Embed Size (px)
Citation preview

5/24/10
1
Type 2 Diabetes – Use of Insulin
Robert J. Rushakoff, MD Professor of Medicine
University of California, San Francisco
Today
Quick Year in Review Why do some patients need to take
insulin Insulin Basics Studies on Use of Insulin Actual Use of Insulin
Survival as a function of HbA1c in people with type 2 diabetes: a retrospective cohort study
Lancet. 2010. 375:481-489 Hazard ratios for progression to first large-vessel disease event by HbA1c
5/24/10
2
CVD Intervention Studies
ADVANCE ACCORD VA
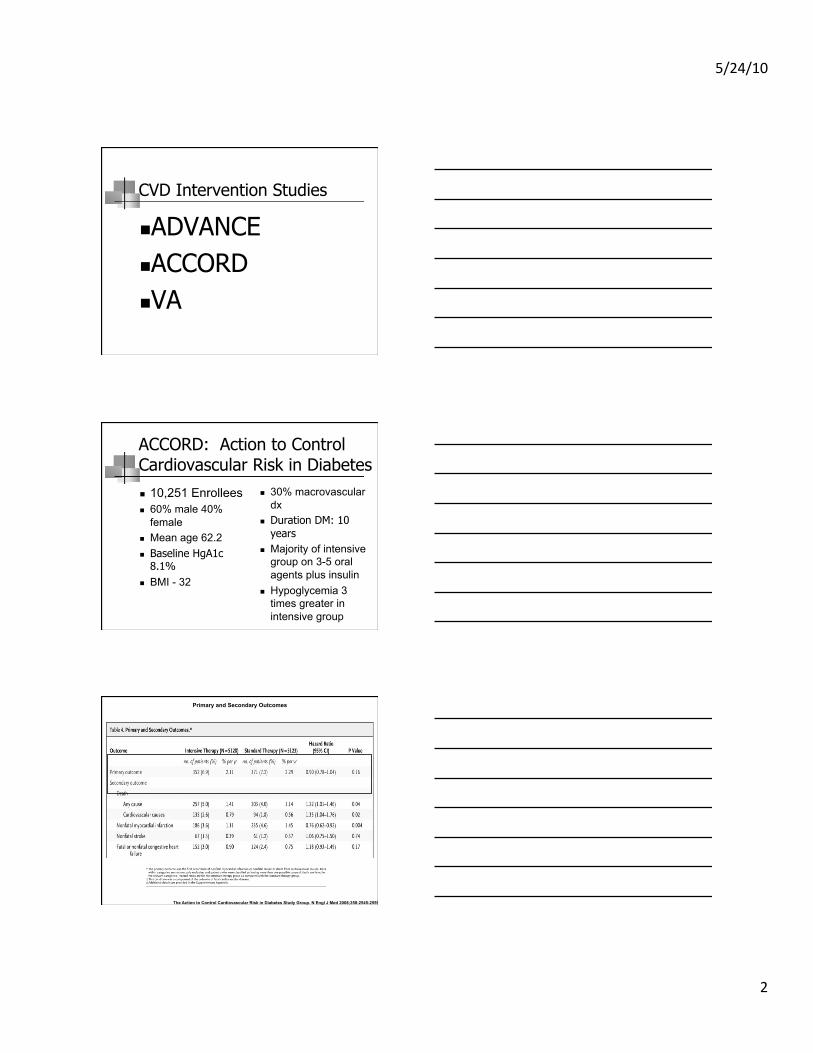
ACCORD: Action to Control Cardiovascular Risk in Diabetes
10,251 Enrollees 60% male 40%
female Mean age 62.2 Baseline HgA1c
8.1% BMI - 32
30% macrovascular dx
Duration DM: 10 years
Majority of intensive group on 3-5 oral agents plus insulin
Hypoglycemia 3 times greater in intensive group
The Action to Control Cardiovascular Risk in Diabetes Study Group. N Engl J Med 2008;358:2545-2559
Primary and Secondary Outcomes

5/24/10
3
ACCORD: Hazard Ratios for the Primary Outcome and Death from Any Cause in Prespecified Subgroups
The Action to Control Cardiovascular Risk in Diabetes Study Group. N Engl J Med 2008;358:2545-2559
Diabetes Care May 2010 vol. 33 no. 5 983-990
Epidemiologic Relationships Between A1C and All-Cause Mortality During a Median 3.4-Year Follow-up of Glycemic Treatment in the ACCORD Trial
Diabetes Care May 2010 vol. 33 no. 5 983-990
Epidemiologic Relationships Between A1C and All-Cause Mortality During a Median 3.4-Year Follow-up of Glycemic Treatment in the ACCORD Trial

5/24/10
4
The ACCORD Study Group. N Engl J Med 2010;10.1056/NEJMoa1001286
Mean Systolic Blood-Pressure Levels at Each Study Visit
Effects of Intensive Blood-Pressure Control in Type 2 Diabetes Mellitus
The ACCORD Study Group. N Engl J Med 2010;10.1056/NEJMoa1001282
Lipid Values
Effects of Combination Lipid Therapy in Type 2 Diabetes Mellitus

5/24/10
5
The ACCORD Study Group. N Engl J Med 2010;10.1056/NEJMoa1001286
Effects of Intensive Blood-Pressure Control and Combination Lipid Therapy in Type 2 Diabetes Mellitus
Kaplan-Meier Analysis of Primary Outcome in the ACCORD Study
The ACCORD Study Group. N Engl J Med 2010;10.1056/NEJMoa1001282
“The interpretation of the ACCORD BP results is
complicated by the fact that the event rate observed in the
standard-therapy group was almost 50% lower than the
expected rate.”
The ACCORD Study Group. N Engl J Med 2010;10.1056/NEJMoa1001286
Effects of Intensive Blood-Pressure Control in Type 2 Diabetes Mellitus
The ACCORD Study Group. N Engl J Med 2010;10.1056/NEJMoa1001282
Hazard Ratios for the Primary Outcome in Prespecified Subgroups
Effects of Combination Lipid Therapy in Type 2 Diabetes Mellitus

5/24/10
6
Metformin and B12 • Decrease in vitamin
B12 levels. (decreased 4.2-47%)
• Metformin is thought to induce malabsorption of vitamin B12 and intrinsic factor in the ileum, an effect that can be reversed by increased calcium intake.
Long term treatment with metformin in patients with type 2 diabetes and risk of vitamin B-12 deficiency: randomized
placebo controlled trial
BMJ 2010;340:c2181
Metformin and B12 • Anemia may be
minimal to severe
• may present only as a peripheral neuropathy, possibly being misdiagnosed as diabetic neuropathy.
5/24/10
7
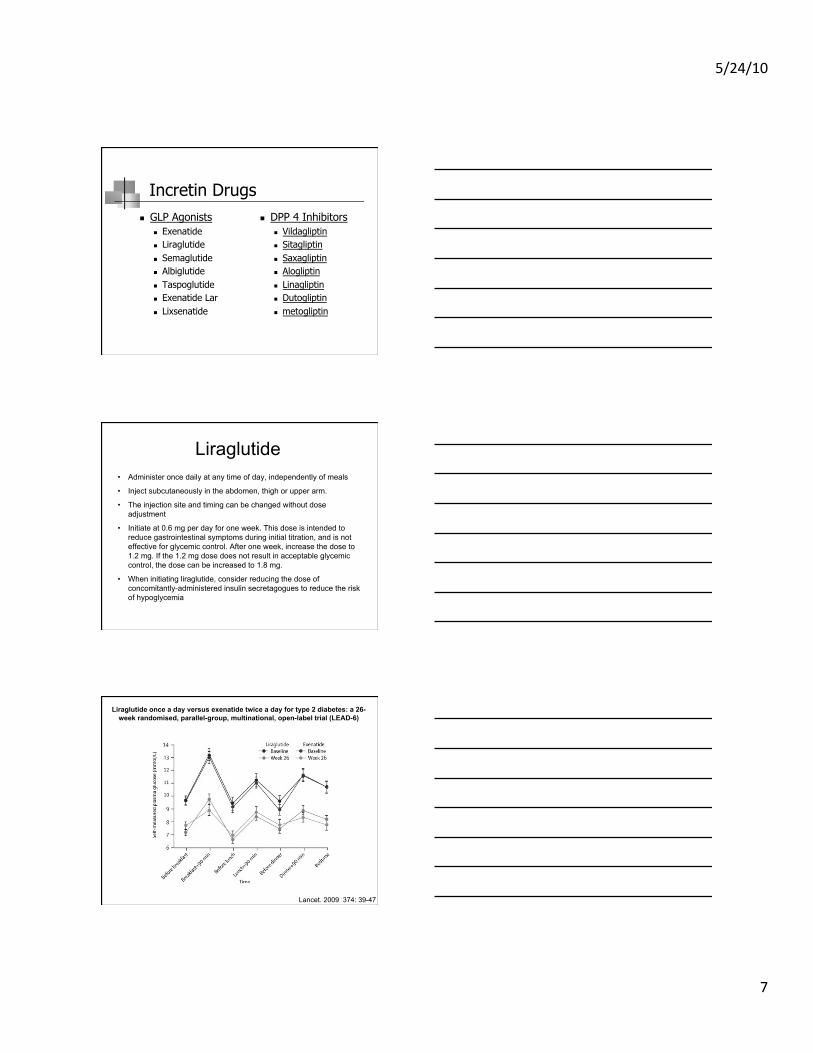
Incretin Drugs GLP Agonists
Exenatide Liraglutide Semaglutide Albiglutide Taspoglutide Exenatide Lar Lixsenatide
DPP 4 Inhibitors Vildagliptin Sitagliptin Saxagliptin Alogliptin Linagliptin Dutogliptin metogliptin
Liraglutide • Administer once daily at any time of day, independently of meals
• Inject subcutaneously in the abdomen, thigh or upper arm.
• The injection site and timing can be changed without dose adjustment
• Initiate at 0.6 mg per day for one week. This dose is intended to reduce gastrointestinal symptoms during initial titration, and is not effective for glycemic control. After one week, increase the dose to 1.2 mg. If the 1.2 mg dose does not result in acceptable glycemic control, the dose can be increased to 1.8 mg.
• When initiating liraglutide, consider reducing the dose of concomitantly-administered insulin secretagogues to reduce the risk of hypoglycemia
Liraglutide once a day versus exenatide twice a day for type 2 diabetes: a 26-week randomised, parallel-group, multinational, open-label trial (LEAD-6)
Lancet. 2009 374: 39-47
5/24/10
8
Diabetic Patients’ Medication Underuse, Illness Outcomes, and Beliefs About Antihyperglycemic and
Antihypertensive Treatments
• Perceived need for antihyperglycemic medication was associated with being younger, being prescribed insulin, and being prescribed multiple medications.
• Concern about antihyperglycemic medications was associated with being younger, African American, dissatisfied with information received about medication, and of low health literacy
Diabetes Care January 2009 32 19-24
Medication Adherence • OHA -- retrospective analysis:
– 36-93% remain on treatment for 6-24 months. – Prospective electronic monitoring – 67-85% to as
prescribed. – Insulin adherence in type 2 was 62-64%.
Diabetes Care 27:1218-1224, 2004
• Patients with Type 2 DM who do not obtain at least 80% of their oral antihyperglycemic medications across 1 year are at a higher risk of hospitalization in the following year.
Diabetes Care 27:2149-2153, 2004.
5/24/10
9
Medication Adherence Problems Paying Out-of Pocket Medication Costs
Among Older Adults with Diabetes • In past year:
– 19% cut back on medication for cost – 11% cut back on DM meds – 7% cut back at least once per month – 28% reported forgoing food or other essentials to pay
medication costs
Diabetes Care 27:384-391, 2004
What does this mean? Why is it occurring?
Changing goals Compliance
Wrong diagnosis Problem with oral hypoglycemic agent Natural progression of disease
Type 2 Diabetes: What to do when the pills don’t work
Latent Autoimmune Diabetes In Adults
Patients usually aged > 25 Clinical presentation “masquerading” as
nonobese type 2 diabetes Initial control achieved with diet alone
or diet and oral hypoglycemic agents Insulin dependency occurs within
months but can take 10 years

5/24/10
10
Latent Autoimmune Diabetes In Adults
Other features of type 1 diabetes: Low fasting and postglucagon stimulated
C-peptide HLA susceptibility alleles ICA + Anti-GAD +
Newly Diagnoses type 2 diabetics in UKPDS
ICA 6% Anti GAD 10% both 4%
What does this mean? Why is it occurring?
Changing goals Compliance Wrong diagnosis
Problem with oral hypoglycemic agent
Natural progression of disease
Type 2 Diabetes: What to do when the pills don’t work
Metformin and eGFR • 186 x (Creat / 88.4)-1.154 x (Age)-0.203 x (0.742 if female) x
(1.210 if black) • Current Guidelines call for discontinuation of Metformin
serum creatinine >150 umol/l (1.7 mg/dl). • Estimated GFR (eGFR) being introduced as possible
better measure of renal function than serum creatinine alone
• eGFR of 36 ml/min per 1.73m2 would be somewhat neutral to current use
5/24/10
11
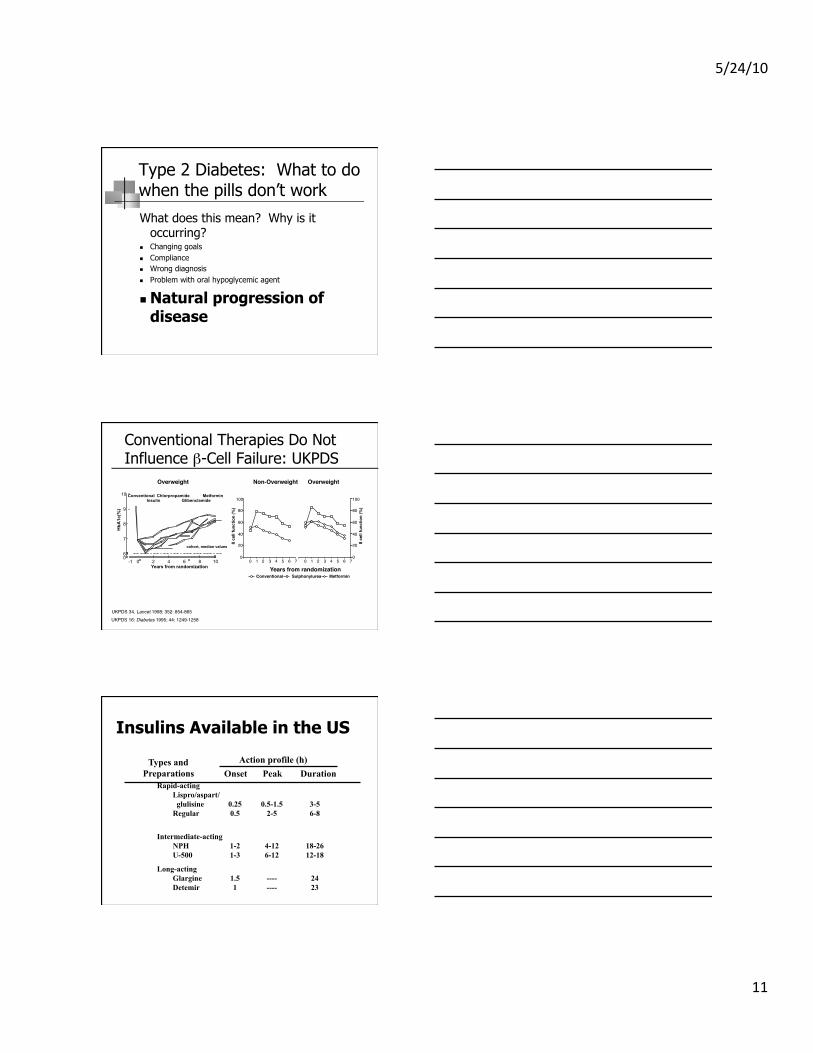
What does this mean? Why is it occurring?
Changing goals Compliance Wrong diagnosis Problem with oral hypoglycemic agent
Natural progression of disease
Type 2 Diabetes: What to do when the pills don’t work
Conventional Therapies Do Not Influence β-Cell Failure: UKPDS
UKPDS 34. Lancet 1998; 352: 854-865!UKPDS 16: Diabetes 1995; 44: 1249-1258!
cohort, median values!0!6!
7!
8!
9!
10!
-1! 0! 2! 4! 6! 8! 10!Years from randomization!
Chlorpropamide!Conventional!Glibenclamide!Insulin! Metformin!
HbA
1c(%
)!
0!20!40!60!80!
100!
0! 1! 2! 3! 4! 5! 6! 7!
ß ce
ll fu
nctio
n (%
)!
0!20!40!60!80!100!
0! 1! 2! 3! 4! 5! 6! 7!
ß ce
ll fu
nctio
n (%
)!
Years from randomization!Conventional! Sulphonylurea! Metformin!
Overweight!Non-Overweight!Overweight!
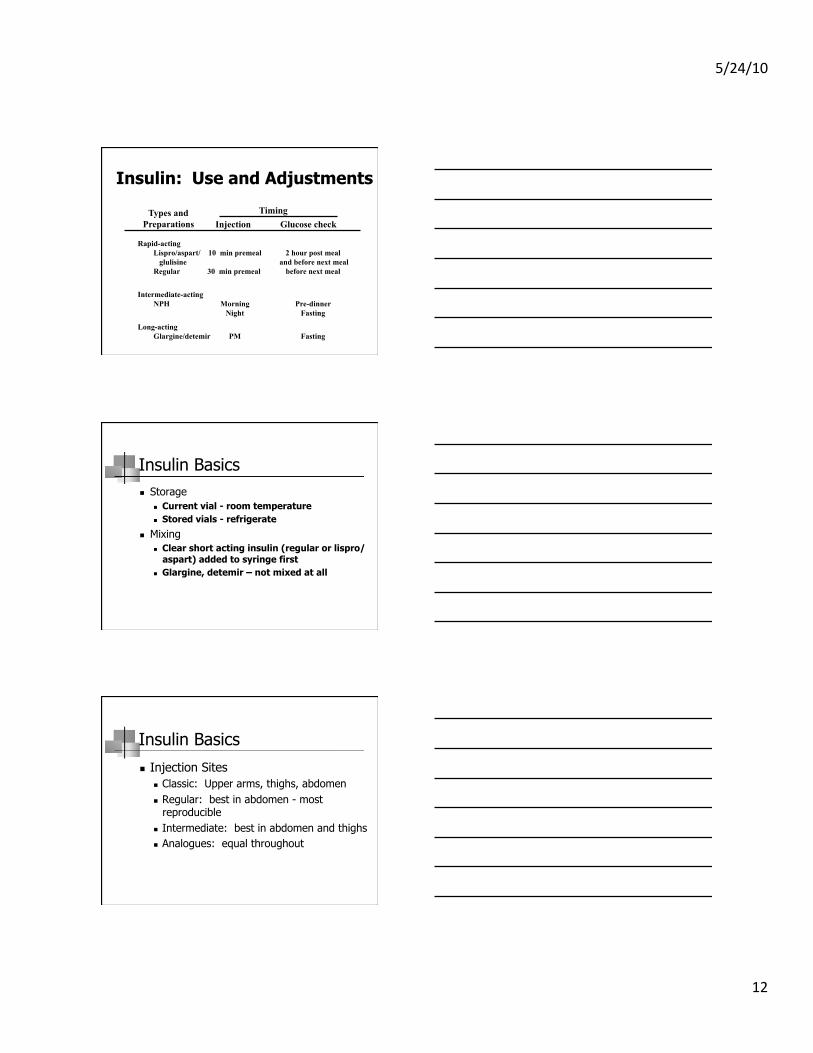
Insulins Available in the US
Types and Preparations
Action profile (h) Onset Peak Duration
Rapid-acting Lispro/aspart/ glulisine 0.25 0.5-1.5 3-5 Regular 0.5 2-5 6-8
Intermediate-acting NPH 1-2 4-12 18-26 U-500 1-3 6-12 12-18
Long-acting Glargine 1.5 ---- 24 Detemir 1 ---- 23
5/24/10
12
Insulin: Use and Adjustments
Types and Preparations
Timing Injection Glucose check
Rapid-acting Lispro/aspart/ 10 min premeal 2 hour post meal glulisine and before next meal Regular 30 min premeal before next meal
Intermediate-acting NPH Morning Pre-dinner Night Fasting
Long-acting Glargine/detemir PM Fasting
Insulin Basics Storage
Current vial - room temperature Stored vials - refrigerate
Mixing Clear short acting insulin (regular or lispro/
aspart) added to syringe first Glargine, detemir – not mixed at all
Insulin Basics
Injection Sites Classic: Upper arms, thighs, abdomen Regular: best in abdomen - most
reproducible Intermediate: best in abdomen and thighs Analogues: equal throughout
5/24/10
13
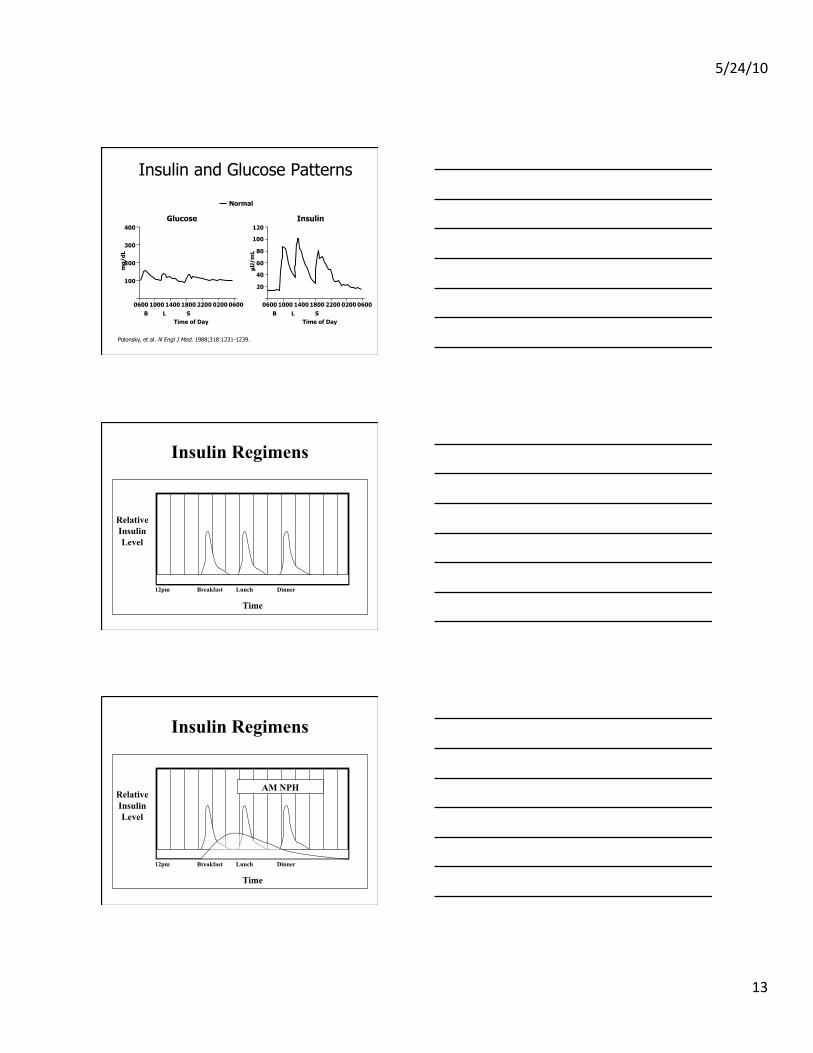
Insulin and Glucose Patterns
Polonsky, et al. N Engl J Med. 1988;318:1231-1239.
100
200
300
400 Glucose Insulin
0600 1000 1800 1400 0200 2200 0600
Time of Day
0600 1000 1800 1400 0200 2200 0600
Time of Day
20 40 60 80
100 120
B L S B L S
Normal
mg/
dL
µU
/mL
Relative Insulin Level
Time
Breakfast 12pm Lunch Dinner
Insulin Regimens
Relative Insulin Level
Time
Breakfast 12pm
AM NPH
Lunch Dinner
Insulin Regimens

5/24/10
14
Relative Insulin Level
Time
Breakfast
PM NPH
Lunch Dinner
NPH
12pm
Insulin Regimens
Profiles of glucose over 24 hours both before (broken line) and after (solid line) treatment of a group of individuals with type 2 diabetes with a single injection of neutral protamine Hagedorn
insulin at bedtime titrated to control fasting glucose. The glucose curve is shifted downward, with nearly normal fasting levels
achieved but also with persistence of postprandial increments
Diabetes Care 18 (1995), pp. 843–851
Relative Insulin Level
Time
Breakfast
BID NPH
Lunch Dinner
NPH
12pm
Insulin Regimens

5/24/10
15
Relative Insulin Level
Time
Breakfast
BID R and NPH
Lunch Dinner
NPH
regular
12pm
Insulin Regimens
Relative Insulin Level
Time
Breakfast
BID R and NPH
Lunch Dinner
NPH
regular
12pm
Insulin Regimens
Relative Insulin Level
Time
Breakfast
TID R and hs NPH
Lunch Dinner
NPH
regular
12pm
Insulin Regimens

5/24/10
16
Relative Insulin Level
Time
Breakfast
BID lispro/aspart
Lunch Dinner
Long analogue
12pm
Lispro/aspart
Insulin Regimens
Relative Insulin Level
Time
Breakfast
TID lispro/aspart/glulisine and hs NPH
Lunch Dinner
NPH
Lispro/aspart/glulisine
12pm
Insulin Regimens

5/24/10
17
Relative Insulin Level
Time
Breakfast
TID lispro/aspart/glulisine and bid NPH
Lunch Dinner
NPH
Lispro/aspart/glulisine
12pm
Insulin Regimens
Relative Insulin Level
Time
Breakfast 12pm
PM glargine
Lunch Dinner
glargine
Insulin Regimens
Correcting Fasting Hyperglycemia…
100
200
300
Normal A1C 5%–6%
PG
(m
g/
dL)
0800 1200 1800 0800
Time of Day
Uncontrolled A1C ~9%
A1C ~6%
“Controlled” A1C <7%
Adapted with permission from Cefalu WT. In: Leahy J, Cefalu W, eds. Insulin Therapy. New York: Marcel Dekker; 2002:1

5/24/10
18
Relative Insulin Level
Time
Breakfast
TID lispro/aspart/glulisine and hs glargine
Lunch Dinner 12pm
glargine
Lispro/aspart/glulisine
Insulin Regimens
Relative Insulin Level
Time
Breakfast
Insulin pump
Lunch Dinner 12pm
Lispro/aspart/glulisine
Insulin Regimens
5/24/10
19
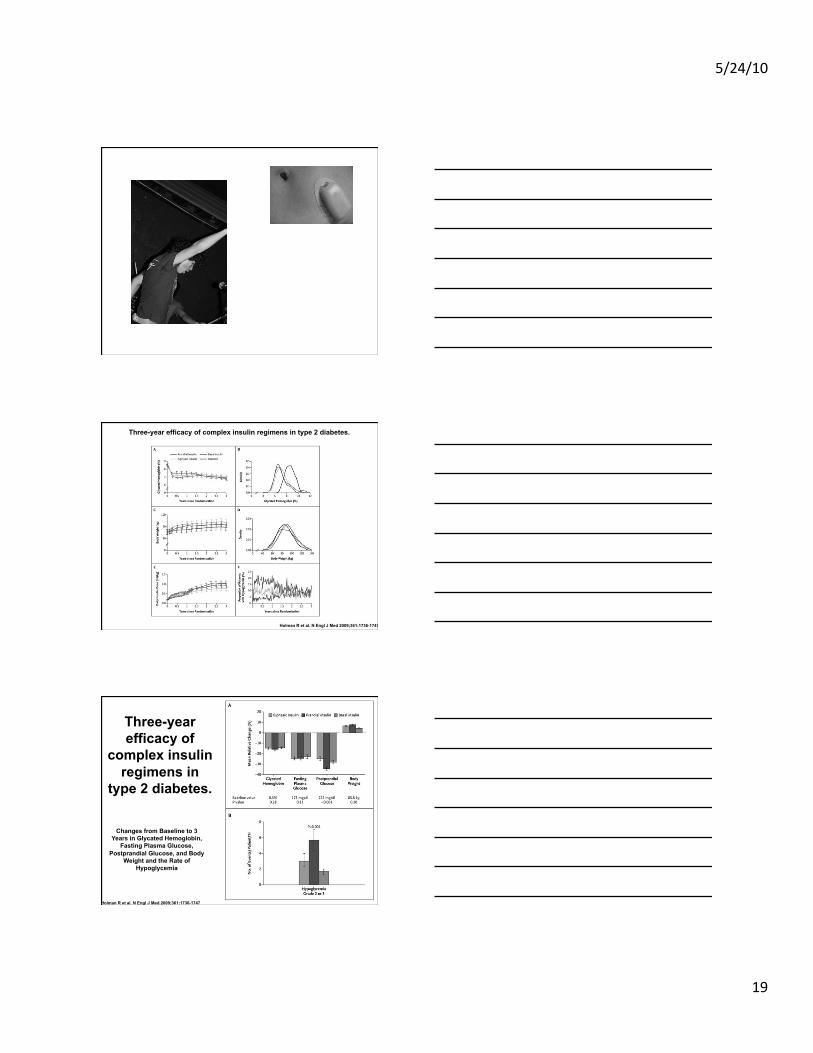
Holman R et al. N Engl J Med 2009;361:1736-1747
Three-year efficacy of complex insulin regimens in type 2 diabetes.
Holman R et al. N Engl J Med 2009;361:1736-1747
Changes from Baseline to 3 Years in Glycated Hemoglobin,
Fasting Plasma Glucose, Postprandial Glucose, and Body
Weight and the Rate of Hypoglycemia
Three-year efficacy of
complex insulin regimens in
type 2 diabetes.

5/24/10
20
Holman R et al. N Engl J Med 2009;361:1736-1747
Three-year efficacy of complex insulin regimens in type 2 diabetes.
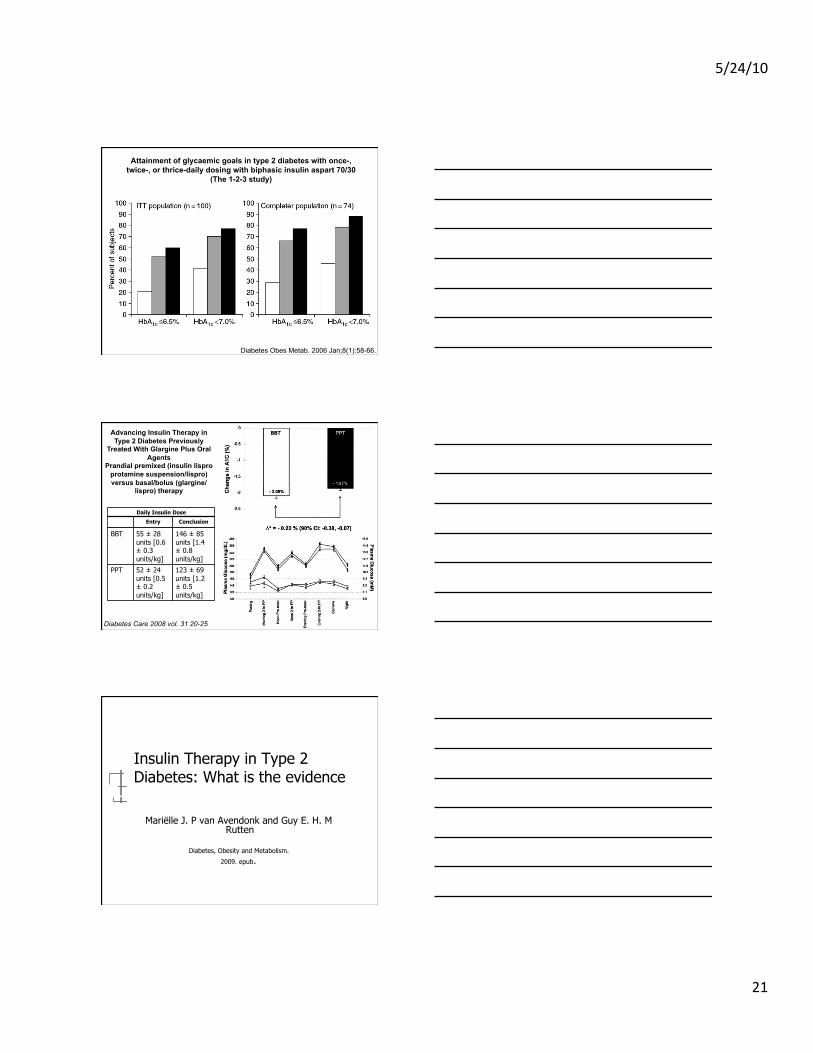
Attainment of glycaemic goals in type 2 diabetes with once-, twice-, or thrice-daily dosing with biphasic insulin aspart 70/30
(The 1-2-3 study)
Diabetes Obes Metab. 2006 Jan;8(1):58-66.
Attainment of glycaemic goals in type 2 diabetes with once-, twice-, or thrice-daily dosing with biphasic insulin aspart 70/30
(The 1-2-3 study)
Diabetes Obes Metab. 2006 Jan;8(1):58-66.
5/24/10
21
Attainment of glycaemic goals in type 2 diabetes with once-, twice-, or thrice-daily dosing with biphasic insulin aspart 70/30
(The 1-2-3 study)
Diabetes Obes Metab. 2006 Jan;8(1):58-66.
Advancing Insulin Therapy in Type 2 Diabetes Previously
Treated With Glargine Plus Oral Agents
Prandial premixed (insulin lispro protamine suspension/lispro) versus basal/bolus (glargine/
lispro) therapy
Diabetes Care 2008 vol. 31 20-25
Daily Insulin Dose
Entry Conclusion
BBT 55 ± 28 units [0.6 ± 0.3 units/kg]
146 ± 85 units [1.4 ± 0.8 units/kg]
PPT 52 ± 24 units [0.5 ± 0.2 units/kg]
123 ± 69 units [1.2 ± 0.5 units/kg]
Insulin Therapy in Type 2 Diabetes: What is the evidence
Mariëlle J. P van Avendonk and Guy E. H. M Rutten
Diabetes, Obesity and Metabolism.
2009. epub.

5/24/10
22
Insulin Therapy in Type 2 Diabetes: Bottom Line
Basal Insulin Premixed Insulin Basal Bolus
Insulin Therapy in Type 2 Diabetes: Bottom Line
Basal Insulin Continuing metformin and/or sulphonylurea after start
of therapy with basal long-acting insulin results in better glycemic control with less insulin requirements, less weight gain and less hypoglycemic events.
Long-acting insulin analogues in combination with oral medication are associated with similar glycemic control but fewer hypoglycemic episodes compared with NPH insulin.
Insulin Therapy in Type 2 Diabetes: Bottom Line
Premixed Insulin Most of the trials demonstrated better glycemic
control with premix insulin therapy than with a long-acting insulin once daily, but premix insulin causes more hypoglycemic episodes.
Analogue premix provides similar HbA1c, but lower postprandial glucose levels compared with human premix, without increase in hypoglycemic events or weight gain.

5/24/10
23
Insulin Therapy in Type 2 Diabetes: Bottom Line
Basal Bolus Drawing conclusions from the limited
number of studies concerning basal-bolus regimen seems not possible. Some studies showed that rapid-acting insulin analogues frequently result in a better HbA1c or postprandial glucose without increase of hypoglycemia than regular human insulin.
Insulin Therapy in Type 2 Diabetes: Bottom Line
A once-daily basal insulin regimen added to oral medication is an ideal starting point. All next steps, from one to two or even more injections per day should be taken very carefully and in thorough deliberation with the patient, who has to comply with such a regimen for many years
Starting Insulin–Patient Barriers
Using insulin as a threat Fear of injections Weight gain Insulin meaning they have bad diabetes
and now will get complications or die Worsening of atherosclerosis Patient leaves and does not come back

5/24/10
24
Starting Insulin
Home glucose Monitoring Reinforce basic diet Discuss reasons that the oral agents are
no longer adequate to control their diabetes
Teach insulin techniques
Starting Insulin Not at goal on Sulfonylurea, Metformin,
Thiazolidinedione, DPP 4 inhib, and/or GLP angonist
Option 1: Start am or hs glargine or hs detemir Start at about 10 Units Titrate up by 2-8 units every 5-7 days
based on fasting glucose level. ? Which other drugs to continue

5/24/10
25
When to go to > 1 shot per day HgA1c >7 or your goal
Morning or evening glucose remains > 140 mg/dl
Options
Split the glargine or detemir Glucose in AM at goal; Glucose before dinner >140 (pm shot)
Glucose in PM at goal; Glucose in AM >140 (am shot)
Add premeal lispro/aspart/glulisine
Change to bid premixed insulin – 70/30, 75/25
Questions
DC sulfonylurea
Continue metformin
? Thiazolidinedione
Insulin Name First Component
Second Component
Component Ratio
First:Second
Humulin 70/30 Human NPH Human Regular 70:30
Humalog 50/50 lispro protamine lispro 50:50
Humalog 75/25 lispro protamine lispro 75:25
Novolin 70/30 Human NPH Human Regular 70:30
Novolog 70/30 aspart protamine aspart 70:30
Premixed Insulins

5/24/10
26
Starting Insulin Patient on Sulfonylurea, Metformin and
Thiazolidinedione
Option 2: Start bid insulin – pre mixed Start at about 20 U am, 10 U pm Titrate up by 2-8 units every 5-7 days based on
fasting and pre dinner glucose levels. DC of sulfonylurea. Continue metformin, ??
Thiazolidinedione

5/24/10
27
A1c Control in a Primary Care Setting: Self-titrating an Insulin Analog Pre-mix (INITIATEplus Trial)
Am J Med 2009 11;122(11):1043-9
A1c Control in a Primary Care Setting: Self-titrating an Insulin Analog Pre-mix (INITIATEplus Trial)
Am J Med 2009 11;122(11):1043-9

5/24/10
28
Adjust to Target in Type
2 Diabetes: Comparison of
a simple algorithm with carbohydrate counting for
adjustment of mealtime
insulin glulisine
Diabetes Care 2008. 31.1305-1310 Diabetes Care 2008. 31.1305-1310
Diabetes Care 2008. 31.1305-1310
Adjust to Target in Type 2 Diabetes: Comparison of a simple algorithm with carbohydrate counting for adjustment of mealtime insulin glulisine

5/24/10
29
Amylin
37-amino acid β-cell hormone that is co-secreted with insulin in response to meals
Acts as a neuroendocrine hormone that binds to specific receptors in the hindbrain, including area postrema
Has both glucoregulatory and anorexigenic actions • decreases the rate of gastric emptying • suppresses hepatic glucose output by inhibiting glucagon secretion
Anti-obesity effects in diet-induced obese (DIO) rodents: • Reductions in food intake • Reductions in body fat, with preservation of lean mass
Pramlintide: Soluble Analog of Human Amylin
Adapted from Weyer C, et al. Curr Pharm Des 2001; 7:1353-73. Mack C, et al. Diabetes 2003; 52: A389. Schmitz O, et al. Diabetes 2004; 53:S233-S2381.
Human amylin
Amide S S A Y
T N S
G V N
T
T T T
N
A A A
L I
K S
S C
C Q R
L N
N N F
G
F L
V H
Pramlintide or Mealtime Insulin Added to Basal Insulin Treatment for Patients With Type 2
Diabetes
Diabetes Care 2009 32:1577-1582

5/24/10
30
DIGAMI2 (European Heart J. Prepublication Feb 2005)
Group 1 – IV insulin then long term SQ insulin Group 2 – IV insulin then standard treatment Group 3 – Standard treatment
Mortality
Effect of different updated glucose lowering treatments on mortality and morbidity
Mellbin, L. G. et al. Eur Heart J 2008 29:166-176
Insulin Treatment and Risk of Cancer 1. Hemkens LG, Grouven U, Bender R et al. Risk of malignancies in patients with diabetes treated with human insulin or insulin analogues: a cohort study. Diabetologia 2009;52:1732-44. 2. Jonasson JM, Ljung R, Talbäck M, Haglund B, Gudbjörnsdòttir S, Steineck G. Insulin glargine use and short-term incidence of alignancies—a population based follow-up study in Sweden. Diabetologia 2009;52:1745- 4. 3. Currie CJ, Poole CD, Gale EAM. The influence of glucose lowering therapies on cancer risk in type 2 diabetes. Diabetologia 2009;52:1766–77. 4. Colhoun HM, SDRN Epidemiology Group. Use of insulin glargine and cancer incidence in Scotland: a study from the Scottish Diabetes Research Network Epidemiology Group. Diabetologia 2009;52:1755-65.

5/24/10
31
Insulin Treatment and Risk of Cancer
Four studies Studies involve convoluted statistical
manipulation of epidemiologic data There are fundamental internal
disagreements and multiple inconsistencies.
Does Diabetes Therapy Influence the Risk of Cancer?
● German study1: N=127,031 – Glargine vs human insulin - a decrease in all cancers with
Glargine
– After adjusting for dose, a dose-dependent increase in cancer risk was found for treatment with glargine compared with human insulin (P<.0001): the adjusted HR was 1.09 for a daily dose of 10 IU, 1.19 for 30 IU, and 1.31 for 50 IU
– No increased risk was found for aspart or lispro compared with human insulin
– did not take into account body mass index and the duration of time that the patients were on insulin.
– time on insulin was very short, only about 1.6 years, 1. Hemkens LG, et al. Diabetologia. 2009. doi:10.1007/s00125-009-1418-4.
Does Diabetes Therapy Influence the Risk of Cancer?
● Swedish study1: N=114,841
– No statistically significant difference in cancer incidence between patients on insulins other than glargine, and those on glargine plus other insulins
– Women on glargine alone, however, had a higher risk of breast cancer than those on insulins other than glargine, with an RR of 1.99
4 Large Observational Studies
1. Jonasson JM, et al. Diabetologia. 2009. doi:10.1007/s00125-009-1444-2.

5/24/10
32
Does Diabetes Therapy Influence the Risk of Cancer?
● Swedish study1: N=114,841
• In Sweden, an increased risk of breast cancer was reported only in women who used glargine insulin alone, but not in those women who used glargine insulin plus other types of insulin
4 Large Observational Studies
1. Jonasson JM, et al. Diabetologia. 2009. doi:10.1007/s00125-009-1444-2.
Does Diabetes Therapy Influence the Risk of Cancer? (cont)
● Scottish study1: N=49,197
– Glargine with rapid-acting insulin had a slightly lower rate of cancer progression than did human insulin (HR 0.8, P<.26), but glargine alone had a higher overall rate (HR 1.55, P=.045)
– The number of site-specific cancers was small, but more cases of breast cancer were noted with glargine alone, compared with nonglargine insulins (HR 3.39, P=.004)
4 Large Observational Studies
1. Colhoun HM; for the SDRN Epidemiology Group. Diabetologia. 2009. doi:10.1007/s00125-009-1453-1.
Does Diabetes Therapy Influence the Risk of Cancer? (cont)
● Scottish study1: N=49,197
– Glargine – overall, no increase in cancer
– Breast Cancer – no increase for all glargine users
– Breast Cancer - Increase for glargine only - only 6 cases
4 Large Observational Studies
1. Colhoun HM; for the SDRN Epidemiology Group. Diabetologia. 2009. doi:10.1007/s00125-009-1453-1.

5/24/10
33
Does Diabetes Therapy Influence the Risk of Cancer? (cont)
● UK study1: N=62,809
– Metformin monotherapy carried the lowest risk of cancer; adjusted HR was 1.08 for metformin + sulfonylurea, 1.36 for sulfonylurea monotherapy, and 1.42 for insulin-based regimens; adding metformin to insulin reduced progression to cancer (HR 0.54); risk for patients on basal human insulin alone vs glargine was 1.24
– Compared with metformin, insulin therapy increased the risk of colorectal (HR 1.69) or pancreatic cancer (HR 4.63) but did not influence the risk of breast or prostate cancer; sulfonylureas were associated with a similar pattern of risk as insulin
4 Large Observational Studies
1. Currie CJ, et al. Diabetologia. 2009. doi:10.1007/s00125-009-1440-6.
Insulin Treatment and Risk of Cancer
Many types of cancer are increased in diabetic patients
Recent retrospective observational studies suggest that long-acting insulin analog glargine may increase and that biguanide metformin may decrease cancer risk
The evidence provided by these studies is weak and disputable because of many experiment and analysis limitations. Therefore it is possible neither to confirm nor to exclude the effect of these drugs on cancer in diabetic patients.
While waiting for more careful studies we have no evidence-based rationale for changing treatment approach to diabetic patients
Drug Cost Comparison Drug and Dose Cost/month
Glucose Strips (2 per day) $66
Sulfonylurea Generic $4-14 Brand $50
Rapaglinide 2 mg tid/nateglinide 120 tid $193/164 Acarbose 100 mg tid $88 Metformin 1000 bid Generic $ 4-32
Brand $161 Rosiglitazone 8 mg qd $266 Pioglitazone 45 mg/d $245 Sitagliptin/Saxagliptin $207/190 Exenatide 10mcg /Liraglutide 1.2mg $271/280 Colesevelam 3750 mg/d $224 Bromocriptine 2.5-5mg $62-130 Glargine, 45 U/d /(pen) $150/182 Salsalate 4g/d $50
24 hour fitness center $35 YMCA $65

5/24/10
34
Drug Cost Comparison Drug and Dose Cost/month
Glucose Strips (2 per day) $66
Sulfonylurea Generic $4-14 Brand $50
Rapaglinide 2 mg tid/nateglinide 120 tid $193/164 Acarbose 100 mg tid $88 Metformin 1000 bid Generic $ 4-32
Brand $161 Rosiglitazone 8 mg qd $266 Pioglitazone 45 mg/d $245 Sitagliptin/Saxagliptin $207/190 Exenatide 10mcg /Liraglutide 1.2mg $271/280 Colesevelam 3750 mg/d $224 Bromocriptine 2.5-5mg $62-130 Glargine, 45 U/d /(pen) $150/182 Salsalate 4g/d $50
24 hour fitness center $35 YMCA $65
Glargine (45 units/d), metformin, glimepiride 1-2 checks per day $226
Glargine (45 units/d), metformin, glimepiride Exenatide (10 bid) 1-2 checks per day $497
Glargine (45 units/d), metformin, glimepiride symlin 1-2 checks per day $537
Novolog 70/30 (80 Units/d), metformin 2 checks per day $423
Glargine (45 units/d), Lispro 50 units/d, Metformin 4 checks per day $507
Metformin, glimepiride, pioglitazone Sitagliptin 1-2 checks per day $526





























