11.1. COURSE AIMS:
..............................................................................
4
2. ECHOCARDIOGRAM (DEMONSTRATION)
.................................... 5
3. AUSCULTATION OF HEART SOUNDS AND PHONOCARDIOGRAM
..........................................................................
7
3.1. INTRODUCTION
..............................................................................
7
3.2. AIMS
............................................................................................
8
Results and Interpretation
...................................................................................
8
4. ELECTROCARDIOGRAM (ECG)
..................................................... 9
4.1. INTRODUCTION
..............................................................................
9 Schematic account of the depolarization and repolarization of the
heart with the
correlating ECG
...................................................................................................
9
ECG electrode positions and ECG measurements
........................................... 10
What are the deflections (peaks and curves) seen on an ECG readout?
.......... 11
Determining the mean electric axis of the heart
................................................ 12
Conclusions
.......................................................................................................
13
Respiratory sinus arrhythmia
.............................................................................
14
5. GLOSSARY
....................................................................................
17
3
1. Introduction The heart is a dual pump made up of two
functionally sequential and anatomically
parallel pumps. An interruption of about 10 seconds in the
circulation of blood to
the brain can lead to loss of consciousness. A break of more than a
few minutes
can lead to irreversible brain damage. Hence it is of vital
importance that the heart
functions stably and continuously.
In this course you will have the opportunity to examine and carry
out important
noninvasive methods used to examine heart function and to assess
their rele-
vance.
How well a particular heart is functioning is first examined by
careful study of the
patients’ case history, physical inspection of the patient,
palpation, and ausculta-
tion. If abnormal heart sounds, heart murmurs, or arrhythmias are
detected during
auscultation, this may indicate a congenital or acquired functional
and/or morpho-
logical defect (i.e. defective valve or other heart
problems).
The ECG registers differences in electrical currents on the body’s
surface. These
differences generated by the depolarization and repolarization of
the heart spread
to surrounding tissues and to the body’s surface. The ECG provides
details about
heart rhythm and allows investigation of the spread of cardiac
excitation. ECGs
are also used to judge myocardial ischemias and heart
attacks.
Echocardiography (ultrasound for the heart) is used to examine the
mechanics of
the heart (valve movement, chamber volumes) with a high resolution
in space
and time. At the same time a Doppler can be employed to measure the
direction
and speed with which the blood is traveling through the
heart.
The more invasive ways in which the heart can be examined (i.e.
catheters) will
not be discussed in this course. However, catheters are used to
determine intra-
cardial pressure and blood flow, visualizing the coronary arteries,
and for intra-
cardial ECGs.
THE HEART-ECG
4
1.1. Course Aims: 1. General: Get to know noninvasive techniques
for examining heart function
2. General: Understanding and interpreting the heart cycle
(electrically as well
as mechanically) as a function of time
3. Echocardiogram (ultrasound of the heart) demonstration:
Introduction to
method and understanding of heart mechanics
4. Auscultation: Become familiar with 1st and 2nd heart sounds and
their ori-
gins. Understanding heart murmurs (pathology). In addition you
should be
able to correlate the heart sounds with the pulse.
5. ECG: carry out ECG (positioning of electrodes) and practice
recording and
interpreting a normal ECG.
2.1. Introduction The echocardiogram is an important noninvasive
method to investigate and diag-
nose the condition of the heart. It is an ultrasound of the heart.
The echocardio-
gram is based on the fact that ultrasound waves are partially
reflected by tissue
boundaries. The echo transducer, which sends and receives
ultrasound waves,
is covered with a special gel and held against the patient’s chest.
Now the ultra-
sound waves can be registered by the machine and projects an image
of the
heart on the monitor.
The dynamic sections visualized using this method allows for
investigations into
the heart’s anatomy and movement (pumping action). For example,
ventricle area
can be measured before and after ventricular contraction allowing
the ejection
fraction to be calculated. At the same time Doppler measurements
can be taken
in order to analyze the direction and speed of blood flowing within
the heart. Con-
sequently heart valves can be examined not only from a physical and
motional
perspective, but their hemodynamic function can also be evaluated.
Finally, pres-
sure gradients can be calculated based on the flow
characteristics.
2.2. Aims
• An echocardiogram demonstration by a qualified USZ
Cardiologist
• To understand the basics of what an echocardiogram is and how it
is useful
as a diagnostic tool
• Understanding the mechanics of the heart by visualizing the heart
cycle
THE HEART-ECG
Central Venous Pressure
3.1. Introduction Heart sounds (physical sounds) are strictly
defined vibrations (≤ 50 Hz) in the
heart. These vibrations can be transmitted to the thorax, and can
then be heard
or registered using a stethoscope or phonocardiogram. The first
heart sound (S1)
results from the closure of the atrioventricular valves, mitral and
tricuspid, at the
beginning of ventricular contraction, or systole. The second heart
sound (S2) is
caused by the closure of the aortic valve and pulmonary valve at
the end of ven-
tricular systole. As the left ventricle empties, its pressure falls
below the pressure
in the aorta, and the aortic valve closes. Similarly, as the
pressure in the right
ventricle falls below the pressure in the pulmonary artery, the
pulmonary valve
closes.
During inspiration, negative intrathoracic pressure causes
increased blood return
into the right side of the heart. The increased blood volume in the
right ventricle
causes the pulmonic valve to stay open longer during ventricular
systole. This
causes an increased delay in the P2 component of S2. During
expiration, the pos-
itive intrathoracic pressure causes decreased blood return to the
right side of the
heart. The reduced volume in the right ventricle allows the
pulmonic valve to close
earlier at the end of ventricular systole, causing P2 to occur
earlier, and "closer"
to A2. It is physiological to hear the splitting of the second
heart sound by younger
people and during inspiration. During expiration normally the
interval between the
two components shortens and the sound becomes merged. A third
(rapid filling
of the ventricle) and/or fourth heart sound (atrium contraction)
are usually only
audible in pathological cases.
Pathological heart murmurs (between sounds, at higher frequency)
are the result
of turbulences in blood flow. Systolic noise is usually only heard
in aortic or pul-
monary valve stenosis (restriction) or insufficiencies of the
atrioventricular valves.
Diastolic noise is audible in patients with stenosis of the
atrioventricular valves
and insufficiencies of the aortic or pulmonary valves. In the case
of anemia, the
decrease in blood viscosity (due to low hematocrit) and increase in
the cardiac
output leads to the development of turbulences.
8
3.2. Aims • Understanding the way in which normal and pathological
heart sounds de-
velop
• Being able to discern the difference between the first and second
heart
sound with auscultation (note position of subject and where
auscultation
is being performed)
3.3. Method Auscultation
Subjects should listen to each others’ auscultations using the
stethoscope in two
different positions. First the subject should be lying down, and
then he should be
sitting up (bent slightly forward towards the listener). Having the
subject bend
towards the listener should make the sounds more audible as the
heart is against
the inside of the thorax. In this position heart tones should be
very clear when the
stethoscope is placed in the 3rd intercostal space on the left
parasternal side.
In order to evaluate the longer and duller first heart tone, it may
be best to listen
for the mitral auscultation and the tricuspid auscultation. For
mitral auscultation
place the stethoscope at the 5th intercostal space medioclavicular
to a subject
lying on his left side to optimize audibility. For optimal
tricuspid auscultation place
the stethoscope in the 5th intercostal space on the right
parastenal side of the
subject. When the carotid artery is palpated simultaneously, the
chronological
correlation of the first heart sound and the pulse can be
determined.
The second heart sound is evaluated using the same criteria. The
components
of the aortic valve are easiest to hear in the 2nd intercostal
space parasternal right
while the pulmonary valve is easiest to hear in the 2nd intercostal
space left. Note
the split in the two components when the subject breathes
deeply.
Results and Interpretation
Each student should be able to hear the heart sounds using the
stethoscope. In
addition you should be able to correlate the heart sounds with the
pulse.
THE HEART-ECG
4. Electrocardiogram (ECG)
4.1. Introduction The ECG registers differences in potential on the
body’s surface which are
generated by the heart’s activity.
General Information on the generation of the measured
potentials:
The progressive stimulation (depolarization) of individual
myocardial cells leads
to a progression of electronegativity on their surfaces. This
causes an electric
dipole to develop between those cells or regions which are
stimulated (electro-
negative) and those which are not yet stimulated (electropositive).
These differ-
ences can be described or interpreted as vectors which move from
the stimulated
(negative) areas to the not yet stimulated (positive) areas. The
sum of all these
single vectors gives rise to a sum or integral vector throughout
heart stimulation.
A large portion of these vectors cancel each other out. During
repolarization the
surface electronegativity has to be reverted so that the next
dipole vector can
again move from the stimulated (negative) to the unstimulated
(positive) areas of
the heart. When this integral vector meets with a positive or
unipolar electrode it
leads to a positive deflection.
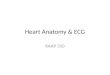
Schematic account of the depolarization and repolarization of the
heart with the correlating ECG
Electrode (-)
Electrode (+)
Progression of the dipolarization
ECG electrode positions and ECG measurements
V1 4 l.C.R. parasternal ri V2 4 l.C.R. parasternal le V3 Between V2
and V4 V4 5 l.C.R. medioclavicular V5 Height of V4, anterior
axillary line V6 Height of V4, left midaxillary line
THE HEART-ECG
11
What are the deflections (peaks and curves) seen on an ECG
readout?
P-wave: represents the wave of depolarization that spreads from the
SA node
throughout the atria, and is usually 0.08 to 0.1 seconds (80-100
ms) in duration.
The brief isoelectric (zero voltage) period after the P-wave
represents the time in
which the impulse is traveling within the AV node (where the
conduction velocity
is greatly retarded) and the bundle of His. Note that the
repolarization of the
atrium is not visible because it correlates chronologically with
the QRS complex.
P-Q (P-R interval): This interval represents the time between the
onset of atrial
depolarization and the onset of ventricular depolarization. Since
the mass of cells
which are depolarizing at this time point is small (AV node and His
bundles) the
P-R segment is isoelectric. If the P-R interval is >0.2 sec,
there is an AV conduc-
tion block, which is also termed a first-degree atrioventricular
block if every im-
pulse is still able to be conducted into the ventricles.
QRS Complex: This complex represents ventricular depolarization. By
definition
a negative peak is called Q when it precedes a positive peak (R). A
positive peak
following a positive peak is referred to as R’ and a negative peak
following a
positive peak is S. First the upper septum muscles are stimulated
from the left
side. This can lead to a small Q peak if we interpret it ‘from the
left perspective’
(I, II, AVL, V4-V6). The stimulation then proceeds down to the
cardiac apex and
beyond by moving along the chamber walls until it reaches the level
of the valves.
In order to understand the direction of the integral vector that
makes up the QRS
complex one must remember that chamber myocardial tissue is always
stimu-
lated from the inside out. Since, under normal circumstances the
integral vector
is mostly defined by the left ventricle (bigger muscle), the vector
usually points
downwards and/or slightly to the left (between -30º and 120º). The
angle at which
the mean electric axis of the heart is positioned in the chest can
be determined
based on ECG peaks (see figure below). Several parameters can
effect the po-
sition of the heart including age, physical build, thorax shape,
and physical fit-
ness. Pathological changes can result from things like cardiac
hypertrophy, re-
duction in physical performance, or a heart attack.
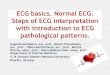
Determining the mean electric axis of the heart
Orientation of the electrical axis of the heart using the Einthoven
triangle. According to the “text- book” method (dashed red line)
specific configurations will not result in a common intersection
point. The underlying problem is that the R-wave from all three
electrodes is not at its maximum at the same time point. In this
example although the R-wave has reached a maximum for elec- trode
II, it has already returned to the baseline in the case of
electrode I and for electrode III it is at some intermediate value.
To overcome this problem, the difference between the R-wave and the
S-wave (green arrow) is used instead of the difference between the
baseline and the R-wave (dashed red arrow). This example results in
an electrical heart axis of 90o (blue). (N.B. Axis nomenclature in
the US is as follows: normal –30o to +90o; left axis deviation:
-30o to – 90o ; right axis deviation: +90o to +180o ; indeterminate
axis: the remainder (from –90o to +/-180o).
ST Segment: This segment represents the time during which the
ventricles are
contracting and emptying. Normally it is isoelectric (except in
right measure-
ments) since the entire chamber is depolarized. A vertical shift in
the ST segment
is often observed in ischemia patients (insufficient blood supply
due to coronary
artery narrowing) or after a heart attack (myocardial cell death
due to interrupted
perfusion of a certain area).
T-Wave: This represents repolarization of the ventricular
myocardium which
starts where the stimulation was active last. This accounts for the
fact that the
Einthoven-Dreieck Cabrera-Kreis
THE HEART-ECG
13
peak is generally concordant (deflecting in the same direction)
with the QRS com-
plex. Possible exceptions to this are measurements taken at V1 and
V2.
QT interval: The stimulation of the entire chamber lasts from the
beginning of the
QRS complex to the end of the T-wave. The time this takes depends
on the heart
rate (~0.25 – 0.45 sec) and, to a lesser extent, on the mass of the
electric diastole
in the chamber.
Conclusions
The ECG can provide important clues about heart rhythm and the
dipole stimula-
tion and conduction from the sino-atrial node via the AV node to
the myocardium
in the ventricle. Additionally, diagnosis of coronary
insufficiencies leading to my-
ocardial ischemia) and heart attacks are possible with information
provided by
the ECG. The role of the ECG has become secondary, however, to an
echocar-
diogram when diagnosing hypertrophy and other morphological
pathologies of
the heart.
4.2. Aims Each experimenter should perform an ECG on a test subject
and be able to an-
alyze the results.
4.3. Method The electrodes are fixed to the subject according to
the scheme provided and
attached to the recording apparatus. Please remember to decrease
the re-
sistance between the electrodes and the skin by applying a small
amount of sa-
line solution at the contact areas.
Recording: The following measurements can all be made at once and
will come
as a printed ECG at the end of each measurement.
1. Einthoven (standard bipolar) 2. Goldberg (peripheral unipolar)
3. Wilson (unipolar chest)
THE HEART-ECG
Standard ECG
1. turn on with green key 2. enter data of patient with patient
data/ECG-shift key 3. go back with same key 4. place electrodes 5.
check ECG-curves on monitor. When ok start recording with green
START-key
Respiratory sinus arrhythmia
1. with key choose Einthoven (I, II, III)
2. press manual start (2nd key from right, below the screen)
P-Q interval:
(Normal: 0.12 – 0.20 Sek. 1 degree AV block: >0.20 sec:)
QRS complex:
Frequency, regularity (difference from P) Length (normal: ≤ 0.10
sec) Geometrical position I the thorax Transition region (R=S in
Wilson) Height of the QRS complex: Sokolow-Lyon Index (S in V1 + R
in V5)
THE HEART-ECG
Are there extrasystoles?
Comments:
Observe the relationship of the Q-T segment and the distance
between T and the
next Q in a few patients with varying heart frequencies.
THE HEART-ECG
Auscultation
Doppler Measurement
exploiting the change in frequency measured by the ultrasound to
determine the
movement (flow) of the erythrocytes
Echocardiography
ECG
an electrocardiogram, used to measure the difference in potential
(differences in
electrical voltage) which are caused by the heart’s activity
Ejection fraction
the portion (in %) of the enddiastolic ventricular volume which is
ejected during
the systole
Heart murmurs
bruits caused by turbulence in the heart which are at higher
frequency than nor-
mal heart sounds
Heart rhythm generation
Heart sounds
sounds at low frequency (< 100 Hz) that occur at regular
intervals which arise
from the oscillation of the heart and/or the large arteries and
from the tension of
the myocardium and/or the closure of valves
Ischemia
Mean electric axis
(cardiac vector) graphical representation of QRS complex from 6
frontal plane
leads (I, II, III, aVR, aVL, aVF) reconstructed from the
instantaneous vectors rep-
resenting ventricular depolarization.
Myocardial Infarct
necrosis of myocardium due to interruption of blood supply to a
certain area
Phonocardiogram
phone)
Stenosis
restriction or narrowing in a blood vessel or heart valve
Transition zone
in the Wilson measurement, the time when S=R (normally between V2
and V5.
Valvular regurgitation
the inability of a valve to close properly leading to a back
current
1. Introduction
2.1. Introduction
The echocardiogram is an important noninvasive method to
investigate and diagnose the condition of the heart. It is an
ultrasound of the heart. The echocardiogram is based on the fact
that ultrasound waves are partially reflected by tissue
boundaries....
The dynamic sections visualized using this method allows for
investigations into the heart’s anatomy and movement (pumping
action). For example, ventricle area can be measured before and
after ventricular contraction allowing the ejection fraction to
...
2.2. Aims
An echocardiogram demonstration by a qualified USZ
Cardiologist
To understand the basics of what an echocardiogram is and how it is
useful as a diagnostic tool
Understanding the mechanics of the heart by visualizing the heart
cycle
The Cardiac Cycle (Timing Diagram)
Central Venous Pressure
3.1. Introduction
3.2. Aims
3.3. Method
4.1. Introduction
Schematic account of the depolarization and repolarization of the
heart with the correlating ECG
ECG
ECG electrode positions and ECG measurements
What are the deflections (peaks and curves) seen on an ECG
readout?
Determining the mean electric axis of the heart
(N.B. Axis nomenclature in the US is as follows: normal –30o to
+90o; left axis deviation: -30o to –90o ; right axis deviation:
+90o to +180o ; indeterminate axis: the remainder (from –90o to
+/-180o).
ST Segment: This segment represents the time during which the
ventricles are contracting and emptying. Normally it is isoelectric
(except in right measurements) since the entire chamber is
depolarized. A vertical shift in the ST segment is often
obse...
T-Wave: This represents repolarization of the ventricular
myocardium which starts where the stimulation was active last. This
accounts for the fact that the peak is generally concordant
(deflecting in the same direction) with the QRS complex.
Possible...
QT interval: The stimulation of the entire chamber lasts from the
beginning of the QRS complex to the end of the T-wave. The time
this takes depends on the heart rate (~0.25 – 0.45 sec) and, to a
lesser extent, on the mass of the electric diastole in ...
Conclusions
4.2. Aims
Each experimenter should perform an ECG on a test subject and be
able to analyze the results.
4.3. Method
The electrodes are fixed to the subject according to the scheme
provided and attached to the recording apparatus. Please remember
to decrease the resistance between the electrodes and the skin by
applying a small amount of saline solution at the cont...
Recording: The following measurements can all be made at once and
will come as a printed ECG at the end of each measurement.
1. Einthoven (standard bipolar)
2. Goldberg (peripheral unipolar)
3. Wilson (unipolar chest)
P-Q interval:
(Normal: 0.12 – 0.20 Sek. 1 degree AV block: >0.20 sec:)
QRS complex:
Length (normal: ≤ 0.10 sec)
Transition region (R=S in Wilson)
Height of the QRS complex: Sokolow-Lyon Index (S in V1 + R in
V5)
ST-segment
Are there extrasystoles?
Comments:
Observe the relationship of the Q-T segment and the distance
between T and the next Q in a few patients with varying heart
frequencies.
5. Glossary
Auscultation
Doppler Measurement
exploiting the change in frequency measured by the ultrasound to
determine the movement (flow) of the erythrocytes
Echocardiography
ECG
an electrocardiogram, used to measure the difference in potential
(differences in electrical voltage) which are caused by the heart’s
activity
Ejection fraction
the portion (in %) of the enddiastolic ventricular volume which is
ejected during the systole
Heart murmurs
bruits caused by turbulence in the heart which are at higher
frequency than normal heart sounds
Heart rhythm generation
Heart sounds
sounds at low frequency (< 100 Hz) that occur at regular
intervals which arise from the oscillation of the heart and/or the
large arteries and from the tension of the myocardium and/or the
closure of valves
Ischemia
Mean electric axis
(cardiac vector) graphical representation of QRS complex from 6
frontal plane leads (I, II, III, aVR, aVL, aVF) reconstructed from
the instantaneous vectors representing ventricular
depolarization.
Myocardial Infarct
necrosis of myocardium due to interruption of blood supply to a
certain area
Phonocardiogram
Sokolow-Lyon Index
Stenosis
restriction or narrowing in a blood vessel or heart valve
Transition zone
in the Wilson measurement, the time when S=R (normally between V2
and V5.
Valvular regurgitation