Embed Size (px)
Citation preview
2018 OPEN ENROLLMENT
BENEFITS PACKET
Open Enrollment Notice
Medical Benefit Comparison
American Worker Enrollment Form
United Healthcare Enrollment Form
Required Notices
2018 OPEN ENROLLMENT We will be holding our 2018 Open Enrollment
December 6 – December 20, 2017
Partners Personnel/Butler America offers eligible, full time employees a comprehensive benefits package. You will have the option to enroll in the following plans: Major Medical – United Healthcare Medical - MEC & Fixed Indemnity – American Worker
Vision & Dental Plans - United Healthcare
See enclosed 2018 Benefit Summary to compare options and employee cost.
401(k) Retirement Plan: The 401k plan is available for enrollment after 90 days of regular employment. Eligible
employees can enroll in the 401k plan and/or change contributions at any time throughout the year and are not limited to the Open Enrollment period. Please contact [email protected] for more information.
IMPORTANT
If you are currently enrolled in company medical, dental or vision benefits, YOU WILL AUTOMATICALLY BE ENROLLED IN THE NEW CORRESPONDING BENEFITS AS OF JANUARY 1, 2018, unless changes are made during this open enrollment. We strongly encourage you to review 2018 benefits to be informed of all plan and rate changes. Please contact [email protected] or call 315-870-4861
IMPORTANT AFFORDABLE CARE ACT (ACA) INFORMATION Partners Personnel/Butler America offers an affordable, minimum value plan option in compliance with the ACA Employer Mandate. Please be advised that because the offer of coverage meets the required minimums, eligible full-time employees do not qualify for premium assistance through the federal or state Marketplace/Health Benefit Exchanges.
To enroll in the United Health Care Plans, including Dental and Vision and view additional detailed information as well as required notices:
Go to www.uhc.com/enroll
Create your account by entering your email address and choosing a password.
Enter the requested information and follow the prompts to complete your profile set up.
Elect your benefit options and continue to complete the enrollment process.
If you need additional assistance, you can contact United Healthcare by calling 1-866-633-2446. Review costs and plan details prior to enrolling including the enclosed Minimum Value Plan,
Affordable Care Act Compliant rate chart for Bronze Medical Coverage.
To enroll in the American Worker Plan which includes MEC and Fixed Indemnity Options, please complete the attached enrollment form (choose from MEC or Fixed Indemnity) and submit using one of the following methods:
1. Submit the form to your local branch 2. Email the form to [email protected] 3. Fax the form to 717-706-3872
**Paper enrollment forms for United HealthCare benefit options and hard copy benefit packets containing all required notices are available by visiting your local branch and/or contacting the benefit department at [email protected]. They can assist in this process as well as answer any questions you may have. The America Worker Enrollment form is enclosed here for your convenience.
Decisions It is important to consider your decisions carefully. The benefits you select now will remain in effect throughout the 2018 plan year. If you do not make any changes to your current enrollments or waive coverage, you will be unable to enroll until the next Open Enrollment period, except in the case of a qualifying life event. If you do experience a life event, changes must be made within 31 days of the event and must be consistent with the event.
Questions? If you have any questions regarding the plans, your eligibility or enrollment email: [email protected].
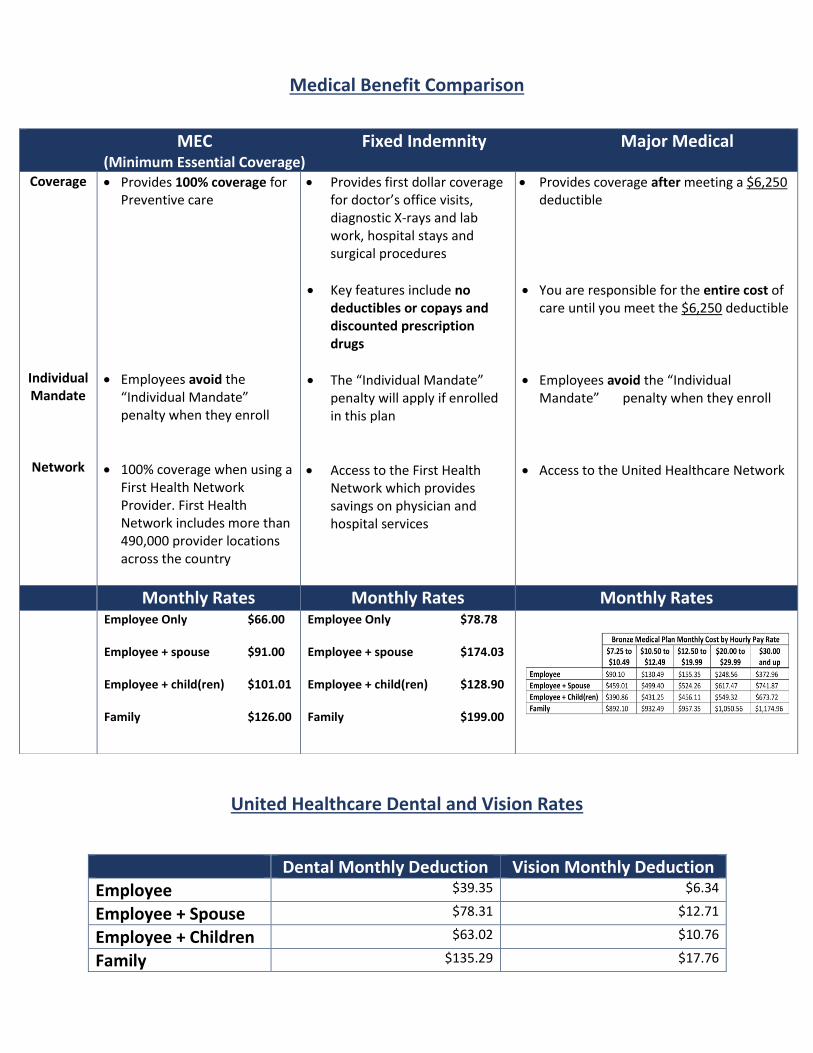
Medical Benefit Comparison
United Healthcare Dental and Vision Rates
Dental Monthly Deduction Vision Monthly Deduction Employee $39.35 $6.34
Employee + Spouse $78.31 $12.71
Employee + Children $63.02 $10.76
Family $135.29 $17.76
MEC Fixed Indemnity Major Medical (Minimum Essential Coverage) Coverage
Individual Mandate
Network
• Provides 100% coverage for Preventive care
• Employees avoid the “Individual Mandate” penalty when they enroll
• 100% coverage when using a First Health Network Provider. First Health Network includes more than 490,000 provider locations across the country
• Provides first dollar coverage for doctor’s office visits, diagnostic X-rays and lab work, hospital stays and surgical procedures
• Key features include no deductibles or copays and discounted prescription drugs
• The “Individual Mandate” penalty will apply if enrolled in this plan
• Access to the First Health Network which provides savings on physician and hospital services
• Provides coverage after meeting a $6,250 deductible
• You are responsible for the entire cost of care until you meet the $6,250 deductible
• Employees avoid the “Individual Mandate” penalty when they enroll
• Access to the United Healthcare Network
Monthly Rates Monthly Rates Monthly Rates
Employee Only $66.00 Employee + spouse $91.00
Employee + child(ren) $101.01 Family $126.00
Employee Only $78.78
Employee + spouse $174.03
Employee + child(ren) $128.90
Family $199.00
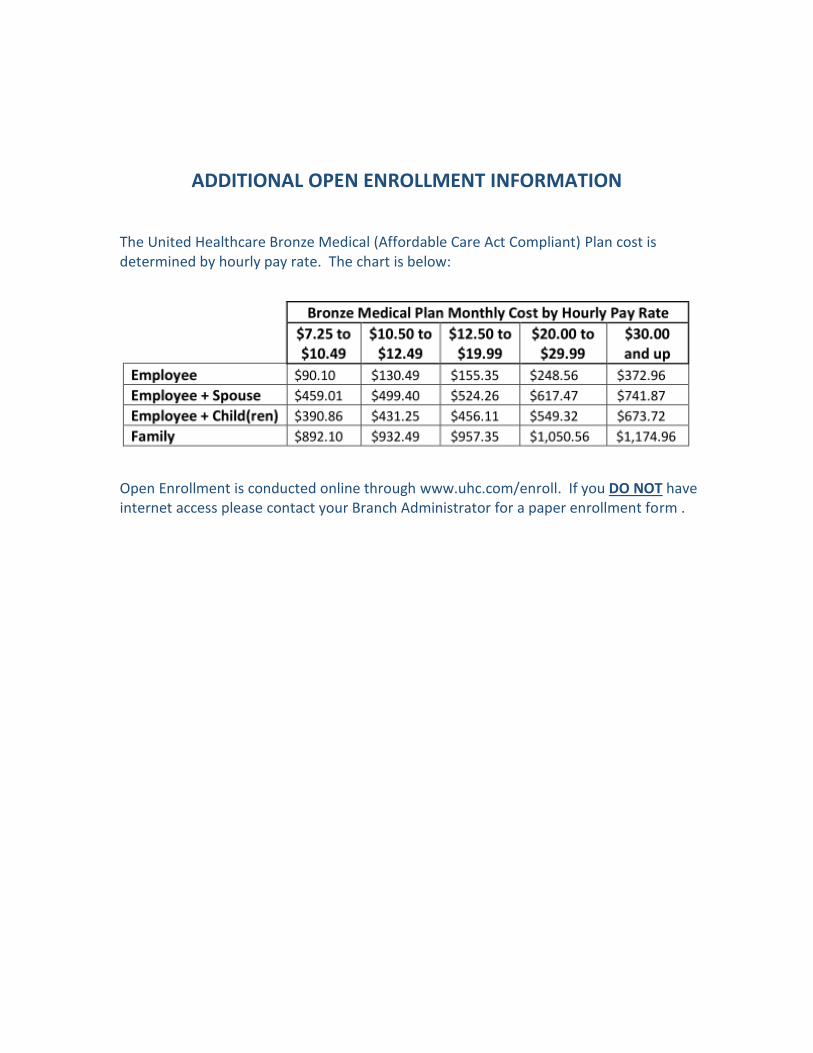
ADDITIONAL OPEN ENROLLMENT INFORMATION The United Healthcare Bronze Medical (Affordable Care Act Compliant) Plan cost is determined by hourly pay rate. The chart is below:
Open Enrollment is conducted online through www.uhc.com/enroll. If you DO NOT have internet access please contact your Branch Administrator for a paper enrollment form .
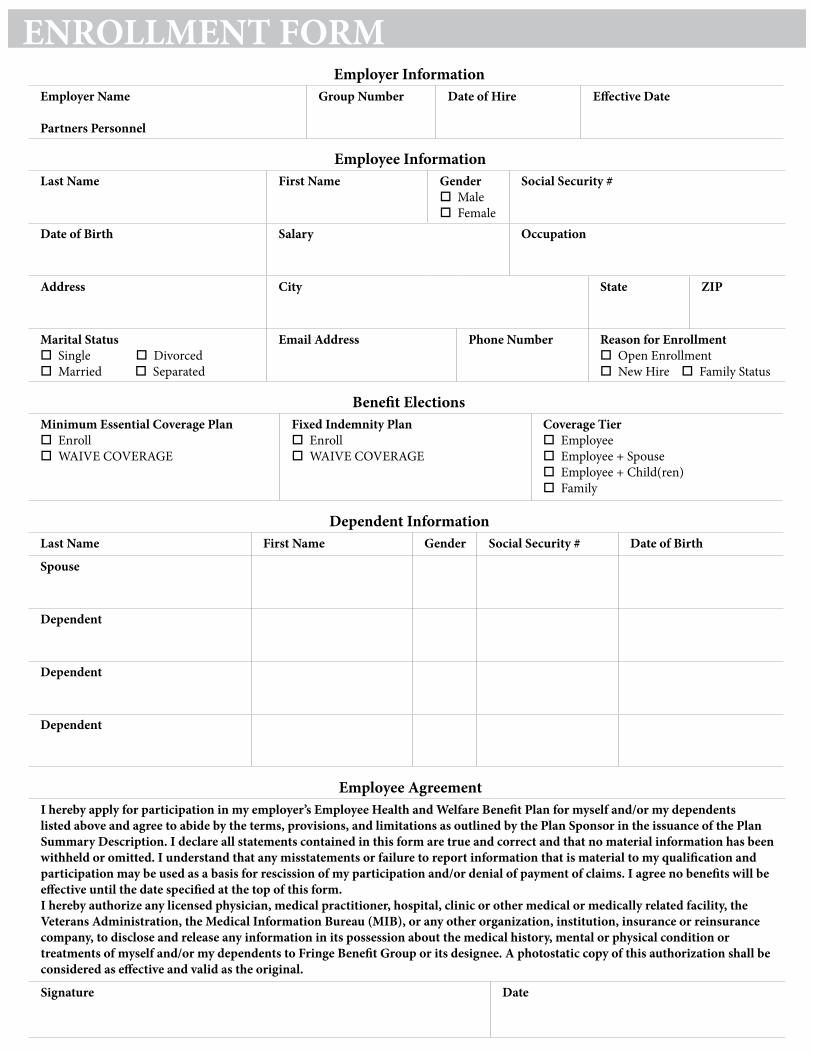
ENROLLMENT FORMEmployer Information
Employer Name
Partners Personnel
Group Number Date of Hire Effective Date
Benefit ElectionsMinimum Essential Coverage Plan Enroll WAIVE COVERAGE
Fixed Indemnity Plan Enroll WAIVE COVERAGE
Coverage Tier Employee Employee + Spouse Employee + Child(ren) Family
Dependent InformationLast Name First Name Gender Social Security # Date of Birth
Spouse
Dependent
Dependent
Dependent
Employee InformationLast Name First Name Gender
Male Female
Social Security #
Date of Birth Salary Occupation
Address City State ZIP
Marital Status Single Divorced Married Separated
Email Address Phone Number Reason for Enrollment Open Enrollment New Hire Family Status
Employee AgreementI hereby apply for participation in my employer’s Employee Health and Welfare Benefit Plan for myself and/or my dependents listed above and agree to abide by the terms, provisions, and limitations as outlined by the Plan Sponsor in the issuance of the Plan Summary Description. I declare all statements contained in this form are true and correct and that no material information has been withheld or omitted. I understand that any misstatements or failure to report information that is material to my qualification and participation may be used as a basis for rescission of my participation and/or denial of payment of claims. I agree no benefits will be effective until the date specified at the top of this form.I hereby authorize any licensed physician, medical practitioner, hospital, clinic or other medical or medically related facility, the Veterans Administration, the Medical Information Bureau (MIB), or any other organization, institution, insurance or reinsurance company, to disclose and release any information in its possession about the medical history, mental or physical condition or treatments of myself and/or my dependents to Fringe Benefit Group or its designee. A photostatic copy of this authorization shall be considered as effective and valid as the original.
Signature Date
Last Name First Name MI Social Security Number
Address Apt # City State Zip Code Home/Cell Phone
Date of Birth Sex Marital Status Work Phone/ / �� M �� F �� Single �� Divorced �� Married �� Widowed
Email Address Race – Check all that apply (Optional)2
�� American Indian/Alaska Native �� Asian �� Black/African-AmericanLanguage Preference, if not English �� Hispanic/Latino �� Native Hawaiian/Pacific Islander �� White
�� Other–Please specify ___________________________________
Primary Physician1 Primary Dentist1
Physician First & Last Name __________________________________ Dentist First & Last Name __________________________________ID # ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ - ___ ___ ___ ___ ID# ___________________________________________________
Page 1 of 4
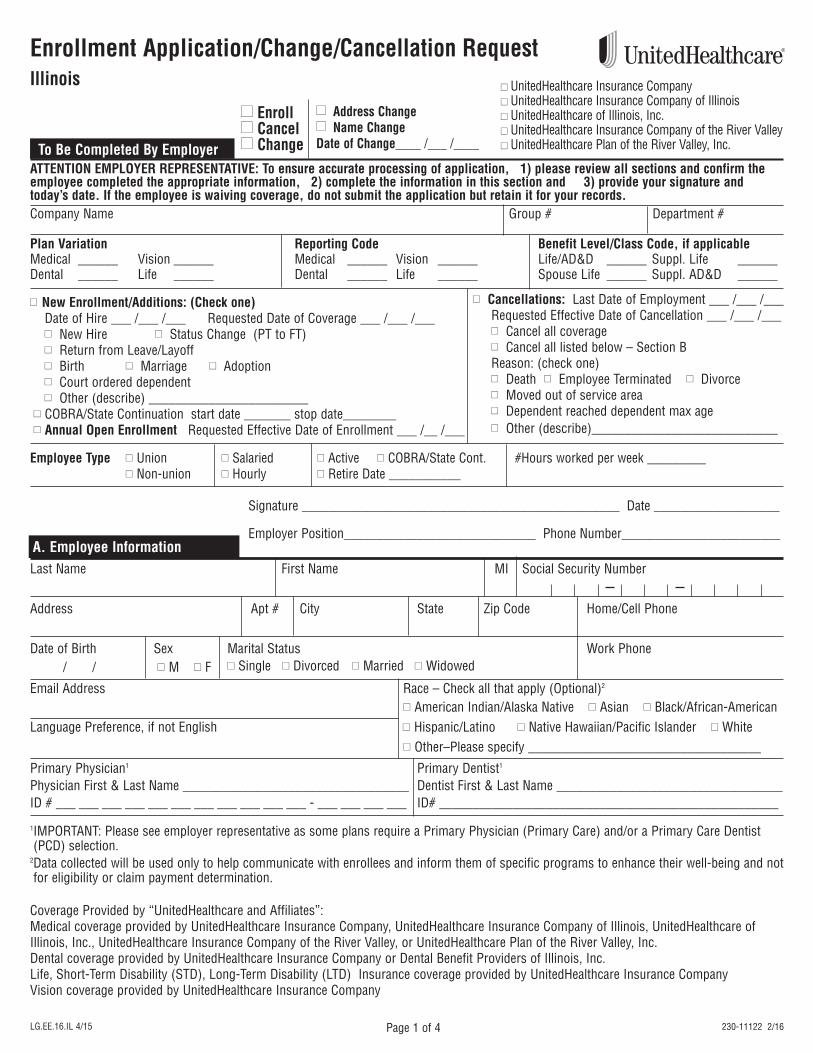
A. Employee Information
Enrollment Application/Change/Cancellation Request Illinois
�� Address Change�� Name ChangeDate of Change____ /___ /____
�� Enroll �� Cancel �� ChangeTo Be Completed By Employer
ATTENTION EMPLOYER REPRESENTATIVE: To ensure accurate processing of application, 1) please review all sections and confirm theemployee completed the appropriate information, 2) complete the information in this section and 3) provide your signature andtoday’s date. If the employee is waiving coverage, do not submit the application but retain it for your records.Company Name Group # Department #
Plan Variation Reporting Code Benefit Level/Class Code, if applicableMedical ______ Vision ______ Medical ______ Vision ______ Life/AD&D ______ Suppl. Life ______Dental ______ Life ______ Dental ______ Life ______ Spouse Life ______ Suppl. AD&D ______
�� New Enrollment/Additions: (Check one)Date of Hire ___ /___ /___ Requested Date of Coverage ___ /___ /___�� New Hire �� Status Change (PT to FT)�� Return from Leave/Layoff �� Birth �� Marriage �� Adoption �� Court ordered dependent �� Other (describe) ________________________
�� COBRA/State Continuation start date _______ stop date________�� Annual Open Enrollment Requested Effective Date of Enrollment ___ /__ /___
�� Cancellations: Last Date of Employment ___ /___ /___Requested Effective Date of Cancellation ___ /___ /___�� Cancel all coverage �� Cancel all listed below – Section BReason: (check one)�� Death �� Employee Terminated �� Divorce �� Moved out of service area�� Dependent reached dependent max age �� Other (describe)____________________________
Signature ________________________________________________ Date ___________________
Employer Position_____________________________ Phone Number________________________
Employee Type �� Union �� Salaried �� Active �� COBRA/State Cont. #Hours worked per week _________�� Non-union �� Hourly �� Retire Date ___________
Coverage Provided by “UnitedHealthcare and Affiliates”:Medical coverage provided by UnitedHealthcare Insurance Company, UnitedHealthcare Insurance Company of Illinois, UnitedHealthcare ofIllinois, Inc., UnitedHealthcare Insurance Company of the River Valley, or UnitedHealthcare Plan of the River Valley, Inc.Dental coverage provided by UnitedHealthcare Insurance Company or Dental Benefit Providers of Illinois, Inc.Life, Short-Term Disability (STD), Long-Term Disability (LTD) Insurance coverage provided by UnitedHealthcare Insurance CompanyVision coverage provided by UnitedHealthcare Insurance Company
LG.EE.16.IL 4/15 230-11122 2/16
1IMPORTANT: Please see employer representative as some plans require a Primary Physician (Primary Care) and/or a Primary Care Dentist(PCD) selection.
2Data collected will be used only to help communicate with enrollees and inform them of specific programs to enhance their well-being and notfor eligibility or claim payment determination.
�� UnitedHealthcare Insurance Company�� UnitedHealthcare Insurance Company of Illinois�� UnitedHealthcare of Illinois, Inc.�� UnitedHealthcare Insurance Company of the River Valley�� UnitedHealthcare Plan of the River Valley, Inc.
Page 2 of 4
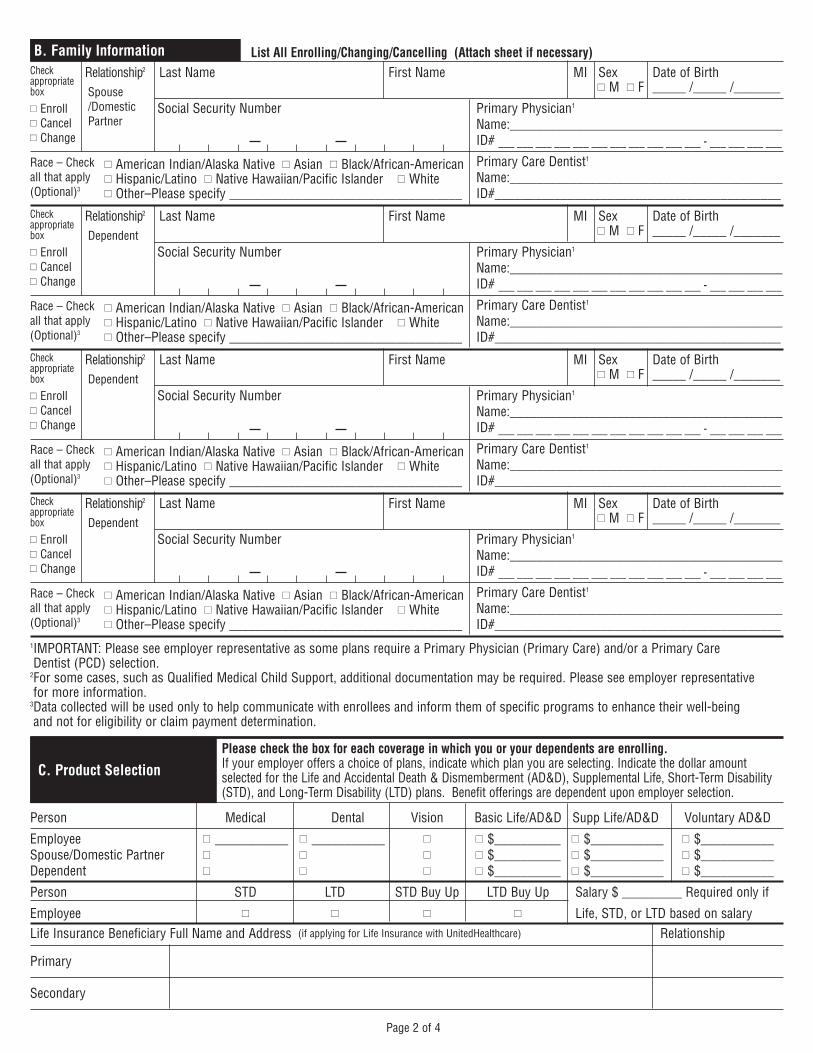
List All Enrolling/Changing/Cancelling (Attach sheet if necessary) Relationship2 Last Name First Name MI Sex Date of Birth
�� M �� F _____ /_____ /_______
Social Security Number Primary Physician1
Name:_________________________________________ ID# ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ - ___ ___ ___ ___Primary Care Dentist1
Name:_________________________________________ ID#___________________________________________
Relationship2 Last Name First Name MI Sex Date of Birth�� M �� F _____ /_____ /_______
Social Security Number Primary Physician1
Name:_________________________________________ ID# ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ - ___ ___ ___ ___Primary Care Dentist1
Name:_________________________________________ ID#___________________________________________
Relationship2 Last Name First Name MI Sex Date of Birth�� M �� F _____ /_____ /_______
Social Security Number Primary Physician1
Name:_________________________________________ ID# ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ - ___ ___ ___ ___Primary Care Dentist1
Name:_________________________________________ ID#___________________________________________
Relationship2 Last Name First Name MI Sex Date of Birth�� M �� F _____ /_____ /_______
Social Security Number Primary Physician1
Name:_________________________________________ ID# ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ - ___ ___ ___ ___Primary Care Dentist1
Name:_________________________________________ ID#___________________________________________
B. Family InformationCheckappropriatebox
�� Enroll�� Cancel�� Change
Please check the box for each coverage in which you or your dependents are enrolling. If your employer offers a choice of plans, indicate which plan you are selecting. Indicate the dollar amountselected for the Life and Accidental Death & Dismemberment (AD&D), Supplemental Life, Short-Term Disability(STD), and Long-Term Disability (LTD) plans. Benefit offerings are dependent upon employer selection.
Person Medical Dental Vision Basic Life/AD&D Supp Life/AD&D Voluntary AD&D
Employee �� ___________ �� ___________ �� �� $__________ �� $___________ �� $___________ Spouse/Domestic Partner �� ___________ �� _____________ �� �� $__________ �� $___________ �� $___________Dependent �� ___________ �� _____________ �� �� $__________ �� $___________ �� $___________
Person STD LTD STD Buy Up LTD Buy Up Salary $ _________ Required only if
Employee �� �� �� �� Life, STD, or LTD based on salaryLife Insurance Beneficiary Full Name and Address (if applying for Life Insurance with UnitedHealthcare) Relationship
Primary
Secondary
C. Product Selection
1IMPORTANT: Please see employer representative as some plans require a Primary Physician (Primary Care) and/or a Primary Care Dentist (PCD) selection.
2For some cases, such as Qualified Medical Child Support, additional documentation may be required. Please see employer representative for more information.
3Data collected will be used only to help communicate with enrollees and inform them of specific programs to enhance their well-being and not for eligibility or claim payment determination.
Race – Checkall that apply(Optional)3
�� American Indian/Alaska Native �� Asian �� Black/African-American �� Hispanic/Latino �� Native Hawaiian/Pacific Islander �� White �� Other–Please specify ___________________________________
Spouse/DomesticPartner
Checkappropriatebox
�� Enroll�� Cancel�� Change
Race – Checkall that apply(Optional)3
�� American Indian/Alaska Native �� Asian �� Black/African-American �� Hispanic/Latino �� Native Hawaiian/Pacific Islander �� White �� Other–Please specify ___________________________________
Dependent
Checkappropriatebox
�� Enroll�� Cancel�� Change
Race – Checkall that apply(Optional)3
�� American Indian/Alaska Native �� Asian �� Black/African-American �� Hispanic/Latino �� Native Hawaiian/Pacific Islander �� White �� Other–Please specify ___________________________________
Dependent
Checkappropriatebox
�� Enroll�� Cancel�� Change
Race – Checkall that apply(Optional)3
�� American Indian/Alaska Native �� Asian �� Black/African-American �� Hispanic/Latino �� Native Hawaiian/Pacific Islander �� White �� Other–Please specify ___________________________________
Dependent
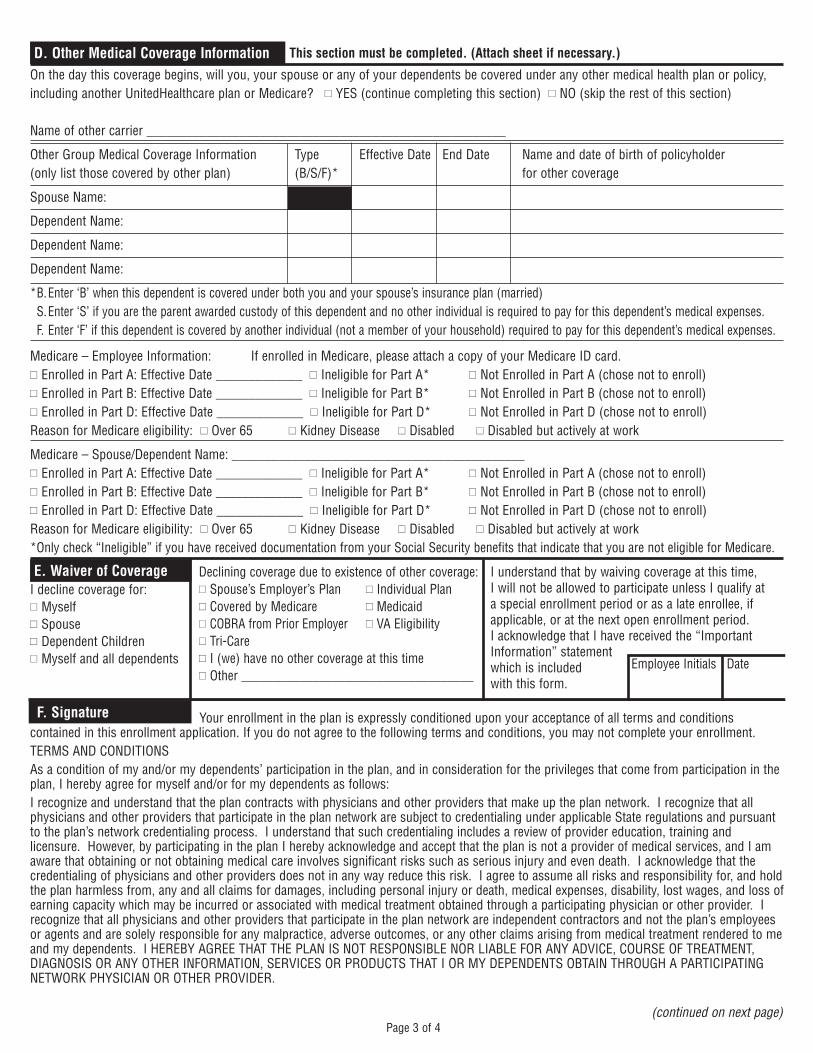
F. Signature Your enrollment in the plan is expressly conditioned upon your acceptance of all terms and conditionscontained in this enrollment application. If you do not agree to the following terms and conditions, you may not complete your enrollment.TERMS AND CONDITIONSAs a condition of my and/or my dependents’ participation in the plan, and in consideration for the privileges that come from participation in theplan, I hereby agree for myself and/or for my dependents as follows:I recognize and understand that the plan contracts with physicians and other providers that make up the plan network. I recognize that allphysicians and other providers that participate in the plan network are subject to credentialing under applicable State regulations and pursuantto the plan’s network credentialing process. I understand that such credentialing includes a review of provider education, training andlicensure. However, by participating in the plan I hereby acknowledge and accept that the plan is not a provider of medical services, and I amaware that obtaining or not obtaining medical care involves significant risks such as serious injury and even death. I acknowledge that thecredentialing of physicians and other providers does not in any way reduce this risk. I agree to assume all risks and responsibility for, and holdthe plan harmless from, any and all claims for damages, including personal injury or death, medical expenses, disability, lost wages, and loss ofearning capacity which may be incurred or associated with medical treatment obtained through a participating physician or other provider. Irecognize that all physicians and other providers that participate in the plan network are independent contractors and not the plan’s employeesor agents and are solely responsible for any malpractice, adverse outcomes, or any other claims arising from medical treatment rendered to meand my dependents. I HEREBY AGREE THAT THE PLAN IS NOT RESPONSIBLE NOR LIABLE FOR ANY ADVICE, COURSE OF TREATMENT,DIAGNOSIS OR ANY OTHER INFORMATION, SERVICES OR PRODUCTS THAT I OR MY DEPENDENTS OBTAIN THROUGH A PARTICIPATINGNETWORK PHYSICIAN OR OTHER PROVIDER.
Medicare – Employee Information: If enrolled in Medicare, please attach a copy of your Medicare ID card.�� Enrolled in Part A: Effective Date _____________ �� Ineligible for Part A* �� Not Enrolled in Part A (chose not to enroll)�� Enrolled in Part B: Effective Date _____________ �� Ineligible for Part B* �� Not Enrolled in Part B (chose not to enroll)�� Enrolled in Part D: Effective Date _____________ �� Ineligible for Part D* �� Not Enrolled in Part D (chose not to enroll)Reason for Medicare eligibility: �� Over 65 �� Kidney Disease �� Disabled �� Disabled but actively at work
Medicare – Spouse/Dependent Name: ____________________________________________�� Enrolled in Part A: Effective Date _____________ �� Ineligible for Part A* �� Not Enrolled in Part A (chose not to enroll)�� Enrolled in Part B: Effective Date _____________ �� Ineligible for Part B* �� Not Enrolled in Part B (chose not to enroll)�� Enrolled in Part D: Effective Date _____________ �� Ineligible for Part D* �� Not Enrolled in Part D (chose not to enroll)Reason for Medicare eligibility: �� Over 65 �� Kidney Disease �� Disabled �� Disabled but actively at work*Only check “Ineligible” if you have received documentation from your Social Security benefits that indicate that you are not eligible for Medicare.
E. Waiver of CoverageI decline coverage for:�� Myself �� Spouse�� Dependent Children�� Myself and all dependents
Declining coverage due to existence of other coverage:�� Spouse’s Employer’s Plan �� Individual Plan�� Covered by Medicare �� Medicaid�� COBRA from Prior Employer �� VA Eligibility�� Tri-Care�� I (we) have no other coverage at this time�� Other ____________________________________
I understand that by waiving coverage at this time, I will not be allowed to participate unless I qualify at a special enrollment period or as a late enrollee, ifapplicable, or at the next open enrollment period. I acknowledge that I have received the “ImportantInformation” statementwhich is includedwith this form.
Employee Initials Date
On the day this coverage begins, will you, your spouse or any of your dependents be covered under any other medical health plan or policy,including another UnitedHealthcare plan or Medicare? �� YES (continue completing this section) �� NO (skip the rest of this section)
Name of other carrier ______________________________________________________
Other Group Medical Coverage Information Type Effective Date End Date Name and date of birth of policyholder (only list those covered by other plan) (B/S/F)* for other coverage
Spouse Name:
Dependent Name:
Dependent Name:
Dependent Name:
*B.Enter ‘B’ when this dependent is covered under both you and your spouse’s insurance plan (married)S.Enter ‘S’ if you are the parent awarded custody of this dependent and no other individual is required to pay for this dependent’s medical expenses.F. Enter ‘F’ if this dependent is covered by another individual (not a member of your household) required to pay for this dependent’s medical expenses.
D. Other Medical Coverage Information This section must be completed. (Attach sheet if necessary.)
Page 3 of 4(continued on next page)
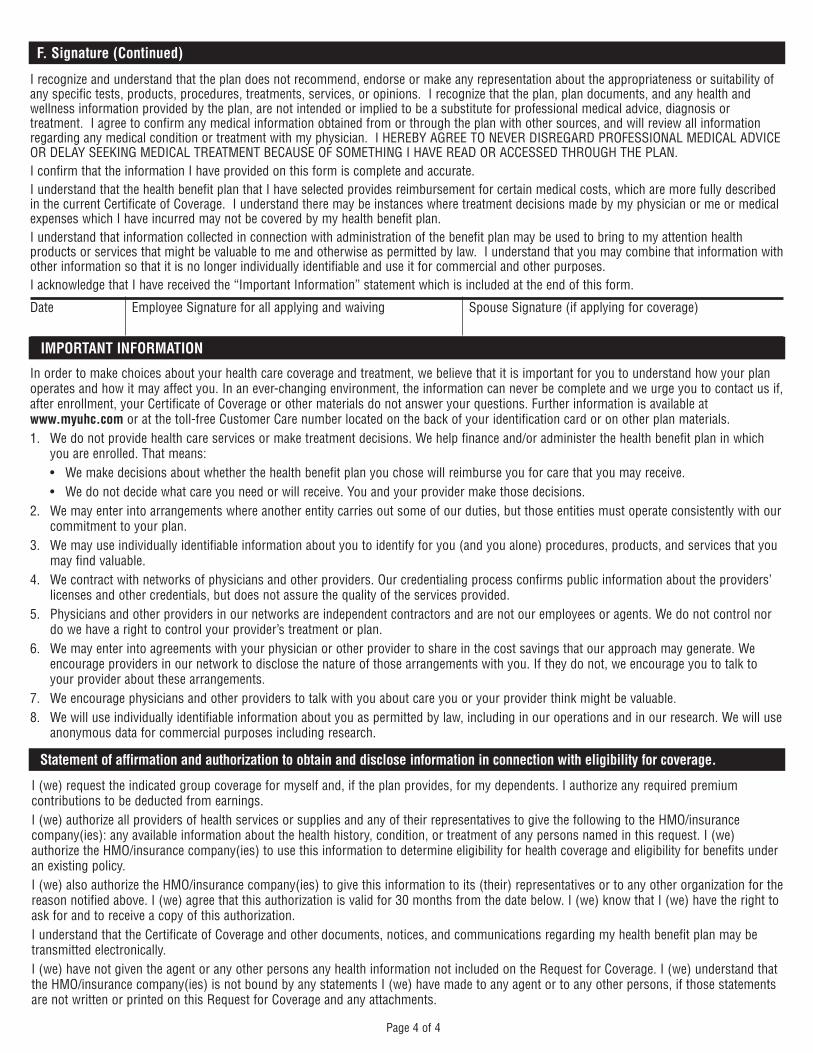
IMPORTANT INFORMATION
In order to make choices about your health care coverage and treatment, we believe that it is important for you to understand how your planoperates and how it may affect you. In an ever-changing environment, the information can never be complete and we urge you to contact us if,after enrollment, your Certificate of Coverage or other materials do not answer your questions. Further information is available atwww.myuhc.com or at the toll-free Customer Care number located on the back of your identification card or on other plan materials.1. We do not provide health care services or make treatment decisions. We help finance and/or administer the health benefit plan in which
you are enrolled. That means:• We make decisions about whether the health benefit plan you chose will reimburse you for care that you may receive.• We do not decide what care you need or will receive. You and your provider make those decisions.
2. We may enter into arrangements where another entity carries out some of our duties, but those entities must operate consistently with ourcommitment to your plan.
3. We may use individually identifiable information about you to identify for you (and you alone) procedures, products, and services that youmay find valuable.
4. We contract with networks of physicians and other providers. Our credentialing process confirms public information about the providers’licenses and other credentials, but does not assure the quality of the services provided.
5. Physicians and other providers in our networks are independent contractors and are not our employees or agents. We do not control nordo we have a right to control your provider’s treatment or plan.
6. We may enter into agreements with your physician or other provider to share in the cost savings that our approach may generate. Weencourage providers in our network to disclose the nature of those arrangements with you. If they do not, we encourage you to talk toyour provider about these arrangements.
7. We encourage physicians and other providers to talk with you about care you or your provider think might be valuable.8. We will use individually identifiable information about you as permitted by law, including in our operations and in our research. We will use
anonymous data for commercial purposes including research.
I (we) request the indicated group coverage for myself and, if the plan provides, for my dependents. I authorize any required premiumcontributions to be deducted from earnings.I (we) authorize all providers of health services or supplies and any of their representatives to give the following to the HMO/insurancecompany(ies): any available information about the health history, condition, or treatment of any persons named in this request. I (we)authorize the HMO/insurance company(ies) to use this information to determine eligibility for health coverage and eligibility for benefits underan existing policy.I (we) also authorize the HMO/insurance company(ies) to give this information to its (their) representatives or to any other organization for thereason notified above. I (we) agree that this authorization is valid for 30 months from the date below. I (we) know that I (we) have the right toask for and to receive a copy of this authorization.I understand that the Certificate of Coverage and other documents, notices, and communications regarding my health benefit plan may betransmitted electronically.I (we) have not given the agent or any other persons any health information not included on the Request for Coverage. I (we) understand thatthe HMO/insurance company(ies) is not bound by any statements I (we) have made to any agent or to any other persons, if those statementsare not written or printed on this Request for Coverage and any attachments.
Statement of affirmation and authorization to obtain and disclose information in connection with eligibility for coverage.
Page 4 of 4
F. Signature (Continued)
Date Employee Signature for all applying and waiving Spouse Signature (if applying for coverage)
I recognize and understand that the plan does not recommend, endorse or make any representation about the appropriateness or suitability ofany specific tests, products, procedures, treatments, services, or opinions. I recognize that the plan, plan documents, and any health andwellness information provided by the plan, are not intended or implied to be a substitute for professional medical advice, diagnosis ortreatment. I agree to confirm any medical information obtained from or through the plan with other sources, and will review all informationregarding any medical condition or treatment with my physician. I HEREBY AGREE TO NEVER DISREGARD PROFESSIONAL MEDICAL ADVICEOR DELAY SEEKING MEDICAL TREATMENT BECAUSE OF SOMETHING I HAVE READ OR ACCESSED THROUGH THE PLAN.I confirm that the information I have provided on this form is complete and accurate. I understand that the health benefit plan that I have selected provides reimbursement for certain medical costs, which are more fully describedin the current Certificate of Coverage. I understand there may be instances where treatment decisions made by my physician or me or medicalexpenses which I have incurred may not be covered by my health benefit plan.I understand that information collected in connection with administration of the benefit plan may be used to bring to my attention healthproducts or services that might be valuable to me and otherwise as permitted by law. I understand that you may combine that information withother information so that it is no longer individually identifiable and use it for commercial and other purposes. I acknowledge that I have received the “Important Information” statement which is included at the end of this form.
2018 Annual Notices
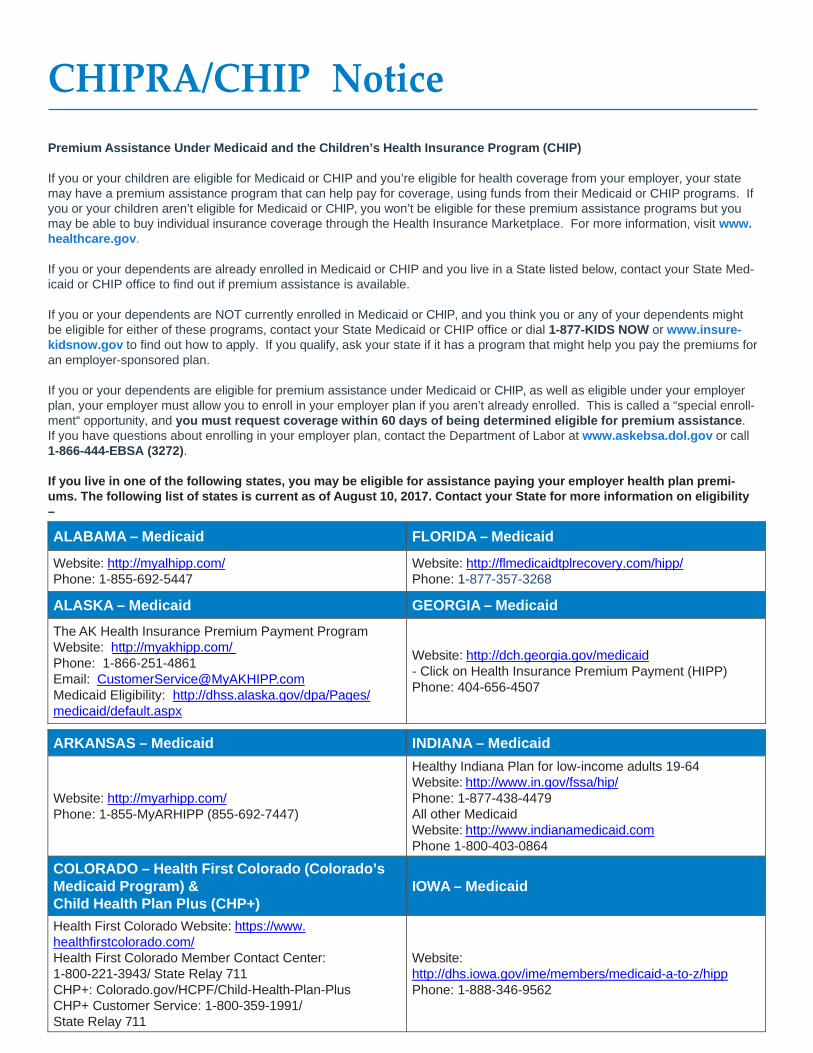
CHIPRA/CHIP Notice
Premium Assistance Under Medicaid and the Children’s Health Insurance Program (CHIP)
If you or your children are eligible for Medicaid or CHIP and you’re eligible for health coverage from your employer, your state may have a premium assistance program that can help pay for coverage, using funds from their Medicaid or CHIP programs. If you or your children aren’t eligible for Medicaid or CHIP, you won’t be eligible for these premium assistance programs but you may be able to buy individual insurance coverage through the Health Insurance Marketplace. For more information, visit www. healthcare.gov.
If you or your dependents are already enrolled in Medicaid or CHIP and you live in a State listed below, contact your State Med- icaid or CHIP office to find out if premium assistance is available.
If you or your dependents are NOT currently enrolled in Medicaid or CHIP, and you think you or any of your dependents might be eligible for either of these programs, contact your State Medicaid or CHIP office or dial 1-877-KIDS NOW or www.insure- kidsnow.gov to find out how to apply. If you qualify, ask your state if it has a program that might help you pay the premiums for an employer-sponsored plan.
If you or your dependents are eligible for premium assistance under Medicaid or CHIP, as well as eligible under your employer plan, your employer must allow you to enroll in your employer plan if you aren’t already enrolled. This is called a “special enroll- ment“ opportunity, and you must request coverage within 60 days of being determined eligible for premium assistance. If you have questions about enrolling in your employer plan, contact the Department of Labor at www.askebsa.dol.gov or call 1-866-444-EBSA (3272).
If you live in one of the following states, you may be eligible for assistance paying your employer health plan premi- ums. The following list of states is current as of August 10, 2017. Contact your State for more information on eligibility –
ALABAMA – Medicaid FLORIDA – Medicaid
Website: http://myalhipp.com/ Phone: 1-855-692-5447
Website: http://flmedicaidtplrecovery.com/hipp/ Phone: 1-877-357-3268
ALASKA – Medicaid GEORGIA – Medicaid
The AK Health Insurance Premium Payment Program Website: http://myakhipp.com/ Phone: 1-866-251-4861 Email: [email protected] Medicaid Eligibility: http://dhss.alaska.gov/dpa/Pages/ medicaid/default.aspx
Website: http://dch.georgia.gov/medicaid - Click on Health Insurance Premium Payment (HIPP) Phone: 404-656-4507
ARKANSAS – Medicaid INDIANA – Medicaid Website: http://myarhipp.com/ Phone: 1-855-MyARHIPP (855-692-7447)
Healthy Indiana Plan for low-income adults 19-64 Website: http://www.in.gov/fssa/hip/ Phone: 1-877-438-4479 All other Medicaid Website: http://www.indianamedicaid.com Phone 1-800-403-0864
COLORADO – Health First Colorado (Colorado’s Medicaid Program) & Child Health Plan Plus (CHP+)
IOWA – Medicaid
Health First Colorado Website: https://www. healthfirstcolorado.com/ Health First Colorado Member Contact Center: 1-800-221-3943/ State Relay 711 CHP+: Colorado.gov/HCPF/Child-Health-Plan-Plus CHP+ Customer Service: 1-800-359-1991/ State Relay 711
Website: http://dhs.iowa.gov/ime/members/medicaid-a-to-z/hipp Phone: 1-888-346-9562
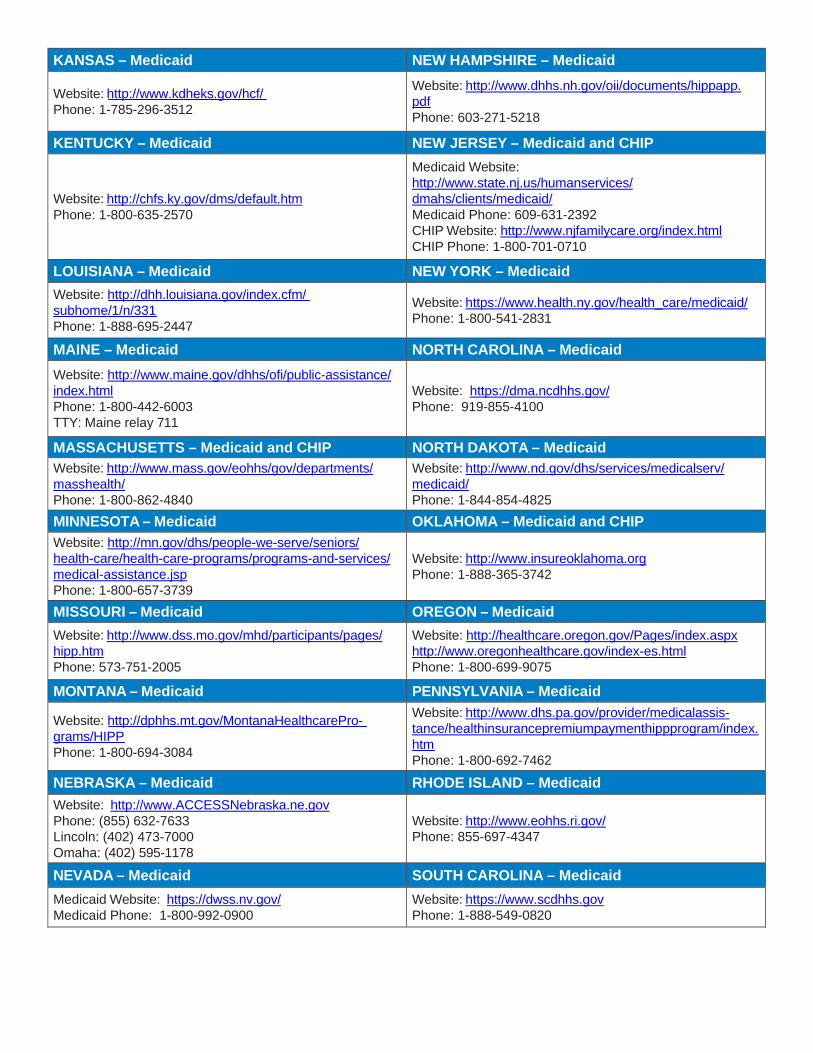
KANSAS – Medicaid NEW HAMPSHIRE – Medicaid Website: http://www.kdheks.gov/hcf/ Phone: 1-785-296-3512
Website: http://www.dhhs.nh.gov/oii/documents/hippapp. pdf Phone: 603-271-5218
KENTUCKY – Medicaid NEW JERSEY – Medicaid and CHIP
Website: http://chfs.ky.gov/dms/default.htm Phone: 1-800-635-2570
Medicaid Website: http://www.state.nj.us/humanservices/ dmahs/clients/medicaid/ Medicaid Phone: 609-631-2392 CHIP Website: http://www.njfamilycare.org/index.html CHIP Phone: 1-800-701-0710
LOUISIANA – Medicaid NEW YORK – Medicaid
Website: http://dhh.louisiana.gov/index.cfm/ subhome/1/n/331 Phone: 1-888-695-2447
Website: https://www.health.ny.gov/health_care/medicaid/ Phone: 1-800-541-2831
MAINE – Medicaid NORTH CAROLINA – Medicaid
Website: http://www.maine.gov/dhhs/ofi/public-assistance/ index.html Phone: 1-800-442-6003 TTY: Maine relay 711
Website: https://dma.ncdhhs.gov/ Phone: 919-855-4100
MASSACHUSETTS – Medicaid and CHIP NORTH DAKOTA – Medicaid Website: http://www.mass.gov/eohhs/gov/departments/ masshealth/ Phone: 1-800-862-4840
Website: http://www.nd.gov/dhs/services/medicalserv/ medicaid/ Phone: 1-844-854-4825
MINNESOTA – Medicaid OKLAHOMA – Medicaid and CHIP Website: http://mn.gov/dhs/people-we-serve/seniors/ health-care/health-care-programs/programs-and-services/ medical-assistance.jsp Phone: 1-800-657-3739
Website: http://www.insureoklahoma.org Phone: 1-888-365-3742
MISSOURI – Medicaid OREGON – Medicaid
Website: http://www.dss.mo.gov/mhd/participants/pages/ hipp.htm Phone: 573-751-2005
Website: http://healthcare.oregon.gov/Pages/index.aspx http://www.oregonhealthcare.gov/index-es.html Phone: 1-800-699-9075
MONTANA – Medicaid PENNSYLVANIA – Medicaid
Website: http://dphhs.mt.gov/MontanaHealthcarePro- grams/HIPP Phone: 1-800-694-3084
Website: http://www.dhs.pa.gov/provider/medicalassis- tance/healthinsurancepremiumpaymenthippprogram/index. htm Phone: 1-800-692-7462
NEBRASKA – Medicaid RHODE ISLAND – Medicaid Website: http://www.ACCESSNebraska.ne.gov Phone: (855) 632-7633 Lincoln: (402) 473-7000 Omaha: (402) 595-1178
Website: http://www.eohhs.ri.gov/ Phone: 855-697-4347
NEVADA – Medicaid SOUTH CAROLINA – Medicaid
Medicaid Website: https://dwss.nv.gov/ Medicaid Phone: 1-800-992-0900
Website: https://www.scdhhs.gov Phone: 1-888-549-0820
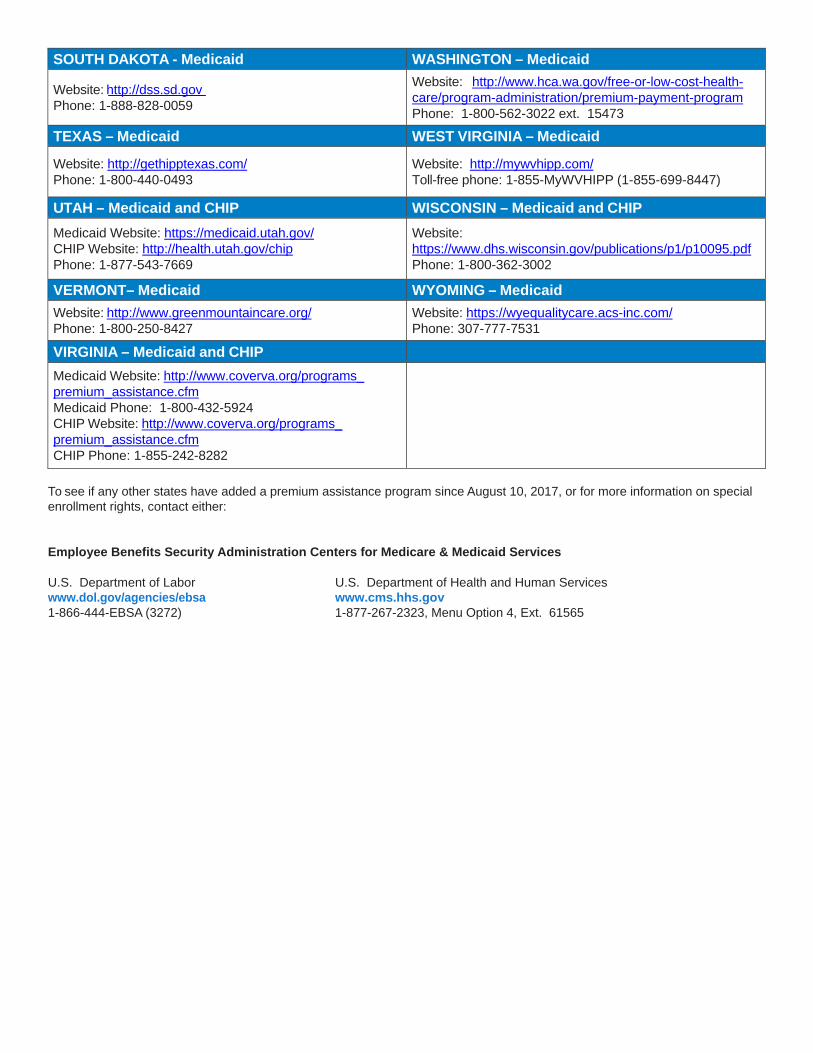
SOUTH DAKOTA - Medicaid WASHINGTON – Medicaid
Website: http://dss.sd.gov Phone: 1-888-828-0059
Website: http://www.hca.wa.gov/free-or-low-cost-health- care/program-administration/premium-payment-program Phone: 1-800-562-3022 ext. 15473
TEXAS – Medicaid WEST VIRGINIA – Medicaid
Website: http://gethipptexas.com/ Phone: 1-800-440-0493
Website: http://mywvhipp.com/ Toll-free phone: 1-855-MyWVHIPP (1-855-699-8447)
UTAH – Medicaid and CHIP WISCONSIN – Medicaid and CHIP
Medicaid Website: https://medicaid.utah.gov/ CHIP Website: http://health.utah.gov/chip Phone: 1-877-543-7669
Website: https://www.dhs.wisconsin.gov/publications/p1/p10095.pdf Phone: 1-800-362-3002
VERMONT– Medicaid WYOMING – Medicaid
Website: http://www.greenmountaincare.org/ Phone: 1-800-250-8427
Website: https://wyequalitycare.acs-inc.com/ Phone: 307-777-7531
VIRGINIA – Medicaid and CHIP
Medicaid Website: http://www.coverva.org/programs_ premium_assistance.cfm Medicaid Phone: 1-800-432-5924 CHIP Website: http://www.coverva.org/programs_ premium_assistance.cfm CHIP Phone: 1-855-242-8282
To see if any other states have added a premium assistance program since August 10, 2017, or for more information on special enrollment rights, contact either:
Employee Benefits Security Administration Centers for Medicare & Medicaid Services
U.S. Department of Labor U.S. Department of Health and Human Services www.dol.gov/agencies/ebsa www.cms.hhs.gov 1-866-444-EBSA (3272) 1-877-267-2323, Menu Option 4, Ext. 61565
Annual Notice of Women’s Health and Cancer Rights Act
Do you know that your plan, as required by the Women’s Health and Cancer Right Act of 1998, provides benefits for mastectomy-related services, including all stages of reconstruction and surgery to achieve symmetry between the breasts, prostheses and treatment for complications resulting from a mastectomy, including lymphedema? Call your local Human Resource representative for more information.
Important Notice From Partners Personnel About Your Prescription Drug Coverage and Medicare
Please read this notice carefully and keep it where you can find it. This notice has information about your current prescription drug coverage with Partners Personnel and about your options under Medicare’s prescription drug coverage. This information can help you decide whether or not you want to join a Medicare drug plan. Information about where you can get help to make decisions about your prescription drug coverage is at the end of this notice. There are three important things you need to know about your current coverage and Medicare’s prescription drug coverage:
1. Medicare prescription drug coverage became available in 2006 to everyone with Medicare. You can get this
coverage if you join a Medicare Prescription Drug Plan or join a Medicare Advantage Plan (like an HMO or PPO) that offers prescription drug coverage. All Medicare drug plans provide at least a standard level of coverage set by Medicare. Some plans may also offer more coverage for a higher monthly premium.
2. Partners Personnel has determined that your prescription drug coverage offered by the Bronze plan is, on average
for all plan participants, NOT expected to pay out as much as standard Medicare prescription drug coverage pays. Therefore, your coverage is considered Non-Creditable Coverage. This is important because, most likely, you will get more help with your drug costs if you join a Medicare drug plan, than if you only have prescription drug coverage from the Bronze plan. This is also important because it may mean that you may pay a higher premium (a penalty) if you do not join a Medicare drug plan when you first become eligible.
3. You can keep your current coverage from the Bronze plan. However, because your coverage is non-creditable, you have decisions to make about Medicare prescription drug coverage that may affect how much you pay for that coverage, depending on if and when you join a drug plan. When you make your decision, you should compare your current coverage, including what drugs are covered, with the coverage and cost of the plans offering Medicare prescription drug coverage in your area. Read this notice carefully - it explains your options.
When Can You Join A Medicare Drug Plan? You can join a Medicare drug plan when you first become eligible for Medicare and each year from October 15th through December 7th. However, if you decide to drop your current coverage with Partners Personnel, since it is employer/union sponsored group coverage, you will be eligible for two (2) month Special Enrollment Period (SEP) to join a Medicare drug plan; however you may also pay a higher premium (a penalty) because you did not have creditable coverage under the Bronze plan. When Will You Pay A Higher Premium (Penalty) To Join A Medicare Drug Plan? Since the coverage under the Bronze plan, is not creditable, depending on how long you go without creditable prescription drug coverage you may pay a penalty to join a Medicare drug plan. Starting with the end of the last month that you were first eligible to join a Medicare drug plan but didn’t join, if you go 63 continuous days or longer without prescription drug coverage that’s creditable, your monthly premium may go up by at least 1% of the Medicare base beneficiary premium per month for every month that you did not have that coverage. For example, if you go nineteen months without creditable coverage, your premium may consistently be at least 19% higher than the Medicare base beneficiary premium. You may have to pay this higher premium (penalty) as long as you have Medicare prescription drug coverage. In addition, you may have to wait until the following October to join. What Happens To Your Current Coverage If You Decide to Join A Medicare Drug Plan? If you decide to join a Medicare drug plan, your current coverage may be affected. Moreover, if you do decide to join a Medicare drug plan and drop your current coverage, be aware that you and your dependents may not be able to get this coverage back. Please contact your Human Resources Department for more information about what happens to your coverage if you enroll in a Medicare Part D prescription drug plan. For More Information About This Notice Or Your Current Prescription Drug Coverage…
Contact the person listed below for further information. You can also refer to the Summary Plan Description (SPD) for your current Bronze plan prescription drug plan design details. NOTE: You’ll get this notice each year. You will also get it before the next period you can join a Medicare drug plan, and if this coverage through Partners Personnel changes. You also may request a copy. For More Information About Your Options Under Medicare Prescription Drug Coverage…
More detailed information about Medicare plans that offer prescription drug coverage is in the “Medicare & You” handbook. You’ll get a copy of the handbook in the mail every year from Medicare. You may also be contacted directly by Medicare drug plans. For more information about Medicare prescription drug coverage:
Visit www.medicare.gov Call your State Health Insurance Assistance Program (see the inside back cover of your copy of the “Medicare &
You” handbook for their telephone number) for personalized help, Call 1-800-MEDICARE (1-800-633-4227). TTY users should call 1-877-486-2048.
If you have limited income and resources, extra help paying for Medicare prescription drug coverage is available. For information about this extra help, visit Social Security on the web at www.socialsecurity.gov, or call them at 1-800-772-1213 (TTY 1-800-325-0778). Date: 12/4/2017 Name of Entity/Sender: Partners Personnel Contact--Position/Office: Human Resources Department Address: 3820 State Street, Suite B, Santa Barbara, CA 93105 Phone Number: (805)-456-5200
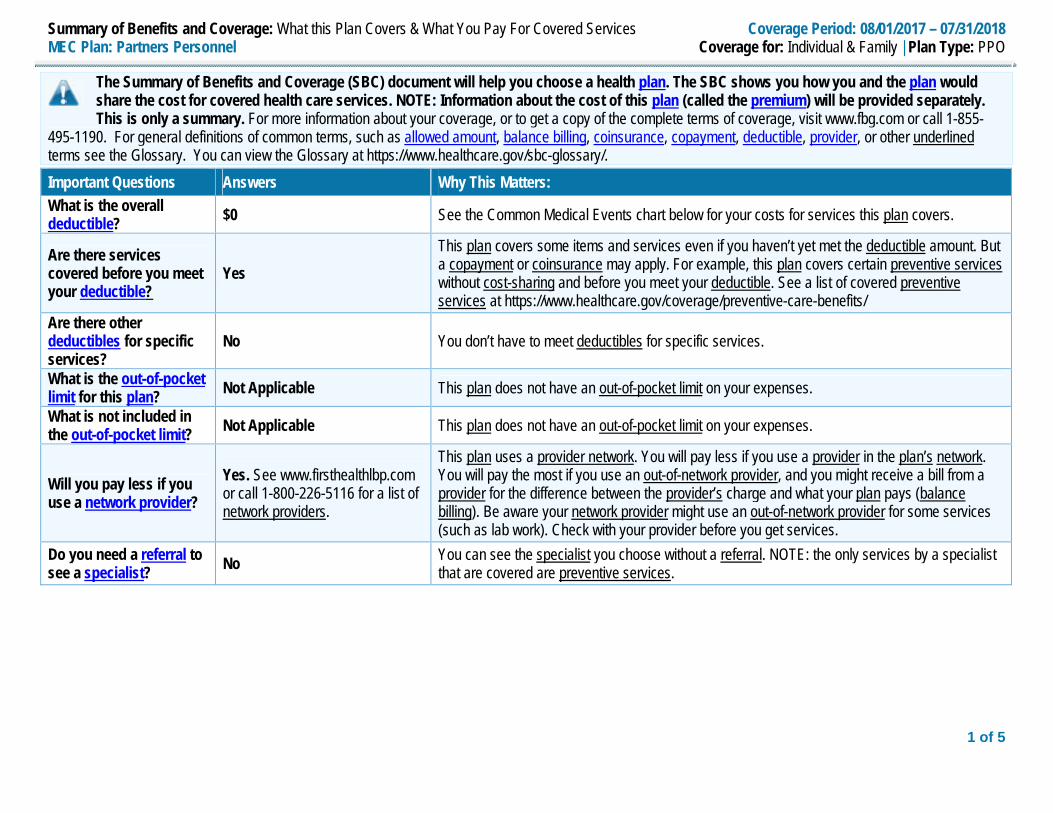
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 08/01/2017 – 07/31/2018 MEC Plan: Partners Personnel Coverage for: Individual & Family | Plan Type: PPO
1 of 5
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about the cost of this plan (called the premium) will be provided separately. This is only a summary. For more information about your coverage, or to get a copy of the complete terms of coverage, visit www.fbg.com or call 1-855-
495-1190. For general definitions of common terms, such as allowed amount, balance billing, coinsurance, copayment, deductible, provider, or other underlined terms see the Glossary. You can view the Glossary at https://www.healthcare.gov/sbc-glossary/.
Important Questions Answers Why This Matters: What is the overall deductible? $0 See the Common Medical Events chart below for your costs for services this plan covers.
Are there services covered before you meet your deductible?
Yes This plan covers some items and services even if you haven’t yet met the deductible amount. But a copayment or coinsurance may apply. For example, this plan covers certain preventive services without cost-sharing and before you meet your deductible. See a list of covered preventive services at https://www.healthcare.gov/coverage/preventive-care-benefits/
Are there other deductibles for specific services?
No You don’t have to meet deductibles for specific services.
What is the out-of-pocket limit for this plan? Not Applicable This plan does not have an out-of-pocket limit on your expenses.
What is not included in the out-of-pocket limit? Not Applicable This plan does not have an out-of-pocket limit on your expenses.
Will you pay less if you use a network provider?
Yes. See www.firsthealthlbp.com or call 1-800-226-5116 for a list of network providers.
This plan uses a provider network. You will pay less if you use a provider in the plan’s network. You will pay the most if you use an out-of-network provider, and you might receive a bill from a provider for the difference between the provider’s charge and what your plan pays (balance billing). Be aware your network provider might use an out-of-network provider for some services (such as lab work). Check with your provider before you get services.
Do you need a referral to see a specialist? No You can see the specialist you choose without a referral. NOTE: the only services by a specialist
that are covered are preventive services.
2 of 5 * For more information about limitations and exceptions, see the plan or policy document at www.fbg.com.
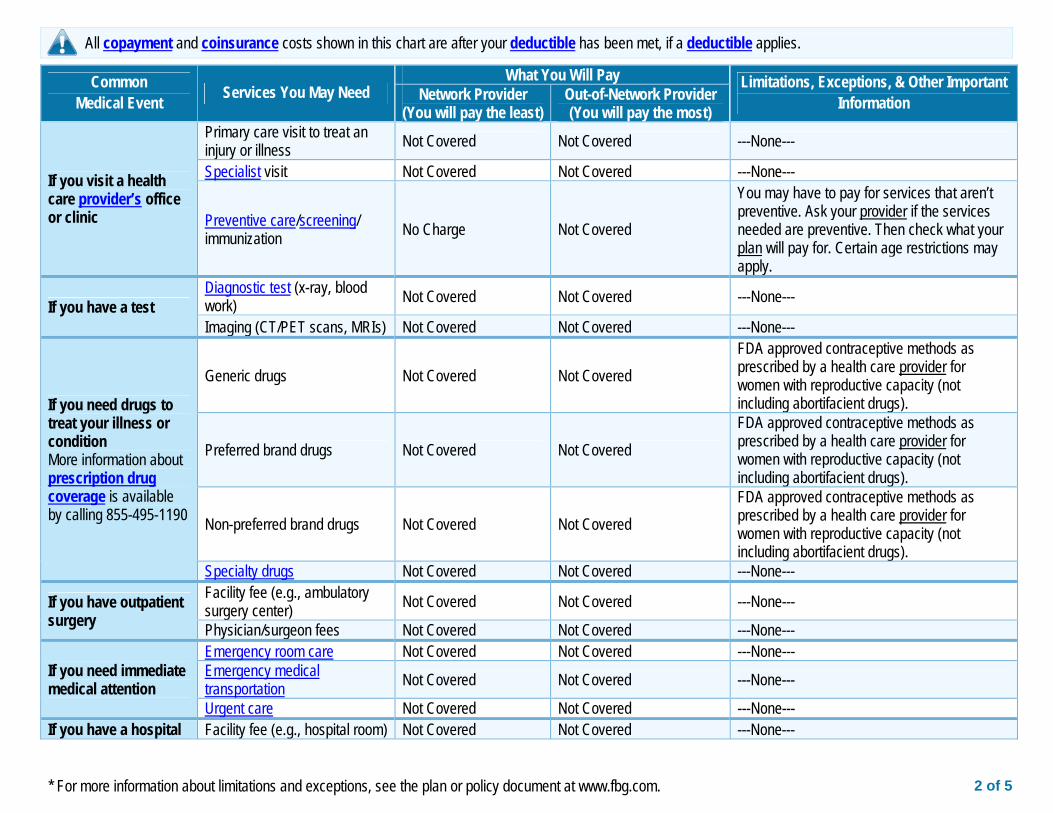
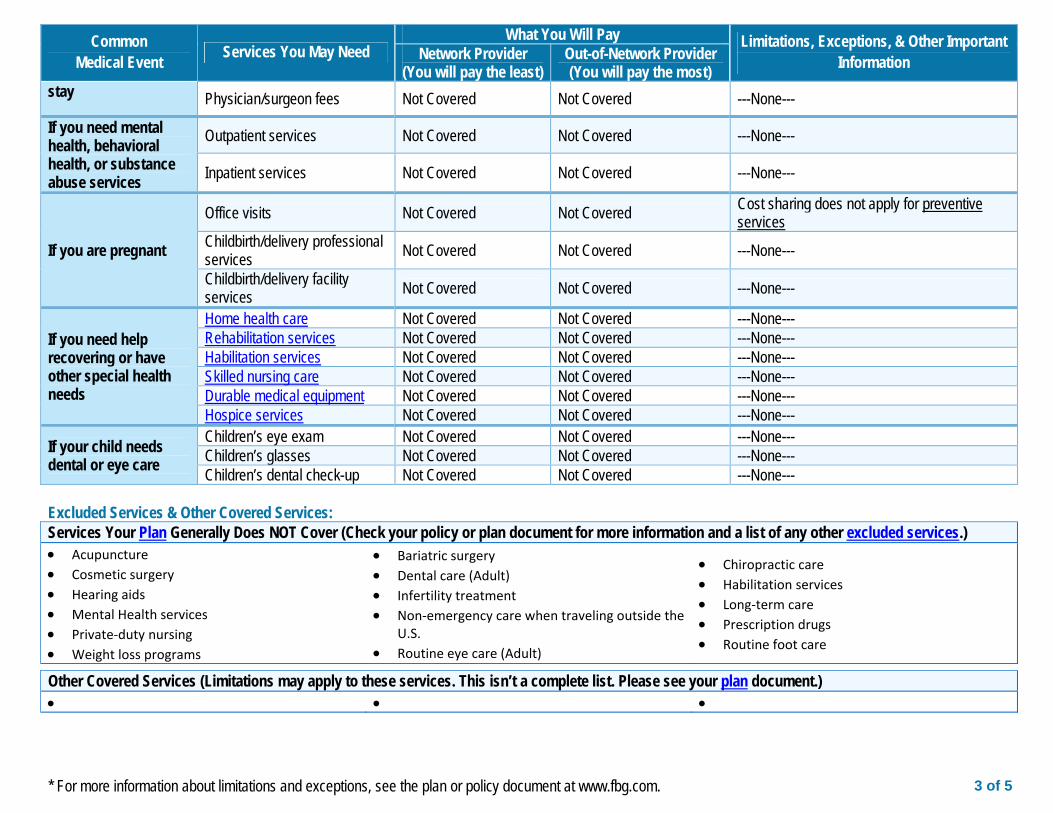
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies.
Common Medical Event Services You May Need
What You Will Pay Limitations, Exceptions, & Other Important Information Network Provider
(You will pay the least) Out-of-Network Provider (You will pay the most)
If you visit a health care provider’s office or clinic
Primary care visit to treat an injury or illness Not Covered Not Covered ---None---
Specialist visit Not Covered Not Covered ---None---
Preventive care/screening/ immunization No Charge Not Covered
You may have to pay for services that aren’t preventive. Ask your provider if the services needed are preventive. Then check what your plan will pay for. Certain age restrictions may apply.
If you have a test Diagnostic test (x-ray, blood work) Not Covered Not Covered ---None---
Imaging (CT/PET scans, MRIs) Not Covered Not Covered ---None---
If you need drugs to treat your illness or condition More information about prescription drug coverage is available by calling 855-495-1190
Generic drugs Not Covered Not Covered FDA approved contraceptive methods as prescribed by a health care provider for women with reproductive capacity (not including abortifacient drugs).
Preferred brand drugs Not Covered Not Covered FDA approved contraceptive methods as prescribed by a health care provider for women with reproductive capacity (not including abortifacient drugs).
Non-preferred brand drugs Not Covered Not Covered FDA approved contraceptive methods as prescribed by a health care provider for women with reproductive capacity (not including abortifacient drugs).
Specialty drugs Not Covered Not Covered ---None---
If you have outpatient surgery
Facility fee (e.g., ambulatory surgery center) Not Covered Not Covered ---None---
Physician/surgeon fees Not Covered Not Covered ---None---
If you need immediate medical attention
Emergency room care Not Covered Not Covered ---None--- Emergency medical transportation Not Covered Not Covered ---None---
Urgent care Not Covered Not Covered ---None--- If you have a hospital Facility fee (e.g., hospital room) Not Covered Not Covered ---None---
3 of 5 * For more information about limitations and exceptions, see the plan or policy document at www.fbg.com.
Common Medical Event Services You May Need
What You Will Pay Limitations, Exceptions, & Other Important Information Network Provider
(You will pay the least) Out-of-Network Provider (You will pay the most)
stay Physician/surgeon fees Not Covered Not Covered ---None---
If you need mental health, behavioral health, or substance abuse services
Outpatient services Not Covered Not Covered ---None---
Inpatient services Not Covered Not Covered ---None---
If you are pregnant
Office visits Not Covered Not Covered Cost sharing does not apply for preventive services
Childbirth/delivery professional services Not Covered Not Covered ---None---
Childbirth/delivery facility services Not Covered Not Covered ---None---
If you need help recovering or have other special health needs
Home health care Not Covered Not Covered ---None--- Rehabilitation services Not Covered Not Covered ---None--- Habilitation services Not Covered Not Covered ---None--- Skilled nursing care Not Covered Not Covered ---None--- Durable medical equipment Not Covered Not Covered ---None--- Hospice services Not Covered Not Covered ---None---
If your child needs dental or eye care
Children’s eye exam Not Covered Not Covered ---None--- Children’s glasses Not Covered Not Covered ---None--- Children’s dental check-up Not Covered Not Covered ---None---
Excluded Services & Other Covered Services: Services Your Plan Generally Does NOT Cover (Check your policy or plan document for more information and a list of any other excluded services.) Acupuncture Cosmetic surgery Hearing aids Mental Health services Private‐duty nursing Weight loss programs
Bariatric surgery Dental care (Adult) Infertility treatment Non‐emergency care when traveling outside the
U.S. Routine eye care (Adult)
Chiropractic care Habilitation services Long‐term care Prescription drugs Routine foot care
Other Covered Services (Limitations may apply to these services. This isn’t a complete list. Please see your plan document.)
4 of 5 * For more information about limitations and exceptions, see the plan or policy document at www.fbg.com.
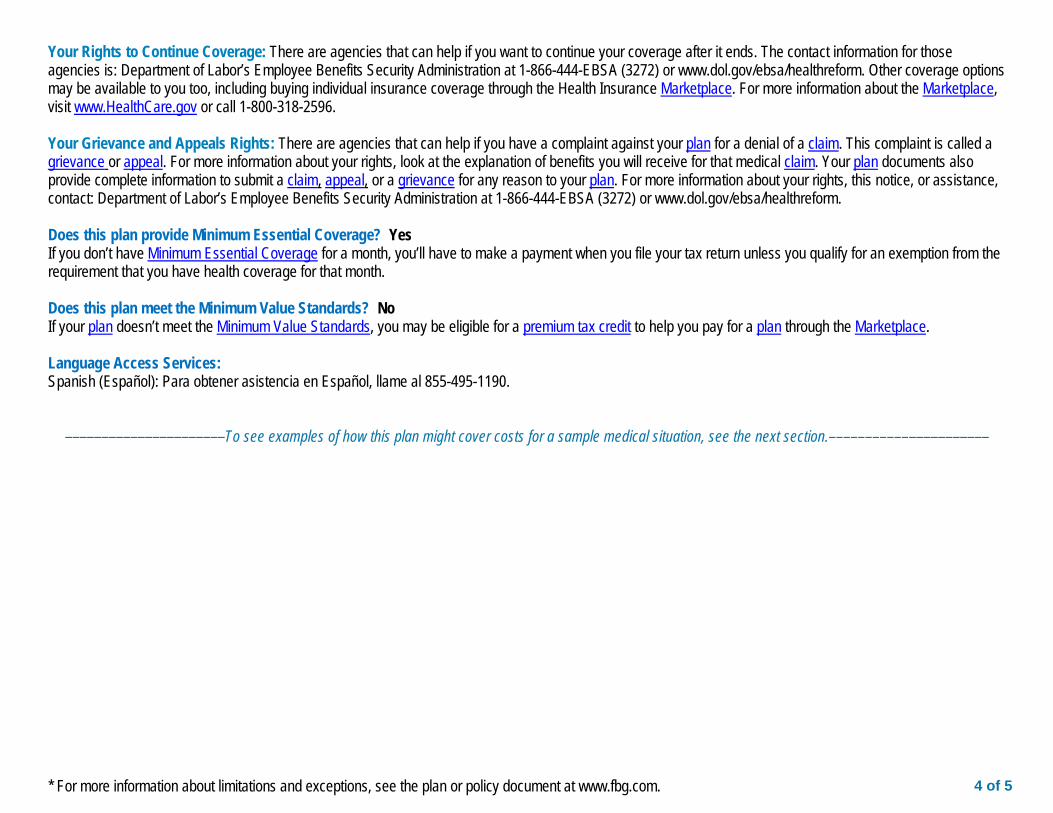
Your Rights to Continue Coverage: There are agencies that can help if you want to continue your coverage after it ends. The contact information for those agencies is: Department of Labor’s Employee Benefits Security Administration at 1-866-444-EBSA (3272) or www.dol.gov/ebsa/healthreform. Other coverage options may be available to you too, including buying individual insurance coverage through the Health Insurance Marketplace. For more information about the Marketplace, visit www.HealthCare.gov or call 1-800-318-2596. Your Grievance and Appeals Rights: There are agencies that can help if you have a complaint against your plan for a denial of a claim. This complaint is called a grievance or appeal. For more information about your rights, look at the explanation of benefits you will receive for that medical claim. Your plan documents also provide complete information to submit a claim, appeal, or a grievance for any reason to your plan. For more information about your rights, this notice, or assistance, contact: Department of Labor’s Employee Benefits Security Administration at 1-866-444-EBSA (3272) or www.dol.gov/ebsa/healthreform. Does this plan provide Minimum Essential Coverage? Yes If you don’t have Minimum Essential Coverage for a month, you’ll have to make a payment when you file your tax return unless you qualify for an exemption from the requirement that you have health coverage for that month. Does this plan meet the Minimum Value Standards? No If your plan doesn’t meet the Minimum Value Standards, you may be eligible for a premium tax credit to help you pay for a plan through the Marketplace. Language Access Services: Spanish (Español): Para obtener asistencia en Español, llame al 855-495-1190.
––––––––––––––––––––––To see examples of how this plan might cover costs for a sample medical situation, see the next section.––––––––––––––––––––––
5 of 5
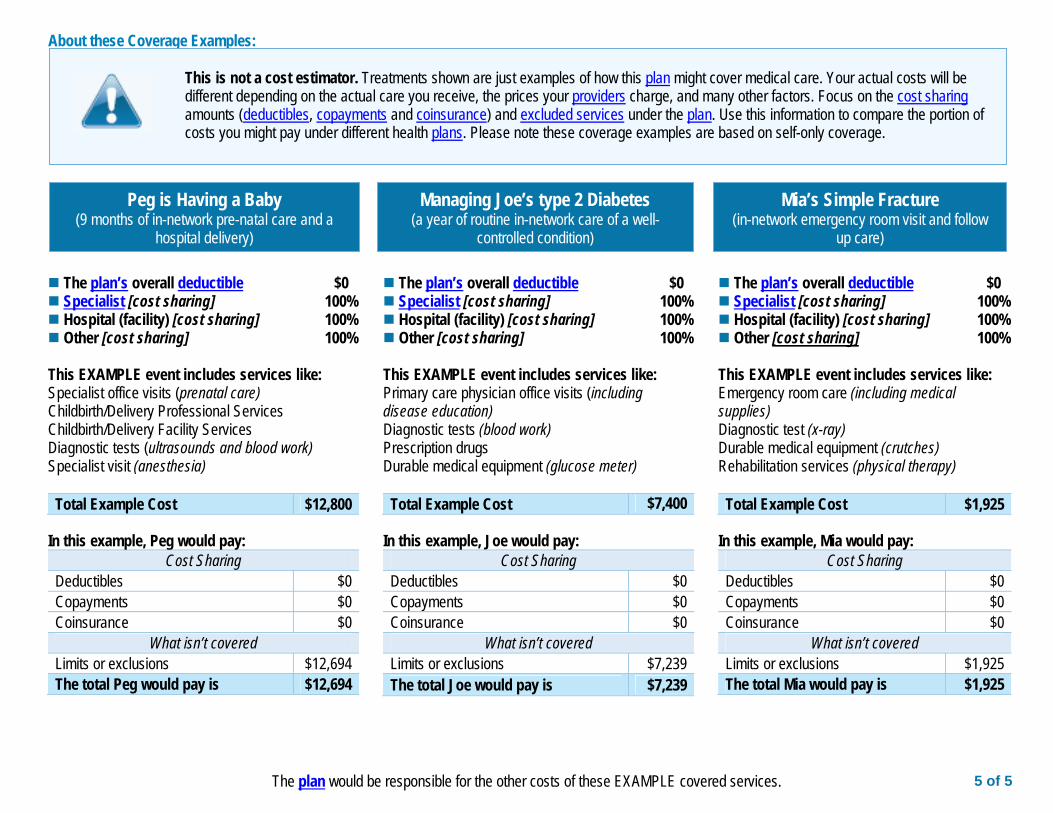
The plan would be responsible for the other costs of these EXAMPLE covered services.
Peg is Having a Baby (9 months of in-network pre-natal care and a
hospital delivery)
Mia’s Simple Fracture (in-network emergency room visit and follow
up care)
Managing Joe’s type 2 Diabetes (a year of routine in-network care of a well-
controlled condition)
The plan’s overall deductible $0 Specialist [cost sharing] 100% Hospital (facility) [cost sharing] 100% Other [cost sharing] 100% This EXAMPLE event includes services like: Specialist office visits (prenatal care) Childbirth/Delivery Professional Services Childbirth/Delivery Facility Services Diagnostic tests (ultrasounds and blood work) Specialist visit (anesthesia) Total Example Cost $12,800
In this example, Peg would pay:
Cost Sharing Deductibles $0 Copayments $0 Coinsurance $0
What isn’t covered Limits or exclusions $12,694 The total Peg would pay is $12,694
The plan’s overall deductible $0 Specialist [cost sharing] 100% Hospital (facility) [cost sharing] 100% Other [cost sharing] 100% This EXAMPLE event includes services like: Primary care physician office visits (including disease education) Diagnostic tests (blood work) Prescription drugs Durable medical equipment (glucose meter) Total Example Cost $7,400
In this example, Joe would pay:
Cost Sharing Deductibles $0 Copayments $0 Coinsurance $0
What isn’t covered Limits or exclusions $7,239 The total Joe would pay is $7,239
The plan’s overall deductible $0 Specialist [cost sharing] 100% Hospital (facility) [cost sharing] 100% Other [cost sharing] 100% This EXAMPLE event includes services like: Emergency room care (including medical supplies) Diagnostic test (x-ray) Durable medical equipment (crutches) Rehabilitation services (physical therapy) Total Example Cost $1,925
In this example, Mia would pay:
Cost Sharing Deductibles $0 Copayments $0 Coinsurance $0
What isn’t covered Limits or exclusions $1,925 The total Mia would pay is $1,925
About these Coverage Examples:
This is not a cost estimator. Treatments shown are just examples of how this plan might cover medical care. Your actual costs will be different depending on the actual care you receive, the prices your providers charge, and many other factors. Focus on the cost sharing amounts (deductibles, copayments and coinsurance) and excluded services under the plan. Use this information to compare the portion of costs you might pay under different health plans. Please note these coverage examples are based on self-only coverage.
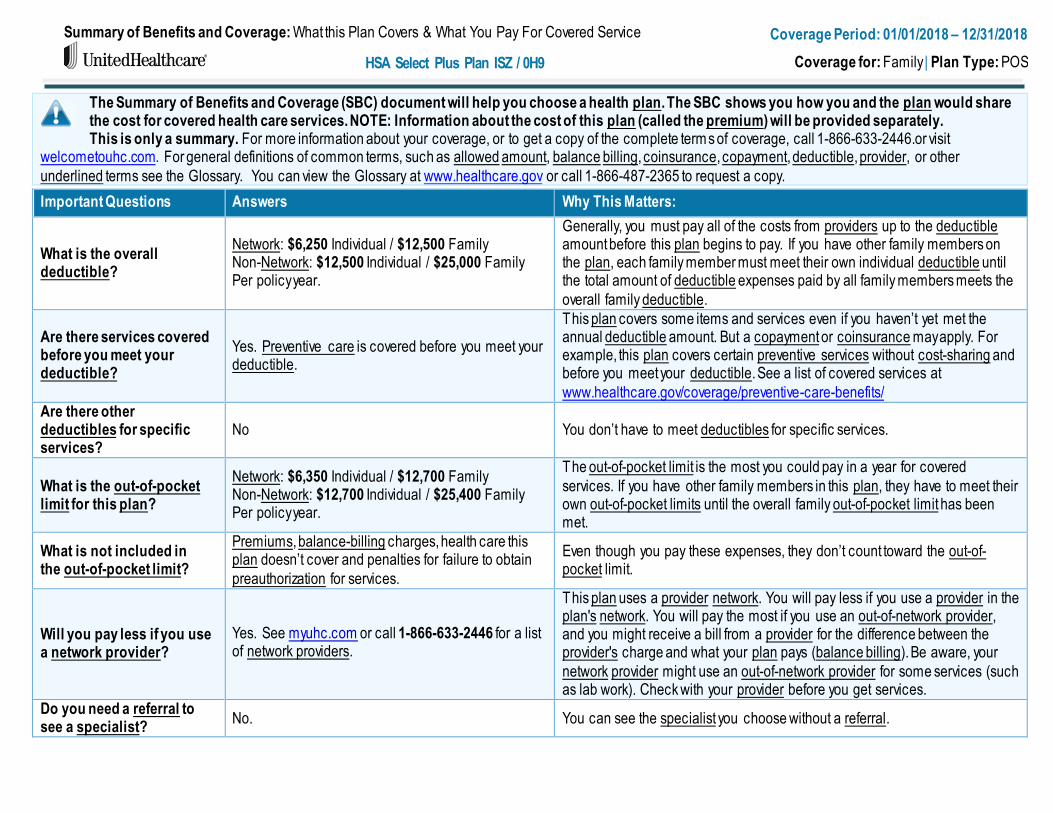
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Service
HSA Select Plus Plan ISZ / 0H9
Coverage Period: 01/01/2018 – 12/31/2018
Coverage for: Family | Plan Type: POS
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about the cost of this plan (called the premium) will be provided separately. This is only a summary. For more information about your coverage, or to get a copy of the complete terms of coverage, call 1-866-633-2446.or visit
welcometouhc.com. For general definitions of common terms, such as allowed amount, balance billing, coinsurance, copayment, deductible, provider, or other
underlined terms see the Glossary. You can view the Glossary at www.healthcare.gov or call 1-866-487-2365 to request a copy.
Important Questions Answers Why This Matters:
What is the overall deductible?
Network: $6,250 Individual / $12,500 Family Non-Network: $12,500 Individual / $25,000 Family Per policy year.
Generally, you must pay all of the costs from providers up to the deductible amount before this plan begins to pay. If you have other family members on the plan, each family member must meet their own individual deductible until the total amount of deductible expenses paid by all family members meets the
overall family deductible.
Are there services covered before you meet your deductible?
Yes. Preventive care is covered before you meet your deductible.
This plan covers some items and services even if you haven’t yet met the annual deductible amount. But a copayment or coinsurance may apply. For example, this plan covers certain preventive services without cost-sharing and before you meet your deductible. See a list of covered services at
www.healthcare.gov/coverage/preventive-care-benefits/
Are there other deductibles for specific services?
No You don’t have to meet deductibles for specific services.
What is the out-of-pocket limit for this plan?
Network: $6,350 Individual / $12,700 Family Non-Network: $12,700 Individual / $25,400 Family Per policy year.
The out-of-pocket limit is the most you could pay in a year for covered
services. If you have other family members in this plan, they have to meet their own out-of-pocket limits until the overall family out-of-pocket limit has been met.
What is not included in the out-of-pocket limit?
Premiums, balance-billing charges, health care this plan doesn’t cover and penalties for failure to obtain
preauthorization for services.
Even though you pay these expenses, they don’t count toward the out-of-pocket limit.
Will you pay less if you use a network provider?
Yes. See myuhc.com or call 1-866-633-2446 for a list of network providers.
This plan uses a provider network. You will pay less if you use a provider in the plan's network. You will pay the most if you use an out-of-network provider, and you might receive a bill from a provider for the difference between the provider's charge and what your plan pays (balance billing). Be aware, your
network provider might use an out-of-network provider for some services (such as lab work). Check with your provider before you get services.
Do you need a referral to see a specialist?
No. You can see the specialist you choose without a referral.
* For more information about limitations and exceptions, see the plan or policy document at welcometouhc.com. 2 of 6
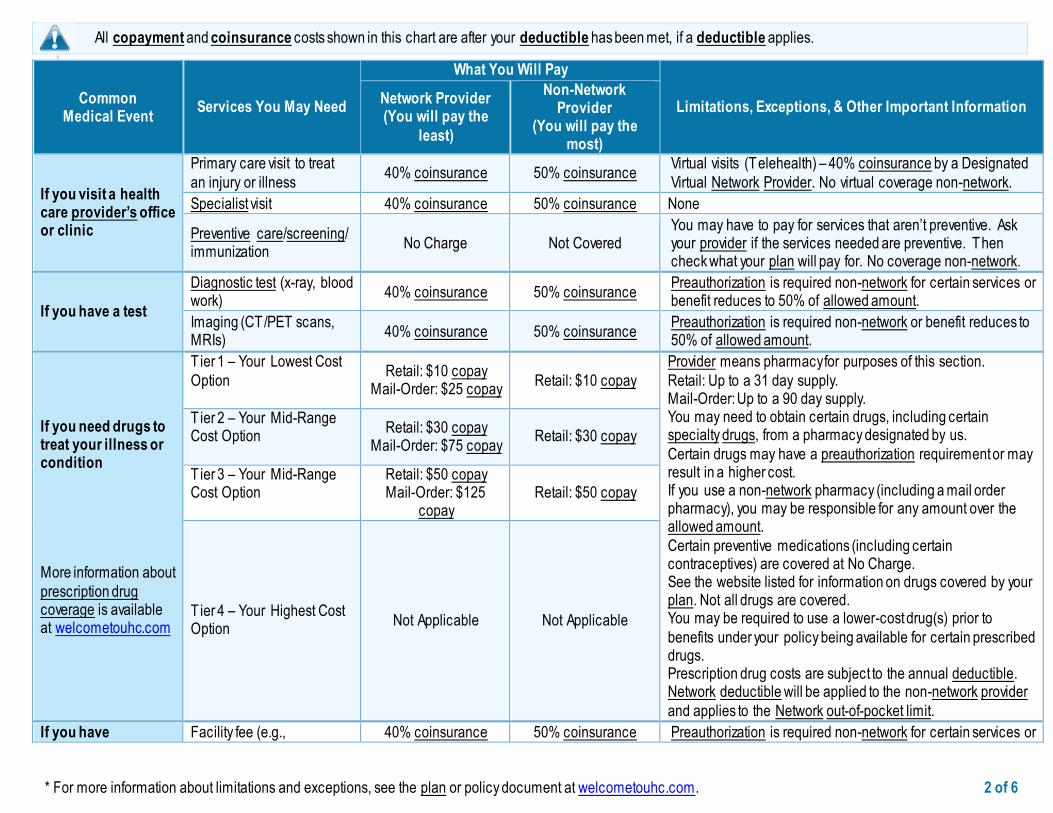
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies.
i
Common Medical Event
Services You May Need
What You Will Pay
Limitations, Exceptions, & Other Important Information Network Provider (You will pay the
least)
Non-Network Provider
(You will pay the most)
If you visit a health care provider’s office or clinic
Primary care visit to treat
an injury or illness 40% coinsurance 50% coinsurance
Virtual visits (Telehealth) – 40% coinsurance by a Designated
Virtual Network Provider. No virtual coverage non-network.
Specialist visit 40% coinsurance 50% coinsurance None
Preventive care/screening/ immunization
No Charge Not Covered You may have to pay for services that aren’t preventive. Ask your provider if the services needed are preventive. Then check what your plan will pay for. No coverage non-network.
If you have a test
Diagnostic test (x-ray, blood work)
40% coinsurance 50% coinsurance Preauthorization is required non-network for certain services or benefit reduces to 50% of allowed amount.
Imaging (CT/PET scans, MRIs)
40% coinsurance 50% coinsurance Preauthorization is required non-network or benefit reduces to 50% of allowed amount.
If you need drugs to treat your illness or condition
More information about
prescription drug coverage is available at welcometouhc.com
Tier 1 – Your Lowest Cost
Option
Retail: $10 copay Mail-Order: $25 copay
Retail: $10 copay
Provider means pharmacy for purposes of this section.
Retail: Up to a 31 day supply. Mail-Order: Up to a 90 day supply. You may need to obtain certain drugs, including certain specialty drugs, from a pharmacy designated by us.
Certain drugs may have a preauthorization requirement or may result in a higher cost. If you use a non-network pharmacy (including a mail order pharmacy), you may be responsible for any amount over the allowed amount.
Certain preventive medications (including certain contraceptives) are covered at No Charge. See the website listed for information on drugs covered by your plan. Not all drugs are covered. You may be required to use a lower-cost drug(s) prior to
benefits under your policy being available for certain prescribed drugs. Prescription drug costs are subject to the annual deductible. Network deductible will be applied to the non-network provider
and applies to the Network out-of-pocket limit.
T ier 2 – Your Mid-Range Cost Option
Retail: $30 copay Mail-Order: $75 copay
Retail: $30 copay
T ier 3 – Your Mid-Range Cost Option
Retail: $50 copay Mail-Order: $125
copay Retail: $50 copay
T ier 4 – Your Highest Cost Option
Not Applicable Not Applicable
If you have Facility fee (e.g., 40% coinsurance 50% coinsurance Preauthorization is required non-network for certain services or
* For more information about limitations and exceptions, see the plan or policy document at welcometouhc.com. 3 of 6
Common Medical Event
Services You May Need
What You Will Pay
Limitations, Exceptions, & Other Important Information Network Provider (You will pay the
least)
Non-Network
Provider (You will pay the
most)
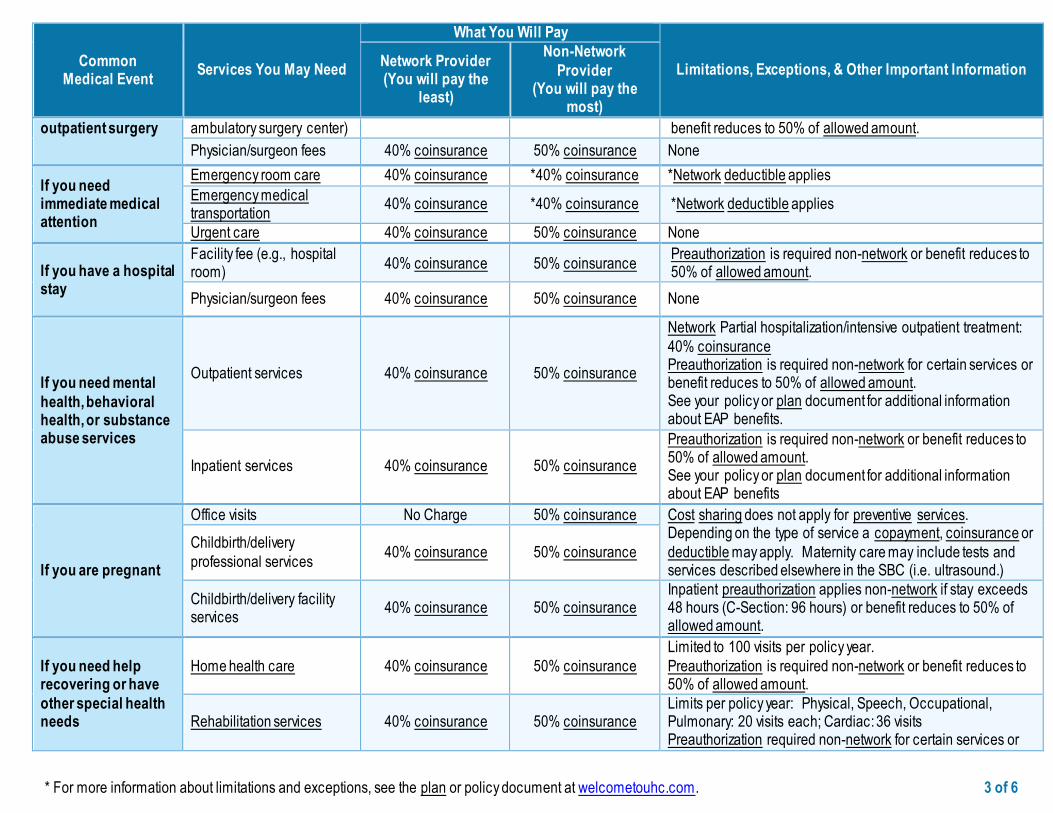
outpatient surgery ambulatory surgery center) benefit reduces to 50% of allowed amount.
Physician/surgeon fees 40% coinsurance 50% coinsurance None
If you need immediate medical attention
Emergency room care 40% coinsurance *40% coinsurance *Network deductible applies
Emergency medical transportation
40% coinsurance *40% coinsurance *Network deductible applies
Urgent care 40% coinsurance 50% coinsurance None
If you have a hospital stay
Facility fee (e.g., hospital room)
40% coinsurance 50% coinsurance Preauthorization is required non-network or benefit reduces to 50% of allowed amount.
Physician/surgeon fees 40% coinsurance 50% coinsurance None
If you need mental
health, behavioral health, or substance abuse services
Outpatient services 40% coinsurance 50% coinsurance
Network Partial hospitalization/intensive outpatient treatment:
40% coinsurance Preauthorization is required non-network for certain services or benefit reduces to 50% of allowed amount. See your policy or plan document for additional information about EAP benefits.
Inpatient services 40% coinsurance 50% coinsurance
Preauthorization is required non-network or benefit reduces to 50% of allowed amount. See your policy or plan document for additional information about EAP benefits
If you are pregnant
Office visits No Charge 50% coinsurance Cost sharing does not apply for preventive services. Depending on the type of service a copayment, coinsurance or
deductible may apply. Maternity care may include tests and services described elsewhere in the SBC (i.e. ultrasound.)
Childbirth/delivery
professional services 40% coinsurance 50% coinsurance
Childbirth/delivery facility services
40% coinsurance 50% coinsurance Inpatient preauthorization applies non-network if stay exceeds 48 hours (C-Section: 96 hours) or benefit reduces to 50% of allowed amount.
If you need help recovering or have
other special health needs
Home health care 40% coinsurance 50% coinsurance
Limited to 100 visits per policy year.
Preauthorization is required non-network or benefit reduces to 50% of allowed amount.
Rehabilitation services 40% coinsurance 50% coinsurance Limits per policy year: Physical, Speech, Occupational, Pulmonary: 20 visits each; Cardiac: 36 visits Preauthorization required non-network for certain services or
* For more information about limitations and exceptions, see the plan or policy document at welcometouhc.com. 4 of 6
Common Medical Event
Services You May Need
What You Will Pay
Limitations, Exceptions, & Other Important Information Network Provider (You will pay the
least)
Non-Network
Provider (You will pay the
most)
benefit reduces to 50% of allowed amount.
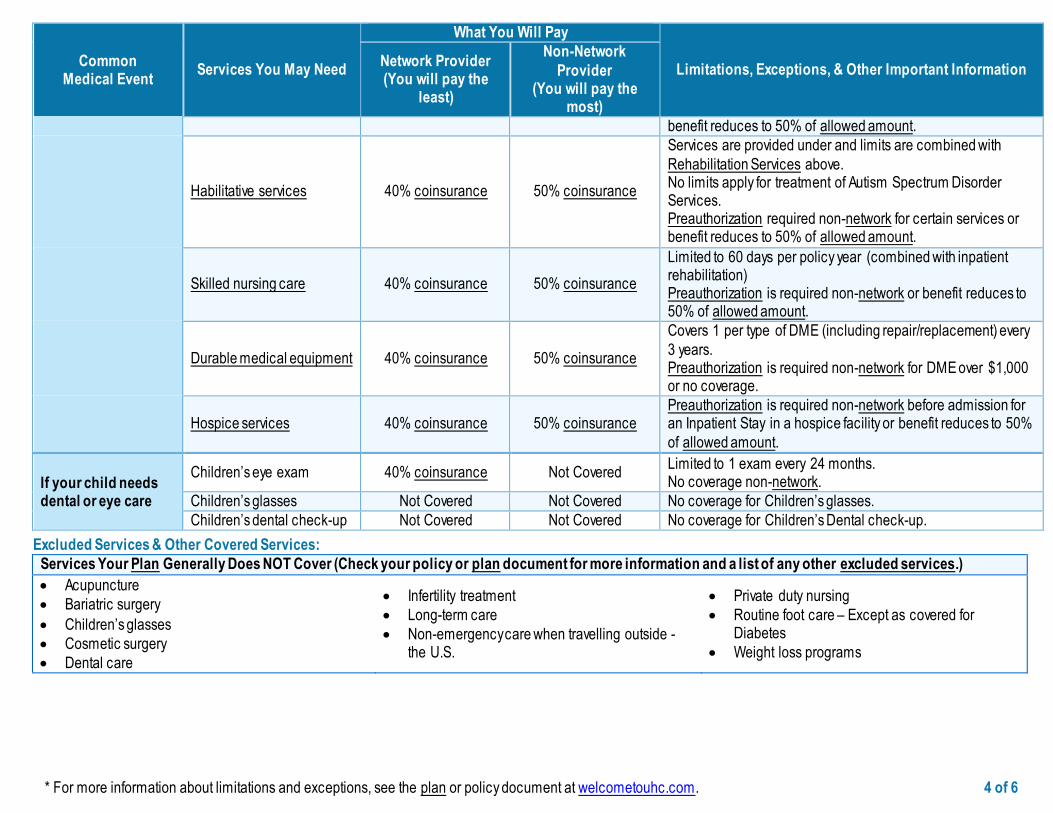
Habilitative services 40% coinsurance 50% coinsurance
Services are provided under and limits are combined with
Rehabilitation Services above. No limits apply for treatment of Autism Spectrum Disorder Services. Preauthorization required non-network for certain services or benefit reduces to 50% of allowed amount.
Skilled nursing care 40% coinsurance 50% coinsurance
Limited to 60 days per policy year (combined with inpatient rehabilitation) Preauthorization is required non-network or benefit reduces to 50% of allowed amount.
Durable medical equipment 40% coinsurance 50% coinsurance
Covers 1 per type of DME (including repair/replacement) every
3 years. Preauthorization is required non-network for DME over $1,000 or no coverage.
Hospice services 40% coinsurance 50% coinsurance Preauthorization is required non-network before admission for an Inpatient Stay in a hospice facility or benefit reduces to 50%
of allowed amount.
If your child needs dental or eye care
Children’s eye exam 40% coinsurance Not Covered Limited to 1 exam every 24 months. No coverage non-network.
Children’s glasses Not Covered Not Covered No coverage for Children’s glasses.
Children’s dental check-up Not Covered Not Covered No coverage for Children’s Dental check-up.
Excluded Services & Other Covered Services:
Services Your Plan Generally Does NOT Cover (Check your policy or plan document for more information and a list of any other excluded services.)
Acupuncture
Bariatric surgery
Children’s glasses
Cosmetic surgery
Dental care
Infertility treatment
Long-term care
Non-emergency care when travelling outside - the U.S.
Private duty nursing
Routine foot care – Except as covered for Diabetes
Weight loss programs
* For more information about limitations and exceptions, see the plan or policy document at welcometouhc.com. 5 of 6
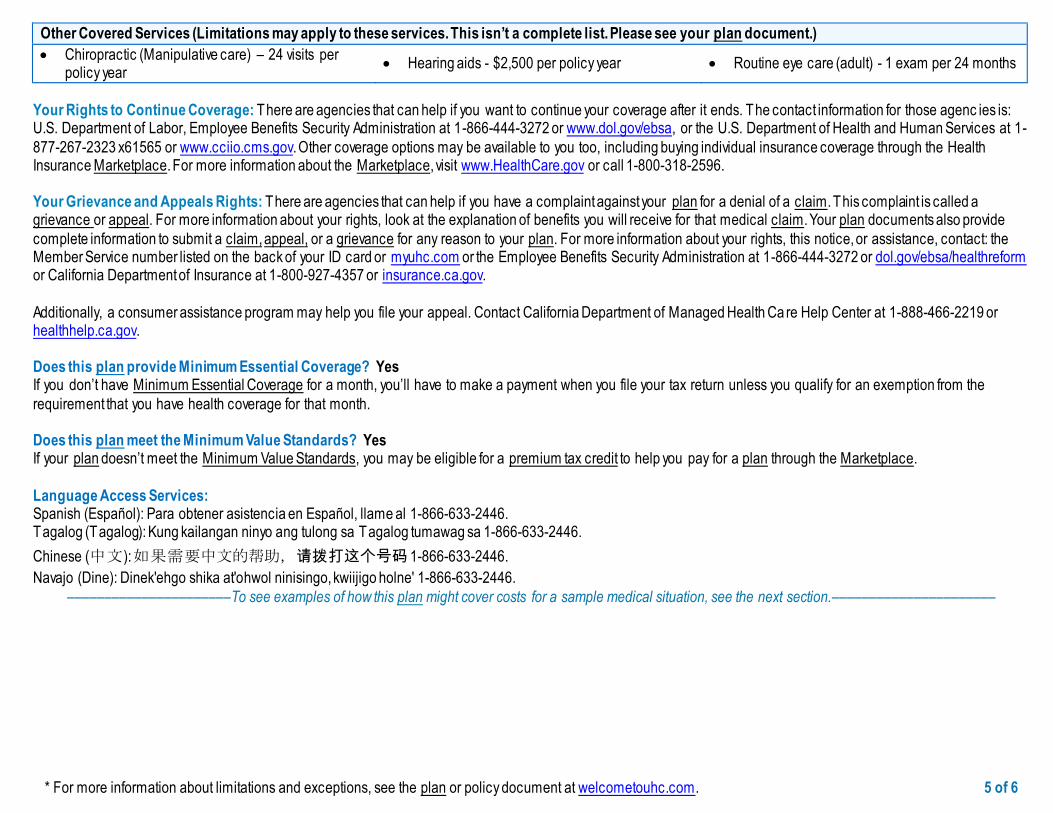
Other Covered Services (Limitations may apply to these services. This isn’t a complete list. Please see your plan document.)
Chiropractic (Manipulative care) – 24 visits per policy year
Hearing aids - $2,500 per policy year Routine eye care (adult) - 1 exam per 24 months
Your Rights to Continue Coverage: There are agencies that can help if you want to continue your coverage after it ends. The contact information for those agenc ies is: U.S. Department of Labor, Employee Benefits Security Administration at 1-866-444-3272 or www.dol.gov/ebsa, or the U.S. Department of Health and Human Services at 1-
877-267-2323 x61565 or www.cciio.cms.gov. Other coverage options may be available to you too, including buying individual insurance coverage through the Health Insurance Marketplace. For more information about the Marketplace, visit www.HealthCare.gov or call 1-800-318-2596. Your Grievance and Appeals Rights: There are agencies that can help if you have a complaint against your plan for a denial of a claim. This complaint is called a grievance or appeal. For more information about your rights, look at the explanation of benefits you will receive for that medical claim. Your plan documents also provide
complete information to submit a claim, appeal, or a grievance for any reason to your plan. For more information about your rights, this notice, or assistance, contact: the Member Service number listed on the back of your ID card or myuhc.com or the Employee Benefits Security Administration at 1-866-444-3272 or dol.gov/ebsa/healthreform or California Department of Insurance at 1-800-927-4357 or insurance.ca.gov.
Additionally, a consumer assistance program may help you file your appeal. Contact California Department of Managed Health Ca re Help Center at 1-888-466-2219 or healthhelp.ca.gov. Does this plan provide Minimum Essential Coverage? Yes If you don’t have Minimum Essential Coverage for a month, you’ll have to make a payment when you file your tax return unless you qualify for an exemption from the
requirement that you have health coverage for that month. Does this plan meet the Minimum Value Standards? Yes If your plan doesn’t meet the Minimum Value Standards, you may be eligible for a premium tax credit to help you pay for a plan through the Marketplace.
Language Access Services: Spanish (Español): Para obtener asistencia en Español, llame al 1-866-633-2446. Tagalog (Tagalog): Kung kailangan ninyo ang tulong sa Tagalog tumawag sa 1-866-633-2446.
Chinese (中文): 如果需要中文的帮助,请拨打这个号码 1-866-633-2446.
Navajo (Dine): Dinek'ehgo shika at'ohwol ninisingo, kwiijigo holne' 1-866-633-2446.
––––––––––––––––––––––To see examples of how this plan might cover costs for a sample medical situation, see the next section.––––––––––––––––––––––
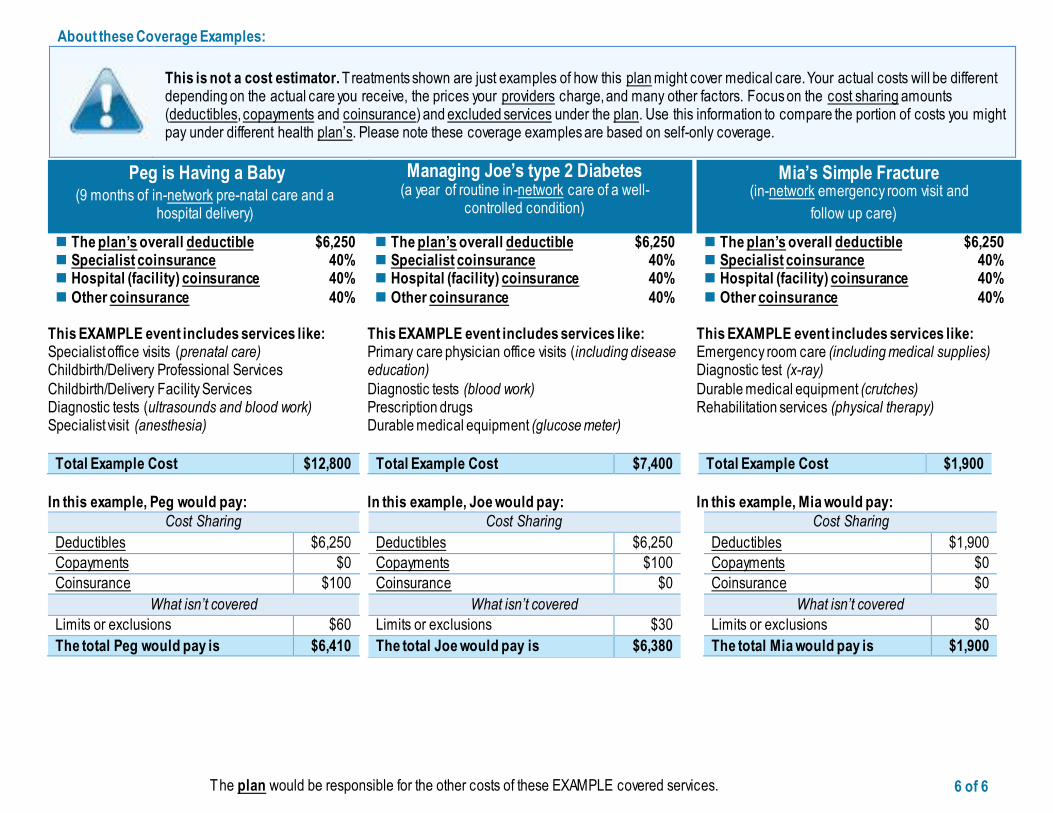
The plan would be responsible for the other costs of these EXAMPLE covered services. 6 of 6
About these Coverage Examples:
This is not a cost estimator. Treatments shown are just examples of how this plan might cover medical care. Your actual costs will be different depending on the actual care you receive, the prices your providers charge, and many other factors. Focus on the cost sharing amounts (deductibles, copayments and coinsurance) and excluded services under the plan. Use this information to compare the portion of costs you might pay under different health plan’s. Please note these coverage examples are based on self-only coverage.
Peg is Having a Baby (9 months of in-network pre-natal care and a
hospital delivery)
The plan’s overall deductible $6,250 Specialist coinsurance 40% Hospital (facility) coinsurance 40%
Other coinsurance 40% This EXAMPLE event includes services like: Specialist office visits (prenatal care) Childbirth/Delivery Professional Services
Childbirth/Delivery Facility Services Diagnostic tests (ultrasounds and blood work) Specialist visit (anesthesia)
Total Example Cost $12,800
In this example, Peg would pay:
Cost Sharing
Deductibles $6,250
Copayments $0
Coinsurance $100
What isn’t covered
Limits or exclusions $60
The total Peg would pay is $6,410
Managing Joe’s type 2 Diabetes (a year of routine in-network care of a well-
controlled condition)
The plan’s overall deductible $6,250 Specialist coinsurance 40% Hospital (facility) coinsurance 40%
Other coinsurance 40% This EXAMPLE event includes services like: Primary care physician office visits (including disease education)
Diagnostic tests (blood work) Prescription drugs Durable medical equipment (glucose meter)
Total Example Cost $7,400
In this example, Joe would pay:
Cost Sharing
Deductibles $6,250
Copayments $100
Coinsurance $0
What isn’t covered
Limits or exclusions $30
The total Joe would pay is $6,380
Mia’s Simple Fracture (in-network emergency room visit and
follow up care)
The plan’s overall deductible $6,250 Specialist coinsurance 40% Hospital (facility) coinsurance 40%
Other coinsurance 40% This EXAMPLE event includes services like: Emergency room care (including medical supplies) Diagnostic test (x-ray)
Durable medical equipment (crutches) Rehabilitation services (physical therapy)
Total Example Cost $1,900
In this example, Mia would pay:
Cost Sharing
Deductibles $1,900
Copayments $0
Coinsurance $0
What isn’t covered
Limits or exclusions $0
The total Mia would pay is $1,900
We do not treat members differently because of sex, age, race, color, disability or national origin. If you think you were treated unfairly because of your sex, age, race, color, disability or national origin, you can send a complaint to the Civil
Rights Coordinator. Online: [email protected] Mail: Civil Rights Coordinator. UnitedHealthcare Civil Rights Grievance. P.O. Box 30608 Salt Lake City, UTAH 84130
You must send the complaint within 60 days of when you found out about it. A decision will be sent to you within 30 days. If you disagree with the decision, you have 15 days to ask us to look at it again. If you need help with your complaint, please call the toll-free number listed within this Summary of Benefits and Coverage (SBC) , TTY 711, Monday through Friday, 8 a.m. to 8 p.m.
You can also file a complaint with the U.S. Dept. of Health and Human Services. Online: https://ocrportal.hhs.gov/ocr/portal/lobby.jsf Complaint forms are available at http://www.hhs.gov/ocr/office/file/index.html.
Phone: Toll-free 1-800-368-1019, 800-537-7697 (TDD) Mail: U.S. Dept. of Health and Human Services. 200 Independence Avenue, SW Room 509F, HHH Building Washington, D.C. 20201 We provide free services to help you communicate with us. Such as, letters in other languages or large print. Or, you can ask for an interpreter. To
ask for help, please call the number contained within this Summary of Benefits and Coverage (SBC) , TTY 711, Monday through Friday, 8 a.m. to 8 p.m.