Embed Size (px)
Citation preview
Periapical periodonitis
Pulpitis, trauma or endodontic treatment
Pulpitis and pulp necrosis:If pulpitis is untreated, bacteria ,bacterial
toxins , or the products of inflammation will extend down to the root canal and through the apical foramina to cause periodontitis with time.
Aetiology
Traumatic periodonitis is often acute and transitory occlusal trauma.
High restoration. Undue pressure during orthodentic
treatment. Direct blow on a tooth.
Trauma
Mechanical instrumentation.
Chemical irritation.
Endodontic treatment
This is characterized by an acute inflammatory exudates in the periodontal ligament within the confined space between the root apex and the alveolar bone.
Acute periapical periodonitis
Pain when the external pressure is applied to the tooth.
Well located by the patient.
No pain in hot or cold stimulation. No –or little- radiographic changes ,or slight
widening of the periodontal ligament
Clinically
Persistent irritation leads to chronic periapical periodontitis , which characterized by:
Resorption of the periapical alveolar bone. Replaced by chronically inflamed
granulation tissue to form periapical granuloma.
Chronic periapical periodontitis
Histologically:
The lesion consists mainly of granulation tissue infiltrated by lymphocytes , plasma cells and, macrophages and T-lymphocyte.
Cont.
Clinically:
Periapical granulomas tend to be asymptomatic, but may be associated with occasional tenderness.
Percussion may produce a dull note.
Radiological examination at first shows a widening of the periodontal ligament space around the apex.
In some instances this radiolucency is well circumscribed and clearly demarcated from the surrounding bone by a corricated margin , while in others the border is poorly defined.
Clinically cont.
Acute periapical abscess and spreading of the inflammation.
An acute periapical abscess may develop either directly from acute periapical periodontitis or more from chronic periapical granuloma.
Generally, it’s a result of mixed bacterial infection, culture of pus yielding a wide range of different species.
Aetiology
If the cause of the abscess is not removed for example by , extraction , ondodontic treatment or antibiotic therapy , suppuration will continue and the abscess continue to enlarge , with progressive suppuration causes the pus to track in one of number of direction.
Routes of spread
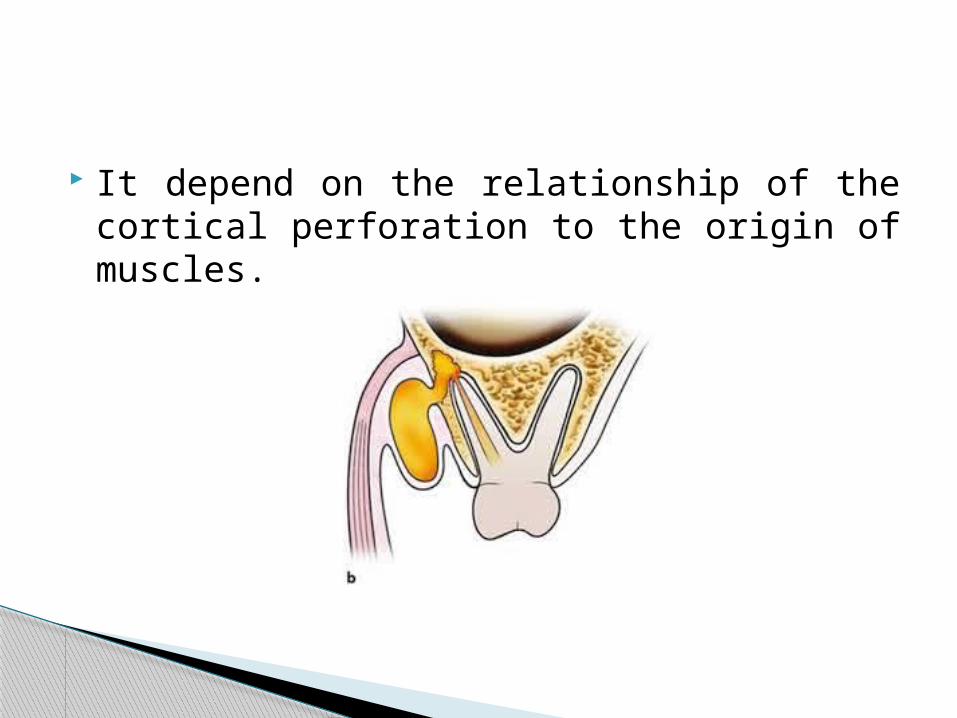
It depend on the relationship of the cortical perforation to the origin of muscles.
1. The puss may discharge directly into the oral cavity through a sinus following local penetration of the overlying periosteum and mucosa , this may occur with little or no pain and only a small swelling on the oral mucosa.
Possible outcomes
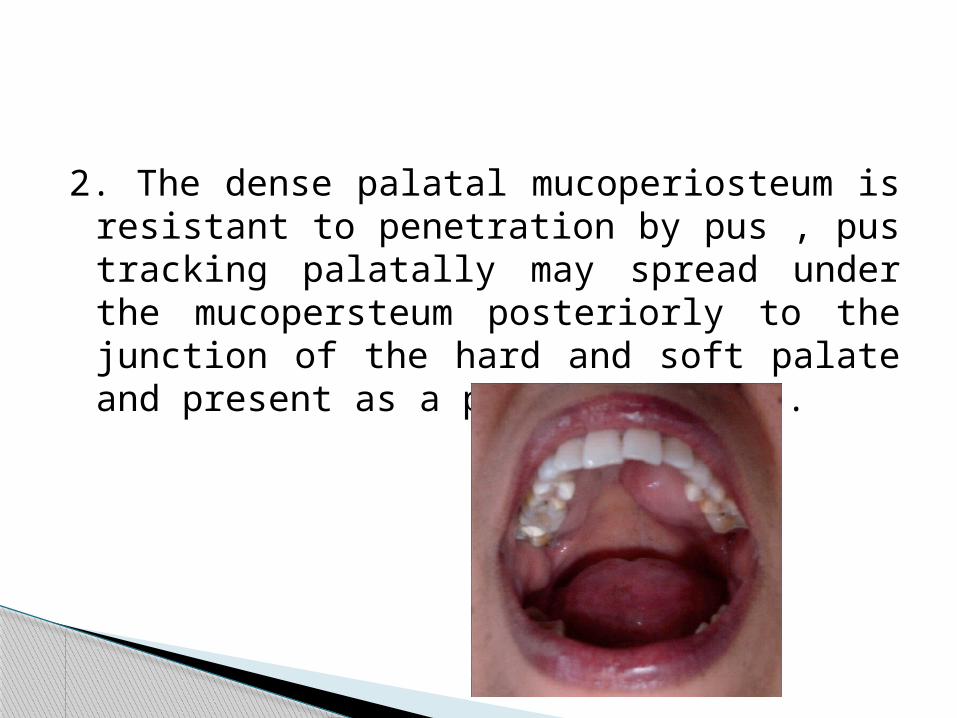
2. The dense palatal mucoperiosteum is resistant to penetration by pus , pus tracking palatally may spread under the mucopersteum posteriorly to the junction of the hard and soft palate and present as a palatal abscess.
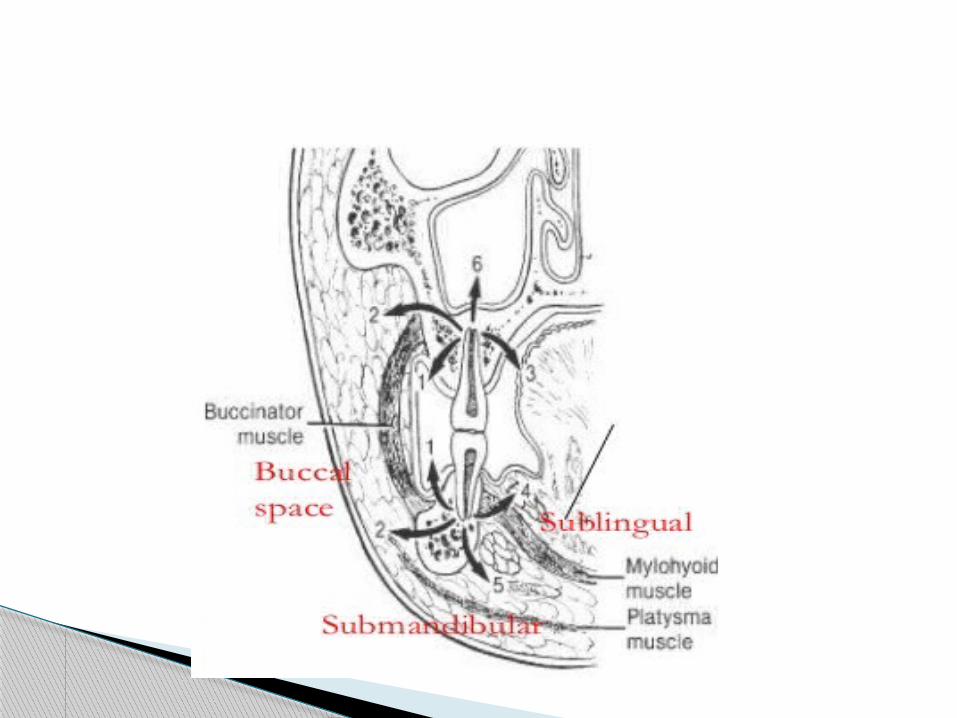
3. Abscess of molar region of either jaw may penetrate the buccal cortical plate above ( in the maxilla) or below (in the mandible) the attachment of buccinator muscle , in such cases acute inflammatory oedema and suppuration spread onto the soft tissues of the face or neck , this may present as a cellulitis , or less frequently as a localized soft tissue abscess.
4- abscesses related to anterior maxillary teeth may perforate the labial bone above the attachment of the levator anguli oris muscle, the infection may then pass medially and upwards towards inner canthus of the eye, obliterating the nasiolabial fold. Alternatively, the infection may pass into the upper lip.
5-abscesses developing at the root apices of maxillary molars and premolars are very close to the floor of the maxillary sinus and may discharge into the sinus.
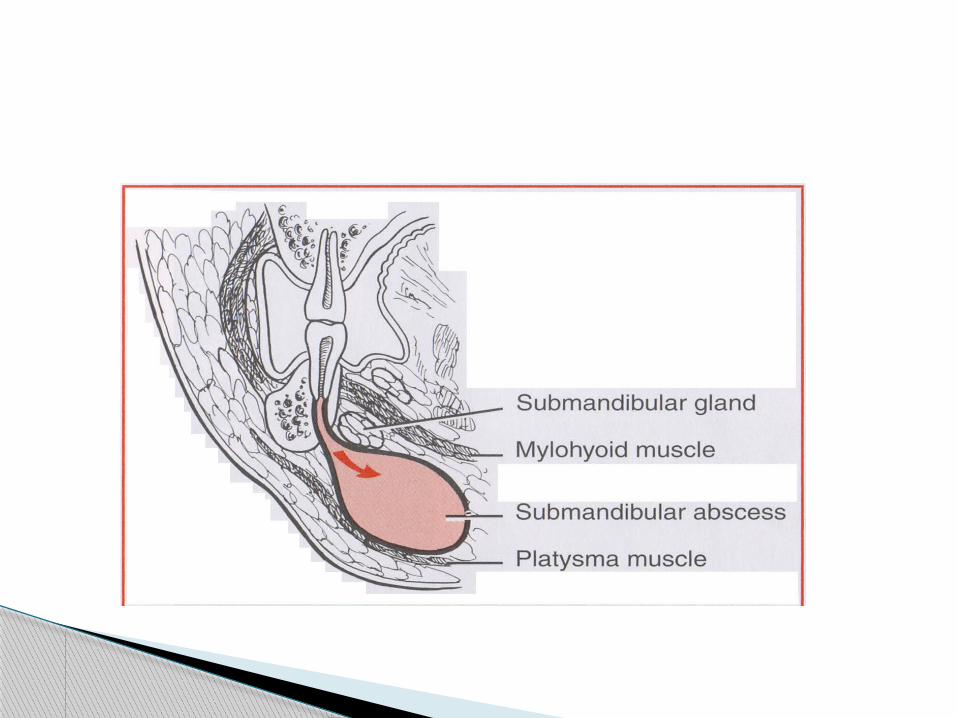
6-abscesses related to a mandibular molar and premolar tooth may perforate the lingual plate of the mandible below the attachment of the mylohyiod muscle to involve the submandibular space.
The submandibular space has communications with the sublingual and lateral pharyngeal spaces.
7-abcesses from madibular anterior and canine may track labially and perforate the bone below the insertion of the mentalis muscle and pass downword to present as a subcatenous abscess.
Cellulitis is a rapidly spreading inflammation of the soft tissues particularly associated with streptococcal infections.
Not well-localized.
cellulitis

Clinically:
There is diffuse, tense, painful swelling. Associated with malaise and an elevated
temperature Abscess formation occur later if treatment is
delayed.
Cellulitis associated with maxillary teeth initially invloves the upper half of the face.
Extension towards the eye is a potentially serious complication because of risk of cavernous sinus thrombosis as a result of infection invloving veins at the inner canthus of the eye which communicate with cavernous sinus.
Cellulitis associated with mandibular teeth initially involves the lower half of the face.
Extension into submandibular and cervical tissues may cause respiratory embarrassment.
Ladwig’s angina is severe cellulitis involving the submandibular, sublingual and submental spaces as a result of initial submandibular space.
The diffuse cellulitis produces a broad-like swelling of the floor of the mouth, the tongue being elevated and displaced posteriorly.
Ludwig’s angina
There is difficulty in eating, swallowing and breathing
Oedema of the glottis may occur with risk of death by suffocation