Embed Size (px)
Citation preview

1
Remembering the forgotten ventricle:Management of acute right ventricular failure in
Pulmonary Hypertension
Mandar Aras, MD, PhDAssistant Professor
Advanced heart failure and heart transplantUniversity of California, San Francisco
Objectives
• Review the descriptive and hemodynamic classification of pulmonary hypertension
• Discuss the significance of acute right heart failure (ARHF) in PH
• Discuss management principles for ARHF in setting of pre-capillary vs. post-capillary PH, including the role of:– Oxygenation– Pulmonary vasodilator therapies– Inopressors– MCS, transplantation
Pulmonary Hypertension(PH)
Sustained elevation of mean pulmonary artery pressure*:
mPAP > 25 mmHg
Simonneau et al, J Am Coll Cardiol. 2013;62:D34-41
* mPAP = Normal: 8 - 20 mmHgePASP Echo Doppler > 40 mmHg
PH ≠ PAH

2
5th WSPH Updated Classification of Pulmonary Hypertension, Nice 2013
GROUP 1 – Pulmonary Arterial Hypertension (PAH) 1.1 Idiopathic PAH1.2 Heritable PAH1.3 Drug- and Toxin-Induced1.4 Associated with:
1.4.1 Connective Tissue Disease1.4.2 Human Immunodeficiency Virus (HIV)
Infection1.4.3 Portal Hypertension1.4.4 Congenital Heart Disease1.4.5 Schistosomiasis
1’ PVOD and/or PCH
1” Persistent PH of the Newborn (PPHN)
GROUP 2 – PH Due to Left Heart Disease2.1 LV Systolic Dysfunction (HFrEF)2.2 LV Diastolic Dysfunction (HFpEF)2.3 Valvular Disease
2.4 Congenital/Acquired Left Heart Inflow/ Outflow Tract Obstruction and Congenital Cardiomyopathies
GROUP 3 –PH Due to Lung Disease and/or Hypoxia3.1 Chronic Obstructive Pulmonary Disease3.2 Interstitial Lung Disease3.3 Other Pulmonary Diseases With Mixed Restrictive
and Obstructive Pattern3.4 Sleep-disordered Breathing3.5 Alveolar Hypoventilation Disorders3.6 Chronic Exposure to High Altitude3.7 Developmental Lung Diseases
GROUP 4–Chronic Thromboembolic PH (CTEPH)
GROUP 5 – PH With Unclear Multifactorial Mechanisms5.1 Hematologic Disorders: Chronic Hemolytic Anemia,
Myeloproliferative Disorders, Splenectomy
5.2 Systemic Disorders: Sarcoidosis, Pulmonary Histiocytosis, Lymphangioleiomyomatosis
5.3 Metabolic Disorders: Glycogen Storage Disease, Gaucher Disease, Thyroid Disorders
5.4 Others: Tumoral Obstruction, Fibrosing Mediastinitis, Chronic Renal Failure, Segmental PH
Simmoneau G, et al. JACC. 2013; 62:D34-41.
Strange G et al. Heart 2012;98:1806-1811.
• Single center study from Australia • 6,994 screened 936 pts (9.1%) with PH on
ECHO Doppler (defined as ePASP >40 mmHg)
Etiology of PH on Echocardiogram
VC RA RV PA PVPC
LA LV Ao
PH Hemodynamic Profiles:
Vachiery JL et al, J Am Coll Cardiol 2013;62: D100-8Fang J et al, J Heart Lung Transplant 2012;31:913–33Galie N et al, Eur Respir J 2009;34(6):1219-63
VC RA RV PA PVPC
LA LV Ao
PH Hemodynamic Profiles:
Pre-capillaryPH
Vachiery JL et al, J Am Coll Cardiol 2013;62: D100-8Fang J et al, J Heart Lung Transplant 2012;31:913–33Galie N et al, Eur Respir J 2009;34(6):1219-63
Post-capillaryPH
Combined post-& pre-capillary
PH(Mixed PH)

3
VC RA PA PVPC
LA LV Ao
Group 1 – PAHGroup 3,4,5
Pre-capillary PHPA mean ≥ 25mmHg
PAWP < 15 mmHg
TPG > 12PVR > 3 Wu
RV
Modified from: Galie N et al. Eur Respir J. 2009. 34(6):1219-63
Fang J et al. J Heart Lung Transplant 2012;31:913–33Vachiery JL et al, J Am Coll Cardiol 2013;62: D100-8
Normal
PAH
FDA-Approved Specific Therapies for PAHEndothelin Receptor Antagonists (oral)
• Bosentan• Ambrisentan• Macitentan
Phosphodiesterase Type-5 Inhibitors (oral)
• Sildenafil• Tadalafil
Prostacyclin Derivatives
• Epoprostenol: IV
• Iloprost: inhalational
• Treprostinil: inhalational, oral, SQ or IV
Soluble Guanylate Cyclase Stimulators (oral)
• Riociguat (also approved for CTEPH)
Prostacyclin Receptor Agonist (oral)• Selexipag
Simonneau G et al, J Am Coll Cardiol 2013;62:D34-41Vachiery JL et al, J Am Coll Cardiol 2013;62: D100-8Fang J et al, J Heart Lung Transplant 2012;31:913–33Galie N et al, Eur Respir J 2009;34(6):1219-63
Group 2: PH due to left heart diseaseLV Systolic dysfunctionLV Diastolic dysfunctionValvular disease LH obstruction & Congenital CMP
VC RA RV
Isolated Post-Capillary PHPAWP>15 mmHg
TPG < 12PVR nl range
• Myocardial DiseaseCMP-ischemic/non-isc.
Hypertrophic CMPRestrictive/infiltrative CMP
• Pericardial disease
PA PVPVPPC
LALAP
LV Ao
Systemic HTNAoV Disease
LVEDP
MR
HFrEF, HFpEF
Combined post- & pre-capillary PH(CpcPH)
Mixed hemodynamic profile PAWP > 15 mmHg
TPG>12 PVR > 3 Wu
VC RA PAPC
LALAP
LV Ao
LVEDP
PVPVP
RV
Left sided filling pressure Neurohormones, cytokines, other mediators
Fang J et al, J Heart Lung Transplant 2012;31:913–33Galie N et al, Eur Respir J 2009;34(6):1219-63
Moraes et al, Circ 2000; 1718
Simonneau et al, J Am Coll Cardiol 2013;62:D34-41Vachiery JL et al, J Am Coll Cardiol 2013;62: D100-8

4
Combined post- & pre-capillary PH(CpcPH)
Mixed hemodynamic profile PAWP > 15 mmHg
TPG>12 PVR > 3 Wu
VC RA PAPC
LALAP
LV Ao
LVEDP
PVPVP
RV
Left sided filling pressure Neurohormones, cytokines, other mediators
Fang J et al, J Heart Lung Transplant 2012;31:913–33Galie N et al, Eur Respir J 2009;34(6):1219-63
Moraes et al, Circ 2000; 1718
Simonneau et al, J Am Coll Cardiol 2013;62:D34-41Vachiery JL et al, J Am Coll Cardiol 2013;62: D100-8
FDA-Approved Specific Therapies for PAHEndothelin Receptor Antagonists (oral)
• Bosentan• Ambrisentan• Macitentan
Phosphodiesterase Type-5 Inhibitors (oral)
• Sildenafil• Tadalafil
Prostacyclin Derivatives• Epoprostenol: IV
• Iloprost: inhalational
• Treprostinil: inhalational, oral, SQ or IV
Soluble Guanylate Cyclase Stimulators (oral)
• Riociguat (also approved for CTEPH)
Prostacyclin Receptor Agonist
• Selexipag
Pulmonary hypertension (PH) from any etiology is associated with:
• Worse prognosis due to right heart failure
• Increased morbidity and mortality • Reduced exercise capacity
A clinical syndrome due to an alteration ofstructure and/or function of the right heart systemthat leads to a sub-optimal delivery of blood flowto the pulmonary circulation and/or elevatedvenous pressures - at rest or with exercise.
Working Definition of Right Heart Failure
Right Heart Failure Summit: Towards a Common LanguageBoston, MA 2012, 2013

5
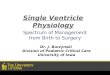
PAH: It’s all about the RV!!
Van de Veerdonk MC, et al. J Am Coll Cardiol. 2011;58:2511-2519.
100
80
60
40
20
0
Sur
viva
l, %
0 0 50 75 100 125
Time, months
1. RVEF > 35%, PVR < 650 (n=36)2. RVEF > 35%, PVR > 650 (n=20)3. RVEF < 35%, PVR < 650 (n=13)4. RVEF < 35%, PVR > 650 (n=41)
p < 0.01
PH in LHD: It’s all about the RV!
Voelkel NF, et al. Circulation. 2006;114:1883-1891.
1.0
0.8
0.6
0.4
0.2
0.0
-0.2
Cum
ula
tive
Pro
po
rtio
n S
urv
ivin
g
0 10 20 30 40 50 60 70
months
P<0.001
Group 1: Normal PAP, preserved RVEF Group 2: Normal PAP, low RVEF Group 3: High PAP, preserved RVEF Group 4: High PAP, low RVEF
Category High Risk Variables Predicting RVF
Demographic • Age• Female gender
Clinical setting • Need for mechanical ventilation• Need for dialysis/CRRT
Biomarkers • High INR• High NT-proBNP (heterogenous)
Hemodynamic (RHC) • Low RVSWI• High CVP
Echocardiography • Moderate to severe RVD• Elevated RV/LV ratio• Low RV free wall longitudinal systolic
strain
Bellavia D et al.Eur J Heart Fail 2017; 9, 926–946
LVAD outcomes:It’s all about the RV (RV/PA
coupling)
Meta-analysis of:-36 studies-4428 pts-35% (995) pts developed RHF
Pulmonary hypertension
RV Pressure overload
Adaptive RV hypertrophy
Decreased wall stress
Maladaptive RV hypertrophy & fibrosisDiastolic dysfunction
De Marco T. Advances PH 2005;4:16Nootens et al. J Am Coll Cardiol 1995;26:1581 Voelkel et al. Circ 2006;114:1883

6
Pulmonary hypertension
RV Pressure overload
Adaptive RV hypertrophy
Decreased wall stress
Maladaptive RV hypertrophy & fibrosisDiastolic dysfunction
Compensated Phase
• Normal CO • Normal RAP
Decompensating Phase
• Higher RAP to maintain
adequate CO• CO with exercise
De Marco T. Advances PH 2005;4:16Nootens et al. J Am Coll Cardiol 1995;26:1581
Neurohormonal
Cytokine,
& other
mediator activation
Altered gene
expression
RV remodeling
Voelkel et al. Circ 2006;114:1883
De Marco T. Advances PH 2005;4:16 Haddad et al. Circ 2008;117;1717Belenkie et al. Ann Med 2001;33:236
Decompensated Phase
RAP CO
• Congestive hepatopathy/ascites/
peripheral edema
• Renal congestion
•Hypoperfusion
• Hypoxemia (PFO)
• Acidosis
• Life-threatening
dysrrhythmias
Morris-Thurgood et al, Heart Fail Rev 2000;5:307Watanabe et al, Circ Res 1990;67:923
Cont.
LV
RV
Normal PAH
LVRV
RA LA
Api
cal F
ou
r C
ha
mb
er
Par
aste
rnal
Sho
rt A
xis
PAHNormal
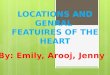
Echocardiogram in PAH Measuring RV systolic function
• TAPSE (Tricuspid annular plane systolic excursion)– TAPSE < 1.6 indicates RV systolic dysfunction
• Fractional area change (FAC)– Two-dimensional FAC (as a percentage) provides an estimate of RV
systolic function.
– Two-dimensional FAC < 35% indicates RV systolic dysfunction.
• Tissue doppler S’ – Easy to measure, reliable and reproducible.
– S’ velocity < 10 cm/s indicates RV systolic dysfunction.
J Am Soc Echocardiogr 2010;23:685-713.

7
Management of Acute Right Heart Failure (ARHF) in PH
ARHF: Goals of Management
• Immediate– Restore oxygenation – Treat congested/ volume overload state– Restore vital organ perfusion (kidneys, brain, heart, liver)
• Short Term– Identify and treat precipitating factors– Initiate/readjust maintenance regimen– Minimize ICU time and length of stay
• Intermediate and Long Term– Prevent early readmission– Optimize medical regimen to
• Alleviate symptoms• Slow disease progression• Reduce morbidity & mortality• Successfully bridge patients to more definitive therapy
– PAH lung tx– PH in LHD with VAD Heart Transplant
De Marco T. Advances PH 2005;4:16 ; Haddad et al, Circ 2008;117;1717
Medical Management Principles in ARHF
Hoeper MH, et al. Am J Respir Crit Care Med.2011;184:1114-1124. (modified)
Identify and Treat Triggering Factor(s)
Reduce RV Afterload: - External (PVR, PAC) - Internal (Wall Stress)
Optimize Cardiac OutputCVO2 >65%, CI >2.0 l/min/m2
Optimize Perfusion Pressure
Optimize Preload
Medical Management Principles in ARHF
Hoeper MH, et al. Am J Respir Crit Care Med.2011;184:1114-1124. (modified)
Identify and Treat Triggering Factor(s)
• Dietary indiscretion, infections, anemia, arrhythmias, co-morbidities
• Rule out PE, MI, other conditions• Discontinue use of NSAIAs, COX-2 inhibitors• Hypoxemia (Maintain SaO2 >90%); Avoid intubation in severe PAHReduce RV Afterload:
- External (PVR, PAC) - Internal (Wall Stress)
Optimize Cardiac OutputCVO2 >65%, CI >2.0 l/min/m2
Optimize Perfusion Pressure
Optimize Preload

8
Medical Management Principles in ARHF
Hoeper MH, et al. Am J Respir Crit Care Med.2011;184:1114-1124. (modified)
Identify and Treat Triggering Factor(s)
Reduce RV Afterload: - External (PVR, PAC) - Internal (Wall Stress)
• iNO, IV and/or inhaled Prostanoids (PAH) • PDE5 inhibitors (IV, oral); others• Optimal fluid management
Optimize Cardiac OutputCVO2 >65%, CI >2.0 l/min/m2
Optimize Perfusion Pressure
Optimize Preload
• Use of pulmonary vasodilators in chronic PAH differs from acute PH/ RH failure
• Potential adverse hemodynamic effects of non-selective pulmonary vasodilators VQ mismatch– Inhaled treatments most selective– iNO most selective; no effect on SVR,but may lead to pulmonary
edema in PH due to LHD • Systemic administration of pulmonary vasodilators can induce
hypotension worsen RV ischemia • In presence of fixed pulmonary venous hypertension (PVOD), in
transpulmonary flow may precipitate pulmonary edema• Monitor renal function closely!!
Kieler-Jensen N et al. J Heart Lung Transplant. 1995; 14:436. McNeil K et al. Thorax 2003;58:157.Galie N, Eur Respir J 2009;34:1219. Price LC et al. Critical Care 2010;14:169
Reducing RV External Afterload (PVR)Pulmonary Vasodilators - General Considerations:
• Oxygen
– Aim for SpO2 >90%
– Avoid intubation in severe PAH cardio-circulatory collapse
• Inhaled NO in pre-capillary PH (PAH)
– selective pulmonary vasodilator
– PVR, no Δ on SVR, MAP
– no V/Q mismatch
• Other inh. Prostanoids (iloprost, epoprostenol) beneficial in pre-capillary PH (PAH)
– enhanced effect with PDE 5-Inhibitors
• IV, oral PDE-5 Inhibitors Frostell CG et al. Anesthesiology 1993;78(3):427-35Hoeper MM et al. J Am Coll Cardiol 2000;35:176
McLaughlin VV et al. J Am Coll Cardiol 2009;53:1573. Sitbon O et al. J Am Coll Cardiol 2002,40:780. Preston IR et al. Pulm Circ 2013,;3:1
Reducing RV External Afterload (PVR): Pulmonary Vasodilators
Loe E et al. Circulation. 1994;90:2780-2785
19 patients with class III (n=5) to IV (n=14) HF; mean PVR 2.8 WUProtocol: 80 ppm inhaled nitric oxide (iNO) over 10 minutes
PH in LHD: iNO
PCWP

9
PA Vasodilation PA flow
No venous dilation(inactivated by Hgb)
Hydrostatic pressure in capillary bed Pulmonary edema
Effect of INO On Pulmonary CirculatoryIn Setting of PVH
Left sided filling pressure
Fixed PVH (PVOD)• IV prostacyclin derivatives initial treatment of choice in PAH
(epoprostenol, treprostinil, iloprost)
– All reduce PVR and improve RV performance
– Epoprostenol preferred agent in ARHF• Short acting
• Shown to improve survival
• Caveat: systemic hypotension which can limit use
– May need concomitant pressors
– Avoid tachyarrhythmia
Frostell CG et al. Anesthesiology 1993;78(3):427-35McLaughlin VV et al. J Am Coll Cardiol 2009;53:1573. Sitbon O et al. J Am Coll Cardiol 2002,40:780.
De Marco T. Advances PH 2005; 4:16;
Reducing RV External Afterload (PVR, PAC): Pulmonary Vasodilators
• Sildenafil highly selective (>4000 fold) for PDE-5 over PDE-3
– Shown to exert milrinone-like effect via PDE-3 inhibition, augmenting RV function
• No significant effect on SBP or heart rate
• Other effects:
– Increase in coronary perfusion– Enhances endothelial mediated vasodilation
– Attenuates adrenergic stimulated contractility– In severe HF: PCWP and CO
• Oral or IV sildenafil may provide a transition method from iNO or inhaled epoprostenol
Degerman E et al. J Biol Chem 1997;272:6823 Aladdini J et al. Am J Cardiol 2004;94:1475Katz SD et al. J Am Coll Cardiol 2000;36:845 Borlaug BA et al. Circulation 2005;112:2642Hermann HC et al. N Engl J Med 2000;342:1622 Vachiery JL et al. BJCP 2011; 71:289
Reducing RV External Afterload (PVR): Pulmonary Vasodilators: Sildenafil
Sildenafil in PH due to Advanced HF
• 14 pts with AHF (EF<24+14%) and Cpc PH refractory to milrinone, dobutamine, nitroprusside, nesiritide
• Sildenafil 25-50 mg administered orally q 8hr <3 doses• 93% of pts:mPAP >20%; 20% pts PVR/SVR (relative PA
selectivity); 50 mg more effective; sildenafil safe & effective to improve candidacy for OHT
Aleaddini et al. Am J Cardiol 2004; 94; 1475
Baseline Post-sild. P value
mPAP (mmHg) 44+11 31+14 <0.001
PAWP (mmHg) 25+6 18+6 <0.001
CI (L/min/m2) 2.4+0.9 2.8+1.0 <0.01
PVR
(dyne.s/cm5)311+115
(3.9 Wu)
191+74
(2.4 Wu)
<0.01
SAP (mmHg) 108+19 104+21 NS
DAP (mmHg) 62+10 59+11 NS

10
VADs in PH due to Advanced HF
Masri CS et al. ASAIO J. 2017 Mar/Apr;63(2):139-143.
Hemodynamics were collected and analyzed both pre and post (w/in 48-72 hrs) LVAD implantation on a cohort of 64 HFrEF pts.
RV afterload almost always declines with LVAD insertion and does so rapidly
LVADs Decrease “Fixed” PH in Cardiac Transplant Candidates(Reduction in Left Sided Filling Pressures)
Zimpfer et al. J Thorac Cardiovsc Surg 2007;133:689
• Prospective, 6 week study• N= 35 pts• Severe HF and indication for LVAD• “Fixed” Cpc PH: PVR >3.5 Wu despite vasodilators/inodilators• RH cath before LVAD, then 3 days and 6 weeks post- LVAD• Device: MicroMed DeBakey (24), DuraHeart (3), Novacor (8)
Baseline 3 Days 6 Weeks
MPAP (mmHg) 44.0+6.2 28.6+7.3* 18.4+4.3*
PAWP (mmHg) 28.1+6.0 12.0+5.7* 10.0+3.6*
CO (L/min) 3.1+0.8 5.7+0.7* 4.0+0.9**
PVR (Wood units) 5.1+2.6 2.9+1.3* 2.0+0.8*
* P< .0001; **P= .002 [ TPG from >16 to <8 mmHg]
PDE-5 Inhibitor Treatment for Persistent PH after MCS
Study N Design Results
Tedford
2008
138
LVAD
PVR> 3 W u
N=58 : no in PVR 1-2 wks post VAD despite in PAWP
•26 consecutive pts received sildenafil (mean dose 52 mg TID)
•32 controls
Sildenafil Group (12-15 wks post-LVAD):
PVR 5.87 + 1.9 to 2.96+ 0.92*
MPAP 36.5 + 24.3 to 24.3 + 3.6*
• PVR sign. lower in sildenafil rx pts vs control
• Sildenafil resulted in improved RV function (dp/dt; TAPSE) vs control
Tedford et al. Circ Heart Fail 2008; 1:213
*P< .001
In patients with persistent mixed PH after LVAD, sildenafil is a useful adjunctive therapy to PVR and
potentially facilitate heart transplantation
Medical Management Principles in ARHF
Hoeper MH, et al. Am J Respir Crit Care Med.2011;184:1114-1124. (modified)
Identify and Treat Triggering Factor(s)
Reduce RV Afterload: - External (PVR, PAC)
- Internal (Wall Stress)
Optimize Cardiac OutputCVO2 >65%, CI >2.0 l/min/m2
Optimize Perfusion Pressure
Optimize Preload
• Hypervolemia IV diuresis/hemofiltration • Hypovolemia with hypoperfusion (no evidence
for congestion, rare) Administer fluid

11
Reduce RV internal afterload (Wall Stress ≈ P x R/ h)Decompress RV to preload/wall stress MVO2 , CPP, RV ischemia; improve LV filling and systemic CO ; relieve organ congestion
•Avoid volume loading in setting of hypotension or pre-renal azotemia
– No benefit from RV Frank-Starling mechanism
– Dilates RV LV filling CO
•Diuretics
– intermittent or continuous infusion loop diuretics, +/-thiazide, +/-aldosterone antagonists
•Mechanical fluid removal: CVVH/Aquapheresis
De Marco T. Advances PH 2005; 4:16Brown N. Curr Opinion Nephrol Hyperten 2005;14:235
Mebazaa et al. Int Care Med 2004;30:185Haddad et al. Circ 2008;117:1717
Medical Management Principles in ARHF
Hoeper MH, et al. Am J Respir Crit Care Med.2011;184:1114-1124. (modified)
Identify and Treat Triggering Factor(s)
Reduce RV Afterload: - External (PVR, PAC)
- Internal (Wall Stress)
Optimize Cardiac OutputCVO2 >65%, CI >2.0 l/min/m2
• Dobutamine/dopamine (monitor fortachyarrhythmia)
• Milrinone (caveat: systemic hypotension in PAH) favored in PH due to LHD)
Optimize Perfusion Pressure
Optimize Preload
Augment RV contractility• Inotropes
– Dobutamine/dopamine – Other adrenergic agents (NE, epinephrine)– Milrinone in PH due to LHD (Ipc-PH; Cpc-PH)– Addition of IV epoprostenol (PAH)– Combination– Caveat: tachyarrhythmias, hypotension
(HTN concerning esp with milrinone in PAH)
De Marco T. Advances PH 2005: 4:16Montalescot et al. Am J Cardiol 1998;82:749
Mebazaa et al. Int Care Med 2004;30:185Haddad et al. Circ 2008;117:1717
Medical Management Principles in ADRHF
Hoeper MH, et al. Am J Respir Crit Care Med.2011;184:1114-1124. (modified)
Identify and Treat Triggering Factor(s)
Reduce RV Afterload: - External (PVR, PAC)
- Internal (Wall Stress)
Optimize Cardiac OutputCVO2 >65%, CI >2.0 l/min/m2
Optimize Perfusion Pressure
Optimize Preload
•Norepinephrine•Vasopressin

12
Optimize Perfusion Pressure– Systemic vasodilatory state:
Vasopressors norepinephrine vasopressin (PVR/SVR ratio)
– Systemic vasodilatory state + tachycardia Vasopressors vasopressin
phenylephrine (caution PVR)Dysrrhythmias:– usual therapy – avoid β-blockers, CCB in acute RHF
De Marco T. Advances PH 2005: 4:16Montalescot et al. Am J Cardiol 1998;82:749
Mebazaa et al. Int Care Med 2004;30:185Haddad et al. Circ 2008;117:1717
Non- Pharmacologic Treatment ofARHF in PAH
Percutaneous graded blade-balloon atrial septostomywith stent• R L shunt: decompresses failing RV & improves LV filling systemic CO
• Recurrent ARHF, syncope, BTT, no other options
Mechanical support (BTR/BTT)
• ECLS: Traditional ECMO, Artificial lung [PA-LA]
Bilateral lung transplantation
• Viable option: 1 yr survival: 70-90%; 5 yr survival: 50-60%
• Mortality on waiting list remains high (20% yr despite LAS)
• Aggressive pre-transplant management can mortality
Keogh AM, et al. J Am Coll Cardiol 2009;54:S67Chen H, et al. Am J Resp Crit Care Med 2009;180:468
Proposed Algorithm:Treatment of ADRHF in PAH
Identify and treat underlying precipitating factors(Dietary indiscretion, infection, anemia/erythrocytosis, thyroid disorders,
dysrrhythmia, ischemia, PE, NSAID’s, COX-2 I)
Restore oxygenation•Supplemental/ high flow O2
•Avoid mechanical ventilation•Avoid excess PEEP, • Avoid acidosis
Restore vital organ perfusion•Pulmonary vasodilators ( afterload)
•O2/iNO/ prostanoids (IV, Inh.)•Combination therapy
•Inotropes / vasopressors•Adrenergic agents,?PDE-3 Inh.•Add/change to IV epoprostenol
Relieve congestion•IV loop diuretics•IV, oral thiazide diuretic•Oral aldosterone antagonist•Mechanical fluid removal(CVVH or Aquapheresis)
Stabilization achievedTransition to chronic therapy
•Wean NO with epoprostenol•Wean IV inotropes•Optimize chronic therapies•Evaluate for transplantation
Unresponsive/refractoryTransplant Candidates: Bridge to Transplant• Continuous IV inotropes• Atrial Septostomy• ECLS (ECMO, Artificial lung)Not Transplant Candidate• Palliation of symptoms• Hospice Care
De Marco T. Advances PH 2005;4:16Haddad et al. Circ 2008;117:1717
Proposed Algorithm for Management of Cpc-PH due to LHD On optimal, guideline directed therapy for HFrEF
Transplant eligible Not transplant eligible
Vasoreactive Not vasoreactive
Heart transplant
PH resolves or becomes vasoreactive
Persistent PH• Continue HF
Therapy
• DT VAD
•Investigational Trials
•Aggressive chronicpharmacologic rx
(IV inodilators, po PDE5-I)•MCS•Combination rx;trials
Considerheart-lungtransplantation
Acutevasoreactivitytesting
(q 3-6mosRHC)
Adapted from Murali S, Adv in PH 2006;5:33 Mehra et al. J Heart Lung Transplant 2006; 25:1024
(FrequentRHC q 3-6 mos)

13
• ARHF in PH is associated with morbidity and mortality• ARHF is a syndrome with complex pathophysiology
– Characterized by dyspnea, fatigue, edema, syncope, CVP, vital organ congestion +/- hypoperfusion
• Pharmacologic strategies should be aimed at:– Restoring oxygenation– Relieving congestion and hypoperfusion maintaining vital organ perfusion is critical
• Management includes judicious- individualized use of: – Pulmonary vasodilators – Diuretics/ hemofiltration– Inotropes– Vasopressors– Atrial septostomy, mechanical circulatory support (BTT), and
transplantation
Conclusions
Thank you!!