-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
1/76
2012 Surviving Sepsis
Campaign Guidelines
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
2/76
AgendaUnderstand the scope of the sepsis epidemic1
Become familiar with the Surviving SepsisCampaign and the SCCM
defined sepsis
bundles2
Recognize how time-criticaltherapies can save lives inthe
emergency departments and ICUs
3
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
3/76
Comparable GlobalEpidemiology
95 cases per 100,000
2 week surveillance
206 French ICUs 95 cases per 100,000
3 month survey
23 Australian/New
Zealand ICUs
51 cases per 100,000
England, Wales andNorthern Ireland.
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
4/76
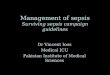
Severe Sepsis: Comparison With
Other Major Diseases
0
50
100
150
200
250
300
AIDS* Colon Breast
Cancer
CHF Severe
Sepsis
Cases/100,0
00
Incidence of Severe Sepsis Mortality of Severe Sepsis
0
50,000
100,000
150,000
200,000
250,000
AIDS* Severe
SepsisAMIBreast
Cancer
Deaths/Year
National Center for Health Statistics, 2001.
American Cancer Society, 2001. *American Heart Association.
2000.Angus DC
et al. Crit Care Med.2001
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
5/76
Sepsis Epidemiology: Effect of the Aging Population
0
5
10
15
20
25
30
35
40
45
0 1 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85
Without Comorbidity
With Comorbidity
Overal
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
6/76
Economics of Sepsis Severe Sepsis
$22,000 per case
US annual cost $16.7Billion
Nosocomial Sepsis
increased LOS - ICU 8 days, Hosp 24 days $40,890 per case
Angus CCM, 2001
Pittet JAMA, 1994
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
7/76
Time Sensitive Interventions
AMI
StrokeTime is Brain
The sooner that treatment begins, the better are ones
chances of survival without disability.
TraumaThe Golden Hour
Requires immediate response and medical care on the scene.
Patients typically transferred to a qualified trauma center for
care.
Door to PCI
Focus on the timely return of blood flow to the affected
areas of the heart.
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
8/76
Severe Sepsis vs. Current Care Priorities
Care PrioritiesU.S.
Incidence# of Deaths Mortality Rate
AMI (1) 900,000 225,000 25%
Stroke (2) 700,000 163,500 23%
Trauma (3)
(Motor Vehicle)
2.9 million(injuries)
42,643 1.5%
Severe Sepsis (4) 751,000 215,000 29%
Source: (1) Ryan TJ, et al. ACC/AHA Guidelines for management of
patients with AMI. JACC. 1996; 28: 1328-1428. (2) American
HeartAssociation. Heart Disease and Stroke Statistics2005 Update.
Available at: www.americanheart.org. (3) National Highway
TrafficSafety Administration. Traffic Safety Facts 2003: A
Compilation of Motor Vehicle Crash Data from the Fatality Analysis
Report ingSystem and the General Estimates System. Available at
http://www.nhtsa.dot.gov/. (4) Angus DC et al. Crit Care
Med2001;29(7): 1303-1310.
http://www.nhtsa.dot.gov/http://www.nhtsa.dot.gov/
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
9/76
Surviving Sepsis Campaign
Launched in Autumn 2002 as a collaborativeeffort of European
Society of Intensive Care
Medicine, the International Sepsis Forum, andthe Society of
Critical Care Medicine
Goal: reduce sepsis mortality by 25% in the next5 years
Guidelines revealed at SCCM in Feb 2004,REVISED 2008
Critical Care MedicineMarch 2004 32(3):858-87.
Website: survivingsepsis.org
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
10/76
What is sepsis?
Sepsis, Septic Shock,
SIRS (systemic inflammatory responsesyndrome),
SSI (signs and symptoms of infection),
Septicaemia, Bacteraemia,Toxic Shock Syndrome,
Bloodstream infection etc, etc.
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
11/76
Infection
Inflammatory response to
microorganisms, or
Invasion of normally steriletissues
Systemic Inflammatory
Response Syndrome (SIRS)
Systemic response to a
variety of processes
Sepsis
Infection plus
2 SIRS criteria
Severe Sepsis
Sepsis
Organ dysfunction
Septic shock Sepsis
Hypotension despite fluid
resuscitation
Bone RC et al. Chest.1992;101:1644-55.
ACCP/SCCM Consensus Def ini t ions
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
12/76
A systemic response to a nonspecific insult
Infection, trauma, surgery, massive transfusion, etc
Defined as 2 of the following:
Temperature >38.3 or 90 min-1
Respiratory rate >20 min-1
White cells 12
Acutely altered mental state
Hyperglycaemia (BM>7.7) in absence of DM
SIRSSEVERE SEPSIS
What is SIRS?
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
13/76
Pneumonia 50%
Urinary Tract infection
Meningitis
Endocarditis
Device related
Central line
Cannula
Abdominal 25%Pain
DiarrhoeaDistension
Urgent laparotomy
Soft tissue/ musculoskeletal
Cellulitis
Septic arthritisFasciitis
Wound infection
What counts as an infection?
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
14/76
SIRS due to an infection
what is Sepsis?
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
15/76
Sepsis with organ dysfunction, hypoperfusion or hypotension
CNS: Acutely altered mental status
CVS: Syst < 90 or mean < 65 mmHg
Resp: SpO2>90% only with new/ more O2
Renal: Creatinine >177 mol/l
or UO 34 mol/l
Bone marrow: Platelets 2 mmol/l
Coagulopathy: INR>1.5 or aPTT>60secs
What is Severe Sepsis?
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
16/76
Tissue perfusion is not adequate for the
tissuesmetabolic requirements
What is shock?
Septic Shock
Shock secondary to systemic
inflammatory response to a
new infection
Types of Shock
Cardiogenic
Neurogenic
Hypovolaemic
Anaphylacticand
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
17/76
Tissue perfusion is not adequate for the
tissuesmetabolic requirements
For sepsis, shock is one of:
SBP < 90 mmHg
MBP < 65 mmHg after IV
fluidsDrop of < 40 mmHg
Lactate > 4 mmol/l
What is shock?
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
18/76
The Sepsis Continuum
A clinical responsearising from anonspecific insult, with2 of
the following:
T >38oC or 90 beats/min
RR >20/min
WBC >12,000/mm3or 10% bands
SIRS = systemic inflammatoryresponse syndrome
SIRS with a
presumed
or confirmed
infectiousprocess
Chest 1992;101:1644.
SepsisSIRSSevereSepsis
Septic
Shock
Sepsis with
organ failure
Refractory
hypotension
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
19/76
Are any 2of the following SIRS criteria present and new to your
patient?
Obs: Temperature >38.3 or 20 min-1
Heart rate >90 bpm Acutely altered mental state
Bloods: White cells 12x109/l Glucose>7.7mmol/l
(if patient is not diabetic)
If yes,
patient has SIRS
Severe Sepsis Screen ing Too l
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
20/76
Is this likely to be due to an infection?For example
Cough/ sputum/ chest pain Dysuria
Abdo pain/ diarrhoea/ distension Headache with neck
stiffness
Line infection Cellulitis/wound infection/septic arthritis
Endocarditis
If yes,
patient has SEPSIS
Start SEPSIS BUNDLE
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
21/76
Severe Sepsis: Ensure Senior Doctor/ITU to
attend NOW!
Check for SEVERE SEPSIS
BP Syst < 90 / Mean < 65 mmHg
(after initial fluid challenge)
Lactate > 4 mmol/l
Urine output < 0.5 ml/kg/hr for 2 hrs
INR > 1.5
aPTT > 60 s
Bilirubin > 34 mol/l
O2 Needed to keep SpO2 > 90%
Platelets < 100 x 109/l
Creatinine > 177 mol/l or UO < 0.5 ml/kg/hr
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
22/76
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
23/76
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
24/76
What is a Bundle?
Specifically selectedcare elements
From evidence basedguidelines
Implemented togetherprovide improved
outcomes compared toindividual elementsalone
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
25/76
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
26/76
Initial Resuscitation
Protocolized, quantitative resuscitation of
patients with sepsis- induced tissue
hypoperfusion (defined in this document as
hypotension persisting after initial fluidchallenge or blood
lactate concentration 4
mmol/L).
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
27/76
Initial Resuscitation
Goals during the first 6 hrs of resuscitation:
Central venous pressure812 mm Hg
Mean arterial pressure(MAP) 65 mm Hg
Urine output 0.5 mL/kg/hr
Central venous (superior vena cava) or mixed venous
oxygen saturation 70% or 65%, respectively (grade 1C).
In patients with elevated lactate levels targetingresuscitation
to normalize lactate (grade 2C).
Screening for Sepsis and
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
28/76
Screening for Sepsis and
Performance Improvement
Routine screening of potentially infected
seriously ill patients for severe sepsis to
allow earlier implementation of therapy
(grade 1C).
Hospitalbased performance improvement
efforts in severe sepsis (UG).
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
29/76
Diagnosis
Culturesas clinically appropriate before
antimicrobial therapyif no significant delay
(> 45 mins) in the start of antimicrobial(s)
(grade 1C).
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
30/76
Diagnosis
At least 2 sets of blood cultures (both aerobic
and anaerobic bottles) be obtained before
antimicrobial therapy with at least 1 drawn
percutaneouslyand 1 drawn through eachvascular access device,
unless the device was
recently (
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
31/76
Diagnosis
Use of the 1,3 beta-D-glucan assay (grade 2B),
mannan and anti-mannan antibody assays (2C), if
available and invasive candidiasis is in differential
diagnosis of cause of infection.
Imaging studies performed promptly to confirm a
potential source of infection (UG).
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
32/76
Antimicrobial Therapy
Administration of effective intravenous antimicrobials within
the firsthour of recognition of septic shock (grade 1B) and severe
sepsiswithout septic shock (grade 1C) as the goal of therapy.
Initial empiric anti-infective therapy of one or more drugs that
haveactivity against all likely pathogens (bacterial and/or fungal
or viral) andthat penetrate in adequate concentrations into tissues
presumed to bethe source of sepsis (grade 1B).
Antimicrobial regimen should be reassessed daily for
potentialdeescalation(grade 1B).
Use of low procalcitonin levels or similar biomarkers to assist
theclinician in the discontinuation of empiric antibiotics in
patients whoinitially appeared septic, but have no subsequent
evidence of infection(grade 2C).
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
33/76
Antimicrobial Therapy
Combination empirical therapy for neutropenicpatients with
severe sepsis (grade 2B) and forpatients with difficult-to-treat,
multidrug resistantbacterial pathogens such as Acinetobacterand
Pseudomonas spp. (grade 2B).
For patients with severe infections associated withrespiratory
failure and septic shock, combination
therapy with an extended spectrum beta-lactam andeither an
aminoglycoside or a fluoroquinolone is forP. aeruginosa bacteremia
(grade 2B).
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
34/76
Antimicrobial Therapy
A combination of beta-lactam and macrolide forpatients with
septic shock from bacteremicStreptococcus pneumoniae infections
(grade 2B).
Empiric combination therapy should not beadministered for more
than 35 days.
De-escalation to the most appropriate singletherapyshould be
performed as soon as thesusceptibility profile is known (grade
2B).
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
35/76
Antimicrobial Therapy
Duration of therapy typically 710 days; longer courses may
be appropriate in patients who have a slow clinical
response,
undrainable foci of infection, bacteremia with S. aureus;
some fungal and viral infections or immunologic
deficiencies, including neutropenia (grade 2C).
Antiviral therapy initiated as early as possible in patients
with
severe sepsis or septic shock of viral origin (grade 2C).
Antimicrobial agents should not be used in patients with
severe inflammatory states determined to be of
noninfectious cause(UG).
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
36/76
Source Control
A specific anatomical diagnosis of infection requiring
consideration for emergent source control be sought and
diagnosed or excluded as rapidly as possible, and
intervention be undertaken for source control within
the first 12 hr after the diagnosis is made, if feasible(grade
1C).
When infected peripancreatic necrosis is identified as a
potential source of infection, definitive intervention isbest
delayed until adequate demarcation of viable and
nonviable tissues has occurred (grade 2B).
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
37/76
Source Control
When source control in a severely septic patient is
required, the effective intervention associated with the
least physiologic insult should be used (eg,
percutaneous rather than surgical drainage of an
abscess) (UG).
If i.v access devices are a possible source of severe
sepsis or septic shock, they should be removed promptly
after other vascular access has been established (UG).
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
38/76
Infection Prevention
Selective oral decontamination and selectivedigestive
decontamination should beintroduced and investigated as a method
toreduce the incidence of ventilator-associatedpneumonia;
This infection control measure can then beinstituted in health
care settings and regions
where this methodology is found to be effective(grade 2B).
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
39/76
Infection Prevention
Oral chlorhexidine gluconate be used as a form of
oropharyngeal decontamination to reduce the risk of
ventilator-associated pneumonia in ICU patients with
severe sepsis (grade 2B).
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
40/76
Fluids
Why?
To reduce organ dysfunction and
multi-organ failure
By optimising tissue oxygen delivery
By increasing organ perfusion
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
41/76
DO2 = Oxygen delivery to the tissue
CaO2= Amount of O2 in arterial blood
Fluid therapy improves cardiac output by increasing
venous return to the heart
CaO2= ([Hb] x SaO2x 1.34) + (PaO2x 0.0225)
DO2= CaO2x CO
Optimising oxygen delivery
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
42/76
Fluid Therapy of Severe Sepsis
Crystalloidsas the initial fluid of choice inthe resuscitation
of severe sepsis and septicshock (grade 1B).
Against the use of HESfor fluid resuscitationof severe sepsis
and septic shock (grade 1B).
Albuminin the fluid resuscitation of severesepsis and septic
shock when patients requiresubstantial amounts of crystalloids
(grade 2C).
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
43/76
Fluid Therapy of Severe Sepsis
Initial fluid challenge in patients with sepsis-induced
tissuehypoperfusion with suspicion of hypovolemia to achieve
aminimum of 30 mL/kg of crystalloids(a portion of this may
bealbumin equivalent).
More rapid administration and greater amounts of fluid may
beneeded in some patients (grade 1C).
Fluid challenge technique be applied wherein fluid
administration is continued as long as there is
hemodynamicimprovement either based on dynamic(eg, change in
pulsepressure, stroke volume variation) or static(eg,
arterialpressure, heart rate) variables (UG).
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
44/76
Vasopressors
Vasopressor therapy initially to target a meanarterial pressure
(MAP) of 65 mm Hg (grade 1C).
Norepinephrineas the first choice vasopressor(grade 1B).
Epinephrine(added to and potentiallysubstituted for
norepinephrine) when anadditional agent is needed to maintain
adequateblood pressure (grade 2B).
Vasopressin0.03 units/minute can be added tonorepinephrine (NE)
with intent of either raisingMAP or decreasing NE dosage (UG).
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
45/76
Vasopressors
Low dose vasopressin is not recommended as single initial
vasopressor for treatment of sepsis-induced hypotension
.vasopressin doses higher than 0.030.04 units/minute
should be reserved for salvage therapy (failure to achieve
adequate MAP with other vasopressor agents) (UG).
Dopamineas an alternative vasopressor agent to
norepinephrine only in highly selected patients (eg,
patients
with low risk of tachyarrhythmias and absolute or
relativebradycardia) (grade 2C).
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
46/76
Vasopressors
Phenylephrineis not recommended in thetreatment of septic shock
exceptin circumstanceswhere
(a) NEis associated with serious arrhythmias,(b) cardiac output
is known to be highand bloodpressure persistently low or
(c) as salvage therapy when combined
inotrope/vasopressor drugs and low dosevasopressin have failed
to achieve MAP target(grade 1C).
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
47/76
Vasopressors
Low-dose dopamine should not be used for
renal protection(grade 1A).
All patients requiring vasopressors have an
arterial catheterplaced as soon as practical if
resources are available (UG).
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
48/76
Inotropic Therapy
A trial of dobutamine infusion up to 20mcg/kg/min be
administered or added tovasopressor (if in use) in the presence
of:-
(a) myocardial dysfunction as suggested byelevated cardiac
filling pressures and lowcardiac output,
(b) ongoing signs of hypoperfusion, despiteachieving adequate
intravascular volume andadequate MAP (grade 1C).
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
49/76
Inotropic Therapy
Not using a strategy to increase cardiac index to
predetermined supranormal levels (grade 1B).
C i id
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
50/76
Corticosteroids
Not using intravenous hydrocortisone to treatadult septic shock
patients if adequate fluidresuscitationand vasopressortherapy are
able torestore hemodynamic stability.
In case this is not achievable, i.v hydrocortisonealone at a
dose of 200 mg per day (grade 2C).
Not using the ACTH stimulation test to identifyadults with
septic shock who should receivehydrocortisone (grade 2B).
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
51/76
Corticosteroids
In treated patients hydrocortisone taperedwhen
vasopressors are no longer required (grade 2D).
Corticosteroids not be administered for the treatment of
sepsis in the absence of shock (grade 1D).
When hydrocortisone is given, use continuous flow
(grade 2D).
l d d d i i i
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
52/76
Blood Product Administration
Once tissue hypoperfusion has resolved and in
the absence myocardial ischemia, severe
hypoxemia, acute hemorrhage, or IHD
guideline recommends red blood cell
transfusion occur only when Hb concentration
decreases to
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
53/76
Blood Product Administration
Not using erythropoietin as a specific treatment of
anemiaassociated with severe sepsis (grade 1B).
Fresh frozen plasma not be usedto correct laboratoryclotting
abnormalities in the absence of bleeding or plannedinvasive
procedures (grade 2D).
Not using antithrombin for the treatment of severe sepsisand
septic shock (grade 1B).
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
54/76
Blood Product Administration
In patients with severe sepsis, administer platelets
prophylactically when counts are 50,000/mm3 [50 x 109/L]) are
advised
for active bleeding, surgery, or invasive procedures (grade
2D).
I l b li
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
55/76
Immunoglobulins
Not using intravenous immunoglobulins
in adult patients with severe sepsis or septic
shock (grade 2B).
S l i
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
56/76
Selenium
Not using intravenous selenium for the
treatment of severe sepsis (grade 2C).
History of Recommendations Regarding Use of
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
57/76
y g g
Recombinant Activated Protein C (rhAPC)
A history of the evolution of SSC
recommendations as to rhAPC (no longer
available) is provided.
Mechanical Ventilation of Sepsis-Induced Acute
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
58/76
p
Respiratory Distress Syndrome (ARDS)
Target a tidal volume of 6 mL/kg predicted body weight in
patientswith sepsis-induced ARDS (grade 1A vs. 12 mL/kg).
Plateau pressures be measured in patients with ARDS and
initial
upper limit goal for plateau pressures in a passively inflated
lung be
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
59/76
Mechanical Ventilation of Sepsis-Induced Acute
Respiratory Distress Syndrome (ARDS)
Recruitment maneuvers be used in sepsis patientswith severe
refractory hypoxemia (grade 2C).
Prone positioning be used in sepsis-induced ARDSpatients with a
P:F ratio < 100 mm Hg in facilities that
have experience with such practices (grade 2B). That
mechanically ventilated sepsis patients be
maintained with the head of the bed elevated to 3045 degreesto
limit aspiration risk and to prevent the
development of ventilator-associated pneumonia(grade 1B).
M h i l V il i f S i I d d A
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
60/76
Mechanical Ventilation of Sepsis-Induced Acute
Respiratory Distress Syndrome (ARDS)
Noninvasive mask ventilation (NIV) be used in
that minority of sepsis-induced ARDS patients in
whom the benefits of NIV have been carefullyconsidered and are
thought to outweigh the
risks (grade 2B).
M h i l V til ti f S i I d d A t
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
61/76
Mechanical Ventilation of Sepsis-Induced Acute
Respiratory Distress Syndrome (ARDS)
A weaning protocol be in place and that mechanically
ventilatedpatients with severe sepsis undergo spontaneous breathing
trialsregularly to evaluate the ability to discontinue mechanical
ventilationwhen they satisfy the following criteria:
a) arousable; b) hemodynamically stable (without vasopressor
agents);
c) no new potentially serious conditions;
d) low ventilatory and end-expiratory pressure requirements;
e) low Fio2 requirements which can be met safely delivered with
a
face mask or nasal cannula.
If the spontaneous breathing trial is successful, consideration
shouldbe given for extubation (grade 1A).
M h i l V til ti f S i I d d A t
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
62/76
Mechanical Ventilation of Sepsis-Induced Acute
Respiratory Distress Syndrome (ARDS)
Againstthe routine use of the pulmonary arterycatheter for
patients with sepsis-induced ARDS(grade 1A).
A conservative rather than liberal fluid strategyfor patients
with established sepsis-induced ARDSwho do not have evidence of
tissuehypoperfusion (grade 1C).
In the absence of specific indications such asbronchospasm, not
using beta 2-agonistsfortreatment of sepsis-induced ARDS (grade
1B).
Sedation, Analgesia, and
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
63/76
, g ,Neuromuscular Blockade in Sepsis
Continuous or intermittent sedation beminimizedin mechanically
ventilated sepsispatients, targeting specific titration
endpoints
(grade 1B). Neuromuscular blocking agents (NMBAs) be
avoided if possible in the septic patientwithout ARDS due to the
risk of prolonged
neuromuscular blockade followingdiscontinuation.
Sedation Analgesia and
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
64/76
Sedation, Analgesia, and
Neuromuscular Blockade in Sepsis
If NMBAs must be maintained, eitherintermittent bolus as
required or continuousinfusion with train-of-four monitoring of
the
depth of blockade should be used (grade 1C).
A short course of NMBA of not greater than48 hours for patients
with early sepsis-induced ARDS and a Pao2/Fio2 < 150 mm Hg(grade
2C).
Glucose Control
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
65/76
Glucose Control
A protocolized approach to blood glucosemanagement in ICU
patients with severesepsis commencing insulin dosing when 2
consecutive blood glucose levels are >180mg/dL.
This protocolized approach should target anupper blood glucose
180 mg/dL rather than
an upper target blood glucose 110 mg/dL(grade 1A).
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
66/76
Glucose Control
Blood glucose values be monitored every 12hrs until glucose
values and insulin infusionrates are stable and then every 4
hrs
thereafter (grade 1C). Glucose levels obtained with
point-of-care
testing of capillary blood be interpreted withcaution, as such
measurements may not
accurately estimate arterial blood or plasmaglucose values
(UG).
Renal Replacement Therapy
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
67/76
Renal Replacement Therapy
Continuous renal replacement therapies and
intermittent hemodialysis are equivalent in
patients with severe sepsis and acute renal
failure (grade 2B). Use continuous therapiesto facilitate
management of fluid balance in
hemodynamically unstable septic patients(grade 2D).
Bicarbonate Therapy
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
68/76
Bicarbonate Therapy
Not using sodium bicarbonate therapy for
the purpose of improving hemodynamics or
reducing vasopressor requirements in
patients with hypoperfusion-induced lacticacidemia with pH 7.15
(grade 2B).
Deep Vein Thrombosis Prophylaxis
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
69/76
Deep Vein Thrombosis Prophylaxis
Patients with severe sepsis receive dailypharmacoprophylaxis
against venous thromboembolism(VTE) (grade 1B).
This should be accomplished with daily subcutaneous
low-molecular weight heparin (LMWH) (grade 1B versus twicedaily
UFH, grade 2C versus three times daily UFH).
If creatinine clearance is
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
70/76
Deep Vein Thrombosis Prophylaxis
Septic patients who have a contraindication forheparin use(eg,
thrombocytopenia, severecoagulopathy, active bleeding, recent
intracerebralhemorrhage) not receive pharmacoprophylaxis
(grade 1B), but receive mechanical prophylactictreatment, such
as graduated compression stockingsor intermittent compression
devices (grade 2C),unless contraindicated.
When the risk decreases start pharmacoprophylaxis(grade 2C).
Stress Ulcer Prophylaxis
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
71/76
Stress Ulcer Prophylaxis
Stress ulcer prophylaxis using H2 blocker or
proton pump inhibitor be given to patients
with severe sepsis/septic shock who have
bleeding risk factors (grade 1B). When stress ulcer prophylaxis
is used, proton
pump inhibitors rather than H2RA(grade 2D)
Patients without risk factors do not receiveprophylaxis (grade
2B).
Nutrition
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
72/76
Nutrition
Administer oral or enteral (if necessary)feedings, as tolerated,
rather than eithercomplete fasting or provision of onlyintravenous
glucose within the first 48 hours
after a diagnosis of severe sepsis/septic shock(grade 2C).
Avoid mandatory full caloric feeding in the first
weekbut rather suggest low dose feeding (eg, upto 500 calories
per day), advancing only astolerated (grade 2B).
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
73/76
Nutrition
Use intravenous glucose and enteral nutritionrather than total
parenteral nutrition (TPN)alone or parenteral nutrition in
conjunction withenteral feeding in the first 7 days after a
diagnosis
of severe sepsis/septic shock (grade 2B).
Use nutrition with no specificimmunomodulating
supplementationrather
than nutrition providing specificimmunomodulating
supplementation in patientswith severe sepsis (grade 2C).
Setting Goals of Care
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
74/76
Setting Goals of Care
Discuss goals of care and prognosis withpatients and
families(grade 1B).
Incorporate goals of care into treatment and
end-of-life care planning, utilizing palliativecare principles
where appropriate (grade 1B).
Address goals of care as early as feasible, but
no later than within 72 hours of ICU admission(grade 2C).
ED Critical Care Bringing Upstairs
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
75/76
ED Critical Care Bringing Upstairs
Care, Downstairs
-
7/26/2019 2012 Surviving Sepsis Campaign Guidelines SYED
76/76
THANk YoU