-
8/6/2019 1974 Tumors of the Nasopharynx in Tunisia an Anatomic
and Clinical Study Based on 143 Cases
1/9
T U M O R S OF THE N A S O P H A RY N X I N T U N I S I AAn A n
a t o m i c a n d Clinical S tudy Based o n 143 Cases
M . C A M M O U N , . VOCTHOERNER,ND N . MOURALI
This study is based on 143 instances of malignant nasopharyngeal
tumors ob-served at the National Cancer Institute in Tunisia. This
is the most commontumor in Tunisia. The ages of the patients varied
between 10 and 78 years, thepeak ages being between 50 and 59
years, and between the ages of 10 and 19years (14.6% under age of
16 years). So-called lyniphoepitheliomas were theprevalent tumor
type in the younger age group.
HE RELATIVE FREQUENCY OF CANCER OF THE
T asopharynx in Tunisia has been men-tioned by Chadli4 and
Zaouche.18 Th e epi-demiologic study of cancer of the cavum bythe
International Cancer Union1 does notmention this frequency. In
Europe, the inci-dence is low, about 0.2'y0of all malignant
tu-mors. However, it is high in other parts ofthe world, especially
south of China: HongKong, Formosa, Malay, and Singapore. InHong
Kong, 124 cases per million inhabitantshave been recorded, 25 times
the number esti-mated by Godtfresden in Denmark and Swe-den.7Our
material consisted of 143 nasopharyn-geal tumors observed and
treated at the Na-tional Cancer Institute from March 10, 1969to
March 22 , 1971. All the patients were Mos-lems, and all were
Tunisians, except for threewho were Libyans. Among the Tunisian
hos-pitals, the National Cancer Institute is theonly one to have a
telecobalt installation, sonearly every patient treated by
irradiation hasbeen seen at this Institute.
We had histologic confirmation on every pa-tient except for two,
for whom we had only ahistologic report. In three others, in spite
otobvious symptoms of nasopharyngeal cancer,the biopsy was
negative, but the histologic ex-amination of the cervical
adenopathy showedtypical metastases from the cavum. In 24
pa-tients, we obtained biopsies of both the cavumand lymph nodes,
which made it possible tomake a comparative histologic study.
Ordi-nary stains were used for all the biopsies(Hemalum
eosine-safran). Reticulin stain wasemployed in the
less-differentiated cancers;
From the National Cancer Institute, Tunis, Tunisia.Received for
publication May 1 7 , 1973.
mucicarmin was also used, as was PAS in sus-picious cases of
glandular cancers.
Every patient (except two who refused) re-ceived radiotherapy.
For 24 , there were nofurther therapeutic resources; 4 were
givenpalliation.
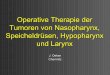
There were 102 males and 41 females. Theage of the patients
varied between 10 and 78years; the average age for men was 44.6,
andfor women 42.7. The peak incidence wasreached between 50 and 59
years for bothsexes, but there was also a high frequency inpatients
between 10 and 19 years; 21 casesunder 16 years represented 14.6sy0
of the en-tire group. The age curve was the same forboth sexes.
(Fig. 1).
Th e general nasopharyngeal cancer inci-dence in Tunisia is
difficult to establish. Thisis an undeveloped country, where the
healthfacilities, especially in the country, are insuffi-cient.
There are probably many people withcancer who die without ever
having seen aphysician. For 1970, we estimate that theremight be an
incidence of 2.05 cancers per100,000 inhabitants (personal
communicationfrom D. Muir.)Cancer of the nasopharynx is the most
fre-quent malignant tumor of the otdaryngologicarea. In 1970, the
National Cancer Institutereported 78 cancers of the cavum, 61 of
thelarynx, and 20 of the tongue and mouth. Dur-ing this same year,
1050 cases of cancer weretreated: 7.390/, were of the
nasopharynx;10.1% in men and 7.3a/, in women. They rep-resented
38.80/, of all cancers in men and53.4% in women (42.3% for both
sexes).
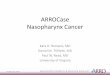
The geographical distribution on the map(Fig. 2) illustrates the
proportional incidenceof cancer of the nasopharynx related to
thedensity of the population. T he northern Gov-
18 4
-
8/6/2019 1974 Tumors of the Nasopharynx in Tunisia an Anatomic
and Clinical Study Based on 143 Cases
2/9
No. 1 NASOPHARYNGEALUMORSC a m m o i i n et al. 185
40
30
2(
1c
0
a EMALES0 ALES
1-19 20-29 0-3: -10-5960.69 7069 AG EFIG. 1 . Distribution of
cases by age and sex
ernorats Provinces are more densely inhabitedthan those in the
center and south. However,it is interesting to note that this
incidenceseems relatively lower in the region of Sfax,the second
most important town in Tunisiaand the most populated Governorat
afterTunis and Sousse. This is not due to an insuf-ficient sanitary
installation, because Sfax hasan excellent health service and has
regularconsultations and histologic examinations forall
biopsies.
CLINICALSPECTSThere are many advanced cases of cancer of
the nasopharynx for which all therapeutic in-tervention is
useless (about 16%). The hid-den time, i.e., the time between the
manifes-tation of the tumor and the day the patientcomes for the
first consultation is not easy toestablish: in 30 cases this could
not be deter-mined, but it was about 8 months in other pa-tients.
The times ranged between 8 days and 4years.The most frequent
clinical signs are cervical
adenopathy, epistaxis, nasal obstruction, audi-tory problems,
and neurologic disorders suchas paralysis of the cranial nerves,
headaches,and trismus. Rarely, a single sign, such as par-alysis of
the 6th nerve, may be the first indica-tion of a nasopharyngeal
cancer, but oftenwhen the patient is seen there are
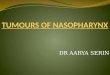
numerousclinical findings. Table 1 shows the number ofpatients with
adenitis (Fig. 3) . In at least 24cases, the histologic examination
of the biopsyof a cervical lymph node led to the search forand
discovery of a nasopharyngeal tumor. Th eordinary clinical signs of
a neoplasm of thecavum were insignificant or absent. In 22
pa-tients, there were enlarged cervical nodeswithout any alteration
of the cavum. Theselymph node metastases were often first treatedas
tuberculous adenites. The neurologic signsmay be dominant, and thus
the patient maybe treated for a relatively long time period
inneurology before he visits an otolaryngologist.T h e lesion of
the base of the skull was noticedin onIy 18 cases, some at clinical
examinationand others during its evolution by
radiologicexamination. This bony involvement was ac-
FIG. 2 . Map of geographical distribution illustratingthe
proportional incidence of cancer of the naso-pharynx related to the
density of the population.
-
8/6/2019 1974 Tumors of the Nasopharynx in Tunisia an Anatomic
and Clinical Study Based on 143 Cases
3/9
186 CANCERanTABLE . The Most Frequent Clinical Signs
ofNasopharyngeai Tumors in TunisiaCervical adenopathy 86Auditory
signs 67Nasal obstruction 61Epistaxis 64Neurologic signs; injury of
thecranial nerves 28
companied by neurologic signs in only five pa-tients. The
precise location of the tumor wasnot always identified (104 cases);
in 24, thetumor occupied the whole cavum. Table 2shows the possible
locations of the neoplasms,the roof and lateral walls being the
most fre-quent areas (56.~37~nd 59%).
PATHOOG YFungiform tumors made up about 811%of
the entire series. Only 11 cases showed infiltra-tion or
ulceration. In five patients, the clinicalexamination of the cavum
was not remarka-ble. Th e tumor was not described macroscopi-cally
in 5 0 cases (35%), because a tight trismusexcluded
examination.Histopathology: Epitheliomas were dividedas follows: 1.
Differentiated epidermoid carci-noma; 2. Undifferentiated
epidermoid carci-noma; 3. Nasopharyngeal type carcinoma(which we
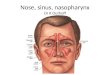
consider typical for this location; 4.Anaplastic carcinoma.1. The
differentiated epidermoid carcinomais a cancer in which the
squamous structure i sobvious (22 or 17.7%) (Fig. 4).2. The
undifferentiated epidermoid carci-noma largely resembles the
malpighian mu-cosa which is without any keratinization, andthe
cells of which (instead of being always po-lyhedral) can be
spindle-shaped (Fig. 5),
iinry 1974 Vol. 33rounded, or ovoid. The cells demonstrated
adefinite cellular border. They showed trabecu-lar and lobular
patterns, sometimes with base-ment membrane. This kind of tumor can
beseen at any level of the malpighian layer orparamalpighian layer,
especially in the cervix,esophagus, and the oral cavity. They
represent42.5% of all epitheliomas (5 3 cases).
3. The nasopharyngeal type carcinoma(NPTC) is a peculiar
neoplasm of the cavumin that its fundamental histologic feature
iscellular. T he tumor cells borders are not defi-nite, their
nuclei are clear, and chromatin isscarce. Th e nuclei look holed.
They exhibitoften two or three distinct nucleoli. They maybe
spindle-cell, rounded, or polyhedric. T h esyncytial aspect and the
poor chromatin of thenuclei are the fundamental features. Thestroma
varies sometimes; it is lymphoid, fib-rous, or granular, and
inflammatory (Figs. 6-8). We had 49 cases, (39% of all the
epithe-liomas).
4. Th ere were only two cases each of adeno-carcinoma and
anaplastic epithelioma. Amongthe hematosarcomas there were four
reticulo-sarcomas, two lymphosarcomas (Fig. 9), andone
plasmocytoma. Eight epitheliomas werenot classified, either because
the biopsy wastoo small, or because we did not receive
thehistologic slides.Th e distribution of the histologic types
ac-cording to age i s interesting. There was onlyone patient under
40 with differentiated epi-dermoid carcinoma. This held true also
forthe undifferentiated carcinomas: nine casesunder 53 years of
age. On the other hand, thenasopharyngeal type carcinoma is more
fre-quent in younger people, 28 of 42 patientswere under 40, and
all the patients under 20years of age had this type of tumor.
FIG.3. Clinical pho-tograph of a youngboy with involvementof the
high cervicallymph nodes, a typicallocation for metastaticcarcinoma
from thenasopharynx.
-
8/6/2019 1974 Tumors of the Nasopharynx in Tunisia an Anatomic
and Clinical Study Based on 143 Cases
4/9
No. 1 NASOPHARYNGEALUMORSCammoun et al . 187TABLE. Observed
Sites of t h e T u m o r
Late ral walls 62 59%To p roof 59 56%Poster ior wall 34 3 2 . 5
0 / ,Floor 24 23 %T h e w hole c a vum 24 23%I t is seldom th a t
the tu mo r a ffects a precise place i nexcluding others . I t is
most ly riding over severa l a t t hesame t ime .
DISCUSSIONThe incidence of nasopharyngeal cancer in
Tunisia seems high, it appears to be a.bout2.05 per 100,000
inhabitants in 1 year. Thisfrequency is probably higher inasmuch
asmany cases are not recognized or diagnosed.
Tunisia is not the only country in NorthAfrica with a high
incidence. In Algeria, Man-souri et al. observed 105 cancers of the
cavumout of 613 between 1962 and 1967. Sitbon, a tthe M. and P.
Curie Center of Algiers, re-ported 145 between 1950 and 1960.
Personal
information in Morocco led us to believe thatthere is a high
incidence there also.
In Europe, the average incidence per100,000 inhabitants is low:
0.7 for men and0.4 for women (these statistics were quoted
byGodtfredsen for the northern countries as re-ported by Muir).
Although the frequency issignificantly higher in Tunisia than in
Eu-rope, it does not reach that of the Far Eastwhere the average
yearly incidence of naso-pharyngeal cancers in Hong Kong is 12.4
per100,000 inhabitants,' with the same percent-age for Formosa and
Singapore.
Our peak age curve in comparison with thatof Hong Kong shows a
slight divergence: forTunisia it is between 50 and 59 years,
forHong Kong between 40 and 44 years. TheChinese evidently do not
have another peakbetween 10 and 20 years as we do in Tunisia.In
this latter younger age group were 14.6%of our cases, whereas in
the quoted series fromthe Far East there were in Formosa 13
casesout of 1000 (l%).I7 Muir in Singapore re-
FIG. 4. Photomicrograph of keratinizing squamous cancer in a
male 54 years of age (747)(X150, W.U. NG. 73-456).
-
8/6/2019 1974 Tumors of the Nasopharynx in Tunisia an Anatomic
and Clinical Study Based on 143 Cases
5/9
188 CANCERanuary 1974 VOl. 43
ported 8 out of 974 cases (0.870);10 nd Ho inHong Kong reported
no more than 15 out of1438 (170).7t seems that the Caucasian
childis more susceptible than the Oriental child.The statistics
compiled by Martin and Bladyin the United States corroborate this
impres-sion. They found in a series of 87 cases that9% were under
15 years of age, and 18%under 30 years of age. They believe that
thiskind of cancer affects the child much moreoften that any other
kind of cancer of the res-piratory and digestive tracts. The number
of
FIG. 5. Photomicro-graph of a nasopha-r y ng e a l c a nc e r i
nwhich the individualcells have a spindle-like pattern (~100).
affected men is three times that of women,which corresponds to
the findings of otherauthors.709
From the clinical point of view, there doesnot seem to be a
notable difference in thosecountries with a high incidence.
Scarcelyknown clinically in Tunisia., the nasopharyn-geal cancer is
often discovered too late. Theclinical aspect is the same as that
seen in theFar East,7 in Europe,ll and in the Unitedstate^.^
Cervical adenopathy is easily noticedon the first examination, and
should lead to a
FIG. 6. This tumorhas a somewhat syn-c y t i a l a s pe c t w i
t hscattered lymphocytes(x250).
-
8/6/2019 1974 Tumors of the Nasopharynx in Tunisia an Anatomic
and Clinical Study Based on 143 Cases
6/9
No. 1 NASOPHARYNGEALUMORS C a m m o u n e t al. 189
FIG. 7. Photomicrograph of so-called lymphoepithelioma in a
female 45 years of age. Noteprominent nucleoli and lymphocytic
infiltrate (2766) (X350, W.U. Neg. 73-458).
systematic examination of the cavum. T he lo-cation of the tumor
appears most often in thelateral and posterior walls.
From the pathologic point of view, the na-sopharyngeal cancer
appears frequently as afungating tumor, but also as a diffuse
submu-cous infiltration, somewhat deforming thewalls. At times the
macroscopic examinationis negative, leading to several successive
biop-sies done blindly.T he histopathology of this type of tumor
isdebatable. Several classifications have beenproposed. Shu Yeh,
after about 1,000biopsies,created a very detailed classification
which in-cluded 9 histologic types. After having studiedthis
classification as it related to prognosis, hefound tha t survival
did not depend on the his-tologic types, and finally retained only
two;the classic epidermoid epithelioma, and theundifferentiated
epidermoid epithelioma.
We believe that the lymphoepithelioma ofRegaud and Schmincke is
debatable and doesnot seem to be an established entity.e~15~17Teoh
argues against the existence of such a
histologic entity based on his study of 32 ne-cropsies. The
lymphoid tissue, intimatelymixed with the epithelioma spans, does
notappear in the visceral metastases. YehI7 foundthat the tumor
cells of the lymphoepitheliomawere similar to the cells of the
transitional cellepithelioma described by Cappell.3 He notedseveral
biopsies in which the lymphoepithe-lioma and transitional cell
epithelioma weresituated side by side. He demonstrated withbiopsies
taken from people in good health andof al l ages, that the lymphoid
tissue was al-ways present, and as such, it was an integralpart of
the nasopharyngeal mucosa. So it is tobe expected that the
epithelioma cells aremore or less lost in this tissue.
A comparison between the nasopharyngealand lymph node biopsies
on the same patientshows that the important lymphoid elementin the
cavum can be absent and substituted bya fibrous tissue on the
adenopathic level. Thecontrary is also true: a fibrous stroma on
thenasopharyngeal level can be lymphoid type inthe invaded lymph
node. Furthermore, in the
-
8/6/2019 1974 Tumors of the Nasopharynx in Tunisia an Anatomic
and Clinical Study Based on 143 Cases
7/9
190 CANCERanuary 1974 VOl. 33
FIG. 8. Photomicro-g r a p h of a tu morwith the characteristicn
u c l ear ap p earan ce(X400).
same biopsy, the histologic aspect can varyfrom one zone to
another, seen especially inthe larger fragments.various histologic
types, such as the differen-
tiated epidermoid epithelioma, the undifferen-tiated
epithelioma, and the transitional cellepithelioma, may all be found
in the same ad-
Besides the lymphoepithelioma debate, the enopathy or in the
same nasopharyngealbiopsy. We have a typical example of these
FIG. 9. Photomicrograph of a lymphosarcoma of the nasopharynx of
a male 68 years of age(619) ( ~ 6 0 0 , .U . Neg. 73-457).
-
8/6/2019 1974 Tumors of the Nasopharynx in Tunisia an Anatomic
and Clinical Study Based on 143 Cases
8/9
No. 1 NASOPHARYNGEALUMORSCammoun et al. 191three histologic
forms in the same lymph nodemetastasis. We do not think that these
mor-phological types are unchanging entities.Surely there must be
transitions from one formto another. Nevertheless, for every
pathologistworking in areas where this kind of cancer isfrequent,
the diagnosis of a single lymph nodebiopsy should point most surely
to a primarynasopharyngeal origin. We have noticed sev-eral times
that study of these metastases ledthe pathologist toward the cavum.
Indeed,there exists a certain morphological individu-ality of this
type of cancer. The transitionalcell epithelioma as described by
Cappell seemsspecific for cancer of the nasopharynx. Its
fun-damental histologic aspect is not constructivebut cellular. Th
e tumor cells have a clear nu-clei with sparse chromatin (holed),
butshowing always one or two nucleoli. Th ei r cy-toplasm is clear
and granular, and their bor-ders vague and indeterminate. They form
al-veolar structures resembling protoplasmicsyncytium. T h e stroma
can be fibrous, lym-phoid, granular, or inflammatory. Th is form
ofcancer should be called nasopharyngeal-typeepithelioma because it
is not found in anyother part of the body.
Clinically, it is seen often in young adults,especially in
children. Of 24 patients under 20years of age, 16 showed this
histologic type,while 5 were undifferentiated epitheliomas, (3of
the biopsies were too small to be classified).These nasopharyngeal
type epitheliomas r e presented 76% of the cancers among
adoles-cents and children.
The anaplastic form (only two cases in ourseries), is often
difficult to distinguish from re-ticulum cell sarcoma. Th e
evolution of thedisease in our two cases showed that they weretrue
epitheliomas.
Other malignant tumors of the cavum arerare. We had only two
adenocarcinomas, sixhematosarcomas, and one plasmocytoma.
Various authors have noted the influence ofrace with regard to
this tumor: American au-thors have reported a high incidence
amongAmerican-born Chinese.16 T h e MongolianRace seems to be
especially predisposed, so i t
is difficult to explain why cancer is so scarce inJapan,lu and
why in Tunisia, which is inhab-ited by Caucasian people, it is so
frequent.Bailar thinks that the environmental factorcombined with
the racial factor might explainthis frequency.1
The discovery of the high incidence of naso-pharyngeal cancer in
Tunisia raises an etio-logic problem, and the hypotheses advancedto
date have not explained our findings. Simi-larly, neither the
racial nor the environmentalfactor explain i t satisfactorily.
Recently, G. deTh e demonstrated a type of herpes virus seenin
certain cells of culture tissue of nasopharyn-geal carcinoma in
China. This suggests thepossibility of a viral basis which better
ex-plains the frequency of this cancer amongsuch diverse
populations.
SUMMARYThis study is based on 143 anatomo-clinical
observations of malignant nasopharyngeal tu-mors observed over a
2-year period at the Na-tional Cancer Institute of Tunisia.
The average age of the patients was 44.6years. Two peaks were
noticed on the agecurve; between 50 and 59 years, and between10 and
19 years (14.60/, were under 16). Therewas a clear predominance of
males (102 men,41 women). Th e general incidence of the
naso-pharyngeal cancer in Tunisia can be esti-mated to be 2.05
cases per 100,000 population.
A study of the geographic distributionshowed a relation between
incidence and pop-ulation density.
From the clinical point of view, cervical ad-enopathy was a
significant symptom. Histolog-ically, there was a specific
morphological typeof nasopharyngeal epithelioma often seen inyoung
patients. There did not seem to be anotable difference between the
epithelioma ofthe cavum in Tunisia and that of SoutheastAsia, but
there was a higher frequency amongchildren in Tunisia. T he racial
factor did notseem to be important. A type of herpes virusmight be
the origin of this kind of cancer.
REFERENCES1. Bailar, J.: Nasopharyngeal cancer in white popu- 2.
Cappell, D. F. : On lympho-epithbl ioma of naso-lations-A world-w
ide survey. I n Cancer of the Naso - pharynx and tonsils. J. P at h
o l . Bacterial. 3949-64 ,pharynx: A symposium Organized by the
InternationalUnion Against C ancer, mono graph series, vol. 1 , C.
S . 3. --: Pathology of the nasopharyngeal tumors.Muir and K.
Shamugaratnan, Eds., Copenhagen, J. Lnryngol. O t o l . 53:55-580,
1938.Munksgaard, 1967. 4.Chadli, A., and Ph ilippe, E.: La
physionomie du
1934.
-
8/6/2019 1974 Tumors of the Nasopharynx in Tunisia an Anatomic
and Clinical Study Based on 143 Cases
9/9
192 CANCERanuary 1974 VOl. 33cancer en Tunisie. Archives de
I'lnstitut Pasteur deTunis 37:397,441, 1960.
5. Godfredsen, E.: Cited by Ho.: Ophtalmology andneurology
symptoms of malignant naso-pharyngeal tu-mors, a clinical study
comprising 454 cases. with specialreference to histopathology and
possibility of earlierrecognition. Acta. Psychiatr . Scand. [Suppl
.] 34: 1-323,1944.6. Hawser, I. J., and Brownell, D. H.:
Malignantneoplasms of nasopharynx. J A M A 11~2467 , 473, 1938.7.
Ho, H. C.: Nasopharyngeal carcinoma in H ongKong. In Cancer of the
Naso-pharynx; A SymposiumOrganized by the International Union
Against Cancer,Monograph series, vol. 1, C. S. Muir and K.
Shamugar-atnan, Eds. Copenhagen, Munksgaard, 1967; pp. 58-63.8.
Mansouri et al.: Difficulties et erreurs de diagnos-tic dans les
tumeurs malignes du cavum. T u n i s . M e d .9. Martin, H. E., and
Baldy, J. V.: Cancer of the na-sopharynx. Arch. Oto la tyngol .
32:692-727, 1940.10. Muir, C. S., and Shamugartnan, K.: The
inci-dence of nasopharyngeal cancer in Singapore. In Can-cer of the
Nasopharynx; A Symposium Organized bythe International Union
Against Cancer, monograph
1:81-83, 1968.
series vol. 1, C. S . Muir and K. Shamugaratnan, Eds.Copenhagen,
Munksgaard, 1967; pp. 47-53.11. Nelsen, J.: Roentgen treatment of
malignant tu-mors of nasopharynx. Acta Radiol . 26: 133-154,
1945.12. Regaud.: Personal communication cited by Rev-erchon and
Coutard.13. Reverchon and Coutard: LymphoQpith&liomade
l'hypopharynx trait6 par roentgentherapie sans
rkaction notable du pharynx et du larynx. Bull. M L m .SOC.
Franq. Oto-Rh ino-Laryngol . 34:209-214, 1921.14. Sitbon, J.: La
cancer du cavum en Algbrie. Bull.Alg . Carcinol. 2:385, 1959.15.
Teoh, T. B.: Epidmmoid carcinoma of nasophar-ynx among Chinese
study of 31 necropsies. J. Puthol .Bacteriol . 73:451-465, 1957.16.
Vaeth, J. M.: Nasopharyngeal malignant tu-mo rs -8 2 consecutive
patients treated in a period of 22years. Radio logy 742366372,
1960.17. Yeh, Shu: A histological classification of carcino-mas of
the nasopharynx with a critical review as to ex-istence of
lymphoepitheliomas. Cancer 15:895-920,1962.18. Zaouche, A.: Les
tumeurs malignes de la sphhreO.R.L. en Tunisie. Th&e de
Mkdecine facultt deMkdecine de Paris. 37:397-441, 1960.