Embed Size (px)
Citation preview

www.AJOG.org Hypertension, Diabetes, Prematurity, Physiology Poster Session II
preeclampsia remained independently associated with cardiovascularhospitalizations (adjusted HR, 1.7; 95% CI, 1.6-1.9; P¼0.001).CONCLUSION: Previous pregnancy with preeclampsia is an indepen-dent risk factor for long-term maternal CVD. The risk is moresubstantial for patients with severe and recurrent preeclampsia.
311 Recurrent pregnancy lossea new risk factor for long
term maternal cardiovascular morbidityRoy Kessous1, Ilana Shoham-Vardi2, Gali Pariente1,Ruslan Sergienko2, Gershon Holcberg1, Eyal Sheiner11Soroka University Medical Center, Ben-Gurion University of the Negev,Department of Obstetrics and Gynecology, Faculty of Health Sciences, Beer-Sheva, Israel, 2Ben-Gurion University of the Negev, Epidemiology and HealthServices Evaluation, Beer-Sheva, IsraelOBJECTIVE: To investigate whether patients with a history of recur-rent pregnancy loss (RPL) have an increased risk for future maternalcardiovascular (CV) morbidity.STUDY DESIGN: A population-based study compared the incidence oflong-term CV morbidity in a cohort of women with and without adiagnosis of RPL. Deliveries occurred since the year 1988, with amean follow-up duration of 11.2 years. We excluded from the studywomen with known CV disease and congenital cardiovascularmalformations, chronic hypertension and multiple pregnancies. CVmorbidity was divided into 4 categories according to severity andtype including simple and complex CV events (eg, angina pectorisand congestive heart failure, respectively), and invasive and nonin-vasive cardiac procedures (eg, insertion of a stent and a treadmill
Supplem
stress test, respectively). Kaplan-Meier survival curve was used toestimate cumulative incidence of CV hospitalizations. Cox propor-tional hazards models were used to estimate the adjusted hazardratios (HR) for CV morbidity.RESULTS: During the study period 99,285 parturient met the inclu-sion criteria; 6.7% (n¼6690) occurred in patients with a history ofRPL. During the follow-up period patients with RPL had higherrates of cardiovascular morbidity including cardiac invasive andnoninvasive diagnostic procedures, simple as well as complex car-diovascular events, and hospitalizations due to cardiovascular causes(table). Using a Kaplan-Meier survival curve, patients with a previ-ous diagnosis of RPL had a significantly higher cumulative incidenceof cardiovascular hospitalizations (Figure). Using a Cox proportionalhazards model, adjusted for confounders such as preeclampsia,diabetes mellitus, and obesity, a history of RPL remained indepen-dently associated with CV hospitalizations (adjusted HR, 1.7; 95%CI, 1.5-1.8; P¼0.001).CONCLUSION: Recurrent pregnancy loss is an independent risk factorfor long term maternal cardiovascular complications and for hos-pitalizations due to a cardiovascular cause.
312 Hypertension-related intrauterine fetal demise in rural
HaitiNandini Raghuraman1, Melissa March2, Michele Hacker1,Anna Modest1, Jennifer Scott3, Sarosh Rana21Beth Israel Deaconess Medical Center, Obstetrics and Gynecology, Boston,MA, 2Beth Israel Deaconess Medical Center, Divison of Maternal FetalMedicine, Boston, MA, 3Brigham and Women’s Hospital, Divison ofWomen’s Health, Boston, MAent to JANUARY 2014 American Journal of Obstetrics & Gynecology S163
Poster Session II Hypertension, Diabetes, Prematurity, Physiology www.AJOG.org
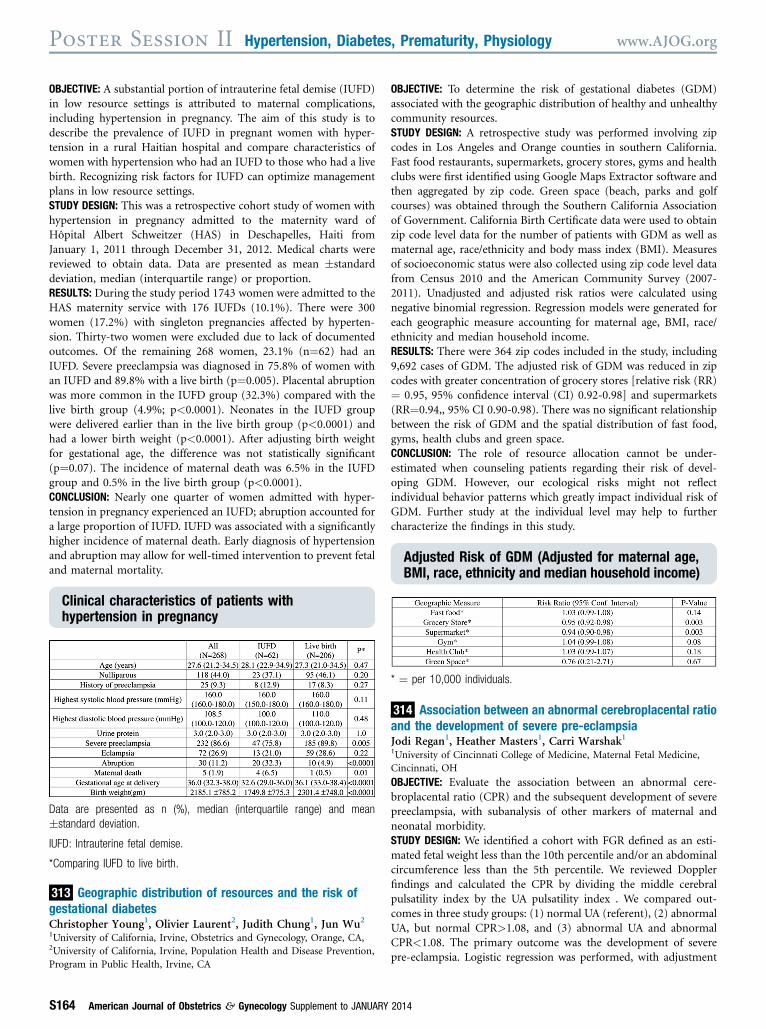
OBJECTIVE: A substantial portion of intrauterine fetal demise (IUFD)in low resource settings is attributed to maternal complications,including hypertension in pregnancy. The aim of this study is todescribe the prevalence of IUFD in pregnant women with hyper-tension in a rural Haitian hospital and compare characteristics ofwomen with hypertension who had an IUFD to those who had a livebirth. Recognizing risk factors for IUFD can optimize managementplans in low resource settings.STUDY DESIGN: This was a retrospective cohort study of women withhypertension in pregnancy admitted to the maternity ward ofHôpital Albert Schweitzer (HAS) in Deschapelles, Haiti fromJanuary 1, 2011 through December 31, 2012. Medical charts werereviewed to obtain data. Data are presented as mean �standarddeviation, median (interquartile range) or proportion.RESULTS: During the study period 1743 women were admitted to theHAS maternity service with 176 IUFDs (10.1%). There were 300women (17.2%) with singleton pregnancies affected by hyperten-sion. Thirty-two women were excluded due to lack of documentedoutcomes. Of the remaining 268 women, 23.1% (n¼62) had anIUFD. Severe preeclampsia was diagnosed in 75.8% of women withan IUFD and 89.8% with a live birth (p¼0.005). Placental abruptionwas more common in the IUFD group (32.3%) compared with thelive birth group (4.9%; p<0.0001). Neonates in the IUFD groupwere delivered earlier than in the live birth group (p<0.0001) andhad a lower birth weight (p<0.0001). After adjusting birth weightfor gestational age, the difference was not statistically significant(p¼0.07). The incidence of maternal death was 6.5% in the IUFDgroup and 0.5% in the live birth group (p<0.0001).CONCLUSION: Nearly one quarter of women admitted with hyper-tension in pregnancy experienced an IUFD; abruption accounted fora large proportion of IUFD. IUFD was associated with a significantlyhigher incidence of maternal death. Early diagnosis of hypertensionand abruption may allow for well-timed intervention to prevent fetaland maternal mortality.
Clinical characteristics of patients withhypertension in pregnancy
Data are presented as n (%), median (interquartile range) and mean
�standard deviation.
IUFD: Intrauterine fetal demise.
*Comparing IUFD to live birth.
313
Geographic distribution of resources and the risk ofgestational diabetesChristopher Young1, Olivier Laurent2, Judith Chung1, Jun Wu21University of California, Irvine, Obstetrics and Gynecology, Orange, CA,2University of California, Irvine, Population Health and Disease Prevention,Program in Public Health, Irvine, CAS164 American Journal of Obstetrics & Gynecology Supplement to JANUARY
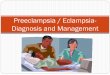
OBJECTIVE: To determine the risk of gestational diabetes (GDM)associated with the geographic distribution of healthy and unhealthycommunity resources.STUDY DESIGN: A retrospective study was performed involving zipcodes in Los Angeles and Orange counties in southern California.Fast food restaurants, supermarkets, grocery stores, gyms and healthclubs were first identified using Google Maps Extractor software andthen aggregated by zip code. Green space (beach, parks and golfcourses) was obtained through the Southern California Associationof Government. California Birth Certificate data were used to obtainzip code level data for the number of patients with GDM as well asmaternal age, race/ethnicity and body mass index (BMI). Measuresof socioeconomic status were also collected using zip code level datafrom Census 2010 and the American Community Survey (2007-2011). Unadjusted and adjusted risk ratios were calculated usingnegative binomial regression. Regression models were generated foreach geographic measure accounting for maternal age, BMI, race/ethnicity and median household income.RESULTS: There were 364 zip codes included in the study, including9,692 cases of GDM. The adjusted risk of GDM was reduced in zipcodes with greater concentration of grocery stores [relative risk (RR)¼ 0.95, 95% confidence interval (CI) 0.92-0.98] and supermarkets(RR¼0.94,, 95% CI 0.90-0.98). There was no significant relationshipbetween the risk of GDM and the spatial distribution of fast food,gyms, health clubs and green space.CONCLUSION: The role of resource allocation cannot be under-estimated when counseling patients regarding their risk of devel-oping GDM. However, our ecological risks might not reflectindividual behavior patterns which greatly impact individual risk ofGDM. Further study at the individual level may help to furthercharacterize the findings in this study.
Adjusted Risk of GDM (Adjusted for maternal age,BMI, race, ethnicity and median household income)
* ¼ per 10,000 individuals.
314
Association between an abnormal cerebroplacental ratioand the development of severe pre-eclampsiaJodi Regan1, Heather Masters1, Carri Warshak11University of Cincinnati College of Medicine, Maternal Fetal Medicine,Cincinnati, OHOBJECTIVE: Evaluate the association between an abnormal cere-broplacental ratio (CPR) and the subsequent development of severepreeclampsia, with subanalysis of other markers of maternal andneonatal morbidity.STUDY DESIGN: We identified a cohort with FGR defined as an esti-mated fetal weight less than the 10th percentile and/or an abdominalcircumference less than the 5th percentile. We reviewed Dopplerfindings and calculated the CPR by dividing the middle cerebralpulsatility index by the UA pulsatility index . We compared out-comes in three study groups: (1) normal UA (referent), (2) abnormalUA, but normal CPR>1.08, and (3) abnormal UA and abnormalCPR<1.08. The primary outcome was the development of severepre-eclampsia. Logistic regression was performed, with adjustment
2014





![Conditions Associated with Intrauterine Fetal Demise (IUFD ... · A. M. Kafy, A. Oraif DOI: 10.4236/ojog.2017.713129 1263 Open Journal of Obstetrics and Gynecology 500 gm [3]. In](https://img.pdfslide.net/doc/110x75/5d4f3d7388c9937a2b8b57ab/conditions-associated-with-intrauterine-fetal-demise-iufd-a-m-kafy-a.jpg)



















![Early intrauterine development of mixed giant … · Early intrauterine development of mixed giant ... but with intrauterine death at 29 weeks [5]. Fetal . Early intrauterine development](https://img.pdfslide.net/doc/110x75/5b63022f7f8b9ade588b8aac/early-intrauterine-development-of-mixed-giant-early-intrauterine-development.jpg)