Embed Size (px)
Citation preview
ANNUAL BENEFITS OPEN ENROLLMENT PACKET - MyChoice Dear McLaren Colleague:
McLaren’s Benefits Open Enrollment for 2022 is Monday, November 1, 2021 through Monday, November 15, 2021 at 5 p.m.
For this year’s Open Enrollment, you MUST participate in Open Enrollment if: - You want to enroll or continue in a Flexible Spending Account in plan year 2022. - You want to enroll or continue dental and/or vision coverage for a dependent who is currently 18 – 22 years old and is a full-time student and your tax dependent. The Dependent Child Certification Form can be found in your Open Enrollment Guide. The Dependent Child Certification Form MUST be submitted no later than Monday, November 15, 2021. - You want to change your medical, dental or vision plan. - You want to change who is covered on your medical, dental or vision plan. - You want to change your life insurance or long-term disability coverage, if eligible.
Open Enrollment materials included with this communication:
• Rate Sheet for medical, dental, vision plans, • Open Enrollment Guide and • Brochures for Critical Illness, Hospital Indemnity, Accident, and Whole Life Insurances.
Review your Open Enrollment materials before completing your online Open Enrollment session. IMPORTANT: You will need birth dates and social security numbers for dependents you wish to enroll. This year, if you do not participate in Open Enrollment, your benefits from 2021 will rollover into 2022 (EXCEPT FOR Flexible Spending Accounts). If enrolling dependent(s) for the first time, in addition to birth date(s) and social security number(s), the following documentation is required:
• SPOUSE – copy of marriage license • CHILD(REN) – copy of birth certificate, adoption documents, full guardianship documents, Dependent Child
Certification Forms
Required documentation and form(s) mentioned above must be provided to your Human Resources Department, your Benefits Analyst or uploaded into the Dependent/Beneficiary Info area (located within Employee Self Service of PeopleSoft-MyHR) no later than 5:00 p.m., Monday, November 15, 2021. If you have any questions regarding Open Enrollment, contact a Benefit Communication Specialist for a telephonic appointment at https://go.oncehub.com/McLaren for appointments between November 1st and November 15th, call the Open Enrollment Call Center at 1-877-368-5789 from 9 a.m. to 6 p.m. (starting November 1st) or contact your Benefits Analyst or Human Resources Department. Sincerely, Corporate Benefits McLaren Corporate Human Resources
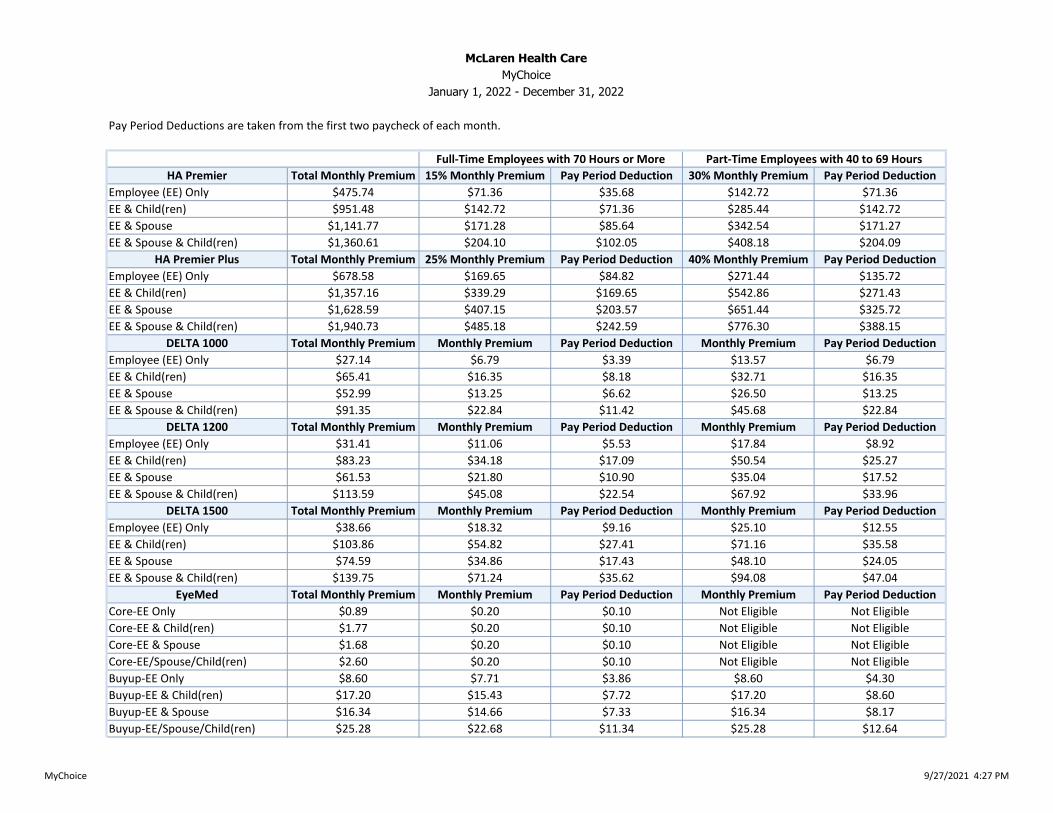
Pay Period Deductions are taken from the first two paycheck of each month.
HA Premier Total Monthly Premium 15% Monthly Premium Pay Period Deduction 30% Monthly Premium Pay Period Deduction
Employee (EE) Only $475.74 $71.36 $35.68 $142.72 $71.36
EE & Child(ren) $951.48 $142.72 $71.36 $285.44 $142.72
EE & Spouse $1,141.77 $171.28 $85.64 $342.54 $171.27
EE & Spouse & Child(ren) $1,360.61 $204.10 $102.05 $408.18 $204.09
HA Premier Plus Total Monthly Premium 25% Monthly Premium Pay Period Deduction 40% Monthly Premium Pay Period Deduction
Employee (EE) Only $678.58 $169.65 $84.82 $271.44 $135.72
EE & Child(ren) $1,357.16 $339.29 $169.65 $542.86 $271.43
EE & Spouse $1,628.59 $407.15 $203.57 $651.44 $325.72
EE & Spouse & Child(ren) $1,940.73 $485.18 $242.59 $776.30 $388.15
DELTA 1000 Total Monthly Premium Monthly Premium Pay Period Deduction Monthly Premium Pay Period Deduction
Employee (EE) Only $27.14 $6.79 $3.39 $13.57 $6.79
EE & Child(ren) $65.41 $16.35 $8.18 $32.71 $16.35
EE & Spouse $52.99 $13.25 $6.62 $26.50 $13.25
EE & Spouse & Child(ren) $91.35 $22.84 $11.42 $45.68 $22.84
DELTA 1200 Total Monthly Premium Monthly Premium Pay Period Deduction Monthly Premium Pay Period Deduction
Employee (EE) Only $31.41 $11.06 $5.53 $17.84 $8.92
EE & Child(ren) $83.23 $34.18 $17.09 $50.54 $25.27
EE & Spouse $61.53 $21.80 $10.90 $35.04 $17.52
EE & Spouse & Child(ren) $113.59 $45.08 $22.54 $67.92 $33.96
DELTA 1500 Total Monthly Premium Monthly Premium Pay Period Deduction Monthly Premium Pay Period Deduction
Employee (EE) Only $38.66 $18.32 $9.16 $25.10 $12.55
EE & Child(ren) $103.86 $54.82 $27.41 $71.16 $35.58
EE & Spouse $74.59 $34.86 $17.43 $48.10 $24.05
EE & Spouse & Child(ren) $139.75 $71.24 $35.62 $94.08 $47.04
EyeMed Total Monthly Premium Monthly Premium Pay Period Deduction Monthly Premium Pay Period Deduction
Core-EE Only $0.89 $0.20 $0.10 Not Eligible Not Eligible
Core-EE & Child(ren) $1.77 $0.20 $0.10 Not Eligible Not Eligible
Core-EE & Spouse $1.68 $0.20 $0.10 Not Eligible Not Eligible
Core-EE/Spouse/Child(ren) $2.60 $0.20 $0.10 Not Eligible Not Eligible
Buyup-EE Only $8.60 $7.71 $3.86 $8.60 $4.30
Buyup-EE & Child(ren) $17.20 $15.43 $7.72 $17.20 $8.60
Buyup-EE & Spouse $16.34 $14.66 $7.33 $16.34 $8.17
Buyup-EE/Spouse/Child(ren) $25.28 $22.68 $11.34 $25.28 $12.64
Full-Time Employees with 70 Hours or More Part-Time Employees with 40 to 69 Hours
McLaren Health Care
MyChoice
January 1, 2022 - December 31, 2022
MyChoice 9/27/2021 4:27 PM
DOING WHAT’S BEST.®
2022 Open Enrollment GuideMyCHOICE
2
2022 MyChoiceOpen Enrollment Guide
WELCOME TO McLAREN’S BENEFITS OPEN ENROLLMENT FOR 2022McLaren’s annual Benefits Open Enrollment will be held Monday, November 1 through Monday, November 15, 2021. This is the time of the year when benefits-eligible McLaren employees can re-evaluate their benefits needs and make changes to their benefits selections. This Open Enrollment Guide contains information about the benefits options available for benefits-eligible employees in the 2022 plan year. Please review this Open Enrollment Guide before completing your Open Enrollment.
IMPORTANT NOTE: This is a summary of your benefits options provided by McLaren Health Care Corporation. This information is meant to be a general guide. If there is a difference between the information presented in this benefits enrollment guide and the contents of the official plan documents, the Plan documents will prevail.
2
3
2022 MyChoiceOpen Enrollment Guide
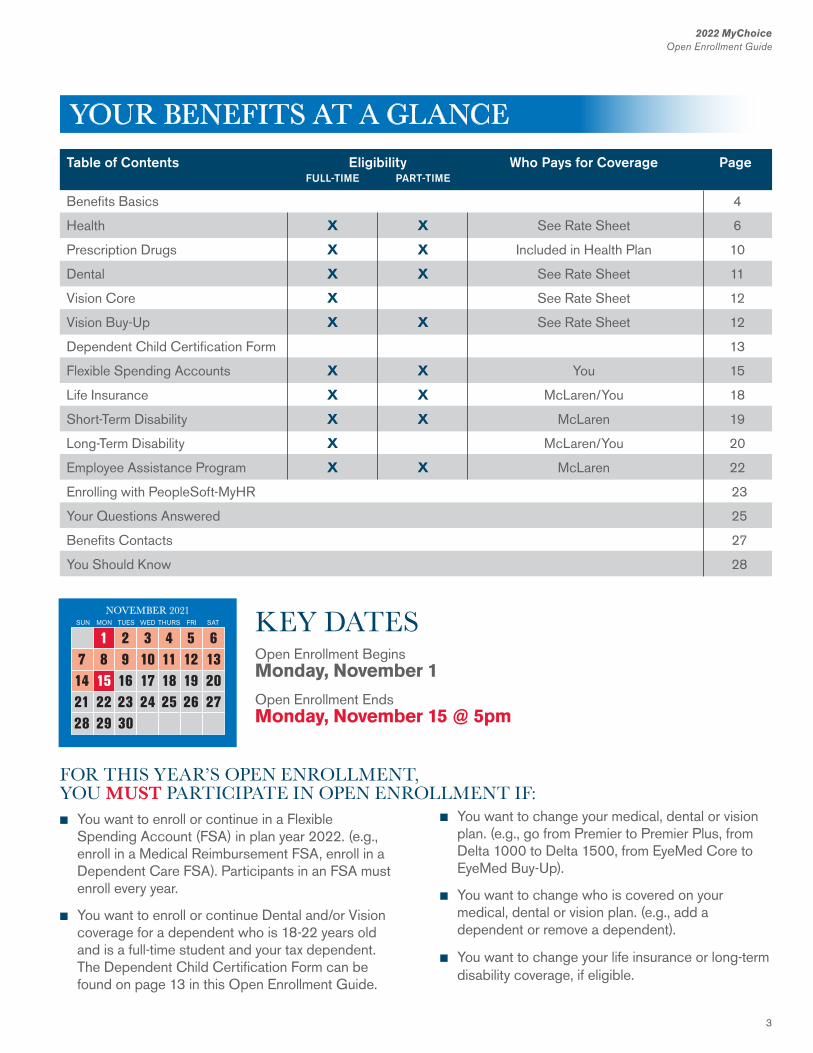
KEY DATESOpen Enrollment Begins Monday, November 1
Open Enrollment Ends Monday, November 15 @ 5pm
n You want to enroll or continue in a Flexible Spending Account (FSA) in plan year 2022. (e.g., enroll in a Medical Reimbursement FSA, enroll in a Dependent Care FSA). Participants in an FSA must enroll every year.
n You want to enroll or continue Dental and/or Vision coverage for a dependent who is 18-22 years old and is a full-time student and your tax dependent. The Dependent Child Certification Form can be found on page 13 in this Open Enrollment Guide.
Table of Contents Eligibility Who Pays for Coverage Page FULL-TIME PART-TIME
Benefits Basics 4
Health X X See Rate Sheet 6
Prescription Drugs X X Included in Health Plan 10
Dental X X See Rate Sheet 11
Vision Core X See Rate Sheet 12
Vision Buy-Up X X See Rate Sheet 12
Dependent Child Certification Form 13
Flexible Spending Accounts X X You 15
Life Insurance X X McLaren/You 18
Short-Term Disability X X McLaren 19
Long-Term Disability X McLaren/You 20
Employee Assistance Program X X McLaren 22
Enrolling with PeopleSoft-MyHR 23
Your Questions Answered 25
Benefits Contacts 27
You Should Know 28
n You want to change your medical, dental or vision plan. (e.g., go from Premier to Premier Plus, from Delta 1000 to Delta 1500, from EyeMed Core to EyeMed Buy-Up).
n You want to change who is covered on your medical, dental or vision plan. (e.g., add a dependent or remove a dependent).
n You want to change your life insurance or long-term disability coverage, if eligible.
FOR THIS YEAR’S OPEN ENROLLMENT,YOU MUST PARTICIPATE IN OPEN ENROLLMENT IF:
YOUR BENEFITS AT A GLANCE
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
SUN MON TUES WED THURS FRI SAT
NOVEMBER 2021

4
2022 MyChoiceOpen Enrollment Guide
4
2022 MyChoiceOpen Enrollment Guide
EligibilityFor YouFull-time and part-time employees are eligible to participate in the health, dental, and vision plans as well as the other benefits described in this enrollment guide, unless otherwise indicated. Full-time employees are regularly scheduled to work 70 or more hours per pay period. Part-time employees are regularly scheduled to work 40 to 69 hours per pay period.
For your dependentsIf you are eligible for coverage, you can also enroll your eligible dependents for health, dental, vision, and voluntary life coverage.
Eligible dependents include:
n Your legal spouse
n Your children up to age 26 (for health) even if employed or married
n Your children up to age 23 (for dental and vision) if they are full-time students and tax dependents
n Your disabled children age 19 and over if not married and if disabled before age 19
Children include your natural children, stepchildren, adopted children, children placed for adoption, and children for whom you have legal guardianship. Dependent children do not include grandchildren or other family relations unless you have legal guardianship.
Eligibility DocumentationWhen you complete your online enrollment, you are required to provide documentation that supports the eligibility of your dependents. Supporting documentation includes, but is not limited to marriage and birth certificates, adoption certifications, social security numbers, Dependent Child Certification Forms, qualified domestic relations orders, qualified medical child support orders, physician certifications, federal income tax returns, divorce decrees, and order of separate maintenances.
If documentation is requested and you do not provide the documentation, you will not be allowed to enroll your dependents.
Note: A dependent eligibility audit may be conducted to:
n Update the records of all covered family members
n Confirm that each dependent is eligible for benefits under the rules of the plan
n Remove any ineligible dependents
EnrollmentGenerally, there are two times when you can enroll for benefits: when you first become eligible and during the annual benefits open enrollment. Each fall, Open Enrollment is held so you can make changes to your benefits elections for the upcoming calendar year. Coverage elected during Open Enrollment is effective January 1, 2022 through December 31, 2022.
BENEFITS BASICS
IMPORTANT NOTE: Dependent Child Certification for 2022 – Children who will be at least 18 years of age on December 31, 2021 and not more than 22 years of age on December 31, 2021, may be eligible for dental and vision coverage if they are full-time students and tax dependents. The “Dependent Child Certification Form” (found on page 13) that is included in this Open Enrollment Guide, must be completed and returned to Human Resources in order to complete dental and/or vision enrollments for these children.
5
2022 MyChoiceOpen Enrollment Guide
BENEFITS BASICS CONTINUED
IMPORTANT NOTE:Divorce/ Legal SeparationTo ensure that your former spouse can enroll in COBRA, your divorce or legal separation must be reported to Human Resources within 60 days of the divorce judgment or legal separation.
5
2022 MyChoiceOpen Enrollment Guide
Changing Your BenefitsOnce you enroll, your elections remain in effect for the entire calendar year. Because you pay for many of your benefits with pretax dollars, the IRS does not allow you to change your benefits elections during the year unless you experience a change in status event described below.
Change in status events include, but are not limited to:
n Birth, adoption, or placement for adoption of a child
n Marriage or annulment
n Divorce, legal separation (see important note)
n Gain or loss of coverage through your spouse’s employer
n A child’s gain or loss of eligibility status
n Death of a spouse or dependent child
n A change in work status that affects benefits eligibility (e.g., casual to full-time)
n A qualified medical child support order
n Eligibility for Medicare
n The start or end of a leave of absence
You have 30 days from the date of a change in status event to change your coverage. Any change to your benefits will be effective on the first of the month following the date of the change, provided you notify Human Resources within 30 days after the status event. Exceptions to this rule are marriage, birth and adoption, which are effective on the date of the event.
Paying for Your BenefitsYou and McLaren share the cost of many of your benefits. The rate sheet provided with this Open Enrollment guide shows your portion of the cost. For health, dental, vision, and flexible spending accounts benefits, you pay your contributions with pretax dollars. Paying with pretax dollars reduces your taxable income, so you pay less in taxes.
When Coverage EndsUnless otherwise stated, your benefits coverage ends on the last day of the month in which the event occurs.
Coverage for your dependents ends on the earliest of the following dates:
n The day your coverage ends (or)
n End of the month your dependent no longer meets eligibility requirements (in most situations)
COBRAIf your coverage ends, you may be able to continue your health, dental, vision, and medical reimbursement FSA coverage through COBRA.
See your summary plan description or Corporate Benefits for more information about COBRA coverage.
6
2022 MyChoiceOpen Enrollment Guide
6
How the Plan WorksMyChoice provides two McLaren Health Advantage (MHA) PPO health plans:n MHA Premier andn MHA Premier Plus
(A BlueCross BlueShield traditional plan option is available to employees who live outside the McLaren Health Advantage network area. Contact Corporate Benefits to see if you qualify.)
Both McLaren Health Advantage PPOs cover the same health care services, including preventive care, office visits, hospital services, emergency care, and prescription drugs, including but not limited to those listed in the charts on pages 8 and 9; however, your coinsurance, copays, deductibles and out-of-pocket maximum costs may differ significantly depending on the health plan you choose and the providers you seek treatment from.
NOTE: You receive the highest level of benefits when you use McLaren’s domestic network or McLaren’s direct contracted network. Use the charts on pages 8 and 9 to compare your options.
Health Plan DefinitionsCoinsurance – Your share of the cost of a covered health care service, calculated as a percent (e.g., 10%) of the allowed amount for the service. You pay coinsurance plus any deductibles you owe. For example, if the health plan’s allowed amount for a covered service is $100 and you have met your deductible, your coinsurance payment of
10% is $10 (payable to that health care provider). The health plan would pay the remainder of the allowed amount.
Copay – A fixed dollar amount (e.g., $25) you pay for a covered health care service. The fixed amount can vary by type of covered health care service.
Deductible – The amount you owe for health care services, before your health plan begins to pay. For example, if your deductible is $200, your health plan will not pay for covered health care services until your deductible has been met. The deductible may not apply to all services.
Out-of-Pocket Maximum – The most you pay during a plan year (usually a calendar year) before your health plan begins to pay 100% of the allowed amount.
In-Plan Networks (e.g., Domestic Network or Direct Contracted Network) – if your doctor, hospital or health care facility is part of your insurance company’s network, you’ll get your health care at lower prices. If you go out of your network for health care, it will become a lot more expensive.
Out-of-Plan Networks (e.g., Secondary Network or Out-of-Network) – if your doctor, hospital or health care facility is NOT part of your insurance company’s network, you’ll get your health care at higher prices. You may pay a higher coinsurance percentage and have higher annual coinsurance and out-of-pocket maximums.
2022 MyChoiceOpen Enrollment Guide
HEALTHWith today’s rising medical costs, we all need some kind of protection against health care expenses that, in the event of a major illness or accident, could put a family’s entire financial future at risk.
Comprehensive medical coverage can help make the rising cost of healthcare more affordable. Health plans offered through MyChoice cover a wide range of services, including doctor visits, surgery, hospitalization, preventive care, prescription drugs, and more.
6

7
2022 MyChoiceOpen Enrollment Guide
7
McLAREN HEALTH ADVANTAGE (MHA)MHA Premier/MHA Premier Plus Non-Hospital Services and Hospital ServicesWhen you use either a McLaren facility and employed providers (domestic network) or the McLaren Health Advantage network, you will receive the highest level of benefit coverage and generally pay less out-of-pocket.
You may use providers outside these networks and still receive benefits; however, you may receive a lower level of benefit coverage and likely pay more out-of pocket. Out-of-pocket benefits are also subject to reasonable and customary limits.
To locate a Health Advantage provider:
1. Go to www.mclarenhealthplan.org
2. Move cursor over “Are You A Member?”
3. Choose Your Plan – Select “McLaren Health Advantage”
4. Select the “Find A Provider” icon.
7
2022 MyChoiceOpen Enrollment Guide
8
2022 MyChoiceOpen Enrollment Guide
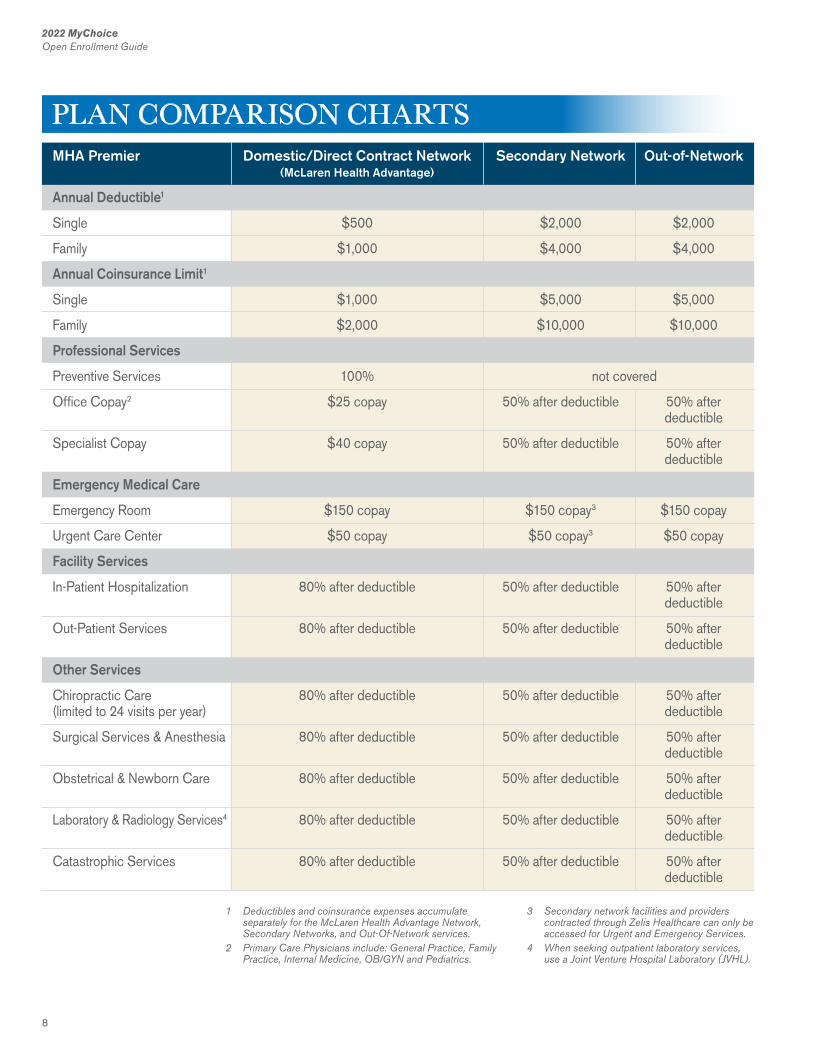
MHA Premier Domestic/Direct Contract Network Secondary Network Out-of-Network (McLaren Health Advantage)
Annual Deductible1
Single $500 $2,000 $2,000
Family $1,000 $4,000 $4,000
Annual Coinsurance Limit1
Single $1,000 $5,000 $5,000
Family $2,000 $10,000 $10,000
Professional Services
Preventive Services 100% not covered
Office Copay2 $25 copay 50% after deductible 50% after deductible
Specialist Copay $40 copay 50% after deductible 50% after deductible
Emergency Medical Care
Emergency Room $150 copay $150 copay3 $150 copay
Urgent Care Center $50 copay $50 copay3 $50 copay
Facility Services
In-Patient Hospitalization 80% after deductible 50% after deductible 50% after deductible
Out-Patient Services 80% after deductible 50% after deductible 50% after deductible
Other Services
Chiropractic Care 80% after deductible 50% after deductible 50% after(limited to 24 visits per year) deductible
Surgical Services & Anesthesia 80% after deductible 50% after deductible 50% after deductible
Obstetrical & Newborn Care 80% after deductible 50% after deductible 50% after deductible
Laboratory & Radiology Services4 80% after deductible 50% after deductible 50% after deductible
Catastrophic Services 80% after deductible 50% after deductible 50% after deductible
1 Deductibles and coinsurance expenses accumulate separately for the McLaren Health Advantage Network, Secondary Networks, and Out-Of-Network services.
2 Primary Care Physicians include: General Practice, Family Practice, Internal Medicine, OB/GYN and Pediatrics.
3 Secondary network facilities and providers contracted through Zelis Healthcare can only be accessed for Urgent and Emergency Services.
4 When seeking outpatient laboratory services, use a Joint Venture Hospital Laboratory (JVHL).
PLAN COMPARISON CHARTS
9
2022 MyChoiceOpen Enrollment Guide
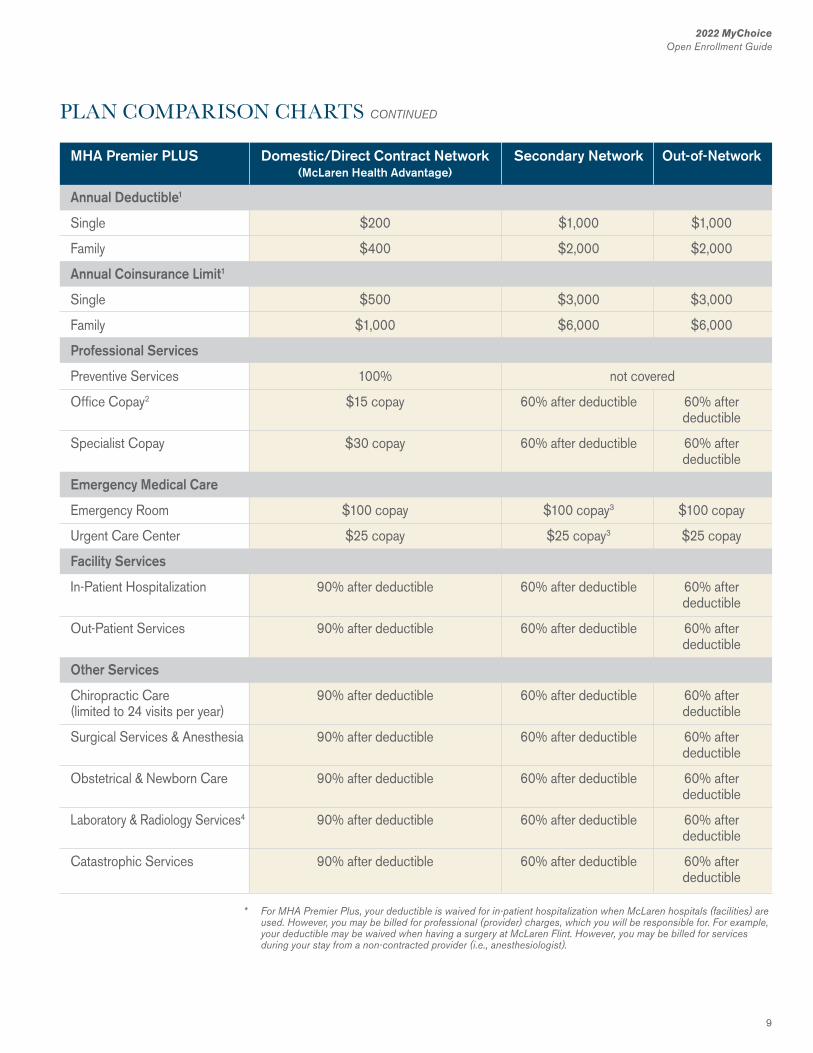
MHA Premier PLUS Domestic/Direct Contract Network Secondary Network Out-of-Network (McLaren Health Advantage)
Annual Deductible1
Single $200 $1,000 $1,000
Family $400 $2,000 $2,000
Annual Coinsurance Limit1
Single $500 $3,000 $3,000
Family $1,000 $6,000 $6,000
Professional Services
Preventive Services 100% not covered
Office Copay2 $15 copay 60% after deductible 60% after deductible
Specialist Copay $30 copay 60% after deductible 60% after deductible
Emergency Medical Care
Emergency Room $100 copay $100 copay3 $100 copay
Urgent Care Center $25 copay $25 copay3 $25 copay
Facility Services
In-Patient Hospitalization 90% after deductible 60% after deductible 60% after deductible
Out-Patient Services 90% after deductible 60% after deductible 60% after deductible
Other Services
Chiropractic Care 90% after deductible 60% after deductible 60% after(limited to 24 visits per year) deductible
Surgical Services & Anesthesia 90% after deductible 60% after deductible 60% after deductible
Obstetrical & Newborn Care 90% after deductible 60% after deductible 60% after deductible
Laboratory & Radiology Services4 90% after deductible 60% after deductible 60% after deductible
Catastrophic Services 90% after deductible 60% after deductible 60% after deductible
* For MHA Premier Plus, your deductible is waived for in-patient hospitalization when McLaren hospitals (facilities) are used. However, you may be billed for professional (provider) charges, which you will be responsible for. For example, your deductible may be waived when having a surgery at McLaren Flint. However, you may be billed for services during your stay from a non-contracted provider (i.e., anesthesiologist).
PLAN COMPARISON CHARTS CONTINUED
10
2022 MyChoiceOpen Enrollment Guide
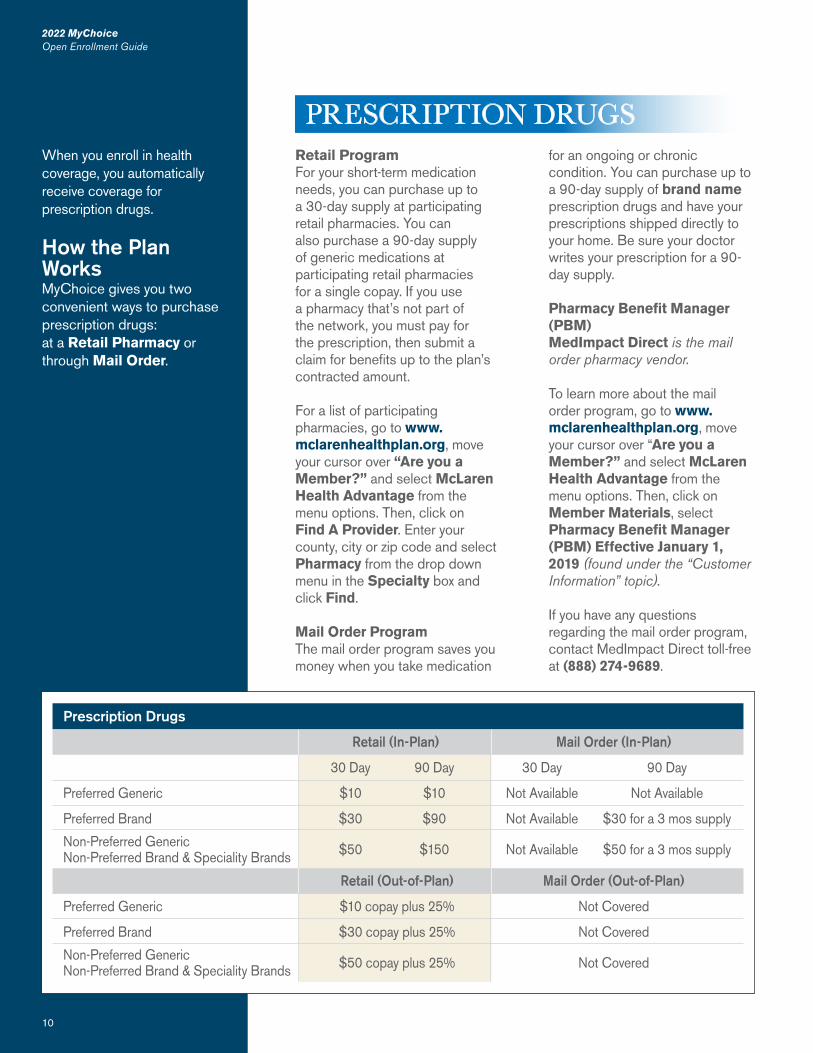
Retail ProgramFor your short-term medication needs, you can purchase up to a 30-day supply at participating retail pharmacies. You can also purchase a 90-day supply of generic medications at participating retail pharmacies for a single copay. If you use a pharmacy that’s not part of the network, you must pay for the prescription, then submit a claim for benefits up to the plan’s contracted amount.
For a list of participating pharmacies, go to www.mclarenhealthplan.org, move your cursor over “Are you a Member?” and select McLaren Health Advantage from the menu options. Then, click on Find A Provider. Enter your county, city or zip code and select Pharmacy from the drop down menu in the Specialty box and click Find.
Mail Order ProgramThe mail order program saves you money when you take medication
for an ongoing or chronic condition. You can purchase up to a 90-day supply of brand name prescription drugs and have your prescriptions shipped directly to your home. Be sure your doctor writes your prescription for a 90-day supply.
Pharmacy Benefit Manager (PBM)MedImpact Direct is the mail order pharmacy vendor.
To learn more about the mail order program, go to www.mclarenhealthplan.org, move your cursor over “Are you a Member?” and select McLaren Health Advantage from the menu options. Then, click on Member Materials, select Pharmacy Benefit Manager (PBM) Effective January 1, 2019 (found under the “Customer Information” topic).
If you have any questions regarding the mail order program, contact MedImpact Direct toll-free at (888) 274-9689.
2022 MyChoiceOpen Enrollment Guide
10
When you enroll in health coverage, you automatically receive coverage for prescription drugs.
How the Plan WorksMyChoice gives you two convenient ways to purchase prescription drugs:at a Retail Pharmacy or through Mail Order.
PRESCRIPTION DRUGS
Prescription Drugs
Retail (In-Plan) Mail Order (In-Plan)
30 Day 90 Day 30 Day 90 Day
Preferred Generic $10 $10 Not Available Not Available
Preferred Brand $30 $90 Not Available $30 for a 3 mos supply
Non-Preferred Generic $50 $150 Not Available $50 for a 3 mos supplyNon-Preferred Brand & Speciality Brands
Retail (Out-of-Plan) Mail Order (Out-of-Plan)
Preferred Generic $10 copay plus 25% Not Covered
Preferred Brand $30 copay plus 25% Not Covered
Non-Preferred Generic $50 copay plus 25% Not CoveredNon-Preferred Brand & Speciality Brands
11
2022 MyChoiceOpen Enrollment Guide
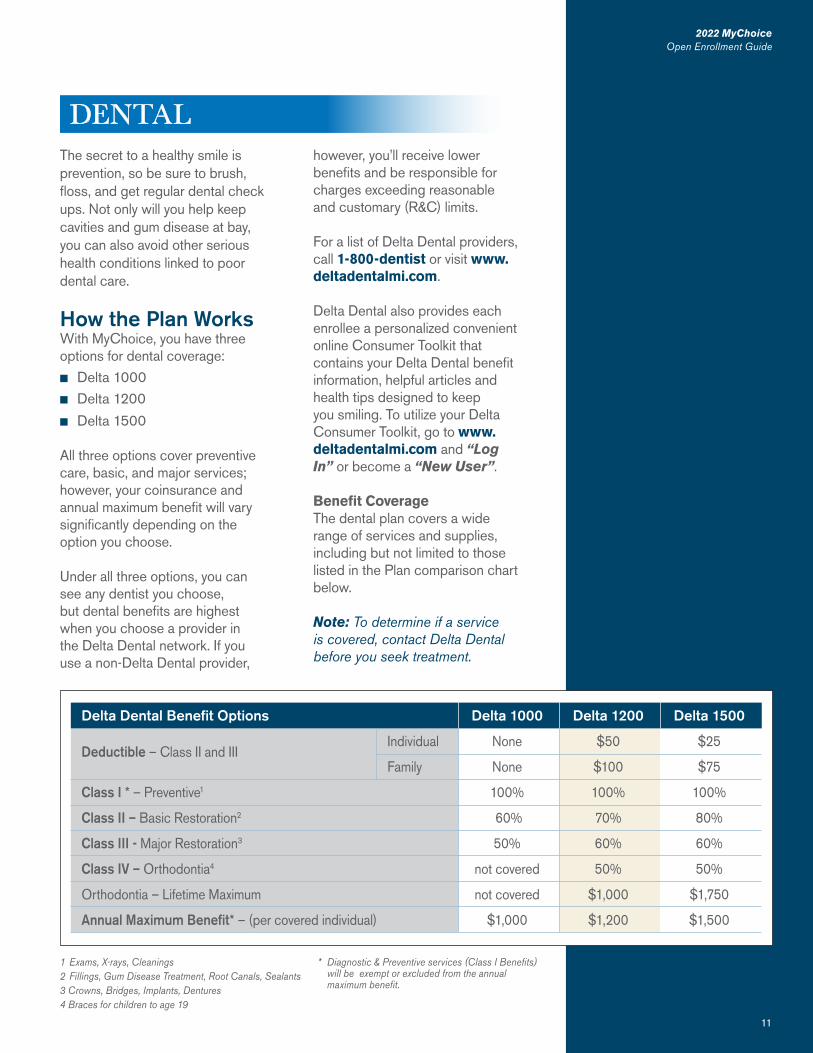
The secret to a healthy smile is prevention, so be sure to brush, floss, and get regular dental check ups. Not only will you help keep cavities and gum disease at bay, you can also avoid other serious health conditions linked to poor dental care.
How the Plan WorksWith MyChoice, you have three options for dental coverage:n Delta 1000n Delta 1200
n Delta 1500
All three options cover preventive care, basic, and major services; however, your coinsurance and annual maximum benefit will vary significantly depending on the option you choose.
Under all three options, you can see any dentist you choose, but dental benefits are highest when you choose a provider in the Delta Dental network. If you use a non-Delta Dental provider,
11
2022 MyChoiceOpen Enrollment Guide
DENTALhowever, you’ll receive lower benefits and be responsible for charges exceeding reasonable and customary (R&C) limits.
For a list of Delta Dental providers, call 1-800-dentist or visit www.deltadentalmi.com.
Delta Dental also provides each enrollee a personalized convenient online Consumer Toolkit that contains your Delta Dental benefit information, helpful articles and health tips designed to keep you smiling. To utilize your Delta Consumer Toolkit, go to www.deltadentalmi.com and “Log In” or become a “New User”.
Benefit CoverageThe dental plan covers a wide range of services and supplies, including but not limited to those listed in the Plan comparison chart below.
Note: To determine if a service is covered, contact Delta Dental before you seek treatment.
Delta Dental Benefit Options Delta 1000 Delta 1200 Delta 1500
Deductible – Class II and III Individual None $50 $25
Family None $100 $75
Class I * – Preventive1 100% 100% 100%
Class II – Basic Restoration2 60% 70% 80%
Class III - Major Restoration3 50% 60% 60%
Class IV – Orthodontia4 not covered 50% 50%
Orthodontia – Lifetime Maximum not covered $1,000 $1,750
Annual Maximum Benefit* – (per covered individual) $1,000 $1,200 $1,500
1 Exams, X-rays, Cleanings2 Fillings, Gum Disease Treatment, Root Canals, Sealants3 Crowns, Bridges, Implants, Dentures4 Braces for children to age 19
* Diagnostic & Preventive services (Class I Benefits) will be exempt or excluded from the annual maximum benefit.
12
2022 MyChoiceOpen Enrollment Guide
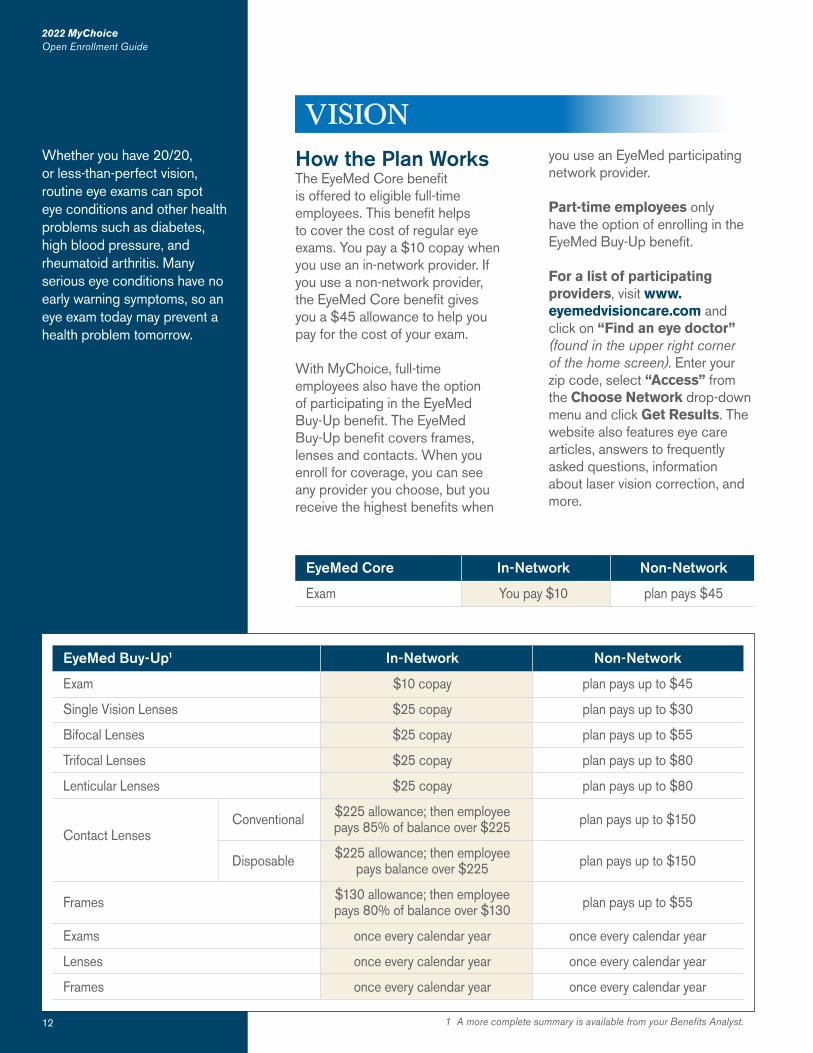
How the Plan WorksThe EyeMed Core benefit is offered to eligible full-time employees. This benefit helps to cover the cost of regular eye exams. You pay a $10 copay when you use an in-network provider. If you use a non-network provider, the EyeMed Core benefit gives you a $45 allowance to help you pay for the cost of your exam.
With MyChoice, full-time employees also have the option of participating in the EyeMed Buy-Up benefit. The EyeMed Buy-Up benefit covers frames, lenses and contacts. When you enroll for coverage, you can see any provider you choose, but you receive the highest benefits when
you use an EyeMed participating network provider.
Part-time employees only have the option of enrolling in the EyeMed Buy-Up benefit.
For a list of participating providers, visit www.eyemedvisioncare.com and click on “Find an eye doctor” (found in the upper right corner of the home screen). Enter your zip code, select “Access” from the Choose Network drop-down menu and click Get Results. The website also features eye care articles, answers to frequently asked questions, information about laser vision correction, and more.
2022 MyChoiceOpen Enrollment Guide
12
Whether you have 20/20, or less-than-perfect vision, routine eye exams can spot eye conditions and other health problems such as diabetes, high blood pressure, and rheumatoid arthritis. Many serious eye conditions have no early warning symptoms, so an eye exam today may prevent a health problem tomorrow.
1 A more complete summary is available from your Benefits Analyst.
EyeMed Buy-Up1 In-Network Non-Network
Exam $10 copay plan pays up to $45
Single Vision Lenses $25 copay plan pays up to $30
Bifocal Lenses $25 copay plan pays up to $55
Trifocal Lenses $25 copay plan pays up to $80
Lenticular Lenses $25 copay plan pays up to $80
Conventional $225 allowance; then employee plan pays up to $150Contact Lenses pays 85% of balance over $225
Disposable $225 allowance; then employee plan pays up to $150 pays balance over $225
Frames $130 allowance; then employee plan pays up to $55 pays 80% of balance over $130
Exams once every calendar year once every calendar year
Lenses once every calendar year once every calendar year
Frames once every calendar year once every calendar year
EyeMed Core In-Network Non-Network
Exam You pay $10 plan pays $45
VISION
13
2022 MyChoiceOpen Enrollment Guide
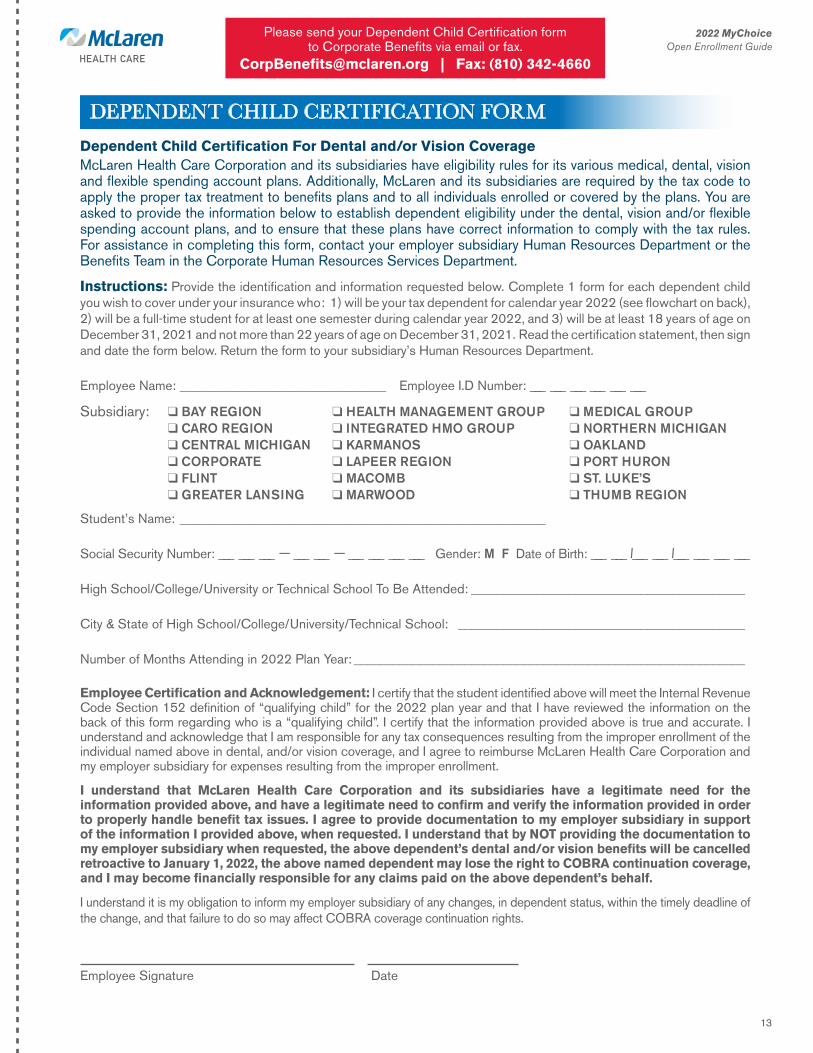
Dependent Child Certification For Dental and/or Vision CoverageMcLaren Health Care Corporation and its subsidiaries have eligibility rules for its various medical, dental, vision and flexible spending account plans. Additionally, McLaren and its subsidiaries are required by the tax code to apply the proper tax treatment to benefits plans and to all individuals enrolled or covered by the plans. You are asked to provide the information below to establish dependent eligibility under the dental, vision and/or flexible spending account plans, and to ensure that these plans have correct information to comply with the tax rules. For assistance in completing this form, contact your employer subsidiary Human Resources Department or the Benefits Team in the Corporate Human Resources Services Department.
Instructions: Provide the identification and information requested below. Complete 1 form for each dependent child you wish to cover under your insurance who: 1) will be your tax dependent for calendar year 2022 (see flowchart on back), 2) will be a full-time student for at least one semester during calendar year 2022, and 3) will be at least 18 years of age on December 31, 2021 and not more than 22 years of age on December 31, 2021. Read the certification statement, then sign and date the form below. Return the form to your subsidiary’s Human Resources Department.
Employee Name: _______________________________ Employee I.D Number: ___ ___ ___ ___ ___ ___
Subsidiary: q BAY REGIONq CARO REGIONq CENTRAL MICHIGANq CORPORATEq FLINTq GREATER LANSING
q HEALTH MANAGEMENT GROUPq INTEGRATED HMO GROUPq KARMANOSq LAPEER REGIONq MACOMBq MARWOOD
q MEDICAL GROUPq NORTHERN MICHIGANq OAKLANDq PORT HURONq ST. LUKE’Sq THUMB REGION
DEPENDENT CHILD CERTIFICATION FORM
Student’s Name: _______________________________________________________
Social Security Number: ___ ___ ___ – ___ ___ – ___ ___ ___ ___ Gender: M F Date of Birth: ___ ___ /___ ___ /___ ___ ___ ___
High School/College/University or Technical School To Be Attended: __________________________________________
City & State of High School/College/University/Technical School: ____________________________________________
Number of Months Attending in 2022 Plan Year: ____________________________________________________________
Employee Certification and Acknowledgement: I certify that the student identified above will meet the Internal Revenue Code Section 152 definition of “qualifying child” for the 2022 plan year and that I have reviewed the information on the back of this form regarding who is a “qualifying child”. I certify that the information provided above is true and accurate. I understand and acknowledge that I am responsible for any tax consequences resulting from the improper enrollment of the individual named above in dental, and/or vision coverage, and I agree to reimburse McLaren Health Care Corporation and my employer subsidiary for expenses resulting from the improper enrollment.
I understand that McLaren Health Care Corporation and its subsidiaries have a legitimate need for the information provided above, and have a legitimate need to confirm and verify the information provided in order to properly handle benefit tax issues. I agree to provide documentation to my employer subsidiary in support of the information I provided above, when requested. I understand that by NOT providing the documentation to my employer subsidiary when requested, the above dependent’s dental and/or vision benefits will be cancelled retroactive to January 1, 2022, the above named dependent may lose the right to COBRA continuation coverage, and I may become financially responsible for any claims paid on the above dependent’s behalf.
I understand it is my obligation to inform my employer subsidiary of any changes, in dependent status, within the timely deadline of the change, and that failure to do so may affect COBRA coverage continuation rights.
Employee Signature Date
Please send your Dependent Child Certification formto Corporate Benefits via email or fax.
[email protected] | Fax: (810) 342-4660
14
2022 MyChoiceOpen Enrollment Guide
NO
YES
NO
YES
NO
YES
NO
YES
NO
YES
NO
YES
NO YES
NO
YES
NO
YES
NO
YES
NO
YES
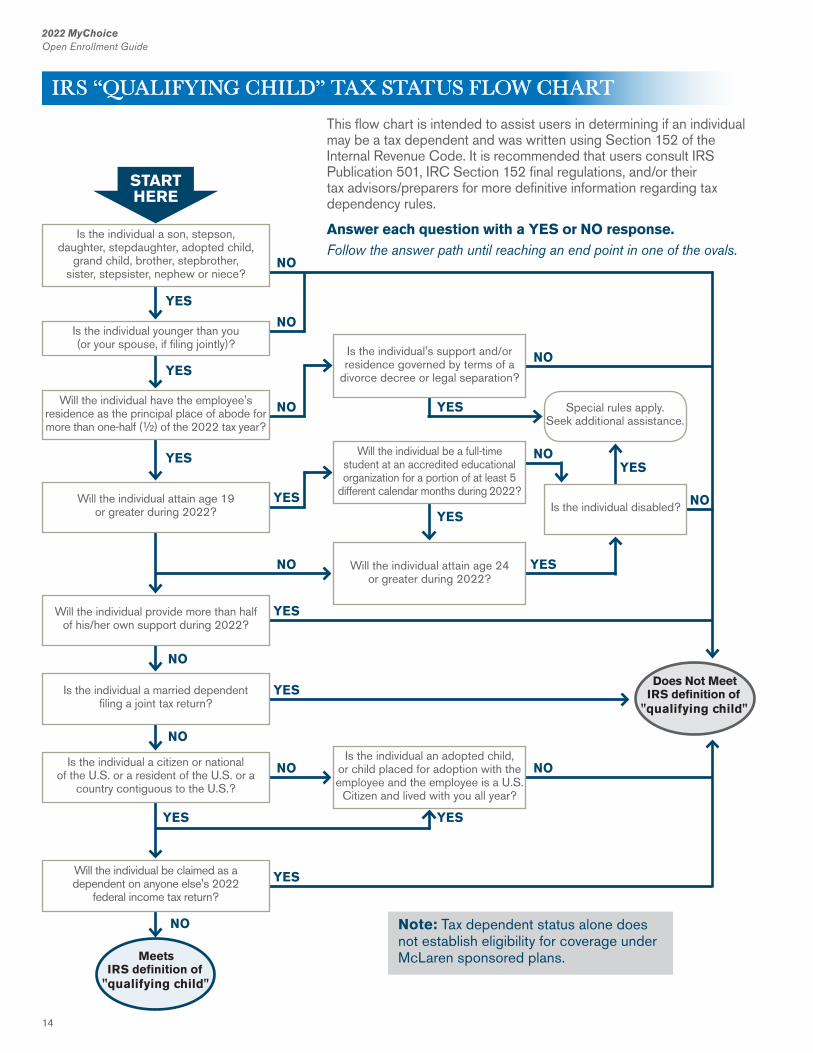
Will the individual have the employee's residence as the principal place of abode for more than one-half (½) of the 2022 tax year?
Will the individual attain age 19or greater during 2022?
Will the individual provide more than half of his/her own support during 2022?
Is the individual a married dependent filing a joint tax return?
Is the individual a citizen or national of the U.S. or a resident of the U.S. or a
country contiguous to the U.S.?
Will the individual be claimed as adependent on anyone else's 2022
federal income tax return?
Is the individual's support and/or residence governed by terms of a
divorce decree or legal separation?
Will the individual be a full-time student at an accredited educational organization for a portion of at least 5
different calendar months during 2022?
Will the individual attain age 24or greater during 2022?
Is the individual an adopted child, or child placed for adoption with the employee and the employee is a U.S.
Citizen and lived with you all year?
Special rules apply. Seek additional assistance.
Is the individual disabled?
YES
Does Not Meet IRS definition of
"qualifying child"
Meets IRS definition of
"qualifying child"
Note: Tax dependent status alone does not establish eligibility for coverage under McLaren sponsored plans.
NO
YES
Is the individual a son, stepson, daughter, stepdaughter, adopted child,
grand child, brother, stepbrother, sister, stepsister, nephew or niece?
Is the individual younger than you (or your spouse, if filing jointly)?
STARTHERE
This flow chart is intended to assist users in determining if an individual may be a tax dependent and was written using Section 152 of the Internal Revenue Code. It is recommended that users consult IRS Publication 501, IRC Section 152 final regulations, and/or their tax advisors/preparers for more definitive information regarding tax dependency rules.
Answer each question with a YES or NO response.Follow the answer path until reaching an end point in one of the ovals.
IRS “QUALIFYING CHILD” TAX STATUS FLOW CHART
15
2022 MyChoiceOpen Enrollment Guide
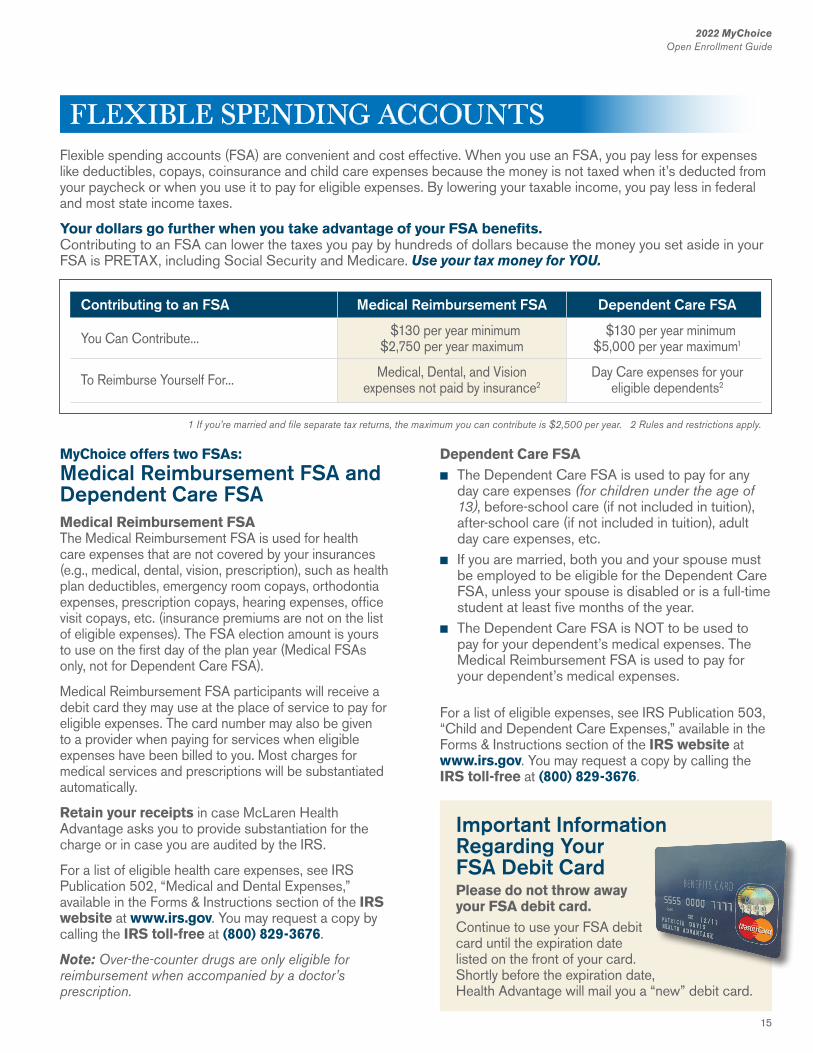
Flexible spending accounts (FSA) are convenient and cost effective. When you use an FSA, you pay less for expenses like deductibles, copays, coinsurance and child care expenses because the money is not taxed when it’s deducted from your paycheck or when you use it to pay for eligible expenses. By lowering your taxable income, you pay less in federal and most state income taxes.
Your dollars go further when you take advantage of your FSA benefits.Contributing to an FSA can lower the taxes you pay by hundreds of dollars because the money you set aside in your FSA is PRETAX, including Social Security and Medicare. Use your tax money for YOU.
1 If you’re married and file separate tax returns, the maximum you can contribute is $2,500 per year. 2 Rules and restrictions apply.
Contributing to an FSA Medical Reimbursement FSA Dependent Care FSA
You Can Contribute... $130 per year minimum $130 per year minimum $2,750 per year maximum $5,000 per year maximum1
To Reimburse Yourself For... Medical, Dental, and Vision Day Care expenses for your expenses not paid by insurance2 eligible dependents2
MyChoice offers two FSAs: Medical Reimbursement FSA and Dependent Care FSA Medical Reimbursement FSA The Medical Reimbursement FSA is used for health care expenses that are not covered by your insurances (e.g., medical, dental, vision, prescription), such as health plan deductibles, emergency room copays, orthodontia expenses, prescription copays, hearing expenses, office visit copays, etc. (insurance premiums are not on the list of eligible expenses). The FSA election amount is yours to use on the first day of the plan year (Medical FSAs only, not for Dependent Care FSA).
Medical Reimbursement FSA participants will receive a debit card they may use at the place of service to pay for eligible expenses. The card number may also be given to a provider when paying for services when eligible expenses have been billed to you. Most charges for medical services and prescriptions will be substantiated automatically.
Retain your receipts in case McLaren Health Advantage asks you to provide substantiation for the charge or in case you are audited by the IRS.
For a list of eligible health care expenses, see IRS Publication 502, “Medical and Dental Expenses,” available in the Forms & Instructions section of the IRS website at www.irs.gov. You may request a copy by calling the IRS toll-free at (800) 829-3676.
Note: Over-the-counter drugs are only eligible for reimbursement when accompanied by a doctor’s prescription.
Dependent Care FSAn The Dependent Care FSA is used to pay for any
day care expenses (for children under the age of 13), before-school care (if not included in tuition), after-school care (if not included in tuition), adult day care expenses, etc.
n If you are married, both you and your spouse must be employed to be eligible for the Dependent Care FSA, unless your spouse is disabled or is a full-time student at least five months of the year.
n The Dependent Care FSA is NOT to be used to pay for your dependent’s medical expenses. The Medical Reimbursement FSA is used to pay for your dependent’s medical expenses.
For a list of eligible expenses, see IRS Publication 503, “Child and Dependent Care Expenses,” available in the Forms & Instructions section of the IRS website at www.irs.gov. You may request a copy by calling the IRS toll-free at (800) 829-3676.
Important Information Regarding YourFSA Debit Card Please do not throw away your FSA debit card.Continue to use your FSA debit card until the expiration date listed on the front of your card. Shortly before the expiration date, Health Advantage will mail you a “new” debit card.
FLEXIBLE SPENDING ACCOUNTS

16
2022 MyChoiceOpen Enrollment Guide
Planning anFSA Amount How to calculate an FSA election amount to deduct from your paycheck: When you are deciding how much money you want to contribute to one or both FSAs, it is important to know the best value comes from FSA participation that is close to the amount you expect to spend on eligible health or dependent care expenses. If you do not spend all of the money in your Medical Reimbursement FSA Account, you are allowed to rollover up to $550 of unused FSA funds into the following plan year.
The $550 Rollover RuleDOES NOT APPLY to the Dependent Care FSA account.
For a Medical Reimbursement FSA, first review your health plan,
dental plan, vision plan, etc. Look at the out-of-pocket expenses (e.g., deductibles, coinsurance, copayments, etc.) for each benefit plan. Use this past year’s expenses as a guide, list how many prescription copays you paid, how many medical copays you paid, how many dental services you paid for, how many vision services you paid for, etc. Once you have added up your expenses, then you can decide your Medical FSA election amount for the year.
When determining your Dependent Care FSA election amount, look at how much you spent on last year’s child day care expenses and/or adult day care expenses.
Once you decide on the FSA election amount(s) that you would like to have deducted from your paycheck for 2022, when you enroll, that amount is divided by
the number of pay periods in the year to determine how much will be deducted from your paycheck each pay day and then deposited into the applicable spending account. As you incur expenses, you use the money in the spending account to pay the providers or reimburse yourself (for charges that you paid directly to the provider).
Your FSA election amount must be used to pay for expenses incurred during the calendar year in which your contributions are made. You will have until March 31, 2023 to submit claims for expenses incurred in 2022. If you have money left over in your Medical Reimbursement FSA account at the end of the year, you are allowed to rollover up to $550 of unused FSA funds into the following plan year.
FSA Reimbursement for Medical (not paid with your FSA debit card) & Dependent Care expenses
You may receive your reimbursement in one of two ways:
1. Receive a check (mailed to you) for the FSA reimbursement amount you requested, or
2. Direct deposit makes it easier and quicker to receive your FSA reimbursement. Have your reimbursement directly deposited into your checking or savings account instead of waiting for a check to be mailed to you.
IMPORTANT NOTE: Submit your request for reimbursement along with an itemized receipt or bill that shows the date, type of service, and amount you paid.
The FSA Direct Deposit and FSA Reimbursement Forms can be accessed and downloaded by visiting www.mclarenhealthplan.org. Once on this page, move your cursor over “Are you a Member?” and select McLaren Health Advantage from the menu of options.
Then, click on the Member Materials icon, this page contains: n Direct Deposit
Authorization Formn Flexible Spending Account (FSA)
Dependent Care Reimbursement Formn Flexible Spending Account (FSA)
Health Care Reimbursement Form
(All found under the “Benefit and Customer Information” topic.)
FLEXIBLE SPENDING ACCOUNTS CONTINUED

17
2022 MyChoiceOpen Enrollment Guide
Medical ReimbursementFSA $550 Rollover Medical Reimbursement FSA participants may rollover up to $550 of unused FSA funds in the Medical Reimbursement FSA into the following plan year (this does NOT apply to the dependent care FSA accounts). The rollover amount does not count against the indexed $2,750 salary reduction limit. Participants are allowed to rollover up to $550 and still make a salary reduction up to $2,750 into their Medical Reimbursement FSA.
This FSA change allows for more flexibility and less risk in the FSA program for the FSA participants. You no longer need to precisely budget your out-of-pocket health care expenses - reducing the risk of “overfunding” and forfeiting FSA funds. No more rushing to spend Medical Reimbursement FSA funds on unnecessary items by year-end.
More About FSAs No TransfersIf you participate in both spending accounts, you cannot transfer money between your two accounts or use money in one account to pay expenses related to the other.
No Contribution ChangesOnce you decide on the FSA election amount, you cannot change the amount until the next calendar year unless you experience a “change in status” event.
Dependent Care FSA vs. Federal Tax CreditYou may use the Dependent Care FSA or the Child and Dependent Care Tax Credit but not for the same expenses. Talk to your financial advisor to find out how you can save the most on your taxes when it comes to child care.
1717
2022 MyChoiceOpen Enrollment Guide
FLEXIBLE SPENDING ACCOUNTS CONTINUED
18
2022 MyChoiceOpen Enrollment Guide
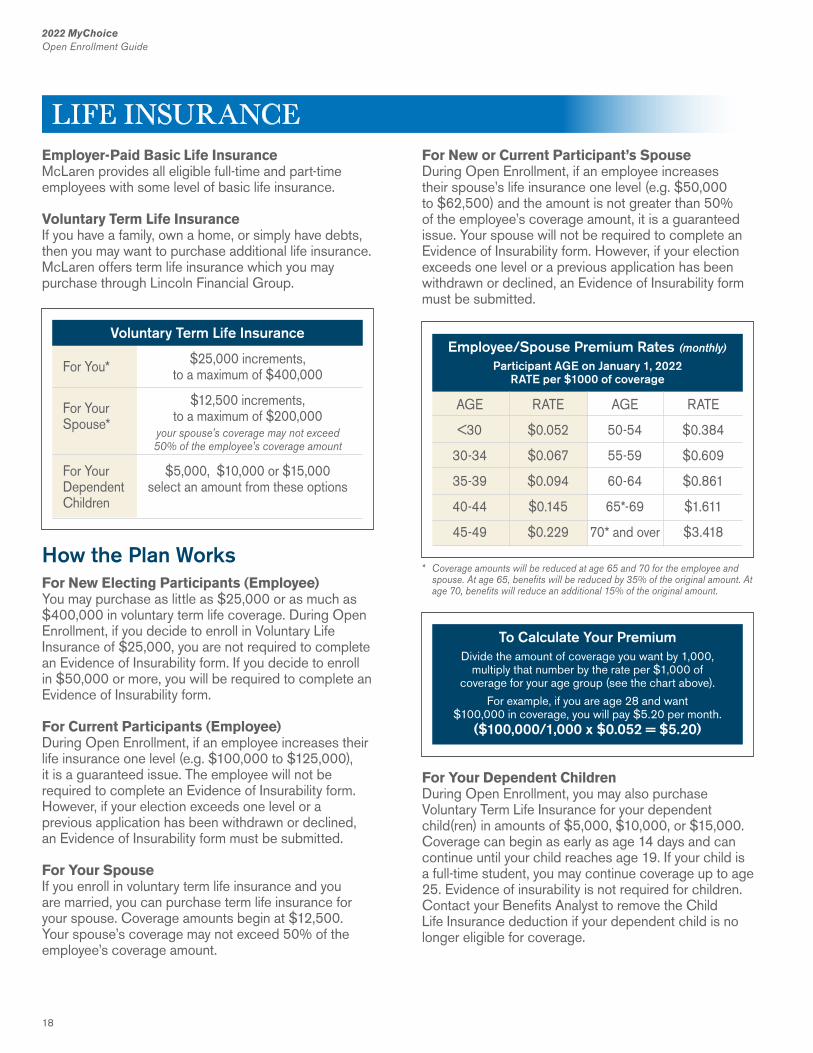
Employer-Paid Basic Life InsuranceMcLaren provides all eligible full-time and part-time employees with some level of basic life insurance.
Voluntary Term Life InsuranceIf you have a family, own a home, or simply have debts, then you may want to purchase additional life insurance. McLaren offers term life insurance which you may purchase through Lincoln Financial Group.
How the Plan WorksFor New Electing Participants (Employee)You may purchase as little as $25,000 or as much as $400,000 in voluntary term life coverage. During Open Enrollment, if you decide to enroll in Voluntary Life Insurance of $25,000, you are not required to complete an Evidence of Insurability form. If you decide to enroll in $50,000 or more, you will be required to complete an Evidence of Insurability form.
For Current Participants (Employee)During Open Enrollment, if an employee increases their life insurance one level (e.g. $100,000 to $125,000), it is a guaranteed issue. The employee will not be required to complete an Evidence of Insurability form. However, if your election exceeds one level or a previous application has been withdrawn or declined, an Evidence of Insurability form must be submitted.
For Your SpouseIf you enroll in voluntary term life insurance and you are married, you can purchase term life insurance for your spouse. Coverage amounts begin at $12,500. Your spouse’s coverage may not exceed 50% of the employee’s coverage amount.
For New or Current Participant’s SpouseDuring Open Enrollment, if an employee increases their spouse’s life insurance one level (e.g. $50,000 to $62,500) and the amount is not greater than 50% of the employee’s coverage amount, it is a guaranteed issue. Your spouse will not be required to complete an Evidence of Insurability form. However, if your election exceeds one level or a previous application has been withdrawn or declined, an Evidence of Insurability form must be submitted.
For Your Dependent ChildrenDuring Open Enrollment, you may also purchase Voluntary Term Life Insurance for your dependent child(ren) in amounts of $5,000, $10,000, or $15,000. Coverage can begin as early as age 14 days and can continue until your child reaches age 19. If your child is a full-time student, you may continue coverage up to age 25. Evidence of insurability is not required for children. Contact your Benefits Analyst to remove the Child Life Insurance deduction if your dependent child is no longer eligible for coverage.
Voluntary Term Life Insurance
For You* $25,000 increments, to a maximum of $400,000
$12,500 increments,For Your to a maximum of $200,000Spouse* your spouse’s coverage may not exceed 50% of the employee’s coverage amount
For Your $5,000, $10,000 or $15,000Dependent select an amount from these optionsChildren
* Coverage amounts will be reduced at age 65 and 70 for the employee and spouse. At age 65, benefits will be reduced by 35% of the original amount. At age 70, benefits will reduce an additional 15% of the original amount.
Employee/Spouse Premium Rates (monthly)
Participant AGE on January 1, 2022 RATE per $1000 of coverage
AGE RATE
<30 $0.052
30-34 $0.067
35-39 $0.094
40-44 $0.145
45-49 $0.229
AGE RATE
50-54 $0.384
55-59 $0.609
60-64 $0.861
65*-69 $1.611
70* and over $3.418
To Calculate Your PremiumDivide the amount of coverage you want by 1,000,
multiply that number by the rate per $1,000 of coverage for your age group (see the chart above).
For example, if you are age 28 and want $100,000 in coverage, you will pay $5.20 per month.
($100,000/1,000 x $0.052 = $5.20)
LIFE INSURANCE
19
2022 MyChoiceOpen Enrollment Guide
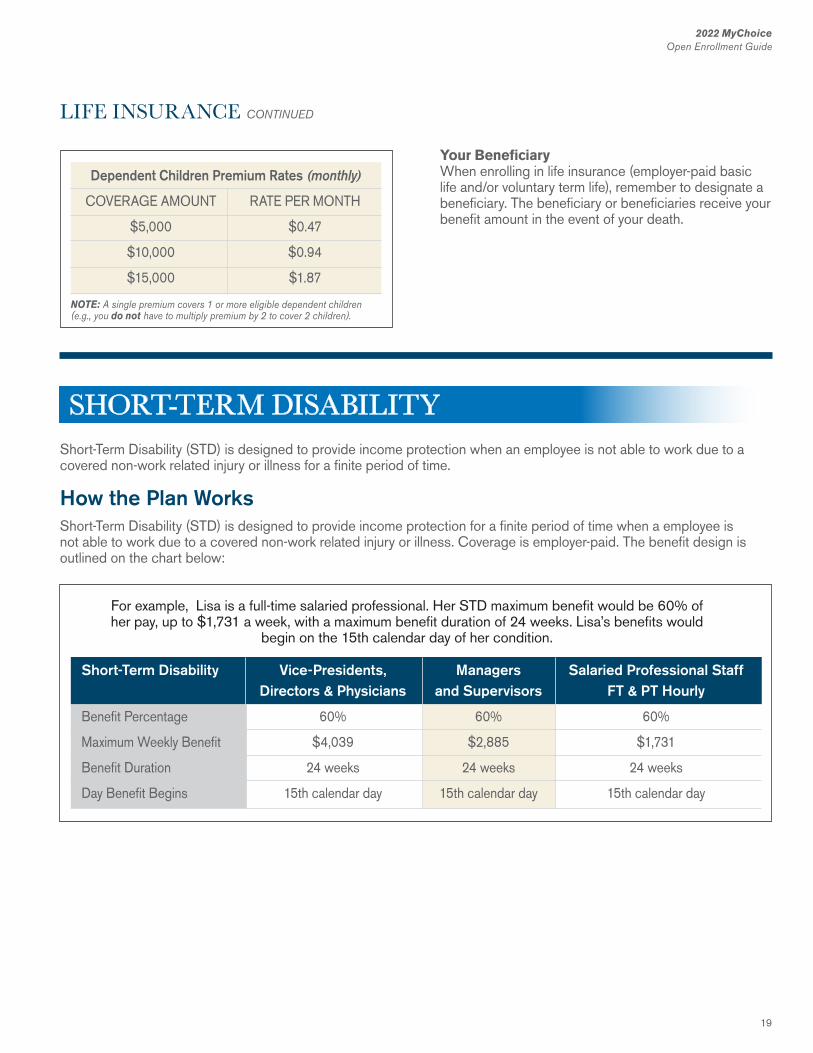
Dependent Children Premium Rates (monthly)
COVERAGE AMOUNT RATE PER MONTH
$5,000 $0.47
$10,000 $0.94
$15,000 $1.87
NOTE: A single premium covers 1 or more eligible dependent children (e.g., you do not have to multiply premium by 2 to cover 2 children).
Your BeneficiaryWhen enrolling in life insurance (employer-paid basic life and/or voluntary term life), remember to designate a beneficiary. The beneficiary or beneficiaries receive your benefit amount in the event of your death.
LIFE INSURANCE CONTINUED
Short-Term Disability (STD) is designed to provide income protection when an employee is not able to work due to a covered non-work related injury or illness for a finite period of time.
How the Plan WorksShort-Term Disability (STD) is designed to provide income protection for a finite period of time when a employee is not able to work due to a covered non-work related injury or illness. Coverage is employer-paid. The benefit design is outlined on the chart below:
Short-Term Disability Vice-Presidents, Managers Salaried Professional Staff Directors & Physicians and Supervisors FT & PT Hourly
Benefit Percentage 60% 60% 60%
Maximum Weekly Benefit $4,039 $2,885 $1,731
Benefit Duration 24 weeks 24 weeks 24 weeks
Day Benefit Begins 15th calendar day 15th calendar day 15th calendar day
For example, Lisa is a full-time salaried professional. Her STD maximum benefit would be 60% of her pay, up to $1,731 a week, with a maximum benefit duration of 24 weeks. Lisa’s benefits would
begin on the 15th calendar day of her condition.
SHORT-TERM DISABILITY
20
2022 MyChoiceOpen Enrollment Guide
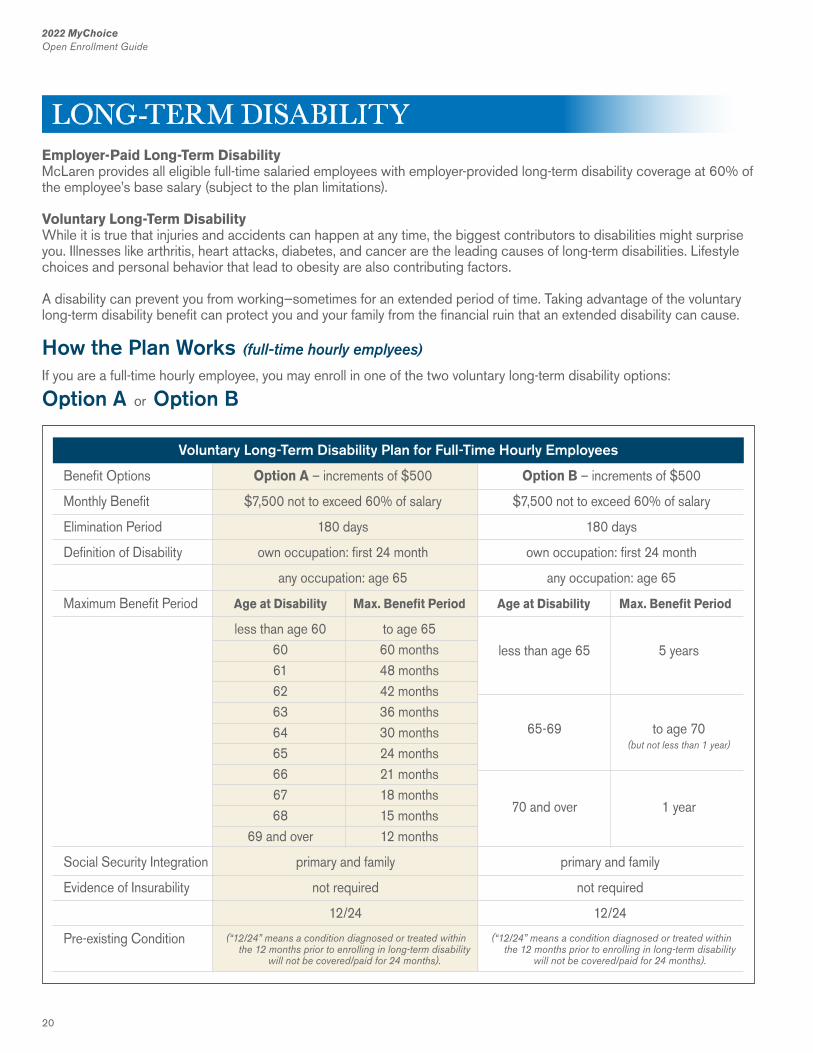
Employer-Paid Long-Term DisabilityMcLaren provides all eligible full-time salaried employees with employer-provided long-term disability coverage at 60% of the employee’s base salary (subject to the plan limitations).
Voluntary Long-Term DisabilityWhile it is true that injuries and accidents can happen at any time, the biggest contributors to disabilities might surprise you. Illnesses like arthritis, heart attacks, diabetes, and cancer are the leading causes of long-term disabilities. Lifestyle choices and personal behavior that lead to obesity are also contributing factors.
A disability can prevent you from working—sometimes for an extended period of time. Taking advantage of the voluntary long-term disability benefit can protect you and your family from the financial ruin that an extended disability can cause.
How the Plan Works (full-time hourly emplyees)
If you are a full-time hourly employee, you may enroll in one of the two voluntary long-term disability options:
Option A or Option B
Voluntary Long-Term Disability Plan for Full-Time Hourly Employees
Benefit Options Option A – increments of $500 Option B – increments of $500
Monthly Benefit $7,500 not to exceed 60% of salary $7,500 not to exceed 60% of salary
Elimination Period 180 days 180 days
Definition of Disability own occupation: first 24 month own occupation: first 24 month
any occupation: age 65 any occupation: age 65
Maximum Benefit Period Age at Disability Max. Benefit Period Age at Disability Max. Benefit Period
less than age 60 to age 65 60 60 months 61 48 months 62 42 months 63 36 months 64 30 months 65 24 months 66 21 months 67 18 months 68 15 months 69 and over 12 months
Social Security Integration primary and family primary and family
Evidence of Insurability not required not required
12/24 12/24
Pre-existing Condition (“12/24” means a condition diagnosed or treated within the 12 months prior to enrolling in long-term disability
will not be covered/paid for 24 months).
(“12/24” means a condition diagnosed or treated within the 12 months prior to enrolling in long-term disability
will not be covered/paid for 24 months).
less than age 65
65-69
70 and over
5 years
to age 70
1 year
(but not less than 1 year)
LONG-TERM DISABILITY

21
2022 MyChoiceOpen Enrollment Guide
2121
2022 MyChoiceOpen Enrollment Guide
Option A or Option B allows you to purchase coverage in $500 increments, subject to a $500 minimum and a $7,500 maximum, not to exceed 60% of your base pay per month. Benefits begin after a 180-day waiting period and will be paid according to the maximum benefit period (see chart on previous page).
Note: When a covered disability keeps you out of work, long-term disability insurance helps keep your finances protected. It pays a portion of your income while you recover, with benefits continuing for the policy’s benefit period or until you are no longer disabled – whichever comes first.
Conditions that could lead to a long-term disability claim include:n Surgeryn Injuryn Illnessn Accident
The monthly cost of Options A and B is the coverage amount multiplied by the age-based rate
For example, if you are age 40 and want $1,500 in coverage you would pay $14.09 per month for Option A and Option B would cost $7.03 per month.
Option A – $1,500/100 x 0.939 = $14.09 and Option B – $1,500/100 x 0.469 = $7.03
Age Rate (as a % of benefit)
Option A Option B
<30 0.324% 0.210%
30-34 0.502% 0.283%
35-39 0.719% 0.396%
40-44 0.939% 0.469%
45-49 1.602% 0.825%
50-54 2.257% 1.327%
55-59 3.317% 2.516%
60-64 3.156% 4.142%
65-69 2.079% 3.519%
70 and over 2.079% 3.519%
How the Plan Works (full-time salaried emplyees)
If you are a full-time salaried employee, you may enroll in the 10% Buy-Up voluntary long-term disability option.
Full-time salaried employees covered by the employer-provided long-term disability coverage at 60% of your pay will have the option of buying additional coverage equal to 10% of your pay, subject to the plan limitations. The monthly cost of this benefit is 0.198% of your base monthly salary.
The Monthly Cost of the 10% Buy-Upis the covered base monthly salary multiplied by the 0.198% factor. For example, if your base monthly salary is $6,000, your monthly cost would be $11.88.
$6,000/100 x 0.198 = $11.88
22
2022 MyChoiceOpen Enrollment Guide2022 MyChoiceOpen Enrollment Guide
22
24/7 SUPPORT, RESOURCES AND INFORMATIONYour ComPsych® GuidanceResources® program offers someone to talk to and resources to consult whenever and wherever you need them.
Call (844) 449-6539TDD: (800) 697-0353Your toll-free number gives you direct, 24/7 access to a GuidanceConsultant™, who will answer your questions and, if needed, refer you to a counselor or other resources.
Online:guidanceresources.comApp:GuidanceResources® NowWeb ID:MCLAREN
Log on today to connect directly with a GuidanceConsultant about your issue or to consult articles, podcasts, videos, and other helpful tools.
Confidential Emotional SupportOur highly trained clinicians will listen to your concerns and help you or your family members with any issues, including:n Anxiety, depression, stressn Grief, loss and life adjustmentsn Relationship/marital conflicts
Work-Life SolutionsOur specialists provide qualified referrals and resources for just about anything on your to-do list, such as:n Finding child and elder caren Hiring movers or home repair contractorsn Planning events, locating pet care
Legal GuidanceTalk to our attorneys for practical assistance with your most pressing legal issues, including:n Divorce, adoption, family law, wills, trusts and more
Need representation? Get a free 30-minute consultation and a 25% reduction in fees.
Financial ResourcesOur financial experts can assist with a wide range of issues. Talk to us about:n Retirement planning, taxesn Relocation, mortgages, insurancen Budgeting, debt, bankruptcy and more
Online SupportGuidanceResources® Online is your 24/7 link to vital information, tools and support. Log on for:n Articles, podcasts, videos, slideshowsn On-demand trainingsn “Ask the Expert” personal responses to your questionsn Working Advantage discounts
CONTACT US... ANYTIME... ANYWHERENo cost, confidential solutions to life’s challenges.
Contact Your GuidanceResources® ProgramCall: (844) 449-6539TDD: (800) 697-0353Online: guidanceresources.comApp: GuidanceResources® NowWeb ID: MCLAREN©2017 ComPsych Corporation. All rights reserved. To view the ComPsych HIPAA privacy notice, please go to www.guidanceresources.com/privacy. ComPsych complies with applicable federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability, or sex.
EMPLOYEE ASSISTANCE PROGRAM
23
2022 MyChoiceOpen Enrollment Guide
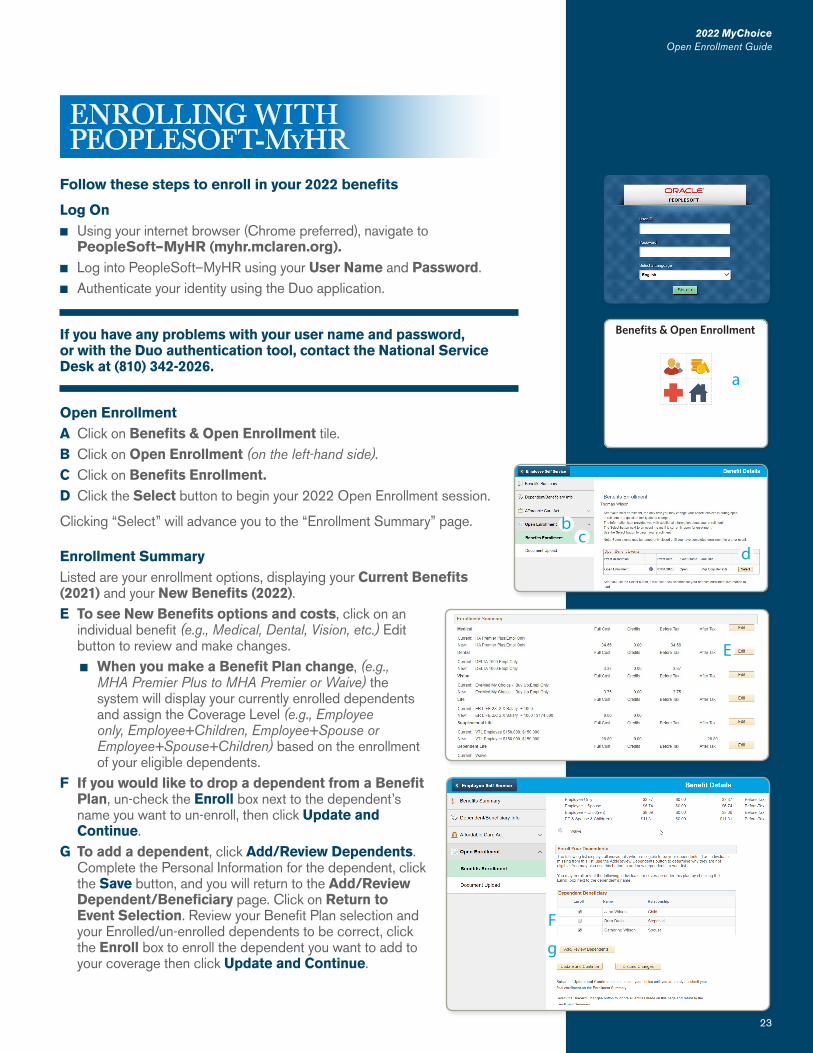
Follow these steps to enroll in your 2022 benefits
Log Onn Using your internet browser (Chrome preferred), navigate to
PeopleSoft–MyHR (myhr.mclaren.org).n Log into PeopleSoft–MyHR using your User Name and Password.n Authenticate your identity using the Duo application.
If you have any problems with your user name and password,or with the Duo authentication tool, contact the National Service Desk at (810) 342-2026.
Open EnrollmentA Click on Benefits & Open Enrollment tile.B Click on Open Enrollment (on the left-hand side).C Click on Benefits Enrollment.D Click the Select button to begin your 2022 Open Enrollment session.
Clicking “Select” will advance you to the “Enrollment Summary” page.
Enrollment SummaryListed are your enrollment options, displaying your Current Benefits (2021) and your New Benefits (2022).E To see New Benefits options and costs, click on an
individual benefit (e.g., Medical, Dental, Vision, etc.) Edit button to review and make changes.n When you make a Benefit Plan change, (e.g.,
MHA Premier Plus to MHA Premier or Waive) the system will display your currently enrolled dependents and assign the Coverage Level (e.g., Employee only, Employee+Children, Employee+Spouse or Employee+Spouse+Children) based on the enrollment of your eligible dependents.
F If you would like to drop a dependent from a Benefit Plan, un-check the Enroll box next to the dependent’s name you want to un-enroll, then click Update and Continue.
G To add a dependent, click Add/Review Dependents. Complete the Personal Information for the dependent, click the Save button, and you will return to the Add/Review Dependent/Beneficiary page. Click on Return to Event Selection. Review your Benefit Plan selection and your Enrolled/un-enrolled dependents to be correct, click the Enroll box to enroll the dependent you want to add to your coverage then click Update and Continue.
23
2022 MyChoiceOpen Enrollment Guide
ENROLLING WITH PEOPLESOFT-MyHR
E
Benefits & Open Enrollment
a
F
g
bc
d
24
2022 MyChoiceOpen Enrollment Guide
H You must click on Update and Continue to store your choice until you are ready to submit your elections on the Enrollment Summary page.
Select the Discard Changes button to ignore all entries made on this page and return to the Enrollment Summary page.
I Once you click on Update Elections, you are returned to the Enrollment Summary page. Your benefit(s) changes are listed for each offering, on its New Benefits description line.n Use this same process to make changes to other benefits, if desired.
Flexible Spending Account Enrollment InstructionsYou cannot finish your Open Enrollment session without making a selection to either “Enroll” and enter an amount or “Waive” the benefit for both the:
J Flex Spending Health – U.S. and theK Flex Spending Dependent Care.L Click on Update and Continue to store your FSA choices until you are
ready to submit your elections on the Enrollment Summary page.
Select the Discard Changes button to ignore all entries made on this page and return to the Enrollment Summary page.
ENROLLING WITH PEOPLESOFT-MyHR CONTINUED
2022 MyChoiceOpen Enrollment Guide
24
n
o
jk
h
l
i
m
P
M Once you click on Update Elections, you are returned to the Enrollment Summary page. Your benefit(s) changes are listed for each offering, on its New Benefits description line.
If you do not click on “Update and Continue”, you will receive errors, and will not be able to complete your Open Enrollment session.
N Once you have completed your enrollments, scroll to the bottom of the Enrollment Summary page and click the Save and Continue button.
Clicking “Save and Continue” will advance to the last page titled, “Submit Benefit Choices”.
O Complete your 2022 Open Enrollment by clicking the Submit button and authorizing your elections.
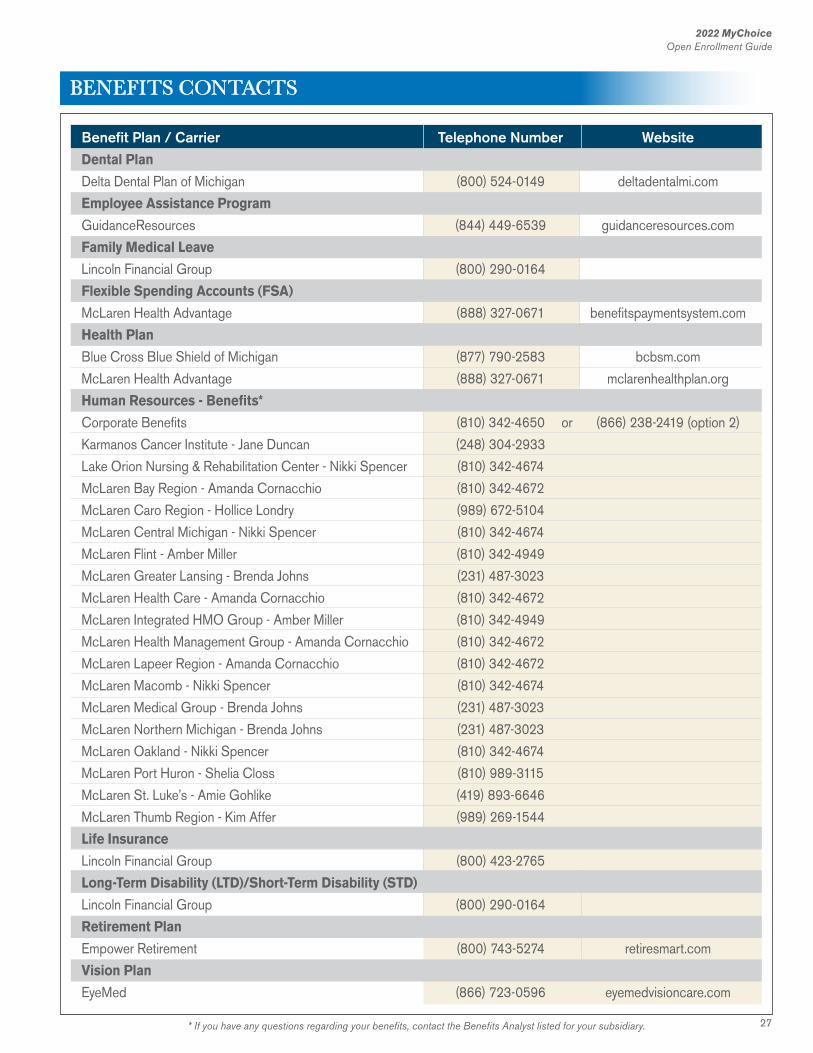
Dependent/Beneficiary InfoIf you are adding a new dependent and need to submit supporting documentation (e.g., marriage license, birth certificate, etc.) or need to submit a Dependent Child Certification Form (for a dependent), P for dental/vision coverage, please go to Dependent/
Beneficiary Info after you complete your Open Enrollment session. Dependent/Beneficiary Info is located in Employee Self Service of PeopleSoft-MyHR.
NOTE: Only submit one document per transaction.
Modifying Your 2022 Open Enrollment Electionsn You may revise and submit your elections as many times as you
want during Open Enrollment which begins Monday, November 1 and ends Monday, November 15, 2021 at 5 pm.
25
2022 MyChoiceOpen Enrollment Guide
1. Do I need to do anything during Open Enrollment if I don’t want to make any changes?
For this year’s Open Enrollment, you MUST participate in Open Enrollment if:n You want to enroll or continue in a Flexible
Spending Account (FSA) in plan year 2022. Participants in an FSA must enroll every year.
n You want to enroll or continue Dental and/or Vision coverage for a dependent who is 18-22 years old and is a full-time student and your tax dependent. The Dependent Child Certification Form can be found on page 13 in this Open Enrollment Guide.
n You want to change your Medical, Dental or Vision plan.
n You want to change who is covered on your Medical, Dental or Vision plan.
n You want to change your Life Insurance or Long-Term Disability coverage, if eligible.
2. When will our 2022 benefits coverage be effective?
Coverage elected during Open Enrollment is effective on January 1, 2022 and will be in effect through December 31, 2022.
3. What happens if I miss Open Enrollment? This year, if you do not participate in Open
Enrollment your 2021 benefits will rollover into 2022 (EXCEPT for Flexible Spending Accounts,
enrollment is required every year).
4. When do I need to submit a Dependent Child Certification Form?
The form must be submitted for a dependent child who will be at least 18 years of age on December 31, 2021 and not more than 22 years of age on December 31, 2021 and is enrolled in Dental and/or Vision coverage for 2022 (and are full-time students and tax dependents).
5. If I am enrolling a dependent on my Health insurance for the first time or continuing to cover a Dependent (age 19-22) on my Dental/Vision insurance, do I need to provide any documentation to Human Resources?
Yes. If you are enrolling or continuing coverage for a Dependent (age 19-22) on Dental/Vision insurance for 2022, or if you are enrolling a new dependent you will need to provide supporting documentation. For a new dependent, please provide your Human Resources Department a copy of your marriage
license, a birth certificate, etc. For a Dependent (age 19-22) on Dental/Vision insurance, you MUST complete the Dependent Child Certification Form (included in your Open Enrollment material in the “yellow” envelope or in your Open Enrollment Guide). Documentation MUST be submitted to establish/continue eligibility.
6. Are the deductibles and out-of-pocket maximums separate for the different networks within the Health insurance plans?
Yes, deductible and out-of-pocket maximums are maintained separately for each network.
7. How long may my child remain on my Health insurance?
Children of an employee are eligible for coverage under the health plan until their 26th birthday, regardless of student status. Coverage is generally extended to the end of the month in which the child turns age 26. Different rules apply to Dental and Vision coverage.
8. How long may my child remain on my Dental or Vision insurance?
Children of an employee can remain on the Dental and/or Vision coverage to the end of the calendar year in which they have their 18th birthday. Children who are age 19 to 23 may be covered on the Dental and Vision insurance as long as they are full-time students and tax dependents of the employee. Coverage is generally extended to the end of the year in which the child turns age 23 (with completion of a Dependent Child Certification Form).
9. How is the single deductible met? The single deductible is met by any single covered
member who incurs expenses subject to the deductible. When the total expenses reach the limit for the plan, the deductible has been met. For example, MHA Premier has an individual deductible of $500, once the person reaches $500 in expenses, the single deductible has been met.
10. How is the family deductible met? The family deductible can be met by any combination
of two or more covered members in the family incurring expenses subject to the deductible. For example, MHA Premier has a family deductible of $1,000, if the first family member reaches $500 of the deductible, then the second family member reaches $250 of the deductible and finally the third family member reaches $250 of the deductible, the family deductible has been met ($500 + 250 + 250 = $1,000). If, however, only one family member has
YOUR QUESTIONS ANSWERED
26
2022 MyChoiceOpen Enrollment Guide
YOUR QUESTIONS ANSWERED CONTINUED
$1,000, in expenses, the family deductible has not been met (because a single member’s deductible is capped at the individual level).
11. If I miss the Open Enrollment period entirely, when can I make changes to my Health benefits?
You may make changes if you experience a change in status event (i.e. loss of coverage, marriage, birth of a child, divorce, etc). You have 30 days from the date of the change in status event to notify Human Resources and change your coverage. Notices received after 30 days cannot be accepted and you will have to wait until the next Open Enrollment to make the desired changes.
12. If I elect coverage during my Open Enrollment and my spouse has Open Enrollment at a later date, can I make changes to my plan?
Yes, we will require documentation from the spouse’s employer on company letterhead identifying the Open Enrollment deadline, effective dates and persons who are being added to or dropped from the other employer’s policy.
13. May I enroll in the FSAs even if I don’t elect Health insurance?
Yes, you do not need to enroll in any of the health care benefits in order to take advantage of the FSAs.
14. How does the Voluntary Long-Term Disability plan define total disability?
Total disability means that due to an injury or sickness, during the elimination and own occupation periods, you are unable to perform each of the main duties of you regular occupation due to an injury or sickness. Upon completion of the own occupation period, total disability means you are unable to perform the main duties of any gainful occupation which your training, education, or experience will reasonably allow. Contact your Human Resources Department or Benefits Analyst with questions regarding Long-Term Disability.
15. Will I receive a confirmation statement after Open Enrollment?
No. However, you will be able to go into PeopleSoft-MyHR, click on the “Benefits Details” tile (in Employee Self Service), change the “As Of” date to 01/01/2022 to see the 2022 elections you made during Open Enrollment. You will not be able to see this information until Open Enrollment has been finalized and approved. Corporate Benefits will send out an email to all employees when they can go
into Employee Self Service to look at their elections for 2022. Look for this announcement sometime in December 2021.
16. I do not have access to a computer at work. How can I enroll online?
You may use any computer (on-site kiosk, home, library, family member) that has internet access with a Chrome browser for optimal use when enrolling online.
17. Will the online Open Enrollment system be available 24 hours a day?
The online Open Enrollment system will be available from November 1 through November 15 at 5 pm and can be accessed 24 hours a day through the PeopleSoft-MyHR system.
18. What should I do if I have problems accessing the PeopleSoft-MyHR system?
You may contact the National Service Desk by calling (810) 342-2026.
27
2022 MyChoiceOpen Enrollment Guide
* If you have any questions regarding your benefits, contact the Benefits Analyst listed for your subsidiary.
BENEFITS CONTACTS
Benefit Plan / Carrier Telephone Number WebsiteDental Plan
Delta Dental Plan of Michigan (800) 524-0149 deltadentalmi.com
Employee Assistance Program
GuidanceResources (844) 449-6539 guidanceresources.com
Family Medical Leave
Lincoln Financial Group (800) 290-0164
Flexible Spending Accounts (FSA)
McLaren Health Advantage (888) 327-0671 benefitspaymentsystem.com
Health Plan
Blue Cross Blue Shield of Michigan (877) 790-2583 bcbsm.com
McLaren Health Advantage (888) 327-0671 mclarenhealthplan.org
Human Resources - Benefits*
Corporate Benefits (810) 342-4650 or (866) 238-2419 (option 2)
Karmanos Cancer Institute - Jane Duncan (248) 304-2933
Lake Orion Nursing & Rehabilitation Center - Nikki Spencer (810) 342-4674
McLaren Bay Region - Amanda Cornacchio (810) 342-4672
McLaren Caro Region - Hollice Londry (989) 672-5104
McLaren Central Michigan - Nikki Spencer (810) 342-4674
McLaren Flint - Amber Miller (810) 342-4949
McLaren Greater Lansing - Brenda Johns (231) 487-3023
McLaren Health Care - Amanda Cornacchio (810) 342-4672
McLaren Integrated HMO Group - Amber Miller (810) 342-4949
McLaren Health Management Group - Amanda Cornacchio (810) 342-4672
McLaren Lapeer Region - Amanda Cornacchio (810) 342-4672
McLaren Macomb - Nikki Spencer (810) 342-4674
McLaren Medical Group - Brenda Johns (231) 487-3023
McLaren Northern Michigan - Brenda Johns (231) 487-3023
McLaren Oakland - Nikki Spencer (810) 342-4674
McLaren Port Huron - Shelia Closs (810) 989-3115
McLaren St. Luke’s - Amie Gohlike (419) 893-6646
McLaren Thumb Region - Kim Affer (989) 269-1544
Life Insurance
Lincoln Financial Group (800) 423-2765
Long-Term Disability (LTD)/Short-Term Disability (STD)
Lincoln Financial Group (800) 290-0164
Retirement Plan
Empower Retirement (800) 743-5274 retiresmart.com
Vision Plan
EyeMed (866) 723-0596 eyemedvisioncare.com
28
2022 MyChoiceOpen Enrollment Guide
Premium Assistance Under Medicaid and theChildren’s Health Insurance Program (CHIP) If you or your children are eligible for Medicaid or CHIP and you’re eligible for health coverage from your employer, your state may have a premium assistance program that can help pay for coverage, using funds from their Medicaid or CHIP programs. If you or your children aren’t eligible for Medicaid or CHIP, you won’t be eligible for these premium assistance programs but you may be able to buy individual insurance coverage through the Health Insurance Marketplace. For more information, visit www.healthcare.gov.
If you or your dependents are NOT currently enrolled in Medicaid or CHIP, and you think you or any of your dependents might be eligible for either of these programs, contact your State Medicaid or CHIP office or dial 1-877-KIDS-NOW or www.insurekidsnow.gov to find out how to apply. If you qualify, ask your state if it has a program that might help you pay the premiums for an employer-sponsored plan.
If you or your dependents are eligible for premium assistance under Medicaid or CHIP, as well as eligible under your employer plan, your employer must allow you to enroll in your employer plan if you aren’t already enrolled. This is called a “special enrollment” opportunity, and you must request coverage within 60 days of being determined eligible for premium assistance. If you have questions about enrolling in your employer plan, contact the Department of Labor at www.askebsa.dol.gov or call 1-866-444-EBSA (3272).
Newborn’s and Mother’s Health Protection ActGroup health plans and health insurance issuers may not, under federal law, restrict benefits for any hospital length of stay in connection with childbirth for the mother or newborn child to less than 48 hours following a vaginal delivery or less than 96 hours following a cesarean section; however, federal law does not prohibit the mother’s or newborn’s attending provider, after consulting with the mother, from discharging the mother or her newborn earlier than 48 hours (or 96 hours as applicable). In any case, plans and issuers may not, under federal law, require that a provider obtain authorization from the plan or the issuer for prescribing a length of stay not in excess of 48 hours (or 96 hours).
Special Enrollment RightsYou and your eligible dependents may enroll in the medical benefit program (or change medical benefit options) under the McLaren Health Care Employee Benefit Plan (the “Plan”) under the following circumstances. Individuals Losing Other Coverage. If you declined coverage under the medical benefit program when it was first available because of other health coverage, and that coverage is later lost on account of:n Exhaustion of COBRA continuation coverage, Lost
eligibility for other coverage, orn Termination of employer premiums toward the other
coverage.
You and your eligible dependents may enroll in the medical benefit program on or before the date that is 30 days after the date you lost that other coverage.
Lost Eligibility for Other Coverage includes a loss of other health coverage as a result of your legal separation or divorce, a dependent’s loss of dependent status, death, termination of employment or reduction in number of hours of employment, or you no longer reside, live or work in the service area of a health maintenance organization in which you participated. Coverage will be effective as of the first day of the next calendar month following receipt of the request for special enrollment.
You must request enrollment on or before the date that is 30 days after the qualifying life event.
New Eligible Dependents. If you initially declined enrollment for yourself or your eligible dependents and you later have a new eligible dependent because of marriage, birth, adoption or placement for adoption, you may enroll yourself and your new eligible dependents (including an eligible dependent spouse if you have a new eligible dependent child), as long as you request enrollment on or before the date that is 30 days after the marriage, birth, adoption or placement for adoption. For example, if you and your eligible dependent spouse have a child, you may enroll yourself, your eligible dependent spouse and your new child in the Plan’s medical benefit program, even if you were not previously enrolled. You will not, however, be able to enroll existing
28
YOU SHOULD KNOW...
29
2022 MyChoiceOpen Enrollment Guide
eligible dependent children for whom coverage has been waived in the past.
For marriage, birth, adoption or placement for adoption, you or your eligible dependent’s participation will start as of the date of the marriage, birth, adoption or placement for adoption, as long as you timely request enrollment and you submit the Enrollment Form and proof of your dependent’s status as an eligible dependent to Corporate Benefits, McLaren Corporate Human Resources, within 30 days after the marriage, birth, adoption or placement for adoption.
Medicaid and CHIPIf you or your eligible dependent children are eligible for, but not enrolled in, the Plan’s medical benefit program and you or your eligible dependent children:n Lose coverage under Medicaid or a State child
health plan (“CHIP”), orn Become eligible for a premium assistance subsidy
through Medicaid or CHIP,
you and your eligible dependent children may enroll in the medical benefit program, as long as you request enrollment on or before the date that is 60 days after
the loss of coverage or the date you or your eligible dependent children became eligible for the premium subsidy. Your or your eligible dependent’s enrollment and coverage will take effect as of the date of the loss of coverage, or the date you or your eligible dependents became eligible for the premium subsidy, as long as you timely request to enroll.
These 30-day and 60-day periods are “special enrollment periods.” To request special enrollment or to obtain more information, contact the Corporate Benefits, McLaren Corporate Human Resources.
Women’s Health and Cancer Rights Act of 1998The McLaren health plans cover surgery after a mastectomy to:n Reconstruct the breast on which the mastectomy
was performedn Reconstruct the other breast to produce a
symmetrical appearance
This coverage is required by law. Prostheses and physical complications in all stages of the mastectomy, including lymphedemas, are also covered.
The plan will determine the manner of coverage in consultation with the attending physician and patient. Coverage for breast reconstruction and related services will be subject to deductibles and coinsurance amounts consistent with those that apply to other benefits under the plan.
Women’s Preventive Care:The Affordable Care Act requires that health plans cover and eliminate cost sharing for the following eight women’s preventive services:1. Well-woman visits2. Gestational diabetes screening3. Human Papillomavirus (HPV) DNA testing4. Sexually-transmitted infections (STIs) counseling5. Human Immunodeficiency Virus (HIV) screening and
counseling6. Contraception and contraceptive counseling7. Breastfeeding support, supplies and counseling8. Interpersonal and domestic violence screening and
counseling
Effective January 1, 2013, any women seeking the above services will not be subject to cost sharing, coinsurance or deductibles.
Qualifying Life EventsYou may qualify to enroll during
special enrollment periods if you:
moved to a new area
got married
lost coverage
got divorced
had a baby or adopted
had errors enrolling
changed your income
aged off a parents plan
lost student health insurance
You must request enrollment on or beforethe date that is 30 days after the qualifying life event.
29
30
2022 MyChoiceOpen Enrollment Guide
30
YOU SHOULD KNOW... CONTINUED
Notice of Privacy PracticesFor McLaren Health Care Employee Benefit Plan, McLaren Health Care Retiree Welfare Benefit Plan and McLaren Health Care Retiree Benefit Plan
Version effective: May 2020
THIS NOTICE DESCRIBES HOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY.
The Health Insurance Portability and Accountability Act of 1996 (HIPAA), and the rules to carry out this law (Privacy Rules), require health plans to notify participants and beneficiaries about the policies and practices the Plan has adopted to protect the confidentiality of their health information, including health care payment information.
This Notice describes the privacy policies of the group health benefits, including the medical, prescription drug , dental, vision, health reimbursement account and health flexible spending account benefit programs, and the employee assistance program, offered under the McLaren Health Care Employee Benefit Plan, McLaren Health Care Retiree Welfare Benefit Plan, or the McLaren Health Care Retiree Benefit Plan (the “Plan” or “Plans”) sponsored by McLaren Health Care Corporation and on which subsidiaries participate (the “Corporation”). These policies protect medical information (including genetic information) relating to your past, present and future medical conditions, health care treatment and payment for that treatment (Protected Health Information or PHI).
The law requires the Plan to maintain the privacy of your PHI, to provide you with this Notice of its legal duties and to abide by the terms of this Notice. In general, the Plan may only use and/or disclose your PHI where required or permitted by law or when you authorize the use or disclosure. The Plan may also only use the minimum amount of your PHI that is necessary to accomplish the intended purpose of the use or disclosure as permitted by HIPAA.
HEALTH INFORMATION NOT COVERED BY THIS NOTICE
This Notice does not cover:
n Health information that does not identify you and with respect to which there is no reasonable basis to believe that the information could be used to identify you, or
n Health information that the Corporation can have under applicable law (e.g., the Family and Medical Leave Act, the Americans with Disabilities Act, workers’ compensation laws, federal and State occupational health and safety laws, and other State and federal laws), or that the Corporation properly can get for employment-related purposes through sources other than the Plan and that is kept as part of your employment records (e.g., pre-employment physicals, drug testing and fitness for duty examinations)
WHEN THE PLAN MUST DISCLOSE YOUR PHI
The Plan must disclose your PHI:
n To you,
n To the Secretary of the United States Department of Health and Human Services (DHHS) to determine whether the Plan is in compliance with HIPAA, and
n Where required by law. This means the Plan will make the disclosure only when the law requires it do so, but not if the law would just allow it to do so.
WHEN THE PLAN MAY DISCLOSE YOUR PHI WITHOUT YOUR AUTHORIZATION
Treatment. The Plan does not provide medical treatment directly, but it may disclose your PHI to a health care provider who is giving treatment. The Plan may also send your PHI to health care providers for patient safety or other treatment-related reasons. For example, the Plan may disclose the types of prescription drugs you currently take to an emergency room physician, if you are unable to provide your medical history due to an accident.
Payment. The Plan may disclose your PHI, as needed, to pay for your medical benefits. For example, the Plan may tell a doctor whether you are eligible for coverage or what percentage of the bill the Plan might pay. The Plan may also use or disclose your PHI in other ways to administer benefits — for example, to process and review claims, to coordinate benefits with other health plans, to exercise its subrogation rights, to obtain payment under stop-loss insurance or re-insurance policies and to do utilization review and pre-authorizations.
Health Care Operations. The Plan may use and/or disclose your PHI to make sure the Plan is well run, administered properly and does not waste money. For example, the Plan may use information about your claims to project future benefit costs or audit the accuracy of its claims processing functions. The Plan may also disclose your PHI for placing a contract under a stop-loss or re-insurance policy. Among other things, the Plan may also use your PHI to undertake underwriting, premium rating and other insurance activities relating to changing health insurance contracts or health benefits. However, federal law prohibits the Plan from using or disclosing PHI that is genetic information (e.g., family medical history) for underwriting purposes, which include eligibility determinations, calculating premiums, and any other activities related to the creation, renewal or replacement of a health insurance contract or health benefits.
To the Corporation. In certain cases, the Plan may disclose your PHI to the Corporation.
n Some of the people who administer the Plan work for the Corporation. Before your PHI can be used by or disclosed to these Corporate employees, the Corporation must certify that it has: (1) amended the Plan documents to explain how your PHI will be protected; (2) identified the Corporation employees who need your PHI to carry out their duties to administer the Plan; and (3) separated the work of these employees from the rest of the workforce so that the Corporation cannot use your PHI for employment-related purposes or to administer other benefit plans. For example, these designated employees will be able to contact an insurer or third-party administrator to find out about the status of your benefit claims without your specific authorization.
n The Plan may disclose information to the Corporation that summarizes the claims experience of Plan participants as a group, but without identifying specific individuals, to get new benefit insurance or to change or terminate the Plan. For example, if the Corporation wants to consider adding or changing organ transplant benefits, it may receive this summary health information to assess the costs of those services.

31
2022 MyChoiceOpen Enrollment Guide
31
n The Plan may also disclose limited health information to the Corporation in connection with the enrollment or disenrollment of individuals into or out of the Plan.
To Business Associates. The Plan may hire third parties that may need your PHI to perform certain services on behalf of the Plan. These third parties are Business Associates of the Plan. Business Associates (and their subcontractors) must protect any PHI they receive from, or create and maintain on behalf of, the Plan. For example, the Plan may hire a third-party administrator to process claims, an auditor to review how an insurer or third-party administrator is processing claims, an insurance agent to assess coverages and help with claim problems or a service provider to provide health benefits (such as wellness benefits).
To Individuals Involved with Your Care or Payment for Your Care. The Plan may disclose your PHI to adult members of your family or another person identified by you who is involved with your care or payment for your care if: (1) you authorize the Plan to do so; (2) the Plan informs you that it intends to do so and you do not object; or (3) the Plan infers from the circumstances, based upon professional judgment, that you do not object to the disclosure. The Plan will, whenever possible, try to get your written objection to these disclosures (if you wish to object), but in certain circumstances, it may rely on your oral agreement or disagreement to disclosures to family members.
To Personal Representatives. The Plan may disclose your PHI to someone who is your personal representative. Before the Plan will give that person access to your PHI or allow that person to take any action on your behalf, it will require him or her to give proof that he or she may act on your behalf — for example, a court order or power of attorney granting that person such power. Generally, the parent of a minor child will be the child’s personal representative. In some cases, however, State law allows minors to obtain treatment (e.g., sometimes for pregnancy or substance abuse) without parental consent, and in those cases, the Plan may not disclose certain information to the parents. The Plan may also deny a personal representative access to PHI to protect people, including minors, who may be subject to abuse or neglect.
To Spouses and Other Family Members. With only limited exceptions, the Plan will send all mail to the employee. This includes mail relating to the employee’s spouse and other family members who are covered under the Plan, and includes mail with information on the use of Plan benefits by the employee’s spouse and other family members and information on the denial of any Plan benefits to the employee’s spouse and other family members. If you have requested restrictions or confidential communications (see “Your Individual Rights”), and if the Plan has agreed to the request, the Plan will send mail as provided by the request.
For Treatment Alternatives or Health-Related Benefits and Services. The Plan may contact you to provide information about treatment alternatives or other health-related benefits or services that may be of interest to you.
For Public Health Purposes. The Plan may: (1) report specific disease or birth/death information to a public health authority authorized to collect that information; (2) report reactions to medication or problems with medical products to the Food and Drug Administration to help ensure the quality, safety or effectiveness of those medications or medical products; or (3) if authorized by law, disclose PHI to a person who may have been exposed to a communicable disease or who may otherwise be at risk of contracting or spreading a disease or medical condition.
For Fundraising. The Plan may use, and disclose to a business or to an institutionally related foundation, certain types of PHI for the purpose of raising funds. The type of information that may be disclosed without your authorization is: (1) demographic information relating to an individual; (2) dates of health care provided to an individual; and (3) health insurance status. The Plan may also contact you to raise funds as permitted by HIPAA, and you have a right to opt out of receiving such communications.
To Report Violence and Abuse. The Plan may report information about victims of abuse, neglect or domestic violence to the proper authorities.
For Health Oversight Activities. The Plan may disclose PHI for civil, administrative or criminal investigations, oversight inspections, licensure or disciplinary actions (e.g., to investigate complaints against medical providers), and other activities for the oversight of the health care system or to monitor government benefit programs.
For Lawsuits and Disputes. The Plan may disclose PHI in response to an order of a court or administrative agency, but only to the extent expressly authorized in the order. The Plan may also disclose PHI in response to a subpoena, a lawsuit discovery request or other lawful process, but only if the Plan has received adequate assurances that the information to be disclosed will be protected. The Plan may also disclose PHI in a lawsuit if necessary for payment or health care operations purposes.
For Law Enforcement. The Plan may disclose PHI to law enforcement officials for law enforcement purposes and to correctional institutions regarding inmates.
To Coroners, Funeral Directors and Medical Examiners. The Plan may disclose PHI to a coroner or medical examiner — for example, to identify a person or determine the cause of death. The Plan may also release PHI to a funeral director who needs it to perform his or her duties.
For Organ Donations. The Plan may disclose PHI to organ procurement organizations to facilitate organ, eye or tissue donations.
For Limited Data Sets. The Plan may disclose PHI for use in a limited data set for purposes of research, public health or health care operations, but only if a data use agreement has been signed.
To Avert Serious Threats to Health or Safety. The Plan may disclose PHI to avert a serious threat to your health or safety or that of members of the public.
For Special Governmental Functions. The Plan may disclose PHI to authorized federal officials in certain circumstances. For example, disclosure may be made for national security purposes or for members of the armed forces if required by military command authorities.
For Workers’ Compensation. The Plan may disclose PHI for workers’ compensation if necessary to comply with these laws.
For Research. The Plan may disclose PHI for research studies, subject to special procedures intended to protect the privacy of your PHI.
For Emergencies and Disaster Relief. The Plan may disclose PHI to organizations engaged in emergency and disaster relief efforts.

YOU SHOULD KNOW... CONTINUED
In addition to the Privacy Rules, special protections under State or other federal law may apply to the use and disclosure of your PHI. The Plan will comply with these State or federal laws where they are more protective of your privacy, but only to the extent these laws are not superseded by federal preemption.
WITH YOUR WRITTEN AUTHORIZATION
In most cases, if you give us permission in writing, we may use and disclose your health information to the extent you have given us authorization. If you give us permission, you have the right to change your mind and revoke it. This must be in writing, too. We cannot take back any uses or disclosures already made with your permission. Note: We are prohibited from and will not use your genetic information for underwriting purposes even with your permission or authorization
YOUR PRIVACY RIGHTS
You have the following rights regarding your PHI that we maintain.
Right to Inspect and Copy. In most cases, you have the right to look at or get copies of your records. You may be charged a fee for the cost of copying your records.
Right to Amend. You may ask us to change your records that are in our possession if you feel that there is a mistake. We can deny your request for certain reasons, but we must give you a written reason for our denial.
Right to a List of Disclosures. At your request, the Plan must provide you with a list of the Plan’s disclosures of your PHI made within the six-year period just before the date of your request, except disclosures made:
n For purposes of treatment, payment or health care operations,
n Directly to you or close family members involved in your care,
n For purposes of national security,
n Incidental to otherwise permitted or required disclosures,
n As part of a limited data set,
n To correctional institutions or law enforcement officials, or
n With your express authorization.
You may request one accounting, which the Plan must provide at no charge, within a single 12-month period. If you request more than one accounting within the same 12-month period, the Plan may charge you a reasonable fee.
Right to Request Restrictions on Our Use or Disclosure of your PHI. You have the right to ask for limits on how your PHI is used or disclosed. We are not required to agree to such requests. A restriction cannot prevent uses or disclosures that are required by the Secretary of DHHS to determine or investigate the Plan’s compliance with the Privacy Rules or that are otherwise required by law. You may also request that your health care provider not disclose your PHI for a health care item or service to the Plan for purposes of payment or health care operations if you have paid the item or service out-of-pocket in full. Please note that if your health care provider does not disclose the item or service to the Plan, the amount you paid for the item or service will not count toward your annual deductible or any out-of-pocket maximums under the Plan. The provider may also charge you the out-of-network rate for the item or service.
Right to Receive Notification of a Breach. If our actions result in a breach of your unsecured PHI we will notify you of that breach.
Right to Request Confidential Communications. You have the right to ask that we share information with you in a certain way or in a certain place. For example, you may ask us to send you information at your work address instead of your home address. The Plan will accommodate any reasonable request, though it will require that any alternative used still allow for payment information to be effectively communicated and for payments to be made.
Genetic Information. Genetic information is health information. We are prohibited from and do not use or disclose your genetic information for underwriting purposes.
CHANGES TO THIS NOTICE
The Plan reserves the right to change the terms of this Notice and to make the new revised Notice provisions effective for all PHI that it maintains, including any PHI created, received or maintained by the Plan before the date of the revised Notice. If you agree, the Plan may provide you with a revised Notice electronically. Otherwise, the Plan will provide you with a paper copy of the revised Notice. In addition, the Plan will post the revised Notice on its website used to provide information about the Plan’s benefits.
OTHER INFORMATION
Copies of Our Notice of Privacy Practices. You may ask for a copy of our current Notice at any time. If the Notice was sent to you electronically, you may request a paper copy.
Complaints. If you have any questions about this Notice of Privacy Practices, or questions or complaints about the handling of your health information, you may contact the Information Privacy Office, in writing or call or submit a report to our Compliance Line. You may also send a written complaint to the Secretary of the United States Department of Health and Human Services. You will not be penalized for filing a complaint.
Who to contact. To exercise any of the rights described above, please submit a written request to the Plan’s Information Privacy Office by mail at the address below, by email to [email protected] or by fax to 810-342-1450.
McLaren Health CareInformation Privacy Office
One McLaren ParkwayGrand Blanc, MI 48439
Compliance Line: 1-866-642-2667
00 MyChoice 2022 OE (10.21)
Corporate Human ResourcesOne McLaren ParkwayGrand Blanc, Michigan 48439
mclaren.org

ReliaStar Life Insurance Company a member of the Voya® family of companies
Accident Insurance Explore Your Benefits & Costs
Cleaning the gutters. Yoga class. Soccer practice. Life offers plenty of opportunities
for accidental injuries. When an injury happens, Accident Insurance can help. This document includes expanded cost and benefit information for Accident Insurance. As you explore, keep in mind:
Accident Insurance doesn’t replace your medical coverage; instead, it complements it. The benefit payments
don’t go out to pay for medical bills or treatments you may need, instead they come in—directly to you—
to be used however you’d like. Choose this supplemental health insurance product for added protection if one of the following covered conditions comes your way.
Accident Insurance is a limited benefit policy. It is not health insurance, and does not satisfy the requirement of minimum essential coverage under the Affordable Care Act.
No medical questions or tests are required for Accident
coverage.
Simplified claims process has limited paperwork and can be
submitted/tracked online.
Benefit payments go directly to you. Use them how you’d like!
Group Name: McLaren Health Care Corporation Group Number: 696030 Class: Employees working 20+ hours per week
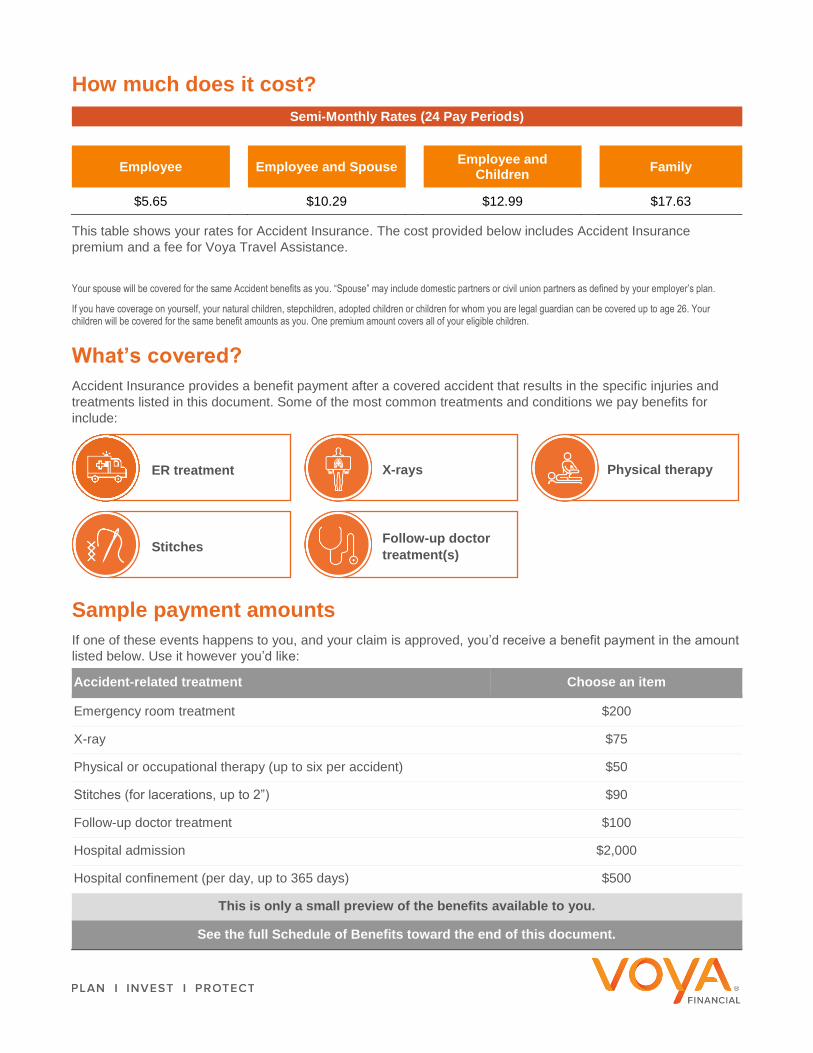
How much does it cost?
Semi-Monthly Rates (24 Pay Periods)
Employee Employee and Spouse
Employee and Children
Family
$5.65 $10.29 $12.99 $17.63
This table shows your rates for Accident Insurance. The cost provided below includes Accident Insurance premium and a fee for Voya Travel Assistance. Your spouse will be covered for the same Accident benefits as you. “Spouse” may include domestic partners or civil union partners as defined by your employer’s plan.
If you have coverage on yourself, your natural children, stepchildren, adopted children or children for whom you are legal guardian can be covered up to age 26. Your children will be covered for the same benefit amounts as you. One premium amount covers all of your eligible children.
What’s covered?
Accident Insurance provides a benefit payment after a covered accident that results in the specific injuries and treatments listed in this document. Some of the most common treatments and conditions we pay benefits for include:
Sample payment amounts
If one of these events happens to you, and your claim is approved, you’d receive a benefit payment in the amount
listed below. Use it however you’d like:
Accident-related treatment Choose an item
Emergency room treatment $200
X-ray $75
Physical or occupational therapy (up to six per accident) $50
Stitches (for lacerations, up to 2”) $90
Follow-up doctor treatment $100
Hospital admission $2,000
Hospital confinement (per day, up to 365 days) $500
This is only a small preview of the benefits available to you.
See the full Schedule of Benefits toward the end of this document.
ER treatment X-rays Physical therapy
Stitches Follow-up doctor
treatment(s)
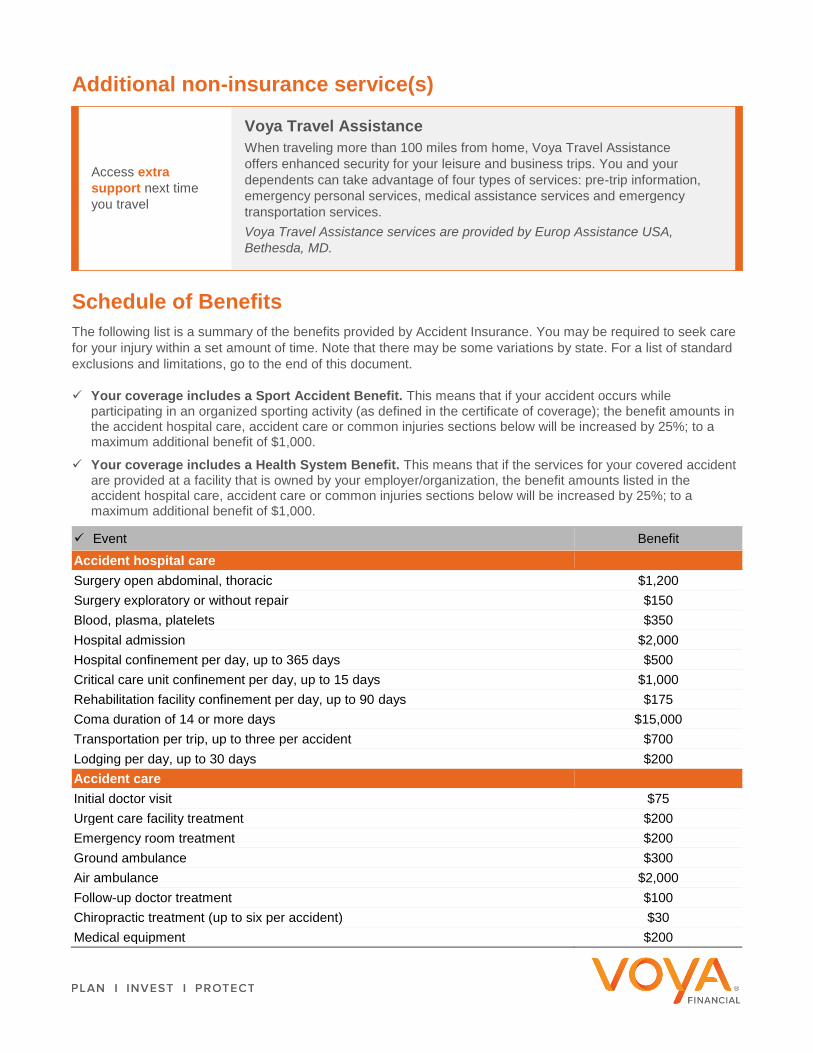
Additional non-insurance service(s)
Schedule of Benefits
The following list is a summary of the benefits provided by Accident Insurance. You may be required to seek care for your injury within a set amount of time. Note that there may be some variations by state. For a list of standard exclusions and limitations, go to the end of this document.
Your coverage includes a Sport Accident Benefit. This means that if your accident occurs while participating in an organized sporting activity (as defined in the certificate of coverage); the benefit amounts in the accident hospital care, accident care or common injuries sections below will be increased by 25%; to a maximum additional benefit of $1,000.
Your coverage includes a Health System Benefit. This means that if the services for your covered accident are provided at a facility that is owned by your employer/organization, the benefit amounts listed in the accident hospital care, accident care or common injuries sections below will be increased by 25%; to a maximum additional benefit of $1,000.
Event Benefit Accident hospital care
Surgery open abdominal, thoracic $1,200 Surgery exploratory or without repair $150 Blood, plasma, platelets $350 Hospital admission $2,000 Hospital confinement per day, up to 365 days $500 Critical care unit confinement per day, up to 15 days $1,000 Rehabilitation facility confinement per day, up to 90 days $175 Coma duration of 14 or more days $15,000 Transportation per trip, up to three per accident $700 Lodging per day, up to 30 days $200 Accident care
Initial doctor visit $75 Urgent care facility treatment $200 Emergency room treatment $200 Ground ambulance $300 Air ambulance $2,000 Follow-up doctor treatment $100 Chiropractic treatment (up to six per accident) $30 Medical equipment $200
Voya Travel Assistance
When traveling more than 100 miles from home, Voya Travel Assistance offers enhanced security for your leisure and business trips. You and your dependents can take advantage of four types of services: pre-trip information, emergency personal services, medical assistance services and emergency transportation services. Voya Travel Assistance services are provided by Europ Assistance USA,
Bethesda, MD.
Access extra
support next time you travel

Event Benefit Physical Therapy (up to six per accident) $50 Occupational & Speech therapy (up to six per accident) $50 Prosthetic device (one) $1,000 Prosthetic device (two or more) $2,000 Major diagnostic exam $250 Outpatient surgery (one per accident) $250 X-ray $75 Common injuries
Burns second degree, at least 36% of the body $1,500 Burns third degree, at least nine but less than 35 square inches of the body $8,500 Burns third degree, 35 or more square inches of the body $20,000 Skin grafts 50% of the burn benefit Emergency dental work: crown $400 Extraction $125 Eye injury removal of foreign object $500 Eye injury surgery $500 Torn knee cartilage surgery with no repair or if cartilage is shaved $250 Torn knee cartilage surgical repair $900 Laceration1 treated no sutures $50 Laceration1 sutures up to 2” $90 Laceration1 sutures 2” – 6” $350 Laceration1 sutures over 6” $800 Ruptured disk surgical repair $1,000 Tendon/ligament/rotator cuff exploratory arthroscopic surgery with no repair $400 Tendon/ligament/rotator cuff one, surgical repair $1,200 Tendon/ligament/rotator cuff two or more, surgical repair $1,800 Concussion $300 Paralysis - paraplegia $10,000 Paralysis - quadriplegia $20,000
Dislocations Non-surgical/ surgical
repair2
Hip joint $4,000/$8,000 Knee $2,500/$5,000 Ankle or foot bone(s) other than toes $1,700/$3,400 Shoulder $2,000/$4,000 Elbow $1,250/$2,500 Wrist $1,250/$2,500 Finger/toe $300/$600 Hand bone(s) other than fingers $1,250/$2,500 Lower jaw $1,250/$2,500 Collarbone $1,250/$2,500

Event Benefit
Fractures Non-surgical/ surgical
repair3
Hip $5,000/10,000 Leg $2,700/$5,400 Ankle $2,250/$4,500 Kneecap $2,250/$4,500 Foot excluding toes, heel $2,250/$4,500 Upper arm $2,400/$4,800 Forearm, hand, wrist except fingers $2,250/$4,500 Finger, toe $300/$600 Vertebral body $4,000/$8,000 Vertebral processes $1,750/$3,500 Pelvis except coccyx $3,500/$7,000 Coccyx $450/$900 Bones of face except nose $1,300/$2,600 Nose $650/$1,300 Upper jaw $1,600/$3,200 Lower jaw $1,750/$3,500 Collarbone $1,750/$3,500 Rib or ribs $450/$900 Skull – simple except bones of face $1,500/$3,000 Skull – depressed except bones of face $4,000/$8,000 Sternum $400/$800 Shoulder blade $2,250/$4,500 Chip fractures 25% of the closed
reduction amount
Laceration benefits are a total of all lacerations per accident. 2 Non-surgical repair of a completely separated joint may be referred to in your policy documentation as a “closed reduction.” Surgical repair of a completely separated joint may be referred to in your policy documentation as an “open reduction.” 3 Non-surgical repair of a fracture may be referred to in your policy documentation as a “closed reduction.” Surgical repair of a fracture may be referred to in your policy documentation as an “open reduction.”
Accidental Death & Dismemberment
Your coverage also includes Accidental Death & Dismemberment benefits. This means that if you are severely injured or pass away due to an accident, additional benefits may apply. See the chart below for more details. A “common carrier” is commercial transportation that operates on a regular schedule, between predetermined points or cities (such as a bus or airline route).
Benefit Accidental Death Benefits
Common carrier accident Employee $200,000 Spouse $200,000 Children $50,000
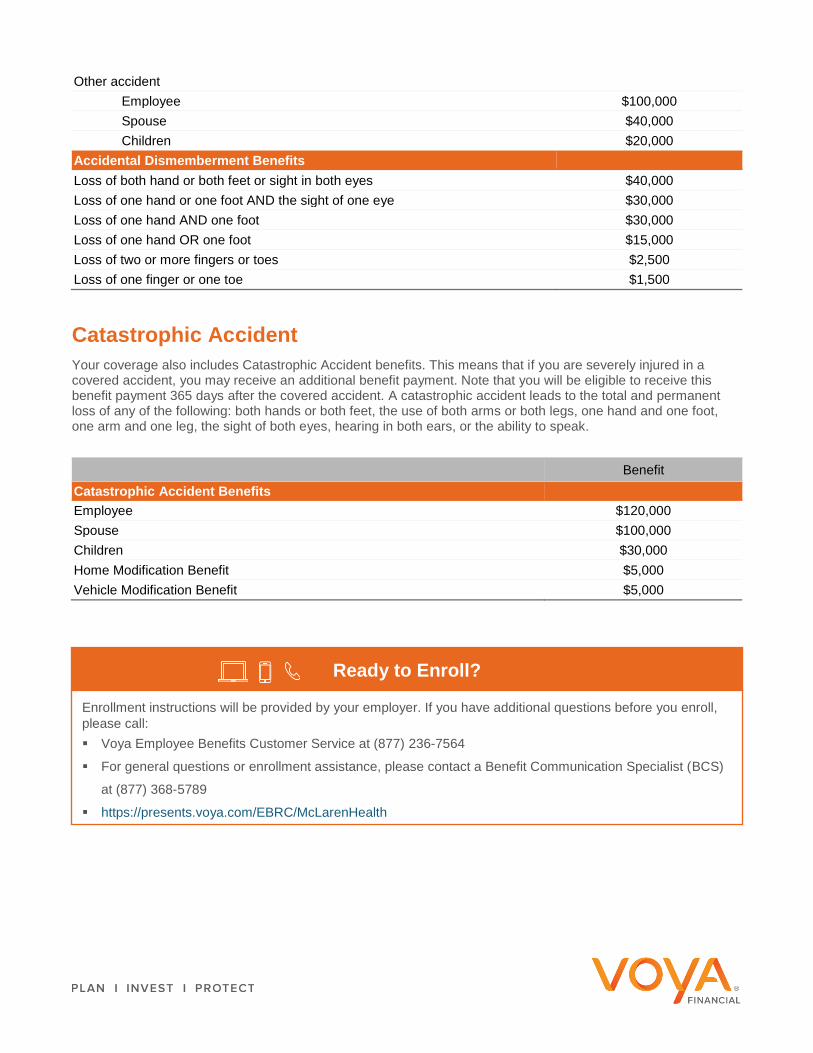
Other accident Employee $100,000 Spouse $40,000 Children $20,000
Accidental Dismemberment Benefits Loss of both hand or both feet or sight in both eyes $40,000 Loss of one hand or one foot AND the sight of one eye $30,000 Loss of one hand AND one foot $30,000 Loss of one hand OR one foot $15,000 Loss of two or more fingers or toes $2,500 Loss of one finger or one toe $1,500
Catastrophic Accident
Your coverage also includes Catastrophic Accident benefits. This means that if you are severely injured in a covered accident, you may receive an additional benefit payment. Note that you will be eligible to receive this benefit payment 365 days after the covered accident. A catastrophic accident leads to the total and permanent loss of any of the following: both hands or both feet, the use of both arms or both legs, one hand and one foot, one arm and one leg, the sight of both eyes, hearing in both ears, or the ability to speak.
Benefit Catastrophic Accident Benefits
Employee $120,000 Spouse $100,000 Children $30,000 Home Modification Benefit $5,000 Vehicle Modification Benefit $5,000
Ready to Enroll?
Enrollment instructions will be provided by your employer. If you have additional questions before you enroll, please call: Voya Employee Benefits Customer Service at (877) 236-7564
For general questions or enrollment assistance, please contact a Benefit Communication Specialist (BCS)
at (877) 368-5789
https://presents.voya.com/EBRC/McLarenHealth

Exclusions and limitations
Standard exclusions for the Certificate, Spouse Accident Insurance, and Children’s Accident Insurance and AD&D are listed below. (These may vary by state.) For a complete description of your available benefits, exclusions and limitations, see your certificate of insurance and any riders.
Benefits are not payable for any loss caused in whole or directly by any of the following*: Participation or attempt to participate in a felony or illegal activity. An accident while the covered person is operating a motorized vehicle while intoxicated. Intoxication means
the covered person’s blood alcohol content meets or exceeds the legal presumption of intoxication under the laws of the state where the accident occurred.
Suicide, attempted suicide or any intentionally self-inflicted injury, while sane or insane. War or any act of war, whether declared or undeclared, other than acts of terrorism. Loss sustained while on active duty as a member of the armed forces of any nation. We will refund, upon
written notice of such service, any premium which has been accepted for any period not covered as a result of this exclusion.
Alcoholism, drug abuse, or misuse of alcohol or taking of drugs, other than under the direction of a doctor. Riding in or driving any motor-driven vehicle in a race, stunt show or speed test. Operating, or training to operate, or service as a crew member of, or jumping, parachuting or falling from, any
aircraft or hot air balloon, including those which are not motor-driven. Flying as a fare-paying passenger is not excluded. Performing these acts as part of your employment with the employer is not excluded.
Engaging in hang-gliding, bungee jumping, parachuting, sail gliding, parasailing, parakiting, kite surfing or any similar activities.
Practicing for, or participating in, any semi-professional or professional competitive athletic contests for which any type of compensation or remuneration is received.
Any sickness or declining process caused by a sickness.
Exclusions and limitations for Catastrophic Accident coverage (may vary by state) are the same as the exclusions in the Certificate, plus the catastrophic accident benefit reduces to 50% at age 65 and to 25% of the initial benefit amount at age 70.
This is a summary of benefits only. A complete description of benefits, limitations, exclusions and termination of coverage will be provided in the certificate of insurance and
riders. All coverage is subject to the terms and conditions of the group policy. If there is any discrepancy between this document and the group policy documents, the policy
documents will govern. To keep coverage in force, premiums are payable up to the date of coverage termination. Accident Insurance is underwritten by ReliaStar Life
Insurance Company (Minneapolis, MN), a member of the Voya® family of companies. Policy Form #RL-ACC3-POL-16; Certificate Form #RL-ACC3-CERT-16; and Rider
Forms: Spouse Accident Rider Form #RL-ACC3-SPR-16, Children's Accident Rider Form #RL-ACC3-CHR-16, Wellness Benefit Rider Form #RL-ACC3-WELL-16, Accidental
Death & Dismemberment (AD&D) Rider Form #RL-ACC3-ADR-16, Catastrophic Accident Rider Form #RL-ACC3-CAR-16, Off Job Accident Disability Income Rider form
#RL-ACC3-DIR-16, Sickness Hospital Confinement Rider Form #RL-ACC3-HCR-16, Waiver of Premium Rider form #RL-ACC3-WOP-16, Continuation of Insurance Rider
form #RL-ACC3-CNT-16. Form numbers, provisions and availability may vary by state and employer’s plan.
1222304
ACC2 Only
Acct #0001 Date Prepared: 07/09/2021
212309-08152020

ReliaStar Life Insurance Company a member of the Voya® family of companies
Critical Illness Insurance Explore Your Benefits & Costs
There are more than just medical bills to pay after a heart attack, stroke, or other unexpected
covered medical condition. Critical Illness Insurance provides a benefit payment that can help. This document includes expanded cost and benefit information for Critical Illness Insurance. As you explore, keep in mind:
Critical Illness Insurance doesn’t replace your medical coverage; instead, it complements it. The benefit
payments don’t go out to pay for medical bills or treatments you may need, instead they come in—
directly to you—to be used however you’d like. Choose this supplemental health insurance product for added protection if one of the following covered conditions comes your way.
Critical Illness Insurance is a limited benefit policy. It is not health insurance, and does not satisfy the requirement of minimum essential coverage under the Affordable Care Act.
No medical questions or tests are required for coverage.
Employees get an annual Wellness Benefit of $50 for
completing an eligible health screening test.
Benefit payments go directly to you. Use them however you’d
like!
Group Name: McLaren Health Care Corporation Group Number: 696030 Class: Employees working 20+ hours per week
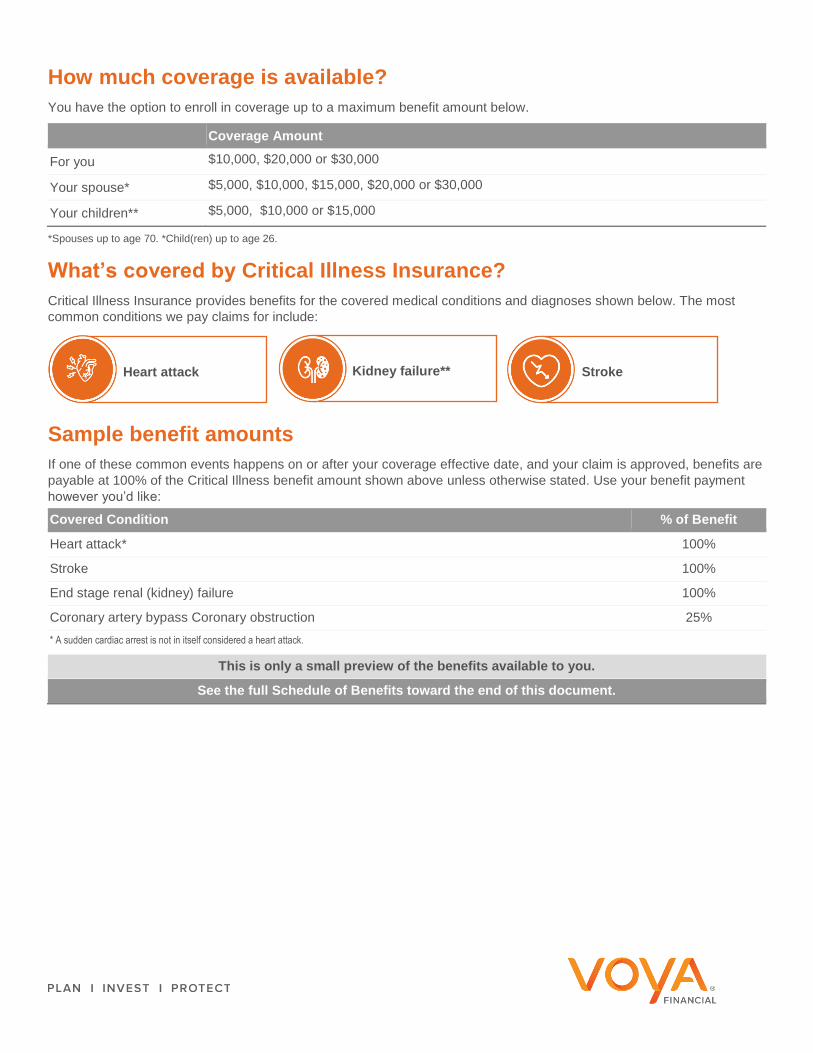
How much coverage is available?
You have the option to enroll in coverage up to a maximum benefit amount below.
Coverage Amount
For you $10,000, $20,000 or $30,000
Your spouse* $5,000, $10,000, $15,000, $20,000 or $30,000
Your children** $5,000, $10,000 or $15,000
*Spouses up to age 70. *Child(ren) up to age 26.
What’s covered by Critical Illness Insurance?
Critical Illness Insurance provides benefits for the covered medical conditions and diagnoses shown below. The most common conditions we pay claims for include:
Sample benefit amounts
If one of these common events happens on or after your coverage effective date, and your claim is approved, benefits are payable at 100% of the Critical Illness benefit amount shown above unless otherwise stated. Use your benefit payment however you’d like:
Covered Condition % of Benefit
Heart attack* 100%
Stroke 100%
End stage renal (kidney) failure 100%
Coronary artery bypass Coronary obstruction 25% * A sudden cardiac arrest is not in itself considered a heart attack.
This is only a small preview of the benefits available to you.
See the full Schedule of Benefits toward the end of this document.
Heart attack Kidney failure** Stroke
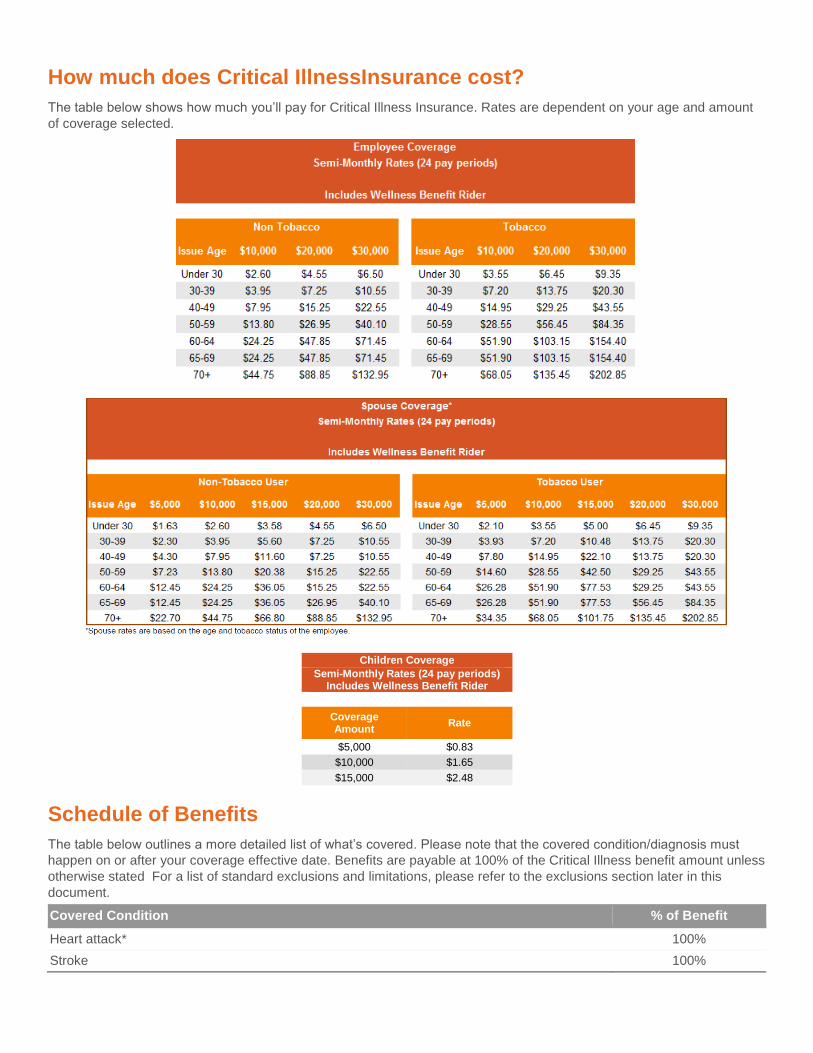
How much does Critical IllnessInsurance cost?
The table below shows how much you’ll pay for Critical Illness Insurance. Rates are dependent on your age and amount of coverage selected.
Children Coverage
Semi-Monthly Rates (24 pay periods) Includes Wellness Benefit Rider
Coverage Amount
Rate
$5,000 $0.83 $10,000 $1.65 $15,000 $2.48
Schedule of Benefits
The table below outlines a more detailed list of what’s covered. Please note that the covered condition/diagnosis must
happen on or after your coverage effective date. Benefits are payable at 100% of the Critical Illness benefit amount unless otherwise stated For a list of standard exclusions and limitations, please refer to the exclusions section later in this document.
Covered Condition % of Benefit
Heart attack* 100% Stroke 100%
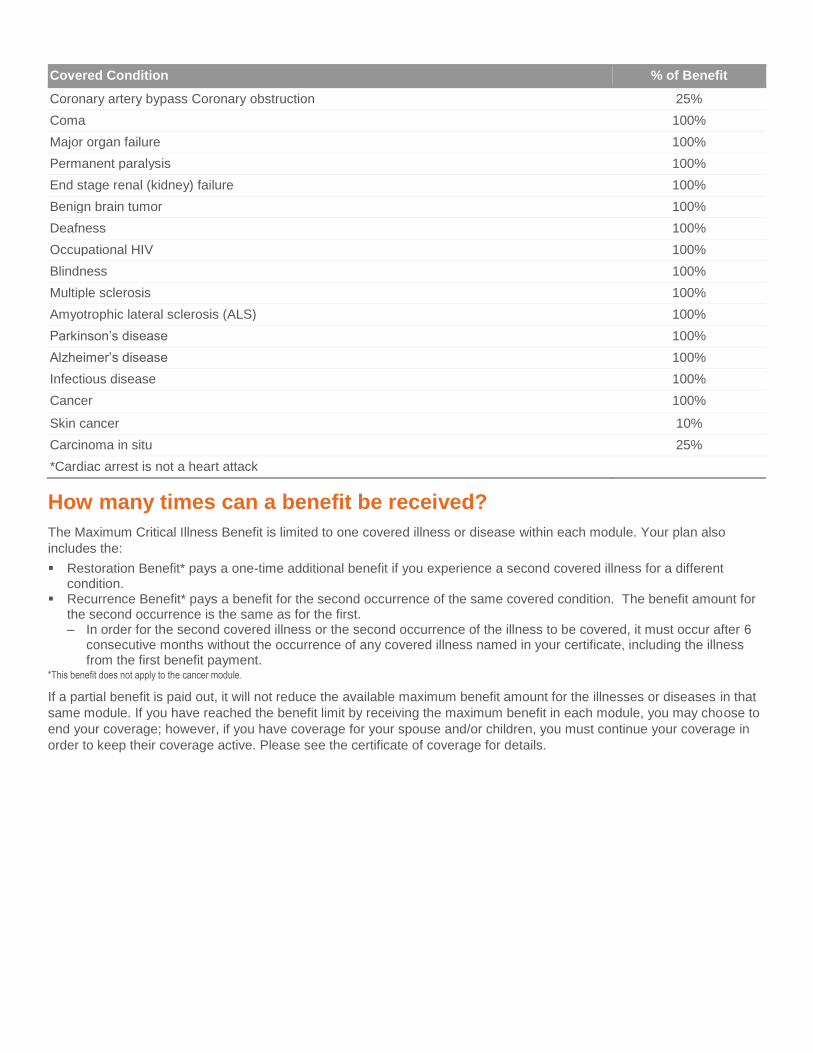
Covered Condition % of Benefit
Coronary artery bypass Coronary obstruction 25% Coma 100% Major organ failure 100% Permanent paralysis 100% End stage renal (kidney) failure 100% Benign brain tumor 100% Deafness 100% Occupational HIV 100% Blindness 100% Multiple sclerosis 100% Amyotrophic lateral sclerosis (ALS) 100% Parkinson’s disease 100% Alzheimer’s disease 100% Infectious disease 100% Cancer 100%
Skin cancer 10% Carcinoma in situ 25% *Cardiac arrest is not a heart attack
How many times can a benefit be received?
The Maximum Critical Illness Benefit is limited to one covered illness or disease within each module. Your plan also includes the: Restoration Benefit* pays a one-time additional benefit if you experience a second covered illness for a different
condition. Recurrence Benefit* pays a benefit for the second occurrence of the same covered condition. The benefit amount for
the second occurrence is the same as for the first. ‒ In order for the second covered illness or the second occurrence of the illness to be covered, it must occur after 6
consecutive months without the occurrence of any covered illness named in your certificate, including the illness from the first benefit payment.
*This benefit does not apply to the cancer module.
If a partial benefit is paid out, it will not reduce the available maximum benefit amount for the illnesses or diseases in that same module. If you have reached the benefit limit by receiving the maximum benefit in each module, you may choose to end your coverage; however, if you have coverage for your spouse and/or children, you must continue your coverage in order to keep their coverage active. Please see the certificate of coverage for details.
What else is included?
The Critical Illness Insurance available through your employer includes the following additional benefits:
Exclusions and limitations
Benefits are not payable for any Critical Illness caused in whole or directly by any of the following*: Participation or attempt to participate in a felony or illegal activity. Suicide, attempted suicide or any intentionally self-inflicted injury, while sane or insane. War or any act of war, whether declared or undeclared, other than acts of terrorism. Loss that occurs while on full-time active duty as a member of the armed forces of any nation. We will refund, upon
written notice of such service, any premium which has been accepted for any period not covered as a result of this exclusion
Alcoholism, drug abuse, or misuse of alcohol or taking of drugs, other than under the direction of a doctor. *See the certificate of insurance and any riders for a complete list of available benefits, along with applicable provisions, exclusions and limitations.
This is a summary of benefits only. A complete description of benefits, limitations, exclusions and termination of coverage will be provided in the certificate of insurance and riders. All
coverage is subject to the terms and conditions of the group policy. If there is any discrepancy between this document and the group policy documents, the policy documents will govern.
To keep coverage in force, premiums are payable up to the date of coverage termination. Critical Illness Insurance is underwritten by ReliaStar Life Insurance Company (Minneapolis,
MN), a member of the Voya® family of companies. Policy form #RL-CI3-POL-12; Certificate form #RL-CI3-CERT-12; Spouse Critical Illness Rider form #RL-CI3-SPR-12; Children's
Critical Illness Rider form #RL-CI3-CHR-12; Wellness Benefit Rider form #RL-CI3-WELL-12; Recurrence Rider Form #RL- CI3-REC-12. Restoration of Benefits Rider form #RL-CI3-
REST-12. Form numbers, provisions and availability may vary by state and employer’s plan.
1293341
CI/SD 1 Only
Acct #0001 Date Prepared: 07/09/2021
212569-09012020
Receive $50
to use
however
you’d like
Wellness Benefit Complete an eligible health screening test, and we’ll send you a benefit
payment to use however you’d like. Employees receive an annual benefit payment of $50. Spouses receive an annual benefit payment of $50. Children receive 50% of your benefit amount per child, with an annual
maximum of $100 for all children.
Ready to Enroll?
Enrollment instructions will be provided by your employer. If you have additional questions before you enroll, please call: Voya Employee Benefits Customer Service at (877) 236-7564 For general questions or enrollment assistance, please contact a Benefit Communication Specialist (BCS)
at (877) 368-5789 https://presents.voya.com/EBRC/McLarenHealth

ReliaStar Life Insurance Company a member of the Voya® family of companies
Hospital Indemnity Insurance Explore Your Benefits & Costs
Out-of-pocket costs from a stay in a hospital or other medical facility can be
overwhelming. As expenses add up, Hospital Indemnity Insurance can help. This document includes expanded cost and benefit information for Hospital Indemnity Insurance. As you explore, keep in mind:
Hospital Indemnity Insurance doesn’t replace your medical coverage; instead, it complements it. The benefit
payments don’t go out to pay for medical bills or treatments you may need, instead they come in—
directly to you—to be used however you’d like. Choose this supplemental health insurance product for added protection if one of the following covered conditions comes your way.
Hospital Indemnity Insurance is a limited benefit policy. It is not health insurance, and does not satisfy the requirement of minimum essential coverage under the Affordable Care Act.
No medical questions or tests are required for coverage.
Simplified claims process has limited paperwork and can be
submitted/tracked online.
Benefit payments go directly to you. Use them however
you’d like!
Group Name: McLaren Health Care Corporation Group Number: 696030 Class: Employees working 20+ hours per week
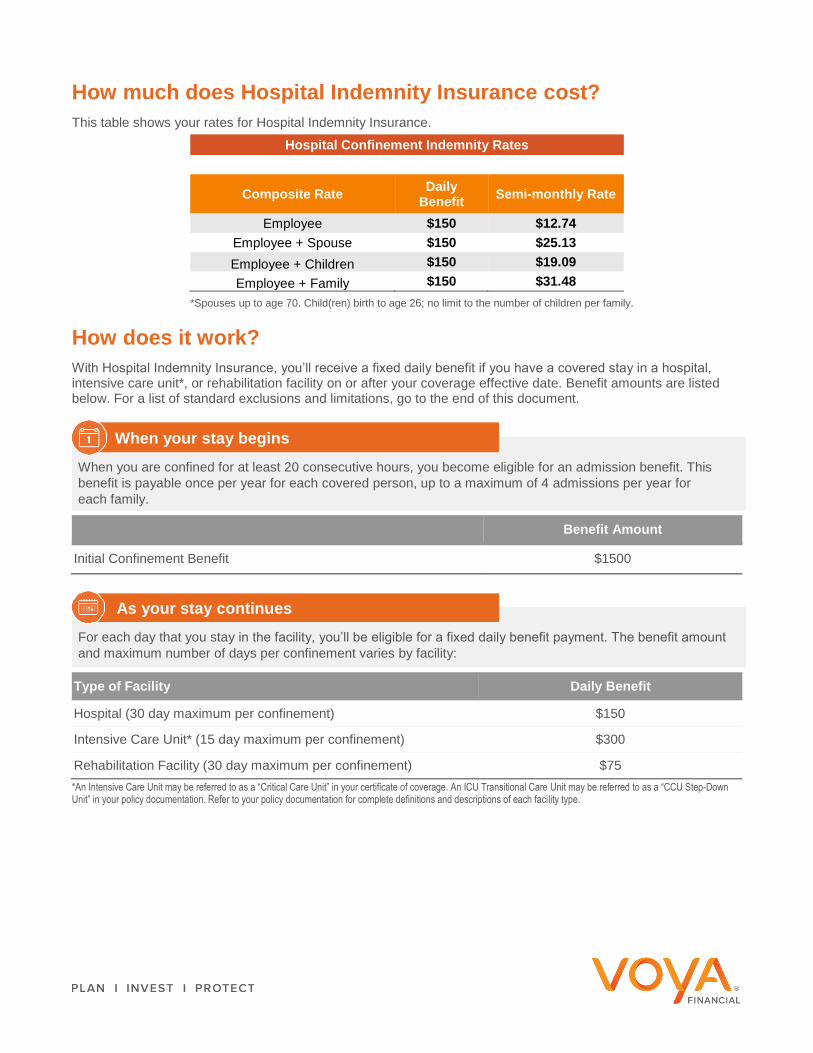
How much does Hospital Indemnity Insurance cost?
This table shows your rates for Hospital Indemnity Insurance. Hospital Confinement Indemnity Rates
Composite Rate Daily
Benefit Semi-monthly Rate
Employee $150 $12.74
Employee + Spouse $150 $25.13
Employee + Children $150 $19.09
Employee + Family $150 $31.48
*Spouses up to age 70. Child(ren) birth to age 26; no limit to the number of children per family.
How does it work?
With Hospital Indemnity Insurance, you’ll receive a fixed daily benefit if you have a covered stay in a hospital, intensive care unit*, or rehabilitation facility on or after your coverage effective date. Benefit amounts are listed below. For a list of standard exclusions and limitations, go to the end of this document.
Benefit Amount
Initial Confinement Benefit $1500
Type of Facility Daily Benefit
Hospital (30 day maximum per confinement) $150
Intensive Care Unit* (15 day maximum per confinement) $300
Rehabilitation Facility (30 day maximum per confinement) $75 *An Intensive Care Unit may be referred to as a “Critical Care Unit” in your certificate of coverage. An ICU Transitional Care Unit may be referred to as a “CCU Step-Down Unit” in your policy documentation. Refer to your policy documentation for complete definitions and descriptions of each facility type.
When you are confined for at least 20 consecutive hours, you become eligible for an admission benefit. This benefit is payable once per year for each covered person, up to a maximum of 4 admissions per year for each family.
When your stay begins
For each day that you stay in the facility, you’ll be eligible for a fixed daily benefit payment. The benefit amount
and maximum number of days per confinement varies by facility:
As your stay continues
Exclusions and limitations
The standard exclusions are listed below. (These may vary by state and/or your employer’s plan.)
Hospital Indemnity and Initial Confinement is not payable for any loss caused in whole or directly by any of the following*: Participation or attempt to participate in a felony or illegal activity. Operation of a motorized vehicle while intoxicated. Suicide, attempted suicide or any intentionally self-inflicted injury, while sane or insane. War or any act of war, whether declared or undeclared, other than acts of terrorism. Loss that occurs while on full-time active duty as a member of the armed forces of any nation. We will refund,
upon written notice of such service, any premium which has been accepted for any period not covered as a result of this exclusion.
Alcoholism, drug abuse, or misuse of alcohol or taking of drugs, other than under the direction of a doctor. Elective surgery, except when required for appropriate care as a result of the covered person’s injury or
sickness. Riding in or driving any motor-driven vehicle in a race, stunt show or speed test. Operating, or training to operate, or service as a crew member of, or jumping, parachuting or falling from, any
aircraft or hot air balloon, including those which are not motor-driven. Flying as a fare-paying passenger is not excluded.
Engaging in hang-gliding, bungee jumping, parachuting, sail gliding, parasailing, parakiting, kite surfing or any similar activities.
Practicing for, or participating in, any semiprofessional or professional competitive athletic contests for which any type of compensation or remuneration is received.
This is a summary of benefits only. A complete description of benefits, limitations, exclusions and termination of coverage will be provided in the certificate of insurance and
riders. All coverage is subject to the terms and conditions of the group policy. If there is any discrepancy between this document and the group policy documents, the policy
documents will govern. To keep coverage in force, premiums are payable up to the date of coverage termination. Hospital Confinement Indemnity Insurance is underwritten
by ReliaStar Life Insurance Company (Minneapolis, MN), a member of the Voya® family of companies. Policy form #RL-HI-POL-12; Certificate form #RL-HI-CERT-12;
Spouse Hospital Confinement Indemnity Rider form #RL-HI-SPR-12; Children’s Hospital Confinement Indemnity Rider form# RL-HI-CHR-12; Initial Confinement Benefit Rider
form #RL-HI-ICN-12; Diagnostic Test Benefit Rider form #RL-HI-DGR-12; Wellness Benefit Rider form #RL-HI-WELL-12; Accident Benefit Rider form #RL-HI-ACD-12; and
Critical Illness Benefit Rider form #RL-HI-CIR-12. Form numbers, provisions and availability may vary by state and by your employer’s plan.
1293347
HI1 Only
Acct #0001 Date Prepared: 07/09/2021
212571-091520
Ready to Enroll?
Enrollment instructions will be provided by your employer. If you have additional questions before you enroll, please call: Voya Employee Benefits Customer Service at (877) 236-7564
For general questions or enrollment assistance, please contact a Benefit Communication Specialist (BCS)
at (877) 368-5789
https://presents.voya.com/EBRC/McLarenHealth

FOR EMPLOYEES
Whole Life Insurance
Benefits Guarantees
Affordable Flexible Worldwide coverage Portable
Premium – As long as you continuously pay yourpremiums, the cost of your life insurance policy cannever go up.
Cash Value – The cash value illustrated at the time ofpurchase are guaranteed as long as your coverage staysin force*.
Interest Rate – This policy provides a 3% guaranteedcredited interest rate on accruing cash values.
Portability – Even if your employer changes, you canarrange to pay us directly and keep your coverage.
Coverage Issued – Employees and their spouses who are actively at work for a minimum of 20 hours per weekcan purchase this insurance up to certain limits, despitepast or present health problems.
Additional Purchase – If you buy a minimum amountof coverage, you guarantee yourself the right to purchaseany remaining portion of the guaranteed issue limit atfuture approved enrollments (subject to product andpayroll deduction availability).
Available for you, your spouse, children, andgrandchildren.
Guaranteed coverage with no medical questions,up to certain amounts.
You select the amount of insurance you need andhow much you can afford.
Payroll deduction makes payment easy.
Your payment amount will stay the same, even ifyou change employment or retire.
Builds cash value.
Annual statements provide current policy valueinformation.
Paid up options, based on accrued cash values.
$HIGHLIGHTS
see other side
Boston Mutual Life Insurance Company | WHOLE LIFE INSURANCE
* The actual cash value may be decreased by loans or withdrawals.
Our Whole Life workplace insurance is an endowment at age95 policy, which means the face value would be paid to theinsured, if living, at age 95.
Policy Series ICC18 END-95 (ESO)(6/18) 335-4611 9/19
Employers want to provide employees with a benefits package that fitstheir ever-changing needs. With its guaranteed premiums, benefits, andvalues, as well as the option to insure your entire family, Boston Mutual’swhole life insurance can help complete your benefit package.
Life changes…so it may be time to review how much coverage you have andconsider what your family might need if something should happen. Whetheryou’re just starting out at your first job, or nearing retirement, whole life insuranceshould be an integral part of your financial plan.
Just like Boston Mutual has always been there for our policyholders, whole life coveragewill always be there to provide you and your family protection and security for the future.
WL

Policies underwritten by Boston Mutual Life Insurance Company. This information is not intended to be a complete description of the insurance coverage available. For complete details of coverage and availability, please refer to the policy form or contact your Boston Mutual representative.
Accidental Death Benefit – doubles or triples the amount paid in the event of accidental death. This benefit pays an additional amount equal to the basic coverage to the beneficiary if the insured is killed accidentally. If accidental death occurs while the insured is a passenger on a bus, plane, train or any other common carrier, this benefit pays the accidental death benefit as above but will also pay an additional benefit of the basic coverage (up to $100,000).
Children’s Insurance Benefit – covers all eligible natural children, stepchildren, or legally adopted children fromage 15 days through age 25.
Payor Waiver of Premium – pays premiums on the employee, spouse, or dependent’s policy or policies in the event the payor (employee) becomes totally disabled before age 60.
Additional features that may be available to you
120 Royall Street, Canton, MA 02021 | 800.669.2668 | www.bostonmutual.com
Not all riders will be available for purchase as they are options made available to you by your employer in their benefits offering. Riders are not approved in all states.
For specific information – speak to your Boston Mutual representative.
Boston Mutual Life Insurance Company | WHOLE LIFE INSURANCE
Policy Series ICC18 END-95 (ESO)(6/18) 335-4611 9/19
My interests today areName Face Amount Premium Face Amount Premium Face Amount Premium
Pay Frequency: q Weekly q Bi-Weekly q Monthlyq Semi-Monthly





























