Embed Size (px)
Citation preview

413ISSN 1758-1869Pain Manag. (2014) 4(6), 413–426
part of
Pain Management
10.2217/PMT.14.38 © 2014 Future Medicine Ltd
REVIEW
A practical approach to ocular pain for the non-ophthalmologist
Corey W Waldman*,1, Steven D Waldman2 & Reid A Waldman3
1Sinai Hospital, Krieger Eye Institute, Baltimore, MD 21215, USA 2Kansas City School of Medicine, University of Missouri, MO 65211, USA 3Vision Research Center, Kansas City School of Medicine, University of Missouri, MO 65211, USA
*Author for correspondence: [email protected]
SUMMARY Pain involving the eye has numerous etiologies and is a feared challenge of many clinicians. Between a fear of the patient losing vision and a lack of familiarity with the ophthalmic equipment necessary to diagnose the problem, working up eye pain can be a daunting task. While the ophthalmologist can be indispensable in challenging cases of eye pain, this article will help clarify the unique clinical features of each etiology that can help clinicians narrow down the differential and arrive at a diagnosis.
KEYWORDS • chalazion • conjunctivitis • corneal abrasion • eye pain • ocular pain • referred eye pain • retrobulbar hematoma • scleritis • uveitis
An appropriate history will lead the clinician down the right path when approaching a patient with eye pain. While many of the below etiologies can have some overlap in historical features, each has a unique history that can help one narrow down the differential, especially when taking a patient phone call from home, in which case an immediate exam is not available and determining concern for a vision or life threatening etiology can be the difference between making that trip in or getting a few extra hours of sleep. Below are important causes of eye pain and their unique components to both the history and exam.
Corneal abrasion●● History
A corneal abrasion occurs when the corneal epithelium is disrupted or damaged by a foreign body, be it a finger nail, metallic object or plant matter [1,2].
●● SymptomsPatients often report a significant amount of sharp pain, a gritty, foreign body sensation (even in the absence of a foreign body), and photophobia that is relieved upon the instillation of a topical anesthetic such as proparacaine [3]. Vision may be reported as blurry, especially if the abrasion is in the visual axis or there is significant tearing [4].
Practice Points
● Diagnosing the etiology of eye pain can be a daunting task for the non-ophthalmologist. ● Key clinical features can help the clinician distinguish one etiology from another, thus providing more assurance in ruling out a vision threatening problem.
● While some situations (e.g., retrobulbar hematoma, angle closure glaucoma, endophthalmitis) are acutely vision threatening and must be identified, many causes of eye pain are either self-limiting and not vision threatening in the short term.
● Referred causes of eye pain must be considered as some of these (e.g., cavernous sinus syndrome) can be acutely vision threatening.
● Whenever there is any doubt with regards to either the diagnosis or treatment of the problem at hand, prompt referral to an ophthalmologist is necessary.
For reprint orders, please contact: [email protected]

Pain Manag. (2014) 4(6)414
REviEW Waldman, Waldman & Waldman
future science group
●● Signs The conjunctival vessels are often injected and the patient may be tearing. Observing the abra-sion with a slit lamp and staining of the affected area with fluorescein observed under a cobalt blue light is diagnostic [5].
●● Treatment A topical antibiotic drop or ointment should be prescribed [6]. Ointments provide comfort to the abraided cornea but have the side effect of blurred vision, which is problematic if the abrasion is bilat-eral. If the injury was not with a fingernail or plant matter, then erythromycin or bacitracin ophthal-mic ointments four-times a day can be used poly-myxin B/trimethoprim drops four-times a day are also reasonable [7]. If plant matter or fingernails were involved, then a fluoroquinolone drop should be used four-times per day [8]. Patching is some-times used for patient comfort, but should not be used in the setting of contact lens wear, finger-nail injury or plant matter injury [9]. Despite their request for the ‘magic drops’ that you gave them for the exam, the patient should never be sent home with topical anesthetic drops as continued use of these drops can cause a corneal melt [10].
●● Follow-up If the abrasion is large or central, the patient should be referred to an ophthalmologist and fol-lowed daily. If the abrasion is small or peripheral, the patient may follow-up 2–5 days later, but sooner if any worsening symptoms.
●● Important pointsWhen diagnosing a corneal abrasion, one should rule out the presence of a corneal foreign body, including everting the eyelids to look underneath them. If a foreign body penetrates the full thick-ness of the cornea and into the anterior cham-ber, this must be removed in the operating room by an ophthalmologist. This situation can be evidenced by a positive Seidel sign, which refers to leakage from the wound seen with changes in the color of fluorescein.
Viral conjunctivitis●● Symptoms
Patients with viral conjunctivitis will complain of a red, watery eye, with mild to moderate discomfort described as a foreign body sensation or itching or burning [11]. The patient will often report that it started in one eye and spread to the other, and may have a history of sick contacts or recent viral
infection. Significantly decreased vision is not a common complaint in viral conjunctivitis.
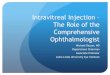
●● SignsConjunctival injection, chemosis, eyelid swell-ing and watery discharge are all common findings [12]. Subconjunctival hemorrhage can occur in viral conjunctivitis as well, and may be quite alarming to the patient (Figure 1) [13]. The clinician should examine for preauricular lymphadenopathy. Under a slit lamp, follicles can be seen on the palpebral conjunctiva.
●● ManagementReassurance is important as this is a self-limited viral illness that will resolve in couple of weeks, typically without any sequellae [14]. The patient continues to be highly contagious as long as the eye is red, thus hand hygiene should be rein-forced. Cool compresses and artificial tears can provide symptomatic relief [15]. The patient can follow-up in 1 week, but should return sooner if worsening symptoms or vision.
●● Important pointsIf purulent discharge is present, the suspicion for a bacterial etiology (e.g., Staphylococcus aureus, Neisseria gonorrhea or Streptococcus pneumoniae should be raised. If such is the case, the patient should be referred urgently to ophthalmology for cultures and prompt antibiotic treatment [16].
Chalazion/hordeolumA chalazion, or stye, occurs when a meibomian gland or a gland of Zeis is blocked and becomes inflamed [17]. Ahordeolum is an infection of this blocked gland [18].
●● SymptomsThe patient will typically complain of the grad-ual onset of an eyelid ‘bump’ that is painful when infected, but may be painless otherwise.
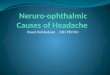
●● SignsA focal eyelid nodule can be palpated and sur-rounding eyelid swelling may be present. If sig-nificant erythema or warmth is present in the setting of a chalazion/hordeolum, concern for preseptal cellulitis should be present (Figure 2) [19].
●● ManagementThe key to treating chalazia/hordeola, is warm compresses for about 10 min at a time at least four-times per day [20]. The patient can provide

415
Figure 1. Hemorrhagic epidemic keratoconjunctivitis. This patient presented with a classic viral conjunctivitis, which evolved into bullous subconjunctivial hemorrhage. Despite the alarming appearance of this condition, it is self-limited and often resolves without sequellae.
Figure 2. Chalazion with possible early preseptal cellulitis. This chalazion appeared to be rather inflamed and patient was treated with oral antibiotics for concern for possible early preseptal cellulitis.
A practical approach to ocular pain for the non-ophthalmologist REviEW
future science group www.futuremedicine.com
gentle massage to the lesion while performing warm compresses as well. If the lesion does not resolve with these conservative measures after several weeks, referral to an ophthalmologist comfortable with a chalazion removal procedure can be consulted. Some ophthalmologists may try injecting the lesion with steroids instead of surgery [21].
●● Important pointsThe clinician should monitor for the develop-ment of preseptal cellulitis which requires more aggressive treatment with oral antibiotics [22]. If chalazia are recurrent, especially in an elderly patient, referral to ophthalmology for evaluation for sebaceous adenocarcinoma may be warranted [23].
Preseptal/orbital cellulitisHistory and exam are essential in distinguish-ing the more mild preseptal cellulitis, from the more severe orbital cellulitis. Preseptal celluli-tis is an infection of the skin and soft tissue of the eyelid, anterior to the orbital septum [24]. If the infection is posterior to this structure, then orbital cellulitis is the diagnosis.
●● SymptomsIn preseptal cellulitis, patients will complain of redness, pain and swelling of the eyelid and may report a recent chalazion or hordeolom, injury to eyelid skin or sinusitis. In orbital cellulitis, patients may report pain with eye movements, significantly decreased vision, a ‘bulging eye’ or diplopia (Figure 3).
●● SignsThe most important part of the exam is to dis-tinguish preseptal from orbital cellulitis. In pre-septal cellulitis, the eyelid will be red, warm and tender to palpation. Swelling may make it so that the patient is unable to open the eye. There will be no pain with eye movements, no prop-tosis, no optic nerve compromise (evidenced by decreased vision, aferrant pupillary defect and decreased color vision) and no limited extraocu-lar motility. The aforementioned are all signs of orbital cellulitis. Table 1 helps the clinician with a side by side comparison of these conditions.
●● ManagementFor a mild preseptal cellulitis in a patient older than 5 years of age, treatment with amoxicillin/clavulanate, bactrim or
moxifloxacin for 10 days can be started [20]. If methicillin-resistant Staphylococcus aureus is a possibility, then bactrim, doxycycline or clinda-mycin are all reasonable options [25]. However, if the presentation is more severe, the patient may not comply with treatment, there is worsening after 24–48 h of oral antibiotics, or the child is

Pain Manag. (2014) 4(6)416
Figure 3. Orbital cellulitis. This pediatric patient presents with swelling and erythema of the eyelids and was found to have restricted extraocular motility, proptosis and diplopia. The patient was thus admitted for intravenous antibiotics.
REviEW Waldman, Waldman & Waldman
future science group
less than 5 years of age, then the patient should be admitted to the hospital for intravenous (IV) antibiotics [20]. Vancomycin and ampicillin/sulbactam can be used [26]. If orbital cellulitis is suspected, then the patient must be admit-ted for broad spectrum IV antibiotics and ophthalmology and ENT should be consulted as surgical management may be necessary [20]. CT scan of the orbits withcontrast should be ordered in severe cases or if there is concern for orbital cellulitis. Patients with either of these conditions should be followed daily initially, until improvement is noted.
Episcleritis/scleritisEpiscleritis refers to inflammation of the tis-sue in between the more superficial conjunc-tiva and the underlying sclera, whereas scleri-tis refers to inflammation of the sclera itself. Distinguishing between these two etiologies is important as they bear different prognostic implications [27].
●● SymptomsIn episcleritis patients will present with acute redness and mild discomfort of the affected eye [28]. On the other hand, scleritis tends to be a more severe, deep, aching pain in a patient
with a complaint of ‘red eye’ [29]. Either of these conditions may be recurrent [30].
●● SignsEpiscleritis manifests with prominent episcleral vessels, often involving only one segment of the eye instead of the entire episclera. Nodules are sometimes seen over the involved area and visual acuity remains unaffected. These vessels blanch with 2.5% phenylephrine [31]. Scleritis involves engorgement of the deeper scleral vessels, which do not blanch with application of phenylephrine.
●● ManagementEpiscleritis is often idiopathic, however, recur-rent episodes or an appropriate history should alert the clinician towards underlying herpes zoster infection, rosacea or collagen vascular diseases [32]. Thus, work up for these conditions may be warranted. If the episcleritis is very mild, then a conservative approach involving obser-vation and artificial tears for discomfort can be employed; however, more severe cases may require oral NSAIDS [33].
Scleritis is often associated with an underly-ing condition. Connective tissue diseases, her-pes zoster ophthalmicus, tuberculosis, Lyme disease and sarcoidosis have all been associated with scleritis and work up for these conditions may be indicated [34]. Referral to ophthal-mology is important as scleritis can be vision threatening and the extent of involvement of more posterior structures (e.g., the retina) can be determined and managed accordingly. In conjunction with the ophthalmologist, oral NSAIDS, steroids or immunosuppressives can be used for treating scleritis [35].
Contact lens overwear/intoleranceAny patient with a complaint of eye pain should be inquired about use, hygiene and wearing habits of contact lenses as they can not only cause pain, but also predispose the eye to sight threatening conditions (e.g., corneal ulcers).
●● Symptoms/signsPatients who are having a contact lens related problem of any kind, be it a poorly fitting lens, displaced lens, lens overwear, dry eyes or even an ulcer (Figure 4), abrasion or infection may present with pain, redness, blurry vision and photopho-bia. The clinician should inquire about wearing habits such as time spent in lenses per day, time spent sleeping in lenses and appropriate hygiene.

417
A practical approach to ocular pain for the non-ophthalmologist REviEW
future science group www.futuremedicine.com
Table 1. Distinguishing features of the different etiologies of eye pain.
Etiology Distinguishing features Management
Corneal abrasion ● History of trauma ● Topical antibiotics ● Foreign body sensation ● Staining with fluorescein Viral conjunctivitis ● Sick contacts ● Hand hygiene ● Conjunctival injection spreading from one eye to
the other ● Cool compresses
● Watery discharge ● Artificial tears ● Minimal to mild pain ● Minimally decreased vision ● Preauricular lymphadenopathy Preseptal cellulitis ● Warmth, redness and swelling of eyelid ● <5 years of age: admit for IV antibiotics ● No restricted motility ● >5 years of age: oral antibiotics with close follow-up ● No optic nerve compromise ● No proptosis Orbital cellulitis ● Warmth, redness and swelling of the eyelid ● CT orbits with IV contrast ● Restricted motility ● Admit for IV antibiotics ● Proptosis ● Daily follow-up ● Optic nerve compromise ● Ophthalmology evaluationEpiscleritis ● Sectoral injection of episcleral vessels ● Observation if mild ● Blanching of vessels with 2.5% phenylephrine ● Oral NSAIDS if more severe ● Mild-to-moderate discomfort with minimal
changes in vision
Scleritis ● Deep, boring eye pain ● Oral NSAIDS, steroids or immunosuppressants ● Injection of scleral vessels ● No blanching with 2.5% phenylephrine ● May involve more posterior structures and
threaten vision
Anterior uveitis ● Diffuse injection, especially of perilimbal vessels ● Ophthalmology referral for topical steroids and a cycloplegic
● Significant photophobia ● Decreased vision Acute angle closure glaucoma
● Sudden onset severe eye pain ● Emergent referral for ophthalmology
● Blurry vision with halos ● Pressure lower agents ● Injected conjunctival vessels ● Pressure lower procedures ● Mid-dilated pupil ● Very elevated intraocular pressure ● Hazy cornea Optic neuritis ● Sudden onset deceased vision ● IV steroids ● Decreased color vision ● Ophthalmology and neurology referrals ● Pain with eye movements ● Afferent pupillary defect Retrobulbar hematoma ● Recent history of trauma or eyelid surgery ● Emergent ophthalmology referral for lateral canthotomy
and cantholysis to decompress the orbit ● Tensely swollen eyelids ● Ecchymotic eyelids ● Decreased vision ● Proptosis ● Optic nerve compromise ● Bullous subconjunctival hemorrhageCT: Computed tomography; IV: Intravenous

Pain Manag. (2014) 4(6)418
Figure 5. Pseudodendrites in herpes zoster ophthalmicus. Pseudodendrites on the central cornea staining with fluorescein in a patient with herpes zoster ophthalmicus.
Figure 4. Corneal ulcer due to contact lens overwear. The patient exercised poor contact lens hygiene and developed a large, central ulcer, significant injection of vessels and a large hypopyon.
REviEW Waldman, Waldman & Waldman
future science group
●● ManagementAny contact lens wearer complaining of a red, painful eye and decreased vision warrants an urgent and careful slit lamp examination by and ophthalmologist or optometrist as complications such as a corneal ulcer can be sight threaten-ing if not treated promptly and appropriately. Until seeing ophthalmology or optomety, the clinician should inform the patient to avoid wearing contact lenses.
Herpes zoster ophthalmicusVaricella zoster virus infection involving the V1 distribution of the trigeminal nerve is notorious for involving not just the periocular skin, but the eye itself [36]. Within the eye, it can involve the cornea, cause a uveitis, scleritis, retinitis, optic neuritis and even palsies of the extraocular muscles [37]. Thus, it is clear that considering
herpes zoster ophthalmicus is important when evaluating a patient with eye pain.
●● SymptomsThe clinical presentation can vary greatly depend-ing on which structures of the eye are involved, but in a patient with a dermatomal rash and par-esthesias in the V1 distribution complaining of ocular pain or decreased vision, an evaluation for herpes zoster ophthalmicus needs to be initiated.
●● SignsPatients may present with the characteristic der-matomal rash of herpes zoster (i.e., ipsilateral scalp vesicles); however, in some cases eye involve-ment may precede skin findings [38]. Lesions on the tip of the nose, known as Hutchinson’s sign are predictive of ocular involvement [39]. Injection of the conjunctiva, decreased vision and a characteristic staining pattern of the cornea (pseudodendrites) are possible (Figure 5). A careful slit slam exam and dilated fundus exam are important to look for uveitis and retinitis. Intraocular pressure may be elevated and cranial nerve palsies can occur [20].
●● ManagementOral treatment with valacyclovir given at 1 g three-times per day, acyclovir 800 mg five-times per day or famciclovir 500 mg three-times per day should be started [40]. Ophthalmology should be consulted as a careful slit lamp exam and dilated fundoscopic exam are important to check for and manage vision threatening complications such as corneal involvement, retinal necrosis or uveitis [41]. Topical antibiotic ointment to the skin lesions is helpful in preventing superinfection.
Acute angle closure glaucomaAcute angle closure glaucoma is a condition in which the aqueous outflow of the eye is impeded by the drainage structures, or angle of the anterior chamber being closed off by the iris coming into apposition with the trabecular meshwork [42]. This is a very painful and sight threatening condition, in contrast to primary open angle glaucoma, which is much more common and is asymptomatic for the majority of its course [43].
●● SymptomsPatients experiencing acute angle closure glau-coma present with acute onset of severe eye pain, red eye, blurry vision, halos in vision, brow ache,

419
Figure 6. Iritis in an HLA-B27-positive patient. The patient has significant injection of conjunctival vessels, a perilimbal flush and an irregularly shaped pupil due to synechiae between the iris and the lens due to the inflammation.
A practical approach to ocular pain for the non-ophthalmologist REviEW
future science group www.futuremedicine.com
nausea and vomiting [44]. This is more common in women, those of East Asian descent, those with hyperopia and with a positive family history [45]. It may be precipitated by dim light, reading, mydriatics, miotics or anticholinergics [46].
●● SignsIn addition to severe pain and decreased vision, these patients present with injected conjunctiva and a mid-dilated, poorly reactive pupil. The intra-ocular pressure is highly elevated, often between 40 and 60 mmHg (the upper limit of normal is 21 mmHg) [47]. The cornea is often edematous, or ‘steamy,’ and the anterior chamber is shallow.
●● ManagementAcute angle closure glaucoma is an ophthalmic emergency and if suspected, emergent referral to ophthalmology is imperative as this condition will cost the patient their vision if left untreated. Treatment is aimed at lowering the pressure with both topical and oral pressure lower agents and re-opening the closed drainage structures by means of a laser peripheral iridotomy performed by ophthalmology [48].
Anterior uveitisUveitis is a broad term referring to a myriad of diseases of numerous underlying systemic etiolo-gies that involve inflammation of a part or all of the uveal tract, which consists of the iris, ciliary body and choroid [49]. Anterior uveitis, which consists of inflammation of the iris (iritis) and the ciliary body (iridocyclitis), is discussed here as it is the subset of uveitis most likely to present with pain [20].
●● SymptomsAnterior uveitis presents as gradual onset of a painful, red eye with significant photophobia and blurry vision (Figure 6) [50]. This disease can be recurrent or chronic in nature.
●● SignsAlthough the history in the setting of an eye with diffuse injection of conjunctival vessels, especially around the iris, can point the clinician toward a diagnosis of anterior uveitis, the slit lamp exam is essential. For this, referral to ophthalmology is imperative. On slit lamp exam, inflammatory cells and flare in the anterior chamber as well as inflammatory debris on the posterior cornea (known as keratic precipitates) are diagnostic [51].
●● ManagementPrompt referral to ophthalmology is important in the setting of uveitis as a careful slit lamp exam as well as a careful dilated funduscopic exam needs to be performed. Recurrent episodes need to be worked up for an underlying etiology. Treatment consists of topical steroid drops and a long acting, topical mydriatic such as atropine or cyclopentalate as directed by ophthalmology [52].
●● Important pointsBilateral or recurrent uveitis, or uveitis in the setting of the appropriate clinical history war-rants a systemic workup as many underlying diseases can cause uveitis. Lyme disease, reac-tive arthritis, ankylosing spondylitis, juvenile idiopathic arthritis, sarcoidosis, tuberculosis, syphilis, AIDS, toxoplasmosis and Varicella zoster virus infection all can cause an anterior uveitis, thus an appropriate history and work up may be necessary [53,54]. However, despite the numerous systemic etiologies listed, idiopathic anterior uveitis is the most common cause [55].
EndophthalmitisEndophthalmitis is an inflammation involving the structures within the eyeball itself. It can categorized as exogenous, occurring after trauma or intraocular surgery or endogenous, occurring in the setting of bacteremia and spreading to the eye via the bloodstream. Rapid recognition and treatment of this condition is key, as it can be devastating to the eye [56]. In acute postoperative endophthalmitis, Staphylococcus epidermidis, Staphylococcus aureus, streptococcus species

Pain Manag. (2014) 4(6)420
REviEW Waldman, Waldman & Waldman
future science group
and Gram negatives are all possible infectious agents [57]. Insubacute postoperat ive e ndopht h a l m i t i s , S . e p i d e r m i d i s , Propionibacteriam acnes or fungi are consid-erations. Following trauma, bacillus species, S. epidermidis, Gram-negative organisms and fungi are all possible. Bacillus cereus is common in endogenous endophthalmitis involving IV drug abusers. Fungi and S. auereus can also occur in endogenous endophthalmitis [20].
●● SymptomsPatients with acute exogenous endophthalmi-tis have a history of increasing pain, redness and worsening vision in the setting of either an intraocular surgery (i.e., cataract extraction or glaucoma filtering procedure) or penetrat-ing globe trauma within the past few days [58]. However, in some cases endophthalmitis may present subacutely, occurring weeks or even months after eye surgery with a complaint of redness, pain and decreased vision.
Endogenous endophthalmitis occurs in a few settings: sepsis, indwelling catheter, recent hos-pitalization, IV drug abuse or in an immuno-compromised patient [59]. There is no history of recent eye surgery. As in other types of endophthalmitis, these patients will complain of increasing redness, pain and worsening vision.
●● SignsWhile the clinical findings can vary greatly, decreased visual acuity, conjunctival injec-tion, decreased red reflex, hypopyon, corneal edema, eyelid edema and anterior chamber inflammation (seen with a slit lamp) are com-mon. With endogenous endophthalmitis, orbital inflammation can occur causing proptosis and decreased motility.
●● ManagementIf endophthalmitis of any kind is expected, an emergent ophthalmology consult should be requested. [60]. Management of exogenous endophthalmitis consists of an anterior cham-ber tap for cultures and gram stain and an injection of intravitreal antibiotics. [61]. The eyedrop regimen typically consists of ster-oid drops and fortified antibiotics every hour along with atropine three-times a day [62]. Pars Plana vitrectomy is a consideration and is ben-eficial in many cases, thus a retina specialist should be involved in the management of these patients [63].
Patients with endogenous endophthalmitis should be hospitalized and comanaged with the internist as cultures need to be taken and IV antibiotics need to be started. Topical steroids and cycloplegics are given and intravitreal antibiotics as well as a pars planavitrectomy are considerations [20].
Optic neuritisWhile an in depth review of optic neuritis is beyond the scope of this chapter, including it in the differential of eye pain is important, as this condition is not only vision threatening, but also often has underlying systemic impli-cations. While it is commonly associated with multiple sclerosis, it can occur as an idiopathic phenomenon, a post viral syndrome and as a part of sarcoidosis, syphilis, Lyme disease, cat scratch disease, HIV, toxoplasmosis and systemic lupus erythematosus [64].
●● SymptomsPatients complain of acute vision loss (often uni-lateral), decreased color vision and mild eye pain in 90% of cases [65]. This pain is often described as worse with eye movements, which is an important distinguishing feature of optic neuritis [66].
●● SignsPatients can present with decreased visual acu-ity (often unilateral), decreased color vision, an afferent pupillary defect and pain with eye movements. In some cases, optic disc swelling is present, however, this is not always the case as inflammation may be posterior the disc itself [67].
●● ManagementWhile specific management options will be directed at the suspected underlying cause, all patients, regardless of etiology, should undergo an MRI of the brain and orbits with gadolinium [68]. Ophthalmology and neurology should be consulted, and visual field testing should be per-formed. Lab work may be considered to search for an underlying cause (as mentioned above) if the case warrants. If it is a first episode and the MRI reveals lesions concerning for multiple sclerosis, admission to the hospital for IV steroids is necessary [69].
Retrobulbar hematomaRetrobulbar hematoma refers to a hemorrhage within the orbit surrounding the globe and optic nerve [70]. It can follow trauma or eyelid

421
A practical approach to ocular pain for the non-ophthalmologist REviEW
future science group www.futuremedicine.com
or orbital surgery, especially in the setting of a patient on anticoagulants, and must be recognized promptly as vision loss due to optic nerve damage can occur rapidly [71].
●● SymptomsPatients will report a history of trauma or recent eyelid or orbital surgery and will complain of eye pain, significant eyelid swelling causing difficulty opening the eyes, as well as vision loss [72].
●● SignsOn exam, visual acuity may be decreased. An afferent pupillary defect and decreased color vision may be present if the optic nerve is being compromised. The intraocular pressure will be elevated and the eyelids are often ecchymotic and tensely swollen to a point where opening them is difficult. Bullous subconjunctival hem-orrhage often occurs as well. On fundus exam, the retinal vasculature may be compromised and disc swelling may be present [20].
●● ManagementIn a patient with the above findings in the appro-priate clinical setting who is losing vision, defini-tive treatment need not be delayed on account of ordering a CT of the orbit. Essentially this is a compartment syndrome involving the orbit, thus management revolves around decompressing this area. Thus, if the optic nerve is being com-promised by the hematoma, an immediate lateral canthotomy and cantholysis should be performed to decompress the orbit [73]. Opthalmology should be involved to help monitor and manage intraocular pressure following the procedure.
Common causes of referred eye pain●● Cavernous sinus thrombosis
In the pre-antibiotic era, cavernous sinus throm-bosis was a common sequela to infection of the frontal or maxillary sinuses or the periorbial region. This potentially life threatening condition is now seen primarily in immunocompromised patients, for example, HIV. Occasionally, cavern-ous sinus thrombosis is seen in patients suffering from herpes zoster ophthalmicus and sarcoidosis.
SymptomsThe patient with cavernous sinus thrombosis most often presents with the primary complaint of headache and periorbital and retroocular pain combined with the symptoms of the patient’s
underlying infection, for example, maxillary sinusitis, etc. [74]. As the pathologic process progresses, the pain often becomes more intense. If the infection tracts more posteriorly, the patient may complain of visual abnormalities and swelling around the eyes.
SignsThe patient will exhibit the signs of the underly-ing infection and may appear septic, with fever and chills. Periorbital edema may initially be uni-lateral, but as infection spreads to the contralat-eral eye via the intercavernous sinuses, the other eye will become involved [75]. As the infection and thrombosis spreads, isolated cranial nerve abnormalities, ptosis and ophthalmoplegia are often noted as are signs of meningeal irritation.
ManagementCavernous sinus thrombosis represents a true med-ical emergency. Immediate blood cultures should be obtained and antibiotics capable of treating staphylococcus, streptococcus and pneumococ-cus should be started as quickly as possible [75]. MRI with magnetic resonance venography and/or computerized tomography (CT) should be obtained on an emergent basis to help identify the nidus of infection and the extent of spread and thrombosis. Surgical drainage of abscess formation may be required to try and prevent permanent neurological sequella and in some cases death [76].
Important points If the clinician suspects the patient may be suf-fering from cavernous venous thrombosis, it should be considered the patients primary diag-nosis until it is ruled out. It should be remem-bered that early in the course of this disease, that the symptoms and signs may be nonspecific and may be more related to the patient’s underlying infection. Careful ocular examination may first reveal impairment of lateral gaze due to cranial nerve VI compromise as the abducens nerve lies within the middle of the cavernous sinus [77]. As the entire cavernous sinus becomes involved, cra-nial nerves III and IV which course along the lat-eral wall of the cavernous sinus are compressed resulting in ptosis, mydriasis and upward drift of the affected eye.
Tolosa-Hunt syndromeAn uncommon cause of eye pain, Tolosa-Hunt syndrome should be considered in patients presenting with the unexplained

Pain Manag. (2014) 4(6)422
REviEW Waldman, Waldman & Waldman
future science group
acute onset of unilateral eye pain associated with ophthalmoplegia in the absence of other demonstrable ocular pathology. The exact eti-ology of Tolosa-Hunt syndrome is unknown and is thought to be due to a nonspecific inf lammation of the cavernous sinus and superior orbital fissure [78].
●● SymptomsThe pain of Tolosa-Hunt syndrome is severe in nature and has been characterized as having a constant, deep, boring quality. In most patients, the onset of pain is followed by the complaint of diplopia which is secondary to ophthalmoplegia as the cranial nerves passing through the cav-ernous sinus are affected [79]. If the sympathetic nerves are affected, the patient may complain of a droopy eyelid and unequal pupils. If inflamma-tion of the cavernous sinus extends into the orbit, the optic nerve may become involved leading to visual loss.
●● SignsThe patient with Tolosa-Hunt syndrome will exhibit painful ophthalmoplegia of the cranial nerves III, IV and VI. Inflammation of the sym-pathetic nerves as they traverse the cavernous sinus may produce a Horner syndrome with associated miosis. Ptosis may also be the result of involvement of cranial nerve III. In some patients, decreased visual acuity may be identi-fied as a result of cranial nerve II involvement. Occasionally, involvement of cranial nerve V may result in loss of the ipsilateral corneal reflex.
●● ManagementAlthough the diagnosis of Tolosa-Hunt syn-drome is a diagnosis of exclusion, given the potential for poor outcomes, the clinician should strongly consider the immediate treatment of this syndrome with high dose corticosteroids in a manner analogous to the use of steroids when treating temporal arteritis. [80] Most patients will begin to experience pain relief within 24–72 h with an incremental improvement of ophthal-moplegia over the next 7–10 days. If symptoms persist or if corticosteroids are not tolerated, a trial of azathioprine or methotrexate represent a reasonable next step [81]. As soon as treatment is initiated, MRI of the brain and cavernous sinus with magnetic resonance venography and angiography and/or CT should be obtained on an emergent basis to help identify occult infection, neoplasm or other unsuspected
causes of the patients symptoms as well as to confirm inflammation of the cavernous sinus and the orbital apex and superior orbital fissure [82]. While these findings are nonspecific for Tolosa-Hunt syndrome, their findings certainly strengthen the diagnosis. Rarely, a biopsy of the cavernous sinus is required to confirm the diagnosis and rule out occult neoplasm. Because of the difficulty in confirming the diagnosis, laboratory testing of serum and cerebrospinal fluid to rule out infection, connective tissue disease, syphilis, Lyme disease and HIV are mandatory [83].
●● Important pointsWhile it is important to consider Tolosa-Hunt syndrome in any patient with unexplained uni-lateral eye pain with associated ophthalmople-gia, the disease remains difficult to diagnose. Ophthalmologic and neuro-ophthalmologic consultation on an emergent basis is always indi-cated. It should be remembered that many of the diseases that can mimic Tolosa-Hunt syndrome, for example, HIV, syphilis, infection, cavernous sinus thrombosis, etc. can cause significant morbidity and mortality if undetected.
Cluster headacheCluster headache is a common cause of referred ocular and periocular pain. The presumption is that abnormal modulation of neural traffic between the sphenopalatine ganglion and the trigeminal ganglion results in the patient’s per-ception of eye pain during cluster headache [84]. Cluster headache is a cyclical headache charac-terized by clusters of headache interrupted by headache free periods-hence the name cluster headache [85]. Unlike other migraine and most other types of primary headache which occur much more commonly in females, cluster head-ache occurs primarily in males, although the 5:1 male to female ratio decreases with age. Cluster headache is less common than migraine and tension-type headache affecting approximately 0.5% of the male population. Unlike migraine headache, which almost always presents by the second decade of life, the first episodes of cluster headache most commonly occur in the late third to early fourth decades. There does not appear to be a genetic predilection to the development of cluster headache as is seen in migraineurs. Episodes of cluster headache most commonly occur in the spring and fall with this unique chronobiological pattern thought to be the result

423
A practical approach to ocular pain for the non-ophthalmologist REviEW
future science group www.futuremedicine.com
of seasonal changes in the number of daylight hours the patient is exposed to. Vasoactive substances including alcohol, nitrates, histamine may trigger acute cluster headache as may exposure to high altitude.
●● SymptomsCluster headache is localized to the ocular, retro-orbital, peri-orbital and temporal regions. This unilateral headache has a very short onset-to peak of seconds to minutes and is characterized as having a severe, deep, burning and/or boring quality. In addition to the spring and fall chrono-biologic pattern mentioned above, the onset of cluster headache tends to occur approximately 90 min after the patient falls asleep. Interestingly, this sleep associated onset pattern is preserved in cluster headache sufferers who change from working days to working nights. During an episode of cluster headaches, the patient will experience headaches of 45 min to 1 h duration two- to three-times per 24-h period. Episodes of untreated cluster headaches generally last for 8–12 weeks followed by headache free remission periods of 2 years of less. Occasional the remis-sion periods may become shorter or disappear entirely with a rapid escalation in the increase of daily headaches. Fortunately, these chronic cluster headaches are rare.
●● SignsDuring an acute attack of cluster headache, the clinician will frequently identify a Horner’s syndrome, consisting of ptosis, abnormal pupil constriction, facial flushing and conjunctival injection on the same side as the headache. These findings are often accompanied with profuse lac-rimation and rhinorrhea. If cluster headaches persist, the patient’s ocular changes may become permanent and cutaneous changes including a coarsening of facial features including deeply fur-rowed glabellar folds, telangiectasia and malar Peau d’orange skin may be observed. Unlike patients suffering from other common headache syndromes such as migraine and tension-type headache where the patient may require a dark quiet room to aid in symptom relief, the cluster headache sufferer will often appear agitated and be unable to lie still and prefer to rock or pace back and forth during the acute attack.
●● ManagementThere is no specific test that can reliably diagnose cluster headache and the diagnosis rests
on taking a careful targeted headache history and performing a careful neurologic exam. All patients suspected of suffering from cluster head-ache should magnetic resonance testing with and without gadolinium enhancement and magnetic resonance angiography of the brain to rule out occult pathology. If cranial nerve palsies are also present, magnetic resonance venography of the orbit and cavernous sinus is strongly recom-mended. Ophthalmologic evaluation with care-ful assessment of intraocular pressures is indi-cated in all patients suffering from ocular and periocular pain as is measurement of erythrocyte sedimentation rate, complete blood count and automated blood chemistries.
Predisone in a starting dose of 80 mg per day given in divided doses with the daily dose tapered by 10 mg per dose per day is a reasonable first step in the treatment of acute cluster headache. The addition of daily sphenoplatine nerve blocks with local anesthetic and the administration of 100% oxygen is via a close-fitting mask may also be beneficial in aborting cluster headache [86].
If the patient’s headache symptomatology does not rapidly respond to the above mentioned treatment modalities, the addition of oral lith-ium carbonate is a reasonable next step. Given the small therapeutic window of lithium carbon-ate, it is safest to start the patient on a low dose of lithium carbonate with a 300 mg dose given 1 h before sleep. If the patient does not experi-ence side effects, but the headaches persist, the dose may be increased by 300 mg every 48 h until the headaches are controlled or a maximum dose of 1200 mg is reached. Once headache con-trol is achieved, the patient should be continued at the effective dose for an additional 10 days and then the dosage tapered downward over a 1-week period. If the above mentioned headache treatments fail to control the patient’s headache symptomatology, consideration can be given to short trials of methysergide, sumatriptan or sumatriptan-like drugs.
●● Important pointsCluster headache is one of the most severepain syndromes that man is afflicted with and rapid control of the patient’s headaches is important, or the patient may overuse or misuse prescription or street drugs in an effort to control the pain. The clinician should observe the patient closely for signs of significant depression as suicides have been reported in cluster headache sufferers who are unable to obtain significant pain relief.

Pain Manag. (2014) 4(6)424
REviEW Waldman, Waldman & Waldman
future science group
ReferencesPapers of special interest have been highlighted as:• of interest or; •• of considerable interest
1 Dargin, JM, Lowenstein RA. The painful eye. Emerg. Med. Clin. North Am. 26(1), 199–216 (2008).
• Providesadetailedoverviewforthenonophthalmologistofcommonlyencounteredcausesofeyepainintheemergencysetting.
2 Lin YB, Gardiner MF. Fingernail-induced corneal abrasions: case series from an ophthalmology emergency department. Cornea 33(7), 691–695 (2014).
3 Martin-Doyle JLC. Diseases of the eyelids. In: A Synopsis of Ophthalmology. Martin-Doyle JLC (Ed.). Elsevier Ltd, NY, USA, 25–42 (2013).
4 Aerni GA. Blunt visual trauma. Clin. Sports Med. 32(2), 289–301 (2013).
5 Brunette DD, Ghezzi K, Benner GS. Ophthalmologic disorders. In: Emergency Medicine: Concepts and Clinical Practice. Rosen P, Barkin R (Eds). Elsevier Inc., NY, USA, 2432–2440 (1997).
6 Patterson J, Fetzer D, Krall J et al. Eye patch treatment for the pain of corneal abrasian. South Med. J. 89(2), 227 (1996).
7 Wipperman JL, Dorsch JN. Evaluation and management of corneal abrasions. Am. Fam. Physician 87(2), 114–120 (2013).
8 Waldman CW, Waldman SD, Waldman RA. Pain of ocular and periocular origin. Med. Clin. North Am. 97(2), 293–307 (2013).
• Providesadetailedoverviewofthecommoncausesofeyepainanddiscussesmanyimportantcausesofreferredeyepainandheadaches.
9 Turner A, Rabiu M. Patching for corneal abrasion. Cochrane Database Syst. Rev. 19(2), CD004764 (2006).
10 Stull S, Schultz GS, Downer DM. Science and strategy for preventing and managing corneal ulceration. Ocul. Surf. 5(1), 23–39 (2007).
11 Martin-Doyle JLC. Diseases of the conjunctiva. In: A Synopsis of Ophthalmology. Martin-Doyle JLC (Ed.). Elsevier Inc, PA, USA, 8–24 (2013).
12 Huang AS, Chao YN, Lee PH et al. Epidemiology of acute viral conjunctivitis at a junior high school. Int. J. Infect. Dis. 12(1), e97 (2008).
13 Buttaravoli P, Leffler SM. Subconjunctival Hemorrhage. In: Minor Emergencies: Expert Consult (Third Edition). Buttaravoli P, Leffler SM (Eds). Elsevier Inc, PA, USA, 92–93 (2012).
14 Palay DA, Krachmer J. Primary Care Ophthalmology (2nd Edition). Elsevier Inc, PA, USA, (2005).
15 Shiuey Y, Ambati BK, Adamis AP. A randomized, double-masked trial of topical ketorolac versus artificial tears for treatment of viral conjunctivitis. Ophthalmology 107(8), 1512–1517 (2000).
16 Bersudsky V, Rehany U, Tendler Y. Diagnosis of chlamydial infection by direct enzyme-linked immunoassay and polymerase chain reaction in patients with acute follicular conjunctivitis. Graefes Arch. Clin. Exp. Ophthalmol. 237(8), 617 (1999).
17 Pavan-Langston D. Diagnosis and therapy of common eye infections: bacterial, viral, fungal. Compr. Ther. 9(5), 33 (1983).
18 Deibel JP, Cowling K. Ocular inflammation and infection. Emerg. Med. Clin. North Am. 31(2), 387–397 (2013).
19 Lee S, Yen MT. Management of preseptal and orbital cellulitis. Saudi J. Ophthalmol. 25(1), 21–29 (2011).
20 Gerstenblith A. The Wills Eye Manual (6th Edition). Lippincott Williams and Wilkins, PA, USA (2012).
•• Thecomprehensivetextprovidesfocusedoverviewofthemostimportantandcommonlyencounteredeyeproblemsineachsubspecialty.Itservesnotonlyasadiagnosticmanual,butalsoasatreatmentreference.
21 Watson AP. Treatment of chalazions with injection of a steroid suspension. Br. J. Ophthalmol. 68(11), 833–835 (1984).
ConclusionPain thought to be of ocular or periocular pain origin represents a challenge for the clinician in both diagnosis and treatment. Familiarity with the more common pathologic processes that cause ocular and periocular pain allows the clinician to more readily identify those diseases that present a risk to vision and allows more immediate ophthalmologic referral. The ability to identify the unique clinical features of the common causes of eye pain can help the clinician narrow down the rather large differential that is of ocular pain.
Future perspectiveWhile the basic principles of diagnosing and managing the common eye problems discussed in this section, some aspects in the management of these conditions may evolve in the future. As our understanding of the molecular basis of disease continues to evolve, perhaps fewer of these conditions, such as uveitis or optic
neuritis, will be simply diagnosed as idiopathic and a cellular or genetic cause may be elucidated. As high resolution imaging continues to evolve, perhaps our diagnosis and understanding of con-ditions such as cavernous sinus thrombosis and optic neuritis will improve. However, despite the exciting advances that await us in our future medical practice, it is likely that such advances will not replace a through history and physical exam in the diagnosis and management of these common and important causes of eye pain.
Financial & competing interests disclosureThe authors have no relevant affiliations or financial involvement with any organization or entity with a finan-cial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.

425
A practical approach to ocular pain for the non-ophthalmologist REviEW
future science group www.futuremedicine.com
22 Martin-Doyle JLC. Diseases of the eyelids. In: A Synopsis of Ophthalmology. Martin-Doyle JLC (Ed.). Elsevier, PA, USA, 25–42 (2013).
23 Russo D, Tran J, Louie M et al. Is this a masquerading carcinoma? When a Chalazion is just a Chalazion. Optometry 82(6), 382–383 (2011).
24 Liu IT, Kao SC, Wang AG et al. Preseptal and orbital cellulitis: a 10-year review of hospitalized patients. J. Chin. Med. Assoc. 69(9), 415–422 (2006).
25 Barza M, Baum J. Ocular infections. Med. Clin. North Am. 67(1), 407 (1983).
26 Hauser A, Fagarasi S. Periorbital and orbital cellulitis. Pediatr. Rev. 31(6), 242–249 (2010).
27 Atlas of Clinical Ophthalmology (3rd Edition). Spalton DJ. (Ed.). Elsevier Inc. PA, USA, (2005).
• Providesnumeroushigh-resolutioncolorphotographsofdiseasespertainingtoallsubspecialtiesofophthalmology,aswellasdiscussionsofeachentity,thuseachtopicdiscussedherewaswellrepresented.
28 Horner ME, Abramson AK, Warren RB et al. The spectrum of oculocutaneous disease: Part I. Infectious, inflammatory, and genetic causes of oculocutaneous disease. J. Am. Acad. Dermatol. 70(5), 795e1-705e25 (2014).
29 Yanoff M, Sassani JW. Cornea and Sclera. In: Ocular Pathology (Seventh Edition). Myron Yanoff (Ed.). Elsevier Inc. PA, USA, 227–297 (2015).
30 Bawazeer AM, Raffa LH. Adalimumab in the treatment of recurrent idiopathic bilateral nodular scleritis. Oman J. Ophthalmol. 4(3), 139–141 (2011).
31 Deibel JP, Cowling K. Ocular inflammation and infection. Emerg. Med. Clin. North Am. 31(2), 387–397 (2013).
32 Barankin B, Guenther L. Rosacea and atopic dermatitis: two common oculocutaneous disorders. Can. Fam. Physician. 48, 721–724 (2002).
33 Martin-Doyle JLC. Diseases of the Sclera. In: A Synopsis of Ophthalmology. Martin-Doyle JLC (Ed.). Elsevier Inc. PA, USA, 90–92 (2013).
34 Galor A, Thorne JE. Scleritis and peripheral ulcerative keratitis. Rheum. Dis. Clin. North Am. 33(4), 835–854 (2007).
35 Smith JR, Mackensen F, Rosenbaum RT. Therapy insight: scleritis and its relationship to systemic autoimmune disease. Nat. Clin. Pract. Rheumatol. 3(4), 219–226 (2007).
36 Waldman SD. Acute herpes zoster and post herpetic neuralgia. Intern. Med. 11, 33–37 (1990).
37 Yawn BP, Wollan PC, Sauver JL et al. Herpes zoster eye complications: rates and trends. Mayo Clin. Proc. 88(6), 562–570 (2013).
38 Carter III WP, Germann CA, Baumann M. Ophthalmic diagnoses in the ED: herpes zoster ophthalmicus. Am. J. Emerg. Med. 26(5), 612–617 (2008).
39 Patel LM, Lambert PJ, Gagna CE, Maghari A et al. Cutaneous signs of systemic disease. Clin. Dermatol. 29(5), 511–522 (2011).
40 O’Conner KO, Paauw DS. Herpes zoster. Med. Clin. North Am. 97(4), 503–522 (2013).
41 Wakil SM, Ajlan R, Arthurs B. Herpes zoster ophthalmicus complicated by ipsilateral isolated bell’s palsy: a case report and review of the literature. Can. J. Ophthalmol. 47(4), 339–343 (2012).
42 Mitchell JD. Ocular Emergencies. In: Emergency Medicine: A Comprehensive Study Guide (Edition 5). Tintinalli E (Ed.). McGraw Hill, NY, USA, 1501–1517 (2000).
43 See JLS, D’Aquino MC, Aduan J et al. Management of angle closure glaucoma. Indian J. Ophthalmol. 59(Suppl. 1), S82–S87 (2011).
44 Choong YF, Irfan S, Menage MJ. Acute angle closure glaucoma: an evaluation of a protocol for acute treatment. Eye (London) 13(5), 613 (1999).
45 Sihota R. An Indian perspective on primary angle closure and glaucoma. Indian J. Ophthalmol. 59(Suppl. 1), S76-S81 (2011).
46 Sihota R, Lakshmaiah NC, Agarwal HC, Pandey RM, Titiyal JS. Ocular parameters in the subgroups of angle closure glaucoma. Clin. Exp. Ophthalmol. 28(4), 253–8 (2000).
47 Sihota R, Saxena R, Gogoi M, Sood A, Gulati V, Pandey RM. A comparison of the circadian rhythm of intraocular pressure in primary chronic angle closure glaucoma, primary open angle glaucoma and normal eyes. Indian J. Ophthalmol. 53(4), 243–247 (2005).
48 Cumba RJ, Nagi KS, Bell NP et al. Clinical outcomes of peripheral iridotomy in patients with the spectrum of chronic primary angle closure. ISRN Ophthalmol. 828972 (2013).
49 Nussenblatt R, Whitcup S, Palestine A. Uveitis: Fundamentals of Clinical Practicel. Mosby, MO, USA (1996).
50 Tessler H. Classification and symptoms and signs of uveitis. In: Clinical Ophthalmology. Duane T (Ed.). Harper & Row, NY, USA, 1–10 (1987).
51 Nishimoto JY. Iritis: how to recognize and manage a potentially sight-threatening disease. Postgrad. Med. 99(2), 255 (1996).
52 Buttaravoli P, Leffler SM. Acute uveitis. In: Minor Emergencies: Expert Consult (Third Edition). Buttaravoli P, Leffler SM (Ed.). Elsevier, PA, USA, 81–84 (2012).
53 Pepose JS, Holland GN, Wilhelmus KR. Ocular Infection and Immunity. (Ed.). Mosby, MO, USA (1996).
54 Rathinam SR, Babu M. Algorithmic approach in the diagnosis of uveitis. Indian J. Ophthalmol. 61(6), 255–262 (2013).
55 Lee O. Idiopathic and other anterior uveitis syndromes. In: Ophthalmology (4th Edition). Yanoff M, Duker J (Eds). Elsevier, China, 770–773 (2014).
• Thistextbookprovidesadetailedandcomprehensiveoverviewofophthalmology,thusincludinganindepthdiscussionofeachofthetopicsdiscussedinthebodyofthischapter.
56 Kernt M, Kampik A. Endophthalmitis: pathogenesis, clinical presentation, management, and perspectives. Clin. Ophthalmol. 4, 1–15 (2010).
57 Callegan MC, Englebert M, Parke DW. Bacterial endophthalmitis: Epidemiology, therapeutics, and bacterium-host interactions. Clin. Microbiol. Rev. 15(1), 111–124 (2002).
58 Safneck J. Endophthalmitis: a review of recent trends. Saudi J. Ophthalmol. 26(2), 181–189 (2002).
59 Merkur AB, Hodge WG. Rhodotorula rubra endophthalmitis in an HIV positive patient. Br. J. Ophthalmol. 86(12), 1444–1445 (2002).
60 Nishimoto JY. Iritis: how to recognize and manage a potentially sight-threatening disease. Postgrad. Med. 99(2), 255 (1996).
61 Yanoff M, Sassani JW. Nongranulomatous inflammation: uveitis, endophthalmitis, panophthalmitis, and sequelae. In: Ocular Pathology (7th Edition). Yanoff M, Sassani J (Eds). Elsevier Saunders, PA, USA, 53–66 (2015).
62 Connell PP, O’Neill EC, Fabinyi D et al. Endogenous endophthalmitis: 10-year experience at a tertiary referral centre. Eye (London) 25(1), 66–72 (2011).
63 Zhang YQ1, Wang WJ. Treatment outcomes after pars planavitrectomy for endogenous endophthalmitis. Retina 25(6), 746–750 (2005).
64 Ghezzi A, Martinelli V, Rodegher M et al. The prognosis of idiopathic optic neuritis. Neurol. Sci. 21(4 Suppl. 2), S865 (2000).

Pain Manag. (2014) 4(6)426
REviEW Waldman, Waldman & Waldman
future science group
65 Pau D, Al Zubidi N, Yalamanchili S et al. Optic neuritis. Eye (Lond.) 25(7), 833–842 (2011).
66 Jacobs D, Guercio J. Inflammatory optic neuropathies and neuroretinitis. In: Ophthalmology (4th Edition). Yanoff M, Duker J (Eds). Elsevier, China, 879–883 (2014).
67 Dooley MC, Foroozan R. Optic neuritis. J. Ophthalmic Vis. Res. 5(3), 182–187 (2010).
68 Miller DH, Newton MR, Van der Poel JC et al. Magnetic resonance imaging of the optic nerve in optic neuritis. Neurology 38(2), 175 (1988).
69 Atkins EJ, Drews-Botsch CD, Newman NJ et al. Management of optic neuritis in Canada: survey of ophthalmologists and neurologists. Can. J. Neurol. Sci. 35(2), 179–184 (2008).
70 Yanoff M, Sassani JW. Surgical and non-surgical trauma. In: Ocular Pathology (7th Edition). Yanoff M, Sassani JW (Eds). Elsevier Saunders, PA, USA, 93–145 (2015).
71 Vassallo S, Hartstein M, Howard D et al. Traumaticretrobulbar hemorrhage: emergent decompression by lateral canthotomy and cantholysis. J. Emerg. Med. 22(3), 251–26 (2002).
72 Lang SJ, Lagrèze WA. Spontaneous intraorbital haemorrhage. Klin. Monbl. Augenheilkd. 230(9), 937–938 (2013).
73 McNab AA. Nontraumaticorbital hemorrhage. Surv. Ophthalmol. 59(2), 166–184 (2014).
74 Thomas JE, Yoss RE. The parasellar syndrome: problems in determining etiology. Mayo Clin. Proc. 45(9), 617 (1970).
75 Desa V, Green R. Cavernous sinus thrombosis: current therapy. J. Oral Maxillofac. Surg. 70(9), 2085–2091 (2012).
76 Colbert S, Cameron M, Williams J. Septic thrombosis of the cavernous sinus and dental infection. Br. J. Oral Maxillofac. Surg. 49(6), e25-e26 (2011).
77 Barahimi B, Murchison AP, Bilyk JR. Forget me not. Surv. Ophthalmol. 55(5), 467–480 (2010).
78 Cohn DF, Carasso R, Streifler M. Painful ophthalmoplegia: the Tolosa-Hunt syndrome. Eur. Neurol. 18(6), 373 (1979).
79 Roca PD. Painful ophthalmoplegia: the Tolosa-Hunt syndrome. Ann. Ophthalmol. 71(5), 828 (1975).
80 Anagnostou E, Kouzi I, Kararizou E. Painful ophthalmoplegia: the role of imaging and steroid response in the acute and subacute
setting. J. Neurol. Sci. 331(1–2), 145–149 (2013).
81 Zhang X, Zhang W, Liu R et al. Factors that influence Tolosa-Hunt syndrome and the short-term response to steroid pulse treatment. J. Neurol. Sci. 341(1–2), 13–16 (2014).
82 Yousem DM, Atlas SW, Grossman RI et al. MR imaging of Tolosa-Hunt syndrome. AJR Am. J. Neuroradiol. 10(6), 154–167 (1990).
83 Troost BT. Comprehensive and infiltrative optic neuropathies. In: Walsh & Hoyt’s Clinical Neuro-Ophthalmology. Miller NR, Newman NJ (Eds). Lippincott Williams & Wilkins, PA, USA, 1727–1729 (2008).
84 Feoktistov A, Diamond M. Diagnosing and understanding adult headache. Otolaryngol. Clin. North Am. 47(2), 175–185 (2014).
85 Waldman SD. Cluster headache. In: Common Pain Syndromes. Waldman SD (Ed.). Saunders, PA, USA, 14–16 (2008).
86 Waldman SD. Sphenopalatine ganglion block. In: Atlas of Interventional Pain Management. Waldman SD (Ed.). Saunders Elsevier, PA, USA 12–14 (2009).