-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
1/59
2004 FRACP Written Examination
Paediatrics & Child Health
Paper 2 Clinical Applications
INTRODUCTION
Format
Paper 1 Medical Sciences: 70 questions; time allowed: 2
hoursPaper 2 Clinical Applications: 100 questions; time allowed: 3
hours
All questions are in the A-type multiple-choice format, that is,
the single best answer of the five optionsgiven.
In the questions, values appearing within [ ] refer to normal
ranges.
When visual material has been turned on its side, an arrow on
the page indicates the orientation of thevisual material.
Questions do not necessarily appear in the order in which they
were first printed.
AnswersA table of answers is located at the end of each
paper.
ScoringA correct answer will score one mark and an incorrect
answer zero. There is no negative marking in
the FRACP Written Examination.
QueriesContact the Executive Officer, Examinations Section,
Department of Training and Assessment via e-mail:
[email protected].
Please note that with changes in medical knowledge, some of the
information may no longer becurrent.
Copyright 2005 by The Royal Australasian College of
Physicians
All Written Examination papers are copyright. They may not be
reproduced in whole or part withoutwritten permission from The
Royal Australasian College of Physicians, 145 Macquarie Street,
Sydney,
Australia.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
2/59
2 P204
QUESTION 1
Which of the following vaccines would be most likely to be
transmitted from a normal child to theirimmunocompromised
sibling?
A. Bacille Calmette-Gurin (BCG).
B. Influenza.
C. Measles-mumps-rubella (MMR).
D. Oral polio.
E. Varicella-zoster.
QUESTION 2
An eight-year-old boy is admitted with an episode of acute
asthma. His oxygen saturation is 92% in
air. He is prescribed prednisolone 1 mg/kg and hourly salbutamol
12 puffs. Three hours later hisoxygen saturation in air has dropped
to 89%. He looks well and is less distressed than whenadmitted. He
has widespread wheeze with good air entry.
Based on these findings, the most appropriate next step in his
management is:
A. add ipratroprium bromide.
B. blood gas analysis.
C. change to intravenous salbutamol.
D. chest X-ray to rule out a pneumothorax.
E. reduce frequency of salbutamol.
QUESTION 3
A 13-year-old boy presents with nonspecific abdominal pain. The
boy has a history of seizures. Hismother is known to have chronic
renal failure. Physical examination shows a small 13-year-old who
isnormotensive with small areas of hypopigmentation on his trunk.
The abdominal pain quicklysubsides following hospital admission. A
renal ultrasound scan shows enlarged kidneys and multipleechogenic
foci throughout both kidneys.
Which one of the following is the most likely explanation of the
renal abnormality in this boy?
A. Dominant polycystic kidney disease.
B. Juvenile nephronophthisis.
C. Papillary necrosis.
D. Recessive polycystic kidney disease.
E. Renal angiomyolipomata.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
3/59
3 P204
QUESTION 4
When assessing an adolescent, whose history is likely to have
the greatest sensitivity for the detectionof depressive
symptoms?
A. Friends.
B. Siblings.
C. The adolescent.
D. The classroom teacher.
E. The mother.
QUESTION 5
A 15-year-old girl is brought into the emergency room by friends
after attending a birthday party. Her
friends are concerned because there has been an alteration in
her conscious state. She is febrile andis visibly flushed and
sweating. Her heart rate is 120/minute and regular. Her blood
pressure is160/95 mmHg. Her neurological exam was notable for her
being combative with small but reactivepupils. During your
examination she begins to have a generalised seizure.
She has a history of depression and is being managed by a
psychiatrist.
You suspect an ingestion or intoxication.
Which of the following is the most likely cause?
A. Alcohol.
B. Ecstasy.
C. Marijuana.
D. Mushroom intoxication.
E. Tricyclic antidepressants.
QUESTION 6
A two-year-old boy is taken to the emergency department by his
parents with rectal bleeding. Hepassed about 100 mL of blood per
rectum. The blood is slightly altered. There were no
associatedabdominal pains, and the abdomen is soft and non-tender
on examination. He has no cutaneousstigmata or telangiectasia.
Which of the following is the most likely diagnosis?
A. Campylobacterinfection.
B. Inflammatory bowel disease.
C. Intussusception.
D. Meckel diverticulum.
E. Polyp.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
4/59
4 P204
QUESTION 7
Copyright 2005 by The Royal Australasian College of
Physicians
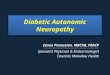
Parasternal long axis echocardiogram
Apical 4-chamber echocardiogram
Key: AO aorta
RA right atriumLA left atriumLV left ventricleRV right
ventricle
The echocardiograms shown above were obtained from an otherwise
healthy three-month-old infantpresenting for assessment of a
murmur. They show multiple intraventricular lesions.
Which of the following is the most likely diagnosis?
A. Neurofibromatosis type 1.
B. Noonan syndrome.
C. Proteus syndrome.
D. Sturge-Weber syndrome.
E. Tuberous sclerosis.
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
5/59
5 P204
QUESTION 8
A five-year-old child has the karyotype shown above. What is the
most likely phenotype at this age?
A. Ambiguous genitalia.
B. Developmental delay.
C. Normal female.
D. Normal male.
E. Short stature.
QUESTION 9
Unawareness of hypoglycaemia is predominantly due to failure of
secretion of which one of thefollowing hormones?
A. Adrenaline.
B. Cortisol.
C. Glucagon.
D. Growth hormone.
E. Somatostatin.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
6/59
6 P204
QUESTION 10
A two-year-old boy from Nigeria immigrated a year ago. He
presents to the emergency departmentwith a fever of 40C. His mother
says that he has known sickle cell disease diagnosed previously
inAfrica. Initial examination reveals a sick child along with an
initial full blood count showing a raisedneutrophil count with left
shift.
The most likely organism causing his fever is:
A. Epstein-Barr virus.
B. Haemophilus influenzaetype b.
C. Plasmodium falciparum.
D. Salmonella typhi.
E. Streptococcus pneumoniae.
QUESTION 11
A three-year-old girl is found floating face down in the family
pool after being missed forapproximately five minutes. Basic life
support is commenced on the scene and on arrival in theemergency
department the girl is in asystole. She is apnoeic and pulseless,
her temperature is 33Cand the maximum estimated period of pulseless
apnoea is 15 minutes. The child is rapidly intubatedand ventilated,
intravenous access is gained and external cardiac compressions are
continued.
Which of the following is the most appropriate next step in the
acute management of this child?
A. Administer intravenous adrenaline.
B. Administer intravenous atropine.
C. Commence active warming measures.
D. Counsel the family and cease active resuscitative
measures.
E. Immediate direct current (DC) defibrillation.
QUESTION 12
Which of the following is least consistent with night
terrors?
A. Amnesia of the episode by the child.
B. Family history.
C. Occurrence in rapid eye movement (REM) sleep.
D. Occurrence in the first third of the night.
E. Onset at five years of age.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
7/59
7 P204
QUESTION 13
A 41-week gestation female infant was born by normal vaginal
delivery with a birth weight of 3045 gand head circumference of
33.5 cm. A rash on her limbs was noted on the first day of life.
Sheestablished breastfeeding very well. At 5 days of age, she was
noted to be irritable and feedingpoorly. She developed left sided
clonic jerks with eye deviation. These were controlled with
intravenous phenobarbitone.
Copyright 2005 by The Royal Australasian College of
Physicians
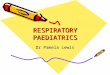
The rash as illustrated above was described as an erythematous
vesicular rash which was crusted inplaces. It was present on the
forearms and lower limbs.
The most likely cause of this rash would be:
A. congenital bullous ichthyosiform erythroderma.
B. congenital varicella.
C. epidermolysis bullosa.
D. herpes simplex virus infection.
E. incontinentia pigmenti.
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
8/59
8 P204
QUESTION 14
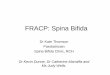
The flow-volume loop shown above is most consistent with:
A. aberrant right subclavian artery.
B. asthma.
C. laryngeal web.
D. subglottic stenosis.
E. tracheomalacia.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
9/59
9 P204
QUESTION 15
A 24-year-old pregnant woman reports at her first antenatal
visit that her sister gave birth to a childwith congenital heart
block (CHB). Which one of the following tests would be most useful
in assessingthe risk of CHB in this pregnancy?
A. Antibodies to DNA.
B. Antibodies to extractable nuclear antigens (ENA).
C. Anticardiolipin antibodies.
D. Fluorescent antinuclear antibody (ANA) test.
E. Lupus anticoagulant.
QUESTION 16
A six-month-old boy presents with a two-month history of
persistent vomiting, loose bowel motions,poor weight gain,
irritability after feeds and a persistent rash on his face and
upper arms. He was bornat term, breastfed to two months of age, and
subsequently changed to a cows milk-based formula.Solids, including
a wheat-based cereal, had been introduced from four months of
age.
The following immunological investigations were performed:
total serum IgE 7 kU/L [0-20]
total serum IgA 0.37 g/L [0.14-0.69]
radioallergosorbent assay to cow's milk
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
10/59
10 P204
QUESTION 17
A mother with a history of genital herpes delivers a baby at
term by normal vaginal delivery. Threedays after birth the infant
is well, but is noted to have two small blistering lesions on the
arm.Investigations confirm herpes simplex virus type 2 from the
skin lesions.
The most appropriate treatment would be:
A. intravenous aciclovir.
B. intravenous ganciclovir.
C. observation.
D. oral aciclovir.
E. oral famciclovir.
QUESTION 18
An eight-year-old child presents to a regional emergency
department with a one-week history ofweakness in both legs,
stumbling gait and complaints of numbness. The family is currently
underconsiderable stress with the suicide of a close relative and
parental fighting. Neurological examinationreveals apparent
reduction in power, variable sensory loss and normal deep tendon
reflexes. The gaitis erratic.
Which of the following is the most likely diagnosis?
A. Conversion disorder.
B. Guillain-Barr syndrome.
C. Multiple sclerosis.
D. Transverse myelitis.
E. Viral myositis.
QUESTION 19
The occurrence of a second malignancy after successful treatment
of a primary tumour is least likelyto be associated with:
A. Bloom syndrome.
B. cyclophosphamide.
C. Fanconi aplastic anaemia.
D. growth hormone treatment.
E. radiotherapy.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
11/59
11 P204
QUESTION 20
A 10-year-boy presents with an episode of acute left-sided loin
pain. He passes bright red urine andrequires intravenous morphine
for analgesia. A plain abdominal X-ray is shown below.
Which one of the following is most likely to play an important
role in the development of this condition?
A. High sodium diet.
B. Hypokalaemia.
C. Hypomagnesaemia.
D. Increased urine citrate concentration.
E. Metabolic alkalosis.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
12/59
12 P204
QUESTION 21
A five-month-old baby boy returns for review of his congenital
hypothyroidism. He continues to growalong the 50th percentile for
his length, weight and head circumference. He has been on
anappropriate dose of daily replacement with thyroid hormone (37.5
g/day).
Repeat thyroid function tests (carried out at his visit) are as
follows:
thyroxine (T4) 18 pmol/L [10-23]
thyroid-stimulating hormone (TSH) 153.0 mU/L [0.4-4.0]
The most likely explanation for the elevated TSH is:
A. expected result, as TSH can take many months to suppress.
B. iodine deficiency.
C. malabsorption.
D. poor parental compliance.
E. thyroid hormone resistance.
QUESTION 22
A seven-year-old boy wakes in the morning and cries out to his
parents to come quickly. Hecomplains to his parents that the room
is spinning. The symptoms seem to be aggravated by headmotion and
change of position from lying down. He becomes pale, sweaty and
nauseated wheneverhe moves or tries to sit up in bed. He is helped
to the bathroom because he has difficulty standingand walking
unsupported and vomits repeatedly. His parents bring him to the
emergency department
soon afterwards.
On examination, he is found to be perfectly conscious and
cooperative if left to lie still in bed. He hasleft-beating
nystagmus in all positions of gaze but otherwise no focal
neurologic findings. His hearingis normal. He has a mild upper
respiratory tract infection.
The most likely diagnosis is:
A. acute disseminated encephalomyelitis (ADEM).
B. acute labyrinthitis.
C. acute vestibular neuritis.
D. cerebellar ataxia.
E. Menires disease.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
13/59
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
14/59
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
15/59
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
16/59
16 P204
QUESTION 30
A seven-year-old girl presents with a history of bleeding gums
after she cleans her teeth. Examinationof her mouth reveals
evidence of gingivitis as shown below.
A defect of which component of immune function is most likely to
be associated with this clinicalpresentation?
A. B cells.
B. Complement.
C. Natural killer cells.
D. Neutrophils.
E. T cells.
QUESTION 31
A four-year-old boy with severe haemophilia A and a high titre
factor VIII inhibitor needs surgery. Theperi-operative replacement
coagulation product of choice is:
A. cryoprecipitate.
B. fresh frozen plasma.
C. recombinant activated factor VII.
D. recombinant factor VIII.
E. recombinant factor IX.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
17/59
17 P204
QUESTION 32
An 11-year-old boy presents to the emergency department
following a fall onto his outstretched leftarm whilst
rollerblading. On examination his left hand is neurovascularly
intact and there is nodeformity. His X-ray is shown below.
Which of the following is the most appropriate next step in
management?
A. Apply backslab and review in one week.
B. Closed reduction in the emergency department.
C. Closed reduction in the operating theatre.
D. Open reduction.
E. Urgent orthopaedic review in the emergency department.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
18/59
18 P204
QUESTION 33
A three-month-old boy, 10% dehydrated with rotavirus diarrhoea,
has a serum sodium of 166 mmol/L[135-145]. He is normotensive, has
just passed urine and when weighed two days ago was 5
kg.Intravenous fluid is commenced.
Which of the following is the most appropriate regimen?
A. 0.18% saline, 4% dextrose and 20 mmol/L potassium chloride at
35 mL/hour.
B. 0.18% saline, 4% dextrose and 20 mmol/L potassium chloride at
50 mL/hour.
C. 0.45% saline, 2.5% dextrose and 20 mmol/L potassium chloride
at 50 mL/hour.
D. 0.9% saline and 20 mmol/L potassium chloride at 35
mL/hour.
E. 0.9% saline and 20 mmol/L potassium chloride at 50
mL/hour.
QUESTION 34
A 12-year-old boy presents with chafed and reddened hands as a
result of frequent washing. Hisfather is an infectious disease
physician. The boy describes intrusive thoughts about infection
withPseudomonas and scrupulously cleans the family bathroom each
time before using it. He isconcerned about his father bringing home
contaminants and has become increasingly isolated fromother members
of the family.
The best treatment will be multimodal. The component with the
best evidence of efficacy is:
A. clomipramine.
B. cognitive-behaviour therapy.
C. family therapy.
D. sertraline.
E. venlafaxine.
QUESTION 35
A nine-month-old boy presents after a three-minute tonic-clonic
seizure, associated with a fever of39C. He is fully immunised. The
infant has a number of small ulcers on the tip of the tongue and
onthe gingival mucosa of the lower incisors. The following day the
infant develops weakness of his leftleg.
The infant is most likely to be infected with:
A. cytomegalovirus (CMV).
B. enterovirus 71.
C. Epstein-Barr virus (EBV).
D. human herpes virus 6 (HHV-6).
E. poliovirus type 3.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
19/59
19 P204
QUESTION 36
A 14-year-old boy complains of heel pain of six months duration.
The following X-ray is obtained.
Which of the following is the most likely cause of his heel
pain?
A. Ankylosing spondylitis.
B. Calcaneal osteomyelitis.
C. Hypermobile pes planus.
D. Reflex sympathetic dystrophy.
E. Sever disease (Achilles tendonitis).
QUESTION 37
A term newborn infant is noted to be tachypnoeic from delivery.
On examination on day 1 he is alsonoted to have prominent pulses
and an active precordium. His liver is palpable 4 cm below the
costalmargin. No murmurs are audible. His arterial oxygen
saturation is 98% in room air.
Which of the following is the most likely diagnosis?
A. Aneurysm of the vein of Galen.
B. Group B streptococcal sepsis.
C. Hypoplastic left heart.
D. Patent (persistent) ductus arteriosus.
E. Thyrotoxicosis.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
20/59
20 P204
QUESTION 38
A 26-year-old woman has a baby with Down syndrome. Subsequent
investigations reveal that thewoman is a carrier of a balanced
Robertsonian translocation involving chromosomes 14 and 21.
Herkaryotype is 45,XX,t(14;21). In a subsequent pregnancy, she
declines the offer of prenatal testing.
If the pregnancy goes to term, the most likely outcome is a baby
with:
A. an attenuated form of Down syndrome due to mosaic trisomy
21.
B. Down syndrome.
C. intrauterine growth retardation due to maternal isodisomy
14.
D. normal phenotype.
E. severe malformations due to trisomy 14.
QUESTION 39
A 12-month-old girl is referred by her general practitioner
because of failure to thrive. Her weight wason the 50th percentile
at six months but had fallen to the 10th percentile at one year.
She had a moistcough at nine months which lasted 10 days. Neonatal
immunoreactive trypsin screening wasnegative.
On examination she has buttock and thigh wasting. A full blood
examination reveals a mildleucocytosis and her electrolyte profile
demonstrates the following:
serum sodium 120 mmol/L [135-145]
serum potassium 2.0 mmol/L [3.5-5.0]
serum chloride 90 mmol/L [90-110]
The most appropriate next investigation is:
A. anti-endomysial antibody.
B. serum and urinary osmolality.
C. serum 17-OH progesterone.
D. sweat test.
E. urinary sodium and potassium.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
21/59
21 P204
QUESTION 40
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
22/59
22 P204
QUESTION 40 (continued)
An eight-year-old girl is referred to hospital because of
progressive pallor for three months. In the pastfour weeks, she has
developed painful lesions on her feet, as shown opposite. There is
no pastmedical history of note.
Initial investigations show the following:
haemoglobin 89 g/L [110-140]
white cell count 6 x 109 /L [4-11]
neutrophils 4.0 x 109 /L [1.4-4.6]
lymphocytes 1.0 x 109 /L [1.4-4.6]
eosinophils 0.20 x 109 /L [
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
23/59
23 P204
QUESTION 42
A 13-year-old girl presents to your office with a six-month
history of daily headaches. The headachesare present on waking and
on occasions are associated with vomiting without nausea. She has
hadintermittent double vision and transient episodes of loss of
vision lasting seconds only. She is takingtetracyclines for
acne.
On examination, she is moderately obese, afebrile, and has no
neurocutaneous stigmata. She has amoderate amount of facial acne.
Her blood pressure is 105/65 mmHg. Her extraocular movementsshow a
partial left sixth nerve palsy and she has gross papilloedema.
There are no other abnormalfindings.
A T2-weighted magnetic resonance imaging (MRI) scan of her brain
is shown below.
The most likely diagnosis is:
A. aqueductal stenosis.
B. benign intracranial hypertension (BIH).
C. craniopharyngioma.
D. meningioma.
E. temporal lobe tumour.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
24/59
24 P204
QUESTION 43
A nine-year-old girl is seen with polyuria and polydipsia. She
is dehydrated and on routineassessment is found to have the
following blood test results:
glucose 38.2 mmol/L [3.8-6.2]
sodium 130 mmol/L [134-143]potassium 4.2 mmol/L [3.5-5.6]
pH 7.12 [7.35-7.45]
bicarbonate 9 mmol/L [18-29]
creatinine 0.035 mmol/L [
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
25/59
25 P204
QUESTION 45
A breastfed four-week-old girl is taken to hospital because of
several episodes of rectal bleeding withmost bowel motions. The
infant is passing four stools daily with visible streaks of bright
red blood andmucus. The infant is otherwise well and thriving.
Stool testing reveals the following findings:
red blood cells +++
white blood cells +
fat globules +
fatty acid crystals negative
reducing sugars 0.25%
Which of the following is the most likely diagnosis?
A. Allergic proctocolitis.
B. Anal fissure.
C. Bacterial gastroenteritis.
D. Juvenile polyp.
E. Swallowed maternal blood.
QUESTION 46
The distribution of joint involvement indicated by the red
colour in the diagram above is mostcharacteristic of which form of
childhood arthritis?
A. HLA B27-associated arthropathy.
B. Polyarticular juvenile idiopathic arthritis.
C. Psoriatic arthritis.
D. Rheumatic fever.
E. Systemic lupus erythematosus.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
26/59
26 P204
QUESTION 47
Diagnosis of a major depressive disorder according to the
Diagnostic and Statistical Manual, 4thedition (DSM-IV) requires a
number of symptoms to have been present nearly every day during
thesame two-week period.
Which of the following symptoms is least helpful in the
diagnosis of adolescent depression?
A. Anhedonia (feeling of loss of pleasure in all, or almost all,
activities).
B. Depersonalisation (feeling of being detached from
oneself).
C. Impaired concentration.
D. Irritable mood.
E. Marked change in appetite.
QUESTION 48
Serological evidence of recent streptococcal infection is least
likely to be associated with which of thefollowing manifestations
of rheumatic fever?
A. Carditis.
B. Erythema marginatum.
C. Migratory polyarthritis.
D. Subcutaneous nodules.
E. Sydenham chorea.
QUESTION 49
Infusion of cryoprecipitate is principally indicated for the
replacement of:
A. anti-thrombin.
B. factor IX.
C. fibrinogen.
D. IgG.
E. protein C.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
27/59
27 P204
QUESTION 50
An 11-year-old boy is admitted to hospital because he has been
lethargic for the past three to fourweeks. He appears to be thirsty
all the time with recent weight loss. He has been getting up to
passurine three times each night for the past two weeks. There is
no history of drug ingestion or infection.There is no past history
of note. Clinical examination is unremarkable.
His initial investigations show the following:
serum:
sodium 135 mmol/L [135-146]
potassium 3.0 mmol/L [3.5-5.0]
urea 16.0 mmol/L [3.2-7.7]
creatinine 0.29 mmol/L [0.04-0.08]
glucose 3.5 mmol/L [2.5-7.0]
urinalysis 1+ protein, no blood, moderate glucose
urine microscopy 40 white cells,
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
28/59
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
29/59
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
30/59
30 P204
QUESTION 53 (continued)
An eight-month-old girl presents with a history of cough and
recurrent chest infections. A clinicalphotograph and chest X-ray of
the patient are shown opposite.
Which one of the following is the most likely cause of this
infants clinical presentation?
A. Lymphoma.
B. Neuroblastoma.
C. Retinoblastoma.
D. Sarcoidosis.
E. Thymoma.
QUESTION 54
An 11-year-old boy has the facial appearance shown above. He has
a history of cleft palate repairand has borderline developmental
delay.
Which of the following is the most likely diagnosis?
A. Fetal alcohol syndrome.
B. Fragile X syndrome.
C. Kabuki make-up syndrome.
D. Myotonic dystrophy.
E. Velocardiofacial syndrome.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
31/59
31 P204
QUESTION 55
Following a normal pregnancy a male infant has a normal vaginal
delivery at term in the presence ofclear liquor. Immediately
following delivery, he is in severe respiratory distress with
marked subcostaland sternal recession. A normal cry is heard. A
soft, high-pitched, biphasic stridor is audible.
The most likely cause of this infants respiratory distress
is:
A. bilateral abductor vocal cord paralysis.
B. laryngo-oesophageal cleft.
C. lingular cyst.
D. severe laryngomalacia.
E. unilateral vocal cord paralysis.
QUESTION 56
A 14-month-old boy is brought to see you by his mother for
advice about his diet and which foodsshould be avoided because of
his allergies. At seven months of age, following his first exposure
toegg, he developed perioral urticaria within 10 minutes which
resolved after 15 minutes. There were noother symptoms. At 12
months of age, 5 minutes after ingestion of a small amount of
peanut butter ontoast, he developed generalised erythema, cough and
seemed distressed. No medical attention wassought and the symptoms
resolved spontaneously over 30 minutes. He has not had egg or
peanutsince these reactions and has not been exposed to other nut
products. He drinks soymilk because hismother believes this is
better for allergies than cows milk, however he can eat yoghurt and
ice creamwithout any obvious symptoms. He had atopic dermatitis on
the face and flexures until 12 months ofage but this has resolved.
Allergen skin prick tests show:
Allergen Wheal diameter (mm)Cows milk 5Egg white 0Peanut 9Cashew
nut 9Soy 3
Histamine control 5Saline control 0
On the basis of the history and the results of skin prick tests
the most appropriate advice would be toavoid:
A. peanut alone.
B. peanut and cashew nut.
C. peanut, cashew nut and cows milk.
D. peanut, cashew nut, cows milk and soy.
E. peanut, cashew nut, cows milk, soy and egg.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
32/59
32 P204
QUESTION 57
A five-year-old girl is brought to her paediatrician because of
recurrent headaches. During thephysical examination a number of
skin lesions were found. These are demonstrated in thephotograph
below.
Which of the following is the least likely to be associated with
her condition?
A. Acoustic neuroma.
B. Learning difficulties.
C. Macrocephaly.
D. Pseudoarthrosis.
E. Scoliosis.
QUESTION 58
An infant is noted on day 2 of life to be cyanosed. The arterial
oxygen saturation is 88% in room air.The remainder of the
examination is normal, including normal cardiac and respiratory
examinations.
Which of the following is the most likely diagnosis?
A. Alveolar capillary dysplasia.
B. Extralobar sequestration.
C. Tetralogy of Fallot.
D. Totally anomalous pulmonary venous return.
E. Transposition of the great arteries.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
33/59
33 P204
QUESTION 59
A four-year-old boy is referred to you for investigation of
persistent diarrhoea and poor weight gain.The following results are
obtained:
haemoglobin 100 g/L [110-150]
mean corpuscular volume (MCV) 70 fL [75-90]total serum IgA 0.07
g/L [1.23-2.32]
antigliadin-IgG antibody 88 U/L [
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
34/59
34 P204
QUESTION 62
A 10-year-old boy is referred with concerns regarding his
behaviour. His teachers are concerned thathe is easily distracted,
has a poor attention span and appears to have low self-esteem. He
oftenappears blank and seems to miss instructions. Over the past
six months he has been increasinglydefiant towards teachers, and he
has begun acting the class clown. He has had two detentions
this
term for inappropriate behaviour.
At home he has been moody and at times aggressive toward his
parents. He was an easy child untilhe was seven or eight years old,
but has been increasingly unhappy since. He has never reallyenjoyed
school.
He had language delay identified at age three, and had some
speech therapy. Otherwise hisdevelopmental milestones were achieved
age-appropriately.
The school arranged psychometric testing. On the Wechsler
Intelligence Scale for Children-ThirdRevision he had a full-scale
intelligence quotient (IQ) of 82, with a performance scale score of
104 anda verbal scale score of 72. On academic achievement testing
his arithmetic score was within theaverage range, but his reading
and spelling scores were both more than two standard deviations
below the mean. His literacy level was assessed at two years
below his current grade level. Theeducational psychologist noted
that he was reluctant to attempt some tasks.
Which of the following is the most likely primary diagnosis?
A. Attention deficit/hyperactivity disorder.
B. Depression.
C. Intellectual disability.
D. Primary generalised epilepsy with absence seizures.
E. Specific learning disability.
QUESTION 63
A four-year-old girl with Alagille syndrome (intrahepatic
hypoplasia of bile ducts) and long-standingcholestatic jaundice
presents with a broad-based ataxic gait. On examination her tendon
reflexes areabsent.
Which of the following is the most likely cause?
A. Folate deficiency.
B. Hypothyroidism.
C. Posterior fossa tumour.
D. Vitamin B12 deficiency.
E. Vitamin E deficiency.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
35/59
35 P204
QUESTION 64
An eight-year-old boy presents with a two-month history of
fever, night sweats, abdominal pain, achingjoints and weight loss
of 2 kg. He has developed the rash shown above over the last two
weeks. Hewas previously well.
Examination shows the rash but no other significant clinical
findings.
Which of the following is the most likely diagnosis?
A. Dermatomyositis.
B. Henoch-Schnlein purpura.
C. Parvovirus infection.
D. Polyarteritis nodosa.
E. Tuberculosis.
l Australasian College of PhysiciansCopyright 2005 by The
Roya
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
36/59
36 P204
QUESTION 65
A 14-year-old girl complains of tiredness. She has no
significant past medical history and denies anymedications. Apart
from being thin, there are no abnormal findings on examination. Her
bloodpressure is 105/70 mmHg.
Results of investigations are listed below.
Serum biochemistry:
sodium 138 mmol/L [135-145]
potassium 2.3 mmol/L [3.4-5.0]
chloride 85 mmol/L [103-109]
creatinine 0.10 mmol/L [0.06-0.12]
Arterial blood gases:
pH 7.50 [7.34-7.45]
PaO2 95 mmHg [80-100]PaCO2
42 mmHg [35-45]
bicarbonate 39 mmol/L [22-28]
Urinary biochemistry:
sodium 30 mmol/L
potassium 42 mmol/L
chloride 13 mmol/L
The most likely explanation for these results is:
A. Bartter syndrome.
B. occult diuretic use.
C. occult laxative use.
D. primary hyperaldosteronism.
E. self-induced vomiting.
QUESTION 66
An 18-month-old child presents after swallowing a 20-cent piece.
At which of the following anatomicalsites is the foreign body most
likely to become impacted?
A. Duodeno-jejunal junction.
B. Gastro-oesophageal junction.
C. Ileocaecal valve.
D. Oesophagus at level of cricoid.
E. Pylorus.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
37/59
37 P204
QUESTION 67
A four-year-old boy presents with worsening back pain, which is
more severe at night. The pain firststarted about three weeks
previously after a minor upper respiratory infection and was
initiallyintermittent. There has not been any recent history of
fever. He had previously been well, with nosignificant infections
other than otitis media.
Examination reveals tenderness over the lumbar spine at L2/3,
limited straight leg raising and a loss ofthe normal lumbar
lordosis. His erythrocyte sedimentation rate (ESR) is 60 mm/hr and
his C-reactiveprotein is 4 mg/L [
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
38/59
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
39/59
39 P204
QUESTION 69
The most common adverse effect of methylphenidate is:
A. appetite suppression.
B. headache.
C. sleep difficulty.
D. tics.
E. withdrawn behaviour.
QUESTION 70
The parents of a two-year-old boy seek advice about their past
reproductive and family history. Theyhave recently immigrated from
Vietnam. The pedigree is as shown below. There have been four
miscarriages, all between six and eight weeks of gestation.
Their first child (III:4) was born withmultiple congenital
anomalies and had severe developmental delay. He died aged two
years, ofunspecified causes. No other information is available
about him. The only other family history of noteis that the
deceased childs uncle (II:1) also had developmental delay and died
in childhood. Thesurviving child (III:6) is normal.
Which of the following investigations is most likely to prove
useful for counselling about futurechildren?
A. Haemoglobin electrophoresis of both parents.
B. Karyotypes of both parents.
C. Maternal fragile X triplet repeats.
D. Maternal lupus serology.
E. Maternal plasma very long chain fatty acids.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
40/59
40 P204
QUESTION 71
A six-month-old girl presents with a short history of fever
(38C) and exacerbation of her facialeczema, as shown in the
photograph above. She has a strong family history of asthma.
Initial treatment with oral flucloxacillin and topical 1%
hydrocortisone ointment shows no improvement.
Which of the following is most likely to improve her
condition?
A. Intravenous aciclovir.
B. Intravenous amoxycillin/clavulanic acid.
C. Intravenous flucloxacillin.
D. More potent topical steroids.
E. Wet saline dressings.
QUESTION 72Which of the following symptoms or signs would be
least likely in a child with Kawasaki disease?
A. Arthritis.
B. Erythema of buttocks.
C. Jaundice.
D. Purulent conjunctivitis.
E. Right hypochondrial tenderness.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
41/59
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
42/59
42 P204
QUESTION 74
Antenatal maternal smoking is least associated with which one of
the following effects in children?
A. Decreased lung compliance.
B. Decreased maximal expiratory flow.
C. Increased risk of lower respiratory tract infections.
D. Increased risk of sudden infant death syndrome.
E. Increased risk of wheezing.
QUESTION 75
A 10-year-old girl with a longstanding history of migraine, on
no medications, presents with severeheadache and left upper limb
weakness.
Which of the following medications should not be used at this
point?
A. Codeine.
B. Cyproheptadine.
C. Dihydroergotamine.
D. Ibuprofen.
E. Propranolol.
QUESTION 76
A previously well six-year-old girl presents for assessment of
pubertal development. On examinationher height is above the 97th
percentile and her weight is on the 25th percentile. She has
Tannerstage 3 breast development. Pubic hair is Tanner stage 1. She
has no skin markings. Investigationshows her bone age is equivalent
to that of an eight-year two-month-old girl.
Which of the following is the most likely diagnosis?
A. Adrenal tumour.
B. Congenital adrenal hyperplasia.
C. Ovarian cyst.
D. Pituitary hamartoma.
E. Premature thelarche.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
43/59
43 P204
QUESTION 77
A five-year-old girl presents with a two-day history of fever to
38C axillary and a swollen, tender rightknee. She has previously
been well, and has had no rash and no previous episodes of joint
pain. Onexamination, she is febrile (37.9C) and flushed. She has a
heart rate of 100/minute with normal heartsounds. She has shotty
cervical lymphadenopathy, but no palpable liver or spleen. Her
right knee is
warm, swollen, red, and slightly tender. She has no effusion
clinically. She can straighten her leg andflex the right knee, but
there is pain at the extreme of knee flexion.
Her blood test results are as follows:
haemoglobin 112 g/L [110-140]
white cell count 10.8 x 109 /L [4.0-11.0]
differential:
neutrophils 3.5 x 109 /L [1.0-4.0]
lymphocytes 7.3 x 109 /L [3.0-8.0]
platelet count 170 x 109 /L [150-400]
erythrocyte sedimentation rate (ESR) 18 mm/hr [
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
44/59
44 P204
QUESTION 79
A one-week-old full term baby girl is noted to be tachypnoeic.
Her chest X-ray is shown below.
The most likely diagnosis is:
A. cardiac failure.
B. congenital cystic adenomatous malformation.
C. congenital lobar emphysema.
D. diaphragmatic hernia.
E. staphylococcal pneumonia.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
45/59
45 P204
QUESTION 80
A nine-year-old boy presents with a two-week history of cough,
tachypnoea, recession and increasing
cyanosis. The chest X-ray and a lung biopsy (stained with
methenamine silver nitrate) are shownabove.
The underlying immune deficiency is most likely to be primarily
affecting his:
A. B lymphocytes.
B. macrophages.
C. natural killer cells.
D. neutrophils.
E. T lymphocytes.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
46/59
46 P204
QUESTION 81
A newborn is receiving assist-control ventilation with the
following ventilator settings:
peak inspiratory pressure 17 cmH2O
positive end-expiratory pressure 4 cmH2O
back-up ventilator rate 20/minute
inspiratory time 0.5 seconds
The infants spontaneous breathing rate is 40/minute.
The number of breaths per minute which are assisted by the
ventilator is which one of the following?
A. 0.
B. 20.
C. 25.
D. 40.
E. 60.
QUESTION 82
A 13-year-old boy with focal segmental glomerulosclerosis
presents to hospital with a four-day historyof vomiting and
diarrhoea. He has not passed urine for at least 12 hours. Six weeks
before, he had aserum creatinine of 0.11 mmol/L. He has been on 40
mg frusemide daily and an angiotensin-converting enzyme (ACE)
inhibitor.
On examination, he is well-perfused, moderately oedematous, with
a pulse of 110/minute and bloodpressure of 90/60 mmHg. His
biochemistry on admission shows serum creatinine 0.50 mmol/L
[0.05-0.08] and sodium 130 mmol/L [135-145]. His serum albumin was
12 g/L [35-50].
Which of the following would be the most appropriate next step
in management?
A. Dialysis.
B. Fluid restriction.
C. Increase dose of frusemide.
D. Maintenance intravenous fluids.
E. Volume replacement with concentrated albumin solution.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
47/59
47 P204
QUESTION 83
A six-year-old boy presents with a sore throat, high fever and
anorexia. The appearance of his mouthand tongue is shown below.
The most likely organism responsible for this picture is:
A. Candida albicans.
B. Coxsackievirus A16.
C. Epstein-Barr virus.
D. Fusobacterium necrophorum.
E. herpes simplex virus.
QUESTION 84
A previously settled breastfed infant of four weeks demonstrates
increasing crying behaviour over aweek. The infant continues to
feed well, though fussily, and continues to gain weight. The
babyeffortlessly vomits small amounts of milk four or five times a
day. Faeces are watery, yellow and
occasionally explosive. The perianal skin is normal.
The change of behaviour is most likely to be associated
with:
A. change in the mothers diet.
B. gastro-oesophageal reflux.
C. lactose intolerance.
D. normal variation in infant behaviour.
E. urinary tract infection.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
48/59
48 P204
QUESTION 85
A six-year-old girl presents with a six-month history of staring
spells associated with eye flickering andlip smacking movements. An
electroencephalogram (EEG) is performed and is shown below.
Which of the following anticonvulsants is most appropriate?
A. Carbamazepine.
B. Clonazepam.
C. Phenytoin.
D. Sodium valproate.
E. Vigabatrin.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
49/59
49 P204
QUESTION 86
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
50/59
50 P204
QUESTION 86 (continued)
A nine-year-old boy presents to the emergency department with
chest pain. He had cardiac surgery ininfancy, but the parents are
vague about the diagnosis. His electrocardiogram (ECG) is
shownopposite.
The most likely cardiac lesion was:
A. atrioventricular canal defect.
B. hypoplastic right ventricle.
C. perimembranous ventricular septal defect.
D. tetralogy of Fallot.
E. truncus arteriosus.
QUESTION 87
Which one of the following confers the greatest risk for the
development of fungal infection in a patientundergoing
chemotherapy?
A. Central venous lines.
B. Long-term antibiotics.
C. Prolonged neutropenia.
D. Use of monoclonal antibodies.
E. Use of steroids.
QUESTION 88
A 13-year-old girl presents with excessive bleeding following a
tooth extraction. She has a history ofheavy menstrual loss. The
following coagulation tests are obtained:
activated partial thromboplastin time (APTT) 40 seconds
[27.5-34.5]
50:50 mix with normal plasma 32 seconds
prothrombin time (PT) 14 seconds [14-18]
thrombin clotting time (TCT) 16 seconds [14-18]
Which one of the following is the most likely diagnosis?
A. Dysfibrinogenaemia.
B. Factor XII deficiency.
C. Haemophilia A.
D. Lupus anticoagulant.
E. von Willebrand disease.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
51/59
51 P204
QUESTION 89
A 12-year-old boy with longstanding asthma presents with a
six-week history of increased cough anddyspnoea. The cough comes on
suddenly in the day, but not usually at night. It lasts for a
minute ortwo, during which time he finds it hard to get his breath.
Usually his asthma is well controlled onregular betamethasone by
inhaler two puffs twice daily, and he rarely needs to use his
salbutamol
puffer. For the last month, however, he has often had to stop
when playing soccer because of a boutof prolonged coughing.
The following results are obtained:
haemoglobin 112 g/L [110-140]
white cell count 18.6 x 109 /L [4.0-11.0]
neutrophils 2.5 x 109 /L [1.0-4.0]
lymphocytes 14.1 x 109 /L [3.0-7.0]
eosinophils 1.1 x 109 /L [
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
52/59
52 P204
QUESTION 91
A three-year-old boy presents with a 10-day history of cough and
fever unresponsive to oralantibiotics. His chest X-ray is shown
above.
Which of the following best explains the appearance shown on the
X-ray?
A. Left-sided consolidation and pleural effusion.
B. Left-sided pulmonary abscess.
C. Obstruction of right main bronchus.
D. Right-sided pneumothorax.
E. Unilateral left-sided pulmonary oedema.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
53/59
53 P204
QUESTION 92
A four-year-old girl is noted by her parents to have a funny
looking eye (pictured). She has notcomplained of anything herself
but seems to be bumping into things more often recently.
On examination, the only other finding is a swollen right knee.
There is a history of back problems onher fathers side of the
family. Her maternal grandmother has rheumatoid arthritis.
Which of the following tests is most likely to be diagnostically
useful?
A. Anti-double stranded DNA antibody (anti-dsDNA).
B. Antinuclear antibody (ANA).
C. Antineutrophil cytoplasmic antibody (ANCA).
D. HLA-B27.
E. Rheumatoid factor.
QUESTION 93
A child presents with a sore throat. Which of the following
clinical features is least likely in Group Astreptococcal
tonsillitis?
A. Age 10 years.
B. Cough.
C. Exudate.
D. Fever >39C.
E. Tender enlarged cervical lymph nodes.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
54/59
54 P204
QUESTION 94
A three-month-old boy is referred to clinic because an antenatal
ultrasound showed a dilated left renalpelvis. This is confirmed by
postnatal ultrasound. His left renal pelvic diameter is 25 mm [
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
55/59
55 P204
QUESTION 95
A four-week-old girl presents with prolonged neonatal jaundice
and poor weight gain. On examination,a small and firm liver is
found and the spleen is palpable 2 cm below the left costal margin.
She alsohas a harsh 3/6 systolic murmur radiating widely.
The following liver function tests were obtained:
total bilirubin 85 mol/L [0-15]
conjugated bilirubin 65 mol/L [0-5]
alanine aminotransferase (ALT) 45 U/L [
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
56/59
56 P204
QUESTION 97
A five-month-old boy presents with chronic diarrhoea, failure to
thrive and recent onset coughassociated with feeding intolerance.
Blood test results show:
haemoglobin 98 g/L [110-150]
white cell count 14 x 109 /L [4-11]differential:
neutrophils 11 x 109 /L [1-7]
lymphocytes 3 x 109 /L [1-4]
platelet count 90 x 109 /L [150-400]
IgG 9.0 g/L [3.3-6.4]
IgA 0.67 g/L [0.30-0.70]
IgM 1.90 g/L [0.25-0.60]
A chest X-ray was taken and is shown below.
Which one of the following is the most likely cause of this
clinical presentation?
A. Human immunodeficiency virus (HIV) infection.
B. Hyper IgM syndrome.
C. Severe combined immunodeficiency.
D. Wiskott-Aldrich syndrome.
E. X-linked agammaglobulinaemia.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
57/59
57 P204
QUESTION 98
A 10-year-old boy presents with a six-month history of lethargy
and weight gain. History reveals thathe has been on thyroxine in
the past and that his parents are first cousins. On examination he
has afirm moderately sized goitre. His thyroid function tests are
as follows:
free thyroxine (free T4) 9 pmol/L [10-20]thyroid-stimulating
hormone (TSH) 37.00 mU/L [0.03-4.00]
Thyroid technetium pertechnetate scan is demonstrated below and
shows increased uptake.
Which one of the following is the most likely diagnosis?
A. Autoimmune hypothyroidism.
B. Dyshormonogenesis.
C. Graves disease.
D. Iodine excess.
E. Thyroid dysgenesis.
QUESTION 99
It is considered inappropriate to perform predictive genetic
testing on young children for Huntingtondisease, an adult-onset
neurodegenerative disorder. Which of the following is the most
importantreason for this?
A. Positive status for a Huntington disease mutation would block
the childs future access to life,mortgage and income protection
insurance.
B. Such testing is a violation of the childs autonomy, in that
they lose the freedom to choosewhether to have the test later in
life.
C. The main reason for testing adults for Huntington disease is
to allow mutation carriers theoption of prenatal diagnosis, an
issue which is irrelevant in childhood.
D. There is no currently available treatment for Huntington
disease.
E. The testing process would place excessive psychological
stress on a child, as children lackthe emotional maturity to cope
with such testing.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
58/59
58 P204
QUESTION 100
A multigravida is induced by artificial rupture of the membranes
and syntocinon infusion at 41 weeksgestation. After 16 hours of
labour she is noted to be fully dilated. Ninety minutes later,
after fourunsuccessful attempts at delivery by vacuum extraction,
she is taken to the operating theatre for anemergency Caesarean
section. At delivery a 3800 g male infant is in poor condition
requiring full
resuscitation. He is transferred, intubated and ventilated, to
an intensive care unit. At 12 hours of agehe deteriorates with
pallor and poor perfusion. His haemoglobin is 95 g/L and mean
arterial bloodpressure is 30 mmHg. Extensive bruising is noted over
his head. His head circumference is 38 cm.His pupils are unable to
be examined due to marked oedema of his upper eyelids.
The most likely cause for his deterioration is blood loss due
to:
A. cephalohaematoma.
B. intracerebral haemorrhage.
C. intraventricular haemorrhage.
D. subaponeurotic haemorrhage.
E. subdural haemorrhage.
Copyright 2005 by The Royal Australasian College of
Physicians
-
8/14/2019 2004 FRACP Written Examination Paediatrics &
Child
59/59
59 P204
2004 FRACP Written Examination
Paediatrics & Child Health
Paper 2 Clinical Applications
Answers
1. D 34. B 67. B
2. E 35. B 68. C
3. E 36. A 69. A
4. C 37. A 70. B
5. B 38. D 71. A
6. D 39. D 72. D
7. E 40. C 73. D
8. D 41. A 74. A
9. A 42. A 75. C
10. E 43. D 76. C
11. A 44. A 77. E
12. C 45. A 78. C
13. E 46. C 79. B
14. E 47. B 80. E
15. B 48. E 81. D
16. B 49. C 82. E
17. A 50. B 83. E
18. A 51. D 84. D
19. D 52. A 85. D
20. A 53. B 86. A
21. D 54. E 87. C
22. C 55. A 88. E
23. D 56. B 89. D
24. C 57. A 90. C
25. A 58. D 91. A26. C 59. E 92. B
27. B 60. A 93. B
28. C 61. B 94. D
29. B 62. E 95. A
30. D 63. E 96. E