Embed Size (px)
Citation preview

2. Classification and Diagnosis ofDiabetes: Standards of MedicalCare in Diabetesd2018Diabetes Care 2018;41(Suppl. 1):S13–S27 | https://doi.org/10.2337/dc18-S002
The American Diabetes Association (ADA) “Standards of Medical Care in Diabetes”includes ADA’s current clinical practice recommendations and is intended to providethe components of diabetes care, general treatment goals and guidelines, and toolsto evaluate quality of care. Members of the ADA Professional Practice Committee, amultidisciplinary expert committee, are responsible for updating the Standards ofCare annually, or more frequently as warranted. For a detailed description of ADAstandards, statements, and reports, aswell as the evidence-grading system forADA’sclinical practice recommendations, please refer to the Standards of Care Introduc-tion. Readers who wish to comment on the Standards of Care are invited to do soat professional.diabetes.org/SOC.
CLASSIFICATION
Diabetes can be classified into the following general categories:
1. Type 1 diabetes (due to autoimmune b-cell destruction, usually leading to absoluteinsulin deficiency)
2. Type 2 diabetes (due to a progressive loss of b-cell insulin secretion frequently onthe background of insulin resistance)
3. Gestational diabetes mellitus (GDM) (diabetes diagnosed in the second or thirdtrimester of pregnancy that was not clearly overt diabetes prior to gestation)
4. Specific types of diabetes due to other causes, e.g., monogenic diabetes syndromes(such as neonatal diabetes and maturity-onset diabetes of the young [MODY]),diseases of the exocrine pancreas (such as cystic fibrosis and pancreatitis), anddrug- or chemical-induced diabetes (such as with glucocorticoid use, in the treat-ment of HIV/AIDS, or after organ transplantation)
This section reviews most common forms of diabetes but is not comprehensive. Foradditional information, see the American Diabetes Association (ADA) position state-ment “Diagnosis and Classification of Diabetes Mellitus” (1).
Type 1 diabetes and type 2 diabetes are heterogeneous diseases in which clinicalpresentationanddiseaseprogressionmay vary considerably. Classification is importantfor determining therapy, but some individuals cannot be clearly classified as havingtype 1 or type 2 diabetes at the time of diagnosis. The traditional paradigms of type 2diabetes occurring only in adults and type 1 diabetes only in children are no longeraccurate, as both diseases occur in both age-groups. Children with type 1 diabe-tes typically present with the hallmark symptoms of polyuria/polydipsia, and approx-imately one-third present with diabetic ketoacidosis (DKA) (2). The onset of type 1diabetes may be more variable in adults, and they may not present with the classicsymptoms seen in children. Occasionally, patients with type 2 diabetes may presentwith DKA, particularly ethnic minorities (3). Although difficulties in distinguishing
Suggested citation: American Diabetes Associa-tion. 2. Classification and diagnosis of diabetes:Standards of Medical Care in Diabetesd2018.Diabetes Care 2018;41(Suppl. 1):S13–S27
© 2017 by the American Diabetes Association.Readers may use this article as long as the workis properly cited, the use is educational and notfor profit, and the work is not altered. More infor-mation is available at http://www.diabetesjournals.org/content/license.
American Diabetes Association
Diabetes Care Volume 41, Supplement 1, January 2018 S13
2.CLA
SSIFICATIO
NANDDIAGNOSIS
OFDIABETES

diabetes typemay occur in all age-groupsat onset, the true diagnosis becomesmore obvious over time.In both type 1 and type 2 diabetes,
various genetic and environmental fac-tors can result in the progressive loss ofb-cell mass and/or function that mani-fests clinically as hyperglycemia. Oncehyperglycemia occurs, patients with allforms of diabetes are at risk for devel-oping the same chronic complications,although rates of progression may differ.The identification of individualized thera-pies for diabetes in the future will requirebetter characterization of themany pathsto b-cell demise or dysfunction (4).Characterization of the underlying
pathophysiology is more developed intype 1 diabetes than in type 2 diabetes.It is now clear from studies of first-degreerelatives of patients with type 1 diabetesthat the persistent presence of two ormore autoantibodies is an almost certainpredictor of clinical hyperglycemia anddiabetes. The rate of progression is de-pendent on the age at first detection ofantibody, number of antibodies, antibodyspecificity, and antibody titer. Glucoseand A1C levels rise well before the clinicalonset of diabetes, making diagnosisfeasiblewell before theonset ofDKA. Threedistinct stages of type 1 diabetes can beidentified (Table 2.1) and serve as aframework for future research and regu-latory decision-making (4,5).The paths to b-cell demise and dys-
function are less well defined in type 2diabetes, but deficient b-cell insulin se-cretion, frequently in the setting of insulinresistance, appears tobe the commonde-nominator. Characterization of subtypesof this heterogeneous disorder have beendeveloped and validated in Scandinavianand Northern European populations buthave not been confirmed in other ethnicand racial groups. Type 2 diabetes is pri-marily associated with insulin secretory
defects related to inflammation andmet-abolic stress among other contributors,including genetic factors. Future classi-fication schemes for diabetes will likelyfocus on the pathophysiology of the un-derlying b-cell dysfunction and the stageof disease as indicated by glucose status(normal, impaired, or diabetes) (4).
DIAGNOSTIC TESTS FOR DIABETES
Diabetes may be diagnosed based onplasma glucose criteria, either the fastingplasma glucose (FPG) or the 2-h plasmaglucose (2-h PG) value during a 75-g oralglucose tolerance test (OGTT), or A1C cri-teria (6) (Table 2.2).
Generally, FPG, 2-h PG during 75-gOGTT, and A1C are equally appropriatefor diagnostic testing. It should be notedthat the tests do not necessarily detectdiabetes in the same individuals. The ef-ficacy of interventions for primary pre-vention of type 2 diabetes (7,8) hasprimarily been demonstrated among in-dividuals who have impaired glucose tol-erance (IGT) with or without elevatedfasting glucose, not for individuals withisolated impaired fasting glucose (IFG)or for those with prediabetes defined byA1C criteria.
The same tests may be used to screenfor and diagnose diabetes and to detectindividuals with prediabetes. Diabetesmay be identified anywhere along thespectrum of clinical scenarios: in seem-ingly low-risk individuals who happen tohave glucose testing, in individuals testedbased on diabetes risk assessment, and insymptomatic patients.
Fasting and 2-Hour Plasma GlucoseThe FPG and 2-h PG may be used to di-agnose diabetes (Table 2.2). The concor-dance between the FPG and 2-h PG testsis imperfect, as is the concordance be-tween A1C and either glucose-basedtest. Numerous studies have confirmed
that compared with FPG and A1C cutpoints, the 2-h PG value diagnoses morepeople with diabetes.
A1C
Recommendations
c To avoid misdiagnosis or misseddiagnosis, the A1C test should beperformed using a method that iscertified by the NGSP and standard-ized to the Diabetes Control andComplications Trial (DCCT) assay. B
c Marked discordance between mea-sured A1C and plasma glucoselevels should raise the possibilityof A1C assay interference due tohemoglobin variants (i.e., hemoglo-binopathies) and consideration ofusing an assay without interferenceor plasma blood glucose criteria todiagnose diabetes. B
c In conditions associated with in-creased red blood cell turnover,such as sickle cell disease, pregnancy(second and third trimesters), hemo-dialysis, recent blood loss or transfu-sion, or erythropoietin therapy, onlyplasma blood glucose criteria shouldbe used to diagnose diabetes. B
The A1C test should be performed using amethod that is certified by the NGSP(www.ngsp.org) and standardized ortraceable to the Diabetes Control andComplications Trial (DCCT) reference as-say. Although point-of-care A1C assaysmaybeNGSP certified, proficiency testingis not mandated for performing the test,so use of point-of-care assays for diagnos-tic purposes is not recommended butmay be considered in the future if pro-ficiency testing is performed, documented,and deemed acceptable.
The A1C has several advantages com-pared with the FPG and OGTT, includinggreater convenience (fasting not required),
Table 2.1—Staging of type 1 diabetes (4,5)
Stage 1 Stage 2 Stage 3
Characteristics c Autoimmunity c Autoimmunity c New-onset hyperglycemia
c Normoglycemia c Dysglycemia c Symptomatic
c Presymptomatic c Presymptomatic
Diagnostic criteria c Multiple autoantibodies c Multiple autoantibodies c Clinical symptoms
c No IGT or IFG c Dysglycemia: IFG and/or IGT c Diabetes by standard criteria
c FPG 100–125 mg/dL (5.6–6.9 mmol/L)
c 2-h PG 140–199 mg/dL (7.8–11.0 mmol/L)
c A1C 5.7–6.4% (39–47 mmol/mol) or$10% increase in A1C
S14 Classification and Diagnosis of Diabetes Diabetes Care Volume 41, Supplement 1, January 2018

greater preanalytical stability, and lessday-to-day perturbations during stressand illness. However, these advantagesmay be offset by the lower sensitivity ofA1C at the designated cut point, greatercost, limited availability of A1C testing incertain regions of the developing world,and the imperfect correlation betweenA1C and average glucose in certain indi-viduals. National Health and NutritionExamination Survey (NHANES) data indi-cate that an A1C cut point of $6.5%(48 mmol/mol) identifies a prevalenceof undiagnosed diabetes that is one-thirdof that using glucose criteria (9).When using A1C to diagnose diabetes,
it is important to recognize that A1C isan indirect measure of average bloodglucose levels and to take other factorsinto consideration that may impact he-moglobin glycation independently ofglycemia including age, race/ethnicity,and anemia/hemoglobinopathies.
Age
The epidemiological studies that formedthe basis for recommending A1C to diag-nose diabetes included only adult popula-tions. Therefore, it remains unclearwhetherA1C and the same A1C cut point should beused to diagnose diabetes in children andadolescents (see p. S20 SCREENING AND TESTING
FOR TYPE 2 DIABETES AND PREDIABETES IN CHILDREN
AND ADOLESCENTS for additional information)(9,10).
Race/Ethnicity/Hemoglobinopathies
Hemoglobin variants can interfere withthe measurement of A1C, although most
assays in use in the U.S. are unaffected by
the most common variants. Marked dis-
crepancies between measured A1C andplasma glucose levels should prompt con-
sideration that the A1C assay may not be
reliable for that individual. For patients
with a hemoglobin variant but normal
red blood cell turnover, such as thosewith the sickle cell trait, an A1C assaywith-out interference fromhemoglobin variantsshould be used. An updated list of A1Cassays with interferences is available atwww.ngsp.org/interf.asp.
African Americans heterozygous for thecommon hemoglobin variant HbS mayhave, for any given level ofmean glycemia,lower A1C by about 0.3% than those with-out the trait (11). Another genetic variant,X-linked glucose-6-phosphate dehydro-genase G202A, carried by 11% of AfricanAmericans,was associatedwith a decreasein A1C of about 0.8% in hemizygous menand 0.7% in homozygous women com-pared with those without the variant (12).
Even in the absence of hemoglobinvariants, A1C levels may vary with race/ethnicity independently of glycemia(13–15). For example, African Americansmay have higher A1C levels than non-Hispanic whites with similar fasting andpostglucose load glucose levels (16), andA1C levelsmaybehigher for a givenmeanglucose concentration when measuredwith continuous glucose monitoring(17). Though conflicting data exists, AfricanAmericans may also have higher levelsof fructosamine and glycated albuminand lower levels of 1,5-anhydroglucitol,suggesting that their glycemic burden(particularly postprandially) may be higher(18,19). The association of A1C with riskfor complications appears to be similar inAfrican Americans and non-Hispanicwhites (20,21).
Red Blood Cell Turnover
In conditions associated with increasedred blood cell turnover, such as sicklecell disease, pregnancy (second and thirdtrimesters), hemodialysis, recent bloodloss or transfusion, or erythropoietin ther-apy, only plasma blood glucose criteriashould be used to diagnose diabetes (22).
Confirming the DiagnosisUnless there is a clear clinical diagnosis(e.g., patient in a hyperglycemic crisisor with classic symptoms of hyperglyce-mia and a random plasma glucose$200mg/dL [11.1 mmol/L]), a second test isrequired for confirmation. It is recom-mended that the same test be repeatedor a different test be performed withoutdelay using a new blood sample for con-firmation. For example, if the A1C is 7.0%(53mmol/mol) and a repeat result is 6.8%(51 mmol/mol), the diagnosis of diabetesis confirmed. If two different tests (suchas A1C and FPG) are both above the di-agnostic threshold, this also confirmsthe diagnosis. On the other hand, if a pa-tient has discordant results from twodifferent tests, then the test result thatis above the diagnostic cut point shouldbe repeated, with consideration of thepossibility of A1C assay interference. Thediagnosis is made on the basis of the con-firmed test. For example, if a patientmeetsthe diabetes criterion of the A1C (tworesults $6.5% [48 mmol/mol]) but notFPG(,126mg/dL [7.0mmol/L]), that per-son should nevertheless be considered tohave diabetes.
Since all the tests have preanalytic andanalytic variability, it is possible that anabnormal result (i.e., above the diagnosticthreshold), when repeated,will produce avalue below the diagnostic cut point. Thisscenario is likely for FPG and 2-h PG if theglucose samples remain at room temper-ature and are not centrifuged promptly.Because of the potential for preanalyticvariability, it is critical that samples forplasma glucose be spun and separatedimmediately after they are drawn. If pa-tients have test results near the marginsof thediagnostic threshold, thehealth careprofessional should follow the patientclosely and repeat the test in 3–6 months.
CATEGORIES OF INCREASED RISKFOR DIABETES (PREDIABETES)
Recommendations
c Screening for prediabetes and riskfor future diabetes with an informalassessment of risk factors or vali-dated tools should be consideredin asymptomatic adults. B
c Testing for prediabetes and risk forfuture diabetes in asymptomaticpeople should be considered inadults of any age who are over-weight or obese (BMI $25 kg/m2
Table 2.2—Criteria for the diagnosis of diabetesFPG$126 mg/dL (7.0 mmol/L). Fasting is defined as no caloric intake for at least 8 h.*
OR
2-hPG$200mg/dL (11.1mmol/L) duringOGTT. The test should be performedas described by theWHO, using a glucose load containing theequivalent of 75-g anhydrous glucosedissolved inwater.*
OR
A1C$6.5% (48 mmol/mol). The test should be performed in a laboratory using a method that isNGSP certified and standardized to the DCCT assay.*
OR
In a patient with classic symptoms of hyperglycemia or hyperglycemic crisis, a random plasmaglucose $200 mg/dL (11.1 mmol/L).
*In the absence of unequivocal hyperglycemia, results should be confirmed by repeat testing.
care.diabetesjournals.org Classification and Diagnosis of Diabetes S15

or $23 kg/m2 in Asian Americans)and who have one or more addi-tional risk factors for diabetes (Table2.3). B
c For all people, testing should beginat age 45 years. B
c If tests arenormal, repeat testing car-ried out at a minimum of 3-year in-tervals is reasonable. C
c To test forprediabetes, fastingplasmaglucose, 2-h plasma glucose during75-g oral glucose tolerance test, andA1C are equally appropriate. B
c In patients with prediabetes, identifyand, if appropriate, treat other car-diovascular disease risk factors. B
c Testing for prediabetes should beconsidered in children and adoles-cents who are overweight or obese(BMI .85th percentile for age andsex, weight for height .85th per-centile, or weight .120% of idealfor height) and who have additionalrisk factors for diabetes (Table 2.5). E
Description“Prediabetes” is the termused for individ-ualswhose glucose levels donotmeet thecriteria for diabetes but are too high to beconsidered normal (23,24). Patients withprediabetes are defined by the presenceof IFG and/or IGT and/or A1C 5.7–6.4%(39–47 mmol/mol) (Table 2.4). Prediabe-tes should not be viewed as a clinicalentity in its own right but rather as anincreased risk for diabetes and cardio-vascular disease (CVD). Criteria for testingfor diabetes or prediabetes in asymp-tomatic adults is outlined in Table 2.3.Prediabetes is associatedwithobesity (es-pecially abdominal or visceral obesity),dyslipidemia with high triglycerides and/orlow HDL cholesterol, and hypertension.
DiagnosisIFG is defined as FPG levels between100 and 125 mg/dL (between 5.6 and6.9 mmol/L) (24,25) and IGT as 2-h PGduring 75-g OGTT levels between 140 and199mg/dL (between 7.8 and 11.0mmol/L)(23). It should be noted that the WorldHealth Organization (WHO) and numerousother diabetes organizations define the IFGcutoff at 110 mg/dL (6.1 mmol/L).As with the glucose measures, several
prospective studies that used A1C topredict the progression to diabetes asdefined by A1C criteria demonstrated astrong, continuous association between A1Cand subsequent diabetes. In a systematic
review of 44,203 individuals from 16 co-hort studies with a follow-up intervalaveraging 5.6 years (range 2.8–12 years),those with A1C between 5.5 and 6.0%(between 37 and 42 mmol/mol) had asubstantially increased risk of diabetes(5-year incidence from 9 to 25%). Thosewith an A1C range of 6.0–6.5% (42–48 mmol/mol) had a 5-year risk of devel-oping diabetes between 25 and 50%and a relative risk 20 times higher com-pared with A1C of 5.0% (31 mmol/mol)(26). In a community-based study of Afri-can American and non-Hispanic whiteadults without diabetes, baseline A1Cwas a stronger predictor of subsequentdiabetes and cardiovascular eventsthan fasting glucose (27). Other analysessuggest that A1C of 5.7% (39 mmol/mol)or higher is associatedwith a diabetes risksimilar to that of the high-risk participantsin theDiabetes Prevention Program (DPP)(28), and A1C at baseline was a strongpredictor of the development of glucose-defined diabetes during the DPP and itsfollow-up (29).
Hence, it is reasonable to consider anA1Crange of 5.7–6.4% (39–47 mmol/mol) asidentifying individuals with prediabe-tes. Similar to those with IFG and/orIGT, individuals with A1C of 5.7–6.4%(39–47 mmol/mol) should be informedof their increased risk for diabetes andCVD and counseled about effectivestrategies to lower their risks (see Sec-tion 5 “Prevention or Delay of Type 2Diabetes”). Similar to glucose measure-ments, the continuum of risk is curvi-linear, so as A1C rises, the diabetes riskrises disproportionately (26). Aggressive
interventions and vigilant follow-up shouldbe pursued for those considered at veryhigh risk (e.g., those with A1C .6.0%[42 mmol/mol]).
Table 2.4 summarizes the categories ofprediabetes and Table 2.3 the criteria forprediabetes testing. The ADA diabetesrisk test is an additional option for screen-ing (Fig. 2.1) (diabetes.org/socrisktest).For additional background regarding riskfactors and screening for prediabetes, seepp. S19–S20 (SCREENING AND TESTING FOR TYPE 2
DIABETES AND PREDIABETES IN ASYMPTOMATIC ADULTS
and SCREENING AND TESTING FOR TYPE 2 DIABETES
AND PREDIABETES IN CHILDREN AND ADOLESCENTS).
TYPE 1 DIABETES
Recommendations
c Plasma blood glucose rather thanA1C should be used to diagnose theacute onset of type 1 diabetes in in-dividualswith symptomsofhypergly-cemia. E
c Screening for type 1 diabetes with apanel of autoantibodies is currentlyrecommended only in the settingof a research trial or in first-degreefamily members of a proband withtype 1 diabetes. B
c Persistence of two or more autoan-tibodies predicts clinical diabetesand may serve as an indication forintervention in the setting of a clin-ical trial. B
DiagnosisIn a patient with classic symptoms,measurement of plasma glucose is suf-ficient to diagnose diabetes (symptoms
Table 2.3—Criteria for testing for diabetes or prediabetes in asymptomatic adults
1. Testing should be considered in overweight or obese (BMI $25 kg/m2 or $23 kg/m2 in AsianAmericans) adults who have one or more of the following risk factors:c First-degree relative with diabetesc High-risk race/ethnicity (e.g., African American, Latino, Native American, Asian American, PacificIslander)
c History of CVDc Hypertension ($140/90 mmHg or on therapy for hypertension)c HDL cholesterol level,35 mg/dL (0.90 mmol/L) and/or a triglyceride level.250 mg/dL(2.82 mmol/L)
c Women with polycystic ovary syndromec Physical inactivityc Other clinical conditions associated with insulin resistance (e.g., severe obesity, acanthosisnigricans)
2. Patients with prediabetes (A1C $5.7% [39 mmol/mol], IGT, or IFG) should be tested yearly.
3. Women who were diagnosed with GDM should have lifelong testing at least every 3 years.
4. For all other patients, testing should begin at age 45 years.
5. If results are normal, testing should be repeated at a minimum of 3-year intervals, withconsideration of more frequent testing depending on initial results and risk status.
S16 Classification and Diagnosis of Diabetes Diabetes Care Volume 41, Supplement 1, January 2018

of hyperglycemia or hyperglycemic crisisplus a random plasma glucose $200 mg/dL [11.1 mmol/L]). In these cases, know-ing the plasma glucose level is critical be-cause, in addition to confirming thatsymptoms are due to diabetes, it will in-form management decisions. Some pro-viders may also want to know the A1C todetermine how long a patient has hadhyperglycemia. The criteria to diagnosediabetes are listed in Table 2.2.
Immune-Mediated DiabetesThis form, previously called “insulin-dependent diabetes” or “juvenile-onsetdiabetes,” accounts for 5–10% of diabetesand is due to cellular-mediated autoimmunedestruction of the pancreatic b-cells. Auto-immune markers include islet cell auto-antibodies and autoantibodies to GAD(GAD65), insulin, the tyrosine phospha-tases IA-2 and IA-2b, and ZnT8. Type 1diabetes is defined by the presence ofone ormore of these autoimmunemarkers.The disease has strong HLA associations,with linkage to the DQA and DQB genes.These HLA-DR/DQ alleles can be eitherpredisposing or protective.The rate of b-cell destruction is quite
variable, being rapid in some individuals(mainly infants and children) and slow inothers (mainly adults). Children and ado-lescentsmay presentwith DKA as the firstmanifestation of the disease. Others havemodest fasting hyperglycemia that canrapidly change to severe hyperglycemiaand/or DKAwith infection or other stress.Adultsmay retain sufficientb-cell functionto prevent DKA for many years; such in-dividuals eventually become dependenton insulin for survival and are at risk forDKA. At this latter stage of the disease,there is little or no insulin secretion, asmanifested by low or undetectable levelsof plasmaC-peptide. Immune-mediated di-abetes commonly occurs in childhood andadolescence, but it can occur at any age,even in the 8th and 9th decades of life.Autoimmune destruction ofb-cells has
multiple genetic predispositions and is
also related to environmental factorsthat are still poorly defined. Although pa-tients are not typically obese when theypresent with type 1 diabetes, obesityshould not preclude the diagnosis. Pa-tients with type 1 diabetes are also proneto other autoimmune disorders such asHashimoto thyroiditis, Graves disease,Addison disease, celiac disease, vitiligo,autoimmune hepatitis, myasthenia gravis,and pernicious anemia (see Section 3“Comprehensive Medical Evaluation andAssessment of Comorbidities”).
Idiopathic Type 1 DiabetesSome forms of type 1 diabetes have noknown etiologies. These patients havepermanent insulinopenia and are proneto DKA, but have no evidence of b-cellautoimmunity. Although only a minorityof patients with type 1 diabetes fall intothis category, of those who do, most areof African or Asian ancestry. Individualswith this form of diabetes suffer from ep-isodic DKA and exhibit varying degrees ofinsulin deficiency between episodes. Thisform of diabetes is strongly inherited andis not HLA associated. An absolute re-quirement for insulin replacement therapyin affected patients may be intermittent.
Testing for Type 1 Diabetes RiskThe incidence and prevalence of type 1diabetes is increasing (30). Patients withtype 1 diabetes often present with acutesymptoms of diabetes and markedlyelevated blood glucose levels, and ap-proximately one-third are diagnosedwith life-threatening DKA (2). Severalstudies indicate that measuring islet au-toantibodies in relatives of those withtype 1 diabetes may identify individualswho are at risk for developing type 1 di-abetes (5). Such testing, coupled with ed-ucation about diabetes symptoms andclose follow-up, may enable earlier iden-tificationof type 1 diabetes onset. A studyreported the risk of progression to type 1diabetes from the time of seroconversionto autoantibody positivity in three pediatric
cohorts from Finland, Germany, and theU.S. Of the 585 children who developedmore than two autoantibodies, nearly70% developed type 1 diabetes within10 years and 84% within 15 years (31).These findings are highly significant be-cause while the German group was re-cruited from offspring of parents withtype 1 diabetes, the Finnish and Americangroups were recruited from the generalpopulation. Remarkably, the findingsin all three groups were the same, sug-gesting that the same sequence of eventsled to clinical disease in both “sporadic”and familial cases of type 1 diabetes. In-deed, the risk of type 1 diabetes increasesas the number of relevant autoantibodiesdetected increases (32–34).
Although there is currently a lack ofaccepted screening programs, one shouldconsider referring relatives of those withtype 1 diabetes for antibody testing forrisk assessment in the setting of a clinicalresearch study (www.diabetestrialnet.org).Widespread clinical testing of asymp-tomatic low-risk individuals is not currentlyrecommended due to lack of approvedtherapeutic interventions. Individuals whotest positive should be counseled aboutthe risk of developing diabetes, diabetessymptoms, and DKA prevention. Numer-ous clinical studies are being conductedto test various methods of preventingtype 1 diabetes in those with evidence ofautoimmunity (www.clinicaltrials.gov).
TYPE 2 DIABETES
Recommendations
c Screening for type 2 diabetes withan informal assessment of risk fac-tors or validated tools should beconsidered in asymptomatic adults.B
c Testing for type 2 diabetes in asymp-tomatic people should be consid-ered in adults of any age who areoverweight or obese (BMI $25kg/m2 or$23 kg/m2 in Asian Amer-icans) and who have one or moreadditional risk factors for diabetes(Table 2.3). B
c For all people, testing should beginat age 45 years. B
c If tests are normal, repeat testingcarried out at a minimum of 3-yearintervals is reasonable. C
c To test for type 2 diabetes, fastingplasma glucose, 2-h plasma glucoseduring 75-g oral glucose tolerance test,and A1C are equally appropriate. B
Table 2.4—Categories of increased risk for diabetes (prediabetes)*FPG 100 mg/dL (5.6 mmol/L) to 125 mg/dL (6.9 mmol/L) (IFG)
OR
2-h PG during 75-g OGTT 140 mg/dL (7.8 mmol/L) to 199 mg/dL (11.0 mmol/L) (IGT)
OR
A1C 5.7–6.4% (39–47 mmol/mol)
*For all three tests, risk is continuous, extending below the lower limit of the range and becomingdisproportionately greater at the higher end of the range.
care.diabetesjournals.org Classification and Diagnosis of Diabetes S17
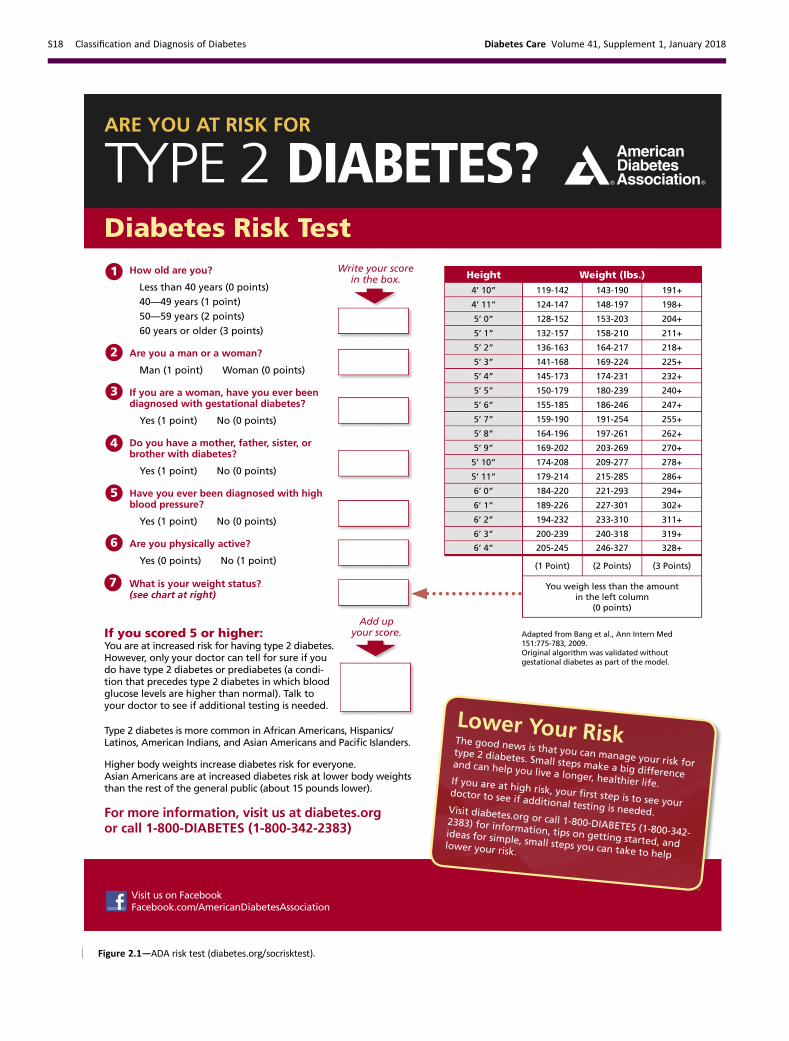
Figure 2.1—ADA risk test (diabetes.org/socrisktest).
S18 Classification and Diagnosis of Diabetes Diabetes Care Volume 41, Supplement 1, January 2018

c In patients with diabetes, identifyand treat other cardiovascular dis-ease risk factors. B
c Testing for type 2 diabetes shouldbe considered in children and ado-lescents who are overweight orobese (BMI .85th percentile forage and sex, weight for height.85thpercentile, orweight.120%of ideal for height) and who haveadditional risk factors for diabetes(Table 2.5). E
DescriptionType 2 diabetes, previously referred toas “noninsulin-dependent diabetes” or“adult-onset diabetes,” accounts for 90–95% of all diabetes. This form encom-passes individuals who have relative(rather than absolute) insulin deficiencyand have peripheral insulin resistance.At least initially, and often throughouttheir lifetime, these individuals may notneed insulin treatment to survive.There are various causes of type 2 di-
abetes. Although the specific etiologiesare not known, autoimmune destructionof b-cells does not occur and patients donot have any of the other known causesof diabetes.Most but not all patientswithtype 2 diabetes are overweight or obese.Excess weight itself causes some degreeof insulin resistance. Patients who are notobese or overweight by traditionalweightcriteria may have an increased percent-age of body fat distributed predominantlyin the abdominal region.DKA seldom occurs spontaneously in
type 2 diabetes; when seen, it usuallyarises in association with the stress of an-other illness such as infection or with theuse of certain drugs (e.g., corticosteroids,atypical antipsychotics, and sodium–
glucose cotransporter 2 inhibitors) (35,
36). Type 2 diabetes frequently goes un-diagnosed for many years because hy-perglycemia develops gradually and,at earlier stages, is often not severeenough for the patient to notice the clas-sic diabetes symptoms. Nevertheless,even undiagnosed patients are at in-creased risk of developing macrovascularand microvascular complications.
Whereas patients with type 2 diabetesmay have insulin levels that appear nor-mal or elevated, the higher blood glucoselevels in these patients would be expectedto result in even higher insulin values hadtheir b-cell function been normal. Thus,insulin secretion is defective in these pa-tients and insufficient to compensate forinsulin resistance. Insulin resistance mayimprove with weight reduction and/orpharmacologic treatment of hyperglyce-mia but is seldom restored to normal.
The risk of developing type 2 diabe-tes increases with age, obesity, and lackof physical activity. It occurs more fre-quently in women with prior GDM, inthose with hypertension or dyslipidemia,and in certain racial/ethnic subgroups(African American, American Indian,Hispanic/Latino, and Asian American). Itis often associated with a strong geneticpredisposition or family history in first-degree relatives, more so than type 1 di-abetes. However, the genetics of type 2diabetes is poorly understood. In adultswithout traditional risk factors for type 2diabetes and/or younger age, considerantibody testing to exclude the diagnosisof type 1 diabetes (i.e., GAD).
Screening and Testing for Type 2Diabetes and Prediabetes inAsymptomatic AdultsScreening for prediabetes and type 2 di-abetes through an informal assessmentof risk factors (Table 2.3) or with an
assessment tool, such as the ADA risktest (Fig. 2.1) (diabetes.org/socrisktest),is recommended to guide providers onwhether performing a diagnostic test(Table 2.2) is appropriate. Prediabetesand type 2 diabetes meet criteria for con-ditions in which early detection is appro-priate. Both conditions are common andimpose significant clinical and publichealth burdens. There is often a long pre-symptomatic phase before the diagnosisof type 2 diabetes. Simple tests to detectpreclinical disease are readily available.The duration of glycemic burden is a strongpredictor of adverse outcomes. There areeffective interventions that prevent pro-gression from prediabetes to diabetes (seeSection 5 “Prevention or Delay of Type 2Diabetes”) and reduce the risk of diabetescomplications (see Section 9 “Cardiovas-cular Disease and Risk Management” andSection 10 “Microvascular Complicationsand Foot Care”).
Approximately one-quarter of peoplewith diabetes in the U.S. and nearly halfof Asian and Hispanic Americans with di-abetes are undiagnosed (37,38). Althoughscreening of asymptomatic individuals toidentify those with prediabetes or diabe-tes might seem reasonable, rigorous clin-ical trials to prove the effectiveness ofsuch screening have not been conductedand are unlikely to occur.
A large European randomized con-trolled trial compared the impact ofscreening for diabetes and intensivemultifactorial intervention with that ofscreening and routine care (39). Generalpractice patients between the ages of40 and 69 years were screened for diabe-tes and randomly assigned by practice tointensive treatment of multiple risk fac-tors or routine diabetes care. After 5.3years of follow-up, CVD risk factors weremodestly but significantly improved withintensive treatment compared with rou-tine care, but the incidence of first CVDevents or mortality was not significantlydifferent between the groups (39). Theexcellent care provided to patients inthe routine care group and the lack ofan unscreened control arm limited theauthors’ ability to determine whetherscreening and early treatment improvedoutcomes compared with no screeningand later treatment after clinical diag-noses. Computer simulation modelingstudies suggest that major benefits arelikely to accrue from the early diagnosisand treatment of hyperglycemia and
Table 2.5—Risk-based screening for type 2 diabetes or prediabetes in asymptomaticchildren and adolescents in a clinical setting*
Criteriac Overweight (BMI.85th percentile for age and sex, weight for height .85th percentile, orweight.120% of ideal for height) A
Plus one or more additional risk factors based on the strength of their association with diabetes asindicated by evidence grades:c Maternal history of diabetes or GDM during the child’s gestation Ac Family history of type 2 diabetes in first- or second-degree relative Ac Race/ethnicity (Native American, African American, Latino, Asian American, Pacific Islander) Ac Signs of insulin resistance or conditions associated with insulin resistance (acanthosis nigricans,hypertension, dyslipidemia, polycystic ovary syndrome, or small-for-gestational-age birthweight)B
*Persons aged,18 years.
care.diabetesjournals.org Classification and Diagnosis of Diabetes S19

cardiovascular risk factors in type 2diabetes (40); moreover, screening, be-ginning at age 30 or 45 years and indepen-dent of risk factors, may be cost-effective(,$11,000 per quality-adjusted life-yeargained) (41).Additional considerations regarding
testing for type 2 diabetes and prediabe-tes in asymptomatic patients include thefollowing.
Age
Age is a major risk factor for diabetes.Testing should begin at age 45 years forall patients. Screening should be consid-ered in overweight or obese adults ofany age with one or more risk factors fordiabetes.
BMI and Ethnicity
In general, BMI$25 kg/m2 is a risk factorfor diabetes. However, data suggest thatthe BMI cut point should be lower forthe Asian American population (42,43).The BMI cut points fall consistently be-tween 23 and 24 kg/m2 (sensitivity of80%) for nearly all Asian American sub-groups (with levels slightly lower for Jap-anese Americans). This makes a roundedcut point of 23 kg/m2 practical. An argu-ment can be made to push the BMI cutpoint to lower than 23 kg/m2 in favor ofincreased sensitivity; however, this wouldlead to an unacceptably low specificity(13.1%). Data from theWHO also suggestthat a BMI of$23 kg/m2 should be usedto define increased risk in Asian Ameri-cans (44). The finding that half of diabetesin Asian Americans is undiagnosed sug-gests that testing is not occurring at lowerBMI thresholds (37,38).Evidence also suggests that other pop-
ulations may benefit from lower BMI cutpoints. For example, in a large multiethniccohort study, for an equivalent incidencerate of diabetes, a BMI of 30 kg/m2 in non-Hispanic whites was equivalent to a BMIof 26 kg/m2 in African Americans (45).
Medications
Certain medications, such as glucocorti-coids, thiazide diuretics, and atypical an-tipsychotics (46), are known to increasethe risk of diabetes and should be consid-ered when deciding whether to screen.
Testing Interval
The appropriate interval between screen-ing tests is not known (47). The rationalefor the 3-year interval is that with this in-terval, the number of false-positive teststhat require confirmatory testing will be
reduced and individuals with false-negativetestswill be retestedbefore substantial timeelapses and complications develop (47).
Community Screening
Ideally, testing should be carried outwithin a health care setting because ofthe need for follow-up and treatment.Community screening outside a healthcare setting is generally not recom-mended because people with positivetests may not seek, or have access to,appropriate follow-up testing and care.However, in specific situations where anadequate referral system is establishedbeforehand for positive tests, communityscreening may be considered. Commu-nity testing may also be poorly targeted;i.e., it may fail to reach the groupsmost atrisk and inappropriately test those at verylow risk or even those who have alreadybeen diagnosed (48).
Screening in Dental Practices
Because periodontal disease is associatedwith diabetes, the utility of screening in adental setting and referral to primary careas a means to improve the diagnosis ofprediabetes and diabetes has been ex-plored (49–51), with one study estimatingthat 30% of patients $30 years of ageseen in general dental practices had dys-glycemia (51). Further research is neededto demonstrate the feasibility, effective-ness, and cost-effectiveness of screeningin this setting.
Screening and Testing for Type 2Diabetes and Prediabetes in Childrenand AdolescentsIn the last decade, the incidenceandprev-alence of type 2 diabetes in adolescentshas increased dramatically, especially inracial and ethnic minority populations(30). See Table 2.5 for recommendationson risk-based screening for type 2 diabe-tes or prediabetes in asymptomatic chil-dren and adolescents in a clinical setting. SeeSection 12 “Children and Adolescents” foradditional information on type 2 diabetesin children and adolescents.
Some studies question the validity ofA1C in the pediatric population, especiallyamong certain ethnicities, and suggestOGTT or FPG as more suitable diagnos-tic tests (52). However, many of thesestudies do not recognize that diabetes di-agnostic criteria are based on long-termhealth outcomes, and validations are notcurrently available in the pediatric popu-lation (53). The ADA acknowledges the
limited data supporting A1C for diag-nosing type 2 diabetes in children andadolescents. Although A1C is not recom-mended for diagnosis of diabetes in chil-dren with cystic fibrosis or symptomssuggestive of acute onset of type 1 diabe-tes and only A1C assays without interfer-ence are appropriate for children withhemoglobinopathies, the ADA continuesto recommendA1C for diagnosis of type 2diabetes in this cohort (54,55).
GESTATIONAL DIABETES MELLITUS
Recommendations
c Test for undiagnosed diabetes atthe first prenatal visit in thosewith risk factors, using standard di-agnostic criteria. B
c Test for gestational diabetes melli-tus at 24–28 weeks of gestation inpregnant women not previouslyknown to have diabetes. A
c Test womenwith gestational diabe-tes mellitus for persistent diabetesat 4–12 weeks postpartum, usingthe oral glucose tolerance test andclinically appropriate nonpregnancydiagnostic criteria. E
c Women with a history of gesta-tional diabetes mellitus shouldhave lifelong screening for the de-velopment of diabetes or prediabe-tes at least every 3 years. B
c Women with a history of gesta-tional diabetes mellitus found tohave prediabetes should receive in-tensive lifestyle interventions ormetformin to prevent diabetes. A
DefinitionFor many years, GDM was defined as anydegree of glucose intolerance that wasfirst recognized during pregnancy (23), re-gardless of whether the condition mayhave predated the pregnancy or persistedafter the pregnancy. This definition facili-tated a uniform strategy for detection andclassification ofGDM, but itwas limitedbyimprecision.
The ongoing epidemic of obesity anddiabetes has led to more type 2 diabetesin women of childbearing age, with an in-crease in the number of pregnant womenwith undiagnosed type 2 diabetes (56).Because of the number of pregnantwomenwith undiagnosed type 2 diabetes,it is reasonable to test women with riskfactors for type 2 diabetes (Table 2.3) attheir initial prenatal visit, using standard
S20 Classification and Diagnosis of Diabetes Diabetes Care Volume 41, Supplement 1, January 2018

diagnostic criteria (Table 2.2). Women di-agnosed with diabetes by standard diag-nostic criteria in the first trimester shouldbe classified as having preexisting preges-tational diabetes (type 2 diabetes or, veryrarely, type 1 diabetes or monogenic dia-betes). GDM is diabetes that is first diag-nosed in the second or third trimester ofpregnancy that is not clearly either preex-isting type1or type2diabetes (see Section13 “Management of Diabetes in Preg-nancy”). The International Association ofthe Diabetes and Pregnancy Study Groups(IADPSG) GDM diagnostic criteria for the75-g OGTT as well as the GDM screeningand diagnostic criteria used in the two-step approach were not derived fromdata in the first half of pregnancy, sothe diagnosis of GDM in early pregnancyby either FPG or OGTT values is not evi-dence based (57).Because GDM confers increased risk
for the development of type 2 diabetesafter delivery (58,59) and because effec-tive prevention interventions are avail-able (60,61), women diagnosed withGDM should receive lifelong screeningfor prediabetes and type 2 diabetes.
DiagnosisGDM carries risks for the mother and ne-onate. Not all adverse outcomes are ofequal clinical importance. The Hypergly-cemia and Adverse Pregnancy Outcome(HAPO) study (62), a large-scale multina-tional cohort study completed by morethan 23,000 pregnant women, demon-strated that risk of adverse maternal, fe-tal, and neonatal outcomes continuouslyincreased as a function of maternal glyce-mia at 24–28 weeks of gestation, evenwithin ranges previously considered nor-mal for pregnancy. For most complications,there was no threshold for risk. These re-sults have led to careful reconsideration ofthe diagnostic criteria for GDM. GDM di-agnosis (Table 2.6) can be accomplishedwith either of two strategies:
1. “One-step” 75-g OGTT or
2. “Two-step” approachwith a 50-g (non-fasting) screen followed by a 100-gOGTT for those who screen positive
Different diagnostic criteria will identifydifferent degrees of maternal hypergly-cemia and maternal/fetal risk, leadingsome experts to debate, and disagree on,optimal strategies for the diagnosis ofGDM.
One-Step Strategy
The IADPSG defined diagnostic cut pointsfor GDM as the average fasting, 1-h, and2-h PG values during a 75-g OGTT inwomen at 24–28 weeks of gestationwho participated in the HAPO study atwhich odds for adverse outcomes reached1.75 times the estimated odds of theseoutcomes at the mean fasting, 1-h, and2-h PG levels of the study population.This one-step strategy was anticipated tosignificantly increase the incidence ofGDM (from 5–6% to 15–20%), primarilybecause only one abnormal value, nottwo, became sufficient to make the di-agnosis (63). The anticipated increase inthe incidence of GDM could have a sub-stantial impact on costs and medical in-frastructure needs and has the potentialto “medicalize” pregnancies previouslycategorized as normal. Nevertheless,the ADA recommends these diagnosticcriteria with the intent of optimizinggestational outcomes because these cri-teria were the only ones based on preg-nancy outcomes rather than end pointssuch as prediction of subsequent mater-nal diabetes.
The expected benefits to the offspringare inferred from intervention trials thatfocused on women with lower levels ofhyperglycemia than identified using olderGDM diagnostic criteria. Those trialsfound modest benefits including reducedrates of large-for-gestational-age birthsand preeclampsia (64,65). It is importantto note that 80–90% of women beingtreated for mild GDM in two randomizedcontrolled trials could be managed withlifestyle therapy alone. The OGTT glucosecutoffs in these two trials overlappedwith the thresholds recommended bythe IADPSG, and in one trial (65), the 2-hPG threshold (140 mg/dL [7.8 mmol/L])was lower than the cutoff recommendedby the IADPSG (153 mg/dL [8.5 mmol/L]).No randomized controlled trials of identi-fying and treating GDM using the IADPSGcriteria versus older criteria have beenpublished to date. Data are also lackingon how the treatment of lower levels ofhyperglycemia affects a mother’s futurerisk for the development of type 2 diabe-tes and her offspring’s risk for obesity,diabetes, and other metabolic disorders.Additional well-designed clinical studiesare needed to determine the optimal in-tensity of monitoring and treatment ofwomen with GDM diagnosed by theone-step strategy (66,67).
Two-Step Strategy
In 2013, the National Institutes of Health(NIH) convened a consensus develop-ment conference to consider diagnosticcriteria for diagnosing GDM (68). The15-member panel had representativesfrom obstetrics/gynecology, maternal-fetal medicine, pediatrics, diabetes re-search, biostatistics, and other relatedfields. The panel recommended a two-step approach to screening that used a1-h 50-g glucose load test (GLT) followedbya3-h100-gOGTTfor thosewhoscreenedpositive. The American College of Ob-stetricians and Gynecologists (ACOG) rec-ommends any of the commonly usedthresholds of 130, 135, or 140 mg/dL forthe 1-h 50-g GLT (69). A systematic reviewfor the U.S. Preventive Services Task Forcecompared GLT cutoffs of 130 mg/dL(7.2 mmol/L) and 140 mg/dL (7.8 mmol/L)(70). The higher cutoff yielded sensitivityof 70–88% and specificity of 69–89%,while the lower cutoff was 88–99% sensi-tive and 66–77% specific. Data regardinga cutoff of 135 mg/dL are limited. As forother screening tests, choice of a cutoffis based upon the trade-off between sen-sitivity and specificity. The use of A1C at24–28 weeks of gestation as a screeningtest for GDM does not function as well asthe GLT (71).
Key factors cited by the NIH panel intheir decision-making process were thelack of clinical trial data demonstratingthe benefits of the one-step strategyand the potential negative consequencesof identifying a large group of womenwith GDM, including medicalization ofpregnancy with increased health care uti-lization and costs. Moreover, screeningwith a 50-g GLT does not require fastingand is therefore easier to accomplish formanywomen.Treatmentofhigher-thresholdmaternal hyperglycemia, as identified by thetwo-step approach, reduces rates of neona-tal macrosomia, large-for-gestational-agebirths (72), and shoulder dystocia, withoutincreasing small-for-gestational-age births.ACOG currently supports the two-step ap-proach (69) but most recently noted thatone elevated value, as opposed to two,maybe used for the diagnosis of GDM. If thisapproach is implemented, the incidence ofGDM by the two-step strategy will likely in-creasemarkedly. ACOG recommends eitherof two sets of diagnostic thresholds for the3-h 100-g OGTT (73,74). Each is based ondifferent mathematical conversions ofthe original recommended thresholds,
care.diabetesjournals.org Classification and Diagnosis of Diabetes S21

whichusedwholebloodandnonenzymaticmethods for glucose determination. A re-cent secondary analysis of data from a ran-domized clinical trial of identification andtreatment of mild GDM (75) demon-strated that treatment was similarly ben-eficial in patients meeting only the lowerthresholds (73) and in thosemeeting onlythe higher thresholds (74). If the two-stepapproach is used, it would appear advan-tageous to use the lower diagnostic thresh-olds as shown in step 2 in Table 2.6.
Future Considerations
The conflicting recommendations fromexpert groups underscore the fact thatthere are data to support each strategy.A cost-benefit estimation comparing thetwo strategies concluded that the one-step approach is cost-effective only ifpatients with GDM receive postdeliverycounseling and care to prevent type 2 di-abetes (76). The decision of which strategyto implement must therefore be madebased on the relative values placed on fac-tors that have yet to be measured (e.g.,willingness to change practice based oncorrelation studies rather than interventiontrial results, available infrastructure, andimportance of cost considerations).As the IADPSG criteria (“one-step strat-
egy”) have been adopted internationally,further evidence has emerged to supportimproved pregnancy outcomes with costsavings (77) and may be the preferred ap-proach. Data comparing population-wide
outcomes with one-step versus two-stepapproaches have been inconsistent to date(78,79). In addition, pregnancies compli-cated by GDM per the IADPSG criteria, butnot recognized as such, have comparableoutcomes to pregnancies diagnosed asGDMby themore stringent two-step crite-ria (80,81). There remains strong consen-sus that establishing a uniform approachto diagnosing GDM will benefit patients,caregivers, and policy makers. Longer-term outcome studies are currently underway.
MONOGENIC DIABETESSYNDROMES
Recommendations
c All children diagnosed with diabe-tes in the first 6 months of lifeshould have immediate genetictesting for neonatal diabetes. A
c Children and adults, diagnosed inearly adulthood, who have diabetesnot characteristic of type 1 or type 2diabetes that occurs in successivegenerations (suggestive of an auto-somal dominant pattern of inheri-tance) should have genetic testingfor maturity-onset diabetes of theyoung. A
c In both instances, consultationwith a center specializing in diabe-tes genetics is recommended tounderstand the significance ofthese mutations and how best to
approach further evaluation, treat-ment, and genetic counseling. E
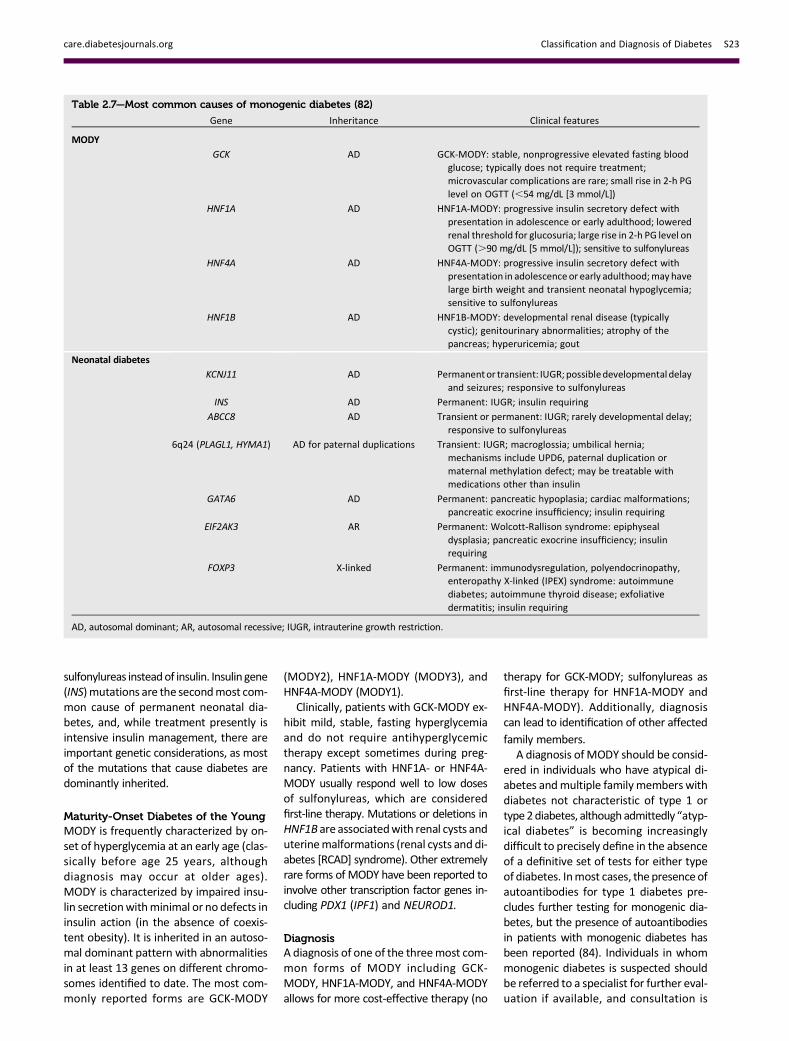
Monogenic defects that cause b-cell dys-function, such as neonatal diabetes andMODY, represent a small fraction of pa-tients with diabetes (,5%). Table 2.7describes the most common causes ofmonogenic diabetes. For a comprehen-sive list of causes, see Genetic Diagnosisof Endocrine Disorders (82).
Neonatal DiabetesDiabetes occurring under 6months of ageis termed “neonatal” or “congenital” di-abetes, and about 80–85%of cases can befound to have an underlying monogeniccause (83).Neonatal diabetes occursmuchless often after 6 months of age, whereasautoimmune type 1 diabetes rarely occursbefore 6months of age. Neonatal diabetescan either be transient or permanent. Tran-sient diabetes is most often due to over-expression of genes on chromosome 6q24,is recurrent in about half of cases, and maybe treatable with medications other thaninsulin. Permanent neonatal diabetes ismost commonly due to autosomal domi-nant mutations in the genes encoding theKir6.2 subunit (KCNJ11) and SUR1 subunit(ABCC8) of theb-cell KATP channel. Correctdiagnosis has critical implications becausemost patients with KATP-related neonataldiabetes will exhibit improved glycemiccontrol when treated with high-dose oral
Table 2.6—Screening for and diagnosis of GDMOne-step strategyPerform a 75-g OGTT, with plasma glucosemeasurementwhen patient is fasting and at 1 and 2 h, at 24–28weeks of gestation in women not previously
diagnosed with overt diabetes.The OGTT should be performed in the morning after an overnight fast of at least 8 h.The diagnosis of GDM is made when any of the following plasma glucose values are met or exceeded:
c Fasting: 92 mg/dL (5.1 mmol/L)c 1 h: 180 mg/dL (10.0 mmol/L)c 2 h: 153 mg/dL (8.5 mmol/L)
Two-step strategyStep 1: Perform a 50-g GLT (nonfasting), with plasma glucosemeasurement at 1 h, at 24–28weeks of gestation in women not previously diagnosedwith
overt diabetes.If the plasma glucose level measured 1 h after the load is$130mg/dL, 135mg/dL, or 140mg/dL (7.2 mmol/L, 7.5mmol/L, or 7.8mmol/L), proceed to a
100-g OGTT.Step 2: The 100-g OGTT should be performed when the patient is fasting.The diagnosis of GDM is made if at least two* of the following four plasma glucose levels (measured fasting and 1 h, 2 h, 3 h during OGTT) are met or
exceeded:
Carpenter-Coustan (73) or NDDG (74)
c Fasting 95 mg/dL (5.3 mmol/L) 105 mg/dL (5.8 mmol/L)c 1 h 180 mg/dL (10.0 mmol/L) 190 mg/dL (10.6 mmol/L)c 2 h 155 mg/dL (8.6 mmol/L) 165 mg/dL (9.2 mmol/L)c 3 h 140 mg/dL (7.8 mmol/L) 145 mg/dL (8.0 mmol/L)
NDDG, National Diabetes Data Group. *ACOG recently noted that alternatively one elevated value can be used for diagnosis.
S22 Classification and Diagnosis of Diabetes Diabetes Care Volume 41, Supplement 1, January 2018
sulfonylureas insteadof insulin. Insulin gene(INS)mutations are the secondmost com-mon cause of permanent neonatal dia-betes, and, while treatment presently isintensive insulin management, there areimportant genetic considerations, as mostof the mutations that cause diabetes aredominantly inherited.
Maturity-Onset Diabetes of the YoungMODY is frequently characterized by on-set of hyperglycemia at an early age (clas-sically before age 25 years, althoughdiagnosis may occur at older ages).MODY is characterized by impaired insu-lin secretionwithminimal or no defects ininsulin action (in the absence of coexis-tent obesity). It is inherited in an autoso-mal dominant pattern with abnormalitiesin at least 13 genes on different chromo-somes identified to date. The most com-monly reported forms are GCK-MODY
(MODY2), HNF1A-MODY (MODY3), andHNF4A-MODY (MODY1).
Clinically, patients with GCK-MODY ex-hibit mild, stable, fasting hyperglycemiaand do not require antihyperglycemictherapy except sometimes during preg-nancy. Patients with HNF1A- or HNF4A-MODY usually respond well to low dosesof sulfonylureas, which are consideredfirst-line therapy. Mutations or deletions inHNF1B are associatedwith renal cysts anduterinemalformations (renal cysts and di-abetes [RCAD] syndrome). Other extremelyrare forms of MODY have been reported toinvolve other transcription factor genes in-cluding PDX1 (IPF1) and NEUROD1.
DiagnosisA diagnosis of one of the threemost com-mon forms of MODY including GCK-MODY, HNF1A-MODY, and HNF4A-MODYallows for more cost-effective therapy (no
therapy for GCK-MODY; sulfonylureas asfirst-line therapy for HNF1A-MODY andHNF4A-MODY). Additionally, diagnosiscan lead to identification of other affected
family members.A diagnosis ofMODY should be consid-
ered in individuals who have atypical di-abetes andmultiple familymembers withdiabetes not characteristic of type 1 ortype2diabetes, althoughadmittedly “atyp-ical diabetes” is becoming increasinglydifficult to precisely define in the absenceof a definitive set of tests for either typeof diabetes. Inmost cases, the presenceofautoantibodies for type 1 diabetes pre-cludes further testing for monogenic dia-betes, but the presence of autoantibodiesin patients with monogenic diabetes hasbeen reported (84). Individuals in whommonogenic diabetes is suspected shouldbe referred to a specialist for further eval-uation if available, and consultation is
Table 2.7—Most common causes of monogenic diabetes (82)
Gene Inheritance Clinical features
MODY
GCK AD GCK-MODY: stable, nonprogressive elevated fasting bloodglucose; typically does not require treatment;microvascular complications are rare; small rise in 2-h PGlevel on OGTT (,54 mg/dL [3 mmol/L])
HNF1A AD HNF1A-MODY: progressive insulin secretory defect withpresentation in adolescence or early adulthood; loweredrenal threshold for glucosuria; large rise in 2-h PG level onOGTT (.90 mg/dL [5 mmol/L]); sensitive to sulfonylureas
HNF4A AD HNF4A-MODY: progressive insulin secretory defect withpresentation in adolescence or early adulthood;may havelarge birth weight and transient neonatal hypoglycemia;sensitive to sulfonylureas
HNF1B AD HNF1B-MODY: developmental renal disease (typicallycystic); genitourinary abnormalities; atrophy of thepancreas; hyperuricemia; gout
Neonatal diabetes
KCNJ11 AD Permanentor transient: IUGR; possibledevelopmentaldelayand seizures; responsive to sulfonylureas
INS AD Permanent: IUGR; insulin requiring
ABCC8 AD Transient or permanent: IUGR; rarely developmental delay;responsive to sulfonylureas
6q24 (PLAGL1, HYMA1) AD for paternal duplications Transient: IUGR; macroglossia; umbilical hernia;mechanisms include UPD6, paternal duplication ormaternal methylation defect; may be treatable withmedications other than insulin
GATA6 AD Permanent: pancreatic hypoplasia; cardiac malformations;pancreatic exocrine insufficiency; insulin requiring
EIF2AK3 AR Permanent: Wolcott-Rallison syndrome: epiphysealdysplasia; pancreatic exocrine insufficiency; insulinrequiring
FOXP3 X-linked Permanent: immunodysregulation, polyendocrinopathy,enteropathy X-linked (IPEX) syndrome: autoimmunediabetes; autoimmune thyroid disease; exfoliativedermatitis; insulin requiring
AD, autosomal dominant; AR, autosomal recessive; IUGR, intrauterine growth restriction.
care.diabetesjournals.org Classification and Diagnosis of Diabetes S23

available from several centers. Readilyavailable commercial genetic testing fol-lowing the criteria listed below nowenables a cost-effective (85), often cost-saving, genetic diagnosis that is increas-ingly supported by health insurance. Abiomarker screening pathway such as thecombination of urinary C-peptide/creatinineratio and antibody screening may aid indetermining who should get genetictesting for MODY (86). It is critical to cor-rectly diagnose one of the monogenicforms of diabetes because these pa-tients may be incorrectly diagnosedwith type 1 or type 2 diabetes, leading tosuboptimal, evenpotentially harmful, treat-ment regimens and delays in diagnosingother familymembers (87). The correct di-agnosis is especially critical for those withGCK-MODY mutations where multiplestudies have shown that no complicationsensue in the absence of glucose-loweringtherapy (88). Genetic counseling is rec-ommended to ensure that affected individ-uals understand the patterns of inheritanceand the importance of a correct diagnosis.The diagnosis of monogenic diabetes
should be considered in children andadults diagnosed with diabetes in earlyadulthood with the following findings:
○ Diabetes diagnosed within the first6 months of life (with occasional casespresenting later,mostly INS andABCC8mutations) (83,89)
○ Diabetes without typical features oftype 1 or type 2 diabetes (negative di-abetes-associated autoantibodies,nonobese, lacking othermetabolic fea-tures, especially with strong familyhistory of diabetes)
○ Stable, mild fasting hyperglycemia(100–150 mg/dL [5.5–8.5 mmol/L]),stable A1C between 5.6 and 7.6% (be-tween 38 and 60 mmol/mol), espe-cially if nonobese
CYSTIC FIBROSIS–RELATEDDIABETES
Recommendations
c Annual screening for cystic fibrosis–related diabetes with oral glucosetolerance test should begin by age10 years in all patients with cystic fi-brosis not previously diagnosed withcystic fibrosis–related diabetes. B
c A1C is not recommended as ascreening test for cystic fibrosis–related diabetes. B
c Patients with cystic fibrosis–relateddiabetes should be treated with in-sulin to attain individualized glyce-mic goals. A
c Beginning 5 years after the diagnosisof cystic fibrosis–related diabetes,annual monitoring for complicationsof diabetes is recommended. E
Cystic fibrosis–related diabetes (CFRD) isthe most common comorbidity in peoplewith cystic fibrosis, occurring in about20%of adolescents and 40–50%of adults.Diabetes in this population, comparedwith individuals with type 1 or type 2 di-abetes, is associated with worse nutri-tional status, more severe inflammatorylung disease, and greater mortality. Insu-lin insufficiency is the primary defect inCFRD.Genetically determinedb-cell func-tion and insulin resistance associatedwithinfection and inflammation may also con-tribute to the development of CFRD.Milder abnormalities of glucose toleranceare evenmore common and occur at ear-lier ages than CFRD. Whether individualswith IGT should be treated with insulinreplacement has not currently been de-termined. Although screening for diabe-tes before the age of 10 years can identifyrisk for progression to CFRD in those withabnormal glucose tolerance, no benefithas been established with respect toweight, height, BMI, or lung function.Continuous glucose monitoring or HOMAof b-cell function (90) may be more sen-sitive than OGTT to detect risk for pro-gression to CFRD; however, evidencelinking these results to long-term out-comes is lacking, and these tests are notrecommended for screening (91).
CFRD mortality has significantly de-creased over time, and the gap in mortal-ity between cystic fibrosis patients withand without diabetes has considerablynarrowed (92). There are limited clinicaltrial data on therapy for CFRD. The largeststudy compared three regimens: premealinsulin aspart, repaglinide, or oral placeboin cystic fibrosis patients with diabetes orabnormal glucose tolerance. Participantsall had weight loss in the year preced-ing treatment; however, in the insulin-treated group, this pattern was reversed,and patients gained 0.39 (6 0.21) BMIunits (P 5 0.02). The repaglinide-treatedgroup had initial weight gain, but this wasnot sustained by 6 months. The placebogroup continued to lose weight (93).
Insulin remains the most widely usedtherapy for CFRD (94).
Additional resources for the clinicalmanagement of CFRD can be found inthe position statement “Clinical CareGuidelines for Cystic Fibrosis–Related Di-abetes: A Position Statement of theAmerican Diabetes Association and a Clin-ical Practice Guideline of the Cystic Fibro-sis Foundation, Endorsed by the PediatricEndocrine Society” (95) and in the Interna-tional Society for Pediatric and Adoles-cent Diabetes’s 2014 clinical practiceconsensus guidelines (96).
POSTTRANSPLANTATIONDIABETES MELLITUS
Recommendations
c Patients should be screened afterorgan transplantation for hypergly-cemia, with a formal diagnosis ofposttransplantation diabetes melli-tus being best made once a patientis stable on an immunosuppressiveregimen and in the absence of anacute infection. E
c The oral glucose tolerance test isthe preferred test to make a diag-nosis of posttransplantation diabe-tes mellitus. B
c Immunosuppressive regimens shownto provide the best outcomes for pa-tient and graft survival should beused, irrespective of posttransplanta-tion diabetes mellitus risk. E
Several terms are used in the literature todescribe the presence of diabetes follow-ing organ transplantation. “New-onset di-abetes after transplantation” (NODAT) isone such designation that describes indi-viduals who develop new-onset diabetesfollowing transplant. NODAT excludes pa-tients with pretransplant diabetes thatwas undiagnosed as well as posttrans-plant hyperglycemia that resolves by thetime of discharge (97). Another term,“posttransplantation diabetes mellitus”(PTDM) (97,98), describes the presenceof diabetes in the posttransplant settingirrespective of the timing of diabetes onset.
Hyperglycemia is very common duringthe early posttransplant period, with;90% of kidney allograft recipients ex-hibiting hyperglycemia in the first fewweeks following transplant (97–100).In most cases, such stress- or steroid-induced hyperglycemia resolves by thetime of discharge (100,101). Although
S24 Classification and Diagnosis of Diabetes Diabetes Care Volume 41, Supplement 1, January 2018

the use of immunosuppressive therapiesis amajor contributor to the developmentof PTDM, the risks of transplant rejectionoutweigh the risks of PTDM and the roleof the diabetes care provider is to treathyperglycemia appropriately regard-less of the type of immunosuppression(97). Risk factors for PTDM include bothgeneral diabetes risks (such as age, fam-ily history of diabetes, etc.) as well astransplant-specific factors, such as useof immunosuppressant agents (102).Whereas posttransplantation hyperglyce-mia is an important risk factor for subse-quent PTDM, a formal diagnosis of PTDMis optimally made once the patient is sta-ble on maintenance immunosuppressionand in the absence of acute infection(100–102). The OGTT is considered thegold standard test for the diagnosis ofPTDM (97,98,103,104). However, screen-ing patients using fasting glucose and/orA1C can identify high-risk patients requir-ing further assessment and may reducethe number of overall OGTTs required.Few randomized controlled studies
have reported on the short- and long-term use of antihyperglycemic agents inthe setting of PTDM (102,105,106). Moststudies have reported that transplant pa-tients with hyperglycemia and PTDM af-ter transplantation have higher rates ofrejection, infection, and rehospitalization(100,102,107).Insulin therapy is the agent of choice
for the management of hyperglycemiaand diabetes in the hospital setting. Afterdischarge, patients with preexisting dia-betes could go back on their pretransplantregimen if they were in good control be-fore transplantation. Those with previ-ously poor control or with persistenthyperglycemia should continue insulinwith frequent home self-monitoring ofblood glucose to determine when insulindose reductions may be needed andwhen it may be appropriate to switch tononinsulin agents.No studies to date have established
which noninsulin agents are safest ormost efficacious in PTDM. The choice ofagent is usually made based on the sideeffect profile of the medication and pos-sible interactions with the patient’s im-munosuppression regimen (102). Drugdose adjustments may be required be-cause of decreases in the glomerularfiltration rate, a relatively common com-plication in transplant patients. A smallshort-term pilot study reported that
metformin was safe to use in renal trans-plant recipients (108), but its safety hasnot been determined in other types oforgan transplant. Thiazolidinedioneshave been used successfully in patientswith liver and kidney transplants, butside effects include fluid retention, heartfailure, and osteopenia (109,110). Dipep-tidyl peptidase 4 inhibitors donot interactwith immunosuppressant drugs and havedemonstrated safety in small clinical trials(111,112). Well-designed intervention tri-als examining the efficacy and safety ofthese and other antihyperglycemic agentsin patients with PTDM are needed.
References1. American Diabetes Association. Diagnosis andclassification of diabetes mellitus. Diabetes Care2014;37(Suppl. 1):S81–S902. Dabelea D, Rewers A, Stafford JM, et al.;SEARCH for Diabetes in Youth Study Group. Trendsin the prevalence of ketoacidosis at diabetes diag-nosis: the SEARCH for Diabetes in Youth Study.Pediatrics 2014;133:e938–e9453. Newton CA, Raskin P. Diabetic ketoacidosis intype 1 and type 2 diabetes mellitus: clinical andbiochemical differences. Arch Intern Med 2004;164:1925–19314. Skyler JS, Bakris GL, Bonifacio E, et al. Differen-tiation of diabetes by pathophysiology, natural his-tory, and prognosis. Diabetes 2017;66:241–2555. Insel RA, Dunne JL, Atkinson MA, et al. Stagingpresymptomatic type 1 diabetes: a scientificstatement of JDRF, the Endocrine Society, andthe American Diabetes Association. DiabetesCare 2015;38:1964–19746. International Expert Committee. InternationalExpert Committee report on the role of the A1Cassay in the diagnosis of diabetes. Diabetes Care2009;32:1327–13347. Knowler WC, Barrett-Connor E, Fowler SE,et al.; Diabetes Prevention Program ResearchGroup. Reduction in the incidence of type 2 di-abetes with lifestyle intervention or metformin.N Engl J Med 2002;346:393–4038. Tuomilehto J, Lindstrom J, Eriksson JG, et al.;FinnishDiabetes Prevention StudyGroup. Preven-tion of type 2 diabetes mellitus by changes inlifestyle among subjects with impaired glucosetolerance. N Engl J Med 2001;344:1343–13509. Cowie CC, Rust KF, Byrd-Holt DD, et al. Preva-lence of diabetes and high risk for diabetes usingA1C criteria in the U.S. population in 1988–2006.Diabetes Care 2010;33:562–56810. Nowicka P, Santoro N, Liu H, et al. Utility ofhemoglobin A1c for diagnosing prediabetes anddiabetes in obese children and adolescents. Dia-betes Care 2011;34:1306–131111. LacyME,Wellenius GA, Sumner AE, Correa A,CarnethonMR, Liem RI, et al. Association of sicklecell trait with hemoglobin A1c in African Ameri-cans. JAMA 2017;317:507–51512. Wheeler E, Leong A, Liu C-T, et al.; EPIC-CVDConsortium; EPIC-InterAct Consortium; LifelinesCohort Study. Impact of common genetic deter-minantsof hemoglobinA1con type 2diabetes riskand diagnosis in ancestrally diverse populations: a
transethnic genome-wide meta-analysis. PLoSMed 2017;14:e100238313. Ziemer DC, Kolm P, Weintraub WS, et al.Glucose-independent, black-white differences inhemoglobin A1c levels: a cross-sectional analysisof 2 studies. Ann Intern Med 2010;152:770–77714. Kumar PR, Bhansali A, RavikiranM, et al. Util-ity of glycated hemoglobin in diagnosing type 2diabetes mellitus: a community-based study.J Clin Endocrinol Metab 2010;95:2832–283515. HermanWH.Are there clinical implications ofracial differences in HbA1c? Yes, to not considercan do great harm! Diabetes Care 2016;39:1458–146116. HermanWH, Ma Y, Uwaifo G, et al.; DiabetesPrevention Program Research Group. Differencesin A1C by race and ethnicity among patients withimpaired glucose tolerance in the Diabetes Pre-vention Program. Diabetes Care 2007;30:2453–245717. Bergenstal RM, Gal RL, Connor CG, et al.; T1DExchange Racial Differences Study Group. Racialdifferences in the relationship of glucose concen-trations and hemoglobin A1c levels. Ann InternMed 2017;167:95–10218. Selvin E, Steffes MW, Ballantyne CM,Hoogeveen RC, Coresh J, Brancati FL. Racial differ-ences in glycemic markers: a cross-sectional anal-ysis of community-based data. Ann Intern Med2011;154:303–30919. Herman WH, Dungan KM, WolffenbuttelBHR, et al. Racial and ethnic differences in meanplasma glucose, hemoglobin A1c, and 1,5-anhydroglucitol in over 2000 patients withtype 2 diabetes. J Clin Endocrinol Metab 2009;94:1689–169420. Selvin E, Rawlings AM, Bergenstal RM, CoreshJ, Brancati FL. No racial differences in the associ-ation of glycated hemoglobin with kidney diseaseand cardiovascular outcomes. Diabetes Care2013;36:2995–300121. Selvin E. Are there clinical implications of ra-cial differences in HbA1c? A difference, to be adifference, must make a difference. DiabetesCare 2016;39:1462–146722. Welsh KJ, Kirkman MS, Sacks DB. Role of gly-cated proteins in the diagnosis and managementof diabetes: research gaps and future directions.Diabetes Care 2016;39:1299–130623. Expert Committee on the Diagnosis and Clas-sification of Diabetes Mellitus. Report of theExpert Committee on the Diagnosis and Classifi-cation of Diabetes Mellitus. Diabetes Care 1997;20:1183–119724. Genuth S, Alberti KG, Bennett P, et al.; ExpertCommittee on the Diagnosis and Classification ofDiabetes Mellitus. Follow-up report on the diag-nosis of diabetesmellitus. Diabetes Care 2003;26:3160–316725. American Diabetes Association. Diagnosisand classification of diabetes mellitus. DiabetesCare 2011;34(Suppl. 1):S62–S6926. Zhang X, Gregg EW,Williamson DF, et al. A1Clevel and future risk of diabetes: a systematic re-view. Diabetes Care 2010;33:1665–167327. Selvin E, Steffes MW, Zhu H, et al. Glycatedhemoglobin, diabetes, and cardiovascular risk innondiabetic adults. N Engl J Med 2010;362:800–81128. Ackermann RT, Cheng YJ, Williamson DF,Gregg EW. Identifying adults at high risk for diabe-tes and cardiovascular disease using hemoglobin
care.diabetesjournals.org Classification and Diagnosis of Diabetes S25

A1c National Health and Nutrition ExaminationSurvey 2005-2006. Am J PrevMed 2011;40:11–1729. Diabetes Prevention Program ResearchGroup. HbA1c as a predictor of diabetes and asan outcome in the Diabetes Prevention Program:a randomized clinical trial. Diabetes Care 2015;38:51–5830. Dabelea D, Mayer-Davis EJ, Saydah S, et al.;SEARCH for Diabetes in Youth Study. Prevalenceof type 1 and type 2 diabetes among children andadolescents from 2001 to 2009. JAMA 2014;311:1778–178631. Ziegler AG, Rewers M, Simell O, et al. Sero-conversion to multiple islet autoantibodies andrisk of progression to diabetes in children. JAMA2013;309:2473–247932. Sosenko JM, Skyler JS, Palmer JP, et al.; Type 1Diabetes TrialNet Study Group; Diabetes Preven-tion Trial-Type 1 Study Group. The prediction oftype 1 diabetes by multiple autoantibody levelsand their incorporation into an autoantibody riskscore in relatives of type 1 diabetic patients. Di-abetes Care 2013;36:2615–262033. Steck AK, Vehik K, Bonifacio E, et al.; TEDDYStudy Group. Predictors of progression from theappearance of islet autoantibodies to early child-hood diabetes: The Environmental Determinantsof Diabetes in the Young (TEDDY). Diabetes Care2015;38:808–81334. Orban T, Sosenko JM, Cuthbertson D, et al.;Diabetes Prevention Trial-Type 1 Study Group.Pancreatic islet autoantibodies as predictors oftype 1 diabetes in the Diabetes Prevention Trial–Type 1. Diabetes Care 2009;32:2269–227435. Umpierrez G, Korytkowski M. Diabeticemergencies - ketoacidosis, hyperglycaemic hy-perosmolar state and hypoglycaemia. Nat Rev Endo-crinol 2016;12:222–23236. Fadini GP, Bonora BM, Avogaro A. SGLT2 in-hibitors and diabetic ketoacidosis: data from theFDA Adverse Event Reporting System. Diabetolo-gia 2017;60:1385–138937. Menke A, Casagrande S, Geiss L, Cowie CC.Prevalence of and trends in diabetes amongadults in the United States, 1988-2012. JAMA2015;314:1021–102938. Centers for Disease Control and Prevention.National diabetes statistics report: estimates ofdiabetes and its burden in the United States,2017 [Internet]. Available from https://www.cdc.gov/diabetes/data/statistics/statistics-report.html. Accessed 22 September 201739. Griffin SJ, Borch-Johnsen K, Davies MJ, et al.Effect of early intensive multifactorial therapy on5-year cardiovascular outcomes in individuals withtype 2 diabetes detected by screening (ADDITION-Europe): a cluster-randomised trial. Lancet 2011;378:156–16740. Herman WH, Ye W, Griffin SJ, et al. Early de-tection and treatment of type 2 diabetes reducecardiovascular morbidity and mortality: a simu-lation of the results of the Anglo-Danish-DutchStudy of Intensive Treatment in People withScreen-Detected Diabetes in Primary Care(ADDITION-Europe). Diabetes Care 2015;38:1449–145541. Kahn R, Alperin P, Eddy D, et al. Age at initi-ation and frequency of screening to detect type 2diabetes: a cost-effectiveness analysis. Lancet2010;375:1365–137442. Araneta MRG, Kanaya A, Fujimoto W, et al.Optimum BMI cut-points to screen Asian
Americans for type 2 diabetes: The UCSD FilipinoHealth Study and the North Kohala Study [Ab-stract]. Diabetes 2014;63(Suppl. 1):A2043. Hsu WC, Araneta MRG, Kanaya AM, ChiangJL, Fujimoto W. BMI cut points to identify at-riskAsian Americans for type 2 diabetes screening.Diabetes Care 2015;38:150–15844. WHOExpert Consultation. Appropriate body-mass index for Asian populations and its implica-tions for policy and intervention strategies. Lancet2004;363:157–16345. Chiu M, Austin PC, Manuel DG, Shah BR, TuJV. Deriving ethnic-specific BMI cutoff points forassessing diabetes risk. Diabetes Care 2011;34:1741–174846. Erickson SC, Le L, Zakharyan A, et al. New-onset treatment-dependent diabetes mellitusand hyperlipidemia associated with atypical anti-psychotic use in older adults without schizophre-nia or bipolar disorder. J Am Geriatr Soc 2012;60:474–47947. Johnson SL, Tabaei BP, Herman WH. The ef-ficacy and cost of alternative strategies for sys-tematic screening for type 2 diabetes in the U.S.population 45–74 years of age. Diabetes Care2005;28:307–31148. Tabaei BP, Burke R, Constance A, et al.Community-based screening for diabetes inMichigan. Diabetes Care 2003;26:668–67049. Lalla E, Kunzel C, Burkett S, Cheng B, LamsterIB. Identification of unrecognized diabetes andpre-diabetes in a dental setting. J Dent Res2011;90:855–86050. Lalla E, Cheng B, Kunzel C, Burkett S, LamsterIB. Dental findings and identification of undiag-nosed hyperglycemia. J Dent Res 2013;92:888–89251. HermanWH, Taylor GW, Jacobson JJ, Burke R,Brown MB. Screening for prediabetes and type 2diabetes in dental offices. J Public Health Dent2015;75:175–18252. Buse JB, Kaufman FR, Linder B, Hirst K, ElGhormli L,Willi S; HEALTHY Study Group. Diabetesscreening with hemoglobin A1c versus fastingplasma glucose in a multiethnicmiddle-school co-hort. Diabetes Care 2013;36:429–43553. Kapadia C, Zeitler P; Drugs and TherapeuticsCommitteeof the Pediatric Endocrine Society. He-moglobin A1c measurement for the diagnosis oftype 2 diabetes in children. Int J Pediatr Endocri-nol 2012;2012:3154. Kester LM, Hey H, Hannon TS. Using hemo-globin A1c for prediabetes and diabetes diagnosisin adolescents: can adult recommendations beupheld for pediatric use? J Adolesc Health 2012;50:321–32355. Wu E-L, Kazzi NG, Lee JM. Cost-effectivenessof screening strategies for identifying pediatric di-abetes mellitus and dysglycemia. JAMA Pediatr2013;167:32–3956. Lawrence JM, Contreras R, ChenW, Sacks DA.Trends in the prevalence of preexisting diabe-tes and gestational diabetes mellitus among aracially/ethnically diverse population of pregnantwomen, 1999–2005. Diabetes Care 2008;31:899–90457. McIntyre HD, Sacks DA, Barbour LA, et al. Is-sues with the diagnosis and classification of hy-perglycemia in early pregnancy. Diabetes Care2016;39:53–5458. NoctorE, CroweC, CarmodyLA, et al.; ATLANTIC-DIP investigators. Abnormal glucose tolerance
post-gestational diabetes mellitus as defined bythe International Association of Diabetes andPregnancy Study Groups criteria. Eur J Endocrinol2016;175:287–29759. Kim C, Newton KM, Knopp RH. Gestationaldiabetes and the incidence of type 2 diabetes: asystematic review. Diabetes Care 2002;25:1862–186860. Ratner RE, Christophi CA, Metzger BE, et al.;Diabetes Prevention Program Research Group.Prevention of diabetes in women with a historyof gestational diabetes: effects of metformin andlifestyle interventions. J Clin Endocrinol Metab2008;93:4774–477961. Aroda VR, Christophi CA, Edelstein SL, et al.;Diabetes Prevention Program Research Group.The effect of lifestyle intervention andmetforminon preventing or delaying diabetes amongwomen with and without gestational diabetes:the Diabetes Prevention Program OutcomesStudy 10-year follow-up. J Clin Endocrinol Metab2015;100:1646–165362. Metzger BE, Lowe LP, Dyer AR, et al.; HAPOStudy Cooperative Research Group. Hyperglycemiaand adverse pregnancy outcomes. N Engl J Med2008;358:1991–200263. SacksDA,HaddenDR,MareshM, et al.; HAPOStudy Cooperative Research Group. Frequency ofgestational diabetesmellitus at collaborating centersbased on IADPSG consensus panel-recommendedcriteria: the Hyperglycemia and Adverse PregnancyOutcome (HAPO) Study. Diabetes Care 2012;35:526–52864. Landon MB, Spong CY, Thom E, et al.; EuniceKennedy Shriver National Institute of Child Healthand Human Development Maternal-Fetal Medi-cine Units Network. A multicenter, randomizedtrial of treatment for mild gestational diabetes.N Engl J Med 2009;361:1339–134865. Crowther CA, Hiller JE, Moss JR, McPhee AJ,Jeffries WS, Robinson JS; Australian CarbohydrateIntolerance Study in Pregnant Women (ACHOIS)Trial Group. Effect of treatment of gestational di-abetes mellitus on pregnancy outcomes. N Engl JMed 2005;352:2477–248666. Tam WH, Ma RCW, Ozaki R, et al. In uteroexposure to maternal hyperglycemia increaseschildhood cardiometabolic risk in offspring. Dia-betes Care 2017;40:679–68667. Landon MB, RiceMM, Varner MW, et al.; Eu-nice Kennedy Shriver National Institute of ChildHealth and Human Development Maternal-FetalMedicine Units (MFMU) Network. Mild gesta-tional diabetes mellitus and long-term childhealth. Diabetes Care 2015;38:445–45268. Vandorsten JP, Dodson WC, Espeland MA,et al. NIH consensus development conference: di-agnosing gestational diabetes mellitus. NIH Con-sens State Sci Statements 2013;29:1–3169. CommitteeonPracticeBulletinsdObstetrics.Practice Bulletin No. 180: gestational diabetesmellitus. Obstet Gynecol 2017;130:e17–e3770. Donovan L, Hartling L, Muise M, Guthrie A,Vandermeer B, Dryden DM. Screening tests forgestational diabetes: a systematic review for theU.S. Preventive Services Task Force. Ann InternMed 2013;159:115–12271. Khalafallah A, Phuah E, Al-Barazan AM, et al.Glycosylated haemoglobin for screening and di-agnosis of gestational diabetes mellitus. BMJOpen 2016;6:e011059
S26 Classification and Diagnosis of Diabetes Diabetes Care Volume 41, Supplement 1, January 2018

72. Horvath K, Koch K, Jeitler K, et al. Effects oftreatment in women with gestational diabetesmellitus: systematic review and meta-analysis.BMJ 2010;340:c139573. Carpenter MW, Coustan DR. Criteria forscreening tests for gestational diabetes. Am JObstetGynecol 1982;144:768–77374. National Diabetes Data Group. Classificationand diagnosis of diabetes mellitus and other cat-egories of glucose intolerance. Diabetes 1979;28:1039–105775. Harper LM, Mele L, Landon MB, et al.; EuniceKennedy Shriver National Institute of Child HealthandHumanDevelopment (NICHD)Maternal-FetalMedicine Units (MFMU) Network. Carpenter-Coustan compared with National Diabetes DataGroup criteria for diagnosing gestational diabetes.Obstet Gynecol 2016;127:893–89876. Werner EF, Pettker CM, Zuckerwise L, et al.Screening for gestational diabetes mellitus: arethe criteria proposed by the International Associ-ation of theDiabetes andPregnancy StudyGroupscost-effective? Diabetes Care 2012;35:529–53577. DuranA, Saenz S, TorrejonMJ, et al. Introduc-tion of IADPSG criteria for the screening and di-agnosis of gestational diabetes mellitus results inimprovedpregnancyoutcomes at a lower cost in alarge cohort of pregnant women: the St. CarlosGestational Diabetes Study. Diabetes Care 2014;37:2442–245078. Wei Y, Yang H, Zhu W, et al. InternationalAssociation of Diabetes and Pregnancy StudyGroup criteria is suitable for gestational diabetesmellitus diagnosis: further evidence from China.Chin Med J (Engl) 2014;127:3553–355679. FeldmanRK, TieuRS, Yasumura L. Gestationaldiabetes screening: the International Associationof theDiabetes and Pregnancy StudyGroups com-pared with Carpenter-Coustan screening. ObstetGynecol 2016;127:10–1780. Ethridge JK Jr, Catalano PM, Waters TP. Peri-natal outcomes associated with the diagnosis ofgestational diabetes made by the InternationalAssociation of the Diabetes and Pregnancy StudyGroups criteria. Obstet Gynecol 2014;124:571–57881. Mayo K, Melamed N, Vandenberghe H,Berger H. The impact of adoption of the Interna-tional Association of Diabetes in Pregnancy StudyGroup criteria for the screening and diagnosis ofgestational diabetes. Am J Obstet Gynecol 2015;212:224.e1–224.e982. Carmody D, Støy J, Greeley SA, Bell GI,Philipson LH. A clinical guide tomonogenic diabe-tes. In Genetic Diagnosis of Endocrine Disorders.2nd ed.Weiss RE, Refetoff S, Eds. Philadelphia, PA,Elsevier, 201683. De Franco E, Flanagan SE, Houghton JAL, et al.The effect of early, comprehensive genomic test-ing on clinical care in neonatal diabetes: an inter-national cohort study. Lancet 2015;386:957–96384. Urbanova J, Rypackova B, Prochazkova Z,et al. Positivity for islet cell autoantibodies in pa-tients withmonogenic diabetes is associated with
later diabetes onset and higher HbA1c level. Dia-bet Med 2014;31:466–47185. Naylor RN, John PM, Winn AN, et al. Cost-effectiveness ofMODYgenetic testing: translatinggenomic advances into practical health applica-tions. Diabetes Care 2014;37:202–20986. Shields BM, Shepherd M, Hudson M, et al.;UNITED study team. Population-based assess-ment of a biomarker-based screening pathwayto aid diagnosis of monogenic diabetes in young-onset patients. Diabetes Care 2017;40:1017–102587. Hattersley A, Bruining J, Shield J, Njolstad P,Donaghue KC. The diagnosis and management ofmonogenic diabetes in children and adolescents.Pediatr Diabetes 2009;10(Suppl. 12):33–4288. Rubio-Cabezas O, Hattersley AT, Njølstad PR,et al.; International Society for Pediatric and Adoles-cent Diabetes. ISPAD Clinical Practice ConsensusGuidelines 2014. The diagnosis and managementof monogenic diabetes in children and adolescents.Pediatr Diabetes 2014;15(Suppl. 20):47–6489. Greeley SAW,Naylor RN, Philipson LH, Bell GI.Neonatal diabetes: an expanding list of genes al-lows for improved diagnosis and treatment. CurrDiab Rep 2011;11:519–53290. Mainguy C, Bellon G, Delaup V, et al. Sensi-tivity and specificity of different methods for cys-tic fibrosis-related diabetes screening: is the oralglucose tolerance test still the standard? J PediatrEndocrinol Metab 2017;30:27–3591. Ode KL, Moran A. New insights into cysticfibrosis-related diabetes in children. Lancet Dia-betes Endocrinol 2013;1:52–5892. Moran A, Dunitz J, Nathan B, Saeed A, HolmeB, ThomasW.Cystic fibrosis-related diabetes: cur-rent trends in prevalence, incidence, and mortal-ity. Diabetes Care 2009;32:1626–163193. Moran A, Pekow P, Grover P, et al.; CysticFibrosis Related Diabetes Therapy Study Group.Insulin therapy to improve BMI in cystic fibrosis-related diabetes without fasting hyperglycemia:results of the Cystic Fibrosis Related DiabetesTherapy Trial. Diabetes Care 2009;32:1783–178894. Onady GM, Stolfi A. Insulin and oral agentsfor managing cystic fibrosis-related diabetes. Co-chrane Database Syst Rev 2016;4:CD00473095. Moran A, Brunzell C, Cohen RC, et al.; CFRDGuidelines Committee. Clinical care guidelines forcystic fibrosis-related diabetes: a position state-ment of the American Diabetes Association and aclinical practice guideline of the Cystic FibrosisFoundation, endorsed by the Pediatric EndocrineSociety. Diabetes Care 2010;33:2697–270896. Moran A, Pillay K, Becker DJ, Acerini CL; In-ternational Society for Pediatric and AdolescentDiabetes. ISPAD Clinical Practice ConsensusGuidelines 2014. Management of cystic fibrosis-related diabetes in children and adolescents. Pe-diatr Diabetes 2014;15(Suppl. 20):65–7697. Sharif A, Hecking M, de Vries APJ, et al. Pro-ceedings from an international consensus meet-ing on posttransplantation diabetes mellitus:
recommendations and future directions. Am JTransplant 2014;14:1992–200098. Hecking M, Werzowa J, Haidinger M, et al.Novel views on new-onset diabetes after trans-plantation: development, prevention and treat-ment. Nephrol Dial Transplant 2013;28:550–56699. Ramirez SC, Maaske J, Kim Y, et al. The asso-ciation between glycemic control and clinical out-comes after kidney transplantation. Endocr Pract2014;20:894–900100. ThomasMC, Moran J, Mathew TH, Russ GR,Rao MM. Early peri-operative hyperglycaemiaand renal allograft rejection in patients withoutdiabetes. BMC Nephrol 2000;1:1101. Chakkera HA,Weil EJ, Castro J, et al. Hypergly-cemiaduring the immediateperiodafter kidney trans-plantation. Clin J Am Soc Nephrol 2009;4:853–859102. Wallia A, Illuri V, Molitch ME. Diabetes careafter transplant: definitions, risk factors, and clin-ical management. Med Clin North Am 2016;100:535–550103. Sharif A, Moore RH, Baboolal K. The use oforal glucose tolerance tests to risk stratify fornew-onset diabetes after transplantation: anunderdiagnosed phenomenon. Transplantation2006;82:1667–1672104. Hecking M, Kainz A, Werzowa J, et al. Glu-cose metabolism after renal transplantation. Di-abetes Care 2013;36:2763–2771105. Galindo RJ, Fried M, Breen T, Tamler R. Hy-perglycemia management in patients with post-transplantation diabetes. Endocr Pract 2016;22:454–465106. Jenssen T, Hartmann A. Emerging treat-ments for post-transplantation diabetes mellitus.Nat Rev Nephrol 2015;11:465–477107. ThomasMC,MathewTH, Russ GR, RaoMM,Moran J. Early peri-operative glycaemic controland allograft rejection in patients with diabetesmellitus: a pilot study. Transplantation 2001;72:1321–1324108. Kurian B, Joshi R, Helmuth A. Effectivenessand long-term safety of thiazolidinediones andmetformin in renal transplant recipients. EndocrPract 2008;14:979–984109. Budde K, Neumayer H-H, Fritsche L,Sulowicz W, Stompor T, Eckland D. The pharma-cokinetics of pioglitazone in patients with im-paired renal function. Br J Clin Pharmacol 2003;55:368–374110. Luther P, Baldwin D Jr. Pioglitazone in themanagement of diabetesmellitus after transplan-tation. Am J Transplant 2004;4:2135–2138111. StrømHalden TA, Asberg A, Vik K, HartmannA, Jenssen T. Short-term efficacy and safety ofsitagliptin treatment in long-term stable renal re-cipients with new-onset diabetes after transplan-tation. Nephrol Dial Transplant 2014;29:926–933112. Lane JT, Odegaard DE, Haire CE, Collier DS,Wrenshall LE, Stevens RB. Sitagliptin therapy inkidney transplant recipients with new-onset dia-betes after transplantation. Transplantation2011;92:e56–e57
care.diabetesjournals.org Classification and Diagnosis of Diabetes S27





























