RIGHT HEART ASSESMENT
Is It Important?Not just a conduitConnected and affectedRisk
stratificationTherapy guidanceControversialUnderstudiedExaminers
favorite
The Purposes Of GuidelinesDescribe the acoustic windowsDescribe
the echocardiographic parameters of RV size and function.Advantages
and disadvantages of each measure or technique.Recommend which
right-sided measures should be included in the standard
echocardiographic report.Provide revised reference values
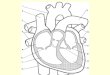
BASIC VIEWS
BASIC VIEWS
BASIC VIEWS
Segmental Nomenclature
Right Heart DimensionsRight ventricle-focused apical 4 chamber
viewMeasured at end-diastole
Which of the following is an abnormal right ventricular (RV)
dimension in an adult 30 years old?A. Basal RV diameter of 2.5
cm.B. Mid RV diameter of 3.8 cm.C. Right ventricular outflow tract
(RVOT) diameterabove the aortic valve of 2.6 cm.D. Base to apex RV
length of 7.5 cm.
Right ventricular dimensions
Basal RV diameterMid cavitary RV diameterRV longitudinal
dimension4.2 cm indicates dilatation3.5 cm indicates dilatation8.6
cm indicates RV enlargement
13
RV size should be routinely assessed by conventional 2DE using
multiple acoustic windowsReport should include both qualitative and
quantitative parameters. In laboratories with experience in 3DE, 3D
measurement of RV volumes is recommended.RV EDVs of 87 mL/m2 in men
and 74 mL/m2 in women RV ESVs of 44 mL/m2 for men and 36 mL/m2 for
women
TAPSETAPSE and RV ejection fraction TAPSE 2cm = RVEF 50% TAPSE
1.5cm = RVEF 40% TAPSE 1cm = RVEF 30% TAPSE 0.5cm = RVEF 20%
Event free survival according to TAPSE in patients with CHF
RV Diastolic FunctionFrom the apical 4-chamber view, the Doppler
beam should be aligned parallel to RV inflowSample volume is placed
at the tips of the tricuspid valve leafletsMeasure at held
end-expiration and/or take the average of 5 consecutive
beatsMeasurements are essentially the same as those used for the
left side
RecommendationMeasurement of RV diastolic function should be
considered in patients with suspected RV impairment as a marker of
early or subtle RV dysfunction, or in patients with known RV
impairment as a marker for poor prognosisTranstricupsid E/A ratio,
E/E ratio, and RA size have been most validated are the preferred
measuresGrading of RV Diastolic Dysfunction should be done as
follows: E/A ratio < 0.8 suggests impaired relaxationE/A ratio
0.8-2.1 with an E/E > 6 or diastolic prominence in the hepatic
veins suggest pseudonormal fillingE/A ratio > 2.1 with
deceleration time < 120 ms suggests restrictive filling
RecommendationsThe recommended parameter to assess RA size is RA
volume, calculated using single-plane area-length or disk summation
techniques in a dedicated apical four-chamber view.The normal
ranges for 2D echocardiographic RA volume are :Males25 7
ml/m2Females21 6 ml/m2
RA PressureMeasurement of the IVC should be obtained at
end-expiration To accurately assess IVC collapse, the change in
diameter of the IVC with a sniff and also with quiet
respiration
RecommendationsFor simplicity and uniformity of reporting,
specific values of RA pressure , rather than ranges, should be used
in the determination of SPAPIVC diameterIVC collapsibilityRA
pressure 2.1 cm> 50% with a sniff3 mmHg > 2.1 cm < 50 %
with a sniff15 mmHgIn indeterminate cases in which IVC diameter and
collapse do not fit this paradigm, an intermediate value of 8 mmHg
may be used, preferably with use of secondary indices of RA
pressures such as: RA dilatation, abnormal bowing of the IAS into
the left atrium throughout the cardiac cycle
AdvantagesDisadvantagesIVC dimensions are usually obtainable
from the subcostal windowIVC collapse does not accurately reflect
RA pressure in ventilator-dependent patientsIt is less reliable for
intermediate values of RA pressure
Which of the following is the correct measurement of the IVC
diameter in estimating RA pressureA. AB. BC. CD. None of the
above
ABC
The end-systolic and end-diastolic parasternal short-axis views
of a 75-year-old patient are shown. Which of the following
statements is more likely to be true?A. This patient likely has
carcinoid heart disease.B. This patient likely has Eisenmenger
physiology.C. There is evidence of a restrictive VSD.D. Pulmonic
stenosis is suspected.E. These images are classic for Ebstein
anomaly
Other RecommendationsVisual assessment of ventricular septal
curvature looking for a D-shaped pattern in systole and diastole
should be used to help in the diagnosis of RV volume an/or pressure
overload
RV pressure overload-septal shift throughout cardiac cycle with
most marked distortion of LV at end systoleRV volume
overload-septal shift occurs predominately in mid to late
diastole
Pulmonary Artery PressuresPASP should be estimated and reported
in all subjects with reliable tricuspid regurgitant jets
Which of the following parameters are used to calculate
Pulmonary artery systolic pressure?A. TR onlyB. TR and PR onlyC. TR
and VSD onlyD. TR, PR, and VSD onlyE. TR, AR, PR, and VSD
What is the PA systolic pressure of the patient with pulmonary
stenosis, where peak TR velocity is 4 m/sec, peak velocity across
pulmonic valve 3 m/sec, and RA pressure 10 mm Hg?A. PA systolic
pressure 46 mm Hg.B. PA systolic pressure 74 mm Hg.C. PA systolic
pressure 38 mm Hg.D. PA systolic pressure 50 mm Hg.
What is the PA systolic pressure of the patient with pulmonary
stenosis, where peak TR velocity is 4 m/sec, peak velocity across
pulmonic valve 3 m/sec, and RA pressure 10 mm Hg?A. PA systolic
pressure 46 mm Hg.B. PA systolic pressure 74 mm Hg.C. PA systolic
pressure 38 mm Hg.D. PA systolic pressure 50 mm Hg.RVSP4 (4)2 +
1064 + 107474 PSPG74 4 (3)274 - 3638PASP = RVSP - PSPG
28-year-old man with liver disease presents with jugular venous
distensions
A. Right ventricular systolic function is markedly diminished.B.
Peak velocity of 2.2 m/sec excludes the diagnosis of pulmonary
HTNC. Tricuspid regurgitation is likely mild.There is right
ventricular midcavitary gradient during systole. Right ventricular
systolic function can not be accurately assessed.
A patient with holosystolic murmur at the left sternal border.
What is RVSP?Blood Pressure150/80 mmHgRA Pressure15 mmHg35 mmHg65
mmHg50 mmHgCan not be calculated
Other Recommendations
1/3 (SPAP) + 2/3 (PADP)1. Mean PA pressure =2. Mean PA pressure
= 79 (0.45 x AT)3. Mean PA pressure = 90 (0.62 x AT)4. Mean PA
pressure = 4 x (early PR vel) + est. RAP
What is the PA diastolic pressure in this patient with dyspnea
on exertion? The IVC is dilated and does not collapse with
sniffing.A. PA diastolic pressure 14 mm Hg.B. PA diastolic pressure
17 mm Hg.C. PA diastolic pressure 28 mm Hg.D. PA diastolic pressure
19 mm Hg.
Pulmonary Vascular Resistance
PVR = TRV max / RVOT TVI x 10 + 0.16 Significant PHTN exists
when PVR is > 3 Wood units
RV dP/dtThe rate of pressure rise in the right
ventricleEstimated from the ascending limb of the tricuspid
regurgitant CW Doppler signal
RV dP/dt < 400 mmHg/s is likely abnormal
Hepatic Vein DopplerThe normal HV waveform has three antegrade
wavesA larger systolic S wave A smaller diastolic D waveA small
retrograde flow reversal from atrial contraction A wave
The following statement is TRUE regarding below given Hepatic
vein Doppler:A. Abnormal interventricular septal motion is due to
right ventricular volume overload.B. Inspiratory increase in
forward hepatic vein flow velocities is abnormal.C. Above M-mode
recordings are diagnostic of a large pericardial effusion and
tamponadeD. Patient has ventricular interdependence.
Which of the following is most compatible with the hepatic
venous flow in Figure below:A. 56-year-old man with systemic
hypertension under control with medical therapy.B. 39-year-old
woman with hypotension in the setting of acute inferior wall MI.C.
25-year-old man with recurrent septic pulmonary embolism.D.
63-year-old man in atrial fibrillation
Thanks for your patience
56