Embed Size (px)
Citation preview

A PILOT STUDY OF THE SIMULTANEOUS USE OF DERMAL FILLER FOR RESTORATION OF DEFICIENT
PAPILLAE AND ENAMEL MATRIX DERIVATIVE FOR ROOT COVERAGE IN CONJUNCTION WITH MINIMALLY
INVASIVE SURGERY: PATIENT REPORTED OUTCOMES
by
Stephen Julius Spano
A thesis submitted in conformity with the requirements for the degree of Master of Science Periodontology
Faculty of Dentistry University of Toronto
© Copyright by Stephen Julius Spano 2018
ii
A PILOT STUDY OF THE SIMULTANEOUS USE OF DERMAL FILLER FOR RESTORATION OF DEFICIENT
PAPILLAE AND ENAMEL MATRIX DERIVATIVE FOR ROOT COVERAGE IN CONJUNCTION WITH MINIMALLY
INVASIVE SURGERY: PATIENT REPORTED OUTCOMES
Stephen Julius Spano
Master of Science Periodontology
Faculty of Dentistry University of Toronto
2018
Abstract
Gingival recession, including interdental papilla loss, is considered by most patients as
aesthetically unpleasant. Yet, in most instances, no treatment is available. Our aim was to
develop a minimally invasive and predictable approach to treat papilla deficiencies and gingival
recession. We hypothesized that, following the formation of a subperiosteal space, dermal filler
administration into deficient papillae and a coronally advanced flap with enamel matrix
derivative application to exposed roots will provide significant improvements in patient
satisfaction with papillary fill and root coverage. Six months following treatment there was a
significant increase in patient-satisfaction regarding improvement of gingival deficiencies shown
by a mean increase in visual analogue scale (VAS) measurements of 68.3% (p<0.01; CI=52.11-
84.51). Mean root coverage and papilla fill were 60.4%±43.3% and 1.3mm±0.7mm, respectively.
This novel surgical technique demonstrates successful restoration of deficient interdental papillae
with or without gingival recession and perhaps more importantly, a dramatic improvement in
different patient-based-outcomes.
iii
Acknowledgments
Without the continued and unconditional support of my family, I would not be here today. Mom
and Dad thank you for your countless sacrifices. You have played a significant role in my
personal accomplishments in life. Thank you to my older brothers, Frank and Vincent, who I
look up to and strive to emulate as they have had to endure an even longer educational journey as
medical doctors. Lastly, thank you to my sister Valerie who, I can proudly say, has also chosen a
path in dentistry, following in my footsteps.
I would like to thank my mentor and supervisor Dr. Howard Tenenbaum. Dr. Tenenbaum first
approached me about this clinical research study during my Hospital Dental Residency at Mount
Sinai Hospital. We made an immediate connection and worked diligently together towards
developing this novel surgical technique. He has provided unwavering guidance throughout my
early career in periodontology, and I feel very privileged to have had this opportunity to work
with him. I can only hope to continue such a fruitful relationship in the future. His passion for
knowledge and advancement in dental research is remarkable. I must also recognize Dr.
Christopher McCulloch who initially piloted my interest in dental research and paved the way for
me pursuing a career in Periodontology and eventually meeting Dr. Tenenbaum. When I first
started dental school, he gave me an opportunity to work in dental research in the field of
periodontology. He was there guiding me through my first publications and many presentations
and helped me mature into a research clinician. Thank you Dr. McCulloch. I would also like to
extend an appreciation to my advisory committee members Dr. Michael Goldberg, Dr. Romanita
Ghilzon and Dr. David Lam. Furthermore, my clinical director, Dr. Jim Lai, has always been
available for support and advice.
I would also like to thank my senior co-residents Dr. Siavash Hassanpour, Dr. Adam Ohayon and
Dr. Hendrik Doering. They have guided me through my three years and provided much needed
comic relief during such a rigorous program. Notably, Dr. Siavash Hassanpour has provided me
with additional support through his distinguished research career and strong educational
background. I can’t wait to join all of them upon my graduation as a professional colleague in
such a respectable healthcare field.
Thank you, everyone!
iv
Table of Contents Acknowledgments ......................................................................................................................... iii Table of Contents ........................................................................................................................... iv
List of Tables .................................................................................................................................. v List of Figures ................................................................................................................................ vi
List of Appendices ........................................................................................................................ vii Abbreviations ............................................................................................................................... viii
Chapter 1: Introduction ................................................................................................................... 1 Chapter 2: Literature Review .......................................................................................................... 2
2.1 The Interdental Papilla .......................................................................................................... 2 2.2 Classification Systems for Papilla Defects and Gingival Recession .................................... 4 2.3 Treatment of Gingival Recession ......................................................................................... 6 2.4 Dermal Fillers and the Treatment of Papillary Defects ........................................................ 8 Statement of the Problem .............................................................................................................. 14
Chapter 3: Materials and Methods ................................................................................................ 16 3.1 Human Subjects .................................................................................................................. 16
3.2 Inclusion and Exclusion Criteria ......................................................................................... 16 3.3 Materials ............................................................................................................................. 17 3.4 Examination and Surgical Protocol .................................................................................... 17 3.5 Post-Surgical Assessments and Data Collection ................................................................. 20 3.6 Statistical Analysis .............................................................................................................. 21
Chapter 4: Results ......................................................................................................................... 22
4.1 Subjective Outcomes/Patient- and Clinician-Based ........................................................... 22 4.2 Clinical Measurements ........................................................................................................ 23
Chapter 5: Discussion ................................................................................................................... 24 Conclusion and Future Directions ................................................................................................ 31
Tables and Figures ........................................................................................................................ 32 Appendices ................................................................................................................................... 45
Appendix A: Medical Questionnaire ........................................................................................ 45 Appendix B: Consent Meeting Script/Interview Guide ............................................................ 47 Appendix C: Information Letter for Research Participants ...................................................... 51 Appendix D: Eligibility Screening Consent Form .................................................................... 55 Appendix E: Treatment Consent Form ..................................................................................... 57 Appendix F: Postoperative Instructions .................................................................................... 59 Appendix G: Case Report Form ............................................................................................... 60
Contributions to the Thesis Manuscript ........................................................................................ 74 References ..................................................................................................................................... 75
v
List of Tables
Table 1: Primary VAS scores at baseline, six weeks and six months following treatment.
Table 2: Secondary VAS scores one-two weeks following treatment.
Table 3: Secondary VAS scores one-two weeks following treatment, in comparison to other
periodontal surgeries.
Table 4: Secondary VAS scores six weeks after treatment.
Table 5: Secondary VAS scores six months after treatment.
Table 6: VAS scores by periodontists and periodontal residents following photographic
evaluation of treatment outcomes.
Table 7: Papilla fill at baseline, six weeks after treatment and six months after treatment.
Table 8: Root coverage at initial examination and six months after treatment.

vi
List of Figures
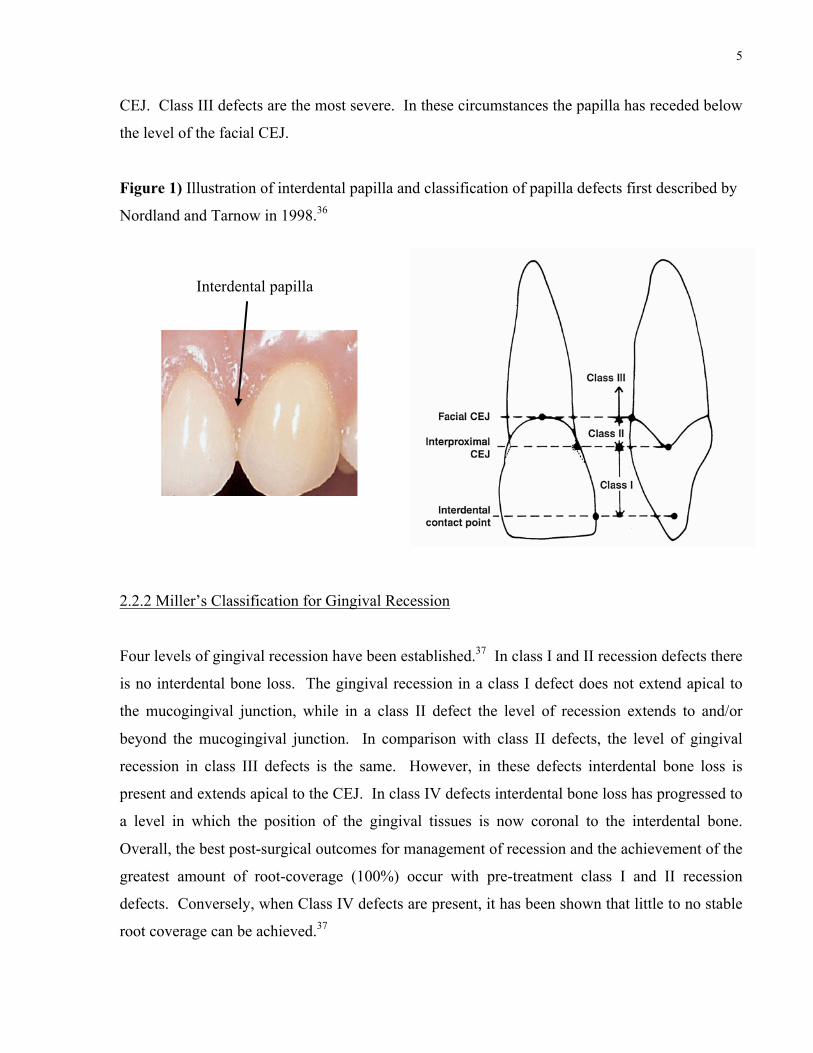
Figure 1) Illustration of interdental papilla and classification of papilla defects first described by
Nordland and Tarnow in 1998.
Figure 2) Juvéderm® and Emdogain® used for clinical treatment.
Figure 3) Surgical protocol.
Figure 4) Six month postoperative outcomes in the treatment of isolated papilla defects and
gingival recession in combination with papilla deficiencies.

vii
List of Appendices
Appendix A: Medical Questionnaire
Appendix B: Consent Meeting Script/Interview Guide
Appendix C: Information Letter for Research Participants
Appendix D: Eligibility Screening Consent Form
Appendix E: Treatment Consent Form
Appendix F: Postoperative Instructions
Appendix G: Case Report Form

viii
Abbreviations
CAL – Clinical attachment level
EMD - Emdogain®
HA – Hyaluronic Acid
SCTG- Subepithelial connective tissue graft
Cemento-enamel junction (CEJ)
VAS(s) - Visual analogue scale(s)
1
Chapter 1: Introduction
The treatment of papilla defects and gingival recession is an ongoing problem facing patients and
clinicians alike. The surgery involved during for the correction of these defects makes most
patients consider any form of treatment with trepidation. Even if a patient chooses to proceed
with therapy, it can be challenging for clinicians to provide the aesthetic results that they and
their patients desire. Several well-documented and successful surgical interventions have been
developed in managing gingival recessions, but most of these techniques can be very invasive
and painful as, in many instances, two separate surgical procedures are required (one for the
recipient site and one on the palate for the harvesting of autologous donor tissue).1-3 Further, for
papilla defects no predictable treatment is even available.4,5
Our primary goal in this clinical trial is to develop a novel therapeutic modality to restore papilla
defects, in the presence or absence of gingival recession. Interdental papillary loss is one of the
most challenging problems in dentistry for clinicians to treat and, in many instances, requires an
interdisciplinary approach involving the periodontist, restorative dentist and orthodontist.6-9 The
correction of these defects has become even more difficult in the presence of implants.10 In order
to address such a complex issue we conducted a clinical pilot trial that involves a relatively pain-
free, minimally invasive, and predictable surgical approach to rebuild lost interdental papillary
tissues and obtain root coverage in areas of gingival recession, with the use of a dermal filling agent
(for the former) and enamel matrix derivative (for the latter). We hypothesized that following the
formation of a subperiosteal space, dermal filler (Juvéderm®) administration into deficient
papillae and the use of enamel matrix derivative (Emdogain®) application to exposed roots as an
adjunct to the use of a coronally positioned flap will provide significant improvements in patient
satisfaction with papillary fill and root coverage respectively. Restoration of isolated papilla
defects will also be obtained through localized subperiosteal papilla augmentation, using a non-
animal derived hyaluronic acid osteoid-overlay. First, in order to evaluate this novel treatment
modality, we will provide a thorough review of the biological nature of the interdental papilla, how
papilla loss and gingival recession may occur and the current and limited evidence on managing
such defects. In addition, we will present a unique approach for the assessment of clinical
outcomes, by using patient-based-outcomes that, although subjective in nature, can be quantified
with visual analogue scales [VAS(s)].

2
Chapter 2: Literature Review 2.1 The Interdental Papilla
2.1.1 The Interdental Papilla and its Role and Impact on Dental Aesthetics
There is an increasing awareness amongst patients regarding the aesthetic appearance of their
dentition. These aesthetic concerns also encompass the health and appearance of the gingival
tissues surrounding the teeth and/or dental implants. Periodontal plastic surgery is a significant
component of aesthetic dentistry and was first described by Miller in 1993 as “surgical
procedures performed to prevent or correct anatomic, developmental, traumatic or disease-
induced defects of the gingiva, alveolar mucosa or bone”.4,11,12 Thus, periodontal plastic surgery
includes the treatment of gingival recession and papilla deficiencies. In most cases, patients
present with gingival recession or papilla loss secondary to aggressive tooth brushing or a history
of periodontal disease, including treatment of that disease.4 Some studies have even shown that
these conditions can simply be related to a patient’s age or sex.13 The interdental papillae of the
anterior maxillary dentition is the most aesthetic area in a patient’s mouth. On average, 91% of
patients show the interdental papilla upon smiling and even patients with a low smile line still
show interdental papillae 87% of the time.14,15 Moreover, it has been documented that there is a
significant psycho-social impact related to compromised aesthetics of a patient’s teeth and
gingival tissues, so this is not merely a frivolous issue.16,17 There are even concerns relating to
one’s ability to obtain a job, when there are significant problems with dento-alveolar aesthetics.18
This is concerning, as close to 50% of patients have been found to have some sort of papillary
deficency.19 When determining the impact of these defects on patients in comparison to other
dental aesthetic concerns, patients rated “black triangles” as a significantly displeasing aesthetic
factor, ranked only behind the presence of visible caries or an exposed crown margin.20 Both
patients and general dentists consider embrasure spaces caused by loss of or damage to the dental
papillae as unattractive and non-ideal, in comparison to those with healthy papillary volume.21
This issue is even more relevant around dental implants, where it has been reported more than
60% of papillae surrounding implant-supported crowns may not completely fill the embrasure
space.22 In addition to compromised aesthetics, loss of the interdental papilla can have negative
consequences including the development of caries, food or plaque accumulation, and altered

3
word pronunciation.10,23 A healthy papilla is also required to provide a protective barrier for the
underlying periodontium.24
2.1.2 Anatomy of the Interdental Papilla
In a healthy periodontium, the gingiva fills the space between teeth and implants up to the apical
extent of the contact point. This gingiva is called the “interdental gingiva or gingival papilla”
and lies within an interdental triangular space called the embrasure.25 It is pyramidal in shape,
with its tip extending to the apical extent of the contact point (See Figure 1). As one proceeds
posteriorly, the interdental contact points broaden buccolingually, creating a gingival col
between the two dental papillae on the facial and lingual surfaces. The col has non-keratinized
epithelium that is more permeable than the keratinized gingiva from which it extends. Its
formation is due to the combination of both junctional epithelia of the adjacent teeth or implants.
The col is an area with increased susceptibility to toxic substances and physical trauma and is
often the site where disease initiates, resulting in destruction of the periodontal apparatus.25
2.1.3 Possible Risk Factors for Interdental Papilla Loss
Several factors may contribute to the presence or absence of papilla fill. It has been proposed
that ideal papillary fill is significantly influenced by five main factors: “age, tooth form/shape,
proximal contact length, crestal bone height and interproximal gingival thickness.”26 Complete
papillary fill appears to occur under the following conditions: young adults with a favourable
crown width/length ratio of ≥0.87, a distance from the bone crest to the contact point of ≤5 mm,
a gingival tissue thickness of ≥1.5mm and a contact length between adjacent teeth of ≥2.8mm.7,26
Interestingly, papilla height has been shown to decrease by about 0.012mm with each additional
year of age.26 This papillary tissue loss can begin at early as 30 years of age.13 In addition to
age, the sex of an individual has also been associated with papilla loss. Individuals aged 65 and
older and those who are male are more likely to have deficient interdental papillary tissue.19
Several studies have evaluated the effect of the vertical distance from the height of crestal bone
to the contact point on the presence of interdental papillae. The ideal distance from the contact
point between two teeth and the interdental alveolar crest was found to be ≤5mm and when this
dimension was satisfactory, complete interdental papillary fill was present 98% of the time.27
4
Complete papilla fill is also most likely to occur where interproximal heights and widths are
either: 4mm x 1.5mm, 4mm x 2mm, 4mm x 2.5mm or 5mm x 1.5mm. As the interproximal
distance between roots increases, there is a corresponding decrease in papilla fill.28 Lastly, a
strong association between a thick periodontal biotype and the presence of interdental papillae of
the maxillary anterior dentition in comparison to thin periodontal biotype has been
demonstrated.29
Around endosseous implants, the presence of a ‘reasonable’ papilla is dictated by the bone level
of the adjacent tooth.30,31 Salama et al.32 concluded that up to 4.5mm of interproximal papillary
tissue height could be achieved when the inter-implant distance was no greater than about
1.5mm. Thus, the horizontal distance between a tooth and an implant or two implants also
contributes significantly to the presence or absence of papilla fill. In the presence of two
adjacent implants, the ideal horizontal spacing and vertical distance from the alveolar bone crest
to the contact point to achieve papillary fill is 3-4mm and 3mm, respectively.33 This correlates
well to earlier studies by Tarnow and colleagues34,35 who showed that the ideal distance between
two adjacent implants for inter-implant bone height and resultant papillary fill was 3mm and that
the mean height of papillary tissue between two implants was 3.4mm. Additional potential risk
factors associated with papilla loss are a history of periodontal disease, large embrasure areas and
root angulations.9
2.2 Classification Systems for Papilla Defects and Gingival Recession
2.2.1 Nordland and Tarnow’s Classification for Papilla Defects
A classification system to interpret and describe papilla defects was first proposed by Nordland
and Tarnow (See Figure 1).36 This system is based on the position of the interdental papilla in
regard to the contact point between two adjacent teeth. As already discussed, the dental papilla
should occupy the entire space between two adjacent teeth with no opening between the papilla
and the most apical extent of the interdental contact point (i.e. for best aesthetic impact). In class
I defects, the papilla is apical to the interdental contact point, but coronal to the interproximal
CEJ. In class II defects, the papilla is apical to the interproximal CEJ, but coronal to the facial
5
CEJ. Class III defects are the most severe. In these circumstances the papilla has receded below
the level of the facial CEJ.
Figure 1) Illustration of interdental papilla and classification of papilla defects first described by
Nordland and Tarnow in 1998.36
2.2.2 Miller’s Classification for Gingival Recession
Four levels of gingival recession have been established.37 In class I and II recession defects there
is no interdental bone loss. The gingival recession in a class I defect does not extend apical to
the mucogingival junction, while in a class II defect the level of recession extends to and/or
beyond the mucogingival junction. In comparison with class II defects, the level of gingival
recession in class III defects is the same. However, in these defects interdental bone loss is
present and extends apical to the CEJ. In class IV defects interdental bone loss has progressed to
a level in which the position of the gingival tissues is now coronal to the interdental bone.
Overall, the best post-surgical outcomes for management of recession and the achievement of the
greatest amount of root-coverage (100%) occur with pre-treatment class I and II recession
defects. Conversely, when Class IV defects are present, it has been shown that little to no stable
root coverage can be achieved.37
974 Reconstructive Therapy
Pedicle soft tissue graft procedures
Rotational fl ap proceduresThe use of a laterally repositioned fl ap to cover areas with localized recession was introduced by Grupe and Warren (1956). This technique, which was called the laterally sliding fl ap operation, involved the refl ec-tion of a full-thickness fl ap in a donor area adjacent to the defect and the subsequent lateral displacement of this fl ap to cover the exposed root surface (Fig. 44-19). In order to reduce the risk for recession on the donor tooth, Grupe (1966) suggested that the mar-ginal soft tissue should not be included in the fl ap. Staffi leno (1964) and Pfeifer and Heller (1971) advo-cated the use of a split-thickness fl ap to minimize the potential risk for development of dehiscence at the donor tooth. Other modifi cations of the procedure presented are the double papilla fl ap (Fig. 44-31) (Cohen & Ross 1968), the oblique rotational fl ap (Pennel et al. 1965), the rotation fl ap (Patur 1977), and the transposi-tioned fl ap (Bahat et al. 1990).
The technique is as follows:
• The rotational fl ap procedure (Fig. 44-32) is initi-ated with the preparation of the recipient site. A reverse bevel incision is made all along the soft tissue margin of the defect (Fig. 44-32a). After removal of the dissected pocket epithelium, the exposed root surface is thoroughly curetted.
• At a distance of approximately 3 mm from the wound edge, which delineates the defect at the side opposite the donor area, a superfi cial incision is performed extending from the gingival margin to a level approximately 3 mm apical to the defect (Fig. 44-32b). Another superfi cial incision is placed horizontally from this incision to the opposite wound edge. The epithelium together with the outer portion of the connective tissue within the area delineated by these incisions and the wound edges is removed by sharp dissection (Fig. 44-32c). In this way a 3 mm wide recipient bed is created at the one side of the defect, as well as apical to the defect.
• A tissue fl ap to cover the recession is then dis-sected in the adjacent donor area. The preparation of this fl ap is initiated by a vertical superfi cial inci-sion placed parallel to the wound edge of the recession and at a distance that exceeds the width of the recipient bed and the exposed root surface by approximately 3 mm (Fig. 44-32c). This incision is extended beyond the apical level of the recipient bed and is terminated within the lining mucosa with an oblique releasing incision directed towards the recession site. An incision connecting the verti-cal incision and the incision previously made around the recession is placed approximately 3 mm apical to the gingival margin of the donor site.
a b
a
c
a
c
bb
dd
Fig. 44-31 Double papilla fl ap procedure. (a) Pre-treatment view of a maxillary canine with facial soft tissue recession. Using split incisions, soft tissue fl aps are mobilized from both sides of the recession (b) and sutured together for coverage of the exposed root (c). The healing result 6-month post-operatively shows complete root coverage (d).
Interdental papilla

6
2.2.3 Relevance and Impact of Classification Systems
Currently, the overall predictability for the reconstruction of deficient interdental papillae is
poor. Regardless of the surgical treatment described, there have been no reports of consistent,
effective and long-term success in papilla regeneration of any type of papillary defect.4,36 Even
when the treatment of these problems have provided beneficial results, one must consider that
most approaches used to evaluate outcomes presented data that were essentially non-parametric,
making statistical analysis, along with assessments related to clinical significance, difficult at
best. It is also important to note that, in most cases, only clinical measurements/scales were
utilized to assess treatment outcomes. These approaches overlook patient-based-outcomes
including, but not limited to, pre- and post-treatment satisfaction with appearance of gingival
tissues. Evaluation of these patient-based-outcomes is possibly even more important than
findings derived from clinical indices or measurements.
2.3 Treatment of Gingival Recession
2.3.1 Tunneling Techniques
Zabalegui et al.38 helped lay the foundation and principles for the use of soft tissue tunneling at
the recipient site for root coverage. In general, a split thickness flap is made in the area of
gingival recession and the overlying tissues are released beyond the mucogingival junction as
well as interdentally underneath the dental papilla. This flap is not reflected. Once the tissues
have been mobilized to the point where there is no tension, they are then positioned coronally
over the exposed roots to cover the area of recession. This type of ‘passive’ or tension-free
release is obtained in order to insure, as predictably as possible, that there will be no apical
migration of the flap and concomitant re-exposure of the root surface during and/or after healing.
Once this is achieved, a connective tissue graft (usually derived from the palate) or acellular
dermal matrix is teased gently into place under the released gingival tissue and secured with non-
resorbable sutures. Sutures may also be placed in the overlying mobilized tissue for proper
positioning over the root. This procedure has been modified over the years and has been proven
to achieve a good degree of root coverage, especially when dealing with multiple sites of

7
recession defects at adjacent teeth and even in the presence of Miller class III recession
defects.39,40
Two recent modifications of the tunneling technique focus considerably on the development of a
less invasive approach. The majority of tunneling procedures require the use of intra-sulcular
incisions at the gingival margin in the area of recession, which results in unavoidable trauma and
occasionally even in perforation of the tissue at the recipient site. The vestibular incision
subperiosteal tunnel access or “VISTA” technique uses an access incision 5-10mm in length
within the attached and unattached mucosa away from the gingival margin of the teeth with
recession.41 This allows for minimal trauma to the treatment site during subperiosteal release
and provides a portal for graft placement. However, the subperiosteal access incision design
used in the VISTA technique has been considered by others as too large.42 Hence, an even less
invasive approach has been developed that requires only a 2-3mm entry incision.42
2.3.2 Newer Method for (Development of) Root Coverage and Repair of Interdental Papillae
Using the various techniques described above, in addition to other approaches, we have
developed a novel minimally invasive tunneling method for root coverage with simultaneous
repair of the dental papilla, as needed. We have included the use of enamel matrix derivative
(Emdogain®; see Section 2.3.3) on exposed root surfaces as well as the use of dermal filler
(Juvéderm®; see Section 2.4.1) in surgically prepared spaces underneath deficient dental
papillae. Our method allows for coronal advancement of tissues to reduce/eliminate recession
defects and at the same time the repair of papillary defects.41,42
2.3.3 Enamel Matrix Derivative (EMD; Emdogain®) for the Improvement of Root Coverage
Enamel matrix proteins are the initiating factors that drive cementogenesis during development
of the dental root and periodontium. Emdogain® is composed of enamel matrix derivative
(EMD) proteins that have been extracted and purified from developing porcine teeth.43 During
surgery, EMD is applied to the exposed root surface following root debridement and
conditioning (for surface demineralization purposes), in an attempt to replicate dental root
development and facilitate periodontal regeneration. The use of EMD increases periodontal

8
regeneration in intraosseous defects. EMD is also useful for treatment of gingival recession
without the requirement of a second surgical site for the harvesting of donor tissue (e.g.
connective tissue from the palate).4,43
2.3.4 Root Coverage Procedures with EMD
In relation to the success of root coverage procedures in general, it has been shown that mean
root coverage success rates range from 51.5% to 98.1% for Miller class I and II recession defects
and 54.8% to 85.0% for Miller class III defects.3 The application of EMD in combination with
coronally positioned flaps provides a significant increase in post-operative root coverage as well
as long-term stability in comparison with coronally positioned flaps alone.44,45 This decrease in
post-operative relapse with EMD is most significant when treating Miller class I and II defects.45
Subepithelial connective tissue grafts (SCTG) are considered the gold standard in treating
gingival recession and, when EMD is used in conjunction with a coronally positioned flap,
comparable root coverage success rates as observed with SCTGs have been demonstrated.44,46
One significant advantage for the use of EMD instead of a SCTG is that, when using the former,
a donor site is not required, thereby minimizing the amount of anxiety and discomfort
experienced by the patient prior to, during, and following the surgical procedure. Furthermore,
EMD has been proven to facilitate early post-operative wound healing by significantly
decreasing bleeding on probing and post-operative patient discomfort.47 Given the above, we
suggest that using EMD over exposed cementum after root planing and conditioning, followed
by the coronal repositioning of gingival tissues will produce stable and aesthetically pleasing
repair of recession defects. As well, we anticipate minimal postoperative discomfort, given that
the surgical method itself is minimally invasive and that the EMD contributes to the reduction in
postoperative pain and inflammation.
2.4 Dermal Fillers and the Treatment of Papillary Defects
2.4.1 Dermal Fillers
The utilization of dermal fillers in plastic surgery and dermatology has been an effective and
long-standing therapeutic modality for treatment of a variety of aesthetic problems related to the

9
skin.48,49 There are currently three classes of injectable dermal fillers primarily used in facial
rejuvenation. These include hyaluronic acid (HA) derivatives, synthetic fillers and autologous
fat.49 We have focused on the HA-derivative class of dermal fillers such as Restylane® or
Juvéderm® in this clinical trial. HA derivatives are generally biodegradable fillers composed of
a natural glycosaminoglycan called hyaluronic acid, which is found in human skin.50 When in
contact with water, the hyaluronic acid swells, allowing expansion of the tissue contours within
which it resides.48,49,51 Restylane is derived from the fermentation of streptococcus species and
exists as a gel (suspended in liquid). It is composed of 20 mg/ml of HA with a mean particle size
of 400µm and is administered with a 30-gauge needle.48 There are approximately 100,000 of
these particles/ml.48,52 Unlike Restylane, Juvéderm dermal fillers are not filtered based on the
size of the HA moieties, but rather consist of a cohesive monophasic gel of cross-linked HA
derived from Streptococcus equi by bacterial fermentation.53 Juvéderm Ultra and Ultra Plus are
two of several different types of Juvéderm dermal fillers that are currently available. Juvéderm
Ultra and Ultra Plus contain 24 mg/ml of HA, but the latter contains HA with about 2% greater
cross-linking, which decreases water solubility. This allows for slower degradation of the
material and increased longevity in situ.54 Juvéderm Ultra XC and Ultra Plus XC have 0.3%
lidocaine added to them, to increase patient tolerability during administration.49,54
Restylane was the first dermal filler, approved by the Food and Drug Administration (USA) in
2003, for use in the medical field. Juvéderm Ultra and Ultra Plus were introduced in the USA
and Canada in 2006 and 2008, respectively.54,55 Since their introduction, dermal fillers have
been used successfully for various procedures including lip augmentation and the restoration of
facial volume loss as well as decreasing the presence of nasolabial folds, facial wrinkling and
undesirable facial lines.56 Interestingly, tissue fillers have been used in dentistry to increase lip
volume in order to obtain coverage of dental implants for patients with a high smile line or to aid
in the retention of a removable prosthesis.57 Dermal fillers have also been injected into the
gingival papilla to help restore papilla loss following implant surgery.58
2.4.2 Treatment of Deficient Interdental Papillae Prior to Dermal Fillers
To date, several non-surgical and surgical methods have been developed to obtain papillary fill,
but in many respects the results have not been overly robust. Non-surgical procedures pertain to
10
those that are prosthetic or orthodontic. Restorative techniques require that changes be made to
the shapes of the teeth in the involved area, in order to close the interproximal spaces and
minimize the presence of ‘black triangles’. However, the amount of closure that can be achieved
is limited, as the crowns can be become quite large, abnormally shaped and thus, unaesthetic in
and of themselves; the impact on the ‘black triangles’ notwithstanding.59 Where significant
periodontal defects are present, pink porcelain can also be added to substitute for gingiva and fill
the defect. However, this approach is not overly satisfactory.60
Orthodontic repositioning and extrusion are additional techniques in managing open embrasure
spaces. Movement of the dentition closer together can help close the space. This can be
enhanced through interproximal stripping of the interproximal tooth surfaces, allowing flatter
contacts and a smaller area requiring papilla fill. However, caution is advised as moving teeth
too close together could potentially result in unintended localized periodontal bone loss.8,61
Vertical extrusion of the involved dentition can cause concomitant coronal advancement of the
periodontal apparatus increasing overall soft tissue height. This is a time consuming and tedious
process, but has been shown to be successful when used under appropriate clinical
circumstances.62,63
From a surgical approach, pedicle flaps, free gingival grafts, connective tissue grafts and even
repeated subgingival curettage have been used in attempts to surgically regenerate the interdental
papilla.64-66 Unfortunately, the frail interproximal papillary tissue and lack of adequate blood
supply results in the necrosis of any graft material used to augment interproximal papillae.9,23
Thus, most of these techniques have been unsuccessful or provide only mild improvements with
significant morbidity to the patient. Beagle64 published one of the first case reports on surgical
interdental papilla reconstruction. His technique involved the labial repositioning of a palatal
split thickness flap into the interproximal papilla position. Carnio’s66 attempts to regenerate one
interdental papilla required three separate surgeries at eight week intervals. Each surgery
involved the harvesting and placement of a connective tissue graft in the interproximal area
under the deficient interdental papilla.
There are also preemptive surgical techniques designed to prevent loss of the interdental papilla
following treatment. Clinicians now anticipate papilla loss and attempt to minimize this through
11
their incision design at the time of surgery. The Split-Finger and ‘Palacci’ techniques are
performed during surgery to manipulate and augment soft tissue in between dental implants at
the time of surgery to not only preserve but also augment the interdental soft tissue and avoid the
development of black triangles during post-operative healing.67,68
Papilla-shaped titanium inserts have also been used to avoid the morbidity of hard and/or soft
tissue augmentation. These titanium inserts are pyramidal in shape and come in an assortment of
different sizes. They are screwed into the bone between two teeth with papilla loss. They
provide bony support for the overlying soft tissue between two dental implants and can be easily
adjusted to fit the size of the interdental space. The insert can be placed during implant surgery
or anytime thereafter. This technique was never successful due to complications related to
ongoing flap dehiscence and exposure of the papillary insert.69
A recent systematic review in 2016 on available treatment techniques over the last six years for
papilla defects identified only eight studies. None of the studies reviewed were randomized
controlled trials and they all provided weak evidence for treatment at best. Interdental papilla fill
varied exceptionally, with reductions of 0.73mm to 2.8mm in the distance of the tip of the papilla
to the interdental contact point. In five of the eight studies, the placement of a subepithelial
connective tissue graft with or without a coronally advanced flap was performed. No consensus
or clinical recommendations could be made to assist clinicians in deciding on the best therapeutic
modality.5
2.4.3 The Novel use of Hyaluronic Acid Derivatives in Papilla Rejuvenation
Currently, the literature lacks strong clinical evidence suggesting that the use of dermal fillers in
providing papilla rejuvenation is highly successful. Becker et al.58 published the first case report
on the use of hyaluronic acid injections (Restylane®) in the restoration of minor papillary
deficiencies adjacent to dental implants and/or teeth. Fourteen sites were treated in eleven
patients. A total 0.2ml of Restylane was administered several millimeters apical to the papillae,
using a 23-gauge needle, 2-3 times. This was followed by repeated injections of Restylane at
three-week intervals with no more than three applications. Cases were followed for a 25-month
period. Three sites had 100% fill while the remaining eleven sites had papillary fill ranging from
12
57-97%. The authors concluded that it was possible to obtain ‘modest’ improvements in papilla
fill. Importantly it should be pointed out here that the investigators did not evaluate patient
related outcomes.
Reconstruction of the dental papilla was attempted by others and followed the methods described
previously by Becker et al.58,70 HA was injected into twenty-one deficient interdental papillae
between natural teeth.70 Injections were repeated at three weeks and three months. By the six-
month time-point, a statistically significant improvement in papilla fill of ≥50% was found in
43% of treated sites. In a more recent case series71 seventeen class 1 and 2 papilla defects
associated with the natural dentition of nine female patients were treated. The investigators,
using a 23-gauge needle, injected 0.2ml of cross-linked HA into sites with deficient papillae.
These injections were repeated at three weeks and six weeks. Photographs were taken at
baseline (i.e. prior to treatment), and photographs taken four- and six-months after treatment.
The investigators demonstrated a statistically significant mean increase in papilla height in the
treated sites by six months (0.5mm). About 66% of patients indicated that they would be willing
to have this type of procedure done again, if necessary. The patient assessments implemented in
this study highlight an important step towards the use of patient-based outcome measures.
Due to concerns regarding the assessment of papillary fill following dermal filler injection, Lee
et al.61 introduced the ‘photographic standardization device’ and ‘injection-assisted device’ for
more precise analysis of papilla dimensional changes and hyaluronic acid administration.61 A
total of forty-three maxillary anterior sites were treated among four males and six females. The
investigators utilized an injection-assisted device with a 30-gauge needle to introduce 0.002ml of
hyaluronic acid gel up to five times for a total of 0.01ml of HA. Each injection was performed
three weeks apart and administered ‘as needed’ to achieve complete papillary fill. With the aid
of the ‘photographic standardization device’ changes in black triangle area, height, and width
were calculated. The data showed that there was a 0.2mm2 reduction in black triangle area,
along with a reduction of 0.71mm and 0.32mm in black triangle height and width, respectively.
The number of injections required ranged between three-four times and this produced a mean
papillary fill of 92.6%. Furthermore, of the forty-three treated sites, twenty-nine had complete
fill.

13
Lastly, the first and only randomized controlled trial performed studied the effects of HA
injections compared to saline injections into the deficient papillae of twenty-two patients.72
VASs were also included to quantify patient-reported outcomes. In this study, it was not
possible to demonstrate any differences in the morphological characteristics of papillae in either
the control or treatment groups, even up to and including a post-treatment time point of six
months. Patients experienced moderate pain for both saline and HA injections, as demonstrated
in pain levels averaging between 50-60 using a 100mm VAS assessment on pain during
injection. However, significantly more discomfort was associated with the injection of HA in the
first week following treatment (VAS of 28 for HA and 5mm for placebo). When measuring the
aesthetic impact of treatment for patients, their general perception of improvement was
somewhat modest as based on VAS measures with satisfaction scores of <30mm. Interestingly,
this response fits with the clinical findings reported for this study.

14
Statement of the Problem Various surgical interventions are available for the management of gingival recession, but these
methods are invasive and painful, often requiring two surgical sites (donor and recipient) and in
many instances fail to provide complete root-coverage. Moreover, most papilla defects and their
associated ‘black triangles’ remain untreatable. Although these ‘black triangles’ appear quite
small from a clinician’s viewpoint, they seem to have a rather significant impact on oral health
satisfaction for patients. This variability in results and lack of success along with the associated
morbidity from these procedures highlights the need for less invasive, less painful and more
predictable approaches to manage root exposure and papilla deficiencies. It is our intent to
develop such a procedure, as described below, with the use of EMD and a dermal filler.
The application of dermal fillers in dentistry is in its infancy. HA has been used recently for
treatment of deficient papillae, but the results have been generally unpredictable with only
modest improvements at best. In this regard, previous investigators utilized direct injection of
dermal fillers into deficient papillae without the creation of a ‘tissue space’ that would facilitate
the delivery and retention of the dermal filler into the site. Thus, one might have predicted
minimal success using these types of approaches since, unlike in the pliable skin where dermal
fillers are most commonly used, the interdental papillary tissues are dense and immobile. This
underscores the rationale for the development of the approach described here. It is our
hypothesis that a subperiosteal tissue space underneath the papilla must be created first, in order
to receive the dermal filler and thereby produce visible and substantial morphological changes.
Thus, the aim of this pilot study was to develop a minimally invasive and predictable approach to
restore papilla deficiencies and correct gingival recession either concurrently or separately,
depending on the clinical situation. Our clinical trial investigates the restoration of papilla
deficiencies and correction of gingival recession using a surgical technique that involves the use
of modified HA dermal filler (Juvéderm®) for reconstruction of deficient interdental papillae as
well as enamel matrix derivative (Emdogain®) for obtaining root coverage. It is our intention to
use Juvéderm to rebuild deficient papillae and to utilize EMD to promote root coverage in a
single procedure. The surgical technique in this clinical research trial is based loosely on the
methods described by Zadeh41 and Chao42 and should be considered to be a minimally invasive

15
surgical approach. We predict that localized administration of a dermal filler and EMD,
following the formation of a subperiosteal tissue space to receive the material, will provide root
coverage and the restoration of interdental papilla deficiencies.

16
Chapter 3: Materials and Methods
3.1 Human Subjects
The calculated sample size for this study was based on a model described by Norman and
Streiner.73 We predicted a minimum 30% improvement (effect size) in gingival aesthetics from
our VAS scores to be clinically significant. Based on this improvement along with an
anticipated standard deviation of 25, a significance of ≤0.05 and a power set at 0.9, we estimated
a sample size requiring at least 15 patients.73,74 Prior to patient recruitment, this clinical pilot
study received approval for scientific merit and ethics from the University of Toronto’s Faculty
of Dentistry and Research Ethics Board. All patients were selected from the Graduate
Periodontics clinic at the Faculty of Dentistry, University of Toronto. Overall, twelve patients (9
females and 3 males) were screened. This was quite close to our initial convenience sample size
of fifteen participants. We did not use a ‘control’ group, but instead all comparisons were
performed pre- and post-operatively.
3.2 Inclusion and Exclusion Criteria
Specific inclusion and exclusion criteria are highlighted below and were evaluated via a
comprehensive medical history form (Appendix A):
• Patient inclusion criteria
o Eighteen years of age or older and willing to proceed with all treatment and
follow-up appointments
o Presence of localized areas of recession and/or interdental papilla loss
o No contraindications to periodontal surgery
o Presence of class 1 or 2 papilla deficiencies and class 1, 2, or 3 recessions
• Patient exclusion criteria
o Active periodontal disease or presence of gingivitis in the proposed surgical area
o Pregnant women
o Patients with severe systemic disease (we enrolled patients with an American
Society of Anesthesiologists’ physical status classification of 1 and 2 only)
o Smokers or patients with a history of smoking in the past 5 years
17
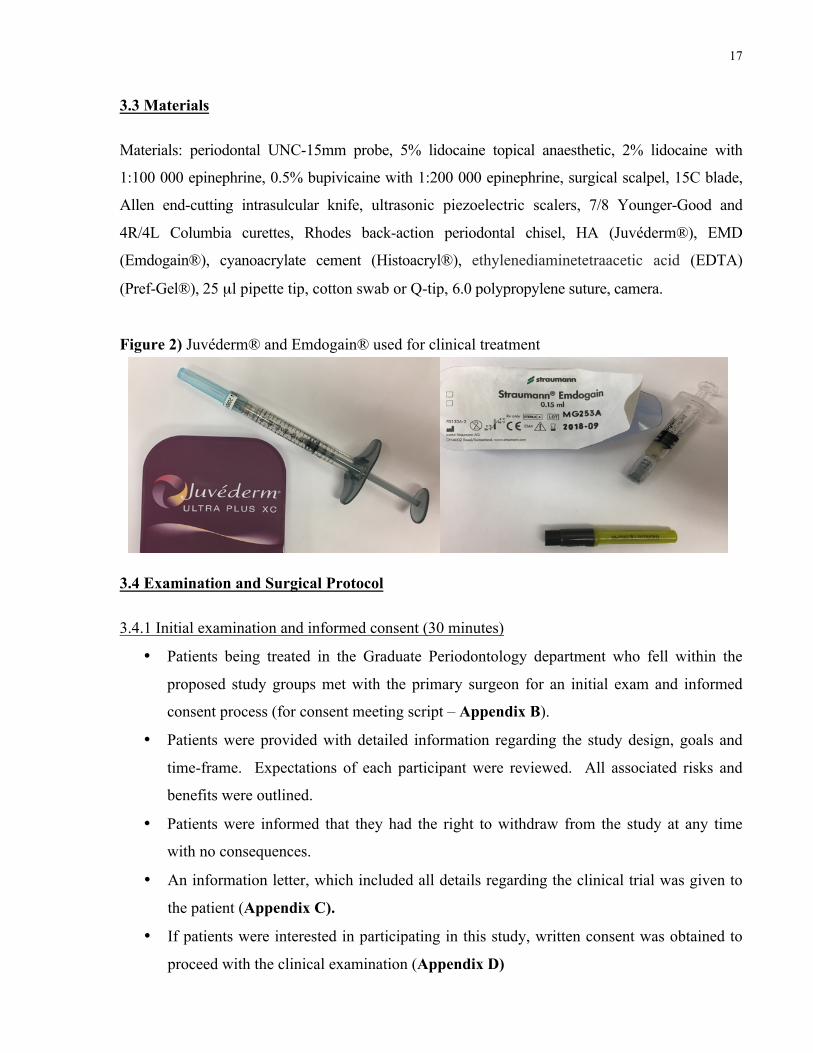
3.3 Materials
Materials: periodontal UNC-15mm probe, 5% lidocaine topical anaesthetic, 2% lidocaine with
1:100 000 epinephrine, 0.5% bupivicaine with 1:200 000 epinephrine, surgical scalpel, 15C blade,
Allen end-cutting intrasulcular knife, ultrasonic piezoelectric scalers, 7/8 Younger-Good and
4R/4L Columbia curettes, Rhodes back-action periodontal chisel, HA (Juvéderm®), EMD
(Emdogain®), cyanoacrylate cement (Histoacryl®), ethylenediaminetetraacetic acid (EDTA)
(Pref-Gel®), 25 µl pipette tip, cotton swab or Q-tip, 6.0 polypropylene suture, camera.
Figure 2) Juvéderm® and Emdogain® used for clinical treatment
3.4 Examination and Surgical Protocol 3.4.1 Initial examination and informed consent (30 minutes)
• Patients being treated in the Graduate Periodontology department who fell within the
proposed study groups met with the primary surgeon for an initial exam and informed
consent process (for consent meeting script – Appendix B).
• Patients were provided with detailed information regarding the study design, goals and
time-frame. Expectations of each participant were reviewed. All associated risks and
benefits were outlined.
• Patients were informed that they had the right to withdraw from the study at any time
with no consequences.
• An information letter, which included all details regarding the clinical trial was given to
the patient (Appendix C).
• If patients were interested in participating in this study, written consent was obtained to
proceed with the clinical examination (Appendix D)
18
• Initial clinical measurements were obtained:
o buccal recession measured from cemento-enamel junction (CEJ) to free gingival
margin at the mid-facial and line angles of each tooth
o distance from the tip of papilla to interdental contact point
o pre-operative photographs of proposed surgical site (not-standardized)
o radiographic assessment of bone levels
• Following initial examination and determination of sites requiring treatment, patients who
met the inclusion criteria were provided the opportunity to participate in the study.
• Patients had the opportunity to ask any questions regarding the study and detailed
responses were provided. We offered a telephone number to each patient, so that they
could contact the PI or other investigators, if they had additional questions.
• If the patient agreed to proceed with treatment, informed consent was signed (Appendix
E). A copy of the signed consent form was given to each participant.
• Patients were provided with post-operative instructions (written and verbal) that they
would be required to follow after surgery (Appendix F).
• Patients completed the pre-operative assessments in the case report form (Appendix G).
3.4.2 Surgical Protocol
On the day of surgery, the surgeon reviewed the previously signed consent form with the patient
and asked the patient if he or she had any further questions. Once verbal consent to proceed was
given, topical lidocaine 5% was applied in area of the surgical site. Buccal and lingual infiltration
using 2% lidocaine with 1:100 000 epinephrine and 0.5% bupivicaine with 1:200 000 epinephrine
was administered. Scaling and root planing of the teeth involved with ultrasonic piezoelectric
scalers and hand instruments was performed. A 3-5mm horizontal incision was made in the
alveolar mucosa at a minimum of 2mm beyond the mucogingival junction. Using the incision as
access, a subperiosteal tunnel was created toward the area of recession and deficient interdental
papilla(e), while leaving the interdental and marginal tissue intact. Juvéderm was administered
into the papilla(e) and the tissue space underneath to achieve ideal papillary fill after the
preparation of the surgical space was completed. Cyanoacrylate was then used to seal the free
gingival margins surrounding the papilla(e) with a 25µl pipette tip (gently tap or push on pipette
to control release, soak cotton swab in saline and dab area to facilitate set). This was done to
19
prevent ‘leakage’ of the HA from the treated site. Cyanoacrylate was not used if papilla defects
were treated in combination with recession (in these cases a sling suture was placed instead, to
coronally advance the gingival margin and papilla). The exposed root cementum was
conditioned with EDTA followed by placement of EMD and coronal repositioning of the
gingiva/alveolar mucosa over the area of recession. A 6-0 polypropylene sling suture was used
to maintain coronal advancement. During the surgical procedure, additional dermal filler was
administered into the interdental papilla as needed, in order to maintain the best papillary
correction. An average of 0.2-0.6 ml of dermal filler was required per papilla, depending on the
extent of the papilla loss. Post-operative instructions were reviewed verbally in detail, and a
written copy was provided (Appendix F). Figure 3 below provides a visual demonstration of the
surgical technique.
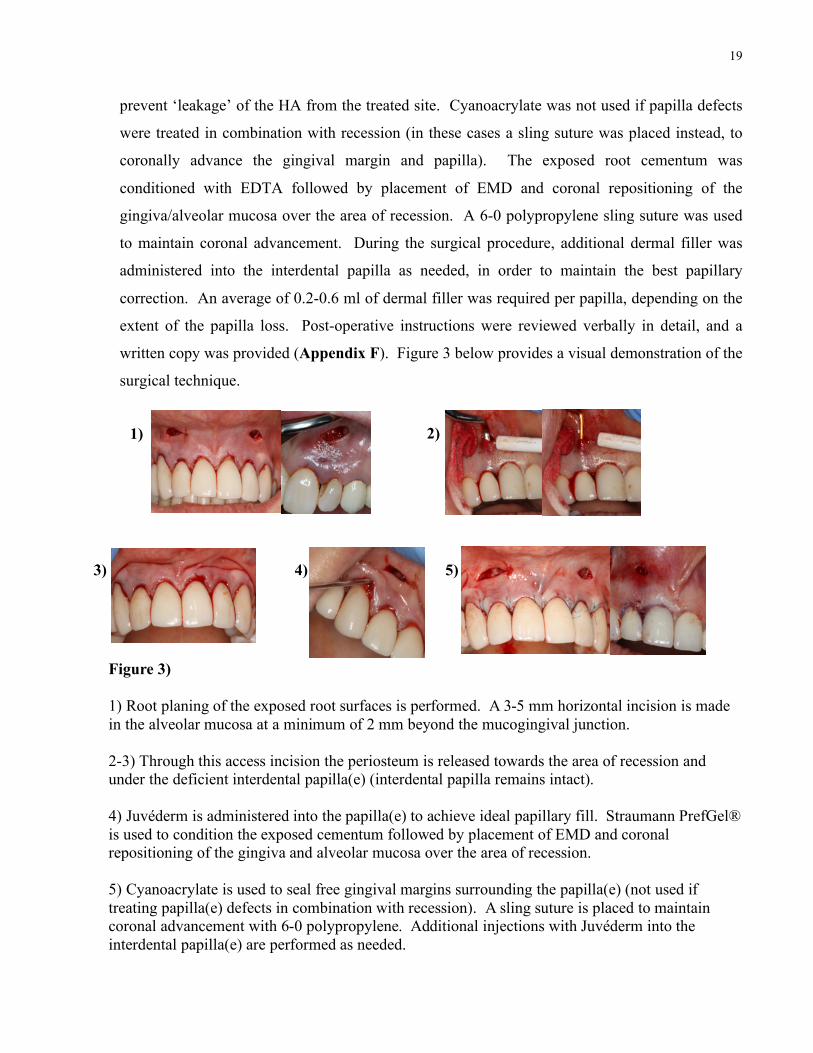
Figure 3) 1) Root planing of the exposed root surfaces is performed. A 3-5 mm horizontal incision is made in the alveolar mucosa at a minimum of 2 mm beyond the mucogingival junction. 2-3) Through this access incision the periosteum is released towards the area of recession and under the deficient interdental papilla(e) (interdental papilla remains intact). 4) Juvéderm is administered into the papilla(e) to achieve ideal papillary fill. Straumann PrefGel® is used to condition the exposed cementum followed by placement of EMD and coronal repositioning of the gingiva and alveolar mucosa over the area of recession. 5) Cyanoacrylate is used to seal free gingival margins surrounding the papilla(e) (not used if treating papilla(e) defects in combination with recession). A sling suture is placed to maintain coronal advancement with 6-0 polypropylene. Additional injections with Juvéderm into the interdental papilla(e) are performed as needed.
1)
3 4 5
2)
3) 4) 5)

20
3.5 Post-Surgical Assessments and Data Collection
Treatment outcomes involved the assessment of aesthetics using VASs to measure an array of
patient-reported/subjective outcomes. These scales were also used to assess clinician-based
subjective assessments (Appendix G). Prior to completion of the clinical report-related VASs,
patients practiced and familiarized themselves with the concepts associated with VAS-based
measurements of subjective data. The practice sessions included the assessment of ‘blackness’
of four different box-shapes using VAS measurement. More importantly, patients were
presented with clinical photographs demonstrating recession/papillary presentations ranging
from those considered by the investigator to represent poor to excellent gingival appearances.
Patients who were unable to provide appropriate VAS measures could be either re-trained or not
be included in the study (this did not actually occur). VASs pertaining to post-treatment results
included both the patients’ subjective perceptions as well as clinician-based assessments of
aesthetic outcomes using pre- and post-operative photographs taken of the patients’ surgically
treated areas. By using VASs, it was also possible to measure other secondary subjective
outcomes including pain and tolerance of the procedure in its own right, as well as how this
procedure was tolerated in comparison to previous periodontal treatments the patients might have
had. The VAS-based outcomes were analyzed in such a way as to be able to differentiate and
measure improvements in aesthetics as perceived by patients and clinicians regarding root
surface coverage and/or interdental papillary fill. In all cases, patient information and dates of
the pre- and post-operative treatment photos was concealed, which provided for blinding.
In addition to patient- and clinician-based subjective assessments, it was also considered
critically important to use more commonly accepted measures to evaluate the outcomes of this
surgical study. Initial recession and percent root coverage before and after therapy was
measured. The pre- and post-operative distance from the tip of the papilla to the interdental
contact point was used as an objective measure of papilla reconstruction/fill. All pre- and post-
operative measurements, photographs and VAS assessments were performed by the same
clinician. See below for the details of assessment at each follow-up appointment.
1) 1-2 week follow up – 30 minutes
• Assessment of healing of surgical site and removal of sutures. Oral hygiene instructions.
Answer patient questions or concerns.
21
• Measurements of recession, complete root coverage percentage, distance from papilla tip
to interdental contact point.
• Post-op photographs for clinician and patient specific visual analog scale assessment of
outcomes (pre- and post-operatively where appropriate) including, but not limited to,
satisfaction with appearance of papillae, satisfaction of overall gingival appearance,
success of root coverage and post-operative pain.
2) 6-week follow-up – 30 minutes
• Assessment of healing, provide supra-gingival debridement as needed. Hygiene re-
instruction. Answer patient questions and concerns.
• Measurements of recession, complete root coverage percentage, distance from papilla tip
to interdental contact point.
• Post-op photographs for clinician and patient specific VAS assessment of outcomes (pre-
and post-operatively where appropriate) including, but not limited to, satisfaction with
appearance of papillae, satisfaction of overall gingival appearance, success of root
coverage and post-operative pain.
3) 6-month follow-up – repeat steps of 6-week follow-up
3.6 Statistical Analysis
Pre- and post-treatment VAS scores were recorded in tables for assessment and comparison. The
following null hypothesis was considered to test our VAS assessment: there is no difference
between the pre- and post-VAS assessments and papillary fill. We predicted that the creation of a
subperiosteal tissue space followed by the administration of a dermal filler and EMD will lead to
statistically and clinically significant improvements in the aesthetic appearance of either or both root
exposure and papilla defects, as reported by patients and clinicians. The primary VAS score in
testing this hypothesis was a question regarding patient satisfaction with papilla fill and/or root
coverage. Secondary VAS scores addressed different exploratory outcomes of this novel
surgical technique to help provide clinicians with a means of evaluating this technique further
and establish new or adapt existing treatment modalities. Data obtained from the primary VAS
scores and quantitative assessments were analyzed using paired sample t-tests with a significance
level set at α = ≤0.01 for rejection of the null hypothesis.
22
Chapter 4: Results 4.1 Subjective Outcomes: Patient- and Clinician-Based Seven females and two males (mean, 54.3±7.2 years old) among the 12 patients initially screened
underwent treatment and completed the required follow-up period. One patient came back and
underwent the procedure twice, resulting in ten cases among the nine patients. Primary and
secondary VAS scores were the principal method used for assessment of patient-based outcomes,
as noted above. The primary VAS outcome used to assess treatment success was the VAS
response to the question: “How would you rate your papilla fill and/or root coverage?” (Table 1;
Figure 4; Appendix G). There was a 61% and 68% improvement in patients’ perceptions of
papilla fill and/or root coverage when comparing pre- versus post-operative appearances (60.7%;
p<0.01; CI=42.0-79.3 and 68.3%; p<0.01; CI=52.1-84.5) at six weeks and six months after
treatment, respectively. An even greater improvement was found when analysis was restricted to
the treatment of Tarnow class 1 and/or Miller class 1 or 2 defects (Mean VAS increase of 65.8%;
p<0.01; CI=46.7-85.0 at six weeks and of 70.6%; p<0.01; CI=47.3-94.0 at six months) (Table
1). A series of secondary subjective outcomes were also assessed (Tables 2-5; Appendix G).
When patients were asked if they were happy with the overall aesthetics and if they thought the
surgery was successful, the level of VASs showed satisfaction measures of 73% and 81% at six
months, respectively. This increased substantially for both overall aesthetics (89.8%±19.0%)
and treatment success (96.3%±5.1%) when analyzing only cases with pretreatment Miller class 1
and 2 recession defects and/or Tarnow class 1 papilla defects. Further, in most instances,
patients who underwent this minimally invasive surgery indicated that they experienced less
pain, increased procedure-tolerance, and faster postoperative recovery, as compared to their
experiences with previous periodontal surgical procedures such as open flap debridement,
gingival grafting and implant placement (Table 3).
When periodontists were asked to evaluate papilla fill and/or root coverage before and after
treatment, their subjective clinical assessments of improvements were more modest than those
reported by patients. The average VAS increase noted after surgery based on overall clinical
improvement was 27% (VAS= 27.4%±6.2%). Similarly, when assessing whether treatment was
23
clinically successful, they rated it at a level of about 68% (VAS = 68.0%±7.0%), but this still
represented a substantial increase over baseline assessments (Table 6).
4.2 Clinical Measurements Mean papilla fill of 61.8%±26.7% was observed at six months, among the 26 treated papilla
defects. This corresponded to a statistically significant mean increase in papilla size/fill of
1.3mm±0.7mm (p<0.01) (Table 7; Figure 4). In addition to this overall result, it was also noted
that more than half of the treated defects resulted in ≥2/3 of papilla fill after surgery. The
average amount of root coverage obtained was 60.4%±43.3% in 52 treated sites, and 26 of the
sites demonstrated 100% root coverage (Table 8). Simultaneous root coverage and papilla
correction treatment did not alter outcomes for either clinical parameter.
24
Chapter 5: Discussion
To the best of our knowledge, this is the first clinical study evaluating the use of dermal fillers in
the augmentation of deficient interdental papilla through the creation of a subperiosteal tissue
space. It is also the first attempt at treating deficient papillae with dermal fillers at the same time
as treatment of gingival recession using EMD. Our results indicate that both clinically and
statistically significant improvements in interdental papilla fill can be achieved. We also
demonstrate that the presence of both gingival recession and papilla deficiency should not be a
deterrent to treatment.
There was a substantial improvement in patient satisfaction relating to the appearance of their
gingival tissues (papilla fill and root coverage) following dermal filler injection and/or gingival
coronal advancement. Even though we originally predicted that an improvement (effect size) in
VASs of 30% pertaining to gingival aesthetics among at least fifteen patients would be required
to reach significance, we achieved a statistically significant increase in patient satisfaction post-
treatment with only 9/10 patients. Moreover, these results correlate well with our quantitative
post-operative percentages and measurements in papilla fill and/or root coverage obtained,
suggesting VASs used to measure subjective outcomes are reliable assessments of treatment
success. According to the literature, VASs are considered as one of the best techniques for
measuring levels of chronic and acute pain.75 They have also been used extensively to evaluate
other subjective parameters involving patient perceptions.76,77 As in our study, VAS assessments
was performed by using a 100mm scale anchored by particular descriptors that are considered to
be opposites of one another. Patients’ ability to use these continuous scales to quantify
subjective parameters is the key to their strength. This is in contrast to discontinuous scales that
evaluate subjective outcomes using ratings based on numerical or verbal values.75 The power of
VAS-generated data results is exemplified further by the difference between patients’ opinions
related to improvements in gingival aesthetics following treatment, compared to those of
periodontists. Patients were clearly more satisfied with post-treatment gingival aesthetics and
overall success, highlighting the importance of understanding patient concerns and meeting their
expectations. Perhaps there should be less of a concern that in many cases, ‘perfect’ clinical
results cannot be obtained, since the ultimate arbiter of treatment success, when considering
procedures in periodontal plastics surgery, is in fact the patient. It is interesting to note that what
25
a periodontist might consider as an acceptable or aesthetic result differs from the patients’
assessments. Contributing factors to this difference may be the fact that patients are usually
more aware of the appearance of their papilla defects, fail to understand the difficulty in
achieving papilla fill and the lack of treatment options available to them or they may have
previously experienced unsuccessful therapy. Thus, we believe the improvements in our patient
reported outcomes as per primary and secondary VAS scores confirm the true value of this novel
and minimally invasive surgical technique. Furthermore, in our investigation, patients were
trained in the use of a VAS to score gingival aesthetics (Appendix G). This training likely added
an additional degree of confidence in the outcomes of VAS measurements obtained in our study
as compared to VAS readings obtained from patients who would be otherwise unfamiliar with
the use of a VAS. Other studies that implement VASs for assessing pain or aesthetics associated
with papilla fill or root coverage do not report the use of pre-operative practice VASs for their
patients.72,78 In these studies we don’t know whether the patients understood the concept of a
VAS or how to complete them appropriately. In addition, it is important to emphasize that had
subjective outcomes not been measured, it was still possible to demonstrate statistically and
clinically significant improvements, based on clinical measures of treatment.
As reported in the literature, when carrying out treatment for recession, the clinical
measurements show that root-coverage improvements can range from 51.5% to 98.1% for class I
and II recession defects and 54.8% to 85.0% for class III defects.3 In our study, the average
amount of root coverage achieved was about 60.4%±43.3%. Although this is on the lower end of
the expected root coverage following treatment, we believe the true value of this surgical
technique lies in the fact that one can treat root recession and papilla deficiencies concurrently
and without the requirement of a donor site. The amount of papilla fill achieved six months
following treatment in our study appears comparable to other studies. Through the simple
injection of dermal filler into the papilla Becker et al. showed papillary fill ranging from 57-
97%.58 Other studies report a ≥50% improvement in papilla fill among 43% of treated sites.70
Awartani and Tatakis71 treated Tarnow class 1 and 2 papilla defects in seventeen sites with a
mean increase in papillary fill of 0.5mm at six months. The percentage of papilla fill reported in
our investigation is similar to that reported by Awartani and Tatakis71. However, the average
amount of papilla fill obtained in our investigation was 1.3mm±0.7mm; an almost 3-fold increase
in comparison. This additional 0.8mm increase in papilla fill over six months suggests the

26
papilla defects treated in our investigation could have been more severe than those treated by
Awartani and Tatakis71 (Table 7) and represents the potential for a greater effect, depending on
the size of the defect being treated, using the methods described here.
We suggest that one of the important factors relating to generating more fill of deficient papillae
in our study can be attributed to surgical release of the gingival tissue and creation of a
subperiosteal space prior to insertion of dermal filler. When HA gel is ‘merely’ injected into a
deficient papilla, it has been shown, using a randomized controlled trial approach, that there were
no significant improvements in papilla fill compared to control (saline) injections.72 However,
the failure to demonstrate a significant difference in this study could have also been related to the
rather small sample size that was used, and perhaps to the somewhat limited injection protocol in
comparison to other studies including ours (i.e. the investigators used a different injection
technique and only a single follow-up injection at four weeks).72 Others have also suggested that
detaching the gingiva by way of a tunneling procedure, prior to HA injection, could provide for
mobilization of the soft tissue prior to injection, thereby producing a more satisfactory
outcome.72
When dermal fillers are used to treat skin problems (e.g. wrinkles), there is no need to create a
surgical space. However, in the treatment of deficient dental papillae, as opposed to the skin,
there are significant anatomical constraints that must be considered. In contrast to skin, gingival
tissues, including the papillae, are firmly bound down to an underlying periosteal bed with very
limited elasticity. Without this elasticity it is unlikely to be able to expand a deficient papilla
using injections alone. By tunneling under the interdental papilla, we were able to release the
interdental collagen-rich connective tissues, allowing mobilization for both coronal advancement
and expansion of the papilla immediately following injection. All previous studies have relied
on the ability of HA to expand the interdental papilla over time through its absorption of water
along with the use of up to five separate injections to obtain meaningful results.51,58,70-72 By
using the approach described here, similar clinical results (papilla fill) were obtained in a single
surgical appointment. Furthermore, as noted above, the procedure was tolerated well by the
patients.
When we treated papilla defects in combination with gingival recession, the gingival margin was

27
positioned at the level of the CEJ. We suggest that even more papilla fill, as well as root
coverage might be achieved by advancing the gingival margin coronally past the CEJ, onto
enamel. Indeed, this concept has been illustrated and discussed by others who obtained
improved root coverage, when flaps were fixed at approximately 2mm beyond the CEJ.79
Therefore, we postulate that further advancement of the flap beyond the CEJ, even in areas
without root exposure, could allow for the creation of a larger subperiosteal space, allowing for
the introduction of more dermal filler and, subsequently, the development of even more papilla
augmentation than demonstrated here or in other studies. We anticipate that, as shown by others,
when the site heals, the ‘overextended’ gingival margins will recede back to their normal
physiologic position, while the papilla would retain its increased size due to the dermal filler
placed at the time of surgery.
Through clinical observation, we noted additional factors that might affect results such as the
width of the interdental black triangle. In this regard, we observed that if the embrasure space
was too wide or too narrow, papillary fill following HA injection was less likely to occur. This
seems to correlate with more definitive findings by Lee and colleagues80 who demonstrated that
defect dimensions including black triangle area, height and width appear to affect treatment
success. When the area of the black triangle was 0.25mm2 with a 1mm height and 0.5mm width,
complete fill of the deficient papilla was most likely to occur. To the best of our knowledge, this
is the first prognostic criterion proposed that clinicians may be able to use to predict future
papilla fill for patients.80 In our study, the amount of hyaluronic acid we injected at each site
ranged from 0.2-0.6ml. This was based on need and not on a pre-determined amount of filler to
be utilized. Lee and colleagues61 demonstrated that using smaller injection amounts minimizes
dermal filler loss, while providing additional injections increased the amount of papilla fill.
There also appears to be no set limit to the number of injections that can be performed. All
previous studies show that multiple dermal injections over time were required to obtain optimal
results.58,61,70,71 However, this might be due to the fact that in these studies, a surgical space for
placement of dermal filler (and also mobilization of the papilla itself) was not created.
Considering the biodegradable nature of dermal fillers such as Juvéderm, it may not be possible
to achieve long-term stability. In this regard, a previous study showed that papillary
improvements with the use of injected HA can be maintained for up to at least two years.58
28
Thus, time will tell if, during maintenance therapy, the sites will need to be re-injected to regain
the surgically created improvement. If additional therapy is required long-term, we suggest that
treatment might consist of ‘touch-up’ injections only due to the presence of an already-
established surgical ‘space’. With our surgical technique, patients appreciated significant
improvements with high levels of treatment acceptance and tolerability. Therefore, even if
surgery is necessary again at some point, this might not be perceived as being too onerous for the
patient. Further, in regard to the potential need for re-treatment, it has been demonstrated in vitro
that injection of cross-linked HA in reconstructed 3-D skin models induces an increase in
fibroblast activity and production of type 1 and 3 procollagens. Results also indicate that HA
may impact fibroblast regulation of MMP-1 secretion.81 Interestingly, Lee and colleagues80
found that when the distance from the alveolar bone crest to the interdental contact point was
≤6mm complete papilla fill was obtained. In comparison to Nordland and Tarnow’s classical
study on papillary height, HA injections appear to promote an additional 1mm of papilla fill,
possibly through collagen production, beyond the ‘normal’ physiological interdental papillary fill
of 5mm.36,80 These assumptions are also based on HA’s role in tissue healing through enhancing
cell proliferation, re-epithelialization, migration and blood vessel formation. Its ability to
enhance wound repair results in reduction in scar tissue formation.82 In dentistry, HAs have been
useful in the treatment of aphthous ulcers through a barrier effect with immediate reduction in
soreness. There was also a decrease in the recurrence of these ulcers.83 HAs have even been
shown to have potential anti-inflammatory effects in the treatment of gingivitis.84 With respect
to papillary fill, some studies have shown improvements can be maintained over time while
others indicate relapse does occur. For instance, Mansouri et al.70 found 10% of treated patients
had 50% improvement at three months in comparison to 43% of patients at six months, and
Becker et al.58 showed a 94% improvement in papilla fill over a span up to twenty-five months.
However, Awartani and Tatakis71 found there was relapse in some cases four and six months
post-treatment. Similarly, a small amount of relapse was evident in localized sites among some
of our patients. This was not evident in our mean papilla fill at six weeks (61.2%±39.3%) or six
months (61.8%±26.7%) because, over time, other sites had an increase in papilla fill (Table 7).
If the dermal filler does degrade over time, then one would expect to see volume loss occurring
in all treated sites. This was not the case in our study. Therefore, it is likely this relapse in
localized sites can be attributed to a multitude of other factors such as the patients’ own post-
operative care. In fact, one patient in our study who actually experienced relapse, admitted later
29
on to the repeated use of tooth picks in between her maxillary anterior teeth, including the area of
treatment. Hence, control of patients’ habits would also seem to be critically important in order
to ensure good treatment outcomes. It may also be the fact that relapse or lack of complete fill is
only present in the larger defects as was the case in the clinical trial by Lee et al.61 Overall,
whether or not relapse will occur is unclear at this time and longer follow-up studies are required.
However, based on the direction of the findings reported above, one can speculate that once
treated with HA, the clinical and subjective improvements achieved following surgery may be
quite stable.
Other Applications of this New Surgical Model
A unique element of this novel surgical approach for papilla fill is the ability to combine it with
restorative or even orthodontic treatment modalities. In areas of deficient papilla, the simple
administration of HA has already been used with other restorative techniques. A case report
demonstrated the successful use of direct composite resin with dermal filler application to close a
midline diastema with an embrasure space of 1.5-2mm.85 Following the placement of
provisional crowns to form an ideal contact point, Juvéderm® Ultra XC injections into the
papilla were performed, followed by repeated injections twenty-one and forty-eight days later.
At one month, about 1mm of papilla fill had been achieved, and final crowns were made to fill
the remaining space. Eighteen months following treatment, complete papilla fill was still
maintained. This patient was provided with an ideal esthetic result without the need for further
orthodontic treatment, which would have resulted in prolonged treatment time at additional
cost.85
Possible Sources of Error and Opportunities for Improvement
A possible error in our clinical assessments was the use of a UNC-15mm probe to measure the
distance from the contact point to the tip of the interdental papilla and rounding these
measurements to the nearest half millimeter. An assessment of intra-examiner variability in
periodontal probing reproducibility with the calculation of a correlation coefficient would have
enabled self-calibration and reduced potential bias. However, studies assessing intra-examiner
variability on periodontal probing have concluded there are no statistically significant differences

30
in measurement error.86 One must also consider these surgical treatments were performed by a
novice clinician in a periodontal residency program. Perhaps even better outcomes might have
occurred were the surgical treatments performed by a more experienced periodontist.
Furthermore, our ability to accurately reproduce photographs at follow-up appointments was
limited. As in previous studies by other investigators, photographs were taken in an attempt to
reproduce the same horizontal and vertical distances and angulation each time.58,70,71 This has
been minimized, but not eliminated, by Lee et al. 61 with the introduction of a ‘photographic
standardization device’ and should be considered for use in future studies. We also recommend
the utilization of a controlled injection device.61 Such a device could provide for more accurate
drug administration, while minimizing the volume required.

31
Conclusion and Future Directions This clinical pilot study presents a unique, minimally invasive surgical approach for
simultaneous treatment of deficient interdental papillae and gingival recession defects (when
both are present) with minimal marginal tissue trauma and post-operative morbidity. Unlike
most investigations in this area, we chose to place an emphasis on the understanding and
quantification of subjective outcome measures from the perspective of both patients and
clinicians. In particular, we showed that, with respect to patient-based-outcome measures, it was
possible to demonstrate statistically significant improvements and even more importantly;
clinically significant improvements. However, the measurement of clinical outcomes is also
critically important when assessing this type of treatment intervention. It was also possible to
demonstrate statistically significant improvements in these outcomes as well. Thus, the collection
and objective interpretation of post-operative data, along with patient-reported outcomes, shows
that this treatment modality produces predictable results that are highly valued by patients. We
hope that in developing this novel surgical treatment we have laid the foundation for longer-term,
more comprehensive and randomized clinical trials, to study and possibly improve this treatment
approach. We hope that in the not too distant future, we will have demonstrated that this surgical
method as well as our approach to evaluation of treatment outcomes an important part of the
armamentarium of clinicians who treat aesthetic gingival problems.
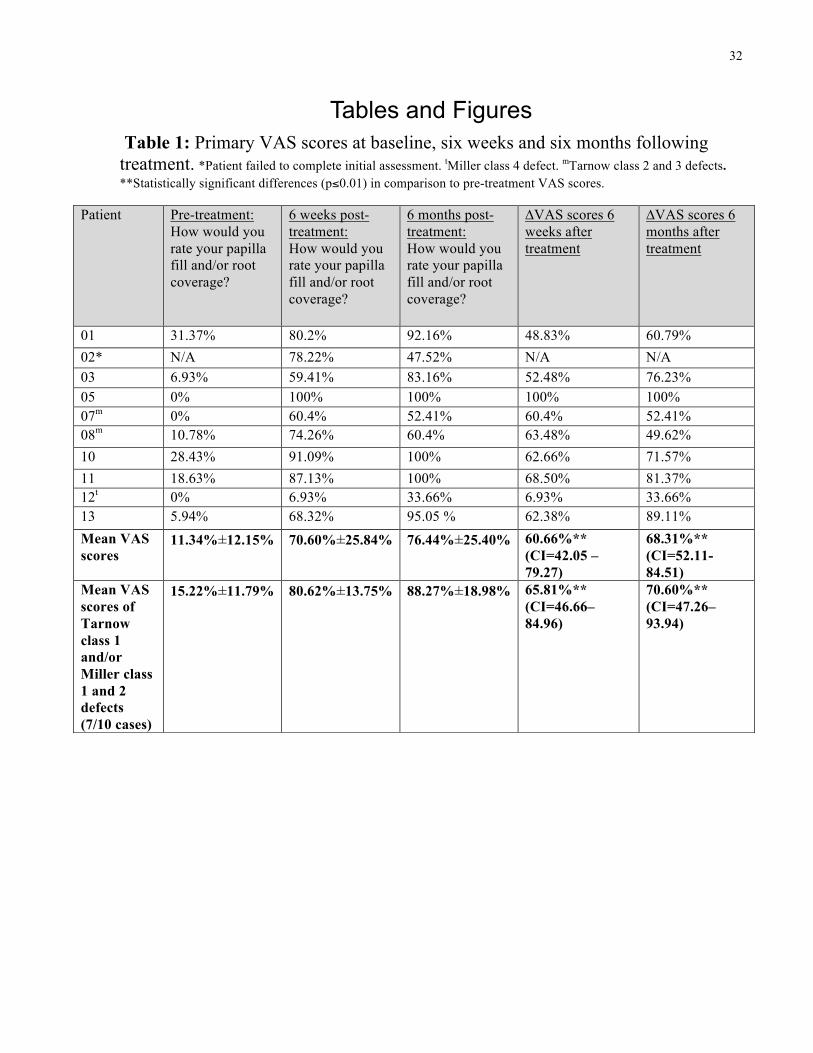
32
Tables and Figures Table 1: Primary VAS scores at baseline, six weeks and six months following treatment. *Patient failed to complete initial assessment. tMiller class 4 defect. mTarnow class 2 and 3 defects. **Statistically significant differences (p≤0.01) in comparison to pre-treatment VAS scores.
Patient Pre-treatment: How would you rate your papilla fill and/or root coverage?
6 weeks post-treatment: How would you rate your papilla fill and/or root coverage?
6 months post-treatment: How would you rate your papilla fill and/or root coverage?
∆VAS scores 6 weeks after treatment
∆VAS scores 6 months after treatment
01 31.37% 80.2% 92.16% 48.83% 60.79% 02* N/A 78.22% 47.52% N/A N/A 03 6.93% 59.41% 83.16% 52.48% 76.23% 05 0% 100% 100% 100% 100% 07m 0% 60.4% 52.41% 60.4% 52.41% 08m 10.78% 74.26% 60.4% 63.48% 49.62% 10 28.43% 91.09% 100% 62.66% 71.57% 11 18.63% 87.13% 100% 68.50% 81.37% 12t 0% 6.93% 33.66% 6.93% 33.66% 13 5.94% 68.32% 95.05 % 62.38% 89.11% Mean VAS scores
11.34%±12.15% 70.60%±25.84% 76.44%±25.40% 60.66%** (CI=42.05 – 79.27)
68.31%** (CI=52.11-84.51)
Mean VAS scores of Tarnow class 1 and/or Miller class 1 and 2 defects (7/10 cases)
15.22%±11.79% 80.62%±13.75% 88.27%±18.98% 65.81%** (CI=46.66– 84.96)
70.60%** (CI=47.26–93.94)
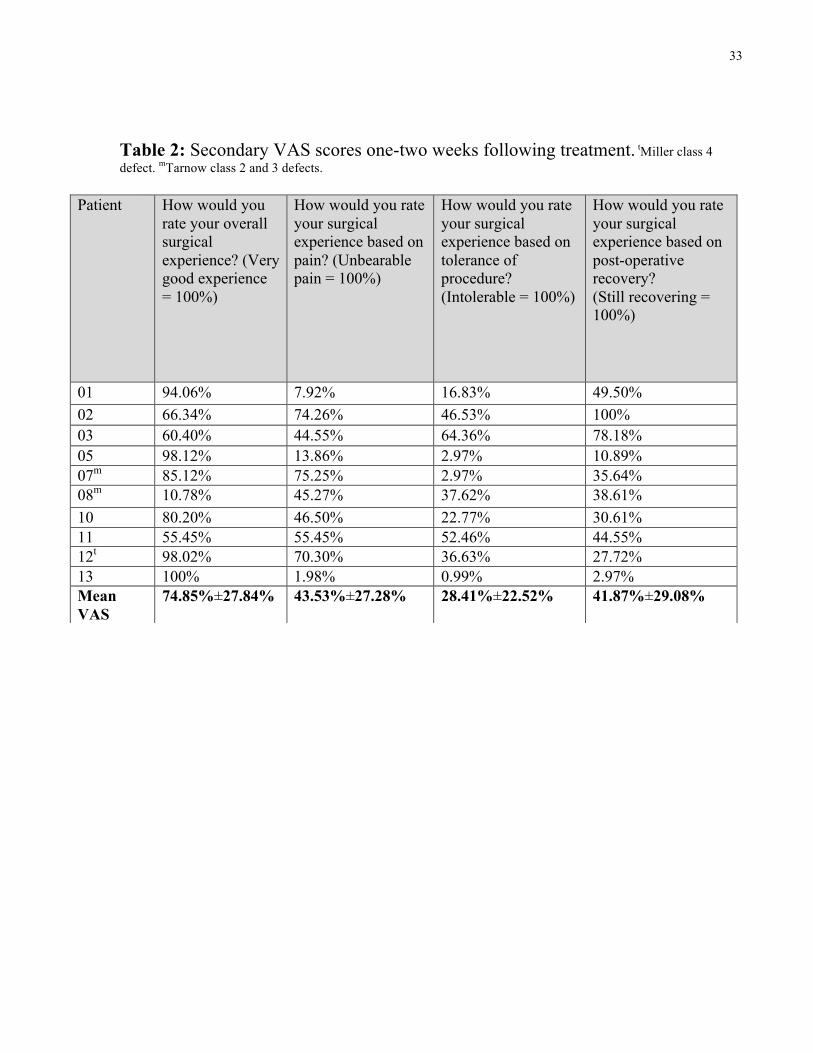
33
Table 2: Secondary VAS scores one-two weeks following treatment. tMiller class 4 defect. mTarnow class 2 and 3 defects.
Patient How would you rate your overall surgical experience? (Very good experience = 100%)
How would you rate your surgical experience based on pain? (Unbearable pain = 100%)
How would you rate your surgical experience based on tolerance of procedure? (Intolerable = 100%)
How would you rate your surgical experience based on post-operative recovery? (Still recovering = 100%)
01 94.06% 7.92% 16.83% 49.50% 02 66.34% 74.26% 46.53% 100% 03 60.40% 44.55% 64.36% 78.18% 05 98.12% 13.86% 2.97% 10.89% 07m 85.12% 75.25% 2.97% 35.64% 08m 10.78% 45.27% 37.62% 38.61% 10 80.20% 46.50% 22.77% 30.61% 11 55.45% 55.45% 52.46% 44.55% 12t 98.02% 70.30% 36.63% 27.72% 13 100% 1.98% 0.99% 2.97% Mean VAS
74.85%±27.84% 43.53%±27.28% 28.41%±22.52% 41.87%±29.08%
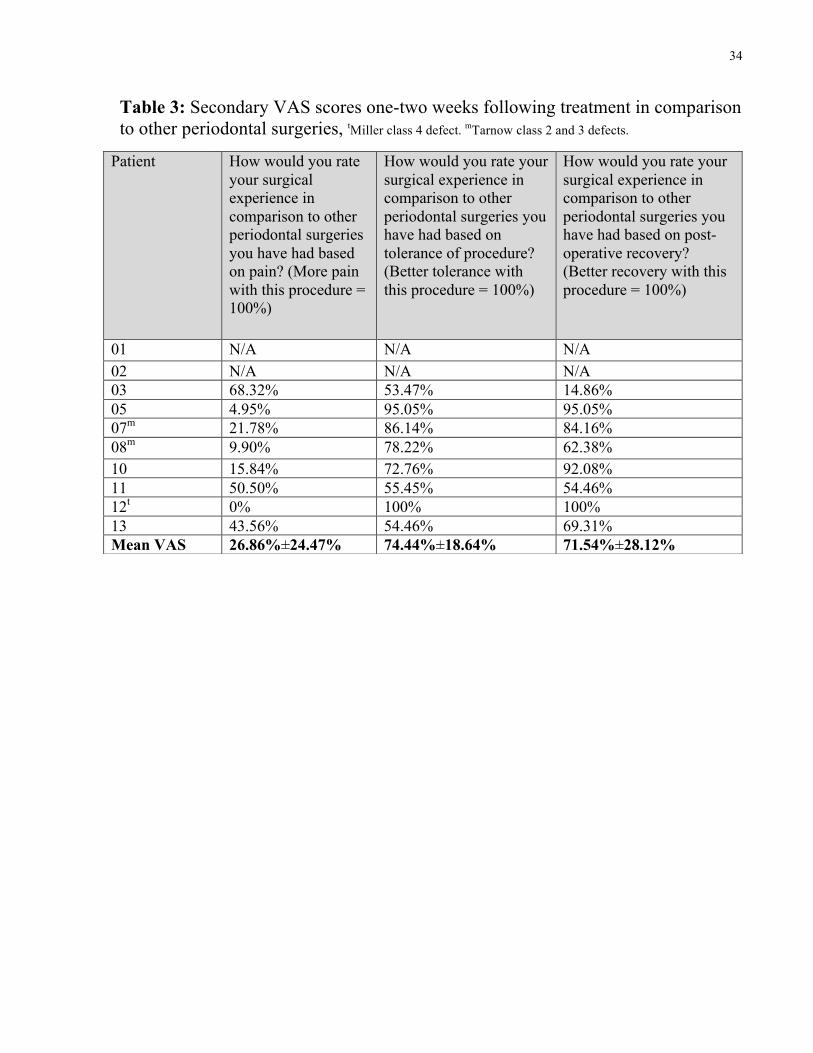
34
Table 3: Secondary VAS scores one-two weeks following treatment in comparison to other periodontal surgeries, tMiller class 4 defect. mTarnow class 2 and 3 defects.
Patient How would you rate your surgical experience in comparison to other periodontal surgeries you have had based on pain? (More pain with this procedure = 100%)
How would you rate your surgical experience in comparison to other periodontal surgeries you have had based on tolerance of procedure? (Better tolerance with this procedure = 100%)
How would you rate your surgical experience in comparison to other periodontal surgeries you have had based on post-operative recovery? (Better recovery with this procedure = 100%)
01 N/A N/A N/A 02 N/A N/A N/A 03 68.32% 53.47% 14.86% 05 4.95% 95.05% 95.05% 07m 21.78% 86.14% 84.16% 08m 9.90% 78.22% 62.38% 10 15.84% 72.76% 92.08% 11 50.50% 55.45% 54.46% 12t 0% 100% 100% 13 43.56% 54.46% 69.31% Mean VAS 26.86%±24.47% 74.44%±18.64% 71.54%±28.12%
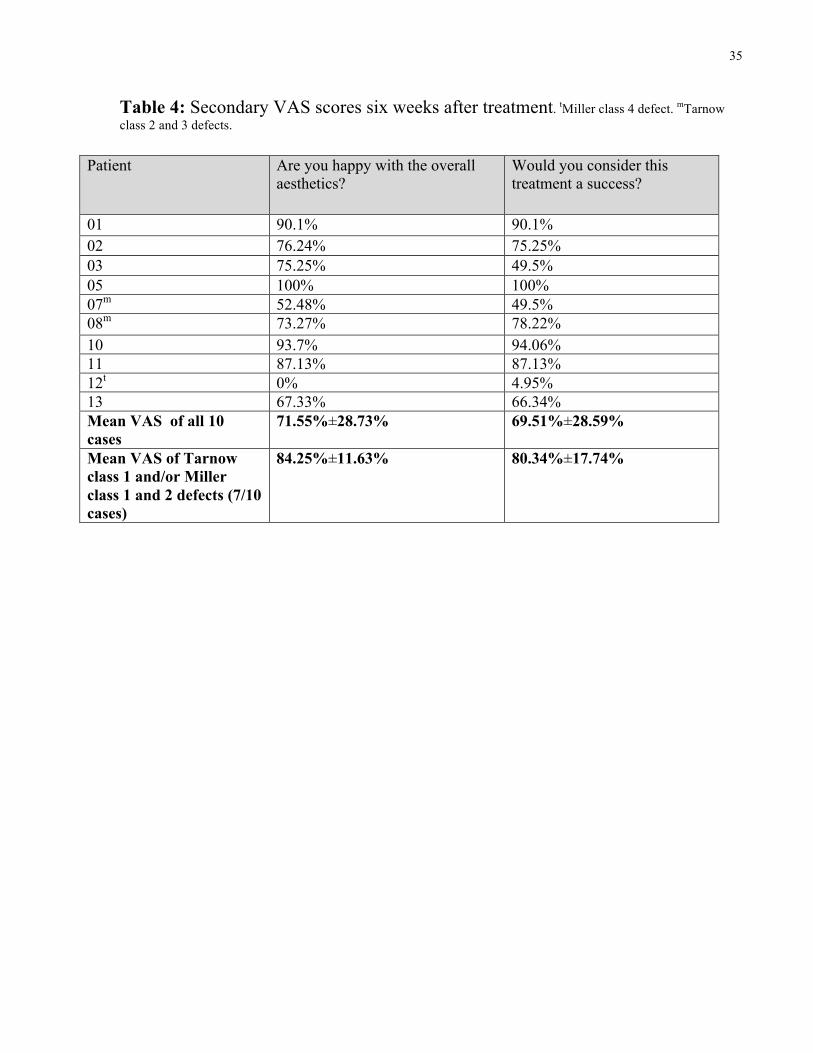
35
Table 4: Secondary VAS scores six weeks after treatment. tMiller class 4 defect. mTarnow class 2 and 3 defects.
Patient Are you happy with the overall aesthetics?
Would you consider this treatment a success?
01 90.1% 90.1% 02 76.24% 75.25% 03 75.25% 49.5% 05 100% 100% 07m 52.48% 49.5% 08m 73.27% 78.22% 10 93.7% 94.06% 11 87.13% 87.13% 12t 0% 4.95% 13 67.33% 66.34% Mean VAS of all 10 cases
71.55%±28.73% 69.51%±28.59%
Mean VAS of Tarnow class 1 and/or Miller class 1 and 2 defects (7/10 cases)
84.25%±11.63% 80.34%±17.74%
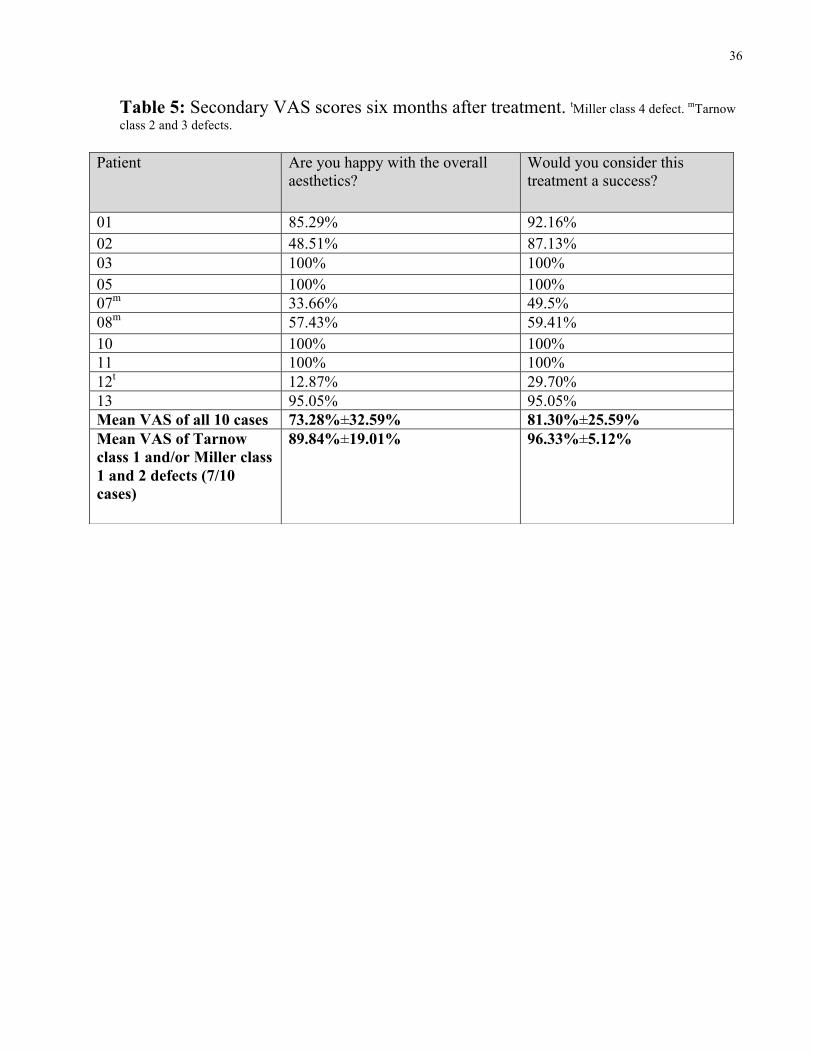
36
Table 5: Secondary VAS scores six months after treatment. tMiller class 4 defect. mTarnow class 2 and 3 defects.
Patient Are you happy with the overall aesthetics?
Would you consider this treatment a success?
01 85.29% 92.16% 02 48.51% 87.13% 03 100% 100% 05 100% 100% 07m 33.66% 49.5% 08m 57.43% 59.41% 10 100% 100% 11 100% 100% 12t 12.87% 29.70% 13 95.05% 95.05% Mean VAS of all 10 cases 73.28%±32.59% 81.30%±25.59% Mean VAS of Tarnow class 1 and/or Miller class 1 and 2 defects (7/10 cases)
89.84%±19.01% 96.33%±5.12%

37
Table 6: VAS scores by a periodontist (1) and periodontal residents (8) following photographic evaluation of treatment outcomes. tMiller class 4 defect. mTarnow class 2 and 3 defects.
Periodontist/Periodontal resident
Pre-treatment: How would you rate this papilla fill and/or root coverage? (mean VAS of all 10 cases)
6 months post-treatment: How would you rate this papilla fill and/or root coverage? (mean VAS of all 10 cases)
∆VAS scores 6 months after treatment: How would you rate this papilla fill and/or root coverage?
6 months post-treatment: Would you consider this treatment a success?
1 35.1% 65.0% 29.9% 63.9% 2 30% 57.5% 27.5% 60.1% 3 44.2% 71.2% 27.0% 76.6% 4 40.8% 65.3% 24.5% 73.7% 5 60.6% 77% 16.4% 80.2% 6 33% 55.2% 22.2% 64.4% 7 34.5% 61.7% 27.2% 62.5% 8 28.1% 62.3% 34.2% 64.8% 9 19.9% 57.4% 37.5% 65.74% Mean VAS 36.2%±11.5% 63.6%±7.01% 27.38%±6.24% 68.0%±7.01%
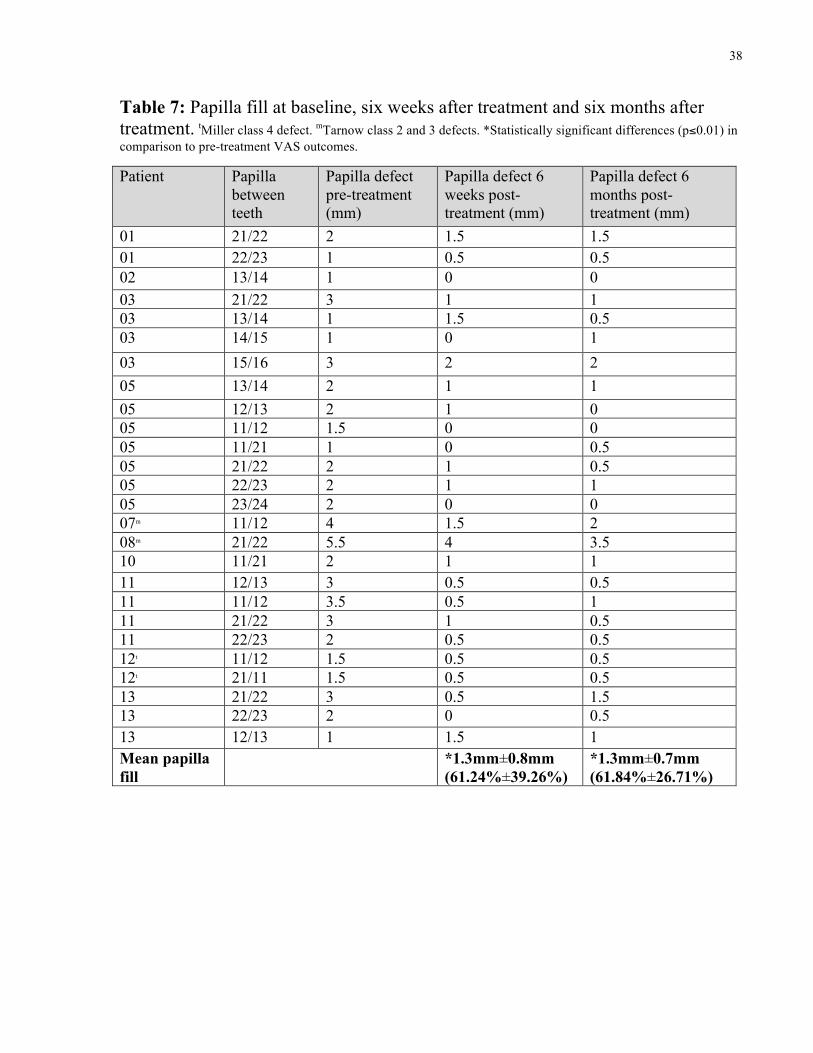
38
Table 7: Papilla fill at baseline, six weeks after treatment and six months after treatment. tMiller class 4 defect. mTarnow class 2 and 3 defects. *Statistically significant differences (p≤0.01) in comparison to pre-treatment VAS outcomes.
Patient Papilla between teeth
Papilla defect pre-treatment (mm)
Papilla defect 6 weeks post-treatment (mm)
Papilla defect 6 months post-treatment (mm)
01 21/22 2 1.5 1.5 01 22/23 1 0.5 0.5 02 13/14 1 0 0 03 21/22 3 1 1 03 13/14 1 1.5 0.5 03 14/15 1 0 1 03 15/16 3 2 2 05 13/14 2 1 1 05 12/13 2 1 0 05 11/12 1.5 0 0 05 11/21 1 0 0.5 05 21/22 2 1 0.5 05 22/23 2 1 1 05 23/24 2 0 0 07m 11/12 4 1.5 2 08m 21/22 5.5 4 3.5 10 11/21 2 1 1 11 12/13 3 0.5 0.5 11 11/12 3.5 0.5 1 11 21/22 3 1 0.5 11 22/23 2 0.5 0.5 12t 11/12 1.5 0.5 0.5 12t 21/11 1.5 0.5 0.5 13 21/22 3 0.5 1.5 13 22/23 2 0 0.5 13 12/13 1 1.5 1 Mean papilla fill
*1.3mm±0.8mm (61.24%±39.26%)
*1.3mm±0.7mm (61.84%±26.71%)
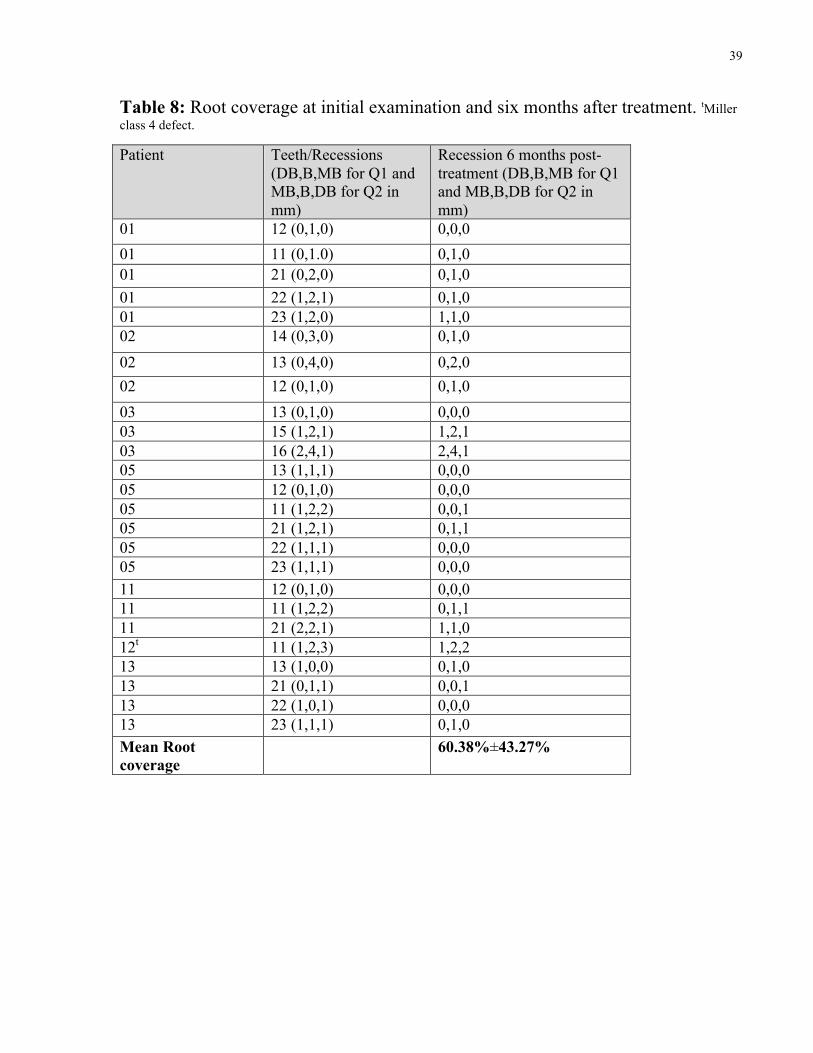
39
Table 8: Root coverage at initial examination and six months after treatment. tMiller class 4 defect.
Patient Teeth/Recessions (DB,B,MB for Q1 and MB,B,DB for Q2 in mm)
Recession 6 months post-treatment (DB,B,MB for Q1 and MB,B,DB for Q2 in mm)
01 12 (0,1,0) 0,0,0 01 11 (0,1.0) 0,1,0 01 21 (0,2,0) 0,1,0 01 22 (1,2,1) 0,1,0 01 23 (1,2,0) 1,1,0 02 14 (0,3,0) 0,1,0 02 13 (0,4,0) 0,2,0 02 12 (0,1,0) 0,1,0 03 13 (0,1,0) 0,0,0 03 15 (1,2,1) 1,2,1 03 16 (2,4,1) 2,4,1 05 13 (1,1,1) 0,0,0 05 12 (0,1,0) 0,0,0 05 11 (1,2,2) 0,0,1 05 21 (1,2,1) 0,1,1 05 22 (1,1,1) 0,0,0 05 23 (1,1,1) 0,0,0 11 12 (0,1,0) 0,0,0 11 11 (1,2,2) 0,1,1 11 21 (2,2,1) 1,1,0 12t 11 (1,2,3) 1,2,2 13 13 (1,0,0) 0,1,0 13 21 (0,1,1) 0,0,1 13 22 (1,0,1) 0,0,0 13 23 (1,1,1) 0,1,0 Mean Root coverage
60.38%±43.27%
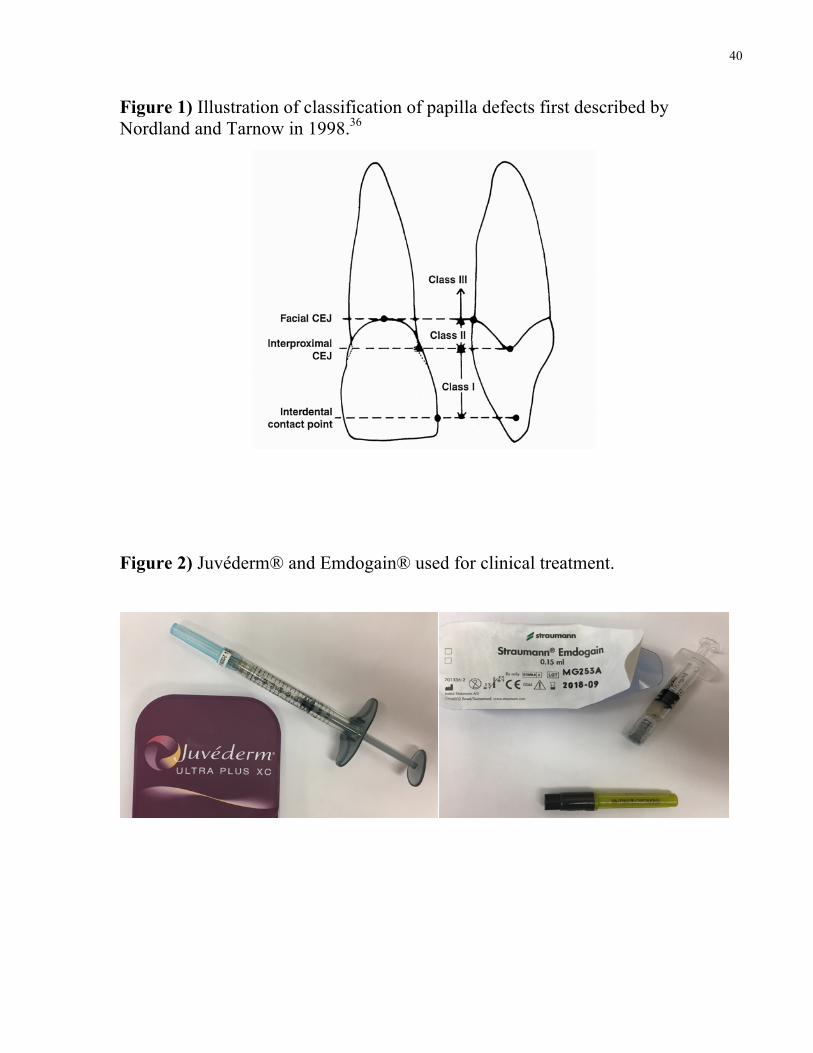
40
Figure 1) Illustration of classification of papilla defects first described by Nordland and Tarnow in 1998.36
Figure 2) Juvéderm® and Emdogain® used for clinical treatment.
41
Figure 3) Surgical protocol
1) Root planing of the exposed root surfaces is performed. A 3-5 mm horizontal incision is made in the alveolar mucosa at a minimum of 2 mm beyond the mucogingival junction. 2-3) Through this access incision the periosteum is released towards the area of recession and under the deficient interdental papilla(e) (interdental papilla remains intact). 4) Juvéderm is administered into the papilla(e) to achieve ideal papillary fill. Straumann PrefGel® is used to condition the exposed cementum followed by placement of EMD and coronal repositioning of the gingiva and alveolar mucosa over the area of recession. 5) Histoacryl® is used to seal free gingival margins surrounding the papilla(e) (not used if treating papilla(e) defects in combination with recession). A sling suture is placed to maintain coronal advancement with 6.0 polypropylene. Additional injections with Juvéderm into the interdental papilla(e) are performed as needed.
1)
3 4 5
2)
3) 4) 5)

42
Figure 4) Six month postoperative outcomes in the treatment of isolated papilla defects and gingival recession in combination with papilla deficiencies. Case 03
Preoperative Six months postoperative
Case 05
Preoperative Six months postoperative
Case 11
Case 11

43
Case 11 Preoperative Six months postoperative
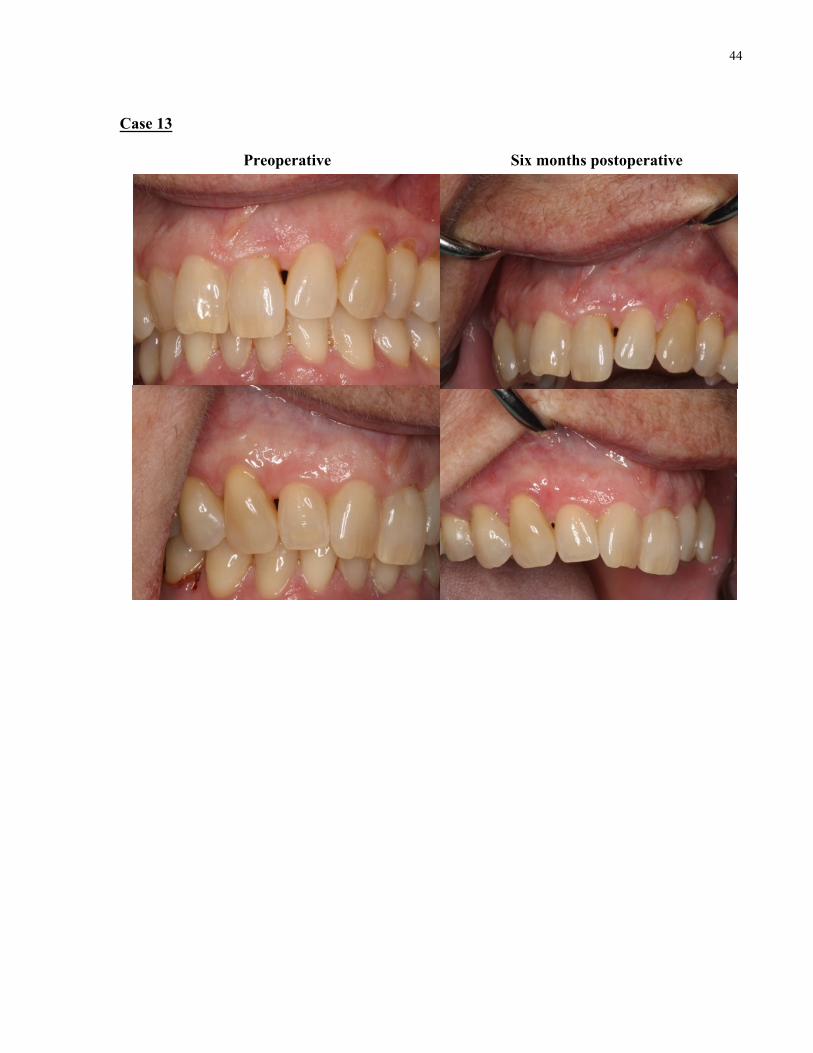
44
Case 13
Preoperative Six months postoperative

45
Appendices Appendix A: Medical Questionnaire
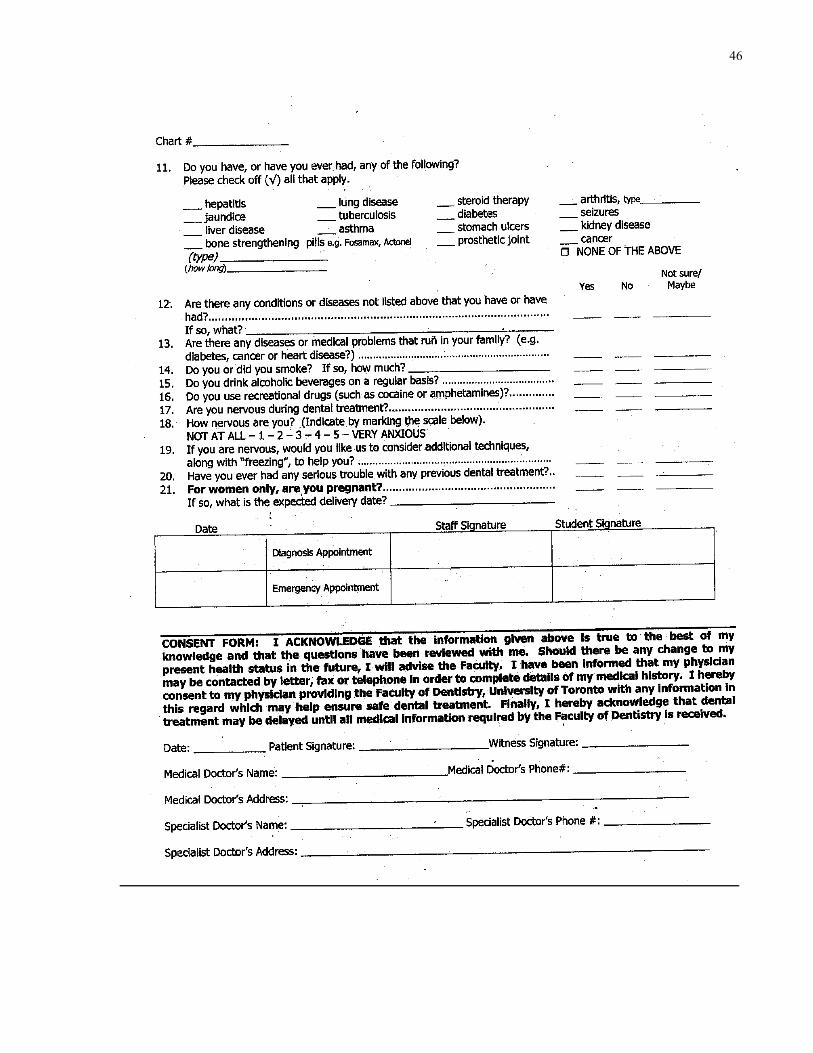
46
47
Appendix B: Consent Meeting Script/Interview Guide CONSENT MEETING SCRIPT FOR RESEARCH PARTICIPANTS
AT THE UNIVERSITY OF TORONTO Individuals who wish to participate and are selected for the clinical trial will be asked to sign an informed consent (see appendix E). A sample consent meeting script has been provided below to help simulate the process in which informed consent will be obtained. Examiner: Welcome, my name is Dr. Stephen Spano and I am a graduate periodontics resident here in the Graduate Program in Periodontology, within the Faculty of Dentistry, University of Toronto. You have been selected to be a potential participant in a clinical trial that I am conducting in the graduate periodontics clinic for my Masters’ project. With your permission, I would like to inform you of the trial in detail. You can stop me at any point if you have any questions. The purpose of our experiment is to provide patients with the option of restoring the original position of their receding gums below and/or in between their teeth through a new conservative surgical technique we have developed. It is our intent that this novel minimally invasive surgery will provide you with effective treatment results in addition to minimal discomfort and optimal healing time. It is also our hope this study will allow for an effective treatment alternative for future clinicians to provide to their patients. Questions so far? Participant: Can you please explain further the treatment I will be receiving? Examiner: Of course I can. This treatment will be based on a minor surgical procedure that creates a tiny hole in your gums in the area of your gum defect followed by the placement of a natural based dermal filler called Juvéderm® as well as a protein factor called Emdogain®. Dermal fillers are materials composed of a natural protein and sugar compound found in human skin. They have been used extensively in medicine for procedures involving lip augmentation as well as elimination of facial folds, facial wrinkling and undesirable facial lines. Emdogain® is a natural material that enhances the regeneration of your gums and will be placed over the exposed root surfaces in areas where you have recession. It also assists in post-operative healing and minimizes patient’s recovery time. Through the use of these two materials we hope to achieve root coverage and fill papilla deficiencies. Root coverage is defined as the restoration of the receded gums to their original position over the entire root surface. Papilla deficiencies are spaces that occur between teeth as a result of receding gums. Following the insertion of the dermal filler and Emdogain, stitches will be placed to hold the tissues and material in position during healing. We will then follow you closely over a 6-month period to evaluate the success of the surgical procedure. Participant: Is this surgery required? Examiner: It is always your choice whether you wish to proceed with treatment or not. The main reasons for undergoing this procedure are to improve the aesthetics of the gingival tissues around your teeth and in some cases of where your roots may be exposed, for the management of dentinal hypersensitivity. It is our hope that this surgery will address both these issues by providing root coverage (restore the gums that have receded and exposed the roots of your teeth) and/or papilla regeneration (restore the position of the gums in between your teeth).
48
Participant: What other options do I have? Examiner: Unfortunately, there is currently no predictable way to recreate the gums between your teeth to fill papilla deficiencies. However, there are a variety of different treatments available for receding gums. These techniques can be very invasive and painful. Further, the most predictable treatment options require two separate surgical sites (one for the recipient site and one on the roof of your mouth to obtain tissue to place over the site with the defect). As previously stated, with our treatment we would not have to obtain additional tissue from the roof of your mouth, significantly decreasing post-operative pain. All alternative treatment options are highlighted below. In different situations some treatment options are better than others. All involve similar risks and sequelae. This includes pain, bruising, bleeding, swelling, infection, temporary or permanent dental sensitivity to heat or cold and treatment failure. During your treatment at the Faculty of Dentistry you will be provided with contact information for any questions or emergencies and routine post-operative appointments to follow-up and confirm the site is healing accordingly. Treatment options for gum recession
a. Gum graft – this involves taking tissue from the roof of your mouth and is the standard procedure offered for the treatment of gum recession o Advantages
§ Most predictable surgery for root coverage o Disadvantages
§ requires a donor site (second surgical site) to obtain the gum tissue 2. Moving of your remaining gums in the area over the exposed root surface
o Advantages § Only one surgical site
o Disadvantages § Can only be performed in specific circumstances § No new gum tissue provided
b. Gum from a “bottle” o Advantages
§ only one surgical site o Disadvantages
§ Unpredictable long term root coverage § Donated human tissue
4. No treatment o Advantages
§ No surgery o Disadvantages
§ Recession likely to progress § Ongoing and/or worsening dental sensitivity § Chronic inflammation
Participant: Are dermal fillers safe? Examiner: The dermal filler we will be using is a very safe material. The Food and Drug Administration in the USA as well as the regulatory factions in Canada have approved the use

49
and safety of dermal fillers for over a decade. The utilization of dermal fillers in plastic surgery and dermatology is now a very common, effective and long-standing therapeutic modality for treatment of a variety of different aesthetic problems related to the skin. There have also been studies to prove their compatibility inside the mouth. Participant: What if I do not want to participate. Will this affect my current treatment here? Examiner: Not at all! There will be no consequences if you choose not to participate or if you agree to participate and change your mind later on. The quality of your care here at the Faculty of Dentistry, University of Toronto, will not be affected by your decision. Participant: How many appointments will be required of me? Examiner: Including today, you will require another appointment for the surgery and 3 to 4 follow-up appointments. The surgical appointment will be about an hour and the follow-up appointments will range from 15-45 minutes. At some of these follow-up appointments we will be taking photographs and will be asking you to complete simple questionnaires regarding your surgical experience. Participant: Will I get anything for participating aside from the surgery? Examiner: Unfortunately, there is no monetary compensation for participating in the study. The treatment of the surgical site will be free of charge including any required follow-up appointments. There will be a $100.00 fee charged to the patient prior to treatment. This will be reimbursed in full at the 6-month follow-up after treatment. If you drop out of the study prior to completion no compensation will be provided. Furthermore, due the limited finances provided for this study, no compensation can be provided in the event of a personal injury or unexpected complication that forces the participant to withdraw from the study. You will also be shown proper oral hygiene techniques and provided with free oral hygiene supplies. Participant: What guarantee do I have that this treatment will work? Examiner: Unfortunately, this new treatment that has never been attempted before. There is no research on the success rates for this type of therapy. However, the clinical protocol and approach we have developed has been reviewed and is based on sound periodontal principles and surgical techniques. Nonetheless, it is important to keep in mind that this is an innovative surgical technique and I cannot guarantee it will be successful. If treatment does fail, the condition becomes worse, or if you develop a complication such as an infection, the cost of additional treatment or medication through the Faculty of Dentistry or an outside clinic will not be covered. It is very unlikely that the condition worsens post-surgery. The risk for this is minimal and would be equal to that of any type of root coverage procedure whether or not dermal filler is used. In fact, on the basis of our understanding relating to how these treatments work, it is highly probable in our opinion that there will actually be reduced risk for worsening of a patient’s condition. Participant: How much is this going to hurt and how long will it take me to recover? Examiner: This is a very minor surgical procedure. It is much less invasive and traumatic then a tooth extraction. If you have had any previous gum grafting surgery this would likely be less uncomfortable than that as well. However, everyone responds differently to surgery and post-operative pain. You will be followed up with carefully to confirm normal healing and for the management of any post-op complications that may arise. As with all dental surgeries patients

50
may experience some post-operative discomfort, bruising, swelling and bleeding. Post-operative instructions will be reviewed in detail with you to minimize any of these potential complications. An emergency contact number will be provided as well. Participant: Who will have access to my personal information? Examiner: Participant’s records and consent forms will be kept in locked filing cabinets at the University of Toronto’s dental clinic. Only myself and the other investigators in this study will have access to your information. Photographs will be immediately erased from the digital camera and computer the day of and stored on an encryption protected USB flash drive. All electronic information will be saved and stored on the encryption protected USB flash drive as well. This information will be uploaded and analyzed only on computers linked to the Faculty of Dentistry’s secured server. However, the information will only be stored on the USB memory device and not on the computer server. The USB memory device will be kept in a locked desk drawer in a locked room. Participant: That’s all the questions I have for now. I would be interested in participating. However, are you available if I have any other questions? Examiner: I will now be handing you an information letter (see appendix C) that includes all the things we just spoke about. As you look through them, feel free to contact me if you have any further questions. Participant: Thank you Dr. Spano. Examiner: You are very welcome. At this time do you have any questions regarding the trial? Do you have any questions regarding what we expect from the participants in the trial? Do you have any questions regarding your option not to participate? Participant: No, you explained everything quite clearly. Examiner: Great! I will now ask you to take your time and read through this consent form (see appendix D). If you are okay with everything it outlines please sign where indicated. I will keep this in your chart. If you wish, you can have a copy of the signed consent form as well. Please keep in mind the next appointment will be for your surgery. Here is some post-operative instructions you can review that will be important for you to follow after treatment. I will provide you with the same instructions on the day of the surgery as well.

51
Appendix C: Information Letter for Research Participants INFORMATION LETTER FOR RESEARCH PARTICIPANTS
AT THE UNIVERSITY OF TORONTO
Title of research project: The use of dermal filler in root coverage and the restoration of
papilla deficiencies through a conservative surgical approach
Introduction Thank you for considering taking part in our research. This is a Masters research project being conducted by the periodontal resident Dr. Stephen Spano in the Graduate Program in Periodontology, within the Faculty of Dentistry, University of Toronto. The information below will help explain our study, the treatment you will be electing to receive and the associated risks and benefits to you. It is up to you to decide whether you would like to participate in the clinical trial. Please make sure that all of your questions are answered before you provide consent. Background Healthy gums are the foundation to optimal oral health and are very important in the overall aesthetics of your teeth. Abnormal brushing techniques or gum disease can cause a loss or a change in the appearance of your gums. Many patients have receding gums exposing the roots of their teeth and the spaces between their teeth. This can cause outstanding grief due to the resultant unpleasant appearance and increased tooth sensitivity. These spaces that occur between the teeth as a result of gum recession are called papilla deficiencies. Treatment that involves the use of a material to cover the exposed root surface and restore the original position of the receded gums is termed root coverage. Unfortunately, patients frequently undergo multiple invasive surgeries to obtain root coverage and fix papilla deficiencies that require extensive healing time. Furthermore, in many cases no predictable treatment is even available. Thus, using a new conservative surgical technique we have developed, it is our intent to provide you with a minimally invasive surgical procedure with little discomfort, optimal healing time and effective results. Purpose of the Research: The purpose of our research is to provide patients with the option to restore the original position of their receding gums through a new conservative surgical technique. It is ultimately our hope this study will allow for an effective treatment alternative for future clinicians to provide to their patients. This treatment will consist of making a tiny hole in your gums and placing dermal filler underneath them to bulk up and fill the gums around your teeth. These dermal fillers are biodegradable materials composed of a natural complex of protein and sugar found in human skin. They have been used extensively in medicine for procedures involving lip augmentation as well as eliminating facial folds, facial wrinkling and undesirable facial lines. The dermal filler we will be using is called Juvéderm® and is a very safe material. Previous studies have shown mild success in using dermal fillers in restoring the natural appearance of gums and it is our hope that our advanced method in dermal filler placement will allow for even greater improvements in root coverage and gum restoration.

52
Description of the Research: This research clinical plot trial will be composed of about 15 patients from the graduate periodontics clinic. Patients will be selected on a wide range of medical and clinical criteria. Those who are acceptable candidates will be asked to return and participate in the study. Following surgery we will follow you closely over a 6-month period to evaluate the success of the treatment. Participants’ Duties Participants will undergo an initial examination, surgery and multiple follow-up appointments. Please review the information below for a detailed explanation of each appointment: Appointment 1) – 45-60 minutes
• Review of medical history, initial oral examination, informed consent, and pre-operative photographs. Following an initial examination at the Faculty of Dentistry, patients that meet the inclusion criteria will be invited back to participate in the study and asked to complete some quick pre-operative assessments.
Appointment 2) - 120 minutes
• Patient’s undergo minor surgery to restore area of receding gums. This includes the administration of dental freezing, incision of the gums and placement of the dermal filler. Patients will also receive a few stitches in the area to hold the gums and materials in place during the healing process. A thorough review of post-operative instructions verbally and written will be provided.
Appointment 3) – 30 minutes
• A 1-week follow-up will be scheduled to assess healing of surgical site and review oral hygiene as well as any patient questions or concerns. Patients will be asked to complete some post-operative assessments. Post-operative measurements and photographs will be taken.
Appointment 4) – 30 minutes
• 6-week follow-up to assess healing, review oral hygiene and address patient questions or concerns. Data will be collected through photography and specific assessments the participants will be asked to complete. Several different clinical measurements will be taken of the gums and teeth in the treated area.
Appointment 5) – 30 minutes
• 6-month follow-up to assess healing, review oral hygiene and address patient questions or concerns. Data will be collected through photography and specific assessments the participants must complete. Several different clinical measurements will be taken of the gums and teeth in the treatment area.
Appointment 6)
• Patients may be asked for an additional appointment to complete any outstanding clinical assessments.

53
Potential Harms or Injuries: This is a minor surgical procedure. As with all dental surgeries patients may experience some post-operative discomfort, bruising, swelling and bleeding. Post-operative instructions will be reviewed in detail to minimize any of these potential complications. An emergency contact number will also be provided. The Food and Drug Administration in the USA as well as the regulatory factions in Canada have approved the use and safety of dermal fillers for over a decade. Further, the utilization of dermal fillers in plastic surgery and dermatology is now a very common, effective and long-standing therapeutic modality for treatment of a variety of different aesthetic problems related to the skin. There have also been studies to prove their compatibility inside the mouth. It is important to understand that this is an innovative surgical technique that has never been tested before. However, the clinical protocol and approach we have developed has been reviewed and is simply a modification of current and sound periodontal principles and surgical techniques. Considering dermal fillers do degrade over time please understand it will be impossible to obtain long-term stability. However, if significant results are obtained this may allow for an effective treatment alternative for clinicians and patients that we estimate would require simple and much less invasive ongoing 2-3-year maintenance visits to essentially “touch-up” the affected area(s). Confidentiality: All personal information including participants’ records, consent forms and questionnaires will be kept in the patient’s dental chart at the Faculty of Dentistry. Photographs will be immediately erased from the digital camera and computer and stored on an encryption protected USB flash drive. All electronic information will be saved and stored on the encryption protected USB flash drive as well. This information will be uploaded and analyzed only on computers linked to the Faculty of Dentistry’s secured server. However, the information will be stored only on the USB memory device and not on the computer server. The USB memory device will be kept in a locked desk drawer in a locked room. We will not release or publish any information that reveals the participants' identity. All patient identifying information will be removed during clinician and participant assessments of pre- and post-operative photographed treatment results. All personal records obtained will be securely stored for 25 years and then shredded and erased. Participation and Compensation: Participation in this study is voluntary and no monetary compensation will be offered. However, other forms of compensation include: 1) All examinations, treatment and follow-up appointments will be free of charge. 2) Proper oral hygiene instruction and free oral hygiene supplies will be given to all
participants. 3) There will be a $100.00 fee charged to the patient prior to treatment. This will be
reimbursed in full at the 6-month follow-up after treatment. If you drop out of the study prior to completion no compensation will be provided.
Participation in this study may contribute to the development of new treatments or other events that may have commercial value. Your participation will not entitle you or other trial participants to a share in any future economic benefits. Furthermore, due the limited finances provided for this study, no compensation can be provided in the event of a personal injury or unexpected complication that forces the participant to withdraw from the study. If treatment does fail, the condition becomes worse, or if you develop a complication such as an infection, the cost of additional treatment or medication through the Faculty of Dentistry or an outside clinic will not be covered. However, it is very unlikely that the condition worsens post-surgery.

54
The risk for this is minimal and equal to that of any root coverage procedure whether or not dermal filler is used. In fact, on the basis of our understanding relating to how these treatments work, it is highly probable in our opinion that there will actually be reduced risk for worsening of a patient’s condition. Withdrawal Participants who are not interested in undergoing treatment are not obliged to continue with the study and can leave at any time. We strongly encourage you to consider this prior to undergoing surgery. However, patients must understand that once treatment is provided we highly recommend attending all follow-up appointments to confirm the site of surgery is healing normally and ask you kindly to complete the simple post-operative assessments we will be requesting from you.

55
Appendix D: Eligibility Screening Consent Form ELIGIBILITY SCREENING CONSENT FORM FOR PATIENTS
AT THE UNIVERSITY OF TORONTO The use of dermal filler in root coverage and the restoration of papilla deficiencies through a
conservative surgical approach
Eligibility Consent:
1) The study has been explained to me and I am aware this research is part of a Masters project. This
Masters research project is being conducted by the periodontal resident Dr. Stephen Spano in the
Graduate Program in Periodontology, within the Faculty of Dentistry, University of Toronto.
2) I understand that I have the right not to participate and the right to stop at any time. The decision about
whether or not to participate will not affect my other dental care at the Faculty of Dentistry.
3) I understand and accept that by signing this form I am only providing consent for a consultation that will
involve further discussion with Dr. Spano of his research and the completion of medical and research
questionnaire forms. I am also providing consent for a detailed clinical examination of the status of my
teeth and gums as well as intra-oral photographs.
4) At this appointment I understand I am not committed to undergoing any treatment proposed by Dr. Spano.
5) I realize that I am free now, and in the future, to ask any questions or request further consultations about
the research study. The costs involved in obtaining a consult or second opinion regarding the treatment
required outside of the Faculty of Dentistry will not be covered.
6) I am aware that researchers will use data from my dental chart, including demographics, a detailed
medical history, social history and periodontal status and diagnosis. I understand photographs will also be
taken and that all data obtained will be used for research purposes only. I recognize that no information
that would identify me will be released or printed. I understand that some of the information collected
may be used in hopes of publication or public presentations even if I do not proceed with treatment and
that my personal information will remain protected. I agree to release and exchange of my dental/medical
information between the investigators of this study only.
7) I was given the opportunity to ask questions and my questions have been answered to my satisfaction. I
have been provided with adequate information and wish to be screened for eligibility for this research
study.
I, ______________________(Participant), hereby consent to participate. Date:______________
Signature: ___________________
56
Name of person who obtained consent _________________________ Date:______________
Signature of person who obtained consent ___________________________ Date:______________

57
Appendix E: Treatment Consent Form
TREATMENT CONSENT FORM FOR PATIENTS AT THE UNIVERSITY OF TORONTO
The use of dermal filler in root coverage and the restoration of papilla deficiencies through a conservative surgical approach
Consent:
By signing this form:
1) The study has been explained to me and I am aware this research is part of a Masters project. This Masters research
project is being conducted by the periodontal resident Dr. Stephen Spano in the Graduate Program in
Periodontology, within the Faculty of Dentistry, University of Toronto.
2) I understand that I have the right not to participate and the right to stop at any time during the research study. I am
under no obligation to participate and free to withdraw without any consequences. Further, the decision about
whether or not to participate will not affect any other dental care I may have at the Faculty of Dentistry.
3) I realize that I am free now, and in the future, to ask any questions about the study. The costs involved in obtaining a
consult or second opinion regarding the treatment required outside of the Faculty of Dentistry will not be covered.
4) I understand the written and verbal information provided to me by Dr. Spano. The normal course of treatment,
expected outcomes, associated risks and complications have been thoroughly explained to me. The nature and
purpose of the treatment, possible treatment alternatives with their associated benefits and risks, and the potential
complications have been thoroughly explained to me in a manner that I understand. I am aware the risks and
complications resulting from this procedure may include but are not limited to:
• Pain, bruising, swelling, bleeding and infection
• Damage to adjacent teeth, fillings or other dental restorations
• Treatment failure
• Teeth may become temporarily or permanently sensitive to heat, cold or sweets
• Several days of at-home recovery may be required
5) I recognize it is essential for me to follow all the post-operative instructions highlighted below after my surgery:
• No rinsing, spitting or drinking with a straw for 24 hours to prevent bleeding. • Pain and swelling: Pain and occasional swelling may occur and is normal. Pain peaks after a few days
and can persist for one week. Pain is normally managed with acetaminophen (Tylenol®) and/or ibuprofen (Advil®). Only use the pain medication as needed and instructed by the clinician.
Note: It is normal when the dental freezing wears off to have some additional discomfort. Use the pain medication as needed to help manage the increase in pain at this time.
• Bleeding: A small amount of bleeding is normal. If there is considerable bleeding do not spit or rinse repeatedly. Very gently take a piece of sterile gauze or tea bag and hold it over the area for 20-30 minutes (do not talk or release the pressure). If the bleeding persists contact the office.
• Mouth Rinses: You will be provided with a germ killing mouth rinse called chlorhexidine to reduce the risk of post-operative infection. Begin rinsing the day after surgery as instructed. Do not rinse the first day of surgery as this can cause additional bleeding.
• Brushing: Maintaining good oral hygiene will minimize the risk of infection. Provided there is no bleeding resume gentle brushing of all areas except the site of surgery the following day. Avoid
58
brushing over the surgical site for 3-5 days, then brush very gently after meals to remove any food debris that accumulates. Normal brushing can resume 2 weeks following surgery.
• Antibiotics: An antibiotic is normally not required. If prescribed, finish it all as directed. • Sutures: Sutures have been placed and will dissolve on their own in 7-14 days. Do not touch or play
with the sutures. • Smoking: No smoking of any kind should take place for two weeks following surgery. • Diet: A soft diet is recommended for the first 5 days (mashed potatoes, soups, yogurt, etc.) following
surgery. Normal diet can usually resume in one week. • Infection: If the site becomes very swollen, extremely painful with or without a bad taste call the
periodontal office.
6) I accept, understand and agree to follow the instructions provided to me before and after the procedure.
7) Due the limited finances provided for this study, I recognize that in the event of a personal injury or unexpected
complication that forces me to withdraw from the study no compensation can be provided. I also understand there is
a $100.00 fee prior to treatment. This is reimbursed in full at the 6-month follow-up after treatment.
8) I understand if treatment fails, the cost of additional treatment through the Faculty of Dentistry or an outside clinic
will not be covered.
9) By consenting to treatment I have not waived any rights to legal recourse in the event of research-related
harm.
10) I was given the opportunity to ask questions and my questions have been answered to my satisfaction. I have been
provided with adequate information and wish to proceed with treatment.
I, (Participant), hereby consent to participate. Date:______________
Signature: ___________________
Participants’ data collection
1) I am aware that researchers will use data from my dental chart, including demographics, a detailed medical history,
social history and periodontal status and diagnosis. I understand photographs and/or video will also be taken and that
all data obtained will be used for research purposes only. I recognize that no information that would identify me will
be released or printed. I understand that some of the information collected may be used in hopes of publication or
public presentations and that my personal information will remain protected. I agree to release and exchange of my
dental/medical information between the investigators of this study only.
Signature: ___________________
Name of person who obtained consent Date:______________
Signature of person who obtained consent Date:______________
59
Appendix F: Postoperative Instructions
Instructions Following Surgery
1. No rinsing, spitting or drinking with a straw for 24 hours to prevent bleeding. 2. Pain and swelling: Pain and occasional swelling may occur and is normal. Pain peaks after a few
days and can persist for one week. Pain is normally managed with acetaminophen (Tylenol®) and/or ibuprofen (Advil®). Only use the pain medication as needed and instructed by the clinician.
Note: It is normal when the dental freezing wears off to have some additional discomfort. Use the pain medication as needed to help manage the increase in pain at this time.
3. Bleeding: A small amount of bleeding is normal. If there is considerable bleeding do not spit or rinse repeatedly. Very gently take a piece of sterile gauze or tea bag and hold it over the area for 20-30 minutes (do not talk or release the pressure). If the bleeding persists contact the office.
4. Mouth Rinses: You will be provided with a germ killing mouth rinse called chlorhexidine to reduce the risk of post-operative infection. Begin rinsing the day after surgery as instructed. Do not rinse the first day of surgery as this can cause additional bleeding.
5. Brushing: Maintaining good oral hygiene will minimize the risk of infection. Provided there is no bleeding resume gentle brushing of all areas except the site of surgery the following day. Avoid brushing over the surgical site for 3-5 days, then brush very gently after meals to remove any food debris that accumulates. Normal brushing can resume 2 weeks following surgery.
6. Antibiotics: An antibiotic is normally not required. If prescribed, finish it all as directed. 7. Sutures: Sutures have been placed and will dissolve on their own in 7-14 days. Do not touch or
play with the sutures. 8. Smoking: No smoking of any kind should take place for two weeks following surgery. 9. Diet: A soft diet is recommended for the first 5 days (mashed potatoes, soups, yogurt, etc.)
following surgery. Normal diet can usually resume in one week. 10. Infection: If the site becomes very swollen, extremely painful with or without a bad taste call the
periodontal office.
For emergencies call our periodontal office
60
Appendix G: Case Report Form
CASE REPORT FORM
Clinical Pilot Trial: The use of dermal filler in root coverage and the restoration of papilla deficiencies through a
conservative surgical approach
Investigator: Dr. Stephen Spano
Case # |__|__|
61
SCREENING VISIT (Initial Consultation and Assessment)
Date of Visit: |__|__||__|__||__|__|__|__| Day / Month/ Year
Written Informed Date obtained: Consent: |__|__||__|__||__|__|__ |__| (Day / Month /
Year)
Demographic Year of Birth: Sex: Details: |__|__|__|__| Male ___ Female ___
Inclusion Criteria Over 18 years of age
Yes
No
Informed consent obtained. Patient is willing to proceed with all treatment and follow-up appointments.
Yes
No
Presence of localized areas of recession and/or interdental papilla loss
Yes
No
No contraindications to periodontal surgery
Yes
No
Exclusion criteria Active periodontal disease
Yes
No
Presence of gingivitis in the proposed surgical area
Yes
No
Pregnant
Yes
No
American Society of Anaesthesiologists’ physical status classification of 3 or greater Yes
No
Smokers or patients with a history of smoking in the past 10 years
Yes
No
62
Recession and/or Papilla Defects
Pre-Operative Clinical Measurements
Clinical attachment loss (CAL)
_____mm
Recession from cemento-enamel junction (CEJ) to free gingival margin (FGM)
_____mm
Tip of papilla to interdental contact point
_____mm
Recession
Yes No Class 1 Teeth:
Class 2 Teeth:
Class 3 Teeth:
Papilla Deficiencies
Yes No Class 1 Teeth:
Class 2 Teeth:
Recessions with Papilla Deficiencies
Yes No Teeth:

63
Pre-Operative Practice Visual Analogue Scale (VAS) Assessment Black Box Series 1) How black/dark is this square?
Not at all____________________________________ Extremely 2) How black/dark is this square?
Not at all Extremely 3) How black/dark is this square?
Not at all Extremely 4) How black/dark is this square?
Not at all Extremely
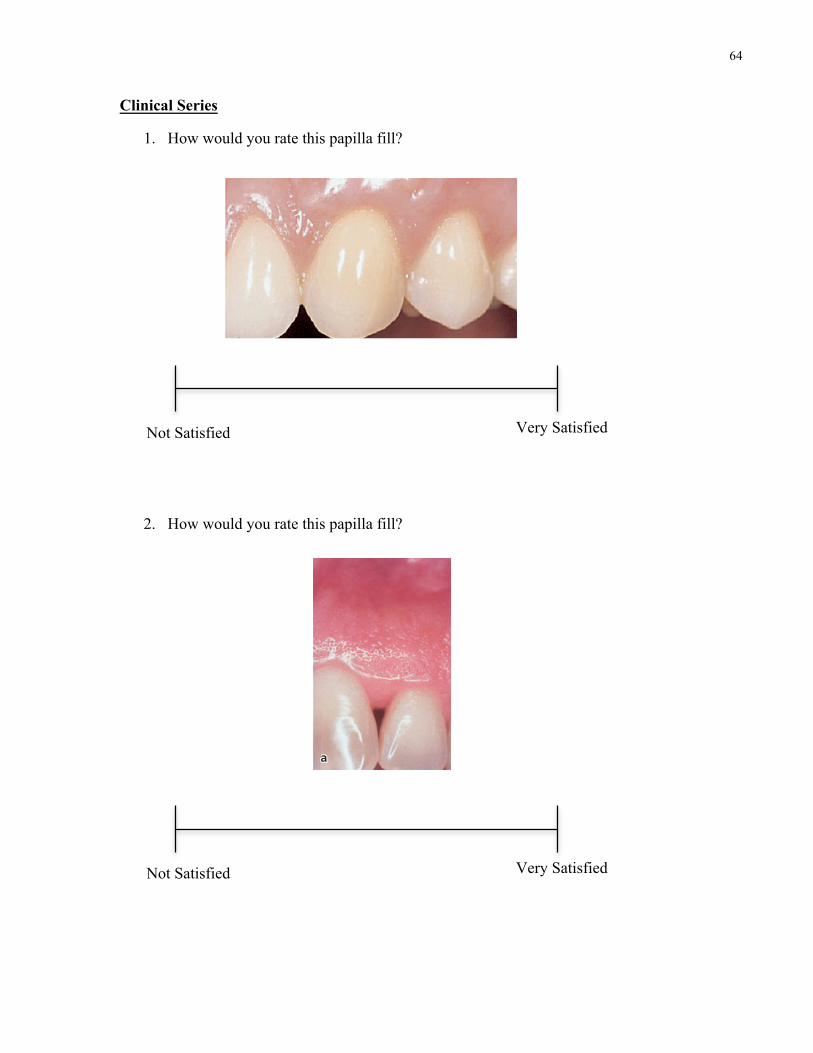
64
Clinical Series
1. How would you rate this papilla fill?
2. How would you rate this papilla fill?
Not Satisfied Very Satisfied
Not Satisfied Very Satisfied
974 Reconstructive Therapy
Pedicle soft tissue graft procedures
Rotational fl ap proceduresThe use of a laterally repositioned fl ap to cover areas with localized recession was introduced by Grupe and Warren (1956). This technique, which was called the laterally sliding fl ap operation, involved the refl ec-tion of a full-thickness fl ap in a donor area adjacent to the defect and the subsequent lateral displacement of this fl ap to cover the exposed root surface (Fig. 44-19). In order to reduce the risk for recession on the donor tooth, Grupe (1966) suggested that the mar-ginal soft tissue should not be included in the fl ap. Staffi leno (1964) and Pfeifer and Heller (1971) advo-cated the use of a split-thickness fl ap to minimize the potential risk for development of dehiscence at the donor tooth. Other modifi cations of the procedure presented are the double papilla fl ap (Fig. 44-31) (Cohen & Ross 1968), the oblique rotational fl ap (Pennel et al. 1965), the rotation fl ap (Patur 1977), and the transposi-tioned fl ap (Bahat et al. 1990).
The technique is as follows:
• The rotational fl ap procedure (Fig. 44-32) is initi-ated with the preparation of the recipient site. A reverse bevel incision is made all along the soft tissue margin of the defect (Fig. 44-32a). After removal of the dissected pocket epithelium, the exposed root surface is thoroughly curetted.
• At a distance of approximately 3 mm from the wound edge, which delineates the defect at the side opposite the donor area, a superfi cial incision is performed extending from the gingival margin to a level approximately 3 mm apical to the defect (Fig. 44-32b). Another superfi cial incision is placed horizontally from this incision to the opposite wound edge. The epithelium together with the outer portion of the connective tissue within the area delineated by these incisions and the wound edges is removed by sharp dissection (Fig. 44-32c). In this way a 3 mm wide recipient bed is created at the one side of the defect, as well as apical to the defect.
• A tissue fl ap to cover the recession is then dis-sected in the adjacent donor area. The preparation of this fl ap is initiated by a vertical superfi cial inci-sion placed parallel to the wound edge of the recession and at a distance that exceeds the width of the recipient bed and the exposed root surface by approximately 3 mm (Fig. 44-32c). This incision is extended beyond the apical level of the recipient bed and is terminated within the lining mucosa with an oblique releasing incision directed towards the recession site. An incision connecting the verti-cal incision and the incision previously made around the recession is placed approximately 3 mm apical to the gingival margin of the donor site.
a b
a
c
a
c
bb
dd
Fig. 44-31 Double papilla fl ap procedure. (a) Pre-treatment view of a maxillary canine with facial soft tissue recession. Using split incisions, soft tissue fl aps are mobilized from both sides of the recession (b) and sutured together for coverage of the exposed root (c). The healing result 6-month post-operatively shows complete root coverage (d).
906 Reconstructive Therapy
(2002), Jepsen et al. (2002), and Murphy and Gunsol-ley (2003).
For intrabony defects, 26 controlled trials with 867 intrabony defects were included (Murphy & Gunsol-ley 2003). The application of barrier membranes resulted in an additional clinical attachment level gain of more than 1 mm compared to an access fl ap approach control (Fig. 43-6).
For class II furcation defects, 15 controlled trials with 376 involved teeth were included (Murphy & Gunsolley 2003). Membrane application resulted in additional vertical and horizontal (depth of the furca-tion involvement) clinical attachment level gains (Fig. 43-7).
These data alone, however, did not present con-clusive evidence of effi cacy as the possibility of bias
aa bb cc dd
gg
jj kk ll
ee hhff
ii
Fig. 43-4 (a,b) Left maxillary lateral incisor with a deep interproximal intrabony defect on the mesial surface. (c) Flaps are raised according to the modifi ed papilla preservation technique, and a titanium-reinforced barrier membrane is placed over the defect. (d) By coronal displacement of the fl ap and preservation of the interdental papilla, the membrane is completely covered. (e,f) After 6 weeks of uneventful post-operative healing the membrane was removed, (g) and the newly formed tissue was completely covered. (h) At 1 year, residual probing pocket depth was 2 mm and no buccal or interdental recession had occurred. (i) The baseline radiograph shows radiolucency approaching the apex of the tooth, but after 1 year the intrabony defect is resolved and some supracrestal bone apposition seems to have occurred (j). The radiograph taken at 6 years confi rms the supracrestal bone regeneration (k) and the clinical image shows the integrity of the interdental papilla with optimal preservation of the esthetic appearance (l).
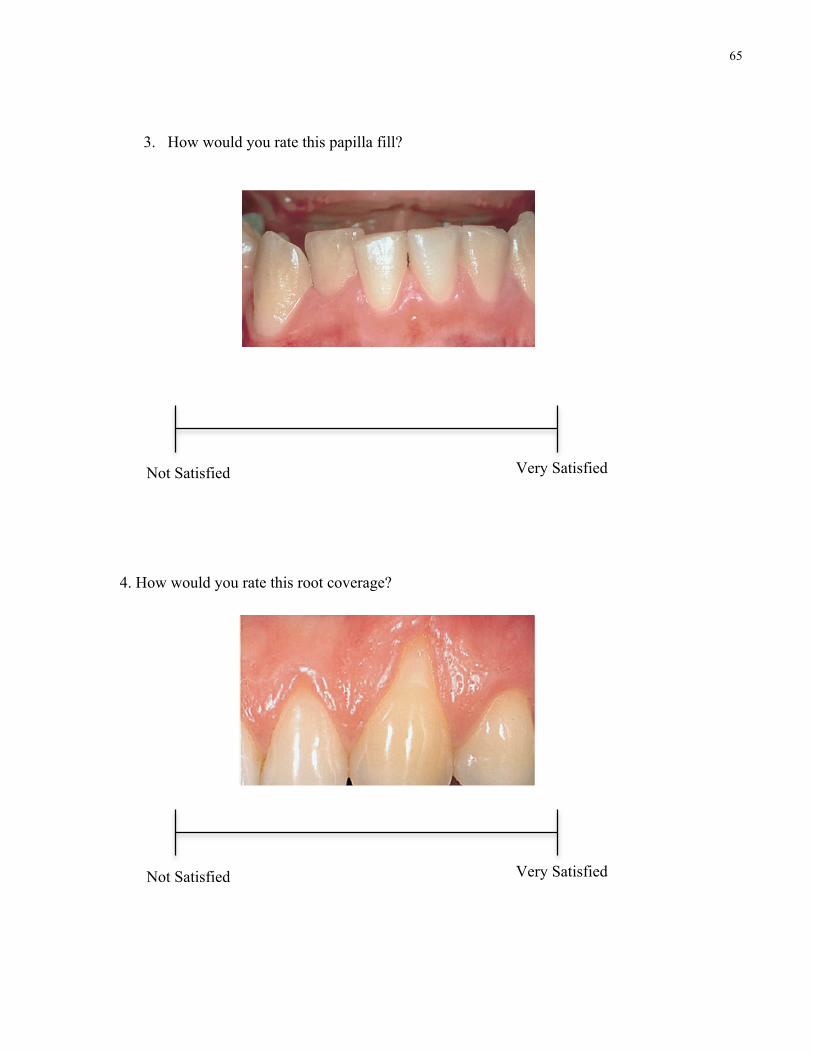
65
3. How would you rate this papilla fill?
4. How would you rate this root coverage?
Not Satisfied Very Satisfied
Not Satisfied Very Satisfied
972 Reconstructive Therapy
The pedicle graft procedures are, depending on the direction of transfer, grouped as (1) rotational fl ap procedures (e.g. laterally sliding fl ap, double papilla fl ap, oblique rotated fl ap) or (2) advanced fl ap proce-dures (e.g. coronally repositioned fl ap, semilunar coronally repositioned fl ap). The latter procedures do not include rotation or lateral movement of the pedicle graft. Regenerative procedures are also included within the group of pedicle graft proce-dures, i.e. rotational and advanced fl ap procedures
involving the placement of a barrier membrane between the graft and the root or the application of enamel matrix proteins.
The autogenous free soft tissue graft procedure may be performed as (1) an epithelialized graft or as (2) a subepithelial connective tissue graft (non-epithelialized graft), both usually taken from the area of the masticatory mucosa in the palate.
Factors, such as depth and width of recession, availability of donor tissue, presence of muscle
a b
a b
I
III
I
III
IIII
IVIV
Fig. 44-27 The Miller classifi cation of recession defects (see text).
aa bb
a b
Fig. 44-28 A 9-year-old boy showing recession at tooth 41. (a) The tooth is rotated and buccally positioned. The minimal amount of gingiva found apical to the recession shows pronounced signs of infl ammation. The plaque control in the region was improved but surgical intervention was postponed. (b) The same tooth area at the age of 14 years. Note the spontaneous soft tissue repair that has taken place at tooth 41 as a consequence of the improved plaque control and the growth in the alveolar process.
974 Reconstructive Therapy
Pedicle soft tissue graft procedures
Rotational fl ap proceduresThe use of a laterally repositioned fl ap to cover areas with localized recession was introduced by Grupe and Warren (1956). This technique, which was called the laterally sliding fl ap operation, involved the refl ec-tion of a full-thickness fl ap in a donor area adjacent to the defect and the subsequent lateral displacement of this fl ap to cover the exposed root surface (Fig. 44-19). In order to reduce the risk for recession on the donor tooth, Grupe (1966) suggested that the mar-ginal soft tissue should not be included in the fl ap. Staffi leno (1964) and Pfeifer and Heller (1971) advo-cated the use of a split-thickness fl ap to minimize the potential risk for development of dehiscence at the donor tooth. Other modifi cations of the procedure presented are the double papilla fl ap (Fig. 44-31) (Cohen & Ross 1968), the oblique rotational fl ap (Pennel et al. 1965), the rotation fl ap (Patur 1977), and the transposi-tioned fl ap (Bahat et al. 1990).
The technique is as follows:
• The rotational fl ap procedure (Fig. 44-32) is initi-ated with the preparation of the recipient site. A reverse bevel incision is made all along the soft tissue margin of the defect (Fig. 44-32a). After removal of the dissected pocket epithelium, the exposed root surface is thoroughly curetted.
• At a distance of approximately 3 mm from the wound edge, which delineates the defect at the side opposite the donor area, a superfi cial incision is performed extending from the gingival margin to a level approximately 3 mm apical to the defect (Fig. 44-32b). Another superfi cial incision is placed horizontally from this incision to the opposite wound edge. The epithelium together with the outer portion of the connective tissue within the area delineated by these incisions and the wound edges is removed by sharp dissection (Fig. 44-32c). In this way a 3 mm wide recipient bed is created at the one side of the defect, as well as apical to the defect.
• A tissue fl ap to cover the recession is then dis-sected in the adjacent donor area. The preparation of this fl ap is initiated by a vertical superfi cial inci-sion placed parallel to the wound edge of the recession and at a distance that exceeds the width of the recipient bed and the exposed root surface by approximately 3 mm (Fig. 44-32c). This incision is extended beyond the apical level of the recipient bed and is terminated within the lining mucosa with an oblique releasing incision directed towards the recession site. An incision connecting the verti-cal incision and the incision previously made around the recession is placed approximately 3 mm apical to the gingival margin of the donor site.
a b
a
c
a
c
bb
dd
Fig. 44-31 Double papilla fl ap procedure. (a) Pre-treatment view of a maxillary canine with facial soft tissue recession. Using split incisions, soft tissue fl aps are mobilized from both sides of the recession (b) and sutured together for coverage of the exposed root (c). The healing result 6-month post-operatively shows complete root coverage (d).

66
5. How would you rate this root coverage?
6. Are you happy with the overall aesthetics?
Not Satisfied Very Satisfied
Before
After
Not Satisfied Very Satisfied
Mucogingival Therapy – Periodontal Plastic Surgery 971
instructed to use a technique creating as little apically directed pressure on the soft tissue margin as possi-ble. A soft toothbrush should, of course, be used.
Miller (1985a) described a useful classifi cation of recession defects taking into consideration the antici-pated root coverage that is possible to obtain (Fig. 44-27):
• Class I: marginal tissue recession not extending to the mucogingival junction. No loss of interdental bone or soft tissue.
• Class II: marginal tissue recession extends to or beyond the mucogingival junction. No loss of interdental bone or soft tissue.
• Class III: marginal tissue recession extends to or beyond the mucogingival junction. Loss of inter-dental bone or soft tissue is apical to the CEJ, but coronal to the apical extent of the marginal tissue recession.
• Class IV: marginal tissue recession extends beyond the mucogingival junction. Loss of interdental bone extends to a level apical to the extent of the marginal tissue recession.
While complete root coverage can be achieved in class I and II defects, only partial coverage may be expected in class III. Class IV recession defects are not amenable to root coverage. Consequently, the critical clinical variable to assess in order to deter-mine the possible outcome of a root coverage proce-dure is the level of periodontal tissue support at the proximal surfaces of the tooth.
Recession defects in the child need particular attention. In the growing child recession defects may be eliminated spontaneously, provided adequate plaque control is established and maintained (Fig. 44-28). Andlin-Sobocki et al. (1991) reported from a 3-year prospective study that 25 out of 35 recession defects with an initial depth of 0.5–3.0 mm healed spontaneously following improvement of the oral hygiene standard. Furthermore, all but three remain-ing recessions showed a decrease and no site demon-strated an increase in depth. Hence, reparative surgical treatment of soft tissue recessions in the developing dentition may not be necessary and should preferably be postponed until the growth is completed.
In an orthodontic case showing a recession defect and a thin (delicate) gingiva associated with a promi-nent, facially positioned tooth (Fig. 44-29a), surgical treatment for root coverage should be postponed until the orthodontic therapy is completed. The reces-sion, as well as the dehiscence, will decrease as a consequence of the lingual movement of the tooth into a more proper position within the alveolar bone (Fig. 44-29b), and, if still indicated, the root coverage procedure will show higher predictability if performed after rather than before the tooth movement.
Root coverage procedures
Surgical procedures used in the treatment of reces-sion defects may basically be classifi ed as (1) pedicle soft tissue graft procedures and (2) free soft tissue graft procedures.
aa bb
a b
I
III
II
IV
Fig. 44-25 (a) A 25-year-old woman with esthetic concerns due to multiple soft tissue recessions in the maxilla and a high lip line. The gingiva is healthy and several of the exposed root surfaces show abrasion defects, indicating toothbrushing trauma as the causative factor for the development of the recessions. The brushing technique was altered and root coverage was achieved surgically. (b) The 2-year post-treatment view.
a b
aa bb
I
III
II
IV
Fig. 44-26 (a) A mandibular canine with a deep recession, which offers problems with respect to self-performed plaque control. (b) To facilitate plaque control the position of the soft tissue margin was altered surgically.
Mucogingival Therapy – Periodontal Plastic Surgery 971
instructed to use a technique creating as little apically directed pressure on the soft tissue margin as possi-ble. A soft toothbrush should, of course, be used.
Miller (1985a) described a useful classifi cation of recession defects taking into consideration the antici-pated root coverage that is possible to obtain (Fig. 44-27):
• Class I: marginal tissue recession not extending to the mucogingival junction. No loss of interdental bone or soft tissue.
• Class II: marginal tissue recession extends to or beyond the mucogingival junction. No loss of interdental bone or soft tissue.
• Class III: marginal tissue recession extends to or beyond the mucogingival junction. Loss of inter-dental bone or soft tissue is apical to the CEJ, but coronal to the apical extent of the marginal tissue recession.
• Class IV: marginal tissue recession extends beyond the mucogingival junction. Loss of interdental bone extends to a level apical to the extent of the marginal tissue recession.
While complete root coverage can be achieved in class I and II defects, only partial coverage may be expected in class III. Class IV recession defects are not amenable to root coverage. Consequently, the critical clinical variable to assess in order to deter-mine the possible outcome of a root coverage proce-dure is the level of periodontal tissue support at the proximal surfaces of the tooth.
Recession defects in the child need particular attention. In the growing child recession defects may be eliminated spontaneously, provided adequate plaque control is established and maintained (Fig. 44-28). Andlin-Sobocki et al. (1991) reported from a 3-year prospective study that 25 out of 35 recession defects with an initial depth of 0.5–3.0 mm healed spontaneously following improvement of the oral hygiene standard. Furthermore, all but three remain-ing recessions showed a decrease and no site demon-strated an increase in depth. Hence, reparative surgical treatment of soft tissue recessions in the developing dentition may not be necessary and should preferably be postponed until the growth is completed.
In an orthodontic case showing a recession defect and a thin (delicate) gingiva associated with a promi-nent, facially positioned tooth (Fig. 44-29a), surgical treatment for root coverage should be postponed until the orthodontic therapy is completed. The reces-sion, as well as the dehiscence, will decrease as a consequence of the lingual movement of the tooth into a more proper position within the alveolar bone (Fig. 44-29b), and, if still indicated, the root coverage procedure will show higher predictability if performed after rather than before the tooth movement.
Root coverage procedures
Surgical procedures used in the treatment of reces-sion defects may basically be classifi ed as (1) pedicle soft tissue graft procedures and (2) free soft tissue graft procedures.
aa bb
a b
I
III
II
IV
Fig. 44-25 (a) A 25-year-old woman with esthetic concerns due to multiple soft tissue recessions in the maxilla and a high lip line. The gingiva is healthy and several of the exposed root surfaces show abrasion defects, indicating toothbrushing trauma as the causative factor for the development of the recessions. The brushing technique was altered and root coverage was achieved surgically. (b) The 2-year post-treatment view.
a b
aa bb
I
III
II
IV
Fig. 44-26 (a) A mandibular canine with a deep recession, which offers problems with respect to self-performed plaque control. (b) To facilitate plaque control the position of the soft tissue margin was altered surgically.
Mucogingival Therapy – Periodontal Plastic Surgery 981
• The membrane barrier to be used is trimmed to cover the exposed root and approximately 3 mm of the bone lateral and apical to the dehiscence (Fig. 44-40c) and anchored to the tooth by a sling suture placed at the level of the CEJ.
• The mobilized fl ap is positioned coronally and secured by interdentally placed interrupted sutures (Fig. 44-40d). The membrane should be completely covered by the fl ap to reduce the risk for bacterial contamination during healing. Additional sutures are placed to close the lateral wound of the releas-ing incisions.
• The patient is advised to use a chlorhexidine mouth rinse for infection control and not to use any mechanical cleaning devices for at least 6 weeks in the tooth region subjected to surgery.
• The use of non-biodegradable membrane barriers requires a second surgery for membrane removal,
usually after 5–6 weeks (Fig. 44-40e,f). A partial-thickness trapezoidal fl ap is raised to expose the membrane. Following its removal, the fl ap is repositioned at the level of the CEJ to completely cover the newly formed tissue. Mechanical plaque control is reinstituted 4 weeks after membrane removal.
Pedicle soft tissue graft procedures combined with enamel matrix proteinsAbbas et al. (2003) described a surgical procedure for periodontal regenerative therapy of recession defects utilizing enamel matrix derivative bioactive material (Emdogain®):
• The surgical technique utilized is the coronally advanced fl ap as described above (Fig. 44-33). The interdental papillae should be de-epithelialized to
aa bb
cc dd
ee ff
Fig. 44-38 Coronally advanced fl ap procedure for multiple recessions (see text for explanation). (a–e) The oblique incisions over the interdental areas are placed in such a manner that the “surgically created papillae” mesial to the midline of the surgical fi eld are dislocated apically and distally, while the papillae of the fl ap distal to the midline are shifted in a more apical and mesial position. (f) The 1-year post-treatment view.
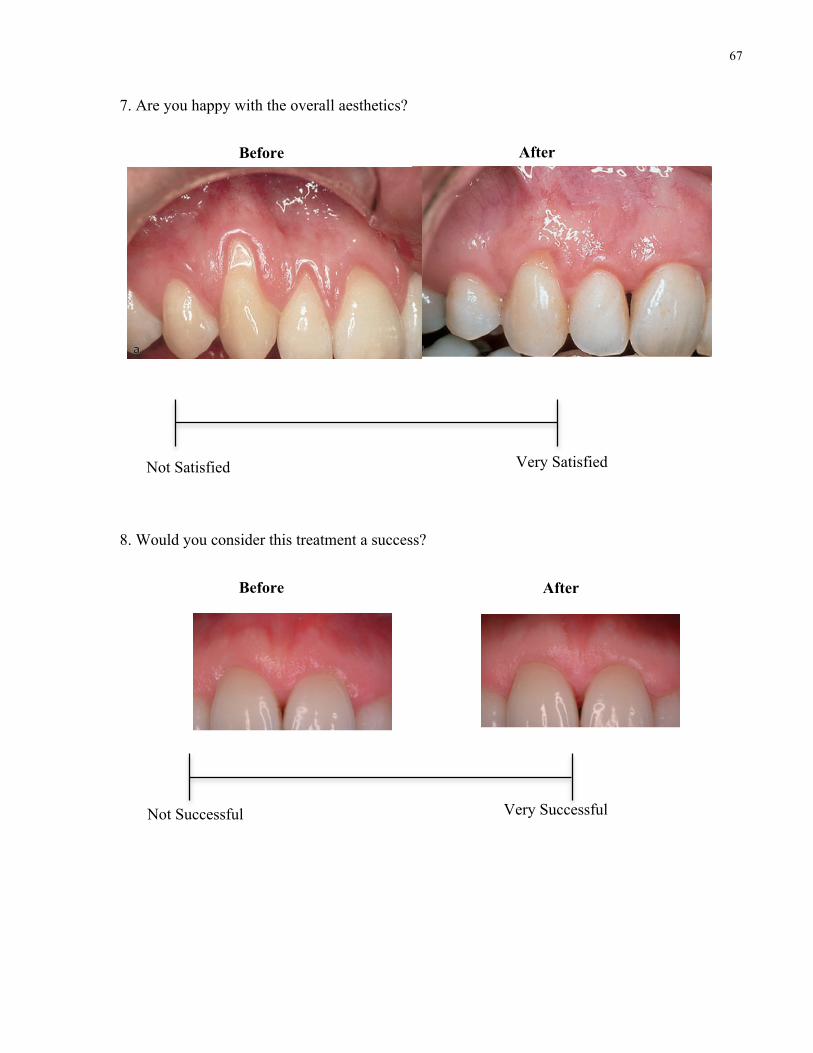
67
7. Are you happy with the overall aesthetics?
8. Would you consider this treatment a success?
Before
After
Not Satisfied Very Satisfied
Not Satisfied Very Satisfied
Before After
Not Successful Very Successful
962 Reconstructive Therapy
Alterations occurring in gingival dimensions and marginal tissue position in conjunction with orth-odontic therapy are related to the direction of tooth movement. Facial movement results in reduced facial gingival dimensions, while an increase is observed following lingual movement (Coatoam et al. 1981;
Andlin-Sobocki & Bodin 1993). Recession of the labial gingival margin and loss of attachment was demon-strated in experimental studies in the monkey follow-ing either tipping and extrusion movements or bodily movements of incisors (Batenhorst et al. 1974; Steiner et al. 1981). However, similarly designed studies carried out in dogs (Karring et al. 1982; Nyman et al. 1982) and humans (Rateitschak et al. 1968) failed to demonstrate that labial tooth movement is accompa-nied by marginal tissue recession and attachment loss. The confl icting results may be related to differ-ences with respect to e.g. (1) the amount of labial tooth displacement, (2) the presence/absence of plaque and gingival infl ammation in the regions sub-jected to tooth movement, and/or (3) differences in gingival dimensions. Steiner et al. (1981) speculated on mechanisms by which gingival tissue could be lost as a result of labial tooth movement and suggested that tension in the marginal tissue created by the forces applied to the teeth could be an important factor. If this hypothesis were valid, obviously the volume (thickness) of the gingival tissue at the pres-
Fig. 44-12 Soft tissue recession at tooth 11 observed during the course of active orthodontic treatment.
Muco-gingivalline
a b
Toothmovement
Coronal migration ofthe soft tissue margin
Increasedgingival height
Increasedboneheight
Fig. 44-13 (a) Schematic drawing illustrating alterations occurring in the marginal periodontal tissues following lingual movement of a tooth prominently positioned in the arch and having a bone dehiscence. (b) An increase in bone height and gingival height will be seen as well as a coronal migration of the soft tissue margin following lingual positioning of the tooth.
aa bb
a
b
Fig. 44-14 (a) A prominently positioned 13 showing soft tissue recession. (b) The same tooth following the completion of the orthodontic tooth movement. Note the reduction of the recession that has taken place as a consequence of the changed position of the tooth.
958 Reconstructive Therapy
gingiva possess the same “resistance” to continuous attachment loss as teeth with a wide zone of gingiva. Hence, the traditional dogma of the need of an “ade-quate” width (in millimeters) of gingiva, or attached portion of gingiva, for prevention of attachment loss is not scientifi cally supported.
Marginal tissue recession
Marginal tissue recession, i.e. displacement of the soft tissue margin apical to the cemento-enamel junc-tion (CEJ) with exposure of the root surface, is a common feature in populations with high standards of oral hygiene (e.g. Sangnes & Gjermo 1976; Murtomaa et al. 1987; Löe et al. 1992; Serino et al. 1994), as well as in populations with poor oral hygiene (e.g. Baelum et al. 1986; Yoneyama et al. 1988; Löe et al. 1992; Susin et al. 2004). In populations maintaining high standards of oral hygiene, loss of attachment and marginal tissue recession are predominantly found at buccal surfaces (Löe et al. 1992; Serino et al. 1994), and are frequently associated with the pres-ence of a “wedge-shaped defect in the crevicular area of one or several teeth” (Sangnes & Gjermo 1976). In contrast, all tooth surfaces are usually affected with soft tissue recession in periodontally untreated popu-lations, although the prevalence and severity is more pronounced at single-rooted teeth than at molars (Löe et al. 1978; 1992; Miller et al. 1987; Yoneyama et al. 1988).
Tissue trauma caused by vigorous toothbrushing is considered to be a predominant causative factor for the development of recessions, particularly in young individuals. Traumatizing toothbrushing and tooth malposition are the factors most frequently found to be associated with marginal tissue recession (Sangnes 1976; Vekalahti 1989; Checchi et al. 1999). In addition, Khocht et al. (1993) showed that recessions are related to the use of hard toothbrushes. Other local factors that have been associated with marginal tissue reces-sion are (1) alveolar bone dehiscences (Bernimoulin & Curilivic 1977; Löst 1984), (2) high muscle attach-ment and frenal pull (Trott & Love 1966), (3) plaque
and calculus (van Palenstein Helderman et al. 1998; Susin et al. 2004), and (4) iatrogenic factors related to restorative and periodontal treatment procedures (Lindhe & Nyman 1980; Valderhaug 1980).
At least three different types of marginal tissue recessions may exist:
• Recessions associated with mechanical factors, predomi-nately toothbrushing trauma (Fig. 44-4). Recessions resulting from improper toothbrushing techniques are often found at sites with clinically healthy gingiva and where the exposed root has a wedge-shaped defect, the surface of which is clean, smooth and polished.
• Recessions associated with localized plaque-induced infl ammatory lesions (Fig. 44-5). Such recessions may be found at teeth that are prominently posi-tioned, i.e. the alveolar bone is thin or absent (bone dehiscence), and where in addition the gingival tissue is thin (delicate). An infl ammatory lesion that develops in response to subgingival plaque occupies the connective tissue adjacent to the den-togingival epithelium. Measurements made by Waerhaug (1952) suggest that the distance between the periphery of microbial plaque on the tooth surface and the lateral and apical extension of the
aa bb
Fig. 44-4 Recessions associated with toothbrushing trauma. The marginal gingiva is clinically healthy and abrasion defects of various extension can be noted in the exposed roots.
a b
c
Fig. 44-5 A recession associated with localized plaque-induced infl ammatory lesion.
924 Reconstructive Therapy
defect also extends to the buccal or the palatal side of the involved tooth, or when it involves the two interdental spaces of the same tooth (Fig. 43-27) or two approximal teeth (Fig. 43-28). In the latter instance a second interdental papilla is accessed, either with a SPPF or a MPPT, according to indica-tions. Vertical releasing incisions are performed when fl ap refl ection causes tension at the extremities of the fl ap(s). The vertical releasing incisions are always kept very short and within the attached gingiva (never involving the mucogingival junction). The overall aim of this approach is to avoid using vertical incisions whenever possible or to reduce their number and extent to a minimum when there is a clear
indication for them. Periosteal incisions are never performed.
The defects are debrided with a combined use of mini curettes and power-driven instruments and the roots carefully planed. During the instrumentation the fl aps are slightly refl ected, carefully protected with periosteal elevators and frequent saline irriga-tions. At the end of instrumentation the biologically active agent is applied. Then the fl aps are repositioned.
The suturing approach in most of the instances consists of a single modifi ed internal mattress suture at the defect-associated interdental area to achieve primary closure of the papilla in the absence of any
aa bb cc
dd ee ff
gg
hh
Fig. 43-23 Clinical case illustrating the clinical application of the simplifi ed papilla preservation fl ap in conjunction with the application of a biologically active regenerative material (enamel matrix derivative in gel form). At re-evaluation following completion of successful initial cause-related therapy, an 8-mm pocket was detected on the mesial palatal aspect of the left central incisor (a). An angular defect was evidenced on a peri-apical radiograph (b). The complex anatomy of the defect is apparent following access to the defect with the modifi ed papilla preservation technique: a buccal fenestration is apparent with the majority of the defect extending palatally to the apical third of the root (c). Following application of the enamel matrix derivative, primary closure of the fl ap was achieved with a multilayered suture (d). At the 1-week suture removal appointment, excellent maturation of the soft tissue healing is apparent (e). At 6 months, a well represented interdental papilla is present thanks to both the papilla preservation approach and the presence of a bony bridge that assisted in soft tissue support, in spite of the gel formulation of the enamel matrix derivative (f). Clinical and radiographic outcomes at 1 year show preservation of excellent esthetics and elimination of the defect (g,h). Probing depths were in the 2 to 3 mm range.
924 Reconstructive Therapy
defect also extends to the buccal or the palatal side of the involved tooth, or when it involves the two interdental spaces of the same tooth (Fig. 43-27) or two approximal teeth (Fig. 43-28). In the latter instance a second interdental papilla is accessed, either with a SPPF or a MPPT, according to indica-tions. Vertical releasing incisions are performed when fl ap refl ection causes tension at the extremities of the fl ap(s). The vertical releasing incisions are always kept very short and within the attached gingiva (never involving the mucogingival junction). The overall aim of this approach is to avoid using vertical incisions whenever possible or to reduce their number and extent to a minimum when there is a clear
indication for them. Periosteal incisions are never performed.
The defects are debrided with a combined use of mini curettes and power-driven instruments and the roots carefully planed. During the instrumentation the fl aps are slightly refl ected, carefully protected with periosteal elevators and frequent saline irriga-tions. At the end of instrumentation the biologically active agent is applied. Then the fl aps are repositioned.
The suturing approach in most of the instances consists of a single modifi ed internal mattress suture at the defect-associated interdental area to achieve primary closure of the papilla in the absence of any
aa bb cc
dd ee ff
gg
hh
Fig. 43-23 Clinical case illustrating the clinical application of the simplifi ed papilla preservation fl ap in conjunction with the application of a biologically active regenerative material (enamel matrix derivative in gel form). At re-evaluation following completion of successful initial cause-related therapy, an 8-mm pocket was detected on the mesial palatal aspect of the left central incisor (a). An angular defect was evidenced on a peri-apical radiograph (b). The complex anatomy of the defect is apparent following access to the defect with the modifi ed papilla preservation technique: a buccal fenestration is apparent with the majority of the defect extending palatally to the apical third of the root (c). Following application of the enamel matrix derivative, primary closure of the fl ap was achieved with a multilayered suture (d). At the 1-week suture removal appointment, excellent maturation of the soft tissue healing is apparent (e). At 6 months, a well represented interdental papilla is present thanks to both the papilla preservation approach and the presence of a bony bridge that assisted in soft tissue support, in spite of the gel formulation of the enamel matrix derivative (f). Clinical and radiographic outcomes at 1 year show preservation of excellent esthetics and elimination of the defect (g,h). Probing depths were in the 2 to 3 mm range.
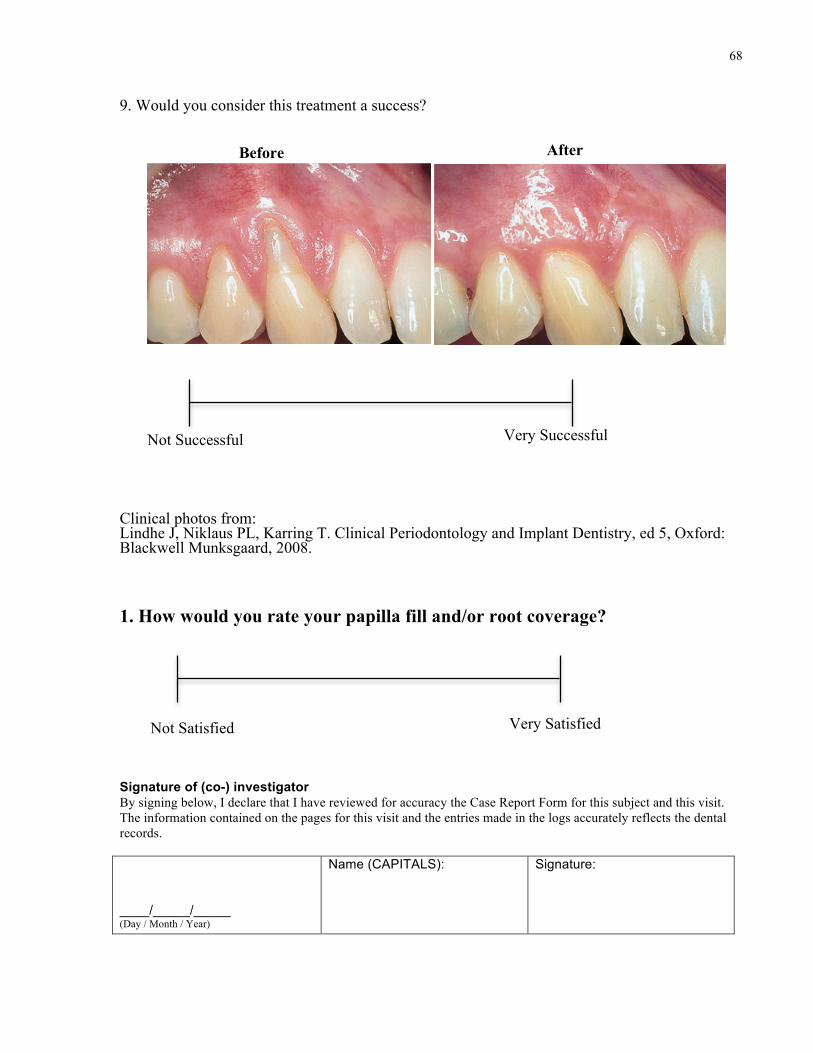
68
9. Would you consider this treatment a success?
Clinical photos from: Lindhe J, Niklaus PL, Karring T. Clinical Periodontology and Implant Dentistry, ed 5, Oxford: Blackwell Munksgaard, 2008. 1. How would you rate your papilla fill and/or root coverage?
Signature of (co-) investigator By signing below, I declare that I have reviewed for accuracy the Case Report Form for this subject and this visit. The information contained on the pages for this visit and the entries made in the logs accurately reflects the dental records. ____/_____/_____ (Day / Month / Year)
Name (CAPITALS):
Signature:
Before After
Not Successful Very Successful
Not Successful Very Successful
Not Satisfied Very Satisfied
Mucogingival Therapy – Periodontal Plastic Surgery 973
attachments, and esthetics, have to be taken into consideration in the selection of treatment procedure.
Treatment of the exposed root surface
Before root coverage is attempted the exposed portion of the root should be rendered free from bacterial plaque. Preferably, this is achieved by the use of a rubber cup and a polishing paste. Controlled clinical trials have shown no differences in terms of root coverage or residual probing depth between teeth that had been instrumented (root planed) or polished only (Oles et al. 1988; Pini Prato et al. 1999). Extensive root planing may therefore only be performed in situ-ations where a reduced root prominence would be considered benefi cial for graft survival or tissue regeneration, or if a shallow root caries lesion is diag-nosed. The presence of a fi lling in the root does not preclude the possibility for root coverage (Fig. 44-30), but the fi lling should be removed before the root is covered with soft tissue.
The use of root surface demineralization agents has been advocated as important not only for the removal of the smear layer, but also to facilitate the
formation of a new fi brous attachment through expo-sure of collagen fi brils of the dentine matrix and to allow subsequent interdigitation of these fi brils with those in the covering connective tissue. However, controlled clinical trials comparing the clinical outcome of root coverage procedures with and without root conditioning (Ibbott et al. 1985; Oles et al. 1985; Bertrand & Dunlap 1988; Laney et al. 1992; Bouchard et al. 1997; Caffesse et al. 2000) failed to demonstrate a benefi cial effect from the use of acid root biomodifi cation. Gottlow et al. (1986) evaluated the healing following treatment of localized gingival recessions with coronally positioned fl aps and citric acid root biomodifi cation in a controlled study in dogs. Histologic analysis after 3 months of healing disclosed no differences in the amount of root cover-age or new connective tissue attachment between citric acid-treated sites and saline-treated control sites. Although root resorption was a common fi nding among the citric acid-treated teeth in this dog model, such a fi nding has not been reported to be common in humans. In conclusion, the literature clearly indi-cates that the inclusion of root conditioning does not improve the healing outcome of root coverage procedures.
a b
aa bb
Fig. 44-29 Spontaneous repair of soft tissue recessions following orthodontic tooth movement. (a) A 22-year-old woman showing recessions and thin marginal tissues at prominently positioned teeth, particularly 23, 33, 41, and 43. (b) Following proper alignment of the teeth, the recessions have spontaneously been resolved and an increased gingival height can be noted.
aa bb
a
c
b
d
Fig. 44-30 (a) A canine showing pronounced recession and a composite resin restoration in the exposed root. Following removal of the restoration the exposed root was surgically covered with soft tissue (pedicle graft). (b) 2-year post-operative healing result.
Mucogingival Therapy – Periodontal Plastic Surgery 973
attachments, and esthetics, have to be taken into consideration in the selection of treatment procedure.
Treatment of the exposed root surface
Before root coverage is attempted the exposed portion of the root should be rendered free from bacterial plaque. Preferably, this is achieved by the use of a rubber cup and a polishing paste. Controlled clinical trials have shown no differences in terms of root coverage or residual probing depth between teeth that had been instrumented (root planed) or polished only (Oles et al. 1988; Pini Prato et al. 1999). Extensive root planing may therefore only be performed in situ-ations where a reduced root prominence would be considered benefi cial for graft survival or tissue regeneration, or if a shallow root caries lesion is diag-nosed. The presence of a fi lling in the root does not preclude the possibility for root coverage (Fig. 44-30), but the fi lling should be removed before the root is covered with soft tissue.
The use of root surface demineralization agents has been advocated as important not only for the removal of the smear layer, but also to facilitate the
formation of a new fi brous attachment through expo-sure of collagen fi brils of the dentine matrix and to allow subsequent interdigitation of these fi brils with those in the covering connective tissue. However, controlled clinical trials comparing the clinical outcome of root coverage procedures with and without root conditioning (Ibbott et al. 1985; Oles et al. 1985; Bertrand & Dunlap 1988; Laney et al. 1992; Bouchard et al. 1997; Caffesse et al. 2000) failed to demonstrate a benefi cial effect from the use of acid root biomodifi cation. Gottlow et al. (1986) evaluated the healing following treatment of localized gingival recessions with coronally positioned fl aps and citric acid root biomodifi cation in a controlled study in dogs. Histologic analysis after 3 months of healing disclosed no differences in the amount of root cover-age or new connective tissue attachment between citric acid-treated sites and saline-treated control sites. Although root resorption was a common fi nding among the citric acid-treated teeth in this dog model, such a fi nding has not been reported to be common in humans. In conclusion, the literature clearly indi-cates that the inclusion of root conditioning does not improve the healing outcome of root coverage procedures.
a b
aa bb
Fig. 44-29 Spontaneous repair of soft tissue recessions following orthodontic tooth movement. (a) A 22-year-old woman showing recessions and thin marginal tissues at prominently positioned teeth, particularly 23, 33, 41, and 43. (b) Following proper alignment of the teeth, the recessions have spontaneously been resolved and an increased gingival height can be noted.
aa bb
a
c
b
d
Fig. 44-30 (a) A canine showing pronounced recession and a composite resin restoration in the exposed root. Following removal of the restoration the exposed root was surgically covered with soft tissue (pedicle graft). (b) 2-year post-operative healing result.

69
One-Week Post-Treatment Visit Date of Visit: |__|__||__|__||__|__|__|__| Day / Month/ Year Clinical attachment loss (CAL)
_____mm
Recession from cemento-enamel junction (CEJ) to free gingival margin (FGM)
_____mm
Tip of papilla to interdental contact point
_____mm
Calculated percentage of new root coverage
______%
Visual Analog Scale (patients only):
Section 1 1. How would you rate your overall surgical experience?
2. How would you rate your surgical experience based on: Pain
Tolerance of Procedure
Very Satisfied
Not Satisfied
Unbearable Painless
Intolerable Comfortable
70
Post-operative recovery
3. How would you rate your surgical experience in comparison to other periodontal surgeries you have had based on: Pain
Tolerance of Procedure
Post-operative recovery
Still Recovering Minimal
Least Most
Best
Worst
Best Worst
71
Section 2 1. How would you rate this papilla fill and/or root coverage?
2. Are you happy with the overall aesthetics?
3. Would you consider this treatment a success?
Signature of (co-) investigator By signing below, I declare that I have reviewed for accuracy the Case Report Form for this subject and this visit. The information contained on the pages for this visit and the entries made in the logs accurately reflects the dental records. ____/_____/_____ (Day / Month / Year)
Name (CAPITALS):
Signature:
Not Satisfied Very Satisfied
Very Satisfied Not Satisfied
Not Successful Very Successful

72
Six-Week Post-Treatment Visit
Date of Visit: |__|__||__|__||__|__|__|__| Day / Month/ Year
Clinical Measurements Clinical attachment loss (CAL)
_____mm
Recession from cemento-enamel junction (CEJ) to free gingival margin (FGM)
_____mm
Tip of papilla to interdental contact point
_____mm
Calculated percentage of new root coverage
______%
1. How would you rate your papilla fill and/or root coverage?
2. Are you happy with the overall aesthetics?
3. Would you consider this treatment a success?
Signature of (co-) investigator By signing below, I declare that I have reviewed for accuracy the Case Report Form for this subject and this visit. The information contained on the pages for this visit and the entries made in the logs accurately reflects the dental records. ____/_____/_____ (Day / Month / Year)
Name (CAPITALS):
Signature:
Not Satisfied Very Satisfied
Very Satisfied Not Satisfied
Not Successful Very Successful
73
Six-Month Post-Treatment Visit
Date of Visit: |__|__||__|__||__|__|__|__| Day / Month/ Year
Clinical attachment loss (CAL)
_____mm
Recession from CEJ to FGM
_____mm
Tip of papilla to interdental contact point
_____mm
Calculated percentage of new root coverage
______%
1. How would you rate your papilla fill and/or root coverage post-treatment?
2. Are you happy with the overall aesthetics?
3. Would you consider this treatment a success?
Signature of (co-) investigator By signing below, I declare that I have reviewed for accuracy the Case Report Form for this subject and this visit. The information contained on the pages for this visit and the entries made in the logs accurately reflects the dental records. ____/_____/_____ (Day / Month / Year)
Name (CAPITALS):
Signature:
Not Satisfied Very Satisfied
Very Satisfied Not Satisfied
Not Successful Very Successful

74
Contributions to the Thesis Manuscript
Stephen Spano is responsible for all contents of this thesis. All aspects of the clinical research
pertaining to this thesis, including case report form development, patient consults, surgeries,
follow-ups, measurements, VAS assessments and statistical analysis were performed solely by
Stephen Spano.
75
References 1. Cairo F, Nieri M, Pagliaro U. Efficacy of periodontal plastic surgery procedures in the
treatment of localized facial gingival recessions. A systematic review. Journal of Clinical Periodontology. 2014;41(s15). doi:10.1111/jcpe.12182.
2. Greenwell H, Fiorellini J, Giannobile W, et al. Oral reconstructive and corrective considerations in periodontal therapy. J Periodontol. 2005;76(9):1588-1600. doi:10.1902/jop.2005.76.9.1588.
3. Chambrone L, Tatakis DN. Periodontal Soft Tissue Root Coverage Procedures: A Systematic Review From the AAP Regeneration Workshop. J Periodontol. 2015;86(2-s):S8-S51. doi:10.1902/jop.2015.130674.
4. Lang NP, Lindhe J. Clinical Periodontology and Implant Dentistry, 2 Volume Set. John Wiley & Sons; 2015.
5. Matas Hennig MA, Marconato Mustafa J, Musskopf ML. Absence of interdental papilla – Systematic review of available therapeutic modalities. Stomatos. 2016;22(43).
6. Chu SJ, Hochman MN, Tarnow DP. Loss of the interdental papilla. Inside Dentistry. 2014.
7. Lung H, Liao SC, Yuan K, Tseng CC. Interdental and Inter-implant Papilla: Literature Review and Management. 2012;12(1). doi:10.5297/ser.1201.002.
8. Kokich VG. Esthetics: the orthodontic-periodontic restorative connection. Semin Orthod. 1996;2(1):21-30.
9. Sharma AA, Park JH. Esthetic considerations in interdental papilla: remediation and regeneration. J Esthet Restor Dent. 2010;22(1):18-28. doi:10.1111/j.1708-8240.2009.00307.x.
10. Pradeep AR, Karthikeyan BV. Peri-implant papilla reconstruction: realities and limitations. J Periodontol. 2006;77(3):534-544. doi:10.1902/jop.2006.050068.
11. Miller PD. Periodontal plastic surgery. Curr Opin Periodontol. 1993:136-143.
12. Agudio G, Cortellini P, Buti J, Prato GP. Consensus Report Mucogingival Therapy. Annals of …. 1996. doi:10.1902/annals.1996.1.1.702.
13. Chang L-C. Comparison of age and sex regarding gingival and papillary recession. Int J Periodontics Restorative Dent. 2012;32(5):555-561.
14. Tjan AH, Miller GD, The JG. Some esthetic factors in a smile. J Prosthet Dent. 1984;51(1):24-28.
15. Hochman MN, Chu SJ, Tarnow DP. Maxillary anterior papilla display during smiling: a clinical study of the interdental smile line. Int J Periodontics Restorative Dent. 2012;32(4):375-383.
76
16. Singhal S, Mamdani M, Mitchell A, Tenenbaum H, Quiñonez C. An exploratory pilot study to assess self-perceived changes among social assistance recipients regarding employment prospects after receiving dental treatment. BMC Oral Health. 2015;15(1):138. doi:10.1186/s12903-015-0119-2.
17. Singhal S, Mamdani M, Mitchell A, Tenenbaum H, Lebovic G, Quiñonez C. Dental treatment and employment outcomes among social assistance recipients in Ontario, Canada. Health Policy. 2016;120(10):1202-1208. doi:10.1016/j.healthpol.2016.08.011.
18. Singhal S, Correa R, Quiñonez C. The impact of dental treatment on employment outcomes: a systematic review. Health Policy. 2013;109(1):88-96. doi:10.1016/j.healthpol.2012.09.016.
19. Ioannou AL, Koidou VP, Kamintzi GI, Hinrichs JE, Kotsakis GA, Romanos GE. Risk Indicators of Papillary Recession in the Anterior Maxilla. J Esthet Restor Dent. 2015;27(6):367-373. doi:10.1111/jerd.12164.
20. Cunliffe J, Pretty I. Patients' ranking of interdental ‘black triangles’ against other common aesthetic problems. Eur J Prosthodont Restor Dent. 2009;17(4):177-181.
21. Kokich VO, Kiyak HA, Shapiro PA. Comparing the Perception of Dentists and Lay People to Altered Dental Esthetics. J Esthet Restor Dent. 1999;11(6):311-324. doi:10.1111/j.1708-8240.1999.tb00414.x.
22. Schropp L, Isidor F. Papilla dimension and soft tissue level after early vs. delayed placement of single-tooth implants: 10-year results from a randomized controlled clinical trial. Clin Oral Implants Res. 2015;26(3):278-286. doi:10.1111/clr.12489.
23. Singh VP, Uppoor AS, Nayak DG, Shah D. Black triangle dilemma and its management in esthetic dentistry. Dent Res J (Isfahan). 2013;10(3):296-301.
24. Checchi L, Zelent ME, Rizzi GP, D'Achille C. Normality and pathology of the interdental papilla. Dental Cadmos. 1989.
25. Hassell TM. Tissues and cells of the periodontium. Periodontol 2000. 1993;3:9-38.
26. Chow YC, Eber RM, Tsao Y-P, Shotwell JL, Wang H-L. Factors associated with the appearance of gingival papillae. Journal of Clinical Periodontology. 2010;37(8):719-727. doi:10.1111/j.1600-051X.2010.01594.x.
27. Tarnow DP, Magner AW, Fletcher P. The effect of the distance from the contact point to the crest of bone on the presence or absence of the interproximal dental papilla. J Periodontol. 1992;63(12):995-996. doi:10.1902/jop.1992.63.12.995.
28. Cho H-S, Jang H-S, Kim D-K, et al. The effects of interproximal distance between roots on the existence of interdental papillae according to the distance from the contact point to the alveolar crest. J Periodontol. 2006;77(10):1651-1657. doi:10.1902/jop.2006.060023.
29. Ahmed AJ, Nichani AS, Venugopal R. An Evaluation of the Effect of Periodontal Biotype
77
on Inter-Dental Papilla Proportions, Distances Between Facial and Palatal Papillae in the Maxillary Anterior Dentition. J Prosthodont. August 2017. doi:10.1111/jopr.12640.
30. Grunder U. Stability of the mucosal topography around single-tooth implants and adjacent teeth: 1-year results. Int J Periodontics Restorative Dent. 2000;20(1):11-17.
31. Choquet V, Hermans M, Adriaenssens P, Daelemans P, Tarnow DP, Malevez C. Clinical and radiographic evaluation of the papilla level adjacent to single-tooth dental implants. A retrospective study in the maxillary anterior region. J Periodontol. 2001;72(10):1364-1371. doi:10.1902/jop.2001.72.10.1364.
32. Salama H, Salama MA, Garber D, Adar P. The interproximal height of bone: a guidepost to predictable aesthetic strategies and soft tissue contours in anterior tooth replacement. Pract Periodontics Aesthet Dent. 1998;10(9):1131–41–quiz1142.
33. Gastaldo JF, Cury PR, Sendyk WR. Effect of the vertical and horizontal distances between adjacent implants and between a tooth and an implant on the incidence of interproximal papilla. J Periodontol. 2004;75(9):1242-1246. doi:10.1902/jop.2004.75.9.1242.
34. Tarnow DP, Cho SC, Wallace SS. The effect of inter-implant distance on the height of inter-implant bone crest. J Periodontol. 2000;71(4):546-549. doi:10.1902/jop.2000.71.4.546.
35. Tarnow D, Elian N, Fletcher P, et al. Vertical distance from the crest of bone to the height of the interproximal papilla between adjacent implants. J Periodontol. 2003;74(12):1785-1788. doi:10.1902/jop.2003.74.12.1785.
36. Nordland WP, Tarnow DP. A classification system for loss of papillary height. J Periodontol. 1998;69(10):1124-1126. doi:10.1902/jop.1998.69.10.1124.
37. Miller PD. A classification of marginal tissue recession. Int J Periodontics Restorative Dent. 1985;5(2):8-13.
38. Zabalegui I, Sicilia A, Cambra J, Gil J, Sanz M. Treatment of multiple adjacent gingival recessions with the tunnel subepithelial connective tissue graft: a clinical report. Int J Periodontics Restorative Dent. 1999;19(2):199-206.
39. Aroca S, Keglevich T, Nikolidakis D, et al. Treatment of class III multiple gingival recessions: a randomized-clinical trial. Journal of Clinical Periodontology. 2010;37(1):88-97. doi:10.1111/j.1600-051X.2009.01492.x.
40. Cairo F. Periodontal plastic surgery of gingival recessions at single and multiple teeth. Periodontol 2000. 2017;75(1):296-316. doi:10.1111/prd.12186.
41. Zadeh HH. Minimally invasive treatment of maxillary anterior gingival recession defects by vestibular incision subperiosteal tunnel access and platelet-derived growth factor BB. Int J Periodontics Restorative Dent. 2011;31(6):653-660.
42. Chao JC. A novel approach to root coverage: The pinhole surgical technique.
78
International Journal of Periodontics and …. 2012.
43. Venezia E, Goldstein M, Boyan BD, Schwartz Z. The use of enamel matrix derivative in the treatment of periodontal defects: a literature review and meta-analysis. Crit Rev Oral Biol Med. 2004;15(6):382-402.
44. Koop R, Merheb J, Quirynen M. Periodontal regeneration with enamel matrix derivative in reconstructive periodontal therapy: a systematic review. J Periodontol. 2012;83(6):707-720. doi:10.1902/jop.2011.110266.
45. Spahr A, Haegewald S, Tsoulfidou F, et al. Coverage of Miller class I and II recession defects using enamel matrix proteins versus coronally advanced flap technique: a 2-year report. J Periodontol. 2005;76(11):1871-1880. doi:10.1902/jop.2005.76.11.1871.
46. Sayar F, Akhundi N, Gholami S. Connective tissue graft vs. emdogain: A new approach to compare the outcomes. Dent Res J (Isfahan). 2013;10(1):38-45. doi:10.4103/1735-3327.111768.
47. Wennström JL, Lindhe J. Some effects of enamel matrix proteins on wound healing in the dento-gingival region. Journal of Clinical Periodontology. 2002;29(1):9-14. doi:10.1034/j.1600-051x.2002.290102.x/asset/j.1600-051x.2002.290102.x.pdf?v=1&t=i9zuj4b8&s=ee66df28ea4488c6ea58ca1e7c043ca17651145d.
48. Maas CS, Bapna S. Pins and needles: minimally invasive office techniques for facial rejuvenation. Facial plast Surg. 2009;25(4):260-269. doi:10.1055/s-0029-1242038.
49. Attenello NH, Maas CS. Injectable Fillers: Review of Material and Properties. Facial plast Surg. 2015;31(01):029-034. doi:10.1055/s-0035-1544924.
50. Gold M. The science and art of hyaluronic acid dermal filler use in esthetic applications. J Cosmet Dermatol. 2009;8(4):301-307. doi:10.1111/j.1473-2165.2009.00464.x.
51. Kontis TC. Contemporary review of injectable facial fillers. JAMA Facial Plast Surg. 2013;15(1):58-64. doi:10.1001/jamafacial.2013.337.
52. Brandt FS, Cazzaniga A. Hyaluronic acid fillers: Restylane and Perlane. Facial Plast Surg Clin North Am. 2007;15(1):63–76–vii. doi:10.1016/j.fsc.2006.11.002.
53. Bogdan Allemann I, Baumann L. Hyaluronic acid gel (Juvéderm) preparations in the treatment of facial wrinkles and folds. Clin Interv Aging. 2008;3(4):629-634.
54. Brandt FS, Cazzaniga A. Hyaluronic acid gel fillers in the management of facial aging. Clin Interv Aging. 2008;3(1):153-159.
55. Burchard AE, Ellis DAF. The Canadian experience with fillers. Facial plast Surg. 2009;25(2):129-134. doi:10.1055/s-0029-1220654.
56. Dover JS, Carruthers A, Carruthers J, Alam M. Clinical Use of RESTYLANE. Skin Therapy Lett. 2005;10(1):5-7.
79
57. Sinha A, Hurakadli M, Yadav P. Botox and dermal fillers: The twin-face of cosmetic dentistry. International Journal of Contemporary Dental and Medical Reviews. February 2015:1-4. doi:10.15713/ins.ijcdmr.27.
58. Becker W, Gabitov I, Stepanov M, Kois J, Smidt A, Becker BE. Minimally invasive treatment for papillae deficiencies in the esthetic zone: a pilot study. Clin Implant Dent Relat Res. 2010;12(1):1-8. doi:10.1111/j.1708-8208.2009.00247.x.
59. Blatz MB, Hürzeler MB, Strub JR. Reconstruction of the lost interproximal papilla--presentation of surgical and nonsurgical approaches. Int J Periodontics Restorative Dent. 1999;19(4):395-406.
60. Cronin RJ, Wardle WL. Loss of anterior interdental tissue: periodontal and prosthodontic solutions. J Prosthet Dent. 1983;50(4):505-509.
61. Lee W-P, Kim H-J, Yu S-J, Kim B-O. Six Month Clinical Evaluation of Interdental Papilla Reconstruction with Injectable Hyaluronic Acid Gel Using an Image Analysis System. J Esthet Restor Dent. 2016;28(4):221-230. doi:10.1111/jerd.12216.
62. Salama H, Salama M. The role of orthodontic extrusive remodeling in the enhancement of soft and hard tissue profiles prior to implant placement: a systematic approach to the management …. International Journal of Periodontics …. 1993.
63. Goldberg PV, Higginbottom FL, Wilson TG. Periodontal considerations in restorative and implant therapy. Periodontol 2000. 2001;25(1):100-109. doi:10.1034/j.1600-0757.2001.22250108.x.
64. Beagle JR. Surgical reconstruction of the interdental papilla: case report. … Journal of Periodontics & Restorative Dentistry. 1992.
65. Shapiro A. Regeneration of interdental papillae using periodic curettage. Int J Periodontics Restorative Dent. 1985;5(5):26-33.
66. Carnio J. Surgical reconstruction of interdental papilla using an interposed subepithelial connective tissue graft: a case report. Int J Periodontics Restorative Dent. 2004;24(1):31-37.
67. Misch CE, Al-Shammari KF, Wang H-L. Creation of Interimplant Papillae Through a Split-Finger Technique. Implant Dentistry. 2004;13(1):20-27. doi:10.1097/01.ID.0000116368.76369.78.
68. Palacci P, Nowzari H. Soft tissue enhancement around dental implants. Periodontol 2000. 2008;47(1):113-132. doi:10.1111/j.1600-0757.2008.00256.x.
69. el-Salam AA. Use of a titanium papillary insert for the construction of interimplant papillae. Implant Dentistry. 1999.
70. Mansouri SS, Ghasemi M, Salmani Z. Clinical application of hyaluronic acid gel for reconstruction of interdental papilla at the esthetic zone. Journal of Islamic Dental ….
80
2013.
71. Awartani FA, Tatakis DN. Interdental papilla loss: treatment by hyaluronic acid gel injection: a case series. Clin Oral Investig. 2016;20(7):1775-1780. doi:10.1007/s00784-015-1677-z.
72. Bertl K, Gotfredsen K, Jensen SS, Bruckmann C, Stavropoulos A. Can hyaluronan injections augment deficient papillae at implant-supported crowns in the anterior maxilla? A randomized controlled clinical trial with 6 months follow-up. Clin Oral Implants Res. July 2016. doi:10.1111/clr.12917.
73. Norman GR, Streiner DL. Biostatistics: the bare essentials, ed 4, Connecticut: PMPH-USA, 2014.
74. Triola MF, Triola MM, Roy J. Biostatistics for the Biological and Health Sciences. Pearson; 2017.
75. Carlsson AM. Assessment of chronic pain. I. Aspects of the reliability and validity of the visual analogue scale. Pain. 1983;16(1):87-101.
76. Matthews DC, McCulloch CA. Evaluating patient perceptions as short-term outcomes of periodontal treatment: a comparison of surgical and non-surgical therapy. J Periodontol. 1993;64(10):990-997. doi:10.1902/jop.1993.64.10.990.
77. McCreary CP, Clark GT, Oakley ME, Flack V. Predicting response to treatment for temporomandibular disorders. J Craniomandib Disord. 1992;6(3):161-169.
78. Rocha dos Santos M, Sangiorgio JPM, Neves FLDS, et al. Xenogenous Collagen Matrix and/or Enamel Matrix Derivative for Treatment of Localized Gingival Recessions: A Randomized Clinical Trial. Part II: Patient-Reported Outcomes. J Periodontol. 2017;88(12):1319-1328. doi:10.1902/jop.2017.170127.
79. Pini Prato GP, Baldi C, Nieri M, et al. Coronally advanced flap: the post-surgical position of the gingival margin is an important factor for achieving complete root coverage. J Periodontol. 2005;76(5):713-722. doi:10.1902/jop.2005.76.5.713.
80. Lee W-P, Seo Y-S, Kim H-J, Yu S-J, Kim B-O. The association between radiographic embrasure morphology and interdental papilla reconstruction using injectable hyaluronic acid gel. J Periodontal Implant Sci. 2016;46(4):277-287. doi:10.5051/jpis.2016.46.4.277.
81. Girardeau-Hubert S, Teluob S, Pageon H, Asselineau D. The reconstructed skin model as a new tool for investigating in vitro dermal fillers: increased fibroblast activity by hyaluronic acid. Eur J Dermatol. 2015;25(4):312-322. doi:10.1684/ejd.2015.2563.
82. Chen WY, Abatangelo G. Functions of hyaluronan in wound repair. Wound Repair Regen. 1999;7(2):79-89.
83. Nolan A, Baillie C, Badminton J, Rudralingham M, Seymour RA. The efficacy of topical hyaluronic acid in the management of recurrent aphthous ulceration. J Oral Pathol Med.

81
2006;35(8):461-465. doi:10.1111/j.1600-0714.2006.00433.x.
84. Jentsch H, Pomowski R, Kundt G, Göcke R. Treatment of gingivitis with hyaluronan. Journal of Clinical Periodontology. 2003;30(2):159-164.
85. Naorungroj S. Esthetic Reconstruction of Diastema with Adhesive Tooth-Colored Restorations and Hyaluronic Acid Fillers. Case Rep Dent. 2017;2017:5670582. doi:10.1155/2017/5670582.
86. Lafzi A, Mohammadi AS, Eskandari A, Pourkhamneh S. Assessment of Intra- and Inter-examiner Reproducibility of Probing Depth Measurements with a Manual Periodontal Probe. J Dent Res Dent Clin Dent Prospects. 2007;1(1):19-25. doi:10.5681/joddd.2007.004.




![Comparison of the abrasive properties of two …...interdental gingival papilla retraction [1–5]. It is frequently used as part of treatment in combination with clear aligners [6]](https://img.pdfslide.net/doc/110x75/5e4244609105141a5a2d2628/comparison-of-the-abrasive-properties-of-two-interdental-gingival-papilla-retraction.jpg)