-
8/16/2019 2 PARA 1 - Protozoa - Flagellates
1/13oup # 36 | Villanueva, M., Violanta, Yadao, Yau, Yee Page 1
o
Parasitology 2.1
PROTOZOA - FLAGELLATESDr. FontanillaJanuary 6, 2014
UTLINEProtozoa
Nucleus and Cytoplasm Locomotor Organelles
Pseudopodia Cilia Flagella
Encystment
Feeding and Metabolism ClassificationFlagellates
Genus Trypanosoma Trypanosoma brucei Trypanosoma cruzi
Genus Leishmania Visceral Cutaneous Mucocutaneous
PROTOZOAWas once a phylum nameActually refers to a number of
phyla
Explains diversity and complexity of membersCurrently used
colloquially as a common noun
NUCLEUS AND CYTOPLASMProtozoa consist of a single cell
Many species contain more than one nucleus during all or
portionsof their life cycles.
Nucleus and cytoplasm Like all cells, the bodies of protozoa are
covered by plasma
membrane which may contain glycocalyx that may haveimmunologic
importance
Pellicular microtubules or fibrils may course beneath the
plasmamembrane. Examples:
o Kinetoplastid flagellates - microtubules underlie aflexible
membrane
o Trypanosome and trichomonas - adjoining membraneshave a
fibrous connection between them such asbetween the body and
undulating membrane
Mitochondria Examples:
o Amoeba - branched tubular cristaeo Flagellates - a single,
large bodyo Ciliates - arranged as elongated sausage-shaped
structures Golgi apparatus (dictyosome)
Examples:o Flagellates - large and/or multiple parabasal bodies
in
association with kinetosomes, the “basal bodies” or“parabasal
bodies”
Microbodies Peroxisomes contain oxidases and catalases.
Examples:
o Trichomonas spp - hydrogenosomeso Kinetoplastida – glycosomes
which contain glycolytic
enzymes used in carbohydrate and fat synthesizingpathway called
glyoxylate cycle
Cytoplasmic matrix Low density colloid Can exist as fluid (sol
state) or relatively solid (gel state) Central zone of
cytoplasm
o ENDOplasmo SOL stateo Contains nucleus, mitochondrion, Golgi
bodies
Peripheral zone of cytoplasmo ECTOplasmo GEL stateo More
transparent than solo Maintains cell shapeo Base of flagella or
cilia are embedded in the ectoplasm Protozoa, like fungi, are
described as eukaryotes.
Eukaryotes - the genetic material, DNA, is carried on weldefined
chromosomes contained within a membrane-boundnucleus
Nuclei - oval, discoid, or round that appear vesicular
witirregular distribution of chromatino Examples:
CiliatesMicronucleus – reproductive; undergo meprior to sexual
reproduction (conjugation)*some protozoan members reproduce
basexual reproduction such as binary fission budding
Macronucleus – dense, elongated, chainlike; considered as
somatic; function cell metabolism and growth; does not
undmeiosis
Nucleoplasm – finely granular with aggregation of
denchromatin
Endosomes – nucleoli; do not disappear during mitosis Nuclear
envelope – consists of two membranes
LOCOMOTOR ORGANELLES Protozoa move by 3 basic types:
Pseudopods (amoeba) Flagella (flagellates)* Cilia
(ciliates)*
*called undulopodia Some amoebas possess both flagella and
pseudopods – transform
from flagellated to amoeboid cell occurs in response to
environmentalconditions and is a recognized life cycle event.
Figure 1. Euglenoid Flagellum; Paramecium Cilia, Amoeba
Pseudopodia
PSEUDOPODIA Temporary extensions of the cell membrane and are
found in amoebas
as well as in a variety of cell types Movement by means of
pseudopodia is a complex form of
protoplasmic streaming involving protrusion of the cell,
adhesion tosubstrate, and subsequent contraction.
Pseudopodia may also be used for amoeboid feeding
-
8/16/2019 2 PARA 1 - Protozoa - Flagellates
2/13oup # 36 | Villanueva, M., Violanta, Yadao, Yau, Yee Edited:
AFV Page 2 of
PARASITOLOGY 2.1
Figure 2. Mechanism of pseudopod feeding
An amoeba feeds on small organisms such as bacteria.↓
As an amoeba approaches food, pseudopodia form and
eventuallysurround the food.
↓ The food becomes enclosed in a food vacuole.
↓ Digestive enzymes break down the food, and the nutrients
diffuse into
the cytoplasm.
CILIA
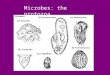
Figure 3. Schematic representation of a ciliate
Structurally similar to flagellaWith a kinetosome and an axoneme
composed of two central and nineperipheral microtubulesAppear to
beat regularly, with a back-and-forth stroke in a two-dimensional
plane
FLAGELLA
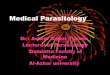
Figure 4. Cilia and Flagella Structure
Undulipodia Slender, whip-like structures Composed of a central
axoneme and an outer sheath that is a
continuation of the cell membrane The axoneme consists of nine
peripheral and one central pair of
microtubules. The axoneme arises from a kinetosome (basal body)
which is similar to
centrioles of other eukaryotic cells. The flagellum may also be
bent back along and loosely attached to the
lateral cell surface, forming a fin-like undulating membrane
(anadaptation in a viscous environment).
A dark staining body, the kinetoplast found near the kinetosome;
discmade of DNA circles (kDNA)
May be directed anteriorly, posteriorly or laterally regardless
ofdirection of movement
Heterkonts are flagellates with two or more flagella with
differeinstructures
Figure 5. Flagellum, kinetosome, and associated organelles are
called the“ mastigont ” or “ mastigont system ”.
ENCYSTMENT Many protozoa can secrete a resistant covering and
enter a resting
stage – cyst.
Conditions favoring encystment involve some adverse
environmentalevents such as food deficiency, desiccation, increased
tonicity,decreased oxygen concentration or pH, or temperature
change.
During encystment, a cyst wall is secreted and starch or
glycogen isincorporated in the cyst as energy source
During excystation, there is return to a favorable environment
usuallyassociated with absorption of water from environment, cell
swelling,activation of lytic enzymes and of normal physiologic
pathways
In coccidians , the cystic form is an oocyst which is formed
after gamunion and in which multiple fission occurs (sporogony)
with cytokinesisto produce sporozoites.
Figure 6. Different flagellate morphologies
-
8/16/2019 2 PARA 1 - Protozoa - Flagellates
3/13oup # 36 | Villanueva, M., Violanta, Yadao, Yau, Yee Edited:
AFV Page 3 of
PARASITOLOGY 2.1
Figure 7. Different amoebae morphologies
FEEDING AND METABOLISMProtozoa lacking chloroplasts are all
heterotrophic . They get energyfrom complex carbohydrates and
nitrogen from amino acids.Mouth parts: Amoeba – temporary
pseudopod
Ciliates – permanent cytostome Excretion of indigestible
material Ciliates – cytopyge
CLASSIFICATIONProtozoa have been divided traditionally on the
basis of their means oflocomotion, although this character is no
longer believed to representgenuine relationships.
Flagellates (e.g. Giardia lamblia ) Amoeboids (e.g. Entamoeba
histolytica ) Sporozoans (e.g. Plasmodium )
Apicomplexa Microsporidia
Ciliates (e.g. Balantidium coli )
FLAGELLATESPresence of several, long, thread-like extensions of
ectoplasm calledflagella during their trophozoite stageFlagella
arises from axoneme which is associated with a
kinetoplastconstituting the neuromotor apparatusFree-living or
parasiticFlagellates of importance to man:
Flagellates of the blood and tissues (to be discussed here)
Hemoflagellates Requires a blood-sucking insect to complete life
cycle Four basic morphologic forms differing in position of
kinetoplast, presence/absence of undulating membrane Flagellates
of the digestive tract and genitals ( Trans 2.2)
ylum EuglenozoaClass Kinetoplasta
Order TrypanosomatidaGenera: Trypanosoma
LeishmaniaLeptomonas (no medical importance)Crithidia (in
insects)
TRYPANOSOMAAll trypanosomes are heteroxenous .
During one stage of their lives, they live in the blood and/or
fixedtissues of all vertebrate classes. During other stages, they
live inthe intestines of bloodsucking invertebrates.
They are called hemoflagellates - laboratory culture media
usuamust contain blood.
In the past (in manual), stages were named after the genera they
mostresembled. (e.g. Leptomonad – for a stage resembling species of
genLeptomonas)
The nomenclature used today refers to kinetoplast and
nuclposition .
STAGES
Various species pass through amastigote , promastigote ,
epimastiand/or trypomastigote stages
Figure 8. Stages of Trypanosoma
Amastigote - basal body anterior of nucleus, with a short,
essentiallynon-functional flagellum
Promastigote - basal body anterior of nucleus, with a long,
detachedflagellum
Epimastigote - basal body anterior of nucleus, with a long
flagellumattached along the cell body
Trypomastigote - basal body posterior of nucleus, with a long
flagellumattached along the cell body
These names are derived from the Greek mastig , meaningreferring
to the trypanosome's whip-like flagellum .
Figure 9. Trypanosoma VS Leishmania morphologies
-
8/16/2019 2 PARA 1 - Protozoa - Flagellates
4/13oup # 36 | Villanueva, M., Violanta, Yadao, Yau, Yee Edited:
AFV Page 4 of
PARASITOLOGY 2.1
The mammalian stages of T. brucei exist primarily in the
bloodstream.In contrast, most of the mammalian developmental stages
of T. cruzi and Leishmania spp. reside within the cytoplasm of a
wide range ofhost cells or the phagolysosome of host macrophages
respectively.Proliferative and non-proliferative (boxed) stages and
the locations ofthe flagellum (blue) and kinetoplast (red) relative
to the nucleus (grey)are indicated. T. cruzi and Leishmania
amastigotes may undergoperiods of proliferative and
non-proliferative growth.
CLASSIFICATIONTrypanosomes are divided into two broad groups
based on thecharacteristics of their development in the insect
hosts.
Section Salivaria - the species develops in the anterior portion
ofthe digestive tract of the insect host
Section Stercoraria - the species develops in the vector’s
hindgut
SECTION SALIVARIA – TRYPANOSOMA BRUCEIThe genus includes about
30 species and subspecies.Most of these are not associated with
transmission of sleeping sickness,although many transmit animal
trypanosomiasis to game and domesticlivestock.Members of the genus
Glossina are divided conveniently into threegroups which are often
given subgeneric status. These divisions are:
The fusca group (subgenus Austenina ) The palpalis group
(subgenus Nemorhina ) The morsitans group (subgenus Glossina
s.s.)
VECTORS - tsetse flies (Dipteran: Glossinidae; Genus: Glossina )
Tsetse flies are now restricted to continental Africa. About half
of
Africa is infested, some 10.4 million square kilometres in all.
Glossina species are large (6-15mm), narrow-bodied flies,
brownish or greyish in color, with a stout proboscis that
projectswell forward in front of the head.
Figure 10. Tsetse Fly
3 subspecies that are morphologically indistinguishable:
Trypanosoma brucei brucei Trypanosoma brucei gambiense Trypanosoma
brucei rhodesiense
TRYPANOSOMA BRUCEI BRUCEIA bloodstream parasite of native
antelopes and other African ruminantProduces a disease called
nagana Humans are not susceptible .
TRYPANOSOMA BRUCEI GAMBIENSEThe etiologic agent of African
sleeping sickness CHRONIC form of sleeping sicknessFound in west
central and central AfricaVectors
G. palpalis and G. tachinoides - riverine flies Breed in shady,
moist areas along rivers
Reservoirs Found mostly in domestic pigs , cattle , and dogs
There is evidence that antelopes in certain areas may also ca
the parasite. Man-fly-man transmission is hence, more common in
West and Centr
Africa. Asymptomatic persons can carry the parasites in their
blood for long
periods and could be continuously infective for the vectors.
TRYPANOSOMA BRUCEI RHODESIENSE ACUTE form of sleeping sickness
Found in east central and central Africa Vectors
G. morsitans, G. pallidipes, G. swynnertoni - inhabit the
savannah and pupate in dry friable earth
Reservoirs Wild game mammals (bushbuck, hartebeest, lion, hyena)
as well
as cattle The more virulent of the two, is thus, maintained in
the most
resistant reservoirs, resulting in continuous selection of
aggressivestrains.
LIFE CYCLE ofTrypanosoma brucei gambiense and Trypanosoma
brucerhodesiense
During a blood meal on the mammalian host, an infected tsetse
fly(genus Glossina ) injects metacyclic trypomastigotes into skin
tissue.
The parasites enter the lymphatic system and pass into
thebloodstream inside the host. They transform into
bloodstreamtrypomastigotes which are carried to other sites
throughout the body,reach other blood fluids (e.g. lymph, spinal
fluid), and continue thereplication by binary fission.
The entire life cycle of African Trypanosomes is represented
byextracellular stages. The tsetse fly becomes infected with
bloodstreamtrypomastigotes when taking a blood meal on an infected
mammalianhost.
In the fly’s midgut, the parasites transform into procyclic
trypomastigotes, multiply by binary fission, leave the midgut,
andtransform into epimastigotes.
The epimastigotes rea ch the fly’s salivary glands and
continmultiplication by binary fission.
The cycle in the fly takes approximately 3 weeks. Humans are the
mainreservoir for Trypanosoma brucei gambiense but this species can
alsobe found in animals. Wild game animals are the main reservoir
ofTrypanosoma brucei rhodesiense.
IMPORTANT Infective stage to man - metacyclic trypomastigote
Mode of transmission - inoculation of metacyclic trypomastigote
from a bite of a tsetse fly Diagnostic stage - trypomastigot e
in blood or lymph
-
8/16/2019 2 PARA 1 - Protozoa - Flagellates
5/13oup # 36 | Villanueva, M., Violanta, Yadao, Yau, Yee Edited:
AFV Page 5 of
PARASITOLOGY 2.1
Figure 11. Domestic and Wild Cycles of Gambian and Rhodesian
types of African Sleeping Sickness
) In West Africa, riverine tsetse flies (palpalis group) living
in the bushnsmit the Gambian forms to humans (man-fly cycle) and
sometimes tomestic animals, particularly pigs.) In East Africa,
tsetse flies (morsitans group) of the open savannahnsmit the
Rhodesian form to various mammals, mainly antelopes, and tomans.
The Gambian cycle can result in an epidemic.
PATHOGENESIS of Trypanosoma brucei gambiense and
Trypanosomabrucei rhodesiense
The clinical features of Gambian and Rhodesian disease are the
same;however, they vary in severity and duration.Rhodesian disease
progresses more rapidly and the symptoms areoften more
pronounced.The symptoms of the two diseases are also more
pronounced inCaucasians than in the local African
population.Classically, the progression of African trypanosomiasis
can be dividedinto three stages:1. The bite reaction (chancre)
A non-pustular, painful, itchy chancre forms 1-3 weeks afterthe
bite and lasts for 1-2 weeks. It leaves no scar.
2. Parasitemia (blood and lymphoid tissues) Parasitemia is more
prominent during the acute stage than
during the recurrence episodes. Parasitemia and lymph node
invasion is marked by attacks of
fever which starts 2-3 weeks after the bite and isaccompanied by
malaise, lassitude, insomnia, headache,lymphadenopathy, and
edema.
Febrile episodes may last few months as in Rhodesian diseaseor
several years as in Gambian disease.
Painful sensitivity of palms and ulnar region to
pressure(Kerandel's sign ) may develop in some Caucasians.
Very characteristic of Gambian disease is visible enlargementof
the glands of the posterior cervical region ( Winterbottom'ssign
).o Swollen nodes at the base of the skullo Lymph nodes become
swollen and congested especially
in the neck, groin, and legso Named after a British officer who
recognized the sign
among slaves bound for the Caribbean Marketo Symptoms are more
marked in newcomers than in
people native to the area
Figure 12.(Left) Winterbottom’s sign - swollen nodes at base of
skull
(Right) Kerandel’s sign - delayed sensation of pain after the
release of pressure of the hands
3. CNS stage Marked by changes in character and personality Lack
of interest and disinclination to work Avoidance of acquaintances
Morose and melancholic attitude alternating with exaltation Mental
retardation and lethargy Low and tremulous speech Tremors of tongue
and limbs Slow and shuffling gait Altered reflexes
Males become impotent. There is a slow progressive involvement
of cardiac tissue. The later stages are characterized by drowsiness
and uncontrollable
urge to sleep. The terminal stage is marked by wasting and
emaciation. Death results from coma, malnutrition, intercurrent
infection or cardiac
failure, or a severe fall.
Some differences of T b rhodesiense from T b gambiense Rarely
invades the nervous system Rapid weight loss and heart involvement
No somnambulism or other protracted nervous disorders Patients die
before CNS disorders develop Death within a few months of infection
Causes a more rapid course toward death
Figure 13. Comparison of West and East African Sleeping
Sickness
-
8/16/2019 2 PARA 1 - Protozoa - Flagellates
6/13oup # 36 | Villanueva, M., Violanta, Yadao, Yau, Yee Edited:
AFV Page 6 of
PARASITOLOGY 2.1
IMMUNOLOGYAfrican trypanosomes express a glycosylphosphatidyl
inositol (GPI) -anchored variable surface glycoprotein (VSG) as a
protective coat.
During infection, large amounts of VSG molecules are
releasedinto the circulation.
Their interaction with various cells of the immune
systemunderlies the severe infection-associated pathology.
Recent results have shown that anti-GPI vaccination can
preventthe occurrence of this pathology.
The two properties of the VSG coat that allow immune evasion
are: Shielding - the dense nature of the VSG coat prevents the
immune
system of the mammalian host from accessing the plasmamembrane
or any other invariant surface epitopes (such as ionchannels,
transporters, receptors, etc.) of the parasite
Periodic antigenic variation - the VSG coat undergoes
frequentgenetic modification, 'switching', allowing variants
expressing anew VSG coat to escape the specific immune response
raisedagainst the previous coat
Figure 14. VSG, the major surface component of Trypanosomes, is
alsoleased in host fluids. VSG induce resistance to complement
lysis, escape tospecific immune response, persistent cytokine
production, autoantibody
synthesis by molecule mimicry with host tissues.
Infectivity of Trypanosoma brucei rhodesiense to humans is due
to itsresistance to a lytic factor present in human serum.Host
immune response
↑ Ig (host immune system greatly stimulated) ↑ complement →
lysis of RBC → anemia
DIAGNOSISDemonstration of parasite in blood, bone marrow, CSF
cardagglutination test (CATT) to detect antibodies in whole blood
or serum
Figure 15. Diagnosis by demonstration of parasite in blood
sample
TREATMENTArsenicals – eye damage; trypanosomes become
tolerantOther drugs
Suramin Pentamidine Berenil Difluoromethylornithine (DFMO) –
brain infections
EPIDEMIOLOGY AND PREVENTION Transmission of trypanosomiasis
involves four interacting organisms:
The human host The insect vector The pathogenic parasite The
domestic and wild animal reservoirs
Glossina are efficient vectors and are responsible for linking
theseorganisms. Any reduction of their numbers should lead to
significantlyreduced transmission and hence, contribute to
elimination and thesustainability of control efforts.
Current vector control interventions involve the use of
insecticideseither through:
Sequential aerosol spraying technique (SAT) Ground spraying
Insecticide-treated targets or insecticide-treated animals
baits Use of traps Sterile insect technique (SIT)
Bush clearing (tsetse fly habitat destruction) or elimination of
wildanimals (tsetse reservoir hosts) have been discarded for
ecological andenvironmental concerns.
Odor baited traps and screen impregnated with insecticide
andappropriate attractive colors have been used in many countries
toeffectively suppress tsetse fly population by 99%.
These artificial bait methods are cheaper than ground and
aerialspraying but communities and governments cannot deploy themon
sustainable bases, as they are labor and managementintensive.
The Sterile Insect Technique (SIT) is another approach to reduce
tsetsefly populations.
Females mate only once in their lifetime thus, any mating with
asterile male will prevent females from giving birth to any
offspring.
SIT consists in rearing a large numbers of laboratory male
tsetseflies which are irradiated and subsequently released in the
wild tocompete with wild (naturally occurring) males so that
femalesinseminated by them produce no offspring.
SECTION STERCORARIA – TRYPANOSOMA CRUZI Depending on its host
environment, the organism occurs in three
different forms. The trypanosomal (trypomastigote) form ,
foumammalian blood, is 15 to 20 microns long and morphologically
similarto African trypanosomes.
The crithidial (epimastigote) form is found in the insect
intestine. The leishmanial (amastigote) form , found
intracellularly or
pseudocysts in mammalian viscera (particularly in myocardium
andbrain), is round or oval in shape, measures 2-4 microns, and
lacks aprominent flagellum.
-
8/16/2019 2 PARA 1 - Protozoa - Flagellates
7/13oup # 36 | Villanueva, M., Violanta, Yadao, Yau, Yee Edited:
AFV Page 7 of
PARASITOLOGY 2.1
Figure 16. Trypanosoma cruzi
American trypanosomiasis (Chagas Disease ) Widespread in the
American continent chiefly among small wild
mammals (enzootic sylvatic cycle) Human Chagas Disease -
bio-ecological and socioeconomic factors
leave rural poor populations of South and Central America
incontact with the sylvatic cycle, where the parasite is
transmittedby natural vectors of the infection
From the Public Health standpoint, the importance of
ChagasDisease remains correlated to so called "domestic” cycle, not
onlybecause millions of human beings are involved but also because
allthe available control measures are directed against it.
The most important mechanism of transmission of T. cruzi
tohumans and other mammals is the feces of infected
triatomines.
The vectors of Chagas Disease are insects of the order
Hemiptera,family Reduviidae, subfamily Triatominae.
These are species that colonize poorer quality rural houses,
wherecolonies of hundreds of individuals (or even thousands) can
befound.
The Triatominae (commonly known as kissing bugs) are defined
assubfamily of Reduviidae (commonly known as assassin bugs)
thatsuck vertebrate blood (strictly hematophagous) and are
mainlyrestricted to the New World
Within the subfamily, genera Triatoma, Rhodnius,
andPanstrongylus contain species of bugs that are
especiallyimportant vectors of Trypanosoma cruzi, the agent of
ChagasDisease in humans.
Figure 17. Kissing Bug (Rhodnius prolixus) Feeding on a
Human
LIFE CYCLE The organism is transmitted to mammalian host by many
species of
kissing (riduvid) bug. Transmission takes place during the
feeding of the bug which normally
bites in the facial area (hence the name, kissing bug) and has
the habitof defecating during feeding.
The metacyclic trypomastigotes, contained in the fecal material,
gainaccess to the mammalian tissue through the wound which is
oftenrubbed by the individual that is bit ten.
Subsequently, they enter various cells, including macrophages,
wherethey differentiate into amastigotes and multiply by binary
fission.
Figure 18. The amastigotes differentiate into
non-replicatingtrypomastigotes and the cells rupture to release
them into the bloodstream.
Additional host cells, of a variety of types, can become
infected and thetrypomastigotes once again form amastigotes inside
these cells.
Figure 19. Entry of metacyclic trypanomastigota via break on
skin Uninfected insect vectors acquire the organism when they feed
on
infected animals or people containing trypomastigotes
circulating intheir blood.
Inside the alimentary tract of the insect vector, the
trypomastigotesdifferentiate to form epimastigotes and divide
longitudinally in themidgut and hindgut of the insect where they
develop into infectivemetacyclic trypomastigotes.
Transmission may also occur from man to man by blood
transfusionand by the transplacental route.
IMPORTANT Infective stage to man: metacycylic trypomastigote
Mode of transmission: entry of metacyclic trypomastigote from a
break on the skin Diagnostic stage : trypomastigote in blood,
CSF, fixed tissues, or
-
8/16/2019 2 PARA 1 - Protozoa - Flagellates
8/13oup # 36 | Villanueva, M., Violanta, Yadao, Yau, Yee Edited:
AFV Page 8 of
PARASITOLOGY 2.1
SYMPTOMSChagas Disease can be divided into three stages:
The primary lesion The primary lesion, chagoma, appearing at the
site of
infection and within a few hours of a bite, consists of
aslightly raised, flat, non-purulent erythematous plaquesurrounded
by a variable area of hard edema.
It is usually found on the face, eyelids, cheek, lips or
theconjunctiva, but may occur on the abdomen or limbs.
When the primary chagoma is on the face, there is anenlargement
of the pre- and post- auricular and thesubmaxillary glands on the
side of the bite.
Infection in the eyelid, resulting in a unilateral
conjunctivitisand orbital edema ( Romaňa's sign), is the most
commonfinding.
The acute stage The acute stage appears 7-14 days after
infection. It is characterized by restlessness, sleeplessness,
malaise,
increasing exhaustion, chills, fever, and bone and
musclepains.
Other manifestations of the acute phase are cervical,
axillaryand iliac adenitis, hepatomegaly, erythematous rash,
andacute myocarditis. There is a general edematous
reactionassociated with lymphadenopathy.
Diffuse myocarditis, sometimes accompanied by
seriouspericarditis and endocarditis, is very frequent during
theinitial stage of the disease.
In children, Chagas Disease may cause meningo-encephalitisand
coma. Death occurs in 5-10 percent of infants.
Hematologic examination reveals lymphocytosis
andparasitemia.
The chronic stage The acute stage is usually not recognized and
often resolves
with little or no immediate damage and the infected hostremains
an asymptomatic carrier. An unknown proportion(guessed at 10-20%)
of victims develop a chronic disease.They alternate between
asymptomatic remission periods andrelapses characterized by
symptoms seen in the acute phase.
Cardiac arrhythmia is common. The chronic disease results in an
abnormal function of the
hollow organs, particularly the heart, esophagus, and colon.The
cardiac changes include myocardial insufficiency,cardiomegaly,
disturbances of atrio-ventricular conduction,and the Adams-Stoke
Syndrome. Disturbances of peristalsislead to megaesophagus and
megacolon.
PATHOLOGY AND IMMUNOLOGYThe pathological effects of acute phase
Chagas Disease largely resultfrom direct damage to infected
cells.In later stages, the destruction of the autonomic nerve
ganglions may
be of significance. Immune mechanisms, both cell mediated
andhumoral involving reaction to the organism and to autologous
tissues,have been implicated in pathogenesis.T. cruzi stimulates
both humoral and cell mediated immune responses .The infection
causes severe depression of both cell mediated andhumoral immune
responses.Antibody has been shown to lyse the organism , but rarely
causeseradication of the organism, perhaps due to its
intracellularlocalization.Cell mediated immunity may be of
significant value. While normalmacrophages are targeted by the
organism for growth, activatedmacrophages can kill the organism
.Unlike T. brucei, T. cruzi does not alter its antigenic coat.
Antibodies directed against heart and muscle cells have also
detected in infected patients leading to the supposition that there
is anelement of autoimmune reaction in the pathogenesis of
ChagasDisease.
Immunosuppression may be due to induction of suppressor
T-cand/or overstimulation of macrophages .
DIAGNOSIS Demonstration of the causal agent is the diagnostic
procedure in acute
Chagas Disease. It almost always yields positive results and can
beachieved by:
Microscopic examination of fresh anticoagulated blood or its
buffycoat for motile parasites and of thin and thick blood
smearsstained with Giemsa, for visualization of parasites.
Figure 20. The most reliable method for differentiating the
trypomastigotes(motile blood stage forms) of T. brucei and T. cruzi
is by the size of th
kinetoplast (see arrows). T. brucei has a relatively small
kinetoplast , T. cruzi has a larger kinetoplast . T. cruzi
trypomastigotes also commonly
form a "C" shape, although this is a less reliable feature.
Finally, T. cruzi mayalso be found as a non-motile amastigote form
in various tissues, while T.
brucei is only found in the trypomastigote form in humans.
Isolation of the agent:
Inoculation in culture with specialized media (e.g. NNN, LIT)
Inoculation into mice Xenodiagnosis where uninfected triatomine
bugs are fed on the
patient's blood and their gut contents examined for parasites
4weeks later
TREATMENT The most effective drugs kill only extracellular
protozoa. Nifurtimox and benznidazole
Somewhat effective in curing acute infections Require long
treatment duration With significant side effects Patients remain
seropositive even after disappearance of parasites
in the blood.
LEISHMANIA
Like trypanosomes – heteroxenous Part of life cycle in sandflies
– promastigote Remainder of life cycle in vertebrate tissues
Only amastigotes are found Known as Leishmania-Donovan (L-D)
bodies
Mammals most commonly affected - humans, dogs, and rodents
VECTORS: SANDFLIESFamily Psychodidae
Subfamily PhlebotominaeGenera: Phlebotomus (old world)
Sergentomyia (old world)Lutzomyia (new world)Bromptomyia (new
world)
-
8/16/2019 2 PARA 1 - Protozoa - Flagellates
9/13oup # 36 | Villanueva, M., Violanta, Yadao, Yau, Yee Edited:
AFV Page 9 of
PARASITOLOGY 2.1
ETIOLOGYSeveral species of Leishmania are pathogenic for
man:
L. donovani causes visceral leishmaniasis (Kala-azar, black
disease,dumdum fever)
L. tropica (L. t. major, L. t. minor, and L. ethiopica )
causecutaneous leishmaniasis (oriental sore, Delhi ulcer, Aleppo,
Delhior Baghdad boil)
L. braziliensis (also L. mexicana and L. peruviana ) are
etiologicagents of mucocutaneous leishmaniasis (espundia, Uta,
chiclero
ulcer)
VISCERAL LEISHMANIASISCaused by Leishmania donovaniDiscovered by
William Leishman (1900) in spleen smears of a soldierwho died of a
fever in Dum-Dum, IndiaDisease known as Dum-Dum fever or
kala-azarLife Cycle
Female sand fly takes a blood meal from mammals and
transferamastigotes in its mid gut
Amastigotes transform into procyclic promastigotes Procyclic
promastigotes change into metacyclic promastigotes by
simple division Promastigotes migrate to the pharyngeal valve
and are transferred
to mammals through blood meal as metacyclic promastigotes
Metacyclic promastigotes actively invade macrophages,
granulocyctes or are phagocytosed Promastigotes transform into
amastigotes and multiply by simple
division in the macrophages Amastigotes leave infected cells to
infect new macrophages or
transferred to vector via blood meal Pathogenesis
Clinically, L. donovani infections may range from asymptomatic
toprogressive to fully developed kala-azar
Incubation period – 2-4 months Begins slowly with low grade
fever and malaise Followed by progressive wasting and anemia,
protrusion of the
abdomen from enlarged liver and spleen Finally death in 2 -3
years
Treatment Antimony compounds applied to lesions or injected
intravenously
or intramuscularly The immediate cause of death is often
invasion of secondary
pathogen.
Figure 21. Amastigotes in macrophage (?? Unlabeled in slide)
CUTANEOUS LEISHMANIASISCaused by: Leishmania tropica and
Leishmania major Found in west central Africa, the Middle East, and
Asia Minor into IndiaThe 2 species are found in different
localities and have differentreservoir and intermediate hosts.
Figure 22. Sandflies of the Genus Phlebotomus - Intermediate
Hosts andVectors
Life Cycle When a fly takes blood meal-containing amastigotes,
parasites
multiply in the midgut and then move to the pharynx. Sandfly
saliva contains low molecular weight compound and
peptides that serve as vasodilators and facilitate infection.
Leishmaniasis is transmitted by the bite of infected female
phlebotomine sandflies. The sandflies inject the infective stage
(i.e. promastigotes) from
their proboscis during blood meals. Promastigotes that reach the
puncture wound are phagocytized by
macrophages and other types of mononuclear phagocytic cells.
Progmastigotes transform in these cells into the tissue stage of
the
parasite (i.e., amastigotes), which multiply by simple division
andproceed to infect other mononuclear phagocytic cells.
Parasite, host, and other factors affect whether the
infectionbecomes symptomatic and whether cutaneous or
visceralleishmaniasis results. Sandflies become infected by
ingestinginfected cells during blood meals.
In sandflies, amastigotes transform into promastigotes, develop
inthe gut (in the hindgut for leishmanial organisms in the
Vsubgenus; in the midgut for organisms in the Leishsubgenus), and
migrate to the proboscis.
Figure 23. In cutaneous leishmaniasis, the organism (L. tropica)
multiplieslocally, producing a papule 1-2 weeks (or as long as 1-2
months) after thebite. The papule gradually grows to form a
relatively painless ulcer. Thecenter of the ulcer encrusts while
satellite papules develop at the periphery.The ulcer heals in 2-10
months, even if untreated but leaves a disfiguringscar. The disease
may disseminate in the case of depressed immune function.The sores
can change in size and appearance over time. They often end
uplooking somewhat like a volcano, with a raised edge and central
crater. A
-
8/16/2019 2 PARA 1 - Protozoa - Flagellates
10/13oup # 36 | Villanueva, M., Violanta, Yadao, Yau, Yee
Edited: AFV Page 10 o
PARASITOLOGY 2.1
ab covers some sores. The sores can be painless or painful. Some
peopleve swollen glands near the sores (for example, in the armpit
if the sorese on the arm or hand).
Diagnosis Scrapings from the side of an ulcer smeared on a slide
and stained
with Wright’s or Giemsa stain will show parasites in
endothelialcells and monocytes, even if they cannot be found in
circulatingblood.
Amastigotes of Leishmania are spherical to ovoid and measure
1-5µm long by 1-2µm wide. They possess a large nucleus, aprominent
kinetoplast, and a short axoneme, the last of which israrely
visible by light microscopy. The organisms reside inmacrophages of
the host and can be found throughout the body.
Figure 24. Parasites in endothelial cells and monocytes
MUCOCUTANEOUS LEISHMANIASIS Caused by Leishmania braziliensis
Produces a disease known as espundia, uta, mucocutaneous
leishmaniasis Found in vast area between central Mexico and
northern Argentina Life cycle and Pathogenesis
Similar to L. tropica except that the promastigotes reproduce
inthe hindgut of the sandfly
Figure 25. Mucocutaneous Leishmaniasis
Symptoms Initial symptoms of mucocutaneous leishmaniasis are the
same as
those of cutaneous leishmaniasis except that in this disease,
theorganism can metastasize and the lesions can spread to
mucoid(oral, pharyngeal, and nasal) tissues and lead to their
destructionand hence, sever deformity.
-
8/16/2019 2 PARA 1 - Protozoa - Flagellates
11/13oup # 36 | Villanueva, M., Violanta, Yadao, Yau, Yee
Edited: AFV Page 11 o
PARASITOLOGY 2.1
APPENDIX
Figure 1. Tsetse Fly Stages (Trypanosoma brucei)
Figure 2. Triatomine Bug Stages (Trypanosoma cruzi)
-
8/16/2019 2 PARA 1 - Protozoa - Flagellates
12/13oup # 36 | Villanueva, M., Violanta, Yadao, Yau, Yee
Edited: AFV Page 12 o
PARASITOLOGY 2.1
Figure 3. Visceral Leishmaniasis
Figure 4. Sandfly Stages (Cutaneous Leishmaniasis)
-
8/16/2019 2 PARA 1 - Protozoa - Flagellates
13/13
PARASITOLOGY 2.1
SUMMARY
CHARACTERISTIC STAGES OF SPECIES OF LEISHMANIA AND TRYPANOSOMA
IN MAN AND IN THE INSECT HOST (FROM PARA MANUALStages of
Parasite
Parasite Leishmania Leptomonad Crithidial Trypanosomaltropica In
macrophages of skin &
subcutaneous tissuesIn midgut, proboscis ofsandfly
Absent Absent
braziliensis Same as L. tropica Same as L. tropica Absent
Absentdonovani In macrophages of liver,
spleen, bone marrow andlymph nodes
Same as L. tropica Absent Absent
rhodesiense Absent Absent In salivary glands of tsetse fly In
proboscis of tsetse fly; inbloodstream and lynode
gambiense Absent Absent Same as T. rhodesiense Same as T.
rhodesiensecruzi In macrophages of skin,
lymph node, liver, spleen,brain etc.
Transitional stage only In midgut of triatomid bug In hindgut,
feces of bug; inblood stream during acattacks