Embed Size (px)
Citation preview
9. Cardiovascular Disease and RiskManagement: Standards ofMedical Care in Diabetesd2018Diabetes Care 2018;41(Suppl. 1):S86–S104 | https://doi.org/10.2337/dc18-S009
The American Diabetes Association (ADA) “Standards of Medical Care in Diabetes”includes ADA’s current clinical practice recommendations and is intended to providethe components of diabetes care, general treatment goals and guidelines, and toolsto evaluate quality of care. Members of the ADA Professional Practice Committee, amultidisciplinary expert committee, are responsible for updating the Standards ofCare annually, or more frequently as warranted. For a detailed description ofADA standards, statements, and reports, as well as the evidence-grading systemfor ADA’s clinical practice recommendations, please refer to the Standards of CareIntroduction. Readers who wish to comment on the Standards of Care are invited todo so at professional.diabetes.org/SOC.
For prevention and management of diabetes complications in children andadolescents, please refer to Section 12 “Children and Adolescents.”Atherosclerotic cardiovascular disease (ASCVD)ddefined as coronary heart
disease, cerebrovascular disease, or peripheral arterial disease presumed to be ofatherosclerotic origindis the leading cause ofmorbidity andmortality for individualswith diabetes and is the largest contributor to the direct and indirect costs ofdiabetes. Common conditions coexisting with type 2 diabetes (e.g., hypertensionand dyslipidemia) are clear risk factors for ASCVD, and diabetes itself confers in-dependent risk. Numerous studies have shown the efficacy of controlling individualcardiovascular risk factors in preventing or slowing ASCVD in people with diabetes.Furthermore, large benefits are seen when multiple cardiovascular risk factors areaddressed simultaneously. Under the current paradigm of aggressive risk factormodification in patients with diabetes, there is evidence that measures of 10-yearcoronary heart disease (CHD) risk among U.S. adults with diabetes have improvedsignificantly over the past decade (1) and that ASCVD morbidity and mortality havedecreased (2–4).Therefore, cardiovascular risk factors should be systematically assessed at least
annually in all patients with diabetes. These risk factors include hypertension, dyslipi-demia, smoking, a family history of premature coronary disease, chronic kidney dis-ease, and the presence of albuminuria. Modifiable abnormal risk factors should betreated as described in these guidelines.
HYPERTENSION/BLOOD PRESSURE CONTROL
Hypertension, defined as a sustained blood pressure $140/90 mmHg, is commonamong patients with either type 1 or type 2 diabetes. Hypertension is a major riskfactor for both ASCVD and microvascular complications. Moreover, numerous studieshave shown that antihypertensive therapy reduces ASCVD events, heart failure, andmicrovascular complications. Please refer to the American Diabetes Association (ADA)
Suggested citation: American Diabetes Association.9. Cardiovascular disease and risk management:Standards of Medical Care in Diabetesd2018.Diabetes Care 2018;41(Suppl. 1):S86–S104
© 2017 by the American Diabetes Association.Readers may use this article as long as the workis properly cited, the use is educational and notfor profit, and the work is not altered. More infor-mation is available at http://www.diabetesjournals.org/content/license.
American Diabetes Association
S86 Diabetes Care Volume 41, Supplement 1, January 2018
9.CARDIOVASCULA
RDISEA
SEANDRISKMANAGEM
ENT

position statement “Diabetes and Hyper-tension” for a detailed review of the epi-demiology, diagnosis, and treatment ofhypertension (5).
Screening and Diagnosis
Recommendations
c Blood pressure should bemeasuredat every routine clinical visit. Pa-tients found to have elevated bloodpressure ($140/90) should haveblood pressure confirmed usingmultiple readings, including meas-urments on a separate day, to diag-nose hypertension. B
c All hypertensive patients with dia-betes should monitor their bloodpressure at home. B
Blood pressure should be measured by atrained individual and should follow theguidelines established for the generalpopulation: measurement in the seatedposition, with feet on the floor and armsupported at heart level, after 5 min ofrest. Cuff size should be appropriate forthe upper-arm circumference. Elevatedvalues should be confirmed on a separateday. Postural changes in blood pressureand pulse may be evidence of autonomicneuropathy and therefore require adjust-mentof bloodpressure targets.Orthostaticblood pressure measurements should bechecked on initial visit and as indicated.Home blood pressure self-monitoring
and 24-h ambulatory blood pressuremonitoring may provide evidence ofwhite coat hypertension, masked hyper-tension, or other discrepancies betweenoffice and “true” blood pressure (5). Inaddition to confirming or refuting a diag-nosis of hypertension, home blood pres-sure assessment may be useful to monitorantihypertensive treatment. Studies of indi-viduals without diabetes found that homemeasurements may better correlate withASCVD risk than office measurements(6,7). Moreover, home blood pressuresmay improve patientmedication adherenceand thus help reduce cardiovascular risk (8).
Treatment Goals
Recommendations
c Most patients with diabetes andhypertension should be treatedto a systolic blood pressure goal of,140 mmHg and a diastolic bloodpressure goal of,90 mmHg. A
c Lower systolic and diastolic bloodpressure targets, such as 130/80mmHg, may be appropriate forindividuals at high risk of cardio-vascular disease, if they can beachieved without undue treat-ment burden. C
c In pregnant patients with diabetesand preexisting hypertension whoare treated with antihypertensivetherapy, blood pressure targets of120–160/80–105 mmHg are sug-gested in the interest of optimiz-ing long-term maternal healthand minimizing impaired fetalgrowth. E
Randomized clinical trials have demon-strated unequivocally that treatment ofhypertension to blood pressure ,140/90mmHg reduces cardiovascular eventsas well as microvascular complications(9–15). Therefore, patients with type 1or type2 diabeteswhohavehypertensionshould, at a minimum, be treated to bloodpressure targets of ,140/90 mmHg. In-tensification of antihypertensive ther-apy to target blood pressures lowerthan ,140/90 mmHg (e.g., ,130/80 or,120/80 mmHg) may be beneficial forselected patients with diabetes such asthose with a high risk of cardiovasculardisease. Such intensive blood pressurecontrol has been evaluated in large ran-domized clinical trials and meta-analysesof clinical trials.
Randomized Controlled Trials of Intensive
Versus Standard Blood Pressure Control
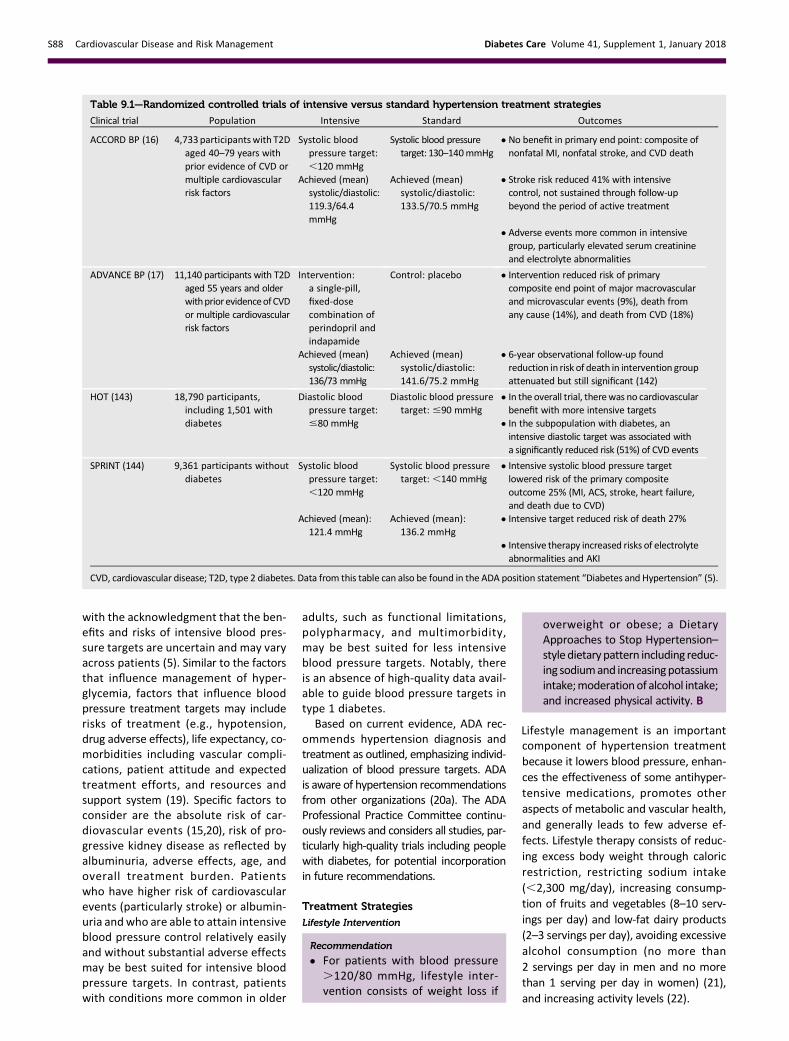
The Action to Control Cardiovascular Riskin Diabetes blood pressure (ACCORD BP)trial provides the strongest direct assess-ment of the benefits and risks of intensiveblood pressure control among peoplewith type 2 diabetes (16). In ACCORD BP,compared with standard blood pres-sure control (target systolic blood pres-sure ,140 mmHg), intensive bloodpressure control (target systolic bloodpressure,120 mmHg) did not reduce to-tal major atherosclerotic cardiovascularevents but did reduce the risk of stroke,at the expense of increased adverseevents (Table 9.1). The ACCORD BP re-sults suggest that blood pressure targetsmore intensive than,140/90 mmHg arenot likely to improve cardiovascular out-comes among most people with type 2 di-abetes but may be reasonable in selected
patients who have been educated aboutadded treatment burden, side effects, andcosts, as discussed below.
Additional studies, such as the SystolicBlood Pressure Intervention Trial (SPRINT)and the Hypertension Optimal Treatment(HOT) trial, also examined effects of inten-sive versus standard control (Table 9.1),though the relevance of their results topeople with diabetes is less clear. TheAction in Diabetes and Vascular Disease:Preterax and Diamicron MR ControlledEvaluation–Blood Pressure (ADVANCEBP) trial did not explicitly test blood pres-sure targets (17); the achieved bloodpressure in the intervention group washigher than that achieved in the ACCORDBP intensive arm andwould be consistentwith a target blood pressure of,140/90mmHg. Notably, ACCORD BP and SPRINTmeasured blood pressure using auto-mated office blood pressure measure-ments, which yields values that aregenerally lower than typical office bloodpressure readings by approximately5–10 mmHg (18), suggesting that imple-menting the ACCORD BP or SPRINT pro-tocols in an outpatient clinic might requirea systolic blood pressure target higherthan,120 mmHg.
Meta-analyses of Trials
To clarify optimal blood pressure targetsin patients with diabetes, meta-analyseshave stratified clinical trials by meanbaseline blood pressure or mean bloodpressure attained in the intervention (orintensive treatment) arm. Based on theseanalyses, antihypertensive treatment ap-pears to be beneficial when mean base-line blood pressure is$140/90 mmHg ormean attained intensive blood pressureis $130/80 mmHg (5,9,12–14). Amongtrials with lower baseline or attainedblood pressure, antihypertensive treat-ment reduced the risk of stroke, reti-nopathy, and albuminuria, but effectson other ASCVD outcomes and heartfailure were not evident. Taken to-gether, these meta-analyses consis-tently show that treating patients withbaseline blood pressure$140 mmHg totargets ,140 mmHg is beneficial, whilemore intensive targets may offer addi-tional, though probably less robust, ben-efits.
Individualization of Treatment Targets
Patients and clinicians should engage in ashared decision-making process to deter-mine individual blood pressure targets,
care.diabetesjournals.org Cardiovascular Disease and Risk Management S87
with the acknowledgment that the ben-efits and risks of intensive blood pres-sure targets are uncertain and may varyacross patients (5). Similar to the factorsthat influence management of hyper-glycemia, factors that influence bloodpressure treatment targets may includerisks of treatment (e.g., hypotension,drug adverse effects), life expectancy, co-morbidities including vascular compli-cations, patient attitude and expectedtreatment efforts, and resources andsupport system (19). Specific factors toconsider are the absolute risk of car-diovascular events (15,20), risk of pro-gressive kidney disease as reflected byalbuminuria, adverse effects, age, andoverall treatment burden. Patientswho have higher risk of cardiovascularevents (particularly stroke) or albumin-uria andwho are able to attain intensiveblood pressure control relatively easilyand without substantial adverse effectsmay be best suited for intensive bloodpressure targets. In contrast, patientswith conditions more common in older
adults, such as functional limitations,polypharmacy, and multimorbidity,may be best suited for less intensiveblood pressure targets. Notably, thereis an absence of high-quality data avail-able to guide blood pressure targets intype 1 diabetes.
Based on current evidence, ADA rec-ommends hypertension diagnosis andtreatment as outlined, emphasizing individ-ualization of blood pressure targets. ADAis aware of hypertension recommendationsfrom other organizations (20a). The ADAProfessional Practice Committee continu-ously reviews and considers all studies, par-ticularly high-quality trials including peoplewith diabetes, for potential incorporationin future recommendations.
Treatment Strategies
Lifestyle Intervention
Recommendation
c For patients with blood pressure.120/80 mmHg, lifestyle inter-vention consists of weight loss if
overweight or obese; a DietaryApproaches to Stop Hypertension–style dietarypattern including reduc-ing sodiumand increasingpotassiumintake;moderationof alcohol intake;and increased physical activity. B
Lifestyle management is an importantcomponent of hypertension treatmentbecause it lowers blood pressure, enhan-ces the effectiveness of some antihyper-tensive medications, promotes otheraspects of metabolic and vascular health,and generally leads to few adverse ef-fects. Lifestyle therapy consists of reduc-ing excess body weight through caloricrestriction, restricting sodium intake(,2,300 mg/day), increasing consump-tion of fruits and vegetables (8–10 serv-ings per day) and low-fat dairy products(2–3 servings per day), avoiding excessivealcohol consumption (no more than2 servings per day in men and no morethan 1 serving per day in women) (21),and increasing activity levels (22).
Table 9.1—Randomized controlled trials of intensive versus standard hypertension treatment strategies
Clinical trial Population Intensive Standard Outcomes
ACCORD BP (16) 4,733participantswith T2Daged 40–79 years withprior evidence of CVD ormultiple cardiovascularrisk factors
Systolic bloodpressure target:,120 mmHg
Systolic blood pressuretarget: 130–140mmHg
c No benefit in primary end point: composite ofnonfatal MI, nonfatal stroke, and CVD death
Achieved (mean)systolic/diastolic:119.3/64.4mmHg
Achieved (mean)systolic/diastolic:133.5/70.5 mmHg
c Stroke risk reduced 41% with intensivecontrol, not sustained through follow-upbeyond the period of active treatment
c Adverse events more common in intensivegroup, particularly elevated serum creatinineand electrolyte abnormalities
ADVANCE BP (17) 11,140 participants with T2Daged 55 years and olderwithpriorevidenceofCVDor multiple cardiovascularrisk factors
Intervention:a single-pill,fixed-dosecombination ofperindopril andindapamide
Control: placebo c Intervention reduced risk of primarycomposite end point of major macrovascularand microvascular events (9%), death fromany cause (14%), and death from CVD (18%)
Achieved (mean)systolic/diastolic:136/73 mmHg
Achieved (mean)systolic/diastolic:141.6/75.2 mmHg
c 6-year observational follow-up foundreduction in risk of death in intervention groupattenuated but still significant (142)
HOT (143) 18,790 participants,including 1,501 withdiabetes
Diastolic bloodpressure target:#80 mmHg
Diastolic blood pressuretarget: #90 mmHg
c In the overall trial, therewas no cardiovascularbenefit with more intensive targets
c In the subpopulation with diabetes, anintensive diastolic target was associated witha significantly reduced risk (51%) of CVD events
SPRINT (144) 9,361 participants withoutdiabetes
Systolic bloodpressure target:,120 mmHg
Systolic blood pressuretarget: ,140 mmHg
c Intensive systolic blood pressure targetlowered risk of the primary compositeoutcome 25% (MI, ACS, stroke, heart failure,and death due to CVD)
Achieved (mean):121.4 mmHg
Achieved (mean):136.2 mmHg
c Intensive target reduced risk of death 27%
c Intensive therapy increased risks of electrolyteabnormalities and AKI
CVD, cardiovascular disease; T2D, type 2 diabetes. Data from this table can also be found in the ADA position statement “Diabetes and Hypertension” (5).
S88 Cardiovascular Disease and Risk Management Diabetes Care Volume 41, Supplement 1, January 2018

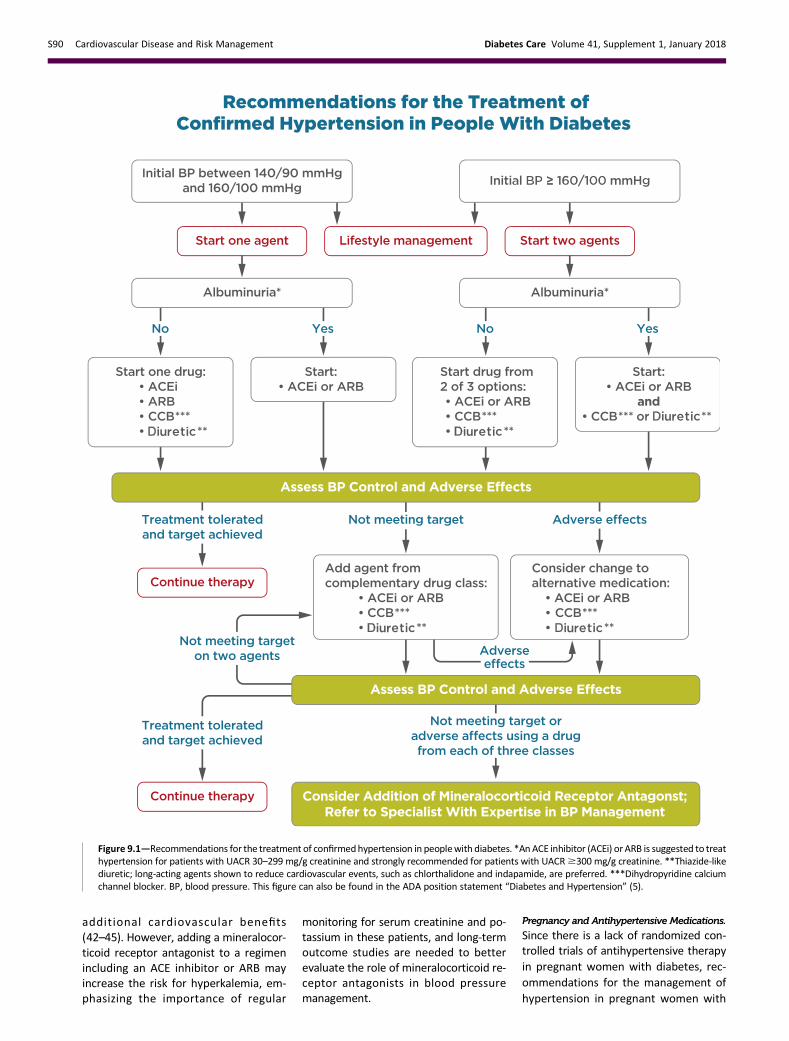
These lifestyle interventions are rea-sonable for individuals with diabetesand mildly elevated blood pressure(systolic .120 mmHg or diastolic .80mmHg) and should be initiated along withpharmacologic therapy when hypertensionis diagnosed (Fig. 9.1) (22). A lifestyle ther-apy plan should be developed in collabo-ration with the patient and discussed aspart of diabetes management.
Pharmacologic Interventions
Recommendations
c Patients with confirmed office-basedblood pressure $140/90 mmHgshould, in addition to lifestyle ther-apy,haveprompt initiationand timelytitration of pharmacologic therapy toachieve blood pressure goals. A
c Patients with confirmed office-basedblood pressure $160/100 mmHgshould, in addition to lifestyle ther-apy, have prompt initiation andtimely titration of two drugs or a sin-gle-pill combination of drugs dem-onstrated to reduce cardiovascularevents in patients with diabetes. A
c Treatment for hypertension shouldinclude drug classes demonstratedto reduce cardiovascular events inpa-tients with diabetes (ACE inhibitors,angiotensin receptor blockers, thiazide-likediuretics, or dihydropyridine calciumchannel blockers). A
c Multiple-drug therapy is generallyrequired to achieve blood pressuretargets. However, combinations ofACE inhibitors and angiotensin re-ceptor blockers and combinationsof ACE inhibitors or angiotensin re-ceptor blockers with direct renin in-hibitors should not be used. A
c An ACE inhibitor or angiotensin re-ceptor blocker, at the maximumlytolerated dose indicated for bloodpressure treatment, is the recom-mended first-line treatment for hy-pertension in patients with diabetesand urinary albumin-to-creatinineratio $300 mg/g creatinine A or30–299 mg/g creatinine B. If oneclass is not tolerated, the othershould be substituted B.
c For patients treated with an ACE in-hibitor, angiotensin receptor blocker,or diuretic, serumcreatinine/estimatedglomerular filtration rate and serumpotassium levels should be monitoredat least annually. B
Initial Number of AntihypertensiveMedications.
Initial treatment for people with diabetesdepends on the severity of hypertension(Fig. 9.1). Those with blood pressure be-tween 140/90 mmHg and 159/99 mmHgmay begin with a single drug. For patientswith blood pressure $160/100 mmHg,initial pharmacologic treatment withtwo antihypertensive medications is rec-ommended in order to more effectivelyachieve adequate blood pressure control(23,24). Single-pill antihypertensive com-binations may improve medication ad-herence in some patients (25).Classes of AntihypertensiveMedications. Ini-tial treatment for hypertension shouldinclude any of the drug classes demon-strated to reduce cardiovascular eventsin patients with diabetes: ACE inhibitors(26,27), angiotensin receptor blockers(ARBs) (26,27), thiazide-like diuretics(28), or dihydropyridine calcium channelblockers (29). For patients with albumin-uria (urine albumin-to-creatinine ratio[UACR] $30 mg/g), initial treatmentshould include an ACE inhibitor or ARBin order to reduce the risk of progressivekidney disease (5) (Fig. 9.1). In the ab-sence of albuminuria, risk of progressivekidney disease is low, and ACE inhibitorsand ARBs have not been found to affordsuperior cardioprotection when comparedwith thiazide-like diuretics or dihydro-pyridine calcium channel blockers(30).b-Blockersmay beused for the treatmentof prior myocardial infarction (MI), ac-tive angina, or heart failure but have notbeen shown to reduce mortality as bloodpressure-lowering agents in the absenceof these conditions (11,31).Multiple-DrugTherapy.Multiple-drug ther-apy is often required to achieve bloodpressure targets (Fig. 9.1), particularly inthe setting of diabetic kidney disease.However, the use of both ACE inhibitorsand ARBs in combination, or the combina-tion of an ACE inhibitor or ARB and a directrenin inhibitor, is not recommended giventhe lack of added ASCVD benefit and in-creased rate of adverse eventsdnamely,hyperkalemia, syncope, and acute kidneyinjury (AKI) (32–34). Titration of and/oraddition of further blood pressure medi-cations should be made in a timely fash-ion to overcome clinical inertia inachieving blood pressure targets.BedtimeDosing.Growingevidence suggeststhat there is an association between theabsence of nocturnal blood pressure dip-ping and the incidence of ASCVD. A meta-
analysis of randomized clinical trials found asmall benefit of evening versus morningdosing of antihypertensive medicationswith regard to blood pressure control buthad no data on clinical effects (35). In twosubgroup analyses of a single subsequentrandomized controlled trial, moving atleast one antihypertensive medicationto bedtime significantly reduced cardio-vascular events, but results were basedon a small number of events (36).
Hyperkalemia and AKI. TreatmentwithACEinhibitors or ARBs can cause AKI and hyper-kalemia, while diuretics can cause AKI andeither hypokalemia or hyperkalemia (de-pending on mechanism of action) (37,38).Detection and management of these ab-normalities is important because AKI andhyperkalemia each increase the risks ofcardiovascular events and death (39).Therefore, serum creatinine and potassiumshouldbemonitoredduring treatmentwithan ACE inhibitor, ARB, or diuretic, particu-larly among patients with reduced glomer-ular filtration who are at increased risk ofhyperkalemia and AKI (37,38,40).
Resistant Hypertension
Recommendation
c Patients with hypertension who arenot meeting blood pressure targetson three classes of antihypertensivemedications (including a diuretic)shouldbeconsideredformineralocor-ticoid receptor antagonist therapy. B
Resistant hypertension is defined asblood pressure $140/90 mmHg despitea therapeutic strategy that includes ap-propriate lifestyle management plus a di-uretic and two other antihypertensivedrugs belonging to different classes atadequate doses. Prior to diagnosing resis-tant hypertension, a number of otherconditions should be excluded, includingmedication nonadherence, white coathypertension, and secondary hyperten-sion. In general, barriers to medicationadherence (such as cost and side effects)should be identified and addressed(Fig. 9.1). Mineralocorticoid receptor an-tagonists are effective formanagement ofresistant hypertension in patients withtype 2 diabetes when added to existingtreatment with a ACE inhibitor or ARB,thiazide-like diuretic, and dihydropyridinecalcium channel blocker (41). Miner-alocorticoid receptor antagonistsalso reduce albuminuria and have
care.diabetesjournals.org Cardiovascular Disease and Risk Management S89
additional cardiovascular benefits(42–45). However, adding a mineralocor-ticoid receptor antagonist to a regimenincluding an ACE inhibitor or ARB mayincrease the risk for hyperkalemia, em-phasizing the importance of regular
monitoring for serum creatinine and po-tassium in these patients, and long-termoutcome studies are needed to betterevaluate the role of mineralocorticoid re-ceptor antagonists in blood pressuremanagement.
Pregnancy and Antihypertensive Medications.
Since there is a lack of randomized con-trolled trials of antihypertensive therapyin pregnant women with diabetes, rec-ommendations for the management ofhypertension in pregnant women with
Figure 9.1—Recommendations for the treatment of confirmedhypertension in peoplewith diabetes. *An ACE inhibitor (ACEi) or ARB is suggested to treathypertension for patients with UACR 30–299 mg/g creatinine and strongly recommended for patients with UACR$300 mg/g creatinine. **Thiazide-likediuretic; long-acting agents shown to reduce cardiovascular events, such as chlorthalidone and indapamide, are preferred. ***Dihydropyridine calciumchannel blocker. BP, blood pressure. This figure can also be found in the ADA position statement “Diabetes and Hypertension” (5).
S90 Cardiovascular Disease and Risk Management Diabetes Care Volume 41, Supplement 1, January 2018

diabetes should be similar to those for allpregnant women. The American Collegeof Obstetricians and Gynecologists (ACOG)has recommendedthatwomenwithmild tomoderate gestational hypertension (systolicblood pressure ,160 mmHg or diastolicblood pressure,110mmHg) donot needto be treated with antihypertensive med-ications as there is no benefit identifiedthat clearly outweighs potential risks oftherapy (46). A 2014 Cochrane systematicreview of antihypertensive therapy formild to moderate chronic hypertensionthat included 49 trials and over 4,700women did not find any conclusive evi-dence for or against blood pressure treat-ment to reduce the risk of preeclampsiafor the mother or effects on perinataloutcomes such as preterm birth, small-for-gestational-age infants, or fetal death(47). For pregnant women who requireantihypertensive therapy, systolic bloodpressure levels of 120–160 mmHg and di-astolic blood pressure levels of 80–105mmHg are suggested to optimize mater-nal health without risking fetal harm.Lower targets (systolic blood pressure110–119 mmHg and diastolic blood pres-sure 65–79mmHg) may contribute to im-proved long-termmaternal health; however,they may be associated with impaired fetalgrowth. Pregnantwomenwithhypertensionand evidence of end-organ damage fromcardiovascular and/or renal disease maybe considered for lower blood pressuretargets to avoid progression of these con-ditions during pregnancy.During pregnancy, treatment with ACE
inhibitors, ARBs, and spironolactone arecontraindicated as they may cause fetaldamage. Antihypertensive drugs known tobe effective and safe in pregnancy includemethyldopa, labetalol, and long-actingnifedipine, while hydralzine may be consid-ered in the acutemanagement of hyperten-sion in pregnancy or severe preeclampsia(46). Diuretics are not recommended forblood pressure control in pregnancy butmay be used during late-stage pregnancyif needed for volume control (46,48).ACOG also recommends that postpartumpatients with gestational hypertension, pre-eclampsia, and superimposed preeclampsiahave their bloodpressures observed for 72hin the hospital and for 7–10 days postpar-tum. Long-term follow-up is recommendedfor thesewomen as they have increased life-time cardiovascular risk (49). See Section 13“Management of Diabetes in Pregnancy”for additional information.
LIPID MANAGEMENT
Lifestyle Intervention
Recommendations
c Lifestyle modification focusing onweight loss (if indicated); the reduc-tion of saturated fat, trans fat, andcholesterol intake; increase of die-tary n-3 fatty acids, viscous fiber,and plant stanols/sterols intake;and increased physical activityshould be recommended to im-prove the lipid profile in patientswith diabetes. A
c Intensify lifestyle therapy and opti-mize glycemic control for patientswith elevated triglyceride levels($150 mg/dL [1.7 mmol/L]) and/or low HDL cholesterol (,40 mg/dL[1.0 mmol/L] for men, ,50 mg/dL[1.3 mmol/L] for women). C
Lifestyle intervention, including weightloss, increased physical activity, andmed-ical nutrition therapy, allows some pa-tients to reduce ASCVD risk factors.Nutrition intervention should be tailoredaccording to each patient’s age, diabetestype, pharmacologic treatment, lipid lev-els, and medical conditions.
Recommendations should focus on re-ducing saturated fat, cholesterol, and transfat intake and increasing plant stanols/sterols, n-3 fatty acids, and viscous fiber(such as in oats, legumes, and citrus) in-take. Glycemic controlmay also beneficiallymodify plasma lipid levels, particularly inpatients with very high triglycerides andpoor glycemic control. See Section 4“Lifestyle Management” for additionalnutrition information.
Ongoing Therapy andMonitoringWithLipid Panel
Recommendations
c In adults not taking statins or otherlipid-lowering therapy, it is reasonableto obtain a lipid profile at the time ofdiabetes diagnosis, at an initial medi-cal evaluation, and every 5 yearsthereafter ifunder theageof40years,or more frequently if indicated. E
c Obtain a lipid profile at initiation ofstatins or other lipid-lowering ther-apy, 4–12weeks after initiation or achange indose,andannually thereafteras itmay help tomonitor the responseto therapy and inform adherence. E
In adults with diabetes, it is reasonable toobtain a lipid profile (total cholesterol,LDL cholesterol, HDL cholesterol, and tri-glycerides) at the time of diagnosis, at theinitial medical evaluation, and at least ev-ery 5 years thereafter in patients underthe age of 40 years. In younger patientswith longer duration of disease (such asthose with youth-onset type 1 diabetes),more frequent lipid profiles may be rea-sonable. A lipid panel should also be ob-tained immediately before initiatingstatin therapy. Once a patient is taking astatin, LDL cholesterol levels should beassessed 4–12 weeks after initiation ofstatin therapy, after any change in dose,and on an individual basis (e.g., to moni-tor for medication adherence and effi-cacy). In cases where patients areadherent but the LDL cholesterol level isnot responding, clinical judgment is rec-ommended to determine the need forand timing of lipid panels. In individualpatients, the highly variable LDL choles-terol–lowering response seenwith statinsis poorly understood (50). Cliniciansshould attempt to find a dose or alterna-tive statin that is tolerable, if side effectsoccur. There is evidence for benefit fromeven extremely low, less than daily statindoses (51).
Statin Treatment
Recommendations
c For patients of all ages with diabe-tes and atherosclerotic cardiovas-cular disease, high-intensity statintherapy should be added to lifestyletherapy. A
c For patients with diabetes aged,40 years with additional athero-sclerotic cardiovascular diseaserisk factors, the patient and providershould consider using moderate-intensity statin in addition to lifestyletherapy. C
c For patients with diabetes aged 40–75 yearsA and.75 years Bwithoutatherosclerotic cardiovascular dis-ease, use moderate-intensity statinin addition to lifestyle therapy.
c In clinical practice, providers mayneed to adjust the intensity of statintherapy based on individual patientresponse to medication (e.g., sideeffects, tolerability, LDL cholesterollevels, or percent LDL reduction onstatin therapy). For patientswho donot tolerate the intended intensity
care.diabetesjournals.org Cardiovascular Disease and Risk Management S91
of statin, the maximally toleratedstatin dose should be used. E
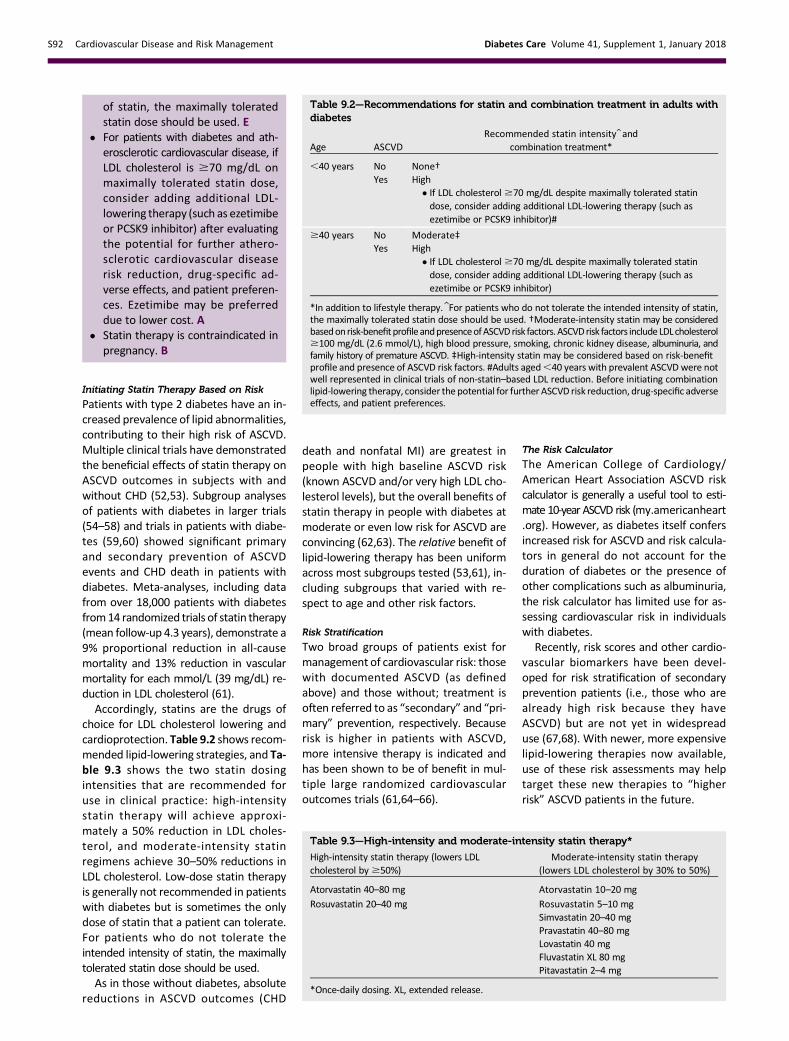
c For patients with diabetes and ath-erosclerotic cardiovascular disease, ifLDL cholesterol is $70 mg/dL onmaximally tolerated statin dose,consider adding additional LDL-lowering therapy (such as ezetimibeor PCSK9 inhibitor) after evaluatingthe potential for further athero-sclerotic cardiovascular diseaserisk reduction, drug-specific ad-verse effects, and patient preferen-ces. Ezetimibe may be preferreddue to lower cost. A
c Statin therapy is contraindicated inpregnancy. B
Initiating Statin Therapy Based on Risk
Patients with type 2 diabetes have an in-creased prevalence of lipid abnormalities,contributing to their high risk of ASCVD.Multiple clinical trials have demonstratedthe beneficial effects of statin therapy onASCVD outcomes in subjects with andwithout CHD (52,53). Subgroup analysesof patients with diabetes in larger trials(54–58) and trials in patients with diabe-tes (59,60) showed significant primaryand secondary prevention of ASCVDevents and CHD death in patients withdiabetes. Meta-analyses, including datafrom over 18,000 patients with diabetesfrom14 randomized trials of statin therapy(mean follow-up 4.3 years), demonstrate a9% proportional reduction in all-causemortality and 13% reduction in vascularmortality for each mmol/L (39 mg/dL) re-duction in LDL cholesterol (61).Accordingly, statins are the drugs of
choice for LDL cholesterol lowering andcardioprotection. Table 9.2 shows recom-mended lipid-lowering strategies, and Ta-ble 9.3 shows the two statin dosingintensities that are recommended foruse in clinical practice: high-intensitystatin therapy will achieve approxi-mately a 50% reduction in LDL choles-terol, and moderate-intensity statinregimens achieve 30–50% reductions inLDL cholesterol. Low-dose statin therapyis generally not recommended in patientswith diabetes but is sometimes the onlydose of statin that a patient can tolerate.For patients who do not tolerate theintended intensity of statin, the maximallytolerated statin dose should be used.As in those without diabetes, absolute
reductions in ASCVD outcomes (CHD
death and nonfatal MI) are greatest inpeople with high baseline ASCVD risk(known ASCVD and/or very high LDL cho-lesterol levels), but the overall benefits ofstatin therapy in people with diabetes atmoderate or even low risk for ASCVD areconvincing (62,63). The relative benefit oflipid-lowering therapy has been uniformacross most subgroups tested (53,61), in-cluding subgroups that varied with re-spect to age and other risk factors.
Risk Stratification
Two broad groups of patients exist formanagement of cardiovascular risk: thosewith documented ASCVD (as definedabove) and those without; treatment isoften referred to as “secondary” and “pri-mary” prevention, respectively. Becauserisk is higher in patients with ASCVD,more intensive therapy is indicated andhas been shown to be of benefit in mul-tiple large randomized cardiovascularoutcomes trials (61,64–66).
The Risk Calculator
The American College of Cardiology/American Heart Association ASCVD riskcalculator is generally a useful tool to esti-mate 10-year ASCVD risk (my.americanheart.org). However, as diabetes itself confersincreased risk for ASCVD and risk calcula-tors in general do not account for theduration of diabetes or the presence ofother complications such as albuminuria,the risk calculator has limited use for as-sessing cardiovascular risk in individualswith diabetes.
Recently, risk scores and other cardio-vascular biomarkers have been devel-oped for risk stratification of secondaryprevention patients (i.e., those who arealready high risk because they haveASCVD) but are not yet in widespreaduse (67,68). With newer, more expensivelipid-lowering therapies now available,use of these risk assessments may helptarget these new therapies to “higherrisk” ASCVD patients in the future.
Table 9.2—Recommendations for statin and combination treatment in adults withdiabetes
Age ASCVDRecommended statin intensity and
combination treatment*
,40 years No None†Yes High
c If LDL cholesterol$70 mg/dL despite maximally tolerated statindose, consider adding additional LDL-lowering therapy (such asezetimibe or PCSK9 inhibitor)#
$40 years No Moderate‡Yes High
c If LDL cholesterol$70 mg/dL despite maximally tolerated statindose, consider adding additional LDL-lowering therapy (such asezetimibe or PCSK9 inhibitor)
*In addition to lifestyle therapy. For patients who do not tolerate the intended intensity of statin,the maximally tolerated statin dose should be used. †Moderate-intensity statin may be consideredbasedonrisk-benefitprofileandpresenceofASCVDrisk factors.ASCVDrisk factors includeLDLcholesterol$100 mg/dL (2.6 mmol/L), high blood pressure, smoking, chronic kidney disease, albuminuria, andfamily history of premature ASCVD. ‡High-intensity statin may be considered based on risk-benefitprofile and presence of ASCVD risk factors. #Adults aged,40 years with prevalent ASCVDwere notwell represented in clinical trials of non-statin–based LDL reduction. Before initiating combinationlipid-lowering therapy, consider the potential for further ASCVD risk reduction, drug-specific adverseeffects, and patient preferences.
Table 9.3—High-intensity and moderate-intensity statin therapy*
High-intensity statin therapy (lowers LDLcholesterol by $50%)
Moderate-intensity statin therapy(lowers LDL cholesterol by 30% to 50%)
Atorvastatin 40–80 mg Atorvastatin 10–20 mg
Rosuvastatin 20–40 mg Rosuvastatin 5–10 mgSimvastatin 20–40 mgPravastatin 40–80 mgLovastatin 40 mgFluvastatin XL 80 mgPitavastatin 2–4 mg
*Once-daily dosing. XL, extended release.
S92 Cardiovascular Disease and Risk Management Diabetes Care Volume 41, Supplement 1, January 2018

Primary Prevention (Patients Without ASCVD)
For primary prevention, moderate-dosestatin therapy is recommended for those40 years and older (55,62,63), thoughhigh-intensity therapy may be consideredon an individual basis in the context of ad-ditional ASCVD risk factors. The evidence isstrong for patients with diabetes aged 40–75 years, an age-group well representedin statin trials showing benefit.The evidence is lower for patients
aged .75 years; relatively few older pa-tientswith diabetes havebeen enrolled inprimary prevention trials. However, het-erogeneity by age has not been seen inthe relative benefit of lipid-lowering ther-apy in trials that included older partici-pants (53,60,61), and because older ageconfers higher risk, the absolute benefitsare actually greater (53,65). Moderate-intensity statin therapy is recommendedin patients with diabetes that are 75 yearsor older. However, the risk-benefit profileshould be routinely evaluated in this pop-ulation, with downward titration of doseperformed as needed. See Section 11“Older Adults” for more details on clinicalconsiderations for this population.
Age <40 Years and/or Type 1 Diabetes. Verylittle clinical trial evidence exists for pa-tients with type 2 diabetes under the ageof 40 years or for patients with type 1 di-abetes of any age. In the Heart ProtectionStudy (lower age limit 40 years), the sub-group of ;600 patients with type 1 dia-betes had a proportionately similar,although not statistically significant, re-duction in risk as patients with type 2 di-abetes (55). Even though the data are notdefinitive, similar statin treatment ap-proaches should be considered for pa-tients with type 1 or type 2 diabetes,particularly in the presence of other car-diovascular risk factors. Patients belowthe age of 40 have lower risk of devel-oping a cardiovascular event over a10-year horizon; however, their lifetimerisk of developing cardiovascular diseaseand suffering an MI, stroke, or cardiovas-cular death is high. For patients under theage of 40 years and/or who have type 1diabetes with other ASCVD risk factors,we recommend that the patient andhealth care provider discuss the relativebenefits and risks and consider the useof moderate-intensity statin therapy.Please refer to “Type 1 Diabetes Mellitusand Cardiovascular Disease: A ScientificStatement From the American Heart
Association and American Diabetes Asso-ciation” (69) for additional discussion.
Secondary Preventions (Patients With
ASCVD)
High-intensity statin therapy is recommen-ded for all patients with diabetes andASCVD. This recommendation is based onthe Cholesterol Treatment Trialists’ Collab-oration involving 26 statin trials, of which5 compared high-intensity versus moderate-intensity statins. Together, they found re-ductions in nonfatal cardiovascular eventswith more intensive therapy, in patientswith and without diabetes (53,57,64).
Over the past few years, there havebeen multiple large randomized trials in-vestigating the benefits of adding nonsta-tin agents to statin therapy, includingthree that evaluated further lowering ofLDL cholesterol with ezetimibe (65),PCSK9 inhibitors (66), and, cholesteryl es-ter transfer protein [CETP] inhibitors, aninvestigational class of drugs with somerecent supportive data (70). Each trialfound a significant benefit in the reduc-tion of ASCVD events that was directlyrelated to the degree of further LDL cho-lesterol lowering. These three large trialscomprised over 75,000 patients and250,000 patient-years of follow-up, andapproximately one-third of participantshad diabetes. For patients with ASCVDwho are on high-intensity (and maximallytolerated) statin therapy and have an LDLcholesterol $70 mg/dL, the addition ofnonstatin LDL-lowering therapy is recom-mended after considering the potential forfurther ASCVD risk reduction, drug-specificadverse effects, and patient preferences.
Combination Therapy for LDLCholesterol Lowering
Statins and Ezetimibe
The IMProved Reduction of Outcomes:Vytorin Efficacy International Trial(IMPROVE-IT) was a randomized con-trolled trial in 18,144 patients comparingthe addition of ezetimibe to simvastatintherapy versus simvastatin alone. Individualswere$50 years of age, had experienced arecent acute coronary syndrome (ACS),and were treated for an average of6 years. Overall, the addition of ezetimibeled to a 6.4% relative benefit and a 2% ab-solute reduction inmajor adversecardiovas-cular events, with the degree of benefitbeing directly proportional to the changein LDL cholesterol, which was 70 mg/dL inthe statin grouponaverageand54mg/dL inthe combination group (65). In those with
diabetes (27% of participants), the com-bination of moderate-intensity simvasta-tin (40 mg) and ezetimibe (10 mg)showed a significant reduction of majoradverse cardiovascular eventswith an ab-solute risk reduction of 5% (40% vs. 45%)and relative risk reduction of 14% (RR0.86 [95% CI 0.78–0.94]) over moderate-intensity simvastatin (40 mg) alone (65).
Statins and PCSK9 Inhibitors
Placebo-controlled trials evaluating theaddition of the PCSK9 inhibitors evolo-cumab and alirocumab to maximallytolerated doses of statin therapy in par-ticipants who were at high risk for ASCVDdemonstrated an average reduction inLDL cholesterol ranging from 36 to 59%.These agents have been approved as ad-junctive therapy for patients with ASCVDor familial hypercholesterolemia who arereceiving maximally tolerated statin ther-apy but require additional lowering of LDLcholesterol (71,72).
The effects of PCSK9 inhibition onASCVD outcomes was investigated inthe Further Cardiovascular Outcomes Re-search With PCSK9 Inhibition in SubjectsWith Elevated Risk (FOURIER) trial, whichenrolled 27,564 patients with priorASCVD and an additional high-risk featurewhowere receiving their maximally toler-ated statin therapy (two-thirds were onhigh-intensity statin) but who still had anLDL cholesterol$70 mg/dL or a non-HDLcholesterol $100 mg/dL (66). Patientswere randomized to receive subcutane-ous injections of evolocumab (either140 mg every 2 weeks or 420 mg everymonth based on patient preference) ver-sus placebo. Evolocumab reduced LDLcholesterol by 59% from a median of92 to 30 mg/dL in the treatment arm.
During the median follow-up of 2.2years, the composite outcome of cardio-vascular death,MI, stroke, hospitalizationfor angina, or revascularization occurredin 11.3% vs. 9.8% of the placebo and evo-locumab groups, respectively, represent-ing a 15% relative risk reduction (P ,0.001). The combined end point of cardio-vascular death,MI, or stroke was reducedby 20%, from 7.4 to 5.9% (P , 0.001).Importantly, similar benefits were seenin prespecified subgroup of patientswith diabetes, comprising 11,031 patients(40% of the trial) (73).
Statins and CETP Inhibitors
Inhibition of CETP increases HDL choles-terol and further reduces LDL cholesterol.
care.diabetesjournals.org Cardiovascular Disease and Risk Management S93

This class of drugs is not likely to be avail-able for clinical use, but studies pro-vide further insight into the effects ofLDL cholesterol lowering on cardiovascularevents.A total of four trials have been con-
ducted, three of which failed to showbenefit (74–76). Of these, one showedharmand twowere stopped after approx-imately 2 years and thus did not havesufficient time or power to identify thebenefit. The final study, the RandomizedEvaluation of the Effects of AnacetrapibThrough Lipid-modification (REVEAL) trialenrolled 30,449 patientswithASCVD (70).All patients received intensive atorvasta-tin therapy and were randomized to ana-cetrapib or placebo.During the median follow-up of 4.1
years, the primary outcome (coronarydeath, MI, or coronary revascularization)was significantly reduced with the addi-tion of anacetrapib from 11.8 to 10.8%,with a hazard ratio (HR) of 0.91 (P 50.004). The relative difference in riskwas similar across multiple prespecifiedsubgroups, including among 11,320 pa-tients with diabetes (37% of the trial).The benefit appeared to be related tothe reduction in LDL (and more broadlynon-HDL) as opposed to the raising ofHDL. The mean achieved LDL cholesterolwas 63 mg/dL vs. 53 mg/dL at the trialmidpoint in the placebo and anacetrapibgroups, respectively. This study reaffirmsthe benefit of further lowering of LDLcholesterol on reducing cardiovascularevents.
Treatment of Other LipoproteinFractions or Targets
Recommendation
c For patientswith fasting triglyceridelevels $500 mg/dL (5.7 mmol/L),evaluate for secondary causes ofhypertriglyceridemia and considermedical therapy to reduce the riskof pancreatitis. C
Hypertriglyceridemia should be ad-dressedwith dietary and lifestyle changesincluding abstinence from alcohol (77).Severe hypertriglyceridemia (.1,000mg/dL) may warrant pharmacologic ther-apy (fibric acid derivatives and/or fish oil)to reduce the risk of acute pancreatitis.Low levels of HDL cholesterol, often
associated with elevated triglyceridelevels, are the most prevalent pattern of
dyslipidemia in individuals with type 2 di-abetes. However, the evidence for theuse of drugs that target these lipid frac-tions is substantially less robust than thatfor statin therapy (78). In a large trial inpatients with diabetes, fenofibrate failedto reduce overall cardiovascular out-comes (79).
Other Combination Therapy
Recommendations
c Combination therapy (statin/fibrate)has not been shown to improve ath-erosclerotic cardiovascular diseaseoutcomes and is generally not rec-ommended. A
c Combination therapy (statin/niacin)has not been shown to provide addi-tional cardiovascular benefit abovestatin therapy alone, may increasethe risk of stroke with additionalside effects, and is generally notrecommended. A
Statin and Fibrate
Combination therapy (statin and fibrate)is associated with an increased risk forabnormal transaminase levels, myositis,and rhabdomyolysis. The risk of rhabdo-myolysis is more common with higherdoses of statins and renal insufficiencyand appears to be higher when statinsare combined with gemfibrozil (com-pared with fenofibrate) (80).
In the ACCORD study, in patients withtype 2 diabetes who were at high risk forASCVD, the combination of fenofibrateand simvastatin did not reduce the rateof fatal cardiovascular events, nonfatalMI, or nonfatal stroke as compared withsimvastatin alone. Prespecified subgroupanalyses suggested heterogeneity intreatment effects with possible benefitfor men with both a triglyceride level$204 mg/dL (2.3 mmol/L) and an HDLcholesterol level#34 mg/dL (0.9 mmol/L)(81).
Statin and Niacin
The Atherothrombosis Intervention inMetabolic Syndrome With Low HDL/HighTriglycerides: Impact on Global HealthOutcomes (AIM-HIGH) trial randomizedover 3,000 patients (about one-thirdwith diabetes) with established ASCVD,low LDL cholesterol levels (,180 mg/dL[4.7 mmol/L]), low HDL cholesterol levels(men ,40 mg/dL [1.0 mmol/L] andwomen ,50 mg/dL [1.3 mmol/L]), andtriglyceride levels of 150–400 mg/dL
(1.7–4.5 mmol/L) to statin therapy plusextended-release niacin or placebo. Thetrial was halted early due to lack of effi-cacy on the primary ASCVDoutcome (firstevent of the composite of death fromCHD, nonfatal MI, ischemic stroke, hospi-talization for an ACS, or symptom-drivencoronary or cerebral revascularization)and a possible increase in ischemic strokein those on combination therapy (82).
The much larger Heart ProtectionStudy 2–Treatment of HDL to Reducethe Incidence of Vascular Events (HPS2-THRIVE) trial also failed to show a benefitof adding niacin to background statintherapy (83). A total of 25,673 patientswith prior vascular disease were random-ized to receive 2 g of extended-releaseniacin and 40mgof laropiprant (an antag-onist of the prostaglandin D2 receptorDP1 that has been shown to improve ad-herence to niacin therapy) versus amatching placebo daily and followedfor a median follow-up period of 3.9years. There was no significant differencein the rate of coronary death, MI, stroke,or coronary revascularizationwith the ad-dition of niacin–laropiprant versus pla-cebo (13.2% vs. 13.7%; rate ratio, 0.96;P5 0.29). Niacin–laropiprant was associ-ated with an increased incidence of new-onset diabetes (absolute excess, 1.3percentage points; P, 0.001) and distur-bances in diabetes control among thosewith diabetes. In addition, there was anincrease in serious adverse events associ-ated with the gastrointestinal system,musculoskeletal system, skin, and, unex-pectedly, infection and bleeding.
Therefore, combination therapy with astatin and niacin is not recommendedgiven the lack of efficacy on major ASCVDoutcomes and side effects.
Diabetes With Statin UseSeveral studies have reported a modestlyincreased risk of incident diabetes withstatin use (84,85), which may be limitedto those with diabetes risk factors. Ananalysis of one of the initial studiessuggested that although statin use wasassociated with diabetes risk, the cardio-vascular event rate reduction with statinsfar outweighed the risk of incident diabe-tes even for patients at highest risk fordiabetes (86). The absolute risk increasewas small (over 5 years of follow-up,1.2% of participants on placebo devel-oped diabetes and 1.5% on rosuvastatindeveloped diabetes) (86). A meta-analysis
S94 Cardiovascular Disease and Risk Management Diabetes Care Volume 41, Supplement 1, January 2018

of 13 randomized statin trials with 91,140participants showed an odds ratio of 1.09for a new diagnosis of diabetes, so that(on average) treatment of 255 patientswith statins for 4 years resulted in oneadditional case of diabetes while simulta-neously preventing 5.4 vascular eventsamong those 255 patients (85).
Statins and Cognitive FunctionA recent systematic review of the U.S.Food and Drug Administration’s (FDA’s)postmarketing surveillance databases,randomized controlled trials, and cohort,case-control, and cross-sectional studiesevaluating cognition in patients receivingstatins found that published data do not re-veal anadverse effect of statins on cognition(87). In addition, no change in cognitivefunction has been reported in studies withthe addition of ezetimibe (65) or PCSK9inhibitors (66,88) to statin therapy, includ-ing among patients treated to very low LDLcholesterol levels. Therefore, a concern thatstatins or other lipid-lowering agents mightcause cognitive dysfunction or dementia isnot currently supported by evidence andshould not deter their use in individualswith diabetes at high risk for ASCVD (87).
ANTIPLATELET AGENTS
Recommendations
c Useaspirin therapy (75–162mg/day)as a secondary prevention strategyin those with diabetes and a historyof atherosclerotic cardiovasculardisease. A
c For patients with atheroscleroticcardiovascular disease and docu-mented aspirin allergy, clopidogrel(75 mg/day) should be used. B
c Dual antiplatelet therapy (with low-dose aspirin and a P2Y12 inhibitor)is reasonable for a year after anacutecoronary syndrome A and may havebenefits beyond this period. B
c Aspirin therapy (75–162 mg/day)may be considered as a primary pre-vention strategy in those with type 1or type 2 diabetes who are at in-creased cardiovascular risk. Thisincludes most men and women withdiabetes aged$50 years who haveat least one additional major riskfactor (family history of prematureatherosclerotic cardiovascular dis-ease, hypertension, dyslipidemia,smoking, or albuminuria) and arenot at increased risk of bleeding. C
Risk ReductionAspirin has been shown to be effective inreducing cardiovascular morbidity andmortality in high-risk patients with previ-ous MI or stroke (secondary prevention).Its net benefit in primary preventionamong patients with no previous cardio-vascular events is more controversialboth for patients with diabetes and forpatients without diabetes (89,90). Previ-ous randomized controlled trials of aspi-rin specifically in patients with diabetesfailed to consistently show a significantreduction in overall ASCVD end points,raising questions about the efficacy of as-pirin for primary prevention in peoplewith diabetes, although some sex differ-ences were suggested (91–93).
The Antithrombotic Trialists’ Collabora-tion published an individual patient–levelmeta-analysis (89) of the six large trials ofaspirin for primary prevention in the gen-eral population. These trials collectivelyenrolled over 95,000 participants, includ-ing almost 4,000 with diabetes. Overall,they found that aspirin reduced the riskof serious vascular events by 12% (RR0.88 [95% CI 0.82–0.94]). The largest re-duction was for nonfatal MI, with littleeffect on CHD death (RR 0.95 [95% CI0.78–1.15]) or total stroke. There wassome evidence of a difference in aspirineffect by sex: aspirin significantly reducedASCVD events in men but not in women.Conversely, aspirin had no effect onstroke in men but significantly reducedstroke in women. However, there wasno heterogeneity of effect by sex in therisk of serious vascular events (P 5 0.9).
Sex differences in the effects of aspirinhave not been observed in studies of sec-ondary prevention (89). In the six trialsexamined by the Antithrombotic Trialists’Collaboration, the effects of aspirin onmajor vascular events were similar for pa-tients with or without diabetes: RR 0.88(95% CI 0.67–1.15) and RR 0.87 (95% CI0.79–0.96), respectively. The CIwaswiderfor those with diabetes because ofsmaller numbers.
Aspirin appears to have a modest ef-fect on ischemic vascular events, with theabsolute decrease in events dependingon the underlying ASCVD risk. The mainadverse effect is an increased risk of gas-trointestinal bleeding. The excess risk maybe as high as 5 per 1,000 per year in real-world settings. In adults with ASCVDrisk.1% per year, the number of ASCVDevents prevented will be similar to or
greater than the number of episodes ofbleeding induced, although these compli-cations do not have equal effects on long-term health (94).
Treatment ConsiderationsIn 2010, a position statement of the ADA,the American Heart Association, and theAmerican College of Cardiology Foun-dation recommended that low-dose(75–162 mg/day) aspirin for primary pre-vention is reasonable for adults with di-abetes andnoprevious history of vasculardisease who are at increased ASCVD riskand who are not at increased risk forbleeding (95). This now out-of-date state-ment included sex-specific recommenda-tions for use of aspirin therapy as primaryprevention in persons with diabetes (95).However, since that time, multiple recentwell-conducted studies andmeta-analyseshave reported a risk of heart disease andstroke that is equivalent if not higher inwomen compared with men with diabe-tes, including among nonelderly adults.Thus, current recommendations for usingaspirin as primary prevention include bothmen and women aged $50 years withdiabetes and at least one additionalmajorrisk factor (family history of prematureASCVD, hypertension, dyslipidemia,smoking, or chronic kidney disease/albuminuria) who are not at increasedrisk of bleeding (e.g., older age, anemia,renal disease) (96–99). While risk calcu-lators such as those from the AmericanCollege of Cardiology/American Heart As-sociation (my.americanheart.org) maybe a useful tool to estimate 10-yearASCVD risk, diabetes itself confers in-creased risk for ASCVD. As a result, suchrisk calculators have limited utility in help-ing to assess the potential benefits of as-pirin therapy in individuals with diabetes.Noninvasive imaging techniques such ascoronary computed tomography angiog-raphy may potentially help further tai-lor aspirin therapy, particularly in thoseat low risk (100), but are not generallyrecommended. Sex differences in theantiplatelet effect of aspirin have been sug-gested in the general population (101);however, further studies are needed toinvestigate the presence of such differen-ces in individuals with diabetes.
Aspirin Use in People <50 Years of AgeAspirin is not recommended for those atlow risk of ASCVD (such asmenandwomenaged ,50 years with diabetes with no
care.diabetesjournals.org Cardiovascular Disease and Risk Management S95

othermajor ASCVD risk factors) as the lowbenefit is likely to be outweighed by therisks of bleeding. Clinical judgment shouldbe used for those at intermediate risk(younger patients with one or more riskfactors or older patients with no risk fac-tors) until further research is available.Patients’ willingness to undergo long-term aspirin therapy should also be con-sidered (102). Aspirin use in patientsaged ,21 years is generally contraindi-cated due to the associated risk of Reyesyndrome.
Aspirin DosingAverage daily dosages used in most clini-cal trials involving patients with diabetesranged from 50 mg to 650 mg but weremostly in the range of 100–325 mg/day.There is little evidence to support anyspecific dose, but using the lowest possi-ble dose may help to reduce side effects(103). In the U.S., the most common low-dose tablet is 81 mg. Although plateletsfrom patients with diabetes have alteredfunction, it is unclear what, if any, effectthat finding has on the required dose ofaspirin for cardioprotective effects in thepatient with diabetes. Many alternatepathways for platelet activation existthat are independent of thromboxaneA2 and thus not sensitive to the effectsof aspirin (104). “Aspirin resistance” hasbeen described in patients with diabeteswhen measured by a variety of ex vivoand in vitro methods (platelet aggregom-etry, measurement of thromboxane B2)(101), but other studies suggest no impair-ment in aspirin response among patientswith diabetes (105). A recent trial suggestedthatmore frequent dosing regimens of aspi-rin may reduce platelet reactivity in individ-uals with diabetes (106); however, theseobservations alone are insufficient to em-pirically recommend that higher doses ofaspirin be used in this group at this time.It appears that 75–162mg/day is optimal.
Indications for P2Y12 UseA P2Y12 receptor antagonist in combina-tion with aspirin should be used for atleast 1 year in patients following anACS and may have benefits beyond thisperiod. Evidence supports use of eitherticagrelor or clopidogrel if no percutane-ous coronary interventionwas performedand clopidogrel, ticagrelor, or prasugrelif a percutaneous coronary interventionwas performed (107). In patients with di-abetes and prior MI (1–3 years before),
adding ticagrelor to aspirin significantlyreduces the risk of recurrent ischemicevents including cardiovascular and coro-nary heart disease death (108). Morestudies are needed to investigate thelonger-term benefits of these therapiesafter ACS among patients with diabetes.
CORONARY HEART DISEASE
Recommendations
Screeningc In asymptomatic patients, routine
screening for coronary artery dis-ease is not recommended as itdoes not improve outcomes as longas atherosclerotic cardiovascular dis-ease risk factors are treated. A
c Consider investigations for coronaryartery disease in the presence of anyof the following: atypical cardiacsymptoms (e.g., unexplaineddyspnea,chest discomfort); signs or symptomsof associated vascular disease includ-ing carotid bruits, transient ischemicattack, stroke, claudication, or periph-eral arterial disease; or electrocardio-gram abnormalities (e.g., Q waves). E
Treatmentc In patients with known atheroscle-
rotic cardiovascular disease, con-sider ACE inhibitor or angiotensinreceptor blocker therapy to reducethe risk of cardiovascular events. B
c In patients with prior myocardial in-farction, b-blockers should be con-tinued for at least 2 years after theevent. B
c In patients with type 2 diabetes withstable congestive heart failure,metformin may be used if estimatedglomerular filtration rate remains.30mL/min but should be avoidedin unstable or hospitalized patientswith congestive heart failure. B
c In patients with type 2 diabetes andestablished atherosclerotic cardio-vascular disease, antihyperglycemictherapy should begin with lifestylemanagement and metformin andsubsequently incorporate an agentproven to reduce major adverse car-diovasculareventsandcardiovascularmortality (currently empagliflozinand liraglutide), after consideringdrug-specific and patient factors(see Table 8.1). A
c Inpatientswith type2diabetes andes-tablishedatheroscleroticcardiovascular
disease, after lifestyle managementandmetformin, the antihyperglyce-mic agent canagliflozin may be con-sidered to reduce major adversecardiovascular events, based ondrug-specific and patient factors(see Table 8.1). C
Cardiac TestingCandidates for advanced or invasive car-diac testing include those with 1) typicalor atypical cardiac symptoms and 2) an ab-normal resting electrocardiogram (ECG).Exercise ECG testingwithout orwith echo-cardiographymaybeused as the initial test.In adults with diabetes $40 years of age,measurement of coronary artery calciumis also reasonable for cardiovascular riskassessment. Pharmacologic stress echo-cardiography or nuclear imaging shouldbe considered in individuals with diabetesin whom resting ECG abnormalities pre-clude exercise stress testing (e.g., leftbundle branch block or ST-T abnormali-ties). In addition, individuals who requirestress testing and are unable to exerciseshould undergo pharmacologic stressechocardiography or nuclear imaging.
Screening Asymptomatic PatientsThe screening of asymptomatic patientswith high ASCVD risk is not recommended(109), in part because these high-risk pa-tients should already be receiving inten-sive medical therapydan approach thatprovides similar benefit as invasive revas-cularization (110,111). There is also someevidence that silent MI may reverse overtime, adding to the controversy concern-ing aggressive screening strategies (112).In prospective studies, coronary arterycalcium has been established as an in-dependentpredictorof futureASCVDeventsin patients with diabetes and is consistentlysuperior toboththeUKProspectiveDiabetesStudy (UKPDS) risk engine and the Framing-ham Risk Score in predicting risk in thispopulation (113–115). However, a random-ized observational trial demonstrated noclinical benefit to routine screening ofasymptomatic patients with type 2 dia-betes and normal ECGs (116). Despiteabnormal myocardial perfusion imagingin more than one in five patients, cardiacoutcomes were essentially equal (andvery low) in screened versus unscreenedpatients. Accordingly, indiscriminatescreening is not considered cost-effective.Studies have found that a risk factor–
S96 Cardiovascular Disease and Risk Management Diabetes Care Volume 41, Supplement 1, January 2018
Tab
le9.4—CVOTsco
mpletedafterissu
ance
oftheFD
A2008guidan
ce
DPP
-4inhibitors
GLP-1
receptoragonists
SGLT2inhibitors
SAVOR-TIM
I53
(129)
(n5
16,492)
EXAMINE
(145)
(n5
5,380)
TECOS
(132)
(n5
14,671)
ELIXA
(140)
(n5
6,068)
LEADER
(138)
(n5
9,340)
SUSTAIN-6
(139)*
(n5
3,297)
EXSC
EL(141)
(n5
14,752)
EMPA
-REG
OUTC
OME(133)
(n5
7,020)
CANVAS
(135)
(n5
4,330)
CANVAS-R
(135)
(n5
5,812)
Intervention
Saxagliptin/
placebo
Alogliptin/
placebo
Sitagliptin/
placebo
Lixisenatide/
placebo
Liraglutide/
placebo
Semaglutide/
placebo
Exen
atideQW/
placebo
Empaglifl
ozin/
placebo
Can
aglifl
ozin/placebo
Maininclusioncriteria
Type2diabetes
andhistory
of
ormultiple
risk
factorsfor
CVD
Type2diabetes
andACS
within
15–90
days
before
rand
omization
Type2
diabetes
and
preexisting
CVD
Type2
diabetes
and
history
ofACS
(,180days)
Type2
diabetes
and
preexisting
CVD,kidney
disease,o
rHF
at$50
yearsof
ageor
cardiovascular
risk
at$60
yearsof
age
Type2
diabetes
and
preexisting
CVD,HF,or
CKD
at$50
yearsof
ageor
cardiovascular
risk
at$60
yearsof
age
Type2diabetes
withorwithout
preexistingCVD
Type2diabetes
andpreexisting
CVDwithBMI
#45
kg/m
2and
eGFR
$30
mL/min/1.73m
2
Type2diabetes
andpreexisting
CVDat
$30
yearsof
ageor
$2
cardiovascular
risk
factorsat
$50
yearsof
age
A1C
inclusioncriteria(%)
$6.5
6.5–11.0
6.5–8.0
5.5–11.0
$7.0
$7.0
6.5–10.0
7.0–10.0
7.0–10.5
Age
(years)††
65.1
61.0
65.4
60.3
64.3
64.6
6263
.163
.3
Diabetesduration(years)††
10.3
7.1
11.6
9.3
12.8
13.9
1257
%.10
13.5
Medianfollow-up(years)
2.1
1.5
3.0
2.1
3.8
2.1
3.2
3.1
5.7
2.1
Statinuse(%)
7891
8093
7273
7477
75
Metform
inuse(%)
7066
8266
7673
7774
77
PriorCV
D/CHF(%)
78/13
100/28
74/18
100/22
81/18
60/24
73.1/16.2
99/10
65.6/14.4
MeanbaselineA1C
(%)
8.0
8.0
7.2
7.7
8.7
8.7
8.0
8.1
8.2
Meandifference
inA1C
betw
eengrou
psat
endof
treatm
ent(%)
20.3
20.3
20.3
20.3
20.4
20.7or
21.0†
20.53
20.3‡
20.58
Year
started/repo
rted
2010
/201
320
09/201
320
08/201
520
10/201
520
10/201
620
13/20
16
2010/20
17
2010/20
15
2009
/201
7
Primaryou
tcom
e§3-pointMACE
3-pointMACE
4-pointMACE
4-pointMACE
3-pointMACE
3-pointMACE
3-pointMACE
3-pointMACE
3-pointMACE
Progressionto
albuminuria**
1.00
(0.89–1.12)
0.96
(95%
UL#1.16)
0.98
(0.89–1.08)
1.02
(0.89–1.17)
0.87
(0.78–0.97)
0.74
(0.58–0.95)
0.91
(0.83–1.00)
0.86
(0.74–0.99)
0.86
(0.75–0.97)§
0.73
(0.47–0.77)
Keysecond
aryou
tcom
e§Expanded
MACE
4-pointMACE
3-pointMACE
Expanded
MACE
Expan
ded
MACE
Expanded
MACE
Individual
componen
tsofMACE(see
below)
4-pointMACE
All-cause
and
cardiovascular
mortality(see
below)
40%reductionin
compositeeG
FR,
renalreplacement,
renaldeath
0.60
(0.47–0.77)
1.02
(0.94–1.11)
0.95
(95%
UL#
1.14)
0.99
(0.89–1.10)
1.00
(0.90–1.11)
0.88
(0.81–0.96)
0.74
(0.62–0.89)
0.89
(0.78–1.01)
Continuedon
p.S98
care.diabetesjournals.org Cardiovascular Disease and Risk Management S97
Tab
le9.4—Continued
DPP
-4inhibitors
GLP-1
receptoragonists
SGLT2inhibitors
SAVOR-TIM
I53
(129)
(n5
16,492)
EXAMINE
(145)
(n5
5,380)
TECOS
(132)
(n5
14,671)
ELIXA
(140)
(n5
6,068)
LEADER
(138)
(n5
9,340)
SUSTAIN-6
(139)*
(n5
3,297)
EXSC
EL(141)
(n5
14,752)
EMPA
-REG
OUTC
OME(133)
(n5
7,020)
CANVAS
(135)
(n5
4,330)
CANVAS-R
(135)
(n5
5,812)
Cardiovasculardeath§
1.03
(0.87–1.22)
0.85
(0.66–1.10)
1.03
(0.89–1.19)
0.98
(0.78–1.22)
0.78
(0.66–0.93)
0.98
(0.65–1.48)
0.88
(0.76–1.02)
0.62
(0.49–0.77)
0.96(0.77–1.18)¶
0.87
(0.72–1.06)#
MI§
0.95
(0.80–1.12)
1.08
(0.88–1.33)
0.95
(0.81–1.11)
1.03
(0.87–1.22)
0.86
(0.73–1.00)
0.74
(0.51–1.08)
0.97
(0.85–1.10)
0.87
(0.70–1.09)
0.85
(0.65–1.11)
0.85
(0.61–1.19)
Stroke§
1.11
(0.88–1.39)
0.91
(0.55–1.50)
0.97
(0.79–1.19)
1.12
(0.79–1.58)
0.86
(0.71–1.06)
0.61
(0.38–0.99)
0.85
(0.70–1.03)
1.18
(0.89–1.56)
0.97
(0.70–1.35)
0.82
(0.57–1.18)
HFho
spitalization§
1.27
(1.07–1.51)
1.19
(0.90–1.58)
1.00
(0.83–1.20)
0.96
(0.75–1.23)
0.87
(0.73–1.05)
1.11
(0.77–1.61)
0.94
(0.78–1.13)
0.65
(0.50–0.85)
0.77
(0.55–1.08)
HR0.56
(0.38–0.83)
Unstableangina
hospitalization§
1.19
(0.89–1.60)
0.90
(0.60–1.37)
0.90
(0.70–1.16)
1.11
(0.47–2.62)
0.98
(0.76–1.26)
0.82
(0.47–1.44)
1.05
(0.94–1.18)
0.99
(0.74–1.34)
d
All-causemortality§
1.11
(0.96–1.27)
0.88
(0.71–1.09)
1.01
(0.90–1.14)
0.94
(0.78–1.13)
0.85
(0.74–0.97)
1.05
(0.74–1.50)
0.86
(0.77–0.97)
0.68
(0.57–0.82)
0.87(0.74–1.01)‡‡
0.90
(0.76–1.07)##
Worsening
neph
ropathy§|
1.08
(0.88–1.32)
dd
d0.78
(0.67–0.92)
0.64
(0.46–0.88)
d0.61
(0.53–0.70)
0.60(0.47–0.77)
d,notassessed/reported;CANVAS-R,CANVAS-Renal;CHF,congestive
heartfailure;CVD,cardiovasculard
isease;eGFR,estimated
glom
erularfiltration
rate;M
ACE,major
adversecardiacevent;UL,up
perlimit.D
atafrom
thistablewas
adaptedfrom
Cefaluet
al.(146)
intheJanu
ary2018
issueof
DiabetesCa
re.*Po
wered
toruleou
tan
HRof
1.8;superiorityhypo
thesisno
tprespecified.**O
nthebasisof
prespecified
outcom
es,the
renaloutcomes
areno
tview
edas
statistically
significant.††Age
was
repo
rted
asmeans
inalltrialsexcept
EXAMINE,which
repo
rted
medians;diabetesdu
ration
was
repo
rted
asmeans
inallbut
four
trials,withSAVOR-
TIMI58,EXAMINE,andEXSCEL
repo
rtingmedians
andEM
PA-REG
OUTCOMErepo
rtingas
percentage
ofpo
pulation
withdiabetes
duration
.10
years.†A1C
change
of0.66%with0.5mgand1.05%with1mgdo
seof
semaglutide.‡A1C
change
of0.30
inEM
PA-REG
OUTCOMEisbasedon
pooled
resultsforbo
thdo
ses(i.e.,0.24%
for10
mgand0.36%for25
mgof
empagliflozin).§O
utcomes
repo
rted
asHR(95%
CI).|Worsening
neph
ropathyisdefinedas
thenewon
setof
UACR
.300mg/gcreatinine
orado
ublingof
theserum
creatinine
leveland
anestimated
glom
erular
filtration
rate
of#45
mL/min/1.73m
2,the
need
forcontinuo
usrenal-replacementtherapy,ordeathfrom
renaldisease
inEM
PA-REG
OUTCOME,LEADER,and
SUSTAIN-6andasdoublingofcreatinine
level,initiation
ofdialysis,renaltransplantation,orcreatinine
.6.0mg/dL
(530
mmol/L)
inSAVOR-TIM
I53.Worsening
neph
ropathywas
aprespecified
exploratoryadjudicatedou
tcom
einSA
VOR-TIM
I53,LEADER,and
SUSTAIN-6
butno
tinEM
PA-REG
OUTCOME.¶Trun
cateddata
set(prespecified
intreatin
ghierarchyastheprincipaldatasetforanalysisforsuperiorityofall-cause
mortalityandcardiovasculardeathintheCA
NVASProgram).Significant
difference
inA1C
betw
eengrou
ps(P,
0.05).#N
ontrun
cateddata
set.‡‡Trun
catedintegrated
dataset(refersto
pooleddatafrom
CANVASafter20
November
2012
plusCANVAS-R;prespecified
intreatinghierarchyas
theprincipaldatasetforan
alysisforsuperiority
of
all-cause
mortalityan
dcardiovasculardeath
intheCANVASProgram
).##Non
trun
catedintegrated
data
(refersto
pooled
data
from
CANVAS,includ
ingbefore
20Novem
ber2012
plus
CANVAS-R).
S98 Cardiovascular Disease and Risk Management Diabetes Care Volume 41, Supplement 1, January 2018

based approach to the initial diagnosticevaluation and subsequent follow-up forcoronary artery disease fails to identifywhich patients with type 2 diabetes willhave silent ischemia on screening tests(117,118). Any benefit of newer nonin-vasive coronary artery disease screeningmethods, such as computed tomographyand computed tomography angiography,to identify patient subgroups for differenttreatment strategies remains unproven.Although asymptomatic patients with di-abetes with higher coronary disease bur-den have more future cardiac events(113,119,120), the role of these tests be-yond risk stratification is not clear. Their rou-tineuse leads to radiationexposureandmayresult in unnecessary invasive testing such ascoronary angiography and revascularizationprocedures. The ultimate balance of bene-fit, cost, and risks of such an approach inasymptomaticpatientsremainscontroversial,particularly in the modern setting of aggres-sive ASCVD risk factor control.
Lifestyle and PharmacologicInterventionsIntensive lifestyle intervention focusingon weight loss through decreased caloricintake and increased physical activity asperformed in the Action for Health in Di-abetes (Look AHEAD) trial may be con-sidered for improving glucose control,fitness, and some ASCVD risk factors(121). Patients at increased ASCVD riskshould receive aspirin and a statin andACE inhibitor orARB therapy if the patienthas hypertension, unless there are con-traindications to a particular drug class.While clear benefit exists for ACE inhibitoror ARB therapy in patients with diabetickidney disease or hypertension, the bene-fits in patients with ASCVD in the absenceof these conditions are less clear, espe-cially when LDL cholesterol is concomi-tantly controlled (122,123). In patientswith prior MI, active angina, or heart fail-ure, b-blockers should be used (124).
Diabetes and Heart FailureAs many as 50% of patients with type 2diabetes may develop heart failure (125).Data on the effects of glucose-loweringagents on heart failure outcomes havedemonstrated that thiazolidinedioneshave a strong and consistent relation-ship with increased risk of heart failure(126–128). Therefore, thiazolidinedioneuse should be avoided in patients withsymptomatic heart failure.
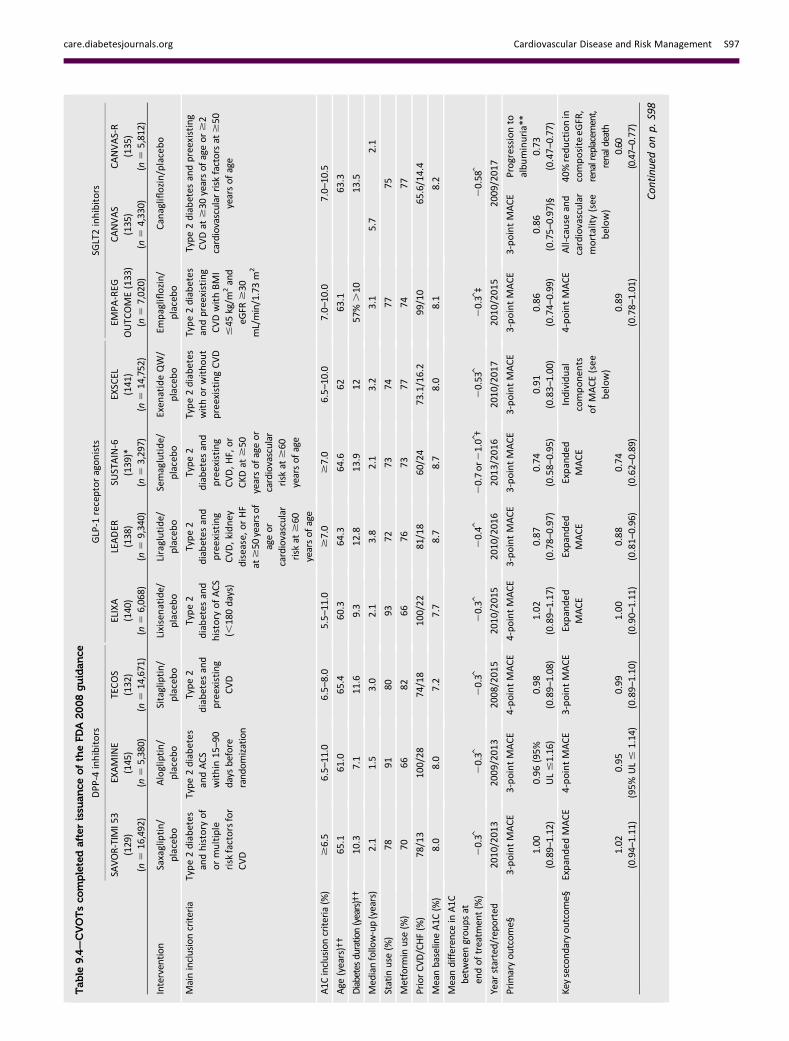
Recent studies have also examined therelationship between dipeptidyl pep-tidase 4 (DPP-4) inhibitors and heartfailure and have had mixed results.The Saxagliptin Assessment of VascularOutcomes Recorded in Patients with Di-abetes Mellitus–Thrombolysis in Myocar-dial Infarction 53 (SAVOR-TIMI 53) studyshowed that patients treated withsaxagliptin (a DPP-4 inhibitor) were morelikely to be hospitalized for heart failurethan were those given placebo (3.5% vs.2.8%, respectively) (129). Two other re-cent multicenter, randomized, double-blind, noninferiority trials, Examination ofCardiovascular Outcomes with Alogliptinversus Standard of Care (EXAMINE) andTrial Evaluating Cardiovascular Outcomeswith Sitagliptin (TECOS), did not show asso-ciations between DPP-4 inhibitor use andheart failure. The FDA reported that thehos-pital admission rate for heart failure inEXAMINEwas 3.9% for patients randomlyassigned to alogliptin compared with3.3% for those randomly assigned toplacebo (130). Alogliptin had no effecton the composite end point of cardiovas-cular death and hospital admission forheart failure in the post hoc analysis (HR1.00 [95% CI 0.82–1.21]) (131). TECOSshowed no difference in the rate of heartfailure hospitalization for the sitagliptingroup (3.1%; 1.07 per 100 person-years)compared with the placebo group (3.1%;1.09 per 100 person-years) (132).
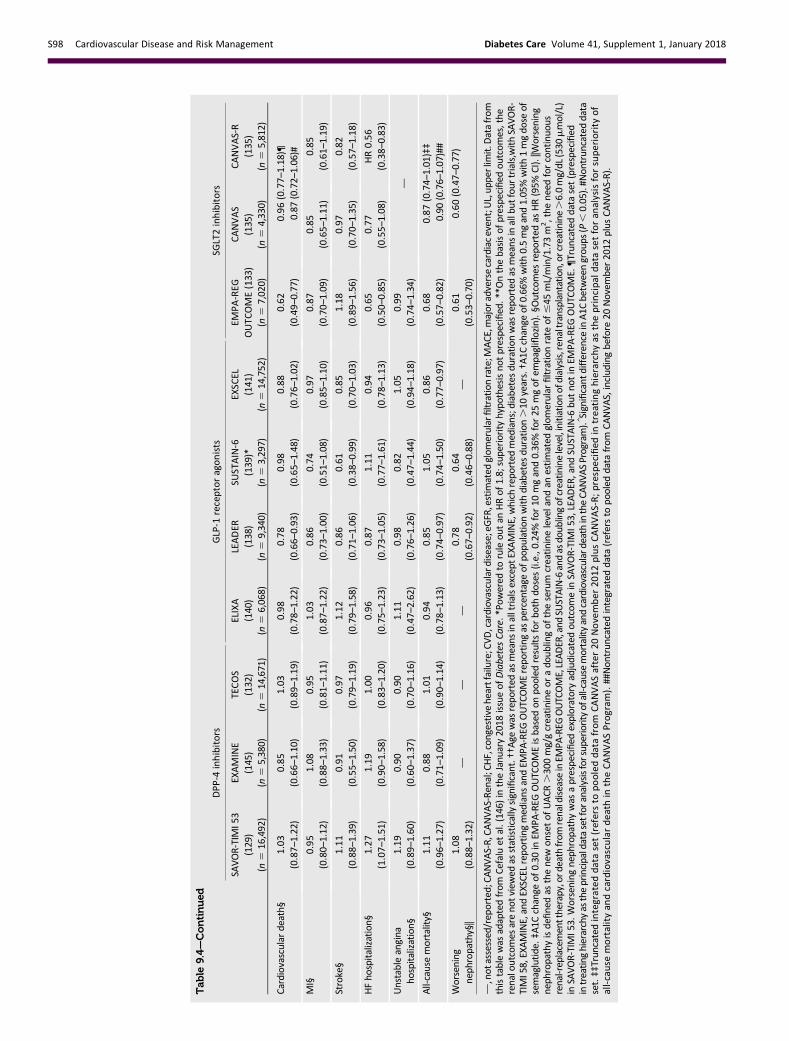
A benefit on the incidence of heart fail-ure has been observed with the use ofsome sodium–glucose cotransporter2 (SGLT2) inhibitors. In the BI 10773(Empagliflozin) Cardiovascular OutcomeEvent Trial in Type 2 Diabetes MellitusPatients (EMPA-REG OUTCOME), the ad-dition of empagliflozin to standard careled to a significant 35% reduction in thehospitalization for heart failure comparedwith placebo (133). Although themajorityof patients in the study did not have heartfailure at baseline, this benefit was con-sistent in patients with and without aprior history of heart failure (134). Simi-larly, in the Canagliflozin Cardiovascu-lar Assessment Study (CANVAS), therewas a 33% reduction in hospitalizationfor heart failure with canagliflozin versusplacebo (135). Although heart failure hos-pitalizations were prospectively adjudicatedin both trials, the type(s) of heart failureevents prevented were not characterized.These preliminary findings, which stronglysuggest heart failure–related benefits of
SGLT2 inhibitors (particularly the preven-tion of heart failure), are being followedup with new outcomes trials in patientswith established heart failure, both withand without diabetes, to determine theirefficacy in treatment of heart failure.
Antihyperglycemic Therapies andCardiovascular OutcomesIn 2008, the FDA issued a guidance forindustry to perform cardiovascular out-comes trials for all new medications forthe treatment for type 2 diabetes amidconcerns of increased cardiovascular risk(137). Previously approved diabetesmed-ications were not subject to the guidance.Recently published cardiovascular outcomestrials have provided additional data on car-diovascular outcomes in patients with type 2diabetes with cardiovascular disease or athigh risk forcardiovasculardisease (seeTable9.4). Cardiovascular outcomes trials ofDPP-4 inhibitors have all, so far, not showncardiovascular benefits relative to placebo.However, results from other new agentshave provided a mix of results.
EMPA-REG OUTCOME trial was a ran-domized, double-blind trial that assessedthe effect of empagliflozin, a SGLT2 inhib-itor, versus placebo on cardiovascularoutcomes in 7,020 patients with type 2diabetes and existing cardiovascular dis-ease. Study participants had a mean ageof 63 years, 57% had diabetes for morethan 10 years, and 99% had establishedcardiovasculardisease.EMPA-REGOUTCOMEshowed that over a median follow-up of3.1 years, treatment reduced the compos-ite outcome of MI, stroke, and cardiovas-cular death by 14% (absolute rate 10.5%vs. 12.1% in the placebo group, HR in theempagliflozin group 0.86; 95% CI 0.74–0.99; P = 0.04 for superiority) and cardio-vascular death by 38% (absolute rate3.7% vs. 5.9%, HR 0.62; 95% CI 0.49–0.77; P , 0.001) (133). The FDA recentlyadded a new indication for empagliflozin,to reduce the risk of major adverse car-diovascular death in adults with type 2diabetes and cardiovascular disease.
A second large cardiovascular out-comes trial program of an SGLT2 inhibi-tor, canagliflozin, has been reported(135). The CANVAS Program integrateddata from two trials, including the CANVAStrial that started in 2009 before the ap-proval of canagliflozin and the CANVAS-Rtrial that started in 2014 after the approvalof canagliflozin. Combiningboth these trials,10,142participantswith type2diabetesand
care.diabetesjournals.org Cardiovascular Disease and Risk Management S99

high cardiovascular riskwere randomized tocanagliflozin or placebo and were followedfor an average 3.6 years. The mean age ofpatientswas 63 years and 66%hada historyof cardiovascular disease. The combinedanalysis of the two trials found thatcanagliflozin significantly reduced the com-posite outcome of cardiovascular death,MI, or stroke versus placebo (occurring in26.9 vs. 31.5 participants per 1,000 patient-years; HR 0.86 [95% CI 0.75–0.97];P , 0.001 for noninferiority; P 5 0.02for superiority). The specific estimatesfor canagliflozin versus placebo on theprimary composite cardiovascular out-come were HR 0.88 (0.75–1.03) for theCANVAS trial, and 0.82 (0.66–1.01) forthe CANVAS-R, with no heterogeneityfound between trials. In the combinedanalysis, there was not a statistically sig-nificant difference in cardiovascular death(HR 0.87 [95% CI 0.72–1.06]). The initialCANVAS trial was partially unblinded priorto completion because of the need to fileinterim cardiovascular outcome data forregulatory approval of the drug (136). Ofnote, there was an increased risk of am-putationwith canaglifozin (6.3 vs. 3.4 par-ticipants per 1,000 patient-years; HR 1.97[95% CI 1.41–2.75]) (135).The Liraglutide Effect and Action in Di-
abetes: Evaluation of CardiovascularOutcome ResultsdA Long Term Evalua-tion (LEADER) trial was a randomized,double-blind trial that assessed the effectof liraglutide, a glucagon-like peptide1 (GLP-1) receptor agonist, versus placeboon cardiovascular outcomes in 9,340 pa-tients with type 2 diabetes at high risk forcardiovascular disease orwith cardiovascu-lar disease. Study participants with ameanage of 64 years and a mean duration ofdiabetes of nearly 13 years. Over 80% ofstudy participants had established cardio-vascular disease. After a median follow-upof 3.8 years, LEADER showed that the pri-mary composite outcome (MI, stroke, orcardiovascular death) occurred in fewerparticipants in the treatment group(13.0%) when compared with the placebogroup (14.9%) (HR 0.87; 95% CI 0.78–0.97;P, 0.001 for noninferiority; P = 0.01 forsuperiority). Deaths from cardiovascularcauses in the were significantly reducedin the liraglutide group (4.7%) comparedto the placebo group (6.0%) (HR 0.78;95% CI 0.66–0.93; P = 0.007) (138). TheFDA recently approved use of liraglutideto reduce the risk of major adverse car-diovascular events, includingheart attack,
stroke and cardiovascular death, in adultswith type 2 diabetes and established car-diovascular disease.
Results fromamoderate-sized trial of an-other GLP-1 receptor agonist, semaglutide,were consistent with the LEADER trial(139). Semaglutide, a once-weekly GLP-1receptor agonist, has not yet been ap-proved by the FDA for the treatment oftype 2 diabetes. The preapproval Trial toEvaluate Cardiovascular and Other Long-term Outcomes with Semaglutide in Sub-jects With Type 2 Diabetes (SUSTAIN-6)was the initial randomized trial poweredto test noninferiority of semaglutide forthe purpose of initial regulatory approval.In this study, 3,297 patients with type 2 di-abetes were randomized to receive once-weekly semaglutide (0.5 mg or 1.0 mg) orplacebo for 2 years. The primary outcome(the first occurrence of cardiovasculardeath, nonfatal MI, or nonfatal stroke)occurred in 108 patients (6.6%) in thesemaglutide group vs. 146 patients (8.9%)in the placebo group (HR 0.74 [95% CI0.58–0.95]; P, 0.001).More patients dis-continued treatment in the semaglutidegroup because of adverse events, mainlygastrointestinal.
The Evaluation of Lixisenatide in AcuteCoronary Syndrome (ELIXA) trial studiedthe once-daily GLP-1 receptor agonistlixisenatide on cardiovascular outcomesin patients with type 2 diabetes whohad had a recent acute coronary event(140). A total of 6,068 patients with type 2diabetes with a recent hospitalization forMI or unstable angina within the previ-ous 180 days were randomized to re-ceive lixisenatide or placebo in additionto standard care and were followed fora median of approximately 2.1 years.The primary outcome of cardiovasculardeath, MI, stroke, or hospitalization forunstable angina occurred in 406 patients(13.4%) in the lixisenatide group vs.399 (13.2%) in the placebo group (HR1.02 [95% CI 0.89–1.17]), which demon-strated the noninferiority of lixisenatideto placebo (P, 0.001) but did not showsuperiority (P5 0.81).
Most recently, the Exenatide Study ofCardiovascular Event Lowering (EXSCEL)trial also reported results with the once-weekly GLP-1 receptor agonist extended-release exenatide and found that majoradverse cardiovascular events were nu-merically lower with use of extended-release exenatide compared with placebo,although this differencewas not statistically
significant (141). A total of 14,752 pa-tients with type 2 diabetes (of whom10,782 [73.1%] had previous cardiovascu-lar disease) were randomized to receiveextended-release exenatide 2 mg or pla-cebo and followed for a median of 3.2years. The primary end point of cardio-vascular death, MI, or stroke occurredin 839 patients (11.4%; 3.7 events per100 person-years) in the exenatide groupand in 905 patients (12.2%; 4.0 events per100 person-years) in the placebo group(HR 0.91 [95% CI 0.83–1.00]; P , 0.001for noninferiority) butwas not superior toplacebo with respect to the primary endpoint (P5 0.06 for superiority). However,all-cause mortality was lower in the exe-natide group (HR 0.86 [95% CI 0.77–0.97].The incidence of acute pancreatitis, pan-creatic cancer, medullary thyroid carci-noma, and serious adverse events didnot differ significantly between the twogroups.
In summary, there are now largerandomized controlled trials reportingstatistically significant reductions in car-diovascular events for two of the FDA-approved SGLT2 inhibitors (empagliflozinand canagliflozin) and one of the FDA-approvedGLP-1receptoragonists (liraglutide)where the majority, if not all, patients inthe trial had ASCVD. The empagliflozinand liraglutide trials further demon-strated significant reductions in cardio-vascular death. Once-weekly exenatidedid not have statistically significant re-ductions in major adverse cardiovascu-lar events or cardiovascular mortalitybut did have a significant reduction inall-cause mortality. In contrast, otherGLP-1 receptor agonists have notshown similar reductions in cardiovas-cular events (Table 9.4). Whether thebenefits of GLP-1 receptor agonists are aclass effect remains to be definitivelyestablished. Additional large randomizedtrials of other agents in these classes areongoing.
Of note, these studies examined thedrugs in combinationwithmetformin (Ta-ble 9.4) in the great majority of patientsfor whom metformin was not contraindi-cated or was tolerated. For patients withtype 2 diabetes who have ASCVD, on life-style and metformin therapy, it is recom-mended to incorporate an agent withstrong evidence for cardiovascular riskreduction, especially those with provenbenefit on both major adverse cardiovas-cular events and cardiovascular death,
S100 Cardiovascular Disease and Risk Management Diabetes Care Volume 41, Supplement 1, January 2018

after consideration of drug-specific pa-tient factors (Table 8.1). See Fig. 8.1 foradditional recommendations on antihy-perglycemic treatment in adults withtype 2 diabetes.
References1. Ali MK, Bullard KM, Saaddine JB, Cowie CC,Imperatore G, Gregg EW. Achievement of goalsin U.S. diabetes care, 1999–2010. N Engl J Med2013;368:1613–16242. Rawshani A, Rawshani A, Franzen S, et al. Mor-tality and cardiovascular disease in type 1 and type2 diabetes. N Engl J Med 2017;376:1407–14183. Gregg EW, Li Y, Wang J, et al. Changes in di-abetes-related complications in theUnited States,1990–2010. N Engl J Med 2014;370:1514–15234. Ford ES, Ajani UA, Croft JB, et al. Explaining thedecrease in U.S. deaths from coronary disease,1980–2000. N Engl J Med 2007;356:2388–23985. de Boer IH, Bangalore S, Benetos A, et al. Di-abetes and hypertension: a position statement bythe American Diabetes Association. Diabetes Care2017;40:1273–12846. Bobrie G, Genes N, Vaur L, et al. Is “isolatedhome” hypertension as opposed to “isolated of-fice” hypertension a sign of greater cardiovascularrisk? Arch Intern Med 2001;161:2205–22117. Sega R, Facchetti R, Bombelli M, et al. Prognos-tic value of ambulatory and homeblood pressurescompared with office blood pressure in thegeneral population: follow-up results from thePressioni Arteriose Monitorate e Loro Associa-zioni (PAMELA) study. Circulation 2005;111:1777–17838. Omboni S, Gazzola T, Carabelli G, Parati G.Clinical usefulness and cost effectiveness ofhome blood pressure telemonitoring: meta-analysisof randomizedcontrolled studies. J Hypertens 2013;31:455–467; discussion 467–4689. Emdin CA, Rahimi K, Neal B, Callender T,Perkovic V, Patel A. Blood pressure lowering intype 2 diabetes: a systematic review and meta-analysis. JAMA 2015;313:603–61510. Arguedas JA, Leiva V, Wright JM. Blood pres-sure targets for hypertension in people with di-abetes mellitus. Cochrane Database Syst Rev2013;10:CD00827711. Ettehad D, Emdin CA, Kiran A, et al. Bloodpressure lowering for prevention of cardiovascu-lar disease and death: a systematic review andmeta-analysis. Lancet 2016;387:957–96712. Brunstrom M, Carlberg B. Effect of antihy-pertensive treatment at different blood pressurelevels in patients with diabetes mellitus: system-atic review and meta-analyses. BMJ 2016;352:i71713. Bangalore S, Kumar S, Lobach I, Messerli FH.Blood pressure targets in subjects with type 2diabetesmellitus/impaired fasting glucose: obser-vations from traditional and bayesian random-effects meta-analyses of randomized trials.Circulation 2011;123:2799–281014. Thomopoulos C, Parati G, Zanchetti A. Effectsof blood-pressure-lowering treatment on out-come incidence in hypertension: 10 - should bloodpressure management differ in hypertensive pa-tients with and without diabetes mellitus? Over-view and meta-analyses of randomized trials. JHypertens 2017;35:922–944
15. Xie X, Atkins E, Lv J, et al. Effects of intensiveblood pressure lowering on cardiovascular andrenal outcomes: updated systematic review andmeta-analysis. Lancet 2016;387:435–44316. Cushman WC, Evans GW, Byington RP, et al.;ACCORD Study Group. Effects of intensive blood-pressure control in type 2 diabetes mellitus. NEngl J Med 2010;362:1575–158517. Patel A, MacMahon S, Chalmers J, et al.;ADVANCE Collaborative Group. Effects of a fixedcombination of perindopril and indapamide onmacrovascular andmicrovascular outcomes in pa-tientswith type 2 diabetesmellitus (the ADVANCEtrial): a randomised controlled trial. Lancet 2007;370:829–84018. Bakris GL. The implications of blood pressuremeasurement methods on treatment targets forblood pressure. Circulation 2016;134:904–90519. Association AD; American Diabetes Associa-tion. Glycemic targets. Sec. 6. In Standards ofMedical Care in Diabetesd2017. Diabetes Care2017;40(Suppl. 1):S48–S5620. Blood Pressure Lowering Treatment Trialists’Collaboration. Blood pressure-lowering treat-ment based on cardiovascular risk: a meta-analysisof individual patient data. Lancet 2014;384:591–59820a. Whelton PK, Carey RM, Aronow WS, et al.2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the preven-tion, detection, evaluation, and managementof high blood pressure in adults. J Am Coll Cardiol.In press21. Sacks FM, Svetkey LP, Vollmer WM, et al.;DASH-Sodium Collaborative Research Group. Ef-fects onbloodpressureof reduceddietary sodiumand the Dietary Approaches to Stop Hypertension(DASH) diet. N Engl J Med 2001;344:3–1022. James PA, Oparil S, Carter BL, et al. 2014evidence-based guideline for the management ofhigh blood pressure in adults: report from the panelmembers appointed to the Eighth Joint NationalCommittee (JNC 8). JAMA 2014;311:507–52023. Bakris GL, Weir MR; Study of Hypertensionand the Efficacy of Lotrel in Diabetes (SHIELD)Investigators. Achieving goal blood pressure inpatientswith type 2 diabetes: conventional versusfixed-dose combination approaches. J Clin Hyper-tens (Greenwich) 2003;5:202–20924. Feldman RD, Zou GY, Vandervoort MK,WongCJ, Nelson SAE, Feagan BG. A simplified approachto the treatment of uncomplicated hypertension:a cluster randomized, controlled trial. Hyperten-sion 2009;53:646–65325. Bangalore S, Kamalakkannan G, Parkar S,Messerli FH. Fixed-dose combinations improvemedication compliance: a meta-analysis. Am JMed 2007;120:713–71926. Catala-Lopez F, Macıas Saint-Gerons D,Gonzalez-Bermejo D, et al. Cardiovascular and re-nal outcomes of renin-angiotensin system block-ade in adult patients with diabetes mellitus:a systematic review with network meta-analyses.PLoS Med 2016;13:e100197127. Palmer SC, Mavridis D, Navarese E, et al.Comparative efficacy and safety of blood pressure-lowering agents in adults with diabetes and kidneydisease: a networkmeta-analysis. Lancet 2015;385:2047–205628. Barzilay JI, Davis BR, Bettencourt J, et al.;ALLHAT Collaborative Research Group. Cardiovas-cular outcomesusing doxazosin vs. chlorthalidone
for the treatment of hypertension in older adultswith andwithout glucose disorders: a report fromthe ALLHAT study. J Clin Hypertens (Greenwich)2004;6:116–12529. Weber MA, Bakris GL, Jamerson K, et al.;ACCOMPLISH Investigators. Cardiovascular eventsduring differing hypertension therapies in pa-tients with diabetes. J Am Coll Cardiol 2010;56:77–8530. Bangalore S, Fakheri R, Toklu B, Messerli FH.Diabetes mellitus as a compelling indication foruse of renin angiotensin system blockers: system-atic review and meta-analysis of randomized tri-als. BMJ 2016;352:i43831. Carlberg B, Samuelsson O, Lindholm LH. Ate-nolol in hypertension: is it a wise choice? Lancet2004;364:1684–168932. Yusuf S, Teo KK, Pogue J, et al.; ONTARGETInvestigators. Telmisartan, ramipril, or both in pa-tients at high risk for vascular events. N Engl JMed2008;358:1547–155933. Fried LF, Emanuele N, Zhang JH, et al.; VANEPHRON-D Investigators. Combined angiotensininhibition for the treatment of diabetic nephrop-athy. N Engl J Med 2013;369:1892–190334. Makani H, Bangalore S, Desouza KA, Shah A,Messerli FH. Efficacy and safety of dual blockadeof the renin-angiotensin system: meta-analysis ofrandomised trials. BMJ 2013;346:f36035. Zhao P, Xu P, Wan C, Wang Z. Evening versusmorning dosing regimen drug therapy for hyper-tension. Cochrane Database Syst Rev 2011 (10):CD00418436. Hermida RC, Ayala DE, Mojon A, FernandezJR. Influence of time of day of blood pressure-lowering treatment on cardiovascular risk in hy-pertensive patientswith type 2 diabetes. DiabetesCare 2011;34:1270–127637. Nilsson E, Gasparini A, Arnlov J, et al. Inci-dence and determinants of hyperkalemia andhypokalemia in a large healthcare system. Int JCardiol 2017;245:277–28438. Bandak G, Sang Y, Gasparini A, et al. Hyper-kalemia after initiating renin-angiotensin systemblockade: the Stockholm Creatinine Measure-ments (SCREAM) project. J Am Heart Assoc2017;6:e00542839. Hughes-Austin JM, Rifkin DE, Beben T, et al.The relation of serum potassium concentra-tion with cardiovascular events and mortality incommunity-living individuals. Clin J Am Soc Nephrol2017;12:245–25240. James MT, Grams ME, Woodward M, et al.;CKDPrognosis Consortium. Ameta-analysis of theassociation of estimated GFR, albuminuria, diabe-tes mellitus, and hypertension with acute kidneyinjury. Am J Kidney Dis 2015;66:602–61241. Iliescu R, Lohmeier TE, Tudorancea I, Laffin L,Bakris GL. Renal denervation for the treatment ofresistant hypertension: review and clinical perspec-tive. Am J Physiol Renal Physiol 2015;309:F583–F59442. Bakris GL, Agarwal R, Chan JC, et al.; Miner-alocorticoid Receptor Antagonist TolerabilityStudy–Diabetic Nephropathy (ARTS-DN) StudyGroup. Effect of finerenone on albuminuria in pa-tients with diabetic nephropathy: a randomizedclinical trial. JAMA 2015;314:884–89443. Williams B, MacDonald TM, Morant S, et al.;British Hypertension Society’s PATHWAY StudiesGroup. Spironolactone versus placebo, bisoprolol,and doxazosin to determine the optimal treatment
care.diabetesjournals.org Cardiovascular Disease and Risk Management S101

for drug-resistant hypertension (PATHWAY-2):a randomised, double-blind, crossover trial. Lancet2015;386:2059–206844. Filippatos G, Anker SD, Bohm M, et al. Arandomized controlled study of finerenone vs.eplerenone in patients with worsening chronicheart failure and diabetes mellitus and/or chronickidney disease. Eur Heart J 2016;37:2105–211445. Bomback AS, Klemmer PJ. Mineralocorticoidreceptor blockade in chronic kidney disease.Blood Purif 2012;33:119–12446. American College of Obstetricians and Gyne-cologists; Task Force on Hypertension in Preg-nancy. Hypertension in pregnancy. Report of theAmerican College of Obstetricians and Gynecolo-gists’ Task Force on Hypertension in Pregnancy.Obstet Gynecol 2013;122:1122–113147. Abalos E, Duley L, Steyn DW. Antihyperten-sive drug therapy for mild to moderate hyperten-sion during pregnancy. Cochrane Database SystRev 2014;2:CD00225248. Al-Balas M, Bozzo P, Einarson A. Use of diu-retics during pregnancy. Can Fam Physician 2009;55:44–4549. IrgensHU, Reisaeter L, Irgens LM, Lie RT. Longterm mortality of mothers and fathers after pre-eclampsia: population based cohort study. BMJ2001;323:1213–121750. Chasman DI, Posada D, Subrahmanyan L,Cook NR, Stanton VP Jr, Ridker PM. Pharmacoge-netic study of statin therapy and cholesterol re-duction. JAMA 2004;291:2821–282751. Meek C, Wierzbicki AS, Jewkes C, et al. Dailyand intermittent rosuvastatin 5 mg therapy instatin intolerant patients: an observational study.Curr Med Res Opin 2012;28:371–37852. Mihaylova B, Emberson J, Blackwell L, et al.;Cholesterol Treatment Trialists’ (CTT) Collabora-tors. The effects of lowering LDL cholesterolwith statin therapy in people at low risk of vascu-lar disease: meta-analysis of individual data from27 randomised trials. Lancet 2012;380:581–59053. Baigent C, Keech A, Kearney PM, et al.; Cho-lesterol Treatment Trialists’ (CTT) Collaborators.Efficacy and safety of cholesterol-lowering treat-ment: prospective meta-analysis of data from90,056 participants in 14 randomised trials of sta-tins. Lancet 2005;366:1267–127854. Pyorala K, PedersenTR, KjekshusJ, FaergemanO,Olsson AG, Thorgeirsson G. Cholesterol loweringwith simvastatin improves prognosis of diabeticpatients with coronary heart disease. A subgroupanalysis of the Scandinavian Simvastatin SurvivalStudy (4S). Diabetes Care 1997;20:614–62055. Collins R, Armitage J, Parish S, SleighP, PetoR;Heart Protection Study Collaborative Group.MRC/BHF Heart Protection Study of cholesterol-lowering with simvastatin in 5963 people withdiabetes: a randomised placebo-controlled trial.Lancet 2003;361:2005–201656. Goldberg RB,MelliesMJ, Sacks FM, et al.; TheCare Investigators. Cardiovascular events andtheir reduction with pravastatin in diabeticand glucose-intolerant myocardial infarctionsurvivors with average cholesterol levels: sub-group analyses in the Cholesterol And Recur-rent Events (CARE) trial. Circulation 1998;98:2513–251957. Shepherd J, Barter P, Carmena R, et al. Effectof lowering LDL cholesterol substantially belowcurrently recommended levels in patients withcoronary heart disease and diabetes: the Treating
to New Targets (TNT) study. Diabetes Care 2006;29:1220–122658. Sever PS, Poulter NR, Dahlof B, et al. Reduc-tion in cardiovascular events with atorvastatinin 2,532 patients with type 2 diabetes: Anglo-Scandinavian Cardiac Outcomes Trial–lipid-lower-ing arm (ASCOT-LLA). Diabetes Care 2005;28:1151–115759. Knopp RH, d’Emden M, Smilde JG, Pocock SJ.Efficacy and safety of atorvastatin in the preven-tion of cardiovascular end points in subjects withtype 2 diabetes: the Atorvastatin Study for Pre-ventionof CoronaryHeartDiseaseEndpoints inNon-Insulin-Dependent Diabetes Mellitus (ASPEN).Diabetes Care 2006;29:1478–148560. Colhoun HM, Betteridge DJ, Durrington PN,et al.; CARDS investigators. Primary prevention ofcardiovascular disease with atorvastatin in type 2diabetes in the Collaborative Atorvastatin Diabe-tes Study (CARDS): multicentre randomisedplacebo-controlled trial. Lancet 2004;364:685–69661. Kearney PM, Blackwell L, Collins R, et al.; Cho-lesterol Treatment Trialists’ (CTT) Collaborators.Efficacy of cholesterol-lowering therapy in18,686 people with diabetes in 14 randomisedtrials of statins: a meta-analysis. Lancet 2008;371:117–12562. Taylor F, HuffmanMD,Macedo AF, et al. Sta-tins for the primary prevention of cardiovasculardisease. Cochrane Database Syst Rev 2013 (1):CD00481663. Carter AA, Gomes T, Camacho X, Juurlink DN,Shah BR, Mamdani MM. Risk of incident diabetesamong patients treated with statins: populationbased study [published correction appears in BMJ2013;347:f4356]. BMJ 2013;346:f261064. Cannon CP, Braunwald E, McCabe CH, et al.;Pravastatin or Atorvastatin Evaluation and In-fection Therapy-Thrombolysis in Myocardial In-farction 22 Investigators. Intensive versusmoderate lipid lowering with statins after acutecoronary syndromes. N Engl J Med 2004;350:1495–150465. Cannon CP, Blazing MA, Giugliano RP, et al.;IMPROVE-IT Investigators. Ezetimibe added tostatin therapy after acute coronary syndromes.N Engl J Med 2015;372:2387–239766. Sabatine MS, Giugliano RP, Keech AC, et al.;FOURIER Steering Committee and Investigators.Evolocumab and clinical outcomes in patientswith cardiovascular disease. N Engl J Med 2017;376:1713–172267. Bohula EA, Morrow DA, Giugliano RP, et al.Atherothrombotic risk stratification and ezetimibefor secondary Prevention. J Am Coll Cardiol 2017;69:911–92168. Bohula EA, Bonaca MP, Braunwald E, et al.Atherothrombotic risk stratification and the effi-cacy and safety of vorapaxar in patients withstable ischemic heart disease and previousmyocardial infarction. Circulation 2016;134:304–31369. de Ferranti SD, de Boer IH, Fonseca V, et al.Type 1 diabetes mellitus and cardiovascular dis-ease: a scientific statement from the AmericanHeart Association and American Diabetes Associ-ation. Circulation 2014;130:1110–113070. Bowman L, Hopewell JC, Chen F, et al.; HPS3/TIMI55–REVEAL Collaborative Group. Effectsof anacetrapib in patients with atheroscleroticvascular disease. N Engl J Med 2017;377:1217–1227
71. Moriarty PM, Jacobson TA, Bruckert E, et al.Efficacy and safety of alirocumab, a monoclonalantibody to PCSK9, in statin-intolerant patients:design and rationale of ODYSSEY ALTERNATIVE,a randomized phase 3 trial. J Clin Lipidol 2014;8:554–56172. Zhang X-L, Zhu Q-Q, Zhu L, et al. Safety andefficacy of anti-PCSK9 antibodies: a meta-analysisof 25 randomized, controlled trials. BMC Med2015;13:12373. Sabatine MS, Leiter LA, Wiviott SD, et al. Car-diovascular safety and efficacy of the PCSK9 in-hibitor evolocumab in patients with and withoutdiabetes and the effect of evolocumab on glycae-mia and risk of new-onset diabetes: a prespecifiedanalysis of the FOURIER randomised controlledtrial [article online]. Lancet Diabetes Endocrinol2017. Available from http://www.thelancet.com/journals/landia/article/PIIS2213-8587(17)30313-3/abstract. Accessed 28 September 201774. Barter PJ, Caulfield M, Eriksson M, et al.;ILLUMINATE Investigators. Effects of torcetrapibin patients at high risk for coronary events. N EnglJ Med 2007;357:2109–212275. Schwartz GG, Olsson AG, Abt M, et al.; dal-OUTCOMES Investigators. Effects of dalcetrapib inpatients with a recent acute coronary syndrome.N Engl J Med 2012;367:2089–209976. Lincoff AM, Nicholls SJ, Riesmeyer JS, et al.;ACCELERATE Investigators. Evacetrapib and car-diovascular outcomes in high-risk vascular dis-ease. N Engl J Med 2017;376:1933–194277. Berglund L, Brunzell JD, Goldberg AC, et al.;Endocrine society. Evaluation and treatment ofhypertriglyceridemia: an Endocrine Society clini-cal practice guideline. J Clin Endocrinol Metab2012;97:2969–298978. Singh IM, Shishehbor MH, Ansell BJ. High-density lipoprotein as a therapeutic target: a sys-tematic review. JAMA 2007;298:786–79879. Keech A, Simes RJ, Barter P, et al.; FIELD studyinvestigators. Effects of long-term fenofibratetherapy on cardiovascular events in 9795 peoplewith type 2 diabetes mellitus (the FIELD study):randomised controlled trial. Lancet 2005;366:1849–186180. Jones PH, Davidson MH. Reporting rate ofrhabdomyolysis with fenofibrate 1 statin versusgemfibrozil 1 any statin. Am J Cardiol 2005;95:120–12281. Ginsberg HN, Elam MB, Lovato LC, et al.;ACCORDStudyGroup. Effects of combination lipidtherapy in type 2 diabetes mellitus. N Engl J Med2010;362:1563–157482. Boden WE, Probstfield JL, Anderson T, et al.;AIM-HIGH Investigators. Niacin in patients withlow HDL cholesterol levels receiving intensive sta-tin therapy. N Engl J Med 2011;365:2255–226783. Landray MJ, Haynes R, Hopewell JC, et al.;HPS2-THRIVE Collaborative Group. Effects ofextended-release niacin with laropiprant in high-risk patients. N Engl J Med 2014;371:203–21284. Rajpathak SN, Kumbhani DJ, Crandall J,Barzilai N, AldermanM, Ridker PM. Statin therapyand risk of developing type 2 diabetes: a meta-analysis. Diabetes Care 2009;32:1924–192985. Sattar N, Preiss D, Murray HM, et al. Statinsand risk of incident diabetes: a collaborativemeta-analysis of randomised statin trials. Lancet2010;375:735–74286. Ridker PM, Pradhan A, MacFadyen JG, LibbyP, Glynn RJ. Cardiovascular benefits and diabetes
S102 Cardiovascular Disease and Risk Management Diabetes Care Volume 41, Supplement 1, January 2018

risks of statin therapy in primary prevention: ananalysis from the JUPITER trial. Lancet 2012;380:565–57187. Richardson K, Schoen M, French B, et al. Sta-tins and cognitive function: a systematic review.Ann Intern Med 2013;159:688–69788. Giugliano RP, Mach F, Zavitz K, et al.;EBBINGHAUS Investigators. Cognitive functionin a randomized trial of evolocumab. N Engl JMed 2017;377:633–64389. Baigent C, Blackwell L, Collins R, et al.; Antith-rombotic Trialists’ (ATT) Collaboration. Aspirin inthe primary and secondary prevention of vasculardisease: collaborative meta-analysis of individualparticipant data from randomised trials. Lancet2009;373:1849–186090. Perk J, DeBackerG, GohlkeH, et al.; EuropeanAssociation for Cardiovascular Prevention & Re-habilitation (EACPR); ESC Committee for PracticeGuidelines (CPG). European Guidelines on cardio-vascular disease prevention in clinical practice(version 2012). The Fifth Joint Task Force of theEuropean Society of Cardiology and Other Socie-ties on Cardiovascular Disease Prevention in Clin-ical Practice (constituted by representatives ofnine societies and by invited experts). Eur HeartJ 2012;33:1635–170191. Belch J, MacCuish A, Campbell I, et al. Theprevention of progression of arterial disease anddiabetes (POPADAD) trial: factorial randomisedplacebo controlled trial of aspirin and antioxidantsin patients with diabetes and asymptomatic pe-ripheral arterial disease. BMJ 2008;337:a184092. Zhang C, Sun A, Zhang P, et al. Aspirin forprimary prevention of cardiovascular events inpatients with diabetes: A meta-analysis. DiabetesRes Clin Pract 2010;87:211–21893. De Berardis G, Sacco M, Strippoli GFM, et al.Aspirin for primary prevention of cardiovascularevents in people with diabetes: meta-analysis ofrandomised controlled trials. BMJ 2009;339:b453194. Pignone M, Earnshaw S, Tice JA, Pletcher MJ.Aspirin, statins, or both drugs for the primary pre-vention of coronary heart disease events in men:a cost-utility analysis. Ann Intern Med 2006;144:326–33695. Pignone M, Alberts MJ, Colwell JA, et al.;American Diabetes Association; American HeartAssociation; American College of CardiologyFoundation. Aspirin for primary prevention of car-diovascular events in people with diabetes: a po-sition statement of the American DiabetesAssociation, a scientific statement of the Ameri-can Heart Association, and an expert consensusdocument of the American College of CardiologyFoundation. Diabetes Care 2010;33:1395–140296. HuxleyRR, PetersSAE,MishraGD,WoodwardM.Risk of all-cause mortality and vascular events inwomen versus men with type 1 diabetes: a sys-tematic review and meta-analysis. Lancet Diabe-tes Endocrinol 2015;3:198–20697. Peters SAE, Huxley RR, Woodward M. Diabe-tes as risk factor for incident coronary heart dis-ease in women comparedwithmen: a systematicreview and meta-analysis of 64 cohorts including858,507 individuals and 28,203 coronary events.Diabetologia 2014;57:1542–155198. Kalyani RR, LazoM,Ouyang P, et al. Sex differ-ences in diabetes and risk of incident coronaryartery disease in healthy young and middle-agedadults. Diabetes Care 2014;37:830–838
99. Peters SAE, Huxley RR,WoodwardM. Diabe-tes as a risk factor for stroke in women com-pared with men: a systematic review andmeta-analysis of 64 cohorts, including 775,385individuals and 12,539 strokes. Lancet 2014;383:1973–1980100. Dimitriu-Leen AC, Scholte AJHA, vanRosendael AR, et al. Value of coronary computedtomography angiography in tailoring aspirin ther-apy for primary prevention of atheroscleroticevents in patients at high risk with diabetes melli-tus. Am J Cardiol 2016;117:887–893101. Larsen SB, Grove EL, Neergaard-Petersen S,Wurtz M, Hvas A-M, Kristensen SD. Determinantsof reduced antiplatelet effect of aspirin in patientswith stable coronary artery disease. PLoS One2015;10:e0126767102. Mora S, Ames JM, Manson JE. Low-dose as-pirin in the primary prevention of cardiovasculardisease: shared decision making in clinical prac-tice. JAMA 2016;316:709–710103. Campbell CL, Smyth S, Montalescot G,Steinhubl SR. Aspirin dose for the prevention ofcardiovascular disease: a systematic review. JAMA2007;297:2018–2024104. Davı G, Patrono C. Platelet activation andatherothrombosis. N Engl J Med 2007;357:2482–2494105. Zaccardi F, Rizzi A, Petrucci G, et al. In vivoplatelet activation and aspirin responsiveness intype 1 diabetes. Diabetes 2016;65:503–509106. Bethel MA, Harrison P, Sourij H, et al. Ran-domized controlled trial comparing impact onplatelet reactivity of twice-daily with once-dailyaspirin in people with type 2 diabetes. DiabetMed 2016;33:224–230107. Vandvik PO, Lincoff AM, Gore JM, et al. Pri-mary and secondary prevention of cardiovasculardisease: Antithrombotic Therapy and Preventionof Thrombosis, 9th ed: American College ofChest Physicians Evidence-Based Clinical PracticeGuidelines [published correction appears in Chest2012;141:1129]. Chest 2012;141(Suppl.):e637S–e668S108. Bhatt DL, Bonaca MP, Bansilal S, et al. Re-duction in ischemic events with ticagrelor in di-abetic patients with prior myocardial infarction inPEGASUS-TIMI 54. J Am Coll Cardiol 2016;67:2732–2740109. Bax JJ, Young LH, Frye RL, Bonow RO,Steinberg HO, Barrett EJ; ADA. Screening for cor-onary artery disease in patients with diabetes. Di-abetes Care 2007;30:2729–2736110. Boden WE, O’Rourke RA, Teo KK, et al.;COURAGE Trial Research Group. Optimal medicaltherapy with or without PCI for stable coronarydisease. N Engl J Med 2007;356:1503–1516111. BARI 2D Study Group, Frye RL, August P,et al. A randomized trial of therapies for type 2diabetes and coronary artery disease. N Engl JMed 2009;360:2503–2015112. Wackers FJT, Chyun DA, Young LH, et al.;Detection of Ischemia in Asymptomatic Diabetics(DIAD) Investigators. Resolution of asymptomaticmyocardial ischemia in patients with type 2 dia-betes in the Detection of Ischemia in Asymptom-atic Diabetics (DIAD) study. Diabetes Care 2007;30:2892–2898113. Elkeles RS, Godsland IF, Feher MD, et al.;PREDICT Study Group. Coronary calcium mea-surement improves prediction of cardiovascularevents in asymptomatic patients with type 2
diabetes: the PREDICT study. Eur Heart J 2008;29:2244–2251114. Raggi P, Shaw LJ, Berman DS, Callister TQ.Prognostic value of coronary artery calciumscreening in subjects with and without diabetes.J Am Coll Cardiol 2004;43:1663–1669115. Anand DV, Lim E, Hopkins D, et al. Risk strat-ification in uncomplicated type 2 diabetes: pro-spective evaluation of the combined use ofcoronary artery calcium imaging and selectivemyocardial perfusion scintigraphy. Eur Heart J2006;27:713–721116. Young LH, Wackers FJT, Chyun DA, et al.;DIAD Investigators. Cardiac outcomes afterscreening for asymptomatic coronary artery dis-ease in patients with type 2 diabetes: the DIADstudy: a randomized controlled trial. JAMA 2009;301:1547–1555117. Wackers FJT, Young LH, Inzucchi SE, et al.;Detection of Ischemia in Asymptomatic Dia-betics Investigators. Detection of silent myocar-dial ischemia in asymptomatic diabetic subjects:the DIAD study. Diabetes Care 2004;27:1954–1961118. Scognamiglio R, Negut C, Ramondo A,Tiengo A, Avogaro A. Detection of coronary ar-tery disease in asymptomatic patients withtype 2 diabetes mellitus. J Am Coll Cardiol2006;47:65–71119. Hadamitzky M, Hein F, Meyer T, et al. Prog-nostic value of coronary computed tomographicangiography in diabetic patients without knowncoronary artery disease. Diabetes Care 2010;33:1358–1363120. Choi E-K, Chun EJ, Choi S-I, et al. Assessmentof subclinical coronary atherosclerosis inasymptomatic patients with type 2 diabetesmellitus with single photon emission computedtomography and coronary computed tomogra-phy angiography. Am J Cardiol 2009;104:890–896121. Wing RR, Bolin P, Brancati FL, et al.; LookAHEAD Research Group. Cardiovascular effectsof intensive lifestyle intervention in type 2 diabe-tes. N Engl J Med 2013;369:145–154122. Braunwald E, DomanskiMJ, Fowler SE, et al.;PEACE Trial Investigators. Angiotensin-converting-enzyme inhibition in stable coronary artery dis-ease. N Engl J Med 2004;351:2058–2068123. Telmisartan Randomised AssessmeNt Studyin ACE iNtolerant subjectswith cardiovascular Dis-ease (TRANSCEND) Investigators, Yusuf S, Teo K,et al. Effects of the angiotensin-receptor blockertelmisartan on cardiovascular events in high-riskpatients intolerant to angiotensin-converting en-zyme inhibitors: a randomised controlled trial.Lancet 2008;372:1174–1183124. Kezerashvili A, Marzo K, De Leon J. Betablocker use after acute myocardial infarction inthe patient with normal systolic function: whenis it “ok” to discontinue? Curr Cardiol Rev 2012;8:77–84125. KannelWB,HjortlandM, CastelliWP.Role ofdiabetes in congestive heart failure: the Framing-ham study. Am J Cardiol 1974;34:29–34126. Dormandy JA, Charbonnel B, Eckland DJA,et al.; PROactive Investigators. Secondarypreventionof macrovascular events in patients with type 2diabetes in the PROactive Study (PROspectivepioglitAzone ClinicalTrial InmacroVascularEvents):a randomised controlled trial. Lancet 2005;366:1279–1289
care.diabetesjournals.org Cardiovascular Disease and Risk Management S103

127. Singh S, Loke YK, Furberg CD. Long-term riskof cardiovascular events with rosiglitazone:a meta-analysis. JAMA 2007;298:1189–1195128. Lincoff AM, Wolski K, Nicholls SJ, Nissen SE.Pioglitazone and risk of cardiovascular events inpatients with type 2 diabetes mellitus: a meta-analysis of randomized trials. JAMA 2007;298:1180–1188129. Scirica BM, Bhatt DL, Braunwald E, et al.;SAVOR-TIMI 53 Steering Committee and Investi-gators. Saxagliptin and cardiovascular outcomesin patients with type 2 diabetes mellitus. N Engl JMed 2013;369:1317–1326130. U.S. Food and Drug Administration. Diabe-tes medications containing saxagliptin and alog-liptin: drug safety communication - risk of heartfailure [Internet]. Available from https://www.fda.gov/safety/medwatch/safetyinformation/safetyalertsforhumanmedicalproducts/ucm494252.htm. Accessed 13 October 2017131. Zannad F, Cannon CP, Cushman WC, et al.;EXAMINE Investigators. Heart failure and mortal-ity outcomes in patients with type 2 diabetes tak-ing alogliptin versus placebo in EXAMINE:a multicentre, randomised, double-blind trial.Lancet 2015;385:2067–2076132. Green JB, Bethel MA, Armstrong PW, et al.;TECOS StudyGroup. Effect of sitagliptin on cardio-vascular outcomes in type 2 diabetes. N Engl JMed 2015;373:232–242133. Zinman B, Wanner C, Lachin JM, et al.;EMPA-REG OUTCOME Investigators. Empagliflozin,cardiovascular outcomes, and mortality in type 2diabetes. N Engl J Med 2015;373:2117–2128
134. Fitchett D, Butler J, van de Borne P, et al.Effects of empagliflozin on risk for cardiovasculardeath and heart failure hospitalization across thespectrum of heart failure risk in the EMPA-REGOUTCOME trial [article online]. Eur Heart J 2017.Available from https://academic.oup.com/eurheartj/article/doi/10.1093/eurheartj/ehx511/4096345/Effects-of-empagliflozin-on-risk-for. Ac-cessed 29 September 2017135. Neal B, Perkovic V, Mahaffey KW, et al.;CANVAS Program Collaborative Group. Cana-gliflozin and cardiovascular and renal eventsin type 2 diabetes. N Engl J Med 2017;377:644–657136. Neal B, Perkovic V, Matthews DR, et al. Ra-tionale, design and baseline characteristics of theCANagliflozin cardioVascular Assessment Study-Renal (CANVAS-R): a randomized, placebo controlledtrial. Diabetes Obes Metab 2017;19:387–393137. U.S. Food and Drug Administration. Guid-ance for industry diabetes mellitus: evaluatingcardiovascular risk in new antidiabetic therapiesto treat type 2 diabetes. Silver Spring, MD, 2008.Available from http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/ucm071627.pdf). Accessed 3 November2017138. Marso SP, Daniels GH, Brown-Frandsen K,et al.; LEADER Steering Committee; LEADER TrialInvestigators. Liraglutide and cardiovascular out-comes in type 2 diabetes. N Engl J Med 2016;375:311–322139. MarsoSP, Bain SC, Consoli A, et al.; SUSTAIN-6 Investigators. Semaglutide and cardiovascular
outcomes in patients with type 2 diabetes. NEngl J Med 2016;375:1834–1844140. Pfeffer MA, Claggett B, Diaz R, et al.; ELIXAInvestigators. Lixisenatide in patients with type 2diabetes and acute coronary syndrome. N Engl JMed 2015;373:2247–2257141. Holman RR, Bethel MA, Mentz RJ, et al.;EXSCEL Study Group. Effects of once-weekly exe-natide on cardiovascular outcomes in type 2 di-abetes. N Engl J Med 2017;377:1228–1239142. Zoungas S, Chalmers J, Neal B, et al.;ADVANCE-ON Collaborative Group. Follow-upof blood-pressure lowering and glucose controlin type 2 diabetes. N Engl J Med 2014;371:1392–1406143. Hansson L, Zanchetti A, Carruthers SG, et al.;HOT Study Group. Effects of intensive blood-pressure lowering and low-dose aspirin in pa-tients with hypertension: principal results of theHypertension Optimal Treatment (HOT) rando-mised trial. Lancet 1998;351:1755–1762144. Wright JT Jr, Williamson JD, Whelton PK,et al.; SPRINT Research Group. A randomized trialof intensive versus standard blood-pressure con-trol. N Engl J Med 2015;373:2103–2116145. White WB, Cannon CP, Heller SR, et al.;EXAMINE Investigators. Alogliptin after acute cor-onary syndrome in patients with type 2 diabetes.N Engl J Med 2013;369:1327–1335146. CefaluWT, Kaul S, Gerstein HC, et al. Cardio-vascular outcomes trials in type 2 diabetes: wheredo we go from here? Reflections from a DiabetesCare Editors’ Expert Forum. Diabetes Care. Inpress
S104 Cardiovascular Disease and Risk Management Diabetes Care Volume 41, Supplement 1, January 2018





























