Embed Size (px)
Citation preview

A Novel Radiographic Index for theDiagnosis of Posterior AcromioclavicularJoint Dislocations
Alex Vaisman,*yz MD, Ignacio Eduardo Villalon Montenegro,y MD,Marıa Jesus Tuca De Diego,y MD, and Juanjose Valderrama Ronco,y MDInvestigation performed at Clınica Alemana de Santiago de Chile, Santiago, Chile
Background: Posterior acromioclavicular (AC) joint dislocations are frequently misclassified because posterior translation of theclavicle is difficult to evaluate in Zanca radiograph views. A novel radiographic index was used in this study to accurately diagnoseposterior dislocations of the AC joint.
Hypothesis: This novel index has a high degree of accuracy for the diagnosis of posterior AC joint dislocations.
Study Design: Cohort study (diagnosis); Level of evidence, 2.
Methods: This was an analytic, descriptive study of 150 patients with different grades of AC injuries according to the Rockwoodclassification (30 patients for each grade of injury: I, II, III, IV, and V). The diagnosis of an AC injury was made both clinically andradiographically by using comparative Zanca and axillary views. Two measurements were performed in Zanca views: the cora-coclavicular distance and the AC width distance. A width index was calculated for each patient. The Student t test, Bonferronitest, logistic regression, linear regression, and receiver operating characteristic (ROC) curves were used for statistical analysis.Forty cases were impartially selected to obtain a k concordance value.
Results: The average value of the AC width index per group (according to the Rockwood classification) was as follows: type I,2.1% (range, –12% to 25%); type II, 4.2% (range, –19% to 29%); type III, 19.1% (range, –59% to 91%); type IV, 110.3% (range,47% to 181%); and type V, –3.8% (range, –71% to 62%). There was a significant difference between the average width index inthe patients with type IV injuries and those in the remaining groups (P \ .05). The ROC curve showed that a width index of 60%has a sensitivity of 95.7% and specificity of 97.5%, with a positive predictive value of 96.7% and negative predictive value of95.6% to predict a type IV injury. Intraobserver reliability was rated as substantial agreement for each of 3 observers; the inter-observer reliability of the 3 independent raters was almost perfect.
Conclusion: An AC width index of �60% is highly accurate for the diagnosis of a posterior AC joint dislocation, with high intra-observer and interobserver concordance.
Keywords: acromioclavicular joint dislocation; shoulder; radiographic index; radiograph; sport-specific injuries; instability;diagnosis
Acromioclavicular (AC) lesions represent 40% to 50% of ath-letic shoulder injuries.12,17 To properly assess this injury,a 3-grade injury classification, based on the radiographicfindings in comparative AC joints of the same patient, was
first introduced in the 1960s by Tossy et al19 and Allman.2
Later, with the recognition that many AC joint instabilitieswere not properly assessed by this classification, Rockwoodet al15 introduced a modification, classifying these injuriesas types I to VI: type I, AC ligament sprain with the AC jointcongruence intact; type II, disruption of the AC ligamentswith sprains of the coracoclavicular ligaments; type III,AC and coracoclavicular ligament tears with the coracocla-vicular distance increased between 25% and 100% morethan in the normal shoulder; type IV, complete dislocationwith posterior displacement of the distal clavicle into orthrough the trapezius muscle; type V, increase of the cora-coclavicular distance from 100% to 300% as comparedwith the normal shoulder, including disruption of the delto-trapezius fascia; and type VI, complete dislocation with infe-rior displacement of the distal clavicle into a subacromial orsubcoracoid position.15
*Address correspondence to Alex Vaisman, MD, Facultad de Medic-ina Clınica Alemana Universidad del Desarrollo, Francisco Bulnes Correa3737, dep B-31, Las Condes, Santiago, Chile (e-mail: [email protected]).
yOrthopaedic Surgery Department, Clınica Alemana de Santiago deChile, Santiago, Chile.
zOrthopaedic Surgery, Faculty of Medicine, Clınica Alemana Universi-dad del Desarrollo, Santiago, Chile.
The authors declared that they have no conflicts of interest in theauthorship and publication of this contribution.
The American Journal of Sports Medicine, Vol. 42, No. 1DOI: 10.1177/0363546513506849� 2013 The Author(s)
112

Historically, the diagnosis of AC joint injuries has reliedupon radiographic evaluations, which include the anteropos-terior Zanca view with a 10� to 15� cephalic tilt of the x-ray,and an axillary view, which helps to reveal any posterior dis-placement of the distal clavicle.5-7,9,20 For most of the cases,the diagnosis is properly made, and adequate treatmentcan be advocated. However, Rockwood type IV AC joint dislo-cations can frequently be misdiagnosed.10,11 This is related tothe lack of standardization for axillary views, with no clearpublished recommendations regarding the position of thepatient when the radiograph is taken and no objective meas-urements to define the pathological lesion. Moreover,patients with an acute AC joint injury may suffer discomfortwhile being positioned for this view, which can alter the cor-rect position of the cassette and result in a poor-quality radio-graph.7 All of these factors can cause a misclassification ofthese injuries. Erroneous categorization of AC joint disloca-tions may lead to inadequate management of the lesionwith subsequent poor functional results for the patient.
Because of this diagnostic variability among observers,some authors have proposed the use of computed tomogra-phy, magnetic resonance imaging (MRI), or even dynamicor stress radiograph projections of the AC joint, insteadof plain radiographs, to certify the degree and directionof the clavicle’s displacement and the stabilizing ligaments’status.1,3,4,12,13,16,18 In spite of this, plain radiographs con-tinue to be the initial, most useful test for these injuriesbecause of their wide availability and low cost.3,4,16 Asa result of our experience, a widening of the AC joint’s clearspace in comparative Zanca views has been systematicallynoticed in posterior AC joint dislocations. Although oftendiscussed among surgeons, to our knowledge, this phenom-enon has never been mentioned in the literature. The pur-pose of this study was to introduce and to validate a novelradiographic index, in plain bilateral Zanca views, for theaccurate diagnosis of posterior AC joint dislocations.
MATERIALS AND METHODS
An analytic, descriptive study in 150 patients with differ-ent types of AC joint injuries, according to the Rockwoodclassification (30 patients for each type of injury: I, II,III, IV, and V), was performed at the authors’ institutionsbetween 2004 and 2011. The data were collected retrospec-tively. The inclusion criteria were adult patients (aged �18years) with a recent unilateral AC traumatic event whoarrived at the emergency room and underwent completeand standardized radiographic assessments. Patientswith a degenerative disease of the AC joint or associatedacromion, coracoid, or clavicle fractures, or a previous ACjoint surgery were excluded from this study.
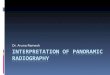
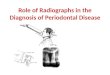
The diagnosis of an AC injury was made both clinicallyand radiographically by using comparative Zanca and ipsilat-eral axillary views. For the bilateral Zanca view, each patientwas standing upright at a distance of 1 to 1.2 m from the x-ray tube, with his or her back against a hard surface to keepa straight position of the spine and shoulders (Figure 1). Forthe axillary view, the patient was in the sitting position, andthe affected shoulder was abducted as close to 90� as possibleuntil pain was felt, with the x-ray tube located at
approximately 0� to 20� of lateral inclination depending onthe abduction achieved by the patient (Figure 2).
The coracoclavicular distance in both shoulders was digi-tally measured (Synapse Enterprise, FUJIFILM MedicalSystems USA Inc, Stamford, Connecticut) in the anteroposte-rior view, as advocated by Rockwood, and registered for eachpatient (Figure 3). In the same view, we measured the newAC width index: to obtain this index, the observer has tomark the upper most lateral aspect of the clavicle and theupper most medial aspect of the acromion in both shoulders(Figure 4A). A straight vertical line is then drawn from these2 marks, parallel between each other, and the distancebetween them is measured in each shoulder, determiningthe AC width (Figure 4B). The width index is then calculatedby the following formula:
ðWidth of Injured Side�Width of Normal SideÞWidth of Normal Side
3100%:
This index was calculated for each patient. The presence orabsence of posterior displacement of the clavicle was also
Figure 1. Position in which bilateral Zanca views were taken.
Figure 2. Position in which axillary view was taken.
Vol. 42, No. 1, 2014 Novel Index for Type IV Acromioclavicular Injuries 113

assessed in the axillary view (Figure 5). Type IV and Vinjuries were treated surgically, and the diagnosis wasreconfirmed intraoperatively.
To validate the intraobserver and interobserver agree-ment of this new index, we impartially selected 40 caseswith Rockwood classifications type I (n = 3), type II (n =3), type III (n = 8), type IV (n = 20), and type V (n = 6).Three independent observers, who were blinded to patientdata, were trained to use the width index. The observersincluded a first-year orthopaedic surgery resident(observer 1), a general orthopaedic surgeon with 3 yearsin practice (observer 2), and a shoulder surgeon withmore than 5 years of experience (observer 3). Eachobserver classified the cases according to the Rockwoodclassification but complemented the ‘‘classic’’ coracoclavic-ular measurement with this new diagnostic tool. Measure-ments were performed on printed radiographs with thesame graded ruler on 2 separate days separated by 1week and the observers registered their classification ofthe injuries on both occasions. A blinded researcherchanged the order of appearance but kept the same casesfor the second evaluation.
Statistical Analysis
Descriptive statistics with paired and unpaired t tests andthe Bonferroni test were used to analyze the overall data.To validate the classification of groups in relation to themagnitude of the width index, we used a logistic regressionand linear regression model. The accuracy of the widthindex was evaluated using receiver operating characteris-tic (ROC) curve analysis. A P value \.05 was consideredstatistically significant.
For all statistical analyses, plain variable descriptionsof Rockwood types I to V and the percentage values ofthe width index were used. To validate this new index,the k index of agreement for intraobserver and interob-server reliability was used. All analyses were performedwith the data analysis and statistical software StataV11.0 (StataCorp LP, College Station, Texas).
The institutional review board approved the study.However, because of the nature of our study in which theclinical data were anonymous and the radiographs andsurgical procedures for each case were indicated for medi-cal purposes, with no investigation intervention whatso-ever, no informed consent was collected for this study.
Figure 3. Bilateral Zanca radiographic views of 2 patientswith a left acromioclavicular (AC) joint injury. The arrowshighlight the coracoclavicular distance in both shoulders.(A) A left type III AC injury. (B) A left type IV AC injury.Although the elevation of the clavicle is similar in both cases,note the increased width of the left AC space in B, which istypical of posterior AC joint dislocations.
Figure 4. Bilateral Zanca radiographic views of a patientwith a left acromioclavicular (AC) joint injury. (A) Two marksare drawn on each side. (B) Parallel lines are drawn fromthese 2 points and the distance betweeen them is mea-sured, determining the AC width distance. The width indexwas then calculated by the following formula: ([width ofinjured side – width of normal side]/width of normal side)3 100%.
Figure 5. Axillary radiograph illustrating the normal radiolog-ical relation between the distal clavicle and the acromion (A)and a posterior acromioclavicular joint dislocation (B,arrows).
114 Vaisman et al The American Journal of Sports Medicine

RESULTS
The AC width index for each group is expressed in Table 1.All of the groups were validated with logistic regression(P \ .05 in each group). The width index for type IV lesions(posterior AC joint dislocations) was significantly higherwhen compared with the other types of injury by using lin-ear regression (P \ .05).
Accuracy of the Index
The ROC curve (Figure 6) showed that a width index of60% has a sensitivity of 95.7% and a specificity of 97.5%and a positive predictive value of 96.7% and a negative pre-dictive value of 95.6% for the diagnosis of a type IV ACjoint dislocation.
Intraobserver and Interobserver Reliability
The intraobserver reliability was rated as substantialagreement for each of the 3 observers (k values = .68[observers 1 and 2], .64 [observer 3]). The interobserverreliability of the 3 independent raters for the width indexwas almost perfect, with a k value of .82.
DISCUSSION
The key factor to properly approach an AC joint injury isits adequate classification. If an injury is misclassified,incorrect treatment will be advocated, with poor final func-tional results.8,14 One of the most common problems whenclassifying an AC joint injury is that posterior dislocationsmay be inconsistently detected on plain radiographs.18
Multiple factors can be related to this phenomenon andcould be divided into 2 groups: first, problems related tothe radiographic technique, and second, problems relatedto the interpretation of the images.
Problems related to the radiograph technique includeimproper positioning of the patient or the cassette, whichmay be caused by great patient discomfort while takingthese views in the acute setting. Problems related to theinterpretation of the radiographs include the lack of anobjective definition of AC joint displacement in the axillaryviews; frequent anatomic variations between patients orwithin the same individual patient, which may considerably
influence the radiological relations between the distal clav-icle and the acromion; and a poor concordance betweenobservers.
Some authors agree that a plain radiographic assess-ment of an AC joint dislocation is too limited, proposingthe use of stress or dynamic radiograph views. Regardingthis issue, Alexander1 described a modified stress lateralview to demonstrate the displacement of the clavicle thatoccurs when true ligament disruption is present. Withthe patient sitting or standing, the shoulders are thrustforward at the time when the radiograph is taken. In casesof AC ligament disruption, the distal clavicle is superiorlydisplaced and overlaps the acromion. Even with this spe-cial lateral stress view, the problems of drooping of theshoulder and subsequent anteroinferior rotation of thescapula and patient discomfort in the acute setting haveto be considered. Moreover, the original publicationdescribed just 3 cases, and there is no statistical validationof this technique.
On the other hand, Tauber et al18 proposed a supine,dynamic axillary lateral shoulder view with the arm in90� of abduction and 60� of flexion and extension to detecthorizontal instability of the distal clavicle in patients withacute AC joint dislocations. The researchers describeda new angle defined as the glenoacromioclavicular angle(GACA), which is measured in the axillary view with theshoulder in 2 different positions. A GACA difference of12.3� is associated with a sensitivity of 93% and a specific-ity of 92% for the diagnosis of posterior AC joint instability.However, the GACA is measured in the axillary view,which is often poorly standardized. Moreover, to obtainthe different views, the patient has to move the abductedinjured shoulder into different positions, which will bepainful in the acute setting, and more views imply moreirradiation for the patient and a higher cost. In our study,using only 1 bilateral Zanca view, we found that witha width index of �60%, we could recognize a posterior dis-location of the AC joint with a sensitivity of 95.7% and
TABLE 1Average Width Index for
Each Type of AC Joint Dislocationa
Type of AC Joint Injury Average Width Index, %
I 2.1 (–12 to 25)II 4.2 (–19 to 29)III 19.1 (–59 to 91)IV 110.3 (47 to 181)V –3.8 (–71 to 62)
aInjury categorized according to the Rockwood classification.AC, acromioclavicular.
Figure 6. Receiver operating characteristic (ROC) curveshowing a high sensitivity and specificity when the widthindex is at least 60%.
Vol. 42, No. 1, 2014 Novel Index for Type IV Acromioclavicular Injuries 115

a specificity of 97.5%. The widening observed in type IVinjuries could be explained by the fact that posterior dis-placement of the clavicle generates a ‘‘shortening’’ of theclavicle in anteroposterior views, increasing the distancebetween the lateral aspect of the clavicle and the medialaspect of the acromion when compared with the uninjuredside, but this is only a theory. However, this index is easilymeasured in plain Zanca views, with high intraobserverand interobserver concordances, and does not require thepatient to adopt difficult or painful positions. Furthermore,with this novel index, the axillary view could be obviated,bearing in mind that the very uncommon coracoid fracture,usually recognized in this view, could be misdiagnosed.
There are other radiographic stress views for AC jointinjuries utilizing weights with wrist straps, but apartfrom adding discomfort to the patient the real utility ofthis radiographic technique has been questioned in the lit-erature.17 To improve the diagnostic accuracy of AC jointdislocations some authors13 have proposed that MRIshould be routinely performed. Nemec et al13 reporteda 52.2% correlation between radiographs and MRI afterevaluating 40 patients with type I to IV AC jointdislocations.
Although MRI can accurately show both osseous andsoft tissues involved with an AC joint and directly detectligament injuries, it is well known that it may also overes-timate these lesions, inducing other types of error in thediagnosis. Additional drawbacks of routinely taken MRIscans are the elevated cost and the limited availability ofthis examination.
Computed tomography can aid in the proper diagnosisof acute AC joint injuries. Nevertheless, if we considerthat, at the present time, its accuracy has not been wellvalidated in the literature and that it can expose patientsto a high dose of radiation when compared with simpleradiographs, we cannot recommend its routine use in theclinical setting as a first-line diagnostic tool.
To our knowledge, plain radiographs are still consideredto be the most common diagnostic method defined in theliterature. However, one major drawback of any diagnosticstudy of AC joint injuries is defining the ‘‘true positive’’type IV injury. Our study is not the exception. We usedplain radiographs and intraoperative findings as ourmethod of confirming the proper diagnoses of type IV andV injuries, but we are aware that there is a chance thatwe might have missed ‘‘true’’ type IV injuries in the nonop-erative group. Interestingly, we found a higher interob-server agreement than an intraobserver agreement,which means that the observers made the same misdiagno-ses, agreeing even when being wrong. A high interobserveragreement, however, suggests a high reliability of thisindex.
The AC joint width index is a novel tool that can comple-ment the classic measurements used in the Rockwood clas-sification of AC joint injuries. It is simple to use, with lowdiscomfort, low cost, and minimum irradiation for thepatient. Its high accuracy and intraobserver and
interobserver concordance may help to identify patientswho need surgical treatment by indirectly detecting poste-rior AC joint dislocations independent of the grade of ver-tical displacement of the distal clavicle in the coronalplane. Further prospective clinical studies are needed todemonstrate this issue.
REFERENCES
1. Alexander OM. Dislocation of the acromioclavicular joint. Radiogra-
phy. 1949;15(179):260.
2. Allman FL Jr. Fractures and ligamentous injuries of the clavicle and its
articulation. J Bone Joint Surg Am. 1967;49:774-784.
3. Alyas F, Curtis M, Speed C, Saifuddin A, Connell D. MR imaging
appearances of acromioclavicular joint dislocation. Radiographics.
2008;28:463-479.
4. Antonio GE, Cho JH, Chung CB, Trudell DJ, Resnick D. Pictorial
essay: MR imaging appearance and classification of acromioclavicu-
lar joint injury. AJR Am J Roentgenol. 2003;180:1103-1110.
5. Cox JS. The fate of the acromioclavicular joint in athletic injuries. Am
J Sports Med. 1981;9(1):50-53.
6. Dawson PA, Adamson GJ, Pink MM, et al. Relative contribution of acro-
mioclavicular joint capsule and coracoclavicular ligaments to acromio-
clavicular stability. J Shoulder Elbow Surg. 2009;18(2):237-244.
7. Ernberg LA, Potter HG. Radiographic evaluation of the acromioclavic-
ular and sternoclavicular joints. Clin Sports Med. 2003;22(2):255-275.
8. Galpin RD, Hawkins RJ, Grainger RW. A comparative analysis of
operative versus nonoperative treatment of grade III acromioclavicu-
lar separations. Clin Orthop Relat Res. 1985;193:150-155.
9. Hegedus EJ, Goode A, Campbell S, et al. Physical examination tests
of the shoulder: a systematic review with meta-analysis of individual
tests. Br J Sports Med. 2008;42:80-92.
10. Mazzocca AD, Arciero RA, Bicos J. Evaluation and treatment of acro-
mioclavicular joint injuries. Am J Sports Med. 2007;35:316-329.
11. McFarland EG, Blivin SJ, Doehring CB, Curl LA, Silberstein C. Treat-
ment of grade III acromioclavicular separations in professional throw-
ing athletes: results of a survey. Am J Orthop. 1997;11:771-774.
12. Melenevsky Y, Yablon CM, Ramappa A, Hochman MG. Clavicle and
acromioclavicular joint injuries: a review of imaging, treatment, and
complications. Skeletal Radiol. 2011;40:831-842.
13. Nemec U, Oberleitner G, Nemec SF, et al. MRI versus radiography of
acromioclavicular joint dislocation. AJR Am J Roentgenol.
2011;197(4):968-973.
14. Rios CG, Arciero RA, Mazzocca AD. Anatomy of the clavicle and cor-
acoid process for reconstruction of the coracoclavicular ligaments.
Am J Sports Med. 2007;35:811-817.
15. Rockwood CA, Williams GR, Youg DC. Disorders of the acromiocla-
vicular joint. In: Rockwood CA, Masten FA II, eds. The Shoulder. Phil-
adelphia: Saunders; 1998:483-553.
16. Schaefer FK, Schaefer PJ, Brossmann J, Hilgert RE, Heller M,
Jahnke T. Experimental and clinical evaluation of acromioclavicular
joint structures with new scan orientations in MRI. Eur Radiol.
2006;16:1488-1493.
17. Simovitch R, Sanders B, Ozbaydar M, Lavery K, Warner JJ. Acromio-
clavicular joint injuries: diagnosis and management. J Am Acad
Orthop Surg. 2009;17:207-219.
18. Tauber M, Koller H, Hitzl W, Resch H. Dynamic radiologic evaluation
of horizontal instability in acute acromioclavicular joint dislocation.
Am J Sports Med. 2010;38:1188-1195.
19. Tossy JD, Mead NC, Sigmond HM. Acromioclavicular separations:
useful and practical classification for treatment. Clin Orthop Relat
Res. 1963;28:111-119.
20. Walton J, Mahajan S, Paxinos A, et al. Diagnostic values of tests for
acromioclavicular joint pain. J Bone Joint Surg Am. 2004;86:807-812.
For reprints and permission queries, please visit SAGE’s Web site at http://www.sagepub.com/journalsPermissions.nav
116 Vaisman et al The American Journal of Sports Medicine