell Phone Provider
Wireless Provider
Work
Email Address
Other
( ) Child ( ) Parent
Change From:
Change To:
(Please Circle: ADD or DELETE or CHANGE)
Child's Health Insurance:
Parent/Guardian Signature Date
*Is the Parent a Policy Council Representative/
Alternative/ Officer Yes / No (circle one)
LOC ID # Birthdate:
LOC ID # Birthdate:
Staff Name: Date:
Withdraw Date:
Reason for Withdrawal:
Put Back On Wait List? Yes No
If Yes, Model or Site Requested: AM / PM
(Please Circle: ADD or DELETE or CHANGE)
1. Name:
Relation to Child:
Address:
Phone: Home
Cell
Work
(Please Circle: ADD or DELETE or CHANGE)
2. Name:
Relation to Child:
Address:
Phone: Home
Cell
Work
(Please Circle: ADD or DELETE or CHANGE)
3. Name:
Relation to Child:
Address:
Phone: Home
Cell
Work
*Does the student ride a bus? Yes/ No (circle one)
(If “yes”, provide copy to bus driver for phone, address, or
emergency contact changes)
FAMILY ADDRESS/PHONE
LEGAL NAME CHANGE
HEALTH INSURANCE
OTHER - i.e., Custody Information, Restraining
Orders, Additions to Family, etc.
WITHDRAW
STUDENT EMERGENCY CONTACT
ERSEA 1f
Lower Columbia College Head Start/EHS/ECEAP (C: 11/13)
PO Box 3010 – Longview, WA 98632 360-442-2800 FAX 360-442-2819
Lower Columbia College Head Start/EHS/ECEAP
Adult Permission to Reveal or Obtain Confidential Information
Please complete this form with ALL information.
Adult Name: DOB:
Address: Phone:
City/State:
I hereby authorize Lower Columbia College Head Start/EHS/ECEAP to provide/receive information
to/from the following individual/agencies:
Name of Individual/Agency: _____________________________________________________________
Address: ______________________________________________ Phone: ___________________
City, State, Zip: ________________________________________ Fax #: ____________________
My authorization is for the use and disclosure of the following information: ___ Immunizations ___ Record of Health Care Provider Visits ___ Physical Exam ___ Statements of Charges & Payments
___ Medication ___ Lab Reports
___ Surgery ___ Reports of x-rays & Other Images
___ Dental ___ Educational
___ Mental Health (_____ initial) ___ IEP
___ Screening/Assessment ___ AIDS (Acquired Immunodeficiency Syndrome) or HIV (Human Immunodeficiency Virus) information
___ Other: _______________________ ___ All of the above
My authorization pertains to information generated on the following date(s) or in the following
time period: __________________________________________________________________________
Released in the following manner: Copies by mail Copies by fax Copies to be picked-up
Chart Review by RN Health/RDH Dental Consultant Other:
All methods listed
My authorization is given freely with the understanding that:
I may refuse to sign this permission form.
I may revoke this authorization at any time in writing, except where information has already
been released based upon my prior authorization.
This authorization will expire on: _____________________________________________ A photocopy or fax of this authorization is as valid as the original.
Lower Columbia College Head Start/EHS/ECEAP, its director, officers, employees and
agents are hereby released from any legal responsibility or liability for disclosure of the
above
information to the extent indicated and authorized herein.
This information will be used for the following purpose:
At the request of the parent/legal guardian and/or Lower Columbia College Head
Start/EHS/ECEA Program for ongoing care.
I understand that the information used or disclosed pursuant to this authorization may be subject to re-disclosure
and no longer protected under federal law. However, I also understand that federal or state law may restrict
re-disclosure of HIV/AIDS information, mental health information and genetic information.
Name (Please Print)
Signature Date
ERSEA 2a
(C: 08/98; R: 03/18)
Lower Columbia College Head Start/EHS/ECEAP
Attendance and Meal Count Procedure
Instruction for ChildPlus Report 2315:
1. Fill in the “Attendance for” blanks at the top of the form.
2. The five columns reflect Monday through Friday. Use the appropriate column for the day of
the week. If you are not in session on Monday and/or Friday, write “N” to indicate a non-
scheduled day. Include the date next to the name of each day of the week.
3. If you enroll a child after the first day of the week, add their name to the bottom of the list.
At the beginning of the following week, the new child’s name will appear on your next Daily
Attendance and Meals Worksheet.
4. Program office staff will email new “Daily Attendance and Meals Worksheets” at the end of
each week to the lead teacher and Area Manager in preparation for the following week.
5. CIRCLE the Breakfast (B), Lunch (L), or PM Snack (P) area after the toddler or preschool
child is seated, the meal is served and the child has been offered each food component at
least twice. (Infant meals must be counted on the Daily Infant Meal Record, ERSEA 2b1.)
6. REFER to the legend on the top of the form to accurately record the child’s attendance and
meals.
7. Add up the totals at the bottom of the page for each area (i.e. those present, eating breakfast,
lunch or snack). For accuracy, recheck by adding totals a second time and verifying that
appropriate meals are selected.
8. The original attendance form is to be routed to Program Coordinator (CM) and a copy to
your supervisor. Please make a second copy to remain at your site. Attendance/Meal Forms
are due each Friday at 5:00PM. Program office staff will enter attendance into a tracking
database for monthly reporting of child, class and site and program percentages by month.
9. If attendance falls below 85% for the month for classroom and/or individual child, staff and
Area Managers must analyze the attendance concerns. See Attendance Policy & Procedure
in ERSEA Section of Volume I Handbook for further directions on this procedure.
EHS Attendance Tracking:
Home Base: Attendance percentages, for the Home Base model (HB1, HB2, HB3, HB4
and HB5) are based upon Home Visits only that are tracked on ChildPlus EHS Tracking
Event Attendance and Prenatal Attendance Tracking Form ERSEA 2e2. EHS Area
Managers calculate the attendance percentages. They include them on their End of
Month reports.
PAL: PAL attendance and meal counts are tracked separately on ChildPlus Report 2315
and are not included to calculate attendance percentages. (USDA requires that infant
meals are also recorded on Daily Infant Meal Record forms.)

ERSEA 2a
(C: 08/98; R: 03/18)
Teen Model (EHS/Even Start): The Teen model tracks attendance and Home Visits in
ChildPlus EHS Tracking Event Attendance and Prenatal Attendance Tracking Form
ERSEA 2e2. Meal counts are recorded and tracked by Even Start staff members, on a
separate form, for USDA reimbursement by the Longview School District. Attendance
percentages are based upon classroom attendance by children and on completed Home
Visits with enrolled expectant mothers. The EHS Supervisor will receive copies of
completed ERSEA 2e2 forms monthly with EOM report. The EHS Area Managers
calculate the attendance percentages. They include them on their End of the Month
reports.
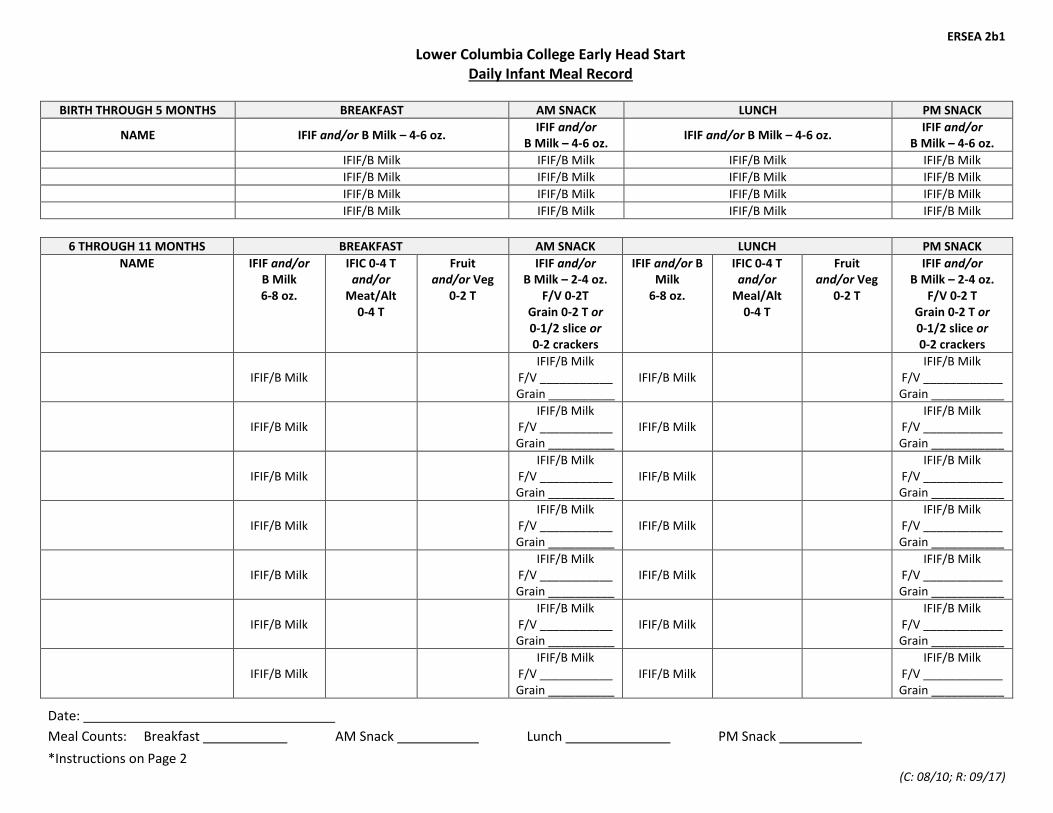
ERSEA 2b1
(C: 08/10; R: 09/17)
Lower Columbia College Early Head Start Daily Infant Meal Record
BIRTH THROUGH 5 MONTHS BREAKFAST AM SNACK LUNCH PM SNACK
NAME IFIF and/or B Milk – 4-6 oz. IFIF and/or
B Milk – 4-6 oz. IFIF and/or B Milk – 4-6 oz.
IFIF and/or B Milk – 4-6 oz.
IFIF/B Milk IFIF/B Milk IFIF/B Milk IFIF/B Milk
IFIF/B Milk IFIF/B Milk IFIF/B Milk IFIF/B Milk
IFIF/B Milk IFIF/B Milk IFIF/B Milk IFIF/B Milk
IFIF/B Milk IFIF/B Milk IFIF/B Milk IFIF/B Milk
6 THROUGH 11 MONTHS BREAKFAST AM SNACK LUNCH PM SNACK
NAME IFIF and/or B Milk 6-8 oz.
IFIC 0-4 T and/or
Meat/Alt 0-4 T
Fruit and/or Veg
0-2 T
IFIF and/or B Milk – 2-4 oz.
F/V 0-2T Grain 0-2 T or 0-1/2 slice or 0-2 crackers
IFIF and/or B Milk
6-8 oz.
IFIC 0-4 T and/or
Meal/Alt 0-4 T
Fruit and/or Veg
0-2 T
IFIF and/or B Milk – 2-4 oz.
F/V 0-2 T Grain 0-2 T or 0-1/2 slice or 0-2 crackers
IFIF/B Milk
IFIF/B Milk F/V ___________ Grain __________
IFIF/B Milk
IFIF/B Milk F/V ____________ Grain ___________
IFIF/B Milk
IFIF/B Milk F/V ___________ Grain __________
IFIF/B Milk
IFIF/B Milk F/V ____________ Grain ___________
IFIF/B Milk
IFIF/B Milk F/V ___________ Grain __________
IFIF/B Milk
IFIF/B Milk F/V ____________ Grain ___________
IFIF/B Milk
IFIF/B Milk F/V ___________ Grain __________
IFIF/B Milk
IFIF/B Milk F/V ____________ Grain ___________
IFIF/B Milk
IFIF/B Milk F/V ___________ Grain __________
IFIF/B Milk
IFIF/B Milk F/V ____________ Grain ___________
IFIF/B Milk
IFIF/B Milk F/V ___________ Grain __________
IFIF/B Milk
IFIF/B Milk F/V ____________ Grain ___________
IFIF/B Milk
IFIF/B Milk F/V ___________ Grain __________
IFIF/B Milk
IFIF/B Milk F/V ____________ Grain ___________
Date:
Meal Counts: Breakfast AM Snack Lunch PM Snack
*Instructions on Page 2
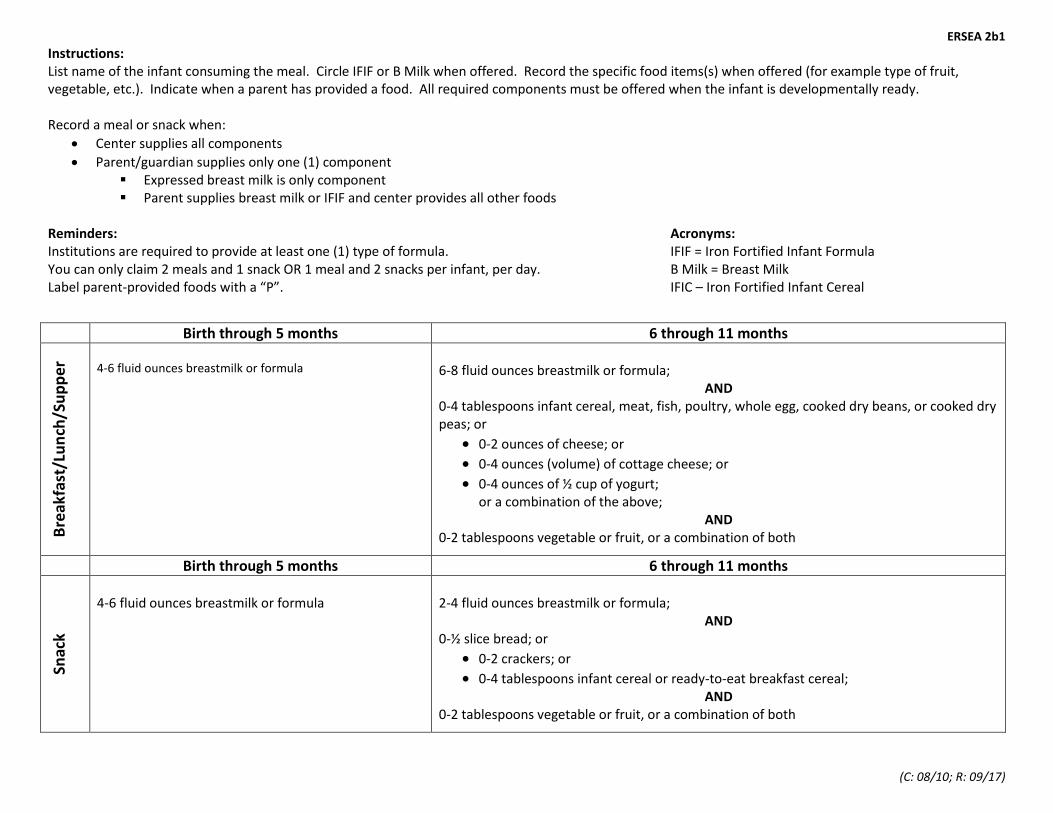
ERSEA 2b1
(C: 08/10; R: 09/17)
Instructions: List name of the infant consuming the meal. Circle IFIF or B Milk when offered. Record the specific food items(s) when offered (for example type of fruit, vegetable, etc.). Indicate when a parent has provided a food. All required components must be offered when the infant is developmentally ready. Record a meal or snack when:
Center supplies all components
Parent/guardian supplies only one (1) component Expressed breast milk is only component Parent supplies breast milk or IFIF and center provides all other foods
Reminders: Acronyms: Institutions are required to provide at least one (1) type of formula. IFIF = Iron Fortified Infant Formula You can only claim 2 meals and 1 snack OR 1 meal and 2 snacks per infant, per day. B Milk = Breast Milk Label parent-provided foods with a “P”. IFIC – Iron Fortified Infant Cereal
Birth through 5 months 6 through 11 months
Bre
akfa
st/L
un
ch/S
up
per
4-6 fluid ounces breastmilk or formula
6-8 fluid ounces breastmilk or formula;
AND 0-4 tablespoons infant cereal, meat, fish, poultry, whole egg, cooked dry beans, or cooked dry peas; or
0-2 ounces of cheese; or
0-4 ounces (volume) of cottage cheese; or
0-4 ounces of ½ cup of yogurt; or a combination of the above;
AND 0-2 tablespoons vegetable or fruit, or a combination of both
Birth through 5 months 6 through 11 months
Snac
k
4-6 fluid ounces breastmilk or formula
2-4 fluid ounces breastmilk or formula;
AND 0-½ slice bread; or
0-2 crackers; or
0-4 tablespoons infant cereal or ready-to-eat breakfast cereal; AND
0-2 tablespoons vegetable or fruit, or a combination of both
ERSEA 2c
1 (C: 06/03; R: 08/17)
Lower Columbia College Head Start/ECEAP
Attendance Policy and Procedure
Policy
Lower Columbia College Head Start/ECEAP will follow the Federal and State Performance
Standards, which require that Head Start/ECEAP programs analyze the causes of absenteeism
when the monthly average daily attendance rate falls below 85% in each classroom and/or for
each individual child. This analysis must include a study of the pattern of absences for each
child, including the reasons for absences as well as the number of absences that occur on
consecutive days.
Procedure
1. Staff Strategies to Promote Attendance
Inform parents of the benefits of regular attendance and about attendance/absence
procedure at first home visit, orientation and as needed to notify the center when a
child will be absent.
Provide parents with information about the benefits of regular attendance throughout
the year.
Support families to promote the child’s regular attendance.
Make direct contact or conduct a home visit with a child’s parent if a child has two
unexplained absences.
Analyze individual child attendance monthly and develop strategies to improve
individual attendance such as direct contact with parents or intensive case
management as necessary.
2. Attendance Procedures for Parents to be Notified
Parents will be expected to call or email if the child cannot attend the program on a
school day. The explanation will include why the child cannot attend and when the
child will return (if known). All absences are to be documented in case management.
The following shall be considered excused absences:
Hospitalization
Illness
Communicable disease
Death in the family
Medical and dental appointments/treatment
Family situations
Social services appointments
If a child is unexpectedly absent and a parent has not contacted the program within
one hour of program start time, staff will contact the parent/guardian to determine the
reason for absence in order to ensure the child’s safety and well-being.
Children are expected to arrive on time and be picked up on time. Parents need to
call if their child will be late to class and/or if they will be late picking the child up.
If the child is not picked up within one hour of the scheduled ending class time, and
staff cannot reach an alternate care provider from the Family Information
Form/ChildPlus, staff will be required to notify an immediate supervisor, which may
result in notification of Child Protective Services (CPS). This may result in the child
being turned over to a CPS worker and/or police officer.
ERSEA 2c
2 (C: 06/03; R: 08/17)
Parents will be expected to notify staff if someone besides themselves will be picking
up the child. No child will be released to a person not authorized by the parent to
pick-up the child. Staff must be notified (in person or by telephone) when a person
not listed on the Family Information Form/ChildPlus, will be picking up the child.
Identification of this person must be reviewed by staff before releasing the child. If
the family does not have a telephone or is otherwise hard to reach, the staff will then
attempt to contact the family at their place of residence or through emergency
contacts.
If a child ceases to attend, the program must make appropriate efforts to reengage the
family to resume attendance. If the child’s attendance does not resume, then the
program must fill the slot with a new student.
3. Staff Attendance Documentation a. Attendance will be reviewed and documented in case management by the staff as
absences occur. Attendance percentages per child will be entered into the attendance
event in ChildPlus monthly. Teachers will turn in Attendance/Meal Count sheets
weekly to the Program Coordinator.
b. If the family does not have a telephone or is otherwise hard to reach, the staff will
then attempt to contact the family at their place of residence or through emergency
contacts.
c. Attendance will be reviewed and documented in case management by the staff as
absences occur. Attendance percentages will be entered into the attendance event in
ChildPlus monthly.
4. Absences
a. If a child has two consecutive unexplained absences or if an individual child’s
attendance has fallen below 85% the following steps will be taken:
a. Staff will conduct a home visit with the child’s parent/guardian.
b. Staff will use the attendance data to support their concern and provide family
support as needed. All contacts will be noted in case management including
the agreed upon return date.
c. If the child doesn’t return to regular attendance based on the agree date at the
home visit, irregular attendance will be discussed with the Area Manager
immediately. Next steps will be documented in case management.
d. For children who are out due to surgery or lengthy illness, the staff will
provide the parent with a parent/child activity packet to be completed at home.
e. The staff will contact the Area Manager for additional support as needed.
5. Failure to Establish Regular Attendance
If attendance falls below 85% for two consecutive months or does not become regular
within 7 school days, and intensive family support efforts to improve attendance have
been made; or contact cannot be made with the parent, or cooperation cannot be
elicited from the parent/guardian the following steps will be taken:
a. The staff will inform the Area Manager of the continued absence and draft a
letter.
b. If there is no response from the parent within the timeframe of the letter, the
family will be withdrawn on the 7th day from the program.
c. The staff will complete a Child-Family File Transfer Checklist (FS/PI 7k)
when a family is withdrawn from the program and will request that the
ERSEA 2c
3 (C: 06/03; R: 08/17)
ERSEA Team place the family back on the waitlist unless the family requests
otherwise. Referrals may be made to other community services.
d. The child’s site file will accompany the completed Child-Family File
Transfer Checklist (FS/PI 7k) and be sent to the ERSEA Team at the main
LCC office.
e. Extended Absence – If a family situation results in an absence lasting more
than two weeks and following discussion with Area Manager, the child could
be placed back on the waiting list. Upon return, the child will be placed in a
classroom if space is available. All correspondence needs to be documented
in case management.
6. Classroom Attendance falls below 85% and/or individual child attendance falls
below 85% a. The analysis will include at a minimum the following:
Review the Attendance and Meal Count Forms for the month and
ensure all absences are documented in case management.
Review individual pattern of absences for each child, including
reasons and numbers of absences occurring on consecutive days.
Review any closure days or scheduled day off in the month.
Review any transportation concerns (i.e. bus not operating).
Review homelessness for any enrollment needs.
Review of communicable disease trends/concerns.
b. Staff is to review the ChildPlus report #2305 that gives the classroom attendance
percentage as well as individual child attendance by percentage.
c. For each child below 85% attendance, run a ChildPlus report #4110 for the
Attendance event only. Analyze the documentation and ensure specific reasons
for absences, communication with parents, and specific steps needed to improve
attendance are documented. Follow-up with parents as needed and document
your communication.
d. Once documentation is current, print the reports #2305 and #4110 (for Attendance
event only) and submit to Area Manager.
e. The Area Manager will review the reports and follow-up with staff as needed.
Area Managers document written updates/clarifications/action steps on the #4110
reports as needed and file with monitoring.
This policy complies with Head Start Performance Standard 1305.8 (a) (b) (c)
ERSEA 2e1
(C: 04/12; R: 12/13) Key: C= Visit Completed MV= Make Up Visit MVD= Make Up Visit Declined E= Enrollment Date NS= No Show X= Parent Cancelled SC= Staff Cancelled W/D= Withdrawn
Lower Columbia College Early Head Start EHS Attendance Tracking Form
Month: LOC ID:
Child’s Name
Week 1 Date
Week 2 Date
Week 3 Date
Week 4 Date
Week 5 Date
PAL Date Total
ERSEA 2e2
(C: 04/12; R: 12/13)
Monday Tuesday Wednesday Thursday Friday
Prenatal Topics
Date
Benefits of Breast Feeding _____
Dental Care _____
Depression/Mental Health _____
Family Planning _____
Fetal Development _____
Labor and Delivery _____
Nutrition _____
Post Partum Health Care _____
Prenatal Health Care _____
SIDS _____
Substance Abuse
Prevention _____
Actual Date of Delivery
________________________
Edinburgh Date Completed
pre ________ post ________
High Risk Pregnancy? Y N
Date Diagnosed: __________
Concerns/Risk ____________
_____________________________
_____________________________
______________
_____________________________
___________________
# Visits Complete: _________
# Visits Cancelled: _________
FPA Updated: ____________
Transition from Prenatal Mom to
Baby _________________
Month: ________________________ Year _____________ Prenatal Mom’s Name:
Due Date:
Lower Columbia College Early Head Start
Prenatal Attendance Tracking Form (EOM)
Key: C= Visit Completed MV= Make Up Visit MVD= Make Up Visit Declined E= Enrollment Date
NS= No Show X= Parent Cancelled SC= Staff Cancelled W/D= Withdrawn
LOC ID:
ERSEA 2e
1 (C: 07/10; R: 06/16)
Lower Columbia College Early Head Start
Attendance Policy and Procedure
EHS HOME BASE HOME VISIT GUIDANCE REGARDING MISSED HOME VISITS
Schedule families at the beginning of the week whenever possible. Home visits must be
done with the parent/guardian. If they cancel, give them the option of rescheduling for
later in the week.
Discuss what is blocking the family from attendance and brainstorm which times and
days work best. Assess the roadblocks to regular home visit completion with the family.
Discuss the importance of keeping the home visit appointments and the model they have
chosen. Remind them that the model requires a minimum of 46 weekly home visits per
year.
Discuss the importance of developing routines and that adults and children benefit from
predictability in their lives.
Try to schedule families for the same time and day, unless you are making up a visit. If
making up a visit, you can schedule more than 1 per week.
Use a planning calendar regularly on your home visits with the families.
Attendance and absences will be documented in ChildPlus.
If a family has missed two consecutive home visits for the month, and you have
attempted to make them up without success, contact family, send a form letter
documenting the attempts to contact and visit them. (Place one copy of the letter in the
family file, ERSEA 2f1.)
If family reconnects with EHS staff but attendance continues to be inconsistent, staff will
discuss with EHS Supervisor and problem-solve a plan using Home Base
Attendance/Agreement Plan with Parent/Guardian (ERSEA 2g1). EHS staff will discuss
with parent/guardian and place form in child’s file, copy sent to EHS Supervisor.
Drop by the home to try to speak to the family personally. Give them one week to
contact you.
If there is no contact, we will fill their spot with a family from the waiting list.
If there is contact with the family, we will discuss the results with the
EHS Supervisor. An individual plan will be made with each family dependent upon
circumstances to maintain successful attendance.
For families discontinuing services, send a final letter notifying the family that they are
officially dropped from the home based program and that they can call the main office to
be put back on the waiting list for other programs that will better fit their needs. (Copy of
letter placed in family file).
EARLY HEAD START COMBINATION AND
FULL DAY/FULL YEAR (FDFY) TEEN PROGRAM
1. Early Head Start (EHS) Staff Notification
Parents will be informed upon enrollment and reminded periodically to notify the
EHS Staff and center when their child will be absent.
ERSEA 2e
2 (C: 07/10; R: 06/16)
Parents will be expected to call if their child cannot attend the program on a school
day. The explanation should include why the child cannot attend and when the child
will return, if known. All absences excused or not are to be documented in ChildPlus.
The following shall be considered excused absences:
Hospitalization
Illness
Communicable disease
Death in the family
Emergency medical treatment
Family situations
Social Service appointments
Parents will also be expected to call if their child will be late to class and/or if they
will be late picking the child up from class. Children are expected to arrive on time
and be picked up on time. If the child is not picked up within one-hour of the
scheduled ending class time, and staff cannot reach an alternate care provider from
the Family Information Form, staff will be required to notify the EHS Supervisor,
which may result in notification of Child Protective Services (CPS).
Parents will be expected to notify staff if someone else besides themselves will be
picking up their child from the center. No child will be released to a person not
authorized by the parent to pick-up the child. Staff must be notified (in person or by
telephone) when a person not listed on the Family Information Form will be picking
up the child. Identification of this person must be reviewed by staff before releasing
the child.
If EHS staff is not contacted about a child’s absence, the EHS staff will contact the
family on the day of the third consecutive absence. Attendance, absences and Home
Visits are recorded on the Attendance Tracking Form (ERSEA 2e1).
If the family does not have a telephone or is otherwise hard to reach, the EHS staff
member will then attempt to contact the family at their place of residence.
Attendance will be reviewed and documented on the case management form by the
EHS staff.
2. Absences
Chronic Absenteeism. If a child has three or more unexcused absences, or three
consecutive excused absences the following steps will be taken:
a. The EHS staff will contact the family to find out why the child has been
absent, and emphasize the necessity of notifying the classroom if the child is
going to be absent and what the benefits are of regular attendance.
b. The EHS staff will provide appropriate family support as needed. Irregular
attendance will be discussed with the EHS Supervisor and may result in the
development of an Attendance Agreement Plan with the parent to insure
regular attendance of the child.
c. Should a pattern of absences due to illness occur, the EHS staff will follow-up
with the family to make certain that the child has adequate health care.
d. For children who are out due to surgery or lengthy illness, the EHS staff with
the parent will write a parent/child activity plan for the child to be completed
at home.
ERSEA 2e
3 (C: 07/10; R: 06/16)
e. Documentation of absences, contacts with parents and results of conferences
are kept on the education event in ChildPlus.
Extended Absence. If a family situation results in an absence lasting more than two
weeks and following discussion with the EHS Supervisor and EHS Manager/Health
Specialist, the child could be placed back on the waiting list. Upon return, the child
will be placed in the classroom if space is available. All correspondence needs to be
documented in case management.
Failure to Establish Regular Attendance. If attendance does not become regular, and
intensive family support efforts to improve attendance have been made, the contact
cannot be made with the parent, or cooperation cannot be elicited from the parent the
following steps will be taken:
a. The EHS staff will inform the EHS Supervisor of the continued absence.
b. A letter to the parent will be sent by the EHS staff which states the problem,
offers support and gives the parents a deadline to respond to the absence
(ERSEA 2f).
c. If there is no response from the parent within the timeframe of the letter, the
family will be dropped from the program. The EHS Supervisor will make this
decision.
d. The EHS staff member will generate a Change of Status Form stating the
reasons for the drop (See Change of Status (ERSEA 1e). When a family is
dropped from the program due to attendance issues, the EHS staff will request
that the Program Coordinator place the family back on the waitlist if the
family requests or referrals may be made to other community services.
e. The child’s site file will accompany the Change of Status Form and be sent to
the Records Program Coordinator at the main LCC office.
3. Classroom Attendance falls below 85%
The EHS staff with the EHS Supervisor will discuss and analyze the causes of the
absenteeism.
The analysis and action plan will be documented on the Analyzing Attendance Form
located in the Lesson Plan Notebook.
The analysis will include at a minimum the following:
Review any closure days or scheduled days off in the month;
Review any transportation concerns (i.e. applies only to FDFY Teen program);
Review individual pattern of absences for each child, including reasons and
numbers of absences occurring on consecutive days;
Review attendance plans already in place with individual families;
Follow the Attendance Policy and Procedure for individual attendance concerns.
This policy complies with Head Start Performance Standard 1305.8 (a) (b) (c) and Memorandum
Cited (ACYF-IF-HS-00-22)
EHS Home Base Child Attendance ERSEA 2f1
(C: 07/10)
Date________________________
Dear________________________
We are sending this letter because you have missed several home visits and we have been unable
to reschedule them. The Early Head Start staff has made several attempts to contact you by
telephone or in person by leaving you a message at your home. Please contact your Child and
Family Development Specialist______________________ as soon as you receive this letter to
schedule our next visit. If the EHS staff does not hear from you by___________________, you
and your child will be put back on the waiting list and another family will be offered services in
your place.
We look forward to hearing from you.
Sincerely,
________________________ (EHS staff name)
_______________________ _ (phone number)
_________________________ (EHS Supervisor)
If I do not answer, please leave a message with your updated contact information and I will call
you as soon as I possible. Thank you.
EHS Home Base Child Attendance ERSEA 2f1
(C: 07/10; R: 07/11)
Fecha________________________
Estimada________________________
Estamos enviando está carta porque ha perdido varias visitas a su casa y no hemos podido
programar otra. El personal de Early Head Start ha hecho varios intentos para comunicarse con
usted por teléfono o en persona y le hemos dejado mensajes en su casa. Por favor comuníquese
con la Especialista de Desarrollo Infantil y Familiar tan pronto como
reciba esta carta para programar nuestra próxima visita. Si usted no se comunica con el personal
de EHS antes del , usted y su niño serán puestos nuevamente
en la lista de espera y los servicios serán ofrecidos a otra familia.
Estaremos esperando que se comunique con nosotros.
Sinceramente,
________________________ (nombre del personal de EHS)
________________________ (número de teléfono)
_________________________ (Supervisora de EHS)
Si no puedo contestar su llamada, por favor deje un mensaje con su actual información de
contacto y yo me comunicaré con usted tan pronto como me sea posible. Gracias.
EHS Home Base Unable to Contact ERSEA 2f2
(C: 06/11; R: 07/12)
Date________________________
Dear________________________
I’ve really enjoyed our visits and look forward to seeing your family again soon. Unfortunately,
I have been unable to contact you using the contact information I have on file. Please contact me
as soon as you receive this letter so we can schedule your next home visit. As a reminder, Early
Head Start requires that we meet once a week so your family can fully benefit from our program.
If you are having a hard time with this, please call me so we can talk about it.
If I do not hear from you by , your family will have to be put
back on the waiting list and another family will be offered services in your place.
(Home Visitor Name)
(Phone Number)
If I do not answer, please leave a message with your updated contact information and I will call
you as soon as I possibly can. Thank you.
3-5 Child Attendance Letter ERSEA 2f
(R: 07/10)
Fecha:
RE:
Estimado ____________________________:
El Head Start/EHS/ECEAP del Lower Columbia College ha hecho varios intentos para
contactarlo ya sea en persona o por teléfono dejándole un recado en su casa. Su niño ha estado
ausente las siguientes fechas: ______________________________________. Cuando su niño
no se presenta a la escuela por un período de tiempo y no hemos sido capaces de contactarlo o no
hemos sabido nada de usted, es una norma dar de baja a su niño y ponerlo en la lista de espera.
Por favor, póngase en contacto con nosotros al ________________________ antes del
_______________________________ acerca de la inscripción de su niño. Si nosotros no hemos
sabido nada de usted para esta fecha, se seleccionará otro niño para ocupar su lugar en el salón
de clases. Si podemos ayudarlo para el regreso de su niño a la escuela, por favor llámenos.
Atentamente,
Maestra / Personal de EHS
Trabajadora Social
Supervisora
Cc: Child Site File
ERSEA 2f
(R: 07/10)
Date:
RE:
Dear ____________________________:
Lower Columbia College Head Start/EHS/ECEAP has made several attempts to contact you
either by telephone or in person by leaving a message at your home. Your child has been absent
the following dates: ______________________________________. When your child does not
appear at school for a period of time and we have been unable to contact you or have not heard
from you, it is our policy to withdraw your child and place him/her on the waitlist.
Please contact us at ________________________ by _______________________________
regarding your child’s enrollment. If we have not heard from you by this date, another child will
be selected to fill his/her space in the classroom. If we can assist you in returning your child to
school, please call.
Sincerely,
Teacher / EHS Staff
Family Advocate
Supervisor
Cc: Child Site File
ERSEA 2g1
Distribution: Original in file Copies: 1 to parent/guardian, 1 to EHS Supervisor (C: 06/15; R: 06/16)
Lower Columbia College Early Head Start Home Base Attendance/Agreement Plan with Parent/Guardian
Child’s Name Date
Parent’s Name LOC ID
Type of Contact: Phone Personal Contact
% Attendance for month Reason for Absence:
Solution agreed upon:
Family will be placed back on waitlist.
2 consecutive missed visits at any time during the month will result in notification by mail or phone that family will be placed back on the waitlist.
Family will develop an individualized plan with EHS supervisor.
Attendance % will be discussed monthly with family.
Other
EHS Attendance Plan Follow-Up
Date Attendance Improved: Yes No % Attendance Follow-Up Notes:
Plan of Action:
No further action.
Continue with current plan for another: 3 months 6 months
Placed on waitlist: notified by mail notified in person
Develop an individualized plan with EHS Supervisor
Other

ERSEA 3a
1 (C: 03/00; R: 01/16)
Lower Columbia College Head Start/EHS/ECEAP
Selection of Families
Policy
The Selection process will follow the federal and state income guidelines with the goal of
serving the lowest of low-income and those with the greatest need for Head Start/EHS/ECEAP
services following the Selection Criteria approved by Policy Council (see Selection Criteria
Definition ERSEA 3c).
Procedure
1. In order to obtain all necessary data essential in determining eligible children, applicants
for the Head Start/EHS/ECEAP programs will be required to fill out an application and
provide income documentation. Staff will assist parents, as needed. Applications are
accepted year round.
2. To be considered eligible for Head Start/EHS/ECEAP enrollment, the following
requirements must be met:
a. EHS eligibility is prenatal to 3 years’ old.
b. Traditional Head Start/ECEAP eligibility is 3 years old by August 31st.
c. Children must live in the Cowlitz County service area.
d. Families must meet the Head Start/EHS/ECEAP Income Guidelines based on
Federal Poverty Level.
e. Verification of income eligibility may include examination of any of the following:
Income Tax form for the previous year;
W-2 forms for the previous year;
Public Assistance – TANF (Temporary Assistance for Needy Families) or SSI
(Supplemental Security Income); TANF benefits or services include: cash
payments, job training, vouchers, transportation and subsidized child care, such as
Working Connections Child Care (WCCC);
Unemployment history from the Employment Security Office;
Social Security statement for 12 months;
A child in foster care is categorically eligible;
A homeless child is categorically eligible;
For ECEAP – A child who is on an IEP is categorically eligible regardless of
income.
f. Income eligibility will be documented on the Eligibility Verification Form (ERSEA 3b)
by the Program Coordinator. The Eligibility Verification Form notes which documents
were examined to verify income eligibility and both are placed in the child’s site file
along with the Selection Criteria Score Sheet. (See Selection Criteria Score Sheet
ERSEA 3d for 3-5 year program and ERSEA 3d1 for EHS.)
g. A 3-year old child who has been found income eligible and is participating in the
Head Start/ECEAP program remains income eligible throughout that enrollment year
and the following year. An EHS child remains income eligible until transitioning
from EHS at age 3 years as outlined in the Transition from EHS to Head Start /
ECEAP or Appropriate Placement. A child transitioning from EHS to the 3 – 5 year
program must reapply and provide current income verification.
ERSEA 3a
2 (C: 03/00; R: 01/16)
h. A child who is applying for enrollment who resides outside of Cowlitz County must
have permission in writing from the director of their local Head Start/ECEAP
program and will only be considered after exhausting all income eligible children on
the waitlist.
i. When the waitlist is exhausted of all income eligible and categorically eligible
families, Head Start/EHS families who have incomes within 100 – 130% of the
Federal Poverty Level are contacted for enrollment following the selection criteria.
3. Once a child’s family income has been verified the application will be processed through
the Selection Criteria established by the program to give priority to those who are in most
need of Head Start/EHS/ECEAP services. The Selection Criteria gives points for the
following areas: (See Selection Criteria Form ERSEA 3d and/or ERSEA 3d1 for the
number of points given)
a. Parental Status;
b. Disability;
c. Income;
d. Age;
e. Prior status;
f. Need.
4. Requests for transfer within the Head Start/EHS/ECEAP program (because of a change in
the family’s living, working or childcare arrangements) will be given top priority by
following the Request for Change of Classroom (MSYS 7p) procedure set up in
connection with the Content Expert Team.
5. Vacancies will be filled as soon as possible not to exceed 30 days.
a. The intake team member will contact the first family on the waitlist to determine
if the family would like to accept the vacancy.
b. In rare cases, the intake team member (in consultation with the Content Expert
Team) may move to the next child on the waitlist due to age and/or emergent
need. Documentation regarding reasons for this exception will be noted.
6. Over-income children will be placed on the waiting list following any income-eligible
children, and will be considered only if no income-eligible children are on the waiting
list.
7. The Intake Team will contact selected families to complete an enrollment intake. Letters
will be sent to those who remain on the waitlist in September/October. (See Enrollment
Policy and Procedure ERSEA 3c)
Policy complies with Performance Standard 1305.6
Selection of Families ERSEA 3a
(C: 03/00; R: 01/16)
Lower Columbia College Head Start/EHS/ECEAP
Selección de Familias
Política
El proceso de Selección seguirá las pautas federales y estatales acerca de los ingresos, con la meta de
servir a las familias que tengan los ingresos más bajos entre el grupo de familias de ingresos bajos y a las
que tengan más necesidad de los servicios del Head Start/EHS/ECEAP según el Criterio de Selección
aprobado por la Mesa Directiva (ver la Definición de Criterio de Selección ERSEA 3c).
Procedimiento
1. Con el fin de obtener todos los datos esenciales para determinar cuáles de los niños son elegibles,
se les requerirá a los solicitantes al programa Head Start/EHS/ECEAP que completen una
solicitud y provean documentación de sus ingresos. El personal ayudará a los padres como sea
necesario. Las solicitudes se aceptan durante todo el año.
2. Para ser consideradas como elegibles para la inscripción en los programas Head
Start/EHS/ECEAP, las familias necesitan cumplir con los siguientes requisitos:
a. Los niños son elegibles para el EHS desde el período prenatal hasta los 3 años de edad.
b. Los niños son elegibles para el programa tradicional Head Start/ECEAP si tienen 3 años
de edad el 31 de agosto.
c. Los niños tienen que vivir en el área de servicios del condado Cowlitz.
d. Las familias tienen que cumplir con las Pautas de Ingresos del programa Head
Start/EHS/ ECEAP, basadas en el Nivel Federal de Pobreza.
e. La verificación de elegibilidad por los ingresos puede incluir la examinación de cualquier
de los siguientes:
El formulario de impuestos sobre la renta del año anterior.
Formularios W-2 del año anterior.
Asistencia Pública—el TANF (asistencia temporal para las familias necesitadas) o el
SSI (ingresos suplementarios de seguridad); los beneficios del TANF incluyen: pagos
en efectivo, capacitación para el trabajo, vales, transporte y subsidios para la guardería,
como el WCCC (“Working Connections Child Care” o cuidado de niños con
conexiones con el trabajo)
Historial de desempleo de la Employment Security Office (oficina de seguridad de
empleo);
Declaración de Seguro Social, mostrando los beneficios de 12 meses
Un niño que esté en un hogar de acogida es categóricamente elegible;
Un niño sin hogar es categóricamente elegible;
Para el programa ECEAP—un niño que tenga un IEP (plan de educación
individualizada), es categóricamente elegible sin importar los ingresos de su familia.
f. La elegibilidad por los ingresos será documentada en el Formulario de Verificación de
Ingresos (ERSEA 3b) por el Coordinador de Programa. Los documentos que fueron
examinados para verificar su elegibilidad por los ingresos son registrados en el
formulario de verificación de elegibilidad. Los documentos examinados, el formulario de
verificación de elegibilidad y la Puntuación del Criterio de Selección se colocan en el
expediente del niño. (Ver la Puntuación del Criterio de Selección ERSEA 3d para el
programa de 3-5 años y el ERSEA 3d1 para el EHS.)
g. Si se ha determinado que un niño de 3 años es elegible por los ingresos de su familia y
ese niño está participando en el programa Head Start/ECEAP, ese niño se quedará
elegible por los ingresos durante todo ese año programático y durante todo el siguiente.
Un niño del EHS permanece elegible por los ingresos hasta hacer la transición del EHS a
Selection of Families ERSEA 3a
(C: 03/00; R: 01/16)
otro programa, como se describe en la política Transition from EHS to Head
Start/ECEAP or Appropriate Placement (transición del EHS al Head Start/ECEAP o a la
colocación adecuada). La familia de un niño que hace la transición del EHS al programa
de niños de 3-5 años necesita completar otra solicitud y proveer una verificación actual
de sus ingresos.
h. La familia de un niño que solicite la inscripción y resida fuera del condado Cowlitz
necesita el permiso escrito del director de su programa local del Head Start/ECEAP y el
niño sólo será considerado después que estén inscritos todos los niños de la lista de
espera que sean elegibles por los ingresos de sus familias.
i. Cuando estén inscritos todos los niños de la lista de espera que sean categóricamente
elegibles o que sean elegibles por sus ingresos, las familias del Head Start/ECEAP que
tengan ingresos dentro de 100-130% del nivel federal de pobreza serán contactadas según
el criterio de selección.
3. Después de ser verificados los ingresos de la familia de un niño, la solicitud será tramitada
siguiendo el Criterio de Selección establecido por el programa con el propósito de dar la prioridad
a las personas que más necesiten los servicios del Head Start/EHS/ECEAP. El Criterio de
Selección asigna puntos a los niños en las siguientes áreas (Ver el Formulario de Criterio de
Selección ERSEA 3d o 3d1 para ver el número de puntos otorgados)
a. Situación Familiar
b. Discapacidad
c. Ingreso
d. Edad al 31 de agosto
e. Situación Anterior
f. Necesidades
4. La más alta prioridad será dada a las peticiones de traslado dentro del programa Head
Start/ECEAP/EHS (por causa de un cambio de la situación de vivienda, el trabajo o la guardería
de una familia), siguiendo el procedimiento del formulario para solicitar un cambio de clase (el
MSYS 7p—“Request for Change of Classroom”), que es desarrollado con la ayuda del equipo de
expertos de contenido (Content Expert Team).
5. Las vacantes serán cubiertas lo más antes posible, en un plazo que no exceda 30 días.
a. El miembro del equipo de inscripciones (Intake Team) contactará a la familia que esté
más alta en la lista de espera para determinar si la familia quisiera aceptar la vacante.
b. En casos muy raros, el miembro del equipo de inscripciones (en consultación con el
equipo de expertos de contenido) puede contactar a la familia del siguiente niño debido a
la edad y/o una necesidad emergente que tenga. Se anotará la documentación sobre los
motivos de esta excepción.
6. Los niños de familias cuyos ingresos excedan los límites de ingresos serán colocados en la lista
de espera después de los niños de familias elegibles por sus ingresos y solamente serán
considerados si no hay niños en la lista de espera que sean de familias elegibles por los ingresos.
7. El equipo de inscripciones contactará a las familias seleccionadas para completar una entrevista
de inscripción. Se les mandarán cartas a las familias de niños que todavía estén en la lista de
espera en el septiembre o el octubre. (Ver la Inscripción de Familias--ERSEA 3c)
Esta política cumple con la norma de rendimiento “Performance Standard 1305.6”
ERSEA 3b1
Print on Yellow (R: 04/11; C: 04/09)
Lower Columbia College Head Start / EHS / ECEAP
Verification of Homeless Status
Homelessness means individuals who lack a fixed, regular, and adequate nighttime residence.
1. Child’s Name: ___________________________________________________________
2. Child’s date of birth: ______________________________________________________
3. Verify status. Check which category children and youths are in:
Children and youth who are sharing housing of other persons due to loss of housing,
economic hardship, or similar reason; Living in motels, hotels, trailer parks, or
camping grounds due to lack of alternative adequate accommodations; Living in
emergency or transitional shelters; Are abandoned in hospitals; or are awaiting foster
care placement;
Children and youths who have a primary nighttime residence that is a public or
private place not designed for or ordinarily used as a regular sleeping accommodation
for human beings; and
Children and youths who are living in cars, parks, public space, abandoned buildings,
substandard housing, bus or train stations, or similar settings.
Staff Signature _______________________________ Date of eligibility verification: _________________
Staff Name: ______________________________________ Title: ________________________________
ERSEA 3b
Print on Yellow (C: 04/09; R: 07/17)
Lower Columbia College Head Start/EHS/ECEAP
Eligibility Verification
1. Child’s Name:
2. Child’s date of birth:
3. Staff conducted interview with family:
In person
By telephone
4. Verify Eligibility. Check which category of eligibility this child falls into:
Public Assistance
SSI (Head Start ONLY!)
IEP (ECEAP Only)
Homeless
Foster Care
Income
Head Start/Early Head Start:
Below federal poverty guidelines
Between 100 < 130% of Federal Poverty Guidelines (no more than 35% of
Head Start enrolled children may fall into this category)
Over-Income
ECEAP:
Below ECEAP Income Eligibility Guidelines (up to 110% of the Federal Poverty
Guidelines (FPL))
Over-Income
5. What documentation was used to determine eligibility?
Income Tax Form 1040 Written statements from employers
W-2 Foster care reimbursement
TANF documentation SSI documentation
Pay stub or pay envelopes Other
Unemployment If other, please explain:
Documentation of no income
I have carefully reviewed the documents and information that has been provided to me by the
applicant, and, by signing this form, certify to the best of my knowledge and belief that all
information regarding eligibility provided to me is true and accurate.
6. Staff Signature: Date of eligibility verification:
7. Staff Name: Title:
ERSEA 3c
(C: 09/10; R: 02/16)
Lower Columbia College Early Head Start
Enrollment of Families
Procedure
1. Definition of Program Models
a. Home Base – Weekly home visits (1.5 hours); twice monthly Play and Learn
Groups (Socializations)
b. Full Day Teen Program with Longview School District – 5 days a week; 7 hours a
day; September to June (Summer goes to home base)
c. Pregnant Mothers – Services are provided as indicated on the individualized
Home Visit Plan form for Prenatal Families through the Family Partnership
process.
2. For the purpose of determining eligibility based on family income, the pregnant woman is
counted as two members of the household. In the case of an unmarried pregnant teen, her
own income determines her eligibility regardless of her parent’s income.
3. For the purpose of determining the number of individuals enrolled in an EHS program,
the pregnant woman is counted as the one who is enrolled. One month following the
birth of the child, it is the child who is enrolled in the EHS program. Regulations
governing Program Models do not apply to pregnant women. EHS Staff are not required
to follow the frequency and duration of home visits that are required in the Home Base
Program.
4. Upon completion of the selection process of eligible children and/or pregnant mother the
Program Coordinator will generate a child/family site file, which is given to the
appropriate EHS staff member after the enrollment intake is complete. If needed, an
interpreter will assist with the non-English speaking families.
5. Once the pregnant mother delivers the baby the EHS Staff member will add information
on the newborn to the existing EHS application. Entry in Early Head Start will not begin
until child is at least 4 weeks old.
6. A Parent Orientation will be completed on the Home Visit.
7. Once a child is selected from the waitlist and the Program Coordinator completes an
intake, the child is accepted and considered enrolled in the Early Head Start program.
8. Vacancies will be filled within 30-days following the selection criteria.
9. Children who are enrolled in EHS will remain income eligible while they are
participating in the program. When a child moves from a program serving infants and
toddlers to a Head Start program serving children age three and older, they family income
must be re-verified.
10. When an eligible child is enrolled in EHS and they reach 30 months of age, a transition
plan in implemented.
EHS Enrollment of Families ERSEA 3c
(C: 09/10; R: 02/16)
Lower Columbia College Early Head Start
Inscripción de Familias
Procedimiento
1. Definición de Modelos del Programa
a. Home Base – Visitas semanales al hogar (1.5 horas), dos veces al mes Grupos de Juego
y Aprendizaje (Socializaciones)
b. Programa de Todo el Día para Adolecentes con el Distrito Escolar de Longview– 5 días
a la semana, 7 horas al día, Septiembre a Junio (el verano va a home base)
c. Madres embarazadas –Los servicios son provistos como es indicado en la forma del Plan
de Visitas al Hogar para Familias Prenatales a través del proceso de Asociación de la
Familia.
2. Con el propósito de determinar la elegibilidad en base al ingreso de la familia, la mujer
embarazada es contada como dos miembros en el hogar. En el caso de una adolescente soltera
embarazada, su propio ingreso determina su elegibilidad sin tener en cuenta el ingreso de sus
padres.
3. Con el propósito de determinar el número de individuos inscritos en un programa de EHS, la
mujer embarazada es contada como uno que está inscrito. Un mes de seguimiento del nacimiento
del niño, esto es el niño que está inscrito en el programa de EHS. Las Normas de gobierno de los
Modelos de Programas no se aplica para la mujer embarazada. El personal de EHS no está
obligado a seguir la frecuencia y duración de las visitas al hogar que son requeridos en el
Programa de Home Base.
4. Una vez finalizado el proceso de selección de los niños elegibles y/o madre gestante, el
Coordinador de Programa iniciará un expediente del niño/familia, el cual es entregado al
miembro apropiado del personal de EHS después que el proceso de inscripción sea completado.
Si es necesario, una intérprete apoyará a las familias que no hablan inglés.
5. Una vez que la madre embarazada da a luz, el miembro del personal de EHS añadirá información
en la solicitud existente del recién nacido. El ingreso del niño en Early Head Start no comenzará
hasta que el niño tenga al menos 4 semanas de edad.
6. La Orientación de Padres será completado en la Visita al Hogar.
7. Una vez que el niño sea seleccionado de la lista de espera y el Coordinador del Programa
completa la admisión, el niño es aceptado y considerado inscrito en el programa de Early Head
Start.
8. Las vacantes serán cubiertas dentro de los 30 días siguiendo el criterio de selección.
9. Los niños quienes están inscritos en EHS permanecerán siendo de ingreso elegible, mientras ellos
estén participando en el programa. Cuando el niño se traslada de un programa sirviendo a bebés y
niños pequeños a un programa de Head Start sirviendo a niños de edad de tres años y mayor de 3
años, el ingreso de la familia debe ser verificado nuevamente.
10. Cuando un niño elegible es inscrito en EHS y ellos alcanzan los 30 meses de edad, un plan de
transición es implementado.
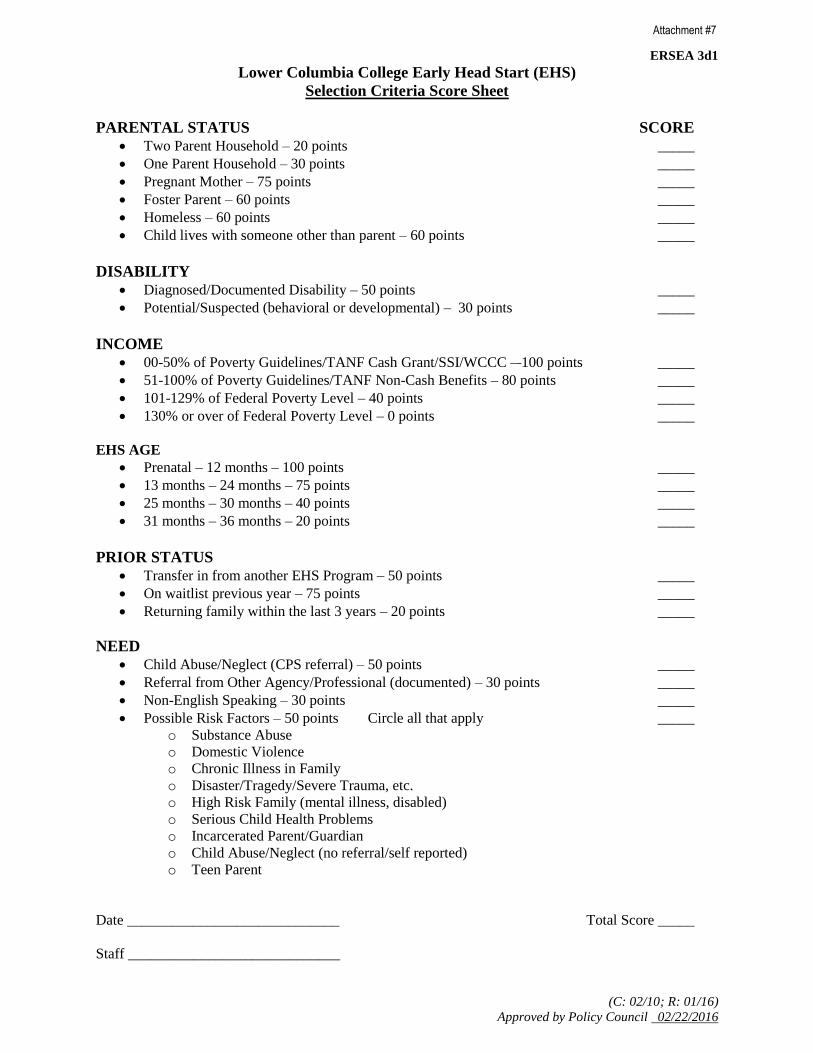
ERSEA 3d1
(C: 02/10; R: 01/16)
Approved by Policy Council 02/22/2016
Attachment #7
Lower Columbia College Early Head Start (EHS)
Selection Criteria Score Sheet
PARENTAL STATUS SCORE
Two Parent Household – 20 points _____
One Parent Household – 30 points _____
Pregnant Mother – 75 points _____
Foster Parent – 60 points _____
Homeless – 60 points _____
Child lives with someone other than parent – 60 points _____
DISABILITY
Diagnosed/Documented Disability – 50 points _____
Potential/Suspected (behavioral or developmental) – 30 points _____
INCOME
00-50% of Poverty Guidelines/TANF Cash Grant/SSI/WCCC – 100 points _____
51-100% of Poverty Guidelines/TANF Non-Cash Benefits – 80 points _____
101-129% of Federal Poverty Level – 40 points _____
130% or over of Federal Poverty Level – 0 points _____
EHS AGE
Prenatal – 12 months – 100 points _____
13 months – 24 months – 75 points _____
25 months – 30 months – 40 points _____
31 months – 36 months – 20 points _____
PRIOR STATUS
Transfer in from another EHS Program – 50 points _____
On waitlist previous year – 75 points _____
Returning family within the last 3 years – 20 points _____
NEED
Child Abuse/Neglect (CPS referral) – 50 points _____
Referral from Other Agency/Professional (documented) – 30 points _____
Non-English Speaking – 30 points _____
Possible Risk Factors – 50 points Circle all that apply _____
o Substance Abuse
o Domestic Violence
o Chronic Illness in Family
o Disaster/Tragedy/Severe Trauma, etc.
o High Risk Family (mental illness, disabled)
o Serious Child Health Problems
o Incarcerated Parent/Guardian
o Child Abuse/Neglect (no referral/self reported)
o Teen Parent
Date _____________________________ Total Score _____
Staff _____________________________
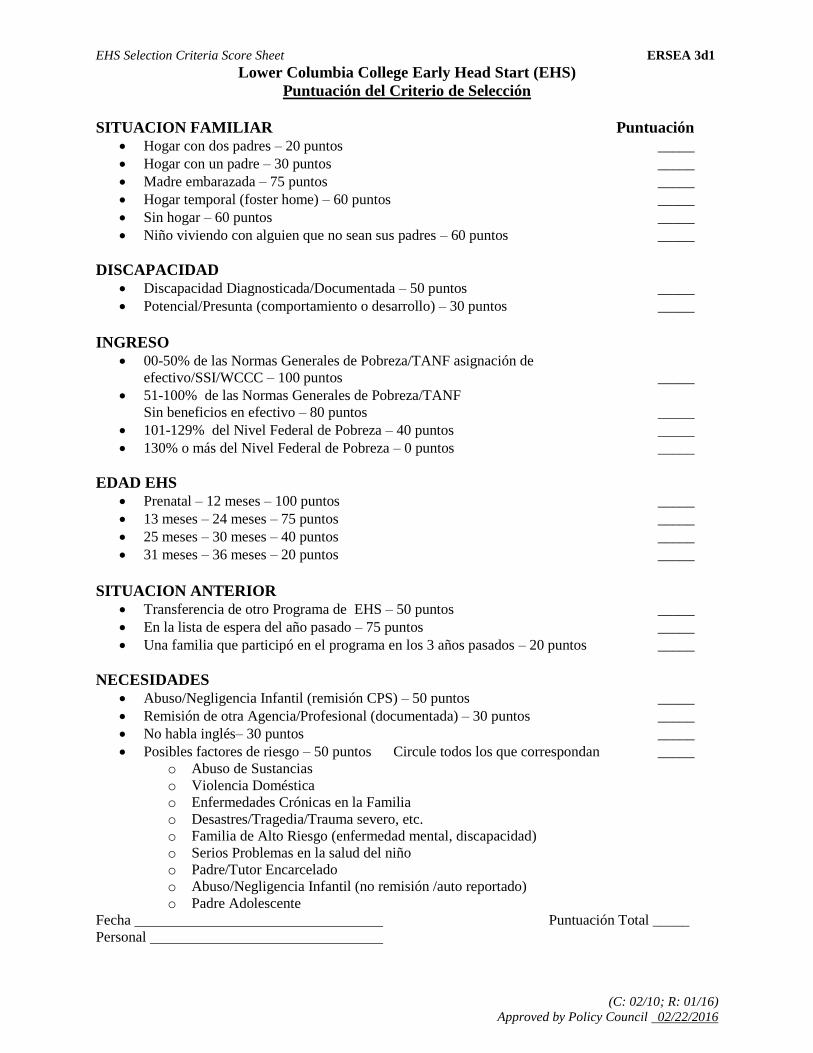
EHS Selection Criteria Score Sheet ERSEA 3d1
(C: 02/10; R: 01/16)
Approved by Policy Council 02/22/2016
Lower Columbia College Early Head Start (EHS)
Puntuación del Criterio de Selección
SITUACION FAMILIAR Puntuación
Hogar con dos padres – 20 puntos _____
Hogar con un padre – 30 puntos _____
Madre embarazada – 75 puntos _____
Hogar temporal (foster home) – 60 puntos _____
Sin hogar – 60 puntos _____
Niño viviendo con alguien que no sean sus padres – 60 puntos _____
DISCAPACIDAD
Discapacidad Diagnosticada/Documentada – 50 puntos _____
Potencial/Presunta (comportamiento o desarrollo) – 30 puntos _____
INGRESO
00-50% de las Normas Generales de Pobreza/TANF asignación de
efectivo/SSI/WCCC – 100 puntos _____
51-100% de las Normas Generales de Pobreza/TANF
Sin beneficios en efectivo – 80 puntos _____
101-129% del Nivel Federal de Pobreza – 40 puntos _____
130% o más del Nivel Federal de Pobreza – 0 puntos _____
EDAD EHS
Prenatal – 12 meses – 100 puntos _____
13 meses – 24 meses – 75 puntos _____
25 meses – 30 meses – 40 puntos _____
31 meses – 36 meses – 20 puntos _____
SITUACION ANTERIOR
Transferencia de otro Programa de EHS – 50 puntos _____
En la lista de espera del año pasado – 75 puntos _____
Una familia que participó en el programa en los 3 años pasados – 20 puntos _____
NECESIDADES
Abuso/Negligencia Infantil (remisión CPS) – 50 puntos _____
Remisión de otra Agencia/Profesional (documentada) – 30 puntos _____
No habla inglés– 30 puntos _____
Posibles factores de riesgo – 50 puntos Circule todos los que correspondan _____
o Abuso de Sustancias
o Violencia Doméstica
o Enfermedades Crónicas en la Familia
o Desastres/Tragedia/Trauma severo, etc.
o Familia de Alto Riesgo (enfermedad mental, discapacidad)
o Serios Problemas en la salud del niño
o Padre/Tutor Encarcelado
o Abuso/Negligencia Infantil (no remisión /auto reportado)
o Padre Adolescente
Fecha Puntuación Total _____
Personal
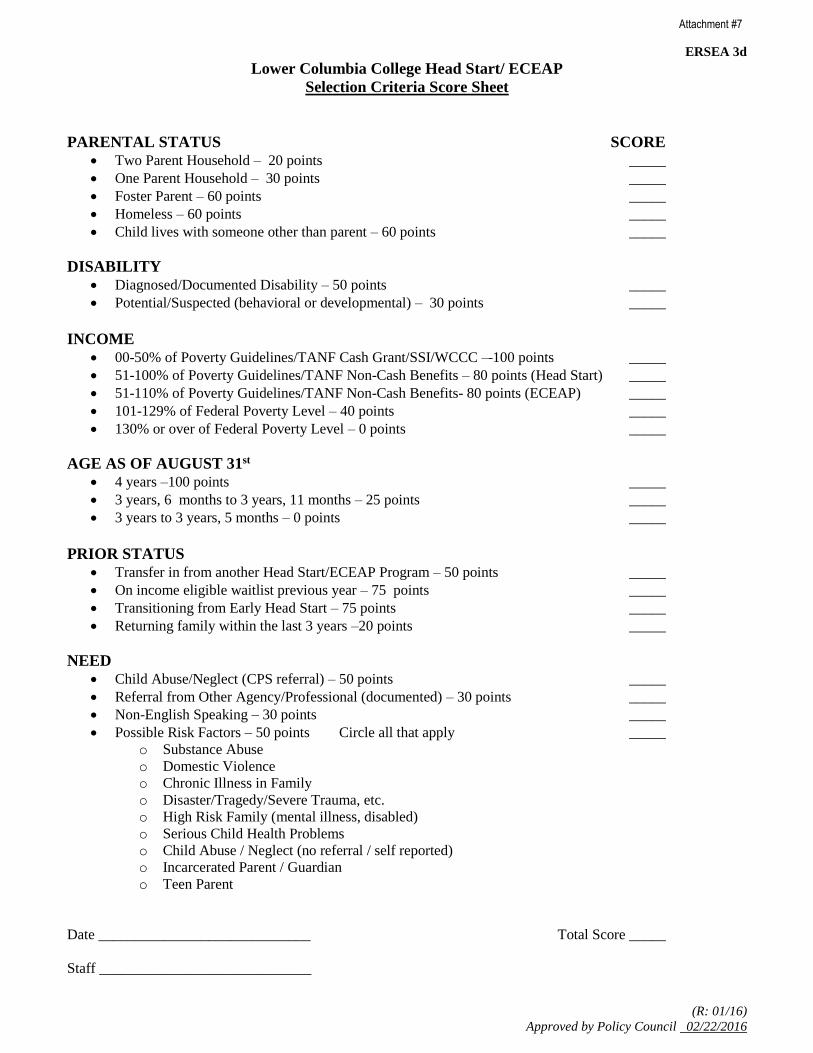
ERSEA 3d
(R: 01/16)
Approved by Policy Council 02/22/2016
Attachment #7
Lower Columbia College Head Start/ ECEAP
Selection Criteria Score Sheet
PARENTAL STATUS SCORE
Two Parent Household – 20 points _____
One Parent Household – 30 points _____
Foster Parent – 60 points _____
Homeless – 60 points _____
Child lives with someone other than parent – 60 points _____
DISABILITY
Diagnosed/Documented Disability – 50 points _____
Potential/Suspected (behavioral or developmental) – 30 points _____
INCOME
00-50% of Poverty Guidelines/TANF Cash Grant/SSI/WCCC – 100 points _____
51-100% of Poverty Guidelines/TANF Non-Cash Benefits – 80 points (Head Start) _____
51-110% of Poverty Guidelines/TANF Non-Cash Benefits- 80 points (ECEAP) _____
101-129% of Federal Poverty Level – 40 points _____
130% or over of Federal Poverty Level – 0 points _____
AGE AS OF AUGUST 31st
4 years –100 points _____
3 years, 6 months to 3 years, 11 months – 25 points _____
3 years to 3 years, 5 months – 0 points _____
PRIOR STATUS
Transfer in from another Head Start/ECEAP Program – 50 points _____
On income eligible waitlist previous year – 75 points _____
Transitioning from Early Head Start – 75 points _____
Returning family within the last 3 years –20 points _____
NEED
Child Abuse/Neglect (CPS referral) – 50 points _____
Referral from Other Agency/Professional (documented) – 30 points _____
Non-English Speaking – 30 points _____
Possible Risk Factors – 50 points Circle all that apply _____
o Substance Abuse
o Domestic Violence
o Chronic Illness in Family
o Disaster/Tragedy/Severe Trauma, etc.
o High Risk Family (mental illness, disabled)
o Serious Child Health Problems
o Child Abuse / Neglect (no referral / self reported)
o Incarcerated Parent / Guardian
o Teen Parent
Date _____________________________ Total Score _____
Staff _____________________________
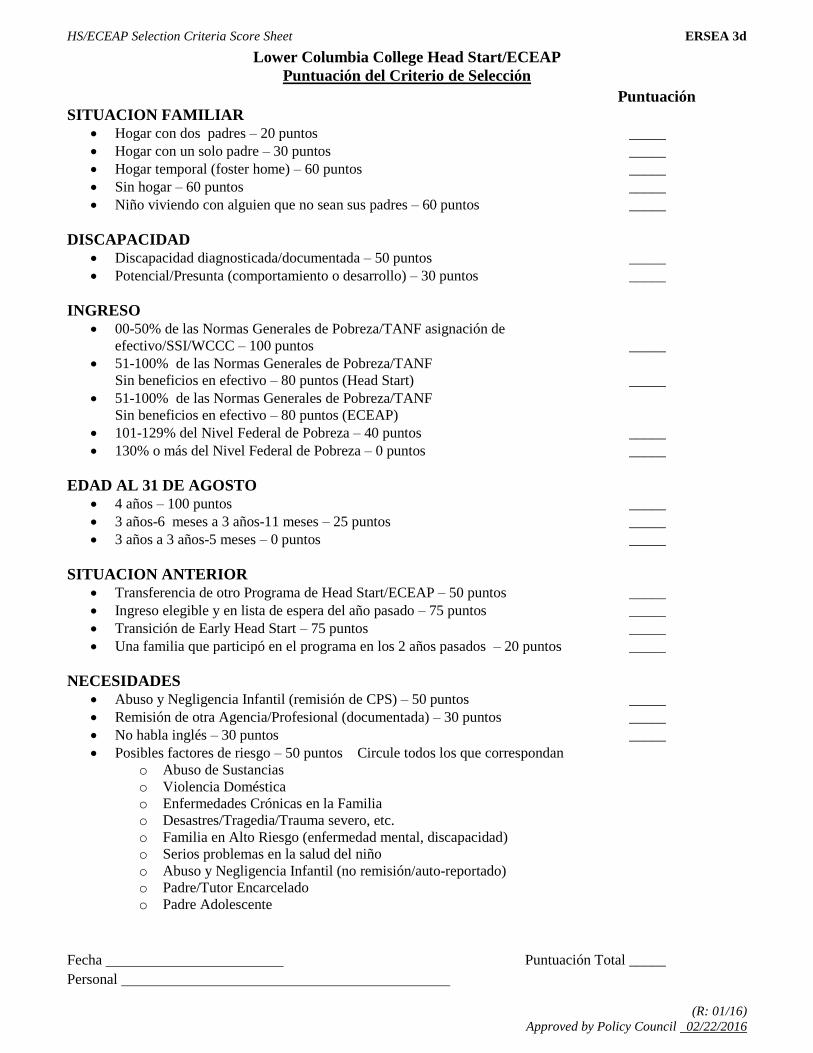
HS/ECEAP Selection Criteria Score Sheet ERSEA 3d
(R: 01/16)
Approved by Policy Council 02/22/2016
Lower Columbia College Head Start/ECEAP
Puntuación del Criterio de Selección
Puntuación
SITUACION FAMILIAR Hogar con dos padres – 20 puntos _____
Hogar con un solo padre – 30 puntos _____
Hogar temporal (foster home) – 60 puntos _____
Sin hogar – 60 puntos _____
Niño viviendo con alguien que no sean sus padres – 60 puntos _____
DISCAPACIDAD
Discapacidad diagnosticada/documentada – 50 puntos _____
Potencial/Presunta (comportamiento o desarrollo) – 30 puntos _____
INGRESO
00-50% de las Normas Generales de Pobreza/TANF asignación de
efectivo/SSI/WCCC – 100 puntos _____
51-100% de las Normas Generales de Pobreza/TANF
Sin beneficios en efectivo – 80 puntos (Head Start) _____
51-100% de las Normas Generales de Pobreza/TANF
Sin beneficios en efectivo – 80 puntos (ECEAP)
101-129% del Nivel Federal de Pobreza – 40 puntos _____
130% o más del Nivel Federal de Pobreza – 0 puntos _____
EDAD AL 31 DE AGOSTO
4 años – 100 puntos _____
3 años-6 meses a 3 años-11 meses – 25 puntos _____
3 años a 3 años-5 meses – 0 puntos _____
SITUACION ANTERIOR
Transferencia de otro Programa de Head Start/ECEAP – 50 puntos _____
Ingreso elegible y en lista de espera del año pasado – 75 puntos _____
Transición de Early Head Start – 75 puntos _____
Una familia que participó en el programa en los 2 años pasados – 20 puntos _____
NECESIDADES
Abuso y Negligencia Infantil (remisión de CPS) – 50 puntos _____
Remisión de otra Agencia/Profesional (documentada) – 30 puntos _____
No habla inglés – 30 puntos _____
Posibles factores de riesgo – 50 puntos Circule todos los que correspondan
o Abuso de Sustancias
o Violencia Doméstica
o Enfermedades Crónicas en la Familia
o Desastres/Tragedia/Trauma severo, etc.
o Familia en Alto Riesgo (enfermedad mental, discapacidad)
o Serios problemas en la salud del niño
o Abuso y Negligencia Infantil (no remisión/auto-reportado)
o Padre/Tutor Encarcelado
o Padre Adolescente
Fecha Puntuación Total _____
Personal
ERSEA 3e
Policy complies with Head Start Program Performance Standards, ECEAP Performance Standards,
Child Care Licensing and WAC (C: 03/00, R: 07/17)
Lower Columbia College Head Start/ECEAP
Enrollment of Families
Policy Lower Columbia College Head Start/Early Childhood Education and Assistance Program will serve
children who will be three years old by August 31st. Ninety percent of children served will meet the Head
Start/ECEA Program income eligibility standards. A maximum of ten (10) percent of enrolled children
per funding source of Head Start/ECEAP may be over income. At least ten (10) percent of the total
number enrolled in Head Start / ECEAP will be children with disabilities.
Procedure
1. Definition of Program Models
a. Traditional (Part-day) Head Start classrooms – 3.5 hours a day, 4 days a week September to
June.
b. Traditional (Part-day) ECEAP classrooms – 3.5 hours a day, 3 or 4 days a week September to
June.
c. Full Day (6 hour) ECEAP classrooms, 5 days a week September to June.
d. Full Day (6 hour) Head Start classrooms, 5 days a week September to June.
2. Upon completion of the selection process of eligible children, an appointment will be made with
individual families by an Intake Team member to complete an enrollment intake with the family. An
interpreter will complete intakes for non-English speaking families.
3. The parent is asked to bring to the enrollment intake appointment their child’s immunization record,
birth certificate, and proof of insurance information. They are also asked to make an appointment for
their child’s physical and dental exam and provide those dates at the time of their enrollment intake.
If they do not have insurance or a physician/dentist, the Intake Team member will provide a list of
providers.
4. An intake packet will be completed with a member of intake team.
5. After the intake process is completed a child site file is generated on the child/family and is given to
the Family Advocate or Child Family Development Specialist of the classroom the child will be
attending. (See MSYS 7a Record Keeping Policy and Procedure MSYS 7a).
6. Prior to the beginning of class if possible, the family will receive a Welcome Visit by the Family
Advocate or Child Family Development Specialist. (See FS/PI 7a Welcome Visit Policy and
Procedure).
7. At the beginning of the program year a Parent/Child Orientation will be held to introduce the
child/family to the classroom, center, program services, and staff. During the program year, if a new
child/family enrolls the Family Advocate or Child Family Development Specialist will complete a
parent orientation. (See FS/PI 13a Parent/Child Orientation Policy and Procedure).
8. Once a child is accepted and an intake completed the child is considered enrolled in Head
Start/ECEAP. Those children accepted for the upcoming program year will be considered enrolled on
the first service day of class.
9. For families who are returning, the Family Advocate or Child Family Development Specialist will
review in the spring of the current year all pertinent information with the family (i.e. address, phone,
emergency contacts, and additions to the family unit, etc). Any changes will be documented on the
Change of Status form, signed by the parent and turned into the Program Coordinator.
10. After the start of the enrollment year, vacancies are filled as they occur from the waitlist. Families
are notified that they are on a waitlist in September / October.
11. Vacancies in both Head Start and ECEAP part-day sessions will not be filled when 30 days or less
remain in the programs enrollment year.
Enrollment of Families ERSEA 3e
Esta política cumple con la norma de rendimiento “Performance Standard 1305.7(a)(b)(c)” (C: 03/00; R: 02/16)
Lower Columbia College Head Start/ECEAP
Inscripción de Familias
Política El Head Start/Early Childhood Education and Assistance Program (programa de educación y asistencia de
la primera infancia) servirá a niños que van a cumplir los 3 años de edad el 31 de agosto o antes. Noventa
por ciento de los niños servidos cumplirán con las pautas de elegibilidad del programa Head Start/ECEAP
sobre los ingresos. Entre los niños inscritos, un máximo de diez (10) por ciento por fuente de
financiación puede ser de familias que tengan más ingresos que el límite. Por lo menos diez (10) por
ciento de todos los niños inscritos en los programas de Head Start/ECEAP serán niños con una
discapacidad.
Procedimiento 1. Definiciones de Modelos del Programa
a. Clases Tradicionales (de día parcial) del Head Start—3.5 horas al día, 4 días a la semana
de septiembre hasta junio.
b. Clases Tradicionales (de día parcial) del ECEAP—3.5 horas al día, 3 o 4 días a la semana
de septiembre a junio.
c. Clases de Todo el Día (6 horas) del ECEAP, 5 días a la semana de septiembre a junio.
2. Después de ser finalizado el proceso de inscripción de los niños elegibles, uno de los miembros
del equipo de inscripciones (Intake Team) programará una cita con cada familia para completar
una entrevista de inscripción con la familia. Un intérprete completará la entrevista de inscripción
para las familias que no hablen inglés.
3. A los padres se les pide llevar las siguientes cosas a la entrevista de inscripción: el registro de
vacunas de su hijo, su acta de nacimiento y su información de cupón médico o una prueba de
seguros médicos. También se les pide que programen una cita para un examen dental y un
examen físico y que provean esas fechas a la hora de su entrevista de inscripción. Si no tienen
seguros médicos o si no tienen doctor o dentista, el miembro del equipo de inscripciones le dará
una lista de proveedores de esos servicios.
4. Un paquete de inscripción será completado con un miembro del equipo de inscripciones.
5. Después de completar el proceso de inscripción, un expediente del niño/familia será generado y
será entregado a la trabajadora social de la clase a que asistirá el niño. (Ver MSYS 7a--Record
Keeping Policy and Procedure).
6. Antes del comienzo de clases, si es posible, la familia recibirá una visita de bienvenida de la
trabajadora social. (Ver FS/PI 7a Welcome Visit Policy and Procedure).
7. Al comienzo del año programático, se realizará una reunión de Orientación de Padres y Niños
para que el niño y la familia conozcan el salón, el centro, los servicios del programa y al personal.
Durante el año programático, si un nuevo niño o familia se inscribe en el programa, la trabajadora
social completará una orientación de padres con la familia. (Ver FS/PI 13a Parent/Child
Orientation Policy and Procedure).
8. Una vez que un niño sea aceptado y una entrevista de inscripción sea completada, el niño será
considerado inscrito en el Head Start/ECEAP. Los niños inscritos en el siguiente año
programático serán considerados inscritos el primer día de clases.
9. Para las familias que regresen, la trabajadora social revisará con la familia toda la información
relevante (o sea, el domicilio, el teléfono, los contactos de emergencia, los miembros adicionales
de la familia, etc.) en la primavera del año actual. Los cambios serán documentados en el
formulario “Change of Status” (cambio de situación), que será firmado por el padre o la madre y
será entregado al Coordinador del Programa.
10. Después de comenzar el año programático, cuando ocurran vacantes éstas serán cubiertas con
niños que estén en la lista de espera. En septiembre u octubre las familias serán notificadas que
están en la lista de espera.
11. Cuando 60 días o menos quedan del año programático, no se cubrirán las vacantes de las clases
de día parcial en el Head Start/ECEAP.
ERSEA 4a1
Print on Yellow (C: 06/10; R: 08/16)
LOWER COLUMBIA COLLEGE EARLY HEAD START
Intake/Enrollment Appointment
Child: Birthdate:
Parent/Guardian:
Phone: Other Phone:
Intake Date: Time: First Home Visit Date: Time:
Reminder(s)
EHS Staff Member: LOC ID:
Enrollment Date:
When calling to schedule Intake Appointment/Home Visit, discuss the items below with parent.
Shot Records
Medical Coupon/Insurance Card
Birth Certificate
Physician/Clinic
Appt:
Dentist
Appt:
WIC
Specialist
Progress Center
==========================================================================
INTAKE FORMS CHECKLIST
Date Completed/Reviewed:
_______ ChildPlus Contact Information #1520 _______ Health History/Nutrition Intake
_______ Parent Agreement Contract _______ PIR Health & Child Care
Releases: Questionnaire
_______ Medical _______ WA State Immunization Form
_______ Dental (with parent signature and date 2 times)
_______ Birth Hospital (for infants only i.e. PeaceHealth/ _______ Caries Risk Assessment
St. John and Legacy Salmon Creek Medical Centers) _______ Case Management (Intake Event
_______ Specialists Entry on ChildPlus, Family Services)
_______ Mental Health _______ USDA Enrollment
_______ Progress Center _______ Formula Offer Form (Infant)
_______ WIC _______ Diaper/Pull-Up Offer Form
_______ OHSU _______ Review Application
_______ Other ____________________
Prior to child being at a program center: A completed Washington State Immunization form, a
completed USDA Enrollment form and Formula Offer Form (infants only) must be on file. A child,
attending a center-based model, must also have a completed Health History/Nutrition Intake form and a
completed Parent Agreement Contract on file.
ERSEA 4a2
Print on Yellow (C: 07/10; R: 06/16)
LOWER COLUMBIA COLLEGE EARLY HEAD START – PRENATAL
Intake/Enrollment Appointment
Expectant Mother: Birthdate:
Due Date of Baby: ____________________________________
Phone: Other Phone:
Home Visit Date: Time:
Reminder(s)
EHS Staff Member: LOC ID:
When calling to schedule Intake Appointment/Home Visit, discuss the items below with expectant mother.
Medical Coupon / Insurance Card
Physician / Clinic
Appt:
Dentist
Appt:
WIC
==========================================================================
INTAKE FORMS CHECKLIST
Date Completed/Reviewed:
_______ ChildPlus Contact Information #1520
_______ Prenatal Emergency Information Form
_______ WIC Release
_______ First Steps Release
_______ Review Application
_______ Releases (Optional)
_______ Medical
_______ Dental
_______ Mental Health
_______ Other ____________________
_______ Prenatal Health/Dental/Nutrition
History
_______ Prenatal Dental History Questionnaire
_______ Case Management (Intake Event Entry
on ChildPlus, Family Services)
_______ Parent Agreement Contract
ERSEA 4a
Print on Yellow (C: 05/05; R: 03/15)
Lower Columbia College Head Start/ECEAP
INTAKE APPOINTMENT
Child: Birthdate:
Does the child need an interpreter? (circle one) Yes No If yes, what language?
Parent/Guardian:
Phone: Other Phone:
Appointment Date: Time:
Reminder(s)
Teacher: LOC ID:
When calling to remind of appointment, remind parent of items they
are to bring including appointment dates if they’ve already made them.
Parent to bring in:
□ Shot Records □ Insurance Card □ Birth Certificate
□ Physician / Clinic
Appt:
Dentist:
Appt:
WIC
Specialist
=====================================================================
INTAKE FORMS CHECKLIST
□ ChildPlus Contact Information #1520
□ Birth Certificate
□ Application Information/Income
Verification/Criteria Score Sheet
□ Releases
□ Medical
□ Dental
□ Specialists
□ Mental health
□ WIC
□ OHSU
□ School Districts
□ Other ______________________
□ HOFL Registration Form
□ PIR Enrollment Questionnaire
□ Immunization Form (with parent
signature)
□ Health History/Nutrition Intake
□ Caries Risk Assessment
□ Intake Event Entry on ChildPlus,
Family Services
□ Review Application
□ Sex Offender verification of parents/
emergency contact
HANDOUTS:
□ Bright Futures “3 or 4 yr. visit”
□ Dental Do’s/Health Exam Do’s
□ Healthy Eating/Active Play
□ Lead Screening
Signature
Date
ERSEA 5a
(C: 03/00, R: 02/12)
Lower Columbia College Head Start/EHS/ECEAP
Recruitment Plan
Policy
In order to reach those most in need of Lower Columbia College Head Start (HS) / Early Head
Start (EHS) / Early Childhood Education Assistance Program (ECEAP) availability of services
the recruitment process will be followed to actively inform and encourage all income eligible
families, pregnant women and children with disabilities regardless of sex, race, creed, color or
national origin to apply for admission to the program.
Procedure
A Recruitment/Selection committee will be established in October of each year comprised of
parents, staff and leadership. The main goal of this committee is to identify families whose
children are age eligible for Head Start/EHS/ECEAP, meet the income guidelines and the
recruitment efforts throughout the county. In order to serve the families with the greatest need
the following recruitment process takes place.
1. Obtain current information for returning Head Start / EHS/ ECEAP students by the end of
the program year.
2. Update the existing waitlist showing only age eligible children.
3. Parents and staff will talk with local agencies, service organizations, PTA/PTO
organizations, and elementary teachers to promote Head Start/ EHS / ECEAP in the
community.
4. Local radio stations will air spots for public service announcements that run several times
a day through out the recruitment period.
5. The local newspaper will be contacted year round for possible feature stories about Head
Start / EHS / ECEAP focusing on recruitment.
6. The Lower Columbia College reader board will be utilized to promote enrollment.
7. On the campus of Lower Columbia College, the registration office, student center, ESL
and ABE classes and campus bulletin boards are provided with flyers and asked to refer
students/families.
8. The Community Partnership/Public Relations Specialist heads up public relations events
throughout the year. For example: Earth Day, Safe Kids Day, the Hispanic Health Fair,
Holiday Parade, Prevention Fair, National Night Out, Go 4th
Parade and the International
Festival are possible recruitment events during the year.
9. The Direct Service Teams will provide current parents with applications in the spring for
any age eligible siblings listed on our database.
ERSEA 5a
(C: 03/00, R: 02/12)
10. Each parent will be provided with recruitment flyers to give to a friend or neighbor that
has an eligible child.
11. Address lists of low-income families in the Cowlitz County service area provided by
DSHS are utilized for recruitment mailings.
12. Rally Day Events:
Head Start/EHS/ECEAP brochures, flyers and posters are delivered to agencies,
churches, dental offices, medical offices, child care providers and schools. All area
elementary schools are also asked to distribute recruitment flyers to kindergarten, first
and second grades. All of these agencies will be asked to refer eligible families to our
program.
Committee members will canvas the county to distribute flyers to local businesses,
grocery stores, Laundromats, bread stores, resale outlets, thrift centers, trailer parks,
swimming pools, park and recreation facilities, school carnivals, area fairs, Special
Olympics and businesses with sizeable employee numbers.
Door to door campaigns in low economic areas will be done by parents and staff.
Interpreters will contact and provide flyers and applications to businesses that provide
ethnic foods and services, churches providing non-English speaking services and
other agencies providing assistance to non-English speaking families
Policy complies with Performance Standard 1305.5

Quality Preschool and Family Support Program for Prenatal to Age Five
Lower Columbia College
Head Start, Early Head Start, ECEAP
360.442.2800
360.442.2800
Head Start, Early Head Start (EHS) and Early Childhood Educa-tion Assistance Program (ECEAP) assist low income families in raising healthy children, in preparing children for future academic success, and in identifying pathways for family mobility.
WHO QUALIFIES FOR THE PROGRAM?
We serve families in Cowlitz County whose income is at or below the Federal/State Poverty Guidelines. Children with special needs, foster children, homeless families or families who are at risk, are encouraged to apply. Applications are accepted throughout the year.
HEAD START/ECEAPFree Preschool Services for 3-5 year olds
• Children must be age 3 by September 1st• Classes run from September – June• Class options include: 3.5 hours a day, 3-4 days a week or 6
hour days, 5 days a week
EARLY HEAD START• Free year round home visiting services - prenatal to age three• Services and support for Teen Parents• Monthly Play Groups for parents and children
We o�er 8 di�erent locations in Cowlitz County to serve your family. We have classes in Longview, Kelso, and Castle Rock. Limited transportation is available.
MAIN OFFICE1720 20th Ave Longview, WA 98632
Call 360-442-2800 – Fax 360-442-2819 Apply Online at:
https://lowercolumbia.edu/head-start/Facebook
https://www.facebook.com/LCCHeadStart/
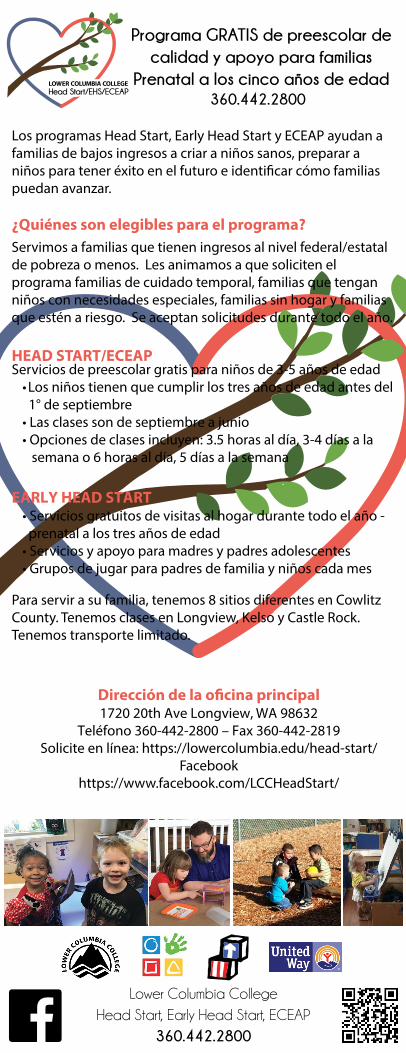
Programa GRATIS de preescolar de calidad y apoyo para familias
Prenatal a los cinco años de edad
Lower Columbia College
Head Start, Early Head Start, ECEAP
360.442.2800
360.442.2800
Los programas Head Start, Early Head Start y ECEAP ayudan a familias de bajos ingresos a criar a niños sanos, preparar a niños para tener éxito en el futuro e identi�car cómo familias puedan avanzar.
¿Quiénes son elegibles para el programa?Servimos a familias que tienen ingresos al nivel federal/estatal de pobreza o menos. Les animamos a que soliciten el programa familias de cuidado temporal, familias que tengan niños con necesidades especiales, familias sin hogar y familias que estén a riesgo. Se aceptan solicitudes durante todo el año.
HEAD START/ECEAPServicios de preescolar gratis para niños de 3-5 años de edad
•Los niños tienen que cumplir los tres años de edad antes del 1° de septiembre• Las clases son de septiembre a junio• Opciones de clases incluyen: 3.5 horas al día, 3-4 días a la
semana o 6 horas al día, 5 días a la semana
EARLY HEAD START• Servicios gratuitos de visitas al hogar durante todo el año -prenatal a los tres años de edad
• Servicios y apoyo para madres y padres adolescentes• Grupos de jugar para padres de familia y niños cada mes
Para servir a su familia, tenemos 8 sitios diferentes en Cowlitz County. Tenemos clases en Longview, Kelso y Castle Rock. Tenemos transporte limitado.
Dirección de la o�cina principal 1720 20th Ave Longview, WA 98632
Teléfono 360-442-2800 – Fax 360-442-2819Solicite en línea: https://lowercolumbia.edu/head-start/
Facebookhttps://www.facebook.com/LCCHeadStart/
HeadStart.Spanish.pdf 1 2/16/2018 1:21:18 PM


Free preschool for children 3-5 years old and services for pregnant women and children 0-3 years of age.
Serving children and families in Longview, Kelso, Castle Rock, Toutle and Kalama.
Now Enrolling!
Call 360-442-2800 or apply online at:
https://lowercolumbia.edu/head-start/
Free preschool for children 3-5 years old and services for pregnant women and children 0-3 years of age.
Serving children and families in Longview, Kelso, Castle Rock, Toutle and Kalama.
Now Enrolling!
Call 360-442-2800 or apply online at:
https://lowercolumbia.edu/head-start/
Free preschool for children 3-5 years old and services for pregnant women and children 0-3 years of age.
Serving children and families in Longview, Kelso, Castle Rock, Toutle and Kalama.
Now Enrolling!
Call 360-442-2800 or apply online at:
https://lowercolumbia.edu/head-start/
Free preschool for children 3-5 years old and services for pregnant women and children 0-3 years of age.
Serving children and families in Longview, Kelso, Castle Rock, Toutle and Kalama.
Now Enrolling!
Call 360-442-2800 or apply online at:
https://lowercolumbia.edu/head-start/

Prescolar gratis para niños de 3-5 ded edad y servicios para mujeres embarazadas y niños de 0-3 años de edad.
Ayudamos a niños y familias de Longview, Kelso, Castle Rock, Toutle y Kalama.
¡Estamos aceptando a niños ahora!
Llame al 360-442-2800 o solicite en línea:
https://lowercolumbia.edu/head-start/
Prescolar gratis para niños de 3-5 ded edad y servicios para mujeres embarazadas y niños de 0-3 años de edad.
Ayudamos a niños y familias de Longview, Kelso, Castle Rock, Toutle y Kalama.
¡Estamos aceptando a niños ahora!
Llame al 360-442-2800 o solicite en línea:
https://lowercolumbia.edu/head-start/
Prescolar gratis para niños de 3-5 ded edad y servicios para mujeres embarazadas y niños de 0-3 años de edad.
Ayudamos a niños y familias de Longview, Kelso, Castle Rock, Toutle y Kalama.
¡Estamos aceptando a niños ahora!
Llame al 360-442-2800 o solicite en línea:
https://lowercolumbia.edu/head-start/
Prescolar gratis para niños de 3-5 ded edad y servicios para mujeres embarazadas y niños de 0-3 años de edad.
Ayudamos a niños y familias de Longview, Kelso, Castle Rock, Toutle y Kalama.
¡Estamos aceptando a niños ahora!
Llame al 360-442-2800 o solicite en línea:
https://lowercolumbia.edu/head-start/
ERSEA 5e
(C: 02/18)
Lower Columbia College Head Start/EHS/ECEAP Procedure and Guide for Logo Use in Marketing Materials and Correspondence
Procedure
LCC Head Start/EHS/ECEAP received LCC Cabinet approval January 2018 to implement a logo created by On The Mark Associates for branding and marketing purposes. The logo was brought to Policy Council for review and approval on January 22, 2018. The LCC Head Start/EHS/ECEAP logo (a brown branch and green leaves inside a red and blue heart) represents the diverse families, relationships and growth that occur among families, staff, and the positive impact our program has in our community. The Lower Columbia College name, font, and color meet the guidelines set forth in the Lower Columbia College Brand and Style Guide (see https://lcc.ctc.edu/info/webresources/Institutional-Research/LCC_Brand_Style_Guide.pdf). The logo created by On The Mark Associates is not to be altered in any way and should be used in all marketing materials. You can access the logo and its variations by visiting our Head Start webpage, under Reports and Handbooks, it is found in ERSEA 5e.
Minimum Size for Reproduction
If the logo is too small, the intended audience may not clearly recognize it as part of our brand. To maximize readability and clarity of our logo, the minimum size for reproduction is 1” in width (for reference, that’s the size used on LCC business cards). Clear Space
To ensure proper readability, provide visual impact and protect brand identity, the LCC Head Start/EHS/ECEAP logo should always have space around it (generally referred to as “clear space.”) This space should be free of other graphic elements such as photos, artwork, etc. Logos Do’s and Don’ts
Do display the logo and other branding elements correctly. Do request assistance from Administrative Services Manager or Public Relations Specialist if you have questions or have a special project or need. Do not alter the logo and other branding elements in any way. This includes the shape, proportion of elements, and/or typeface. Do not alter the color of the logo, or add special effects. The logo and other branding elements should not appear in any color other than those provided.
ERSEA 5e
(C: 02/18)
Email and Email Signatures
Email signatures (used at the bottom of email correspondence) constitute an important aspect of brand identity. As with other aspects of communication, consistent application of branding guidelines helps to bolster our reputation and subsequently support enrollment. Do not use backgrounds in email under any circumstances. Email signatures should contain your name, title, and contact information. Graphic elements are optional. If you choose to use graphic elements, you should use only the graphic elements included in this guide as part of your email signature. To set up an email signature in Outlook, select “new email.” In the new email window, select “signatures.” From the “signatures and stationery” window, you can create, rename, edit or delete email signatures. From the same window, you can also select which signature you would like to use (if you have more than one) on any given email you send. Early Childhood Education Assistance Program (ECEAP) Logo
LCC Head Start/EHS/ECEAP will use the Department of Early Learning (DEL) ECEAP logo on all marketing materials, recruitment flyers and annual reports. The full-color or black-and-white DEL or DEL ECEAP logo must appear in its entirety without modification (see 2017-2018 ECEAP Client Service Contract p. 7).
Office of Head Start – National Head Start Logo
LCC Head Start/EHS/ECEAP will use the Office of Head Start – National Head Start logo in its entirety, without modification, in all marketing materials.
United Way Logo
LCC Head Start/EHS/ECEAP will use the United Way Logo on agency communications, such as newsletters, reports, signs, etc. Additionally, the Leadership team will use the United Way Logo in the signature line of their email.
References
LCC Brand and Style Guide https://lcc.ctc.edu/info/webresources/Institutional-Research/LCC_Brand_Style_Guide.pdf
ERSEA 5f
(C: 02/18)
Lower Columbia College Head Start/EHS/ECEAP Logos for use in Marketing Materials and Correspondence
The LCC Head Start/EHS/ECEAP logo was created by On the Mark Associates and approved by LCC Cabinet and Policy Council January 2018. The logos are not to be altered in any way and should be used in all marketing materials and correspondence*.
Head Start Small Logo
Black and White Logo
Head Start jpg.
Head Start Shadow Logo
*See ERSEA 5d “Procedure and Guide for Logo use in Marketing Materials and Correspondence” for further instruction.
ERSEA 6a
(R: 07/10; C: 07/03)
Lower Columbia College Head Start / EHS / ECEAP
Community Assessment
Policy Every three years Lower Columbia College Head Start/EHS/ECEAP will conduct a community
assessment to collect data about community strengths, needs and resources. This data will be
used to make decisions about the type of services provided for children and families and to
determine collaboration possibilities with other agencies.
Approved by Policy Council on July 10, 2003
Procedure
1. Every three years Head Start/EHS/ECEAP will conduct a Community Assessment within
its service area of Cowlitz County.
2. The Community Assessment at a minimum will include the collection and analysis of the
following information on eligible children and families:
a) The demographic make-up including the number of eligible children/families,
geographic location and racial ethnic composition.
b) Information on other child development and child care programs within in the
service area that are serving HS/EHS/ECEAP eligible children.
c) The estimated number of children with disabilities four (4) years old or younger,
including the type of disability and relevant services and resources provided these
children by community agencies.
d) All current data regarding education, health, nutrition and social service needs of
eligible children and their families.
e) The education, health, nutrition and social service needs as defined by families of
Head Start/EHS/ECEAP children and by institutions that serve young children.
f) The resources within the community that could be used to address the needs,
which includes the assessment of their availability and accessibility.
3. An analysis of the assessment information will be used to:
a) Determine the program philosophy, and its long and short-term goals and objectives.
b) Determine the type of component services that are most needed and the program
option(s) that will be implemented.
c) Determine the recruitment area to be served.
d) Determine appropriate locations for centers.
e) Set criteria that define the types of children and families who will be given
priority for recruitment / selection.
4. The annual grant planning and budget process will include a review and update of the
assessment information. An analysis of the updated information will determine if the
direction of services to eligible children and families need to be changed.
Policy complies with Head Start Performance Standards 1305.3(c)(d)(e)