Embed Size (px)
Citation preview

60-minutes to E/M Coding Compliance!
Jennifer Godreau, CPC, CPMA, CPEDC
AHIMA Approved ICD-10-CM/PCS Trainer
Director of Development & Operations
1
AAPC Certificate of Attendance for 1 CEU will be emailed to each live attendee’s email id by the end of November 2014.
Agenda
• Inpatient two-midnight rules
• Critical care
• Office visit and screening colonoscopy
• Prescription drug management
• Psychology exam coding
• Babinski
• Double dipping
• Assistant at surgery
• EHR exam cloning
2
Inpatient Two-Midnight Rules: Background April 1, 2014: Protecting Access to Medicare Act of 2014, Section 111:
1. CMS allowed to continue MAC Probe & Educate process through March 31, 2015, and
2. Recovery Auditors not allowed to conduct inpatient hospital patient status reviews on claims with dates of admission Oct. 1, 2013-March 31, 2015.
Aug. 22, 2014: IPPS 2015
1. introduces no new guidelines
2. Responses to numerous comments
3. IPPS: http://www.gpo.gov/fdsys/pkg/FR-2014-08-22/pdf/2014-18545.pdf
3

Inpatient Two-Midnight Rules: Check for Admission Visit and Statement from Provider • a Resident, NP or PA can write the order for INPATIENT admission as
long as the admitting MD signs it prior to discharge
• physician involved in the discussion and decision made prior to admitting the patient.
• Examples of appropriate statement: "Admit to inpatient (v.o) (or t.o) Dr. Smith" or "Admit to observation per Dr. Smith."
4

Inpatient Two-Midnight Rules: Check that Billing Physician Sees Patient 3. Authorization to sign the certification: The certification or recertification may be signed only by one of the following:
(1) A physician who is a doctor of medicine or osteopathy.
(2) A dentist in the circumstances specified in 42 CFR 424.13(d).
(3) A doctor of podiatric medicine if his or her certification is consistent with the functions he or she is authorized to perform under State law.
5

Inpatient Two-Midnight Rules: Know Who Qualifies as Other Authorized Certifier Certifications and recertifications must be signed by the physician responsible for the case, or by another physician who has knowledge of the case and who is authorized to do so by the responsible physician or by the hospital’s medical staff (or by the dentist as provided in 42 CFR 424.11).
Medicare considers only the following physicians, podiatrists or dentists to have sufficient knowledge of the case to serve as the certifying physician:
• the admitting physician of record (“attending”) or a physician on call for him or her;
• a surgeon responsible for a major surgical procedure on the beneficiary or a surgeon on call for him or her; a dentist functioning as the admitting physician of record or as the surgeon responsible for a major dental procedure;
• and, in the specific case of a non‐physician non‐dentist admitting practitioner who is licensed by the State and has been granted privileges by the facility, a physician member of the hospital staff (such as a physician member of the utilization review committee) who has reviewed the case and who also enters into the record a complete certification statement that specifically contains all of the content elements discussed above.
Resource: Sept 5 clarification to the 2014 IPPS Final Rule
6

Inpatient Two-Midnight Rules: No Separate Form Required • Consider all provided documentation to determine if the certification
requirements for billing a two midnights hospital admission are met.
• When a less than 2 day stay is coded with a hospital admission, deny the inpatient admission but consider extenuating circumstances.
• Email concerns to [email protected]
7

Inpatient Two-Midnight Rules: Look for Length of Stay Statement 1. Reason for inpatient services
2. The estimated (or actual) time the beneficiary requires or required in the hospital is indicated as two midnights or more
Important: The duration may be inferred from the documentation provided and is based on the provider's original intent and estimation, not on unforeseen instances that may cause the patient's stay to be less in length than predicted.
8
Inpatient Two-Midnight Rules: Code Per CPT
• When the requirements are not met, coding guidelines should be applied.
• Report observation care or emergency room visit
• "If the physician or healthcare professional is uncertain if an inpatient admission is appropriate, then the physician or healthcare professional should consider admitting the patient for observation." (UnitedHealthcare, Inc., UHC MA Coverage Summary: Observation Care [Outpatient Hospital])
• Email payment concerns to: [email protected].
9

Critical Care: Requirements Hourly critical care’s requirements (99291 and 99292) include:
1. elements counted in the critical care time all meet the requirements to be allowed as counting towards critical care time including requirements such as location, patient status and topic;
2. documentation that indicates that the critical care code’s time requirement is met;
3. documentation that supports the patient’s condition as meeting the CPT and CMS definitions of critically ill person or critically ill injury;
4. documentation that supports the direct treatment of the critical illness or injury by the provider billing for the critical care
10

Critical Care: When to Count Phone Calls
To count a phone call to a family member as critical care:
1. the call has to be made on the unit
2. the patient must be unable to participate in her own care. • CPT allows counting of unit discussions with a family member “when the
patient is unable or lacks capacity to participate in discussions,” according to CPT guidelines.
11

Critical Care: Active Treatment of Critical Condition • provider can directly provide the critical care or direct a team
providing the critical care
• treatment may have critical elements but may not change much from day to day and instead may be directly related to the patient's life-threatening condition/respiratory
12

Critical Care: CPT guidelines
• “Although critical care typically requires interpretation of multiple physiologic parameters and/or application of advanced technology(s), critical care may be provided in life threatening situations when these elements are not present. Critical care may be provided on multiple days, even if no changes are made in the treatment rendered to the patient, provided that the patient's condition continues to require the level of attention described above.”
13

Critical Care: CMS
• “… critical care services encompass both treatment of ‘vital organ failure’ and ‘prevention of further life threatening deterioration of the patient’s condition.’ Therefore, although critical care may be delivered in a moment of crisis or upon being called to the patient’s bedside emergently, this is not a requirement for providing critical care service. The treatment and management of the patient’s condition, while not necessarily emergent, shall be required, based on the threat of imminent deterioration (i.e., the patient shall be critically ill or injured at the time of the physician’s visit).”
• http://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/downloads/R1548CP.pdf, Section B
14

Critical Care: Examples
• An 81 year old male patient is admitted to the intensive care unit following abdominal aortic aneurysm resection. Two days after surgery he requires fluids and vasopressors to maintain adequate perfusion and arterial pressures. He remains ventilator dependent.
• A 67 year old female patient is three days status post mitral valve repair. She develops petechiae, hypotension, and hypoxia requiring respiratory and circulatory support.
• A 70 year old admitted for right lower lobe pneumococcal pneumonia with a history of COPD becomes hypoxic and hypotensive two days after admission.
• A 68 year old admitted for an acute anterior wall myocardial infarction continues to have symptomatic ventricular tachycardia that is marginally responsive to antiarrhythmic therapy.
• https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/downloads/MM5993.pdf
15

Office Visit & Screening Colonoscopy: No EM for Healthy Patient Screening • How do I bill for a patient seen in our office prior to a screening
colonoscopy with no GI symptoms and who is otherwise healthy? A visit prior to a screening colonoscopy for a healthy patient is not billable.
• American Gastroenterological Association, http://www.gastro.org/practice/coding/coding-faqs-screening-colonoscopy#s1
16

Office Visit & Screening Colonoscopy: EM When Treating a Chronic Condition Prior to Screening
To bill a New Patient or Established Patient visit, the patient must require a medically necessary intervention
that the gastroenterologist performs prior to the procedure • Example: Coumadin
17

Prescription Drug Management: Weighing Medication = Moderate Risk Table of Risk lists prescription drug management as a common clinical example of moderate risk.
The provider has to evaluate:
• the suitability of the patient for the medication,
• weigh the benefits and risks of the patient’s disease process and reaction to the medication
• until the next time the provider sees the patient.
18
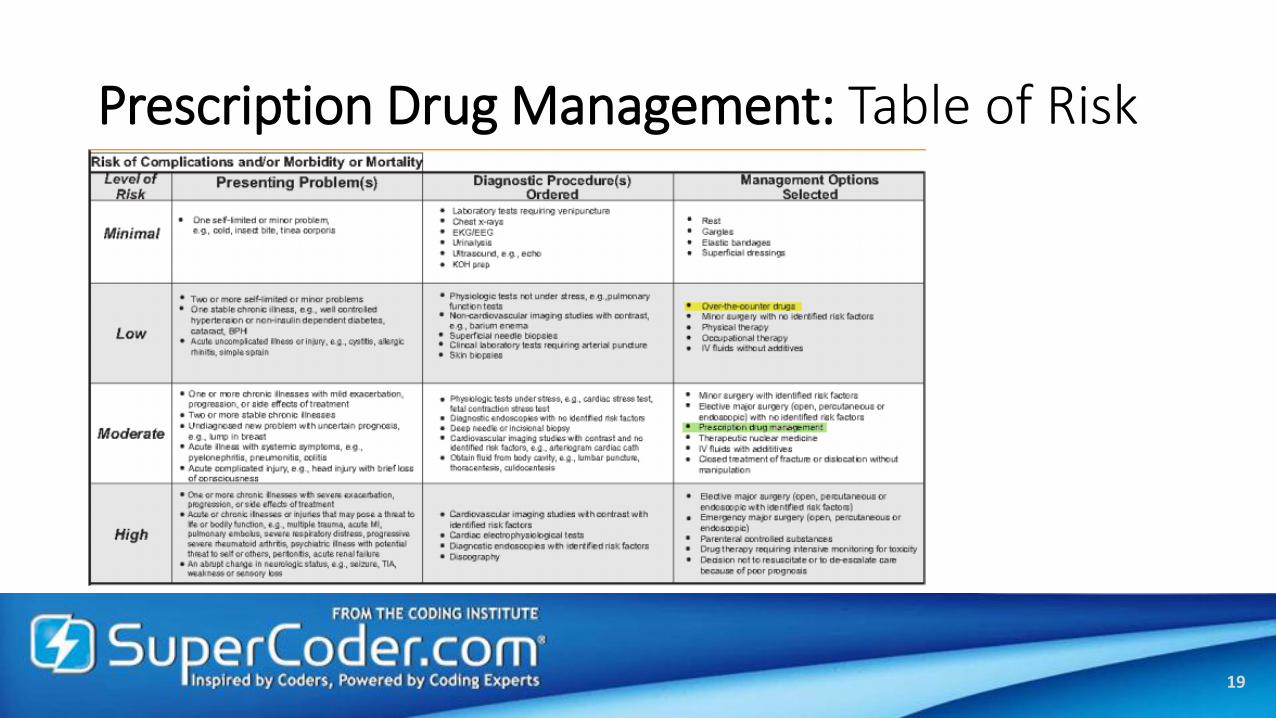
Prescription Drug Management: Table of Risk
19

Prescription Drug Management: Assigning Moderate Risk
What Counts
Dosage adjustment
Brand adjustment
Prescription samples
Treating physician
What Does Not
OTC
Review in PFSH
PQRS measure
EHR pulling forward
Reviewing provider
20

Examination: Joint Stability Tests Commonly Overlooked on 1997 Musculoskeletal Exam
• Anterior Stability Testing • Lachmans Test • Anterior Drawer Test • Pivot Shift Test • KT-1000 Test
• Posterior Stability Testing • Tibial Drop Back Sign • Quad Active Test • Posterior Drawer Test
• Medial Stability Testing • Valgus Stress Test at 0 • Valgus Stress Test at 30 –Flex • Anteromedial Drawer Test
• Posterolateral Stability Testing • External Rotation Recurvatum Test • Varus Stress at 0 • Varus Stress at 30- Flex • Posterolateral Drawer Test • Dial Test at 30 • Dial Test at 90 • Reverse Pivot Shift • Figure 4 Test • Gait Analysis
21
Musculoskeletal, Examination of joints bones and muscles per lower extremity: Assessment of stability with notation of any dislocation (luxation), subluxation, or laxity (per lower extremity) • Tibiofemoral Joint Exam, Assessment of Tibiofemoral Joint

E/M Auditor: Calculates Each Extremity Per Allowance
22

Examination: Novitas Detailed Using 4x4 = 4 Tests in 4 Body Systems • 4 elements examined in 4 body areas or 4 organ systems satisfies a detailed examination
• Clinical inference overrides the 4 x 4 tool • less than 4x4 can be a detailed exam based on the reviewers clinical judgment
• nurse reviewers: • follow the guidelines for auditing E/M services that are provided by CMS and AMA • use their clinical knowledge while reviewing the medical record documentation to determine the
correct and appropriate level of care • utilize one of the following when making a determination on whether an examination is expanded
problem focused or detailed. The method chosen must be the one that is most beneficial to the physician.
• 1997 E&M examination guidelines, • 1995 E&M examination guidelines utilizing the 4 x 4 tool, or • 1995 E&M examination guidelines utilizing clinical inference
• Novitas Solutions, Evaluation and Management Services, Date Posted: 10/05/2009, Date Reviewed: 10/20/2014
23

Examination: Babinski Test Can Be Counted 3 Ways
Medical Info
Reflex occurs after the sole of the foot has been firmly stroked. The big toe then moves upward or toward the top surface of the foot. The other toes fan out.
• normal in children up to 2 years old.
• Abnormal when present in a child older than 2 years or in an adult
• sign of a brain or nervous system disorder.
Count Under: • 1997 Musculoskeletal Exam,
Neurological/Psychiatric • Examination of deep tendon reflexes and/or
nerve stretch test with notation of pathological reflexes (e.g. Babinski)
• 1997 General Multisystem, Neurologic • Examination of deep tendon reflexes with
notation of pathological reflexes (e.g. Babinski)
• 1995 Organ Systems, Neurologic
24
Babinski reflex, Extensor plantar reflex, Babinski sign
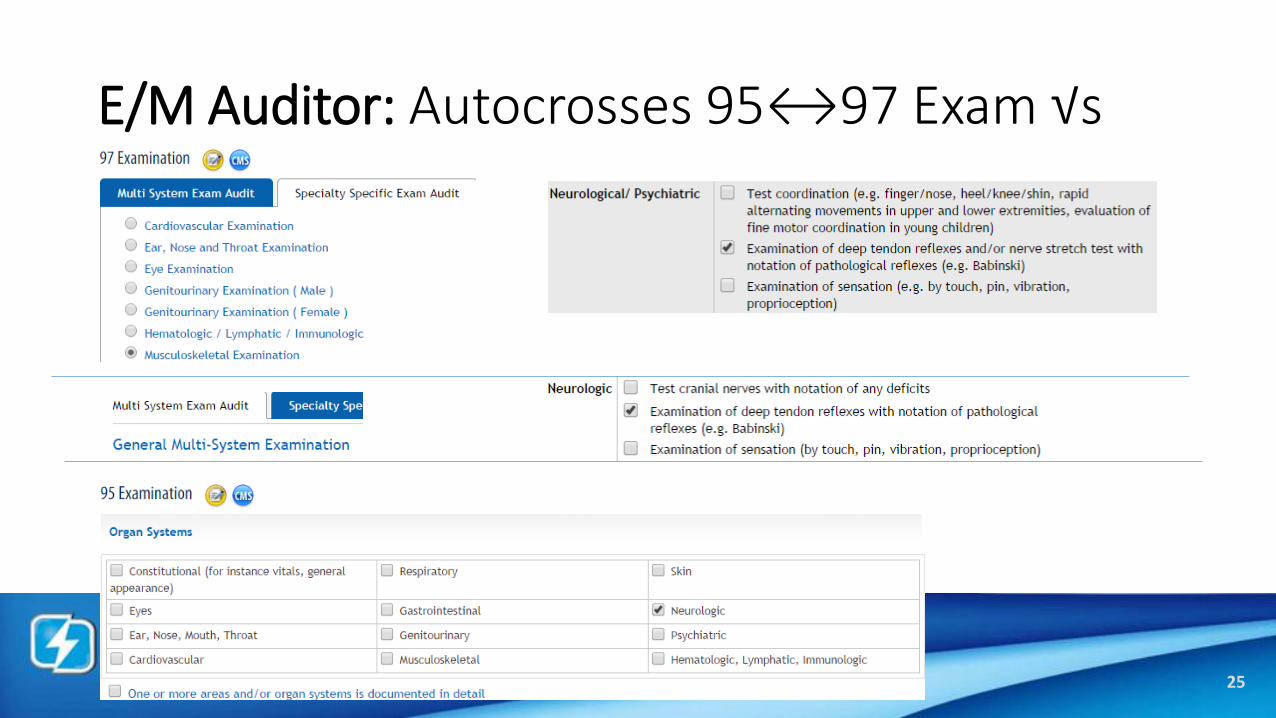
E/M Auditor: Autocrosses 95↔97 Exam √s
25

Examination: Psychiatric 1995 Examc
26
27
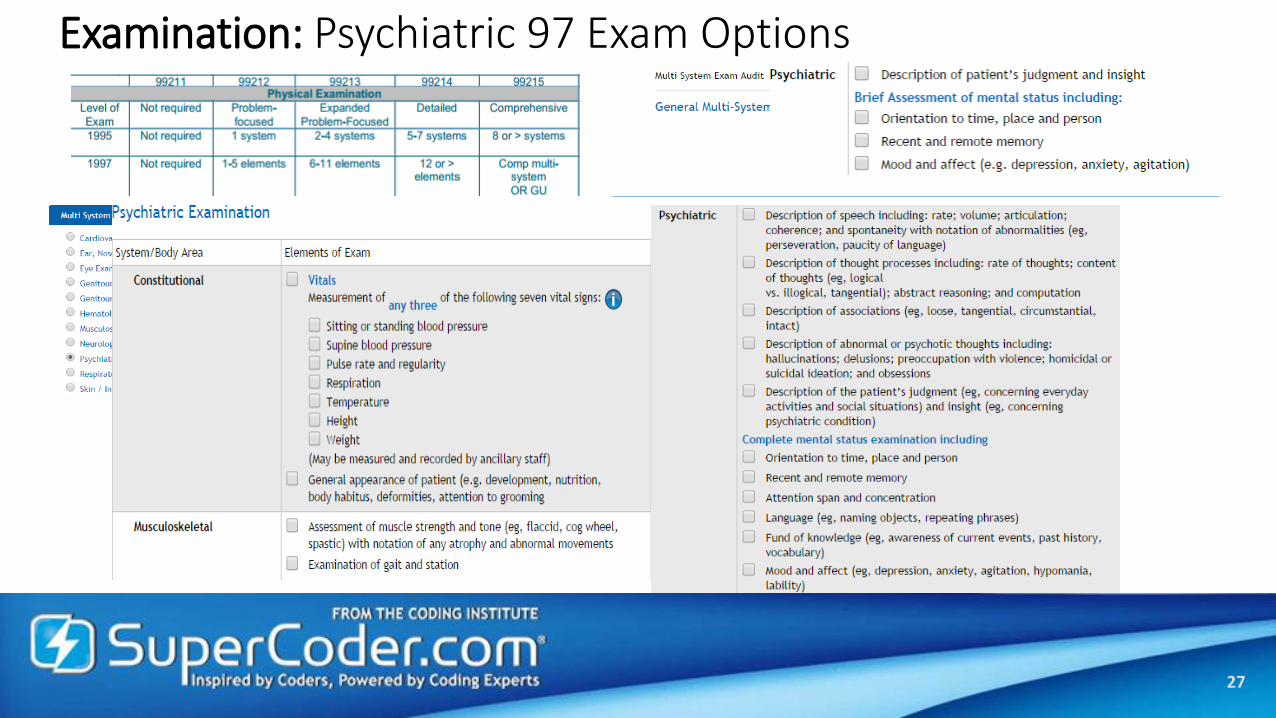
Examination: Psychiatric 97 Exam Options

Double Dipping: Don’t Follow the Urban Legend • originated from misunderstanding at CMS 1997 Train the Trainer
Conference
• Article misinterpreted HCFA director, Bart McCann, MD comment "cannot use one statement to count as two elements"
• Reality: cannot use a single statement to count as two elements within the same component.
• Examples: • " started yesterday" cannot be considered timing and duration within the same HPI
• "no chest pain" cannot be used as cardiovascular and musculoskeletal in the ROS.
28

Double Dipping:
• Mason Smith, MD asked for clarification about using the same statement for HPI and ROS stating "if a notation is made in the HPI section it logically follows that the system relating to the HPI question was reviewed and should be given credit in the ROS“
• "It is not necessary to mention an item of history twice in order to meet the guidelines for Review of Systems. Repetition of information or data is not required as long as it is appropriately referred to. Once should be enough." - John H. Lindberg, MD, Medical Director response
• "We agree with Dr. Lindberg that it is not necessary to mention an item of history twice in order to meet the Documentation Guidelines requirements for the ROS. It is important that the information which is provided can be inferred accurately and appropriately by a reviewer to determine level of service and medical necessity." - Barton C. McCann, MD
• "I do not believe that it is necessary to write the same information in two places in order for it to "count" for E/M coding. I simply believe that you should not try to count a single bit of information twice (i.e., count it as both HPI and ROS). For example, if an associated symptom is written in the HPI section, you must decide whether that information was gathered in obtaining a history of the present illness (as defined by CPT) or whether it was obtained as part of a systems review (also defined by CPT). You may count it in either part of the history regardless of where it is written but you may not count it in both places regardless of whether it is written once or twice." I reviewed a letter from Bart McCann (then at CMS) and one from a CMD from another carrier (I can't think of which one it was now) to the ACEP some time ago regarding this issue. If you have more current information from CMS on this topic, I would be happy to review it." - Deborah Patterson, Texas Trailblazer Medical Director
• www.acep.org.
29

Double Dipping: Opposite Stance
• “I would be willing to accept an element documented as associated signs or symptoms in the HPI as an element of the review of systems. However, in a clearly documented chart it should not be necessary to do so.” - Stephen Boren, MD, WPS Illinois Carrier Medical Director
• “When a provider is establishing the History of the Present Illness (HPI)from a patient, they usually include the pertinent positives and negatives which ordinarily would be part of the ROS. For example, if a doctor is interviewing a patient whose chief complaint is chest pain, questions regarding the character of the pain, what brings it on, what relieves it, if there is SOB, etc.are included in the HPI. For the ROS, the note could say "Cardiovascular: see HPI." So, these questions do not need to be repeated in the ROS to be given credit for them.”
• WPS, June 2003
30

Double Dipping: Look at CC, HPI, ROS
• abdominal pain where the MD inquired about the presence of nausea. • looked beyond the presenting problem
and as such has performed an expanded problem focused history.
• presenting problem of abdominal pain without additional information • do not count single statement as a chief
complaint, location in the HPI and a GI ROS
• no indication that the MD has done anything other than identify the presenting problem.
31

Double Dipping: Novitas
• When scoring the review of systems (ROS), can you use the systems addressed in the history of present illness (HPI) elements or is that "double dipping"?
• ROS inquiries are questions concerning the system(s) directly related to the problem(s) identified in the HPI. Therefore, it is not considered "double dipping" to use the system(s) addressed in the HPI for ROS credit.
• Novitas, Date Posted: 10/16/2009, Date Reviewed: 10/20/2014
32

Double Dipping: WPS
• Can a physician count a single history item in both the HPI and ROS? For example, could we count "shortness of breath" as an associated sign and symptom in the HPI and respiratory system in the ROS?
• A clearly documented medical record would prevent the need to "double-dip" for HPI and ROS, but WPS Medicare, in rare circumstances, could accept counting one statement in both areas if necessary.
• WPS, J5, History Element Of E/M (Q&As)
33

Assistant at Surgery: Check Fee Schedule Allowance
34

Assistant at Surgery: Another Option Is to Check Modifier Crosswalk
35

EHRs: Consider Only Medically Necessary Info
• “Documentation is considered cloned when each entry in the medical record for a beneficiary is worded exactly like or similar to the previous entries. Cloning also occurs when medical documentation is exactly the same from beneficiary to beneficiary. It would not be expected that every patient had the exact same problem, symptoms, and required the exact same treatment.”
• First Coast further states that discovery of this type of documentation will “result in denial of services for lack of medical necessity and recoupment of all overpayments made.”
• First Coast Service Options, the MAC in Florida, prohibited the practice of cloning in its 2006 Medicare Part B newsletter (http://medicare.fcso.com/Publications_A/2006/138374.pdf)

EHRs: OIG Warns of New Vulnerabilities
CMS and its contractors need to revise their approaches to protect against fraud and abuse. • clues within the progress notes, handwriting styles, and other attributes
that help corroborate the authenticity of paper medical records are largely absent in EHRs.
• tracing authorship and documentation in an EHR may not be as straightforward as tracing in a paper record. Health care providers can use EHR software features that may mask true authorship of the medical record and distort information in the record to inflate healthcare claims.
• OIG January 2014. http://oig.hhs.gov/oei/reports/oei-01-11-00571.pdf

EHRs: Features Can Perpetuate Fraud
• technology can make it easier to commit fraud. • Certain EHR documentation features, if poorly designed or used
inappropriately, can result in poor data quality or fraud. • Copy-Pasting (AKA cloning), enables users to select information from one
source and replicate it in another location. • When doctors, nurses, or other clinicians copy-paste information but fail to update it
or ensure accuracy, inaccurate information may enter the patient’s medical record and inappropriate charges may be billed to patients and third-party health care payers.
• inappropriate copy-pasting could facilitate attempts to inflate claims and duplicate or create fraudulent claims.
EHRs: Don’t Code Overdocumentation
• Definition - the practice of inserting false or irrelevant documentation to create the appearance of support for billing higher level services.
• EHR features can produce information suggesting the practitioner performed more comprehensive services than were actually rendered.
1. auto-populate fields in templates built into the system.
2. extensive documentation generation on the basis of a single click of a checkbox, which if not appropriately edited by the provider may be inaccurate.

EHRs: Contractors Can Identify Overdocumentation More Than Copied Language

EHRs: Contractors Received Limited Guidance

EHRs: Best Habits
• The physician or NPP must always document the HPI based on the patient’s description that day.
• Only document those Review of Systems elements that are relevant to the nature of the presenting problems
• Only use medical, family, and social history from a previous date of service if you reviewed the information with the patient that day and it is relevant to that day’s visit
• Double check that the diagnoses in the assessment are only those addressed at that visit. Do not copy and paste all of the diagnoses listed in the problem list or used for PQRS.
• Use exam templates with care, editing them thoroughly and being sure to adjust any medications, specific findings and definitive diagnoses..
• Pay attention to information copy and pasted from another group. Be sure an audit record shows who the author is so that new and established patient status is kept clear. Remember that only the medically necessary work for the nature of the presenting problem are counted in compliant coding.
• Trust your gut and record the cumulative narrative as you usually would without a given system.

Protect E/M Payments for $40 Less
5 Reasons Why You Need E/M Auditor: • Increased Productivity: Automatically calculates 1995 and 1997 levels at the same time eliminating double
auditing of unsupported EM encounters.
• Protected Payments: Insurers are recouping millions of dollars on visits coded based on time. This checklist safeguards time-based encounter pay.
• Improved Documentation: Each EM element includes quotes from CMS Evaluation and Management Documentation Guidelines and AMA CPT® to instantly support compliance audits.
• Compliant 99205s: EM Auditor automatically readjusts review of systems scores for high level codes that have different requirements than lower level codes ensuring 99205 and 99223s withstand scrutiny.
• Trusted Experts: Use the same audit compliance software developed and used by the expert coders and auditors of SuperCoder and the Coding Institute who thousands of clients rely on for authoritative guidance on evaluation and management coding.
43
Save 10% on orders placed through Nov. 21, 2014. Use promo code EM10.

Resources
• www.acep.org.
• American Gastroenterological Association, http://www.gastro.org/practice/coding/coding-faqs-screening-colonoscopy#s1
• https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/downloads/MM5993.pdf
• First Coast Service Options, http://medicare.fcso.com/Publications_A/2006/138374.pdf
• IPPS: http://www.gpo.gov/fdsys/pkg/FR-2014-08-22/pdf/2014-18545.pdf
• Novitas Solutions, Evaluation and Management Services, Date Posted: 10/05/2009, Date Reviewed: 10/20/2014, http://goo.gl/qcVkXx
• OIG January 2014. http://oig.hhs.gov/oei/reports/oei-01-11-00571.pdf
• SuperCoder, E/M Auditor
• SuperCoder, Multispecialty Power Pack
• WPS, J5, History Element Of E/M (Q&As), goo.gl/5TdBvi
44
Thank You from SuperCoder!
• Questions
• Future References: • Auditing and Consulting
• Ask an Expert
• Coding Con, Dec. 5-7, 2014, Orlando, FL
• SuperCoding on Demand
45
AAPC Certificate of Attendance for 1 CEU will be emailed to each live attendee’s email id by the end of November 2014.