Embed Size (px)
Citation preview

The Robert Jones and Agnes HuntOrthopaedic and District Hospital
NHS TrustNHS Trust
Annual Report 2008/09
A first classhospital doingexcellent work
“”

ii
All patient comments in this report are taken frompatients questioned as part of the NationalAnnual Inpatient Survey (Care QualityCommission) which took place between July andSeptember 2008.
The hospital’s Medical Photography andIllustration Department kindly provided all thephotographs used in the report.
Cover photo shows our representative staff L- R
Pauline Rudd, Head Cook
Paul Harrison, Principal Clinical Scientist, Oscell
Helen Yarnold, Staff Nurse, Kenyon Ward
Anwen Evans, Occupational Therapist
Keith Miller, Design and Development Engineer,ORLAU
Linda Butler, Recovery Dept Manager
Back cover photo shows our representative staff L- R
Glen Whitehouse, Radiographer, X Ray Dept
Harriet Egerton-Davies, Medical Secretary
Simon Vernon, Porter
Amy Chana, Physiotherapy
Adrian Davies, Estates
Nichola Wynstanley, Housekeeping
Dr. Siddalingaprabhu Katti, Anaesthetics andTheatres
The Robert Jones and Agnes Hunt Orthopaedic and District Hospital NHS Trust
This was the mostpositive experience I have had of any stay in hospital.
“
”
Mr David Jaffray, Consultant Orthopaedic and Spinal Surgeon, with the new hospital flag

1
The Robert Jones and Agnes Hunt Orthopaedicand District Hospital NHS Trust (RJAH) is one ofthe country’s leading orthopaedic hospitals. Our surrounding geographical area includesShropshire, Wales, Cheshire and the Midlands.
A specialist hospital with a world-wide reputationfor innovation and research, the Trust treatsdisorders of bones, joints and muscles in adultsand children, locally, nationally andinternationally.
Annual Report 2008/09
About Us
1. Chairman’s Introduction and Chief Executive’s Report 2 - 3
2. Supporting our Patients and their Environment 4 - 6
3. Developing Services for the Future 7 – 9
4. Developing our Workforce 10 -12
5. Performance 13 - 14
6. Finance Report 15
7. Trust Board and Structure 28
8. Contacts 29
Contents
Entrance Sign -The hospital signs are now in English and Welsh
2 The Robert Jones and Agnes Hunt Orthopaedic and District Hospital NHS Trust
Russell Hardy, Chairman
This has been an exceptional year for the Trust. Ina year of considerable change and challenge wehave been able, as a team, to continue to makeprogress on our key objectives of deliveringoutstanding patient care and improving ourfinancial viability. As in 2008, we have been votedby our patients to be amongst the very besthospitals in the UK for 2009. This reflects thequality of care and outcomes from our medical,nursing and healthcare professional teams, aswell as support organisations such as TheLeague of Friends and facilities staff. We havealso had another strong year in maintainingconsistently low infection rates. Again we had nocases of MRSA in 2008/09 and very low numbersof C-Difficile. These results reflect oureffectiveness at focusing on what is important toour patients and working as a team to deliver totheir satisfaction and our own high standards.
The focus we put into delivering outstandingpatient care is only possible by us continuing toimprove our financial performance. By becomingfinancially robust, we are able to reinvest inimprovements in facilities, staff training andpatient care. In 2008/09 we were able to make afinancial surplus of £1m whilst investing over £3min new facilities.
Our success reflects both the individual andcombined efforts of those within the Trust andbeyond. I would like to thank all our medical,nursing, healthcare professional and supportteams for their ongoing commitment and hardwork to deliver outstanding patient care. TheExecutive Team, led by Wendy Farrington-Chadd,has worked extremely hard to support our frontline teams and to implement and oversee thechange programmes during the year. The Non-executive Directors have given considerable timeto supporting the Trust and I would particularlylike to thank Professor Robert Tinston for histenure as Chair. Finally thanks are due to ourfriends and colleagues in the local HealthEconomy who continue to support us as wefurther develop your Hospital to its full potential.
2009/10 will see us continue to focus on ourpatients and improve our services to them. Wewill also be commencing the journey to become aFoundation Trust and, as we do so, will proudlycommunicate what makes the Robert Jones andAgnes Hunt such a special organisation.
1. Chairman’s Introduction

3Annual Report 2008/09
My second year as Chief Executive at RJAH hasbeen a fantastic year for the hospital. As anorganisation, we have moved forward in manyareas and we are now well placed to developour vision and direction for the future.
We have maintained our commitment to providethe highest quality care for patients from thesurrounding areas within Shropshire, North andMid Wales, but also from Cheshire, theMidlands, even nationally for some of the veryspecialist care we provide. I am continuallyimpressed and heartened by the huge numberof positive letters we receive, thanking thehospital for the high quality care received fromour highly skilled clinical and support staff, thehigh standards of food, and the cleanlinessmaintained by our housekeeping staff, who areintegral to the ward teams and to quality care provision.
We have continued to monitor our patients’experience of their stay in hospital and for thelast year over 95% of our patients rated the careand treatment they received as excellent - this level of satisfaction would be high in anyservice sector and for a hospital iscommendable. During 2008/09 we were the
highest scoring hospital in England, from theNational Inpatient Survey, and were voted ‘BestHospital’. Our patients are our final arbiter;what they say about their experience is the mostimportant measure. On all counts we heard‘excellent’. These results were a real boost forall our staff and were particularly welcome asthey came at a time when the hospital’s futurewas uncertain.
The last year has been challenging for the Trustin terms of the delivery of key targets – we havemoved during the year from the bottom quartileof performance against our 18 week treatmenttargets for England, to achieving over 95% ofpatients being treated within 18 weeks. For ourWelsh patients, we have achieved the required26 week treatment target, again showing hugeimprovements. This has been achieved throughincreasing the number of patients we treat –over 20% more surgical operations have beenperformed in the last year.
In undertaking this increased level of activity,managing our finances has been particularlyimportant. The Trust has for the second yeardelivered a £1m surplus – this surplus has beenrequired to repay a loan from 2006/07 when the
Wendy Farrington-Chadd, Chief Executive
Chief Executive’s Report
Trust was in deficit – our underlying financialposition has now improved to a level whereeffectively we have been able to repay ourloan commitment in full, one year ahead ofplan. This has all been achieved at thesame time as delivering a £3.4m CostImprovement Programme which has beencrucial to support our longer termsustainability. Achieving improvement tothis degree has meant significant changesand I appreciate changes have beendifficult in many areas; again I have beenimpressed at the commitment to worktogether to find solutions to move thehospital forward and make progress. It isthis progress which has meant we are nowin a much stronger position to determineour own future and direction.
In terms of quality and standards, 2008/09has again shown extremely highperformance – for the second successiveyear we have recorded no MRSA in thehospital. Our levels of Clostridium Difficileremain very low compared to otherhospitals and we have recorded sevencases in the last year. Our post surgicalinfection rates have remained amongst thelowest in the UK, an important qualityindicator for patient outcomes.
As Chief Executive I was very consciousthat 2008/09 would be a challenging year;the challenges were great and we have allresponded to a degree which selfdemonstrably shows a fantasticachievement for everyone at Oswestry. Iwould like to extend real thanks to all staffworking in the hospital at every level – it isthe team approach that makes RJAHspecial and the whole hospital hasdelivered far beyond any expectations. Weare now well placed to progress our plansfor the future, to develop as an NHSFoundation Trust and I look forward, withthe Executive Team, to working with all staffto take the hospital into the next excitingphase of its continuation as a leadinghospital in the UK.
4 The Robert Jones and Agnes Hunt Orthopaedic and District Hospital NHS TrustThe Robert Jones and Agnes Hunt Orthopaedic and District Hospital NHS Trust
Members of the Patients’ Panel with their poster at the 2008 Involvement to Impact AwardsReleasing Time to Care programme – Our Patient Status at a Glance board
Patient Survey
The 2008 Healthcare Commission’s InpatientSurvey again put the hospital amongst the topNHS Trusts in England. On four questions;confidence in doctors, clear medicationinstructions, minimal delay to discharge andhospital food, the Trust scored a higher scorethan any other Trust in England. The responserate was 71% with over 600 patients returningcompleted questionnaires sent to randomlyselected patients.
The survey highlighted many positive aspects ofthe patient experience with patients reportingexcellent scores in:
Overall rate of care received Confidence in nurses Answers from doctors and nurses thatpatients could understandSafety from other patients and visitors Involvement in discharge arrangementsChoice of food Cleanliness
Involving Patients
The Trust is in its second year of workingdirectly with patients to help the hospital and itsstaff to improve services. The Patients’ Panelincludes past and present patients as well asinterested members of the public who havebeen involved in practical work to improve the
patient experience when they visit theOrthopaedic hospital.
The Patients’ Panel has gathered feedback frompatients in the form of stories and diaries abouttheir experiences to help implement change andimprovements in all hospital departments. ThePanel has also joined Trust Board members totake part in the Observations of Careprogramme by observing patients and staff inclinical areas. A number of theirrecommendations have been implemented andthese have led to a better environment,improved clinical practices and more effectivecommunications.
This work was recognised in November 2008when the hospital was one of five organisationsshortlisted for an Involvement to Impact Awardorganised by The NHS Centre for Involvement.
The Patients Panel gave feedback on the2007/08 Annual Report and theserecommendations have now been included,along with the suggestions made by peopleattending the Trust’s Annual General Meeting.
Clean and Safe
The Trust prides itself on its record low levels ofinfection, with no cases of MRSA being reportedfor the third consecutive year and seven casesof Clostridium Difficile (C Diff) reported sinceApril 2008.
2. Supporting our Patients and theirEnvironment
This is an excellenthospital. The overallimpression was of a clean,well organised hospitalwith their dedicated staff.
“
”

5Annual Report 2008/09
New members of the Trust estates team, Estates Managers Dave Thomas and Nick Huband
Senior Physiotherapist Pauline Holbrook with patient Paul Fowler undergoing neuro-rehabilitationin the Pennill Therapeutic Pool, which was funded by the League of Friends
Following a spot inspection by the HealthcareCommission in September 2008, the Trustreceived some recommendations and hasworked on all areas of the HealthcareCommission Hygiene Code to ensure that clinicalstandards are improved, so that the hospitalmaintains its very low infection rates.
The Trust Executive team has undertaken randomchecks to ensure that the required standardsremain in place and have supported the purchaseof additional equipment to improve infection,prevention and control. The Trust has beenbenchmarked with other hospitals and has askedleading experts to advise on certain aspects toensure that we can be leading edge with ourpractices.
Greening the Environment
Greening the Environment is a Government-wideagenda to ensure that sustainable developmentconsiderations permeate all policies. In the NHS,this is focused on the operation and developmentof the service and estate.
A survey of the hospital estate has been takingplace during the last 12 months reviewingenvironmental management, physical condition,fire, health and safety compliance, functionalsuitability, space utilisation and quality.A sustainable energy strategy is part of our fiveyear site development plan and the long termestates strategy.
The hospital takes an innovative approach toenergy saving. Commission Air – a digital aerialimagery company are undertaking a thermalsurvey of the whole site to highlight any hotpots.In 2008 the Trust successfully bid to theDepartment of Health Energy and SustainabilityFund and was granted almost £400,000 toinstall boiler economisers as well as energy andthermal insulation. As part of the hospital’sEnergy Strategy, the Trust has invested £80,000in window replacements and energy efficientlighting schemes.
Emergency Planning
In 2007/8 the Trust carried out a table-top test ofits major Incident plans. Following this, the Trusthas updated its Major Incident Policy in2008/09, which now includes Pandemic Fluplans as well as plans for business continuityand responding to a major Incident. The policyis compliant with the requirements of the NHSEmergency Planning Guidance 2005 and allassociated guidance. The Trust Board approvedthis in November 2008 and has carried outtraining and awareness sessions, followed by a“live test” of the plans in March 2009 inconjunction with the PCT emergency planningofficer.
The personal care wasexcellent. The hospitalspotlessly clean. Staff
worked hard on thecleaning side. The food
was plentiful, a goodchoice and served hot.
“
”

Compliments, Comments andComplaints
Patient comments cards are completed by patientsto report their inpatient and outpatient experiences.These are collated and analysed by the PatientAdvice and Liaison Service (PALS) Officer. In2008/09, over 93% of these ranked staff, food,hygiene and the hospital wards as excellent orgood.
The Trust received 78 complaints in 2008/09,which all received an acknowledgement within thenational target of two working days and 88%received a full written response within the nationaltarget of 25 working days. Where this was notpossible, an interim response was sent.
The Trust’s procedure for handling complaintscomplies with the guidance set out by theParliamentary and Health Service Ombudsman in‘The Principles for Remedy’. All complaints areinvestigated thoroughly to ensure that lessons arelearnt and changes in practice implementedaccordingly. Complaints are discussed as part ofa patient experience report at committees involvingpatient representatives.
From 1st April 2009, new national regulations willaim to resolve complaints in a more personal andpositive manner, ensuring that organisations makethe most of opportunities to learn and improve.
Serious Untoward Incidents
During 2008/09 there were no serious untowardincidents, which require reporting.
The Trust’s Serious Untoward Incident ReportingPolicy has been reviewed to bring it in line with therecently revised Strategic Health Authorityguidance. The policy for investigating seriousuntoward incidents has been revised to ensure amore robust process and thorough root causeanalysis, to allow lessons to be learned in order toprevent recurrence of similar incidents.
Direct Booking
All patients attending outpatient appointments whorequire surgery are now able to agree datesstraight after clinic for their pre-operativeassessment and operation. More than 85% ofpatients are using this facility which is being rolledout across the hospital.
David James, Director of Operations, said: “Wehave made significant progress in reducing waitingtimes for patients. The booking process allows thepatient to agree a provisional date for surgery attheir convenience. This enables the patient toorganise their lives around the operation andreduce their anxiety by knowing what will happenand when.”
League of Friends
The new look League of Friends Summer Fete washeld in conjunction with the Hospital Open Day in2008 and was a major financial success beating allprevious records.
Staff joined in the activities by providing visitorswith the opportunity to look behind the scenes insome departments including X-ray, spinal injuriesand research. Partner organisations such asuniversities and Shropshire County Primary CareTrust’s Health Promotion team were on hand toanswer questions about careers in health, whilstTrust staff encouraged school children to askquestions about the hospital and working for theNHS. The event raised £14,600, an increase ofalmost £3,000 on the previous year. A highlysuccessful sponsored walk around the hospitalgrounds on the same day organised by Professorof Orthopaedics James Richardson and his staffraised an additional £4,930.
Also during 2008, the League shop on thehospital’s main corridor raised £23,000 profit andthe coffee shop, £26,100. League branchesthroughout Shropshire, Mid and North Wales alongwith the Oswestry Rheumatology Associationbranch raised a total of £45,846. Memberscontinue to promote the work of the Trust topeople living in the catchment area of thebranches and beyond.
Various voluntary organisations continue to help inthe Trust in association with the League of Friends.These include the Flower Guild, the PatientsLibrary, the Help Desk, the British Red CrossTherapeutic Care Service, the Spinal Injury FeedingScheme, the Coffee Shop and trolley services andthe Disabled Swimming Club. The dedicated workcarried out by volunteers greatly enhances theexperience of all the hospital’s patients.
During the year the League spent £93,791 onhospital projects. Examples include theDepartment of Pathology, which receivedFluorescent In Situ Hybridisation (FISH) tumouranalysis equipment (£50,000) and a further£15,000 for pain relief pumps was donated to thehospital.
6The Robert Jones and Agnes Hunt Orthopaedic and District Hospital NHS Trust
During my stay in thehospital, I could find noreason for criticism of anysort. Treatment, staff, foodand atmosphere, etc weremore than satisfactory forwhich I was sincerelythankful.
“
”
“I felt in very safe hands atall times.”
“”

7Annual Report 2008/09
An exhibition for staff about the sustainable services work
Sustainable Services
The Trust launched a project called SustainableServices at the beginning of the year. Thepurpose if the project was to reduce waiting timefor patients, increase efficiency and, wherepossible, reduce expenditure. As a result, theTrust has developed plans to progress theorganisation in a sustainable way that form thebasis of moving the organisation forward into thenext few years.
The following are some examples ofimprovements made at the Trust during the last12 months.
Admit on the Day of Surgery
Patients requiring a hip or knee replacement aregiven the option of being admitted on the sameday of surgery rather than coming into hospitalthe night before. This has been enabled thanks tothe introduction of an enhanced one day pre-operative consultation which patients attend sixweeks prior to surgery.
At the consultation, in addition to undergoing theusual clinical tests to ensure patients are fit forsurgery, they also meet a member of the
anaesthetic team to discuss choices ofanaesthesia and receive information to makethem more aware of their operation, theirrehabilitation and discharge arrangements.
This new service has proved a hit with patientswith extremely positive feedback from thoseinvolved.
Rapid Rehabilitation Programme
A number of patients at the Trust are now able togo home just one day after undergoing a hipreplacement following the introduction of newanaesthetic and pain relief combination.
The rapid rehabilitation regime was introduced atthe hospital in December 2008 with only patientssuitable for the new anaesthetic going ahead. Thebreakthrough development is being led by DrJohn C John, Consultant Anaesthetist. He said:“To make the stay in hospital so short, theanaesthetic used is designed for quick recovery.Traditional pain relief methods have involvedusing sedative drugs, like morphine which leavesthe patient groggy and sick or nerve injectionwhich make legs feel heavy and prevent walking.”
3. Developing Services for the Future
The staff were all friendlyand helpful. The team
work was excellent witheveryone’s role respected
and valid from theconsultant to the cleaning
and catering staff.
“
”

8 The Robert Jones and Agnes Hunt Orthopaedic and District Hospital NHS Trust
Mr Len Cater of Shrewsbury who underwent hip replacement surgery was the first patient toundergo the new rapid rehabilitation programme and was happy to go home the following day.
The majority of patients are now admitted for majorsurgery on the same day as their operation.
The new technique involves injecting largevolumes of local anaesthetic directly into the siteof the operation. The surgeon then places asmall tube in the operation site which isconnected to a pump and continues to provideanaesthetic for the first 24 to 48 hours. The tubeis removed by the nurse before leaving hospital.
Innovative Mobile Service forPatients
An innovative intravenous service for patientswith osteoporosis and Paget’s disease wasintroduced by the hospital during 2008/09. Withthe support of Shropshire County PCT, the pilotproject has reached patients in outreach clinicsat hospitals in Telford, Shrewsbury and Ludlow.
Consultant Dr Michael Davie and his team havebeen providing an intravenous service forpatients with metabolic bone disease for anumber of years. These patients havehistorically received their treatment as either in-patients, needing to stay in hospital for three toseven days or more recently as day caseswhere patients may need to stay for six hours.
The mobile service brings the services closer topatient’s homes, therefore reducing travel andinconvenience for patients, many of whom areelderly. The pilot, which ran between February2008 and May 2008, was received so well bypatients that the PCT agreed to extend theservice.
New Trial to Treat Rare GeneticDisorders
RJAH is one of just three hospitals in the countryto lead the way with a new treatment aimed atovercoming the underlying genetic problem inDuchenne Muscular Dystrophy (DMD).
DMD is caused by faults in genes which causeprogressive muscle weakness because musclecells break down and are gradually lost. Itaffects only boys who develop the first signs ofdifficulty in walking between the ages of oneand three. Oswestry is one of just three centresin the UK participating in this international trialwhich could see a real improvement in thequality of life of some of our young patients andtheir families.
The hospital has worked with the NationalMedicines for Children’s Research Network toguarantee its involvement in the trial, which willtake place over the next two years.
Spinal Care
A new set of interventions to avoid furthercomplications for critically injured patients,developed from collaborative research at theMidlands Centre for Spinal Injuries (MSCI) andthe North West Midlands Critical Care Network,was shortlisted for a Nursing Times 2008 Award.
The main focus areas of the spinal care bundleare management of the acute spinally injuredpatient, spinal clearance (where the patient iscarefully checked for having no spinal injury)and referral to specialist care from Critical Careand Acute Trauma Units. This development is inline with Lord Darzi’s recommendations forimproving quality of care and reducing length ofstay in hospital.
The Spinal Injury Care Bundle was developedby consultant nurses Alison Lamb and NickiBellinger and was nominated in the NursingTimes category of innovative and quality care.
In September 2008 Director of MCSI, Wagih ElMasri was elected President of the International
I have been attending this hospital every six months for thelast 10 years for treatment for mybrittle bones, I can only repeatthat I find this hospital and itsstaff one of the best in thecountry. I can’t praise it enough.
“
”
Understanding ofspinal injury wasexcellent and careprovided was veryspecialist.
“
”

9Annual Report 2008/09
Spinal Care Bundle Nursing Times Award Nominationfor Consultant Nurses Alison Lamb and Nicki Bellinger The new TORCH Building which was completed in 2008.
Spinal Cord Society (ISCOS), which aims topromote understanding, share knowledge andset standards about all aspects of managementrelated to spinal injury.
Developing Research Strategy
Through the Trust’s Medical Director, hospitalclinicians work closely with the Institute ofOrthopaedics, a national charity on-site and akey business partner which funds research inseveral research centres and departments andthe School of Postgraduate Medicine of KeeleUniversity.
Some of the recent key developments havebeen in stem cell therapy for a range of clinicalapplications and in neuromuscular work wherethe Wolfson Centre for Inherited MuscularDisease (CIND) has now been recognised as aMuscle Centre by the Muscular DystrophyCampaign. The Oswestry Outcome Centre isinvolved in a number of clinical trials, one beinga 10 year study of the outcomes of a hipprosthesis.
The Orthopaedic Research forChildren (TORCH) Centre
The TORCH building was completed in summer2008 and is a unique centre dedicated to thecomprehensive assessment of children withmobility problems, with an emphasis onfamilies, help, research and knowledge.
TORCH is home to existing specialist centres ofOrthotic Research and Locomotor AssessmentUnit (ORLAU) and CIND as well as providingresearch facilities for the hospital.
David James, Director of Operations andDevelopment, said: “The new state of the art
building that TORCH provides brings thefacilities up to the same standard as the clinicalexpertise we provide and has improved ourpatient’s experience in hospital.”
Staff transferred to the new building in 2008 andthe building will be formally opened duringsummer 2009.
Our Vision is to be:
“ The leading centre for highquality, sustainable Orthopaedicand related care, achievingexcellence in both experience and outcomes for our patients ”
Our Strategic Aims which underpin the visionstatement are:
To be the provider of choice for patientsrequiring orthopaedic care through theprovision of safe, effective, high quality care.To develop a vibrant and viable organisationwhere people achieve their full potential andwhere, as we move forward and continue todevelop as an NHS Foundation Trust,success leads to investment in services forpatients.To improve access to our services andensure that everyone, no matter where theyare from, is seen quickly and treated aseffectively as possible.
We are currently developing our plans for NHSFoundation Trust status, which we believe willprovide an important platform from which wecan further develop the hospital. We will consulton these proposals during 2009/10.
Fantastic. I have anew lease of life.
“”
The opportunity to discussall aspects of my treatment
before entering the hospital,the surgery itself and the
advice and practicefollowing the operation were
all first class.
“
”

10 The Robert Jones and Agnes Hunt Orthopaedic and District Hospital NHS Trust
Andrew Biggs graduated with the highest mark in the country, picking up adistinction in his degree in Medical Illustration during 2008/09. Medical
Illustrator Andy, who began working for the Trust as a YTS Trainee in 1985,pictured at his graduation ceremony at Glasgow Caledonian University.
Our Staff and What They Say AboutRJAH
At the end of March 2009 the Trust employed960 whole time equivalent (WTE) staff, of whichover 60% work in direct patient care areas.9.34% of staff left and 85 WTE new staff joinedthe Trust during the year.
*Medics – this term refers to doctors in trainingsuch as specialist and specialty registrars, nonconsultant Grade Clinicians, such as Staff Gradeand Associate Specialists, and non training TrustGrade doctors.
The Trust has recently been given the greenlight for successfully implementing the coreelements of the national electronic staff recordsystem.
Consultation with staff occurred with the StaffSurvey. The survey published during this year,undertaken at the end of 2007, showed some ofthe following significant changes from theprevious year:-
Improvements in the number of appraisalsundertaken and those with personaldevelopment plans Increases in the number of staff attendinghealth and safety trainingImprovements in the number of errors, nearmisses or incidents reportedDecrease in the number of staff workingextra hoursIncrease in the work pressure felt by staffIncrease in the reported number of staffexperiencing harassment, bullying or abusefrom other staffIncrease in the number of staff reportingsupport from immediate managers
4. Developing our Workforce
Nursing
Medics*
Managers & Senior Managers
Healthcare Scientists
Healthcare Assistants and other support staff
Consultant
Allied Health Proffesionals
Admin & Estates
Skill, kindness and care willalways remain in my mindwhen I recall my stay on thetwo occasions in thiswonderful hospital.
“
”
Seven members of nursing staff graduated from Staffordshire University this year, L-R Glenna Hardy,Ita Arkinson, Helen Smith, Dawn Harris and Wayne Evans, with Julie Huxley and Michael Dean notavailable for the photograph

11Annual Report 2008/09
A Ban Bullying at Work event was held for staff
The Trust publishes a monthly staff newsletterfor staff called Communic@te. Ad hoc bulletinsand messages from the Chief Executive arealso sent to all staff. The Trust Core Brief isproduced after each Board meeting and this iscascaded down within the organisation.
Staff attendance levels
The average sickness absence level throughoutthe year in the Trust was 4.21%. This varied fromthe previous year by an increase of 0.16 %.
Specific attention has been paid to those areaswith continually high trends. Planning andreview meetings have taken place and proactiveaction identified. This has also included anoccupational working group identifying areaswhere follow up action is required across theTrust, such as stress risk assessments.
The Network of Staff Supporters (NOSS) havecontinued to provide a responsive staff supportand counselling service throughout the year.This has included a regular training programmewith sessions such as Stress Awareness andManaging Difficult People.
Equality and Diversity
In putting the diverse needs of our service usersand employees at the forefront, it is essential
that the Trust continues to recognise the rightsof all patients and staff to be treated fairly andconsiderately in accessing services andemployment, irrespective of their age, gender,marital status, religious belief, ethnicbackground, nationality, sexual orientation,disability or social status.
The Trust showed its commitment to equalityand diversity during 2008/09, with the approvalof its updated Dignity at Work Policy whichpromotes a new approach to eliminatingbullying and harassment at work. The newpolicy, supported by the Trust Board, introducesa role of the confidential mediator, to work withall parties to resolve matters at an informal level.
In July 2008, the Trust held a very successful“Equality and Diversity Learning and AwarenessJourney” to celebrate cultural and religiousdifferences and raise awareness about equalityand diversity issues. The event provided anopportunity for over 400 people to learn aboutother communities and to forge links with bothlocal and national ethnic and diverse groups.The Trust encouraged local people to join staffin this celebration of differences and staff wereon hand to explain the Trust’s Equality andDiversity Strategy. Representatives from thehospital unions and hospital chaplaincy werepresent, as well as PALS.
Nurses were discreet andrespectful about yourdignity and privacy.”
“
”

12 The Robert Jones and Agnes Hunt Orthopaedic and District Hospital NHS Trust
Student Nurses at the Equality and Diversity Day which attracted over 400 people
This work was acknowledged by the NursingOfficer for Diversity at the Department of Healthwho advised that she was “extremely impressedwith the significant work that has beenundertaken in taking forward equality anddiversity and embedding the process within theprovision of care at the Trust”. In the last 12months, the Trust has taken the lead inestablishing the Shropshire NHS Equality andDiversity Forum, a cross-county NHS trustpartnership working group.
The Trust continues to implement therecommendations of the DisabilityDiscrimination Audit and has improved physicalaccess to the hospital site, which means theconstruction of appropriate ramps and tactilesurfaces as well as improving the signage for alldepartments. The Trust has also increased thenumber of available parking spaces for use bydisability badge holders. Additionally, we havebeen reaccredited with the two tick disabilitysymbol and promote and deliver equality anddiversity awareness training to staff on anannual basis.
The Trust’s employment policies are compliantwith the equality and diversity legislativerequirements and the Trust encourages flexibleworking and equality of opportunity at all levelswithin the organisation and publishes data tosupport this.
What struck me above all else was the way that the doctors andconsultants knew all the other staff,including domestic staff, and theway there seemed to be completeco-operation between members ofstaff. All in all staff are very friendlyand thoroughly professional.”
“
”
13Annual Report 2008/09
Patients Panel:Back row – Alison Harper, PALS Officer and Panel members, Sheila Ashley and Jenny RoughsedgeFront row – Paul Harris, patient & Montgomery Community Health Council, Dorothy Scholfield, panel member, Vicky Morris (Chair) Director of Nursing and Governance and FrejaEvans Swogger panel member.
Key Performance Indicators
2008/09 has been a successful year for theTrust in which we have continued to deliver safe,effective, high quality care and our patientshave rated us at the very highest levels ofsatisfaction.
We have treated more patients in thehospital than in any previous year and haveachieved our waiting list targets for Englishand Welsh commissioners.We have delivered this record level of patientactivity and have achieved a financialsurplus for the second successive year,reducing our support requirement from theStrategic Health Authority (SHA).
In 2008/09 there have been significant changesto our organisational structures and to ourworkforce which have included;
Increases in staffing establishment withinTheatres to achieve extended hours ofservice provision through new rotas, plannedfor introduction in 2009. Reduction of the overall ward bed base,achieved through shorter lengths of stay andimproved bed utilisation.
All Consultant Job Plans have been reviewedto ensure maximum utilisation of expertiseand clinical sessions in line with servicerequirements and to ensure consistency.
During the year the Trust also appointedadditional consultants specialising in Foot &Ankle, Arthroplasty, Spinal Injuries andAnaesthetics.
Performance against the range of nationalperformance indicators relevant to the Trust wasexcellent during 2008/09:
Quality and Infection
During 2008/09 the Trust has maintained its veryhigh standards in relation to hospital acquiredinfections with:
No cases of MRSA Bacteraemia for asecond successive yearA total of seven cases of C Difficile against atarget ceiling for the year of nineAmongst the lowest levels of Surgical SiteInfection (SSI) rates in the country.
5. Performance
Treatment for the condition was very quick and effective
“
”

14The Robert Jones and Agnes Hunt Orthopaedic and District Hospital NHS Trust
How Many Patients We Treat
Activity levels were higher in 2008/09 than in2007/08 across all categories, as the tablebelow illustrates:
Waiting Times
This is a key area of achievement. Last year thehospital was seeing just 40% of its admittedpatients within 18 weeks against a milestonetarget of 85%. This was the worst performancenationally at that time. Performance for non-admitted patients was 83% against amilestone target of 90%. In the last 12 monthsthe Trust has turned around performanceagainst the 18 week target with sustainedperformance at the end of March 2009 of 90%for admitted patients, which it first achieved inNovember 2008
Similarly, improvements have been madeagainst the Welsh target of 26 weeks and theTrust was meeting the milestones of 80% foradmitted and 85% for non-admitted patientsfrom Welsh purchasers by 31 March 2009.
Quality Accounts
From April 2010 all healthcare providers workingfor the NHS will be legally obliged to publish"quality accounts" on safety, patients’experience, and clinical outcomes, in the sameway that they publish financial accounts.
The Trust Board and sub committees arereviewing clinical measurement methods tobuild on the clinical measures already beingcaptured within the hospital. The work in2008/09 will contribute towards an agreed set ofclinical indicator metrics which will be monitoredand reported in the 2009/10 Annual Report.
Type 2007/08 2008/09 Comparative Variance
First Outpatient (OP) attendance 22,152 24,274 +9.6%
Total OP attendances 66,868 71,762 +7.3%
Planned finished consultant episodes (FCEs) - mainly hospital stays 13, 099 14,379 +9.8%
Emergency FCEs 1013 1042 +2.9%
2008/09 Activity compared with previous year
I felt that all staffwere exceptionallyprofessional andcaring althoughextremely busy.
“
”

15Annual Report 2008/09
Financial Performance
We have made tremendous progress this year instabilising our underlying financial position. At thestart of the year, we reported a £4m underlyingfinancial deficit that it was planned to ‘bridge’ by acombination of cost improvements and nonrecurrent financial support.
Demand for our services continued to grow withan increase of around 10% in the overall numberof inpatients receiving treatment at our Hospital.The additional income generated from this workcombined with more efficient ways of deliveryhave made it possible for us not only to achieveall of our statutory financial duties but have alsoallowed us to generate a reserve that will coverour future loan repayment obligations. This ineffect amounts to the Trust having repaid all of ouroutstanding loans a year ahead of schedule.
As a result of the achievements made in the year,the financial outlook for 2009/10 looks brighterand we welcome the fact that the new nationaltariff better rewards specialist work undertakenand better recognises the complexity of the workdelivered at the Trust.
With the downturn in the economy almost certainto lead to future cuts in public spending, it isessential that we continue to build upon theefficiencies identified to date as we plan for thelong term future of our hospital.
Detailed Performance against NHSStatutory Duties
i. Break Even duty
The operating surplus is used in calculatingperformance against our break even duty.The Trust achieved a gross operating surplus(before impairment) of £1.151m, against atarget of £1.134m. This ensured we were ableto meet our statutory loan repaymentobligations.
ii. To achieve a Capital CostAbsorption rate of 3.5%
The Trust achieved a rate of 3.8%, which iswithin the tolerance limit of 0.5% allowed bythe Department of Health. The overachievement was due to actualFixed Asset values being lower thanestimated when the dividend was set.
iii. To operate within the ExternalFinancing Limit (EFL) whichcontrols the level of externalfinance the Trust may access.
The Trust kept its borrowing within itsstatutory limit.
iv. To operate within the CapitalResource Limit (CRL) whichcontrols the level of capitalexpenditure the Trust may incur.
The Trust contained its net capitalexpenditure within its limit of £2.796m
In addition, the Better Payment Practice Coderequires that undisputed invoices are paid by thedue date or within 30 days of receipt of theinvoice or goods, whichever is later. Both 98% ofNon-NHS and NHS invoices by value were paidwithin this time, which exceeds the target of 95%.The Trust also looked to pay local suppliers within10 days of receipt of invoice to support themduring the current economic climate.
6. Finance Report
Operating & Financial Review 2008/09
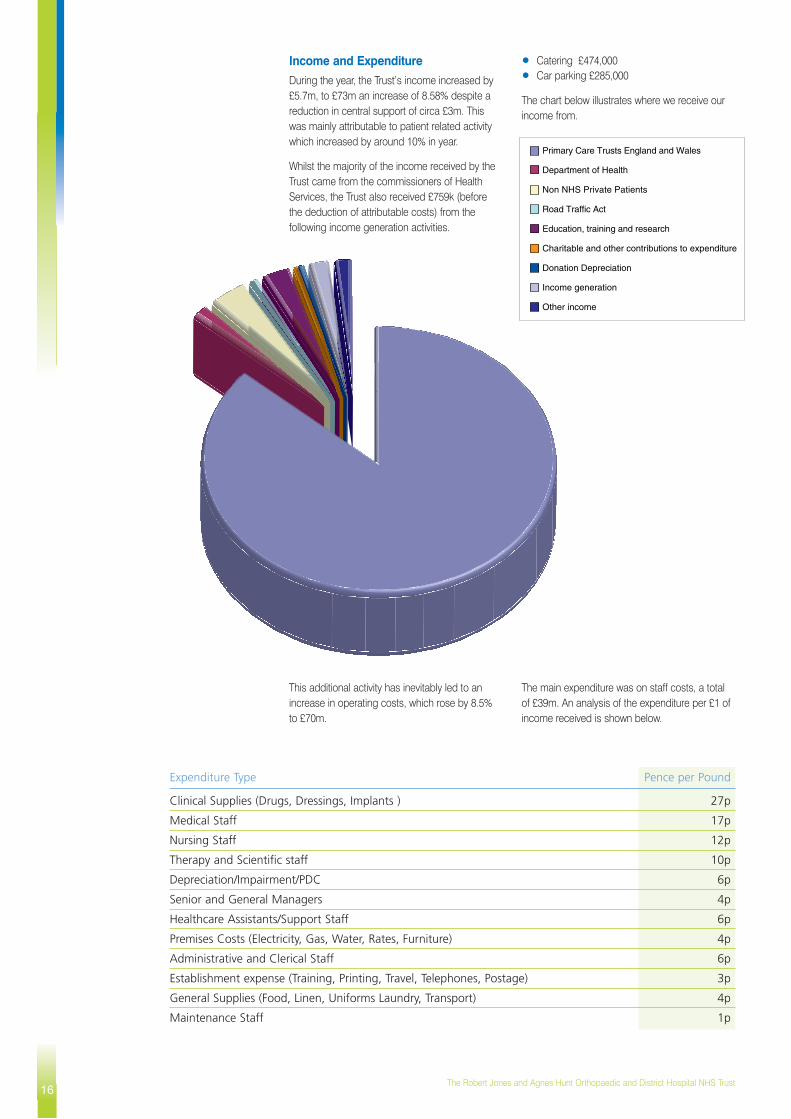
Income and Expenditure
During the year, the Trust’s income increased by£5.7m, to £73m an increase of 8.58% despite areduction in central support of circa £3m. Thiswas mainly attributable to patient related activitywhich increased by around 10% in year.
Whilst the majority of the income received by theTrust came from the commissioners of HealthServices, the Trust also received £759k (beforethe deduction of attributable costs) from thefollowing income generation activities.
Catering £474,000Car parking £285,000
The chart below illustrates where we receive ourincome from.
This additional activity has inevitably led to anincrease in operating costs, which rose by 8.5%to £70m.
The main expenditure was on staff costs, a totalof £39m. An analysis of the expenditure per £1 ofincome received is shown below.
16The Robert Jones and Agnes Hunt Orthopaedic and District Hospital NHS Trust
Primary Care Trusts England and Wales
Department of Health
Non NHS Private Patients
Road Traffic Act
Education, training and research
Charitable and other contributions to expenditure
Donation Depreciation
Income generation
Other income
Expenditure Type Pence per Pound
Clinical Supplies (Drugs, Dressings, Implants ) 27p
Medical Staff 17p
Nursing Staff 12p
Therapy and Scientific staff 10p
Depreciation/Impairment/PDC 6p
Senior and General Managers 4p
Healthcare Assistants/Support Staff 6p
Premises Costs (Electricity, Gas, Water, Rates, Furniture) 4p
Administrative and Clerical Staff 6p
Establishment expense (Training, Printing, Travel, Telephones, Postage) 3p
General Supplies (Food, Linen, Uniforms Laundry, Transport) 4p
Maintenance Staff 1p

Our cost distribution is analysed further in thechart below.
Operating Expenses 2008/09
17Annual Report 2008/09
Directors Costs
Staff Costs
Supplies and services - clinical
Supplies and services - general
Establishment
Transport
Premises
Depreciation
Other
Capital Expenditure
During the year, the Trust spent £3m from itsCapital Programme to upgrade and enhance itsfacilities. Highlights from this investment included:
Completion of TORCH BuildingCommencement of a £0.5m expansion andupgrade to Ludlow WardNew Theatre air filters and cooling system toensure the Trust maintains its excellent lowincidence of infections.Refurbishment of roads, car parks andreplacement of windows, as part of astructured estate maintenance programmeReplacing and upgrading medical equipment Further investment in the Trust’s ITinfrastructure
Plans for 2009/10 include the expansion of theTrust’s Theatre capacity as part of a new ShortStay Surgery Unit due to open in September2009.
External Constraints and KeyDependencies
The Trust is governed by the Department ofHealth, with its performance being monitoredlocally by the NHS West Midlands StrategicHealth Authority, along with other NHSorganisations. The Trust’s ongoing activity isdependant on the continued referral of patientsfrom local healthcare commissioners, the mostsignificant of which are Shropshire CountyPrimary Care Trust (PCT) and the North WalesLocal Health Boards (LHBs).
Auditors
The Trusts external auditors are :
The Audit CommissionSuite 1, Observer HouseHorsefairAbbey ForegateShrewsburyShropshireSY2 5DE
The Audit fee for 2007/08 was £156,000 whichincluded £10,000 relating to the review of workundertaken by the Trust, as it makes the transitionto International Financial Reporting Standards.
Audit Committee
The Audit Committee exists to ensure that theTrust’s activities and financial systems complywith relevant guidelines and codes of conduct.
Membership during the year comprised of the following Non- Executive members of the Trust Board.
Mervyn Dean (Chair)James TurnerLynn Lobley
Their meetings are also attended by the Directorof Finance, Director of Nursing & Governance, the Internal and External Auditors.

Related Party TransactionsDuring the year, none of the Board members ormembers of the key management staff or partiesrelated to them have undertaken any financiallymaterial transactions with the Trust.
The Trust has a long standing relationship withKeele University which is a partner in manyresearch projects. One Non-Executive member ofthe Trust Board is also a Pro-Vice Chancellor ofKeele University.
The following are regarded as related parties withwhom the Trust has had a significant number ofmaterial transactions during 2008-09:
The Department of Health (DoH) and other entitiesfor which the DoH is regarded as the parentDepartment. These entities are listed below:
West Midlands Strategic Health AuthorityShropshire County PCTNHS Litigation AuthorityNHS Purchasing and Supply Agency
Non-English NHS bodies, in particular:
North Wales Consortia of Local Health Boards(Wrexham, Flintshire, Anglesey, Gwynedd,Denbighshire, Conwy)Powys Local Health Board
Other Government Departments and othercentral and local government bodies. Most ofthese transactions have been with theWorkforce Development Confederation.
The Trust has also received revenue and capitalpayments from the RJAH NHS Trust charity, forwhich the Trust is the Corporate Trustee. Duringthe period the charity funded £3m of fixed assets,comprising £2.8m for a treatment and researchfacility (TORCH) building and £200,000 forequipment. The charity prepares a separatelyaudited Trustees Annual Report and Accountswhich are externally audited and submitted to theCharity Commissions. These are also madeavailable via the Trust’s website.
Compliance with Better PaymentsPractice Code
The Trust has continued to ensure that overall aminimum of 95% of invoices are paid within 30days of receipt of the invoice or the goods(whichever was later).
Payments to small and local suppliers are whereverpossible made within ten days following a directivefrom the Government requesting that publicsector organisations support small businessesthrough the current difficult economic conditionsby paying outstanding invoices promptly.
The Trust has not incurred any charges for the latepayment of invoices under the late payment ofCommercial Debts Act 1998.
Management Costs
Management costs include many services anddepartments and do not just represent the costsof individual managers. The Trust keeps itsmanagement costs under continual review andwas successful in reducing them in the year whenmeasured as a percentage of income.
Summary Financial Statements
The summary financial statements are only asummary of the information in the Trust’s AnnualAccounts that have been prepared using UKGAAP principles. The full Statement of InternalControl is available within the full set of accounts,available upon request.
The Trust, in line with the rest of the NHS, movesacross to International Financial ReportingStandards (IFRS) from 2009/10. These statementswill therefore require to be restated as part of thetransition across to IFRS during 2009/10; the auditcommittee continues to monitor the project planin this respect. The Trust is well progressed withthis work and has received a “Green” rating bythe Audit Commission for its readiness to move toIFRS accounting
Copies of the full set of Accounts may be viewedon the Trust’s website at: www.rjah.nhs.uk oralternatively are available from:
Director of Finance, Performance andContracting:The Robert Jones and Agnes HuntOrthopaedic and District Hospital NHS TrustOswestryShropshire SY10 7AG
18The Robert Jones and Agnes Hunt Orthopaedic and District Hospital NHS Trust
Better Payment Practice Code Number of Invoices Value £000s
Non-NHS CreditorsTotal bills paid in the year 33,209 37,167
Total bills paid within target 32,788 36,606
Percentage of bills paid within target 98.7 98.4
NHS CreditorsTotal bills paid in the year 743 12,5434
Total bills paid within target 647 12,335
Percentage of bills paid within target 87.1 98.3
2008/09 2007/08£000 £000
Management Costs 3,186 3,008
Income 72,732 67,043
Percentage 4.38% 4.49%

19Annual Report 2008/09
2008/09£'000
Income from activities 66,191
Other Operating Income 6,541
Operating expenses -70,041
OPERATING SURPLUS 2,691
Loss on disposal of fixed assets -171
SURPLUS BEFORE INTEREST 2,520
Interest receivable 181
Interest payable -125
SURPLUS FOR THE FINANCIAL YEAR 2,576
Public Dividend Capital dividends payable -1577
RETAINED SURPLUS FOR THE PERIOD 999
INCOME AND EXPENDITURE ACCOUNT
This is income from non-patient care services andincludes grants forresearch, training andeducation undertaken bythe Trust as well asincome generated fromcatering, car parking andaccommodation.
The majority of our income comes fromcontracted activity agreements withEnglish Primary Care Trusts and otherNHS bodies including Welsh LocalHealth Boards
Accounting for over half of our totalexpenditure, staff costs are by far thehighest expense. During the period weemployed in the region of 1,300 peoplein a range of full and part timepositions.
Book value of assets written off fromthe balance sheet in year
Interest is received on our cashbalances held throughout the year at avariable rate
Interest is payable on our outstandingloans at a fixed rate
This dividend is paid to Department ofHealth in return for capital provided tofinance the infrastructure of ourHospital.
20The Robert Jones and Agnes Hunt Orthopaedic and District Hospital NHS Trust
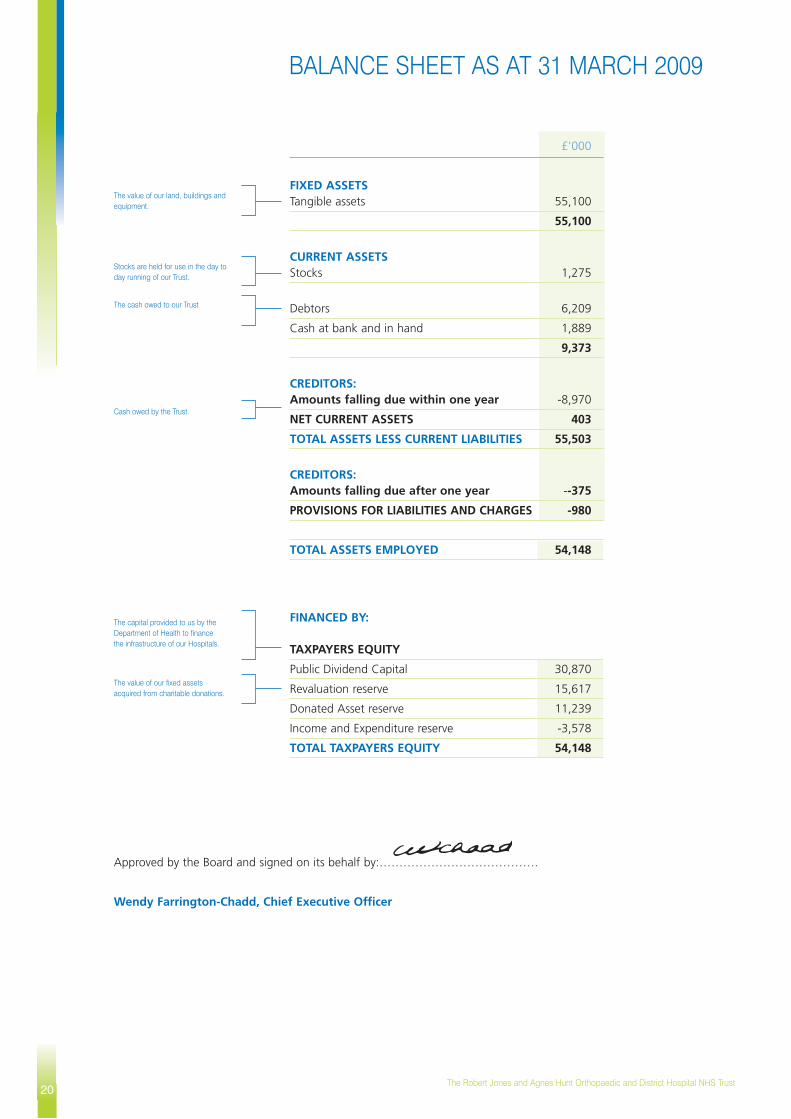
£'000
FIXED ASSETSTangible assets 55,100
55,100
CURRENT ASSETSStocks 1,275
Debtors 6,209
Cash at bank and in hand 1,889
9,373
CREDITORS: Amounts falling due within one year -8,970
NET CURRENT ASSETS 403
TOTAL ASSETS LESS CURRENT LIABILITIES 55,503
CREDITORS: Amounts falling due after one year --375
PROVISIONS FOR LIABILITIES AND CHARGES -980
TOTAL ASSETS EMPLOYED 54,148
FINANCED BY:
TAXPAYERS EQUITY
Public Dividend Capital 30,870
Revaluation reserve 15,617
Donated Asset reserve 11,239
Income and Expenditure reserve -3,578
TOTAL TAXPAYERS EQUITY 54,148
BALANCE SHEET AS AT 31 MARCH 2009
The value of our land, buildings andequipment.
Stocks are held for use in the day today running of our Trust.
The cash owed to our Trust
Cash owed by the Trust.
The capital provided to us by theDepartment of Health to financethe infrastructure of our Hospitals.
The value of our fixed assets acquired from charitable donations.
Approved by the Board and signed on its behalf by:………………………………….
Wendy Farrington-Chadd, Chief Executive Officer

21Annual Report 2008/09
£'000
OPERATING ACTIVITIESNet cash inflow from operating activities 7,542
RETURNS ON INVESTMENTS ANDSERVICING OF FINANCEInterest received 181
Interest paid -132
Net cash inflow from returns on investments and servicing of finance 49
CAPITAL EXPENDITURE
Payments to acquire tangible fixed assets -3,053
Net cash outflow from capital expenditure -3,053
DIVIDENDS PAID -1,577
Net cash inflow before management of liquid resources and financing 2,961
FINANCING
Public dividend capital received 45
Public dividend capital repaid -110
Loans repaid to DH -1,184
Net cash inflow from financing -1,249
Increase in cash 1,712
£'000
Surplus for the year before dividend payments 2,576
Fixed asset impairment losses -614
Unrealised surplus on fixed asset revaluations/indexation -926
Increase in the donated asset reserve due to receipt of donated assets 5,760
Total recognised gains and losses in the financial year 6,796
CASHFLOW STATEMENT FOR THE YEAR ENDED 31 MARCH 2009
Interest is received on our cashbalances held throughout the year at avariable rateInterest is payable on our outstandingloans at a fixed rate
Cash spent on investing in thedevelopment and modernisation of ourHospitals.
An annual dividend payment is madeto the Department of Health inrecognition of the financing providedfor our facilities
Cash received from the Department ofHealth for capital developments.
Cash repaid to the Department ofHealth in respect of 2007/08impairment funds flow
The second instalment of the Trust'sthree year working capital loan andpart repayment of Maternitydevelopment capital
This statement summarises all thegains and losses made by our Trustduring the period
The value of our assets is increasedeach year in line with indices set by theDept of Health
STATEMENT OF RECOGNISED GAINS AND LOSSES FOR THE YEAR ENDED 31 MARCH 2009
The Cash flow statement shows thesource from which cash has flowedinto our Trust, the way cash has beenused and the net increase or decreasein cash during the period

22The Robert Jones and Agnes Hunt Orthopaedic and District Hospital NHS Trust
Remuneration ReportThis discloses the salary and pension entitlements of the Trust Board as senioremployees of the Trust. Note 1.10 to the full accounts provides an explanation ofhow pension liabilities are dealt with.
SALARIES AND ALLOWANCES
2007-08 2008-09
£000 £000 £000 £000 £000 £000
Farrington Chadd, W - Chief Executive 110 - 115 0 0 115 - 120 0 6from 1 March 2007
James, D - Director of Operations & 65 - 70 0 3 75 - 80 0 5Business Development
McCall, I - Medical Director from15 - 20 185 - 190 0 60 - 65 135 - 140 01 November 2007
Grinnell, J - Director of Finance, Contracting & Performance N/A N/A N/A 55 - 60 0 3from July 2008
Gilburt, D - Director of Finance, Contracting & Performance 95 - 100 0 0 40 - 45 0 0from July 2007 to July 2008 (Note 1)
Morris, V - Director of Nursing & Governance
65 - 70 0 3 70 - 75 0 5
Wilkins, R - Associate Director of Estates & Facilities (on partial secondment 70 - 75 0 2 05 - 10 15 - 20 0outside Trust since 19/05/08)
Wafer, A - Associate Director of Human Resources until 31 December 2008
55 - 60 0 2 45 - 50 0 3
Bate, S - Associate Director of Human Resources from 1 January 2009 (Note 2)
N/A N/A N/A 40 - 45 0 0
Edwards, A - Associate Director of Contracting
65 - 70 0 0 65 - 70 0 4
Sear, D - Chairman until 30 June 2008 15 - 20 0 0 0 - 5 0 0
Tinston, R - Chairman from 1 July 2008 to 16 March 2009
N/A N/A N/A 10 - 15 0 0
Hardy, R - Chairman from 17 March 2009 N/A N/A N/A 0 - 5 0 0
Dean, M - Non Executive Director 5 - 10 0 0 5 - 10 0 0
Turner, J - Non Executive Director 5 - 10 0 0 5 - 10 0 0
Lobley, L - Non Executive Director 5 - 10 0 0 5 - 10 0 0
Jones, P - Non Executive Director 0 - 5 0 0 5 - 10 0 0
Bertolini, J - Non Executive Director until 14 September 2008
0 - 5 0 0 0 - 5 0 0
Lawes, G - Non Executive Director from 1 February 2009
N/A N/A N/A 0 - 5 0 0
Bo
ard
Sal
ary
(ban
ds
of
£5,0
00)
Oth
er R
emu
ner
atio
n
(ban
ds
of
£5,0
00)
Ben
efits
in k
ind
(R
ou
nd
ed t
on
eare
st £
000)
Bo
ard
Sal
ary
(ban
ds
of
£5,0
00)
Oth
er R
emu
ner
atio
n
(ban
ds
of
£5,0
00)
Ben
efits
in k
ind
(R
ou
nd
ed t
on
eare
st £
000)
Name and title

23Annual Report 2008/09
2006-07 2007-08
£000 £000 £000 £000 £000 £000 £000 £000
Farrington Chadd, W - Chief Executive 2.5 - 5 7.5 - 10 30 - 35 95 - 100 485 346 130 91
James, D - Director of Operations & Business Development
2.5 - 5 7.5 - 10 30 - 35 90 - 95 647 447 189 132
McCall, I - Medical Director from 1 November 2007 (Note 3)
-10 - 12.5 52.5 - 55 75 - 80 305 - 310 0 0 0 0
Grinnell, J - Director of Finance, Contracting & Performance 0 - 2.5 5 - 7.5 10 - 15 30 - 35 124 78 44 23from July 2008
Gilburt, D - Director of Finance, Contracting & Performance N/A N/A N/A N/A N/A N/A N/A N/Afrom July 2007 to June 2008
Morris, V - Director of Nursing & Governance
0 - 2.5 2.5 - 5 15 - 20 50 - 55 274 195 73 52
Wilkins, R - Associate Director of Estates & Facilities (on secondment 0 - 2.5 0 - 2.5 20 - 25 65 - 70 549 385 154 14outside Trust since 19/05/08)
Wafer, A - Associate Director ofHuman Resources 0 - 2.5 0 - 2.5 15 - 20 55 - 60 354 248 100 53until 31 December 2008
Bate, S - Associate Director of Human Resources from 1 January 2009
N/A N/A N/A N/A N/A N/A N/A N/A
Edwards, A - Associate Director of Contracting
0 - 2.5 2.5 - 5 15 - 20 55 - 60 321 240 76 53
Rea
l In
crea
se in
pen
sio
n a
t ag
e 60
(b
and
s o
f £2
,500
)
Lum
p s
um
at
age
60 r
elat
ed t
ore
al in
crea
se in
pen
sio
n
(ban
ds
of
£2,5
00)
Tota
l acc
rued
pen
sio
n a
t ag
e 60
at
31 M
arch
200
8 (b
and
s o
f £5
,000
)
Lum
p s
um
at
age
60 r
elat
ed t
oac
cru
ed p
ensi
on
at
31st
Mar
ch 2
008
(ban
ds
of
£5,0
00)
Cas
h E
qu
ival
ent
Tran
fer
valu
e at
31st
Mar
h 2
008
Cas
h E
qu
ival
ent
Tran
sfer
Val
ue
at31
st M
arch
200
7
Rea
l in
crea
se in
Cas
h E
qu
ival
ent
Tran
sfer
Val
ue
Emp
loye
r fu
nd
ed c
on
trib
uti
on
to g
row
th in
CET
V
Name and title
PENSION BENEFITS
Note 1: Payments made to PSEC Consulting Ltd
Note 2: Payments made to Coaching Innovations Ltd
Note 3: CETV - £0.00 as over age 60

Pension Benefits
The pension benefits have been calculatedusing information provided by the NHSPensions Agency (now part of theNHSBSA).
The “Cash Equivalent Transfer Value”(CETV) is the value which would betransferred should an individual leave andchoose to have their pension transferred toa different scheme. This sum would betransferred to the new employer’s pensionscheme. This value has been calculated byactuaries and is based on the pensionentitlement which the individual has built upover their years of NHS experience. TheNHS Pensions Agency has advised theTrust that the significant difference whencomparing this year’s values to last year’sis due to a change in the factors used tocalculate the CETV; these were introducedin October 2008.
The Trust’s employees are part of thenational NHS pension scheme. All pensioncontributions and all payments of pensionsor CETV come from this national fund.
The “Employer funded contribution togrowth in CETV” is the amount of growth inthe CETV which was funded by theemployer. This is calculated using aformula provided by the Department ofHealth.
Remuneration and Pension Policy forSenior Managers
The remuneration of the Chief Executive and allother Executive Directors is determined annuallyby the Remuneration Committee and is basedon guidance issued by the Department ofHealth. Membership of the Committeecomprises of the Chairman and Non Executivemembers of the Trust.
The Chief Executive and other ExecutiveDirectors are employed on permanentcontracts. The period of notice required toterminate the employment of the Chief Executiveor any other executive Director is 6 months.There is no entitlement to a termination paymentfor any member of staff.
The tables on these pages outline theremuneration and pension benefits for the yearfor all senior managers
…………………………………………
Wendy Farrington Chadd(Chief Executive on behalf of the Board)
7th May 2009
24The Robert Jones and Agnes Hunt Orthopaedic and District Hospital NHS Trust

25Annual Report 2008/09
Auditor’s Independent ReportIndependent auditor’s statement to the Board of Directors of the Robert Jones and Agnes Hunt Orthopaedicand District Hospital NHS Trust
I have examined the summary financialstatement which comprises the Incomeand Expenditure account, Balance Sheet,Cashflow Statement, and RemunerationReport set out on pages 19 to 24.
This report is made solely to the Board ofDirectors of Robert Jones and AgnesHunt Orthopaedic and District HospitalNHS Trust in accordance with Part II of theAudit Commission Act 1998 and for noother purpose, as set out in paragraph 49of the Statement of Responsibilities ofAuditors and of Audited Bodies preparedby the Audit Commission.
Respective responsibilities ofdirectors and auditor
The Directors are responsible forpreparing the Annual Report.
My responsibility is to report to you myopinion on the consistency of thesummary financial statement within theAnnual Report with the statutory financialstatements.
I also read the other informationcontained in the Annual Report andconsider the implications for my report if Ibecome aware of any misstatements ormaterial inconsistencies with the summaryfinancial statement.
Basis of opinion
I conducted my work in accordance withBulletin 1999/6 ‘The auditors’ statementon the summary financial statement’issued by the Auditing Practices Board.My report on the statutory financialstatements describes the basis of ouraudit opinion on those financialstatements.
Opinion
In my opinion the summary financialstatement is consistent with the statutoryfinancial statements of the Trust for theyear ended 31 March 2009.
Tony Corcoran(Officer of the Audit Commission)
10th June 2009

The Board is accountable for internal control. AsAccountable Officer, and Chief Executive of thisBoard, I have responsibility for maintaining asound system of internal control that supportsthe achievement of the organisation’s policies,aims and objectives. In this role I work withpartner organisations and report progress onagreed service contracts to agreed targets thatare monitored by the Strategic Health Authority.I also have responsibility for safeguarding thepublic funds and the organisation’s assets forwhich I am personally responsible as set out inthe Accountable Officer Memorandum.
The system of internal control is designed tomanage risk to a reasonable level rather than toeliminate all risk of failure to achieve policies,aims and objectives; it can therefore onlyprovide reasonable and not absolute assuranceof effectiveness.
A Risk Management Strategy was in placewhich was endorsed by the Trust Board in May2006, updated to an Assurance FrameworkStrategy in February 2008. This Framework wasreviewed, revised and approved by the TrustBoard in November 2008. This clearly definesrisk management structures, accountability andresponsibilities, and incorporates considerationof stakeholders. All serious untoward incidentsare reported to the Strategic Health Authority. A Board assurance framework was in placethroughout 2008/09 and was reviewed by theBoard on a quarterly basis, which describesaccountabilities for the Chief Executive andExecutive Directors as follows:
The Chief Executive is the AccountableOfficer for the Trust and takes specificresponsibility for the management ofStrategic Risk.All Executive Directors are accountable forCorporate Risk.The Medical Director and Executive Directorof Nursing & Governance are accountablefor Clinical Risk.The Director of Nursing & Governance andthe Director of Operations and Developmentare responsible for supporting Ward andDepartment Managers in the managementof Operational Risk.
As Accountable Officer, I have responsibility forreviewing the effectiveness of the system ofinternal control. My review is informed in anumber of ways. I have been advised on theimplications of the result of my review of theeffectiveness of the system of internal control bythe following Boards and Committees; TrustBoard, Audit Committee, Clinical ManagementBoard, Information Governance Committee,Clinical Audit ,Research and Clinical
Effectiveness Committee, Health and SafetyCommittee, Patient Safety and FocusCommittee and Remuneration Committee . A plan to address weaknesses and ensurecontinuous improvement of the system is inplace.
As part of the Head of Internal Audit Opinion,the auditors have drawn my attention to twoareas of control weakness:
Human Resources: Our review identifiedscope for improvements to pre-employmentchecking procedures as well as to themonitoring of induction attendance andappraisals. The Trust has put in place anaction plan to address these issues.Key financial systems: Our review of the keyfinancial systems identified that further workis also required to tighten controls overdebtors (in particular assuring regular debtchasing and review and segregation of dutyin raising invoices and receipting income)and creditors (where the key areas forimprovement include improving theprocedures for setting up of new suppliersand completion of the register of interests,segregation of duty in the payment ofinvoices, and authorisation of payment runs).
I have noted that these issues were resolved bythe year end.
Actions were undertaken to address areashighlighted by the 2007/08 Declaration ofStandards for Better Health.
The 2007/08 Statement of Internal Controlreported that the Trust had declared insufficientassurance on C12. This related to ResearchGovernance, specifically the audit of practiceand ongoing training of research staff. Thedeclaration of 2008/09 demonstrates that theBoard has reasonable assurance that C12 isnow compliant following considerable focus andimprovement in this area throughout the year.
Wendy Farrington Chadd
Chief Executive and Accountable Officer onbehalf of the RJAH Orthopaedic Hospital TrustBoard.
7th May 2009
26The Robert Jones and Agnes Hunt Orthopaedic and District Hospital NHS Trust
Statement on Internal Control

27Annual Report 2008/09
The Secretary of State has directed that theChief Executive should be the AccountableOfficer to the Trust. The relevant responsibilitiesof Accountable Officers, including theirresponsibility for the propriety and regularity ofthe public finances for which they areanswerable, and for the keeping of proper
records, are set out in the Accountable Officers’Memorandum issued by the Department ofHealth.
To the best of my knowledge and belief, I haveproperly discharged the responsibilities set outin my letter of appointment as an accountableofficer.
Statement of the Chief Executive’sResponsibilities as the Accountable Officer of the Trust
The Directors are required under the NationalHealth Service Act 2006 to prepare accounts foreach financial year. The Secretary of State, withthe approval of the Treasury, directs that theseaccounts give a true and fair view of the state ofaffairs of the Trust and of the income andexpenditure, recognised gains and losses andcash flows for the year. In preparing thoseaccounts, Directors are required to:
apply on a consistent basis accountingpolicies laid down by the Secretary of Statewith the approval of the Treasury;make judgements and estimates which arereasonable and prudent;state whether applicable accountingstandards have been followed, subject toany material departures disclosed andexplained in the accounts.
The Directors are responsible for keepingproper accounting records which disclose withreasonable accuracy at any time the financialposition of the trust and to enable them toensure that the accounts comply withrequirements outlined in the above mentioneddirection of the Secretary of State. They arealso responsible for safeguarding the assets ofthe Trust and hence for taking reasonable stepsfor the prevention and detection of fraud andother irregularities.
The Directors confirm to the best of theirknowledge and belief they have complied withthe above requirements in preparing theaccounts.
Statement Of Directors Responsibilities InRespect Of The Accounts
..............................Date.............................................................Chief Executive7th May 2009
By order of the Board
..............................Date.............................................................Chief Executive
..............................Date.............................................................Director of Finance
7th May 2009
7th May 2009

The Trust’s strategic intention is to become theleading national specialist orthopaedic trust andthe key provider of Choice for musculoskeletalservices, offering high quality patient centredcare. Our unique geographical position, thenature of the services we provide and our leadingreputation in patient care, research andeducation place the Trust in a strong position todevelop as a Foundation Trust.
Non-Executive DirectorsRobert Tinston, Chairman (to 16 March 2009)Russell Hardy, Chairman (from 17 March 2009)Mervyn Dean, Non-Executive DirectorPeter Jones, Non-Executive DirectorGlen Lawes, Non-Executive Director (from 1 February 2009)Lynne Lobley, Non-Executive DirectorJames Turner, Non-Executive Directorr
Executive DirectorsWendy Farrington Chadd, Chief Executive John Grinnell, Director of Finance, Contractingand Performance
David James, Director of Operations andBusiness DevelopmentIain McCall, Medical DirectorVicky Morris, Director of Nursing and Governance
Board CommitteesThe Trust has a governance structure to ensurethe Board can monitor, evaluate and enhanceperformance. Members of the Board also havemembership of the following committees:
Audit Committee The Audit Committee ensures the effectiveinternal control of the Trust by reviewing financialsystems and information used, enabling theBoard to have confidence in its financial and riskmanagement systems. All Directors have statedthat as far as they are aware, there is no relevantaudit information of which the Trust’s auditors areunaware. This statement can be found in theLetter of Representation.
Management BoardThe Management Board includes members ofthe Trust Board and Clinical Directors, bringingtogether managerial and clinical perspectives tohelp shape future strategy for the Trust.
Charitable Funds CommitteeApproves expenditure; recommends andimplements an investment strategy for approvalby the Trust Board as Corporate Trustees andreviews the levels of financial activity on allindividual funds, with a view to ensuringproactively that fund balances are utilised in atimely fashion in accordance with the intention of donors.
Remuneration CommitteeThe remuneration of the Chief Executive and allother Executive Directors is determined annuallyby the Remuneration Committee and is based onguidance issued by the Department of Health.Membership of the Committee comprises of theChairman and Non Executive members of theTrust.
28The Robert Jones and Agnes Hunt Orthopaedic and District Hospital NHS Trust
7. Trust Board and Structure
Director Declaration of Interest
Professor Peter Jones, Non Executive Director Provice Chancellor and Professor at Keele UniversityMember of National Institute of Clinical Excellence (NICE)
Mrs Lynne Lobley, Non Executive Director Member of Merseyside and Cheshire Deanery
Mr James Turner, Non Executive Director James Turner Associates Ltd. Non-Executive Director in private sector: Manbat Ltd, Able Instruments Ltd, Stroll Ltd, 16 Gwendwr Road (Management) Ltd.Non Executive Director in public sector: Navy Board, British Wool Marketing Board, Ministry of Justice, Audit Committee.Other: Diocesan Board of Finance in the Dioceses of St Asaph
Professor Robert Tinston, Chairman Associate of Verita – company dealing with investigations and enquiries into NHS activities.
Mr Russell Hardy, Chairman Chair of Multiple Sclerosis Trust & Chairman of Hunters Moor Neuro-Rehabilitation Limited
Declarations of Interest

Useful Contacts
Fundraising
If you want to find out more about how to getinvolved with fundraising activities for the Trustor how to make a charitable donation, pleasesee our website at: www.rjah.nhs.uk
Becoming a volunteer
Anyone interested in becoming a volunteer atthe Trust should contact the Human Resourcesdepartment on (01691) 404639 or theLeague of Friends on (01691) 404527.
Applying for jobs
To find out more information about possible jobopportunities at the Robert Jones and AgnesHunt Orthopaedic and District Hospital NHSTrust visit: www.rjah.nhs.uk/latest-vacancies.aspxor www.jobs.nhs.ukor contact Human Resources on: (01691) 404639
29Annual Report 2008/09
8. Contacts
The new TORCH Building which was completed in 2008.
Back cover photo - our representative staff: L- RGlen Whitehouse, Radiographer, X Ray DeptHarriet Egerton-Davies, Medical SecretarySimon Vernon, PorterAmy Chana, PhysiotherapistAdrian Davies, EstatesNichola Wynstanley, HousekeepingDr. Siddalingaprabhu Katti, Anaesthetics and Theatres

The Robert Jones and Agnes HuntOrthopaedic and District Hospital NHS Trust
Oswestry, Shropshire SY10 7AGTel: 01691 404358
This report can be made available on request in Braille, on audio cassette, disk or in large print. Arrangements can also be made onrequest for it to be explained in your preferred language. It is also available electronically at: www.rjah.nhs.uk
The Robert Jones and Agnes HuntOrthopaedic and District Hospital
NHS TrustNHS Trust