Embed Size (px)
Citation preview
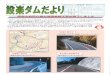
Patient Name: ____________________________________________________________________
DOB: ____________________ Appt. Date: ___________________ Time: ___________________
Phone: _____________________Allergies: q NKA___________________________BUN: ______________________CREATININE: ____________________
q Palms • 14525 Bruce B. Downs Blvd.(813) 972-0669 • Fax: (813) 879-1809
q North Dale Mabry • 17503 N. Dale Mabry Hwy.(813) 968-4540 • Fax: (813) 879-1809
q Habana • 4719 N. Habana Ave.q Bloomingdale • 3350 Bell Shoals Roadq South Tampa • 2106 S. Lois Ave.q BBD • 3069 Grand Pavilion Dr.
q Wesley Chapel • 2324 Oak Myrtle Laneq Northside • 2716 University Square Driveq North Dale Mabry • 17503 N. Dale Mabry Hwy.q Carrollwood • 14499 N. Dale Mabry Hwy., Ste. 150q Brandon • 500 Vonderburg Drive, West Tower, Ste. 111
Di agnosis orSigns/Symptoms: 1.__________________________________2._______________________________________3.__________________________________
Ordering Please Physician OrderPhysician Print ________________________________________________Signature _____________________________________Date_________________
q Radiologist to determine guidance method for breast biopsy
q Stereotactic Breast Biopsy R / Lq Ultrasound Breast Biopsy R / Lq MRI Breast Biopsy R / L
q Brain (COW)q Carotidsq Chestq Chest PE Protocolq Coronary Arteries w/calcium scoreq Coronary Arteries w/o calcium scoreq Aorta Thoracic q Abdomen Aortaq Renal Transplant Evaluationq Renal Arteriesq Pelvisq Abdomen Aorta w/Runoffq Upper Extremityq Lower Extremity (to include Pelvis)
(All CTA’s include IV contrast)PROVIDE BUN/CREATININE
MRI
q Brain (COW) w/o contrastq Arch w/ Carotid w & w/o contrastq Chest w & w/o contrastq Abdomen w & w/o contrastq Pelvis w & w/o contrastq Renals (w/MRI) w & w/o contrastq MRA Run Off to include Pelvis &
Lower Extremity w & w/o contrastPROVIDE CREATININE LEVEL
q Brainq Temporal Bones / IACS /
Mastoids q w/MPRq Facial Bones q w/MPRq Orbits q w/MPRq Sinus Maxillofacialq Sinus Coronalq Soft Tissue Neck q w/MPRq Chest/Thorax w/o contrast
(Pulmonary Nodule Follow-up)q Chest / Thorax q w/MPRq Abdomen & Pelvisq Abdomen q w/MPRq Pelvis q w/MPRq Enterography Protocol -
Abdomen w/ & w/o -3D MPRq Kidney Stone Protocol-Abdomen
& Pelvisq Virtual Colonoscopyq Incomplete colonoscopyq Non-colonoscopy candidateq Other / screening
q Cervical Spine w/3D MPRq Thoracic Spine w/3D MPRq Lumbar Spine w/3D MPRq Upper Extremity w/3D MPR q Lower Extremity w/3D MPRq Urography Protocol-Abdomen
& Pelvis w/ & w/o-3D MPR
m W/ CONTRASTm W/O CONTRASTm W & W/O CONTRAST
MPR: Multiplanar ReconstructionPROVIDE BUN/CREATININE ON CONTRAST EXAMS
MR Angiography
CT
CT Angiography
PET/CT Imaging
Nuclear Medicine
q Digital Bilateral Screening w/CADand Bone Density/DEXA
q Digital Bilateral Screening w/CADq Digital Bilateral Diagnostic
w/ Ultrasound (if medically necessary)q Digital Unilateral Diagnostic R / L
w/ Ultrasound (if medically necessary)Implants: q Yes q Noq Breast Sonogram R / Lq Additional ViewsPrevious Films Are LocatedAt:______________________
Digital Mammography
Breast Biopsy
DEXA
q Bone Densityq Vertebral Fracture Assessmentq Body Composition Analysis
Rev. 1/12
X-Ray
q Brainq Orbitsq Brain w/Orbitsq IAC’sq TMJq Pituitaryq Soft Tissue Neckq Chestq Brachial Plexusq Cervical Spineq Thoracic Spineq Lumbar Spineq Breast - Bilateral Diagnostic W & W/O CONTRASTq Breast - Implant (Rupture) W/O CONTRASTq Abdomenq Abdomen w/ & w/o contrast - Adrenal
Protocolq MRCPq Renalsq Urography-Abdomen & Pelvisq Pelvis - Prostateq Pelvis w/ & w/o contrast - Uterine Fibroid q Pelvis - Routineq Pelvis - Dynamicq Pelvis w/o contrast - Fetal q Shoulder R / Lq Elbow R / Lq Wrist R / Lq Hand R / Lq Hip R / Lq Femur R / Lq Tib/Fib R / Lq Knee R / Lq Ankle R / Lq Foot R / Lq Liver Imaging w/ EOVIST Contrast m W/O CONTRASTm W & W/O CONTRAST
PROVIDE CREATININE LEVEL ON CONTRAST EXAMS
o Other:
Ultrasound
(First) (MI) (Last) o CD o Film: Deliver with Reporto Fax STAT Report: ____________________________
www.TowerRadiologyCenters.com/appointmentrequest
q PET/CT (Non-Diagnostic CT)
q PET/CT (with Diagnostic CT w & w/o)Please specify area for Diagnostic CTqALL OR check all that apply:qNeck qChest qAbd qPelvis
q PET / Brain PROVIDE BUN/CREATININE WHEN ORDERING DIAGNOSTIC CT
Myocardial Perfusion / Nuclear Stress Testq with Treadmill q no Treadmill
q MUGAq Bone Scan - Whole Bodyq Bone Scan - 3 Phaseq Bone Scan - Spine w/SPECTq Biliary Scan with GBEFq 111 Indium WBC Scanq Liver / Spleen Scanq Thyroid Uptake ScanThyroid Therapy to include ConsultqHyperthyroidism q Thyroid Cancer
q 131 I Whole Body Scanq Liver Hemangiomaq Renal Scan with FlowRenal Scan with Flowq Lasix washout q Captopril / Vaso
q Gastric Emptying Studyq Parathyroid scan w/Sestamibi
q Skullq Facialq Orbitsq Sinusq Sinus/Waters1viewq Nasal Bonesq Soft Tissue Neckq Chest (CXR)q Abdominal Seriesq KUBq Pelvisq Hipq SI Jointsq Scoliosisq Sacrum/Coccyxq C Spineq C Spine Complete
w/ Oblique and Flex. and/ or Ext.
q T Spineq L Spineq L Spine Complete
w/Bending Viewsq Bone Ageq TMJq Extremity/Other:_____________R / L_____________R / L
q Thyroidq Echocardiogramq Abdominal Total
(Pancreas, Liver, GB, Kidney, Aorta, IVC, Spleen)Retroperitonealq Kidney / Bladder q Aorta
q GB / Pancreas / Liver (RUQ)q Spleen (Left Upper Quadrant)q Renal transplant w/dopplerq Transvaginalq Pelvic w/transvaginalq Pelvicq OB Transabdominalq OB Transvaginalq Testicular Sono w/dopplerq Appendixq Bladder
Vascular Doppler Ultrasound
q High Field q Open
m Arthrogramm Arthrogramm Arthrogram
m Arthrogram
m Arthrogramm Arthrogram
Scheduling: (813) 874-3177 • Fax: (813) 879-1809
q Pre-Op Chest X-ray / EKG
q Hysterosalpingogramq EKGq Routine Stress Test
(Non Pharmacological - Non Thallium)
Special Exams
FULL SERVICE RADIOLOGY CENTERS OPEN MRI
q Liver Dopplerq Venous Doppler
Lower Extremityq Bilateralq Unilateral R / LUpper Extremityq Bilateralq Unilateral R / L
q Carotid Dopplerq Arterial Doppler w/ABI
Lower Extremityq Bilateralq Unilateral R / LUpper Extremityq Bilateralq Unilateral R / L
q Renal Arterial Dopplerq SMA Doppler
(Superior Mesenteric Arteries)
This exam is medically necessary for this patient
JOHN
MO
ORE
RD.
PARS
ONS
AVE
.
Bloomingdale Radiology Center3350 Bell Shoals Road
813.654.4883
5454
54
56
60
60
41
41
41
92
75
4
75
275
275
275
580 TOLL
589
TOLL
589
TOLL
589
301
301
574
Old Old TTampa Bayampa Bay
HillsboroughHillsboroughBayBay
CO
LUM
BIA D
R.
BAYSHORE
BLVD.
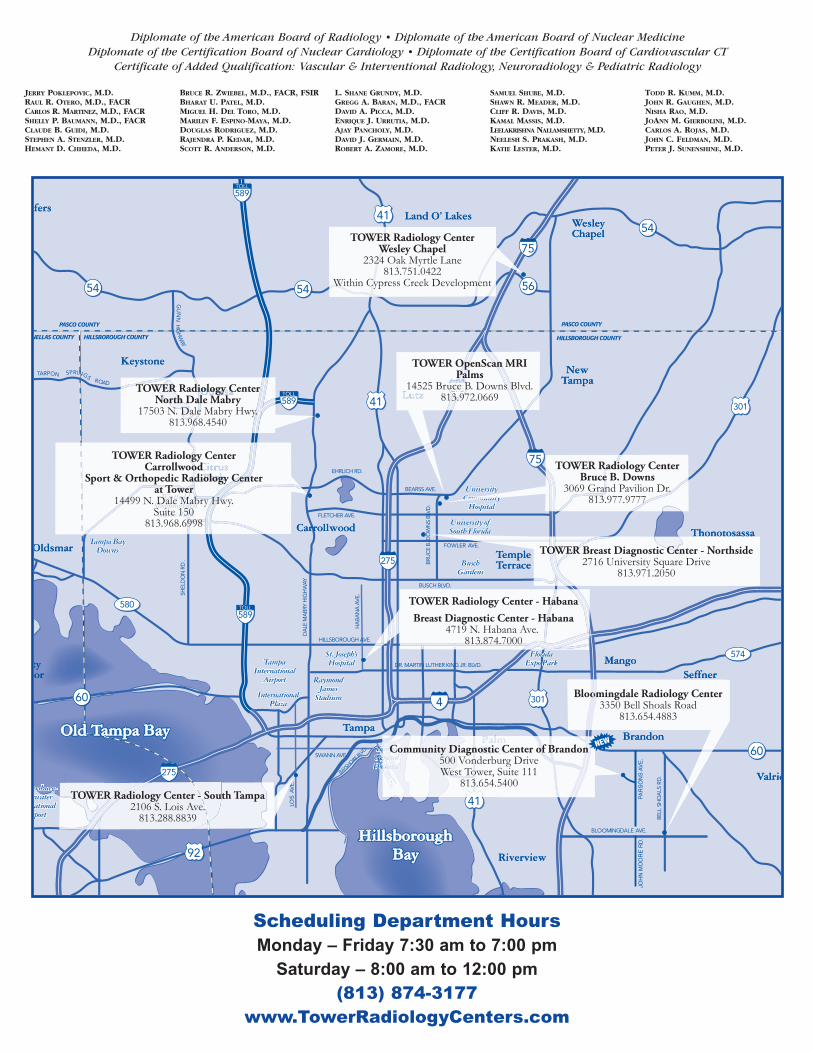
TOWER Radiology CenterWesley Chapel
2324 Oak Myrtle Lane813.751.0422
Within Cypress Creek Development
T
275
41
OLU
MBIA
DR.
LU
LUM
U
M
LUM
U
M
Community Diagnostic Center of Brandon500 Vonderburg DriveWest Tower, Suite 111
813.654.5400
TOWER OpenScan MRIPalms
14525 Bruce B. Downs Blvd.813.972.0669
TOWER Radiology CenterBruce B. Downs
3069 Grand Pavilion Dr.813.977.9777
TOWER Radiology CenterNorth Dale Mabry
17503 N. Dale Mabry Hwy.813.968.4540
TOWER Radiology CenterCarrollwood
Sport & Orthopedic Radiology Centerat Tower
14499 N. Dale Mabry Hwy.Suite 150
813.968.6998
TOWER Radiology Center - HabanaBreast Diagnostic Center - Habana
4719 N. Habana Ave. 813.874.7000
TOWER Radiology Center - South Tampa2106 S. Lois Ave.
813.288.8839
TOWER Breast Diagnostic Center - Northside2716 University Square Drive
813.971.2050
Scheduling Department Hours
Monday – Friday 7:30 am to 7:00 pm
Saturday – 8:00 am to 12:00 pm
(813) 874-3177
www.TowerRadiologyCenters.com
JERRY POKLEPOVIC, M.D.RAUL R. OTERO, M.D., FACRCARLOS R. MARTINEZ, M.D., FACRSHELLY P. BAUMANN, M.D., FACRCLAUDE B. GUIDI, M.D.STEPHEN A. STENZLER, M.D.HEMANT D. CHHEDA, M.D.
BRUCE R. ZWIEBEL, M.D., FACR, FSIRBHARAT U. PATEL, M.D.MIGUEL H. DEL TORO, M.D.MARILIN F. ESPINO-MAYA, M.D.DOUGLAS RODRIGUEZ, M.D.RAJENDRA P. KEDAR, M.D.SCOTT R. ANDERSON, M.D.
L. SHANE GRUNDY, M.D.GREGG A. BARAN, M.D., FACRDAVID A. PICCA, M.D.ENRIQUE J. URRUTIA, M.D.AJAY PANCHOLY, M.D.DAVID J. GERMAIN, M.D.ROBERT A. ZAMORE, M.D.
SAMUEL SHUBE, M.D.SHAWN R. MEADER, M.D.CLIFF R. DAVIS, M.D.KAMAL MASSIS, M.D.LEELAKRISHNA NALLAMSHETTY, M.D.NEELESH S. PRAKASH, M.D.KATIE LESTER, M.D.
TODD R. KUMM, M.D.JOHN R. GAUGHEN, M.D.NISHA RAO, M.D.JOANN M. GIERBOLINI, M.D.CARLOS A. ROJAS, M.D.JOHN C. FELDMAN, M.D.PETER J. SUNENSHINE, M.D.
Diplomate of the American Board of Radiology • Diplomate of the American Board of Nuclear MedicineDiplomate of the Certification Board of Nuclear Cardiology • Diplomate of the Certification Board of Cardiovascular CT
Certificate of Added Qualification: Vascular & Interventional Radiology, Neuroradiology & Pediatric Radiology

![Паспорт на устройство регулирующее ИЗОДРОМ-УМ2 · \o o e.l r! o,q rl.] El U^ ulv ts =* < r_ ilo3 E,Q =-' - 2 E- r \ >-^!v i](https://img.pdfslide.net/doc/110x75/5ead36c0caf0d16b1f470ccc/-f-ff-oe-oe2.jpg)