Embed Size (px)
Citation preview

Antibodies or immunoglobulins are the soluble media-tors of immunological resistance to invading pathogens. Millions of years of evolution have fine-tuned the activity of these very specific and effective mediators of host pro-tection. Most importantly, sophisticated effector systems have co-evolved with antibodies and are responsible for their normally protective biological effects. Principal among these effector systems are those induced via the Fc receptors (FcRs)1–3 — a family of cell surface recep-tors that specifically bind to the Fc portion of antibodies (FIG. 1; TABLE 1). By acting as receptors for antigen–anti-body immune complexes, FcRs provide the humoral immune system with a cellular effector arm that con-nects the adaptive and innate immune systems (FIG. 2).
Following the binding of immune complexes, FcRs induce powerful responses that activate, regulate and modulate immunity. Activation of effector cell func-tion after FcR engagement can result in the release of inflammatory mediators or the activation of cell-based responses such as phagocytosis; alternatively, it can result in the destruction of antibody-coated targets by antibody-dependent cell-mediated cytotoxicity (ADCC). These pro-cesses, under normal circumstances, serve to eliminate invading pathogens.
Although the majority of FcR classes (FIG. 1) normally activate cells, immunomodulatory effects are largely
mediated by a single inhibitory receptor — FcγRIIb — that exists in several forms, mostly as variants of the cyto-plasmic tail. Recently, however, it has become apparent that some of the activating FcRs exhibit a paradoxical dualism of function and may also deliver inhibitory signals4–7.
In the context of drug discovery, FcR targeting can be considered from three unrelated perspectives. First, in autoimmunity or other antibody-dependent hyper-sensitivity reactions, the direct blockade of the immu-noglobulin–FcR interaction can block FcR activation and thereby prevent inflammation. Second, these pow-erful FcR-dependent effector systems can be harnessed to direct destructive pro-inflammatory or cell-based responses to unwanted target cells or pathogens. And last, activating or inhibitory receptors can be co-engaged with each other or with adjacent unrelated cell surface molecules to direct and fine-tune cellular responses.
First, the direct blockade of immunoglobulin–FcR interactions may be a useful strategy in certain major autoimmune inflammatory settings. In several clini-cally significant pathological immune-based diseases, autoantibodies and antigens form immune complexes that bind to FcRs and activate the same effector mecha-nisms that normally protect the host. This can lead to extensive tissue damage in diseases such as rheuma-toid arthritis and systemic lupus erythematosus. Drug
1Inflammation, Cancer and Infection Laboratory, Centre for Immunology, Burnet Institute, 85 Commercial Road, Melbourne 3004, Australia.2Department of Pathology, University of Melbourne, Parkville 3052, Melbourne, Australia.3Department of Immunology, Monash University, Clayton 3168, Melbourne, Australia. 4Bio-Organic and Medicinal Chemistry Laboratory, Centre for Immunology, Burnet Institute, 85 Commercial Road, Melbourne 3004, Australia.Correspondence to P.M.H. e-mail: [email protected]:10.1038/nrd2909
Antibody-dependent cell-mediated cytotoxicity(ADCC). A mechanism of killing antibody-coated cells by effector cells (for example, natural killer cells, neutrophils or eosinophils).
Fc receptor-targeted therapies for the treatment of inflammation, cancer and beyondP. Mark Hogarth1,2,3 and Geoffrey A. Pietersz2,3,4
Abstract | The direct or indirect targeting of antibody Fc receptors (FcRs) presents unique opportunities and interesting challenges for the treatment of inflammatory diseases, cancer and infection. Biological responses induced via the Fc portions of antibodies are powerful, complex and unusual, and comprise both activating and inhibitory effects. These properties can be exploited in the engineering of therapeutic monoclonal antibodies to improve their activity in vivo. FcRs have also emerged as key participants in the pathogenesis of several important autoimmune diseases, including systemic lupus erythematosus and rheumatoid arthritis. Therapeutic approaches based on antagonizing FcR function with small molecules or biological drugs such as monoclonal antibodies and recombinant soluble FcR ectodomains have gained momentum. This Review addresses various strategies to manipulate FcR function to overcome immune complex-mediated inflammatory diseases, and considers approaches to improve antibody-based anticancer therapies.
R E V I E W S
NATURE REVIEWS | DRUG DISCOVERY VOLUME 11 | APRIL 2012 | 311
© 2012 Macmillan Publishers Limited. All rights reserved

Small chemical entitiesChemical compounds that are less than 500 Da in size.
Immunoreceptor tyrosine-based activation motif(ITAM). An amino acid sequence (12–14 amino acids long) containing two precisely spaced tyrosine residues that, upon phosphorylation by the SRC family of tyrosine kinases and following receptor aggregation, initiate an intracellular signalling cascade that leads to cell activation. This motif is typically found in small, often dimeric membrane proteins that are non-covalently associated with major immunoreceptors such as Fc receptors and antigen receptors.
Immunoreceptor tyrosine- based inhibition motif(ITIM). An amino acid sequence, distinct from an immunoreceptor tyrosine-based activation motif, that is present within the cytoplasmic tail of some membrane receptors and functions solely in the transduction of inhibitory signals. ITIMs are normally composed of a six-amino-acid sequence containing a tyrosine residue, a hydrophobic residue two amino acids upstream of the tyrosine residue and a leucine residue three amino acids downstream of the tyrosine residue. The inhibitory function of the ITIM is activated by phosphorylation of the tyrosine residue, which is mediated by the SRC family of kinases. This leads to the recruitment and activation of tyrosine and/or lipid phosphatases including SHP (SH2 domain-containing protein tyrosine phosphatase) and SHIP (SH2 domain- containing inositol-5- phosphatase), respectively. The ITIM of the Fc receptor FcγRIIb is the archetypal ITIM.
discovery strategies that aim to intervene in this process include: the development of recombinant soluble recep-tors that intercept immune complexes and prevent their binding to FcRs; or the direct targeting of FcRs using small chemical entities or monoclonal antibodies (mAbs) to block the binding of immune complexes to receptors.
Second, with the rise of mAbs as therapeutic modali-ties, it is clear that FcR function is important for their therapeutic efficacy in several diseases. Thus, the capac-ity to manipulate mAbs leads to the possibility of selec-tively harnessing, or avoiding, either the activating or the immunomodulatory functions of FcRs in different thera-peutic settings. For example, mAbs with engineered Fc regions may selectively bind to activating FcγRs to induce tissue destruction in cancer; alternatively, they may be designed to exploit the inhibitory function of FcγRIIb or the paradoxical inhibitory functions of normally activat-ing FcRs in the prevention or treatment of inflammation.
The third and highly speculative strategy is the modu-lation of cell surface receptors, inducing cell activation, with a therapeutic antibody that specifically targets a cell surface molecule through its antigen-binding fragment (Fab) and simultaneously engages a single FcR via its Fc portion on the same cell. The resulting ‘scorpion-like’ configuration creates a trimolecular complex of one or two target molecules, the activity of which is modulated by a single, co-engaged FcR (see below).
This Review considers the approaches to harness, avoid or intervene in FcR activation using a new genera-tion of therapeutics that are currently in development for the treatment of a variety of diseases. This Review mostly focuses on the classical human FcRs found on leuko-cytes that are related to the immunoglobulin superfam-ily (FIG. 1). Mouse FcRs have been extensively discussed elsewhere in the literature (reviewed in REFS 8,9).
The human leukocyte FcRsHuman leukocytes express three principal FcR fami-lies: namely, FcγR (which binds to immunoglobulin G (IgG)), FcεR (which binds to IgE) and FcαR (which binds to IgA)1,2 (FIG. 1; TABLES 1,2).
FcγRs are the most diverse family of FcRs and include three distinct classes of receptor encoded by six genes: FCGR1A (which encodes FcγRI; also known as CD64), FCGR2A (which encodes FcγRIIa; also known as CD32A), FCGR2B (which encodes FcγRIIb; also known as CD32B), FCGR2C (which encodes FcγRIIc; also known as CD32C), FCGR3A (which encodes FcγRIIIa; also known as CD16A) and FCGR3B (which encodes FcγRIIIb; also known as CD16B). FCGR2C is the product of a crossover between FCGR2A and FCGR2B, which share a high degree of homology. Within the three classes of FcγRs multiple gene splice variants have been described, especially for FCGR2B (TABLES 1,2). With the exception of FcγRIIb, their engagement by immune complexes induces a range of often pro-inflammatory cellular responses (FIG. 2). These receptors signal via the immunoreceptor tyrosine-based activation motif (ITAM). Receptor aggregation by immune complexes activates a signalling cascade via the SRC family of kinases and spleen tyrosine kinase (SYK)10. However, there are differences in how this is achieved. FcγRI and FcγRIIIa do not contain an ITAM but they independently form multisubunit receptor complexes through their non-covalent association with a disulphide-bonded dimer — the ‘common’ FcR γ-chain — in which an ITAM is contained within the intracellular tail of each chain of the dimer.
FcγRIIIa also associates with other signalling mole-cules, such as the T cell surface glycoprotein CD3 ζ-chain (CD3ζ) dimer in natural killer (NK) cells and the FcR β-chain in mast cells. However, FcγRIIa is unique as it contains a non-classical ITAM in its cytoplasmic tail and appears to require organization into a dimeric state as part of the signalling process11–13. Relatively little is known about FcγRIIc but its amino acid sequence suggests that its ectodomains are homologous to the inhibitory FcγRIIb, whereas its cytoplasmic tail is related to FcγRIIa and con-tains an ITAM-like sequence, suggesting that it too is an activating FcR that acts via SRC–SYK signalling pathways.
By contrast, FcγRIIb — a specialized inhibitory FcγR subclass — is a potent negative regulator and contains an immunoreceptor tyrosine-based inhibition motif (ITIM) in
Nature Reviews | Drug Discovery
FcγRI FcεRI FcαRIFcγRIIa FcγRIIb FcγRIIIa FcγRIIIbFcγRIIc
ITAM ITIMCommon FcRγ-chain
β subunit
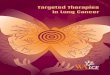
Figure 1 | Diagrammatic representation of the human leukocyte Fc receptors. The Fc receptors (FcRs) consist of an immunoglobulin-binding polypeptide chain containing two immunoglobulin-like domains that form the extracellular region. FcγRI is an exception as it has three such domains, the first two of which are related to those of the other FcγRs and FcεRI, the third domain is unique. FcαR, which also has two extracellular domains, is more closely related to the leukocyte immunoglobulin-like receptors. Signal transduction by the activating FcRs occurs via immunoreceptor tyrosine-based activation motif (ITAM)-dependent mechanisms, usually via a non-covalent association of the immunoglobulin-binding chain with a dimeric, ITAM-containing subunit, typically the ‘common’ FcR γ-chain. In mast cells, FcεRI also associates with a multimembrane-spanning and signal-amplifying β-subunit (the same applies to FcγRIIIa; not shown). FcγRIIa, FcγRIIb and FcγRIIc are unusual as their signalling motifs are contained in the cytoplasmic tail of the ligand-binding chain. This comprises an ITAM for the activating FcγRIIa or FcγRIIc, and an immunoreceptor tyrosine-based inhibition motif (ITIM) for the inhibitory FcγRIIb.
R E V I E W S
312 | APRIL 2012 | VOLUME 11 www.nature.com/reviews/drugdisc
© 2012 Macmillan Publishers Limited. All rights reserved

its intracellular tail. The co-aggregation of this recep-tor with other activating FcRs downregulates activating signals. This capacity to modulate signalling extends beyond FcγRs to include the regulation of FcεRI and FcαRI. Indeed, it also regulates antigen-induced activa-tion of the B cell antigen receptor, and can induce apop-totic signals in activated B lineage cells.
FcεRI and FcαRI are activating FcRs that signal via their non-covalent association with the common FcR γ-chain and, in the case of FcεRI, the FcR β-chain in mast cells. Although FcεRI is closely related to the FcγRs, FcαRI is only distantly related. A second IgE receptor, FcεRII (also known as CD23), which is not structurally related to FcεRI or the FcγRs, has also been identified14.
Another FcR that is expressed on leukocytes, neo-natal FcR (FcRn), is not related to the classical FcRs described above. It interacts with the Fc region of IgG in a location that is distinct from that of the leukocyte FcγRs15. It is structurally related to the major histocom-patibility complex (MHC) class I molecules and can deliver immune complex-bound antigens into the anti-gen presentation pathway16,17. Its major role in humans is the recycling of IgG by non-haemopoietic cells such as endothelial cells, which is crucial for the long serum half-life of IgG1 (REF. 18).
The cell lineage distribution of FcγRs varies con-siderably, as do their affinities and specificities for the different IgG subclasses (FIGS 3,4; TABLE 1). These char-acteristics are defining features of FcγRs and reflect differences in their biological roles. A normal immune response is typically heterogeneous, comprising the production of several IgG subclasses whose concentra-tions change over the course of the immune response. This affects the extent of interactions with different FcγRs, which are engaged at different times during the immune response owing to their different affinities (FIG. 2). Moreover, IgG immune complexes that form dur-ing a natural immune response or after the infusion of therapeutic antibodies will encounter effector cells that simultaneously express different types of FcγRs. These are present, for example, on macrophages, mast cells and neutrophils (TABLE 1). The interactions can be further
modified by the local inflammatory environment, which affects receptor expression and signalling. Thus, the state of effector cells in a local tissue environment and their FcR profile determine the types, strengths and outcome of effector responses19.
Thus, from the drug discovery perspective, strategies that are designed to interfere with or modify FcγR–IgG interactions, as well as a consideration of the fundamen-tal FcR structure, function and biology, are crucial and create interesting and complex challenges.
Cellular expression of FcRs. With the exception of T lymphocytes, all leukocytes and platelets express one or more FcγRs. Moreover, the activation state of the cells and the levels of these receptors change under the influ-ence of various cytokines. For example, γ-interferon and granulocyte–macrophage colony-stimulating fac-tor (GM-CSF) induce changes in the expression of several FcRs.
Thus, strategies that target FcγRs — particularly those that attempt to selectively target only one recep-tor class or subclass — to induce responses such as acti-vation or inhibitory signalling may need to take into account the co-expression of the other FcγRs on effector cells. Indeed, whether they are antibody-coated cancer cells, host tissues or pathogens, IgG immune complexes can simultaneously engage several different FcγRs on one cell. The extent to which this is of practical con-cern for engineered therapeutic antibodies in vivo remains to be determined. However, in principle, IgG immune complexes can simultaneously engage differ-ent subfamilies of activating FcγRs (for example, FcγRI, FcγRIIa and FcγRIIIa), as well as the inhibitory recep-tor FcγRIIb, on cells such as macrophages or mast cells (FIG. 2; TABLE 1). An additional consideration is that the subclasses of IgGs can have different affinities for dif-ferent receptor types. Thus the biological outcome of immune complex binding will depend on several fac-tors, including the type of FcγR expressed and its affin-ity for IgG, the concentration of the different FcγRs on the cell membrane, as well as the activation state of the cells.
Table 1 | Distribution and expression of FcγRs in human leukocytes
FcγRI (CD64) FcγRIIa (CD32A) FcγRIIb (CD32B)‡ FcγRIIc (CD32C) FcγRIIIa (CD16A) FcγRIIIb (CD16B)
T cells No expression No expression No expression No expression No expression No expression
B cells No expression No expression Moderate No expression No expression No expression
Natural killer cells No expression No expression No expression Low# Moderate No expression
Macrophages Low* High Moderate Uncertain Low No expression
Monocytes Low* High Low Uncertain Moderate No expression
Neutrophils Low* High Low§ Uncertain No expression Moderate
Eosinophils Low* Moderate Uncertain No expression No expression Uncertain
Basophils No expression Moderate Moderate No expression No expression Low
Mast cells Low* Moderate¶ Uncertain No expression Uncertain Uncertain
Platelets No expression High No expression No expression No expression No expression
FcγR, Fcγ receptor. *Induced upon exposure to cytokines. ‡Expressed on monocyte subset. §Conflicting reports (see REFS 74,75). ||Exclusive expression on skin-derived cells166. ¶Unstimulated cord blood-derived mast cells167. #Expressed in only 30% of humans.
R E V I E W S
NATURE REVIEWS | DRUG DISCOVERY VOLUME 11 | APRIL 2012 | 313
© 2012 Macmillan Publishers Limited. All rights reserved

Antigen- presentingcell
Nature Reviews | Drug Discovery
Phagocyte
PMN
CD40LMHC-II
CD40TCR
T cell
B cell
Antigenuptake
Antigenreceptoraggregation
Help
Immunecomplex formation
Antibodyproduction
Immune complex uptake:• Phagocytosis• Endocytosis
Antigen
FcγRI FcγRIIa FcγRIIb FcγRIIIa IgG
Mediatorrelease
Mediatorrelease
PlateletNK cell
ADCC
Antigen
Macrophage
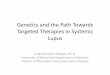
Figure 2 | The role of Fc receptors in normal antibody-based activation of cell responses. Fc receptors (FcRs) provide humoral (antibody-mediated) immunity with a cell-based effector system, as well as a means to regulate cellular responses. This diagram depicts the activation events associated with the binding of immunoglobulin G (IgG) to FcγRs. The interaction of the antibody with a soluble antigen or insoluble targets (such as cells or tissues) results in the formation of immune complexes, which bind to the cell surface of inflammatory leukocytes, resulting in their activation. This, in turn, leads to events such as enhanced presentation of antigens (which are captured as immune complexes, internalized and processed for presentation), the induction of mediator release from FcR-bearing cells (including platelets) as well as antibody-dependent cell-mediated killing of antibody-coated target cells (antibody-dependent cell-mediated cytotoxicity (ADCC)) by natural killer (NK) cells and phagocytosis of target cells by phagocytes such as macrophages or dendritic cells. FcR-dependent activation can be modulated by the engagement of the inhibitory FcγRIIb or through interaction with the C‑type lectin receptor dendritic cell‑specific ICAM3‑grabbing non‑integrin (DC‑SIGN) (not shown). CD40L, CD40 ligand; MHC, major histocompatibility complex; PMN, polymorphonuclear neutrophil; TCR, T cell receptor.
Affinity and specificity of FcRs. The specificity and affinity of the human FcγRs for human IgG classes is well documented, and they are traditionally defined as having a high or low affinity based on the relative differences in their affinity for monomeric IgG (FIG. 3) rather than their avidity for oligomeric immune com-plexes. Historically, different methods have been used to define the affinities of monomeric IgG for its receptors, and an analysis of the literature shows that the absolute values vary considerably, especially for the low-affinity
receptors for which the interaction with monomeric IgG is characterized by very rapid ‘on’ and ‘off ’ rates and is not easily measurable on cells20–22.
Given the challenges in accurately determining the binding affinities of FcγR–IgG interactions, some caution should be exercised in interpreting small dif-ferences in affinity (as reported in the published lit-erature) for IgG binding between different receptor types and different IgG subclasses. The application of surface plasmon resonance has been somewhat helpful
R E V I E W S
314 | APRIL 2012 | VOLUME 11 www.nature.com/reviews/drugdisc
© 2012 Macmillan Publishers Limited. All rights reserved

for measuring the affinities of FcγR–IgG interactions in cell-free systems, but these may not reflect the situation on the cell surface, especially at sites of inflammation19. It should be noted, however, that even though different publications may have generated different values for affinities, the relative differences in affinities are similar in most published cases.
There is also an emerging trend to refer to some receptors or their allelic products as ‘moderate affinity’ receptors, especially FcγRIIIa. For the purposes of this article, we retain the classical terminology as follows. The high-affinity human FcγRI has an affinity in the nanomolar range for IgG1, IgG3 and IgG4, and the bind-ing of monomeric IgG to this receptor is readily detect-able by techniques such as flow cytometry. This affinity is 10–100 times higher than for the low-affinity FcγRII or FcγRIII family of receptors, which interact poorly with monomeric IgG (with an affinity in the micromo-lar range), and the binding of monomeric IgG to these receptors is not readily detectable on cells. However, and most importantly, both high- and low-affinity receptors bind to IgG immune complexes with high avidity, and immune complex binding can be readily detected on the cell surface. It is also important to note that allelic vari-ation, especially in FcγRIIa and FcγRIIIa, considerably affects the affinity and avidity of the interaction with IgG (see below).
Thus, several points can be made. First, within any given FcγR subclass, affinities for different IgG sub-classes may vary in excess of tenfold. For example, the low-affinity FcγRIIa binds IgG4 with a tenfold lower affinity than IgG1 (REFS 20,22). Second, between recep-tor subclasses, substantial differences in the strength
of interaction with one IgG subclass are apparent. For example the binding affinity for monomeric IgG1 is in the nanomolar range for FcγRI, compared to a micro-molar range for FcγRII. Similar observations have been made for the binding of mouse IgG to mouse FcγRs8. Third, genetic polymorphisms of receptors may fur-ther modify these affinities; for example, high- or low-responder forms of FcγRIIa are defined by either Arg131 or His131 residues, respectively. Similarly, FcγRIIIa allelic forms, defined by Val158 or Phe158, also exhibit different affinities for IgG. These polymorphisms are clinically important as they also affect the efficacy of therapeutic antibodies in patients23–25.
With respect to the relative interactions of each IgG subclass with its receptors, several statements can be made: IgG1 and IgG3 bind to all FcγRs; their affinities are in the nanomolar range for FcγRI, and in the submi-cromolar range for FcγRIIb. IgG4 binds to FcγRI with a relatively high affinity, whereas it binds to FcγRII and FcγRIIIa with a low affinity. IgG2 binding is only read-ily detectable to the His131 allelic form of FcγRIIa and weakly to the Val158 allelic form of FcγRIIIa; it appears to have the lowest affinity of all IgG subclasses for FcγRs.
With respect to the relative interactions of each FcγR class with its IgG ligands, FcγRI — whose expression can be induced by GM-CSF and γ-interferon — binds to monomeric IgG1, IgG3 and IgG4 with a high affinity; it does not bind to IgG2. By contrast, the low-affinity receptors FcγRIIa and FcγRIIIa bind to all of the IgG subclasses, and the strength of binding varies consid-erably but is still in the micromolar to submicromolar range20. Of particular interest, for any given IgG class, FcγRIIb is among the receptors with the lowest affinity. This is likely to be biologically significant because dur-ing a normal immune response, as the concentration of immune complexes increases, this inhibitory receptor is likely to be the last FcγR to be engaged. This is perhaps not surprising given that ITIM-driven inhibition is such a powerful inhibitor of ITAM-mediated responses26.
Structural basis of FcR–IgG interactionsThe sites of interaction between FcγRs and IgG are structurally conserved, implying that all FcγRs have similar modes of interaction with different IgG sub-classes11,13,27–32 (FIGS 4–6). Crystallographic structures of liganded FcγRs are available for human IgG1–Fc com-plexed with human FcγRIIIa29,31 or human FcγRIIa11; the structure of FcγRI is known without its ligand33.
IgG interacts in an asymmetrical fashion with FcRs — one FcγR is inserted between the two heavy chains of one IgG (FIGS 4,5), thereby making contacts with both Fc chains.
Mutagenesis studies, in combination with X-ray crys-tallography and homology modelling, have shown that the IgG binding surface of the FcγRs is found largely within the second domain of all FcγRs (FIGS 5,6; TABLE 3). Two tryptophan residues that are found in FcγRIIa at position 87 (or position 90) and position 110 (or posi-tion 113) are conserved in all FcγRs (FIG. 6a–c). Some differences in the sequence numbering of FcγRIIa are apparent in the literature. The most widely used
Rel
ativ
e affi
nity
(log
10)
IgG3
IgG1
IgG4
nm
µm
IgG2
Nature Reviews | Drug Discovery
FcγRI
FcγRIIa-H
131
FcγRIIa-R131
FcγRIIc
FcγRIIIa-V158
FcγRIIIa-F158
FcγRIIb
Human FcγRs
Human Ig
G classes
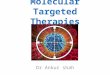
Figure 3 | Graphical representation of the relative differences in affinity among IgG subclasses for human Fcγ receptors. The vertical axis represents the relative differences in affinities of immunoglobulin G (IgG) subclasses for Fcγ receptors (FcγRs) on a log10 scale. See REFS 20–22 and text for details.
R E V I E W S
NATURE REVIEWS | DRUG DISCOVERY VOLUME 11 | APRIL 2012 | 315
© 2012 Macmillan Publishers Limited. All rights reserved

Arthus reactionA type III hypersensitivity reaction of classical antibody (immune complex)-based hypersensitivity, as described by Maurice Arthus.
sequence numbering is based on predictions of the amino terminus from translated cDNA; however, the numbering used by Maxwell et al.13 and Ramsland et al.11 is based on the N-terminal sequence of the recombinant protein, which has an additional three amino acids at the N terminus (Powell et al.22).
Trp87 is part of the linker between the first and second domains of all FcγRs and FceRI, and Trp110 is located
at the boundary between the B strand and the BC loop (FIG. 5). Three additional segments, largely containing resi-dues 110–118 (also known as residues 113–121) (in the BC loop and C strand), residues 125–132 (also known as residues 128–135) (in the C′E loop) and residues 155–158 (also known as residues 158–161) (in the FG loop), pro-vide much of the contact area with IgG13,22 (FIG. 5). Notably, the polymorphisms that affect IgG binding are found in these areas, including the high- or low-responder FcγRIIa polymorphisms in the C′E loop at position 131 (also known as position 134) (FIG. 5; TABLE 3) and the FcγRIIIa V158F polymorphism. The FcγR binding site of IgG (FIG. 4b; TABLE 4) is formed by contacts in both Fc chains. In the lower hinge region of both chains, residues 232–239 (particularly the crucial Leu234-Leu235-Gly236-Gly237 sequence of IgG1) are in contact with the FcR as well as three segments of the Cγ2 domain, which are juxtaposed to the lower hinge region.
For one of the Fc chains of IgG, residues 265–269 can also make contact with the FcγR. These include a crucial aspartate residue that has been substituted in several therapeutic antibodies to ablate FcγR binding. In the same Fc chain, residues 296–300 contain Asn297, which is glycosylated and is crucial for FcR binding. In the second Fc chain, residues 327–333 contain the crucial Pro329 residue that is sandwiched between the two conserved tryptophan residues of the FcγR. The most apparent sequence dif ference between the IgG subclasses, with respect to FcγR binding, occurs in the lower hinge sequences. IgG1 and IgG3 have the Leu234-Leu235-Gly236-Gly237 sequence, and IgG4 is similar (Phe234-Leu234-Gly236-Gly237), whereas the lower hinge of IgG2 (and mouse IgG1) is truncated (TABLE 4). Yet despite this, these IgGs can still interact with some FcγRs. As a rule, the conservation of the lower hinge Leu234-Leu235-Gly236-Gly237 sequence is essential for binding with the highest affinity.
It is noteworthy that the IgE–FcεRI interaction involves structurally equivalent regions to the IgG–FcγR interaction34 (FIG. 6d), whereas the interaction of IgA and FcαRI is entirely distinct35,36. The first domain of FcαRI, not the second, interacts with the Cα2–Cα3 interface of IgA rather than the area adjacent to the hinge region.
Targeting FcRs in inflammationThere is increasing evidence for a major role of FcRs in the induction and maintenance of pathological inflam-matory responses induced by immune complexes, espe-cially autoimmune complexes. In normal immunity, FcR-dependent antibody effector responses are modu-lated by the balance between ‘activating’ and ‘inhibitory’ functions of FcRs but deviation from this fine balance — for example, in some autoimmune diseases — results in reduced control of immune complex-mediated activa-tion of inflammatory cells, which leads to inflammation and tissue damage3,37,38.
A central role for FcγRs in immune complex-based inflammatory processes was suggested by the fact that soluble recombinant human FcRs can block the Arthus reaction39, and was subsequently shown using genetically modified mice in models of inflammation9,37,39–47.
Table 2 | Properties of human leukocyte FcγRs
Receptor Characteristics
FcγRI •Cytokine-inducible (for example, via IFNγ and GM‑CSF), high‑affinity IgG receptor
•Expressed largely on PMNs, macrophages, basophils and mast cells•ITAM-based signalling occurs via association with common FcR γ-chain •Mouse equivalent is FcγRI, which is also a three-domain high-affinity
IgG receptor; however, it displays some differences in cytokine sensitivity and affinity compared with human FcγRI
FcγRIIa •Constitutively expressed low-affinity receptor•Most widespread activating FcR; present on most leukocytes except for
lymphocytes and NK cells; the only FcγR subtype that is expressed on platelets
•Signalling via ITAM in its cytoplasmic tail; note that a functional association with the common FcR γ-chain has occasionally been reported
•Allelic products called ‘high responder’ or ‘low responder’ are associated with susceptibility to autoimmunity, infection and the in vivo efficiency of therapeutic mAbs
•No mouse homologue
FcγRIIb •Inhibitory, low-affinity FcR; co-engagement with ITAM-based receptors modulates their activation; several splice variants of the cytoplasmic tail are known that affect the association of the receptor with the cell cytoskeleton
•Inhibitory signal propagated via ITIM usually requires co-engagement with an ITAM-containing activating receptor target
•Polymorphisms affect receptor expression and have been correlated with malarial resistance or susceptibility to lupus (REF. 59)
•On B lymphocytes, it is the only subtype of FcγR expressed; there is a mouse homologue of FcγRIIb that shows similar inhibitory activity but some differences in the number of splice variants
FcγRIIc •Least characterized FcγR; expressed in only 30% of humans•The extracellular region is homologous to FcγRIIb but its cytoplasmic
tail is homologous to FcγRIIa, including the presence of an ITAM•mRNA expressed in NK cell subset but not lymphocytes; other cell
types uncertain •No defining mAb•No mouse homologue
FcγRIIIa •Low‑affinity activating IgG receptor•The principal IgG receptor of NK cells, and is substantially upregulated
on monocytes and macrophages after stimulation •ITAM-based signalling occurs via the ‘common’ FcR γ-chain or the CD3
ζ-chain•Polymorphisms affect IgG binding and affinity, as well as the efficiency
of therapeutic mAbs in patients•Structurally related to mouse FcγRIII and mouse FcγRIV; however, there
are differences in cell lineage distribution and function in mouse FcγRIII compared with human FcγRIIIa
FcγRIIIb •Unusual low-affinity activating receptor•Attached to cell membrane via GPI anchor•Expression restricted to neutrophils, basophils and possibly eosinophils•Signal transduction possibly involves FcγRIIa?•No mouse homologue
CD3, T cell surface glycoprotein CD3; FcγR, Fcγ receptor; GM‑CSF, granulocyte–macrophage colony‑stimulating factor; GPI, glycosyl phosphatidylinositol; IFNγ, interferon-γ; IgG, immunoglobulin G; ITAM, immunoreceptor tyrosine‑based activation motif; ITIM, immunoreceptor tyrosine-based inhibition motif; mAb, monoclonal antibody; NK, natural killer; PMN, polymorphonuclear neutrophil.
R E V I E W S
316 | APRIL 2012 | VOLUME 11 www.nature.com/reviews/drugdisc
© 2012 Macmillan Publishers Limited. All rights reserved

Despite some differences between mouse and human FcγR cell distribution and orthologues (BOX 1), FcγR-deficient mice or transgenic mice (expressing human FcγRs) have been highly informative. It was established that activating FcγRs, especially FcγRIIIa and FcγRIV (there is no equivalent of FcγRIV in humans), are impor-tant in driving antibody-induced inflammation and are associated with the development or chronicity of inflam-mation in disease models such as collagen-induced arthritis, antibody-induced arthritis, immune anaemia and immune complex glomerulonephritis9,37,41–43,48–56. Their involvement is related to the subclass of IgG invoked or used in the model, especially in passive anti-body transfer models.
Conversely, the ablation of mouse FcγRIIb increases susceptibility to collagen-induced arthritis40 and to many other antibody-dependent autoimmune syndromes38,57–59 owing to a lack of modulation of activating FcR function and alteration of B cell development, or lack of regu-lation of antigen receptor signalling. Transgenic mice expressing human FcγRIIa, which is the most abundant and prevalent activating FcγR in humans, are highly susceptible to tissue damage by pathological antibod-ies in immune complexes, implicating FcγRIIa as a central mediator of inflammation in humans41,46,53,60,61. Furthermore, it has been suggested that FcγRIIa rather than FcγRIIIa has a role in the perpetuation of immuno-logical processes such as the uptake of antibody-coated chromatin in patients with lupus62.
In these animal models, and presumably in patients, immune complex binding to FcγR activates inflamma-tory cells, resulting in mediator release and/or direct tis-sue damage9,46,63,64. Further analysis of the unique human FcγRIIa and FcγRIIIb in transgenic mice showed that
these receptors have distinct roles in aspects of immune complex-induced destruction46. Human FcRs can also have a role in the perpetuation of aberrant immunity via the uptake of antigens contained in immune complexes for subsequent antigen presentation. This has been pro-posed to lead to the exacerbation of autoimmune stimu-lation in diseases such as systemic lupus erythematosus and ulcerative colitis62,63.
Several studies have reported the importance of acti-vating FcγRs in patients with rheumatoid arthritis. In a subgroup of patients with rheumatoid arthritis who had varying levels of anti-collagen II antibodies, it was shown that in vitro stimulation of their blood mono-cytes with solid-phase immune complexes induced the release of the pro-inflammatory cytokines tumour necrosis factor a (TNFa), interleukin-1β (IL-1β) and IL-8. This response was inhibited by blocking FcγRIIa44. Furthermore, in patients who tested positive for rheu-matoid factor, immune complexes from synovial fluid stimulated monocytes and/or macrophages to produce TNFa — a response that was blocked by the binding of mAbs to FcγRIIa but not to FcγRIII44.
Thus, FcγRs are potential targets for the treatment of inflammation involving pathogenic antibodies. With increasing knowledge of the selectivity, function and cellular distribution of the activating and inhibitory receptors, several potential therapeutic strategies may be considered.
Receptor blockade using soluble FcRs as ‘decoy’ competi-tors in vivo. In situations of immune complex-driven inflammation, treatment strategies targeting FcγRs by direct blockade using mAbs or small molecules have shown promising results in animal studies. An alternative
Nature Reviews | Drug Discovery
b IgGa FcγR c IgG–FcγR complexH chain
Fab
L chain
Fc
Domain 1
Domain 2
Figure 4 | Generalized view of the interaction between IgG and an FcγR. The α-carbon skeletons are shown of the extracellular domains of the Fcγ receptor FcγRIIa (part a), of immunoglobulin G (IgG) (part b), and the complex of both (part c). In part a, the surfaces of FcγR that interact with IgG are shown in red. In part b, the surfaces of the lower hinge region and the Cγ2 domain of IgG interacting with an FcγR are shown in purple and orange. In part c, the interaction shown is similar in FcγRIIa, FcγRIIb, FcγRIIc, FcγRIIIa and FcγRIIIb (see also FIGS 5,6). It is likely that the interaction of FcγRI with IgG is very similar, and involves only the first two domains, whereas the third domain supports the first two but does not interact with IgG. Modelling of the interaction was based on the liganded and unliganded X‑ray structures of FcγRIIa (Maxwell et al.13; Protein Data Bank (PDB) ID code: 1FCG), FcγRIIb (Sondermann et al.164; PDB ID code: 2FCB), FcγRIII (Sondermann et al.31 and Radaev et al.29; PDB ID code: 1E4K), FcγRI (Lu et al.33; PDB code: 3RJD) and IgG. The location of these interactions was represented by mouse IgG2a (Harris et al.165; PDB ID code: 1IGT), which is one of the few intact IgG structures known.
R E V I E W S
NATURE REVIEWS | DRUG DISCOVERY VOLUME 11 | APRIL 2012 | 317
© 2012 Macmillan Publishers Limited. All rights reserved

approach has been the targeting of the immune complex rather than FcRs by engineering recombinant soluble FcgRs as ‘decoys’ that prevent binding to surface-bound FcγRs39,65–70 (FIG. 7).
Part of the appeal of this approach is that several FcγRs bind to more than one IgG subclass (FIG. 3) and therefore soluble forms of their ectodomains have the potential to act as universal inhibitors of immune com-plex binding to cells (FIG. 7). Recombinant ectodomains of FcγRI, FcγRII and FcγRIII have all been shown to inhibit inflammation caused by immune complexes in animal models39,65–70, despite the high levels of circulat-ing, competing monomeric IgG (usually about 10–16 g per l) and the considerable variation in affinities for IgG.
A possible further constraint to the use of soluble FcγRs is their relatively small molecular size (approxi-mately 20 kDa for FcγRII and FcγRIII, and 45 kDa for FcγRI), which poses challenges for their formulation as drugs (in terms of pharmacokinetics, such as rapid renal excretion), and it might be difficult to achieve soluble FcγR concentrations that are high enough to be effec-tive. Despite these theoretical considerations, the animal models clearly indicate that soluble receptors can inhibit inflammation in vivo and cell activation in vitro39,65–68.
It appears that the intrinsic affinity of FcRs for the Fc portion of un-complexed monomeric immunoglobulin or immunoglobulin in an immune complex is identical. Thus, for soluble monovalent FcγR ectodomains to act as an effective blocker of immune complex binding to surface FcγRs, high local concentrations of the mono-valent soluble receptor may be required at the site of inflammation.
One strategy to achieve greater retention of recombi-nant soluble FcRs at the site of inflammation may be the oligomerization of soluble, low-affinity receptors. These would retain their inherent low-affinity interaction for IgG but their oligovalency may impart high-avidity inter-actions with oligovalent immune complexes, in the circu-lation as well as at sites of immune complex formation and
deposition in tissues. Thus, although the affinity would be unchanged, the avidity of the multimeric FcγRs for the oligomeric immune complex would be much greater than that of monomeric soluble FcγRs. This strategy could, in principle, confer selective binding in local immune com-plex-rich environments, where small intermolecular dis-tances between the Fc regions of the oligomeric immune complex allow the multimerized oligovalent FcγR protein to effectively remain ‘captured’ by the immune complex. Furthermore, the increased size of the receptor complex as a result of oligomerization may confer more desirable pharmacokinetic properties to the soluble receptor prepa-ration, such as reduced renal excretion.
Recombinant soluble ectodomains of the high affinity receptor FcγRI would normally be expected to be rap-idly and fully occupied by circulating IgG. Surprisingly however, in vivo experiments in mice showed that soluble FcγRI is effective at ameliorating inflammation in anti-body-dependent models of tissue destruction, includ-ing collagen-induced arthritis — the well-characterized model for destructive autoimmune arthritis66,67. However, ‘on’ and ‘off ’ rates of monomeric IgG are sufficiently rapid to allow FcγRI to interact with high concentrations of oligomeric immune complexes in tissues, which may retain the soluble FcγRI in the local setting for a suffi-cient period of time to effectively inhibit inflammatory cell activation via surface FcRs20.
As the recombinant soluble FcγRs can bind to mul-tiple IgG subclasses, there is little selective blockade of individual FcγR subtypes. This is not the case with ligand-blocking mAbs that are directed at specific acti-vating or inhibitory receptors.
Receptor blockade with anti-receptor mAbs. The most direct approach for inhibiting or modulating specific FcRs is the use of mAbs (or small chemical entities; see below) that are directed against the IgG binding site of an individual receptor class, thereby blocking immune complex binding and subsequent cell activation.
FG loop
C′E loop
C′E loop
C′E loop
BC loop
Domain 1
N terminus
C terminusC terminus N terminus
Domain 2
Domain 2
Domain 2Domain 1
Domain 1TrpTrp Trp
Trp
TrpTrp
BC loop
BC loop
FG loop
FG loop
Nature Reviews | Drug Discovery
Figure 5 | Three views of the IgG binding site of FcγR, which is significantly conserved in other FcγRs. The perspectives shown are of two ectodomains of the Fcγ receptor FcγRIIa viewed from the side (part a), the top (part b) and diametrically opposite to the orientation in part a (part c). The elements contributing to the interaction with immunoglobulin G (IgG) are the two tryptophan residues that form the Trp sandwich (shown in red), the BC loop (shown in purple), the C′E loop or strand (shown in dark blue) and the FG loop (shown in light blue). Not all residues are in direct contact with IgG. The amino (N) and carboxyl (C) termini are also shown; see text for details.
R E V I E W S
318 | APRIL 2012 | VOLUME 11 www.nature.com/reviews/drugdisc
© 2012 Macmillan Publishers Limited. All rights reserved

Protein AAn immunoglobulin G binding protein of Staphylococcus aureus that is useful in the purification of immunoglobulin.
Phage displayThe expression of recombinant proteins by a bacteriophage typically displayed on the phage coat. The technology is usually used for the discovery and generation of antigen-combining sites of antibodies but also used for the display of peptide- and/or protein-based ligands.
Indeed, mouse anti-human FcγR antibodies have been developed to block ligand binding of each of the FcR classes39,71–75. Yet despite clear evidence for the role of immune complexes in autoimmune inflammation, the development of anti-FcγR mAbs for the treatment of human diseases has been slow. Remarkably, the first anti-FcR antibody was tested in primates and humans more than 20 years ago76,77.
The mouse mAb 3G8 targets human FcγRIII and has been used in primates to block the clearance of anti-body-coated cells, as well as in patients with immune thrombocytopaenia (ITP)76,77. This is an autoimmune condition in which circulating immune particulate complexes — that is, antibody-coated platelets — are removed and destroyed by tissue macrophages in an FcR-dependent fashion78. 3G8 successfully prevented platelet loss in clinical trials for ITP77. Intriguingly, in the primate study 3G8 prevented the depletion of antibody-coated cells but not of soluble immune complexes78.
The high-affinity FcγRI has also been tested in clinical trials for ITP. mAb197, which blocks IgG binding, did not improve platelet numbers but it did modulate the levels of FcγRI with limited therapeutic benefit79. A humanized antibody, H22, which binds outside the IgG binding site of FcγRI, was also shown to modulate FcγRI levels in vivo80. However, its effectiveness in ITP was not investigated.
Although the role of FcγRIIIa in human ITP is appar-ent, this is less so in other more complex autoimmune diseases such as rheumatoid arthritis or systemic lupus erythematosus. This underscores the challenges of selecting the ‘right’ FcR for targeting. As indicated above, major classes of leukocytes express several activating FcRs at any given time. Indeed, it is not clear whether one or more FcRs is involved in the development of a particular disease or tissue pathology in humans or whether there is a hierarchy of importance of the differ-ent FcRs in the induction of inflammation.
Whether the different FcRs work independently, cooperatively or competitively, and whether one domi-nates over the other in human inflammation, remains to be determined. It is likely that in humans, as in mice, the relationship between activating and inhibitory receptors is an important determinant in antibody-driven inflam-mation. This is supported by genetic studies, in humans, of FcγRIIb59,81–83, FcγRIIa63,84–86 and FcγRIIIa63,84–88.
Small-molecule approaches targeting FcRsThere have also been several reports of small molecules that have been designed to mimic and/or inhibit Fc–FcγR interactions, with obvious challenges posed by the large surfaces involved in these interactions11,29,31 (FIG. 4).
Peptides and peptidomimetics. Peptides that bind to either the FcγR or the Fc region of antibodies have been synthesized or obtained by phage display techniques. These peptides can inhibit the Fc–FcR interaction by mimicking the immunoglobulin sequences of the Fc region, interacting with the FcR, or by mimicking the shape of the receptor. This strategy was also used in the design of peptides that inhibit the binding of IgE to FcεR for the possible treatment of allergies89–91.
Early studies used peptide sequences based on the Cγ2 or Cγ3 domains of IgG heavy chains to design peptides as potential inhibitors of IgG Fc–FcγR interactions. Among others, the peptide Tyr407-Arg416 of the Cγ3 domain of IgG was found to inhibit the binding of IgG to mouse macrophages and human monocytes92–94. Subsequent X-ray crystallographic structures of the IgG-liganded and unliganded FcγR11,13,30,31 showed that these residues are located at a considerable distance from the known IgG–FcγR binding surface, which involves the lower hinge region and the adjacent residues in Cγ2 (FIG. 4). Thus, the inhibition cannot be mediated by direct competition with immune complex binding, which implies that an unknown secondary effect is responsible for inhibition of function, such as interference with receptor clustering via Fc–Fc interactions once IgG is bound to the receptor. More recently, knowledge of the structure of the IgG1 Fc–FcγRIII crystallographic complex has been used to devise a disulphide-linked hinge peptide that binds specifically to FcγRIII, albeit at a 20-fold lower affinity than IgG30.
In another study, a solid-phase cyclic peptide library was constructed with two identical peptides that were linked by disulphide bonds at the N-terminal cysteine and C-terminal cysteine linked to the ε- and α-amino groups of a common Lys–Gly dipeptide. Using IgG as the target, a peptide (Cys-Phe-His-His) from this library was identified that bound to the Fc and Fab region of all immunoglobulins except for the Fc region of mouse IgG1 (REF. 95). Interestingly, the dimeric peptide mim-ics the two loops of the second domain of FcγRIII (Phe130-His132 and His116-Lys117) that make contact with the lower hinge region of the antibody Fc region (Leu234-Leu235-Gly236-Gly237-Pro238-Ser239). In another study, peptides with the consensus sequence CLRSGXGC (where X represents any amino acid) were found to bind to FcγRI and trigger endocytosis96.
Although unrelated to interactions with the leuko-cyte FcR, peptides have been isolated that target the staphylococcal binding site of IgG: that is, the Cγ2–Cγ3 interface in the Fc region. Two 20-residue cyclic peptides that bound to immobilized Fc and competed with the binding of protein A were isolated by screening a phage display library97. Further optimization of the peptides by random mutagenesis yielded a 13-amino-acid peptide (Fc-III; DCAWHLGELVWCT) with a binding affin-ity that was twofold lower than that of protein A and protein G. This peptide was chemically linked to an N-alkyl-3β-amino-5α-cholestane to act as a membrane anchor, and it generated a synthetic FcR with the capac-ity to induce the internalization of IgG on human cells98.
Immunoglobulin mimetics. A family of cyclic peptides with the consensus sequence TXXCXXθPXLLGCϕXE (θ, ϕ and X represent hydrophobic, acidic and any amino acid residues, respectively), binding specifically to FcγRI, was isolated by screening a cyclic peptide phage library and eluting peptides with an affinity for FcγRI using an IgG1 antibody99. The peptides, when arrayed on beads to generate oligovalent complexes, were capable of induc-ing the generation of reactive oxygen intermediates and triggering phagocytosis in myeloid cells.
R E V I E W S
NATURE REVIEWS | DRUG DISCOVERY VOLUME 11 | APRIL 2012 | 319
© 2012 Macmillan Publishers Limited. All rights reserved

IVIgIntravenous immunoglobulin. A therapeutic modality involving treatment with pooled immunoglobulins derived from thousands of ostensibly healthy donors.
More recently, the 11-mer peptide WAWVWLTETAV, which was isolated from a linear peptide phage library selecting for binding to recombinant FcγRIIa, was shown to bind preferentially to FcγRIIa with an affinity of 0.5 μM. There was little binding to FcγRIIb and no binding to FcγRI and FcγRIIIb100. The peptide bound equally to both of the allelic variants of FcγRIIa (high-responder Arg131 (also known as Arg134) and low-responder His131 (also known as His134); see explanation above for differences in sequence numbering), and mutational analysis of FcγRIIa indicated that Trp87, Trp110 and Phe160 were essential to the interaction of the peptide. Interestingly, Trp87 and Trp110 residues are conserved in all FcγRs and are crucial contacts in their interaction with IgG, but the Phe160 residue — which abuts Trp87 — is replaced by Tyr160 in FcγRIIb and FcγRI, and by Val160 in FcγRIIIb, implying that the preferential binding of the peptide to FcγRIIa is determined by the Phe160 residue.
In separate studies, a low-affinity binding pep-tide (CWPGWDLNC) that was capable of inhibit-ing IgG–FcγRIIa binding was isolated from a cyclic peptide library101. Nuclear magnetic resonance and modelling studies indicated that the peptide inter-acted with Trp87 (also known as Trp90) and Trp110 (also known as Trp113) of FcγRIIa. These synthetic mimics may ultimately have utility in the treatment of autoimmune disease.
Small chemical entities. Small molecules have been designed based on the structure of FcγRIIa, and have been shown to prevent immune complex-triggered inflammation102. X-ray crystallographic analysis of FcγRIIa indicates that it can exist in two dimeric states11,13. In one state13,102, a groove is formed by recep-tor dimerization that is flanked by the regions involved in the binding of the Fc region of immune complexes. Computational methods were used to design several small molecules that interact with residues Phe129 (also known as Phe132) and Lys117 (also known as Lys120) in the groove102. These compounds selectively inhibit the FcγRIIa-dependent activation and aggrega-tion of human platelets by immune complexes in vitro and, importantly, were effective in vivo in FcγRIIa-transgenic mice in a model of collagen-induced arthri-tis. This model is one of the most widely used models of autoimmune destructive arthritis, and has several features in common with human rheumatoid arthritis, including cellular infiltration of the joints with cartilage and bone destruction103.
An alternative approach to the blockade of the interaction between FcγRs and immune complexes is the inhibition of the signalling pathways of activating receptors104. SYK is essential for ITAM-dependent signal transduction of activating FcγRs as well as other multi-subunit immunoreceptors such as the B cell receptor, NK receptors, and several myeloid and platelet receptors. An orally bioavailable small chemical entity (R406) that tar-gets SYK was shown to be effective at reducing immune complex-mediated inflammation in the reverse-passive Arthus reaction (a model of immune complex inflamma-tion) and models of antibody-induced arthritis104. R406 inhibited SYK at concentrations that were 5–100-fold lower than for other kinase targets, and no adverse effects were noted in humans. Recently, a prodrug of R406 — R788 — that was shown to be active in a mouse model of ITP was used in a Phase II clinical trial involv-ing 16 patients with refractory ITP105. Platelet counts were maintained in 50% of patients, without recourse to alternative therapy, and 75% of patients achieved a clinical response. The effect of the drug appears to be directed at the SYK-dependent FcγR-mediated phago-cytosis of antibody-coated platelets in the spleen.
Intravenous immunoglobulinFcRs could be viewed as one of the oldest drug targets in the immune system. The intravenous administration of pooled human immunoglobulin (IVIg) was originally developed to provide passive protection for patients with an immunodeficiency but is now increasingly used in the treatment of diseases mediated by autoantibodies or immune complexes106. Despite its clinical success, the mode of action of IVIg is still unclear and is hotly debated. It is clear, however, that its therapeutic effects involve various mechanisms that involve the Fab107,108 and/or Fc region of the immunoglobulin55, which may work independently or jointly. The effects may, in some cases, be disease-specific109 or they may be more general, including inhibition of cytokine production or suppres-sion of B cell responses110,111.
Domain 1
FcγRI FcγRIIa
FcγRIIIa FcεRI
Domain 2
Domain 3
Domain 2 Domain 2
Domain 2
Domain 1 Domain 1
Domain 1
Nature Reviews | Drug DiscoveryFigure 6 | Comparison of the ectodomains of the immunoglobulin superfamily leukocyte Fc receptors. The immunoglobulin-interactive regions are shown for the immunoglobulin G (IgG) Fcγ receptors FcγRI, FcγRIIa and FcγRIIIa, as well as the IgE receptor FcεRI. The IgG‑interactive regions — the tryptophan residues as well as the BC, C′E and FG loops — are coloured as in FIG. 5.
R E V I E W S
320 | APRIL 2012 | VOLUME 11 www.nature.com/reviews/drugdisc
© 2012 Macmillan Publishers Limited. All rights reserved

Inhibitory ITAM(ITAMi). Tyrosine phosphorylation of the immunoreceptor tyrosine-based activation motif (ITAM) activates negative feedback as well as stimulatory signalling pathways. Under certain circumstances, especially when receptors are stimulated by low-avidity ligands, signalling is biased towards inhibition. This inhibitory bias is associated with monotyrosyl phosphorylation of the ITAM and the recruitment of phosphotyrosine and phosphoinositide phosphatases, which act as effectors.
Early clinical studies using enzymatically generated Fc portions that had therapeutic effects in paediatric patients with ITP provided a clear indication that the Fc part of IgGs in IVIg is responsible for a therapeutic effect. The success of IVIg as an anti-inflammatory agent has considerable implications for FcR-targeted drug devel-opment. Indeed, a significant component of the mode of action of IVIg in the treatment of inflammatory con-ditions appears to be mediated through Fc-dependent mechanisms, including the involvement of FcRs.
Recently, two mechanisms of IVIg action have been suggested, based mostly on observations in mouse stud-ies. These show that FcγRIIb has a central role in the anti-inflammatory effects of IVIg but is not necessarily in direct contact with IVIg.
Lazarus and colleagues111,113, using adoptive trans-fer of ex vivo IVIg-treated dendritic cells and a plate-let depletion model, suggest that IVIg directly engages activating FcγRs on dendritic cells. When these cells are transferred to recipient mice they affect FcγRIIb expres-sion on another cell type, presumably inflammatory macrophages, by an unknown mechanism.
Ravetch and colleagues55 also suggest a two-cell model. However, they suggest that the relatively rare, naturally sialylated IgG in IVIg binds to the lectin SIGN-R1 (known as DC-SIGN (dendritic cell-specific ICAM3-grabbing non-integrin) in humans), inducing a soluble factor that upregulates FcγRIIb expression on other cell types. Human IVIg enriched for a sialylated antibody had a tenfold higher potency in attenuat-ing immune complex arthritis and/or protecting mice from arthritis114. Moreover, sialylated Fc can bind to macrophages and dendritic cells (expressing human DC-SIGN), leading to the production of IL-33, which in turn leads to IL-4+ basophil expansion. IL-4 can upregu-late FcγRIIb, leading to the attenuation of autoantibody-mediated inflammation115.
Sialylated mouse antibody binds less effectively to activating FcγRs, and it was shown to be less destructive in in vivo platelet clearance models. These observations point to a possible practical application of the direct
modification of the sialylation status of the Fc region of IgG as a possible low-cost solution for exploiting the IgG Fc region as a potent anti-inflammatory entity.
The reasons for the differences between the studies of Lazarus and colleagues111,113, which show the need for activating FcRs, and Ravetch and colleagues55, which show a requirement for lectin binding by a sialylated antibody, are not clear and could reflect differences in the models used. But it is conceivable that both mecha-nisms act in vivo. Certainly, the observation that the glycosylation state of IgG influences the pro- or anti-inflammatory nature of IgG is consistent with the clini-cal observation that decreased levels of sialylation and galactosylation of IgG are seen in patients with inflam-matory autoimmune diseases such as rheumatoid arthri-tis and vasculitis116–118.
Equally, it should be noted that the somewhat coun-terintuitive requirement for the engagement of an acti-vating FcR to mediate inhibition may be consistent with the recently described inhibitory ITAM activity (ITAMi; see later section).
Modifications of the immunoglobulin FcThe pioneering clinical use of mAbs has demonstrated their enormous potential as therapeutics for cancer, infectious diseases and inflammatory diseases; almost 200 antibodies have reached clinical trials or the approval stage. The therapeutic mechanisms of action of antibodies can involve the simple neutralization of receptor or cytokine function, but — as demonstrated for the CD20-specific mAb rituximab (Rituxan; Biogen Idec/Genentech/Roche) — they can also induce FcR-dependent responses119–121.
FcR-dependent responses include ‘active’ FcR- dependent effector cell responses such as antibody- dependent phagocytosis or the induction of ADCC. However, there are also more ‘passive’ mechanisms that may not induce an effector cell response but are FcR-dependent. This includes the simple crosslinking of anti-bodies that are attached to a target cell by FcR-expressing effector cells. In such a case, the FcR of the effector cell
Table 3 | Comparison of the regions of FcγR involved in the binding of IgG*
Receptor D1–D2 linker (residues 86–87)
BC loop (residues 110–118)
C′E loop (residues 125–132)
FG loop (residues 155–158)
Human FcγRI GW WKDKLVYNV KAFKFFHW MGKH
Mouse FcγRI DW WKNKLVYNV KSFQF-SS‡ TGRH
Human FcγRIIa EW WKDKPLVKV KSQKFSRL§ IGYT
Human FcγRIIb EW WKDKPLVKV KSKKFSRS IGYT
Mouse FcγRIIb DW WRNKLLNRI KSVRYHHY LGRT
Human FcγRIIIa GW WKHTALHKV KDRKYFHH VGSK§
Mouse FcγRIII DW WRNKLLNRI KSVRYHHY LGST
FcγR, Fcγ receptor; IgG, immunoglobulin G. *Regions involved in interaction with IgG are defined from crystallographic structures of human FcγRIIIa and the Fc of IgG1 (REFS 29,31) as well as human FcγRIIa and the Fc of IgG1 (REF. 11); not all residues are in contact with IgG — flanking residues are also included above. In addition, interactive sites for the other human and mouse FcRs are inferred from mutagenesis studies and by homology with the contact areas from the solved crystallographic structures. The sequence numbering, in parentheses, is based on that of FcγRIIa; the numbering of the equivalent residues in other FcγRs may vary. ‡The dash indicates that an equivalent amino acid is missing in that position. §The amino acid polymorphisms H131 of FcγRIIa or V158 of FcγRIIIa are involved in altered affinity for IgG subclasses.
R E V I E W S
NATURE REVIEWS | DRUG DISCOVERY VOLUME 11 | APRIL 2012 | 321
© 2012 Macmillan Publishers Limited. All rights reserved

OrthologuesGenes of different species that originated from a common ancestor.
simply provides a multivalent array that leads to anti-body-dependent aggregation of the target molecule on the target cell. A recent example of this passive crosslink-ing in mice is the immunostimulatory effect of agonistic anti-CD40 antibodies that target immune cells rather than the cancer cell168. Although any FcR-expressing cell induced activation of target cells coated with the anti-CD40 antibody in vitro, the effect was entirely dependent on the presence of FcγRIIb in vivo, suggest-ing something unique about the anatomical location of FcγRIIb-expressing cells in relation to CD40-expressing immune cells. Similarly, it has been shown that passive FcR crosslinking of an appropriately chosen antibody targeted to cancer cells could potentially induce death pathways169.
The clinical benefit of engaging FcRs by therapeu-tic antibodies can be inferred from the correlation of a better clinical outcome with FcR polymorphisms that are associated with increased IgG binding and stronger induction of effector functions.
Studies in neuroblastoma, using a mouse IgG3 anti-body (3F8) against ganglioside D2 (GD2) in combination with GM-CSF to improve phagocytosis or antibody-dependent killing, indicated that disease-free survival correlated with FcγRIIa high-responder (FcγRIIa-R131) homozygosity122–124. This was also shown in antitumour vaccine studies, in which the clinical outcome was heav-ily influenced by FcR polymorphisms, especially FcγRIII polymorphisms such as FcγRIIIa-V158 (REF. 124).
One of the best characterized anticancer antibodies, rituximab, is used for the treatment of non-Hodgkin’s lymphoma and is also in advanced clinical trials for the treatment of rheumatoid arthritis and other autoim-mune conditions120. Disease-free survival and clinical outcomes in patients with cancer who are treated with rituximab depend on the induction of effector func-tions, and outcomes correlate with FcγR polymor-phisms that are known to increase the strength of IgG binding119,121. Positive outcomes also correlate with the homozygosity of FcγRIIIa-V158 and FcγRIIa-H131,
which implies that ADCC by NK cells via FcγRIIIa- and other FcγRIIa- or FcγRIIIa-dependent func-tions of other effector cells such as macrophages have important roles in the therapeutic effect of the antibody. By contrast, polymorphisms of FcγRIIa and FcγRIIIa do not predict response rates in patients with chronic lymphocytic leukaemia who are treated with rituximab or alemtuzumab (Campath-1H; Genzyme), further implying that other in vivo as yet unknown fac-tors influence effectiveness125,126.
Despite the substantial differences between the biol-ogy of mouse and human FcRs, including the absence of orthologues of human FcγRIIa, FcγRIIc or FcγRIIIb in mice, mouse models have revealed some interesting data in a study of B cell depletion by anti-CD20 treatment. In mice, as in humans, FcγRIII was found to be essen-tial for ADCC-based elimination of cells by rituximab and by an unrelated CD20-specific mAb, ofatumumab (Arzerra; Genmab/GlaxoSmithKline)127. However, it is clear that other factors also influence the induction of ADCC in vivo. CD20-specific antibodies of the differ-ent mouse IgG subclasses engaged different activating receptors but still depleted B cells. For example, mouse IgG1 depleted B cells via FcγRIII, whereas mouse IgG2a and/or IgG2c and mouse IgG2b acted via FcγRI and/or FcγRIV, respectively128. However, a most interesting observation was that the expression of the inhibitory receptor FcγRIIb on the target cell inhibited its deple-tion in vivo129.
These studies emphasize the potential need to tai-lor antibody Fc sequences to trigger specific activating receptors and improve therapeutic outcomes by selec-tively engaging activating receptors over inhibitory receptors. Thus, in the context of anticancer cell killing by mAbs, improved pro-inflammatory or killing activ-ity can potentially be achieved by altering the relative affinities of the antibody Fc region for activating versus inhibitory FcγRs. This has been achieved by mutating the Fc portion of IgG, and also by modification of Fc glycosylation, as discussed below.
Table 4 | Comparison of the regions of IgG involved in the interaction with FcγR*
IgG Lower hinge region (residues 232–239)
Cγ2 domain (residues 265–269)
Cγ2 domain (residues 296–300)‡
Cγ2 domain (residues 327–333)‡
Human IgG1 PELLGGPS DVSHE YNSTY ALPAPI
Human IgG3 PELLGGPS DVSHE YNSTY ALPAPI
Mouse IgG2a PNLLGGPS DVSED YNSTL DLPAPI
Human IgG2 PPVAG‑PS DVSHE FNSTF ALPAPI
Mouse IgG1 PEVS---S§ DISKD FNSTF AFPAPI
Mouse IgG2b PNLEGGPS DVSED YNSTI DLPSPI
Mouse IgG3 GNILGGPS DVSED YNSTF ALPAPI
Human IgG4 PEFLGGPS DVSQE FNSTY GLPSSI
FcR, Fc receptor; IgG, immunoglobulin G. *Regions of IgG subclasses are defined in crystallographic structures of the Fc of human IgG1 and FcgRIIIa29,31 as well as the Fc of human IgG1 and FcγRIIa11; not all residues are in contact with FcγRs — flanking residues are also included above. The interactive sites for other human and mouse Fc IgGs are inferred from mutagenesis studies or by homology with solved crystallographic structures. The sequence numbering, in parentheses, is based on that of human IgG1; the numbering of the equivalent residues in other IgG subclasses may vary (see text for details). ‡Glycosylated Asn297 residue located here; Pro329 residue becomes sandwiched between the tryptophan residues of FcγR during the interaction. §The dash indicates that an equivalent amino acid is missing in that position.
R E V I E W S
322 | APRIL 2012 | VOLUME 11 www.nature.com/reviews/drugdisc
© 2012 Macmillan Publishers Limited. All rights reserved

Engineering the Fc portion for altered and selective FcR binding. Several approaches have been undertaken to engineer modifications into the IgG Fc region for the selective engagement of different FcR types. These approaches have mostly aimed at selectively harness-ing the activating FcγRs while avoiding or minimiz-ing engagement of the inhibitory FcγRIIb. This can be achieved in the following ways: by optimizing the interaction of the Fc portion with the activating recep-tors without altering the interaction with the inhibi-tory receptor FcγRIIb; by eliminating binding to the inhibitory receptor without interfering with binding to the activating receptors; or using a combination of these two approaches. The availability of structural data, including nuclear magnetic resonance and X-ray crystallographic data for complexes of IgG and FcγRs, will further assist in the design and interpretation of improvements in antibody Fc function11,29,31.
Fc mutants of IgG have been designed to optimize FcR binding as well as the specificity of various anti-bodies. These include the CD52-specific antibody alem-tuzumab, the HER2 (also known as ERBB2)-specific antibody trastuzumab (Herceptin; Roche/Genentech), the CD20-specific antibody rituximab and the epider-mal growth factor receptor (EGFR)-specific antibody cetuximab (Erbitux; Bristol-Myers Squibb/Lilly/Merck Serono)130. The single mutation I332E or the double mutation S239D;I332E in the Fc region of trastuzumab increased its affinity for FcγRIIIa-V158 by tenfold and 100-fold, respectively. Further improvement in the induction of effector functions was achieved by intro-ducing the additional mutation A330L into the dou-ble mutant, which increased its affinity for FcγRIIIa and decreased its affinity for the inhibitory receptor FcγRIIb. These variants had 100–1,000-fold enhanced ADCC across a range of target antigen expression lev-els. Interestingly, incorporation of the A330L mutation into the S239D;I332E double mutant results in the loss of complement-dependent cytotoxicity (CDC) activity. This is due to the proximity of the Ala330 residue to the binding site of the complement component C1q, and the loss of CDC activity presumably reflects a structural change in the adjacent C1q binding site because of the mutation131. In this case, the engineered improvement of one Fc-dependent effector function comes at the expense of another.
Other molecular techniques, including yeast surface display together with mammalian expression, have also been used to introduce and select for mutations
in the Fc region of IgG. Some of these have improved differential binding to FcγRIIa or FcγRIIIa compared with binding to the inhibitory FcγRIIb. The R292P mutation in the IgG1 Fc region conferred only a small improvement in binding to activating FcRs but pro-foundly decreased binding to the inhibitory receptor. The incorporation of multiple point mutations resulted in strongly altered kinetics of binding to the activating receptors, with either little change or a reduction in the affinity to FcγRIIb. Furthermore, xenograft mouse models of B cell lymphoma created with the human Daudi cell line indicated that antibodies with altered Fc regions, resulting in increased binding to the inhibitory receptor, were less effective than the corresponding wild-type antibodies132. Improved differential binding to activating FcRs largely correlated with the presence of the IgG Fc mutations F243L, R292P, Y300L, V305I and P396L132.
Mutations that overcome the differences in affinities due to allelic variation of the FcR potentially improve the utility of antibodies as a therapeutic modality in patient populations as a whole. Mutations that overcome differences in FcγRIII allelic binding have been engi-neered into rituximab, the humanized FcγRIIb-specific antibody Hu2B6 and the chimeric HER2-specific anti-body CH4D5 (REF. 132). This has resulted in improved in vitro ADCC by peripheral blood mononuclear cells, probably NK cells, regardless of the FcγRIII genotype. It is also noteworthy that single mutations, notably F243L, generated IgG with selective improvements in binding to both allelomorphs of FcγRIIIa with little impact on binding to FcγRIIb133; furthermore, the improved bind-ing kinetics of the antibodies were reflected in better antitumour effects in animal models.
As the extracellular domains of FcγRIIa are highly related to FcγRIIb (only 13 amino acids are different), whereas the sequence of FcγRIIIa is considerably differ-ent, it is perhaps not surprising that IgG Fc mutations that are aimed at improving selective binding to activat-ing FcγRs are achieved more easily for FcγRIIIa than for FcγRIIa130,132,134.
Thus, a combination of in vitro studies and mouse models supports the concept that the engineering of antibody Fc regions for the selective engagement of activating FcRs over the inhibitory FcγRIIb may well improve treatment outcomes in patients, particularly with antibodies directed at the eradication of cancer or pathogens. Moreover, improvements that overcome the allele-specific differences in IgG binding may also improve therapeutic outcomes in genetically diverse populations.
As discussed below, improvement in selective bind-ing to an activating FcR can also be achieved by the modification of the N-linked glycan of IgG.
The effects of glycosylation of the antibody Fc portion. It is well known that the nature of N-glycosylation of antibody Fc regions has a profound influence on effector functions, and it was shown that the complete removal of the N-linked glycan ablates FcR binding for all IgG sub-classes117. For example, the near-complete removal of the
Box 1 | Relating mouse disease models to human FcR function
MouseandhumanFcγreceptors(FcγRs)arestructurallywellconservedanddisplaysimilarbindingcharacteristicsforimmunoglobulin G.However,thereareconsiderabledifferencesintissuedistributionandinductionbycytokines,andmicelackorthologuesofseveralmajorhumanFcγRssuchasFcγRIIa,FcγRIIcandFcγRIIIb;instead,theyexpressareceptorthatlacksanorthologueinhumans—FcγRIV.AlthoughadirectcomparisonofmouseFcRstotheirhumanorthologuesmaynotbeentirelyappropriate,mousemodelshavebeenveryusefulinestablishingseveralprinciplesofimmunecomplexandFcRactivationindiseaseprocessesandeffectorsystems.
C1qThe q fragment of the first component of serum complement activated by interaction with immune complexes.
AllelomorphsThe related protein products encoded by different alleles.
R E V I E W S
NATURE REVIEWS | DRUG DISCOVERY VOLUME 11 | APRIL 2012 | 323
© 2012 Macmillan Publishers Limited. All rights reserved

N-linked glycan in vivo by injection of endoglycosidase S reduced inflammation in lupus-prone mice135. This was thought to be due to the removal of most of the N-linked glycan from the immune complexes, thus reducing their interaction with FcγR.
There is now considerable interest in manipulating the carbohydrates of IgG to improve Fc function, either for better anti-inflammatory function of IVIg (see above) or for altered FcR engagement by therapeutic mAbs. Several strategies have been used to modify the antibody-associated carbohydrate structure.
The glycosylation pattern in IgG is composed of a con-served pentasaccharide structure containing mannose and N-acetylglucosamine (GlcNAc); the core fucose, bisecting GlcNAc and terminal sialylation vary between species (see REFS 116,117). Bisecting GlcNAc has been implicated in the enhanced ADCC activity of the Campath-1H anti-body produced in a rat myeloma cell line136.
The N-linked glycans of human IgG are attached at the Asn297 residue in the Cγ2 domain, which is also conserved in mouse IgG. The structure of the antibody glycan can be modified by manipulating the transferases and glycosidases present in intracellular compartments. To incorporate a bisecting GlcNAc into the chCE7 anti-neuroblastoma antibody, chCE7 was expressed in Chinese hamster ovary (CHO) cells that had different levels of β(1,4)-N-acetylglucosaminyltransferase III (GnTIII) expression137. These studies demonstrated that there is an optimum level of GnTIII expression that results in the production of antibodies that induce a maximum level of ADCC, and that this corresponds to the level of Fc-associated bisected non-fucosylated complex oligosaccharides.
In fact, non-fucosylated antibodies, produced in cells lacking the fucosyl transferase, bind to FcγRIIIa with an enhanced affinity and are thereby able to induce increased ADCC138–140. Such non-fucosylated antibodies have also been generated in HEK293-EBNA cell lines expressing chimeric enzymes generated by domain swapping of various transferases and mannosidase. CD20-specific antibodies were produced that had a higher affinity for FcγRIIIa and increased ADCC relative to the wild-type antibody, with relatively little change in the binding affin-ity for the inhibitory FcγRIIb141,142.
Similarly, the expression of a CD20-specific anti-body in HEK293-EBNA cells expressing GnTIII alone (this variant was called Glyco-1) or together with α-mannosidase II (this variant was called Glyco-2) resulted in afucosylated glycoengineered antibod-ies with substantially improved binding to recom-binant ectodomains of both FcγRIIIa allelomorphs; with FcγRIIIa-V158, there was a 50-fold improve-ment in binding with the Glyco-2 variant, and with the FcγRIIIa-F158 allelomorph there was an 18-fold improvement in binding with the Glyco-1 variant and a 27-fold improvement in binding with the Glyco-2 vari-ant141,142. There was no change in the binding affinity of these antibodies to the inhibitory FcγRIIb. Similar glyco-engineering strategies have been used to increase the effi-cacy of other therapeutic antibodies143,144. Interestingly, the expression of IgG in HEK-293F cells, in the presence
of kifunensine (which inhibits N-glycosylation), also results in afucosylated antibodies with enhanced ADCC activity145.
The basis of this improved binding of afucosylated IgG to FcγRIIIa has not been structurally defined but a comparison of fucosylated and non-fucosylated anti-bodies suggests that Tyr296, which is adjacent to the gly-cosylated Asn297 in the Cγ2 domain, may be involved28. Furthermore, the carbohydrate of FcγRIIIa at Asn163 may also contribute to the effect, as enhanced binding of the glycoengineered antibodies was not observed when this glycan was removed from the receptor141,142.
The selective engagement of activating FcRs over the inhibitory FcγRIIb may be desirable in the treatment of malignancies, and glycoengineering has effectively achieved this. It is clear that the afucosylated antibod-ies have improved binding, particularly to the activating FcγRIIIa compared with the inhibitory FcγRIIb; most importantly, afucosylated antibodies have now been used in clinical trials for the treatment of malignancies, and have shown improved efficacy over their fucosylated counterparts135,146.
Although non-glycosylated antibodies do not bind to FcRs, their amino acid sequences can be modified to restore FcγR binding. Yeast cell surface display was used to screen three libraries with mutations in the Fc C′E loops (amino acids Tyr296-Asn297-Ser298-Thr299, Asn297- Ser298-Thr299 and Asn297-Ser298-Thr299-Tyr300) of a high-affinity fluorescein-binding antibody. A cell secre-tion capture assay was used to screen the library with fluorophore-labelled FcγRIIa-R131 tetramers147. After multiple rounds of screening, the three aglycosylated motifs S298G;T299A, S298G;T299G and T299A were isolated, with the highest affinity of binding attributed to the double mutant S298G;T299A. It was apparent that the Asn297 residue was crucial for binding to FcγRIIa, even in the absence of glycosylation. The double mutant bound both FcγRIIa allelomorphs and FcRIIb, but not FcγRIIIa or C1q, and had a tenfold lower affinity for FcγRI com-pared with FcγRIIa. The antibodies were active in vivo in a platelet clearance model in FcγRIIa-transgenic mice147.
Manipulation of antibody IgG half-lifeIgG1, IgG2 and IgG4 — but usually not IgG3 — have very long half-lives in the circulation owing to a specific recy-cling system or salvage pathway that acts via the surface receptor FcRn (reviewed in REF. 148). FcRn is expressed primarily on the endothelium but is also expressed on other cell types17.
FcRn regulates IgG concentrations in the serum and tissues by binding to IgG after it is taken up by endothe-lial cells via fluid-phase pinocytosis. The binding and release of IgG to and from FcRn is pH-dependent; as the pH decreases in the acidifying endosome, IgG binds and is trafficked back to the cell surface where it is released back into the extracellular fluids at their near-neutral pH. IgGs that do not bind are not recycled, and are degraded intracellularly.
The site of interaction of IgG with FcRn is distinct from that of the classical FcγRs35 and has been mapped to residues at the interface of the Cγ2–Cγ3 domain
R E V I E W S
324 | APRIL 2012 | VOLUME 11 www.nature.com/reviews/drugdisc
© 2012 Macmillan Publishers Limited. All rights reserved

— especially His435 (REFS 149,150), which is found in IgG1, IgG2 and IgG4. By contrast, most allotypes of IgG3 lack this crucial histidine residue, which accounts for their shorter half-life. However, the IgG3 antibodies of the G3m(s,t) allotype, which is uncommon in Caucasian populations, contain the His435 residue, raising the pos-sibility that it too has a half-life equivalent to the other IgG subclasses151.
The engineering of IgG to control the Fc–FcRn inter-action, especially its pH sensitivity, has made it possible to alter antibody levels in the serum and tissues. This could either prolong antibody half-life for greater thera-peutic benefit or reduce its half-life in situations where more rapid clearance may be desirable.
Increasing IgG half-life. An increase in the half-life of therapeutic antibodies can result in enhanced exposure
to their therapeutic effects, which may allow a reduc-tion in the dose, frequency of administration and cost. By retaining the property of its pH-dependent release from FcRn while simultaneously increasing its bind-ing affinity to FcRn, it is possible to modulate the serum half-life of IgG. This was achieved by mutating residues Thr250 and Met428 of the IgG Cγ2–Cγ3 inter-face located near the FcRn binding site152. In addition, mutagenesis and screening of an IgG2 human hepatitis B virus (HBV)-specific mAb resulted in the double mutant T250Q;M428L with a 28-fold increased pH-dependent affinity for FcRn. Pharmacokinetic analysis of this anti-body and a similarly mutated IgG1 in primates indicated that the half-life of this antibody was doubled compared with the wild-type antibody. Importantly, the mutagen-esis did not substantially affect effector functions such as ADCC and CDC.
Protectedtissue
Protectedtissue
Antigen presentation
SolubleFcγR
Immune complex(antigen) uptake
Blockade
InflammationFcγR
Activation
Inflammatory cell
Nature Reviews | Drug Discovery
mAb or SCEblockade
Inflammed target tissue
Activation
No activation
Mediators
SolubleFcγRblockade
FcγRI FcγRIIa FcγRIIb FcγRIIIa
IgG mAb SCE
Figure 7 | Potential scenarios for the use of soluble Fc receptors in the blockade of immune complex-induced activation of inflammatory cells and tissue destruction. Circulating autoantibody–autoantigen immune complexes — for example, anti‑chromatin–chromatin complexes — can be internalized by Fc receptor (FcR)‑positive antigen‑presenting cells for processing and further antigen presentation. The binding of soluble FcRs to autoantibody Fc regions may prevent this process. Similarly, autoantibody-coated target tissue activates FcR-expressing inflammatory effector cells, inducing mediator release. Soluble FcR ectodomains binding to Fc regions of the tissue-bound autoantibodies may prevent inflammatory cell activation. An alternative approach is the direct blockade of cell bound FcRs using monoclonal antibodies (mAbs) or small chemical entities (SCEs) that bind to specific FcR subtypes.
R E V I E W S
NATURE REVIEWS | DRUG DISCOVERY VOLUME 11 | APRIL 2012 | 325
© 2012 Macmillan Publishers Limited. All rights reserved

Similar results have been achieved using a human-ized respiratory syncytial virus (RSV)-specific antibody with a triple mutation (M252Y, S254T and T256G), which extended the serum half-life by fourfold com-pared with the corresponding wild-type IgG1 (REF. 153).
Mutations in Fc regions to decrease IgG half-life. There are instances in which a decrease in serum half-life is desirable: for example, when radiolabelled mAbs are used for tumour localization studies and when the rapid serum clearance of an unbound antitumour anti-body leads to lower nonspecific binding and therefore improved imaging. To reduce the half-life of mAbs, the FcRn contact residues Ile253 and His310 (in the Cγ2 domain) as well as His435 (in the Cγ3 domain) of IgG have been mutated. In imaging studies, single muta-tions (H435R, H435Q, H310A and I253A), as well as a double mutation (H310A;H435Q), were introduced into the Fc region of an anti-carcinoembryonic anti-gen hybrid fusion protein consisting of an Fc fused to a single-chain variable fragment (scFv)154. Although the wild-type Fc fusion protein had a half-life of 12 days, the half-lives of the mutants were dramatically reduced to as little as 8 hours for the double mutant. Because of the faster clearance rate, this mutant also had the high-est tumour-to-background binding ratios and provided high-contrast images at early time points.
FcRn blockade to improve antibody clearance. The strat-egies outlined above are focused on manipulating the persistence of passively transferred mAbs by directly altering the FcRn binding site of the transferred anti-body. However, the direct blockade of FcRn can reduce the half-life of circulating endogenous IgG by preventing its binding to FcRn and therefore denying it access to the salvage pathway. This leads to the rapid degradation of potentially pathogenic immune complexes composed of IgG. A highly efficient competitor IgG was engineered and the following mutations were introduced around its FcRn binding site18: M253Y, S254T, T256E, H433K and N434F. This variant IgG1 had a higher affinity for mouse and human FcRn at pH 6 and, importantly, also at pH 7.2, reducing the dissociation of IgG from FcRn and effectively blocking the receptor. When used in vivo, the clearance of circulating IgG immune complexes was significantly enhanced. Such antibodies (antibodies that enhance IgG degradation; ‘Abdegs’)18 may have clinical utility in lowering the levels of circulating immune com-plexes in autoimmune diseases.
One cautionary note, however, is that although mouse and human FcRn have similar properties, they also have significant differences, which can lead to unexpected discrepancies in the behaviour of engi-neered antibodies in mouse models155,156.
Future strategies for FcR manipulationThe effectiveness of anticancer antibodies that depend on effector cell functions such as ADCC or phagocyto-sis relies on a ‘trans’ interaction, whereby the therapeu-tic antibody is bound to an antigen on the target cell, and the Fc portion is bound to the FcR on a recruited
effector cell. However, in certain circumstances it may be possible to exploit a ‘cis’ interaction — when a tar-get and FcR are expressed on the same cell. Indeed, an interesting property of antibodies and FcR systems is the little recognized ‘scorpion effect’ or ‘Kurlander effect’, an observation made in 1983 (REF. 157) that showed that an antibody recognizing a cell surface mol-ecule via its Fab antigen binding sites could simultane-ously engage an FcR on the same cell (that is, in a cis fashion), thus creating a usually heterotrimeric complex (FIG. 8); this observation has the potential to be thera-peutically exploitable. In that instance, the ‘scorpion-like’ arrangement led to the activation of the cell, which relied — at least in part — on the recruitment of an activating FcR157.
In the broader context of antibody engineering, these experiments demonstrate the principle that the recruitment of an FcR via the Fc portion of an antibody that is already bound to a target receptor on the surface of the same cell can influence intracellular signalling as well as the biochemical and biological role of the target. Thus, a ‘scorpion effect’ could modify the therapeutic effect of an antibody by co-engaging activating or inhib-itory receptors with an appropriate target, and several speculative points can be made. First, when the inhibi-tory FcγRIIb is co-engaged with an appropriate receptor whose activation can normally be modulated by ITIM-dependent signals, this may result in a downregulation of target receptor signalling, thereby modulating an activated pro-inflammatory response or enhancing an inhibitory response.
Second, although the co-engagement of an activat-ing receptor target with an activating FcR might be expected to lead to further — perhaps undesirable — activation, it has recently become apparent that acti-vating FcRs exhibit a paradoxical dualism of function. Under some circumstances, which are not well defined in vivo, activating FcRs can deliver an inhibitory signal, also known as an ITAMi6,26,158. In this context, a mAb recognizing Toll-like receptor 4 (TLR4) has been devel-oped that was shown to neutralize lipopolysaccharide (LPS)-mediated activation of myeloid cells and ame-liorate endotoxaemia in animal models159. In in vitro studies of normal human myeloid cells, the potency of the inhibitory effect was surprisingly dependent on the simultaneous co-engagement of the activating FcγRIIa and not the inhibitory FcγRIIb159.
Although not strictly related to the ‘scorpion effect’, there is an increasing number of studies, many involv-ing FcRs, that exemplify this enigmatic capacity of ITAMs to deliver inhibitory signals. These include the effectiveness of IgG in preventing basophil degranula-tion in patients desensitized for cat allergy, which was dependent on the engagement of FcγRIIa in concert with the inhibitory FcγRIIb4.
The ITAMi function appears to be induced in cir-cumstances when ITAM-containing receptors are stim-ulated by low-avidity ligands, which induces a signalling bias towards inhibition. This is, for example, the case for low-avidity stimulation of FcαRI6 and FcγRIIIa7. Similar inhibitory effects have been identified for other
R E V I E W S
326 | APRIL 2012 | VOLUME 11 www.nature.com/reviews/drugdisc
© 2012 Macmillan Publishers Limited. All rights reserved

multisubunit receptor complexes — for example, recep-tors utilizing DAP10 and DAP12 on NK cells158, as well as the T- and B cell receptors160. This inhibitory bias is associated with monotyrosyl phosphorylation of the ITAM and the recruitment of phosphotyrosine and phosphoinositide phosphatases6,26,160.
One potential therapeutic benefit of exploiting ITAMi function is that in some cases the inhibitory effect is prop-agated throughout the cell and leads to a generalized lack of responsiveness affecting other receptor classes6,26,160.
The relationship between a given target molecule for an antibody therapeutic and the co-expressed FcRs on the target cells, and the exploitation of the ‘scorpion effect’, clearly has implications for the engineering of the Fc por-tions of antibodies directed at cell surface molecules. For example, these could be engineered to selectively engage activating or inhibitory FcRs in a ‘cis’ configuration; alter-natively, they could be engineered to provide an enhanced therapeutic effect in the context of improved inhibition of inflammation or more effective target cell apoptosis.
How universally exploitable this strategy is remains to be seen. It requires careful consideration, especially if activating receptors are deliberately targeted, as crosslinking these with an additional activating receptor may have adverse consequences in a therapeutic setting. However, it is noteworthy that for the TLR4-specific antibody described above, which prevents the LPS-mediated activation of target cells by blocking the bind-ing of LPS to TLR4, FcR co-engagement is thought to induce further unresponsiveness159. Strategies exploit-ing the ‘scorpion effect’ would largely be restricted to targeting leukocytes and leukocyte malignancies, as FcR expression is largely restricted to these cell types.
ConclusionsThe targeting of FcRs to prevent pathological responses induced by immune complexes in autoimmune disease is still in its infancy. This is somewhat surprising, as there can be few examples where the induction of a patho-logical response can be so readily attributed to a specific
LYN
LYNLYN LYN
P
P
P
PP
P
P PP
SYK
Activation
SYKSYK
Antibody Antibodya
Activating FcRs
CommonFcRγ-chain
ITAM
ITAM
Fc region
Fab regionSurface proteinLow-affinityFcR
b
Inhibition
ITAMi
SHP1SHIP
Nature Reviews | Drug Discovery
Fab region
ActivatingFcR
Fcregion
Figure 8 | The ‘scorpion effect’. An anti-receptor antibody engages its target via the antigen-binding sites in the Fab arms, and a ‘cis’ interaction simultaneously engages an Fc receptor (FcR) on the same cell, thereby forming a trimolecular complex. This effect was originally described for antibodies that bind to activating FcRs with their variable regions157, and to an activating FcR with their Fc region. In this case (part a), a trivalent immunoreceptor tyrosine-based activation motif (ITAM)‑dependent signalling complex is formed, which activates tyrosine kinases such as LYN and spleen tyrosine kinase (SYK), resulting in cell activation. A similar configuration is possible in heterologous systems where the antibody targets a cell surface protein other than an FcR, and the ‘cis’ engagement of either activating157 or inhibitory129 FcRs. Part b illustrates how the scorpion effect can have an inhibitory function. In this case, the antibody recognizes a hypothetical protein (shown in green) and at the same time engages a low-affinity ITAM-containing FcR (for example, FcγRIIa), with low avidity and in a monovalent fashion. The low‑avidity binding to the FcR leads to ITAM monophosphorylation by the LYN kinase, instead of the usual biphosphorylation. This in turn results in the recruitment of protein and lipid phosphatases such as SH2 domain-containing protein tyrosine phosphatase 1 (SHP1) and SH2 domain-containing inositol-5-phos-phatase (SHIP), leading to inhibition of cell activation. Although the mechanism of such an inhibitory ‘scorpion effect’ is still speculative, the monophosphorylation of ITAMs in response to low-avidity ligands, and the resulting function as inhibitory ITAM (ITAMi), has been described for ITAMs of receptors other than FcRs160. However, in the FcR context, such a function may explain the enhanced FcγRIIa-dependent inhibitory activity of an anti-TLR4 (Toll-like receptor 4) antibody159 or the similar phenomenology involving FcεRI, FcγRIIa and FcγRIIb in desensitized patients with cat allergies4.
R E V I E W S
NATURE REVIEWS | DRUG DISCOVERY VOLUME 11 | APRIL 2012 | 327
© 2012 Macmillan Publishers Limited. All rights reserved

receptor type. There is still some lack of understanding of the relative importance of the various FcγRs, as well as the need for validating these targets in humans. Nonetheless, soluble FcRs, small chemical entities and receptor mimet-ics or receptor-blocking antibodies are now in preclinical development. In this context, it is likely that FcγRs will receive greater attention as potential therapeutic targets.
In the context of harnessing FcR-dependent cel-lular effector systems, accumulated data from clinical studies of therapeutic antibodies have identified FcγR-dependent mechanisms as being crucial for the clinical utility of many anticancer antibodies. This has paved the way for a new generation of antibodies, which can be fine-tuned for enhanced effector function by the modi-fication of their Fc region. Antibodies with optimized binding to activating FcγRs, through mutagenesis or modification of the glycosylation of their Fc regions, are becoming a clinical reality and several such antibodies have been evaluated in patients146,161.
Future attempts at improving IgG potency in vivo may well focus less on the manipulation of its Fc portion and more on efforts to alter FcR expression; for example, by increasing the expression of activating receptors in a cancer therapy setting or by increasing the expression of inhibitory receptors in immune complex-driven autoim-mune inflammation (as is suggested by the use of IVIg).
As the majority of therapeutic antibodies are of the IgG class, and the majority of these are of the IgG1 subclass, most of the effort on optimizing Fc–FcR interactions has, not surprisingly, focused on the FcγRs. However, this effort has largely ignored other immunoglobulin classes. Indeed, future improvements to immunoglobu-lins for the purposes of harnessing FcR mechanisms may lie with the development of IgA or IgE antibodies to harness the FcαRI- and FcεRI-dependent responses, respectively. Indeed, the binding of IgA to FcαRI induces powerful antitumour responses in vitro and in transgenic mouse models, outperforming the antitumour responses induced via FcγRs162. Furthermore, therapeutic IgA may be useful for targeting diseases at mucosal surfaces, such as gastrointestinal cancers163.
IgE should also not be ruled out as a therapeutic modality. The IgE–FcεRI interaction is one of the most pharmacologically powerful responses in immunity
and, because this system is such a potent inducer of inflammation, efforts to exploit systems that are dependent on this interaction are worthy of considera-tion. This may offer greater potency against intracta-ble tumours or chronic infections. Although the use of therapeutic IgE runs the risk of inducing systemic hypersensitivity reactions with severe consequences, the application of modern biotechnology to the engineer-ing of IgE therapeutic antibodies should help mitigate the risk of adverse events. This could be achieved by decreasing the strength of the interaction with FcεRI. In any case, it is clear that much is still to be learned about the biology of FcR function; a greater understanding in this regard will be essential in the next phase of anti-inflammatory drug development in autoimmunity, as well as in the development of therapeutic antibodies for cancer and infection.
A crucial area for future development will be animal models for FcR-mediated inflammation resulting from autoimmune diseases. In oncology, antibody-based immunotherapeutics can be readily studied and opti-mized using human effector cells on tumours in vitro, before time-consuming and expensive toxicology and clinical trials are carried out. Such in vitro experiments are not possible for autoimmune diseases. The absence of some activating receptors, such as FcγRIIa, in mouse models complicates the validation of these receptors as targets for anti-inflammatory drugs and also com-promises the evaluation of therapeutic antibodies that may depend on FcγR function in vivo. Better animal models expressing the entire human FcγR repertoire may overcome such obstacles, providing more realistic ‘humanized’ mouse models of autoimmunity and can-cer therapy. In this context, even though the macaque is the fundamental preclinical animal model of mAb test-ing, there is a paucity of studies on macaque FcRs and it is not clear to what degree they recapitulate human IgG binding and effector function.
In addition, a greater understanding of the factors that drive the induction of the ITAMi state, as well as the factors that enhance antibody potency by altering FcR configurations in the cell membrane, will pave the way towards a more sophisticated manipulation of FcγR-dependent antibody effector functions.
1. Hulett, M. D. & Hogarth, P. M. Molecular basis of Fc receptor function. Adv. Immunol. 57, 1–127 (1994).
2. Nakamura, A., Akiyama, K. & Takai, T. Fc receptor targeting in the treatment of allergy, autoimmune diseases and cancer. Expert Opin. Ther. Targets 9, 169–190 (2005).
3. Takai, T. Fc receptors and their role in immune regulation and autoimmunity. J. Clin. Immunol. 25, 1–18 (2005).
4. Cady, C. T. et al. IgG antibodies produced during subcutaneous allergen immunotherapy mediate inhibition of basophil activation via a mechanism involving both FcgRIIA and FcgRIIB. Immunol. Lett. 130, 57–65 (2010).
5. Hamerman, J. A. et al. Cutting edge: inhibition of TLR and FcR responses in macrophages by triggering receptor expressed on myeloid cells (TREM)-2 and DAP12. J. Immunol. 177, 2051–2055 (2006).
6. Pfirsch-Maisonnas, S. et al. Inhibitory ITAM signaling traps activating receptors with the phosphatase SHP-1 to form polarized “inhibisome” clusters. Sci. Signal. 4, ra24 (2011).
7. Pinheiro da Silva, F. et al. CD16 promotes Escherichia coli sepsis through an FcRg inhibitory pathway that prevents phagocytosis and facilitates inflammation. Nature Med. 13, 1368–1374 (2007).
8. Nimmerjahn, F. & Ravetch, J. V. Divergent immunoglobulin G subclass activity through selective Fc receptor binding. Science 310, 1510–1512 (2005).
9. Ravetch, J. In vivo veritas: the surprising roles of Fc receptors in immunity. Nature Immunol. 11, 183–185 (2010).
10. Metzger, H. Transmembrane signaling: the joy of aggregation. J. Immunol. 149, 1477–1487 (1992).
11. Ramsland, P. A. et al. Structural basis for FcgRIIa recognition of human IgG and formation of inflammatory signaling complexes. J. Immunol. 187, 3208–3217 (2011).
12. Powell, M. S. et al. Alteration of the FcgRIIa dimer interface affects receptor signaling but not ligand binding. J. Immunol. 176, 7489–7494 (2006).
13. Maxwell, K. F. et al. Crystal structure of the human leukocyte Fc receptor, FcgRIIa. Nature Struct. Biol. 6, 437–442 (1999).
14. Acharya, M. et al. CD23/FceRII: molecular multi-tasking. Clin. Exp. Immunol. 162, 12–23 (2010).
15. Wines, B. D., Powell, M. S., Parren, P. W., Barnes, N. & Hogarth, P. M. The IgG Fc contains distinct Fc receptor (FcR) binding sites: the leukocyte receptors FcgRI and FcgaRIIa bind to a region in the Fc distinct from that recognized by neonatal FcR and protein A. J. Immunol. 164, 5313–5318 (2000).
16. Baker, K. et al. Neonatal Fc receptor for IgG (FcRn) regulates cross-presentation of IgG immune complexes by CD8–CD11b+ dendritic cells. Proc. Natl Acad. Sci. USA 108, 9927–9932 (2011).
R E V I E W S
328 | APRIL 2012 | VOLUME 11 www.nature.com/reviews/drugdisc
© 2012 Macmillan Publishers Limited. All rights reserved

17. Kacskovics, I., Cervenak, J., Erdei, A., Goldsby, R. A. & Butler, J. E. Recent advances using FcRn overexpression in transgenic animals to overcome impediments of standard antibody technologies to improve the generation of specific antibodies. MAbs 3, 431–439 (2011).
18. Vaccaro, C., Zhou, J., Ober, R. J. & Ward, E. S. Engineering the Fc region of immunoglobulin G to modulate in vivo antibody levels. Nature Biotech. 23, 1283–1288 (2005).
19. van der Poel, C. E. et al. Cytokine-induced immune complex binding to the high-affinity IgG receptor, FcgRI, in the presence of monomeric IgG. Blood 116, 5327–5333 (2010).
20. Bruhns, P. et al. Specificity and affinity of human Fcg receptors and their polymorphic variants for human IgG subclasses. Blood 113, 3716–3725 (2009).
21. Maenaka, K., van der Merwe, P. A., Stuart, D. I., Jones, E. Y. & Sondermann, P. The human low affinity Fcg receptors IIa, IIb, and III bind IgG with fast kinetics and distinct thermodynamic properties. J. Biol. Chem. 276, 44898–44904 (2001).
22. Powell, M. S. et al. Biochemical analysis and crystallisation of FcgRIIa, the low affinity receptor for IgG. Immunol. Lett. 68, 17–23 (1999).
23. Bibeau, F. et al. Impact of FcgRIIa–FcgRIIIa polymorphisms and KRAS mutations on the clinical outcome of patients with metastatic colorectal cancer treated with cetuximab plus irinotecan. J. Clin. Oncol. 27, 1122–1129 (2009).
24. Concetti, F. & Napolioni, V. Insights into the role of Fcg receptors (FcgRs) genetic variations in monoclonal antibody-based anti-cancer therapy. Recent Pat. Anticancer Drug Discov. 5, 197–204 (2010).
25. Zhuang, Y., Xu, W., Shen, Y. & Li, J. Fcg receptor polymorphisms and clinical efficacy of rituximab in non-Hodgkin lymphoma and chronic lymphocytic leukemia. Clin. Lymphoma Myeloma Leuk. 10, 347–352 (2010).
26. Cady, C. T., Rice, J. S., Ott, V. L. & Cambier, J. C. Regulation of hematopoietic cell function by inhibitory immunoglobulin G receptors and their inositol lipid phosphatase effectors. Immunol. Rev. 224, 44–57 (2008).
27. Burton, D. R. & Woof, J. M. Human antibody effector function. Adv. Immunol. 51, 1–84 (1992).
28. Matsumiya, S. et al. Structural comparison of fucosylated and nonfucosylated Fc fragments of human immunoglobulin G1. J. Mol. Biol. 368, 767–779 (2007).
29. Radaev, S., Motyka, S., Fridman, W. H., Sautes-Fridman, C. & Sun, P. D. The structure of a human type III Fcg receptor in complex with Fc. J. Biol. Chem. 276, 16469–16477 (2001).
30. Radaev, S. & Sun, P. D. Recognition of IgG by Fcg receptor. The role of Fc glycosylation and the binding of peptide inhibitors. J. Biol. Chem. 276, 16478–16483 (2001).
31. Sondermann, P., Huber, R., Oosthuizen, V. & Jacob, U. The 3.2-Å crystal structure of the human IgG1 Fc fragment–FcgRIII complex. Nature 406, 267–273 (2000).
32. Sondermann, P. & Oosthuizen, V. X-ray crystallographic studies of IgG–Fcg receptor interactions. Biochem. Soc. Trans. 30, 481–486 (2002).
33. Lu, J., Ellsworth, J. L., Hamacher, N., Oak, S. W. & Sun, P. D. Crystal structure of Fcg receptor I and its implication in high affinity g-immunoglobulin binding. J. Biol. Chem. 286, 40608–40613 (2011).
34. Garman, S. C., Wurzburg, B. A., Tarchevskaya, S. S., Kinet, J. P. & Jardetzky, T. S. Structure of the Fc fragment of human IgE bound to its high-affinity receptor FceRIa. Nature 406, 259–266 (2000).
35. Wines, B. D., Sardjono, C. T., Trist, H. H., Lay, C. S. & Hogarth, P. M. The interaction of FcaRI with IgA and its implications for ligand binding by immunoreceptors of the leukocyte receptor cluster. J. Immunol. 166, 1781–1789 (2001).
36. Herr, A. B., Ballister, E. R. & Bjorkman, P. J. Insights into IgA-mediated immune responses from the crystal structures of human FcaRI and its complex with IgA1–Fc. Nature 423, 614–620 (2003).
37. Takai, T., Li, M., Sylvestre, D., Clynes, R. & Ravetch, J. V. FcRg chain deletion results in pleiotrophic effector cell defects. Cell 76, 519–529 (1994).
38. Pritchard, N. R. et al. Autoimmune-prone mice share a promoter haplotype associated with reduced expression and function of the Fc receptor FcgRII. Curr. Biol. 10, 227–230 (2000).
39. Ierino, F. L., Powell, M. S., McKenzie, I. F. & Hogarth, P. M. Recombinant soluble human FcgRII: production, characterization, and inhibition of the Arthus reaction. J. Exp. Med. 178, 1617–1628 (1993).
40. Yuasa, T. et al. Deletion of Fcg receptor IIB renders H-2b mice susceptible to collagen-induced arthritis. J. Exp. Med. 189, 187–194 (1999).
41. Tan Sardjono, C. et al. Development of spontaneous multisystem autoimmune disease and hypersensitivity to antibody-induced inflammation in Fcg receptor IIa-transgenic mice. Arthritis Rheum. 52, 3220–3229 (2005).
42. van Lent, P. L. et al. Role of Fc receptor g chain in inflammation and cartilage damage during experimental antigen-induced arthritis. Arthritis Rheum. 43, 740–752 (2000).
43. van Lent, P. L. et al. Role of activatory FcgRI and FcgaaRIII and inhibitory FcgRII in inflammation and cartilage destruction during experimental antigen-induced arthritis. Am. J. Pathol. 159, 2309–2320 (2001).
44. Mullazehi, M., Mathsson, L., Lampa, J. & Ronnelid, J. Surface-bound anti-type II collagen-containing immune complexes induce production of tumor necrosis factor a, interleukin-1β, and interleukin-8 from peripheral blood monocytes via Fcg receptor IIA: a potential pathophysiologic mechanism for humoral anti-type II collagen immunity in arthritis. Arthritis Rheum. 54, 1759–1771 (2006).
45. Ravetch, J. V. Fc receptors: rubor redux. Cell 78, 553–560 (1994).
46. Tsuboi, N., Asano, K., Lauterbach, M. & Mayadas, T. N. Human neutrophil Fcg receptors initiate and play specialized nonredundant roles in antibody-mediated inflammatory diseases. Immunity 28, 833–846 (2008).
47. Monach, P. A., Benoist, C. & Mathis, D. The role of antibodies in mouse models of rheumatoid arthritis, and relevance to human disease. Adv. Immunol. 82, 217–248 (2004).
48. Diaz de Stahl, T., Andren, M., Martinsson, P., Verbeek, J. S. & Kleinau, S. Expression of FcgRIII is required for development of collagen-induced arthritis. Eur. J. Immunol. 32, 2915–2922 (2002).
49. Barnes, N. et al. FcgRI-deficient mice show multiple alterations to inflammatory and immune responses. Immunity 16, 379–389 (2002).
50. Baudino, L. et al. Differential contribution of three activating IgG Fc receptors (FcgRI, FcgRIII, and FcgRIV) to IgG2a- and IgG2b-induced autoimmune hemolytic anemia in mice. J. Immunol. 180, 1948–1953 (2008).
51. Bergtold, A., Gavhane, A., D’Agati, V., Madaio, M. & Clynes, R. FcR-bearing myeloid cells are responsible for triggering murine lupus nephritis. J. Immunol. 177, 7287–7295 (2006).
52. Ioan-Facsinay, A. et al. FcgRI (CD64) contributes substantially to severity of arthritis, hypersensitivity responses, and protection from bacterial infection. Immunity 16, 391–402 (2002).
53. McKenzie, S. E. Humanized mouse models of FcR clearance in immune platelet disorders. Blood Rev. 16, 3–5 (2002).
54. Nimmerjahn, F. & Ravetch, J. V. Fcg receptors as regulators of immune responses. Nature Rev. Immunol. 8, 34–47 (2008).
55. Nimmerjahn, F. & Ravetch, J. V. Antibody-mediated modulation of immune responses. Immunol. Rev. 236, 265–275 (2010).
56. Takai, T. Allergy and autoimmunity mediated by IgG and Fcg receptors. Arerugi 54, 1183–1189 (2005).
57. McGaha, T. L., Karlsson, M. C. & Ravetch, J. V. FcgRIIB deficiency leads to autoimmunity and a defective response to apoptosis in Mrl-MpJ mice. J. Immunol. 180, 5670–5679 (2008).
58. Dharajiya, N. et al. FcgRIIb inhibits allergic lung inflammation in a murine model of allergic asthma. PLoS ONE 5, e9337 (2010).
59. Clatworthy, M. R. et al. Systemic lupus erythematosus-associated defects in the inhibitory receptor FcgRIIb reduce susceptibility to malaria. Proc. Natl Acad. Sci. USA 104, 7169–7174 (2007).
60. Tsuboi, N. et al. Regulation of human neutrophil Fcg receptor IIa by C5a receptor promotes inflammatory arthritis in mice. Arthritis Rheum. 63, 467–478 (2011).
61. Van de Velde, N. C. et al. Transgenic mice expressing human FcgRIIa have enhanced sensitivity to induced autoimmune arthritis as well as elevated Th17 cells. Immunol. Lett. 130, 82–88 (2010).
62. Means, T. K. et al. Human lupus autoantibody–DNA complexes activate DCs through cooperation of CD32 and TLR9. J. Clin. Invest. 115, 407–417 (2005).
63. Asano, K. et al. A genome-wide association study identifies three new susceptibility loci for ulcerative colitis in the Japanese population. Nature Genet. 41, 1325–1329 (2009).
64. Hogarth, P. M. Fc receptors are major mediators of antibody based inflammation in autoimmunity. Curr. Opin. Immunol. 14, 798–802 (2002).
65. Ellsworth, J. L. et al. Recombinant soluble human FcgR1A (CD64A) reduces inflammation in murine collagen-induced arthritis. J. Immunol. 182, 7272–7279 (2009).
66. Ellsworth, J. L. et al. Generation of a high-affinity Fcg receptor by Ig-domain swapping between human CD64A and CD16A. Protein Eng. Des. Sel. 23, 299–309 (2010).
67. Ellsworth, J. L. et al. Targeting immune complex-mediated hypersensitivity with recombinant soluble human FcgRIA (CD64A). J. Immunol. 180, 580–589 (2008).
68. Magnusson, S. E. et al. Amelioration of collagen-induced arthritis by human recombinant soluble FcgRIIb. Clin. Immunol. 127, 225–233 (2008).
69. Shashidharamurthy, R. et al. Extravasations and emigration of neutrophils to the inflammatory site depend on the interaction of immune-complex with Fcg receptors and can be effectively blocked by decoy Fcg receptors. Blood 111, 894–904 (2008).
70. Werwitzke, S. et al. Treatment of lupus-prone NZB/NZW F1 mice with recombinant soluble Fcg receptor II (CD32). Ann. Rheum. Dis. 67, 154–161 (2008).
71. Dougherty, G. J., Selvendran, Y., Murdoch, S., Palmer, D. G. & Hogg, N. The human mononuclear phagocyte high-affinity Fc receptor, FcRI, defined by a monoclonal antibody, 10.1. Eur. J. Immunol. 17, 1453–1459 (1987).
72. Fleit, H. B., Wright, S. D. & Unkeless, J. C. Human neutrophil Fcg receptor distribution and structure. Proc. Natl Acad. Sci. USA 79, 3275–3279 (1982).
73. Looney, R. J., Abraham, G. N. & Anderson, C. L. Human monocytes and U937 cells bear two distinct Fc receptors for IgG. J. Immunol. 136, 1641–1647 (1986).
74. Rankin, C. T. et al. CD32B, the human inhibitory Fc-g receptor IIB, as a target for monoclonal antibody therapy of B-cell lymphoma. Blood 108, 2384–2391 (2006).
75. Su, K. et al. Expression profile of FcgRIIb on leuko cytes and its dysregulation in systemic lupus erythema tosus. J. Immunol. 178, 3272–3280 (2007).
76. Kimberly, R. P. et al. In vivo handling of soluble complement fixing Ab/dsDNA immune complexes in chimpanzees. J. Clin. Invest. 84, 962–970 (1989).
77. Clarkson, S. B. et al. Treatment of refractory immune thrombocytopenic purpura with an anti-Fcg-receptor antibody. N. Engl. J. Med. 314, 1236–1239 (1986).
78. Clarkson, S. B. et al. Blockade of clearance of immune complexes by an anti-Fcg receptor monoclonal antibody. J. Exp. Med. 164, 474–489 (1986).
79. Ericson, S. G. et al. Monoclonal antibody 197 (anti-FcgRI) infusion in a patient with immune thrombocytopenia purpura (ITP) results in down-modulation of FcgRI on circulating monocytes. Br. J. Haematol. 92, 718–724 (1996).
80. Wallace, P. K. et al. Humanized mAb H22 binds the human high affinity Fc receptor for IgG (FcgRI), blocks phagocytosis, and modulates receptor expression. J. Leukoc. Biol. 62, 469–479 (1997).
81. Smith, K. G. & Clatworthy, M. R. FcgRIIB in autoimmunity and infection: evolutionary and therapeutic implications. Nature Rev. Immunol. 10, 328–343 (2010).
82. Li, X. et al. A novel polymorphism in the Fcg receptor IIB (CD32B) transmembrane region alters receptor signaling. Arthritis Rheum. 48, 3242–3252 (2003).
83. Kyogoku, C. et al. Fcg receptor gene polymorphisms in Japanese patients with systemic lupus erythematosus: contribution of FCGR2B to genetic susceptibility. Arthritis Rheum. 46, 1242–1254 (2002).
84. Alizadeh, B. Z. et al. Association analysis of functional variants of the FcgRIIa and FcgRIIIa genes with type 1 diabetes, celiac disease and rheumatoid arthritis. Hum. Mol. Genet. 16, 2552–2559 (2007).
85. Harley, J. B. et al. Genome-wide association scan in women with systemic lupus erythematosus identifies susceptibility variants in ITGAM, PXK, KIAA1542 and other loci. Nature Genet. 40, 204–210 (2008).
R E V I E W S
NATURE REVIEWS | DRUG DISCOVERY VOLUME 11 | APRIL 2012 | 329
© 2012 Macmillan Publishers Limited. All rights reserved

86. Weersma, R. K. et al. Association of FcgR2a, but not FcgR3a, with inflammatory bowel diseases across three Caucasian populations. Inflamm. Bowel Dis. 16, 2080–2089 (2010).
87. Fanciulli, M. et al. FCGR3B copy number variation is associated with susceptibility to systemic, but not organ-specific, autoimmunity. Nature Genet. 39, 721–723 (2007).
88. Niederer, H. A. et al. Copy number, linkage disequilibrium and disease association in the FCGR locus. Hum. Mol. Genet. 19, 3282–3294 (2010).
89. Nakamura, G. R., Reynolds, M. E., Chen, Y. M., Starovasnik, M. A. & Lowman, H. B. Stable “zeta” peptides that act as potent antagonists of the high-affinity IgE receptor. Proc. Natl Acad. Sci. USA 99, 1303–1308 (2002).
90. Nakamura, G. R., Starovasnik, M. A., Reynolds, M. E. & Lowman, H. B. A novel family of hairpin peptides that inhibit IgE activity by binding to the high-affinity IgE receptor. Biochemistry 40, 9828–9835 (2001).
91. Rigby, L. J. et al. Monoclonal antibodies and synthetic peptides define the active site of FceRI and a potential receptor antagonist. Allergy 55, 609–619 (2000).
92. Ciccimarra, F., Rosen, F. S. & Merler, E. Localization of the IgG effector site for monocyte receptors. Proc. Natl Acad. Sci. USA 72, 2081–2083 (1975).
93. Ratcliffe, A. & Stanworth, D. R. The use of synthetic g-chain peptides in the localization of the binding site(s) on human IgG1 for the Fc receptors of homologous monocytes and heterologous mouse macrophages. Immunol. Lett. 4, 215–221 (1982).
94. Sondermann, P. & Oosthuizen, V. The structure of Fc receptor/Ig complexes: considerations on stoichiometry and potential inhibitors. Immunol. Lett. 82, 51–56 (2002).
95. Verdoliva, A. et al. A new ligand for immunoglobulin G subdomains by screening of a synthetic peptide library. Chembiochem 6, 1242–1253 (2005).
96. Berntzen, G. et al. Characterization of an FcgRI-binding peptide selected by phage display. Protein Eng. Des. Sel. 19, 121–128 (2006).
97. DeLano, W. L., Ultsch, M. H., de Vos, A. M. & Wells, J. A. Convergent solutions to binding at a protein–protein interface. Science 287, 1279–1283 (2000).
98. Boonyarattanakalin, S., Martin, S. E., Sun, Q. & Peterson, B. R. A synthetic mimic of human Fc receptors: defined chemical modification of cell surfaces enables efficient endocytic uptake of human immunoglobulin-G. J. Am. Chem. Soc. 128, 11463–11470 (2006).
99. Bonetto, S., Spadola, L., Buchanan, A. G., Jermutus, L. & Lund, J. Identification of cyclic peptides able to mimic the functional epitope of IgG1-Fc for human FcgRI. FASEB J. 23, 575–585 (2009).
100. Berntzen, G. et al. Identification of a high affinity FcgRIIA-binding peptide that distinguishes FcgRIIA from FcgRIIB and exploits FcgRIIA-mediated phagocytosis and degradation. J. Biol. Chem. 284, 1126–1135 (2009).
101. Cendron, A. C. et al. An FcgRIIa-binding peptide that mimics the interaction between FcgRIIa and IgG. Mol. Immunol. 45, 307–319 (2008).
102. Pietersz, G. A. et al. Inhibition of destructive autoimmune arthritis in FcgRIIa transgenic mice by small chemical entities. Immunol. Cell Biol. 87, 3–12 (2009).
103. Williams, R. O., Feldmann, M. & Maini, R. N. Anti-tumor necrosis factor ameliorates joint disease in murine collagen-induced arthritis. Proc. Natl Acad. Sci. USA 89, 9784–9788 (1992).
104. Braselmann, S. et al. R406, an orally available spleen tyrosine kinase inhibitor blocks Fc receptor signaling and reduces immune complex-mediated inflammation. J. Pharmacol. Exp. Ther. 319, 998–1008 (2006).
105. Podolanczuk, A., Lazarus, A. H., Crow, A. R., Grossbard, E. & Bussel, J. B. Of mice and men: an open-label pilot study for treatment of immune thrombocytopenic purpura by an inhibitor of Syk. Blood 113, 3154–3160 (2009).
106. Jolles, S., Sewell, W. A. & Misbah, S. A. Clinical uses of intravenous immunoglobulin. Clin. Exp. Immunol. 142, 1–11 (2005).
107. Baerenwaldt, A., Biburger, M. & Nimmerjahn, F. Mechanisms of action of intravenous immunoglobulins. Expert Rev. Clin. Immunol. 6, 425–434 (2010).
108. Ballow, M. The IgG molecule as a biological immune response modifier: mechanisms of action of intravenous immune serum globulin in autoimmune and inflammatory disorders. J. Allergy Clin. Immunol. 127, 315–323 (2011).
109. Viard, I. et al. Inhibition of toxic epidermal necrolysis by blockade of CD95 with human intravenous immunoglobulin. Science 282, 490–493 (1998).
110. Bayary, J. et al. Intravenous immunoglobulin in autoimmune disorders: an insight into the immunoregulatory mechanisms. Int. Immunopharmacol. 6, 528–534 (2006).
111. Crow, A. R., Song, S., Siragam, V. & Lazarus, A. H. Mechanisms of action of intravenous immunoglobulin in the treatment of immune thrombocytopenia. Pediatr. Blood Cancer 47 (Suppl. 5), 710–713 (2006).
112. Debre, M. et al. Infusion of Fcg fragments for treatment of children with acute immune thrombocytopenic purpura. Lancet 342, 945–949 (1993).
113. Siragam, V. et al. Intravenous immunoglobulin ameliorates ITP via activating Fcg receptors on dendritic cells. Nature Med. 12, 688–692 (2006).
114. Kaneko, Y., Nimmerjahn, F. & Ravetch, J. V. Anti-inflammatory activity of immunoglobulin G resulting from Fc sialylation. Science 313, 670–673 (2006).
115. Anthony, R. M., Kobayashi, T., Wermeling, F. & Ravetch, J. V. Intravenous gammaglobulin suppresses inflammation through a novel TH2 pathway. Nature 475, 110–113 (2011).
116. Jefferis, R. Recombinant antibody therapeutics: the impact of glycosylation on mechanisms of action. Trends Pharmacol. Sci. 30, 356–362 (2009).
117. Jefferis, R. Glycosylation as a strategy to improve antibody-based therapeutics. Nature Rev. Drug Discov. 8, 226–234 (2009).
118. Routier, F. H. et al. Quantitation of the oligosaccharides of human serum IgG from patients with rheumatoid arthritis: a critical evaluation of different methods. J. Immunol. Methods 213, 113–130 (1998).
119. Cartron, G. et al. Therapeutic activity of humanized anti-CD20 monoclonal antibody and polymorphism in IgG Fc receptor FcgRIIIa gene. Blood 99, 754–758 (2002).
120. Oflazoglu, E. & Audoly, L. P. Evolution of anti-CD20 monoclonal antibody therapeutics in oncology. MAbs 2, 14–19 (2010).
121. Weng, W. K. & Levy, R. Two immunoglobulin G fragment C receptor polymorphisms independently predict response to rituximab in patients with follicular lymphoma. J. Clin. Oncol. 21, 3940–3947 (2003).
122. Cheung, N. K. et al. FCGR2A polymorphism is correlated with clinical outcome after immunotherapy of neuroblastoma with anti-GD2 antibody and granulocyte macrophage colony-stimulating factor. J. Clin. Oncol. 24, 2885–2890 (2006).
123. Koene, H. R. et al. FcgRIIIa-158V/F polymorphism influences the binding of IgG by natural killer cell FcgRIIIa, independently of the FcgRIIIa-148L/R/H phenotype. Blood 90, 1109–1114 (1997).
124. Weng, W. K., Czerwinski, D., Timmerman, J., Hsu, F. J. & Levy, R. Clinical outcome of lymphoma patients after idiotype vaccination is correlated with humoral immune response and immunoglobulin G Fc receptor genotype. J. Clin. Oncol. 22, 4717–4724 (2004).
125. Farag, S. S. et al. FcgRIIIa and FcgRIIa polymorphisms do not predict response to rituximab in B-cell chronic lymphocytic leukemia. Blood 103, 1472–1474 (2004).
126. Lin, T. S. et al. FCGR3A and FCGR2A polymorphisms may not correlate with response to alemtuzumab in chronic lymphocytic leukemia. Blood 105, 289–291 (2005).
127. de Haij, S. et al. In vivo cytotoxicity of type I CD20 antibodies critically depends on Fc receptor ITAM signaling. Cancer Res. 70, 3209–3217 (2010).
128. Hamaguchi, Y., Xiu, Y., Komura, K., Nimmerjahn, F. & Tedder, T. F. Antibody isotype-specific engagement of Fcg receptors regulates B lymphocyte depletion during CD20 immunotherapy. J. Exp. Med. 203, 743–753 (2006).
129. Lim, S. H. et al. Fcg receptor IIb on target B cells promotes rituximab internalization and reduces clinical efficacy. Blood 118, 2530–2540 (2011).
130. Lazar, G. A. et al. Engineered antibody Fc variants with enhanced effector function. Proc. Natl Acad. Sci. USA 103, 4005–4010 (2006).
131. Burton, D. R. et al. The Clq receptor site on immunoglobulin G. Nature 288, 338–344 (1980).
132. Stavenhagen, J. B. et al. Fc optimization of therapeutic antibodies enhances their ability to kill tumor cells in vitro and controls tumor expansion in vivo via low-affinity activating Fcg receptors. Cancer Res. 67, 8882–8890 (2007).
133. Stavenhagen, J. B. et al. Enhancing the potency of therapeutic monoclonal antibodies via Fc optimization. Adv. Enzyme Regul. 48, 152–164 (2008).
134. Shields, R. L. et al. High resolution mapping of the binding site on human IgG1 for FcgRI, FcgRII, FcgRIII, and FcRn and design of IgG1 variants with improved binding to the FcgR. J. Biol. Chem. 276, 6591–6604 (2001).
135. Albert, H., Collin, M., Dudziak, D., Ravetch, J. V. & Nimmerjahn, F. In vivo enzymatic modulation of IgG glycosylation inhibits autoimmune disease in an IgG subclass-dependent manner. Proc. Natl Acad. Sci. USA 105, 15005–15009 (2008).
136. Lifely, M. R., Hale, C., Boyce, S., Keen, M. J. & Phillips, J. Glycosylation and biological activity of CAMPATH-1H expressed in different cell lines and grown under different culture conditions. Glycobiology 5, 813–822 (1995).
137. Umana, P., Jean-Mairet, J., Moudry, R., Amstutz, H. & Bailey, J. E. Engineered glycoforms of an antineuroblastoma IgG1 with optimized antibody-dependent cellular cytotoxic activity. Nature Biotech. 17, 176–180 (1999).
138. Shields, R. L. et al. Lack of fucose on human IgG1 N-linked oligosaccharide improves binding to human FcgRIII and antibody-dependent cellular toxicity. J. Biol. Chem. 277, 26733–26740 (2002).
139. Shinkawa, T. et al. The absence of fucose but not the presence of galactose or bisecting N-acetylglucosamine of human IgG1 complex-type oligosaccharides shows the critical role of enhancing antibody-dependent cellular cytotoxicity. J. Biol. Chem. 278, 3466–3473 (2003).
140. Yamane-Ohnuki, N. et al. Establishment of FUT8 knockout Chinese hamster ovary cells: an ideal host cell line for producing completely defucosylated antibodies with enhanced antibody-dependent cellular cytotoxicity. Biotechnol. Bioeng. 87, 614–622 (2004).
141. Ferrara, C. et al. Modulation of therapeutic antibody effector functions by glycosylation engineering: influence of Golgi enzyme localization domain and co-expression of heterologous β1, 4-N-acetylglucosaminyltransferase III and Golgi a-mannosidase II. Biotechnol. Bioeng. 93, 851–861 (2006).
142. Ferrara, C., Stuart, F., Sondermann, P., Brunker, P. & Umana, P. The carbohydrate at FcgRIIIa Asn-162. An element required for high affinity binding to non-fucosylated IgG glycoforms. J. Biol. Chem. 281, 5032–5036 (2006).
143. Hodoniczky, J., Zheng, Y. Z. & James, D. C. Control of recombinant monoclonal antibody effector functions by Fc N-glycan remodeling in vitro. Biotechnol. Prog. 21, 1644–1652 (2005).
144. Schuster, M. et al. Improved effector functions of a therapeutic monoclonal Lewis Y-specific antibody by glycoform engineering. Cancer Res. 65, 7934–7941 (2005).
145. van Berkel, P. H. et al. Rapid production of recombinant human IgG with improved ADCC effector function in a transient expression system. Biotechnol. Bioeng. 105, 350–357 (2010).
146. Yamamoto, K. et al. Phase I study of KW-0761, a defucosylated humanized anti-CCR4 antibody, in relapsed patients with adult T-cell leukemia-lymphoma and peripheral T-cell lymphoma. J. Clin. Oncol. 28, 1591–1598 (2010).
147. Sazinsky, S. L. et al. Aglycosylated immunoglobulin G1 variants productively engage activating Fc receptors. Proc. Natl Acad. Sci. USA 105, 20167–20172 (2008).
148. Ward, E. S. & Ober, R. J. Chapter 4. Multitasking by exploitation of intracellular transport functions: the many faces of FcRn. Adv. Immunol. 103, 77–115 (2009).
149. Mezo, A. R., Sridhar, V., Badger, J., Sakorafas, P. & Nienaber, V. X-ray crystal structures of monomeric and dimeric peptide inhibitors in complex with the human neonatal Fc receptor, FcRn. J. Biol. Chem. 285, 27694–27701 (2010).
150. West, A. P. Jr & Bjorkman, P. J. Crystal structure and immunoglobulin G binding properties of the human major histocompatibility complex-related Fc receptor. Biochemistry 39, 9698–9708 (2000).
R E V I E W S
330 | APRIL 2012 | VOLUME 11 www.nature.com/reviews/drugdisc
© 2012 Macmillan Publishers Limited. All rights reserved

151. Stapleton, N. M. et al. Competition for FcRn-mediated transport gives rise to short half-life of human IgG3 and offers therapeutic potential. Nature Commun. 2, 599 (2011).
152. Hinton, P. R. et al. Engineered human IgG antibodies with longer serum half-lives in primates. J. Biol. Chem. 279, 6213–6216 (2004).
153. Dall’Acqua, W. F., Kiener, P. A. & Wu, H. Properties of human IgG1s engineered for enhanced binding to the neonatal Fc receptor (FcRn). J. Biol. Chem. 281, 23514–23524 (2006).
154. Kenanova, V. et al. Tailoring the pharmacokinetics and positron emission tomography imaging properties of anti-carcinoembryonic antigen single-chain Fv-Fc antibody fragments. Cancer Res. 65, 622–631 (2005).
155. Vaccaro, C., Bawdon, R., Wanjie, S., Ober, R. J. & Ward, E. S. Divergent activities of an engineered antibody in murine and human systems have implications for therapeutic antibodies. Proc. Natl Acad. Sci. USA 103, 18709–18714 (2006).
156. Prabhat, P. et al. Elucidation of intracellular recycling pathways leading to exocytosis of the Fc receptor, FcRn, by using multifocal plane microscopy. Proc. Natl Acad. Sci. USA 104, 5889–5894 (2007).
157. Kurlander, R. J. Blockade of Fc receptor-mediated binding to U-937 cells by murine monoclonal antibodies directed against a variety of surface antigens. J. Immunol. 131, 140–147 (1983).
158. Hamerman, J. A. & Lanier, L. L. Inhibition of immune responses by ITAM-bearing receptors. Sci. STKE 2006, re1 (2006).
159. Dunn-Siegrist, I. et al. Pivotal involvement of Fcg receptor IIA in the neutralization of lipopolysaccharide signaling via a potent novel anti-TLR4 monoclonal antibody 15C1. J. Biol. Chem. 282, 34817–34827 (2007).
160. O’Neill, S. K. et al. Monophosphorylation of CD79a and CD79b ITAMs initiates a SHIP-1 phosphatase-mediated inhibitory signaling cascade required for B cell anergy. Immunity 35, 746–756 (2011).
161. Desjarlais, J. R. & Lazar, G. A. Modulation of antibody effector function. Exp. Cell Res. 317, 1278–1285 (2011).
162. Bakema, J. E. et al. Targeting FcaRI on polymorphonuclear cells induces tumor cell killing through autophagy. J. Immunol. 187, 726–732 (2011).
163. Bakema, J. E. & van Egmond, M. Immunoglobulin A: a next generation of therapeutic antibodies? MAbs 3, 352–361 (2011).
164. Sondermann, P., Huber, R. & JacobCrystal, U. Structure of the soluble form of the human Fcg-receptor IIb: a new member of the immunoglobulin superfamily at 1.7 Å resolution. EMBO J. 18, 1095–1103 (1999).
165. Harris, L. J., Larson, S. B., Hasel, K. W. & McPherson, A. Refined structure of an intact IgG2a monoclonal antibody. 36, 1581–1597 (1997).
166. Zhao, W. et al. FcgRIIa, not FcgRIIb, is constitutively and functionally expressed on skin-derived human mast cells. J. Immunol. 177, 694–701 (2006).
167. Kepley, C. L. et al. Co-aggregation of FcgRII with FceRI on human mast cells inhibits antigen-induced secretion and involves SHIP-Grb2-Dok complexes. J. Biol. Chem. 279, 35139–35149 (2004).
168. White, A. L. et al. Interaction with FcγRIIB is critical for the agonistic activity of anti-CD40 monoclonal antibody. J. Immunol. 187, 1754–1763 (2011).
169. Wilson, N. S. et al. An Fcγ receptor-dependent mechanism drives antibody-mediated target-receptor signaling in cancer cells. Cancer Cell 19, 101–113 (2011).
AcknowledgementsThe authors thank J. Stubbs, A. Gavin and J. Cambier for their editorial assistance and scientific advice, and B. Wines and M. Powell for helpful suggestions. P.M.H. is supported by a National Health and Medical Research Council (NHMRC) Senior Principal Research Fellowship, project grants and the Victorian Operational Infrastructure Grant Scheme.
Competing interests statementThe authors declare no competing financial interests.
FURTHER INFORMATIONP. Mark Hogarth’s homepage: http://www.burnet.edu.au/staff_members/182_mark_hogarthGeoffrey A. Pietersz’s homepage: http://www.burnet.edu.au/centres/2_centre_for_immunology/working_groups/12_bio-organic_and_medicinal_chemistry
ALL LINKS ARE ACTIVE IN THE ONLINE PDF
R E V I E W S
NATURE REVIEWS | DRUG DISCOVERY VOLUME 11 | APRIL 2012 | 331
© 2012 Macmillan Publishers Limited. All rights reserved