Embed Size (px)
Citation preview

144 Oman Journal of Ophthalmology, Vol. 7, No. 3, 2014
Correspondence:Dr. Vivek B. Wani, P O. Box 17672, Khaldiya, PC Code 72457, Kuwait. E-mail: [email protected]
Copyright: © 2014 Wani V, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
We report a case of submacular cysticercosis in the left eye of an Indian patient living in Kuwait. Though he was systemically asymptomatic, his magnetic resonance imaging showed multiple cysts in the brain. The patient underwent pars plana vitrectomy (PPV), and the cyst was removed in total through a retinotomy over the cyst. He had another small cyst in the periphery that was also removed. He was treated with oral albendazole and systemic steroids after the surgery to treat his neurocysticercosis. He developed rhegmatogenous retinal detachment after the surgery, and the retina was successfully reattached with scleral
buckling and PPV procedure. His final best corrected visual acuity improved from counting fingers at 1/2 m at presentation to 20/400. This case report shows that the ocular cysticercosis may be seen among expatriates working in the Middle East. It is important to rule out the presence of neurocysticercosis in such patients as well as multiple cysts in the affected eye. However, the functional outcome of surgical treatment of submacular cysticercosis can be disappointing.
Keywords: Ocular cysticercosis, pars plana vitrectomy, submacular
Introduction
Human cysticercosis is caused by the larval form of the tapeworm, Taenia solium. Ocular involvement is common in endemic areas, and its presence in the subretinal space has been reported.[1] However, its presence in the submacular area is rare, and treatment of submacular cysticercosis can be difficult.[2] Pars plana vitrectomy (PPV) offers a safe method of approach to submacular cysticercosis, but the visual results can still be disappointing.[3,4] We are reporting a case of submacular cysticercosis in a young Indian male working in Kuwait who was successfully treated by a vitreoretinal procedure.
Case Report
A 24-year-old Indian male patient presented with a history of
diminished vision in the left eye of 20 days duration in January
2010. He had no other ocular or systemic complaints.
The best corrected visual acuity (BCVA) was counting fingers
at 1/3 m in the left eye. The left eye showed few small keratic
precipitates with no cells in the anterior chamber (AC). The fundus
examination of the left eye showed oval subretinal translucent
cystic lesion of three disc diameters at the posterior pole with
its nasal edge under the fovea [Figure 1] and a white dense
lesion near surface in the center. The cyst showed undulating
movements upon throwing light on the lesion. The right eye
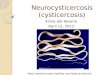
was normal. Optical coherence tomography (OCT) examination
by using Stratus OCT (Carl Zeiss Meditec, Dublin, CA, USA)
showed the presence of well-demarcated cyst wall on the vitreal
side with scolex attached to the wall of the cyst on the vitreal
side [Figure 2]. His physical, blood count and stool examinations
were normal. However, magnetic resonance imaging (MRI) of the
brain showed nearly 50 small cysts spread in cerebral cortex, basal
ganglia, midbrain, thalamus, and cerebellum.
A case of submacular cysticercosis treated by pars plana vitrectomy in Kuwait
Vivek B. Wani1,2, Niranjan Kumar1, Anil K. Uboweja2, Mahmood A. Kazem2
1Departments of Ophthalmology, Al Bahar Ophthalmology Centre, 2Al Adan Hospital, Kuwait City, Al Adan, Kuwait
Case Report
Access this article onlineQuick Response Code:
Website: www.ojoonline.org
DOI: 10.4103/0974-620X.142599
[Downloaded free from http://www.ojoonline.org on Wednesday, January 07, 2015, IP: 41.235.88.16] || Click here to download free Android application for this journal

Wani, et al.: A case of submacular cysticercosis in Kuwait
Oman Journal of Ophthalmology, Vol. 7, No. 3, 2014 145
drugs can enhance the inflammation and lead to loss of vision in the affected eye.[8]
Our patient showed few keratic precipitates with no reaction in the AC or vitreous. Wender et al. reported AC inflammation in 7 of the 22 cases and mild to severe vitritis in all the 22 cases they reported.[9] They observed that the degree of inflammation in the eye depended upon time interval between onset of symptoms and intactness of the cyst.[9] The inflammation in our case might have been mild as
Figure 1: Preoperative photograph of left eye fundus. Vertical arrow: Probable site of entry of the cysticercosis from the choroid showing retinal pigment epithelial disturbance. Horizontal arrow: Shows area of serous retinal detachment
Figure 2: Optical coherence tomography of the cyst with the larva
Figure 3: Postoperative photograph 1-year later
The patient underwent three port 20G PPV in which, after removal of the posterior hyaloid, a small retinotomy was created by endocautery in the superotemporal area and the cyst was extracted in whole by engaging it with a flute needle. Another small cyst of <1 DD was seen superiorly, at 12 o’clock meridian near the ora, which was removed with the vitrectomy cutter. At the end of the vitrectomy, fluid-air exchange, endolaser and injection of perfluoropropane gas (C
3F
8) 14% were performed. He received
antiparasitic treatment with steroids for neurocysticercosis as advised by the neurophysician. The histopathology examination of the cyst confirmed the diagnosis of cysticercosis.
Two months after surgery, he developed localized superonasal retinal detachment due to two tears in the periphery, which was successfully treated with scleral buckling with PPV with endolaser and sulfur hexafluoride (SF
6) 20% injection. One year after surgery,
the BCVA in the left eye had improved to 20/400. The retina was attached in the left eye, but the macular area showed atrophic changes [Figure 3] and he was free of any systemic illness.
Discussion
Human beings are definitive hosts for T. solium and pigs are the intermediate hosts. Humans get the infection when they ingest undercooked pork meat containing the cysts. The larvae in the cysts attach to the human gut and develop into adult tapeworms that shed proglottids containing tapeworm eggs into the human feces. The feces may contaminate the food source of the pigs and eggs ingested by the pigs develop into larvae that pierce the intestinal wall and enter the blood stream and end up in various tissues including the muscles where they develop into cysts. However, the human cysticercosis infection occurs when, humans ingest eggs of T. solium. This could be due to contamination of food by food handlers, who are harboring adult T. solium or auto ingestion of eggs due to poor hygienic practice or contamination of food due to use of human waste or contaminated water to grow vegetables and fruits. When humans ingest the eggs of T. solium, the eggs develop into larvae which pierce the gut and enter the blood stream and enter various tissues where they develop into cysts producing the clinical syndrome of cysticercosis. As pigs are not reared in Middle East, it is extremely rare to see systemic or ocular cysticercosis in this region and hence there are only few reports about ocular and systemic cysticercosis from the Middle East.[5-7] All the cases reported from the region, are among expatriate patients from India or other endemic countries.[5-7] Cysticercosis can occur in those who have never eaten pork and even in vegetarians, as the infection occurs due to consumption of food or water contaminated with fecal matter.[4] Our patient was free from any neurological symptoms, but his MRI showed presence of neurocysticercosis. Neurocysticercosis can be coexisting in up to 24% of the cases.[4] Hence, it is important to perform MRI examination to rule out neurocysticercosis. However, the subretinal cysticercosis should be surgically removed first and then start the antiparasitic treatment for neurocysticercosis. Otherwise, death of the larva in the eye due to antiparasitic
[Downloaded free from http://www.ojoonline.org on Wednesday, January 07, 2015, IP: 41.235.88.16] || Click here to download free Android application for this journal

Wani, et al.: A case of submacular cysticercosis in Kuwait
146 Oman Journal of Ophthalmology, Vol. 7, No. 3, 2014
the patient presented early due to the decreased vision caused by submacular cysticercosis. Wender et al. do not mention about the presence of any submacular cysticercosis in their case series.[9
The OCT examination of our patient showed a clearly demarcated hypereflective cyst wall on the vitreal side with the scolex protruding in the cyst producing a comet shaped reflection. These OCT findings have been well-described by Sinha et al.[10]
Visual results after removal of the cysticercosis from the vitreous and subretinal location other than the macula are satisfactory.[4,11,12] The removal of the submacular cyst by external route with an opening in the sclera and choroid at the site of the cyst can be disastrous, as the area is difficult to reach.[2] Hence, its removal by vitrectomy offers the best chances of some visual recovery. However the visual acuity after its successful removal by vitrectomy can still be disappointing.[3,4] Sharma et al. reported five cases of submacular cysticercosis, and none of them achieved postoperative vision of better than 20/400.[4] We speculate that it could be due to damage to the foveal photoreceptors caused by the toxins released by the cyst in the submacular space.
In summary, we are reporting a case of submacular cysticercosis successfully treated by PPV in Kuwait. The patient had another smaller cyst in the periphery in the same eye. The patient was found to have subclinical neurocysticercosis by radiological examination.
References
1. Cardenas F, Quiroz H, Plancarte A, Meza A, Dalma A, Flisser A. Taenia solium ocular cysticercosis: Findings in 30 cases. Ann Ophthalmol 1992;24:25-8.
2. Bartholowmew RS. Subretinal cysticercosis. Am J Ophthalmol 1975;79:670-3.
3. Lerdvitayasakul R, Lawtiantong T. Removal of submacular cysticercosis: A case report. J Med Assoc Thai 1991;74:675-8.
4. Sharma T, Sinha S, Shah N, Gopal L, Shanmugam MP, Bhende P, et al. Intraocular cysticercosis: Clinical characteristics and visual outcome after vitreoretinal surgery. Ophthalmology 2003;110:996-1004.
5. Sabti K, Chow D, Wani V, Al-Ajmi M. Resolution of bilateral multifocal subretinal cysticercosis without signifi cant infl ammatory sequelae. Can J Ophthalmol 2001;36:214-7.
6. Hira PR, Francis I, Abdella NA, Gupta R, Ai-Ali FM, Grover S, et al. Cysticercosis: Imported and autochthonous infections in Kuwait. Trans R Soc Trop Med Hyg 2004;98:233-9.
7. Al Shahrani D, Frayha HH, Dabbagh O, Al Shail E. First case of neurocysticercosis in Saudi Arabia. J Trop Pediatr 2003;49:58-60.
8. Sundar U, Chawla V, Lakkas Y, Shrivastava M, Asole D, Vaidy M. Monocular blindness during therapy for cerebral neurocysticercosis. J Assoc Physicians India 2010;58:570-2.
9. Wender JD, Rathinam SR, Shaw RE, Cunningham ET Jr. Intraocular cysticercosis: Case series and comprehensive review of the literature. Ocul Immunol Infl amm. 2011;19:240-5.
10. Sinha S, Takkar B, Venkatesh P, Khanduja S. High-resolution Fourier-domain optical coherence tomography fi ndings in subretinal cysticercosis. Retina 2012;32:643-4.
11. Natarajan S, Malpani A, Kumar Nirmalan P, Dutta B. Management of intraocular cysticercosis. Graefes Arch Clin Exp Ophthalmol 1999;237:812-4.
12. Luger MH, Stilma JS, Ringens PJ, van Baarlen J. In-toto removal of a subretinal cysticercus cellulosae by pars plana vitrectomy. Br J Ophthalmol 1991;75:561-3.
Cite this article as: Wani VB, Kumar N, Uboweja AK, Kazem MA. A case of submacular cysticercosis treated by pars plana vitrectomy in Kuwait. Oman J Ophthalmol 2014;7:144-6.
Source of Support: Nil, Confl ict of Interest: None declared.
[Downloaded free from http://www.ojoonline.org on Wednesday, January 07, 2015, IP: 41.235.88.16] || Click here to download free Android application for this journal