Embed Size (px)
DESCRIPTION
22 Accidental Periapical Extrusion of Non-setting Calcium Hydroxide Unusual Bone Response and Management
Citation preview

Journal of Indian Society of Pedodontics and Preventive Dentistry | Jan-Mar 2014 | Vol 32| Issue 1 |63
AbStrActPremixed non-setting calcium hydroxide is frequently used as interim root canal dressing in endodontically involved permanent teeth and as obturating paste in deciduous teeth in pediatric dentistry. Wide apex in both cases makes it more prone for deliberate extrusion especially when applied with pressure delivery systems. Contrary to common belief the mix was not resorbed in two years with the complaint of insufficiency in mastication. Large mass of calcium hydroxide in bone delayed healing process even after its removal. The present case report intends to demonstrate unusual behavior of bone in response to oily non-setting preparation of calcium hydroxide. Therefore its application with pressure syringe should be reconsidered in pediatric dentistry.
KEYWOrDS: Endodontic surgery, non-setting cal-cium hydroxide, periapical extrusion, resorption
Accidental periapical extrusion of non-setting calcium hydroxide: Unusual bone response and management
Divya S Sharma, Shikhar Pratap Singh Chauhan1, Vinaya Kumar Kulkarni, Chitra Bhusari, Rina VermaDepartments of Pedodontics and Preventive Dentistry, Modern Dental College and Research Centre, Gandhi Nagar, Indore, 1Pedodontics and Preventive Dentistry, Hitkarini Dental College, Jabalpur, Madhya Pradesh, India
IntroductionPremixed non-setting calcium hydroxide with iodoform in oil vehicle (NSCI) being easily insertable in canal with plastic applicator tips and having excellent antimicrobial efficiency is a choice of material for interim root canal dressings in permanent teeth and for obturation in primary teeth.[1,2] Abscessed permanent teeth as a sequel of caries or trauma often present with wide root apex in pediatric patient. Accidental extrusion of NSCI is a common phenomenon in deciduous as well as in permanent dentition.[2-8] Some authors speculate that it favor periapical healing and encourage osseous repair.[2,9]
Many case reports are claiming that NSCI is a resorbable material if extruded in periapical area.[2,3,5] Successful healing at periapex has been reported with NSCI used as dressing in tooth.[2,3,5] Nonetheless it may be a frustrating situation when extruded in large quantity through wide apex of an immature permanent
tooth. There are reports that not only it delays primary healing,[10] but also not fully resorbed for long periods of follow-up.[3,4]
The present case reports an unusual behavior of NSCI extruded accidentally into periapex of young permanent first molar. In spite of several claims reported NSCI being resorbable[2,3,5] its resorption was not observed even after 2 years of follow-up and showed very slow healing of lesion after surgical removal of extruded mass till 3 years. This case also attempts to report the behavior of bone in response to NSCI.
Case ReportA patient of 13 year age, reported to the Department of Pedodontics and Preventive dentistry, Modern Dental College and Research Center with the chief complaint of etching in lower right buccal vestibule and emptiness while eating with the recently treated lower posterior tooth. History revealed that patient had gone for root canal treatment in same tooth 2 days ago. Papers showed that patient had intraoral sinus with 16 when first reported to previous dentist. On intraoral examination no adverse finding was
Address for correspondence: Dr. Divya S Sharma, Department of Pedodontics and Preventive Dentistry, Modern Dental College and Research Centre, Gandhi Nagar, Airport Road, Indore - 453 112, Madhya Pradesh, India. E-mail: [email protected]
Case Report
Access this article onlineQuick response code Website:
www.jisppd.com
DOI: 10.4103/0970-4388.127061
PMID: ******

Sharma, et al.: Periapical extrusion of calcium hydroxide
Journal of Indian Society of Pedodontics and Preventive Dentistry | Jan-Mar 2014 | Vol 32| Issue 1 | 64
observed [Figure 1a]. Periapical X-ray showed large radiopaque material in periapical space in relation to mesial root [Figure 2a]. Root canal obturation was found satisfactory. Though patient had no pain, but the complaint of gingival irritation and tooth not taking load while chewing. Conversation with old dentist revealed that he had used NSCI as interim dressing. Probably the same amount of mass was lying buccolingually too that had filled up the sinus tract and was in contact with gingival tissue giving rise to etching sensation. As NSCI is said to be resorbable material, we advised patient to wait for some period. Etching sensation got subsided within a week.
Patient was regularly followed up till next 2 years. But no signs of resorption of NSCI were found. During this period of observation patient left the habit of chewing from right side. He could not get over with the feeling of emptiness on chewing from right side. His parents were worried for this large radiopaque mass in the bone even after 2 years. Considering the patient’s complaint and parent’s worry we decided to surgically remove NSCI from periapex.
After getting parental consent surgery was started under antibiotic coverage after 2 years of primary obturation. After raising the full thickness flap, a clear white spot covered with thin periosteum was seen [Figure 1b]. This confirmed our tentative imagination that NSCI had filled the sinus tract. The
area was entered from this site. The claimed non-setting material was very dry, hard, and light yellow in color. It was excavated in flakes [Figure 1c]. Bone cavity walls were smooth [Figure 1d]. Instead of frank bleeding, blood was oozing from cavity walls. Mesial root was apicoectomized and apical seal was found adequate. Gutta-percha was burnished further [Figure 1e]. Bleeding was induced by rubbing the cavity wall with curette followed by suturing the lesion [Figure 1f]. Immediate postoperative radiograph was taken [Figure 2b]. Patient was advised for permanent custom made crown for 16. But patient was satisfied with stainless steel (SS) crown.
One year follow-up showed very slow healing, perhaps because of the size of lesion [Figure 2c-e]. As lesion was healing, longer follow-up were scheduled. Twenty-eight months later patient was recalled telephonically. Radiograph this time revealed periapical radiolucency with distal root [Figure 2f]. Patient did not complain of any adverse symptom and was chewing on tooth without any pain. Perhaps radiolucency was due to overload on distal root for extended period of time. We removed SS crown to relieve the occlusion. As trauma
a
c
e
b
a
c
e
b
d
f
d
f
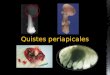
Figure 1: Photographs during surgery (a) Preoperative (b) After raising flap, white color of extruded mas was visible through overlying thin bone (c) Extruded mass was dry and removed in flakes (d) Apex of mesial root visible in mirror with burnished obturation (e) Cleaned cavity with induced bleeding (f) Lesion closed with interrupted mattress sutures
Figure 2: Postsurgical radiographic evaluation for the period of 39 months (a) Preoperative, extruded mass of non-setting calcium hydroxide remained in bone for 2 years (b) Just after surgery, periextrusion thin radiopaque line is visible (c) After 2 months of surgery, healing of bone can be appreciated (d) After 8 months of surgery, slow healing of lesion (e) After 11 months of surgery, still lesion not healed completely (f) After 39 months of surgery, developing periapical radiolucency, perhaps due to extended overload on distal root

Sharma, et al.: Periapical extrusion of calcium hydroxide
Journal of Indian Society of Pedodontics and Preventive Dentistry | Jan-Mar 2014 | Vol 32| Issue 1 |65
giving rise to severe inflammatory response, but was the most resorbed material. Maisto paste and Sealer 26 + iodoform was the most biologically compatible paste owing to less inflammation of tissues, but their resorption was poor, probably owing to the presence of iodoform which counterbalance the severe alkalinity in tissues created by calcium hydroxide. Bramante and Berbert[12] evaluated the bone response with aqueous mix of calcium hydroxide and iodoform in root perforation area. Groups were divided according to days of dressing change in perforation area. In histologic evaluation after 90 days both reparative and inflammatory reaction of small magnitude and perforation sealing by mineralized tissues was found in a group where dressing was not changed at all. In this study no previous pathological inflammation existed at the time of perforation and whole procedure was performed under sterilized condition, thus minimizing the inflammation. Hard tissue formation around paste was observed, but no resorption of paste was found. Findings of these studies are in support of our hypothesis described in beginning of discussion.
Huang et al.,[13] compared the effects of different materials used in primary root canal fillings on the cell viability of human osteosarcoma cell lines and concluded that the calcium hydroxide with iodoform and Vitapex as better options as higher survival of cell lines were found. Nishimura et al.,[14] examined the ability of five root canal antiseptics to induce chromosome aberrations in human dental pulp cells. Calcium hydroxide + iodoform combination paste did not induce any chromosomal aberration in absence or presence of exogenous metabolic activation. All these studies demonstrate good biocompatibility of calcium hydroxide + iodoform pastes, though initial inflammation is there which subsides in due course of time. Our case supports this biocompatibility.
Contrary to these findings many case reports are there
from occlusion was suspected for the new asymptomatic radiolucency, an enzymatic NonSteroidal Anti-Inflammatory Drug (NSAID), that is, serratiopeptidase (10 mg) one tablet TID for 1 week was prescribed. In order to hasten the slowly healing bone defect at mesial root, an ayurvedic immunomodulator, that is, Septilin (Himalaya Herbal Healthcare) two tablets BID for 15 days was prescribed. Both medications were given as supportive therapy only. Patient was asked to come after 15 days, but he failed to do so.
On repeated phone reminders he came to the department after 46 months of surgery and 7 months after last visit. He had discontinued the medications after 15 days. The treated tooth was functioning normally. Extra- or intraorally soft tissues were healthy [Figures 3a and b]. IntraOral PeriApical (IOPA) X-ray revealed bone trabeculae developing in both the radiolucencies [Figure 3c]. Patient was again advised to take Septilin for 15 days more and the tooth was restored with full extracoronal restoration [Figure 4].
DiscussionThe case report might give rise to the discussion that whether some inflammation (periapical pathology) or resorptive process (deciduous root resorption) is required for resorption of NSCI from bony tissues. Murata et al.,[11] analyzed the periapical tissue reaction with three root canal filling materials, that is, Maisto paste (zinc oxide, iodoform, camphorated chlorophenol, and lanolin); Sealer 26 + iodoform (calcium hydroxide, urotropin, bismuth trioxide, titanium dioxide, and epoxy resin mixed with iodoform in equal parts); and L&C paste (calcium hydroxide, olive oil, bismuth carbonate, and rosin) on dog’s anterior deciduous teeth. They found L&C paste the most irritating one
Figure 4: Tooth restored with full coverage porcelain fused to metal crown
Figure 3: Forty-six months postoperative photographs and radiograph (a and b) Normal looking buccal and lingual mucosa (c) Bony trabeculae could be seen in mesial and distal radiolucencies
a b
c

Sharma, et al.: Periapical extrusion of calcium hydroxide
Journal of Indian Society of Pedodontics and Preventive Dentistry | Jan-Mar 2014 | Vol 32| Issue 1 | 66
indicating negative aspect of calcium hydroxide.[3,7,8,15] Necrosed buccal alveolar mucosa and some discharge of material from site was found where non-setting calcium hydroxide (mixed with propylene glycol) was accidentally extruded through external resorptive area in maxillary right lateral incisor under buccal bone.[15] In our case also NSCI was found extruded through sinus under the buccal bone but contrary to above findings,[15] sinus tract healed except from initial etching symptoms. Oily preparation of calcium hydroxide has different physical property than other types, making mixed ingredients remain binded within mass. As no free calcium hydroxide particles were there to occlude blood vessel, our case remained safe with no ischemia of surrounding tissues as in other case reports.[7,8,15] Our case report also confirms the findings of Huang et al.,[13] and Nishimura et al.,[14] that calcium hydroxide + iodoform in silicon oil vehicle is the biocompatible material as compared to freshly mixed calcium hydroxide in aqueous or viscous vehicle. This may be because of high initial alkalinity with aqueous or viscous vehicle. Oily preparations are non-water soluble that promote lowest solubility and diffusion of paste within tissue.[16] Same biocompatibility has been reported when calcium hydroxide + barium sulfate mixed with distilled water was unintentionally extruded into periapical lesion that did not cause any adverse reaction but remained non-resorbed during 36 months period.[4] No sinus tract was there preoperatively in their case,[4] preventing direct contact of aqueous mix of calcium hydroxide with soft tissues.
De Moor and De Witte[3] reported that in cases of accidental extrusion calyx paste was completely resorbed, while Reogan Rapid did not.[3] They hypothesized that presence of barium sulfate in calcium hydroxide made it non-resorbable. Same was the findings by Orucoglu and Cobankara.4 Contrary to these reports, in our case even though barium sulfate was not there in the mix, it was not resorbed. Nonetheless similar to these reports, periradicular and periextrusion radiolucency disappeared.
De Moor and De Witte[3] observed white border surrounding the periapical lesion with a diminished amount of periradicular calcium hydroxide. Similarly we also have observed white border in periextrusion bone [Figure 2a and b]. After surgically exposing the lesion, burnished bone cavity wall was observed which was appearing as white line in radiograph. Similar to our case they also found slow healing of periapical lesion even after resorption of calcium hydroxide.
Extrusion of NSCI might have maintained initial pH because of the presence of exudates there.[16] After drop of pH it induced tissue mineralization around it. Perhaps after alkalinity drop and inflammation resolution, mass became inert with no chemical
signaling to bring macrophages[2] to resorb the material. Large quantity of extruded calcium hydroxide, be it in any vehicle,[3,4] is not found resorbed perhaps because of resolution of inflammation after some time.
While doing surgery, thin line of periosteum was observed over extruded mass, proving the tissue mineralization induction property after pH drop. The NSCI was found hard while excavation, perhaps because of exhaustion and resorption of remaining oil in the span of 2 years. In spite of removal of foreign material bone healing was very slow. We could not find any case report about management of bone cavity created in response to NSCI, therefore just after inducing bleeding by rubbing we closed the lesion as is routinely done while enucleating cysts. Perhaps roughening the burnished cavity walls with/without bone graft would have boosted up the healing rate. Appearance of radiolucency with distal root might be because of constant low grade overload on distal root in presence of slowly healing periradicular lesion with mesial root.
Periapical radiolucencies were healing after 7 months of his last visit. The effect of supportive therapy is unclear as healing may be because of occlusion relief.
ConclusionThe presented case report emphasizes the possible complications with premixed calcium hydroxide dressings applied with pressure insertion systems (lentulo spiral or applicator tips) in root canals should be reconsidered especially in pediatric dentistry.
References1. Estrelac,Estrelacr,HollandaAc,DecurcioDdeA,Pecora
JD. Influence of iodoform on antimicrobial potential ofcalciumhydroxide.JApplOralSci2006;14:33-7.
2. Nurko c, ranly DM, Garcia-Godoy F, Lakshmyya KN.resorptionofacalciumhydroxide/iodoformpaste (Vitapex)inrootcanaltherapyforprimaryteeth:Acasereport.PediatrDent2000;22:517-20.
3. DeMoor rJ, DeWitteAM. Periapical lesions accidentallyfilledwithcalciumhydroxide.IntEndodJ2002;35:946-58.
4. Orucoglu H, cobankara FK. Effect of unintentionallyextruded calcium hydroxide paste including barium sulfateasaradiopaquingagentintreatmentofteethwithperiapicallesions:reportofacase.JEndod2008;34:888-91.
5. KapoorV,PaulS.Non-surgicalendodonticsinretreatmentofperiapicallesions-tworepresentativecasereports.JclinExpDent2012;4:e189-93.
6. SoomroF,AbidiSY,QureshiS,Hoseint.Effectofaccidentalperiapical extrusion of calcium hydroxide paste (A casereport).JPDA2010;19:57-60.
7. Sharma S, Hackett r,Webb r, Macpherson D,WilsonA.Severe tissue necrosis following intra-arterial injection ofendodonticcalciumhydroxide:Acaseseries.OralSurgOralMedOralPatholOralradiolEndod2008;105:666-9.

Sharma, et al.: Periapical extrusion of calcium hydroxide
Journal of Indian Society of Pedodontics and Preventive Dentistry | Jan-Mar 2014 | Vol 32| Issue 1 |67
8. ShahravanA,JalaliS,Mozaffarib,PourdamghanN.Overextensionofnonsettingcalciumhydroxideinendodontictreatment:Literaturereviewandcasereport.IranEndodJ2012;7:102-8.
9. tronstadL,AndreasenJO,HasselgrenG,KristersonL,riisI.pHchangesindentaltissueaftercalciumhydroxideasashorttermintracanaldressing.IntEndodJ1981;7:17-21.
10. VernieksAA,MesserLb.calciumhydroxideinducedhealingofperiapicallesions:Astudyof78non-vitalteeth. JbrEndodSoc1978;11:61-9.
11. MurataSS,Hollandr,SouzaVd,DezanJuniorE,GrossiJA,Percinoto c. Histological analysis of the periapical tissuesofdogdeciduous teeth after root canalfillingwithdifferentmaterials.JApplOralSci2005;13:318-24.
12. bramante cM, berbert A. Influence of time of calciumhydroxideiodoformpastereplacementinthetreatmentofrootperforation.brazDentJ1994;5:45-51.
13. Huang tH, Ding SJ, Kao ct. biocompability of variousformula root filling materials for primary teeth. J biomedMaterresbApplbiomater2007;80:486-90.
How to cite this article: Sharma DS, Chauhan SS, Kulkarni VK, Bhusari C, Verma R. Accidental periapical extrusion of non-setting calcium hydroxide: Unusual bone response and management. J Indian Soc Pedod Prev Dent 2014;32:63-7.Source of Support: Nil, Conflict of Interest: None declared.
14. NishimuraH,HigoY,OhnoM,tsutsuitW,tsutsuit.Abilityof root canal antiseptics used in dental practice to inducechromosome aberrations in human dental pulp cells. Mutatres2008;649:45-53.
15. bramante cM, Luna-cruz SM, Sipert cr, bernadineli N,Garcia rb, deMoraes IG, et al.Alveolar mucosa necrosisinduced by utilisation of calcium hydroxide as root canaldressing.IntDentJ2008;58:81-5.
16. ViannaME,ZilioDM,Ferrazcc,ZaiaAA,deSouza-FilhoFJ,GomesbP.concentrationofhydrogenionsinseveralcalciumhydroxide pastes over different periods of time. braz DentJ2009;20:382-8.

Reproduced with permission of the copyright owner. Further reproduction prohibited withoutpermission.