Embed Size (px)
Citation preview

AG
AA
bst
ract
sSu1122
Efficacy of a Single Day Fecal Immunochemical Occult Blood Testing (FIT)Collection Strategy for Screening Relevant Colorectal NeoplasiasClarence K. Wong, Richard N. Fedorak, Connie I. Prosser, Sander Veldhuyzen vanZanten, Daniel C. Sadowski
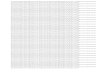
Background and Aim: Fecal occult blood testing has been shown to reduce mortality fromcolorectal cancer. However, patient related factors such as compliance and diet affect canceryield independent of test diagnostic performance. Fecal immunochemical tests (FIT) are notaffected by diet or medications and increase compliance. Our aim was to assess the efficacyof guaiac and immunochemical fecal occult blood testing over 1 and 2 days to detectscreening relevant neoplasias. Methods: We used a prospective observational cohort designin asymptomatic individuals who were referred for colorectal cancer screening. Both averagerisk individuals (50-75 years) and those with a family or personal history of colon canceror polyps (40-75 years) were recruited from April 2008 to October 2009 in Edmonton,Canada. All participants completed 3 stool occult blood kits at home: guaiac based HemoccultII and two immunochemical tests (Hemoccult ICT and MagStream HemSp). Participantswere instructed to complete sampling for all stool kits from one bowel movement andto repeat this on a second day. All participants underwent colonoscopy by experiencedendoscopists. A screen relevant neoplasm (SRN) was defined as any adenoma ≥1.0 cm orgreater in size, any adenoma with villous components or high-grade dysplasia on histologyor carcinoma of any size. Results: Of 2166 referred patients, 1075 (53.8% female, meanage 56.3) completed all stool kits and received a colonoscopy. 69 patients had SRNs.Sensitivity and false positive rates (FPR) were calculated for stool kits in detecting SRNs for3 strategies: either day 1 or 2 sets were positive (baseline comparator), both day 1 and 2were positive, and only assessing samples from one day. While FPR was lowest in the bothdays strategy, there was no significant change in sensitivity for SRNs between testing strategies.The highest one day collection sensitivities for SRNs were in the Magstream at 30 μg/g(39.13%) and 67 μg/g (30.43%) cutoffs. False positive rates were 8.75% and 3.48 %respectively. Results are shown in Table 1. Conclusion: Single day stool testing with FIT iseffective for detecting screening relevant neoplasias and reduces false positive rates. Thissampling strategy may enhance patient compliance which may result in higher SRN orcolorectal cancer yield.Table 1. Diagnostic performance of stool collection strategies
SEN=Sensitivity FPR=False positive rate
Su1123
Plasma MicroRNAs as a Potential Strategy for Non-Invasive Colorectal CancerScreeningMaria Dolores Giraldez, Juan José Lozano, Georgina Ramirez, Antoni Castells, MeritxellGironella
Background: MicroRNAs (miRNAs) are small non-coding RNA molecules which functionas negative gene regulators. Tissue expression profiling of miRNAs has been shown todiscriminate between various types of cancers. The recent discovery of stable miRNAs inplasma has opened up the possibility of using these molecules as non-invasive biomarkersfor cancer diagnosis. Colorectal cancer (CRC) is the second leading cause of cancer deathin Western countries. New non-invasive approaches that can complement and improvecurrent strategies for CRC screening are urgently needed. In that sense, expression patternsof plasma miRNAs could be a useful strategy. Aim: To analyze whether expression patternsof plasma miRNAs are able to successfully discriminate between patients with colorectalneoplasia and healthy individuals. Patients and Methods: 42 newly diagnosed patients withcolorectal neoplasia (21 CRC and 21 advanced adenomas) and 21 matched controls wererecruited. Plasma samples were collected prior to treatment. Total RNA was isolated usingTrizol LS reagent (Invitrogen) and miRNeasy Mini Kit (Qiagen). Genome-wide miRNAprofiling was performed using the SAM-Bead microarray (Illumina,Inc). Bioinformatics toolsas LIMMA (linear models for microarray data) and PAM (prediction analysis for microarrays)were used for the analysis. We also analysed a subset of this data by qRT-PCR. Sensitivity(S), specificity (Sp), and area under receiver operator characteristic curve (AUC) werecalculated for each validated miRNA. Results: We found 154 miRNAs significantly disregu-lated between patients with colorectal neoplasia and controls, a subset of 21 and 28 miRNAswere exclusively upregulated in CRC and advanced adenomas, respectively, meanwhile bothlesions shared 24 upregulated miRNAs. Moreover, we identify a signature of 31 miRNAsdemonstrating a good discriminative ability to identify patient with colorectal neoplasia,with an AUC of 0.85 (95%CI,0.77-0.97). After qRT-PCR validation we confirmed miR-92aand miR-17 as the best plasma biomarkers for colorectal neoplasia with an AUC of 0.81(95%CI,0.64-0.98) and 0.72 (95%CI,0.50-0.94), respectively. For miR-92a and miR-17,
S-410AGA Abstracts
sensitivities were 80% and 76% and specificities were 77% and 76% at the cutoff value of0.6. Combination of both miRNAs did not significantly improve their ability to identifypatients with colorectal neoplasia. Conclusions: Plasma miRNA signatures can discriminatebetween patients with colorectal neoplasia and healthy individuals representing a powerfulnon-invasive strategy for CRC screening. To our knowledge, this is the first report performingplasma miRNAs profiling in patients with colorectal neoplasia by a high-throughput techno-logy. Our results highlight miR-17 and especially miR-92a as adequate candidate biomarkersfor CRC screening.
Su1124
Risk Factors for Proximal Large Serrated PolypsMichal F. Kaminski, Andrzej Mroz, Ewa Kraszewska, Miroslaw Kiedrowski, JaninaOrlowska, Maciej Rupinski, Jaroslaw Regula
Background: Predictors of advanced proximal colonic neoplasia are used to identify a needfor colonoscopy in sigmoidoscopy screening. It is unknown whether the same predictorspermit identification of subjects with the proximal, large serrated polyps that are supposedprecursor lesions of alternative pathways to colorectal cancer. Here we assessed the associ-ations among the risk of proximal large serrated polyps and clinical features and distalcolorectal findings. Methods: We performed a cross-sectional analysis of data from a singlescreening colonoscopy center that from 2000-2006 included 14,168 asymptomatic particip-ants 50 to 66 years of age. We defined a large serrated polyp as a serrated polyp (hyperplasticpolyp, sessile serrated polyp, mixed serrated polyp, or traditional serrated adenoma) thatwas at least 10 mm in diameter. An experienced gastrointestinal pathologist reviewed allhistopathology slides of polyps >10 mm. We used the splenic flexure boundary to definethe proximal large bowel. Distal colonoscopy findings were categorized according to themost advanced lesion identified. Previously identified independent variables were used ina multivariate logistic regression to confirm associations with proximal advanced neoplasiaand with proximal large serrated polyps. Results: Proximal advanced neoplasias and proximallarge serrated polypswere identified in 197 (1.39%) and 76 (0.54%) participants, respectively.A logistic regression model confirmed that male sex, age, and distal advanced neoplasiawere independent risk factors for advanced proximal neoplasia in this study cohort. Malesex was also associated with a reduced risk of proximal large serrated polyps (adjusted oddsratio 0.60; 95% confidence interval 0.36 to 1.00; P=0.051). All types of distal findigs wereassociated with an increased risk of proximal large serrated polyps: small tubular adenomas(adjusted odds ratio 2.35; 95% confidence interval 1.13 to 4.88; P=0.022), hyperplasticpolyps (adjusted odds ratio 5.14; 95% confidence interval 3.00 to 8.80; P<0.001), andadvanced neoplasias (adjusted odds ratio 8.98; 95% confidence interval 4.49 to 17.96;P<0.001). Conclusions: All types of distal polyps were associated with an increased risk ofproximal large serrated polyps, whereas distal advanced neoplasia was the only significantfactor associated with an increased risk of proximal advanced neoplasia. Male sex wasassociated with reduced risk of proximal large serrated polyps but increased risk of proximaladvanced neoplasias. The results may facilitate the choice of an efficient colonoscopy referralalgorithm for use in sigmoidoscopy screening.
Su1125
The Diagnostic Value of Risk Factors in Population Screening for ColorectalCancerInge Stegeman, Thomas R. de Wijkerslooth, Esther M. Stoop, Monique van Leerdam,Evelien Dekker, Ernst J. Kuipers, Paul Fockens, Roderik A. Kraaijenhagen, Patrick M.Bossuyt
Introduction In colorectal cancer (CRC) screening, several screening methods are available.Colonoscopy visualizes the entire colon and is the reference standard for detecting colorectalneoplasia, but is generally not offered to all. Faecal occult blood testing (FOBT) is frequentlyused as initial CRC screening test, but it has a less than perfect specificity and sensitivity.Over the years, several CRC risk factors have been identified in epidemiologic studies. Ifthese risk factors are associated with CRC or advanced adenoma in population screening,they could be used as alternative or additional triage instruments.We evaluated the diagnosticperformance of a series of risk factors in a CRC screening program, where all participantsunderwent colonoscopy. Methods Data were collected in the Colonoscopy or Colonographyfor Screening study, a multicentre trial conducted in the Netherlands, in which 5,924randomly selected, asymptomatic men and women between 50 and 75 were invited toundergo colonoscopy. Based on a review of the literature the following CRC risk factorswere selected: age, sex, family history, first degree relatives with CRC, alcohol, currentsmoking and more than 10 pack years of smoking, BMI, regular aspirin/NSAID use, totalcalcium intake, physical activity and hormone replacement therapy for women. Informationon these risk factors was obtained from screening attendees through a self-administeredquestionnaire. The results of all colonoscopies were recorded, including the presence ofadvanced neoplasia (CRC or advanced adenoma). An advanced adenoma was defined as anadenoma ≥ 10 mm, an adenoma with villous histology (≥25% villous) or an adenomawith high grade dysplasia. For each CRC risk factor, we estimated its diagnostic odds ratio(DOR) relative to the colonoscopy outcome. Results In the 1,236 screening participants,1,022 (83%) completed the questionnaire, of which 82 (8.0%) had advanced neoplasia. Ofthese 6 (7.3%) participants had CRC and 76 (92.7%) had advanced adenoma. The followingrisk factors were significantly associated with advanced neoplasia detected by colonoscopy:age (DOR: 1.07 / year; 95% CI: 1.03 to 1.11) calcium intake (DOR: 0.79 / portion; 95%CI: 0.63 to 0.99) and family history (DOR: 1.71 / first degree family member; 95%CI: 1.13to 2.58). The other nine risk factors were not significantly associated with the presence ofadvanced neoplasia. Conclusion Many putative risk factors are not linked to the presenceof advanced neoplasia in screening participants. Only age, calcium intake and family historywere found to be significantly associated. Including these CRC risk factors in a FOBT basedstrategy may increase the sensitivity and specificity of these screening programs.












![Integrating the Healthcare Enterprise€¦ · Document Source Document ConsumerOn Entry [ITI Document Registry Document Repository Provide&Register Document Set – b [ITI-41] →](https://img.pdfslide.net/doc/110x75/5f08a1eb7e708231d422f7c5/integrating-the-healthcare-enterprise-document-source-document-consumeron-entry.jpg)